
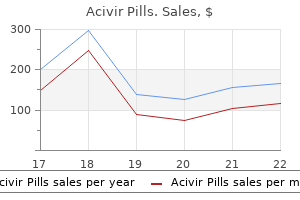
Cheap acivir pills 200 mg on-line
Carrier detection tests are available for many hematologic recessive diseases hiv infection rates us 2012 purchase acivir pills 200 mg on line, including sickle cell disease, - and thalassemia, Gaucher disease, and hemochromatosis. Incomplete penetrance means that individuals who have the disease-causing genotype may not exhibit the disease phenotype at all even though the genotype and the associated disease may be transmitted to the next generation. For example, the penetrance of hemochromatosis, an autosomal recessive condition, increases with age as iron accumulates in organs such as the heart and liver (Chap. If the expressivity of a disease is variable, penetrance may be Page 9 / 20, Lynn B. For example, Countway Medical Library the penetrance of hemochromatosis, an autosomal recessive condition, increases with age as iron accumulates in organs such as the heart and liver Access Provided by: (Chap. The penetrance of the hemochromatosis genotype is higher in males than females because females deplete their iron supplies by menstruation and lactation. If the expressivity of a disease is variable, penetrance may be complete, but the severity of the disease can vary greatly. Many hematologic conditions, including sickle cell disease and -thalassemia, have variable expressivity. Only a few diseases are known to be inherited as X-linked dominant or Y chromosome traits, so only the more common X-linked recessive diseases are discussed here. Because females receive two X chromosomes, one from the father and one from the mother, they can be homozygous for a disease allele at a given locus, homozygous for the normal allele at the locus, or heterozygous. If a male inherits a recessive disease gene on the X chromosome, he will be affected by the disease because the Y chromosome does not carry a normal allele to counteract the effects of the disease gene. Because a single copy of an X-linked recessive gene will cause disease in a male but two copies are required for disease expression in females, more males are affected by X-linked recessive diseases than are females. The inactivated X chromosomes are observable in many interphase cells as highly condensed intranuclear chromatin bodies, termed Barr bodies (after Barr and Bertram, who discovered them in the late 1940s). Normal females have one Barr body in each somatic cell, whereas normal males have no Barr bodies. At some time early in embryogenesis, one X in each cell is inactivated at random and condenses to form the Barr body. The active X remains active not only for the lifetime of that cell but for the lifetime of all of its progeny. At some Countway Medical Library time early in embryogenesis, one X in each cell is inactivated at random and condenses to form the Barr body. In some cells, the inactivated X chromosome is the one contributed by the father; in other cells, it is the one contributed by the mother. Some individuals do not have the normal number of X chromosomes in their somatic cells. For example, males with Klinefelter syndrome typically have two X chromosomes and one Y chromosome. Females whose cell nuclei have three X chromosomes have two Barr bodies in each cell, and females whose cell nuclei have four X chromosomes have three Barr bodies in each cell. Thus, the number of Barr bodies is always one less than the number of X chromosomes in the cell. Persons with abnormal numbers of X chromosomes, such as those with Turner syndrome or Klinefelter syndrome, are not physically normal. This situation presents a puzzle because they presumably have only one active X chromosome, just as individuals with normal numbers of chromosomes do. However, the distal tips of the short and long arms of the X chromosome, as well as several other regions on the chromosome arm, are not inactivated (~15% of the genes on the X chromosome), resulting in excess or deficient gene products and a disease phenotype for these individuals. Inactive X chromosomes can be at least partially reactivated in vitro by administering 5-azacytidine, a demethylating agent. Characteristics of Pedigrees X-linked pedigrees show distinctive modes of inheritance. To express an X-linked recessive trait, a female must be homozygous: Either both her parents are affected, or her father is affected and her mother is a carrier. Access Provided by: the following are important principles of X-linked recessive inheritance: 1. The gene can be transmitted through a series of carrier females, causing the appearance of one or more "skipped generations. The gene is passed from an affected father to all his daughters, who, as phenotypically normal carriers, transmit it to approximately half their sons, who are affected. Recurrence Risks the most common mating type involving X-linked recessive genes is the combination of a carrier female and a normal male. On average, the carrier mother will transmit the disease-causing allele to half her sons (who are affected) and half her daughters (who are carriers). In this situation, all the sons must be normal because the father can transmit only his Y chromosome to them. Because the sons must receive the Y chromosome and the daughters must receive the X chromosome with the disease gene, these are precise outcomes and not probabilities. When the mode of genetic transmission is clear, the diagnostic alternatives can be narrowed considerably. Careful analysis of the family history not only will make possible more appropriate genetic counseling to the patient and family but also will shorten the road to a correct diagnosis. The location and identification of a gene can tell much about the function of the gene, its interaction with other genes, and the likelihood that certain individuals will develop a genetic disease. This law is only partly true, however, because genes located close together on the same chromosome do tend to be transmitted together to the offspring. Alleles A and B are located together on one member of a chromosome pair, and alleles a and b are located on the other member. The analysis of recombination in families is used to determine the locations of disease-causing genes. Consequently, many thousands of individuals have now been sequenced, and the genes responsible for more than 5000 Mendelian conditions have been identified. The classical method by which this is achieved, cloning, is a central technique of molecular biology. An adequate genomic library consists of millions of fragments of the genetic material of a cell that have been ligated (inserted) into a suitable vector. In contrast, a genomic library represents all of the genetic material, coding and noncoding, transcribed and nontranscribed. Much smaller inserts, ranging in size from approximately 3000 to 12,000 bp, can be cloned into bacteriophages. The mixture of nucleotides used contains a nucleotide analogue that results in chain termination when incorporated. Gel electrophoresis of the labeled products produces "ladders" of polynucleotides. The size of each fragment depends on the point at which there exists a nucleotide corresponding to the chain terminating analogue in the mixture. Sequencing can be done rapidly and accurately by automated methods in which the elongation of the strand is terminated by a fluorescent nucleotide and electrophoresis is carried out in capillary tubes rather than slab gels. Similar to the Sanger sequencing process described previously, new complementary bases (to which a base-specific fluorescent label is attached) are added one at a time. The fluorescent signal from each cluster is recorded by a camera, revealing the base-pair sequence of each fragment. In addition, third-generation methods typically yield much longer sequencing reads (>10 kb), which facilitates analysis of large or repetitive structural variants that pose difficulties for short-read technology.
Syndromes
- Bruising
- Pain from teeth and gums
- Collapsed neck veins
- The yawning is associated with excessive daytime sleepiness.
- The symptoms may affect one arm or leg, one side of the body, both legs, or both arms and legs
- Inflammatory bowel disease (IBD)
- Gout medicines
- Blood culture for bacteria infection (E. coli sepsis)
- Parkinson disease
Purchase 200mg acivir pills
Aplastic anemia during pregnancy: a review of obstetrics and anesthetic considerations hiv infection nail salon generic acivir pills 200 mg mastercard. Aplastic anemia: report of a case with recurrent episodes in consecutive pregnancies. Outcome of pregnancy and disease course among women with aplastic anemia treated with immunosuppression. Long term mortality after a single treatment course with x-rays in patients treated with ankylosing spondylitis. The occurrence of malignancy in radioactive persons: a general review of data gathered in the study of the radium dial painters, with special reference to the occurrence of osteogeneic sarcoma and the inter-relationship of certain blood diseases. Consequences of irradiation on bone and marrow phenotypes and its relationship to disruption of hematopoietic precursors. Plasma levels and production of soluble stem cell factor by marrow stromal cells in patients with aplastic anaemia. Plasma/serum levels of flt3 ligand are low in normal individuals and highly elevated in patients with Fanconi anemia and acquired aplastic anemia. Measurement of endogenous plasma granulocyte colony-stimulating factor in patients with acquired aplastic anemia by a sensitive chemiluminescent immunoassay. Human mesenchymal stem cells are not of donor origin in patients with severe aplastic anemia who underwent sex-mismatched allogeneic bone marrow transplant. Clonal cytogenetic abnormalities in patients with otherwise typical aplastic anemia. Evidence for clonal disease by magnetic resonance imaging in patients with hypoplastic marrow disorders. Somatic mutations identify a subgroup of aplastic anemia patients who progress to myelodysplastic syndrome. A pathogenetic link between aplastic anemia and paroxysmal nocturnal hemoglobinuria is suggested by a high frequency of aplastic anemia patients with a deficiency of phosphatidylinositol glycan anchored proteins. Genetic lesions in a preleukemic aplasia phase in a child with acute lymphoblastic leukemia. Three cases of typical aplastic anaemia associated with a Philadelphia chromosome. Paroxysmal nocturnal hemoglobinuria clones in severe aplastic anemia patients treated with horse anti-thymocyte globulin plus cyclosporine. Cyclophosphamide and antithymocyte globulin to condition patients with aplastic anemia for allogeneic marrow transplantation: the experience in four centers. Reducing the iron burden and improving survival in transfusion-dependent thalassemia patients: current perspectives. A restrictive platelet transfusion policy allowing long-term support of outpatients with severe aplastic anemia. Granulocyte concentrates: prolonged functional capacity during storage in the presence of phenotypic 159. Granulocyte concentrates: prolonged functional capacity during storage in the presence of phenotypic changes. Bone marrow transplantation for severe aplastic anemia: a randomized controlled study of conditioning regimens. Allogeneic stem cell transplantation using alemtuzumab-containing regimens in severe aplastic anemia. Alemtuzumab based reduced intensity transplantation for pediatric severe aplastic anemia. Recent improvement in outcome of unrelated donor transplantation for aplastic anemia. Peffault de Latour R, Chevret S, Jubert C, et al; Francophone Society of Bone Marrow Transplantation and Cellular Therapy. Unrelated cord blood transplantation in patients with idiopathic refractory severe aplastic anemia: a nationwide phase 2 study. Cathepsin-B-dependent apoptosis triggered by antithymocyte globulins: a novel mechanism of T-cell depletion. Action of antithymocyte globulin on normal human erythroid progenitor cell proliferation in vitro: erythropoietic growth-enhancing factors are released from marrow accessory cells. Immunostimulatory effects of different antilymphocyte globulin preparations: a possible clue to their clinical effect. Action of antithymocyte globulin on normal human erythroid progenitor cellCountway Medical Library proliferation in vitro: erythropoietic growth-enhancing factors are released from marrow accessory cells. Comparison between horse and rabbit antithymocyte globulin as first-line treatment for patients with severe aplastic anemia: a single-center retrospective study. Rabbit-antithymocyte globulin combined with cyclosporine A as a first-line therapy: improved, effective and safe for children with acquired severe aplastic anemia. The efficacy of rabbit antithymocyte globulin with cyclosporine in comparison to horse antithymocyte globulin as a first-line treatment in adult patients with severe aplastic anemia: a single-center retrospective study. Antithymocyte globulin treatment in patients with aplastic anemia: a prospective randomized trial. A multicenter trial of antithymocyte globulin in aplastic anemia and related diseases. Primary treatment of acquired aplastic anemia: outcomes with bone marrow transplantation and immunosuppressive therapy. Primary treatment of acquired aplastic anemia: outcomes with bone marrow transplantation Countway Medical Library and immunosuppressive therapy. Long-term follow-up of severe aplastic anaemia patients treated with antithymocyte globulin. Short telomeres result in chromosomal instability in hematopoietic cells and precede malignant evolution in human aplastic anemia. Oral cyclosporin-A is effective treatment for untreated and also for previously immunosuppressed patients with severe bone marrow failure. Treatment of pure red-cell aplasia and aplastic anaemia with cyclosporin: long-term clinical effects. Effectiveness of low dose cyclosporine in acquired aplastic anaemia with severe neutropenia. Cyclosporine therapy of aplastic anaemia, congenital and acquired red-cell aplasia. Interferon-g gene expression in unstimulated bone marrow mononuclear cells predicts a good response to cyclosporine therapy in aplastic anemia. Cyclosporine and recombinant granulocyte colony-stimulating factor in severe aplastic anemia [letter]. The successful treatment of two cases of severe aplastic anaemia with granulocyte colony-stimulating factor and cyclosporine A [case report]. Antithymocyte globulin and cyclosporine for severe aplastic anemia: association between hematologic response and long-term outcome. Multicenter randomized study comparing cyclosporine-A alone and antithymocyte globulin with prednisone for treatment of severe aplastic anemia. Antithymocyte globulin and cyclosporine for treatment of 44 children with hepatitis associated aplastic49 / 58 Page, George B. Multicenter randomized study comparing cyclosporine-A alone and antithymocyte globulin Countway Medical Library with prednisone for treatment of severe aplastic anemia. Antithymocyte globulin and cyclosporine for treatment of 44 children with hepatitis associated aplastic anemia. Eltrombopag restores tri-lineage hematopoiesis in refractory severe aplastic anemia which can be sustained on discontinuation of drug.
Discount acivir pills 200mg fast delivery
Dose adjustment may be necessary for patients who have more than grade 3 hematologic or nonhematologic toxicity antiviral bath cheap acivir pills 200 mg visa. Almost half of the patients with ibrutinib experience diarrhea, and approximately one-third of patients develop upper respiratory tract infections, cough, or fatigue. Other adverse effects include nausea, vomiting, constipation, pyrexia, rashes, edema, hypertension, atrial fibrillation, bleeding, and headaches. One case of grade 2 atrial fibrillation and 1 case of grade 3 subcutaneous hemorrhage were reported. The apoptosis pathway activity reflects a balance between proapoptotic and antiapoptotic proteins. Antifungal drugs (posaconazole and voriconazole) strongly inhibit its clearance and necessitate a 75% reduction in dose. Effects on the microenvironment may be an important additional mechanism of action. Copanlisib and umbralisib have shown activity in non-Hodgkin lymphoma and continue in development. No dose adjustments are required for renal impairment, but copanlisib may require dose adjustment for liver dysfunction. As of this writing, umbralisib has a milder side-effect profile, the most common side effects being diarrhea, nausea, fatigue, headache, cough, and appetite loss, but no reported colitis or pneumonitis. The most common grade 3 or 4 adverse events are neutropenia, febrile neutropenia, and diarrhea. Development of monoclonal antibodies against specific targets has been largely accomplished by the empiric method of immunizing mice against human tumor cells and screening the hybridomas for antibodies of interest. Because murine antibodies have a short half-life and induce a human antimouse antibody immune response, antibodies must be partially or fully humanized for clinical use. Infusions are started at 50 mg/h, and in the absence 50 mg/h increments every 30 minutes to a maximum rate of 400 mg/h. Given the risk of infusional reactions, pretreatment with antihistamines, acetaminophen, and glucocorticoids is standard. During the first administration, the rate must be increased slowly to prevent infusional reactions. Infusions are started at 50 mg/h, and in the absence of infusion reactions the rate can be increased in 50 mg/h increments every 30 minutes to a maximum rate of 400 mg/h. On subsequent infusion in the absence of reactions, infusions may start at 100 mg/h and may be increased in 100 mg/h increments every 30 minutes to a maximum rate of 400 mg/h. Patients with a high degree of circulating tumor cells are at increased risk for tumor lysis syndrome and are given a reduced dose of 50 mg/m2 on day 1 of treatment in addition to standard tumor lysis prophylaxis. Most reactions are mild and include fever, chills, throat itching, urticaria, and mild hypotension, all of which can respond to decreased infusion rates and antihistamines. Severe mucocutaneous skin reactions, including Stevens-Johnson syndrome, have been reported. Concurrent hepatitis B therapy may be indicated for patients with prior hepatitis B infection. The overall response rate was 58%, with a median progression-free survival of approximately 14 months. The most common adverse events (>10% of patients) are severe infusion reactions, for which premedication with acetaminophen and antihistamines is advised, as well as neutropenia, pneumonia, pyrexia, cough, diarrhea, anemia, fatigue, dyspnea, rash, nausea, bronchitis, and upper respiratory tract infections. Rarely, it induces multifocal leukoencephalopathy and tumor lysis in patients with more than 25,000 leukocytes/mL. Prophylaxis with antihyperuricemics and hydration should be considered prior to infusion of the antibody. Other common toxicities increased risk of grade 3 neutropenia (33% vs 28%) compared to rituximab, but no increased risk of include anemia, thrombocytopenia, and leukopenia. Obinutuzumab is then infused at the rate of 50 mg/h, escalating in increments of 50 mg/h every 30 minutes to a maximum of 400 mg/h. Thereafter patients receive 1000 mg every 2 months for up to 2 years as maintenance therapy. There is an increased risk of grade 3 neutropenia (33% vs 28%) compared to rituximab, but no increased risk of infection (12% vs 14%). Treatment with venetoclax was given for 12 cycles, and obinutuzumab was given for the first 6 cycles. Venetoclax was given over a 5-week ramp-up period beginning at cycle 1 day 22 to reduce the risk of tumor lysis syndrome. Reactivation of hepatitis B viral infection and progressive multifocal leukoencephalopathy are known to occur during and after obinutuzumab treatment. Opportunistic infections and various autoimmune reactions (including idiopathic thrombocytopenic purpura and glomerulonephritis), stroke, an increased risk of malignancies, and serious infusion reactions limit its use. Serious infections with cytomegalovirus are seen and viral monitoring during treatment is recommended. The use of brentuximab vedotin was associated with an improved median progression-free survival of 48. The main toxicity is cumulative peripheral neuropathy reported in up to 67% of the patients in the above trials, and likely attributable to release of the release of monomethylauristatin E into the systemic circulation. Patients experiencing new or worsening peripheral neuropathy may require a delay, dose reduction, or discontinuation of brentuximab vedotin. Other common toxicities include infusion reactions (requiring prophylactic premedication), neutropenia, thrombocytopenia, fatigue, and nausea. Two-year survival was 23%, with inotuzumab ozogamicin versus 10% for investigator choice. Treatment with inotuzumab ozogamicin can be associated with cytopenias (particularly thrombocytopenia) and transaminitis. To limit infusion reactions, premedication with a glucocorticoid, antipyretic, and antihistamine is recommended. During treatment with inotuzumab ozogamicin, prophylactic use of ursodiol, a bilePage 49 / 82 acid, is, Bruce A. Richardson recommended, as well as close monitoring of patient weight and assessment of liver function before and after each dose of inotuzumab ozogamicin. Two-year survival was 23%, with inotuzumab ozogamicin versus Countway Medical Library 10% for investigator choice. Access Provided by: Treatment with inotuzumab ozogamicin can be associated with cytopenias (particularly thrombocytopenia) and transaminitis. During treatment with inotuzumab ozogamicin, prophylactic use of ursodiol, a bile acid, is recommended, as well as close monitoring of patient weight and assessment of liver function before and after each dose of inotuzumab ozogamicin. Like other bispecific T-cell engager agents, blinatumomab has a short half-life (2 hours), and requires 24-hour continuous intravenous infusion throughout its 4-week cycle of administration. The unique toxic events seen with blinatumomab in clinical trials were neurologic events (including tremors, dizziness, confusion, convulsions, and ataxia), cytokine release syndrome, infections, infusion reactions, and neutropenia. Additionally, it is strongly recommended that patients be hospitalized for at least the first 9 days of the induction cycle and the first 2 days of the following cycles. Thereafter, close monitoring for neurologic and cytokine release syndrome symptoms in clinic are still important. Infusion should be held for grade 3 or higher cytokine release syndrome symptoms, and permanently discontinued after onset of any grade 4 cytokine release syndrome. Infusion should be held for grade 3 or higher neurologic events, and permanently discontinued for grade 4 neurotoxicity or more than 1 convulsive event.
Purchase acivir pills from india
Examples of apoptosis of 2 neutrophils in normal anticoagulated blood during standing at room temperature hiv infection kidney disease cheap acivir pills 200 mg visa. Note also the 2 macrothrombocytes (the size of red cells) characteristic of this disorder (Chap. A strand of endothelial cells derived from vascular tissue caught on the biopsy needle. The nucleus is lobulated, with two to four lobes connected by a thin chromatin thread. The defining feature of the mature neutrophil is the round lobes with condensed chromatin, because the chromatin thread may overlie the nucleus and not be visible. The nucleus of 1% to 16% of the neutrophils from females may have an appendage that is shaped like a drumstick and is attached to one lobe by a strand of chromatin. The cytoplasm is diffusely pale pink and contains many small, tan to pink granules distributed evenly throughout the cell. The chromatin pattern is the same as that of the neutrophil, but the nucleus tends to be more lightly stained. The differentiating characteristic of these cells is the presence of many refractile, orange-red granules that are distributed evenly throughout the cell and may be visible overlying the nucleus. These granules are larger than those in the neutrophil and are more uniform in size. Occasionally, some of the granules in eosinophils stain light blue rather than orange-red. The nucleus may stain more faintly and usually is less segmented and has less distinct chromatin condensation than is the case in neutrophils. The large deeply basophilic granules of basophils are fewer in number and less regular in size and shape than in the eosinophil. In the large lymphocytes, the nuclear-to-cytoplasmic ratio is lower and the chromatin is slightly less condensed than in the small lymphocytes. Basophils are similar to the other polymorphonuclear cells and are slightly smaller than neutrophils (Chap. The nucleus may stain more faintly and Countway Medical Library usually is less segmented and has less distinct chromatin condensation than is the case in neutrophils. The large deeply basophilic granules of Access Provided by: basophils are fewer in number and less regular in size and shape than in the eosinophil. The granules are visible overlying the nucleus and, in some cells, almost completely obscure the lightly stained nuclear chromatin. The small lymphocyte, the predominant type in normal blood, is round and contains a relatively large, round, densely stained nucleus (Chap. Reactive lymphocytes, as seen in viral infections caused by Epstein-Barr virus, cytomegalovirus, adenovirus, or other organisms, are large with indented nuclei and abundant blue cytoplasm (Chap. A low nuclear-to-cytoplasmic ratio and greater degree of chromatin condensation distinguishes reactive lymphocytes from neoplastic cells. The nucleus is of various shapes- round, kidney, oval, or lobular-and frequently appears to be folded (Chap. The cytoplasm is light gray, contains variable numbers of fine lilac or purple granules, and is often vacuolated. The monocyte nuclear chromatin contains a fine, string-like structure as opposed to the smudgy-appearing clumps of the lymphoid chromatin. Nuclear shape and cytoplasmic vacuolization are less reliable for distinguishing features between monocytic and lymphoid cells. These granules if unusually prominent can be confused with the larger granules of basophils. Auer rods are sharply outlined, red-staining rods found in the cytoplasm in blast cells, and occasionally in more mature leukemic cells, in the blood of some patients with acute myeloid leukemia or myelodysplastic syndromes (Chaps. These bodies are thought to be a reflection of accelerated maturation of neutrophils with residual endoplasmic reticulum from the promyelocyte stage. Eosinophils and basophils often are partially or largely degranulated in preparation of the blood film with the granules scattered beside the cell. These cells en face may simulate the appearance of abnormal cells and may be misinterpreted as blasts or metastatic tumor cells. There is no specific association with disease other than chronic lymphocytic leukemia (Chap. Eosinophils and basophils often are partially or largely degranulated in preparation of Access Provided by: the blood film with the granules scattered beside the cell. Aspiration is always attempted because of the superior morphology offered by examination of the aspirate smear. However, a marrow biopsy is essential for quantifying marrow cellularity, diagnosing myeloproliferative neoplasms and other disorders associated with reticulin fibrosis, evaluating lymphoid neoplasms that may not be well-represented in the aspirate, and diagnosing infiltrative diseases of the marrow. Marrow necrosis, amyloid, and gelatinous transformation are more readily detected in marrow sections than in aspirate films. Morphology of marrow cells is still the gold standard for diagnosis of hematologic malignancy and allows construction of a good differential diagnosis for nonmalignant disorders. The International Council for Standardization in Hematology has published guidelines for standardization of marrow immunohistochemistry. However, flow cytometry requires that cells be viable and dissociated from tissue. Nevertheless, many molecular assays may be performed on formalin-fixed, paraffin-embedded tissue as long the tissue has not been decalcified with hydrochloric acid. Fat cells begin to replace hemopoietic marrow in the extremities in the fifth to seventh year. By adulthood, the hemopoietic marrow is limited to the axial skeleton and the proximal portions of the extremities (Chaps. Red marrow contains fat, however, and fat droplets are visible grossly in aspirated marrow specimens. Histologically, yellow marrow consists almost entirely of fat cells and supporting connective tissue. Red marrow contains an abundance of hematopoietic cells, fat cells, and connective tissue. Marrow is soft and friable and can be readily aspirated or biopsied with a needle. The anteromedial surface of the tibia is an option for infants younger than 1 year old (particularly newborns), but the posterior iliac crest is still the preferred site. Serious adverse outcomes after marrow aspiration or biopsy are rare, occurring in less than 0. One direct fatality and 3 episodes of prolonged but not permanent disability were reported in nearly 55,000 marrow biopsies. To prevent this, a guard should be in place on the needle if a sternal aspirate is required. The anterior iliac crest is less preferred than the posterior crest in adults because of its thick cortical bone. The anteromedial surface of the tibia is an option for infants younger than 1 year old (particularly newborns), but the Countway Medical Library posterior iliac crest is still the preferred site. Serious adverse outcomes after marrow aspiration or biopsy are rare, occurringAccess Provided by: in less than 0. Midazolam (Versed) is a popular choice for conscious sedation of adult patients, although a variety of other premedications have been used.

200mg acivir pills
These proteins are responsible for leukocyte rolling over endothelial surfaces and tethering antiviral y antibiotico cheap acivir pills 200 mg, thereby allowing integrin-mediated firm adhesion to the endothelium and mediating cellular homing events using specialized high endothelial venule lymphocyte homing sites. A sequence of specific events by which leukocytes adhere to and migrate through the endothelium begins with tethering of the leukocytes to the luminal surface of the endothelial cells. The rolling leukocytes also receive signals through surface G-protein-coupled receptors that bind chemokines in the heparan sulfate proteoglycans on the endothelial cells. The adherent leukocytes undergo a rapid diapedesis, with migration either through or between the endothelial cells into the abluminal interstitium. When leukocytes follow a paracellular route through the endothelium, they require the coordinated activity of multiple adhesion proteins. The driving force for the migration and homing of leukocytes is the expression of chemoattractants at the site of inflammation or areas of constitutive production, such as the secondary lymphoid organs or the marrow. Bacterial peptides, complement components, and cytokines are produced in inflammatory sites. More than 40 different but structurally related chemotactic cytokines (chemokines) can be produced by leukocytes in inflammatory sites. The chemokines receptors on the surface of leukocytes are coupled to G proteins that initiate signaling for chemotaxis upon chemokine ligand binding. However, within these 2 subfamilies is significant redundancy and promiscuity in chemokine-receptor binding. The chemokines receptors on the surface of Access Provided by: leukocytes are coupled to G proteins that initiate signaling for chemotaxis upon chemokine ligand binding. Gradual loss of these molecules (eg, shedding of L-selectin) during maturation or after activation could permit movement toward the sinus wall. Endothelial cell cytoplasm separates the sinus lumen from the hematopoietic spaces (arrow). Note deformation of the cell producing a narrow waist where the cell passes through endothelium. The remainder of the cytoplasm is granule-rich, possibly reflecting gel-sol transformation during pseudopod formation. Koury migration, whereas shedding of L-selectin has no effect, and 2-integrin binding helps retain the neutrophils in the marrow. Adventitial reticular cell cytoplasm is a barrier to the reticulocytes on the abluminal surface of the endothelium. Egress occurs through a migration pore that is parajunctional in position (arrows point to endothelial cell junctions). The proplatelets can be separated from the megakaryocyte in the marrow, but the fate of these separated proplatelets is not certain, and they may not give rise to platelets. Page 31 / 70 Chapter 4: Structure of the Marrow and the Hematopoietic Microenvironment, Utpal P. The nucleus of a megakaryocyte (N) is indicated, with the cytoplasm of the megakaryocyte invaginating the endothelial concentrations of S-1-P in the circulating blood activate the S-1-P receptor on the megakaryocytes, thereby, promoting proplatelet extension into the Countway Medical Library vascular sinus. The nucleus of a megakaryocyte (N) is indicated, with the cytoplasm of the megakaryocyte invaginating the endothelial cell cytoplasm in three places below the lumen. A small process of megakaryocyte cytoplasm has formed a pore in the endothelial cell and has entered the sinus lumen (L). The marrow sinus lumen (L) and a megakaryocyte nucleus (N) virtually denuded of cytoplasm are indicated. The megakaryocyte nucleus abuts the nucleus of an adventitial reticular cell; the latter is separated from the lumen by the very thin endothelial cell cytoplasm. A portion of residual megakaryocyte cytoplasm (proplatelet) can be seen streaming into the lumen (arrow). The sequence of events, in particular transit through the R point, is tightly regulated by the retinoblastoma reconstitution. The sequence of events, in particular transit through the R point, is tightly regulated by the retinoblastoma tumor-suppressor protein (Rb) and its paralogs, p107 and p130. Cdk4 and Cdk6 are regulated by D-type cyclins (D1, D2, D3), and Cdk2 is regulated by E-type cyclins (E1 and E2), at early and late stages, respectively, of the G1 phase. Hyperphosphorylated Rb releases E2F transcription factors that promote entry into S phase by transcription of multiple genes required for replication. The D cyclins and Cdk4 and Cdk6 kinases are important in these early progenitor cells because knockout mice that lack all 3 D cyclins583 or lack both Cdk4 and Cdk6 kinases584 have specific, lethal hematopoietic failures at the fetal liver stage of definitive hematopoiesis. Because of the exponential expansion of cells in a proliferating population, cell death has a dramatic effect on the numbers of cells in subsequent generations. During various stages of differentiation, hematopoietic cells depend upon specific cytokines to prevent apoptosis. During various stages of differentiation, hematopoietic cells depend Access Provided by: upon specific cytokines to prevent apoptosis. Experiments in knockout mice have identified specific proteins in the Bcl-2 family as principal regulators of the intrinsic or mitochondrial apoptosis pathway in the homeostasis of the hematopoietic cells populations in the marrow. A model of homeostatic human marrow has been based upon marrow films and sections relating differential counts of marrow samples to their content of injected radioactive iron. Under pathologic conditions, such as infection, inflammation, or hematopoietic dysplasia, the proliferation and differentiation of hematopoietic progenitors may be affected by microbial products, cytokines, and cellular interactions that do not have a role in normal hematopoietic development. Infections, for example, can lead to increased myelopoiesis without the involvement of the hematopoietic cytokines. Although these ligands are most commonly associated with pathologic states where they may play a role in the anemias of chronic disease, they also are proposed to have a regulatory role in normal erythropoiesis. Normal Precursor Cell Kinetics Access Provided by: Marrow Cell Type Number (cells/kg) I. Identification of the haematopoietic stem cell niche and control of the niche size. Stem and progenitor cells: origins, phenotypes, lineage commitments, and transdifferentiations. Flk-2 is a marker in hematopoietic stem cell differentiation: a simple method to isolate long-term stem cells. Deep imaging of bone marrow shows non-dividing stem cells are mainly perisinusoidal. Hoxb5 marks long-term haematopoietic stem cells and reveals a homogenous perivascular niche. A transient definitive erythroid lineage with unique regulation of the -globin locus in the mammalian embryo. Hematopoietic stem cells proliferate until after birth and show a reversible phase-specific engraftment defect. A complex linkage in the developmental pathway of endothelial and hematopoietic cells. Embryonic stromal clones reveal developmental regulators of definitive hematopoietic stem cells. In vivo imaging of haematopoietic cells emerging from the mouse aortic endothelium. Bone morphogenetic protein 4 modulates c-Kit expression and differentiation potential in murine embryonic aorta-gonad-mesonephros haematopoiesis in vitro. Detection of human cells in human/sheep chimeric lambs with in vitro human stroma-forming potential. Transplanted adult hematopoietic stems cells differentiate into functional endothelial cells.
Lemon Balm. Acivir Pills.
- Improving the quality of sleep, when taken with valerian.
- What other names is Lemon Balm known by?
- Cold sores.
- What is Lemon Balm?
- Upset stomach (dyspepsia), when a combination of lemon balm and several other herbs is used.
- Are there safety concerns?
- Colic in breast-fed infants.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96446

Generic 200 mg acivir pills fast delivery
A single-cell hematopoietic landscape resolves 8 lineage trajectories and defects in Kit mutant mice antiviral que es buy 200 mg acivir pills. Transcriptional regulation of erythropoiesis: an affair involving multiple partners. Novel and known ribosomal causes of Diamond-Blackfan anaemia identified through comprehensive genomic characterisation. Absence of yolk sac hematopoiesis from mice with a targeted disruption of the scl gene. Selective rescue of early haematopoietic progenitors in Scl(-/-) mice by expressing Scl under the control of a stem cell enhancer. The zinc-finger proto-oncogene Gfi-1b is essential for development of the erythroid and megakaryocytic lineages. Gfi-1B plays a critical role in terminal differentiation of normal and transformed erythroid progenitor cells. Cytoskeletal distribution and function during the maturation and enucleation of mammalian erythroblasts. Mechanism of protein sorting during erythroblast enucleation: role of cytoskeletal connectivity. E2F-2 promotes nuclear condensation and enucleation of terminally differentiated erythroblasts. Molecular identification and functional characterization of a novel protein that mediates the attachment of erythroblasts to macrophages. Retinoblastoma promotes definitive erythropoiesis by repressing Id2 in fetal liver macrophages. Rb intrinsically promotes erythropoiesis by coupling cell cycle exit with mitochondrial biogenesis. Localization of erythropoietin synthesizing cells in murine kidneys by in situ hybridization. Peritubular cells are the site of erythropoietin synthesis in the murine hypoxic kidney. Human erythropoietin gene expression in transgenic mice: multiple transcription initiation sites and cis-acting regulatory elements. Binding and receptor-mediated endocytosis of erythropoietin in Friend virus-infected erythroid cells. Mechanism of homodimeric cytokine receptor activation and dysregulation by oncogenic mutations. Tyrosine 343 in the erythropoietin receptor positively regulates erythropoietin-induced cell proliferation and Stat5 activation. Mouse surviving solely on human erythropoietin receptor (EpoR): model of human EpoR-linked disease. The cytoplasmic region of the erythropoietin receptor contains nonoverlapping positive and negative growth-regulatory domains. A human erythropoietin receptor gene mutant causing familial erythrocytosis is associated with deregulation of the rates of Jak2 and Stat5 inactivation. Genetic alterations activating kinase and cytokine receptor signaling in high-risk acute lymphoblastic leukemia. Erythropoietin has a mitogenic and positive chemotactic effect on endothelial cells. Erythropoietin blockade inhibits the induction of tumor angiogenesis and progression. Hypoxia-inducible factor-1 deficiency results in dysregulated erythropoiesis signaling and iron homeostasis in mouse development. Circulating erythroid progenitors in polycythemia vera are hypersensitive to insulin-like growth factor-1 in 165. Circulating erythroid progenitors in polycythemia vera are hypersensitive to insulin-like growth factor-1 in vitro: studies in an improved serum-free medium. Insulin-like growth factor binding protein-1 is elevated in patients with polycythemia vera and stimulates erythroid burst formation in vitro. Identification and characterization of an 8-kd peptide stimulating late erythropoiesis. Cellular and molecular mechanisms of senescent erythrocyte phagocytosis by macrophages. Evidence for accumulation of lipid hydroperoxides during the aging of human red blood cells in the circulation. Generation of senescent cell antigen on old cells initiates IgG binding to a neoantigen. The role of hemoglobin denaturation and band 3 clustering in red blood cell aging. Red blood cell oxidative stress impairs oxygen delivery and induces red blood cell aging. Naturally occurring anti-band 3 antibodies bind to protein rather than to carbohydrate on band 3. Inhibition by carbohydrates and monoclonal anticomplement receptor type 1, on interactions between senescent human red blood cells and monocytic macrophagic cells. Editorial comment on: Inhibition of Suicidal Erythrocyte Death by Chronic Hypoxia by Tang et al. Synthesis and biological activities of some N4-substituted 4-aminopyrazolo(3,4-d)pyrimidines. Alpha4beta1 integrin and erythropoietin mediate temporally distinct steps in erythropoiesis: integrins in red cell development. Ulk1 plays a critical role in the autophagic clearance of mitochondria and ribosomes during reticulocyte maturation. Loss of autophagy in erythroid cells leads to defective removal of mitochondria and severe anemia in vivo. Distinct routes of lineage development reshape the human blood hierarchy across ontogeny. The measurement of the total volume of red cells in man: a non-radioactive approach using biotin. A simple and efficient method of labelling red cells with 99mTc for determination of red cell volume. Interpretation of measured red cell mass and plasma volume in adults: Expert Panel on Radionuclides of the International Council for Standardization in Haematology. Measurement of red cell survival using biotin-labeled red cells: validation against 51Cr-labeled red cells. Development, validation, and potential applications of biotinylated red blood cells for posttransfusion kinetics and other physiological studies: evidenced-based analysis and recommendations. Measurement of blood volume and red cell mass: re-examination of 51Cr and 125I methods. Studies of the body hematocrit phenomenon: dynamic hematocrit of large vessel and initial distribution space of albumin and fibrinogen in the whole body. Simultaneous determination of the volume of red cells and plasma for survival studies of stored blood. Recommended methods for measurement of red-cell and plasma volume: International Committee for Standardization in Haematology. Quantitation of ineffective erythropoiesis from the incorporation of [15N] delta-aminolaevulinic acid and [15N] glycine into early labelled bilirubin. Plasma and red cell iron turnover in normal subjects and in patients having various hematopoietic disorders. Ferrokinetics and erythropoiesis in man: an evaluation of ferrokinetic measurements. The soluble transferrin receptor: biological aspects and clinical usefulness as quantitative measure of erythropoiesis. The use of Cr51 and Fe59 in a combined procedure to study erythrocyte production and destruction in normal human subjects and in patients with hemolytic or aplastic anemia. A high-resolution, double-labeling method for the study of in vivo red blood cell aging. Measurement of the viability of stored red cells by the single-isotope technique using 51Cr. Posttransfusion 24-hour recovery and subsequent survival of allogeneic red blood cells in the bloodstream of newborn infants.
Trusted acivir pills 200mg
Flexible sigmoidoscopy is viewed as a sufficient diagnostic test in most cases how long after hiv infection will symptoms appear acivir pills 200 mg otc,339,340 and is far easier to perform than full colonoscopy as it does not require an aggressive preparatory regimen. These cytokines enhance alloreactivity of donor T cells by upregulating the expression of major and minor host tissue histocompatibility antigens and also affect other molecules on host antigen-presenting cells. Regimen-related damage to the gastrointestinal tract results in leakage of endotoxins such as lipopolysaccharides into the systemic circulation, where they serve as additional inflammatory stimuli. Other effector cell populations that contribute to local tissue injury by amplifying the proinflammatory response include neutrophils and mononuclear phagocytes. Importantly, relapse rates did not appear to be increased by the addition of Treg, consistent with murine models. Options include enrollment in a clinical trial, treatment with a second-line agent of choice, and palliative care. In the absence of comparative clinical trial data, the choice of second-line agent is often guided by institutional experience, physician preference, and side-effect profiles. Efforts continue to develop more relevant murine models,376 although translational success remains elusive. Treatment choice depends on patient and physician preference, sideeffect profile, and institutional priorities. Every effort should be made to verify relapse pathologically, as it is common for patients to have residual radiographic abnormalities following transplantation, especially in lymphoma. Relapse often occurs at sites of previous disease, suggesting that residual disease within the patient, rather than autograft contamination, is responsible. Relapse often occurs at sites of previous disease, suggesting Countway Medical Library that residual disease within the patient, rather than autograft contamination, is responsible. Treatmentrelated toxicity with this approach is not prohibitive and successful disease eradication has been reported, although relapse remains the major cause of death. Of the 15 patients, 6 developed sustained chimerism and were completely withdrawn from immunosuppressive medication without renal allograft rejection. Four additional chimeric patients were in the midst of drug withdrawal, and only 4 patients were not withdrawn owing to a return of underlying disease or rejection episodes. Modification of irradiation injury in mice and guinea pigs by bone marrow injections. The effect of homologous bone marrow emulsion on rabbits after total body irradiation. Modification of lethal irradiation injury in mice by injection of homologous or heterologous bone. Treatment of murine leukaemia with X rays and homologous bone marrow; preliminary communication. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. Transfusions and grafts of homologous bone marrow in humans after accidental high dosage irradiation. Preliminary observations on the treatment of postirradiation hematopoietic depression in man by the infusion of stored autogenous bone marrow. Thirty-one-year survival following chemotherapy and autologous bone marrow in malignant lymphoma. Transplantation of bone-marrow cells and fetal thymus in an infant with lymphopenic immunological deficiency. Transplantation of marrow from an unrelated donor to a patient with acute leukemia. Reconstitution in severe combined immunodeficiency by transplantation of marrow from an unrelated donor. Successful engraftment of cryopreserved autologous bone marrow in patients with malignant lymphoma. Evidence that hematopoietic stem cells express mouse c-kit but do not depend on steel factor for their generation. Long-term outcome of patients with metastatic breast cancer treated with high-dose chemotherapy and transplantation of purified autologous hematopoietic stem cells. Endothelial selectins and vascular cell adhesion molecule-1 promote hematopoietic progenitor homing to bone marrow. Role of adhesion molecules in the homing and mobilization of murine hematopoietic stem and progenitor cells. Impaired migration but not differentiation of haematopoietic stem cells in the absence of beta1 integrins. Negrin progenitors and bone marrow stromal cells that serves as a potent negative regulator of hematopoiesis. Osteopontin, a key component of the hematopoietic stem cell niche and regulator of primitive hematopoietic progenitor cells. Parathyroid hormone effectively induces mobilization of progenitor cells without depletion of bone marrow. Risk of complications during hematopoietic stem cell collection in pediatric sibling donors: a prospective European Group for Blood and Marrow Transplantation Pediatric Diseases Working Party study. Granulocyte colony-stimulating factor "mobilized" peripheral blood progenitor cells accelerate granulocyte and platelet recovery after high-dose chemotherapy. Spontaneous rupture of spleen during peripheral blood stem-cell mobilisation in a healthy donor. Peripheral blood progenitor cell mobilization for autologous and allogeneic hematopoietic cell transplantation: guidelines from the American Society for Blood and Marrow Transplantation. Randomised trial of filgrastim-mobilised peripheral blood progenitor cell transplantation versus autologous bone-marrow transplantation in lymphoma patients. Autologous peripheral blood stem cell transplantation in patients with relapsed lymphoma results in accelerated haematopoietic reconstitution, improved quality of life and cost reduction compared with bone marrow transplantation: the Hovon 22 study. Long-term outcome and late effects in patients transplanted with mobilised blood or bone marrow: a randomised trial. A randomized multicenter comparison of bone marrow and peripheral blood in recipients of matched sibling allogeneic transplants for myeloid malignancies. Bone marrow versus peripheral blood allogeneic haematopoietic stem cell transplantation for haematological malignancies in adults. Allogeneic peripheral blood stem cell and bone marrow transplantation for hematologic malignancies: meta-analysis of randomized controlled trials. Allogeneic bone marrow transplantation compared to peripheral blood stem cell transplantation for the treatment of hematologic malignancies: a meta-analysis based on time-to-event data from randomized controlled trials. Translation of clinical research into practice: an impact assessment of the results from the Blood and Marrow Transplant Clinical Trials Network Protocol 0201 on Unrelated Graft Source Utilization. Ex vivo mesenchymal precursor cell-expanded cord blood transplantation after reduced-intensity conditioning regimens improves time to neutrophil recovery. Lymphocyte subset reconstitution after unrelated cord blood or bone marrow transplantation in children. Durable engraftment of major histocompatibility complex-incompatible cells after nonmyeloablative 38 / 59 97. Late-onset colitis after cord blood transplantation is consistent with graft-versus-host disease: results of a blinded histopathological review. Durable engraftment of major histocompatibility complex-incompatible cells after nonmyeloablative conditioning with fludarabine, low-dose total body irradiation, and posttransplantation cyclophosphamide. Absence of post-transplantation lymphoproliferative disorder after allogeneic blood or marrow transplantation using post-transplantation cyclophosphamide as graft-versus-host disease prophylaxis. Survival after T cell-depleted haploidentical stem cell transplantation is improved using the mother as donor. Improved outcome of allogeneic bone marrow transplantation due to breastfeeding-induced tolerance to maternal antigens. Gene-marking to trace origin of relapse after autologous bone-marrow transplantation.
Cheap acivir pills 200 mg visa
Access Provided by: It is not always possible to be sure that a left upper quadrant mass is spleen; masses in the stomach main symptoms hiv infection order acivir pills pills in toronto, colon, kidney, or pancreas may mimic splenomegaly on physical examination. When there is uncertainty regarding the nature of a mass in the left upper quadrant, imaging procedures will usually permit an accurate diagnosis. To properly assess liver size, it is necessary to determine both the upper and lower borders of the liver by percussion. The height of liver dullness is best measured in a specific line, 8, 10, or 12 cm to the right of the midline. The vertical span of the normal liver determined in this manner will range approximately 10 cm in an average-size adult male and approximately 2 cm smaller in an adult female. Correlation of radioisotope imaging data with results from routine physical examinations indicates that often a liver of normal size is considered enlarged on physical examination and an enlarged liver is considered normal. Ultrasonography and computed tomography measurements are useful in determining size and demonstrating localized infiltrative lesions. Vitamin B12 deficiency impairs cerebral, olfactory, spinal cord, and peripheral nerve function, and severe chronic deficiency may lead to irreversible neurologic degeneration. Leukemic meningitis is often manifested by headache, visual impairment, or cranial nerve dysfunction. Tumor growth in the brain or spinal cord compression may be caused by malignant lymphoma or plasma cell myeloma. A variety of neurologic abnormalities may develop in patients with leukemias, lymphomas, and myeloma as a consequence of tumor infiltration, bleeding, infection, or a paraneoplastic syndrome. Essential monoclonal gammopathy is associated with several types of sensory and motor neuropathies. The Karnofsky performance status scale: an examination of its reliability and validity in a research setting. A simple visual assessment technique to discriminate between menorrhagia and normal menstrual blood loss. The risk of immune thrombocytopenic purpura after vaccination in children and adolescents. Gait speed, grip strength and clinical outcomes in older patients with hematologic malignancies. Comparing physical examination with sonographic versions of the same examination techniques for splenomegaly. Accuracy of spleen measurement by medical residents using hand-carried ultrasound. Teaching physical examination of the adult liver with the use of real-time sonography. The decision to perform a marrow examination, and the types of special studies required, should follow from a careful analysis of blood cells and the history and physical examination of the patient. Currently available automated blood cell analyzers provide an increasing array of novel quantitative parameters and flag abnormal samples that need manual microscopic review. The marrow should be examined when the clinical history, blood cell counts, blood film, or laboratory test results suggest the possibility of a primary or secondary hematologic disorder for which morphologic analysis or special studies of the marrow would aid in the diagnosis. In addition to determining the cellularity and morphology of precursor cells, or infiltration by nonhematopoietic cells, the marrow aspirate and biopsy provide cells for immunophenotyping by flow cytometry or immunostains, cytogenetic and molecular studies, culture of infectious organisms, and storage for further analysis. The blood and marrow are examined so as to answer these questions: Is the marrow producing appropriate numbers of mature cells in the major hematopoietic lineages When it comes to the blood, quantitative measures available from automated cell counters are reliable and provide a rapid and cost-effective way to screen for primary or secondary disturbances of hematopoiesis. Light microscopic observation of the blood film is essential to confirm certain quantitative results and to investigate qualitatively abnormal differentiation of the hematopoietic lineages. Based on examination of the blood, the physician is directed toward a more focused assessment of marrow function or to systemic disorders that secondarily involve the hematopoietic system. At that point, a marrow examination may be pursued in order to explore marrow disorders as etiologies for blood abnormalities. In 1923, Arinkin devised the marrow aspiration technique,1 which was the prototype for our current aspiration procedure. Regular use of the posterior iliac crest for aspiration and biopsy and regular use of biopsy to complement aspiration did not occur until the 1970s, when staging of lymphoma made biopsy a frequent procedure and new simpler biopsy instruments became readily available. The morphologic and functional complexity of blood cells requires direct microscopic examination of a stained blood film by a trained observer. However, it is possible to use automated techniques to analyze and report on the majority of samples, using defined criteria ("flags") to select those that need further microscopic review. Automated hematology analyzers typically incorporate multiple proprietary software flags based on acceptability criteria related to pattern recognition in the multiparameter displays or comparison of different detection modes for the same cell type. Instruments flag abnormalities they cannot definitively identify, so that a skilled morphologist can then visually evaluate that specimen. Guidelines for manual blood film review based on comparative data have been published, based on instruments then in common use. Automated hematology analyzers typically incorporate Countway Medical Library multiple proprietary software flags based on acceptability criteria related to pattern recognition in the multiparameter displays or comparison of Access Provided by: different detection modes for the same cell type. Some of these flags can be adjusted or suppressed by the user to achieve an appropriate balance that minimizes both false positives and false negatives. The major analytical challenges are the frequency of the different cell types, which vary over many orders of magnitude, from red cells (1012/L) to basophils (106/L), and the complexity of the structure of normal and abnormal blood cells. Over the past several decades, instruments have become increasingly sophisticated with the use of multiple parameters to produce more precise results in the great majority of patient samples. In a typical automated hematology analyzer, the blood sample is aspirated and separated into different fluidic streams. The streams are mixed with various buffers that accomplish specific purposes in the analysis, for instance, using differential lysis to distinguish subsets of leukocytes, reagents to measure hemoglobin or detect myeloperoxidase containing leukocytes, and various fluorescent dyes. Measurements of each fluidic stream are made in flow as the sample passes through a series of detectors in what are essentially modified flow cytometers. Commonly used principles include light scatter at various angles, electrical impedance and conductivity, and fluorescence or light absorption of cells stained in flow. Light scatter yields information about cell size (using scatter at low-incident angles), nuclear lobulation, and cytoplasmic granularity (using high-angle light scatter) and refractive index, with polarization of the scattered light as an additional parameter. If red cells are converted to spherocytes by the buffer solution to eliminate the variability of cell shape, light scatter at different angles can provide information about hemoglobin content, as well as size of individual red cells. Cell size is also estimated by measuring change in electrical resistance, which is proportional to cell size as cells enter a narrow orifice through which a direct current is maintained, the original Coulter principle, which was named for Wallace Coulter, the developer of the electronic particle counter. Differential lysis with detergents of varying strength or pH is used to separate certain leukocyte types, such as basophils and immature granulocytic cells, from the major normal blood cell types. Light absorption is the principle used for hemoglobin measurement and in some instruments for identifying peroxidase-positive granulocytes. The latter are distinguished by extensive use of fluorochrome tagged antibodies to identify cell subtypes. Schematic of multiparameter cell discrimination in an automated hematology analyzer. Point-of-care "bedside" testing is far more challenging in hematology than for typical clinical chemistry analytes for many of the reasons described above. More work remains to be done to demonstrate the reliability and clinical impact of such testing strategies. The hematocrit may also be determined by subjecting the blood to sufficient centrifugal force to pack the cells while minimizing trapped extracellular fluid. This approach was traditionally done in capillary tubes filled with blood and centrifuged at very high speed (referred to as the "microhematocrit" or, informally, as a "spun crit"). However, this is a manual procedure that is not well adapted to routine processing in a high-volume clinical laboratory, and is affected by varying amounts of plasma trapped between red cells in the packed cell volume,12 typically approximately 2% to 3% of the packed volume. To determine hemoglobin concentration in the blood, red cells are lysed and hemoglobin variants are converted to the stable compound cyanmethemoglobin for quantification or, informally, as a "spun crit"). However, this is a manual procedure that is not well adapted to routine processing in a high-volume clinical laboratory, Countway Medical Library and is affected by varying amounts of plasma trapped between red cells in the packed cell volume,12 typically approximately 2% to 3% of the packed volume.
200 mg acivir pills amex
Syngeneic bone marrow transplantation without conditioning in a patient with Countway Medical Library 80 hiv infection nz buy acivir pills toronto. Paroxysmal nocturnal hemoglobinuria and the transfusio of washed red cells: a myth revisited. Syngeneic bone marrow transplantation without conditioning in a patient with paroxysmal nocturnal hemoglobinuria: in vivo evidence that the mutant stem cells have a survival advantage. Hematopoietic cell transplantation from related and unrelated donors after minimal conditioning as a curative treatment modality for severe paroxysmal nocturnal hemoglobinuria. Successful unrelated donor bone marrow transplantation for paroxysmal nocturnal hemoglobinuria. Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays. Clinical course and flow cytometric analysis of paroxysmal nocturnal hemoglobinuria in the United States and Japan. Radiological intervention in Budd-Chiari syndrome: techniques and outcome in 18 patients. Tissue plasminogen activator for hepatic vein thrombosis in paroxysmal nocturnal haemoglobinuria. Paroxysmal nocturnal hemoglobinuria and the risk of venous thrombosis: review and recommendations for management of the pregnant and nonpregnant patient. Outcome of pregnancy and disease course among women with aplastic anemia treated with, Charles J. Thrombolytic therapy for inferior vena cava thrombosis in paroxysmal nocturnal hemoglobinuria. Pregnancy outcomes of patients with paroxysmal nocturnal hemoglobinuria treated with eculizumab: a Japanese experience and updated review. Managing a pregnant patient with paroxysmal nocturnal hemoglobinuria in the era of eculizumab. The management of pregnancy in paroxysmal nocturnal haemoglobinuria on long term eculizumab. A retrospective study of paroxysmal nocturnal hemoglobinuria in pediatric and adolescent patients. Successful use of eculizumab in a pediatric patient treated for paroxysmal nocturnal hemoglobinuria. Efficacy and safety of eculizumab in children and adolescents with paroxysmal nocturnal hemoglobinuria. Long-term safety and efficacy of sustained eculizumab treatment in patients with paroxysmal nocturnal haemoglobinuria. Folate in its tetrahydro form is a transporter of 1-carbon fragments, which it can carry at any of 3 oxidation levels: methanol, formaldehyde, and formic acid. The primary source of the folate-bound 1-carbon fragments is serine, which is converted to glycine as it passes its terminal carbon to folate. The 1-carbon fragments are used for biosynthesis of purines, thymidine, and methionine. During biosynthesis of purines and methionine, free folate is released in its tetrahydro form. During biosynthesis of thymidine, tetrahydrofolate is oxidized to the dihydro form and must again be fully reduced by dihydrofolate reductase to continue functioning in 1-carbon metabolism. Methotrexate acts as an anticancer agent because it is an exceedingly powerful inhibitor of dihydrofolate reductase, thereby interdicting the generation of reduced folate. In the cell, folates are conjugated by the addition of a chain of 7 or 8 glutamic acid residues. Folates travel in the bloodstream and are taken up by the cells, mainly in the form of methyltetrahydrofolate monoglutamate. The newly absorbed folates are rapidly reglutamylated in the cell by the enzyme folylpolyglutamyl synthase. If glutamylation is prevented, the folates cannot be retained in the cell, resulting in an intracellular folate deficiency. Cobalamin is required for two reactions: intramitochondrial conversion of methylmalonyl coenzyme A (CoA), a product of catabolism of branchedchain amino acids and ketogenic amino acids to succinyl CoA, a tricarboxylic acid (Krebs) cycle intermediate, and cytosolic conversion of homocysteine to methionine, a reaction in which the methyl group of methyltetrahydrofolate is donated to the sulfur atom of homocysteine. In cobalamin deficiency, methyltetrahydrofolate accumulates because, for practical purposes, donation of the methyl group to homocysteine is the only method of generating free tetrahydrofolate from methyltetrahydrofolate. Free tetrahydrofolate is an excellent substrate for folylpolyglutamyl synthase; methyltetrahydrofolate is a poor substrate. Consequently, much of the methyltetrahydrofolate taken up by a cobalamin-deficient cell leaks out of the cell before it can be polyglutamylated. Folate (vitamin B9) and cobalamin (vitamin B12) play key roles in the metabolic machinery of proliferating cells. Megaloblastic anemia most commonly results from folate or cobalamin (vitamin B12) deficiency. It may be seen in persons who are alcoholics and the older poor but also is seen in patients on hyperalimentation, with hemolytic anemia, or hemodialysis. The incidence of neural tube defects has fallen considerably in North America since the introduction of folic acid fortification. Access Provided by: Megaloblastic anemia most commonly results from folate or cobalamin (vitamin B12) deficiency. In the many countries that now practice folic acid fortification of the diet, such as the United States and Canada, the prevalence of folate deficiency has been dramatically reduced and nutritional folate deficiency has been virtually eliminated. In pregnancy, even a mild folate deficiency may be associated with defects in neural tube closure in the fetus, so pregnant women should always receive folate supplements. Diagnosis of folate deficiency is based on measurements of folate in serum, which furnishes information about the current level of folate, and in red cells, which provide data on aggregate folate status over the preceding period during which those red cells were produced. Folate deficiency as a result of malabsorption occurs in tropical and nontropical sprue. Folate deficiency as a result of tropical sprue is treated with folate supplements and antibiotics. The parietal cells secrete intrinsic factor, which is essential for physiologic cobalamin absorption. Without intrinsic factor, a state of cobalamin deficiency develops over the course of years. Cobalamin deficiency leads not only to megaloblastic anemia but also to a demyelinating disease that manifests itself as peripheral neuropathy, spastic paralysis with ataxia (so-called combined system disease of the spinal cord), dementia, psychosis, or some combination of these features. Other causes of cobalamin deficiency are gastric resection; stasis of the small intestinal contents as a result of blind loops, strictures, or hypomotility; and disease or resection of the terminal ileum, the site of cobalaminintrinsic factor complex absorption. The cause of cobalamin deficiency was determined by the Schilling test, a measure of cobalamin absorption, but the test is obsolete and no replacement is currently available. In patients with nutritional megaloblastic anemia, folate or cobalamin deficiency as the cause of the anemia must be determined. If a patient with cobalamin deficiency is treated with folic acid, the anemia may be corrected but the neurologic abnormalities persist, progress or may be aggravated. Patients with cobalamin deficiency usually are treated with parenteral cobalamin but large doses of oral cobalamin may be used. Megaloblastic anemia can develop as an acute disorder with rapid development of leukopenia and/or thrombocytopenia. Nitrous oxide anesthesia or abuse is responsible for some cases of acute megaloblastic anemia. The anemia is rarely also seen in patients with a marginal folate status in intensive care units or severe hemolytic anemia through increased folate demand for augmented erythropoiesis. The condition resembles an immune cytopenia but can be ruled out by examining the marrow, which exhibits a floridly megaloblastic picture. Other causes of megaloblastic anemia include drugs (eg, hydroxyurea, nucleoside analogues) and certain inborn errors of metabolism.
Discount acivir pills 200mg line
Because protein C is a natural inhibitor of coagulation with a short half-life (approximately 8 hours) hiv infection impairs what type of immunity purchase acivir pills 200 mg with visa, its level may also fall rapidly, theoretically inducing a procoagulant state during initiation of therapy. Anticoagulation is initiated with a dose near the expected daily maintenance requirement, which is usually between 5 and 10 mg. After a period of five or more days, the necessary anticoagulant effect of warfarin is achieved, and the parenteral anticoagulant can be stopped. In patients with a low level of protein C or protein S as a result of an inherited deficiency, initiation of warfarin therapy without concomitant heparin or other immediately acting anticoagulant can lead to very low levels of these natural anticoagulants with ensuing thrombosis such as skin necrosis. Specialized clinics devoted to monitoring warfarin typically achieve better results in maintaining patients within the therapeutic range, resulting in fewer bleeding complications. Numerous coding polymorphisms have been identified that can affect the response to warfarin. The cumulative risk of bleeding increases with a longer duration of treatment, whereas the absolute risk is greatest early, possibly caused by pathologic lesions present at the time therapy is started. A rare complication of warfarin therapy is skin necrosis; if it occurs, it usually presents early in the course of anticoagulation. Skin necrosis typically begins with burning and tingling at the affected site, which usually involves a region with a large amount of subcutaneous tissue, such as the breast, buttock, or thigh. Painful, hemorrhagic, full-thickness skin infarction may develop and frequently requires skin grafting. Occasionally, patients report alopecia; hypersensitivity reactions are rare and are almost uniformly caused by the dye used in the pill rather than by the warfarin itself. Oral anticoagulation should be avoided in pregnancy because warfarin crosses the placenta, and exposure during organogenesis in the first trimester can lead to fetal embryopathy with significant cranial bone malformations. Anticoagulation must be reversed for episodes of bleeding, surgery, trauma, or overdosage. The rate of adverse events, such as death and thromboembolism, was similar between groups. If four-factor prothrombin complex concentrate not available, administer fresh-frozen plasma. Patients taking anticoagulation medication who need invasive procedures represent management problems, and decisions about periprocedural anticoagulation should be made based on balancing the risk of thromboembolism with that of blood loss from the procedure. Evidence-based guidelines for bridging therapy are available,45 and the topic has been reviewed. In general, the risk of recurrence is greatest in the period shortly after an episode of acute thrombosis and declines progressively over time. A randomized study with 681 patients undergoing pacemaker or defibrillator implantation showed that the procedure can safely be done without stopping warfarin treatment. Postprocedural bridging therapy should be undertaken only in patients in whom the risks of this therapy (principally bleeding) are less than the perceived benefits (a reduced risk of thromboembolism). The anticoagulant effect is immediate, but laboratory monitoring is needed because of the variability in response among patients. Clinically useful nomograms are available for adjusting the heparin dose using either fixed- or weight-based dosing. Therefore, stopping the infusion and local measures are usually adequate to control bleeding. However, in major or life-threatening bleeding, the anticoagulant effect can be neutralized with protamine sulfate, which is a basic polypeptide that binds tightly to the acidic heparin molecule. The dose to be administered is based on the amount of heparin remaining in the circulation. Therefore, Access Provided by: stopping the infusion and local measures are usually adequate to control bleeding. Protamine is routinely used to neutralize heparin after cardiopulmonary bypass using standard formulas and activated clotting time monitoring. Long-term heparin therapy can also cause osteoporosis, and radiographic evidence of bone loss occurs in approximately 15% of women who receive prolonged treatment during pregnancy, with symptomatic vertebrae fractures in approximately 2%. Each preparation differs slightly and is pharmacologically unique, although the agents are likely similarly effective for the treatment and prevention of venous thrombosis. Similarly, monitoring may be necessary to achieve appropriate levels in very obese patients, although weight-based dosing probably achieves better anticoagulation. Similar to unfractionated heparin, the most common adverse effect is bleeding, which occurs at approximately the same frequency and severity when used in similar patient groups for the same indication. Unfractionated heparin may be preferable in patients who require an invasive procedure on an urgent basis because of its shorter half-life. At the time of this writing, danaparoid is not approved in the United States but is available elsewhere. Because it inhibits factor Xa but has no direct action on thrombin, its mechanism of action depends on reducing thrombin generation. Pharmacologic studies show that maximum plasma levels are reached approximately two hours after subcutaneous administration, with an elimination half-life of approximately 17 hours independent of the dose. There is a low intra- and intersubject variability with little accumulation after multiple daily doses. Because elimination is primarily renal and the agent is excreted unchanged in the urine, fondaparinux is contraindicated in patients with severe renal impairment. Elevated levels may occur in patients with renal insufficiency, and caution should be exercised in using fondaparinux in patients with renal compromise. The drug is eliminated by both renal and hepatic clearance, and consequently, dose modification is recommended for patients with moderate-to-severe liver or kidney disease. Bivalirudin is effective when used with aspirin in patients with unstable angina or postinfarction angina undergoing angioplasty, and it is approved for this use. The most common adverse effect is bleeding, and no specific antidote is available. As with other direct thrombin inhibitors, the main side effect is bleeding, and no specific agent is available to reverse its action. For higher argatroban doses, the infusion rate should be reduced to 2 mcg/kg per minute and the aforementioned procedure performed. Dabigatran does not require a cofactor and reversibly inhibits the active site of thrombin. Although not well studied, there are published case reports showing that dialysis or hemoperfusion likely removes this compound from the circulation. Andexanet alfa is a decoy F Xa without its catalytic domain and it competes with the endogenous factor Xa to bind any F Xa inhibitor (Xa-inh), thereby eliminating the anticoagulant effect. Idarucizumab is a monoclonal antibody fragment (Fab) that specifically binds the oral thrombin inhibitor dabigatran (Dabi) 300 times stronger than thrombin.
