
Buy 500mg aleve with visa
Implantation the process of embryo implantation was thought to take place between 6 and 7 days after ovulation hip pain treatment uk cheap aleve 250 mg overnight delivery,1,2 but more contemporary studies suggest that in most successful human pregnancies, the embryo implants approximately 8 to 10 days after ovulation. This implantation process has been reviewed by Norwitz and colleagues5 and Dey and coworkers. In this concept, synchronization between embryonic and uterine receptivity is required for successful nidation. Although the process of embryo implantation requires a receptive endometrium, the process is not exclusive to the endometrium, because advanced ectopic. By day 3 of embryo culture, embryo development is at the six- to eight-cell stage. Embryos placed back into the uterus at this stage remain unattached to the endometrium and continue developing to the blastocyst stage, they "hatch" or escape from the zona pellucida, and they implant by day 6 or 7 of embryo life. Because the implantation potential for each embryo is affected by the age of the mother, and because embryo morphology alone is imprecise for predicting the likelihood of implantation, transfer of multiple embryos can result in higher-order multiple births, such as twins, triplets, or occasionally quadruplets. The overall implantation rate for each goodquality embryo at this stage is between 30% and 50% per embryo. Thus, to achieve a reasonable chance of pregnancy, most women have only one or two good-quality blastocyststage embryos transferred to the uterus, reducing the chances of higher-order multiple births. A recent study from populationbased control data indicates that the use of assisted reproductive technology accounts for a disproportionate number of lowbirth-weight and very-low-birth-weight infants, in part because of multiple births and in part because of higher rates of low birth weight among singleton infants conceived with assisted reproductive technologies. The beginning of endometrial receptivity coincides with the downregulation of progesterone and estrogen receptors induced by the corpus luteum production of progesterone. It was thought that this process required tight regulation, in that the morphologic development of microvilli (pinopodes) in glandular epithelium9 and increased angiogenesis were required for successful embryo nidation. Reviews of embryo implantation have identified an increasing number of factors, such as integrins, mucins, L-selectin, cytokines, proteinases, and glycoproteins, localized to either the embryo or the endometrium during the window of implantation. Integrins are also essential components of the extracellular matrix and function as receptors that anchor extracellular adhesion proteins to cytoskeletal components. At present, the integrin receptor family is composed of at least 14 distinct subunits and more than nine subunits,14 making up to 20 integrin heterodimers. One particular integrin, v3, is expressed on endometrial cells after day 19 of the menstrual cycle. Because v3 is also localized to trophoblast cells, it may participate in cell-tocell interactions between the trophoblast and endometrium acting through a common bridging ligand. It is postulated that after hatching, the blastocyst, through its trophoblastic integrin receptors, attaches to the endometrial surface. Antibodies to v or integrins inhibit the attachment activity of intact blastocysts. Studies with human placental villous explants suggest that chorionic villous cytotrophoblasts can differentiate along two distinct pathways: by fusing to form the syncytiotrophoblast layer or as extravillous trophoblasts that have the potential to invade the inner basalis layer of endometrium and the myometrium to reach the spiral arteries. Once trophoblasts have breached the endometrial blood vessels, decidualized stromal cells are believed to promote endometrial hemostasis by release of tissue factor and by thrombin generation. Around this core are the outer syncytiotrophoblast layer and the inner layer of cytotrophoblast. In general, both cytotrophoblast and syncytiotrophoblast produce peptide hormones, whereas the syncytiotrophoblast produces all of the steroid hormones. Timing of the Luteal-Placental Shift Ovarian progesterone production is essential for maintenance of early pregnancy. During later gestation, placental production of progesterone is sufficient to maintain pregnancy. To uncover the timing of this luteal-placental shift, Csapo and colleagues performed corpus luteum ablation experiments. They demonstrated that removal of the corpus luteum before, but not after, the 7th week of gestation usually resulted in subsequent abortion. Thus, progesterone supplementation is required if corpus luteum function is compromised before 9 to 10 weeks of gestation. The decrease in 17-hydroxyprogesterone and the dip in progesterone levels reflect the transition of progesterone secretion from the corpus luteum to the placenta. The secretion of 17-hydroxyprogesterone during the last third of pregnancy occurs largely from the fetoplacental unit. Estriol is not secreted by the ovary of nonpregnant women, but it makes up more than 90% of the estrogen in the urine of pregnant women and is excreted as sulfate and glucuronide conjugates. During pregnancy, a woman produces more estrogen than a normally ovulating woman could produce in more than 150 years. To form estrogens, the placenta, which has active aromatizing capacity, uses circulating androgens as the precursor substrate. In the past, maternal estriol measurements were often used as an index of fetoplacental function. However, numerous problems have been documented in interpreting low estriol levels, which has limited the use of estriol. A single plasma measurement is meaningless because of moment-to-moment fluctuations. Moreover, numerous drugs, including glucocorticoids and ampicillin, affect estriol levels. It is the 15-hydroxy derivative of estriol and is derived exclusively from fetal precursors. Contributing to fetal and placental activity are the changes occurring in the maternal endocrine milieu. Estrogens, androgens, and progestins are involved in pregnancy from before implantation to parturition. They are synthesized and metabolized in complex pathways involving the fetus, the placenta, and the mother. In contrast, the Leydig cells of the fetal testes are capable of production of large amounts of testosterone, so the circulating testosterone concentration in the first-trimester male fetus is similar to that in the adult man. Fetal testosterone is required for promoting differentiation and masculinization of the male external and internal genitalia. In addition, local conversion of testosterone to dihydrotestosterone by 5-reductase localized in situ at the genital target tissues ensures final maturation of the external male genital structures. The maternal environment is protected from the testosterone produced by the male fetus because of the abundance of placental aromatase, which can convert testosterone to estradiol. Exogenous progesterone must be administered during the first trimester to oocyte recipients who have no ovarian function. About 90% of the progesterone synthesized by the placenta enters the maternal compartment. Most of the progesterone in the maternal circulation is metabolized to pregnanediol and is excreted in the urine as a glucuronide. Hydroxylation at the C2 position of the phenolic A ring results in the formation of so-called catecholestrogens (2-hydroxyestrone, 2-hydroxyestradiol, and 2-hydroxyestriol) and is a major step in estrogen metabolism. Apparently, 2-hydroxyestrone levels increase during the first and second trimesters and decrease in the third trimester. Thus, catecholestrogens, present in large quantities, may have significant effects in pregnancy. About 90% of the estradiol-17 and estriol secreted by the placenta enters the maternal compartment. Pregnancies also reach term accompanied by severe fetal and placental aromatase deficiency. In addition, in the case of aromatase deficiency, both the fetus and the mother are virilized as a consequence of diminished aromatization of androgens. Low levels of estrogens also occur after fetal demise and in most anencephalic pregnancies, in which fetal signals from the fetal hypothalamic-pituitary unit are diminished and do not stimulate synthesis of fetal adrenal androgens. In the absence of a fetus, as occurs in molar pregnancy and in pseudocyesis, estrogen levels are low as well. Because progestins have potent uterine relaxation properties, two pivotal clinical trials have examined the efficacy of progestin administration for prevention of preterm labor. Progesterone may also help to maintain pregnancy by inhibiting T-lymphocyte-mediated processes that play a role in tissue rejection. Progesterone is important in the creation of a cervical mucus barrier that prevents pathogens from penetrating the uterus. The stimulatory effects of estrogen on phospholipid synthesis and turnover, prostaglandin production, and increased formation of lysosomes in the uterine endometrium, as well as estrogen modulation of adrenergic mechanisms in uterine myometrium, may be the means by which estrogens act to time the onset of labor.
Buy genuine aleve on line
Problematic long-term side effects of all antipsychotics include tardive dyskinesia and the metabolic syndrome pain treatment toothache buy aleve master card. Negative and cognitive symptoms, in particular, show little improvement with antipsychotics alone. Instead, the comprehensive treatment of schizophrenia requires integration of pharmacologic treatment with psychologic therapies and concomitant psychosocial rehabilitation. The availability of cognitive-behavioral therapy and cognitive remediation with rehabilitation holds promise for treating persistent symptoms and cognitive deficits. Yet many who drink alcohol do not experience negative health or social consequences, and some health-care studies suggest health benefits may be associated with alcohol consumption. To normalize these guidelines, a "standard drink" is defined as an ethanol alcohol content of 14 grams (equivalent to 12 ounces of beer, 5 ounces of table wine, or 1. It is considered "low-risk" for healthy adult men under age 65 years to consume no more than 14 standard drinks per week, with up to 4 drinks per day, and for healthy adult nonpregnant women under age 65 years and healthy men and women age 65 years and older, no more than 7 standard drinks per week and up to 3 standard drinks per day. The following risk factors may increase the potential negative health consequences of drinking even with "low-risk" patterns of consumption: (1) first-degree relative with alcohol or drug dependence. Conditions wherein no amount of alcohol is established as safe or any amount of alcohol is established as harmful include (1) pregnancy, (2) age younger than 21 years, (3) operating a vehicle or other machinery, (4) taking medications interacting with alcohol, and (5) having active physical or mental health symptoms. These subtypes are briefly described below and represent typical patient presentations (excluding geriatric presentation of alcohol dependence, which typically involves a prominence of alcohol-related health consequences, cognitive deficits, and loss of independent self-care and functioning). Comprising the largest group with alcohol dependence nationally, they tend to lack common risk factors for alcohol dependence (family history of alcohol dependence, co-occurring drug use, or mental illness). This subtype is a priority for medical screening, since they rarely seek treatment. Mid-20s with high rates of co-occurring drug use (>75% smoke cigarettes and cannabis), with strong family alcohol dependence histories. Onset of drinking begins in youth, which may in part Continued use of alcohol despite interpersonal problems Recurrent use of alcohol in hazardous situations Failure to fulfill major obligations at work, school, or home Recurrent legal problems related to alcohol use Other problem patterns of drinking Mon Tues Wed Thur Fri Sat Sun Mon Tues Wed Thur Fri Sat Sun Hazardous behavior Cirrhosis, alcoholic hepatitis Neurologic Belligerence Pancreatitis Cardiovascular Daily alcohol use at levels likely to cause end organ damage account for the severity of alcohol dependence at a young age. Co-occurring mental illnesses are common (depression, anxiety, and personality disorders). This group is of particular importance for pediatrician- and school-based screenings for substance use. Typically, these are welleducated, middle-aged individuals with stable jobs and relationships, colloquially referred to as "highfunctioning alcoholics. About half smoke cigarettes, one third have strong family histories of alcohol dependence, and one quarter have a lifetime history of depression. Spouse abuse Intermittent abuse of alcohol at levels that result in dangerous and destructive behavior Intermediate Family (19%). This group of middleaged individuals, half of whom have a lifetime history of depression and strong family histories of alcohol dependence, has high rates of co-occurring mental illness and drug use, and the majority smoke cigarettes. Despite overt problems with functioning, only 25% actively seek treatment for drinking. This group frequently presents for psychiatric care where screening for substance use is critical to diagnosing alcohol dependence. This group of middle-aged individuals has early age onset of drinking, high rates of co-occurring mental illness and drug use, and high rates of antisocial personality disorder and criminal behavior with legal consequences. Two thirds will actively seek treatment due to prominent negative consequences of drinking. Selfreported drinking (2010) among those age 12 years and older indicates that 23% binge drink (more than five drinks per drinking day), and nearly 7% are heavy drinkers (binge drink on five or more days per month); yet fewer than 2% of the population needing substance use treatment receives treatment. Screening for alcohol use disorders identifies individuals at risk for developing alcohol-related problems and those already meeting criteria for an alcohol use disorder. Treatment for alcohol use disorders begins with an assessment of whether medical detoxification is required for physiologic dependence at risk for dangerous alcohol withdrawal syndromes; this is especially important for patients with co-occurring hypertension, diabetes mellitus, seizure disorder, and history of suicidality. Detoxification may be monitored on an outpatient basis, but many patients will require inpatient detoxification to prevent relapse to drinking. For alcohol-dependent individuals, abstinence from alcohol is most effective at maintaining recovery gains. An antagonist at central mu-opioid receptors, naltrexone attenuates opioid-mediated reward of drinking and clinically reduces alcohol cravings, relapse, and drinking days, and it increases the probability of containing recurrent drinking to a brief episode rather than full relapse. Brief counseling assists patients with alcohol use disorders to create and maintain effective treatment plans to reduce or quit drinking. Lifestyle changes and reducing social drinking risks are recommended to prevent relapse. Patients with alcohol dependence are encouraged to use medication therapies to assist efforts to stop drinking; these include naltrexone, acamprosate, and disulfiram. It poses hepatotoxicity risk and is contraindicated in those with hepatic disease and those requiring narcotic analgesia. Naltrexone is currently the only evidence-based medication for geriatric alcohol dependence. A glutamate neuromodulator, acamprosate is an abstinence-promoting medication appropriate for patients who have achieved early abstinence. It is metabolized within the kidney, providing a good choice for those with hepatic disease. This aldehyde dehydrogenase inhibitor prevents the final metabolic conversion of ethanol to water; usage results in accumulation of toxic acetaldehyde metabolites, leading to flushing, headache, hypertension, sweating, and nausea/vomiting. Disulfiram is most effective at reducing anticipated rewards of alcohol and thus reducing drinking days. Adherence is problematic, and there is a 1 in 50,000 risk of idiopathic fulminant hepatotoxicity; thus careful hepatic monitoring is required. It is a preferred treatment for impaired professionals and parents at risk of losing child custody. Because of its renal metabolism, it is contraindicated with renal calculi or glaucoma. This involves autonomic instability, agitation, altered mental state, hallucinations, and tremor. Moderate scores (8 to 15) reflect autonomic hyperactivity, and high scores (>15) predict seizures and delirium; these scores warrant immediate initiation of medical treatment. Some medical treatments assisting recovery and promoting abstinence are hypothesized to address persistent central hyperexcitability. These include acamprosate, naltrexone, disulfiram, and topiramate (see Plate 4-14). These medications must be combined with complete alcohol abstinence and active attendance at Alcoholics Anonymous or similar support groups. Symptom-triggered detoxification protocols are used because these prevent medical morbidity, and even a very occasional death, while minimizing dosing requirements for benzodiazepines and thus adverse effects. Typical protocols initiate treatment with either short-acting (lorazepam) or longer-acting (diazepam, chlordiazepoxide) benzodiazepines once autonomic arousal is recognized; this is followed by repeated dosing during the first 24 hours, based on resolution of autonomic arousal and patient comfort. Blood pressure Vomiting Sweating Heart rate Nausea Visual, tactile, and auditory hallucinations Tremor Expression and severity of symptoms vary with duration and degree of dependence and with recognition and treatment of early withdrawal. Stages of alcohol withdrawal Stage 1 Hours after alcohol consumption 24 36 (peak) 48 Stage 2 (48-72) Aggravated forms of stage 1 symptoms with severe tremors, agitation, and hallucinations Stage 3 (72-105) Acute organic psychosis (delirium), confusion, and disorientation with severe autonomic symptoms Symptoms Mild-to-moderate anxiety, tremor, nausea, vomiting, sweating, elevation of heart rate and blood pressure, sleep disturbance, hallucinations, illusions, seizures Stage 1 withdrawal usually self-limited. These protocols are guidelines because ongoing clinical assessment is required for safety; doses should be held if increasing sedation or gait instability develops. Treatment must include nutritional repletion of thiamine, folate, and multivitamins. However, the very favorable efficacy and safety of benzodiazepines does not support their use with their weaker evidence for efficacy as primary treatments. This includes medication management per Plate 4-13, treatment of co-occurring psychiatric and medical illnesses, and referral to ongoing care for substance abuse. Level of care determinations may be assisted by evidencebased Patient Placement Criteria developed by clinical researchers in the American Society of Addiction Medicine. Six domains influencing probability of good outcome are assessed to help determine the appropriate level of care; these include (1) severity of intoxication and withdrawal, (2) medical comorbidity, (3) psychiatric illness and psychosocial stability, (4) patient readiness to participate actively in treatment, (5) history of past treatment outcomes, and (6) recovery environment. Levels of care range from least restrictive outpatient to increasing medical and psychiatric outpatient supervision (intensive outpatient, partial hospital) to residential treatment. The highest level of care is inpatient hospitalization with both intensive medical and psychiatric stabilization of life-threatening symptoms.
Buy aleve us
Blood samples should be drawn for analysis and an infusion of normal saline should be started pain treatment buy aleve 250 mg with amex. The initial in hospital, treatment is usually a benzodiazepine, such as lorazepam, administered intravenously. If benzodiazepines fail to terminate the seizure, then phenytoin or phenobarbitone may be administered. If seizures remain uncontrolled, then general anesthesia and artificial ventilation may be required. However, there is debate on whether aggressive therapy with anesthetic agents is warranted. Epilepsia partialis continua refers to the situation in which there is continuous focal motor activity that may last months to years. There are many genetic and neurometabolic causes that lead to seizures, typically beginning in childhood. Genetic disorders include disorders such as severe myoclonic epilepsy of childhood, tuberous sclerosis, Rett syndrome, Angelman syndrome, and fragile X. Neurometabolic disorders, which may also have a genetic cause, result in disturbances of metabolism and can lead to seizures. Disorders such as urea cycle defects, pyridoxine dependency, biotinidase deficiency, and glucose transporter deficiencies can cause severe seizures. The most common types of brain lesions causing seizures are tumors, vascular lesions, head trauma, infectious diseases, congenital malformation of the brain, and biochemical or degenerative disease processes affecting the brain. Brain tumor is an important cause of seizures, particularly in the adult patient, becoming an increasingly likely cause after the second decade of life and one of the main causes in the fourth and fifth decades. A brain tumor should be suspected in any person who has onset of seizures, especially focal seizures, after age 20 years. Head trauma is a major cause of seizures, which may occur shortly after the head injury or, more often, several months to several years later. Factors that increase the chance of development of post-traumatic seizures are a penetrating head injury, severe damage to the brain, prolonged periods of unconsciousness, posttraumatic amnesia, complications of wound healing, and a persistent neurologic deficit. Vascular disease is one of the most common causes of seizures in older persons, particularly after age 50 years. Seizures can occur transiently after an acute stroke (thrombotic, embolic, or hemorrhagic) or may develop later as a sequela of cerebrovascular disease. Although uncommon, arteriovenous malformations are frequently associated with seizures. Other vascular causes include subdural hematomas, venous thrombosis, and hypertensive encephalopathy. Seizures may occur with any acute infection of the nervous system or as a complication of damage to the nervous system by the inflammatory process. With improved neuroimaging, many patients who were thought to have idiopathic epilepsy have now been found to have brain malformations. The severity of the seizures is related to the type and extent of the malformation. Disease processes or disorders that can cause seizures include various types of metabolic, electrolyte, and biochemical disturbances; hypoxia; hypoglycemia; toxic processes; drugs; or abrupt withdrawal from drugs or alcohol. Various conditions, such as fever, fatigue, sleep deprivation, flashing lights, sound, or emotional factors may also precipitate seizures in susceptible individuals. The movement of ions across the cell membrane is dependent upon both concentration and electrostatic forces. Ions flow from high concentrations to lower concentrations as depicted by the flow of K+ ions from inside the cell, where the concentration is high, to outside the cell, where the concentrations is lower. In this example, K+ ions flow from the extracellular environment, which is positive in retationship to the intracellular space, which is negative. The equilibrium potential for the ion is the membrane potential at which a particular ion does not diffuse through the membrane in either direction. Na+ Na+ nEurobiology of EpilEpSy the core feature of brain electrochemical signals is the neuron membrane. This lipid bilayer prevents the exchange of ionized substrates between the cell and its environment, which is critical for electrical signaling. The inside of the cell at rest is negatively charged compared with the outside of the cell, due to concentration differences in ions. Sodium (Na+), calcium (Ca2+), and chloride (Cl-) are predominantly found extracellularly, whereas K+ and organic ions are concentrated intracellularly. These pumps create concentration differences (between the inside and outside of the neuron) by transporting ions against their concentration gradients (from regions of low concentration to regions of high concentration). This concentration gradient across the membrane provides the electrochemical energy to drive signaling. Unlike the continuous transport by the ion pumps, transport by the ion channels is noncontinuous. Voltage-gated channels open or close in response to changes in electrical potential across the cell membrane, whereas ligand-gated channels require a binding of a particular signaling molecule to open or close. The two most important ions in the transmission of action potentials are Na+ and potassium K+. Voltagegated Na+ channels have three types of states: deactivated (closed), activated (open), and inactivated (closed). During excitation of the cell, Na+ channels are activated through removal of an intracellular "activation gate," and Na+ begins flowing into the cell. Once some Na+ ion channels begin opening, the voltage drops further, causing more channels to open until the membrane depolarizes. Na+ channels are more sensitive to voltage change than K+ channels are and open more rapidly. Thus in a depolarization, the Na+ ions will rush into the cell faster than the K+ ions move outward. This sudden depolarization, called an action potential, will briefly result in a +30 millivolt potential difference. Once the slowly-opening voltage-gated K+ ion channels have opened and allowed K+ to flow out, the action potential is ended. Once Na+ channels are activated, they quickly are inactivated due to an "inactivation gate" that blocks the inside of the channel shortly after it has been activated. During an action potential, the channel remains inactivated for a few milliseconds after depolarization. The inactivation is removed when the membrane potential of the cell repolarizes after the falling phase of the action potential. Thus the Na+ ion channels initiate the action potential, and the K+ ion channels terminate it. The channels then close, and the sodium pump can restore the resting potential of -70 millivolts. Membrane polarity is also affected by ligand-gated channels that open when neurotransmitters, the ligands of synaptic transmission, bind to specific receptors connected to the channels. When the membrane begins to depolarize, the activation channel opens and ion flow occurs. As the cell becomes depolarized, the inactivation gate closes and no further ion flow occurs. Only when the cell repolarizes does the sodium channel return to the resting state. The release of a neurotransmitter is triggered by the arrival of a nerve impulse (or action potential) and occurs through a process called exocytosis. Within the presynaptic nerve terminal, vesicles containing neurotransmitter sit "docked" and ready at the synaptic membrane. The arriving action potential produces an influx of Ca2+ ions through voltage-dependent, Ca2+-selective ion channels. Ca2+ ions then bind with the proteins found within the membranes of the synaptic vesicles, allowing the vesicles to "dock" with the presynaptic membrane, resulting in the creation of a fusion pore. An action potential is a short-lasting event in which the electrical membrane potential of a cell rapidly rises and falls.
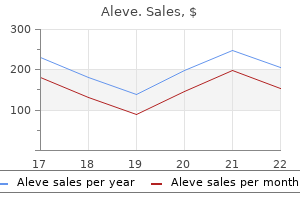
| Comparative prices of Aleve | ||
| # | Retailer | Average price |
| 1 | CVS Caremark | 203 |
| 2 | Delhaize America | 764 |
| 3 | Verizon Wireless | 775 |
| 4 | Raley's | 723 |
| 5 | AutoZone | 179 |
| 6 | RadioShack | 559 |
Purchase aleve online pills
Truncal ataxia occurs with midline lesions chest pain treatment guidelines buy aleve 250 mg overnight delivery, including titubation, that is, oscillations of the head and trunk. The patient has a widened stance and is unable to stand in tandem position or on one foot. Cerebellar ataxic gait is staggering, uneven, irregular, and veers from side to side. Dysmetria (Greek dys, and metron [measure]) is the disordered ability to regulate, judge, and control behavior, both with motor and cognitive domains (see Plate 815). The cerebellar motor syndrome causes difficulty judging distances, trajectory of intended movements, and force required for movements. Rebound is tested by the examiner dis placing the arm downward, observing for overshoot above the starting point. Dysmetria characteristics include endpoint tremor, overshooting targets (hyper metria) or undershooting (hypometria), and oscillation at the elbow. Acute cerebellar lesions produce headache, nausea, vomiting, and vertigo, along with gait ataxia, dysarthria, and sometimes diplopia. Tremor increases with proximity to the target; tremor direction is generally perpendicular to direction of movement. Dysdiadochokinesia is degradation of rapid alternating move ments, tested by forearm pronation/supination. Dysrhythmia is an inability to generate normal rhythms, assessed by rapidly tapping the hand on a surface or the heel on the ground. The heel-to-shin test, performed with the patient supine, assesses leg coordination. In wheelchairbound patients, the heel is brought to the knee of the opposite leg held parallel to the ground. Proximal overshoot occurs as the heel is placed on the knee, and tremor occurs as the heel is maintained in that position. Slowing, jerking, or sidetoside move ments are noted as the heel moves down the shin. In the drawacircle test, the supine patient traces a circle in the air; decomposition manifests as irregular or chaotic motions. Rubral tremor from red nucleus lesions and its connections involves multiple joints, direction changes, and is frequently rotatory. Palatal tremor is slow and semirhythmic, resulting from GuillainMollaret myoclonic triangle lesions of this neuronal brainstem/cerebellum network (dentate nucleus to red nucleus and inferior olivary nucleus). Cognitively relevant areas are situated more laterally in these lobules, whereas the limbic cerebellum is represented in the vermis. Lesions of the sensorimotor cerebellum result in the cerebellar motor syndrome (see Plate 814). This constellation of deficits is characterized by impairments in (1) executive function, (2) visual spatial processing, (3) linguistic deficits, and (4) affective dysregulation. It can be prominent after acute lesions, including stroke, hemorrhage, and infectious or postin fectious cerebellitis but relatively subtle in lateonset hereditary ataxias. Executive function deficits include problems with working memory, as tested with reverse digit span; mental flexibility is tested using tasks of set shifting; and perseveration is demonstrated using bedside tests of mental control. Patients may have concrete thinking, poor problemsolving strategies, and impaired ability to multitask, with trouble planning, sequencing, and orga nizing their activities. Visuospatial disintegration is apparent when attempting to copy or recall visual images. Iden tification of multiple features within a complex diagram (simultanagnosia) is difficult. Expressive language can be abnormal, characterized by long response latency, brief responses, reluctance to engage in conversation, and wordfinding difficulties. Verbal fluency is decreased affecting phonemic (letter) more than semantic (category) naming. Mutism occurs postoperatively for vermis tumors, particularly in children but also in adults subsequent to cerebellitis, infarction, and hemorrhage. Degraded control of volume, pitch, and tone can produce high-pitched, hypophonic speech. Short-term memory impairments include difficulty learning and spontaneously recalling new information, reflecting deficient strategies for organizing verbal or visualspatial material for encoding, and difficulty locat ing information in memory stores. Successful recall is aided by a structured approach to the task, using clues and other prompts. Conditional associative learning is degraded, as shown in studies of classic conditioning in cerebellar patients (as well as in animals). Patients exhibit difficulty modulating behavior and personality style, have flattened affect or disinhibition manifesting as overfamiliarity, and flam boyant or impulsive actions. Behavior may be regressive and childlike, sometimes with obsessivecompulsive traits. Patients can be irritable, with labile affect and poor attentional and behavioral modulation. Neuropsychological consequences of cerebellar tumour resection in children: cerebellar cognitive affective syndrome in a paediatric population. Early evidence indicates that there are five domains of behavioral dysregulation caused by cerebellar damage. These are impairments of attentional control, emo tional control, autism spectrum disorders, psychosis spectrum disorders, and difficulties with the social skill set. Within each of these domains, there are hypometric/ diminished behaviors and hypermetric/exaggerated behaviors, consistent with the dysmetria of thought theory of the cerebellar role in nervous system function. The intellectual and emotional impairments from damage to the cognitive and limbic posterior lobe of the cerebellum may be more disabling than motor defi cits, and when the anterior lobe is spared, these occur in the absence of the motor syndrome. Recognizing the nonmotor manifestations of cerebellar lesions can lead to earlier diagnosis of cerebellar damage and facilitate treatment of cognitive emotional consequences of dis rupted cerebellar modulation of higher function. The nature of these deficits provides new avenues for con ceptualizing mental illnesses, including autism, schizo phrenia, bipolar disorder, attention deficit disorder, and dyslexia. Appreciating the role of the cerebellum beyond motor control therefore has implications for understanding and improving neuropsychiatric disor ders. This represents a radical departure from our pre vious understanding of the functions of the "little brain" and is an area of active investigation in neurosci ence. The neural substrates that support this nonmotor cerebellar role are discussed in Plate 813. The following principles guide the approach: (1) recog nize symptoms and signs of cerebellar disease; (2) deter mine whether peripheral nerves, spinal cord, brainstem, or cerebral hemispheres are also affected; (3) character ize the timing of onset and progression, that is, the temporal profile; (4) search for risk factors, that is, toxins and drugs, recent infections, and systemic features of neoplasms; (5) document family history and country of origin, a critical feature when considering hereditary disorders; (6) brain magnetic resonance imaging is essen tial; and (7) laboratory data may clinch the diagnosis. Note the "posterior fossa mantra" of acute cerebellar and brainstem injury-headache, nausea, vomiting, and vertigo, with or without ataxia, dysarthria, diplopia, and nystagmus. Acute cerebellitis occurs more commonly in children than adults, starting more abruptly than postinfectious cerebellitis; both produce a pancerebellar syndrome. Thiamine deficiency produces Wernicke encephalopathy, a triad of ataxia, confusion, and oculomotor distur bances that is a medical emergency requiring immedi ate repletion of vitamin B1. Cerebellar tumors (benign or malignant) worsen over weeks to months but occasionally present acutely with obstructive hydrocephalus. Alcoholic cerebellar atrophy (anterior superior vermis) may present sub acutely, as can cerebellar leukoencephalopathy from inhaled solvents and heroin, and CreutzfeldtJakob disease, with ataxia, dementia, and myoclonus. Neurodegenerative disorders start insidiously, progress ing over years or decades. Dentatorubropallidoluysian atrophy causes myoclonus, dystonia, and cognitive decline; it is uncommon outside Japan. Ataxia telangiectasia often manifests before telangiectasias develop; features include recurrent infections from immunoglobulin IgA deficiency and radiation sensitivity with risk of neoplasia. Ataxia with oculomotor apraxia types 1 and 2 include peripheral neuropathy, choreiform movements, and cognitive difficulties. Mitochondrial encephalomyopathies cause ataxia and complex clinical constellations. Many disorders of infancy and childhood have cerebellar malformations or disruptions-hypoplasia, agenesis, megacerebellum, Chiari, and DandyWalker malformations. Elicitation of the history is followed by observation of the gait, which facilitates hypothesisdriven examina tion. Focused imaging and laboratory investigations confirm or refute the clinical impression.
Discount aleve online mastercard
Because the attachment to the lower rib is farther forward from the axis of rotation pain treatment and wellness center discount aleve express, contraction raises the lower rib more than it depresses the upper rib. Note how contraction of the diaphragm increases the vertical diameter of the thorax, whereas Clinical note: During normal inhalation at rest, abdominal pressure increases secondary to diaphragmatic contraction. This acts like a vacuum and "sucks open" the airways, causing air to enter the lungs. This increase is then transmitted to the terminal air spaces (alveolar ducts and alveoli) and compresses them, causing air to leave the lungs. This reduction in airway diameter is the primary source of resistance to airflow during expiration. One can imagine the difficulty asthmatic individuals face during exhalation with the addition of bronchoconstriction. Airway resistance normally accounts for approximately 20% of the work of breathing. Pathophysiology note: Airway diameter can be reduced (and airway resistance thereby increased) by a number of mechanisms. Pharmacology note: Many classes of drugs affect large-airway diameter by affecting bronchial smooth muscle tone. For example, b2-adrenergic agonists such as albuterol directly stimulate bronchodilation. Pathology note: In emphysema, compliance work is reduced because of the destruction of lung tissue and the loss of elastin and collagen. In pulmonary fibrosis, compliance work is increased, because the fibrotic tissue requires more work to expand. Tissue resistance: normally small component of work of breathing due to presence of pleural fluid 4. Respiratory Physiology Pathology note: In certain pleuritic conditions, inflammation or adhesions are formed between the two pleural surfaces, which increases tissue resistance substantially. As elastance increases, increasingly greater pressure changes will be required to distend the lungs. Clinical note: In restrictive lung diseases such as silicosis and asbestosis, inspiration becomes increasingly difficult as the resistance to lung expansion increases in response to increased lung elastance, resulting in reduced lung volumes and total lung capacity. In obstructive lung diseases such as emphysema, there is reduced lung elastance secondary to destruction of lung parenchyma and loss of proteins that contribute to the elastic recoil of the lungs. Expiration may therefore become an active process (rather than a passive one), even while at rest, because the easily collapsible airways "trap" air in the lungs. The water molecules are attracted to each other through noncovalent hydrogen bonds and are repelled by the hydrophobic alveolar air. The attractive forces between water molecules generate surface tension (T), which in turn produces a collapsing pressure, which acts to collapse the alveoli. Alveolus Attractive force Alveolar fluid (without surfactant) Repulsion due to lipid Alveolar fluid (with surfactant) Surfactant and the hydrophobic "tail" in the alveolar air. Polar head Lipid tail 5-9: Role of surfactant in reducing alveolar surface tension. Atelectatic lung may result from external compression, as may occur with pleural effusion or tumor; a prolonged period of "shallow breaths," as may occur with pain. Mothers in premature labor are frequently given corticosteroids to stimulate the fetus to produce surfactant. The diffusing capacity of the lungs is normally so great that O2 exchange is perfusion limited; that is, the amount of O2 that enters the arterial circulation is limited only by the amount of blood flow to the lungs (cardiac output). Palv, Alveolar partial pressure; Part, arterial partial pressure; Pven, venous partial pressure. In the upright position, when the effects of gravity are apparent, the lung apices are relatively underperfused, whereas the lung bases are relatively overperfused. Lung apices: relatively underperfused in upright position owing to low arterial hydrostatic pressure at lung apices Zone 1 has no blood flow during the cardiac cycle. Zone 1 blood flow: may be seen with severe hemorrhage and positivepressure ventilation 152 Rapid Review Physiology 3. This pattern of blood flow is characteristic of the lung bases, which are situated below the heart. The catheter is inserted through a central vein and advanced into the pulmonary artery. An inflated balloon at the distal tip of the catheter allows it to "wedge" into a distal branch of the pulmonary artery. Zone 3 blood flow: primarily occurs in the lung bases V/Q matching: important for efficient gas exchange V/Q matching: inefficient to perfuse unventilated alveoli or ventilate nonperfused alveoli Lung apices relatively overventilated at rest Lung bases relatively overperfused at rest Mechanisms of V/Q matching: hypoxiainduced vasoconstriction, pulmonary hemodynamic and ventilatory changes with exercise C. However, in the pulmonary vasculature, hypoxia stimulates vasoconstriction of pulmonary arterioles, essentially preventing the perfusion of poorly ventilated lung segments. During exercise, additional capillaries open (recruitment) because of increased pulmonary artery blood pressure. Anatomic shunt: blood diverted from lungs; examples: fetal blood flow, right-to-left intracardiac shunting Physiologic shunt: blood supplying the lungs is not involved in gas exchange; examples: bronchial arterial circulation, pneumonia, pulmonary edema D. A shunt refers to blood that bypasses the lungs or for another reason does not participate in gas exchange (Table 5-4). In the fetus, gas exchange occurs in the placenta, so most of the cardiac output either is shunted from the pulmonary artery to the aorta through the ductus arteriosus or passes through the foramen ovale between the right and left atria. The bronchial arteries supply the bronchi and supporting lung parenchyma but are not involved in gas exchange at the level of the alveoli. Total lung capacity comprises several individual pulmonary volumes and capacities. There are four pulmonary volumes (tidal volume, inspiratory reserve, expiratory reserve, and residual volume). Note that in patients with both restrictive and obstructive disease, lung volumes may remain relatively normal. Lung volumes: # in restrictive disease; " in obstructive disease Respiratory Physiology 6000 Inspiration 155 5000 Inspiratory reserve volume Tidal volume Inspiratory capacity Vital capacity Total lung capacity 5-17: Spirogram showing changes in lung volume during normal and forceful breathing. Tidal volume: volume of air inspired or expired with each breath; approximately 500 mL Inspiratory reserve volume: volume of air that can be inspired beyond a normal tidal inspiration Expiratory reserve volume: volume of air that can be exhaled after a normal tidal expiration Residual volume: can be measured by helium dilution technique 156 Rapid Review Physiology b. There are four lung capacities: functional residual capacity, inspiratory capacity, vital capacity, and total lung capacity. Inspiratory capacity: maximum volume of air that can be inhaled after a normal tidal inspiration C. In obstructive diseases, expiratory volumes are reduced because of airway narrowing and sometimes a loss of elastic recoil in the lungs. There are three types of dead space: anatomic, alveolar, and physiologic 8 Normal 6 Expiration (L/sec) Total lung capacity: maximum lung volume; " in obstructive disease, # in restrictive disease Types of dead space: anatomic, alveolar, physiologic 5-19: Flow-volume loop showing the difference between an obstructive (A), normal, and restrictive (B) airflow pattern. Before inspired air reaches the terminal respiratory airways, where gas exchange occurs, it must first travel through the conducting airways. It is estimated as approximately 1 mL per pound of body weight for thin adults, or about 150 mL in a 150-pound man.
Purchase generic aleve on line
Patients with psychogenic movement disorders typi cally are unresponsive to appropriate medications hip pain treatment uk discount aleve 250mg overnight delivery, but remission may occur with treatment of the underlying psychiatric disorder. The psychiatric diagnosis may include various somatoform and factitious disorders, depression, anxiety, and histrionic personality disor ders. A specific psychiatric diagnosis cannot always be made despite a high index of suspicion for psycho genicity, and the neurologist and psychiatrist may differ in their assessments of the underlying problem. Complete hemianesthesia or glove-and-stocking anesthesia may be present in conversion disorder or hypochondriasis/ somatization. Symptoms may have developed on an organic basis and then been perpetuated and elaborated psychogenically. Features suggesting a good prognosis are acute onset, short duration of symptoms, healthy premorbid functioning, absence of other organic or psychogenic disorders, and presence of an identifiable precipitant. May show varying degrees of improvement or progress to athetoid or spastic stages. Although the initial lesion may be fixed, the clinical pattern of presentation might vary with growth and development. Approximately 75% of cases are due to prenatal injury, with less than 10% due to birth trauma or asphyxia. Low birth weight and pre maturity are important risk factors for the occurrence of cerebral palsy. Other risk factors include chorioam nionitis, teratogenic exposures, hyperbilirubinemia, and hypoglycemia. Other early signs include hand preference, prominent fisting, persistence of neonatal reflexes, and delay in emergence of protective and postural reflexes. Cases can also be classified into spastic, dyskinetic, ataxic, hypotonic, and mixed. Of these, spastic cerebral palsy with diplegia of the lower extremities and scissoring gait is the most common, accounting for 70% to 75% of cases. Imaging demonstrates periventricular leukomalacia around the lateral ventricles, with ischemia as the most common pathologic finding. Mild cases manifest with toe walking, whereas severe cases have flexion of the hips, knees, and elbows. Quadriplegic cerebral palsy, the most severe form, is characterized by Ataxic cerebral palsy. Pseudobulbar signs and optic atrophy is usually present in up to 50% of affected children. Mental retardation (60%), visual impairment, and oculomotor impairments are common. In those chil dren who develop cerebral palsy as a consequence of kernicterus, deafness, dystonia, choreoathetosis and, to a lesser extent, ataxia are the most common clinical findings, in addition to corticospinal tract involvement in a smaller proportion of patients. These are key points to remember when assessing adults who come for an evaluation of a new movement disorder and have a history of neonatal hyperbilirubinemia. Feeding difficulties, swallowing dys function, and drooling may complicate the clinical picture. Its upper and lower ends become continuous, respectively, with the cerebral (sylvian, or mesencephalic) aqueduct and the central canal of the spinal cord in the lower half of the medulla. The lateral boundaries are formed on each side from above down by the superior cerebellar peduncle, the inferior cerebellar peduncle, and the cuneate and gracile tubercles. The upper and lower parts of the Vshaped roof are formed by the superior and inferior medullary vela, which are thin laminae of white matter between the superior and inferior cerebellar peduncles. The lower part of the inferior velum has a median aperture (foramen of Magendie); cerebrospinal fluid escapes through this opening and the lateral aper ture (foramina of Luschka) into the subarachnoid space. Because these are the only communications between the ventricular and subarachnoid spaces, their blockage can produce hydrocephalus. The lower part of the roof and the posterior walls of the lateral recesses are invaginated by vascular tufts of pia mater, which form the Tshaped choroid plexus of the fourth ventricle. The floor of the fourth ventricle is rhomboid shaped and is divided into symmetric halves by a vertical median sulcus. Its upper (pontine) and lower (medul lary) parts are demarcated by delicate transverse strands of fibers, the striae medullares of the fourth ventricle. On each side of the median sulcus is a longitudinal elevation, the medial eminence, lateral to which runs the sulcus limitans. Its superior part is the locus ceru leus, colored bluishgray from a patch of deeply pig mented nerve cells. Lateral to it is a slight depres sion, the inferior fovea, which, together with the neigh boring vagal trigone, overlies parts of the dorsal nuclei of the glossopharyngeal and vagus nerves. Lateral to the inferior fovea is the lower part of the vestibular area, overlying parts of the vestibular nuclei of the vesti bulocochlear nerve. On a deeper plane, parts of the trigeminal, solitary tract, and ambiguus nuclei also underlie the floor of the fourth ventricle. Some of the nuclei mentioned, such as the dorsal vagal and ambig uus nuclei, as well as others located in the nearby reti cular formation, are concerned with cardiovascular, respiratory, metabolic, and other important functions, and are regarded as vital centers. Any lesion in this rela tively small area of the brain may produce disastrous results. However, its surface area is 40% of the cerebral cortex, containing half the total number of intracerebral neurons. The cerebellum, con sisting of two hemispheres situated contiguously with the midline vermis, is separated from the overlying cere brum by the tentorium cerebelli. Superiorly, in contrast, the vermis appears as a low ridge straddling the midline, extending up 10 mm bilaterally. A wide hollow within the anterior cerebellum is occupied by the pons and upper medulla oblongata, which are separated from the cerebellum by the fourth ventricle. The cerebellum is connected to the brainstem by three white matter tracts: the supe rior, middle, and inferior cerebellar peduncles (described more fully in Plate 83). The cerebellum surfaces include numerous narrow folia separated by parallel, curved, deeply penetrating fis sures. These ten lobules form three lobes: the anterior, posterior, and flocculonodular lobes. Earlier cerebel lum nomenclatures were not uniform (one version is in the diagrams for comparison). The primary fissure separating the anterior from the posterior lobe is deepest and most evident in the mid sagittal plane but not as readily identifiable externally. The paravermian sulcus on each side of the superior cerebellum surface is an indentation formed by the superior cerebellar artery medial branch. The interior of the cerebellum contains a central mass of white matter, the medullary core, surrounded by the deeply folded cerebellar folia. The relationship of the folia to the white matter has a tree branch appearance, hence arbor vitae. The white matter core extends into the folia as narrow laminae, surrounded by the three layered cerebellar cortex. There are no association fibers in the cerebellum linking cerebellar cortical areas with each other. The cerebellar nuclei within the medullary core include, medial to lateral, the fastigial, globose, emboliform, and dentate. Except for the vestibulocerebellum, these nuclei are the primary source of cerebellar efferents. Its open end, or hilus, points medially, conveying fibers that, together with those from the fastigial, globose, and emboliform nuclei, form the superior cerebellar peduncle. The larger is the restiform body, a purely afferent system, whereas the smaller juxtarestiform body carries both afferent and efferent fibers. Entering the cerebellum, it is situated medial to the middle cerebellar peduncle, conveying uncrossed mossy fiber afferents to cerebellum from the ipsilateral spinal cord and brainstem, and crossed climbing fiber inputs from the contralateral inferior olivary nucleus. The rostral spinocerebellar tract carries information from the upper limbs and the central cervical tract arising from upper cervical seg ments. The juxtarestiform body is a small aggregation of fibers situated medial to the restiform body that enters the cerebellum passing through the vestibular nuclei. Primary vestibular afferents arise from the vestibular sense organs (the saccule and utricle) and terminate ipsilaterally; second ary vestibular fibers from the vestibular nuclei termi nate bilaterally. Efferent fibers in the juxtarestiform body arise from the cerebellar cortex and fastigial nucleus. Juxtarestiform body fibers arising from the fastigial nuclei lead to the vestibular and the reticular nuclei. Axons from the rostral half of the fastigial nucleus course to the ipsilateral brainstem in the fastigiobulbar tract.
Buy aleve 250 mg
Adverse effects (1) Dry mouth (2) Sedation (3) Postural hypotension (4) Withdrawal from high-dose therapy may result in life-threatening hypertensive crises due to increased sympathetic activity pain treatment spa discount aleve online master card. These drugs relax the bladder neck and the prostate by blocking the a1-adrenergic receptors located in smooth muscle. This leads to compensatory mechanisms and the need for the use of drug combinations to block these compensatory effects. Oral bioavailability is dependent on the acetylation phenotype (N-acetyltransferase) of patients. Relaxation of the vascular smooth muscle of the arterioles 107 Clonidine is the only antihypertensive agent available as a transdermal patch. Withdrawal from clonidine should occur slowly (over 1 week) to avoid a hypertensive crisis. Abrupt withdrawal of either beta blockers or clonidine leads to rebound hypertension. Combination therapy with isosorbide dinitrate and hydralazine is especially effective in the AfricanAmerican population. Metabolic conversion to cyanide and thiocyanate may cause severe toxic reactions if the infusion of sodium nitroprusside is continued for several days. Arterial pressure may be titrated by intravenous administration because of its rapid action and short (minutes) half-life (t1/2). Decreases both preload and afterload 109 Nitroprusside: metabolic conversion to cyanide (systemic asphyxiant) Nitroprusside: initial drug of choice in lowering blood pressure in aortic dissection. All dihydropyridine calcium channel blockers end in -dipine: amlodipine, felodipine, isradipine, nicardipine, nisoldipine, nifedipine, nimodipine Relative efficacy of calcium channel blockers as vasodilators: nifedipine > diltiazem > verapamil Relative efficacy of calcium channel blockers in control of heart rate: verapamil > diltiazem > nifedipine Calcium channel blockers are noted for causing hypotension and peripheral edema. Occasionally, acute renal failure in patients with bilateral renal artery stenosis d. Rapid-acting agents (1) Amyl nitrite (inhalation) (2) Nitroglycerin (intravenous, sublingual) b. Long-acting agents (1) Isosorbide dinitrate (regular oral, sustained-release oral, sublingual) (2) Nitroglycerin (transdermal, ointment, sustained-release oral) (3) Isosorbide dinitrate (regular oral, sustained-release oral) 2. Nitrates do not increase total coronary blood flow in patients with ischemia (1) But, they redistribute blood to ischemic areas by dilating large supply epicardial arteries (2) Thus, correcting the myocardial oxygen imbalance. Effects of nitrate-induced vasodilation (1) Increases venous capacitance (reducing preload) (2) Decreases arteriole resistance (decreases afterload) (3) Preload is affected more greatly (decreased return of blood to right heart) than afterload. Objective of antianginal therapy: to balance O2 demand with O2 supply in myocardial tissue. Nitrate-induced vasodilation results in Nitrates redistribute blood to ischemic areas but do not increase overall coronary blood flow. The tolerance was reversed over the weekend and the cycle started again on Monday. Methemoglobinemia (nitrites) (1) Methemoglobin contains oxidized iron (ferric) (2) Methemoglobin cannot bind to oxygen 5. Myocardial oxygen requirements are reduced due to decreases in: (1) Heart rate (2) Myocardial contractility (3) Blood pressure 2. Block calcium movement into cells, inhibiting excitation-contraction coupling in myocardial and smooth muscle cells b. The metabolism of lipoproteins and the mechanism of action of some antihyperlipidemic drugs are summarized in. Diet and lifestyle changes are first-line and drug second-line therapy for hyperlipidemias. Resins bind bile acids in the intestine to form an insoluble, nonabsorbable complex that is excreted in the feces along with the unchanged resin. Heterozygous familial hypercholesterolemia (but not effective in the homozygous form) c. Adjunctive treatment of pseudomembranous colitis (binds Clostridium difficile toxin) 4. All these drug names end in -statin: atorvastatin, fluvastatin, lovastatin, pravastatin, rosuvastatin, simvastatin. Treatment of primary dysbetalipoproteinemia, homozygous familial hypercholesterolemia. Adverse effects (1) Generalized pruritus as a result of peripheral vasodilation, characterized by flushing, warmth, and burning or tingling of the skin, especially of the face or neck; reduced by: (a) Taking after meals (b) Taking aspirin 30 minutes prior to dose (c) Using extended-release formulations (2) Increased hepatic enzymes (3) Acanthosis nigricans (4) Leg cramps (5) Myalgia (6) Gout (7) Worsen type 2 diabetes E. Peripheral vasodilation occurs frequently with niacin; pretreatment with aspirin prevents this development. Beta blockers are beneficial but calcium channel blockers are detrimental in patients with heart failure. To slow ventricular rate in tachyarrhythmias such as: (1) Atrial fibrillation (2) Atrial flutter (3) Supraventricular tachycardia (paroxysmal atrial tachycardia) c. Cardiogenic shock Quinidine increases digoxin levels by interfering with tissue protein binding and renal excretion of digoxin. Metoprolol, bisoprolol, and carvedilol are the beta blockers that have been shown to prolong life expectancy in patients with heart failure. Dobutamine and dopamine (b1 receptor stimulants) are useful positive inotropes for acute heart failure. Treatment of toxicity (1) Discontinue medication (2) Correct either potassium or magnesium deficiency (3) Give digoxin antibody (digoxin immune Fab, or Digibind) for severe toxicity 6. Increase life expectancy in patients with mild and moderate congestive heart failure 2. Positive inotropic agents that should be used for acute treatment only Phosphodiesterase inhibitors 1.
Aleve 500mg lowest price
A number of other pain medication for dogs natural generic aleve 500 mg without prescription, less well recognized uterine factors have also been implicated in the generation of uterine contractions. Endothelin receptors have been isolated in amnion, chorion, endometrium, and myometrium,153,203 and they increase in the myometrium during labor. It acts by binding to specific cell-surface tyrosine-kinase receptors that have been identified also in decidua and myometrium, and it appears to be upregulated by estrogen. Relaxin is secreted by the corpus luteum, placenta, and myometrium, and relaxin binding sites have been identified on myometrial cells. It has several functions during development and in adult tissues, including regulation of vascular tone, bone remodeling, placental calcium transport, and myometrial relaxation. Magnesium is present in the extracellular fluid of the myometrium in very high concentrations (10 nM), which results in increased intracellular magnesium levels, inhibition of calcium entry into myometrial cells via L- and T-type voltageoperated calcium channels, and enhanced sensitivity of potassium channels,167,178 all of which lead to hyperpolarization and myometrial cell relaxation. In addition to naturally occurring uterine relaxants, a number of agents have been developed to stop preterm labor (see Box 5-1). Unfortunately, the ability of these tocolytic agents to prevent preterm birth has been largely disappointing. Synthetic competitive oxytocin receptor antagonists such as atosiban (which has mixed vasopressin and oxytocin receptor specificity) inhibit uterine contractility both in vitro and in vivo. Aspirin causes irreversible acetylation of the cyclooxygenase enzyme, whereas indomethacin is a competitive (reversible) inhibitor. Although these agents are relatively effective, their adverse effects on the developing fetus (including premature closure of the ductus arteriosus and persistent pulmonary hypertension) have significantly limited their use. Moreover, these adverse effects can be seen with both nonselective cyclooxygenase inhibitors. Role of the Cervix in Labor the onset of forceful, coordinated uterine contractions was once considered the key initiator of cervical change to facilitate birth. However, studies in humans and animals have confirmed that cervical remodeling begins long before the onset of uterine contractions. Both processes, while independent, must be coordinately regulated for successful parturition. Although understanding of the molecular mechanisms that regulate cervical remodeling remains incomplete, recent advances suggest that remodeling begins early in pregnancy and that a progressive and incremental transformation from a rigid to a compliant cervix occurs over the course of gestation. More recently, the decline in cervical length from early to late pregnancy as measured by transvaginal ultrasound has provided evidence that modifications to cervical structure begin relatively early in pregnancy. Regulated alterations in processing and assembly of collagen fibers, as well as a reduction in the matricellular proteins thrombospondin 2 and tenascin C, lead to modifications of cervical collagen architecture and reduced mechanical strength. In particular, the columnar glandular epithelia undergo a marked proliferation, and these cells secrete mucus that serves as a physical barrier and contains immunoglobulins in addition to other factors that provide immunologic protection against ascending infection. This thick mucus obstructs the cervical canal and is commonly referred to as the mucus plug. Throughout the softening phase of cervical remodeling, the ratio of progesterone to estrogen is high and likely regulates early modifications in cervical structure. Relaxin is a peptide hormone made by the corpus luteum that has been implicated in cervical epithelial and stromal cell proliferation and in connective tissue remodeling. This phase is characterized by increased synthesis of the hydrophilic glycosaminoglycan, hyaluronan, and expression of genes encoding hyaluronan synthase. This isoform is likely to contribute to the increased tissue hydration of the cervix at term, further disorganizing the collagen architecture and resulting in a maximal decline in cervical tensile strength. It also demonstrates that loss of progesterone functional activity leads to cervical ripening and labor. Observations that transvaginal progesterone supplementation from 16 to 20 weeks through 36 weeks of gestation is able to prevent preterm birth in some women who are at high risk due to cervical shortening support the notion that the local steroid hormone milieu is important for cervical ripening. The mucus plug that obstructs the cervical canal is expelled at this time, and the cervix must open to a diameter of 10 cm to allow passage of a term fetus. Cervical effacement describes the process by which the cervix shortens until it becomes a thin, circular opening. Although it is difficult to discern processes that are distinct to this phase of cervical remodeling, compared with ripening or postpartum repair, it is likely that the biochemical changes activated during this phase are regulated by both hormonal factors, mechanical forces induced by myometrial contraction, and descent of the fetus. Hyaluronidase is an enzyme that breaks down large-molecular-weight hyaluronan, and its activity increases during this phase, which may contribute to complete loss of tissue competence. Exogenous administration of prostaglandins promotes cervical changes that mimic ripening and dilation, including increased solubility of collagen and alteration in extracellular matrix composition. Numerous immunohistochemical studies have shown an increase in leukocyte cell infiltration in this phase of cervical remodeling; the leukocytes likely secrete proteases to break down poorly assembled extracellular matrix components. Achieving a Successful Delivery Labor is not a passive process in which uterine contractions push a rigid object through a fixed aperture. The ability of the fetus to successfully negotiate the pelvis during delivery depends on the complex interaction of three critical variables: the forces generated by the uterine musculature (the powers); the size and orientation of the fetus (the passenger); and the size, shape, and resistance of the bony pelvis and soft tissues of the pelvic floor (the passage). Because of the asymmetry in the shape of both the fetal head and the maternal pelvis, the fetus needs to undergo a series of orchestrated rotations (referred to as the cardinal movements) to allow it to negotiate the birth canal successfully. Further discussion of the mechanics of labor and delivery are beyond the scope of this chapter, but they have been reviewed in detail elsewhere. The factors responsible for the onset and maintenance of normal labor at term are not completely understood and continue to be actively investigated. A better understanding of the mechanisms responsible for the onset of labor at term will further knowledge about disorders of parturition, such as preterm and prolonged (postterm) labor, and improve our ability to secure a successful pregnancy outcome. American College of Obstetricians and Gynecologists: Management of postterm pregnancy. Romero R, Nicolaides K, Conde-Agudelo A, et al: Vaginal progesterone in women with an asymptomatic sonographic short cervix in the midtrimester decreases preterm delivery and neonatal morbidity: a systematic review and metaanalysis of individual patient data, Am J Obstet Gynecol 206:124. Facchinetti F, Paganelli S, Comitini G, et al: Cervical length changes during preterm cervical ripening: effects of 17-alpha-hydroxyprogesterone caproate, Am J Obstet Gynecol 196:453.
