
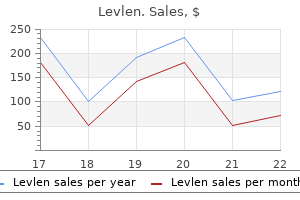
Cheap levlen online
Neutropenic fever syndromes in patients undergoing cytotoxic therapy for acute leukemia and myelodysplastic syndromes birth control 3 hours late buy discount levlen line. Empiric antibiotic and antifungal therapy for cancer patients with prolonged fever and granulocytopenia. Caspofungin versus liposomal amphotericin B for empirical antifungal therapy in patients with persistent fever and neutropenia. Empirical versus preemptive antifungal therapy for high-risk, febrile, neutropenic patients: a randomized, controlled trial. Immune reconstitution inflammatory syndrome in cancer patients with pulmonary aspergillosis recovering from neutropenia: Proof of principle, description, and clinical and research implications. Treatment of aspergillosis: Clinical practice guidelines of the Infectious Diseases Society of America. Bronchoalveolar lavage fluid galactomannan for the diagnosis of invasive pulmonary aspergillosis in patients with hematologic diseases. Liposomal amphotericin B as initial therapy for invasive mold infection: a randomized trial comparing a high-loading dose regimen with standard dosing (AmBiLoad trial). Clinical utility of blood cultures drawn from indwelling central venous catheters in hospitalized patients with cancer. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Central venous catheter care for the patient with cancer: American Society of Clinical Oncology clinical practice guideline. Diagnosis of catheter-related bacteraemia: a prospective comparison of the time to positivity of hub-blood versus peripheral-blood cultures. Differential time to positivity: a useful method for diagnosing catheter-related bloodstream infections. Central lineassociated bloodstream infections in adult hematology patients with febrile neutropenia: an evaluation of surveillance definitions using differential time to blood culture positivity. Mucosal barrier injury laboratoryconfirmed bloodstream infection: results from a field test of a new National Healthcare Safety Network definition. Antibiotic and other lock treatments for tunnelled central venous catheter-related infections in children with cancer. Rescue therapy of difficult-to-treat indwelling central venous catheter-related bacteremias in cancer patients: a review for practical purposes. The diagnostic yield of skin biopsy in patients with leukemia and suspected infection. Outcome of respiratory syncytial virus lower respiratory tract disease in hematopoietic cell transplant recipients receiving aerosolized ribavirin: significance of stem cell source and oxygen requirement. Mortality rates of human metapneumovirus and respiratory syncytial virus lower respiratory tract infections in hematopoietic cell transplantation recipients. Human metapneumovirus infection as an emerging pathogen causing acute respiratory distress syndrome. In vitro and in vivo activities of posaconazole against zygomycetes with various degrees of susceptibility. Accuracy of -D-glucan for the diagnosis of Pneumocystis jirovecii pneumonia: a meta-analysis. A second look at anorectal infections in cancer patients in a large cancer institute: the success of early intervention with antibiotics and surgery. Sharma P, Kozarek R, Practice Parameters Committee of American College of Gastroenterology. Characteristics and treatment outcome of cerebrospinal fluid shunt-associated infections in adults: a retrospective analysis over an 11-year period. The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America. Early detection of Toxoplasma infection by molecular monitoring of Toxoplasma gondii in peripheral blood samples after allogeneic stem cell transplantation. Significant improvement following combination treatment with mefloquine and mirtazapine in a patient with progressive multifocal leukoencephalopathy after allogeneic peripheral blood stem cell transplantation. Current outcome of patients with ureteral stents for the management of malignant ureteral obstruction. Acute renal failure due to adenovirus-associated obstructive uropathy and necrotizing tubulointerstitial nephritis in a bone marrow transplant recipient. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 20092010. Colonization with multidrug-resistant gram-negative bacteria: prolonged duration and frequent cocolonization. Risk factors for infection and treatment outcome of extended-spectrum -lactamase-producing Escherichia coli and Klebsiella pneumoniae bacteremia in patients with hematologic malignancy. Risk factors and treatment outcomes of bloodstream infection caused by extended-spectrum cephalosporin-resistant Enterobacter species in adults with cancer. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Linezolid in methicillinresistant Staphylococcus aureus nosocomial pneumonia: a randomized, controlled study. Daptomycin versus vancomycin plus gentamicin for treatment of bacteraemia and endocarditis due to Staphylococcus aureus: subset analysis of patients infected with methicillin-resistant isolates. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. Multicenter study of high-dose daptomycin for treatment of enterococcal infections. Epidemiology and outcomes of Clostridium difficile infections in hematopoietic stem cell transplant recipients. Risk factors for acquisition of Clostridium difficile-associated diarrhea among outpatients at a cancer hospital. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Fecal microbiota transplantation for Clostridium difficile infection: systematic review and meta-analysis. Saccharomyces boulardii for the prevention of antibiotic-associated diarrhea in adult hospitalized patients: a single-center, randomized, double-blind, placebo-controlled trial. Effectiveness of alcohol-based hand rubs for removal of Clostridium difficile spores from hands. Tracking a hospital outbreak of carbapenem-resistant Klebsiella pneumoniae with whole-genome sequencing. Dosing nomograms for attaining optimum concentrations of meropenem by continuous infusion in critically ill patients with severe gram-negative infections: a pharmacokinetics/pharmacodynamicsbased approach. The combination of doripenem and colistin is bactericidal and synergistic against colistin-resistant, carbapenemase-producing Klebsiella pneumoniae. Aerosolized plus intravenous colistin versus intravenous colistin alone for the treatment of ventilator-associated pneumonia: a matched case-control study. Impact of Bolus dosing versus continuous infusion of Piperacillin and Tazobactam on the development of antimicrobial resistance in Pseudomonas aeruginosa. Optimization of continuous infusion of piperacillin-tazobactam in children with fever and neutropenia. High-dose continuous infusion beta-lactam antibiotics for the treatment of resistant Pseudomonas aeruginosa infections in immunocompromised patients. Carbapenem-resistant Acinetobacter baumannii: epidemiology, surveillance and management. The early multipotent progenitors include the totipotent hematopoietic stem cells, capable of generating both the lymphoid and the myeloid series, and the myeloid and lymphoid stem cells. The totipotent stem cells include different populations of cells: the most primigenius ones with long-term repopulation capacity and the more mature ones with short-term repopulation capacity. The myeloid stem cell undergoes commitment into the myeloid, erythroid, and megakaryocytic progenitors, from which the differentiated marrow precursors of the circulating blood elements are derived. Both stem cells and early progenitors are indistinguishable from lymphocytes in microscopic preparation of the bone marrow and of the peripheral blood. Their existence was established from the ability to generate hematopoietic colonies containing multiple (multipotent progenitors) or single (committed progenitors) cell lines. The stem cell and to some extent the committed progenitors have high self-renewal potential and low proliferative rate, while the differentiated marrow precursors have a low self-replicative capacity and high proliferation.
African Civet (Civet). Levlen.
- Are there safety concerns?
- What is Civet?
- Dosing considerations for Civet.
- How does Civet work?
- Pain relief and sleeplessness.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96707
Buy levlen 0.15mg online
Fibers terminating into main sensory nucleus of trigeminal nerve located in lateral pons-It responsible for tactile and proprioceptive sensation birth control to regulate periods order levlen without a prescription. Third nucleus-mesencephalic nucleus-it receives proprioceptive impulses from (i) masticatory muscles (ii) muscles supplied by other cranial nerves. Ophthalmic nerve supplies: Skin of nose Forehead Upper eyelid Scalp (as far back a lambdoidal suture in the midline) Upper-half of cornea, conjunctiva and iris Mucous membrane of frontal, sphenoidal and ethmoidal sinuses Upper nasal cavity and septum Lacrimal canals Dura mater of anterior cranial fossa Falx cerebri Tentorium cerebelli. Area Supplied Sensory Skin of lower lip, lower jaw, chin Skin of tympanic membrane Auditory meatus Upper ear Mucous membranes of floor of the mouth Lower gum Anterior two-thirds of tongue (not taste sensation) Teeth of lower jaw Dura mater of posterior cranial fossa. Examination of Sensory Function Testing of sensations are mainly based on: 1002 Clinical Methods and Interpretation in Medicine Pain Touch Temperature Vibration sense Joint sense. The following methods can differentiate organic from nonorganic lesion (but they are reliable always): Nonorganic sensory loss may have a demarcation of abnormal area at hairline than scalp vertex In lower face, sensory loss follow jawline and involves notch over the masseter muscle-functional On the trunk-sensory loss-ends short of midline-organic, splitting at midline-nonorganic In face-sensory loss may extend to midline-because of less midline overlap in face-organic or nonorganic. Splitting of vibration sense in midline-nonorganic, because frontal bone and mandible are single bone-so there should not be any difference in vibration sense on either side of mid-line. Response-upward jerk of mandible Pathways: erent arc is through sensory portion of mandibular division Aff of trigeminal nerve to muscle spindles of masseter muscle. In response to corneal stimulus, there is ipsilateral and contralateral blinking-direct and consensual reflex. Nucleus: Nucleus of spinal tract of trigeminal nerve and main sensory nucleus of V nerve. Corneomandibular reflex: Methods of elicitation: Corneal stimulation-produces Bilateral blinking of both eyes. Spectrum of corneal reflex-according to trigeminal nerve and f facial nerve lesion Lesion 1. Bilateral upper motor neuron lesion (pseudobulbar palsy) produces: Massive trigeminal motor paresis Exaggerated Jaw jerk Mastication is severely impaired. Lesions in pontine tegmentum due to involvement of main sensory nucleus of cranial nerve V: Trigeminal sensory neuropathy- producing numbness, paresthesia of half of the face, scalp, ear, tongue. Small left dorsolateral pontine infarct (involving principal sensory nucleus and pars oralis)-produces: Isolated orofacial sensory defect without any sensory deficit of limb and trunk. Hemimasticatory spasm: Sudden, brief spasm of jaw-Closing muscles (masseter, temporalis, and medial pterygoid) lasting for several minutes, with intense pain, aggravated by voluntary jaw closure and relieved by voluntary jaw opening. Involving the nucleus of spinal tract of trigeminal nerve extending from caudal end of pons to 3rd and 4th cervical spinal cord. Th If spinothalamic tract is involved due to close proximity of it with nucleus of spinal tract-it may produce: Contralateral anesthesia, thermoanesthesia and analgesia involving trunk and limbs. Caudal pontine lesion-involving rostral spinal trigeminal nuclei-produces: Diminution of intraoral sensation of all modalities, but facial sensation will be unimpaired. Isolated ventral pontine infarction-produces: Midfacial ipsilateral sensory loss due to involvement of fibers supplying midfacial areas Contralateral hemiparesis Dysarthria. Upper medullary spinal tract lesion-produces: Entire trigeminal cutaneous distribution will be affected. Lower medullary spinal tract lesion produces: Sensory loss in forehead, cheek and jaw (onion-skin pattern sensory loss) Onion-skin-segmental distribution reflects: Rostral-to-caudal somatotropic arrangement of cutaneous distribution of spinal nucleus-perioral area rostral and lateral face caudal area. Neurology 1009 Lateral medullary syndrome-involvement of spinal nucleus of trigeminal nerve. Features of cranial nerve V are: Facial pain Paresthesia Numbness Sensory loss Depressed corneal reflex Cranial nerve V motor function loss. There may be associated following structures involvement: Facial nerve paralysis Cerebellar ataxia-ipsilateral Nystagmus (due to involvement of cerebellar peduncle and cerebellum). Trigeminal neuralgia (tic douloureux): Sudden, lancinating, excruciating, paroxysmal unilateral pain in the distribution of one or more branches of trigeminal nerve. It occurs mostly in female, in advanced age, affects right side more than the left. The painful facial syndrome may occur due to any pathology affecting brainstem, preganglionic root, gasserian ganglion, peripheral trigeminal nerve. The irritating lesion at the entry zone of trigeminal nerve root- multiple sclerosis plaque, brainstem infarction, C-P angle tumor, cavernous malformation 1010 Clinical Methods and Interpretation in Medicine Meningioma, posterior fossa tumors. Brainstem displacement due to type-I Arnold-Chiari malformation or basilar invagination-producing compression of trigeminal nucleus. Lesions Affecting Gasserian Ganglion Lesions responsible for damage of gasserian ganglion: Tumor Sarcoidosis Tuberculosis Arachnoiditis Trauma Abscess. Pain is ipsilateral, severe, hemi-facial or along the distribution of selected branch, starting near midline on the upper lip, chin, progressing laterally to the ear. Bilateral trigeminal neuropathies along with bilateral abducens paralysis occur in Tangier disease. Bilateral trigeminal neuropathies (sensory) may occur in connective tissue disease due to vasculitis. Trigeminal sensory neuropathy can be distinguished from other conditions associated with facial numbness by following features: Sparing the muscles of mastication Frequent bilaterality Disregard the trigeminal boundaries Negative neuroimaging studies. Trauma to trigeminal nerve may occur-due to-blow in auriculotemporal area-produces complete sensory and motor trigeminal neuropathy. Neurology 1011 Site of lesion In the middle cranial fossa in the region between internal carotid artery and trigeminal ganglion near petrous apex. Clinical Features Ophthalmic division of trigeminal nerve: Pain and sensory disturbances in upper part of the face. Abducens nerve paralysis: Ipsilateral lateral rectus paralysis Oculosympathetic paresis: Miosis, Ptosis. Clinical Features Total unilateral ophthalmoplegia If tumor starts laterally: Oculomotor palsy If lesions starts from sella: Pain, paresthesia and sensory loss in the distribution of ophthalmic or maxillary division of trigeminal nerve. Superior Orbital Fissure Syndrome the following nerves pass through superior orbital fissure: Abducens Trochlear nerve Oculomotor nerve Ophthalmic division of trigeminal nerve. Lesions Affecting Peripheral Branches of Trigeminal Nerve Ophthalmic division of trigeminal nerve may be affected by-damage at middle cranial fossa at: Temporal bone apex Lateral wall of cavernous sinus Superior orbital fissure the face. In Neurology 1013 Maxillary division may be affected by: Lower lateral wall of cavernous sinus Foramen rotundum the pterygopalatine fossa In Floor of the orbit Infraorbital foramen On the face. Clinical Feature Numbness involves: One cheek, upper lip, medial and lateral incisor, canine teeth and adjacent gingival, spares posterior teeth and gum. Since distal branches of facial nerve are in close proximity to infraorbital branch of cranial nerve V, lesions in face mainly squamous cell carcinoma is associated with: Paresis of muscles of upper lip and angle of mouth Ipsilateral lower lid droop this is called Numb-cheek-limp-lid syndrome. Mandibular divison: It may be involved by damage of nerve at: Foramen ovale Zygomatic fossa Face. Numb Chin Syndrome Causes Systemic cancer: Lymphoretricular malignancy Carcinoma of breast and lung. Pattern of oral numbness: Numbness of incisor, canine and bicuspid teeth-due to involvement of incisive nerve-Distal lesion. Tongue numbness-unilateral or bilateral-due to: Temporal arteritis Ischemia of brainstem or lingual nerve. Neck Tongue Syndrome Sudden turning of head produces: Pain in upper neck and occiput Ipsilateral numbness of the tongue Lingual pseudoathetosis. Cause Due to irritation of 2nd cervical dorsal root, which also carries proprioceptive fibers through hypoglossal nerve. Periodic hemilingual numbness Due to intermittent compression of the lingual nerve by sialolithiasis. Lingual neuropathy: It involves-hemilingual sensory loss, pain, paresthesia, dysgeusia-due to: Wisdom teeth extraction Other dental procedure Surgery of mandibular ramus T-M joint displacement. Bilateral anterior lingual hypogeusia, hypoesthesia due to: Damage of lingual nerve Damage of chorda tympani branches of facial nerve-conveying taste sensation. They can be tested in following manner: Symmetry of temporal fossa and angle of jaw should be examined. Ask the patient to open his mouth against pressure below the chin given by you-Watch-Any weakness is present or not. You place your hands against the sides of the jaw and instruct the patient to push against it. In case supranuclear lesion: Deviation of jaw occurs towards the opposite side of lesion due to contralateral nucleus involvement.
Order levlen overnight
With associated diaphyseal or distal femur involvement birth control for menstrual cramps buy levlen 0.15 mg low cost, an intramedullary device is indicated in order to span the entire length of the femur. Severity of pain and site and size of the metastatic lesion affect risk of fracture. The Mirels system has been used to help predict the risk of pathologic fractures in weight-bearing bones within 6 months Table 126. Lesions with scores <6 can be treated with radiation; scores >8 should be treated with prophylactic internal fixation. The subtrochanteric segment of the femur extends from the lesser trochanter to the junction of the proximal and middle thirds of the diaphysis. This segment of the femur is subjected to very high axial loads of weight bearing and tremendous bending forces because of the eccentric load application to the femoral head. In the impending group, there was less blood loss (438 ml versus 636 ml), shorter hospital stays (7 days versus 11 days), greater likelihood of discharge home as opposed to an extended-care facility (79% versus 56%), and a greater likelihood of resuming supportfree ambulation (35% versus 12%). For diaphyseal lesions of the femur, the loads are less and the threshold for surgical stabilization is higher. Each case needs to be individualized, taking into consideration the degree of functional impairment, pain, and radiosensitivity of the tumor. The same size lesion in the diaphysis is less of a risk for fracture than in the subtrochanteric region. Recent work at our center on remineralization of bone following radiation may allow us to avoid surgical intervention in the appropriate candidate. Similar to proximal femoral lesions, intramedullary devices are used for fixation. In the case of an impending fracture, a distal vent should be used to allow efflux of marrow contents in order to reduce the risk of fat emboli. Reconstruction of the proximal part of the femur and the acetabulum is often technically demanding, and hardware failure is not uncommon. The implant is at risk of failure because the forces about the hip are extremely high for most normal activities. Where the acetabulum is structurally intact, a conventional total hip arthroplasty can be performed. When the medial wall has an unconstrained defect, techniques are required that transfer the stress of weight bearing away from the deficiency and onto the intact acetabular rim with use of a protrusion ring. Preoperative Embolization of Bone Metastases Metastases from renal cell carcinoma are hypervascular as a result of neovascularization. There is growing experience and evidence that preoperative embolization is a safe and reliable method of reducing intraoperative blood loss at the time of stabilization of bone metastases. The methods of embolization include the use of polyvinyl alcohol, coils, and gel foam. The procedure is performed in the angiography suite, and surgery should be performed within 48 to 96 hours of embolization or revascularization will occur. Comparing 8 patients who underwent perioperative embolization with 20 patients who did not, the blood loss during stabilization for former group averaged 940 ml compared with 1,975 ml in the nonembolized group. Upper Extremity In the upper extremity, the difference in management and patient outcome is less profound between an impending and pathologic fracture. Fractures of the humerus can be managed with plate fixation or with intramedullary devices. Spinal complications are due to loss of mechanical stability creating pain and spinal cord compression causing paralysis. Neurologic compression occurs due to direct tumor load in the epidural space or from a pathologic fracture causing boney compression or vertebral instability. The goals of spinal surgery in metastatic disease are to preserve or restore spinal stability for pain and to restore or protect neurologic function. Because of immunosuppression, poor nutritional status, and medical comorbidities, surgery to the spine may be associated with significant complications. Considerations in decision making are life span of the patient, general medical condition, number of spinal levels involved, age, cancer type, and radiation status. This study also quantified postoperative complication rates and identified significant risk factors that were associated with poor survival and outcome. Increasing age and primary lung cancer were significant risk factors for death within 30 days of surgery. For overall survival, each year of advancing age had a 1% increased risk of dying. The effect of a preoperative neurologic deficit on survivorship has been evaluated by a number of authors. We have shown that patients with preoperative neurologic deficits were 71% more likely to get a postoperative infection, likely from the administration of preoperative radiation. Other authors have likewise found increased infection rates and poorer outcomes following surgery in the presence of preoperative radiation. There were significant improvements in six other domains and trends toward improvement in another one. The major benefit of surgery occurs within the first month and remained stable until death or at least 6 months (length of follow-up). Principles of open surgical techniques and considerations are beyond the scope of this chapter. In general, tumor location within the vertebrae, spinal level, radiation status, neurologic deficit, and number of levels involved affect decision making. Rarely is decompression alone suitable for management of metastatic spinal cord compression. Unless there is solely posterior epidural disease, posterolateral decompression is required with pedicle screw stabilization. These are minimally invasive approaches and an alternative to open surgery for restoring stability to the spine. These same patients may not be suitable for invasive spinal surgery because of medical comorbidities, multilevel disease, or having a profound neurologic deficit. Systemic complications include embolic events due to marrow fat, tumor fragments, or cement entering the circulation. The use of biplanar fluoroscopy and "live" imaging during injection, the addition of increased concentration of barium to facilitate visualization, intraosseous venogram, limiting the volume of fill, gentle and slow injection, and the use of viscous cement are technical details that have been described to minimize the complications of this procedure. The vast majority of extrusions, however, are minor and do not result in neurologic sequelae. In some candidates with or without previous radiation or in the high-risk/poor surgical candidate with multiple-level disease, unifocal decompression can be performed and stabilized in this technique. This minimalistic approach is providing improved outcomes, allowing for greater numbers of patients to be operated on when previously the risks associated with multilevel fixations had unacceptable complication rates. Postoperative anteroposterior (C1) and lateral (C2) radiographs following open posterolateral decompression and vertebroplasty of T8 vertebra. Risk of complications from bone metastases in breast cancer: implications for management. Biomechanical assessment of stability in the metastatic spine following percutaneous vertebroplasty: effects of cement distribution patterns and volume. A study of the biological receptor activator of nuclear factor-kappa B ligand inhibitor, Denosumab, in patients with multiple myeloma or bone metastases from breast cancer. Extended efficacy and safety of denosumab in breast cancer patients with bone metastases not receiving prior bisphosphonate therapy. Denosumab compared with zoledronic Acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. Guidance on the use of bisphosphonates in solid tumours: recommendations of an international expert panel. American Society of Clinical Oncology clinical practice guideline update on the role of bone-modifying agents in metastatic breast cancer. International myeloma working group recommendations for the treatment of multiple myeloma-related bone disease. The palliation of symptomatic osseous metastases: final results of the study by the Radiation Therapy Oncology Group. Update of the international consensus on palliative radiotherapy endpoints for future clinical trials in bone metastases.
Trusted 0.15mg levlen
This area also extends beyond the posterior extent of calcarine fissure and extends up to 1 cm around posterolateral aspect of occipital pole birth control pills questions and answers levlen 0.15 mg with mastercard. This is the primary visual area-the other name of area 17 is striate cortex-this is very rich in granular cells. Superior lip receiver the fibers from superior retinal projection and inferior retinal projections are received by inferior lip. Extreme peripheral part of retina is represented anteriorly by the junction of parieto-occipital fissure and calcarine fissure. Posterior ciliary arteries-supply-by forming vascular arcades around globe: Outer layer of retina including photoreceptor Choroid. Posterior ciliary artery gives: One or more ciliospinal arteries-they supply macular region and papillomacular bundle. Occlusion of one branch of central retinal artery gives rise to altitudinal visual field defect. Causes of central retinal artery obstruction are: Emboli rombus Th Hypercoagulability state Migraine Giant cell arteritis. The differentiation between obstruction of central retinal infarction and posterior ciliary artery infarction: Presence of edema in optic disc in acute stage of central retinal artery infarction. Location of lesions in visual pathways Detailed qualitative testing allows: Detection of subtle defect, which can be escaped during bedside testing Exact shape of visual field defect Quantification of extent intensity of defect. Neurology 979 Lesion in visual pathways produces: Defect in visual acuity Impaired colored perception Contrast discrimination-Impaired discrimination of objects having little contrast with the background Visual field defect. Changes in visual perception Visual acuity: It is the discrimination of the details of high contrast. Subnormal value reflects: Fault in visual system (optic faults, retinal lesions, visual pathways lesion) Faulty foveation (defect in eye motility) Poor co-operation. Most common cause of impaired visual acuity is-refractory changes in eye-Patient with refractory changes can be tested with pin hole (Pin hole test)-this maneuver restricts the vision to central beam of light. Bed side of visual acuity test: By Snellen optotypes-this card should be well-illuminated and the distance between chart and eye should by 14 inches. Lesions responsible are: Compressive and noncompressive lesions of optic nerve-it produces drop in visual acuity before visual field defect will be detected. Medial chiasmal lesion Lateral chiasmal lesion-it produces impairment of visual acuity in ipsilateral eye only. If crossed and uncrossed fibers from fovea will be affected by medial chiasmal lesion. Visual acuity is unaffected if lateral geniculate body, optic tract, optic radiation and visual cortex are affected. Contrast sensitivity: Contrast sensitivity testing detects subtle visual field defect in macula, optic nerve and optic chiasma, even when visual acuity testing is normal. Perception color: Color perception is impaired in the areas of visual field which corresponds to partial visual field defect. Color vision can be tested by following methods: Ask the patient to identify which one of the identically bright red objects is more red. In case of lesion in visual pathways-the red object becomes In orange to yellow even colorless-according to the severity of the disease. Th Since optic nerve and optic chiasma lesion involved macular fibers-so color vision may be defective on the side of lesion-when mono-ocular reading of ishihara chart is being done. Usually color vision defect runs parallel to visual acuity loss in ischemic optic neuropathy. Flight of colors perception phenomenon: Succession of color impression that follows shining a bright light into the eye. Visual Field Defect Lesion in optic pathways can be localized by: Shape Distribution of visual field. The unco-operative patient may be: Inattentive Disturbances in alertness Disturbances in mentation. Visual field can be tested by: Bedside confrontation perimetry Tangent (Bjerrum) screen Static or kinetic perimetry. The lesions are: Retinal detachment Tapetoretinal disorder Anterior visual cortex lesion. During visual field testing, following disorders should be taken into account: Shadowing facial contours: Eyebrows Nose. Ptosis 982 Clinical Methods and Interpretation in Medicine Left Right visual visual field field Left Right visual visual field field Right upper quadrant Visual field of left eye What is observed by the left eye Error of refraction: Ametropia Presbyopia Both ametropia and presbyopia Uncorrected astigmatism-it may cause temporal depression Spherical ametropia-it may cause generalized visual field depression, occasional temporal depression, which may run under blind spot. Neurology 983 Scotoma Localized area of poor vision surrounded by normal vision-it is called scotoma. Physiological scotoma Blind spot: Image of optic nerve over the visual field is called blind spot-it cannot be perceived because it lacks in representation in brain. Image of retinal vessel-superficial on underlying retina-called angioscotoma-it can be noted in certain circumstances. For testing left visual field, patient must cover his right eye and examiner must cover his left eye. A red object is better for this aspect of visual filed testing, as red color desaturation is a marker of lesion in visual pathways. Graying of vision or color desaturation may be noted prior to quantify the visual field defect. Central vision can be detected by utilizing 5 mm white disc attached to rod or long pin. Explain the patient that the object will disappear briefly then reappear and that the patient should indicate when this happens. If there is visual inattention in one field and fingers are moved simultaneously, patient will not perceive the finger subserving the damaged component in visual pathway. If objects of different sizes are used-patient can detect larger object in same sector of visual field where smaller object cannot be seen in that sector of visual filed-this defect is partially caused by edema or pressure phenomena. Constricted visual field can be detected by testing the visual field by small objects (2 mm). Small deep retinal lesions: Discrete defects localized to the point of lesion, nerve fiber layer is unaltered. It gives rise to fan-shaped arcuate defect-with its tip pointing toward the lesion and base fanning peripherally towards the nasal horizontal meridian. Arcuate If shape defect is due to disposition of nerve fiber layer of temporal side is arcuate in course. Straight course of nasal fibers towards nerve head are responsible for sector defect.
Discount levlen 0.15 mg
Increased plasma levels of adipokines in preeclampsia: relationship to placenta and adipose tissue gene expression birth control pills perimenopause purchase online levlen. Adiponectin concentrations in maternal serum: elevated in preeclampsia but unrelated to insulin sensitivity. Circulating highmolecular-weight adiponectin is upregulated in preeclampsia and is related to insulin sensitivity and renal function. Selective increase in high molecular weight adiponectin concentration in serum of women with preeclampsia. A promoter genotype and oxidative stress potentially link resistin to human insulin resistance. A cysteine-rich adipose tissue-specific secretory factor inhibits adipocyte differentiation. Fasting serum triglycerides, free fatty acids, and malondialdehyde are increased in preeclampsia, are positively correlated, and decrease within 48 hours post partum. Increased lipolytic activity and high ratio of free fatty acids to albumin in sera from women with preeclampsia leads to triglyceride accumulation in cultured endothelial cells. Lipoprotein subfraction concentrations in preeclampsia: pathogenic parallels to atherosclerosis. Serum lipoproteins, insulin, and urinary prostanoid metabolites in normal and hypertensive pregnant women. Plasma factors that determine endothelial cell lipid toxicity in vitro correctly identify women with preeclampsia in early and late pregnancy. Fasting serum free fatty acids and triglycerides are increased before 20 weeks of gestation in women who later develop preeclampsia. Variation in lipid levels during pregnancy in women with different types of hypertension. Low-density lipoprotein particle size decreases during normal pregnancy in association with triglyceride increases. Prepregnancy cardiovascular risk factors as predictors of pre-eclampsia: population based cohort study [see comment]. Hypertriglyceridemia and its metabolic consequences as a risk factor for atherosclerotic cardiovascular disease in non-insulin-dependent diabetes mellitus. Association of small low-density lipoprotein particles with the incidence of coronary artery disease in men and women. Small, dense low-density lipoprotein particles as a predictor of the risk of ischemic heart disease in men. Fasting insulin and apolipoprotein B levels and low-density lipoprotein particle size as risk factors for ischemic heart disease. Hypertriglyceridemia during late pregnancy is associated with the formation of small dense low-density lipoproteins and the presence of large buoyant high-density lipoproteins. Elevated serum vascular endothelial growth factor is associated with visceral fat accumulation in human obese subjects. Midpregnancy levels of angiogenic markers in relation to maternal characteristics. Uric acid and diet-insights into the epidemic of cardiovascular disease [comment]. Uric acid and coronary heart disease risk: evidence for a role of uric acid in the obesity-insulin resistance syndrome. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hyperuricemia induces a primary renal arteriolopathy in rats by a blood pressureindependent mechanism. Molecular identification of a danger signal that alerts the immune system to dying cells. Uric acid heralds ischemic tissue injury to mobilize endothelial progenitor cells. Uric acid is as important as proteinuria in identifying fetal risk in women with gestational hypertension [see comment]. Uric acid concentrations in early pregnancy among preeclamptic women with gestational hyperuricemia at delivery. Relationship between obesity, smoking, and the endogenous nitric oxide synthase inhibitor, asymmetric dimethylarginine. The emerging role of asymmetric dimethylarginine as a novel cardiovascular risk factor. Acute elevations of plasma asymmetric dimethylarginine and impaired endothelial function in response to a high-fat meal in patients with type 2 diabetes. Asymmetric dimethylarginine, derangements of the endothelial nitric oxide synthase pathway, and cardiovascular diseases. Suppression of endothelial progenitor cells in human coronary artery disease by the endogenous nitric oxide synthase inhibitor asymmetric dimethylarginine [see comment]. Endothelial dysfunction and raised plasma concentrations of asymmetric dimethylarginine in pregnant women who subsequently develop pre-eclampsia. Elevated asymmetric dimethylarginine concentrations precede clinical preeclampsia, but not pregnancies with small-for-gestational-age infants. C4 deficiency state in antiphospholipid antibody-related recurrent preeclampsia evolving into systemic lupus erythematosus. Death rates from ischemic heart disease in women with a history of hypertensionin pregnancy. Long term mortality of mothers and fathers after pre-eclampsia: population based cohort study. Preeclampsia and risk of cardiovascular disease and cancer in later life: systematic review and meta-analysis [see comment]. Impairment of endothelial function in women with a history of preeclampsia: an indicator of cardiovascular risk. Microvascular dysfunction: a link between pre-eclampsia and maternal coronary heart disease. Haemostatic, endothelial and lipoprotein parameters and blood pressure levels in women with a history of preeclampsia. Pre-eclampsia: contribution of maternal constitutional factors and the consequences for cardiovascular health. Short- and long-term changes in plasma inflammatory markers associated with preeclampsia [see comment]. The short- and long-term implications of maternal obesity on the mother and her offspring. Pregnancy complications and subsequent maternal cerebrovascular events: a retrospective cohort study of 119,668 births. A link among preeclampsia, recurrent pregnancy loss, and future cardiovascular events? Shared constitutional risks for maternal vascular-related pregnancy complications and future cardiovascular disease. Learning from the placenta: acute atherosis and vascular remodeling in preeclampsia-novel aspects for atherosclerosis and future cardiovascular health. An ultrastructural study of uteroplacental spiral arteries in hypertensive and normotensive pregnancy and fetal growth retardation. Increased contents of phospholipids, cholesterol, and lipid peroxides in decidua basalis in women with preeclampsia. Moderate hyperhomocysteinemia decreases endothelial-dependent vasorelaxation in pregnant but not nonpregnant mice. A new animal model for human preeclampsia: ultralow-dose endotoxin infusion in pregnant rats. Moderate ascorbate deficiency increases myogenic tone of arteries from pregnant but not virgin ascorbatedependent rats. Adipose tissue metabolism in pregnancy: the lipolytic effect of human placental lactogen. Hypoxia regulates the expression of fatty acid-binding proteins in primary term human trophoblasts. Paracrine regulation of angiogenesis and adipocyte differentiation during in vivo adipogenesis. Dysmetabolic syndrome, placenta-mediated disease and future risk of cardiovascular disease. Lipid and lipoprotein concentrations in pregnancies complicated by intrauterine growth restriction. He further noted that Dienst had suggested incompatibility of maternal and fetal blood groups in 1905 (edition 1 p.
Buy levlen with a visa
The role of progesterone metabolism and androgen synthesis in renal blood pressure regulation birth control for the arm buy discount levlen 0.15mg on-line. Metabolism of deoxycorticosterone and deoxycorticosterone sulfate in men and women. Increased conversion of plasma progesterone to deoxycorticosterone during estrogen treatment of women pregnant with a dead fetus. Conversion of plasma progesterone to deoxycorticosterone in men, nonpregnant and pregnant women, and adrenalectomized subjects. Deoxycorticosterone biosynthesis in human kidney: potential for formation of a potent mineralocorticoid in its site of action. Longitudinal study of the reninangiotensin-aldosterone system in hypertensive pregnant women: deviations related to the development of superimposed preeclampsia. Increases in plasma atrial natriuretic peptide concentration antedate clinical evidence of preeclampsia. Atrial natriuretic peptide in preeclampsia: metabolic clearance, sodium excretion and renal hemodynamics. Pregnant rats are refractory to the natriuretic actions of atrial natriuretic factor. The natriuretic and diuretic response to dopamine is maintained during rat pregnancy. Sildenafil citrate therapy for severe early-onset intrauterine growth restriction. Aldosterone, maternal volume status and healthy pregnancies: a cycle of differing views. Vascular endothelial growth factor-A and aldosterone: relevance to normal pregnancy and preeclampsia. Angiotensin receptor agonistic autoantibody-mediated soluble fms-like tyrosine kinase-1 induction contributes to impaired adrenal vasculature and decreased aldosterone production in preeclampsia. Direct evidence for a 1-adrenergic receptor-directed autoimmune attack as a cause of idiopathic dilated cardiomyopathy. Endovascular trophoblast invasion, spiral artery remodelling and uteroplacental haemodynamics in a transgenic rat model of pre-eclampsia. Autoantibody-mediated angiotensin receptor activation contributes to preeclampsia through tumor necrosis factor-alpha signaling. Hypertension in response to placental ischemia during pregnancy: role of B lymphocytes. Involvement of functional autoantibodies against vascular receptors in systemic sclerosis. A novel fluorescence method for the rapid detection of functional beta1-adrenergic receptor autoantibodies in heart failure. Value of posttransplant antibody tests in the evaluation of patients with renal graft dysfunction. In earlier editions, this subject was relegated to the chapter on volume homeostasis, but as a true kidney function it has found its way home, chapter-wise! This procedure, already quite restricted indication-wise in pregnant women when discussed in the previous edition, appears even more so as of 2014, probably reflecting the ever-improving technology of non-invasive testing. The marked decline in performing renal biopsies in suspected preeclamptics following the large series that appeared during the last few decades of the 20th century is important to appreciate. That is, interpretive dilemma or misinformation is more likely to appear when the biopsy process focuses more and more on atypical or complicated preeclampsia. This point, already noted in our comments in the previous edition, underscores the importance of the older, larger and extensive series, as well as the signal work of Sheehan and Lynch. The late Harrold Sheehan, then near his 80th year, published an article comparing the value of this autopsy material to renal biopsy descriptions in preeclamptic women, an article that bears reading. One of his earliest contributions was a formula for calculating urea clearance at low urine flow rates. Indeed, his description of renal physiology and pathophysiology of pregnancy in the first edition of this book was encyclopedic in scope. Familiarity with the changes in maternal renal and cardiovascular physiology as well as osmoregulation and volume homeostasis during normal pregnancy is prerequisite to complete understanding, proper diagnosis, and medical management of preeclampsia. General cardiovascular and volume alterations in normal pregnancy are reviewed elsewhere in this book (Chapters 14 and 15). Here, the alterations in renal hemodynamics, glomerular filtration, and osmoregulation during normal pregnancy will be considered first. Then, the dysregulation of renal hemodynamics and glomerular filtration occurring in preeclampsia will be addressed. Although filtration, reabsorption, and excretion of many solutes change in pregnancy, only the renal handling of uric acid and of proteins will be presented here because of their special clinical significance to preeclampsia. Last, we discuss the pathology of the kidney in preeclampsia with focus on its characteristic lesion, glomerular endotheliosis. The kidneys contribute to this reduction in total systemic vascular resistance in a major way. Indeed, the nadir in renal and systemic vascular resistances and peak in renal blood flow, glomerular filtration and cardiac output coincide, and are attained by the end of the first or beginning of the second trimester. The early gestational rise in cardiac output occurs well before major increases in absolute uteroplacental blood flow, and oxygen and nutrient demands of the nascent fetus and placenta. This temporal dissociation is reflected by the oxygen content difference between arterial and mixed-venous blood, which narrows during early pregnancy in both humans and rats. On the other hand, increasing urine flow rate by initiating a water diuresis is an acceptable and effective means to minimize urinary tract dead space error. The reason for this reciprocal relationship is that production of creatinine by skeletal muscle changes little during gestation and since glomerular filtration increases, plasma levels must fall. Although renal handling of urea is more complicated, it is freely filtered like creatinine; consequently, plasma levels are also lower during pregnancy, again primarily because renal clearance of urea is increased. All values during pregnancy are significantly different from those obtained during the midfollicular phase of the cycle before pregnancy. Creatinine undergoes glomerular filtration, and a small degree of proximal tubular secretion, but plasma levels are overestimated because of the presence of a chromagen, which is unavoidably detected in the assay along with creatinine. The authors concluded that in late gestation when a subject assumes a supine position, the enlarged uterus compresses the great veins, which in turn impairs venous return, decreasing both cardiac output and renal perfusion. Solid line, mean; stippled area, range for nine women with normal pregnancy outcomes. Two women designated by the thin and dashed lines had uncomplicated spontaneous abortions. In what appears to be the only comprehensive study of the last few weeks of pregnancy immediately before delivery that we could find, Davison et al. An attractive and plausible theory is that the altered hormonal environment is causal. Unfortunately, so many hormones change during pregnancy that it has been difficult to know which ones to investigate first. Although decrements in plasma oncotic pressure particularly during late pregnancy and increases in Kf especially during early pregnancy may contribute, there was no evidence for alterations in the transglomerular hydrostatic pressure. The mathematical formulae used can skew the results when very small measurement errors occur. Such errors are most likely to occur when values entered into the equation are obtained indirectly, the case here. Thus, the same chronically instrumented, conscious rats were serially examined before, 339 during, and after gestation. Thus, the gravid rat has been extensively investigated to determine the mechanisms underlying these remarkable changes in the renal circulation during pregnancy. Plasma Volume Expansion Pregnancy is accompanied by tremendous expansion of extracellular and plasma volume (see Chapter 15). Thus in one study of humans and a second in baboons, increases in plasma volume and left atrial or left ventricular end diastolic dimensions indicative of plasma volume expansion lagged behind the decline in systemic vascular resistance. Most instances of chronic volume expansion occurring in nature, other than pregnancy of course, result from pathology such as congestive heart failure or cirrhosis in which renal function is often reduced rather than elevated. Pseudopregnancy Study of the renal circulation in rats that become pseudopregnant may provide insights into the mechanisms contributing to renal vasodilatation and hyperfiltration of pregnancy. This finding may shed light on the mechanisms underlying renal vasodilatation and hyperfiltration of pregnancy, because several hormones that increase in the luteal phase also rise during early gestation.
Syndromes
- Stupor (lack of alertness)
- Treatments such as hemodialysis or the use of the heart-lung bypass machine
- Arrive at the hospital on time.
- Thirst
- Pain medications
- Lab tests to check for certain proteins (enzymes) and metabolic problems
Buy genuine levlen online
The diagnostic evaluation in patients with impaired cellular immunity and pulmonary infiltrates is similar to neutropenic patients birth control cost order levlen 0.15 mg fast delivery. Typically, broad-spectrum antibiotics for community-acquired pneumonia requiring hospitalization (see previous discussion) will be started, ideally after obtaining respiratory samples for diagnosis. Dissemination may include brain abscess, meningitis, osteomyelitis, soft tissue mass, cutaneous abscess, and liver abscess. It is important to alert the microbiology laboratory when nocardiosis is suspected so that a modified acid stain is performed and that appropriate culture conditions are used and culture plates are held for weeks instead of days. The most common radiographic findings are bilateral interstitial infiltrates, although unilateral or patchy infiltrates are also observed. Immunofluorescent staining using mAbs is more sensitive than silver staining or Wright-Giemsa staining. Because of neutropenia, physical findings of consolidation and sputum production may be absent. Cavitation usually coincides with neutrophil recovery and does not indicate treatment failure. A new or progressive infiltrate developing while on broad-spectrum antibacterial agents in patients with prolonged neutropenia raises the concern about invasive mold infection, and makes the need for definitive diagnosis more pressing. In patients at risk for invasive mold diseases, a serum galactomannan and -D-glucan may be considered, although the interpretation of a single value of these tests (as opposed to trends) may be difficult. For focal lesions such as nodules, the diagnostic yield is much lower (15% to 50%), and a percutaneous biopsy may be a better diagnostic choice. Video-assisted thoracic surgery has been used successfully in cases with diffuse involvement and with peripheral lesions. Open lung biopsy is the definitive diagnostic method, and it also allows for easier visualization and control of bleeding. Treatment Besides the standard antimicrobials used for fever and neutropenia, we include a macrolide or fluoroquinolone to treat Legionella and agents of atypical pneumonia. Depending on the clinical scenario and preexistent antifungal prophylaxis, we may add voriconazole or a Practice of oncology 1950 Practice of oncology / Management of Adverse Effects of Treatment figure 132. A patient with chronic lymphocytic leukemia developed fever, hypoxemia, and shortness of breath soon after tapering a prednisone course for hemolytic anemia. He was receiving inhaled pentamidine as Pneumocystis jirovecii pneumonia prophylaxis. In patients who are not responding to therapy, repeat bronchoscopy should be considered to exclude additional pathogens. Postobstructive Pneumonia and Pleural Effusion There are no professional guidelines or professional society guidance statements on the indication for airway stenting to relieve malignant obstruction. There are no outcomes reported in sufficiently large series to answer the question as to whether the risk and consequence of infection outweigh the benefit of the relief of obstruction. Retrospective series suggest that stenting is followed by infection with moderate frequency and (predominantly P. A similar lack of controlled data is present in the evaluation of intrapleural catheters placed for the relief of malignant pleural effusion, although infection as a complication seems to be infrequent. Latent infection persists in B cells and produces no disease in the vast majority of people. The lesions may be composed of polyclonal or monoclonal populations of transformed B cells. Patients may have a mononucleosis-like syndrome with fever and localized adenopathy. Oropharyngeal Infections Oropharyngeal infections in patients with cancer usually result from the combination of neutropenia and mucositis. The distinction of chemotherapy-induced mucosal erosions and superimposed infection is difficult. Oral mucosal candidiasis may present with typical thrush, but also with erosions and erythema; diagnosis is made by a wet mount or Gram stain preparation showing pseudohyphal forms (the culture is not of diagnostic value because Candida spp. Severe local bacterial infection may occur with spread to adjacent tissue structures and bacteremia. The antibacterial regimen should cover both common oral flora (gram-positive bacteria and anaerobes) and hospital-acquired gram-negative bacilli. Anorectal Infections Anorectal infections may be life-threatening in patients who are receiving repeated courses of cytotoxic chemotherapy. Once anorectal infection is established, fascial extension to the external genitalia, pelvic floor, retroperitoneum, and peritoneal cavity may occur. Anorectal infections, with or without extensive regional spread, may lead to bacteremia. The most common pathogens in neutropenic patients are Enterobacteriaceae, anaerobes, enterococci, and P. Candida esophagitis is probably most common, but more than one infection may be present. Radiation therapy to the chest and chemotherapy-induced mucositis may produce an erosive esophagitis that is clinically indistinguishable from infection. In the setting of concurrent neutropenic fever, appropriate broad-spectrum antibacterial agents should of course be added. Esophagitis may be complicated by bacteremia by predominantly gram-positive pathogens (viridans group streptococci, S. Distended cecum Neutropenic Enterocolitis (Typhlitis) Typhlitis ("inflammation of the cecum") results from a combination of neutropenia and defects in the bowel mucosa related to figure 132. The computed tomographic scan shows edema of the cecal wall and "stranding" of pericolic fat in a neutropenic patient with fever and abdominal pain. Practice of oncology gastrointestinal tract and abdominal infections cytotoxic chemotherapy. Patients receiving chemotherapy for acute leukemia are at highest risk, but it is also observed in patients with solid tumors receiving taxanes. Suggestive signs include fever, abdominal pain and tenderness, and radiologic evidence of right colonic inflammation. Nausea, vomiting, and diarrhea (sometimes bloody) are the most common associated symptoms. Disease may be limited to the cecum, but more extensive involvement of the large bowel and terminal ileum may occur (neutropenic enterocolitis). The indications for surgery must be individualized, but include (1) persistent gastrointestinal bleeding after resolution of neutropenia, thrombocytopenia, and clotting abnormalities; (2) perforation; (3) uncontrolled sepsis despite fluid and vasopressor support; and (4) an intra-abdominal process (such as appendicitis) that would require surgery in the absence of neutropenia. Therefore, serial examinations of the perianal region are necessary, looking for point tenderness and poorly demarcated induration. Among neutropenic patients, perianal infections are common and are usually managed medically, whereas perirectal infections are uncommon and often warrant surgical intervention. Visual inspection should assess for the presence of perianal fissures, fistulas, cellulitis, and induration. Most cases of anorectal infections can be managed with appropriate broad-spectrum antibiotics and supportive measures without surgical intervention. Intrathecal administration of antibiotics has some chance of success but should be used with caution when the infecting organism is virulent (S. Encephalitis may manifest with signs and symptoms of meningeal inflammation, but is distinguished by the predominance of alterations of consciousness and neurologic deficits. In neutropenic patients, we add fungal culture, -D-glucan, and galactomannan antigen. A reasonable empirical regimen for suspected bacterial meningitis in patients with cancer is ceftriaxone plus ampicillin plus vancomycin. This regimen will cover common causes of bacterial meningitis, including penicillin-resistant pneumococci and listeriosis. Mycobacterial culture has low yield and take many days or weeks, but should be obtained. Professional guidance does exist for esophageal and upper gastrointestinal malignant obstruction. Prior manipulation (endoscopic retrograde cholangiopancreatogram) and incomplete drainage are the most consistently identified risk factors. As such, the dominant infectious events, which have been reported in >10% of cases, are related to contamination at placement or access.
Discount levlen 0.15 mg amex
However birth control 1 order 0.15mg levlen fast delivery, more effective treatments are emerging, notably the angiogenesis inhibitors in renal cell cancer, and the emergence of a range of targeted treatments for patients with specific mutations. Bisphosphonates for Metastatic Bone Disease Over the past 15 years, bisphosphonates have become established as a valuable additional approach to the range of current treatments. Bisphosphonates are analogues of pyrophosphate, characterized by a phosphorus-carbon-phosphoruscontaining central structure that binds to bone and a variable side chain that determines the relative potency, side effects, and the precise mechanism of action. After intravenous administration of a bisphosphonate, the kidney excretes approximately 25% to 40% of the injected dose, and the remainder is taken up by bone where it is retained for months or even years. All bisphosphonates suffer from poor bioavailability when given by mouth and must be taken on an empty stomach, as they bind to calcium in the diet. It is generally accepted that osteoclast activation is the key step in the establishment and growth of bone metastases. Biochemical data indicate that bone resorption is of importance not only in classic "lytic" diseases such as myeloma and breast cancer, but also in prostate cancer. Chemotherapy, biologically targeted agents, and endocrine treatments have direct antitumor effects, whereas agents such as the bisphosphonates and denosumab are effective by preventing host cells (primarily osteoclasts) from reacting to tumor products. In general, the choice of systemic treatment for metastatic bone disease is based on the same criteria as those used for other metastatic manifestations of the malignancy. Objectively responding patients usually gain relief of symptoms (including bone pain) and might become able to resume their previous activities. Although in general the median duration of response to endocrine therapy is around 15 months, prolonged responses to first-line hormone treatments lasting several years are not uncommon in patients with bone metastases. There have been many recent developments in cytotoxic and biologic treatments of relevance to the patient with metastatic bone disease from breast cancer. Response in bone to chemotherapy is nearly always only partial, with a median duration of response of 9 to 12 months. Chemotherapy can be more hazardous for patients with extensive bone disease, because of both poor bone marrow tolerance after replacement of functioning marrow by tumor and the effects of previous irradiation. Primary prophylaxis with hematopoietic growth factors may be required to enable chemotherapy to be administered safely. In prostate cancer, at least 80% of prostate tumors exhibit some degree of hormone responsiveness with a median duration of response of around 2 years. Until recently, treatment to extend oral Bisphosphonates the absorption of bisphosphonates from the gut is poor, variable, and dramatically inhibited by food intake. Nevertheless, oral clodronate and ibandronate have been shown in randomized trials to have useful efficacy in breast cancer. Following a single subcutaneous dose, denosumab caused rapid and sustained suppression of bone turnover in patients with multiple myeloma and patients with breast cancer. However, no differences in overall survival or investigator-reported disease progression were found between the two treatment groups in any of the studies. Denosumab does not adversely affect renal function, eliminating the need for routine monitoring of renal function. Acute-phase reactions are also less common with denosumab, but hypocalcemia is more frequent. As with intravenous bisphosphonates, the most important adverse event associated with denosumab in the oncology setting is osteonecrosis of the jaw. This occurs with similar frequency in patients treated with denosumab or zoledronic acid, affecting 0. These include radium-223, inhibitors of cathepsin K, an osteoclast-derived enzyme that is essential for the resorption of bone, and Src kinase, a key molecule in osteoclastogenesis. Radium-223 is a calcium mimetic that preferentially targets bone metastases and emits high-energy alpha particles resulting in highly localized cytotoxic effects with minimal myelosuppression. Numerous randomized trials have been conducted on dose-fractionation schedules of palliative radiotherapy. Despite that, there is still no uniform consensus on the optimal dose fractionation scheme. One of the first randomized studies on bone metastases was conducted by Radiation Therapy Oncology Group (74-02). The trial concluded that the low-dose, short-course schedules were as effective as the high-dose protracted programs. A reanalysis of the same set of data, grouping solitary and multiple bone metastases, using the end point of pain relief and taking into account of analgesic intake and retreatment, concluded that the number of radiation fractions was statistically significant related to complete combined relief (absence of pain and use of narcotics). The conclusion was that protracted dose-fractionation schedules were more effective than short-course schedules. It is currently impossible to predict whether an individual patient needs or will benefit from a bisphosphonate. Because of the logistics and cost of delivering monthly treatments to all patients with metastatic bone disease, certain empiric recommendations on who should receive treatment are needed. The recent guidelines on the management of metastatic bone disease in breast cancer from the American Society of Clinical Oncology did not recommend one bone-modifying agent (zoledronic acid, pamidronate, denosumab) over another. Denosumab or zoledronic acid is appropriate for patients with endocrine-resistant metastatic bone disease from prostate cancer,25 whereas zoledronic acid or pamidronate are recommended for multiple myeloma. The United Kingdom Bone Pain Trial Working Party randomized 765 patients with bone metastases to either an 8-Gy single fraction or a multifraction regimen (20 Gy in 5 fractions or 30 Gy in 10 fractions). There were no significant differences in the incidence of nausea, vomiting, spinal cord compression, or pathologic fracture between the two groups. The study concluded that a single 8 Gy is as safe and effective as a multifraction regimen for the palliation of metastatic bone pain for at least 12 months. The Dutch Bone Metastases Study included 1,171 patients and found no difference in pain relief or the quality of life following a single 8-Gy or 24-Gy dose in six daily radiation treatments. In the cost-utility analysis of this randomized trial, there was no difference in life expectancy or quality-adjusted life expectancy. The estimated cost of radiotherapy, including retreatments and nonmedical costs, was statistically significantly lower for the single-fraction schedule than for the multiple-fraction schedule. However, two earlier meta-analyses showed no significant difference in complete and overall pain relief between single-fraction and multifraction palliative radiotherapy for bone metastases. Most patients will experience pain relief in the first 2 to 4 weeks after radiotherapy, be it single or multiple fractionations. The Radiation Therapy Oncology Group repeated the randomized study in patients with breast or prostate cancer who had one to three sites of painful bone metastases and moderate to severe pain with patient self-assessment. Grade 2 to 4 acute toxicity was more frequent in the multiple arms (17%) than in the single arm (10%) (p = 0. Complete and partial response rates were 15% and 50%, respectively, in the single-fraction arm compared with 18% and 48%, respectively, in the multiplefractions arm (p = 0. Four Norwegian and six Swedish hospitals planned to recruit 1,000 patients with painful bone metastases. Similar pain relief within the first 4 months was experienced in both groups and this was maintained throughout the 28-week follow-up. No differences were found for fatigue, global quality of life, and survival in both groups. An updated meta-analysis reporting 25 randomized trials totaling 2,818 and 2,799 randomizations in single-fraction and multiple-fraction arms revealed the overall and complete response rates were 60% and 23%, respectively, in single-fraction arm versus 61% and 24%, respectively, in multiple-fraction arms, again demonstrating equal efficacy. They concluded that a single dose was not as effective as multiple fractions for the treatment of neuropathic pain; however, it was also not significantly worse. They recommended that 20 Gy in five fractions be used as standard radiotherapy for patients with neuropathic pain. However, in patients with short survival, poor performance status, where the cost/inconvenience of multiple treatments was a factor, and in treatment centers with lengthy wait times, single fractions could be used instead. The answer most likely resides within the clinical circumstances and individual wishes of each patient. There is no doubt that in patients with short life expectancy, protracted schedules are a burden. However, in patients with a longer expected survival, such as patients with breast cancer and patients with prostate cancer with bone metastases only, other parameters need to be taken into account. Because retreatment rates are known to be higher following a single versus multiple fractions, about 25% versus 10%, respectively, patients with good performance status may wish to share in the decision-making process.
Buy cheap levlen on line
Preeclampsia and subsequent cardiovascular disease: villain or innocent bystander? Effectiveness-based guidelines for the prevention of cardiovascular disease in women 2011 update: a guideline from the American Heart Association birth control pills loestrin levlen 0.15mg online. Physiologic and supraphysiologic increases in lipoprotein lipids and apoproteins in late pregnancy and postpartum. Chesley had a chapter devoted to this topic in his first edition and he would have been delighted by some of the novel twists that have occurred in this important area. Importantly, during human pregnancy, there is a ~12 kg weight gain, as well as a 3050% increase in extracellular fluid, plasma, blood volume, and total body water. Also striking is a resetting of the thresholds for vasopressin secretion and thirst, plasma osmolality averaging 10 mOsm below nonpregnant levels (see Chapter 16). Therefore, pregnancy is a sensitive state relying on a multifactoral autoregulation of blood pressure control mechanisms and body fluid volume homeostasis. Although these autoantibodies have been linked to poor placentation and abnormal renal function, their role in the hypertensive state of preeclampsia has yet to be fully elucidated. Resolving the ongoing debate concerning the cause of the increased plasma volume (does it represent "underfill," "overfill," or "normal fill"? Finally, evolving thoughts regarding treating preeclampsia with sodium loading or plasma volume expansion, a challenging view, were revisited in light of the recent discovery of genetic mutations leading to inefficient aldosterone production in preeclampsia. Contrarily, the possible presence of ouabain-like factors in animal models and women with preeclampsia is also noted. If preeclampsia is the "disease of theories," one of the most far-fetched of these is that agonistic autoantibodies may participate as direct mediators of increased vascular sensitivity and may induce alterations in volume homeostasis. The role of agonistic autoantibodies in Graves disease is well established and, increasingly, circulating immunoglobulins have been associated with hypertension. When these were observed in a hypertensive woman with a history of preeclampsia, it prompted a cohort investigation for such antibodies in archived sera from preeclamptics. The epitope shows signaling events in vascular smooth muscle cells and trophoblasts that could contribute to the development and signs of preeclampsia. The seemingly bizarre concept that circulating agonistic antibodies might mediate vasospasm in preeclampsia stemmed from a serendipitous observation in a single patient. What has evolved in the past decade is an integrated framework of observations that fits into the concept of faulty angiogenesis as a precursor for phenotypic preeclampsia. Autoantibodies that stimulate G protein-coupled receptors have long been accepted as causing diseases of the thyroid gland. Autoantibodies directed against specific epitopes in the insulin receptor exist, but these only rarely cause recurrent hypoglycemia and a severe form of insulin resistance (type B insulin resistance). A goal of this chapter will be to review the notion that such antibodies cause or amplify pathological cardiovascular responses in preeclampsia. Each new steady-state value is then held within relatively narrow limits, that is, these changes are sensed as normal and "defended" in face of variations in fluid and sodium intake. The cause and significance of such changes have been debated for decades by three schools of thought. One advocates that the alterations are secondary to primary arterial vasodilatation causing "underfill" or decreased effective volume. The final concept, "overfill," views pregnant women as overexpanded with intravascular volume. Each camp agrees, however, that primary renal sodium and water retention is presumably responsible for the volume changes associated with normal pregnancy. In the second half of gestation, both pedal and pretibial edema can be detected in the majority of pregnant women, occurring more commonly as the day proceeds, often disappearing with recumbency. Values for oncotic pressure decrease from an average level of 370 mm H2O (27 mm Hg) in nonpregnant individuals to 345 mm H2O (25 mm Hg) in early pregnancy and 300 mm H2O (22 mm Hg) in late gestation. Note that the lowest values are reached in the hours that follow delivery, the period of time when women with preeclampsia are most at risk of both pulmonary and cerebral edema, if fluid administration is not monitored with appropriate care. The reduction in plasma oncotic pressure during pregnancy is mainly due to the ~1 g decrement in plasma albumin in normal gestation. The usual explanations of this decline are that it is a dilutional phenomenon related to the increase in plasma water, as well as in the decrease in plasma tonicity of ~10 mOsm. Data are from Chesley (the first edition of this text) combined with those from Zinaman et al. Finally, women with "normal" peripheral edema and otherwise normal pregnancies also have the greatest weight gain and plasma volume expansion as well as larger neonates with lower perinatal mortality rates than those with less fluid retention. Preeclamptic women with peripheral edema appear to be at risk of developing interstitial and frank pulmonary and cerebral edema. For example, Benedetti and Carlson35 have suggested that the risk of pulmonary edema can be predicted by measuring colloid oncotic pressure, a suggestion supported by the observation that the lowest values are measured in the early postpartum period,32,34 the period of greatest risk of this complication. Given that values in preeclamptic women are the lowest, they would naturally be the group at greatest risk of this life-threatening complication. Finally, Hytten,36 as far back as 1970, wrote that edema is so common in pregnancy that it is not a useful diagnostic criterion to use in the diagnosis of preeclampsia. Still, hypertension plus edema continued to be used to diagnose the disease (often compromising the value of research reports), only disappearing from the diagnostic criteria of all major classifications at the commencement of this millennium. Studies in pregnant animals and humans suggest that sodium and water reabsorption in the proximal nephron (determined by indices such as fractional lithium or solute-free water clearances) are unaltered, and these species dilute their urine normally when water-loaded during gestation. These disorders are considered prototypes of diseases in which absolute extracellular volumes are increased and "effective arterial volume" is low. Hormone-induced vasodilatation creating temporary "underfill" in the early weeks, followed quickly by compensation to a "normal fill" state as pregnancy progresses, fits two of the three theories, whereas during the last trimester natriuretic factors predominate and restore Na balance, at least in some gravidas. The importance of settling this dispute, however, is not trivial, because a better understanding of how the pregnant woman "senses" her volume changes will impact management, particularly for gravidas with hypertensive complications and cardiac disorders. The following observations suggest that primary arterial vasodilatation causing arterial underfilling with secondary sodium and water excretion occurs in early gestation. Supporters of "underfill" note that systolic and diastolic blood pressures decrease early in the first trimester of pregnancy despite an increase in blood volume. Measured were blood pressure, cardiac output, and renal hemodynamics (inulin and para-amino hippurate clearances). Pronounced placental growth occurs at weeks 68 of gestation and is generally complete by week 12. They also note the high levels of circulating natriuretic factors and various inhibitors of the membrane pump, which are expected responses to hypervolemia. There are also increases in renal hemodynamics, and two groups of investigators52,53 have described an increased sodium excretory capacity in response to saline infusions. Although reports are anecdotal, women with cardiac or renal disorders appear more susceptible to volume overload complications, whereas healthy gravidas seem to tolerate blood loss better than nonpregnant women. There are striking increments in intravascular volume during normal pregnancy, mainly the result of plasma water, but also due to a small increase in red blood cell mass. Those studies were in error, because late in gestation the indicator cannot attain complete mixing during the 10 minutes the gravida is positioned in a supine or sitting position. When serial studies are performed with the pregnant woman positioned in lateral recumbency, plasma volume increases were observed to commence in the first trimester, accelerate in the second, peak near gestational week 32, and remain elevated until term. Women with preeclampsia/eclampsia have significantly reduced plasma volumes Table 15. The degree of contraction appears to be an index of severity, and in this respect the greatest decreases (approaching 50% of normal pregnant values) have been reported in nulliparas with eclampsia, the convulsive phase of the disease associated with extreme severity. Freis & Kenny 59 Rottger60,61 Cope62 Freidberg & Lutz63 Kolpakova64 Honger65 Haering et al. Their data suggest that the increases in peripheral vascular resistance and blood pressure that characterize this disorder are mediated, at least in part, by a substantial increase in sympathetic vasoconstrictor activity. Thus, sympathetic nervous system overactivity in preeclampsia may contribute to abrogated vasodilatation expected in normal pregnancy. Their serial study also demonstrated that the increment in plasma volume in preeclamptic women and those whose blood pressure remained normal was similar in the second trimester of pregnancy but plasma volume contraction occurred thereafter, still preceding the development of overt disease by weeks. These observations appear to counter explanations that the decreased volumes reflect the effect of vasoconstriction on efflux of fluid from vessel walls or via the kidney (socalled "pressure naturesis" associated with hypertension). Intervention studies are rare in preeclampia; nevertheless one study compared low vs. Surprisingly, the authors observed a lower incidence of toxemia, edema, perinatal death, and bleeding during pregnancy in those told to consume more salt.
Levlen 0.15mg overnight delivery
Clinical tip Long-term outlook the greatest risk of arrhythmias birth control pills vs shots buy levlen canada, convulsions, and death is in the first 812 hours after ingestion. Patients with severe tricyclic overdose who improve with early appropriate treatment generally have no evidence of any long-term neurological or other physiological sequel. A Final Word from the Expert Tricylic antidepressant poisoning can be associated with severe and potentially lifethreatening toxicity. Significant toxicity can occur with ingestions > 35 mg/kg and lifethreatening effects can be seen with ingestions of > 1015 mg/kg. The Management of Tricyclic Antidepressant Poisoning: the Role of Gut Decontamination, Extracorporeal Procedures and Fab Antibody Fragments. Demographic and electrocardiographic factors associated with severe tricyclic antidepressant toxicity: J Toxicol Clin Toxicol, 1991; 29(1):3143. A meta-analysis of prognostic indicators to predict seizures, arrhythmias or death after tricyclic antidepressant overdose. The use of sodium bicarbonate in the treatment of tricyclic antidepressant-induced arrhythmias. Effect of hypertonic sodium bicarbonate in the treatment of moderate-to-severe cyclic antidepressant overdose. Clinical course, therapy, outcome and analytial data in amitriptyline and combined amitriptyline/chlordiazepoxide overdose. What is the role of lidocaine or phenytoin in tricyclic antidepressant-induced cardiotoxicity? Intralipid Outperforms Sodium Bicarbonate in a Rabbit Model of Clomipramine Toxicity. Successful reversal of life threatening cardiac effect following dosulepin overdose using intravenous lipid emulsion. Case report: Successful lipid resuscitation in multidrug overdose with predominant tricyclic antidepressant toxidrome; Int J Emerg Med 2012; 5(1):8. Tricyclic antidepressant overdose in a toddler treated with intravenous lipid emulsion Pediatrics 2011; 128(6):162832. Management of near fatal mixed tricyclic antidepressants and selective serotonin reuptake inhibitor overdose with intralipid 20% emulsion. The headache has not been relieved by paracetamol and worsens when retching to vomit. She had migraines as a teenager, but these were different in nature and associated with flashing lights. Her only other past medical history is of hypertension that has been well controlled with amlodipine. The pattern of the headache is particularly significant for primary headaches and other associated clinical features suggest a more significant pathology. Classification of headaches2,3 Acute single episode Meningitis Encephalitis Tropical illness. Guidelines for All Healthcare Professionals in the Diagnosis and Management of Migraine, Tension-Type, Cluster and Medication-Overuse Headache. Red-flag features which should prompt referral for further investigation: New onset of, or change in, headache in patients who are aged over 50 years Thunderclap: rapid time to peak headache intensity (seconds5 minutes)-same-day specialist assessment required Focal neurological symptoms. By comparison, the incidence in neurology outpatient clinic is 1 in 100, and in primary care it is 1 in 1000. The majority of patients presenting with headache will have a normal clinical examination but this does not exclude serious pathology. The patient is in obvious distress with a pain score of 6/10 but has only had paracetamol thus far, so prior to further examination you decide to give some further analgesia. The diagnosis is still unclear, but you wonder which would be the most appropriate additional analgesia at this stage. Symptoms may radiate to neck Tenderness to scalp Last 30 mins7 days Typically twice every 24 hrs for 15160 mins Clusters last 412 wks Rapid onset pain around one eye, unilateral headache Cluster headache Oxygen 100 %, 1020 min11 sumatriptan 6 mg s/c12 zolmitriptan nasal spray Prophylaxis: verapamil prednisolone Withdrawal of medication, gradual if opiate. Sumatriptan 50 mg was no better than aspirin alone for 2-hour pain-free and headache relief, but sumatriptan 100 mg was better than the combination of aspirin plus metoclopramide for 2-hour pain-free, but not for headache relief. Cluster headache A study conducted by the National Hospital for Neurology and Neurosurgery11 looked at 109 adults in a double-blind, randomized, placebo-controlled, cross-over trial over a period of 4 cluster headaches. They compared high-flow oxygen over a 15-minute period at the onset of headache with high-flow air. They found that 78 % with oxygen vs 20 % with air reached the primary end-point (p < 0. Non-oral preparations of triptans should be administered if oral medication is not tolerated. Other prophylactic treatments include acupuncture for tension-type headache and verapamil and ambulatory oxygen for recurrent cluster headache. Identifying a likely differential diagnosis is important to avoid treating blindly and ineffectually. Expert comment the relief of pain and suffering is one of the primary duties of the emergency physician and the provision of adequate analgesia should not be delayed until diagnosis is confirmed. If the clinical (continued) Case 15 Headache features suggest that a specific primary headache disorder is present, it is sensible to prescribe a treatment based on that diagnosis where feasible. Another pitfall for the unwary is to assume that a response to a diagnosis-based therapy increases the probability of, or even confirms that diagnosis. The use of triptans resulted in an even higher response rate even in secondary headaches. The most recent of these were compiled by the American Heart Association and published online in Stroke in May 2012. Clinical research studies may be effectively out of date by the time they are published as the imaging technique used has been superseded. Due to the potentially catastrophic result of a second bleed, patients and their physicians may feel that further investigation is still merited to further reduce the chances of missing such a diagnosis. The patient with a low pre-test probability may be more likely to have had a smaller volume bleed. The reliability of a report from a registrar using a laptop from home may be less than that of a consultant neuro-radiologist sitting using a full high-resolution workstation in a darkened room. Case 15 Headache 155 Case progression A lumbar puncture is performed showing no evidence of xanthochromia and the headache is now slowly subsiding with analgesia. Clinical question: Which other diagnoses may present as severe sudden onset headaches? Patients are concerned about being discharged home and want a definitive answer to the aetiology of the headaches. The treatment of tachyarrhythmias with -blockers needs to be balanced against the likelihood of reducing cerebral blood flow. At present hospital resources do not allow for this modality but perhaps this will provide a less invasive definitive investigation in the future. Considered a relatively trivial presentation by some, there is a surprisingly high prevalence of significant secondary headache disorders, yet there may be precious few clues as to which patients harbour serious pathology. For these reasons the emergency physician must strive to limit the exposure of patients to such investigations without missing the life-threatening diagnoses. Guideline for the management of lone acute severe headache for the College of Emergency Medicine. A double-blind study of ibuprofen versus placebo in the treatment of acute migraine attacks. Efficacy and tolerability of prochlorperazine buccal tablets in treatment of acute migraine. Efficacy and safety of sumatriptan tablets (25 mg, 50 mg and 100 mg) in the acute treatment of migraine: defining the optimum doses of oral sumatriptan. Aspirin in episodic tension-type headache: placebo controlled dose-ranging comparison with paracetamol. Comparison of ketoprofen, ibuprofen and naproxen sodium in the treatment of tension-type headache. High risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study.
