
Synthroid 25 mcg with visa
A correlation exists between leukocytes in semen and the generation of superoxide anions treatment eating disorders buy synthroid without prescription, hydrogen peroxide, and hydroxyl radicals (reactive-oxygen species), all of which can damage sperm membranes. Sperm are highly susceptible to the effects of oxidative stress because they possess little cytoplasm and therefore little antioxidant activity. Although genital tract infection has been linked to infertility in epidemiologic studies, the correlation between individual organisms and infertility is unclear. Uncontrolled studies suggest that pregnancy rates may improve after treatment, but controlled studies do not confirm these findings. Varicocele the association of varicoceles with male infertility is well established. Several treatment modalities, both surgical and nonsurgical, are available for varicoceles. These include ligation of the veins through the retroperitoneal, inguinal, or subinguinal approaches; percutaneous embolization; and laparoscopy. The common goal of all treatments is to stop the retrograde flow of venous blood through the internal spermatic veins. Treatments can be compared in terms of expected success rates (semen improvement and pregnancy), cost, and outcomes (pain pills, return to work or other activity), and their relative merits can be analyzed. Erectile Dysfunction Sexual dysfunction stemming from low libido or erectile dysfunction is a frequent cause of infertility. Vasectomy Reversal More than 500,000 men per year undergo vasectomy in the United States, and nearly 6% will eventually wish to have their vasectomies reversed. Causes of vasal obstruction other than vasectomy include infection, congenital, trauma, and previous surgery and are less frequent indications for vasovasostomy or epididymovasostomy. A problem with duct obstruction should be suspected in men with normal testis size, normal hormones and azoospermia. None has proved superior to any other, except that magnification with a surgical microscope results in higher success rates. Although these procedures are technically different, the experience of the surgeon is the most important factor for success. Depending on these factors, 95% or more of patients may have a return rate of 16% can be expected. If vasal fluid below the level of the vasectomy does not contain sperm, there may be a secondary obstruction in the epididymis. Such obstruction may result from rupture of the epididymal tubules in response to increased luminal pressure. A prolonged period of vasectomy or a vasectomy close to the epididymis increases the risk of an epididymal blockage. In this case, the vas must be connected to the epididymis above the area of rupture. The achievement of sperm in the ejaculate after vasovasostomy depends largely on surgical technique, but pregnancy after surgery is dependent upon the fertility potential of the couple. Therefore, it is critical to understand the reproductive health of the female partner before embarking on the procedure. A cystoscope with a resecting loop is used to remove the verumontanum and unroof an associated obstructing cyst that has compressed and obstructed the ejaculatory ducts. Patients with ejaculatory duct obstruction sufficient to cause coital discomfort, recurrent hematospermia, or infertility should be considered for treatment. A small resectoscope is inserted, and the verumontanum is resected in the midline until the ducts are visualized. The concomitant use of real-time, transrectal ultrasound may increase the accuracy of resection. Since the area of resection is at the prostatic apex, near the external urethral sphincter and the rectum, careful positioning of the resectoscope is essential. Most complications are self-limited and include hematospermia, hematuria, urinary tract infection, epididymitis, and a watery ejaculate. Rarely reported complications include retrograde ejaculation, rectal perforation, and urinary incontinence. This condition is generally associated with low ejaculate volume and low sperm concentrations and severely impaired motility. Parameter Ejaculate volume Sperm count Sperm motility Incomplete or partial Complete Functional Low Absent or low Absent or low Absent or low Electroejaculation A complete failure of emission and ejaculation occurs most commonly from spinal cord injury (10,000 cases/year in the United States) and as a result of deep pelvic or retroperitoneal surgery that injured the pelvic sympathetic nerves. With rectal probe electroejaculation, the pelvic sympathetic nerves undergo controlled stimulation, with contraction of the vas deferens, seminal vesicle, and prostate, such that a reflex ejaculation is induced. Semen acquired in this way at minimum requires the use of intrauterine insemination to allow for pregnancy. In men with anejaculation after retroperitoneal surgery or spinal trauma, successful recovery of sperm with electroejaculation is possible in most patients. Sperm motility tends to be lower than normal when obtained in this way, an effect independent of electrical or heat effects inherent to the procedure. In men with spinal cord injuries above the T5 level, it is often possible to induce a reflex ejaculation with high-frequency penile vibration, termed vibratory stimulation. With the use of handheld vibrators set to a frequency of 110 cycles/s (cps) at an amplitude of 3 mm, patients may be taught to perform the procedure and attempt to conceive at home with cervical insemination. Vasal aspiration provides the most mature sperm; however, this procedure is rarely performed, given the technical considerations and poor reliability of identifying healthy sperm from the vas. Epididymal Sperm Aspiration Epididymal sperm aspiration may be performed by two distinct techniques. After sperm are obtained, the epididymal tubule may be closed with fine, microscopic suture, and the sperm are processed. Although this technique is a less invasive, the blind insertion of a needle into the epididymis may be more likely to result in tubule injury; however, decreased success of a subsequent vasectomy reversal has not been demonstrated. Egg fertilization rates of 65% and pregnancy rates of 50% are possible with epididymal sperm, but results vary among individuals owing to differences in sperm and egg quality. Testicular sperm retrieval is also indicated in men with nonobstructive azoospermia who may harbor areas of reduced spermatogenesis within the testes. Given these widely varied indications, retrieval techniques have evolved to include minimally invasive aspiration procedures and more invasive dissections of the testis with the aid of an operating microscope. Although evaluated indirectly by hormone levels and testis volume, the most direct way to verify sperm production is with a testis biopsy. A small "window" incision is made in the scrotum and held open with a small retractor. Studies have suggested that hyperprolactinemia alone, independent of gonadotropin deficiencies can suppress normal testicular function. Testicular sperm retrieval procedures are highly variable in terms of their surgical invasiveness. Whenever possible, the least invasive approach necessary to acquire adequate sperm should be used.
Buy genuine synthroid on line
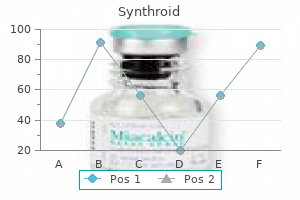
Among the strongest studies is a longitudinal assessment of growth and pubertal timing among a cohort of around 500 boys in Mean testicular volume (ml) 99 treatment norovirus generic synthroid 100 mcg amex. X-axis values are age in years and the y-axis displays gender-appropriate centiles for development. Individuals can have their Tanner stage and testis volume plotted to determine precocity, delay in development, or appropriate progression to determine if development has plateaued or arrested. Such diagrams assist in identifying early and delayed development, as well as finding differences in the progression of puberty. The hamartomas are congenital malformations characterized by heterotropic gray matter, neurons, and glial cells, and they are generally located on the floor of the third ventricle or attached to the tuber cinereum. All clinically affected individuals inherited the mutated allele from their fathers, which can be explained because this gene is maternally imprinted and expressed only from the paternal allele. Both boys and girls are affected, although the degree of precocity appears to be greater in girls than boys. Many boys may have unrecognized testicular pathology, but the predominant finding is Leydig cell hyperplasia, which may not warrant active intervention. Most cases appear to originate from autoimmune thyroid disease, but there are some case reports where the syndrome is secondary to unrecognized congenital hypothyroidism. These are autosomal recessive disorders of cortisol synthesis that present with premature pubic hair development, axillary hair development, accelerated linear growth, and phallic enlargement in the absence of testicular enlargement. Adrenal tumors in children may secrete androgens, and virilization is a common presentation. Whether precocious puberty is gonadotropin dependent or gonadotropin independent not always clear. In contrast, in some cases of precocious pubertal development among girls, pubertal manifestations will stop progressing or regress, making treatment unnecessary; such cases are not as commonly seen in boys. Although available data derive mostly from study of girls with pubertal onset at the earlier end of the normal range, it has been suggested that a higher proportion of early-maturing adolescents within the general population engage in exploratory risky behaviors (sexual intercourse and substance use) at an earlier age than adolescents with average or late timing of maturation. Epidemiological studies have associated earlier pubertal timing with increased risk for a number of negative adult health outcomes, including obesity; reproductive cancers, such as breast cancer in women and prostate cancer in men; type 2 diabetes; and cardiovascular disease. Also most of these studies examined pubertal timing more generally rather than precocious puberty specifically, but many of the observed associations extended into the precocious range. This technique has been used to suggest that it is pubertal timing itself that influences risk of reproductive cancers, including breast, ovarian, and endometrial cancers in women and prostate cancer in men. Pathologic entities leading to sexual precocity warrant treatment, but whether and at what ages one should initiate 18 Premature Adrenarche Another form of early development of secondary sexual characteristics occurs when the zona reticularis of the adrenal cortex matures early, causing premature adrenarche. Usually, there is no substantial advancement in bone age; however, even in the subset with more advanced bone ages there appears to be little to no compromise of adult height, although admittedly, most of these data derive from studies among girls. Evaluation of the Boy With Precocious Development of Secondary Sexual Characteristics Boys with sexual precocity require careful evaluation because many have underlying disorders. Premature adrenarche may be distinguished from true precocity over time by lack of rapid progression. Considerations include first verifying that the pubertal development is occurring outside the range of normal development before initiating an evaluation. It is also important to note that not all tests are appropriate in each case and that the diagnostic yields of various tests are not known. Hence it is important to allow history and physical examination to guide the evaluation. Conversely, the child with bilateral prepubertal-sized testicles is more likely to have peripheral precocity; the child with unilateral testicular enlargement may have a testicular tumor. Testosterone levels will be elevated in instances of isosexual precocity (secondary sexual characteristics consistent with male sex), whereas estradiol levels may be elevated in the rare instances of contrasexual precocity (secondary sexual characteristics inconsistent with sex, such as marked breast development as the presenting sign in a boy). Determining the underlying mechanism for progressive peripheral precocity is important because all instances will result from pathologic conditions or exogenous exposures. Determination of the 17-hydroxyprogesterone concentration is used to screen for congenital adrenal hyperplasia because of 21-hydroxylase deficiency. Congenital adrenal hyperplasia and hormonesecreting tumors of the adrenal gland are discussed in detail in Chapter 14. Evaluation of skeletal maturation with a bone age is an important adjunct, as it allows for prediction of adult height. What is the underlying mechanism, and is that mechanism associated with a risk of a serious condition, such as an intracranial lesion Although the data derive primarily from studies among girls, it appears that the risk of short stature is most pronounced in those children with earlier onset of symptoms. Finally, although the associations with pubertal timing and later life health outcomes mentioned earlier are intriguing, there are no data regarding whether treatment of precocious (or delayed) puberty affects the risk of such outcomes. This question represents an important area of further study because the ability to mitigate risks for cancer or cardiovascular disease would be an important consideration when deciding for or against treatment of precocious puberty. The depot formulations are preferred, as they are easier for patients and families to administer regularly over a long treatment period. The initial depot medications were 1-month formulations, which have been shown to be well tolerated and effective. These outcomes have largely been studied among girls, and the available data are reassuring. Progression of pubertal development or of rapid skeletal maturation indicates a lack of efficacy, poor adherence, or a misdiagnosis. Full endorsement of these regimens awaits further controlled clinical trials, including the evaluation of the long-term effects of such therapy on adult height, fertility, metabolic parameters, cognitive functions,177 and bone health. As noted previously, because of the downward trend in pubertal timing in some but not all reports from the United States,58,180,181 and other countries,66,182 some advocate for younger age cutoffs for the general population or perhaps for particular countries or ethnic groups. However, there is likely to be overlap among these categories, as the same mutation may cause heterogeneous phenotypes even within families. Nonreproductive features may include unilateral renal agenesis and synkinesia ("mirror movements," with movements on one side of the body causing involuntary movements on the contralateral side). These syndromes include Prader-Willi, Bardet-Biedl, Alstr m, and o Bloom syndromes. Developmental anomalies of pituitary development, such as midline defects or septooptic dysplasia, can be associated with gonadotropin and other pituitary hormone deficiencies. Suggested causes include increased total energy expenditure225 and increased insulin sensitivity,226 but no definitive etiology has been identified. In this disorder, the fetal adrenal cortex develops normally, but the adult zone of the adrenal cortex fails to develop. Mutations in this gene may be part of a contiguous gene-deletion syndrome that also causes Duchenne muscular dystrophy and glycerol kinase deficiency. Other symptoms can include decreased growth velocity, headache, polyuria/polydipsia, and visual disturbances. Other tumors include germ cell tumors, epidermoid and dermoid cysts, prolactinomas, and optic gliomas. Histiocytosis X is characterized by infiltration of lipid-laden histiocytes into skin, bone, or visceral organs. Although diabetes insipidus is the most common endocrine manifestation of histiocytosis X, other anterior pituitary hormone deficiencies may occur. Hyperprolactinemia can be caused by a prolactin-secreting tumor, including pituitary microadenomas (adenomas <10 mm) and macroadenomas (>10 mm) and can also be caused by disruption of the pituitary stalk, as hypothalamic dopamine release inhibits prolactin secretion. In the same report parallel studies in a murine model corroborated heterozygous Hs6st1 deficiency as a cause of delayed pubertal timing without compromised fertility. Although anorexia nervosa primarily affects females, approximately 10% of patients are male. Intensive physical activity and the need to "make weight" in wrestlers may disrupt pubertal development. For wrestlers, these changes generally reverse within months of the end of the wrestling season. Hypergonadotropic Hypogonadism Primary gonadal insufficiency leads to loss of negative feedback inhibition and hypergonadotropic hypogonadism.
Discount synthroid american express
Analysis of muscular mass and function: the impact on bone mineral density and peak muscle mass medicine reaction buy synthroid 25 mcg on-line. Osteoclast activity and subtypes as a function of physiology and pathology Implications for future treatments of osteoporosis. Tks5-dependent formation of circumferential podosomes/invadopodia mediates cell-cell fusion. Lysosomal pathology and osteopetrosis upon loss of H+-driven lysosomal Cl- accumulation. Interpretation and application of bone turnover markers in children and adolescents. Melatonin promotes osteoblast differentiation by regulating osterix protein stability and expression. Different roles of Runx2 during early neural crest-derived bone and tooth development. Activation of Sirt1 decreases adipocyte formation during osteoblast differentiation of mesenchymal stem cells. Paracrine and endocrine actions of bone - the function of secretory proteins from osteoblasts, osteocytes, and osteoclasts. Multifaceted interaction of bone, muscle, lifestyle interventions and metabolic and cardiovascular disease: role of osteocalcin. Enpp1 is an anti-aging factor that regulates Klotho under phosphate overload conditions. Biology of bone tissue: Structure, function, and factors that influence bone cells. The concentrations of markers of bone turnover in normal pregnancy and preeclampsia. Biochemical markers of bone turnover and the volume and the density of bone in children at different stages of sexual development. Sex- and agespecific reference curves for serum markers of bone turnover in healthy children from 2 months to 18 years. Validation of a novel, rapid, high [recision sclerostin assay not confounded by sclerostin fragments. Determination of serum and plasma sclerostin concentrations by enzyme-linked immunoassays. Sclerostin and its association with physical activity, age, gender, body composition, and bone mineral content in healthy adults. Increased sclerostin serum levels associated with bone formation and resorption markers in patients with immobilization-induced bone loss. Relation of age, gender, and bone mass to circulating sclerostin levels in men and women. Insights into material and structural basis of bone fragility from diseases associated with fractures. How determinants of the biomechanical properties of bone are compromised by disease. Association between linear growth and bone accrual in a diverse cohort of children and adolescents. The bone mineral density in childhood study: Bone mineral content and density according to age, sex, and race. Distance of walking in childhood and femoral bone density in perimenopausal women. Spatial distribution of growth hormone receptor, insulin-like growth factor-1 receptor and apoptotic chondrocytes during growth plate development. Endocrine assessment, molecular characterization and treatment of growth hormone insensitivity. The endogenous growth hormone secretagogue (ghrelin) is synthesized and secreted by chondrocytes. Thyroid hormones regulate fibroblast growth factor receptor signaling during chondrogenesis. Clinical Review: sex steroids and the periosteum-Reconsidering the roles of androgens and estrogens in periosteal expansion. Glucocorticoids and bone: Consequences of endogenous and exogenous excess and replacement therapy. Height adjustment in assessing dual energy x-ray absorptiometry measurements of bone mass and density in children. Bone mineral density of the spine in 11,898 Chinese infants and young children: A cross-sectional study. Peak bone mineral accrual and age at menarche in adolescent girls: A 6-year longitudinal study. Update on bone density measurements and their interpretation in children and adolescents. Peripheral quantitative computed tomography of the distal and proximal forearm in children and adolescents: bone densities, cross-sectional sizes and soft tissue reference data. Fractures during childhood and adolescence in healthy boys: relation with bone mass, microstructure, and strength. Pediatric reference curves for multisite quantitative ultrasound and its modulators. Measurement of volumetric bone mineral density accurately determines degree of lumbar undermineralization in children with growth hormone deficiency. Factors associated with bone turnover and speed of sound in early and-pubertal females. Structural and functional assessment of trabecular and cortical bone by micro magnetic resonance imaging. Accuracy of high-resolution in vivo micro magnetic resonance imaging for measurements of microstructural and mechanical properties of human distal tibial bone. Natriuretic peptides, their receptors, and cyclic guanosine monophosphate-dependent signaling functions. Circulating osteocrin stimulates bone growth by limiting C-type natriuretic peptide clearance. Medical Imaging 2013: Biomedical Applications in Molecular, Structural, and Functional Imaging. Hormonal and biochemical determinants of trabecular microstructure at the ultradistal radius in women and men. Imaging methods for bone mass evaluation during childhood and adolescence: an update. Clinical use of bone mass measurements in children and adults for the assessment and management of osteoporosis. Increasingly, however, it has become recognized that, for reasons that are poorly understood, several of the genetic forms can initially present with diabetes as late as 9 months to 1 year or even later. Risk for the most common causes, type 1 and type 2 diabetes, depends on many different gene loci with intermediate or low effects and are thus considered polygenic. However, approximately 1% to 5% of all diabetes is caused by abnormalities at a single gene or locus and as a group, these entities are termed monogenic diabetes. In addition, they rarely may have dysmorphic facies, as well as renal tract anomalies, such as hydronephrosis and vesicoureteral reflux, a variety of cardiac anomalies, hypothyroidism, or hand-finger anomalies. Even in those with the severe mutations causing significant neurodevelopmental dysfunction, the abnormalities may often not be recognized until patients are older. It is important to emphasize that these chromosomal changes cause altered expression of genes, rather than representing mutations. There is also a reduction in the number of insulin staining cells and reduced insulin content or insulin secretion despite normal or elevated beta cell mass at all postnatal periods. Also as in humans, the compensatory increase in beta cell mass is not sustained, resulting in a mild diabetes mellitus characterized by normal fasting glucose but hyperglycemia after glucose challenge. Overall, despite the recapitulation of the key features of the human disease, the mouse model displays milder features. Age at presentation was positively correlated to gestational age, but age at remission was negatively correlated with adjusted birth weight. This would be consistent with the effects of insulin on intrauterine growth, so that the larger infants would have the milder defect and therefore tend to enter remission sooner.
Discount synthroid 50 mcg without prescription
They are involved in the flow of water and urea from the inside of the collecting duct cell into the extracellular renal medullary space medicine lyrics synthroid 100mcg visa. Mice made genetically deficient in aquaporin-4 demonstrate a mild urinary concentrating defect,111 whereas those with deficiency of aquaporin3 alone, or together with aquaporin-4, demonstrate more severely impaired urinary concentrating ability. In addition to the well-established endocrine regulatory system, several local renin-angiotensin systems have emerged, with both autocrine and paracrine effects in their tissue of synthesis, whose regulation is independent of the classic system. Depicted, are predicted membrane topology, with the extracellular domain at the top of the figure. The 271-amino-acid protein consists of five transmembrane domains, four intracellular domains, and three extracellular domains. Most mutations are transmitted with an autosomal recessive pattern, with autosomal dominant transmission noted by boxed amino acids. Renin, which is synthesized by the renal juxtaglomerular apparatus, is a proteolytic enzyme that catalyzes the cleavage of angiotensinogen, synthesized by hepatocytes, into the decapeptide angiotensin I. For control of intravascular volume, the primary target of action of aldosterone is the distal nephron. Here, aldosterone increases synthesis of apical membrane sodium channels, mitochondrial enzymes involved in adenosine triphosphate production, and components of Na+, K+ adenosine triphosphatase to cause increased sodium reabsorption and potassium excretion. Decreased intravascular volume as sensed by the renal juxtaglomerular apparatus results in release of renin. Conversely, expanded intravascular volume causes decreased renin output and less sodium and water resorption in the kidney, serving to decrease intravascular volume and restore homeostasis. Changes in vascular volume are not the only regulators of the renin-angiotensin-aldosterone system. Serum potassium concentration directly modulates aldosterone release by the adrenal glomerulosa by its effects on plasma membrane potential and activation of voltage-gated calcium channels. Pituitary adrenocorticotropin hormone and vasopressin act through their respective receptors on the glomerulosa cells to increase acute aldosterone secretion. The interaction of the natriuretic peptide system occurs both in the central nervous system through effects on vasopressin secretion, and peripherally, through its ability to both directly promote natriuresis in the kidney and indirectly inhibit adrenal aldosterone production. The primary sequence of the peptide has been conserved among mammalian species and, in addition to synthesis in cardiac atrial tissue,132 has been detected in brain, spinal cord, pituitary, and adrenal gland. In addition to the well-defined endocrine circuit, the components of the renin-angiotensin system have been found in a wide variety of tissues, including brain, pituitary, arterial wall, heart, ovary, kidney, and adrenal, where paracrine and autocrine regulatory functions122,128 have been postulated, undergoing regulation independent of the systemic counterpart. From the standpoint of regulation of water and volume homeostasis, the brain renin-angiotensin system merits further description. In contrast, renin has been found in high concentration in nerve terminals, with enhanced release on nerve depolarization. Two of the most significant sites include the circumventricular organs and the paraventricular nucleus of the hypothalamus. The signal of hypovolemia is transduced through the vagal nerve from volume sensors to the brain stem and the region of the nucleus tractus solitarius. Amino acids identical between the three peptides are indicated by bold letters, and the disulfide bond between Cys residues is shown. Hypotension and bradycardia have both been observed, as has inhibition of vasopressin, adrenocorticotropic hormone, and gonadotropinreleasing hormone secretion. It is most often caused by intravascular volume depletion or excessive salt loss and is also encountered with hypotonic fluid overload, especially in infants. Inappropriate vasopressin excess is one of the least common causes of hyponatremia in children, except after vasopressin administration for treatment of diabetes insipidus. In evaluating the cause of hyponatremia, one should first determine whether the patient is dehydrated and hypovolemic. This is usually evident from the physical examination (decreased weight, skin turgor, central venous pressure) and laboratory data (high blood urea nitrogen, renin, aldosterone, uric acid). With a decrease in the glomerular filtration rate, proximal tubular reabsorption of sodium and water will be high, leading to a urinary sodium value often less than 10 mEq/L. Patients with decreased "effective" intravascular volume from congestive heart failure, cirrhosis, nephrotic syndrome, or lung disease will present with similar laboratory data, but will also have obvious signs of their underlying disease, which often includes peripheral edema. Because cortisol and thyroid deficiency cause hyponatremia by several mechanisms, discussed subsequently, they should be considered in all hyponatremic patients. Drug-induced hyponatremia should be considered in patients on potentially offending medications, as discussed later. The following questions are asked: Is there a psychosocial reason for either polyuria or polydipsia Renal Diabetes Insipidus Central and Nephrogenic Osmotic diuresis with non-sodium solute Tubulopathy 2. Does the history (including longitudinal growth data) or physical examination suggest other deficient or excessive endocrine secretion or an intracranial neoplasm If pathologic polyuria or polydipsia is present, the following should be obtained. In the outpatient setting: serum osmolality; serum concentrations of sodium, potassium, glucose, calcium, and blood urea nitrogen; and urinalysis, including measurement of urine osmolality, specific gravity, and glucose concentration. A serum osmolality greater than 300 mOsm/kg, with urine osmolality less than 300 mOsm/kg, establishes the diagnosis of diabetes insipidus. If serum osmolality is less than 270 mOsm/kg, or urine osmolality is greater than 600 mOsm/ kg, the diagnosis of diabetes insipidus is unlikely. If, on initial screening, the patient has a serum osmolality less than 300 mOsm/kg, but the intake/output record at home suggests significant polyuria and polydipsia that cannot be attributed to primary polydipsia. After a maximally tolerated overnight fast (based on the outpatient history), the child is admitted to the outpatient testing center in the early morning of a day when an 8- to 10-hour test can be carried out, and the child is deprived of water. If at any time during the test, the urine osmolality exceeds 1000 mOsm/kg, or 600 mOsm/kg and is stable over 1 hour, the patient does not have diabetes insipidus. If at any time the serum osmolality exceeds 300 mOsm/kg and the urine osmolality is less than 600 mOsm/kg, the patient has diabetes insipidus. If the serum osmolality is less than 300 mOsm/kg and the urine osmolality is less than 600 mOsm/kg, the test should be continued unless vital signs disclose hypovolemia. This may be difficult in a young child who may not tolerate a long period of fasting. A common error is to stop a test too soon, based on the amount of body weight lost, before either urine osmolality has plateaued above 600 mOsm/kg or a serum osmolality above 300 mOsm/kg has been achieved. Unless the serum osmolality increases above the threshold for vasopressin release, a lack of vasopressin action (as inferred by a nonconcentrated urine) cannot be deemed pathologic. As an alternative to water deprivation, hypertonic saline can be infused intravenously to raise serum osmolality above the threshold for vasopressin release. If the patient has central diabetes insipidus, urine volume should fall and osmolality should at least double during the next hour, compared with the value before vasopressin therapy. If there is less than a 2-fold increase in urine osmolality after vasopressin administration, the patient probably has nephrogenic diabetes insipidus. Desmopressin should not be used for this test, because it has been associated with water intoxication in small children in this setting. This should not be confused with primary nephrogenic diabetes insipidus, because patients with primary polydipsia should have a tendency toward hyponatremia, rather than hypernatremia, in the basal state. Moreover, this form of secondary nephrogenic diabetes insipidus will reverse after cessation of overdrinking. The hypertonic saline infusion test correctly differentiated between partial diabetes insipidus and primary polyuria in 95. One must beware of intraoperative fluid expansion with subsequent hypoosmolar polyuria masquerading as diabetes insipidus. Elevated copeptin levels within 24 hours after neurosurgery, in the hypothalamicpituitary region, predict the unlikeliness of subsequent central diabetes insipidus, whereas low copeptin levels favor it. Under these conditions, a daily solute load of 500 mOsm/m2 could be excreted in 10 L/m2 of urine per day. Neonates cannot dilute their urine to this degree and are prone to develop water intoxication at levels of water ingestion above 4 L/m2/day (approximately 60 mL/h in a newborn). This may happen when concentrated infant formula is diluted with excess water, either by accident or in a misguided attempt to make it last longer. Long-standing ingestion of large volumes of water will decrease the hypertonicity within the renal medullary interstitium, which will impair water reabsorption and guard against water intoxication. The rare patient in whom the osmotic thresholds for thirst and vasopressin release are reversed illustrates the importance of the normal relationship between these two responses to osmotic stimulation.
Buy synthroid australia
Plasma atrial natriuretic hormone levels in patients with the syndrome of inappropriate antidiuretic hormone secretion symptoms for pregnancy purchase cheap synthroid. Role of atrial natriuretic peptide in the diuresis of a newborn infant with the syndrome of inappropriate antidiuretic hormone secretion. Alterations in plasma concentrations of natriuretic peptides and antidiuretic hormone after subarachnoid hemorrhage. Hyponatremia in neurological patients: cerebral salt wasting versus inappropriate antidiuretic hormone secretion. Prompt recovery of plasma arginine vasopressin in diabetic coma after intravenous infusion of a small dose of insulin and a large amount of fluid. Autosomal recessive familial neurohypophyseal diabetes insipidus with continued secretion of mutant weakly active vasopressin. Mutant vasopressin precursors that cause autosomal dominant neurohypophyseal diabetes insipidus retain dimerization and impair the secretion of wild-type proteins. Cellular toxicity caused by the accumulation of mutant vasopressin precursors within the endoplasmic reticulum. A murine model of autosomal dominant neurohypophyseal diabetes insipidus reveals progressive loss of vasopressin-producing neurons. Mice conditionally lacking the Wolfram gene in pancreatic islet beta cells exhibit diabetes as a result of enhanced endoplasmic reticulum stress and apoptosis. Genotypic classification of patients with Wolfram syndrome: insights into the natural history of the disease and correlation with phenotype. Wolfram Syndrome protein, Miner1, regulates sulphydryl redox status, the unfolded protein response, and Ca2+ homeostasis. Atrial natriuretic peptide and other vasoactive hormones during treatment of severe diabetic ketoacidosis in children. Pediatric central diabetes insipidus: brain malformations are common and few patients have idiopathic disease. Central diabetes insipidus: clinical profile that suggests organicity in Peruvian children: Lima - Peru 2001-2013. Identification of five novel arginine vasopressin gene mutations in patients with familial neurohypophyseal diabetes insipidus. Two novel mutations in seven Czech and Slovak kindreds with familial neurohypophyseal diabetes insipidus-benefit of genetic testing. Hereditary central diabetes insipidus: plasma levels of antidiuretic hormone in a family with a possible osmoreceptor defect. Hereditary diabetes insipidus: an immunohistochemical study of the hypothalamus and pituitary gland. The Human Gene Mutation Database: towards a comprehensive repository of inherited mutation data for medical research, genetic diagnosis and 325. Neurohypophyseal function in postpartum hypopituitarism: impaired plasma vasopressin response to osmotic stimuli. Frequent occurrence of the triphasic response (diabetes insipidus/hyponatremia/diabetes insipidus) after surgery for craniopharyngioma in childhood. Diabetes insipidus with impaired osmotic regulation in septo-optic dysplasia and agenesis of the corpus callosum. A case of Kabuki make-up syndrome with central diabetes insipidus and growth hormone neurosecretory dysfunction. Alobar holoprosencephaly, diabetes insipidus and coloboma without craniofacial abnormalities: a case report. Central diabetes insipidus in infancy with or without hypothalamic adipsic hypernatremia syndrome: early identification and outcome. Diabetes insipidus in pediatric germinomas of the suprasellar region: characteristic features and significance of the pituitary bright spot. Diabetes insipidus in preleukaemic phase of acute myeloid leukaemia in 2 patients with empty sella turcica. Monosomy 7 predisposes to diabetes insipidus in leukaemia and myelodysplastic syndrome. Acute myeloid leukemia, the 3q21q26 syndrome and diabetes insipidus: a case presentation. Acute myeloid leukemia presenting with panhypopituitarism or diabetes insipidus: a case series with molecular genetic analysis and review of the literature. The frequency and natural history of diabetes insipidus in children with Langerhans-cell histiocytosis. Anterior pituitary function and computed tomography/magnetic resonance imaging in patients with Langerhans cell histiocytosis and diabetes insipidus. Radiation therapy for diabetes insipidus caused by Langerhans cell histiocytosis [see comments]. Lymphocytic infundibuloneurohypophysitis as a cause of central diabetes insipidus. Lymphocytic hypophysitis causing hypopituitarism and diabetes insipidus, and associated with autoimmune thyroiditis, in a nonpregnant woman. Lymphocytic hypophysitis presenting with diabetes insipidus: case report and literature review. Necrotizing infundibulo-hypophysitis: a unique syndrome of diabetes insipidus and hypopituitarism. Bronchocentric granulomatosis and central diabetes insipidus successfully treated with corticosteroids. Diabetes insipidus secondary to intracranial sarcoidosis confirmed by low-field magnetic resonance imaging. Detection of vasopressin cell antibodies in some patients with autoimmune endocrine diseases without overt diabetes insipidus. Diabetes insipidus associated with symptomatic congenital cytomegalovirus infection. Central diabetes insipidus caused by nonspecific chronic inflammation of the hypothalamus: case report. Exacerbation of pre-existing diabetes insipidus during pregnancy, mechanisms and management. Vasopressin-resistant diabetes insipidus, liver dysfunction, hyperuricemia and decreased renal function. Abnormal diurnal rhythm of plasma vasopressin and urinary output in patients with enuresis. Desmopressin for bed wetting: length of treatment, vasopressin secretion, and response [see comments]. Comparison of longterm efficacy of desmopressin lyophilisate and enuretic alarm for monosymptomatic enuresis and assessment of predictive factors for success: a randomized prospective trial. Hereditary nephrogenic diabetes insipidus and bilateral nonobstructive hydronephrosis. Dental fluorosis as a complication of hereditary diabetes insipidus: studies of six affected patients [see comments]. Effect of hydrochlorothiazide and indomethacin treatment on renal function in nephrogenic diabetes insipidus. Buccally administered intranasal desmopressin acetate for the treatment of neurogenic diabetes insipidus in infancy. Oral administration of diluted nasal desmopressin in managing neonatal central diabetes insipidus. Effects of vasopressin on the circulation and its baroreflex control in healthy men. Assessment and validation of a defined fluid restriction protocol in the use of subcutaneous desmopressin for children with inherited bleeding disorders. Central diabetes insipidus and cisplatin-induced renal salt wasting syndrome: a challenging combination. Aqueous vasopressin infusion during chemotherapy in patients with diabetes insipidus. Comparison of incidence of hyponatremia between intranasal and oral desmopressin in patients with central diabetes insipidus.
Discount synthroid online
Lys304Glu) symptoms 0f pneumonia purchase synthroid 125mcg overnight delivery, is homozygous in 80% of cases presenting clinically, and in 60% of cases identified by newborn screening. The risk of severe complications, brain damage, and death is very high unless appropriate treatment to reverse the catabolic state is implemented. A high index of suspicion for fatty acid oxidation defects is important because appropriate therapy may result in an interruption and prevention of these potentially lifethreatening episodes. Other tests which may be useful in patients who require further evaluation include assays of fatty acid oxidation and specific enzyme assays in cultured skin fibroblasts or lymphoblasts. Since the early 1990s, the use of tandem mass spectrometry has made newborn screening possible for most fatty acid oxidation disorders, based on the acylcarnitine profile in blood spots. Presymptomatic identification of these individuals can prevent catastrophic events, such as sudden death. On the other hand, as children become older, they are able to tolerate periods of fasting of as long as 10 to 12 hours without decompensation. Glucose monitoring is not useful, because the presence of hypoglycemia is usually an event that occurs late in the evolution of an episode of metabolic decompensation. The use of uncooked cornstarch (as used for the treatment of type 1 glycogen storage disease) is rarely indicated. The biochemical hallmark is the finding of hypoglycorrhachia (low cerebrospinal fluid glucose concentration), despite normal plasma glucose concentrations. The classic phenotype is a severe form of early-onset epileptic encephalopathy in approximately 90% of cases (classic form). A nonepileptic form represents 10% of cases, which includes a broad phenotypic spectrum that may present with paroxysmal nonepileptic manifestations that have been reported to include intermittent ataxia, choreoathetosis, dystonia, and alternating hemiplegia. The typical clinical signs are hepatomegaly caused by glycogen accumulation, a severe Fanconi-type renal tubulopathy with disproportionately severe glucosuria, glucose and galactose intolerance, hypophosphatemic rickets, and severely stunted growth. The hypoglycemia during fasting is explained by altered glucose transport out of the liver, resulting in an increased intracellular glucose concentration that may inhibit glycogen degradation, leading to glycogen storage and hepatomegaly. The hypoglycemia is exacerbated by renal loss of glucose caused by a transport defect for glucose and galactose across the basolateral membranes of the tubular cells. Hyperglycemia (and hypergalactosemia) in the fed state is explained by decreased monosaccharide uptake by the liver and enhanced by an inappropriately low insulin secretion because of impaired glucose-sensing by the pancreatic -cells. In terms of diet, an adequate caloric intake is recommended to compensate for renal and intestinal glucose loss-given as frequent feedings containing slowly absorbed carbohydrates (such as cornstarch) to avoid fasting hypoglycemia. It is advisable to periodically reassess the efficacy of the treatment for any form of hypoglycemia by a formal fasting study on treatment. All patients should have an emergency letter stating their specific diagnosis, advice on prevention of hypoglycemia and information on acute treatment of a hypoglycemia episode, in addition to contact information for the physician of record for ongoing assistance. With the rapid advancement in the understanding of molecular genetics and genotype-phenotype correlations for the different types of congenital hyperinsulinism, the most common cause of persistent hypoglycemia in neonates, a model of personalized medicine is starting to emerge. Cerebral energy metabolism, glucose transport and blood flow: changes with maturation and adaptation to hypoglycaemia. Physiological and molecular characteristics of rat hypothalamic ventromedial nucleus glucosensing neurons. Molecular cloning and characterization of an insulin-regulatable glucose transporter. Identification of a novel gene encoding an insulinresponsive glucose transporter protein. Cerebral blood flow and exchange of oxygen, glucose ketone bodies, lactate, pyruvate and amino acids in anesthetized children. Defective glucose transport across the blood-brain barrier as a cause of persistent hypoglycorrhachia, seizures, and developmental delay. Before that specific diagnosis being made, and before the implementation of individual therapy plans, the goal of therapy is to preserve central nervous system function and to prevent catabolic states in which intermediary metabolites, such as free fatty acids and their acylcarnitines, ketones, or lactate may cause secondary harm. It is important to follow an initial glucose bolus with a continuous glucose infusion to prevent further episodes of hypoglycemia, until specific therapies are established. For neonates in the first 24 to 48 hours of life see earlier (Physiology of Perinatal Glucose Homeostasis). This may be reduced if plasma glucose is greater than 5 mmol/L (>90 mg/dL), but should be rapidly increased if frequent glucose checks indicate failure to elevate plasma glucose to greater than 3. In addition, allowance should be made for the effects of intercurrent illness on glucose regulation and Hypoglycemia in the Newborn and Infant 12. In vivo measurements of brain glucose transport using the reversible Michaelis-Menten model and simultaneous measurements of cerebral blood flow changes during hypoglycemia. Glucose counterregulation, hypoglycemia, and intensive insulin therapy in diabetes mellitus. Incidence of hypoglycemia in newborn infants classified by birth weight and gestational age. The impact of gestational age and fetal growth on the maternal-fetal glucose concentration difference. Glucose uptake, utilization, and transfer by the human placenta as functions of maternal glucose concentration. Spontaneous and amino acid-stimulated glucagon secretion in the immediate postnatal period. Hormonal and metabolic response to hypoglycaemia in small for gestational age infants. The glycemic response of the newborn infant to epinephrine administration: a preliminary report. Tissue-specific disallowance of housekeeping genes: the other face of cell differentiation. Functional beta-cell maturation is marked by an increased glucose threshold and by expression of urocortin 3. Synaptotagmin 4 regulates Pancreatic beta Cell Maturation by Modulating the Ca 197 36. Patterns of metabolic adaptation for preterm and term infants in the first neonatal week. Population meta-analysis of low plasma glucose thresholds in full-term normal newborns. Controversies regarding definition of neonatal hypoglycemia: suggested operational thresholds. Clinical features and insulin regulation in infants with a syndrome of prolonged neonatal hyperinsulinism. Recommendations from the Pediatric Endocrine Society for Evaluation and Management of Persistent Hypoglycemia in Neonates, Infants, and Children. Meeting Materials of the Clinical Chemistry and Clinical Toxicology Devices Panel. High risk of diabetes and neurobehavioral deficits in individuals with surgically treated hyperinsulinism. Effects of hypoglycemia on developmental outcome in children with congenital hyperinsulinism. Metabolic events in infants of diabetic mothers during first 24 hours after birth. Circulating catecholamines and glucagon in infants of strictly controlled diabetic mothers. Idiopathic spontaneously occurring hypoglycemia in infants; clinical significance of problem and treatment. Mechanisms of Disease: advances in diagnosis and treatment of hyperinsulinism in neonates. Human and rat beta cells differ in glucose transporter but not in glucokinase gene expression. Mutations in the sulfonylurea receptor gene in familial persistent hyperinsulinemic hypoglycemia of infancy. Hyperinsulinism and hyperammonemia in infants with regulatory mutations of the glutamate dehydrogenase gene. Hyperinsulinism in short-chain L-3-hydroxyacyl-CoA dehydrogenase deficiency reveals the importance of beta-oxidation in insulin secretion. Physical exercise-induced hypoglycemia caused by failed silencing of monocarboxylate transporter 1 in pancreatic beta cells. Dysregulation of insulin secretion in children with congenital hyperinsulinism due to sulfonylurea receptor mutations. Sulfonylurea receptor type 1 knock-out mice have intact feeding-stimulated insulin secretion despite marked impairment in their response to glucose.
Buy synthroid 100mcg fast delivery
There are several possible components of a clinical trial that also define their strengths and weaknesses treatment upper respiratory infection synthroid 25mcg otc, and these are discussed briefly below: 1. The investigators may assess the blood levels in the population before and after the intervention. If it is done without a comparison group, there is the limitation that an increase in blood level vitamin D due to other factors is not being rigorously controlled. For example, what if the study were conducted between May and July in a Northeastern state where sunlight exposure changes dramatically during this time In this instance, it would be important to have a comparison group that is tracked during the same time interval and that is not provided with the vitamin D supplement; their vitamin D levels at 0 and 12 weeks would be used to inform on background changes in the population and allow the investigators to hone in on the changes due to the supplement alone. Clinical trials without a comparison group are often done during pilot phases of research, to establish feasibility or acceptance or safety, and are often followed up by more rigorous designs. The main benefit of this is that it can potentially minimize confounding by both known and unknown factors. Mathematically speaking, if assignment to the intervention is done randomly, there should be no association between the intervention and other factors-thus, a factor that may have been a "common cause" of the exposure and outcome is now no longer associated with the exposure of interest (or intervention). Because of chance, particularly when there are small numbers, it is possible that the randomization plan will not adequately address confounding-so please check. If the participant or her/his managing physician is unaware as to which group the participant is assigned, this minimizes the chance that the participant or the physician may report on signs or symptoms of the disease or possible side effects in a biased way. For example, if the participant is not masked and knows that s/he is on the drug intervention, perhaps s/he will downplay any small symptoms, or postpone going to the physician for follow-up treatment because s/he believes that the drug is working. In contrast, one can easily imagine the opposite occurring among participants who know they have not received the drug intervention. These individuals may be more likely to report to the physician for further followup at early development of symptoms. There is also a third level of masking that commonly occurs, whereby the statistician who analyzes the data can conduct the analysis by comparing two groups (A vs B), without knowing which group actually received the treatment or placebo. Other scientific investigators on the trial are also typically "masked" whenever possible. Follow-up-Follow-up refers to observing participants over time and assessing the development of the outcomes of interest. This means that all participants enrolled and randomized are tracked and followed to see who develops the outcome and who does not, over the follow-up interval. If participants cannot be observed, then we have an incomplete picture of who develops the outcomes and who does not. In some situations, if the reason for the losses to follow-up are related to the exposure of interest (intervention) or to the outcome of interest, then study results could become biased. Therefore, it is particularly important to develop study procedures that allow the investigator team to keep track of study participants and assess them periodically for the development of the diseases or outcomes of interest. When a study experiences losses to follow-up, it is good practice to examine the baseline characteristics of those who stay in the study, and those who drop out or become lost to follow-up, as a way to explore if these participants differed in some way. A more rigorous clinical trial will have a control group, randomization, multilevel (participant, statistician/other investigators, treatment administrator) masking, and minimal losses to follow-up. There is a natural progression of evaluation of any new agent, device, or intervention and this is divided into "phases. Usually, preclinical work is conducted first in cell-line and animal models, to observe and document how that drug works in other systems. Phase 3 trials are conducted on hundreds to thousands of individuals who have or are at risk for the disease of interest. Once there is compelling evidence from preclinical studies suggesting that an agent may offer benefit in a human disease, then, a series of clinical trials may be mapped out for evaluation in humans. Phase 4: Long-Term Effects A phase 4 clinical study is conducted after the drug or agent has already been approved for use by the general public, and it is conducted to observe the long-term effects of the therapy. First, a phase 0 trial may be done in a small number of people and at a low (subtherapeutic) dose, just to test whether the agent has the expected effects on biological pathways in humans. A phase 0 trial seeks to evaluate whether the agent has the pharmacokinetic effects in humans that one would expect, based on the evidence to date, likely from observational studies or preclinical models. A phase 0 trial is usually conducted in a small number (10) of healthy volunteers. Efficacy is how well a therapy impacts biology or a disease under controlled, ideal conditions. For example, imagine that one is studying whether vigorous aerobic exercise prevents cancer progression. One may observe that a supervised exercise prescription that is implemented at a gym, with a trainer, and among individuals who are highly motivated and adherent (eg, who show up for all their exercise sessions) has a biological benefit in deterring cancer progression, based on assessing changes in intermediate tumor markers, and therefore concludes that the exercise prescription is efficacious. The results of this trial may be very different and maybe no benefits are observed. Not necessarily-it could be that the participants in the second study did not execute the prescribed exercise with the same rigor, intensity, or duration as was experienced in the more controlled supervised setting, and therefore one might conclude that while the exercise prescription had efficacy, the provision of the exercise prescription and education was not effective. A phase 1 trial is usually conducted in <100 people and is designed to test the safety of the drug, often at different doses. For example, different groups of participants in the study may be given different doses of the drug, spanning a range from low to high. Then, the participants are observed to determine what type of side effects they experience at the different doses. A phase 1 trial may be conducted in healthy volunteers, or in the population with the disease of interest. The goal of a phase 1 study is to check that the drug is safe, or that a particular dose of the drug is "safe" and ready to be evaluated further for efficacy. The goal is to identify the dose that appears to have the most biological effect or promise of biological impact, while also balancing side effects. Next, a phase 2 trial may be conducted to evaluate the efficacy and safety profile of the agent in the target population. A phase 2 trial usually consists of a few hundred participants (300), and the outcome is some measure of the biological impact or potential for efficacy on the target disease. For example, the ultimate goal might be to test whether a drug prevents prostate cancer death in individuals with localized prostate cancer. Intention to Treat In a randomized controlled trial, it is important to conduct the main analyses following the "intention to treat" principle. This means that the study population should be analyzed in terms of their original randomization assignment and not according to what they actually do. For example, if a participant is randomized to placebo in a study examining the effects of aspirin on cancer incidence versus placebo, but medical chart review during the trial shows that by chance the participant took aspirin regularly, that participant should still be analyzed as assigned to placebo. Phase 3: Scaleup If a phase 2 trial indicates that the drug may have some therapeutic benefit in a small number of people with a certain disease, then a phase 3 trial is conducted to evaluate the agent more comprehensively for its efficacy, safety, and effectiveness. In a phase 3 trial, one would design a study that could observe an outcome such as prostate cancer death. When conducted well, they should minimize the potential for recall bias and confounding, and the cause (the intervention or exposure) definitely precedes effect (outcome). Occasionally, a trial may accommodate a few interventions simultaneously, but this usually requires the addition of more arms or groups to the trial, and increases the sample size and level of complexity. This means that one cannot study the full range of the exposure and needs to be fairly confident that the dose selected is biologically meaningful in that population for that outcome, before starting the study. Hence, the phases of clinical trials discussed above are all focused on fine-tuning these characterizations about the dose of the intervention in a methodical and incremental way, before launching a full-scale phase 3 trial. In contrast, observational studies are often useful for examining the association between an exposure and an outcome across the spectrum of levels of that exposure. It is best if there are both observational cohort and early phase trial data available to inform on the best dose for a phase 3 trial. This may be a case where the duration of the intervention is too short to observe an effect. In a similar fashion, there may be particular timepoints in the life course when the intervention is more impactful on the outcome of interest. For example, when considering the complex relationships between sex hormones and later development of cancer, exposures during puberty or in utero might be especially important for the development of cancer decades later. A related concept is the recognition that certain interventions work best during certain phases of the disease. For example, in the nutrition and cancer literature, there are examples where supplementation had a large impact in one population but not another, likely because the populations had different levels of dietary sufficiency at the beginning of the study (see "Learning Example" section below). Therefore, the ability to randomize someone to a treatment is ethically grounded in the concept that our knowledge is in equipoise; we truly do not know whether the intervention is going to affect the outcome, and there is no evidence of superiority of one strategy over the other because data are equivocal. This means that there are data supporting varying outcomes-no effect, benefit, or possible risks.
Synthroid 100 mcg on-line
Side effects include gastrointestinal intolerance symptoms 7dp5dt 150mcg synthroid with mastercard, palpitations, headache, agitation, anxiety, and increased blood pressure (precautions are advised in men with cardiovascular disease). Trazodone is also not recommended; efficacy in pooled analyses was statistically equivalent to placebo. Side effects include drowsiness, nausea, emesis, blood pressure changes (both hypotension and hypertension are reported), urinary retention, and priapism (especially at therapeutic antidepressant levels) (Montague et al, 2005). Papaverine Papaverine, an alkaloid isolated from the opium poppy, induces relaxation of cavernous smooth muscle and penile vessels via nonspecific inhibition of phosphodiesterase. Scar tissue can be prevented by >5 minutes of compression of the injection site to reduce bleeding and trauma. Dosage and Administration Patients must have the first injection performed by medical personnel and receive appropriate training and education before home injection. Lower doses are recommended for management of neurogenic and psychogenic impotence. It is metabolized by the enzyme prostaglandin 15-hydroxydehydrogenase, which has been shown to be active in human corpus cavernosum. It is imperative that the clinician prescribing intracavernous therapies emphasize to the patient that priapism represents a urologic emergency and that any erection lasting > 4 hours necessitates urgent medical evaluation. In patients with cardiovascular disease, monitoring of blood pressure and pulse is recommended (Montague et al, 2003). A combination of vasoactive intestinal polypeptide and phentolamine has also been used in other countries. Multiple series have demonstrated patient satisfaction rates of >75% and low rates of priapism or fibrosis. Side effects are reduced, as smaller amounts of each agent are required, and the targeting of multiple pathways increases therapeutic efficacy. Contraindications Intracavernous injection is contraindicated in patients with sickle cell anemia, schizophrenia, or another severe psychiatric disorder. In patients with poor manual dexterity, the sexual partner can be instructed to perform the injection. After the penis is engorged, a constricting ring is applied to the base to maintain the erection. The ring may be uncomfortable or painful; to avoid injury, it should not be left in place for less than 30 minutes. The penile skin may be cold and dusky, and ejaculation may be trapped by the constricting ring. Complications include penile pain and numbness, difficult ejaculation, ecchymosis, and petechiae. Patients taking aspirin or Coumadin (warfarin) should exercise caution when using these devices. In some patients, the device can produce an erection that is of sufficient rigidity for coitus or engorge the glans for men with glanular insufficiency. In patients with severe vascular insufficiency, the device may not produce adequate erection. Traumatic venous leak is usually due to localized damage to the tunica albuginea or formation of a "fistula" between the corpus cavernosum and corpus spongiosum. Repair of the tunica or closure of the fistula can result in significant improvement of erectile function. In older men with chronic systemic diseases, venous leakage is usually caused by atrophy of the cavernous smooth muscle and degeneration of tunica albuginea; ligation of penile vein will only produce transient improvement and is not recommended. Penile prostheses are divided into three general types: malleable (semirigid), mechanical, and inflatable devices. The malleable devices are made of silicone rubber, and several models contain a central intertwined metallic core. The mechanical device is also made of silicone rubber but contains polytetrafluoroethylene-coated interlocking polysulfone rings in a rod column, which provides rigidity when the rings are aligned in a straight line and flaccidity when the penis is bent. Inflatable (hydraulic) devices are further divided into two- and three-piece devices. Two-piece inflatable prostheses consist of a pair of cylinders attached to a scrotal pump reservoir. Recent innovations in penile prosthetics include antibiotic and hydrophilic-coated devices (infection rate <1%), lockout valves to prevent autoinflation, and a Follow-up Strategy Regardless of the treatment regimen chosen, follow-up is essential to ensure optimal outcomes. Modification of lifestyle, diet change, regular exercise, and smoking abstinence or cessation should be reassessed and encouraged at each clinic visit. The most commonly used technique for penile revascularization is placement of a bypass from the inferior epigastric artery to the dorsal artery or deep dorsal vein of the penis. Penile venous surgery is also indicated only in young men with congenital or traumatic venous leakage. The external ejaculation process involves the somatomotor efferent of the pudendal nerve to contract the bulbocavernous muscle. Since this action is involuntary, however, integrated autonomic and somatic action is required. These include involuntary rhythmic contractions of the anal sphincter, hyperventilation, tachycardia, and elevation of blood pressure. Except for nocturnal emissions, or "wet dreams," emission and ejaculation require stimulation of the external genitalia. Impulses traveling from the pudendal nerves reach the upper lumbar spinal sympathetic nuclei. Efferent signals traveling in the hypogastric nerve activate secretions and transport sperm from the distal epididymis, vasa deferentia, seminal vesicles, and prostate to the prostatic urethra. Coordinated closing of the internal urethral sphincter and relaxation of the external sphincter direct the semen into the bulbous urethra (emission). Some propose that the definition of premature ejaculation should include rapidity of ejaculation, lack of control, and negative consequences (McMahon et al, 2004). Although time to ejaculation is prolonged, a significant percentage of men experience decreased pleasure (penile numbness) or loss of erection. Its pharmacokinetic profile is characterized by rapid absorption, a short initial half-life of 1. A history of disease or surgery is helpful in differentiating emission failure from retrograde ejaculation. If microscopic examination confirms the presence of sperm in bladder urine after a dry ejaculation, retrograde ejaculation can be diagnosed. Internal iliac arteriogram in the flaccid penis (A) shows poor visualization of penile arteries, simulating occlusion (arrow). After intracavernous injection of 60 mg of papaverine (B), all the branches of the penile artery are well visualized. Retrograde ejaculation is usually the result of dysfunction of the internal sphincter or the bladder neck, as seen after prostatectomy, with -blocker therapy, and in autonomic neuropathy due to diabetes. Elimination of -adrenergic blockers may cure some patients with emission failure or retrograde ejaculation.
