
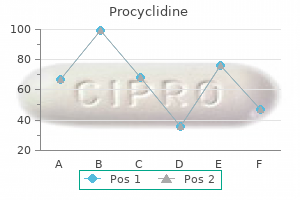
Generic 5 mg procyclidine with amex
Conclusions A strategy of endovascular repair was not associated with significant reduction in either 30-day mortality or cost symptoms xanax withdrawal cheap 5mg procyclidine free shipping. Longer-term cost-effectiveness evaluations are needed to assess the full effects of the endovascular strategy in both men and women. Any trial in the emergency setting is challenging, including giving fully conscious patients a chance to give consent rapidly and using relative and other consents where this was not possible. A decade earlier, I had seen my father die of a more proximal aortic rupture after three hospital transfers over 2 days without any intervention, and I wanted current patients to fare better. In this emergency setting, unselective randomization was challenging and about 10% of each randomized group did not receive their allocated treatment (mainly operational or morbidity issues). At 30 days, mortality was similar (35%) in each group, although women (22% of the cohort) had lower mortality in the endovascular strategy group (24% vs. Other analyses showed that aortic morphology affected survival, a long proximal aneurysm neck favoring survival irrespective of treatment modality. Patients had an input to trial design and running: their preferred outcomes relating to early discharge home and quality of life were significantly better in the endovascular strategy group and their most dreaded outcome (amputation) also was lower after endovascular repair. To provide full health economic outcomes, all patients were followed up for at least 3 years. Interestingly, after 3 years mortality was lower in the endovascular strategy group (48% vs. After 3 years, women continued to gain more survival benefit from the endovascular strategy than men. Pragmatic randomized trials can be conducted successfully in the emergency setting, but should not focus only on short-term outcomes. Michaels 40 Acute care surgery is a discipline born of necessity and forms a core element of our health care safety net. Recognition that many surgical emergencies were not being managed in a timely fashion led to an evolution of trauma and critical care into a more encompassing specialty providing care to all forms of emergencies requiring surgical interventions. This evolution has been a natural extension of the training, experience, and temperament of trauma surgeons, and the application of a systemsbased approach so characteristic of mature trauma programs has greatly benefited this essential component of health care (Institute of Medicine Committee, 2006; Kutcher and Peitzman, 2017). Understanding how the application of these skills- clinical, administrative, and academic-to the global burden of disease that is amenable to surgical intervention can provide many opportunities for a well-rounded acute care surgeon. Global surgery is an area of study, research, practice, and advocacy that seeks to improve health outcomes and achieve health equity for all people who require surgical care, with a special emphasis on underserved populations and populations in crisis. It uses collaborative, cross-sectoral, and transnational approaches and is a synthesis of population-based strategies with individual surgical care (Dare et al. Surgery, because it is neither a disease entity nor does it target a specific demographic, has not been a priority for global health initiatives. The recognition of the enormous proportion of health problems requiring surgical intervention has begun to change that perception (Hedges et al. The Commission was comprised of 25 commissioners and hundreds of collaborators from more than 110 countries and 6 continents. Their report, "Global Surgery 2030: Evidence and Solutions for Achieving Health, Welfare, and Economic Development" (Meara et al. In 2015, 5 billion people lacked access (in four dimensions: timeliness, surgical capacity, safety, and affordability) to safe, affordable surgical and anesthesia care when needed. In 2012, of the more than 300 million surgical procedures performed worldwide, only 6. The distribution of unmet need is greatest in sub-Saharan Africa and south and southeast Asia, and a conservative estimate is that an additional 143 million surgical procedures are needed each year to save lives and prevent disabilities. In addition, when non-medical costs of illness and injury are considered, another 48 million cases of catastrophic expenditure occur annually. Investment in surgical and anesthesia services is affordable, saves lives, and promotes economic growth. The authors state: "broad scale-up of quality surgical services will prevent deaths, limit disability, palliate suffering, promote economic growth, and help achieve maximum gains in health, welfare, and development for all. These indicators include access to timely essential surgery, surgical specialist workforce density, surgical volume, perioperative mortality rate, and protection against catastrophic expenditure. Acute care surgeons have always served as the last line of defense and frequently the first point of contact with the health care system for the most physiologically and socially challenged. Trained in emergency surgery, critical care, trauma, and often systems development, administration, quality, and research, acute care surgeons have opportunities to contribute meaningfully, and these opportunities are becoming both more prevalent and more valid (Krishnaswami et al. This Institute of Medicine report outlines the challenges facing emergency care systems as they struggle to provide, in addition to hospital-based emergency and trauma care, safety net support for the uninsured, public health surveillance, disaster preparedness, and other essential functions. This article outlines the origins and evolution of acute care surgery as a specialty and advocates for the inclusion of elective general surgery into spectrum of care provided by surgeons typically experienced in trauma, critical care, and emergency surgery. Surgery has an important role to play in primary health care, and surgery will play its proper role in bringing the people of the world nearer to the goal of health for all by the turn of the century. This short viewpoint outlines the importance of a robust definition for the multidisciplinary fields that constitute global surgery. The authors emphasize that global refers not only to geographical considerations but also to the holistic nature of surgical service development, practice, and evaluation. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Four-and-a-half billion people do not have access to safe, affordable surgical and anesthesia care. Thirty-three million individuals face catastrophic health expenditure due to payment for surgery and anesthesia care each year. An additional 48 million cases of catastrophic expenditure are attributable to the non-medical costs of accessing surgical care. More than 30% of the global burden of disease requires a surgical or anesthesia intervention. This estimation is robust to multiple estimation methods and avoids limiting the delineation of "surgical disease" only to patients who end up on an operating table. The scale-up of a functional surgical system could have a beneficial impact on a large portion of the global burden of disease. Estimate of the global volume of surgery in 2012: An assessment supporting improved health outcomes. A single-procedure cesarean delivery comprised almost a third of surgical volume in the most resource-limited settings. Surgical care is an essential part of health care and is associated with increased life expectancy, yet many low-income countries fail to achieve basic levels of service. Improvements in capacity and delivery of surgical services must be a major component of health system strengthening. An academic career in global surgery: A position paper from the Society of University Surgeons Committee on Academic Global Surgery. This paper reviews the development of academic global surgery, delineates the framework and factors critical to training global surgeons, and proposes models for establishing an academic career in this field. The task will be most successful (1) if the epidemiologic pattern in each country is taken into account by focusing on those surgically treatable conditions with the highest burdens; (2) if emphasis is placed on those surgical services that are most cost effective and most feasible to scale up; and (3) if efforts are harmonized with local priorities and with existing global initiatives. The ethical principles of maximally and transparently engaging with and deferring to the interests and needs of local surgeons and their patients are of paramount importance. No longer was there a singular method to deliver nutrition, and the benefits of supporting patient physiology through intravenous nutrition were about to flourish in the literature. Further advances came in the 1970s where specific lipid emulsions (macronutrient) were added to the complex carbohydrate, mineral, and salt formulations (Fell et al. Though complex physiologic interactions are beyond the scope of this chapter, parenteral nutrition induced liver disease is less common and its safety has vastly improved. Among clinicians, patients, and even hospital administrators, few can deny the contributions of enteral and parenteral nutrition to the routine or critically ill patient (Herbert et al. The debates of enteral versus parenteral nutrition continue but they should be evidenced based (Sackett, 1997; Chang and Lee, 2018). Both references hold significant importance regardless of topic, and the subject of initiating early versus late parenteral nutrition in the intensive care unit should also be evidence based. Enteral nutrition has been used in hospitalized patients with great success (Zhuang et al. It is easily delivered orally, directly into the stomach, the duodenum, or the jejunum (Gramlich et al. Critically ill patients have similar aspiration risks when fed into the stomach or duodenum. Enteral nutrition is cost effective, simple to prepare, and can be delivered in a variety of methods (Gabriel and Ackermann, 2004).
Procyclidine 5 mg without prescription
From social structural factors to perceptions of relationship quality and loneliness: the Chicago health symptoms 6dpo order procyclidine master card, aging, and social relations study. Loneliness is a unique predictor of age-related differences in systolic blood pressure. As we said, loneliness (not living alone) explains individual differences in sleep quality: Reply. Loneliness predicts reduced physical activity: Cross- sectional and longitudinal analyses. Loneliness predicts increased blood pressure: 5-year cross-lagged analyses in middle- aged and older adults. Loneliness and social isolation as risk factors for mortality: A meta- analytic review. A short scale for mea sur ing loneliness in large surveys: Results from two population-based studies. Loneliness predicts pain, depression, and fatigue: Understanding the role of immune dysregulation. Urinary cortisol levels, cellular immunocompetency, and loneliness in psychiatric inpatients. Perceived social isolation is associated with altered functional connectivity in neural networks associated with tonic alertness and executive control. The lonely mouse: Verification of a separation-induced model of depression in female mice. Perceived stress mediates the relationship between emotional loneliness and sleep quality over time in older adults. Contrasting responses to intruders and to involuntary separation by monogamous and polygynous New World monkeys. Loneliness, depression, and inflammation: Evidence from the multi- ethnic study of atherosclerosis. Trait sensitivity to social disconnection enhances pro-inflammatory responses to a randomized controlled trial of endotoxin. The impact of loneliness on quality of life and patient satisfaction among older, sicker adults. The relationship between perceived loneliness and cortisol awakening responses on work days and weekends. Loneliness accentuates age differences in cardiovascular responses to social evaluative threat. Loneliness, social isolation, and behavioral and biological health indicators in older adults. Loneliness and neuroendocrine, cardiovascular, and inflammatory stress responses in middle- aged men and women. Depressive behav ior in adult monkeys following separation from family environment. The relation of social isolation, loneliness, and social support to disease outcomes among the elderly. Loneliness and the metabolic syndrome in a population-based sample of middle- aged and older adults. Social learning provides unique opportunities to meet such challenges by helping us to reduce uncertainty, update social expectations, and ultimately maximize social gains by developing close relationships. Our days are often spent navigating a complex and dynamic social environment in pursuit of various goals. We typically interact with others on a daily basis who comprise multiple interleaved social networks. Even when we are ostensibly alone, we can still be immersed in a social world when consuming media through a book, television, or the Internet. Given the preponderance of our lives spent embedded in a social context, a key question is understanding how and what types of information we learn from the social environment. Humans have strong motivations to approach resources, while avoiding harm for self and others, and reduce uncertainty about the world (Crockett, KurthNelson, Siegel, Dayan, & Dolan, 2014; FeldmanHall & Chang, 2018). We are also intensely driven to form close relationships with others (Baumeister & Leary, 1995). Similarly, we can also reduce our uncertainty about others by learning about their beliefs, motivations, preferences, and overall character-for example, how does a certain person think about the world The reduction of social uncertainty can facilitate subsequent social interactions and the development of close relationships. This article will review several aspects of social learning, such as how we learn: from and about others, what other people are thinking, and how people are connected to each other. However, rather than simple sensory or affective signals, this information is often gleaned through the lens of social cognition. Thus, much of the literature reviewed involves interactions between neural systems supporting learning, affect, and social reasoning. Learning from Others We are motivated at once to both maximize our selfinterest and minimize our uncertainty about the world. This requires us to frequently switch between exploiting what we know and exploring the unknown (Cohen, McClure, & Yu, 2007). Alternatively, it can be learned from directly communicating these experiences, such as being explicitly told which is the best option. Observational learning Observing the outcomes of others while minimizing our own costs is vital for survival from the earliest stages of life. This extension of Pavlovian learning can provide key insight into the nature of threats in the environment and how to avoid them, thereby ensuring survival (reviewed in Olsson & Phelps, 2007). The observational learning of stimuli 949 paired with aversive outcomes results in equivalent learning as direct experience. Importantly, the extinction of a learned fear association can transmit vicariously across individuals (Golkar, Selbing, Flygare, Ohman, & Olsson, 2013), suggesting that this method of gleaning information from others aids in reducing uncertainty and avoiding harm. Similarly, we can make predictions about whether success will come to others and adjust our expectations after observing their outcomes. Taken together, observational learning is a powerful social mechanism-through which we learn about the environment while reducing exposure to possible harm-that relies heavily on neural circuits supporting learning from direct experiences. Social nudges Efforts to reduce uncertainty in the social world are often complicated by considerations of risk. In such situations we may look to others as a guide for whether to be risky or more prudent. Hearing from a friend or colleague who just invested in a stable rather than a more volatile stock may sway or nudge our own investments, with positive or negative consequences. Social nudges can also arise from evaluative feedback from peers, which is particularly important to consider given the dramatic rise in engagement with social media (Rodman, Powers, & Somerville, 2017). In sum, taking cues from others can significantly influence day-to- day decisions, particularly with respect to reducing uncertainty and validating our own choices. Instructed learning A more explicit way of reducing uncertainty comes through directly receiving rules about environmental contingencies from another person. For example, being provided (incorrect) instructed information about which of two stimuli will most likely lead to a reward will bias choice toward ostensibly more rewarding options, which hold even in the face of inconsistent feedback. Instructions can also impact our ability to learn to avoid harm via corticostriatal circuitry during reversal learning (Atlas, Doll, Li, Daw, & Phelps, 2016). Interestingly, instructions from others concerning the reliability of upcoming feedback may moderate these biased processes (Schiffer, Siletti, Waszak, & Yeung, 2017). This requires building a model of a person that can predict their behav ior across a range of contexts. Trait learning and impression updating We often form simple models of others by trying to infer their traits. Upon meeting someone novel, we might make implicit judgments about their level of trustworthiness or approachability based on facial characteristics (Todorov, Baron, & Oosterhof, 2008), assumed knowledge of their affiliations with a particular social group (Stanley, Sokol-Hessner, Banaji, & Phelps, 2011), or their beliefs about the world. These snap judgments contribute to the initial models we construct about others based on social approach and avoidance motives (Willis & Todorov, 2006). Navigating our social landscapes requires constantly updating our initial models of others.
Diseases
- Chronic spasmodic dysphonia
- Cacchi Ricci disease
- Genetic reflex epilepsy
- Beta-thalassemia major anemia
- Scleromyxedema
- Skeletal dysplasia San diego type
- Walker Dyson syndrome
- Pickardt syndrome
Order generic procyclidine canada
A Large- Scale Network for Lexical Semantic Processing the neuropsychological and neuroimaging literature on lexical concept representation and retrieval is vast and can only be broadly sketched here medications with dextromethorphan cheap procyclidine 5mg overnight delivery. In the neurological syndrome known as transcortical sensory aphasia, patients show an inability to understand spoken and written words despite normal hearing, vision, and phonological abilities, suggesting either damage to , or an inability to access, concept representations. Lesions causing the syndrome are generally large, involving ventral temporal, posterior parietal, and/or prefrontal cortex in the left hemisphere (Alexander, Hiltbrunner, & Fischer, 1989; Jefferies & Lambon Ralph, 2006; Otsuki et al. Beginning around 1990, systematic work on patients with the temporal lobe variant of frontotemporal dementia (semantic dementia, semantic variant primary progressive aphasia) showed that bilateral damage focused on the anterior half of the temporal lobe cortex can also produce a profound loss of lexical concept knowledge (Hodges, Patterson, Oxbury, & Funnell, 1992; Snowden, Goulding, & Neary, 1989). The lesion evidence thus suggests a broadly distributed network for semantic processing, involving much of the temporal lobe, as well as large regions of inferior parietal and prefrontal cortex. Binder, Desai, Conant, and Graves (2009) performed a voxel- wise meta- analysis of 87 neuroimaging studies examining the retrieval of general semantic knowledge. A notable feature of these experiments is that the lexical stimuli were chosen without regard to sensorimotor content or category membership; thus, the results can be interpreted as showing common brain areas involved in semantic processing regardless of specific conceptual content. Each study had to include a nonsemantic comparison task with controls for phonological, orthographic, and cognitive- control demands of the semantic task. The parietal and temporal zones are high-level crossmodal association areas distant from primary sensory and motor cortices and positioned at points of convergence across multiple sensory streams (Jones & Powell, 1970; Mesulam, 1985; Sepulcre, Sabuncu, Yeo, Liu, & Johnson, 2012). Damage to this region impairs the ability to retrieve conceptual information, particularly when the context allows for many salient competing alternatives, the retrieval process is more complex or ambiguous, or retrieved information must be maintained in short-term memory. In contrast, damage to dorsomedial prefrontal cortex (superior frontal gyrus) does not impair concept selection per se but instead the ability to autonomously activate the selection process, manifesting as an inability to spontaneously generate nonformulaic language when no constraining cues are given (Alexander & Benson, 1993; Robinson, Blair, & Cipolotti, 1998). The Case for Experience-Based Concept Representations As mentioned above, the representational content of conceptual knowledge in the brain has been a matter of intense ongoing debate. The "concepts as abstract symbols" approach, which has had many useful applications in artificial intelligence and cognitive science. For example, people can pick out the referent of a word-that is, indicate a thing out in the environment that corresponds to the meaning of the symbol. A conceptual representation composed purely of symbols and their associations with other symbols would not have this capacity, demonstrating that the symbols are not "grounded" in physical reality (Harnad, 1990). They are more like the entries in a monolingual dictionary for a language that one does not know: looking up a word only leads to a set of more words one does not know. People also say they experience feelings, mental images, and other subjective qualia (such as the feeling of sadness or the experience of the color red) when they think about concepts. Such experiences are at the core of what distinguishes people from very sophisticated symbol- computing devices. Finally, symbol-based models are largely silent on the question of how conceptual knowledge is acquired. The view that concepts are acquired as generalizations from everyday experiences provides a natural account of many of these phenomena. Over the course of many real-world experiences with a particular entity, invariant aspects of these sensory, motor, and affective experiences are encoded as increasingly abstract information within modality- specific processing systems. It is easy to see how perceptual "simulation" in these systems during concept retrieval allows people to indicate real-world referents of concepts and experience mental images and other qualia. It has been argued that sensorimotor systems are activated merely as a postconceptual epiphenomenon-that is, that this activation is not critical for concept understanding (Mahon & Caramazza, 2008). Countering this assertion is evidence that patients with specific motor (Bak & Hodges, 2004; Boulenger et al. Underlying some of the ongoing debate about these data are varying interpretations of what sensorimotor cortex refers to . An exclusive focus on primary cortices is unwarranted since all sensory and motor systems in the brain are known to be hierarchically organized, with increasingly abstract. This explains why patients can have severe motor or perceptual deficits from primary cortex lesions or damage in subcortical white matter pathways but have little or no corresponding impairment of modality- specific concept processing (Mahon & Hickok, 2016). The neural representation of concepts that do not have simple physical features presents something of a challenge to embodiment theories. Such "abstract" concepts make up a large portion of the lexicon (Recchia & Jones, 2012) and include, for example, products of cognition (concept, theory, idea), cognitive states or activities (believe, ponder, doubt), abstract situational entities (criterion, clause, factor), abstract attributes (aspect, demeanor, extent), complex social acts and situations (cheat, imply, argument), human mental traits (honesty, curiosity, wisdom), and so on. Barsalou (1999) notes that while such concepts do not have physical features, they are nevertheless learned from experiences, albeit often complex experiences that can include purely mental phenomena. Thus, they could be represented in the brain by spatially and temporally complex scenarios involving physical and mental events, rather than by simple sensorimotor information. Certain types of experience might also play a larger role in learning and representing abstract concepts, compared to concrete concepts. Abstract concepts tend to have strong affective and social content (Borghi, Flumini, Cimatti, Marocco, & Scorolli, 2011; Kousta, Vigliocco, Vinson, Andrews, & Del Campo, 2011; Vigliocco et al. Concept Representation in a Hierarchical Convergence Architecture the model shown in figure 76. The model distinguishes three levels of representation, referred to here as unimodal, multimodal, and transmodal. At the unimodal level, evidence to date implicates ventral visual areas in retrieving conceptual color knowledge (Fernandino, Binder, et al. Emotion can also be considered a unimodal experience, and many imaging studies have examined brain activation as a function of the emotional content of words or phrases. There is a clear preponderance of activations in the temporal pole and ventromedial prefrontal cortex (Binder & Desai, 2011), which are areas believed to support cognitive aspects of emotion (Etkin, Egner, & Kalisch, 2011). Multimodal sensory areas have been extensively documented, yet relatively few studies have addressed multimodal combinations in word meaning. Concept selection and information flow (depth of processing) are controlled by initiation and selection mechanisms in dorsomedial and inferolateral prefrontal cortex. Other regions showed sensitivity to both shape and action (but not color, sound, or motion) content. One of these, the anterior supramarginal gyrus, is located near tertiary somatosensory association cortex and probably combines high-level proprioceptive, motor, and haptic shape information. Another, at the junction of the posterior middle temporal gyrus and the anterior occipital lobe (named the lateral temporal-occipital area by Fernandino, Binder et al. Both areas have been consistently implicated in object- directed action planning, action perception, and action execution (Caspers, Zilles, Laird, & Eickhoff, 2010; Grosbras, Beaton, & Eickhoff, 2012; Lewis, 2006), as well as in prior meta-analyses of tool and action concept processing (Binder et al. At the highest level of convergence are brain regions that combine information from many experiential domains. Debate continues regarding the existence of such regions and the representational content they encode. Information encoded at these high- level hubs is variously claimed to be amodal. We use the neutral term transmodal to suggest a high level of abstraction arising from broadly multimodal conjunctions. Highly abstract, transmodal representations are thought to have several functions in semantic cognition (Binder, 2016). They provide a computationally efficient means of capturing multimodal conceptual similarity (Patterson, Nestor, & Rogers, 2007; Rogers & McClelland, 2004), they provide a mechanism for learning purely thematic (non-feature-based) word associations and word definitions through language (Binder, 2016; Dove, 2011; Hoffman, McClelland, & Lambon Ralph, 2018; Vigliocco et al. Conceptual content activated by a word is not limited to intrinsic attributes of the target concept but also typically includes a network of associated concepts and pragmatic information (Hare, Jones, Thomson, Kelly, & McRae, 2009); frontal lobe mechanisms select. Large, long-range white matter fasciculi that enable rapid communication between frontal, temporal, and parietal cortices- principally the inferior fronto- occipital fasciculus-likely play a central role in these frontal-posterior interactions (Duffau et al. Gray matter density of auditory association cortex relates to knowledge of sound Lexical Semantic Access Given the spatial proximity of the superior temporal lobe phoneme perceptual system to the lateral temporal conceptual hub (figure 76. Long-range temporoparietal white matter fasciculi-principally the inferior and middle longitudinal fasciculi (Zhang et al. Frontal lobe selection mechanisms are engaged to varying degrees during these processes depending on stimulus characteristics and task demands. For example, concept retrieval includes the transient activation of conceptual representations for phonological "neighbors" of the input word (Marslen-Wilson & Welsh, 1978); frontal lobe selection mechanisms likely play a role in inhibiting these activations. Similarly, context-based selection is 884 Language concepts in primary progressive aphasia.
Buy procyclidine with paypal
This is one of the earliest accounts of aphasia therapy medicine xifaxan purchase 5 mg procyclidine with amex, and it demonstrates that even 150 years ago, it was recognized that aphasic patients could potentially benefit from therapy. Today, many dif ferent aphasia treatment approaches are used in clinical practice, and the focus varies from impairmentbased approaches that directly target speech and language improvement to more functional approaches that emphasize successful communication over lessening the severity of the language impairment. Voxel-based morphometry revealed distinct regions where atrophy was predictive of speech (A), lexical (B), or syntactic (C) deficits (Wilson et al. Dorsal and ventral language tracts were identified with diffusion tensor imaging (D). The degeneration of dorsal tracts was associated with deficits in syntactic comprehension (E) and production (F), while the degeneration of ventral tracts had no effects on syntactic comprehension (G) or production (H) (Wilson et al. In the inferior frontal gyrus (J, K) and posterior temporal cortex (L, M), modulation of functional signal by syntactic complexity was predictive of accuracy (J, L), but nonspecific recruitment for the task was not (K, M) (Wilson et al. This is typically referred to as spontaneous recovery, and its extent can vary widely across patients. The bulk of spontaneous aphasia recovery occurs within the first 3 months after stroke onset (Enderby & Petheram, 2002; Pedersen et al. Although it can be difficult to predict if, and how much, individual patients will recover, some general guidelines exist. One of the strongest predictors of poor outcome is larger lesion size (Kertesz, 1988). This makes sense since patients with more extensive cortical damage have less residual brain tissue to assume whatever language functions were lost as a result of the stroke. Naturally, the patients with the largest lesions also tend to have the most extensive language impairment, which is probably why overall aphasia severity predicts long-term recovery (Kertesz, 1988; Kertesz, Harlock, & Coates, 1979). Patients with relatively greater damage to perisylvian regions experience less recovery compared to patients with similar lesion size but less perisylvian involvement, and damage to temporal lobe language areas is more likely to result in lasting language deficits than damage to frontal lobe language areas (Metter et al. Stroke type matters, as patients with ischemic stroke experience less early recovery compared to those with aphasia as a result of hemorrhagic stroke (Holland, Greenhouse, Fromm, & Swindell, 1989). In the acute stage, the sequelae of hemorrhagic stroke are more complicated than in ischemic stroke, and hemorrhagic patients tend to be sicker than those with ischemic stroke, as indicated by higher mortality rates and longer stays in the hospital. However, a surviving hemorrhagic patient can expect to experience a greater return of function compared to patients with ischemic stroke. Even though the bulk of aphasia recovery occurs within the first year after stroke, aphasia severity can sometimes be quite dynamic in the chronic phase. In a longitudinal study, Holland, Fromm, Forbes, and MacWhinney (2017) followed individuals with chronic aphasia who were tested twice at least 1 year apart. They found that over half of their participants experienced improvements in overall aphasia severity that were greater than the standard error of mea surement, whereas approximately a quarter of the participants were stable, and the remaining participants declined. Brain Changes Associated with Aphasia Recovery What are the neural substrates that underlie recovery from aphasia It is clear that the mechanisms of recovery are different at dif ferent stages of recovery. In the acute poststroke period, reperfusion of the ischemic penumbra appears to be a major determinant of the rapid improvements that are often seen (Hillis et al. In the early subacute period (the first few weeks after stroke), there is some evidence that right frontal regions may play a compensatory role (Saur et al. Language outcome has been shown to be associated with the extent to which typical left frontal and temporal language regions can be activated by language processing (Griffis et al. Specifically, patients who fared well in treatment also experienced a significant increase in left-hemisphere activation, suggesting that recovery from anomia in chronic stroke may be mediated by the left hemisphere. In a follow-up study, Fridriksson, Richardson, Fillmore, and Cai (2012) related change in functional activity in perilesional cortex to change in correct naming. A regression analysis revealed that activation change in the perilesional frontal lobe was a predictor of correct naming improvement. Treatment-related change in the production of semantic paraphasias was most robustly predicted by activation change in the temporal lobe, while change in phonemic paraphasias was predicted by activation change involving both the left temporal and parietal lobes. These findings suggest that changes in activation in perilesional regions are associated with treated recovery from anomia. Other researchers have argued that the right hemisphere plays a major role in aphasia recovery. In a larger and more representative group, Crinion and Price (2005) showed that the recruitment of right posterior temporal cortex for narrative comprehension was associated with preserved comprehension in poststroke aphasia. However, this was not interpreted as a finding of reorganization per se because narrative comprehension depends on both temporal lobes in neurologically normal individuals, too. Whereas localized changes in brain activity may be important for aphasia recovery, it seems plausible that changes in functional network connectivity also play a role. In fact, it could be that changes in connectivity are the primary drivers of aphasia recovery. Anatomoclinical correlations of the aphasias as defined through computerized tomography: Exceptions. Reconciling time, space and function: A new dorsal-ventral stream model of sentence comprehension. Capturing multidimensionality in stroke aphasia: Mapping principal behavioural components to neural structures. Right anterior superior temporal activation predicts auditory sentence comprehension following aphasic stroke. Preservation and modulation of specific left hemisphere regions is vital for treated recovery from anomia in stroke. Revealing the dual Conclusion the study of aphasia has provided some groundbreaking findings in regard to the neuroanatomical organization of language. Much of this work has relied on lesion- symptom associations to infer which regions of the brain are crucial for, not just associated with, the execution of given speech or language tasks. Although the technologies and methodologies used in these studies have evolved enormously, especially in the last three decades, the basic premise of the studies has not changed: if a given cortical region or network supports a specific function, then damage to that region should cause an impairment in that same function. The influence of aphasia studies on the neuropsychological understanding of language is perhaps most evident in the current zeitgeist of dual- stream models that have become mainstream in the field. Although much of the work on aphasia has focused on understanding normal brain-behavior relationships, a parallel focus has centered on the clinical manifestations of speech and language impairment to inform clinical practice. Ideally, the study of aphasia will proceed with a united focus where basic science informs clinical research, and vice versa. Wilson and Fridriksson: Aphasia and Aphasia Recovery 913 streams of speech processing. Subcortical aphasia and neglect in acute stroke: the role of cortical hypoperfusion. Computer tomographic localization, lesion size, and prognosis in aphasia and nonverbal impairment. Lesion localization in aphasia with cranial computed tomography and the Boston Diagnostic Aphasia Exam. Differential diagnosis of aphasia with the Minnesota test: Administrative manual for the Minnesota Test for Differential Diagnosis of Aphasia (Vol. Anterior temporal involvement in semantic word retrieval: Voxelbased lesion- symptom mapping evidence from aphasia. Classifying the aphasias: A comparison of the Boston Diagnostic Aphasia Examination and the Western Aphasia Battery. Variable disruption of a syntactic processing network in primary progressive aphasia. Role of the contralateral inferior frontal gyrus in recovery of language function in poststroke aphasia: A combined repetitive transcranial magnetic stimulation and positron emission tomography study. The right inferior frontal gyrus and poststroke aphasia: A follow-up investigation. In contrast to the early days of psychology, which led to the parsing of human mental life and behav ior into subdisciplines for study. As successive generations of psychological scientists have recognized the value of using neuroscience techniques to understand the human mind, they have had to grapple with how to (re)connect the science from the subdisciplines of psychology.
Generic procyclidine 5mg without a prescription
Regardless symptoms bipolar order 5 mg procyclidine amex, these patients should be followed closely, as the risk of traumatic endophthalmitis is high. On the other hand, these cases can be quite gratifying, and occasionally, we are able to save the eye and restore excellent vision. Management of hyphema, repair of iridodialysi1, and repair of corneo1cleral lacerations. Open-globe injuries are rarely hopeless: managing the open globe calls for creativity and flexibility of surgical approacli tailored to the specific case. Incidence and visual outcome of endophthahnitis associated with intraocular foreign bodies. There is so much to cover-so many types of cases, so many possible approaches to each of these cases, and so much incredible variety. Still, starting with setup and preparation for surgery and basic vitrectomy techniques, we have moved through each of the core types of retina surgery. Try the techniques described in this pocket guide, but also use the basic principles to help you try other, varied techniques. In fact, we feel that the privilege ofbeing a vitreoretinal surgeon is truly a gift. Albert has no financial or proprietary interest in the materials presented herein. Crosson has no financial or proprietary interest in the materials presented herein. Thomley has no financial or proprietary interest in the materials presented herein. The patient incurred an Achilles tendon injury at work that necessitated surgical repair. Several weeks after the surgery, the patient continued to have excessive burning pain with associated swelling, persistent erythema, and piercing cold dysesthesias that encompassed the entire lower extremity involving the foot and calf up to the knee. Despite adequate healing, there is no real improvement in the intensity and nature of her pain. She then received a series of lumbar sympathetic blocks as well as medications in conjunction with physical therapy. In addition, allodynia of the right lower limb meant that she could not even have a bed sheet contact it. Diagnostic tests such as inflammatory markers, X-rays, magnetic resonance imaging studies, and bone scans can help exclude other causes and support the diagnosis. These criteria are applied in terms of symptomatic complaints in which case there must be three of the categories fulfilled as well as two distinct categories on physical examination. Not uncommonly, with progression of time, the physical findings can diminish in many patients, but others can remain with chronic edema, lower limb atrophy, and loss of range of motion in the toes and ankle. The use of membrane-stabilizing agents such as gabapentin, pregabalin, or topiramate may offer relief of neuropathic symptoms. Not uncommonly, the relief is modest, and antidepressant medications in the categories of serotonin and norepinephrine reuptake inhibitors or tricyclics are used to enhance analgesia. The current trend is to avoid traditional mu agonist opioids or at least maintain low dose. Finally, the use of ketamine infusions has been established in randomized control trials to offer short-term relief, but insurance coverage is not uncommonly an issue. Alleviation of the neuropathic component can still play a major role to facilitate rehabilitation that may permit more symptomatic control of the trophic changes. Multiple organ systems may be affected that can cause neurocardiogenic syncope, incontinence, feeling of shortness of breath, dysphagia, irritable bowel syndrome, and reflux disease. Patients lose a great deal of autonomy and self-worth that can exacerbate or lead to worsening anxiety and depressive states. There is a steep learning curve of the technology, and patients need to be able to familiarize themselves with the therapy to maximize their chances for relief. The patient may, out of pure desperation, demand the therapy even if the trial was of unclear benefit. Scenario (continued) this woman is counseled that initially she must have a psychological assessment before attempting a trial of stimulation. She agrees, and after this assessment by a qualified professional well versed in evaluating patients with chronic pain and other chronic disorders for implanted devices and their expectations, she is cleared for the trial. The trial procedure can be much more productive when the patient is mentally prepared for the temporary trial phase. Identifying supportive family members who can assist the patient with the technology and offer support can enhance the chances for success. The manipulation of leads in the epidural space during the placement is regarded as a high-risk procedure for intraspinal bleeding. In this regard, anticoagulants are held for the recommended times, in this case, 3 days before the planned procedure. Anticoagulation therapy is held for the duration of the trial, and the plan for cessation of anticoagulants is communicated and agreed upon with the prescribing physician. After consent and intravenous access followed by anxiolysis, the patient is brought to our fluoroscopy suite. An allergy or a history of methicillin-resistant staphylococcus aureus often necessitates a switch to clindamycin or vancomycin. Pillows placed under the abdomen to reduce lumbar lordosis to open the interlaminar space and facilitate lead placement in the upper lumbar or low thoracic levels (T11-L3). For upper extremity, access is usually in the upper thoracic levels (T1-T4) with pillows under the chest and a prone pillow to support and keep the neck midline. Epidural access is gained approximately 1e2 levels below the targeted access vertebral level, which in this case was T11-12. The 14-gauge needle is directed in a shallow needle trajectory using a paramedian approach to the targeted epidural space for the low thoracic-high lumbar region. The upper thoracic levels have much smaller interlaminar spaces necessitating a steeper needle insertion angle, with only Percutaneous trial case for complex regional pain syndrome Chapter 2 17 one vertebral level below and in a paramedian fashion. Anteroposterior, contralateral, and lateral views are used to guide the access needles and cylindrical leads to target levels. The stimulation is then activated, and the paresthesia is set to optimize coverage by real-time patient feedback. It is important to keep the patient lightly sedated to ensure the adequate coverage of patient pain. The lead is then secured on the skin with a strain-relief loop covered by a Tegaderm but leaving the very end of the lead accessible to connect to the trial stimulation device. There is no procedural variation, and the radiation exposure is reduced as well as the most challenging part of the procedure which is lead placement is complete, thereby reducing the risks of repeating the procedure. In our own center, permanent trials are very uncommon because of the risk of false-positives and wound complications. But at times, even with this strategy, the stimulation can be positional, with inadequate coverage, or be associated with extraneous stimulation. This likely reflects the transitional nature of the spinal cord to cauda equina, with additional cerebrospinal fluid making selective stimulation of large fibers to the foot challenging. The mechanism is felt to relate to neurogenic inflammation with microglia and astrocyte activation (17). The disadvantage is the positional nature of stimulation, particularly with cylindrical leads. The only means to reduce positional stimulation with percutaneous leads programmed to deliver traditional paresthesia is far lateral epidural placement of the leads to stimulate the cervical nerve roots. This permits leads to lock in the "gutter" and stabilize the position onto the nerve roots. Additional current options are to convert to subthreshold or high-frequency modes of stimulation. Scenario (continued) the patient spent the next several days resting and engaging in only minimal activities. The needle access area in her back was somewhat uncomfortable, and initially, she had too much distraction from this pain to assess the trial benefit. Eventually, on day 4, she began to realize there was much less allodynia and that clothing and sheets could touch her foot again without eliciting severe pain. She returned to have a small amount of reprogramming from the representative to try to eliminate some stimulation from her upper leg, which was able to be accomplished. After 7 days, she returned to the clinic where the lead was gently pulled out and a small dressing applied to the opening.
Syndromes
- Chronic kidney disease
- They are fairly inexpensive (though more expensive than male condoms).
- DO NOT place cooked meat or fish back onto the same plate or container that held the raw meat, unless the container has been thoroughly washed
- Type 2 disease usually begins in infancy with severe neurologic involvement. This form can lead to rapid, early death.
- Myelodysplasia
- Cardiomyopathy - alcoholic
- Congenital torticollis
- ESR
Order procyclidine 5 mg otc
After 6 months with no recurrent symptoms symptoms pink eye discount procyclidine 5mg with amex, some patients elect to have their device removed. She says that she has pain in the low back and both legs including the feet, equal in intensity on both sides of the body. The patient is informed that during the procedure, she will be awakened for "intraoperative testing" to ensure that stimulation is covering all of her pain areas or a reasonably large amount of the areas. She will feel a tingling sensation (paresthesia), and she needs to identify where she feels it. The goal is for her to feel the tingling sensation in all of her pain areas if possible. Variation: Intraoperative testing is not performed the physician may choose not to do intraoperative testing and to place the leads over a specific vertebral region. In this case, the patient is informed that she may be asleep for the entire procedure or may not be asked for much feedback during the procedure. The patient is informed that after the procedure, she will be provided with a few initial programs to take home as well as details on what will happen during the trial week. In this case, the physician chooses to use two 16-electrode percutaneous leads with 1-mm electrode spacing and a 67-mm electrode span to allow for assessing appropriate levels for coverage of the back and most of the lower extremities during testing in the trial. Before intraoperative testing, impedances of the electrodes are checked, and they are all within the normal range. Variation: Two electrodes in the middle of the right lead (electrodes 8 and 9 counting from the distal end of the lead) have high impedance the physician wipes the proximal end of the lead that inserts into the cable that connects to the external trial stimulator to clear any material that may be causing the high impedance. Variation: Impedances are still high the physician moves the right lead in the rostral direction by two electrodes. The impedances move to electrodes 10 and 11, indicating an anatomical issue such as an air bubble. Variation: Impedances are still high the impedances stay high on electrodes 8 and 9, indicating a mechanical issue. The cable that connects the lead to the external trial stimulator is replaced, and the impedances are normal. Variation: Impedances are still high A different external trial stimulator is used, and the impedances are normal. Variation: Impedances are still high the lead itself is then replaced, and the impedances are found to be normal. During intraoperative testing, a pulse width of 200 ms and a frequency of 40 Hz are used initially. Because the physiological midline does not always coincide with the anatomical midline, stimulating with each lead separately is helpful for identifying the physiological midline and ensuring that stimulation provides bilateral coverage. Stimulation is delivered from the left lead in the middle of T9, and the patient is asked where she feels it. Stimulation is delivered from the right lead in the middle of T9, and she feels it in her right thigh, confirming that the physiological midline coincides with the anatomical midline and the patient has bilateral coverage. Programming concerns with spinal cord stimulation Chapter 10 77 Variation: Physiological midline is offset from anatomical midline the patient feels abdominal stimulation when the left lead is stimulated and left-sided stimulation when the right lead is stimulated, indicating that the physiological midline is toward the right of the anatomical midline. The physician is informed and attempts to reposition the leads by moving the left lead to the right of the right lead, thus trying to more closely bracket the midline. Amplitude is slowly increased until the intensity is strong but not uncomfortable for the patient. She is asked several times during this process where she feels the stimulation in her body and whether the amplitude is high enough or too high. Stimulation often can be moved to the midline by using equal amounts of current on each lead, which stimulates the space between the leads, and the patient reports feeling stimulation equally in both thighs. As the patient is assessed further, she is asked where she feels stimulation, trying to gain coverage all the way into her lower legs and feet, if possible, as well as the low back. Attempts to capture the low back usually require moving the stimulation in the rostral direction. The patient is asked if the stimulation is covering all of her low back pain, and she confirms that it does. At the rostral aspect of T10, she feels stimulation in both legs but not in the feet. The pulse width is increased to 250 ms to capture more dorsal column fibers, and she now reports feeling stimulation in the feet. Variation: Coverage of low back is only at the very top of the lead the patient has low back pain coverage when electrodes 1 and 2 are being used. Because lead migration is possible, especially during a trial when the leads are not usually anchored in place, it is more ideal if the physician moves the lead in the rostral direction by approximately two electrodes. However, it should be noted that focal pain can still be selectively covered using dorsal column stimulation as long as the appropriate fibers can be selectively targeted. Additionally, the spinal cord is likely in a different location when the patient is not lying prone, as she was during placement of the leads. When the caudal aspect of T8 is stimulated in this patient, she reports uncomfortable rib stimulation in addition to low back stimulation. The field shape (current distribution) is adjusted by moving the anodes closer to the cathodes, which decreases the "volume of activation," the three-dimensional space within which nerve fibers are being stimulated. Shaping the volume of activation in this manner avoids stimulating the dorsal root fibers that can cause rib stimulation at this vertebral level. When the rostral aspect of T10 is stimulated, the patient has good coverage of the legs and feet and no unwanted stimulation. Both locations are stimulated simultaneously, and all of her pain areas are covered without any extraneous stimulation. The frequency may be adjusted to affect the character of the stimulation sensation. In this case, when the frequency is increased from 40 Hz to 60 Hz to modulate the sensation of stimulation, she finds this sensation to be smoother and more comfortable. Frequency is increased further to 80 Hz, and the patient says she prefers the previous setting, so the frequency is set to 60 Hz. Variation: Intraoperative testing is not performed during the trial the same strategy described for intraoperative testing to cover all pain areas with stimulation may be followed. Pulse width is adjusted to capture varying dorsal column fibers in the volume of activation. The distance between cathodes and anodes is adjusted to modify the volume of activation: the greater the distance, the larger the volume of activation; although at times, the depth of stimulation may be decreased if the electrodes are far enough apart. Again, amplitude and frequency may be adjusted for character of the stimulation sensation and desired comfort. Due to the short duration of the trial, a thorough titration of stimulation parameters is typically not practical until after the permanent implant except in certain countries that require month-long trials. Therefore, the stimulation parameters used during the trial are generally fixed based on what has been effective in other patients, and titration occurs after the permanent implant. In addition, combination programs may provide greater pain relief by engaging multiple mechanisms of action. In this case, the patient is programmed with a combination program consisting of a paresthesia program and a subperception program. She is instructed to adjust the amplitude of the stimulation (only the paresthesia part of the program) to keep the sensation in a comfortable range as she may experience changes in intensity in different positions. The amplitude of the subperception part of the program may be locked so that it remains constant. She is also provided with additional programs including both paresthesia and subperception options in case they are needed. Functional improvements are often, but not always, correlated with pain scores and may also be important to evaluate. She is again informed that she will be contacted throughout the trial to ask how she is doing with the new programs and she may try different programs depending on how she feels. She reports experiencing 50% pain relief for her chronic pain, although she still has some postoperative pain. She likes the sensation of paresthesia, so she is instructed to continue using this program. She is doing very well, and she is asked to contact the clinical team if anything changes or if she has any questions or concerns.
Purchase procyclidine in india
For benign causes symptoms torn rotator cuff discount 5mg procyclidine otc, attempts can be made to slowly reduce the affected segments with or without resection. One of the most important historic case series, a 29-year retrospective review of 58 cases of surgically proven adult intussusception. A 20-year retrospective review of 24 cases of adult intussusception from a cohort of 292 patients with intussusception, with focus on the interventions performed. A 20-year retrospective review of 48 cases of adult intussusception summed with a previous review of 96 patients is one of the largest cohorts that gives insight on clinical characteristics, treatment, and prognosis of the disease. One of the most comprehensive literature reviews of intussusception, it compares and contrasts it with the pediatric counterpart and has a visual comparison from some of the previously reported case series. Clinical spectrum and surgical approach of adult intussusceptions: A multicentric study. A 25-year retrospective review of 41 cases of adult intussusception with focus on diagnostic tool performance and treatment. Clinical, laboratory, pathological, and follow-up variables were gleaned from medical records. Three had ileocolic disease, including cecal cancer (one), metastatic melanoma (one) and idiopathic (one); whereas five patients had colocolonic intussusception from colon cancer (three), tubulovillous adenoma (one), and local inflammation (one). No patient in the observation group required subsequent operative exploration for intussusception at mean 14. Conclusion Most cases can be treated expectantly despite the presence of gastrointestinal symptoms. The authors concluded that most cases of intussusception in adults can be treated expectantly despite gastrointestinal symptoms, as only a small percentage of patients were found to have a lesion that required excision. The length and diameter of the intussusception, the presence of a lead point, or associated bowel obstruction appeared predictive findings for mandatory exploration. Limitations: the relative rarity of this entity makes accumulation of a large patient experience extremely difficult. No inter- or intrarater variability was determined, so the diagnostic accuracy and consistency of the radiologists to determine intussusception was not established. Despite its limitations, this study permits us to make certain generalizations regarding this entity which is dealt with typically in small case series in the literature. Conclusions: this relatively large experience regarding a fairly unusual lesion informs the clinician on the relative benignity of intussusception in the majority of instances and gives us some clues as to what factors predict the need for exploration. Enterocutaneous fistulas can arise after abdominal trauma, inflammatory bowel disease, operations for oncologic and inflammatory processes in the abdomen, and operations for bowel obstructions. Patients will need aggressive fluid resuscitation along with correction of electrolyte disturbances. The skin must be protected from the draining enteric contents in order to prevent a destructive cellulitis of the abdominal wall. Vacuum-assisted wound closure devices can be used to help close wounds and control fistula output, but these devices can also cause more fistulas to develop and must be used with caution (4). The further use of irrigating vacuum-assisted devices have shown benefit in small case series (5). Antidiarrheals (loperamide, diphenoxylate/atropine, codeine, and tincture of opium) have also been used to decrease fistula output. Somatostatin and octreotide can decrease both biliary and pancreatic secretions, thus decreasing fistula output. In two separate meta-analyses of the use of somatostatin and octreotide, both decreased fistula output and increased the likelihood of enterocutaneous fistula closure, with no mortality benefit (6,7). The goal of providing nutritional support is to achieve an anabolic state with weight gain to allow for optimal healing. Enteral hypo- and isoosmolar feeds should be provided at slow rates to give the compromised bowel time to adapt and absorb the feeds. Be aware that fistula output usually increases proportionally to the amount of tube feeds provided. Defining the anatomy of the fistula and its organ of origin is necessary in planning the long-term care of the patient. Characteristics of the fistula as defined clinically and radiologically can predict if the fistula will spontaneously close or will need a definitive operation. A significant number of patients with enteric fistulas will require an operation to resect and close their fistulas. Definitive operative surgical repair is usually scheduled when the enteric fistula does not spontaneously close by 12 weeks after sepsis control. The patient must be maximized with optimal nutrition, be mentally prepared, have no evidence of ongoing sepsis, have clinical evidence of softening scars, and must be given enough time to allow their obliterative peritonitis adhesions to soften. The definitive operation should avoid any new enterotomies while performing lysis of adhesions, preserve maximal bowel length, completely resect the bowel communicating with the fistula, re-establish bowel continuity, and provide coverage of the bowel with well-vascularized soft tissue. Brenner and coauthors (10), showed that resection of the fistula with performance of a handsewn anastomosis had the lowest frequency of recurrent fistula. Patients who develop enterocutaneous fistulas will require an experienced, multidisciplined, thoughtful, and long-term care team. Often this disease process quickly turns into a chronic disease state requiring complex long-term care needs. Patients find themselves isolated, frustrated, angry, hungry, and depressed, and live in fear of recurrent sepsis and appliance leaks. Patients and their families are often psychologically spent and overwhelmed from the complexity and length of time necessary to heal and be strong enough for definitive surgical repair. The spectrum of clinical challenging problems that these patients and their caregivers encounter requires constant attention and flexibility in being able to adapt to the problems that arise in their care until definitive closure of their fistula. The authors present an authoritative discussion on the management of enterocutaneous fistulas. This is a good start to understanding the process and complexities of managing patients with enterocutaneous fistulas. A good review of the development of a process by which to manage patients with an enterocutaneous fistula. The multiple authors describe their helpful way to manage patients with enterocutaneous fistulas. Using intrawound negative pressure, irrigation, and application of artificial dermis. This article reviews techniques that have helped the authors manage and close difficult wounds and enterocutaneous fistulas. Somatostatin analogues for the treatment of enterocutaneous fistulas: A systemic review and meta-analysis. This is a systemic review and meta-analysis of the use of somatostatin analogs in the treatment of enterocutaneous fistulas. The authors concluded that somatostatin analogs appear to decrease the duration of enterocutaneous fistulas and duration of hospital stay, but no mortality benefit was identified. A meta-analysis of outcomes following the use of somatostatin and its analogues for the management of enterocutaneous fistulas. A meta-analysis of outcomes following the use of somatostatin and its analogs in the management of enterocutaneous fistulas. The authors concluded that somatostatin and octreotide increase the likelihood of fistula closure. Reduction of the closure time of postoperative enterocutaneous fistulas with fibrin sealant. This paper describes the use and success of fibrin sealant as a way to close some postoperative enterocutaneous fistulas. Comprehensive management of full-thickness luminal defects: the next frontier of gastrointestinal endoscopy. The authors report their experience with the endoscopic management and closure of fullthickness luminal defects that prevented or treated potential enterocutaneous fistulas. These authors at a single institution reviewed their experience with the definitive surgical closure of enterocutaneous fistulas. Mortality: No significant difference between somatostatin analogs and controls; P = 0. Results Conclusions Somatostatin and octreotide increase the likelihood of fistula closure.
Buy procyclidine 5 mg online
The primary intent was to determine if the group could prevent caloric deficiencies during critical illness treatment 5th metatarsal shaft fracture order procyclidine with amex. Of the roughly 4000 patients, 3600 were deemed ineligible; most exclusions (1344) were <18 years old, 548 were taking oral nutrition, 458 did not give consent, and 328 did not have a catheter placed centrally. Interestingly, the functional status (6-minute walk distance and activities of daily living) of patients from both arms were equivalent at discharge. This investigation contradicts what many have reported and practiced for years, that early and dense nutrition is beneficial and improves outcomes. This study and subsequent other well-designed, prospective trials have contradicted previous studies and conventional practice. The tendency to "overtreat" rather than "undertreat" should not be taken lightly, as the results of these contemporary studies demonstrate higher risks or no difference in outcomes with increased costs and potential complications. Similarly, thoughtful consideration must be exercised when deciding when to initiate nutritional therapy as well as the route and concentration (energy density). Differences in outcomes of the routine (non-critically ill) patient are challenging to determine, as they may be more immunocompetent. The recent contributions of prospective, randomized, controlled studies introduced in this chapter remain the standard and give the necessary direction required for decision making regarding both evidence-based and interpersonal-based medicine. Long-term total parenteral nutrition with growth, development and positive nitrogen balance. One in a large series of landmark papers demonstrating the ability to treat malnutrition via the bloodstream. Rhoads in the field of parenteral nutrition have saved countless lives and will forever be discussed and challenged in the surgical literature. It further explains the potential pathology and complications associated with and without these formulations. Early versus traditional postoperative oral feeding in patients undergoing elective colorectal surgery: A meta-analysis of randomized clinical trials. Interesting study examining early versus late oral feeding in colorectal patients. Primary outcomes included length of stay, anastomotic dehiscence, and infectious complications. Early postoperative feeding decreased length of stay and total postoperative complications. There was no difference in anastomotic leak, mortality, pneumonia, and wound infections. Does enteral nutrition compared to parenteral nutrition result in better outcomes in critically ill adult patients Early enteral nutrition within 24 hours of lower gastrointestinal surgery versus later commencement for length of hospital stay and postoperative complications. One of the recent advances in enteral nutrition is the external magnetic guidance of a feeding tube. It can be placed at bedside with low cost and has been shown to be safe and effective. This adds to the literature safety profiles for decreased risk of aspiration compared to those placed in the stomach or "post-pyloric" (a more unfortunate and confusing term). Poor validity of residual volumes as a marker for risk of aspiration in critically ill patients. Frequently quoted study examining gastric residual volumes and their lack of utility and poor sensitivity in predicting aspiration when used routinely. It is a small (40 patients), randomized study with multiple samples (>1100 samples) comparing aspirates, residual volume, and patient management based on the residual volume of 200 mL versus 400 mL. The importance of the physical exam, tube placement, and location remain important in preventing aspiration risk. Gastric residual volume is not recommended for routine management of tube-fed patients. Percutaneous gastric tubes may be more beneficial than nasoenteric tubes in decreasing the risk of aspiration. Methods of enteral nutrition administration in critically ill patients: Continuous, cyclic, intermittent, and bolus feeding. The existing studies remain low-level studies without a definitively superior method. Bolus feeds, however, appear to have advantages in muscle protein synthesis, gastrointestinal hormone secretion, and efficiency when the feeding tube is in the stomach. This publication discusses best practices for delivery, formula, cannula, and infusion techniques. Results demonstrated no differences in mortality at 60 days, infectious complications, or ventilator-free days. Patients fed with trophic level supplementation did significantly better, with less vomiting, gastric residual volumes, constipation, and fluid balance at 7 days. This was initiated within 12 hours of delivering nutritional support in ventilated patients. This is an important contribution to the literature due to its design and message that more calories are not equivalent to improved outcomes. It elegantly highlights the concerns and points out the timeless concerns which are being addressed and practiced today. Adding various anticoagulants has not improved thrombosis rates and is not recommended. Ultrasound guidance for placement of centrally placed lines has decreased some complications and is currently the standard of care. These European guidelines do not differ significantly from the American guidelines. With the exception of ultrasound guidance, the evidence in most of the literature thus far remains low (Grade B/C). Well designed multicenter, randomized, controlled trial of >1400 critically ill children. A protocol for the early initiation of enteral nutrition was applied to both groups, and insulin was infused to achieve normoglycemia. Conclusions Late initiation of parenteral nutrition was associated with faster recovery and fewer complications, as compared with early initiation. Coopersmith 42 Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection (Singer et al. Research during the last 15 years has led to a tremendous increase in the understanding of sepsis on multiple scales, ranging from molecular to whole organ (Hotchkiss et al. Despite this, over 150 negative clinical trials have been performed in sepsis, demonstrating profound difficulty in translating preclinical studies to the bedside. In the absence of our ability to manipulate the host response for therapeutic gain, the mainstays of sepsis therapy include antimicrobial therapy, fluid resuscitation, and supportive care. Despite this simple-sounding approach, care of the septic patient is complex, and the most recent Surviving Sepsis campaign guidelines for the management of sepsis include 93 statements on the early management and resuscitation of sepsis and septic shock (Rhodes et al. These include 32 strong recommendations, 39 weak recommendations, and 18 best practice statements. While guidelines are vitally important for the management of septic patients, their length and depth represent a double-edged sword. At the same time, the sheer volume of recommendations and evidence can be overwhelming for many bedside practitioners. In contrast to guidelines, bundles represent a small number of easily followed actions that can be used by practitioners worldwide. The Surviving Sepsis campaign initially instituted the concept of sepsis bundles in 2004, containing a 6-hour resuscitation bundle with six elements and a 24-hour management bundle with four elements. Compliance with the bundles was associated with decreased mortality in multiple studies. The largest of these examined 29,740 patients in 218 hospitals over 7 years and demonstrated that for every quarter that a site participated in the Surviving Sepsis campaign, mortality went down by 0. Notably, mortality varied greatly with bundle compliance, with a nearly 10% absolute difference in mortality between sites with low versus high compliance for the resuscitation bundle (38.
Purchase procyclidine 5mg with mastercard
The mediation findings cited earlier suggest that neuroscience may indeed be a fruitful approach to understanding these facts symptoms 7 days after ovulation purchase generic procyclidine on-line. However, the causal web linking environment, biology, and life outcome is massively complex. External social and economic impediments work alongside these brain-mediated pathways to constrain life chances. The policy implications of our current, rudimentary understanding of these effects is limited, but as the science progresses, so will its potential for translation. At present, neuroscience adds to the weight of evidence for policies already supported by behavioral research, such as the importance of prenatal health, family stress reduction, and conversation with children. Neuroscience has also been used as part of a communication strategy to convey information to policy-makers and the public about the needs of children (Shonkoff & Bales, 2011). In the near future, neuroscience may contribute in more distinctive and consequential ways to guide policy (Farah, 2018). For example, it offers potential biomarkers to screen for the risk of emotional or cognitive difficulties and to facilitate intervention research by providing early predictors of success (Pavlakis et al. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, white women. Closing the achievement gap through modification of neurocognitive and neuroendocrine function: Results from a cluster randomized controlled trial of an innovative approach to the education of children in kindergarten. Protective prevention effects on the association of poverty with brain development. Social class and the motivational relevance of other human beings: Evidence from visual attention. Childhood poverty is associated with altered hippocampal function and visuospatial memory in adulthood. Early educational intervention for poor children modifies brain structure in adulthood. Functional brain organization of working memory in adolescents varies in relation to family income and academic achievement. Nongenomic transmission across generations of maternal behavior and stress responses in the rat. Community socioeconomic disadvantage in midlife relates to cortical morphology via neuroendocrine and cardiometabolic pathways. Inflammatory pathways link socioeconomic inequalities to white matter architecture. Socioeconomic status and the brain: Mechanistic insights from human and animal research. Socioeconomic status is positively correlated with frontal white matter integrity in aging. Socioeconomic disadvantage, neural responses to infant emotions, and emotional availability among first- time new mothers. How socioeconomic disadvantages get under the skin and into the brain to influence health development across the lifespan. A metaanalysis of the relationship between socioeconomic status and executive function per for mance among children. Strengths and weaknesses of neuroscientific investigations of childhood poverty: Future directions. The effects of poverty on childhood brain development: the mediating effect of caregiving and stressful life events. Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Socioecomomic status, amygdala volume and internalizing symptoms in children and adolescents. Socioeconomic inequality and the developing brain: Spotlight on language and executive function. Neural mechanisms linking social status and inflammatory responses to social stress. Family-based training program improves brain function, cognition, and behav ior in lower socioeconomic status preschoolers. Family income, parental education and brain structure in children and adolescents. Brain-behavior relationships in reading acquisition are modulated by socioeconomic factors. Early-life adversity and physical and emotional health across the lifespan: A neuroimmune network hypothesis. Proficiency differences in syntactic processing of monolingual native speakers indexed by event-related potentials. Brain imaging and electrophysiology biomarkers: Is there a role in poverty and education outcome research Socioeconomic status and reading disability: Neuroanatomy and plasticity in response to intervention. Science does not speak for itself: Translating child development research for the public and its policymakers. The impact of socioeconomic status on the neural substrates associated with plea sure. Socioeconomic status and academic achievement: A meta- analytic review of research. An epigenetic mechanism links socioeconomic status to changes in depression-related brain function in high-risk adolescents. Neurocognitive development in socioeconomic context: Multiple mechanisms and implications for mea sur ing socioeconomic status. A mechanistic understanding of addiction is thus crucial for addressing these public health issues. To date, addiction research has made tremendous progress in terms of uncovering the neurobiological and neuropsychological correlates of addiction. However, little is known about the computational principles implemented by the brain. This explanatory gap hinders the understanding of the mechanisms of addiction as well as the development of effective therapeutics. In this article we will review recent efforts in the nascent field of computational psychiatry that have started to address this problem. Second, we will review studies utilizing theory- driven computational approaches, including reinforcement-learning models, Bayesian models, and biophysical models, that address addiction. Last, we will outline a road map for computational work on addiction to move forward. The explanatory gap Addiction remains one of the most serious threats to public health. Much effort has been devoted to the study of the neurobiology of addiction at cellular and molecular levels. Despite the progress made in addiction neuroscience, a major explanatory gap still exists between animal models of addiction and human addiction in real life, which prevents the translation of bench work to patient care. One example of this explanatory gap is the finding that the neuropharmacological effects of drugs on the brain can be overridden by cognitive factors such as beliefs and expectancies in humans (Gu et al. Thus, a purely neurochemical approach alone is not sufficient to account for the complexity of addiction in humans. In this article, we will review recent endeavors in the nascent field of computational psychiatry that have started to address this disconnection. Computational psychiatry seeks to understand the algorithms underlying mental function and dysfunction using computational approaches and has been used to illustrate the mechanisms of addiction in recent years (see Redish, 2004 for an example). Second, we will review studies utilizing theory- driven approaches of computational psychiatry, including reinforcementlearning models, Bayesian models, and biophysical models, that address addiction. Last, we will outline a roadmap for moving forward with computational work on addiction. In particular, Marr proposed that one must understand any information-processing system. The computational level addresses the question of "what"-what problems does the system solve
Buy procyclidine 5mg otc
Pericytes medicine ubrania purchase discount procyclidine online, the mural cells surrounding endothelial cells of small blood vessels, are required for maintaining vessel stability [14]. In addition, pericytes regulate blood flow due to their contractibility properties and contribute to tissue regeneration given their mesenchymal stem cell properties [14,15]. Not surprisingly, the brain has one of the highest pericyte coverage of the vascular network [14,15]. In addition, the interaction between Jagged-1, from endothelial cells, and Notch3, from pericytes, is responsible for vessel stabilization [17]. Eph/ ephrin-B2 signaling is also involved in this cell-to-cell interaction [18,19]. Other non-cancer cells that are known to reside at the perivascular space are stem cells. For instance, 95% of Hoxb5 1, a recently discovered nuclear marker for hematopoietic stem cells, were detected attached to the endothelial cells in the bone marrow [23]. The perivascular location provides stem cells preferential access to molecules from the blood such as nutrients, growth factors, and hormones; as well as angiocrine factors that regulate their differentiation, self-renewal proliferation, and/or migration capacities [24,25]. Recent analyses on cell heterogeneity in brain macrophages and astrocytes have described cellular subtypes that have been mainly defined by their perivascular location [32,33]. In primary tumors, cancer cells in close contact with vessels receive and have access to oxygen, nutrients, and other factors produced by endothelial cells (angiocrine factors) that support their viability and growth [56,57]. As the primary tumor develops, the ability of cancer cells to co-opt the vessels initiates the process by which few of them will get access to systemic circulation upon intravasation, thus starting the metastatic cascade [37]. The interaction between cancer cells and vessels is resumed once metastatic cells reach the capillary network of distal organs after they disseminate from the primary tumor through systemic circulation. Interestingly, those tumor cells that extravasate do not abandon the perivascular niche but remain closely attached to the abluminal side of the vessels performing vascular co-option [50,53]. The initial observation of this process in lung metastasis [1] has been extended to multiorgan metastases, establishing vascular co-option as a hallmark of metastasis-initiating cells [2,38,41,46,50,52,53]. Besides the benefits described in the primary tumor [56,57], there are additional implications of vascular co-option involving several cancer hallmarks [62] such as aggressive growth, immune evasion, latency, and resistance to therapy [8,9,35,37,44,49,55,63,64] that are especially relevant in metastasis. Molecular regulation of vascular co-option Given that vascular co-option has been linked to several cancer hallmarks, its molecular characterization is key to develop novel anticancer strategies, which might have relevant implications to prevent the development of metastasis. This process has been described in multiple organs targeted by metastasis and shown to be independent of the primary tumor type. Vascular co-option Molecular regulation of cell adhesion and proliferation in vascular co-option Immediately after crossing the vascular barrier of any given secondary organ, metastasis-initiating cells remain attached to the abluminal side of the vessels using preexisting capillaries [2,46,50,53]. In addition to favor growth, this molecular mechanism is also important for protecting not aggressive dormant cancer cells, which might drive relapses later on [55]. This scenario is very relevant in breast cancer, which could develop a significant period of time between the removal of the primary tumor until metastases manifest clinically. Thus vascular co-option benefit cancer cells in a 1-integrin-dependent manner by granting access to the components of the basal lamina of co-opted vessels. In addition, cancer cells might also benefit by the influence of 1-integrin on the production of angiocrine factors in endothelial cells. This process has been shown to be dependent on 1-integrin, given its ability to couple growth with blood flow leading to the activation of mechanotransduction processes that induces the secretion of these factors [56]. Additional integrins have been described to participate in vascular co-option, which suggests certain plasticity within the communication between cancer cells and the endothelium. Besides integrins, additional cell adhesion molecules are involved in vascular co-option. This cell adhesion molecule was initially found to be enriched at the interface between tumor and endothelial cell in brain metastasis [50] and later involved multiorgan metastases from different primary tumors [2]. Although the process of vascular co-option involves the cancer cell and the endothelial cell, it could be influenced by additional cells of the microenvironment induced by inflammation. Vascular co-option Molecular regulation of migration and invasion linked to vascular co-option the process of migration is highly relevant in cancer. Dissemination of cancer cells out of the primary tumor is a necessary step for the development of systemic cancer but also local dissemination can have important clinical implications. For instance, intracerebral invasion of glioma cells is a marker of poor prognosis [71]. Vascular co-option is highly relevant in the ability of cancer cells to migrate in the brain. Glioma cells exploit ephrin signaling to move along pre-existing capillaries [35]. Normally, Eph/ephrin signaling constrains the migration of incipient premalignant lesions [72]; however, as the tumor evolves and increases its aggressiveness this initial antitumor mechanism gets rewired. The acquisition of migratory properties in glioma cells could also be linked to the cell of origin [36]. Glioma cells with an Olig2 1 oligodendrocyte precursor origin, which are cells performing vascular co-option during their normal development [12], are more prone to invade using the preexisting vessels [36]. In contrast, the infiltration of immune cells will be higher in angiogenic Olig2 2 tumors than Olig2 1 gliomas. This will define the type of immunophenotype that these tumor types will develop [36], which might have important implications in emerging strategies using the immune system to target cancer cells. Molecular regulation of dormancy, latency, and awakening linked to vascular co-option As slow-proliferative normal stem cells located at the perivascular niche do, cancer cells could develop a state of quiescence associated with vessels. This state could be induced by molecules produced by endothelial cells or derived from the intrinsic properties of cancer cells. Although several programs have been described, it is not known whether they are interconnected. Consequently, the switch from dormant/latent state to a productive proliferative state requires additional regulatory mechanisms. Additional mechanisms developed by cancer cells to escape from the proliferative-checkpoint imposed at the perivascular niche have been described. Both spontaneous and induced metastases from lung cancer, breast cancer, renal cancer Tumor Vascularization 42 3. Vascular co-option and melanoma potentially affecting the bone, lungs, brain, and liver were dramatically reduced after targeting any of these cell adhesion molecules [2,39,50,52]. A similar combination therapy based on capecitabine, an antiangiogenic drug (B20-4. Additional successful therapeutic strategies targeted Ephrin-B2 using blocking antibodies in experimental glioblastoma models [35]. Besides blocking vascular co-option to target metastasis, impairing the support provided by the perivascular niche has been shown to reduce the increased resistance to chemotherapies. For instance, bone metastasis were sensitized to doxorubicin and taxol by using blocking antibodies against 1 and V3 [55]. Consequently, using therapeutic strategies targeting vascular co-option might be useful to reduce resistant cells at the perivascular niche that will drive relapse later on. Similarly, cells that might escape surgery because they have migrated out of the tumor core is a frequent cause of relapse in gliomas. Although several examples of normal cells developing vascular co-option are specific to development. Consequently, besides genetic strategies that have been a valuable proof-of-concept to demonstrate the enormous potential of targeting vascular co-option as a novel anti-metastasis strategy, more pharmacological strategies are needed specially directed against aspects of vascular co-option specific for cancer cells. Expression profiling of angiogenesis-related genes in brain metastases of lung cancer and melanoma. Expression of vascular endothelial growth factor is necessary but not sufficient for production and growth of brain metastasis. Vessel co-option is common in human lung metastases and mediates resistance to antiangiogenic therapy in preclinical lung metastasis models. Competing waves of oligodendrocytes in the forebrain and postnatal elimination of an embryonic lineage. Oligodendrocyte precursors migrate along vasculature in the developing nervous system. Pericytes: developmental, physiological, and pathological perspectives, problems, and promises. EphrinB reverse signaling contributes to endothelial and mural cell assembly into vascular structures. N-cadherin mediates pericytic-endothelial interaction during brain angiogenesis in the chicken. Hoxb5 marks long-term haematopoietic stem cells and reveals a homogenous perivascular niche.
