

Buy atacand online
This test of range of hip extension is performed by flexing both hips antiviral mouthwash safe atacand 4 mg, then holding one in flexion while the patient is asked to extend the other leg. Next, the knee and thigh are held with the hip and knee flexed to 90 degrees, and internal and external rotation are tested and recorded in degrees. The limit is determined by the point at which the pelvis begins to move (normally 45 degrees of abduction and 30 degrees of adduction). Extension is tested with the patient prone by having him or her lift the leg up from the table (normal, 20 to 30 degrees). Internal and external rotation are also tested with the patient prone and the hip and leg in extension. When hip abductor weakness is suspected on the basis of the finding of a gait abnormality, the Trendelenburg test. If instead it drops, abductor weakness is present on the opposite side, and the Trendelenburg test is positive. Knee Importantly, knee pain is a common reason for seeking orthopedic care, and it is often referred from the hip; thus any patient presenting with knee pain should always be examined for possible limitation of hip motion or pain on motion of the hip. The knee examination begins with the examiner viewing the joint from the front, side, and back, looking for differences in contour, swelling or masses, and changes in overlying skin. From the front, the knee is inspected for valgus (lower leg points away from the midline) or varus (lower leg deviates toward the midline) deformity and for evidence of effusion, manifested by obliteration of the normal depressions around the patella or by generalized swelling. In viewing the knee from its lateral aspect, the examiner looks for incomplete extension resulting from flexion contracture or excess hyperextension (recurvatum deformity), as well as for symmetry of the tibial tuberosities. From the rear, the popliteal fossae are checked for symmetry and evidence of swelling. The knees are palpated to assess warmth and check for tenderness along the medial and lateral joint lines, the medial and collateral ligaments, the patella and its supporting ligaments, the femoral and tibial condyles, and the tibial tubercles. Palpation is easier with the knee flexed because the skeletal landmarks are more readily seen and felt, and the muscles, tendons, and ligaments are relaxed in this position. When there is evidence of a marked effusion, landmarks are obscured and the patella is readily ballotable. This is seen with intraarticular hemorrhage, arthritis, and synovitis, and range of motion is usually significantly limited. If landmarks are only mildly obscured (suggestive of a mild joint effusion or fluid collection in the bursae), pressure should be applied over the suprapatellar pouch with the thumb and index finger of one hand, milking down any fluid present while simultaneously pushing the patella up toward the femoral condyles with the other hand. If fluid is present, the patella is ballotable, and a palpable click is noted as the patella strikes the front of the femur. The knee is primarily a hinge joint and is normally capable of 130 to 140 degrees of flexion and 5 degrees of hyperextension. However, it can also rotate approximately 10 degrees internally and externally, and this involves rotation of the tibia on the femur. To test extension, the examiner can have the patient either sit and try to straighten the leg to 0 degrees of flexion or try to lift the straightened leg from the examination table while lying supine. Rotation is assessed by turning the foot medially and then laterally with the knee flexed. With the knees flexed to 80 to 90 degrees, the patellas should face forward when viewed from the front and be located squarely at the ends of the femurs when seen from the side. With the patient sitting, the examiner supports the lower leg and holds the knee flexed to 30 degrees. If left hip abductor weakness were present, the right pelvis would tilt downward when the right leg was lifted. Moderate pressure is applied over the suprapatellar pouch with the thumb and index finger of one hand, milking any fluid present downward. When an effusion is present, the patella becomes ballotable, and a palpable click is felt as the patella strikes the front of the distal femur. With the patient supine, the hips flexed to 45 degrees, and the knees flexed to 90 degrees, the examiner grasps the proximal tibia with his or her fingers behind the knee and thumbs on the anterior joint line and makes a gentle pull/push motion. Similar posterior motion on pushing indicates posterior cruciate instability, representing a positive posterior drawer test. Ligamentous stability of the knee should be assessed in the mediolateral and anteroposterior planes. In patients with acute injuries, especially those involving significant pain and swelling, this should be deferred until radiographs have been obtained to check for associated fractures. The abduction/adduction stress test is used to determine the degree of stability of the medial and lateral collateral ligaments. To test the medial collaterals, the examiner applies valgus stress by pressing medially against the distal thigh with the upper hand while gently abducting the lower leg. To check the lateral collaterals, the examiner applies varus stress by pressing laterally on the inside of the distal thigh while gently adducting the lower leg. Anteroposterior ligamentous stability is provided by the anterior and posterior cruciate ligaments of the knee. The examiner then grasps the proximal tibia with his or her fingers behind the knee and the thumbs over the anterior joint line and gently pulls and pushes. The examiner grasps the distal femur with one hand and the proximal tibia with the other. The thumb of the lower hand is placed on the joint line, and the femur is pushed backward as the tibia is pulled forward. Abnormal anterior displacement of the tibia on the femur can be seen and felt if instability is present. The amount of excursion is estimated in millimeters, and the end point is recorded as soft or firm. Ankle Examination of the ankle begins with inspection for evidence of deformity, swelling, change in color of overlying skin, and abnormal position (especially with weight bearing). In the neutral position, the long axis of the foot should be at 90 degrees to the long axis of the tibia. Normally a child can dorsiflex 20 degrees and plantar flex 30 to 50 degrees from the neutral position, as well as invert and evert approximately 5 degrees. With the patient sitting and the knee supported in 30 degrees of flexion, the patella is gently pushed laterally. Any abnormal amount of lateral displacement, pain, or apprehension constitutes a positive test. With the knee flexed to 15 degrees, the distal femur is grasped with one hand and the proximal tibia with the other, with the thumb on the joint line. Any abnormal displacement of the tibia on the femur indicates anterior cruciate instability and represents a positive test. Similarly, inversion is tested by having him or her walk on the outside of the feet and eversion by having him or her walk on the medial sides. The anterior drawer test is used to assess the stability of the anterior talofibular ligament. Normally there should be no movement, but with instability of the anterior talofibular ligament, the talus slides anteriorly. Lateral instability is seen only with major tears of the anterior talofibular and calcaneofibular ligaments, occasionally accompanied by tears of the posterior talofibular ligament, and is tested by inverting the calcaneus with one hand while grasping the distal tibia with the other. Medial instability is exceptionally rare because of the strength of the fan-shaped deltoid ligament. To test for medial instability, the tibia and calcaneus are held in the same manner as they are in testing lateral instability, but the foot is everted instead. Gait Disturbances Stemming From Pain, Limb Length Inequality, or Stiffness An antalgic gait is a limp caused by pain on weight bearing that results in shortening of the stance phase on the affected side. It can be due to pain referred from the back or pain anywhere in the lower extremity. Causes include trauma, pathologic fracture, infection, inflammatory disorders and other sources of arthritis, malignancy, tight shoes, foreign body in the shoe, and a lesion on the sole of the foot. Careful physical examination combined with a complete history usually enables localization of the problem.
Order atacand paypal
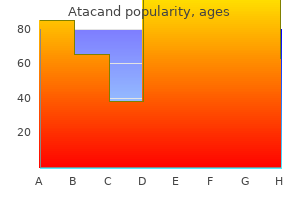
Similarly anti viral throat spray order 8mg atacand free shipping, penetration of vascular channels through the vertebral end plates into the intervertebral disks makes diskitis more likely than vertebral osteomyelitis in early childhood (see Chapter 13). A thorough understanding of musculoskeletal development and of the radiographic findings at differing stages is particularly important in the diagnosis and management of orthopedic injuries. At birth only a few epiphyses have begun to ossify; the remainder is cartilaginous and thus is invisible radiographically. The epiphyseal plates (physes), which are sites of cartilaginous proliferation and growth, do not begin to ossify and thereby close until puberty. When skeletal injuries involve sites where ossification has not begun or is incomplete, radiographic findings may appear normal or may not reflect the full extent of the injury. Before closure of the physis during puberty, the growth plate is actually weaker than nearby ligaments. As a result, injuries that occur near joints are more likely to result in physeal disruption than in ligamentous tearing. Similarly, avulsion fractures at sites where strong muscular attachments join secondary ossification centers are unique to children and adolescents. When there is displacement of an epiphyseal fracture and the fragments are not anatomically reduced, growth disturbances may occur. Because the epiphysis may not be ossified, radiographs often fail to reveal the injury. For this reason, children with injuries at or near joints must be examined with meticulous care so that epiphyseal fractures are not missed. Clinically, pain and swelling may be detected over the epiphyseal plate region and, less notably, over the joint itself. The periosteum of a child is much thicker than that of an adult, strips more easily from the bone, and is rarely disrupted completely when the underlying bone is fractured. Because of the immature elements in the rapidly growing skeleton of the child, the bone has more viscoelasticity and can sustain plastic deformation more easily than the adult skeleton. Consequently, a given compressive force that would produce a comminuted fracture in an adult tends to be dissipated in a child in part by the bending that occurs in the more flexible bone of the child. Such a force is thus more likely to result in plastic deformation or to produce an incomplete fracture, such as a torus fracture or a greenstick fracture, in a child. Their fractures can be considerably more difficult to detect clinically and radiographically, and because the growing cells in the epiphyseal plate may be injured, growth disturbances may occur. Children do have advantages, however, in that their actively growing 759 Children with musculoskeletal injuries and afflictions are brought for care because of pain, deformity, or loss of function. Often the clinical challenge lies not so much in recognizing the impaired or injured part, which in most cases is readily accessible to inspection and examination, but in making an accurate diagnosis in order to plan and initiate appropriate treatment. Because of their rapid physical growth and the special properties of their developing bones, children often pose special problems for the clinician. Linear growth occurs as the result of multiplication of chondrocytes in the epiphyses, which align themselves vertically, forming a transitional zone of endochondral ossification in the metaphyses. The shafts of long bones widen, and flat bones enlarge through the deposition and mineralization of osteoid by the periosteum. Hence, genetic and congenital disorders that affect connective tissue (and thus the skeleton) tend to cause abnormal growth. However, in some conditions such as Marfan syndrome, excessive linear growth occurs, resulting in an abnormally tall stature and unusually long fingers and toes. The terminal arterial loops and sinusoidal veins that form the vascular bed of growing metaphyses have sluggish blood flow, which increases the risk of thrombosis and of the deposition of bacteria during periods of bacteremia. As a result, there is a greater risk of developing hematogenous osteomyelitis in pediatric patients than in adults. This forms the basis for the use of bone age as part of the evaluation of children with growth disorders. When evaluating the radiographs of injured children, it is of crucial importance to bear in mind that fractures involving nonossified epiphyses are radiographically invisible until healing begins. Finally, numerous genetic, metabolic, endocrine, renal, and inflammatory processes can affect not only growth and ultimate height but also skeletal maturation-in some cases delaying it and in others accelerating it. From left, the hands shown are those of a toddler, a young school-age child, and a young adolescent. Injuries affecting unossified bones or growth centers are invisible radiographically. Regional Musculoskeletal Examination In the regional examination, the area of concern is inspected visually for spontaneous movement, guarding, size, swelling, deformity, and the appearance of overlying skin, and the findings are compared with those for its paired structure. After this, the normal side and then the affected side are gently palpated for warmth, induration, and tenderness. Muscle mass, tone, and reflexes on the affected side are compared with those on the normal side, and the presence or absence of spasm is noted. If asymmetry in muscle mass is detected, the circumference is measured bilaterally at a point equidistant from a fixed bony landmark. The child is then asked to move the extremity or is handed objects to get him or her to do so, and active motion is observed. If this appears limited, passive range of motion is tested first on the normal and then on the affected side, taking care not to cause severe pain. Joints are further inspected to determine whether there is erythema, obliteration of landmarks that may indicate the presence of effusion, evidence of deformity, and position of comfort. Further evaluation to detect joint effusion is done by pressing on one side of a visible joint while feeling for the protrusion of fluid on the other. The joints are palpated to check for evidence of heat and tenderness, range of motion is assessed, and evidence of pain on motion is determined. Assessment of ligamentous stability around joints is discussed under specific sections of the regional examination. However, it is important to remember that in cases of acute trauma, especially when deformity or hemarthrosis is evident on initial assessment, tests of ligamentous stability should be deferred, the extremity splinted, and radiographs obtained to check for possible underlying fracture. Physical Examination the orthopedic examination involves a systematic assessment of posture, stance, and gait; the symmetry or asymmetry of paired musculoskeletal structures and their motion; muscle strength and tone; and neurovascular status. Patience and often some degree of creativity are required on the part of the examiner if the patient is very young. This can be assisted by providing age-appropriate toys for him or her to play with while the history is being taken and by engaging the patient in play (if circumstances permit) before starting the more formal physical examination. After spontaneous activity is observed, the relevant parts of the orthopedic examination are typically done by region. A complete orthopedic examination that assesses each bone, muscle, joint, tendon, and ligament is lengthy, detailed, and rarely indicated. Even in multiple-trauma victims and patients whose symptoms point toward an underlying systemic disorder, each region is screened and a full assessment done only of those regions where local musculoskeletal abnormalities are found. Similarly, in patients with focal injuries or deformities, the examination can generally be focused on the region involved, with the clinician bearing in mind referral patterns for pain and the maxim that all extremities "begin at the back. The patient is then turned and viewed from behind, and the shoulder and scapular height, the muscle bulk of the trapezius muscles, and the height of the posterior iliac crests and of the depressions over the sacroiliac joints are checked for symmetry. Trapezius strength is determined by having the patient shrug his or her shoulders, first against gravity and then against resistance, as the examiner presses down on the shoulders. The muscles supplying the scapula are tested by having the patient press his or her outstretched arms against a wall. Winging of the scapula during this maneuver is suggestive of weakness of the serratus anterior muscle. The line of the spinous processes of the vertebrae is observed for straightness, and the position of the head over the trunk is noted. In the immobilized trauma patient, these observations are made largely with the patient supine on a backboard and then log-rolled onto his or her side. Importantly, in checking for neck injury, the cervical spine can be cleared clinically if the patient is awake and alert and has no complaint of neck pain, no evidence of tenderness or paraspinous muscle spasm, and no extremely painful injury elsewhere. A normal child can touch his or her chin to the chest, extend the neck to look directly above, and bend laterally to 45 degrees. He or she is also capable of symmetrical lateral rotation when turning the head from side to side. Strength is tested by applying pressure to the forehead while the patient flexes his or her neck and to the occiput as the patient extends, and by applying resistance to the opposite side of the head as the patient bends and rotates laterally. Thoracolumbar Spine Viewed from the side, the normal child has a lordotic curve in the cervical area with a bony prominence at C7, a mild thoracic kyphosis, a lumbar lordosis, and a sacral kyphosis.

Atacand 16 mg
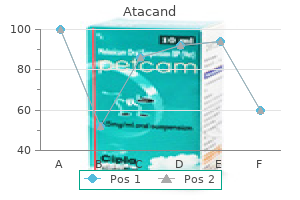
Pain on percussion over the vertebral column may be an early sign of cord compression and should be actively sought in the child with suspected cancer in this region hiv infection rate china order 16 mg atacand free shipping. Spinal tumors often have associated weakness, with the affected muscle group corresponding to the level of the lesion. Spinal cord tumors or tumors that press on the cord may present with bowel/bladder dysfunction, paresthesias, or changes in gait. Clinical presentation varies depending on whether a tumor is supratentorial or infratentorial in location. Last, developmental delay is a symptom of many brain tumors in the pediatric population. Proptosis may be observed with several childhood tumors and may represent either a primary tumor or metastatic disease. The resulting condition has been referred to as "raccoon eyes" and is due to ecchymoses in the periorbital area. Morphologic abnormalities of the ear itself (ear creases or pits) may signal the Beckwith-Wiedemann syndrome, in which patients have a known predisposition to hepatoblastoma, Wilms tumor, and other malignancies. A child with cancer may also present with a lesion of the orofacial region, including the jaw and oral and nasal cavities. Inappropriate loosening of the teeth may represent a clinical manifestation of Burkitt lymphoma. This child demonstrates proptosis due to the retro-orbital tumor, as well as a large head due to the presence of increased intracranial pressure. This clinical finding is characteristic of a retro-orbital metastatic tumor in advanced neuroblastoma. Gingival hyperplasia can be seen in children with leukemia, especially the acute myelomonocytic subtype. Although most physicians look for cervical adenopathy, it is important to remember the other lymph node groups that may be involved by focal or generalized adenopathy in leukemias, lymphomas, or solid tumors. Additional lymph node locations that should be sought during physical examination include supraclavicular, infraclavicular, epitrochlear, inguinal, femoral, and popliteal. Although large, rock-hard nodes that are fixed to the subcutaneous tissue are most convincing for malignancy, texture and size can be misleading. Because Hodgkin disease and non-Hodgkin lymphoma can occur concurrently with or after infectious mononucleosis, a positive monospot test may be a false reassurance. Therefore persistent adenopathy, even in that setting, should be monitored closely. The algorithms for workup of adenopathy and indications for biopsy are reviewed in Chapter 13. Although rare in childhood, a goiter or nodular thyroid with or without bruits may be seen in a patient with thyroid carcinoma. Chest External examination of the chest may disclose obvious skeletal or other chest wall masses that may be asymptomatic or associated with pain. Scoliosis has been associated with paravertebral tumors such as thoracic neuroblastoma (see Chapter 22). The pediatric malignancies of this type include rhabdomyosarcoma, Ewing sarcoma, and osteosarcoma. However, subsequent discussion in this section provides a more focused review of tumors of the mediastinum. The differential diagnosis of a mediastinal mass depends to a certain extent on location. Tumors of the anterior mediastinum in children and young adults are most commonly lymphomas, including both Hodgkin disease and non-Hodgkin lymphoma. Masses of the middle mediastinum and/or hilar adenopathy also most commonly represent lymphoma in childhood. Tumors of the posterior mediastinum are usually of neurogenic origin, including neuroblastoma and Ewing sarcoma. Parenchymal pulmonary nodules, when tumor related, may be asymptomatic and most commonly represent metastatic solid tumor, such as a sarcoma. Cytology, flow cytometry, and cytogenetics performed on pleural fluid may provide diagnostic material with relatively low risk in the patient with compromised respiratory status due to mediastinal disease when surgical approaches are too dangerous. Symptoms of respiratory distress may result from a primary intrathoracic process or may be due to a compromised respiratory effort from an abdominal process, such as an abdominal mass or ascites. Pulmonary findings on physical examination and routine chest radiography allow one to rapidly distinguish an intrathoracic from an intraabdominal process. It is caused by obstruction of venous return to the heart through the superior vena cava by a mass lesion. In caring for the patient with mediastinal disease, one must also pay careful attention to electrolytes and renal function, because patients with non-Hodgkin lymphoma and T-cell leukemia are at high risk of metabolic abnormalities associated with tumor lysis syndrome. Abdomen An observant parent may be the first to detect abdominal swelling or mass. Patients may also demonstrate lower extremity edema and scrotal swelling in the case of male patients or labial swelling in female patients. The patient may experience respiratory difficulties due to limited chest excursion with inspiration and renal dysfunction due to external compression of the renal vasculature. The most common malignant cause of hepatosplenomegaly is leukemia or lymphoma, in which case organomegaly is due to infiltration of the involved organs with malignant cells. The abdominal mass may also reflect a primary tumor originating from an intraabdominal organ, including the kidney, adrenal gland, liver, or ovaries. Children with neuroblastoma and other neuroblastic tumors may also present with an abdominal mass. This tumor may originate from the adrenal gland, resulting in a suprarenal mass, but also may originate anywhere along the sympathetic neural pathway. Unlike the well-encapsulated lesion of Wilms tumor described previously, neuroblastic tumors often wrap around vital vascular structures in the abdomen, making complete resection difficult. Unlike Wilms tumor, many of the patients will have metastatic disease at the time of diagnosis and may appear more ill. This photograph shows a patient with gingival hyperplasia resulting from leukemic invasion of the gums. A, Chest x-ray demonstrating a large anterior mediastinal mass in a teenage male presenting with Hodgkin lymphoma. A, Supine chest x-ray demonstrating a posterior mediastinal mass in a child with neuroblastoma. If malignancy is suspected, the diagnosis can sometimes be made through analysis of the pleural fluid. B, Cytology of the pleural fluid obtained by thoracentesis demonstrates large cells, high nuclear-to-cytoplasmic ratios, and fine nuclear chromatin, which are all features of malignant disease. The mediastinal masses that produce these findings often pose considerable anesthetic risk. Superficial venous distention may also be seen in cases of extensive intraabdominal tumor. The measurement of homovanillic acid and vanillylmandelic acid in the urine is an important aid to diagnosis and may be used to monitor disease status. Non-Hodgkin lymphoma of the abdomen has a wide range of clinical presentations, varying from marked retroperitoneal or mesenteric adenopathy to a clinical scenario that mimics an acute abdominal process, such as appendicitis or intussusception. The two most common hepatic tumors are hepatoblastoma and hepatocellular carcinoma. The former occurs more commonly in young children, with more than 75% of cases reported in children younger than 3 years old. An elevated -fetoprotein level may be observed in both tumors, although it is more often present in cases of hepatoblastoma. Germ cell tumors develop from the primordial germ cells of the embryo that would normally produce sperm or ova. Urogenital Tract Involvement of the genitourinary system or sacral area by tumor in infancy or childhood often results in the presence of visible abnormalities on physical examination. However, these tumors may also occur in retroperitoneal and intraabdominal locations. This teratoma has an external component and is easily visualized on physical examination.

Generic 16 mg atacand with mastercard
Reduction of the dislocated hip is apparent if hiv infection of a cell discount atacand express, on abduction of the hip to 45 degrees, a line drawn through the axis of the metaphysis of the neck crosses the triradiate cartilage. Because ossification is not evident radiographically until 3 to 6 months old, ultrasound evaluation of the hip is often helpful in determining the acetabular/femoral head relationships. Furthermore, in developmental dislocation, ossification may be delayed even longer, because normal articulation forces are absent. In teratogenic hip dislocation, there may be hypoplasia of both the acetabular and femoral sides with non-congruent development of one or both of these structures. Successful correction of congenital hip dislocation depends on early diagnosis and institution of appropriate treatment. In the first 6 months of life, use of a Pavlik harness, which permits gentle motion of the hip in a flexed and abducted position, may achieve and maintain a satisfactory reduction. Between 6 and 18 months old, gentle closed reduction and immobilization in a spica cast with or without surgical release of the contracted iliopsoas and adductor muscles is indicated. After 18 months old, reduction by manipulative measures is difficult owing to contractures of the associated soft tissues. In cases of teratogenic dislocation, underlying maldevelopment makes the outcome less satisfactory, even with optimal management. With early recognition and appropriate treatment, a relatively normal hip with satisfactory function can be anticipated in cases of idiopathic hip dislocation. Failure of concentric reduction or complications, such as avascular necrosis of the femoral head, resulting from overzealous attempts at closed reduction in long-standing cases, may result in a lifelong disability characterized by pain and stiffness in the hip; an antalgic, lurching gait; and shortening of the involved limb. Current theories implicate traumatic disruption of the blood supply and recurrent episodes of synovitis, during which increased intraarticular pressure compromises blood flow to the developing ossific nucleus, as causative. The disorder generally becomes manifest between 4 and 11 years old, with a higher incidence in boys. Affected children often exhibit delayed skeletal maturation and are small for their age. Unilateral involvement is the rule, and if a bilateral case is suspected, some form of epiphyseal dysplasia must be ruled out. The severity of the disease varies greatly, depending on the extent to which the femoral head is affected. Younger children generally have milder involvement, as a larger portion of the femoral head is still cartilaginous and less dependent on vascular supply. The child may present with symptoms characteristic of toxic synovitis without radiographic findings. Many children present with a painless limp, and others complain of thigh or knee pain, fatigue on walking, or hip stiffness. In general, the patient bears less weight on the involved leg when standing, and there is a flexion contracture of the involved hip. Pain and limitation of motion are encountered on attempts at internal rotation and abduction. The Trendelenburg sign (failure to maintain a level pelvis when standing on the involved limb) is positive. A, In cases of unilateral dislocation, the involved extremity is foreshortened and the thigh and groin creases are asymmetric. C, In this anteroposterior radiograph obtained in a 3-month-old child, the proximal left femur is displaced upward and laterally, and the acetabulum is shallow. The femoral head is not visible on the radiograph because of the delayed ossification associated with developmental hip dislocation. D, In the frog-leg view, the long axis of the affected left femur is directed toward a point superior and lateral to the triradiate cartilage, in contrast with that of the right, which points directly toward this structure. Early radiographic findings may include failure of progressive development of the femoral ossific nucleus, a subchondral radiolucent fracture line (Caffey sign), and evidence of slight subluxation. However, in early cases, radiographs may be completely normal, although a nuclear bone scan may be useful in verification of impairment of the blood supply to this region. Later, fragmentation of the femoral ossification center may be evident with flattening of the femoral head, extrusion, and frank subluxation. Although revascularization and reconstitution of the femoral head always occur, loss of mechanical integrity of the head with flattening and fragmentation of its surface may result in an irreversible predisposition to degenerative change. Most treatments are based on the principle of "containment" and the maintenance of a normal relationship of the femoral head within the acetabulum so as to minimize permanent joint incongruity. In young children with minimal symptoms and radiographic findings, decreased activity and close observation may be all that is necessary. In more severe cases, abduction casting, bracing, or surgical treatment with femoral or acetabular osteotomy to reposition the femoral head deeper within the acetabulum may be employed. He is bearing less weight on the involved right leg (note the slightly flexed right knee). On examination, a hip flexion contracture, which was detected by a positive Thomas test. B, In this anteroposterior radiograph, the right femoral epiphysis is flattened and fragmented. Slipped Capital Femoral Epiphysis Slipped capital femoral epiphysis, a disorder seen early in puberty, involves displacement of the femoral head from the femoral neck through the epiphyseal plate. It is seen more frequently in males and occurs bilaterally in approximately 25% of cases. Most commonly, it occurs at the onset of puberty in obese children with delayed sexual maturation. Although the etiology is unclear, it is generally thought that hormonal changes at the time of puberty may result in loss of mechanical integrity of the growth plate, and that if the epiphysis is then subjected to excessive shear stress, slippage through this area may occur. This condition differs from traumatic epiphyseal fractures, because the translational displacement occurs through a different portion of the growth plate. In some cases, an underlying connective tissue disorder (such as Marfan syndrome) or an endocrinologic problem (such as hypothyroidism) can be identified. The clinical presentation is characteristic, although the duration of symptoms varies. The patient presents with a painful limp and may or may not have a history of recent trauma, which is usually minor, or pain may have developed after jumping. This injury may have precipitated a slip in the previously weakened epiphysis or may have increased the degree of displacement of a slip that was already in progress. The lower extremity is held in an externally rotated position secondary to deformity at the site of physeal displacement. A flexion contracture may be noted, and range of hip motion tends to be diminished in all planes, particularly internal rotation. Radiographic findings vary from a widened and radiolucent physis (pre-slip) to a frank deformity with displacement of the femoral head on the proximal femur posteriorly and inferiorly in relation to its normal counterpart. The degree of slippage and deformity correlates with the extent of incongruity of the hip joint and the later development of degenerative change and painful symptoms. Prompt intervention to prevent further displacement is an important factor in preventing lifelong problems, and awareness of the condition, a high index of suspicion, and early recognition are key factors in improving prognosis. In patients with minimally or moderately displaced slips, stabilization of the slip by in situ pin fixation is indicated. In severe slips, especially those that have slipped acutely, pinning may be the treatment of choice initially, but development of avascular changes secondary to disruption of the blood supply to the femoral head may occur and complicate the outcome. When the disease is recognized late and deformity is severe, proximal femoral osteotomy may be necessary. Children with unilateral slipped epiphyses must be monitored closely for signs of involvement of the opposite limb. Femoral Anteversion Femoral anteversion may be viewed as a normal variation of lower extremity positioning in the developing child. In utero and at birth, the femoral neck sits in an anteverted position relative to that of the adult. During childhood, it remodels to a position of slight anteversion and normal alignment of the lower extremities.
Order discount atacand on-line
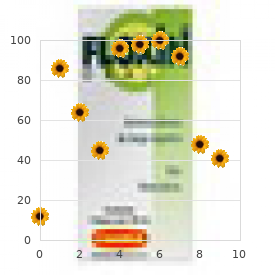
When these facial features are present antiviral infection definition order atacand online pills, the white of the sclera between the cornea and inner canthus frequently may be obscured or asymmetrical between the two eyes, giving the optical illusion that the eyes are esotropic. Parents and caretakers frequently report subtle esodeviations that worsen with gaze to the right or left. This is frequently pointed out in photographs in which careful examination shows the eyes to be in slight right or left gaze. Observation of symmetrical corneal light reflexes or cover testing confirms or excludes the presence of a true deviation. Pointing out the symmetry in the corneal light reflexes seen in photographs that the family is concerned about is frequently helpful. They may complain of images jumping as they switch fixation or of discomfort at night or when tired. Patients with intermittent exotropia usually do not have amblyopia, or it may only be mild. Treatment of intermittent exotropia may not be necessary if the deviation is not present frequently. Treatment consists of glasses to correct refractive errors, patching, and surgery. If there is poor vision in one eye, the decreased visual stimulation may produce a sensory deviation. The appearance of esotropia is due to the presence of a wide and flat nasal bridge, prominent epicanthal folds, and decreased intraorbital distance. Exodeviations may also occur with vision loss in one eye (sensory exotropia) and cranial nerve paralysis (third nerve palsy). An exodeviation may be controlled by fusion (exophoria), be manifest intermittently (intermittent exotropia), or be constant (exotropia). Intermittent exodeviations may become manifest with fatigue, daydreaming, or illness. Patients with exodeviations frequently squint one eye in bright light, but they typically do not experience the pupillary light is centered. It appears as if the right eye is esotropic but the light reflex remains centered in the pupil. This may cause symptoms of discomfort while reading, complaints of images jumping or moving, or intermittent diplopia at near range. To test for convergence insufficiency, the child is asked to fixate on a target with detail as it is brought progressively closer. If the eyes converge, and then break their alignment and diverge at a distance greater than 10 cm from the eyes, the patient should be evaluated for convergence insufficiency. With cover and uncover testing, an exodeviation will be seen at near fixation, and it will be smaller or not seen at distance fixation. Because young children do not complain of monocular vision loss, especially if congenital or with onset during infancy, sensory strabismus is frequently the presenting sign of vision loss caused by pathology of the retina or optic nerve. When the macula is displaced temporally, the eye rotates outward to align its visual axis on the fixation target. This appearance is caused by a temporal displacement of the fovea, usually due to cicatricial changes of the retina after retinopathy of prematurity. Third (Oculomotor) Cranial Nerve Palsy the third cranial nerve innervates the medial rectus muscle. In third nerve paralysis, the action of the lateral rectus muscle, innervated by the sixth cranial nerve, is unopposed and produces an exodeviation. The third nerve also innervates the superior and inferior recti; the inferior oblique muscles; the levator palpebrae superioris, which elevates the lid; the ciliary muscle, which is responsible for accommodation of the lens; and the iris sphincter muscle, which produces miosis of the pupil. In the presence of a complete third cranial nerve palsy, the eye assumes a down and outward position, the eyelid is ptotic, and the pupil is enlarged. The most common causes for acquired third nerve paralysis in children are trauma and tumor. Normal vascular pattern Fovea Vertical deviations may occur in only one field of gaze, or they may be comitant, the same, in all fields of gaze. Vertical deviations may have a cyclotorsional component and be associated with a head tilt or head posture to eliminate double vision. All patients with torticollis should be evaluated for cyclovertical muscle palsies. The most common cyclovertical deviation is due to a palsy of the fourth cranial (trochlear) nerve. The forced opening of tightly closed eyelids will reveal an upward, slightly outward movement of the eye under the closed eyelids (normal Bell response). Other features are elevation of the eye and difficulty depressing the eye in adduction. Children with congenital fourth nerve palsies usually do not have complaints of diplopia; but if they are asked about diplopia when their eyes are in the contralateral field of gaze, especially up and away from the paretic side, they can recognize the presence of diplopia. Later in life, patients with congenital fourth nerve palsy may decompensate in their control of the deviation and develop symptomatic diplopia. Some subtle facial asymmetry, especially of the cheek and jaw line, is almost always seen in congenital cases as the children age. Review of candid photos will frequently display consistently repeated head tilts that usually have not been noticed by the family. Brown syndrome describes an isolated motility disorder in which there is an inability to elevate the eye when in adduction. This may be caused by a congenital anomaly of the superior oblique tendon, or it may be acquired as an idiopathic inflammation or tenosynovitis of the superior oblique tendon. Double elevator palsy is an inherited unilateral or bilateral condition in which there is hypotropia and limitation of elevation of the involved eye. To achieve binocularity, patients tilt their chins up and position their heads back. In primary (straight ahead) gaze (A) and right gaze (B), the eyes are well aligned. In left gaze (C), the right eye is elevated or hypertropic because of overaction of the right inferior oblique. Additional causes of vertical deviations include myasthenia gravis, thyroid ophthalmopathy, chronic progressive external ophthalmoplegia, orbital fractures with muscle entrapment (most commonly the inferior rectus entrapped within a blowout fracture of the orbital floor), and orbital disease with intraorbital masses. Tests for Strabismus Although gross observation may detect the majority of cases of strabismus, pseudostrabismus will lead frequently to unnecessary referrals. More significantly, smaller angle deviations may be missed, leading to delays in treatment if more sensitive tests for strabismus are not employed by the primary care physician. The type and degree of ocular misalignment may be estimated using the corneal light reflex test, or Hirschberg method. Abnormal head posture is common with a head tilt away from the side of the fourth nerve palsy, as is overaction of the direct antagonistic inferior oblique muscle, seen as an elevation of the affected eye in adduction (gaze to the opposite side). The pupillary light reflex is observed and its relationship to the center of the pupil is noted. Normal corneal light reflex the reflexes are symmetrical and slightly displaced nasally to the center of the pupils. Left exotropia the corneal light reflex is displaced nasally to the center of the pupil. Esophoria compared with the reflex seen in the other eye, an esotropia is present. If the light reflex is displaced nasally in comparison with the other eye, an exodeviation is present. Although observation of the corneal light reflexes is more sensitive and specific than gross observation alone, a more accurate method of detecting misalignment of the eyes is cover and uncover testing. The cover test requires cooperation, vision in each eye and use of a target that stimulates accommodation. Cover testing is performed while the patient maintains fixation on targets at 6 m and at 1 m, because some types of strabismus produce misalignment of the eyes that is present only at either distance or near. The test is performed by placing a cover over one eye to disrupt fusion or binocularity. If the eye deviates while covered and then moves to regain fusion and assumes fixation as the cover is removed, a phoria exists.
Cost of atacand
Prolapse of an ureterocele may be associated with a palpable distended bladder or flank mass (hydronephrosis) secondary hiv infection symptoms purchase atacand uk. Ultrasonography of the bladder and kidneys demonstrates unilateral or bilateral hydronephrosis or hydronephrosis of a segment of a complete ureteral duplication, usually the upper pole of an obstructed renal unit. Prolapsed Ureterocele Prolapse of a large ureterocele through the urethral orifice should be considered in the differential diagnosis of all interlabial masses in infants and children. Ureteroceles are cystic dilations Ectopic Ureter Ureteral ectopia may be associated with a single collecting system or a complete duplication of the collecting system (complete ureteral duplication). In females, an ectopic ureter may drain into the bladder neck, urethra, urethrovaginal septum, vagina, or uterus. This is a chronic case in which the initial hemorrhagic nature of the acute prolapse has resolved with observation, leaving a protuberant, edematous urethra. A, A drop of urine exits from the orifice of an ectopic ureter located just below the urethral meatus in the urethrovaginal septum. B, Retrograde pyelography of the same ureter reveals a huge, tortuous ureter subtending the upper pole of a right complete ureteral duplication. The recognition of abnormal genitalia is the first step in the evaluation of intersex. The combination of hypospadias and bilateral or unilateral cryptorchidism should be considered as representative of intersex until proven otherwise. In some of these girls, a tiny ectopic ureter may be seen to drip urine from the introitus. Paraurethral Cysts Cystic lesions of the paraurethral or vaginal mucosa may be found on routine examination and are usually asymptomatic. They rarely cause voiding symptoms and occasionally present in older girls as palpable interlabial masses. Normal mucosa overlies the cyst, which usually displaces the urethral meatus slightly from the midline. Most cysts rupture spontaneously, but aspiration or marsupialization may be necessary. Congenital Obstruction of the Vagina Vaginal obstruction may occur as a result of an imperforate hymen, vaginal atresia or septa, or urogenital sinus malformation. Neonates may have abdominal masses or urinary retention; girls with a didelphic or bicornuate uterus may have pelvic pain or menstrual irregularities at puberty. Examination of the infant may reveal a distended vagina (hydrometrocolpos) with a bulging hymenal membrane. If a vaginal septum or atresia is the cause of the obstruction, external genital examination may be normal and a complete pelvic examination with vaginoscopy may be necessary. All girls with uterine or vaginal anomalies should have imaging of the upper urinary tract, given the high incidence of upper tract anomalies in this group. Pelvic ultrasound examination in the peripubertal period is an effective way to monitor these girls. Genital Ambiguity Associated With Imperforate Anus the embryologic deformity that produces a high imperforate anus in girls occasionally also influences the formation of the external genitalia by presumed local factors. A, Sagittal ultrasound of the pelvis in a neonate with a large pelvic hydrometrocolpos secondary to distal vaginal atresia. B, Catheter drainage of released white mucoid drainage with disappearance of the pelvic mass. A, Trauma to the glans penis from a falling toilet seat; a common injury that is usually best served by observation unless the urethra is disrupted. The testicular tunics were intact, and primary skin closure produced an excellent result. Although genital trauma may not be life-threatening, proper management may be important to the later well-being and psychosocial development of the patient. Trauma to the penis or scrotum should always raise the question of urethral injury. This is easily ruled out in the emergency department or x-ray department by injecting contrast (intravenous contrast in case of extravasation into vascular structures) through the urethral meatus, using a blunt-tipped syringe or a small catheter. Once urethral injury has been excluded, urethral catheterization can be performed safely. When injury is discovered, examination and repair should be performed in the operating room. Scrotal and testicular trauma is not uncommon in breech delivery when the scrotum is the presenting part. Ultrasound examination of the testes may be helpful if massive edema or hematoma precludes thorough examination. Trauma to the female genitalia and perineum usually requires examination under anesthesia to allow a complete evaluation of the injury, with concomitant repair when necessary. Techniques and interpretation of the pediatric neurologic examination are based largely on knowledge of normal growth and development. The examination is preceded by a thorough history of the presenting problem, including timing and mode of onset; course; and a past medical history that focuses on the antenatal, perinatal, and neonatal periods for possible prior insults. Abnormalities of birth weight; the need for resuscitation after delivery; early neonatal problems with hypoglycemia, hypocalcemia, or severe jaundice; and abnormalities in activity or difficulty feeding shortly after birth often serve as red flags. This is followed by a detailed history of behavior; growth and development with attention to evidence of delay, slowing, cessation, or regression of developmental milestones; and any possible association with prior illness or trauma. Obtaining a family history of neurologic, neuromuscular, or developmental problems is also important. The systematic neurologic evaluation proceeds from assessment of mental status and language functions through evaluation of cranial nerves, gross motor function, muscle strength, gait and station, balance and coordination, sensory systems, and deep tendon reflexes. It is applicable to older children and adolescents without significant modification from the evaluation geared to the adult. Tools essential to the neurologist include the reflex hammer, bright penlight, ophthalmoscope, and stethoscope. For evaluation of the primary sensory modalities of light touch, pain, temperature, and vibration, wisps of cotton, sterile disposable pins, glass test tubes (to hold hot and cold water), and a tuning fork (256 Hz for children and young adults, 126 Hz for older persons) are used. Derangements of primary sensory function may be present with lesions at the level of the nerve roots, plexuses, or peripheral nerves. If a particular area of decreased sensation is identified in part of a limb, careful delineation of its boundaries often suggests root (dermatomal), plexus, or peripheral nerve involvement. Neurologic examination of the younger child requires flexibility and a gentle, staged approach. Facies, head shape, body habitus, spontaneous movements, position, and posture are noted, along with spontaneous vocalizations and quality and pitch of cry in infants. In the child old enough to walk, stance and gait, as well as the ability to run, stoop, and recover; climb onto a stool; and rise from the floor (when developmentally appropriate), are observed. Much of the remainder of the neurologic examination also lends itself to play, and in the second stage of observation a more detailed assessment of mental status, language, handedness, and fine and gross motor skills is performed by engaging the child in play. Williams selection of rattles, keys, spinning and mechanical toys, dolls, cars, small blocks, noise makers, tennis balls, hand puppets, crayons, and picture books supplement the traditional instruments. If further observation of gait is necessary, the examiner can have the child walk to or with the parent. Children older than 4 years old love to show what they can do when asked to walk on their heels or toes, hop, or do tandem gait along a line. Pat-a-cake games are popular for testing rapidly alternating movements with young children. Trying to catch the otoscope light as it is shown over various parts of the body can act as the prologue to following the light with the eyes and looking at it. For infants and toddlers, following a face or spinning toy is still better for testing extraocular movements. Asking young children to make faces, stick out their tongues, and blow up balloons is another helpful technique in assessing cranial nerves. These are normally brisk, or 3+, in the young infant, becoming 2+ by 6 months old.
Diseases
- Schwartz lelek syndrome
- Kosztolanyi syndrome
- Leiner disease
- Yim Ebbin syndrome
- Christianson Fourie syndrome
- Mucopolysaccharidosis type IV-A Morquio syndrome
Cheap 4mg atacand visa
Staining of the teeth or fingers or the presence of conjunctivitis may be indirect clues to the underlying cause of the cough hiv infection circumcision purchase 4mg atacand free shipping. Bronchogram shows cylindrical bronchiectasis of the left lower lobe in a 5-year-old girl with recurrent pneumonia and chronic cough. Recurrent infection of the middle lobe can ultimately lead to the development of bronchiectasis or fibrosis. Disorders of ciliary motility (primary ciliary dyskinesia and acquired ciliary dyskinesia) may produce insidious symptoms of chronic productive cough, nasal drainage, recurrent middle ear infections, and fever. Primary ciliary dyskinesia is most often transmitted in an autosomal recessive inheritance pattern. Genetic characteristics are quite heterogenous, with 31 genes presently identified as disease causing. Clinical findings include basilar crackles (which can be expiratory) and, later, radiographic changes of recurrent lower lobe infections and bronchiectasis. Repetitive infections occur unless measures (such as, chest physical therapy, postural drainage, and liberal use of antibiotics) are employed. It is now recognized that the classic triad described by Kartagener of situs inversus, sinusitis, and bronchiectasis fits only a limited number of patients, because situs inversus occurs in only about half of all patients with primary cilia dyskinesia. Far more common is an acquired ciliary dyskinesia that can follow certain lower respiratory infections (including adenovirus, Mycoplasma, respiratory syncytial virus, and influenza). Diagnosis can be made via biopsy of the respiratory epithelium, either from curettage of the nasal turbinate in the office or forceps biopsy of the bronchus via rigid bronchoscope under anesthesia. It may also be suggested by a reduced fraction of nitric oxide in exhalate from the nose. Pulmonary hemosiderosis is a potentially fatal disorder that has been described in association with cardiac or panorganic disease, glomerulonephritis (Goodpasture syndrome), collagen vascular diseases, and as an idiopathic form. Hematemesis or melena may be the only presenting complaint in some patients without symptoms referable to the respiratory tract. A wet-sounding (productive) cough suggests suppurative lung disease, such as cystic fibrosis, other forms of bronchiectasis, or ciliary dyskinesia syndromes. The cough in these patients tends to be most severe in the morning, because excessive secretions pool in the tracheobronchial tree during sleep. Increased morning cough is also common in patients with sinusitis or increased upper airway secretions from viral infection or allergic rhinitis. A croupy cough may be observed in patients with acute laryngotracheobronchitis, and there may be associated wheezing. A dry or brassy cough is generally seen in patients with larger airway pathology, such as in tracheitis or drainage from upper respiratory tract disease; a psychogenic cough may produce similar findings, but this type of cough may be distinguished from the others by its disappearance with sleep. As noted previously, a psychogenic cough is often (but not always) loud, honking, and disruptive. Cough occurring during or shortly after activities suggests exercise-induced asthma, cystic fibrosis, or bronchiectasis. Clinical findings associated with a cough may also point to the nature of the problem. A cough occurring in the presence of poor weight gain and malabsorption makes cystic fibrosis a concern. Cough occurring with wheezing suggests asthma; and if evidence of rhinitis, conjunctivitis, or "allergic shiners" is present, allergic disease may also be a consideration (see Chapter 4). Cough that is worse in spring and summer months or that occurs only after exercise suggests asthma. Worsening of the cough in the winter is consistent with cold-induced bronchospasm or recurrent viral illnesses. Diagnostic Approach the approach to diagnosing a patient with persistent cough begins with a complete history in which some of the factors alluded to earlier are targeted (Box 17. On physical examination, close attention to nutritional status, associated upper respiratory tract disease, or clubbing of the digits is as important as the examination of the chest. On auscultation of the chest, a localized wheeze, particularly if associated with delayed air entry, suggests a foreign body or focal airway lesion leading to narrowing. Crackles are also present during one-third to one-half of untreated asthma exacerbations, even in the absence of infection. Inspiratory and expiratory radiographs and fluoroscopy may be indicated if inhalation of a foreign body is suspected. Pulmonary function testing can detect lower airway obstruction that may be inapparent on physical examination; improvement in airflow with bronchodilator administration supports a diagnosis of asthma. In some cases, an outpatient trial of inhaled corticosteroids lasting several months or an empirical brief course of oral corticosteroids may serve to confirm the suspicion of asthma. Failure to respond to this regimen suggests that asthma is not the problem, but it could be the result of noncompliance with the prescribed medications. This term refers to asthma in which cough, rather than wheezing, is the primary symptom. Such patients always have other signs of small airway obstruction, ranging from hyperinflation evident on percussion of the chest to abnormalities on pulmonary function testing, and as such are diagnosed as having asthma on these grounds. Examination of sputum with Wright or Gram stain or by cultures may lead to a diagnosis. Clear, mucoid sputum containing eosinophils is likely to represent asthma, whereas purulent green sputum is more suggestive of suppurative lung disease, such as cystic fibrosis. The presence of polymorphonuclear leukocytes with organisms suggests bacterial infection. A yellow color can be imparted to the sputum by breakdown products of white blood cells; therefore, yellow sputum can be seen with bacterial infection or asthma. Upper respiratory tract irritation with epistaxis may lead to the mistaken notion that hemoptysis is occurring. Quantitative immunoglobulins and immunoglobulin subclasses may be helpful in detecting some immunodeficiencies, and an elevated immunoglobulin E (IgE) suggests allergic disease. Bronchoscopy may exclude the diagnosis of foreign body or airway malformation as the cause of chronic cough. If foreign body inhalation is likely (based on history and/or physical examination), bronchoscopy is essential and should be performed under general anesthesia with the rigid bronchoscope by a surgeon. A barium swallow is useful in patients with suspected tracheoesophageal fistula or primary swallowing disorders. In patients suspected of having ciliary dysmotility, a nasal or bronchial ciliary biopsy for examination by light and electron microscopy or a nuclear medicine scan measuring the movement of inhaled radiolabeled particles within the central airways may be indicated. Stridor is characteristically a harsh inspiratory noise created by obstruction of the larynx or the extrathoracic trachea. With a mild degree of airway narrowing, breath sounds may be normal when the infant or child is at rest, but with any activity that increases tidal breathing. The most common cause of inspiratory stridor in the pediatric population is infectious croup (acute laryngotracheobronchitis). This disease is most commonly caused by a respiratory virus (parainfluenza, respiratory syncytial, influenza, or rhinovirus), and the patient typically has coryza for 24 to 48 hours before the appearance of croupy cough, hoarseness, and stridor. Occasionally the inflammatory process may spread to the smaller airways and produce wheezing in addition to these symptoms. The "steeple sign" is a characteristic radiographic sign on anteroposterior projections that may be accompanied by marked dilation of supraglottic structures, particularly on lateral films. In the majority of patients, serious airway obstruction does not occur and the disease is self-limited. Some children with anatomically normal airways suffer recurrent bouts of stridor, usually in the middle of the night, in the absence of signs of viral infection. The stridor associated with congenital laryngomalacia generally begins within the first week of life, varies with activity, and is more noticeable in the supine position. Clinical symptoms may suggest the diagnosis; but if severe, bronchoscopic visualization of airway dynamics by flexible bronchoscopy is a safe and reliable method of excluding other causes of stridor. Parents can be reassured that this entity is self-limited, becomes less marked after 6 to 10 months of age, and rarely causes serious problems. Narrowing of the subglottic region can be congenital or acquired, such as in subglottic stenosis associated with endotracheal intubation. Congenital subglottic stenosis improves as the child grows older, but narrowing associated with tracheal intubation may require a tracheostomy, particularly if the infant remains dependent on ventilatory support. Congenital laryngeal or pharyngeal masses can also produce stridor by obstructing airflow. Although inspiratory stridor may be observed, hoarseness is a more common presenting feature. Laryngeal webs, papillomas, or hemangiomas may all present with ongoing stridor, as well as brassy or dry cough.
Cheap atacand online
The latter two components are tested by having the patient turn the palm up and down respectively antiviral garlic generic atacand 16mg without a prescription, with the elbow flexed. Because of the proximity of the brachial artery and the median, radial, and ulnar nerves to the elbow joint, injuries of the elbow necessitate a careful neurovascular examination. Wrist and Hand During examination of the wrist and hand, one should observe skin color, check capillary refill, and palpate the radial and ulnar pulses to assess circulation. Any swelling or edema should be noted, as well as any abnormal posture or position. The presence of intraarticular fluid in the wrist is manifested by swelling and tenderness, especially evident dorsally, and by restriction of wrist motion. Wrist motion has four components: flexion with the hand held down (normally 70 to 80 degrees); extension with the hand held up (normally 70 degrees); and ulnar and radial deviation (normally 25 degrees and 15 to 20 degrees, respectively). With the patient supine, the limb to be tested is grasped behind the ankle and elevated into hip flexion with the knee in full extension. If pain is produced well before 90 degrees of flexion is achieved, the test is positive, indicating irritation of a sciatic nerve root. The examiner should also note any evidence of missing spinous processes (step-off) or their deviation from the midline and palpate the paravertebral muscles for spasm and tenderness. Increased kyphosis, especially in the thoracic region, may be detected when viewing the patient from the side. Leg length inequality may be evaluated during the upright standing portion of this test (see the Lower Extremity Examination section, later) and, if present, should be corrected with appropriate lifts under the short side in order not to cause a false forward bend test. Any examination of the spine must include a neurologic assessment of strength, tone, reflexes, and sensation. The limb to be tested is grasped behind the ankle and elevated passively into hip flexion with the knee fully extended. This maneuver stretches the sciatic nerve as it passes behind the hip joint, and if one of its several roots has been irritated by a protruded disk, mass, or inflammatory process, pain will be felt with only 15 to 30 degrees of hip flexion. Normally the straight leg can be brought to 90 degrees of hip flexion without difficulty. Shoulder When examining the shoulder, first the position of the upper limbs is observed, at the same time noting whether there is any swelling, asymmetry of height, or visible landmarks and looking for any difference in spontaneous movement. Prominent landmarks that are easily palpable include the acromion process lying laterally and subcutaneously, the clavicle, the spine of the scapula, the coracoid process, and the bicipital groove. Swelling of the glenohumeral joint capsule and atrophy of the shoulder muscles are best appreciated by viewing from above with the patient seated and by comparison with the normal side. Assessing range of motion is important because many shoulder problems are manifested by a loss of normal motion. Abduction, a function of the deltoid muscle, is tested by having the patient raise the extended, supinated arm up so that the hand is directly above the shoulder (180-degree abduction). The normal relationship of the extended supinated forearm to the upper arm is not a straight line but involves 5 to 10 degrees of lateral or valgus angulation. Observation of the position at rest (normally a loose fist with all the fingers pointing in the same direction and with the same degree of flexion) and of use during play is often helpful. Having the parent perform various hand and finger motions while trying to get the child to imitate these can be helpful in some cases. Handing the child a small object (such as a key) or a thin piece of paper (such as a dollar bill) may suffice for assessing opposition of thumb to fingers, which in the older child is tested by having him or her touch the tip of the thumb to the tip of the little finger. Because the bones of the hand are subcutaneous, displaced fractures and dislocations are readily evident on inspection. Laceration or rupture of the tendons is common because of their superficial location. Conversely, extensor tendon lacerations result in flexor muscle overpull, with the opposite result. Functional testing of the tendons and intrinsic muscles of the hand is generally possible in older children. They can be asked to extend the fingers at the metacarpophalangeal joints and each interphalangeal joint. The intrinsic muscles of the hand are evaluated by having the child adduct and abduct the fingers toward and away from the middle finger. Sensation is best tested using two-point discrimination and pinprick in older children and by touch in very young children. Muscle strength in the upper extremity is largely tested during assessment of range of motion of the joints, with and without resistance. Signs of neural dysfunction with injury of the upper extremity are listed in Table 22. Lower Extremity Examination Hip Examination of the hip begins by assessing gait (see later discussion) and stance, checking the latter to see if the anterior superior and posterior superior iliac spines and the greater trochanters are level. Total length is measured from the bottom of the anterior superior iliac spine to the medial malleolus of the ankle with the patient supine. If inequality is found, the knees are flexed to 90 degrees with the feet flat on the examination table. If, as the examiner looks from the foot of the examination table, one knee appears higher than the other, the tibias are unequal in length; if one knee is anterior to the other when viewed from the side, the discrepancy involves the femurs. If total leg lengths are equal, the inequality apparent when the patient is standing may be due to pelvic obliquity or flexion contracture of the hip. The latter may also be associated with a compensatory accentuation of lumbar lordosis. If atrophy is found, circumference should be measured and compared at a fixed point below the greater trochanters. Because the hip lies deep and is surrounded by muscles, direct inspection is impossible and palpation is of limited value (although the femoral triangle, greater trochanter, and posterior aspect should be palpated to check for tenderness). As a result, assessment of the position of comfort (abduction and external rotation are seen with effusion, hemarthrosis, and fracture; see. In evaluating range of motion of the hip, care must be taken to distinguish true hip motion from that occurring in combination with pelvic rotation or trunk flexion. The hip to be tested is passively flexed while the contralateral hip and pelvis are observed or stabilized by one hand. The limit of flexion is reached when movement of the contralateral pelvis is noted. Alternatively, both hips can be flexed simultaneously to stabilize the pelvis and eliminate truncal flexion. The Thomas test is performed by flexing both hips so that the thighs touch the abdomen. Then one is held in place, thereby eliminating lumbar lordosis and movement of the lumbosacral joint, and the patient is asked to extend the hip to be tested. Patients with leg length inequality manifest depression of the trunk and pelvis during the stance phase on the shorter leg and circumduction of the longer leg during swing. Some children try to compensate for the leg length inequality by toe-walking on the shorter extremity. Patients with limited hip motion compensate by thrusting the pelvis and trunk forward in the swing phase. When knee flexion is limited, children tend to hike up the pelvis on the involved side during the swing phase and circumduct the leg to clear the foot from the floor. A circumduction gait can also be related to a painful condition involving the ankle or a limitation of ankle motion. By circumducting the leg laterally during swing phase, the patient reduces the need for ankle motion. Gait Disturbances Resulting From Weakness or Spasticity Patients with weakness of the hip abductors (gluteus medius muscle) have a Trendelenburg gait. Because they are unable to maintain a level pelvis and linear progression of their center of gravity, their pelvis tilts toward the unsupported side and their shoulder lurches toward the weak side during stance phase to maintain their center of gravity over the foot. Patients with weakness of the gluteus maximus (seen most commonly in children with Duchenne muscular dystrophy) have to hyperextend their trunk and pelvis to maintain their center of gravity posterior to the hip joint (see Chapter 16). Proximal muscle weakness may also be demonstrated by observing a child getting up from the floor unassisted. A Gower sign indicates weak hip extensors and abductors, necessitating that the patient use his arms to assist in standing by placing his hands on his anterior thighs and pushing up, progressively moving his hands upward along the thighs until erect posture is achieved (see Chapter 16). Children with weakness of the quadriceps femoris muscle may have a relatively normal gait on level ground but difficulty climbing stairs.

Order cheap atacand on-line
The following sections list general types of medical and surgical complications that are experienced by children with skeletal dysplasias xem phim antiviral generic 8mg atacand free shipping. Neurologic Complications Hydrocephalus is a common complication in infants and children with achondroplasia. This results from poor cerebrospinal fluid drainage, due primarily to foramen magnum stenosis. Because an enlarged head is normal in achondroplastic children, pediatricians can use a special head circumference growth chart to distinguish between normal growth and possible hydrocephalus. Treatment for hydrocephalus is surgical, including decompression surgery and placement of a ventriculoperitoneal shunt. Clinical symptoms of hydrocephalus and foramen magnum stenosis include brisk reflexes, numbness, weakness, difficulty walking, loss of bowel and bladder control, and central sleep apnea. Complications Each dysplasia has unique characteristics, making generalizations about medical and surgical complications difficult. A, A 6-month-old female with diastrophic dysplasia showing characteristic facial features of a long, full face; broad forehead; and prominent cheeks and perioral fullness. D, Ear showing malformed pinna; this is called a "cauliflower ear" because of the blister-like sacs filled with fluid on the upper part of the ear. These swollen sacs will drain naturally, but most often leave a misshapen upper ear. In the neonatal period, it is important to monitor the cervical spine for C1 to C2 instability due to odontoid hypoplasia and ligamentous laxity. Screening should be performed within the first 6 months of life and then yearly as indicated. Treatment involves surgical fusion of C1 to C2 to prevent slippage of vertebrae and subsequent death or paralysis. Lumbar-sacral stenosis can be a common complication for adults with achondroplasia. Progressive narrowing of the spinal canal in the lumbar and sacral regions can lead to pain, difficulty in walking, loss of bowel and bladder control, and ultimately paralysis. The risk of lumbar-sacral stenosis can be lessened by providing adequate support to infants in the first year of life who exhibit significant kyphosis. Recent evidence suggests that counseling families on selective bracing and prohibiting unsupported sitting in the first 18 months of life can prevent fixed lumbar lordosis and reduce to zero the risk for severe lumbar-sacral stenosis requiring surgery later in adulthood. This finding demonstrates the positive impact of anticipatory guidance and monitoring early in life for these patients. Orthopedic Complications There are a variety of orthopedic complications seen with skeletal dysplasias. One of the more common and more troublesome adult sequelae is premature and severe osteoarthritis that can develop as early as adolescence. Progression is more rapid than scoliosis in patients without skeletal dysplasia and may result in mechanical, neurologic, and heart/lung complications that necessitate bracing or early surgical repair. Valgus and varus deformities are also common in many of the skeletal dysplasias, due to irregular bone growth. Other Complications Obstructive sleep apnea is common in many skeletal dysplasias but especially achondroplasia. The condition arises from small bony air passages of the midface or a crowded hypopharynx, resulting from a tiny jaw or thickened soft tissues. Symptoms include snoring, apnea, and sweating during sleep; failure to thrive; and developmental delay. Eustachian tube dysfunction due to abnormal craniofacial shape, midface hypoplasia, and shortened eustachian tubes is common in many forms of dwarfism, but most often achondroplasia, resulting in recurrent otitis media. Children should have ear examinations with every upper respiratory infection to prevent chronic otitis media, hearing loss, and speech delay. Treatment may include tympanostomy tube placement, tonsillectomy and adenoidectomy, and repair of cleft palate when present. Development for Children With Skeletal Dysplasias Growth should be monitored using specialized growth charts for height, weight, and head circumference. Special growth charts now exist for achondroplasia, spondyloepiphyseal dysplasia, diastrophic dysplasia, and pseudoachondroplasia. Children with skeletal dysplasias frequently have delayed motor milestones, but they typically have normal cognitive, social, and language development. Depending on the timing of injury, signs may be present at birth or they may become evident in infancy or early childhood. The primary cerebral insult may be intrauterine or perinatal infection; a prenatal or perinatal vascular accident; anoxia due to placental insufficiency, difficult delivery, or neonatal pulmonary disease; hyperbilirubinemia resulting in kernicterus; or neonatal hypoglycemia. Abnormal motor function is the most obvious result and may take the form of a spastic neuromuscular disorder (65% of cases), athetosis (25%), or rigidity and/ or ataxic neuromuscular dysfunction (10%). Sensory deficits and intellectual impairment are common, and there is a significant incidence of associated seizure disorders. Because of the number and variety of possible insulting factors, each of which has its own spectrum of severity, there is a broad range in the location and extent of neural damage, and thus in the degree of functional impairment. Patients with severe afflictions generally have early evidence of gross neuromuscular dysfunction. Those with milder involvement may have subtler abnormalities and may be diagnosed only after they fail to achieve normal developmental and motor milestones. Patterns of the affliction include involvement of one or two limbs (monoplegia or hemiplegia), of both lower extremities (diplegia), of all four extremities (quadriplegia). Those patients with a spastic disorder exhibit flexion contractures of the involved limbs, hyperreflexia, and spasticity; those with athetosis exhibit the characteristic movement disorder. Patients with severe involvement that inhibits sitting and ambulation suffer disuse atrophy of involved muscles and skeletal demineralization that increases their risk of pathologic fractures (see Chapter 6). Although cerebral palsy is by definition a nonprogressive neurologic condition, the orthopedic manifestations of the condition are frequently progressive. The progression of orthopedic problems is related to the severity and distribution of spasticity in the child. Increased spasticity in certain muscle groups leads to shortening and contractures in muscles and tendons, imbalance of mechanical forces across a joint or extremity, and eventual bone and joint deformity secondary to the Hueter-Volkmann principle. This principle states that the growth of any bone or joint can be altered by uneven, nonphysiologic mechanical forces across the bone or joint, leading to permanent deformity. He requires crutches to ambulate, seizure medication, and a specialized educational program. Hip deformity, dislocation, and associated arthritic changes are the result of significant and prolonged imbalance of muscle pull about the hip. It is estimated that in 50% of children with untreated hip dislocation, pain may become significant and problematic, necessitating hip resection or replacement in adolescent or adult life. The development of pain in these children who are non-ambulatory may be significant because the spasticity of their muscles generates forces across the hip joints that are equivalent to those of ambulatory children. Treatment goals in cerebral palsy are to prevent musculoskeletal deformity, to improve function and reduce pain, and to attempt to "balance" the muscle forces across the bones and joints in those children with severe spasticity. Administration of medications that reduce muscle spasm, and carefully timed and selected surgical procedures, are helpful. Oral baclofen can also be helpful in reducing spasticity, ameliorating the pain due to associated muscle spasm, and preventing contractures and bone and joint deformity. Botulinum toxin injections into spastic muscles can also be used to reduce spasm, and these injections can be given in an outpatient clinic. In evaluating patients with apparent cerebral palsy, one must be careful to rule out a progressive neurologic disorder, such as intracranial or spinal cord neoplasia, degenerative neurologic conditions, and tethering of the spinal cord. Spasticity of the extremities can be a physical finding indicative of upper motor neuron pathology from numerous etiologies. A, this 9-year-old with quadriplegic cerebral palsy has a dislocated left hip as a result of spasticity and unbalanced muscle pull. This is a source of significant pain in about 50% of cases whether or not the child is ambulatory, and surgical treatment is indicated. B, this is the proximal femur removed from another child with severe spasticity and a painful dislocated hip. This and disuse osteoporosis make it easy for a metal probe to perforate the femoral head. From an orthopedic standpoint, emphasis is placed on optimizing neuromuscular function by attempting to assist the achievement of progressive motor milestones, including the ability to sit, stand, walk, and perform activities of daily living.
Order atacand 4 mg without a prescription
Vitamin D deficiency may also be the consequence of intestinal malabsorptive disorders antiviral zidovudine order atacand 8mg line, such as celiac disease, biliary obstruction, gastric resection, cystic fibrosis, or pancreatic insufficiency. In the majority of infants and children with rickets, total calcium levels are usually borderline-normal or low; phosphate levels are low. The first step, 25-hydroxylation, occurs in the liver to generate 25-hydroxyvitamin D. The second step, 1-hydroxylation, takes place in the kidney to generate 1,25-dihydroxyvitamin D. The biologic actions of vitamin D are mediated by the vitamin D receptor, which is a member of the steroid/thyroid hormone nuclear receptor family. Measurement of 1,25 dihydroxyvitamin D does not provide information regarding body vitamin D stores and is usually not necessary. It may be indicated when abnormalities of the enzyme that converts 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D, or renal disease, are suspected. Elucidation of the pathways involved in vitamin D metabolism has identified the molecular basis for rickets unresponsive to Table9. In general, approximately 85% to 90% of filtered phosphate is reabsorbed by the kidney. Hypophosphatemic rickets is characterized by severe hypophosphatemia, postnatal growth retardation with short stature, genu varum, and dental anomalies. In addition to the radiographic findings of rickets, affected subjects have low alkaline phosphatase activity and increased urinary phosphoethanolamine excretion. Adrenal Glands the adrenal glands consist of the inner adrenal medulla and the outer adrenal cortex. Cells destined to develop into the adrenal medulla have an ectodermal origin, whereas adrenal cortical cells have a mesodermal origin. At approximately 7 to 8 weeks of gestation, sympathetic cells derived from the neural crest invade the adrenal primordium; these cells will differentiate as the adrenal medulla, which is responsible for the production of epinephrine and norepinephrine. The adrenal cortex utilizes cholesterol is the precursor for all adrenal steroids. Most cholesterol used for steroid hormone biosynthesis is derived from dietary sources. Steroid secretion is dependent on de novo steroid production, because cortisol is not stored in the adrenal cortex. During fetal life, the adrenal cortex consists of the fetal adrenal cortical zone, which involutes during the first year of life, and the outer definitive zone. Postnatally, the definitive adrenal cortex develops into the adult adrenal cortex, comprising three distinct zones. Mineralocorticoids influence electrolyte balance intravascular volume, and blood pressure. Aldosterone secretion is regulated by the renin-angiotensin system and serum potassium concentrations. Aldosterone actions are mediated by the mineralocorticoid receptor, which is a member of the steroid-thyroid hormone-nuclear receptor family. The multiple biologic actions of glucocorticoids include effects on carbohydrate metabolism, immune function, skeletal growth, and cell differentiation. The glucocorticoid receptor, another member of the steroid-thyroid hormone-nuclear receptor family, mediates the tissue specific physiological and pharmacological actions of glucocorticoids. Following glucocorticoid binding to the cytoplasmic receptor, the receptor dimerizes and translocates to the nucleus where the receptor-ligand complex induces or represses target gene transcription. The adrenal androgens do not bind to the androgen receptor but are readily converted to more potent androgens by extraadrenal enzymes. Disorders of the Adrenal Cortex Cushing Syndrome Cushing syndrome, the phenotype resulting from excessive glucocorticoids, can be due to either excessive endogenous or exogenous steroid exposure. The characteristic features of Cushing syndrome include rounded facies, plethora, central obesity, impaired linear growth, fatigue, and hypertension. Muscle weakness and muscle wasting occur, resulting in comparatively thin extremities. Loss of bone mineral density and osteopenia/osteoporosis can occur with chronic glucocorticoid exposure. Treatment with pharmacologic doses of glucocorticoids is the most common cause of Cushing syndrome in children. Adrenal tumors are the most common cause of endogenous Cushing syndrome in children younger than 7 years old, whereas Cushing disease is more common in older children and adolescents. The differential findings in the specific etiology of Cushing syndrome are listed in. The first step in the diagnosis of Cushing syndrome is confirmation of elevated cortisol concentrations. Measurement of midnight salivary cortisol concentrations is helpful, because individuals with Cushing syndrome typically manifest loss of normal cortisol diurnal variation. Some obese individuals have elevated cortisol secretion rates; correction for body surface area generally normalizes the results. Overnight, low-dose, and high-dose dexamethasone suppression tests may help confirm the diagnosis and discriminate among the potential etiologies. Most obese individuals show suppression of the morning cortisol concentration after an overnight dexamethasone stimulation test (1. Once endogenous excessive glucocorticoid secretion is confirmed, additional studies are needed to identify the specific etiology. Because pituitary adenomas may be small, bilateral inferior petrosal sinus sampling may be necessary to localize the adenoma before surgery. These photographs show how dramatic the changes associated with Cushing syndrome are and how rapidly they occur. Note the centripetal obesity of the trunk compared with the extremities after the onset of Cushing syndrome. C, Moon facies, clearly demonstrated, should raise the diagnostic index of Cushing syndrome. Excessive adipose tissue over the lower cervical and upper thoracic spine is characteristic of Cushing syndrome. Primary adrenal insufficiency is characterized by glucocorticoid and mineralocorticoid deficiencies. Hyperpigmentation of the skin and mucous membranes may be striking and appears as bronzing of the skin that is more obvious in flexor creases, in scars, and over the areolae of the nipples. If untreated, patients with Addison disease progressively weaken and vascular collapse ensues. The decreased circulating plasma volume is reflected by the thinned, narrow heart shadow seen on a chest radiograph. Many of these disorders have been found to be associated with monogenic disorders. Autoimmune destruction of the adrenal gland has now replaced tuberculosis as the most common cause of the disease especially among adults. The type 2 form (Schmidt syndrome) is characterized by diabetes, hypothyroidism, and adrenal insufficiency. Neonatal adrenal hemorrhages and meningitis (Waterhouse-Friderichsen syndrome) can destroy the adrenal cortex resulting in acute adrenal insufficiency. Genetic disorders associated with adrenal destruction include adrenoleukodystrophy, Zellweger Syndrome, and Wolman Syndrome. A, this patient shows the thin habitus and ill appearance characteristic of Addison disease. The Zellweger syndrome represents a spectrum of autosomal recessive disorders with three overlapping phenotypes that differ in severity and age at presentation. These disorders include Zellweger syndrome, infantile Refsum disease, and neonatal adrenoleukodystrophy. Ocular abnormalities, hepatic dysfunction, and developmental delay may be present. The diagnosis can be verified by functional assays in cultured skin fibroblasts and followed by mutation analysis.
