
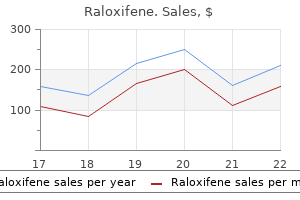
Buy raloxifene us
Local reactions tend to be more frequent with repeated doses or booster doses of vaccine womens health center xenia ohio order generic raloxifene line. Rarely febrile seizures may occur following vaccination with measles, mumps, and rubella vaccine. Reports of syncope following vaccination have been increasing since the approval of human papillomavirus and tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccines. Health care professionals should implement measures to mitigate secondary injuries when vaccinating this age group. Zoster is the reactivation of latent varicella zoster virus in the sensory ganglia. Zoster most frequently occurs in the elderly and immunocompromised individuals who have decreased circulating antibodies to varicella zoster virus. Patient Encounter 2 A 65-year-old patient presents to the pharmacy to pick-up his prescription for blood pressure medication. The pharmacist asks the patient if he would like to receive his vaccines, and the patient accepts. The assumption is that thimerosal, also known as ethyl mercury, causes similar effects as methyl mercury, which has neurotoxic and nephrotoxic effects at high doses. Numerous epidemiologic studies have not shown a higher rate of autism among children receiving thimerosalcontaining vaccines when compared with the normal background rate of autism. Additionally, the mercury exposure with vaccination is much lower than through many other environmental exposures. It is thought to be caused from the development of autoimmune antibodies that cause damage to the peripheral nerves. Caution is still recommended with influenza vaccines since the influenza strains contained in the vaccine has the potential to change each year. The health provider takes the opportunity to review her vaccination records and finds she is due for her routine adolescent vaccines. In general, all vaccinations should be updated prior to the person becoming immunosuppressed. Once a person becomes significantly immunosuppressed, live virus vaccines should be avoided. Inactivated influenza vaccine is given yearly, starting 6 months after transplant. Measles, mumps, and rubella can be given 2 years after transplant and varicella and zoster vaccines are contraindicated. Prior to transplant, children should complete primary immunization schedules if possible. Otherwise primary immunization schedule with inactivated vaccines may continue 2 months following transplantation. Yearly seasonal inactivated influenza vaccination may be given 6 months following transplantation. Children in the household may receive live virus vaccines without special precautions; however, if a rash develops following varicella vaccination, contact should be avoided with the immunocompromised host until the rash resolves. Mothers who are vaccinated in the second half of the pregnancy will have maternal transfer of antibodies through the placenta giving protection to the newborn infant. Pregnant women should be vaccinated with inactivated influenza and tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccines during each pregnancy. Ideally the vaccines should be administered after 20-week gestation, but can be administered at any time during the pregnancy. Women found to be nonimmune to rubella or varicella may be vaccinated soon after delivery, but not during the pregnancy. Health care professionals should have documented immunity to measles, mumps, rubella, and varicella. Health care professionals with direct patient contact should also receive the Hepatitis B vaccine series and have proven immunity following the series. As concerns regarding the rise of pertussis among adults, it is now recommended that all health care professionals receive at least one dose of tetanus, reduced diphtheria, and acellular pertussis vaccine to protect against pertussis. Many health care facilities are now mandating that employees receive yearly influenza vaccination or wear masks during influenza season. From a societal perspective, for every dollar spent on routine childhood vaccines, there will be a $10 savings in direct and indirect costs. This has been attributed to the requirements for proof of vaccination by States for enrollment into daycare centers and school. Adolescents present a unique challenge for vaccinating because they do not have as many encounters with health care professionals as young children do. However, the constantly changing immunization schedules makes this population vulnerable to missing newly approved vaccines and catch-up doses of vaccines that were not recommended when they were younger. Every encounter with a health care establishment should be viewed as an opportunity to evaluate and vaccinate if necessary. Adolescents may also have incomplete medical records due to changes in health care providers. Therefore, it is important for health professionals to regularly utilize universal State immunization databases that document pediatric and adult vaccinations. This eliminates the problems of lost immunization records if a child changes health care providers. Only 50% to 60% of adults who meet criteria have received pneumococcal vaccination, and less than 40% have received seasonal influenza vaccine. Comprehensive initiatives need to be implemented to increase the adult vaccination rate. Pregnancy Vaccination during pregnancy has the ability to protect not only the mother but also the newborn infant. Vaccinations for healthcare personnel: Update on influenza, hepatitis B, and pertussis. Economic evaluation of the routine childhood immunization program in the United States, 2009. Some proven concepts are providing reminders to patients that vaccines are due and implementation of standing orders for vaccines. Educate patients about the disease state, appropriate lifestyle modifications, and drug therapy required for effective treatment. If left untreated, patients experience a prolonged asymptomatic period followed by rapid, progressive immunodeficiency. Approximately 70% of these cases are in Sub-Saharan Africa, with a prevalence of approximately 5%. Central Asia, Eastern Europe, North Africa, and the Middle East are also seeing rapidly rising infection rates. After delivery, mothers are strongly recommended not to breast-feed if safe alternatives are available. These proteins assemble beneath the bilayer of the host cell, a nucleocapsid forms containing these proteins, and the virus buds from the cell. During the early stages of infection, approximately 10 billion virions can be produced each day. Most of the cells containing these viruses will be lysed as a result of budding virions, cytotoxic T-lymphocytes, or undergoing apoptosis. During this time, a high rate of viral replication can be seen in the lymph nodes. Taken together, these are the "acute retroviral syndrome," and 40% to 90% of acutely infected individuals will have symptoms. If patients are not identified during acute infection, they may later present with nonspecific symptoms such as myalgias, fatigue, weight loss, thrush, or symptoms associated with opportunistic infections. Acute Retroviral Syndrome the majority of patients may present with fever, lymphadenopathy, pharyngitis, and/or rash.
Lian Zi (Lotus). Raloxifene.
- How does Lotus work?
- Bleeding, digestion problems, diarrhea, and other conditions.
- What is Lotus?
- Are there safety concerns?
- Dosing considerations for Lotus.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96164
Purchase raloxifene 60mg overnight delivery
Indeed menopause 101 discount 60mg raloxifene otc, many authors recommend that liver transplant is contraindicated in valproate-induced hepatic failure [49,52]. Most studies suggest subclinical hypothyroidism due to carbamazepine and valproate. Multiorgan dysfunction the management of seizures in individuals with multiorgan dysfunction, often in the intensive care unit, is a complicated issue. While it is imperative to control seizures rapidly, the potential consequences of treatment of seizures on the already compromised function of various organs needs to be carefully considered. In addition, multiorgan dysfunction in the intensive care unit is often complicated by hypotension, systemic acidosis and hypoproteinaemia. Continuous electrocardiographic and haemodynamic monitoring is warranted during the administration of these agents. Intravenous valproate and levetiracetam are possibly safe in the presence of hypotension. As a result, total drug concentrations may be normal but free drug levels may be elevated, potentially leading to drug toxicity. Hence, dosage considerations are extremely complicated and should be guided by vigilant observation of the clinical response. Organ transplantation There is a high incidence of new-onset seizures in kidney, liver and cardiac transplant recipients [60]. Diagnostic evaluation of new-onset seizures often involves considerations other than the common causes of new-onset seizures in the general population. In addition, individuals with prior epilepsy may happen to be candidates for transplant procedures. Prevailing concerns in transplant recipients essentially revolve around the administration of immunosuppressive agents, including ciclosporin and tacrolimus. Toxicity due to ciclosporin can result in seizures as one of the features of the reversible posterior leucoencephalopathy syndrome. The other features of this condition include hypertension, cortical blindness and mutism. Tacrolimus might also lead to seizures, although imaging abnormalities due to tacrolimus intoxication are more often diffuse than posterior [61]. The management of seizures caused by immunosuppressive agent toxicity comprises lowering blood pressure, omitting the agent and reorienting its dosage according to serum concentrations. Many of the immunosuppressive agents used in the post-transplant period have a narrow therapeutic index and considerable inter-individual variation in their pharmacokinetics. Carbamazepine, phenytoin and oxcarbazepine reduce blood levels of ciclosporin, tacrolimus and glucocorticoids, thereby compromising their efficacy and fuelling concerns about their potential to cause transplant rejection [62,63]. Levetiracetam holds promise although there are concerns about an increased risk of infection during its use which may be relevant to the transplant population, in whom the risk of infections is already high due to Medical Comorbidity of Epilepsy 253 prolonged administration of immunosuppressive agents [64]. Cancer and epilepsy Both epilepsy and cancer are common disorders and can occur by coincidence in a proportion of the general population. Seizures and epilepsy may occur for the first time in people with cancer and their occurrence should prompt differential diagnoses that are considerably different from those for seizures and epilepsy in the general population [65]. More meaningful, however, is the alteration in cancer treatment and prognosis imposed by the concomitant occurrence of chronic epilepsy. Finally, the occurrence of cancer may modify the treatment and prognosis of epilepsy in some instances. Limited data available from specialist cancer centers suggest that seizures occur in nearly 15% of the selected population [67,68]. There appear to be some differences between adults and children with regard to the incidence and aetiology of seizures [68,69]. In children with cancer, there is a high frequency of seizures associated with the use of high-dose myelo-ablative treatment (busulfan) offered for the treatment of childhood leukaemias. In adults with solid cancers, intracranial (parenchymal or uncommonly leptomeningeal) metastasis may frequently be the cause of seizures. Anticancer drug-induced seizures and metabolic disturbances are the other common causes of seizures in individuals with cancer. Their occurrence is dose-dependent and hence in clinical oncological practice seizures are encountered because of inadvertent overdosing, the administration of high doses of anticancer agents. The treatment of seizures and epilepsy in people with cancer requires special consideration. In the treatment of acute seizures, a drug with a rapid onset of action and parenteral formulation is preferred. Brief and isolated seizures resulting from drugs or metabolic disturbances do not require treatment. Parenteral formulations are available for phenytoin, phenobarbital, valproate, levetiracetam and lacosamide. Oral benzodiazepines (lorazepam or clonazepam) are routinely administered prophylactically before and until 24 hours after high-dose busulfan, given as myeloablative treatment prior to bone marrow transplantation in view of the high incidence of seizures associated with this treatment [70]. For instance, a high incidence of anticonvulsant hypersensitivity syndrome has been reported with phenytoin use in conjunction with cranial irradiation for metastatic brain tumours [75] and after neurosurgery. Haematological toxicity due to cisplatin is enhanced when used in conjunction with valproate by compounding of the potential of both agents to cause thrombocytopenia [76]. Conventionally, surgical treatment for intractable epilepsy is often disregarded in individuals with cancer owing to their limited survival. However, with the prospects of lasting remission in several cancers, particularly childhood leukaemias, surgical treatment becomes an appealing option in the management of intractable epilepsy in individuals with cancer [78]. The risk appears higher following viral encephalitis and is perhaps the highest following herpes simplex encephalitis because of the involvement of the highly epileptogenic mesial temporal cortex. On the basis of limited data derived from highly specialized epilepsy centres, it may be inferred that both acute bacterial meningitis and viral encephalitis constitute antecedent illnesses for the development 254 Chapter 18 of intractable mesial temporal lobe epilepsy with underlying hippocampal sclerosis [84]. In addition, neocortical epilepsy occurs frequently following viral encephalitis but not after bacterial meningitis [85]. The result of these drug interactions is a reduction in plasma concentrations of the protease inhibitors, potentially leading to increased viral replication and the emergence of drug resistance [89]. An interaction between valproate and zidovudine as a result of hepatic microsomal enzyme inhibition by the former has also been reported [90]. Cysticercosis and epilepsy Infestation of the brain parenchyma by larval stage of the pork tapeworm, Taenia solium is the main cause of late-onset epilepsy in much of the developing world [93]. Population-based studies in Central and South America and South Asia have established that roughly one-third of all epilepsies may be attributable to cysticercosis [94,95]. In addition, the parasitic infestation has been documented in large numbers in sub-Saharan Africa. Seizures are the most common presenting manifestation of brain parenchymal cysticercosis [96]. Presumably, these occur as a manifestation of host brain parenchymal inflammatory response to degenerating cysticerci. Hence, most of the seizures appear to be provoked by brain inflammation and the long-term prognosis for seizure control is generally good [96,97]. However, there may be subgroups of individuals in whom seizure remission may be difficult to achieve [96]. Factors that have been identified with an increased risk of seizure relapse include persisting brain cysticercal lesions and residual calcific lesions. In addition, an association with mesial temporal sclerosis has been suggested but it remains to be seen if this association is causal [96]. Benefits of antihelminthic treatment have been demonstrated in the form of superior rates of cyst resolution as well as improved seizure control over short periods of time (usually a few months) in several small placebo-controlled trials [98,99]. Recently, combination antihelminthic treatment (albendazole and praziquantel) was shown to be superior to albendazole alone [100]. First, a slight increase in frequency of seizures may occur during the course of antihelminthic treatment owing to brain parenchymal inflammation provoked by the antihelminthic agent-induced degeneration of the cysticerci [98]. In the case of phenytoin, hypotension is frequently encountered when rates of infusion exceed 50 mg/mL or in critically ill patients. Phenytoin-induced hypotension usually responds to fluid administration and reducing the rate of infusion. Cardiac arrythmias the exact incidence of cardiac arrythmias in epilepsy is not known.
Order generic raloxifene line
For ethosuximide and lamotrigine menstruation gingivitis treatment discount raloxifene 60mg with visa, infant serum concentrations may occasionally reach levels at which pharmacological effects can be seen. Phenobarbital, and phenobarbital as a metabolite of primidone, can accumulate in the suckling infant, and sedation and poor suckling have been reported. Similarly, sedation may occur because of exposure to benzodiazepines such as diazepam, clonazepam and possibly clobazam if taken chronically by the nursing mother. These must be weighed against the possible risks to the infant induced by drug exposure. Taking this into account, women with epilepsy should, in general, be encouraged to nurse their infants, and the risk for adverse effects from drug exposure through breast milk is, in most cases, negligible. Women who nurse while taking phenobarbital, primidone, benzodiazepines and perhaps also ethosuximide and lamotrigine should be encouraged to monitor their infant for side-effects such as sedation or poor suckling, rather than being advised not to nurse. If suspicion of pharmacological effects arises, this could be confirmed or rejected by measuring serum drug levels in the infant. Folate supplementation Low folate intake has been associated with an increased risk of congenital malformations, in particular neural tube defects, in animal studies and in humans. In a randomized study of more than 7000 Hungarian women planning pregnancy, supplementation with 0. A randomized British study [76] assessed the effect of folic acid supplementation on the risk of recurrence of neural tube defects in high-risk pregnancies. Unfortunately, no randomized study has specifically assessed the effectiveness of folic acid supplementation in women with epilepsy. In the absence of data specific for women with epilepsy, recommendations have to be drawn from studies based on the general population. A higher dose of 4 mg/day is recommended for secondary prevention to women with a previous history of giving birth to a child with neural tube defects or with a family history of such malformations. Many guidelines recommend that all women under treatment with such drugs should take up to 5 mg/day folate from before conception and throughout the first trimester [78]. In the pregnancy registers, rates of malformations have not been lower among children of women who have taken folate periconceptionally [46,80]. It remains to be shown that prenatal oral vitamin K supplementation also reduces the risk of neonatal haemorrhage. Hey [81] studied prospectively cord blood prothrombin time in 137 babies born to women on phenobarbital, phenytoin or carbamazepine. Only 14 of the babies had prolonged prothrombin time and none had an overt bleeding tendency. Based on these observations, Hey concluded that evidence is lacking for a particular early form of neonatal haemorrhage related to use of anticonvulsants, and that oral vitamin K supplementation during late pregnancy is unjustified, where intramuscular injections of vitamin K to the newborn infant are routine. Preconception counselling Several surveys have revealed that women with epilepsy often receive insufficient and even inaccurate information concerning issues related to reproductive function. Clinical practical guidelines for the care of women with epilepsy of child-bearing age have been published in many countries [78,84,85,86,]. Unfortunately, many important questions are still unanswered, and many of the recommendations build on rather weak evidence, from observational studies rather than randomized trials. Nevertheless, they provide useful tools and need to be brought to the attention of health-care providers and utilized in their counselling of women with epilepsy. An optimal management of pregnancy depends largely on considerations that have to be made, and measures that have to be taken, before conception. Prepregnancy counselling is therefore essential, and it is an important challenge to change the present situation whereby such counselling seems to be offered to only a minority of women with epilepsy. The possibility that drug treatment may induce endocrine dysfunction affecting fertility should also be addressed. The importance of medication compliance during pregnancy and the risks associated with abrupt withdrawal need to be underlined. Reproductive Aspects of Epilepsy Treatment 319 In conclusion, although there are specific risks and problems associated with pregnancy in women with epilepsy, counselling should focus on the feasibility of reducing risks and on the fact that more than 90% of women with epilepsy can look forward to an uneventful pregnancy and to giving birth to a healthy child. Management during pregnancy Antiepileptic drug treatment during pregnancy the optimal management of a woman with epilepsy during pregnancy relies on a close collaboration, with exchange of information between the physician responsible for epilepsy care and the obstetrician (Table 23. There is, at present, no simple answer to what the suitable alternative could be for women with genetic (idiopathic) generalized epilepsies. Lamotrigine has a reasonable documentation concerning pregnancy outcomes, but the pronounced pharmacokinetic alterations during pregnancy can result in breakthrough seizures. Levetiracetam appears slightly less problematic in this respect, data on malformations rates are promising but limited. Measure unbound concentrations of phenytoin and valproic acid Prescribe folate from before conception During pregnancy Offer prenatal diagnosis Monitor the patient clinically and with serum drug concentrations each trimester, more frequently in patients with poor seizure control or if lamotrigine. Although such seizures are of limited importance during pregnancy, poorly controlled myoclonic seizures can be a problem after birth when the mother has a newborn infant to care for. Irrespective of which of the alternatives is considered, it is necessary to allow sufficient time before conception to assess its effectiveness. An attempt to withdraw treatment should be considered in women who plan pregnancy and who have been seizure-free for 2 years or more. However, this needs to be assessed individually based on the estimated risk of recurrence and potential consequences thereof. In the case of polytherapy, conversion to monotherapy should be considered, and an attempt to establish the lowest effective dosage should always be made. All such major changes should ideally be completed several months before conception to allow a reasonable observation period before pregnancy. It is useful to document the optimal serum drug level before pregnancy to facilitate interpretation of serum concentration measurements during pregnancy. At this stage of pregnancy the potential gain is minor compared with the risks associated with such procedures. This should include clinical evaluation and drug level monitoring where appropriate. Where phenytoin and valproic acid are used, monitoring the unbound levels is preferred. More frequent drug level monitoring may be justified with lamotrigine and possibly also oxcarbazepine and levetiracetam. If a dosage increment was made during pregnancy, serum drug levels should be monitored during the first weeks after delivery, as a dose reduction may be necessary. Vitamin supplementation Women with epilepsy considering pregnancy should be prescribed folic acid. Women need to be informed of the lack of evidence for the relative efficacy of high dose folate. However, delivery should take place in a wellequipped obstetric unit in view of the increased risk of seizures during labour and delivery and the increased risk of neonatal death. Emergency caesarean delivery is indicated during labour when seizures induce fetal asphyxia or cause poor maternal cooperation. Puerperium Stress and sleep deprivation in the puerperium may sometimes adversely affect seizure control. Furthermore, the new responsibilities of the care of the newborn child may necessitate special considerations and precautions at home. It is recommended that the mother with epilepsy is given extra support from her partner or others during the first weeks at home, in particular if she is sensitive to sleep deprivation, when seizures are likely to occur. In order to minimize risks to the infant, care for the child, including breastfeeding, is best carried out on the floor, and another person should supervise bathing of the baby.
Generic raloxifene 60mg overnight delivery
Some cancers produce substances (eg menstruation in the bible raloxifene 60 mg online, proteins) that are detected by a blood test, that may be useful in following response to therapy or detecting a recurrence; these are referred to as tumor markers. Unfortunately, some tumor markers are nonspecific and may be elevated from nonmalignant causes. When malignant cells have traveled to other parts of the body and become established there and are able to grow in this new environment, they are called metastatic cancer cells. Thus, for chemotherapy-sensitive diseases, systemic therapies may be administered after surgery to destroy these microscopic malignant cells; this is called adjuvant chemotherapy. The goals of adjuvant chemotherapy are to decrease the recurrence of the cancer and to prolong survival. Chemotherapy may also be given before surgical resection of the tumor; this is referred to as neoadjuvant chemotherapy. Chemotherapy given before surgery should decrease the tumor burden to be removed (which may result in a shorter surgical procedure or less physical disfigurement to the patient) and make the surgery easier to perform because the tumor has shrunk away from vital organs or vessels. Neoadjuvant chemotherapy also gives the clinician an idea of the responsiveness of the tumor to that particular chemotherapy. Chemotherapy may be given to cure cancers that are curable, or it may be given to help control the symptoms of an incurable cancer, which is referred to as palliative therapy. These mutations will be discussed in depth in the following cancer-specific chapters. Nonpharmacologic Therapy the four primary treatment modalities of cancer are surgery, radiation, biotherapy, and pharmacologic therapy. Surgery is useful to gain tissue for diagnosis of cancer and for treatment, especially those cancers with limited disease. Radiation plays a key role not only in the treatment and possible cure of cancer but also in palliative therapy. Together, surgery and radiation therapy may provide local control of symptoms of the disease. However, when cancer is widespread, surgery may play little or no role, but radiation therapy localized to specific areas may palliate symptoms. Pharmacologic Therapy Chemotherapy of cancer started in the early 1940s when nitrogen mustard was first administered to patients with lymphoma. Since then, numerous agents have been developed for the treatment of different cancers. A cure in oncology implies that the cancer is completely gone, and the patient will have the same life expectancy as a patient without cancer. Some cancers, such as leukemia, cannot be measured by size, so biopsy of the bone marrow provides a cellular indication of the absence or presence of disease. Cancer cells may be sensitive to certain chemotherapy agents, but then with repeated exposure, the cells may become resistant to treatment. Many chemotherapy agents have significant organ toxicities that preclude using steadily increasing doses to treat the cancer. The doses of chemotherapy must be given at a frequency that allows the patient to recover from the toxicity of the chemotherapy; each period of chemotherapy dosing is referred to as a cycle. Each cycle of chemotherapy may have the same dosages; the dosages may be modified based on toxicity; or a chemotherapy regimen may alternate from one set of drugs given during the first, third, and fifth cycles to another set of different drugs given during the second, fourth, and sixth cycles. The dose density of chemotherapy refers to shortening of the period between cycles of chemotherapy. The size of the primary tumor, extent of nodal involvement, and presence of metastases are used to determine the stage. Metastases are cancer cells that have spread to sites distant from the primary tumor site and have started to grow. The most frequently occurring sites of metastases of solid tumors are the brain, bone, liver, and lungs. The chemotherapy regimens that are dose dense tend to be adjuvant regimens, and the goal of therapy is cure. When a chemotherapy regimen is used as palliative therapy (to control symptoms), the dosages of chemotherapy may be decreased based on toxicity or the interval between cycles may be lengthened to maintain quality of life. The patient may have a blood test before irinotecan therapy to determine if this genetic mutation is present. In the case of some monoclonal antibodies, flow cytometry results reveal whether the tumor has the receptor where the drug will bind and exert the pharmacologic effect. Factors that affect chemotherapy selection and dosing are age, concurrent disease states, and performance status. Performance status is a very important prognostic factor for many types of cancer. If a patient has renal dysfunction and the chemotherapy is eliminated primarily by the kidney, dosing adjustments will need to be made. If a patient has had a myocardial infarction recently or preexisting heart disease, the clinician will weigh the risks of anthracycline therapy against the benefit of the treatment of the cancer. Another important consideration for treatment of cancers is reimbursement by third-party payers for compendia off-label use. Because of rapid advancements in oncology, it is estimated that up to 75% of chemotherapy agents are prescribed "off-label. During the time of chemotherapy administration, patients will likely experience various toxicities. Combination Chemotherapy the underlying principles of using combination therapy are to use (1) agents with different pharmacologic actions, (2) agents with different organ toxicities, (3) agents that are active against the tumor and ideally synergistic when used together, and (4) agents that do not result in significant drug interactions (although these can be studied carefully and the interactions addressed). When two or more agents are used together, the risk of development of resistance may be lessened, but toxicity may be increased. Traditional chemotherapy agents have some similar side effects, usually manifested on the most rapidly proliferating cells of the body. However, there are unique toxicities of various pharmacologic categories of antineoplastic agents. Anthracyclines (eg, doxorubicin) have the potential to cause cardiac toxicity, which is related to the cumulative dose. Inhibition of thymidylate synthesis occurs with the continuous infusion regimens, whereas the triphosphate form is associated with bolus administration. Patients with a low activity of dihydropyrimidine dehydrogenase appear to be at risk for life-threatening toxicities. Once administered, this prodrug is metabolized by dihydropyrimidine dehydrogenase. Adverse effects may include stomatitis, diarrhea, esophagitis, gastric ulcerations, cardiac abnormalities, and rarely reported cerebellar toxicities. He has been treated with two courses of antibiotics without improvement of symptoms. What signs and symptoms in this patient are consistent with a cancer presentation The toxicities include myelosuppression; flu-like syndrome with fevers during the first 24 hours after administration; rash that appears 48 to 72 hours after administration; and hemolytic uremic syndrome, a rare but life-threatening adverse effect. Patients should be counseled to use acetaminophen to treat the fevers during the first 24 hours; however, fevers occurring 7 to 10 days after gemcitabine are likely to be febrile neutropenias and need prompt treatment with broad-spectrum antibiotics. Toxicities include diarrhea, mucositis, palmar-plantar erythrodysesthesia, nausea, and myelosuppression. Patients should be counseled to notify the prescriber when this adverse effect occurs. Patients should be instructed to take capecitabine within 30 minutes of a meal to increase absorption of the drug. The drug may be administered as a low-dose continuous infusion, high-dose intermittent infusion, and into the subdural space via intrathecal or intraventricular administration. Cytarabine has shown efficacy in the treatment of acute leukemias and some lymphomas. The toxicities of cytarabine in high doses include myelosuppression; cerebellar syndrome (ie, nystagmus, dysarthria, and ataxia); and chemical conjunctivitis, an eye irritation that requires prophylaxis with steroid eye drops. The risk of neurotoxicity is increased with high doses (greater than 1 g/m2), advanced age, and renal dysfunction. If cerebellar toxicity does occur, the drug needs to be discontinued immediately, and decisions regarding further therapy need to be carefully considered. The most common adverse effects are hematologic toxicities, neutropenic fever, headaches, and gastrointestinal toxicities.
Buy raloxifene with mastercard
Other medication-related factors Mechanisms of action It may sound heretical to state that knowledge of mechanisms of drug action has modest relevance for selecting a drug in the clinic women's health diy boot camp purchase raloxifene 60 mg otc, but this is the way antiepileptic drugs are mostly prescribed at present. In fact, our understanding of the pathophysiology of the epilepsies and of the modes of action of individual drugs is still too fragmentary to allow mechanism-driven rational drug selection. Although primary modes of actions have been described for most antiepileptic drugs, additional mechanisms are often present and their relative contribution to clinical effects in a given individual is poorly understood. How each of these actions could account for therapeutic and adverse effects is unclear. While these limitations should be understood, there are situations in which knowledge of modes of action needs to be considered in choosing a medication. In a patient who has shown a paradoxical aggravation of seizures on carbamazepine, for example, it would be sensible to avoid, if possible, medications such as oxcarbazepine, eslicarbazepine acetate and phenytoin, which have modes of actions similar to carbamazepine. Likewise, as discussed in greater detail in Chapter 9, it has been suggested that in patients with refractory seizures requiring multiple drug therapy, combinations of drugs possessing different modes of action should produce better responses than combinations of drugs acting through a similar mechanism. Although clinical findings in support of this hypothesis are limited and not always consistent [60], evidence exists that combinations of drugs acting primarily by blocking sodium channels are more prone to induce central nervous system side-effects than combinations of drugs acting through other mechanisms [61]. In time, research on the relationship between specific modes of action and clinical response in well-defined epilepsy syndromes could yield important clues for rational treatment; for example, it might be possible in the future to determine which drug produces the best response in a patient whose epilepsy is caused by a specific 370 Chapter 27 Monitoring requirements Some drugs require special monitoring procedures to ensure optimal efficacy and to minimize the risk of adverse effects. For example, individualizing phenytoin dosage can be difficult without measuring its plasma concentration [65], which may argue against the preferential use of this drug in settings where a therapeutic drug monitoring service is unavailable. Likewise, therapy with felbamate requires repeated blood chemistry and haematology tests, so this drug should not be prescribed if compliance with safety monitoring tests cannot be guaranteed. Therefore, it is no surprise that, in many settings, cost is a major consideration not only in deciding which drug to use, but also in determining whether drug treatment is affordable at all. This problem is aggravated by the fact that in many low-income countries the price of antiepileptic drugs is considerably higher than in the industrialized world [66]. For most patients in developing countries, only phenobarbital is available at prices affordable by the general population [67], and many of the newer drugs may not be available at all. Cost is an important issue also for affluent societies, particularly in view of the fact that recently licensed drugs are far more expensive than older agents. In some countries, reimbursement of medication costs by health services or insurance schemes is only applicable to specific drugs (or formulations), specific indications or patients within predefined income limits. The cost of many antiepileptic medications has decreased in recent years because of the introduction of generic products. Advantages and concerns with the use of these products are discussed in Chapter 9. Ease of use Not all antiepileptic drugs are equally easy to use, a consideration that impacts on drug selection. Ease of use encompasses many properties discussed in this chapter: in particular, a broad efficacy spectrum against many seizure types, a good safety and tolerability profile, a low interaction potential, feasibility of once- or twice-daily dosing, availability of convenient formulations, and rapid and simple schemes for dose titration and individualization contribute positively to ease of use (Table 27. Broad spectrum of efficacy against all seizure types High seizure freedom rate Good tolerability No risk of allergic or idiosyncratic reactions (including teratogenicity) Low interaction potential Low variability in dosage requirements Favourable pharmacokinetics (linear kinetics, half-life compatible with once- or twice-daily dosing) Fast and easy dose escalation rate No tolerance to antiepileptic effects No withdrawal seizures No need for intensive laboratory monitoring Availability of convenient formulations (including paediatric dosage forms and a parenteral formulation) Low cost Old or new drugs When the cost of medication is not a major constraint, drug selection should be based primarily on the expected benefit to risk balance in the individual patient. When this is taken into account, the increasing use of newer drugs in the last decade may be justified by the improved tolerability profile and the lower interaction potential which characterize some of these agents. However, evidence concerning merits and demerits of individual medications should be evaluated critically. In some randomized trials that compared newer with older generation drugs, results may have been biased by specificities in the study design which discriminated against the older drugs [68]. For example, when carbamazepine was used as comparator, its target dosage was sometimes higher than necessary, and an immediate-release formulation was almost invariably used despite evidence that sustained-release preparations are associated with superior tolerability [69]. When assessing risks associated with specific medications, it should also be remembered that the latency between the introduction of a drug in the market and the discovery of potentially important adverse effects can be long. It took 10 years since marketing to identify the hepatic toxicity of valproic acid, and 8 years to discover vigabatrin-induced visual field loss [70]. Approved versus off-label use As a general rule, medications should be used according to indications approved by regulatory authorities. The approval of a specific indication is dependent on submission of adequate efficacy and safety data to regulatory agencies. Given the heterogeneity of seizure disorders, however, certain seizure types or syndromes are rarely investigated in regulatory trials. As a result, many antiepileptic drugs are not formally approved for some indications or for specific age groups, despite evidence of clinical usefulness in the same conditions from non-regulatory studies or clinical experience. The situation is further complicated by the fact that regulatory standards for approval have changed over the years, resulting in discrepancies in the quality of supportive evidence between older and newer generation drugs. Other concerns relate to the appropriateness of dose titration schemes and dosing schedules approved by regulatory authorities. These reproduce dosing procedures in regulatory trials and do not necessarily reflect optimal dosing schemes, which are mostly established during post-marketing experience [64]. In view of the above considerations, off-label prescribing is justifiable in selected situations, and in many countries there is a legal framework for this. A recent study from Italy which enrolled 1124 consecutive patients with pharmacoresistant epilepsy found that 53% of children and 31% of adults were receiving at least one off-label antiepileptic drug prescription [73]. Off-label use was especially prevalent in children and in patients with generalized epilepsy syndromes, for which few drugs are formally approved. Physicians prescribing off-label, however, should be aware of legal liability issues, and must ensure that their decisions are backed by the best medical evidence available. In Introduction to the Choice of Antiepileptic Drugs 371 some countries, the cost of drugs prescribed off-label is not reimbursed by the national health system or insurance organizations, a situation that can impact on drug selection. Importance of patient-related factors As rational prescribing requires finding the best match between the properties of a drug and the characteristics of the patient, careful assessment of individual features has a crucial role in drug selection. Some of these characteristics relate to demographics, others to psychosocial aspects, and others to the type and severity of epilepsy, associated conditions and comedications. Seizure types and epilepsy syndrome As discussed earlier in this chapter, antiepileptic drugs differ in their spectrum of efficacy against different seizure types. Therefore, correct identification of seizure type(s) and, whenever possible, epilepsy syndrome is very important for drug selection. Whenever a diagnosis of epilepsy is established but the precise type of seizures or syndrome is uncertain, the probability of achieving seizure control is enhanced by prescribing a drug with a broad efficacy spectrum. Aetiology of epilepsy Defining the aetiology of epilepsy is important to identify conditions that may require specific treatments. Information on aetiology is also important to establish the epilepsy syndrome, and to formulate a prognosis. In a hospitalbased observational survey of 2200 individuals, 1-year remission rates on drug therapy were 82% in patients with genetic (idiopathic) generalized epilepsy, 45% in those with focal epilepsy of unknown (cryptogenic) aetiology, 35% in those with structural-metabolic (symptomatic) focal epilepsy and only 11% in those with focal epilepsy associated with hippocampal sclerosis [74]. Patients with hippocampal sclerosis and another lesion had only a 3% probability of achieving seizure freedom. In the same study, patients with temporal lobe epilepsy responded more poorly to treatment than those with extratemporal foci. Information on aetiology is also important for early identification of candidates for epilepsy surgery. In most epilepsy syndromes, information about aetiology is of little value in predicting which specific treatment will produce the best clinical response. However, there are some notable exceptions, particularly for seizure disorders caused by specific metabolic defects. Likewise, patients with pyridoxine-dependent epilepsies and folinic acid-dependent seizures should be appropriately treated with pyridoxine and folinic acid, respectively [76,77]. Certain epilepsies associated with inborn errors of metabolism may also contraindicate use of specific drugs, such as valproic acid (see Chapter 51). Choice of drugs based on identification of the underlying aetiology is likely to increase in the future, as our understanding of the pathophysiology of the epilepsies and mechanisms of drug action progressively improves. Considerable efforts in current epilepsy research are being dedicated to the development of new treatments that modify the underlying disease by targeting specific causes and mechanisms. Preliminary data suggest that therapeutic response to immunotherapy in patients with epilepsies presumed to be immune-mediated vary according to the specific immunological abnormality involved [82]. Genotypes Variation in genes controlling drug-metabolizing enzymes and/or the expression of voltage-gated sodium channels has been reported to influence dosing requirements for phenytoin and carbamazepine [84,85]. Although a number of gene variants potentially responsible for influencing response to certain antiepileptic drugs have been identified [85], at present no genetic test is available to predict reliably which drug will prove the most efficacious in an individual patient. With expanding pharmacogenomic knowledge, however, this situation may well change in the future. The mechanisms responsible for many adverse drug reactions are also under genetic modulation, and genetic testing is already being used to identify subjects at risk.
Buy raloxifene visa
Summary of drug therapies most commonly used in status epilepticus Here follows a brief summary of the major characteristics and a critique of the usage of those drugs widely used in status epilepticus womens health 3 week diet order raloxifene now. For more detail see the relevant sections in this chapter and the relevant chapters on individual drugs later in this book. Diazepam Use in Acute seizures, premonitory and early stages of status epilepticus. Advantages and disadvantages There is extensive clinical experience in adults, children and the newborn; the drug has well-proven efficacy in many types of status, a rapid onset of action, and well-studied pharmacology and pharmacokinetics. It is now not given by continuous infusion, although this was a method used in the past. Diazepam has two important disadvantages, however, which limit its usefulness in status epilepticus. First, although it has a rapid onset of action, it is highly lipid-soluble and thus has a short duration of action after a single injection. This means that there is a strong tendency for seizures to relapse after initial control. Furthermore, due to its high lipid solubility, the recommended rate of injection of diazepam should not be exceeded, to avoid the risk of sudden excessive brain concentrations. Secondly, diazepam accumulates on repeated injections or after continuous infusion, and this accumulation carries a high risk of sudden respiratory depression, sedation and hypotension. Furthermore, in occasional patients, very low doses of diazepam cause severe respiratory depression. Other disadvantages are its dependency on hepatic metabolism and the formation of an active metabolite, which can complicate prolonged therapy. Diazepam has a tendency to precipitate from concentrated solutions and to interact with other drugs, and is absorbed onto plastic on prolonged contact. Usual preparation Levetiracetam is available as 5-mL vials containing 500 mg levetiracetam (100 mg/mL). The dose must be diluted in at least 100 mL of a compatible diluent and administered over at least 10 minutes as an intravenous infusion. Lorazepam Use in Acute seizures, premonitory and early stages of status epilepticus. Advantages and disadvantages A single injection is highly effective, and the drug has a longer initial duration of action and a lower risk of cardiorespiratory depression than diazepam. The main disadvantage of lorazepam is a stronger tendency for tolerance to develop, the drug being usually effective for about 12 hours only. Lorazepam is a stable compound that is not likely to precipitate in solution, and is relatively unaffected by hepatic or renal disease. Midazolam Use in Acute seizures, premonitory and early stages of status epilepticus, and also intravenously in the stage of refractory status epilepticus. Advantages and disadvantages Midazolam is a water-soluble compound, the ring structure of which closes when in contact with serum to convert it into a highly lipophilic structure. It acts within minutes and although there is a danger of accumulation on prolonged or repeated therapy, this tendency is less than with diazepam. Its side-effect profile has been extensively studied as it has been used for many years in dental anaesthesia. Occasionally, severe cardiorespiratory depression occurs after intramuscular administration although this is rare. It has a stronger anticonvulsant action than other barbiturates and an additional potential cerebral protective action. It has a rapid onset and long-lasting action, and can be administered much faster than can phenytoin. Its safety at high doses has been established, and the drug can be continued as chronic therapy. The disadvantages of the drug relate to prolonged use, where, because of the long elimination half-life, there is a risk of drug accumulation and inevitable sedation, respiratory depression and hypotension. It is also a drug not used much in long-term therapy in epilepsy, and when given in status epilepticus will need a long withdrawal period once the episode of status epilepticus is over. Usual preparation A 1-mL ampoule containing phenobarbital sodium 200 mg/mL in propylene glycol 90% and water for injection 10%. The drug has a prolonged action, with a relatively low risk of respiratory or cerebral depression and no tendency for tachyphylaxis. Its main disadvantage is the time necessary to infuse the drug and its delayed onset of action. Toxic side-effects include cardiac rhythm disturbances, and hypotension and cardiorespiratory depression. The risk of cardiac side-effects is greatly increased if the recommended rate of injection is exceeded, and cardiac monitoring is advisable during phenytoin infusion. There is a risk of precipitation if phenytoin is diluted in other solutions than 0. Usual preparations Phenytoin is usually formulated in a 5-mL ampoule containing 250 mg stabilized in propylene glycol, ethanol and water (alternatives exist. Propofol is an anaesthetic agent of choice for non-barbiturate infusional anaesthesia in status epilepticus. Advantages and disadvantages It is an excellent anaesthetic with very good pharmacokinetic properties. As with all anaesthetics, its use requires assisted ventilation, intensive care and intensive care monitoring. A particular risk is the propofol infusion syndrome, which is a term used to describe the occurrence of hyperkalaemia, lipaemia, metabolic acidosis, myocardial failure, renal failure and rhabdomyolysis. It occurs usually on longterm infusion (>48 hours) but has been reported even after only 5 hours of infusion. It is much more common in young children (and indeed for this reason the use of propofol is relatively contraindicated in children). It may be caused by drug-induced impairment of oxidation of fatty acid chains and inhibition of oxidative phosphorylation in the mitochondria, especially in the presence of high catecholamine and cortisol levels. Rebound seizures are a problem when it is discontinued too rapidly, and a decremental rate of 1 mg/kg every 2 hours is recommended when the drug is to be withdrawn. Unlike isoflurane, it is metabolized in the liver and affected by severe hepatic disease. When seizures have been controlled for 12 hours, drug dosages should be slowly tapered over 12 hours. Thiopental, or its first metabolite pentobarbital, is, in most countries, the usual choice for barbiturate anaesthesia. Both reduce intracranial pressure and cerebral blood flow, have a very rapid onset of action, and there is wide experience of its use. Both thiopental and pentobarbital have a number of pharmacokinetic disadvantages including saturable kinetics, a strong tendency to accumulate and a prolonged recovery time after anaesthesia is withdrawn. Indeed, severe sedation commonly lasts for days after drug infusion, because of their tendency to accumulate and their slow clearance. Serum concentration monitoring of thiopental and pentobarbital (both in the case of thiopental infusions) are advisable on prolonged therapy. There is often some tachyphylaxis to the sedative and, to a lesser extent, the anticonvulsant properties. Other less common side-effects include pancreatitis, hepatic dysfunction and spasm at the injection site. On prolonged use, ileus and other systemic problems can occur and, because of the immunosuppressive effects of barbiturates, intercurrent infections can be a major problem.
Syndromes
- Risky sex behaviors, unplanned or unwanted pregnancy, and sexually transmitted ilnfections (STIs)
- Genetic testing, if there is a family history of ALS
- Gastrointestinal disorders, such as duodenal atresia, esophageal atresia, gastroschisis, and diaphragmatic hernia
- You have blood in your stool
- Fatigue
- If the person has normal breathing, coughing, or movement, do NOT begin chest compressions. Doing so may cause the heart to stop beating.
- Thickened wall of the right ventricle (right ventricular hypertrophy)
- Growth
- Abnormal pupil size
Purchase cheap raloxifene line
Electroencephalographic changes induced by the intravenous administration of acetazolamide (Diamox) in epileptic patients menstruation night sweats proven raloxifene 60 mg. Effects of acetazolamide on epileptic apnea in migrating partial seizures in infancy. Catamenial exacerbation of action myoclonus: successful treatment with acetazolamide. Mechanism of tolerance to the anticonvulsant effects of acetazolamide in mice: relation to the activity and amount of carbonic anhydrase in brain. Tamm-Horsfall protein accumulation in glomeruli during acetazolamide-induced acute renal failure. The influence of supplemental sodium acetate on carbonic anhydrase inhibitor-induced side effects. Calcium metabolism in acidotic patients induced by carbonic anhydrase inhibitors: response to citrate. Effect of chronic carbonic anhydrase inhibitor therapy on bone mineral density in white women. Sacrococcygeal teratoma in a neonate: association with maternal use of acetazolamide. Possible association between acetazolamide administration during pregnancy and metabolic disorders in the newborn. May be of value in other paediatric epileptic encephalopathies Prednisone: tablets: 1, 2. After an appropriate period, dosage is down-escalated gradually Usual preparations Usual dosage Significant drug interactions Enzyme-inducing drugs increase the metabolic clearance of prednisolone (prednisolone is also an active metabolite of prednisone). Binding decreases with increasing drug concentration the effects of prednisone are mediated practically entirely through conversion to prednisolone Plasma clearance Protein binding Active metabolites - Activity resides primarily in the first 20 amino acids from the N-terminal end of the chain. The importance of this finding is noteworthy, as infantile spasms represent a severe epileptic condition which is associated with encephalopathic symptoms and an unfavourable cognitive outcome. These agents have also been applied - and continue to be applied - to the treatment of other severe forms of childhood epilepsy, even though there is a paucity of high-quality studies demonstrating their efficacy in these conditions [2]. Brain lesions associated with these conditions may be diffuse or focal, either unilateral or bilateral. In idiopathic cases, no underlying cause is identified and normal development is present prior to the onset of the epileptic encephalopathy. Its biological activity resides in the first 20 amino acids from the N-terminal end of the chain. Human, sheep, cattle and swine corticotropin have different structures, but the first 20 amino acids are the same and therefore are considered to exert identical biological effects. The corticosteroids most commonly used in epilepsy therapy are prednisone, prednisolone, hydrocortisone and methylprednisolone. In the last few years, increasing evidence has accumulated that certain forms of severe epilepsy have an inflammatory and/or immunological basis [6]. For example, it is possible that synthetic preparations are more potent in activating melanocortin receptors than natural preparations. However, the tetrodotoxin animal model [18] resembles more closely the human condition. With the commonly used sustained-release preparations, however, plasma levels are maintained for many hours after the injection in spite of the short elimination half-life. Corticosteroids Prednisone and prednisolone are probably the most commonly prescribed oral corticosteroids. Prednisone is virtually inactive and is rapidly converted in the liver, partly through a first-pass effect, to prednisolone, which is found in plasma at much higher concentrations than prednisone and is responsible for the pharmacological effects. Both prednisone and prednisolone are rapidly absorbed from the gastrointestinal tract. Partly because of concentration-dependent protein binding, the clearance of total (bound + unbound) prednisolone increases with increasing dose [25]. Prednisolone clearance is also higher in children than in adults [26] and in patients co-medicated with enzyme inducers [27]. The oral bioavailability of hydrocortisone is estimated to be close to 100% [28] and is not expected to be influenced by gender, age or liver disease [29,30]. Because of its high oral bioavailability, orally administered hydrocortisone is almost equally effective 392 Chapter 29 as an identical dose given intravenously. Certain water-soluble esters of hydrocortisone and its synthetic congeners may be administered intravenously in order to achieve rapidly high concentrations in body fluids. More prolonged plasma levels can be obtained by intramuscular injection of a suspension of hydrocortisone, its esters and congeners. Under normal circumstances, cortisol is 90% bound to plasma proteins, and elimination is predominantly metabolic. Drug interactions the metabolism of many corticosteroids, including prednisolone, methylprednisolone and hydrocortisone, is stimulated by concomitant administration of enzyme-inducing agents such as phenytoin, carbamazepine and barbiturates [27]. Serum level monitoring Although the suggestion has been made that measuring serum levels of corticosteroids may facilitate clinical management by identifying pharmacokinetic variability related to factors such as disease states and drug interactions [26], in practice the measurement of the serum concentration of these agents is not routinely carried out. Assessing these outcomes requires long-term follow-up studies which are very scarce in the literature. Most published studies focus exclusively on short-term results in control of spasms. In fact, in order to reduce adverse effects, increasingly lower doses have been used over time. The treatment of responders was tapered off over 12 days, while non-responders were crossed over to the alternative treatment. Spasms and hypsarrhythmia disappeared in all cases, but after 3 months patients in both groups showed either a relapse of spasms or the appearance of focal seizures. Successful treatment of infantile spasms with vigabatrin has also been reported in infants without tuberous sclerosis. After 2 weeks of treatment, spasm cessation was achieved in 40 of 55 (73%) patients randomized to hormonal treatment, compared with only 28 of 52 (54%) infants randomized to vigabatrin [49], even though long-term seizure outcome did not differ between the two treatments [50]. More recently, the treatment of infantile spasms in the context of West syndrome has been addressed by a Cochrane review [51] and by a consensus report [52]. The authors of the Cochrane review selected all randomized controlled trials investigating outcomes of drug therapy in patients with infantile spasms. Hormonal treatment might improve development in those infants with no proven underlying neurological disease, but the evidence is not robust. The consensus report concluded that further studies are warranted, which should include detailed clinical neurophysiological evaluation. Long-term studies Long-term effects on spasms and on developmental outcome are difficult to evaluate. Unknown aetiology (cryptogenic) cases were associated with a more favourable long-term outcome. In the case series of 64 infants with infantile spasms of unknown (cryptogenic) or structural metabolic (symptomatic) aetiology described by Glaze et al. At the final assessment, spasm-free rates were similar in the two groups, with 41 of 55 (75%) patients randomized to hormonal treatment and 39 of 51 (76%) patients randomized to vigabatrin being free from spasms [50].
Generic 60 mg raloxifene mastercard
Recommend a frequency for glaucoma screening based on patient-specific risk factors pregnancy questions hotline order discount raloxifene on line. Compare and contrast the pathophysiologic mechanisms responsible for open-angle glaucoma and acute angle-closure glaucoma. Compare and contrast the clinical presentation of chronic open-angle glaucoma and acute angleclosure glaucoma. Choose the most appropriate therapy based on patient-specific data for open-angle glaucoma, glaucoma suspect, and acute angle-closure glaucoma. Counsel patients about glaucoma, drug therapy options, ophthalmic administration techniques, and the importance of adherence to the prescribed regimen. Glaucoma Suspects are patients with a higher than average risk of developing glaucoma because of the presence of certain clinical findings, family history, or racial background. Glaucoma suspects can be further classified as open-angle glaucoma suspects or angle-closure glaucoma suspects. Examples include pigment dispersion syndrome, neovascular glaucoma, and pseudoexfoliative syndrome. Glaucoma characterized by normal anteriorchamber angles and glaucomatous changes of the optic disc. Iris Cornea Conjuctiva Pupil Lens Anterior chamber Retinal vasculature Vitreous Sclera Choroid Retina Optic nerve Retinal pigmented epithelium Data from Refs. The anterior segment of the eye is separated by the iris into the posterior and anterior chambers. It also produces aqueous humor through the diffusion and ultrafiltration of plasma. The nonpigmented epithelium of the ciliary body secretes the aqueous humor into the posterior chamber. From the anterior chamber, approximately 80% of aqueous humor then exits through the trabecular meshwork while the remaining 20% exits through the uveoscleral pathway. The size of the trabecular meshwork can be altered by the contraction or the relaxation of the ciliary muscle. Stimulation of muscarinic receptors on the ciliary muscle causes contraction, which in turn causes the pores of the trabecular meshwork to open, increasing aqueous humor outflow into Schlemm canal and the episcleral venous system. Uveoscleral outflow can be pharmacologically modulated by adrenoceptors, prostanoid receptors, and prostamide receptors. Pressure independent causes of optic neuropathy include abnormal ocular perfusion, oxidative stress, and inflammation. This stress activates the glial cells in a manner that leads to inappropriate remodeling of the extracellular matrix. Two major mechanisms of trabecular meshwork obstruction by the peripheral iris include pupillary block and an abnormality of the iris called iris plateau. Pupillary block is the more common mechanism of obstruction and results from a complete or functional apposition of the central iris to the anterior lens and is associated with mid-dilation of the pupil. The trapped aqueous humor in the posterior chamber increases pressure behind the iris, causing the peripheral iris to bow forward and obstruct the trabecular meshwork. Plateau iris refers to an anterior displacement of the peripheral iris caused by anteriorly positioned ciliary Optic Nerve In the posterior segment of the eye, retinal ganglion cells are responsible for transmitting visual signaling from the retina to the brain. The axons of the retinal ganglion cells converge at the retinal nerve fiber layer to form the optic nerve. The optic nerve head (also called the optic disc) is the portion of the optic nerve that is visible on funduscopic examination. The optic nerve head is vertically oval and pink to pale yellow with a depression in the center of the optic nerve, called a physiologic cup which is formed as the axons converge and exit the eye as a bundle through the lamina cribrosa. She states that she is concerned about losing her eyesight because her older sister has started losing her vision from glaucoma. Glaucoma risk factors are also useful in deciding when to start therapy and determining the sequence of pharmacotherapeutic or surgical treatment modalities. Recurrent attacks or a prolonged acute attack can lead to the development of peripheral anterior synechia, which partially obstructs the flow of aqueous humor through the trabecular meshwork. The ideal therapeutic regimen should have maximal effectiveness and patient tolerance to achieve the desired therapeutic response. In general, medical and laser trabeculoplasty are preferred as early treatment options over surgical as surgical interventions are not without potential intraoperative or postoperative complications. The ocular hypotensive lipids, timolol, carbonic anhydrase inhibitors, or brimonidine are reasonable choices for addition as a second agent. Benzalkonium chloride is a common eye drop preservative which has been associated with superficial punctate keratitis, corneal erosion, and conjunctival allergy. Intolerances to preservatives can be resolved by changing to a preservativefree eye drop. Surgical or laser intervention are rarely indicated in the treatment of glaucoma suspects. Laser iridotomy uses laser energy to cut a hole into the iris to alleviate the aqueous humor buildup behind the iris, resulting in reversal of appositional angle closure. Most clinicians believe laser procedures should be performed earlier (eg, after three-drug maximum, poorly adherent patient). Corneal indentation with a cotton-tipped applicator or gonioscopic lens may break pupillary block. If laser iridotomy cannot be performed, then surgical incisional iridectomy is used. Incisional iridectomy is the surgical removal of a small portion of the peripheral iris to allow flow of aqueous humor trapped in the posterior chamber to migrate to the anterior chamber (bypassing the normal flow pattern through the pupil). The fellow eye is at high risk to develop an acute attack and should receive prophylactic iridotomy within a reasonable interval of time. Lens extraction surgery may be another treatment modality as it increases the anterior chamber depth. Tachyphylaxis may occur in 20% to 50% of patients on monotherapy with a -blocker, resulting in the need for a different agent or combination therapy. This route bypasses first-pass hepatic metabolism resulting in pharmacologically significant serum drug concentrations. Pulmonary edema, status asthmaticus, and respiratory arrest have been reported with -blockers as well. Cardiovascular effects include bradycardia, hypotension, and congestive heart failure exacerbation. As with systemic -blockers, topical -blockers have also been reported to cause depression and hyperlipidemia and mask symptoms of hypoglycemia. The 1selective properties of betaxolol may cause less exacerbation of pulmonary disease. Despite the intrinsic sympathomimetic activity demonstrated by carteolol, this does not translate to a clinically significant decrease in pulmonary or cardiovascular adverse effects. Other local adverse effects include conjunctivitis, keratitis, dry eyes, and uveitis. Latanoprost and travoprost have dosing aids that help patients administer each medication. Local effects include conjunctival hyperemia, stinging on instillation, increase in iris pigmentation, deepening of the upper eyelid sulcus, hypertrichosis, and darkening of the eyelashes. Increases in iris pigmentation occur most commonly in patients with multicolored irides on long-term prostaglandin analogue therapy. The mechanism of this effect is by its action on melanocytes of the iris, in which the irides become darker because of increased production of melanin in the iris. Conjunctival hyperemia or engorgement of conjunctival blood vessels is a common adverse effect caused by a vasodilatory effect on scleral blood vessels. Although generally a benign adverse effect, patients may have a concern if it affects their cosmetic appearance. Cystoid macular edema has been reported during treatment with the ocular hypotensive lipids; therefore, use caution in patients with intraocular inflammation, aphakic patients, pseudophakic patients with a history of intraoperative complications (eg, torn posterior lens capsule), or in patients with risk factors for macular edema. Patients can develop systemic acidosis, hypokalemia, hyponatremia, and nephrolithiasis due to the inhibition of renal carbonic anhydrase. Blood dyscrasias from bone marrow suppression have been reported and include agranulocytosis, aplastic anemia, neutropenia, and thrombocytopenia.
Buy raloxifene 60 mg without prescription
Patients should also have easy access to medical care and adequate caregiver support women's health nutrition tips cheap 60 mg raloxifene with visa. However, rapid recognition of typical presenting symptoms facilitates referral for tissue diagnosis (if unknown) and treatment. This is thought to be because of its predilection for the central and perihilar areas of the lung. It is a relatively thinwalled vein that is particularly vulnerable to obstruction from adjacent tumor invasion or thrombosis. The obstruction leads to elevated venous pressure, although collateral veins partially compensate. In fact, 75% of patients have signs and symptoms for more than 1 week before seeking medical attention. Thus, therapy can typically be withheld until a definitive tissue diagnosis is established. While biopsy results are pending, supportive measures such as head elevation, diuretics, corticosteroids, and supplemental oxygen may be used. The dosage should be tapered upon completion of radiation therapy or resolution of symptoms. Although patients may derive symptomatic relief from edema, complications such as dehydration and reduced venous blood flow may exacerbate the condition. However, thrombolytics (ie, alteplase) and anticoagulation with heparin and warfarin may be beneficial in patients with thrombosis caused by indwelling catheters if used within 7 days of onset of symptoms, although catheter removal may be required. Practitioners must quickly recognize the signs and symptoms of this condition to facilitate rapid management strategies. Cancers that inherently metastasize to the bone (ie, breast, prostate, and lung) are the most frequent underlying malignancies associated with this complication. Most spinal cord compression occurs in patients with a known malignancy; however, 8% to 34% of cases occur as the initial presentation of cancer, especially in patients with non-Hodgkin lymphoma, multiple myeloma, and lung cancer. The thoracic spine is most vulnerable to cord compression because of natural kyphosis and because the width of the thoracic spinal canal is the smallest among the vertebrae. Most spinal cord compression is caused by adjacent vertebral metastases that compress the spinal cord or from pathologic compression fracture of the vertebra. As indicated earlier, chemotherapy may also be combined with radiotherapy, especially in patients with lymphoma who have bulky mediastinal lymphadenopathy. Surgery is the treatment of choice for the following patients: (a) patients with unstable spine requiring stabilization, (b) immediately impending sphincter dysfunction requiring rapid spinal decompression, (c) patients who do not respond to or have received their maximum dose of radiotherapy, and (d) direct compression of the spinal cord caused by spinal bony fragments. Overall, the risks and benefits of surgery must be weighed against the expected prognosis of the patient in light of the significant rehabilitation required after surgery. Diagnosis is made based on symptoms and imaging studies that show fractured vertebrae. The most important prognostic factor for patients presenting with spinal cord compression is the degree of underlying neurologic dysfunction. Only around 10% of patients who present with paralysis are able to ambulate after treatment. Exceptions to this include patients with prior radiation to the treatment site and patients with inherently radio-resistant tumors (ie, melanoma, renal cell carcinoma). The radiation field should include two vertebral bodies above and below the involved area. Dexamethasone has been shown to improve ambulation in combination with radiation compared with radiation alone. Oral loading doses of 10 to 100 mg followed by 4 to 24 mg orally four times daily have been used. Steroids should be continued during radiation therapy and then tapered appropriately. Pain management is also of critical importance in patients with spinal cord compression. Although dexamethasone will provide some benefit, opioid analgesics should also be used and titrated rapidly to achieve adequate pain control. Approximately 170,000 patients develop brain metastases in the United States each year. Although melanoma is the tumor type most likely to metastasize to the brain, brain metastases caused by lung and breast cancer are seen more often because they are among the most common cancers. In addition, brain metastases may be diagnosed at the same time as the primary malignancy in around 20% of cases. Rapid identification of the signs and symptoms of brain metastases is critical to improve long-term outcome and avoid mortality. The signs and symptoms of brain metastasis can be confused with common psychological distress or other neurologic problems (eg, headaches) that may go unrecognized. It is important that patients A delicate balance of normal pressure is maintained in the brain and spinal cord by brain, blood, and cerebrospinal fluid. Because the brain is contained within a confined space (skull), any foreign mass contained within that space causes adverse sequelae. This results in either destruction or displacement of normal brain tissue with associated edema. Most brain metastases occur through hematogenous spread of the primary tumor and around 80% of patients have multiple sites of metastases within the brain. The goals of treatment of brain metastases are to manage symptoms by reducing cerebral edema, treat the underlying malignancy both locally and systemically, and improve survival. General Approach to Treatment Patients with brain metastases have a poor prognosis. The primary definitive treatments for brain metastases are surgery and radiation therapy. Pharmacologic modalities are primarily used to control symptoms, although cytotoxic chemotherapy plays a limited role in the management. Most patients receive whole-brain radiation because the majority of brain metastases are multifocal. Another method known as stereotactic radiosurgery provides intense focal radiation, typically using a linear accelerator or gamma knife, in patients who cannot tolerate surgery or have lesions that are surgically inaccessible (ie, brain stem). Because brain metastases can occur in up to 50% of patients with small cell lung cancer, prophylactic cranial irradiation is recommended in patients with good performance status who at least partially respond to chemotherapy to both prevent the development of brain metastases and to prolong survival. Surgery may also benefit patients with multiple metastatic sites who have a single dominant lesion with current or impending neurologic sequelae. It should be noted that these strategies only relieve symptoms, and definitive therapy is still required. Symptom relief may occur shortly after the loading dose, although the maximum benefit may not be seen for several days (after definitive therapy). Mannitol is an osmotic diuretic that shifts brain osmolarity from the brain to the blood. Phenytoin is the most frequently used agent with a loading dose of 15 mg/kg followed by 300 mg by mouth daily (titrated to therapeutic levels between 10 and 20 mcg/mL [40 and 79 mol/L]). Prophylactic anticonvulsants have frequently been used; however, a systematic review did not support their use. Although therapy with certain medications is the most common cause, it is also the most preventable. Once it occurs, hemorrhagic cystitis causes significant morbidity and mortality rates between 2% and 4%. This section focuses on preventive strategies for chemotherapeutic causes of hemorrhagic cystitis. Hemorrhagic cystitis is the dose-limiting toxicity of ifosfamide and predisposes patients with bladder cancer.
Generic raloxifene 60mg on-line
During the fine-tuning of the diet to achieve greater efficacy menstruation gift basket discount raloxifene express, children may be given anything from a 2. Research suggests that a 4: 1 ketogenic diet may be more effective; however, a 3: 1 diet is better tolerated and is associated with fewer gastrointestinal symptoms [75]. Calories have historically been restricted to 75% of the recommended daily intake for age, but there is little research that supports the need to restrict calories or fluid to achieve seizure control with the ketogenic diet. Fluids are restricted to caffeine- and carbohydrate-free beverages at 100% of estimated daily needs. Fluids are strongly encouraged even beyond the recommendations in children with a family history of renal calculi, infants and all children during times of acute illness. Initiation of the ketogenic diet Children are traditionally fasted for 24 hours prior to the initiation of the diet, beginning after dinner on the day prior to admission. The decision to fast should be individual and also at the comfort level of the centre [20]. Blood glucose is monitored with finger dextrosticks every 6 hours, unless it falls below 40 mg/dL, after which it is checked every 2 hours. If the child has symptoms of hypoglycaemia, or the glucose level falls below 25 mg/dL, 30 mL orange juice is provided and the glucose is checked 1 hour later. Ketosis can begin during the fasting period, and the resultant nausea and vomiting can occasionally require intravenous hydration using non-dextrose-containing fluids. Anticonvulsant medications are often continued during the fasting and initiation period at their previous doses. All medications are carefully examined for carbohydrate content and formulations changed when necessary. There is no evidence that anticonvulsant serum levels are altered by ketosis [80]. A ketogenic eggnog looks and tastes like a milkshake and can be sipped, frozen as ice cream or cooked as scrambled eggs. Excess ketosis at this time, which causes nausea and vomiting, can be relieved with a small amount of orange juice. Once the child begins eating, serum glucose checks are unnecessary and are discontinued. Breakfast and lunch remain at one-third of the calculated calories as eggnog or formula on day 2, but dinner increases to two-thirds of the usual allowance (still eggnog or formula). On day 3, breakfast and lunch are also increased to two-thirds of allowance, and dinner is then given as the first full ketogenic diet meal (with actual foods provided). On hospital day 4, the child receives a full ketogenic breakfast and lunch and is discharged home. All children are sent home with prescriptions for urine ketosticks, additional calcium and a sugar-free complete vitamin and mineral supplement. This is just as important to achieving a favourable outcome as the actual logistics of the diet initiation. However, it is important to ensure close proximity of the child during the initiation period in case of difficulties. After discharge, parents are instructed to check urine ketones daily, and the diet is individually adjusted after consultation by telephone or email to maximize seizure control. In some cases, additional seizure control was potentially gained when ketosis was pushed higher, to achieve a serum ketone level above 4 mmol/L [81]. Most ketogenic diet centres do not advocate the routine measurement of serum ketones using these 294 Chapter 21 Table 21. Breakfast: eggs with bacon Egg (28 g) Cooked bacon (11 g) 36% heavy whipping cream (37 g) Butter (23 g) Apple (9 g) Snack: peanut butter ball Peanut butter (6 g) Butter (9 g) Lunch: tuna salad Tuna fish (28 g) Mayonnaise (30 g) Celery (10 g) 36% heavy whipping cream (36 g) Lettuce (15 g) Snack: keto yoghurt 36% heavy whipping cream (18 g) Sour cream (17 g) Strawberries (4 g) Artificial sweetener Dinner: cheeseburger Ground beef (22 g) American cheese (10 g) Butter (26 g) Cream (38 g) Lettuce (10 g) Green beans (11 g) Snack: keto custard 36% heavy whipping cream (25 g) Egg (9 g) Pure vanilla flavouring Handling increased seizures Parents and physicians not familiar with the ketogenic diet are often very uncomfortable handling increased seizures. Parents are instructed to maintain seizure calendars which include daily ketone levels, medication changes, illness, diet/food changes or other activities that may affect seizure control. First, try to ensure that no new medications have been added that might contain carbohydrate. If ketones are not moderate to large, the child can be fasted with clear liquids for 24 hours to improve ketosis rapidly. Carnitine is a carrier of fatty acids into the mitochondria for fatty acid oxidation and, although not necessary as a ketogenic diet supplement, serum levels often are reduced with ketogenic diet therapy [84]. Periodic oral or rectal benzodiazepines can be useful for seizure exacerbations as well. Discontinuation of the ketogenic diet meters, however, as the evidence of direct correlation of efficacy to any measure of ketosis remains controversial. Serum glucose or electrolytes are not routinely monitored after discharge, but some centres do this occasionally. Periodic laboratory measures are obtained typically every 3 months in order to monitor for side-effects (lipid profile, electrolytes, anticonvulsant levels, urine calcium/creatinine). Urine alkalinization is accomplished with the use of Cytra-K for all patients if the urine calcium to creatinine ratio is elevated above 0. Medications may be tapered and discontinued on an individual basis, as one of the most common parental reasons for starting the diet is anticonvulsant reduction. Children should be seen in clinic every 3 months for the first year, with more frequent visits for infants and medically fragile patients [20]. In children who are doing well, many parents are reluctant to discontinue a therapy that has been effective for years and risk restarting the anticonvulsants that were either ineffective in the past or caused side-effects. Cases have been reported of patients on the diet for over 20 years with good success and limited side-effects [85]. If the seizures worsen, the diet does not always have to be restarted but most families choose to do so. Several of these children had epilepsy surgery or vagus nerve stimulation implantation, yet even those who did not had a longterm seizure improvement that was better than would be expected considering their intractable epilepsy (even to the ketogenic diet). This evidence, although very limited, suggests that the ketogenic Ketogenic Diets 295 diet may be not only anticonvulsant in the acute setting, but antiepileptogenic in the long term. The timing of dietary discontinuation in the child with no perceived seizure reduction has been investigated. Nearly 90% of children who improve on the ketogenic diet do so within 1 month, and nearly all by 2 months [36]. Therefore, continuing the ketogenic diet beyond 6 months in a child with no seizure improvement would seem inappropriate. If the child is having significant difficulty with the ketogenic diet, he/she can be discontinued immediately, however, without dramatic increase in seizures in most cases [87]. As with any medical therapy for seizures, benefits need to be balanced against risks (Table 21. During the initiation of the ketogenic diet, the fast itself can cause vomiting, dehydration and food refusal. These effects are usually transitory and easily treated; however, if the child has an underlying metabolic disorder, the fast and ketogenic diet can be dangerous. All children, especially infants, need to have a thorough history, physical examination and often screening tests (lactate, pyruvate, carnitine, electrolytes, urine organic acids and serum amino acids) performed prior to initiating the diet.
