
Order dapoxetine 30mg with mastercard
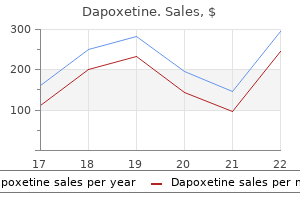
The first time I saw a surface balance was in 1950 in the laboratory of Hans Trurnit erectile dysfunction doctor mumbai discount dapoxetine 90mg overnight delivery. Hans worked in the Medical Laboratories of the Army Chemical Center in Maryland, where I was doing my national service in the Army Medical Corps. Hans burned with a gem-like flame, and nothing seemed to please him more than telling me about his work. Although my main assignment was to improve the treatment of nerve gas casualties, I enjoyed learning about surface effects and adding to what Hans told me by studying relevant textbooks. My formal education had not included any mention of surface properties, and so, without knowing it at the time, I became another in a long line of self-taught students of surface films. The Medical Laboratories had a research contract with the Harvard School of Public Health to study lung edema caused by the war gas phosgene. The work was directed by Jere Mead, a brilliant pulmonary physiologist, and the results led him to wonder what effects the surface tension of the edema fluid and its foam bubbles had on mechanical properties of the lungs. Ted wanted to estimate the area of the alveolar surface by a physicochemical method to check histologic estimates. This method gave an area only one tenth of morphometric estimates, and Ted concluded that the morphologists were wrong. I made a calculation of the diffusion capacity of the lungs using his area value, and it came out far lower than measured diffusion values. His pressure-volume data seemed solid, but his assumption of a particular surface tension bothered me. So I turned the calculation backwards and used the pressure-volume data and morphologic information to compute surface tension. Chapter79-HistoricalPerspective 797 calculation assuming a surface tension of 50 dynes/cm at maximum lung volume and a relative alveolar radius proportional to the cube root of volume gave this astonishing result: on deflation of the lung, computed surface tension fell from 50 dynes/cm to very low values, implying the presence of a unique surfactant in the alveoli. Then in 1955 Pattle reported that bubbles in pulmonary edema foam or squeezed from the cut surface of normal lungs contained "an insoluble protein layer which can abolish the tension of the alveolar surface. Clearly, the next step was to demonstrate the surface tensionarea behavior of the hypothetical surfactant directly. I knew how to do that, from discussions with Trurnit, from papers I had read, and from my previous biochemical research. I presented my results at a 1956 meeting of the American Physiological Society showing that lung extracts could lower surface tension to <10 dynes/cm when surface area was decreased and theorized that this effect could stabilize alveoli against collapse. Despite that cold reception, I was sure that the ideas and data were important and wrote a short paper for Science, which was rejected. After a few months of misery, I asked a friend to introduce it to the Proceedings of the Society for Experimental Biology and Medicine, an unreviewed journal, where it appeared in May 1957. She had gone to Harvard for a fellowship in pediatrics with Clement Smith and in lung physiology with Jere Mead, because of her strong interest in respiratory diseases in infants, especially hyaline membrane disease. I showed her my methods and told her all I knew about lung surfactant and lung physiology. The relevant literature now contains over 15,000 publications, of which more than 500 were added in the last year. Such a mountain of research cannot be properly summarized in this brief historical perspective. It had been obvious from the start that if lack or dysfunction of lung surfactant caused pulmonary failure, this might be ameliorated by replacement therapy. Attempts in the 1960s failed10,11 for various reasons: the necessary composition and physical properties of substitutes were not fully known; doses and delivery methods were inadequate; nursery personnel lacked knowledge and methods of assessing the physiologic status of newborns, especially premature infants. In 1972 Enhorning and Robertson12 showed that instilling surfactant extracted from adult rabbits into the trachea of prematurely delivered rabbit fetuses enabled good expansion of the lung. When area is decreased, both surfaces show surface tension falling to very low values. Blood plasma in the surface balance shows relatively high surface tensions and little hysteresis, unlike the lung extract. This paper stimulated many randomized controlled trials over the next 10 years of a variety of surfactant preparations derived from animal lungs. The current state of the art is well summarized in the report and recommendations of the American Academy of Pediatrics 2012-2013 Committee on the Fetus and Newborn: Surfactant Replacement Therapy for Preterm and Term Neonates with Respiratory Distress. In Insoluble monolayers at liquid-gas interfaces, New York, 1966, Interscience Publishers. Robillard E, Alarie Y, Dagenais Perusse P, et al: Microaerosol administration of synthetic beta-gamma-dipalmitoyl-L-alpha-lecithin in the respiratory distress syndrome. Enhorning G, Robertson B: Lung expansion in the premature rabbit fetus after tracheal deposition of surfactant. Fujiwara T, Maeta H, Chida S, et al: Artificial surfactant therapy in hyaline membrane disease. Whitsett In vertebrates, adaptation to a nonaqueous respiratory environment was achieved by the development of lungs, which provide an extensive surface area for gas exchange. The unique physicochemical boundary between respiratory gases and the alveolar epithelium creates a region of high surface tension, generated by the unequal distribution of molecular forces on water molecules at the air-liquid interface. Unopposed, this surface tension creates collapsing forces that cause atelectasis and respiratory failure. Pulmonary surfactant creates lipid layers separating alveolar gas from the aqueous phase, decreasing these surface forces. It is not surprising that pulmonary surfactant is found in all airbreathing vertebrates studied, including animals as phylogenetically divergent as the lungfish and humans. Synthesis and secretion of an abundance of phospholipid-rich material accompany the maturation of lung before birth. Likewise, loss of surfactant function related to acute lung injury causes postnatal respiratory failure. Hereditary disorders of surfactant homeostasis cause respiratory failure in newborn infants and children. This article considers the maturation and function of the pulmonary surfactant system that is required for adaptation to air breathing after birth. Complex paracrine signaling among diverse pulmonary cells directs stereotypic branching of conducting airways that result in acinar tubules that dilate in late gestation, forming the peripheral saccules that will create the alveolar gas-exchange region after birth. Before birth, the stromal-mesenchymal components of the lung thin and pulmonary capillaries expand, as the pulmonary circulatory system comes into close apposition to the epithelial cells lining the peripheral saccules. The signaling and transcriptional processes directing branching morphogenesis and lung maturation near the time of birth are increasingly understood. Further septation and elongation of the saccules during the alveolar stage occur after birth, resulting in the formation of the mature alveoli. Many of the nuclear transcription factors and signaling processes involved in early branching morphogenesis also play critical roles in the differentiation of the respiratory epithelium before birth. Pulmonary surfactant is composed primarily of lipids present in distinct macromolecular aggregates whose structural forms are conferred by the relative abundance of surfactantassociated proteins and phospholipids, as well as by the impact of mechanical forces on the surfactant material accompanying the compression and decompression during the respiratory cycle. Tubular myelin serves as a reservoir from which multilayered lipid films are formed that spread over the alveolar surface. The stabilization of alveolar structure during breathing-induced expansion and contraction is achieved by the formation and maintenance of a phospholipid-rich film that spreads over the thin liquid layer (the aqueous hypophase) that covers the alveolar epithelial cell surface. The unique biophysical properties of surfactant prevent alveolar collapse (atelectasis) at low lung volumes by reducing surface tension, which is generated by the aqueous hypophase, to very low levels (<2 mN/m). During alveolar expansion, surface tension increases (to a maximum of 20 to 25 mN/m), stabilizing the alveolus at higher lung volumes. Incorporation of small amounts of cholesterol and other phospholipids with the unsaturated acyl chains helps to maintain the fluidity of the surface film at body temperature. Lamellar bodies, the intracellular form of surfactant, are secreted into the alveolar lumen as concentrically arranged layers of tightly packed, phospholipid-richmembranes. Maintenance of the surface film is a highly dynamic process that requires integration of synthesis and assembly, secretion, recycling, and degradation. Thus sensing the size and composition of the alveolar surfactant is essential for normal alveolar homeostasis. Surfactant is composed primarily of phospholipid, which represents approximately 80% to 90% of its mass. Lesser amounts of glycolipids and neutral lipids are detected in approximately equal amounts.
Order dapoxetine 30 mg amex
In contrast erectile dysfunction doctor in patna dapoxetine 60 mg sale, many molecules of IgG must be bound to the surface of a target cell or bacterium in order for two of the IgG molecules to find themselves close enough together to bridge a single C1q. The other classes of Igs-IgD, IgA, and IgE-do not bind to C1q and hence do not activate the classical pathway. C1s, when activated, has proteolytic activity and can also cleave synthetic esters in vitro; hence it is often referred to as C1 esterase. Its physiologic role is to carry out limited proteolytic cleavage of the next two components in the reaction sequence: C4 and C2. Again, a small fragment is released and diffuses, and the conformation and activity of the larger fragment are changed. With C2, the larger fragment is called C2a, which also has a newly exposed proteolytic active site. Together with C4b, which can also hold onto a C3 molecule, C2a forms an enzyme that can cleave and activate C3. C3 is homologous with C4, and on cleavage its larger fragment also transiently acquires the ability to bind covalently to the Ig molecule, surface, or target on which activation is occurring. Some of the newly cleaved C3b molecules diffuse before they can bind to the surface. Many others will bind to the surface at short distances around the convertase; these may serve to opsonize (facilitate phagocytosis of) the target. Some of the C3b molecules may deposit close enough to C4b2a to join with it and provide a binding site for C5 molecules, which will be cleaved by the proteolytic active site on C2a. The larger fragment, C5b, however, undergoes a conformational change that allows it to bind to C6. Theclassical pathway is activated when C1q in the C1 complex binds to antigen-bound immunoglobulin (Ig) G or M. Phylogenetically, the alternative and lectin pathways likely originated earlier than the classical pathway. In that sense, C1q may be seen as an adaptor protein that allowed this important part of the innate immune system to be recruited to enhance the activity of antibodies produced by the adaptive or cognate immune system. The ability of the lectin and alternative pathways to activate complement in the absence of antibody may be particularly important in the neonate, in whom the adaptive immune system is immature. Similarly, early in the course of infections, before antibody production and other specific effector mechanisms of the adaptive immune system are brought to bear, the lectin and alternative pathways provide an important innate system for distinguishing the self from the nonself. Alternative pathway activation is initiated by C3b, which may be formed by one of the other pathways, by nonspecific proteolytic cleavage of C3, or after the spontaneous activation of C3 by water molecules1,3,16-18 (see later). Most investigators visualize native C3 in the circulation as a kind of coiled spring, which holds a unique structure called a thioester in an internal hydrophobic pocket. Cleavage of a short peptide (C3a) from the amino-terminal end of the chain, distant from the thioester, causes conformational changes in which the coiled spring is released, the thioester is transiently exposed, and the carbon on the glutamate can transfer one of its bonds from the sulfur of the cysteine to another acceptor. Transfer of the internal thioester is greatly accelerated by the conformational changes that follow cleavage of the protein chain. Once that occurs, the same sequence of conformational changes in the protein chains will follow, even though no cleavage fragment has been removed. Thus the thioester can be considered an internal latch, which keeps the spring coiled. Hydrolysis of the thioester by water and the subsequent conformational changes occur spontaneously at a slow continuous rate; hence there is always some basal rate of generation of C3 molecules with hydrolyzed thioester bonds. These molecules have a conformation similar to that of C3b and are thus called C3b-like C3 molecules. This allows the alternative pathway of complement to play an important role in recognition of foreign invaders as part of the innate immune system and also allows it to play a role in eliminating dead or damaged body cells. However, it also means that the system must be carefully regulated, as discussed later in the section titled "Control of Complement Activation. Cleavage of factor B by D is analogous to cleavage of C2 by C1s, but the large fragment is named Bb. The C3b or C3b-like C3 molecule that initiated the pathway also serves the same role as C4b in the classical pathway C3 convertase: holding additional molecules of C3 substrate in place, which are then cleaved by Bb. Just as in the classical pathway, some of the newly cleaved C3b molecules will deposit sufficiently close to the C3bBb enzyme to join with it as a subunit that provides a binding site for C5, which can then be cleaved by Bb. Thus the addition of this new C3b molecule changes the alternative pathway C3 convertase C3bBb into the alternative pathway C5 convertase C3bBb3b. Insertion of just one of these channels into an erythrocyte allows enough water to rush into the cell to cause explosive lysis. This ability of a heat-labile fraction of plasma proteins to lyse erythrocytes sensitized by heat-stabile antibodies was recognized more than 100 years ago and led to the elucidation of the complement reaction sequence because the liberated hemoglobin provided a convenient end point for assays. Arguably, however, complement-mediated lysis is not the most important function of the complement system in vivo because nucleated cells can internalize or shed bits of membrane bearing C5 through C9 complexes. Binding with C6 stabilizes and increases the lipophilicity of C5b, and the C5b6 complex can insert into lipid membranes at some distance from the C5 convertase or even on nearby cells. The complex of C5b67 is highly lipophilic and, if formed in the fluid phase, will rapidly insert into plasma membranes, where it will serve as a binding site for C8. Binding of C8 to C5b67 creates an active complex, which can disrupt the phospholipids of target cell membranes and can cause slow lysis of erythrocytes, even without the addition of C9. Isolated C9 can also be induced to undergo these conformational changes and polymerize in vitro under carefully defined chemical conditions. These polymers may contain up to 12 molecules of C9 linked in dimers by disulfide bonds. They appear like grommets or donuts, with a top rim 15 to 20 nm in diameter sitting above a slightly narrower cylinder 15 to 16 nm in length, which spans the plasma membrane. The deposition of large amounts of C3b can opsonize, or target, our own cells for attack by neutrophils and/or destruction by macrophages in the reticuloendothelial system, just as it can opsonize invading microorganisms. This balance depends on a set of control mechanisms no less intricate than the activation pathways discussed previously. The danger of uncontrolled alternative pathway activation is illustrated by observations in a patient with congenital homozygous deficiency of the complement regulatory protein factor H (see later). Incongruously, some of the C3b deposited on his red blood cells caused a mild but chronic hemolytic anemia. However, C3, C4, and other components are acute-phase reactants, whose synthesis by hepatocytes and other types of cells increases rapidly in response to cytokines, hormones, and other signals. The activation cascades are inherently limited by the instability of the multisubunit convertases. In these bimolecular and trimolecular complexes, the proteolytic active sites are on the C2a and Bb fragments, which are not covalently bound to the target or to the other subunits of the convertases. These proteolytically active subunits have relatively weak, noncovalent interactions with C4b and/or C3b and can easily diffuse. The mechanism by which P facilitates activation of the alternative pathway is by holding together the two subunits of the noncovalent C3bBb enzyme so that it will maintain activity. This decay may occur spontaneously, or it may be accelerated by proteins that bind to the covalently attached member of the convertase and push away the loosely held enzymatically active subunit, thereby accelerating decay of the complex. Many of these proteins share homology with each other, as expected because they all bind to C3, C4, or both, which are themselves homologous. These are further grouped into long homologous repeats, which form the binding sites for C4b and C3b. Besides the ability to bind to and push off (or block binding of) the active subunits of convertases, some of these regulatory proteins can also facilitate degradation of the C4b or C3b to which they bind. A circulating protease, called C3b/C4b inactivator (factor I), can cleave C3b and C4b into forms that will no longer bind other components of the convertases. From the viewpoint of a C3b molecule, regulation of the alternative pathway might be seen as a competition between binding of factor B, which would lead to additional activation, and factor H, which would lead to inactivation. An important determinant of the fate of any given C3b molecule is the chemical nature of the surface on which it is bound, which plays a critical role in influencing the binding of B versus H. Surfaces that are rich in sialic acid, like our own cells, favor the binding of H and thus promote the action of I. In contrast, many bacteria and cells from some other species of mammals lack sialic acid. Thus, the binding of P and H versus B serves to distinguish the self from the nonself, even in the absence of a specific antibody or T cell receptor. Antibody molecules provide good acceptor sites for C3b deposition, on which B is favored over H and the C3b is protected against inactivation. Heterozygous deficiency of this protein results in the autosomal dominant condition hereditary angioedema, which is manifest clinically in repeated episodes of swelling, including attacks of laryngeal edema that can be fatal.
Syndromes
- Pernicious anemia
- Tiredness all the time
- Do you have any other symptoms?
- The amount swallowed
- Widening or narrowing of the bronchial (air) tubes
- Low blood pressure, develops rapidly
- Head turns from side to side with sound at the level of the ear
- Are taking ACE inhibitors, angiotensin receptor blockers, spironolactone (Aldactone), amiloride (Midamor), or triamterene (Dyrenium)
- Does the hunger occur during the sleep period?
Purchase 90mg dapoxetine visa
Bosse T impotence word meaning cheap dapoxetine 60 mg online, et al: Gata4 is essential for the maintenance of jejunal-ileal identities in the adult mouse small intestine. Fritsch H, et al: Epithelial and muscular regionalization of the human developing anorectum. Gupta A, Bischoff A, Pena A, et al: the great divide: septation and malformation of the cloaca, and its implications for surgeons. Warot X, Fromental-Ramain C, Fraulob V, et al: Gene dosage-dependent effects of the Hoxa-13 and Hoxd-13 mutations on morphogenesis of the terminal parts of the digestive and urogenital tracts. Que J, et al: Multiple dose-dependent roles for Sox2 in the patterning and differentiation of anterior foregut endoderm. Motoyama J, et al: Essential function of Gli2 and Gli3 in the formation of lung, trachea and oesophagus. Li Y, Litingtung Y, Ten Dijke P, Chiang C: Aberrant Bmp signaling and notochord delamination in the pathogenesis of esophageal atresia. Spencer-Dene B, et al: Stomach development is dependent on fibroblast growth factor 10/fibroblast growth factor receptor 2b-mediated signaling. Self M, Geng X, Oliver G: Six2 activity is required for the formation of the mammalian pyloric sphincter. Mo R, et al: Anorectal malformations caused by defects in sonic hedgehog signaling. Amiel J, et al: Hirschsprung disease, associated syndromes and genetics: a review. Altschuler Multiple maturational milestones, including coordination of sucking and swallowing, effective gastric emptying, propagation of small intestinal contents, and colonic elimination, are necessary for successful enteral feeding of the infant. Smooth muscle cells generate spontaneous electric activity through a fluctuation in resting membrane potential. These periodic depolarizations are below the membrane potential necessary to initiate a contraction and are known as slow waves, electric control activity, basic electric rhythm, or pacesetter potentials. Contractions occur only when a slow wave, after neural or chemical stimulation, exceeds the excitation threshold necessary for an action potential. After depolarization of a smooth muscle cell, an increase occurs in intracellular calcium. Calcium binds to calmodulin, a regulatory protein, and permits binding of the contractile proteins actin and myosin, resulting in a contraction. The sensory fibers travel closely with parasympathetic preganglionic fibers in the vagus nerve and sympathetic postganglionic fibers in the splanchnic nerves. Their neuronal cell bodies are located in the nodose and dorsal root ganglia, respectively. InAmerican gastroenterological association undergraduate teaching project in gastroenterology and liver disease,Timonium,1988,Milner-Fenwich,p1. Most parasympathetic innervation of the gut is supplied by the vagus; the sacral nerves innervate only from the middle of the transverse colon to the rectum. Pseudorabies virus, a swine neurotropic herpesvirus that undergoes retrograde axonal transport, has been instrumental in the colocalization of neurotransmitters within the brain stem neurons involved in esophageal peristalsis. The virus replicates and subsequently undergoes retrograde transport to the synapsing afferent terminals. For example, contraction of an orad segment of bowel to a food bolus is coordinated with relaxation of a caudad segment to attain peristalsis. In addition to the large myenteric and submucosal plexuses, several smaller plexuses are shown. Although many other enteric neurotransmitters have been suggested by immunocytochemical, pharmacologic, and electrophysiologic studies, not all have met the criteria for a neurotransmitter. These criteria are (1) a pharmacologic response to exogenous application of the potential neurotransmitter, (2) a mechanism for transmitter uptake and synthesis, (3) storage in presynaptic vesicles, and (4) a physiologic action following the neurotransmitter release by nerve stimulation. The pathophysiology of antropyloric muscle hypertrophy and decreased neuronal fibers is not known. Patients with Hirschsprung disease commonly present with partial or complete obstruction during the first year of life. The cellular mechanisms for this disease are not known, but animal models such as the lethal spotted (ls/ls) mouse, in which congenital aganglionosis is an autosomal recessive trait, have suggested possible mechanisms. The aganglionosis develops as a result of failure of precursors of enteric neurons75 and enteric glia76 to colonize the bowel wall. Neurotropins77 and laminin,78 in addition to other molecules, may play a role in the control of enteric neuron migration and differentiation. Neural crest cells from the ls/ls mouse can colonize the colonic walls of normal mice but not the distal colon of ls/ls mice. In the mouse, the homeobox-containing gene, Hoxa-4, is expressed in various developing tissues, including the mesodermal layer of the gut. Exploration of the function of Hoxa-4 has used a transgenic mouse expressing multiple copies of the Hoxa-4 gene, which demonstrates congenital megacolon as its phenotype. In this transgenic mouse model, crestderived cells can enter the terminal colon, but their development is abnormal, resulting in hypoganglionosis. The ls/ls mouse has an abnormality of the extracellular matrix that prevents normal migration into the terminal bowel. Pedigree studies have demonstrated that Hirschsprung disease is a heterogenous genetic disorder with autosomal dominant, autosomal recessive, and polygenic forms, as well as a few cases that result from environmental factors. Injections into the vagal crest level resulted in labeled cells in the avian stomach and duodenum. Injections into the sacral crest resulted in labeled cells in the postumbilical bowel; however, injections into the truncal crest localized to the sympathetic ganglia and not to the bowel wall. DiI tracer experiments have also demonstrated that the murine gut is colonized by the vagal and sacral regions of the neural crest. This is illustrated by the transient expression of the catecholaminergic neuronal phenotype by crest-derived cells that colonize the rodent bowel. During their migration through the vagal nerve pathway, transiently catecholaminergic cells express tyrosine hydroxylase, aromatic L-amino acid decarboxylase, dopamine -hydroxylase, catecholamine storage, and norepinephrine transport as is seen in other sympathetic neurons. When these cells reach the bowel, they no longer express the catecholaminergic phenotype. A migrating band of contractions of maximum spiking frequency and pressures is observed throughout the fasting small intestine. The fed pattern does not occur, however, if the noncontiguous bowel is extrinsically denervated. Fats reduce spiking amplitude and intestinal transit104 to a greater extent than do carbohydrates and protein. In stage 1, a high percentage of retrograde propagation of low-amplitude spike bursts occurs, suggesting that its main motor function is to mix intestinal contents. Stage 2, the fetal pattern, exhibits occasional cyclic spike bursts superimposed on slow waves that propagate aborally or orally. The first studies in human fetuses to investigate intestinal transit used amniography. Thereafter, an increasing aboral transit and propagation rate was seen as the pregnancy progressed. Subsequent manometric studies in infants illustrated a gestationally dependent pattern of development of small-intestinal motility, with developmental stages similar to those of dogs and sheep. Tell F, Jean A: Bursting discharges evoked in vitro, by solitary tract stimulation or application of N-methyl-d-aspartate, in neurons of the rat nucleus tractus solitarii. Komuro T, Baluk P, Burnstock G: An ultrastructural study of neurons and nonneuronal cells in the myenteric plexus of the rabbit colon. Malmfors G, Sundler F: Peptidergic innervation in infantile hypertrophic pyloric stenosis. Gabella G: Ultrastructure of the nerve plexuses of the mammalian intestine: the enteric glial cells. Luzzi S, Zilletti L, Franchi-Micheli S, et al: Agonists, antagonists and modulators of excitatory amino acid receptors in the guinea pig myenteric plexus. Cosentino M, De Ponti F, Marino F, et al: N-Methyl-D-aspartate receptors modulate neurotransmitter release and peristalsis in the guinea pig isolated colon. Bueno L, Praddaude F, Ruckebusch Y: Propagation of electrical spiking activity along the small intestine: intrinsic versus extrinsic neural influences. Itoh Z, Nakaya M, Suzuki T: Neurohormonal control of gastrointestinal motor activity in conscious dogs. Bueno L, Ruckebusch Y: Perinatal development of intestinal myoelectrical activity in dogs and sheep. Tomomasa T, Itoh Z, Koizumi T, Kuroume T: Nonmigrating rhythmic activity in the stomach and duodenum of neonates.
Buy dapoxetine master card
Other investigators have also demonstrated early evidence of bronchodilator responsiveness erectile dysfunction pills cvs purchase dapoxetine in united states online. Gomez-Del Rio and colleagues91 found significant improvement in pulmonary resistance in 30 mechanically ventilated preterm infants younger than 20 days of age after isoetharine inhalation. The youngest was only 3 days of age, and gestational ages ranged from 27 to 34 weeks. Denjean and colleagues89 measured significant decreases in respiratory system resistance after salbutamol inhalation in ventilatordependent preterm infants at 13. Regardless of the mechanism, the result of increased airway smooth muscle tone is an interesting adaptive (or possibly maladaptive) response. Although a detriment to inspiratory airflow, as noted above, it holds the benefit of reducing airway compliance to limit stress-induced strain/barotrauma and the inhibition of expiratory flow by compressive forces. These investigators also used fluoroscopy to determine the amount of distending pressure required to maintain airway patency in those infants. A group of seven children of similar age with glottic or supraglottic obstruction but no evidence of lower airway disease was used as a control group. This significant difference in collapsibility was present in a short segment of airway in six children and was diffuse in the other four children. Because narrowing was not always diffuse, these authors speculated that the underlying cause of collapse must include local sites of injury as well as transmural pressure changes. Bhutani and colleagues56 described roentgenographic evidence of acquired tracheomegaly in very preterm neonates. These authors speculated that the persistent airway dimensional deformation seen in those infants resulted in increased anatomic dead space and contributed to carbon dioxide retention after extubation. The ability to evaluate small airway abnormalities with conventional bronchographic agents has been limited by poor resolution of the bronchioles at the secondary lobule level. Both pressure-volume and pressure-area relationships detected significant changes in airway wall stiffness after methacholine administration (p <. In a subsequent study, this same method was used to quantitate airway stiffness in vivo. In this regard, studies conducted using in vivo, in vitro, and muscle bath preparations have provided valuable insight into how the very premature infant may differ from the later-term and term neonate with respect to airway function. Nevertheless, little is known about how positive-pressure ventilation alters the cellular, biochemical, and molecular constituents of the components of the immature airway, and why mechanical ventilation is associated with the development of severe airway dysfunction in some premature infants but not in others. More sophisticated imaging analyses that enable visualization of airway morphology with greater sensitivity coupled with biochemical and molecular analyses assessing the effects of ventilator parameters and experimental/therapeutic interventions on morphology, architecture, and mechanics should improve current understanding of the pathogenesis of pressureor stretch-related injury, and facilitate continual advancement of neonatal and pediatric clinical respiratory management. Endoscopy of the airway was selected when infants presented with acquired lobar emphysema, persistent lobar atelectasis, or unexplained medical failure. Although both rigid and flexible fiberoptic bronchoscopic techniques are available for the study of pediatric airways, rigid bronchoscopy must be performed while the patient is under general anesthesia. Thus many cases of central airway collapse would be underdiagnosed with use of this approach. The patient breathes spontaneously but must breathe around the bronchoscope as well. Variation in expiratory effort can influence the degree of intrathoracic airway collapse. Because of these technical considerations and the lack of universally agreed-on criteria, the frequency of diagnosis of central airway collapse will vary from center to center. To circumvent these inconsistencies, some researchers have based the diagnosis on the extent of airway narrowing observed during exhalation. Other investigators have defined tracheobronchomalacia as collapse resulting in either less than 50%85,114 or less than 75%93 obstruction during spontaneous breathing, with no mention of changes in the proportion of membrane relative to cartilage. Wolinsky H: Long term effects of hypertension on the rat aorta wall and their relation to concurrent aging changes. Aizawa H, Miyazaki N, Shigematsu N, Tomooka M: A possible role of airway epithelium in modulating hyperresponsiveness. The Acute Respiratory Distress Syndrome Network: Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. Masaki T, Takano-Ohmuro H, Suzuki R, et al: Changes in the smooth muscle myosin isoforms during development of chicken gizzard. Uhlig S, Uhlig U: Pharmacological interventions in ventilator-induced lung injury. Arad I, Bar-Yishay E, Eyal F, et al: Lung function in infancy and childhood following neonatal intensive care. Denjean A, Guimaraes H, Migdal M, et al: Dose-related bronchodilator response to aerosolized salbutamol (albuterol) in ventilator-dependent premature infants. Prakash 67 Significant progress has been made in elucidating development of lower airway structures and regulation of their function. During early development, airway smooth muscle differentiates from the mesenchyme of the primordial lung and envelops the emerging bronchial tree. Airway smooth muscle at this early stage provides phasic rhythmic contractility that is thought to propel lung fluid distally and enhance lung development. Neural structures emerge in parallel to airway muscle, and their functional roles are rapidly integrated such that during postnatal life tonic, rather than phasic, contractile and relaxant functions dominate. Although it is well accepted that the potential effect of the lower airway on prenatal and postnatal lung function is considerable, our understanding of the link between neurotransmitterspecific networks involved in the regulation of airway function is incomplete. This subject has gained considerable interest because of the injurious effects of increased inspired oxygen and positive pressure ventilation on neonatal airway function. It is therefore important to gain greater understanding of the normal maturational changes exhibited by airway smooth muscle contractile and relaxant mechanisms superimposed on the immature structural elements that compose the airways. Varicose fibers from these postganglionic neurons are randomly distributed around airway smooth muscle cells, submucosal glands, and arterial blood vessels. In the postnatal period, neuronal innervation is already well developed, and choline acetyltransferase, a specific marker for cholinergic traits that synthesizes acetylcholine, appears in vagal preganglionic neurons, postganglionic neurons, and postganglionic fibers. Signals transmitted through preganglionic nerves are relayed, filtered, integrated, and modulated by intrinsic ganglionic neurons before reaching their airway neuroeffector sites through postganglionic axons. This structural organization could explain the strong effects of a relatively small number of vagal efferent fibers on coordinated reflex changes in airway smooth muscle tone, submucosal gland secretion, and blood flow along the tracheobronchial tree. Each ganglion, located near its effector system, possesses a relatively large number of neurons that can be considered as an expanded parasympathetic, preganglionic efferent motor system. Muscarinic receptors mediate the responsiveness of airway smooth muscle to acetylcholine during early development and adult life. Studies in the developing airways and porcine lung from birth to adulthood reveal maturational changes in muscarinic receptor subtypes (M1, M2, M3) that may explain pharmacologic changes during development. M1 receptors are largely present on neuronal tissue and ganglia, and the selective M1 receptor antagonist pirenzepine reduces the contractile response to vagal stimulation in newborn animals. Selective blockade, or down-regulation, of M2 receptors may enhance vagally mediated bronchoconstrictor responses and cause a reduction in the bradycardia response. M2 autoinhibitory actions may be reduced or absent in the newborn, because blockade of M2 receptors does not enhance bronchoconstrictor responses to vagal stimulation. M3 receptors are present on smooth muscle and mucus glands and airway epithelial cells, where they initiate the events leading to smooth muscle contraction, airway narrowing, and mucus secretion. In the newborn, the density of M3 receptors has been reported to be similar to that in the adult; however, they do not appear to be tightly coupled to G-protein signal transduction mechanisms that lead to smooth muscle contraction. They originate from the bipolar airway vagal afferent neurons that are located in the nodose and jugular ganglia and participate in reflex events. Sensory fibers affect function of lower airway effector units via a local network that includes axon reflex responses. Nevertheless, circulating catecholamines activate airway adrenoreceptors to exert specific actions that affect smooth muscle contractile function. Activation of -adrenergic receptors is the pharmacologic basis for neonatal bronchodilator therapy. Maturational studies have demonstrated that -adrenergic receptors in lung tissue increase with advancing gestation and subsequent postnatal development, but this may be more important for their role in surfactant synthesis and release. The airway relaxant response to -adrenoreceptor stimulation actually appears to decrease with advancing maturation, and several mechanisms, including greater muscarinic antagonism of -receptor responses and attenuated expression of M2 muscarinic receptors, have been proposed. Data indicate that in adult humans -adrenergic contractile responses of airway smooth muscle are weak or absent, although this may not hold true for the newborn. Furthermore, adrenergic agonists having mixed -receptor and -receptor actions cause airway smooth muscle contraction in newborn puppies, and both 1adrenoreceptors and 2-adrenoreceptors appear to be involved in mediating the response. Under these conditions, stimulation of vagal preganglionic axons causes bronchodilation.
Discount 90mg dapoxetine fast delivery
Results comparing data obtained by the single-injection technique with those obtained by the standard inulin clearance method are conflicting erectile dysfunction doctors in ct order genuine dapoxetine line. The overestimation in the younger neonates was ascribed to incomplete equilibration of inulin in its diffusion space during the 130 minutes of the test. The validity of creatinine clearance has been assessed in low-birth-weight infants (mean birth weight, 1600 g; range, 1040 to 2275 g; postnatal age, 10 hours to 10 days). These factors fall into two major categories: (1) those related to the transport of creatinine by the premature kidney and (2) those affecting the accuracy of plasma creatinine assays (noted earlier). Because of the low-normal levels of creatinine in the blood of neonates, small variations in laboratory measurements may spuriously alter the estimated concentration. Creatinine values obtained by the standard (Jaffe) method greatly overestimate the true creatinine concentration at values lower than 1. This formula is based on the assumption that creatinine excretion is proportional to body height and is inversely proportional to plasma creatinine concentration. The mean value of k, calculated in 118 low-birth-weight infants with a corrected age of 25 to 105 weeks, was 0. In both groups, a large scatter of values for k was observed, which the authors ascribed to the variability in body composition, differences in diet and creatinine excretion, errors in collection of urine, and inaccuracies in the measurement of creatinine. In spite of these limitations, the formula was claimed to be useful, because it correlated well with the values obtained with the inulin single-injection technique. Moreover, the regression line relating the clearance estimated from the formula with the results obtained from the standard inulin clearance method differed significantly from the identity line. Calibration of assays of serum cystatin C, as well as of creatinine, will require standardization before the routine use of these formulae. Its production rate is apparently constant and was initially claimed to be independent of inflammatory conditions, muscle mass, and sex. This claim has been questioned by a large study in 8058 adult inhabitants of Groningen. It thus appears that, in adults at least, cystatin C levels are influenced by factors other than renal function alone. Cystatin C does not appear to cross the placental barrier, and no correlation exists between maternal and neonatal serum cystatin C levels. It is uncertain whether cystatin C concentration is significantly higher in premature infants as compared with term infants. A similar pattern of maturation was observed in 66 physiologically stable term and premature infants undergoing creatinine clearance studies. This was true both for absolute values of creatinine clearance and for values expressed in relation to the body surface 250 200 150 120 100 50 0 area. The progressive increase in creatinine clearance observed in the first 15 days of life also correlated significantly with postnatal age. In a large, more recent study, Vieux and colleagues69 described results for the urinary clearance of creatinine in 275 premature neonates (27 to 31 weeks of gestation) on days 7, 14, 21, and 28. In rats, both afferent and efferent arteriolar resistances decrease by a factor of 3 during maturation. The striking increase in systemic blood pressure occurring during the first weeks of life (Table 103-2) is associated with an increase in the glomerular capillary hydrostatic pressure. Creatinine clearances measured on the first 2 days of life in neonates of 28 to 43 gestational weeks have been shown to correlate significantly with blood pressure. The low oncotic pressure present in newborn infants resulting from low plasma protein concentrations favors the ultrafiltration pressure. Furthermore, because the glomerular hydrostatic pressure increases more rapidly than the oncotic Inulin clearance (mL/min per 1. Because of the low systemic blood pressure, the glomerular capillary hydraulic pressure is extremely low in early life and increases in parallel with the rise in blood pressure. The glomerular transcapillary hydraulic pressure difference increases by 10 mm Hg from the third week of life to adulthood in rats. Clearance studies in human infants into whom inulin or polyfructosides with variable molecular masses were infused have clearly shown that the high-molecular-mass inulin did not accumulate in preterm infants (birth weight of 850 to 1250 g) into whom inulin was infused for 2 to 10 days. This does not, however, exclude subtle changes in glomerular capillary permeability during growth. Experimental studies on isolated rat glomeruli also failed to demonstrate an increase in glomerular hydraulic permeability during growth. In immature animals, various conditions such as hypoxemia, hypercapnia, metabolic acidosis and alkalosis, hypothermia, and hyperthermia can dramatically increase renal vascular resistance. In all these situations, the interaction between vasoconstricting and vasodilating forces is rather complex and their effects on the systemic and the intrarenal circulations can differ. The renal vasoconstriction is the consequence of increased activation of the renin-angiotensin system, changes in intrarenal adenosine levels, and increased levels of vasopressin, catecholamines, or other vasoconstrictor substances. The hypothesis that adenosine plays a key role in the pathogenesis of the hypoxemic vasomotor nephropathy is supported by the fact that theophylline, an antagonist of adenosine cell surface receptors, protects the immature kidney from the deleterious hypoxemic stress. In the neonatal rabbit model, the specific adenosine A1 receptor antagonist 8-cyclopentyl-1,3-dipropylxanthine does not offer the same protection as theophylline. Ventilation of human neonates and newborn animals with high airway pressures has deleterious effects on renal function, resulting from decreased venous return and low cardiac output, increased renal sympathetic nervous activity, and high serum vasopressin levels. Tryggvason K, Patrakka J, Wartiovaara J: Hereditary proteinuria syndromes and mechanisms of proteinuria. Angiotensin-converting enzyme inhibitors can lead to a dramatic fall in mean arterial pressure, accompanied by persistent oliguria. Angiotensin-converting enzyme inhibitors interfere with the renin-angiotensin system, which is physiologically active during fetal and neonatal life. Serum prostaglandin levels are also high in infants with chronic cardiac failure, patent ductus arteriosus, hypotension, or hypovolemia. The deleterious effect is usually transient and results in water retention and hyponatemia. Zhao W, Biran V, Jacqz-Aigrain E: Amikacin maturation model as a marker of renal maturation to predict glomerular filtration rate and vancomycin clearance in neonates. Koren G, James A, Perlman M: A simple method for the estimation of glomerular filtration rate by gentamicin pharmacokinetics during routine drug monitoring in the newborn. Cataldi L, Mussap M, Bertelli L, et al: Cystatin C in healthy women at term pregnancy and in their infant newborns: relationship between maternal and neonatal serum levels and reference values. Harmoinen A, Ylinen E, Ala-Houhala M, et al: Reference intervals for cystatin C in pre- and full-term infants and children. Treiber M, Pecovnik Balon B, Gorenjak M: Cystatin C versus creatinine as a marker of glomerular filtration rate in the newborn. Vieux R, Hascoet J-M, Merdariu D, et al: Glomerular filtration rate in very preterm infants. Sonntag J, Prankel B, Waltz S: Serum creatinine concentration, urinary creatinine excretion and creatinine clearance during the first 9 weeks in preterm infants with a birth weight below 1500 g. Marsh D, Frasier C: Reliability of inulin for determining volume flow in rat renal cortical tubules. Forestier F, Daffos F, Rainaut M, et al: Blood chemistry of normal human fetuses at mid-trimester of pregnancy. Gallini F, Maggio L, Romagnoli C, et al: Progression of renal function in preterm neonates with gestational age 32 weeks. Cattarelli D, Spandrio M, Gasparoni A, et al: A randomised, double blind, placebo controlled trial of the effect of theophylline in prevention of vasomotor nephropathy in very preterm neonates with respiratory distress syndrome. Soloveychik V, Bin-Nun A, Lonchev A, et al: Acute hemodynamic effects of caffeine administration in premature infants. Tulassay T, Machay T, Kiszel J, Varga J: Effects of continuous airway pressure on renal function in prematures. Allegaert K, Vanhole C, de Hoon J, et al: Nonselective cyclo-oxygenase inhibitors and glomerular filtration rate in preterm neonates. Vieux R, Desandes R, Boubred F, et al: Ibuprofen in very preterm infants impairs renal function for the first month of life. This steady state is achieved by the remarkable capacity of the kidney to maintain sodium balance between what is absorbed in the intestine and what is excreted in the urine.
Cheap dapoxetine line
They repeat at regular intervals of 1 to 10 seconds erectile dysfunction after radiation treatment for rectal cancer buy dapoxetine on line amex, in the same location and with constant morphology, without evolution. With respect to physiologic delta waves and delta brushes, they lack smoothness and have wider basis and increased peak-to-peak amplitude than physiologic ones. In these newborns, they tend to persist until term-equivalent age even if with decreasing incidence, possibly representing a sign of maturational delay. Similarly, although the reappearance of a sleep-wake cycle is a marker of good prognosis if taking place within 36 hours, in the hypothermic group this was found to be true up to 60 hours after birth, even if with a wide range. Starting with a first recording in the immediate postnatal period, it is possible to establish the timing of an injury (prenatal, perinatal, or postnatal),134 depending on the presence and timing of appearance of acute- versus chronic-stage abnormalities, even if repetitive insults can also occur. Both the severity of acute-stage abnormalities and the type and severity of chronic-stage abnormalities134 can assist prognostication. The best prognostic value has been demonstrated for background abnormalities, similarly to what is already known in term newborns. Tracings with increased discontinuity and decreased amplitude, associated with unfavorable prognosis,66,110 show the best diagnostic and prognostic value if performed soon after birth, especially in the first 2 days of life, whereas afterwards they show a low sensitivity. In this respect, the finding of a suppressive effect of preterm birth on neurogenesis might represent a relevant field for further research. Positive rolandic sharp waves are generally considered as an example of chronic-stage abnormality, although some authors have also interpreted them as acute/subacute signs. They correlate with periventricular leukomalacia when appearing with a high density (especially >1/minute over the temporal and occipital region), and their topography correlates with the extent of underlying white matter damage and the severity of subsequent motor impairment. They are considered definitely abnormal when they are frequent (density cut-off values have been proposed),118 high amplitude, and/or persistent on serial recordings. It has been usually defined as either continuous seizures lasting for more than 30 minutes or seizure present for at least 50% of the recording time, with no return to the baseline neurologic condition. The recognition of epileptic syndromes allows an accurate diagnosis, management, and prognosis and provides useful information for research for discovery of new treatments and etiologies, including the genetic ones. This pattern is typically unreactive and unaltered by exogenous or endogenous stimuli. Steriade and colleagues showed that suppression epochs are due to absence of synaptic activity among cortical neurons. The remaining 30% to 40% of thalamic cells discharged rhythmic (1 to 4 Hz) spike bursts during periods of cortical silence. The neurologic status is always abnormal at onset:182 neonates are hypotonic and poorly responsive. They are often restricted in a finger, a toe, the eyebrows, eyelids, or lips, occurring in the same muscle group and often migrating elsewhere. Massive, usually bisynchronous, axial myoclonic jerks may start from the onset of the disease or occur later, often interspersed with erratic myoclonias. Simple focal seizures are usually subtle with eye deviation or autonomic symptoms such as flushing of the face or apnea, but they can be focal clonic involving any part of the body. Epileptic spasms are rare and generally appear late in the course of the disease, usually at around 3 to 4 months of age. A metabolic etiology is highest on the differential, including glycine encephalopathy, propionic academia, D-glyceric acidemia, and methylmalonic aciduria. The distinctive seizure type in this condition consists of tonic spasms, isolated or in cluster, symmetric or asymmetric. Bursts of 1 to 3 seconds comprise 150- to 350-microvolt high-voltage slow waves intermixed with multifocal spikes. Typically, seizures occur on day 2 or 3 of life, with the majority in the first week of life. Seizures are brief (1 to 2 minutes in duration) but can occur up to 30 times per day, sometimes evolving into status epilepticus. Within the last 2 years, a number of studies with several dozen patients have been reported. Most affected infants start to have seizures in the first few weeks of life, and all start having seizures by 6 months of age. The location of the ictal onset varies not only from side to side but also within a hemisphere. The clinical semiology of seizures begins with focal motor movements that can alternate from one side of the body to another with lateral deviation of the head and eyes, eye jerks, twitching of the eyelids, limb myoclonic jerks, and increased tone of one or both limbs. The focal motor component is often accompanied by autonomic signs, including flushing of the face, salivation, and apnea. Prolonged observation soon shows that both sides are alternatively affected, which demonstrates the involvement of the whole brain cortex. A three-stage electroclinical course was described by Bahi-Buisson and colleagues. Some of these children may reach seizure control after several weeks to months, with some even achieving a "honeymoon period" of seizure freedom. Regardless of ultimate epilepsy course, all patients at this stage already exhibit hypotonia and poor eye contact. Finally, in the third stage, at approximately 2 to 3 years of age, children suffer from severe refractory epilepsy with multiple seizure types, including tonic, myoclonic, and spasms. A distinctive seizure type seen during the course of this epileptic encephalopathy is the hypermotor-tonic-spasms sequence. The gene discovery efforts of the past decade for severe epilepsies, particularly early onset epileptic encephalopathies, have shown that genetic mutations play a major role, and they must be considered in the differential diagnosis of seizures in newborns and infants. Additionally, mutations in the same gene can be associated with both benign and severe epilepsies. In conclusion, the definition of the electroclinical phenotype remains an important piece for a correct diagnosis, management, and prognosis. In the context of early diagnosis and targeted treatment, an accurate characterization of the neonatal phenotype is key to determine the best strategy to manage and treat neonatal-onset epilepsies, especially if the goal is not only seizure control but also a normal developmental outcome. We believe that similar care should be applied in neonates with seizures because a number of them may benefit from an epileptologic approach. Staudt and colleagues203 argued that infants with phenobarbital plasma levels above 6 mg/dL show significant background suppression. Other authors also reported the appearance of isoelectric204 or invariant discontinuous recording205 after treatment with phenobarbital. However, he developed some cerebral activity when the phenobarbital level fell to zero. Benda and colleagues by studying 46 preterm infants found that a mean serum level of phenobarbital of 34. Pisani F, Cerminara C, Fusco C, Sisti L: Neonatal status epilepticus vs recurrent neonatal seizures: clinical findings and outcome. Dreyfus-Brisac C, Minkowski A: Electroencephalographic maturation and too low birth weight. Okumura A, Hayakawa F, Kato T, et al: Ictal electroencephalographic findings of neonatal seizures in preterm infants. Pisani F, Piccolo B, Cantalupo G, et al: Neonatal seizures and postneonatal epilepsy: a 7-y follow-up study. Dulac O: Epileptic encephalopathy with suppression-bursts and nonketotic hyperglycinemia. Watanabe K, Iwase K, Hara K: Development of slow-wave sleep in lowbirthweight infants. Curzi-Dascalova L, Peirano P, Morel-Kahn F: Development of sleep states in normal premature and full-term newborns. Karch D, Rothe R, Jurisch R, et al: Behavioural changes and bioelectric brain maturation of preterm and fullterm newborn infants: a polygraphic study. Kostovi I, Judas M: the development of the subplate and thalamocortical connections in the human foetal brain. Kato T, Tsuji T, Hayakawa F, et al: A new electroencephalogram classification with reduced recording time in asphyxiated term infants.
Indigo (Isatis). Dapoxetine.
- Dosing considerations for Isatis.
- Prostate cancer, upper respiratory infections, inflammation in the brain, hepatitis, lung abscess, psoriasis, diarrhea, and HIV.
- Are there safety concerns?
- How does Isatis work?
- What is Isatis?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96877
Buy 90 mg dapoxetine fast delivery
Studies of the intercellular distribution of hemoglobin F erectile dysfunction medications generic trusted 60 mg dapoxetine, using the relatively insensitive acid-elution technique, have shown that during the first few months of life the distribution of hemoglobin F is quite heterogeneous. At 3 months the distribution of hemoglobin F becomes bimodal, with populations of cells that contain acid-resistant hemoglobin F and populations of adult "ghost" cells. These observations have suggested that fetal hemoglobin-containing cells are replaced by a population of cells containing adult hemoglobin during the early postnatal period. Profound changes occur in the rates of red blood cell production immediately before birth and during the first few months after birth. On a body-weight basis, red blood cell production during the latter months of gestation is significantly greater compared with that in adult life. Immediately after birth, erythropoiesis is considerably reduced, presumably as an adaptation to the extrauterine environment, and red blood cell production occurs at a low level for the first few weeks of life. It is clear from globin-chain synthetic studies that there is a steady and linear decline in -chain synthesis during the period of reduced neonatal erythropoiesis. Newly synthesized red blood cells appearing in the circulation when erythropoiesis resumes contain predominantly adult hemoglobin. These findings, together with the results of analyses of the intercellular distribution of fetal and adult hemoglobin by sensitive immunologic methods, suggest, although they do not prove, that the transition from fetal to adult hemoglobin production occurs in the same erythrocyte population. This conclusion is also consistent with the patterns of fetal and chain production in red blood cell colonies grown from neonatal blood. Although glucose is the preferred carbohydrate, the red blood cell metabolizes fructose or mannose almost as readily. Intracellular glucose concentrations equilibrate immediately with changes in plasma glucose concentrations. Metabolism by way of the pentose phosphate pathway produces reduced intermediates and a phosphorylated pentose sugar (ribulose 5-phosphate). Finally, glucose 6-phosphate may be converted to glucose 1-phosphate and then to glycogen, although less than 1% of glucose is metabolized to glycogen within the red blood cell. These cells consume greater quantities of glucose than do the red blood cells of adults. The glycolytic enzymes phosphoglycerate kinase and enolase are much more active in the cells of the fetus and newborn infant than would be anticipated from their young cell age. The decreased phosphofructokinase activity of fetal cells may be a consequence of accelerated decay of an unstable enzyme. The relative deficiency of this enzyme appears to result in alterations in glucose metabolism, and it could be functionally significant. Several of the other enzymes of the Embden-Meyerhof pathway have shown differences in the staining intensity of certain isoenzyme zones as compared with adult controls, although the significance of this observation is not known. Not all these synthesizing functions are important in the mature red blood cell, which lacks a nucleus. The pentose pathway requires nicotinamide adenine dinucleotide phosphate as a cofactor. This step is followed by enzymatic hydrolysis of 6-phosphogluconolactone to 6-phosphogluconate, which is then oxidized (in the presence of 6-phosphogluconic dehydrogenase) to ribulose 5-phosphate, with the production of carbon dioxide. Approximately 3% to 10% of all glucose metabolized by the cell is cycled through the pentose phosphate pathway. Hypoxia and acidosis increase the proportion of glucose metabolism shunted through this pathway. Reduced glutathione ultimately serves as a substrate for the enzyme glutathione peroxidase, which is responsible for the detoxification of hydrogen peroxide. Hydrogen peroxide is a byproduct of the conversion of oxyhemoglobin to methemoglobin, which is a naturally occurring reaction inside the red blood cell in the presence of oxidative stress. The pentose phosphate pathway in the newborn red blood cell differs from that in the adult red blood cell. Two enzymes of the pentose pathway, glucose 6-phosphate dehydrogenase and 6-phosphogluconic acid dehydrogenase, are active at levels higher than those seen in adult red blood cells. Although there are suggestions that the pentose phosphate pathway activity in the newborn is normal, there is also evidence that newborn infants are more susceptible to oxidantinduced injury, leading to glutathione instability, Heinz body formation, and the development of methemoglobinemia. For example, the red blood cell membrane in the fetus and newborn may have a decreased number of membrane sulfhydryl groups, making these cells more susceptible than mature red blood cells to Heinz body formation. In addition, the newborn red blood cell may have a diminished capacity for handling other activated oxygen radicals, such as singlet oxygen and the superoxide radical. Diminished activity of superoxide dismutase Chapter116-DevelopmentalErythropoiesis 1125 could result in accumulation of superoxide radicals. Free radicals are generally detoxified by antioxidants such as -tocopherol (vitamin E). However, if superoxide dismutase levels are increased (as has been described in some infants), the hydrogen peroxide presented to reduced glutathione may not be adequately detoxified. The use of inhaled nitric oxide as treatment for pulmonary hypertension in sick neonates may affect this balance, and further studies are required to determine its impact on oxidant injury beyond an increase in methemoglobin formation. During the first year of life red blood cells continue to diminish in size, and at 1 year of life they resemble adult red blood cells (Table 116-5). The half-saturation pressure (P50) of fetal blood is 19 to 21 mm Hg, some 6 to 8 mm Hg lower than that of adult blood. Irregularly shaped cells are present in much greater numbers in the peripheral blood of newborn infants than in that of adults. For example, a greater percentage of neonatal red blood cells have membrane surface pits, which are most likely the sites of formation of endocytic vacuoles. Red blood cell deformability is principally governed by three factors: the surface area to volume relationship of the red blood cell, the viscosity of the cytoplasm of the cell, and intrinsic red blood cell membrane rigidity. First, red blood cell deformability appears to be an important determinant of red blood cell life span in vivo. The removal of a red blood cell from the circulation is thought to be a consequence of declining deformability, making the red blood cell susceptible to sequestration in the spleen and other organs, where it must negotiate extraordinarily narrow passages. Second, red blood cell deformability directly influences blood flow in the peripheral circulation. Third, red blood cell deformability affects whole blood viscosity, which, in turn, affects peripheral vascular resistance and cardiac workload. This suggests an accelerated decrease in deformability of aging red blood cells related to a more pronounced increase in the mean corpuscular hemoglobin concentration, the principal determinant of the internal viscosity of the red blood cell. Neonatal red blood cell membranes deform more readily to a given shear force than do adult red blood cell membranes, resulting in greater susceptibility of neonatal cell membranes to yield and fragment. Specific characteristics of fetal red blood cells include a shortened life span, macrocytosis, high fetal hemoglobin content with a G/A ratio of 3: 1, the presence of i antigen,156 and low carbonic anhydrase enzyme activity. The average life span for a neonatal red blood cell is 60 to 90 days,158 approximately half to two thirds that of an adult red blood cell. When neonatal red blood cells are transfused into adults, they exhibit a shortened life span, owing to alterations intrinsic to the neonatal red blood cell. Fetal studies using [14C]cyanate-labeled red blood cells in sheep revealed an average red blood cell life span of 63. The negative charge at the red blood cell surface is largely responsible for the electrophoretic mobility of the cell, and it appears to reflect the sialic acid content of the red blood cell membrane. For example, the neonatal red blood cell binds more insulin than the adult red blood cell because of the presence of greater numbers of insulin receptors per cell. This may explain the greater tolerance of newborns who are receiving maintenance digoxin therapy. Another unique characteristic of the fetal red blood cell is the manifestation of the i antigen on the cell surface (adult red blood cells express I antigen). Membrane i antigen is a carbohydrate moiety located on protein membrane band 3, which, during development, is converted from a linear polylactosamine to a branched carbohydrate chain of N-acetyllactosamine units. It has been suggested that the switch from fetal to adult hemoglobin and the transformation of i antigen expression that occur during the first year of life are governed by a common control mechanism; therefore, the presence of i antigen can serve as a marker of fetal hematopoiesis. Other antigens, such as the Lutheran and Xg systems, develop more slowly but are present at birth. There is no known advantage to the increased osmotic resistance seen in the neonatal red blood cell.

Dapoxetine 90 mg sale
Beutler E erectile dysfunction medication nhs purchase dapoxetine 90mg otc, Gelbart T: Estimating the prevalence of pyruvate kinase deficiency from the gene frequency in the general white population. Bianchi P, Zanella A: Hematologically important mutations: red cell pyruvate kinase (third update). Iolascon A, Miraglia del Giudice E, Perrotta S, et al: Hereditary spherocytosis: from clinical to molecular defects. Maruo Y, Nishizawa K, Sato H, et al: Prolonged unconjugated hyperbilirubinemia associated with breast milk and mutations of the bilirubin uridine diphosphate- glucuronosyltransferase gene. Lamola the pathways by which light reduces levels of circulating bilirubin and how this mechanism leads to the reduction of possible toxic byproducts has been the subject of intense inquiry and debate since the 1960s. Over the intervening years, the mechanism of action of phototherapy has been extensively studied, and sufficient evidence is available to guide its use in term and late-preterm neonates. Prescription of phototherapy for neonatal hyperbilirubinemia is relatively simple and efficacious if properly applied. Furthermore, a much better definition of the phototherapy "action spectrum" has emerged, taking into account improvements in light sources, variables affecting efficacy (such as dosimetry and hematocrit levels), and potential undesirable effects (such as heating by absorption of light wavelengths that are relatively useless therapeutically). In this articler, we review the issues related to bilirubin photochemistry, photobiology, and photomedicine to delineate our understanding of how phototherapy light (photons) should be viewed as a drug that interacts with bilirubin molecules (Table 98-1). A review of selected terms related to photobiology products can be found in Box 98-1. In the spirit of primum non nocere, there is an obligation for clinicians to optimize therapy through translation of this science to clinical practice to deliver the safest and most effective care. They provided the "evidence for the reduction of circulating bilirubin levels in some cases of neonatal jaundice by exposing these infants to sunlight. Eight 24-inch 40-watt blue fluorescent tubes (General Electric Corporation) at 2-inch separation were arranged around the curve of the reflector. Although the Lancet recognized this as a contribution of importance to merit publication, it received only limited attention both in Europe and North America. The breakthrough scientific concepts, novel prototype device, and change in clinical practice, however, subsequently made their way to Italy, Brazil, and other Latin American nations. Almost all of the bilirubin in blood is reversibly bound to its transport protein, albumin, in a form that can be distributed to a variety of tissues. The normal lipid- to watersoluble conversion of unconjugated bilirubin is mediated through a process of conjugation occurring in the liver. Phototherapy-induced conversion of bilirubin to more water-soluble and colorless products bypasses this hepatobiliary excretion process. Precise assessment of neurotoxicity must address multiple domains of sensory processing. Table 98-2 lists current and prospective biomarkers for identifying infants most at risk for neurotoxicity. The perception of light as a continuous energy stream obscures the reality that it comprises discrete packets (quanta) of energy called photons. All photochemical reactions require, in ordinary circumstances, the absorption of single photons by individual molecules. The absorption spectrum is a plot of the probability of light absorption as a function of the wavelength of the light. The spectrum in this illustration is actually that of bilirubin bound to albumin, which is the form of virtually all the bilirubin in blood. Therefore the wavelength (color) of light (drug) designed to interact with the molecular target (bilirubin) can be predicted by determining its absorption by the molecular target. Additional specificity of the wavelength range may be dictated by the avoidance of untoward side effects. However, nucleic acids and proteins without prosthetic groups do not absorb blue light; therefore it is possible to have blue light absorbed by bilirubin without affecting proteins and nucleic acids. The number of therapeutic photons absorbed by the molecular target is analogous to the dose of a drug. The intensity or irradiance (photons per unit time) of the light is analogous to the drug dose rate. One way absorbed light generally differs from molecular drugs is in the deposition of heat. When a photon is absorbed by a molecule of bilirubin, the energy of the photon is transferred to the molecule and transformed into heat that is quickly transferred to the surrounding environment. For a sufficiently dilute solution of a photochemically reactive material, the action spectrum generally is identical to the absorption spectrum. This follows the basic law of photochemistry that states that light must be absorbed for a photochemical reaction to occur. In complex environments, such as in vivo, other materials present in tissues may compete for the light, acting as filters to block some wavelengths. Hemoglobin in the skin of adults and newborns is the main absorber of visible light, especially blue light, and is, in fact, an effective filter. Recently, Lamola and colleagues proposed a semi-empirical model for the calculation of the action spectrum for bilirubin photochemistry in vivo using available data on skin optics. In the model, key factors include: the diffuse nature of light entering the skin, the wavelength dependence of back scatter of light from the skin, the absorbance due to melanin in the epidermis, the wavelength dependence of bilirubin photochemistry, the oxygenation level of the blood, the hemoglobin and bilirubin levels, and both the vascular and extravascular bilirubin. The calculations based on the model showed that the effect of competitive absorption of light by hemoglobin remains the predominant factor controlling the light that is absorbed by the bilirubin. The result is that the probability of light-driven alteration of bilirubin in the skin of neonates as a function of wavelength. The relative magnitudes of the two spectra represent that for total serum/plasma bilirubin at 15mg/dL and blood Hb at 16. A corollary of the predominance of light absorption by hemoglobin in the range of light used in phototherapy is a predicted dependence of phototherapy efficacy upon the hemoglobin level of the infant; the higher the hemoglobin concentration, the lower the expected efficacy. Almost from the beginning of the development of phototherapy, it was recognized that blue light should be effective because the visible absorption spectrum of bilirubin, presumed to reflect the action spectrum, is mainly in the blue region. Therefore if the irradiance of a 460-nm light source was increased by 15%, it should equalize the rate of bilirubin photo-alteration by a 476-nm light source. The risk-benefit ratio of that approach versus using longer-wavelength light (476 nm) would need to be ascertained to inform clinical decisions. The use of a source that is the most effective at providing wavelengths of light that are maximally absorbed by bilirubin while reducing therapeutically useless and possibly harmful light absorption by other entities, a priori, should underscore clinical practice. This spectrum has very good overlap with the bilirubin-albumin absorption spectrum. Also shown is the emission spectrum of a turquoise colored fluorescent lamp (Osram Turquoise), which has less overlap with the bilirubin-albumin spectrum. The effect of the deposition of the absorbed light energy has not been clinically determined. However, this energy load has to be dissipated and could be potentially deleterious for a sick preterm infant. The irradiance at the distance from the light source to the skin surface should be measured with an appropriate spectroradiometer. If desired, the dose measured in joules can be converted to photons, remembering that the conversion factor depends on the wavelength such that for the same energy there are more photons at higher wavelengths. Although this may be of interest to researchers, in clinical practice commercial radiometers measure the average irradiance over a wavelength range determined by the bandwidth filters in the device. Unfortunately, the various available radiometers have different wavelength ranges and can give different readings for the same light source. This has not generally been done in practice, so although intrastudy comparisons of efficacy can be made, comparisons of observations from one study to another may not be reliable. The phototherapy-mediated excretion rate depends on the therapy light intensity or irradiance at the exposed skin, the area of skin irradiated, the spectrum of the light, the action spectrum, the quantum efficiency of conversion of bilirubin to photoproducts, and the excretion rates of the photoproducts. It is also important to remember that radiometers from different suppliers can have different ranges of sensitivity that are specific to their device. This brief description does not begin to honor the painstaking work required to uncover the complicated chemistry by many experts. Interested readers are directed to the recent, well-detailed historical and technical treatise by D.
Buy cheap dapoxetine 30mg
The characteristic yellow color of bile is due to the presence of bilirubin erectile dysfunction treatment alprostadil order 30 mg dapoxetine with visa, which is secreted mainly in its diglucuronide form. Because bile is a primary mechanism for excretion of many toxic substances, varying concentrations of drugs, vitamins, steroids, xenobiotics, endobiotics, proteins, and products of lipid metabolism are also present. Bile is also the primary route for excretion of metals such as iron, copper, manganese, and zinc. Retention of these substances during periods of cholestasis, from any mechanism, serves to promulgate ongoing liver damage. Moreover, impairments in the handling of potentially toxic substances due to inherited mutations in genes involved in these pathways can contribute to liver disease, as evidenced in adult-onset hemochromatosis (iron) and Wilson disease (copper), but impairments in metal-handling processes are not clinically relevant in infants and young children. Water flows from the sinusoids to the bile canaliculi mainly via the paracellular pathway via tight junctions, with limited contribution from transcellular and transcytotic routes. In addition to bile acid pool size and efficiency of enterohepatic circulation, the choleretic potency of different bile acids modulates this process. The bile acid pool size can be manipulated pharmacologically to produce increased bile flow via administration of certain bile acids. Therefore the creation, maintenance, and regulation of bile formation rests mainly on the functional competency of membrane transporters, with central reliance on the transport of bile acids. This process is extremely efficient, with 75% to 90% first-pass clearance of bile acids from the sinusoidal blood. These studies highlight the coordinated response designed to help shield the hepatocyte from bile acid damage. They participate in the bidirectional transport of solutes across membranes as diverse as the liver, kidney, intestine, choroid plexus, and retina. How bile acids traverse the cytosol is unknown but likely involves at least one member of the fatty-acid-binding protein family. Because efflux of bile acids is the driving force for bile flow, their intracellular retention leads to the consequences of cholestasis and liver injury. They serve to export cholesterol and phytosterols across both of these membranes, thereby excluding them from the circulation. Mutations in either of these half-transporters result in defective biliary sterol transport, leading to the human disease sitosterolemia. There is a single cilium on each cholangiocyte, which participates in signaling and responses to flow. As this mixture passes down the length of the intestinal lumen, various receptors and transporters on the apical surface of enterocytes may absorb or respond to select molecules. The principal site of intestinal absorption of conjugated bile acids resides within the distal part of the small intestine-the final sections of the ileum just proximal to the ileocecal valve. This leads to increased concentrations of mono- and dihydroxylated bile acids (litho- and deoxycholates, respectively) that affect gut motility and colonocyte transformation. These bile acids are modestly absorbed in the colon and, after transport to the liver, are reconjugated to participate in the enterohepatic recirculation of bile acids. Individual microbiome communities among various individuals may lead to vastly distinct alternative bile acid species including iso-bile acids. Little is known of such alternative bile acid species in the normal or ill newborn infant. The intracellular accumulation of retained biliary constituents, especially hydrophobic bile acids, can be toxic to the liver and other tissues even at submicellar concentrations. Exposure to micromolar concentrations of bile acids causes disruption of the lipid bilayer of cell membranes in a detergent-like manner, leading to dissociation of many membrane proteins. These accumulated bile acids can also increase calcium fluxes across membranes, leading to altered mitochondrial function, cell toxicity, and apoptosis. In addition, bile acids are potent modulators of cell-signaling processes in the liver, including those linked to growth and the development of hepatocellular carcinoma. Determining whether the process is acquired or congenital is the next issue and is where much of the difficulty lies in evaluating the infant with persistent elevation of conjugated bilirubin levels. In general, all forms of cholestasis lead to elevated conjugated (direct) bilirubin levels of greater than 1 mg/dL and thus warrant consideration of underlying liver disease. However, sepsis, parenteral nutrition, and certain drugs and infections can lead to liver injury and elevated conjugated bilirubin levels, which can improve with time. Clinically, patients with cholestasis appear jaundiced (although it is often difficult to tell in a newborn) and often have dark urine and pale stools. With severe liver disease or long-standing cholestasis, the results of hepatocyte damage are seen as impairments in hepatocellular synthetic dysfunction reflected in hypoalbuminemia, hypoglycemia, coagulopathy, hyperammonemia, impaired drug metabolism, and elevated levels of conjugated bilirubin and serum bile acids. When there is a defect in bile acid synthesis, precursor molecules accumulate and can be readily measured with specific urinary metabolite analyses. To date, there are no effective therapies for this disorder (although some variants may respond to chaperones177), leaving liver transplant as the only curative option. It is postulated to be an aminophospholipid transporter (flippase) responsible for maintaining the asymmetrical distribution of phosphatidylserine, phosphatidylethanolamine, and cholesterol on the inner leaflet of the canalicular membrane, thus protecting it from the detergent effects of high bile salt concentrations in the canalicular lumen. Elevated maternal bile acid levels lead to reversal of this gradient, leading to elevated levels in both the mother and the fetus. The fetus, however, suffers more serious consequences, including increased risk for preterm delivery, fetal distress, and fetal loss. The enhanced susceptibility of infants to the cholestatic effects of certain drugs may be related to immature protective measures against apoptosis and necrosis, an enhanced inflammatory response to damaged tissues, and decreased developmental expression of detoxification and transport genes. Cholestasis is the common endpoint of many toxin-related injuries but may evolve from a variety of mechanisms, including direct toxicity and necrosis of hepatocytes and cholangiocytes, impaired bile acid transport, and alterations in the viscosity of bile. For example, cephalosporins are highly concentrated in bile, which is one of the routes of elimination. This can result in increased viscosity of biliary fluid, leading to the formation of sludge or stones and ultimately obstructive cholestasis. Research demonstrated that administration of an intravenous solution composed of concentrated glucose solutions containing amino acids, micronutrients, vitamins, and minerals could support both growth and weight gain in children and adults. The clinical presentation is characterized by jaundice, conjugated hyperbilirubinemia, and hepatomegaly. With progression of this process, hepatocellular dysfunction is evidenced by elevated transaminases, portal hypertension followed by the development of hypoalbuminemia, elevated clotting times, hypoglycemia, and hyperammonemia with end-stage liver failure. In earlier stages, this process is generally reversible if enteral nutrition can be achieved. In contrast to older children and adults, up to 65% of the most severely affected infants will progress rapidly (over 4 to 6 months) from the onset of cholestasis to end-stage liver disease, highlighting the unique and serious risk to the neonate. Phytosterols cannot be fully metabolized by the body and are usually excluded from the body by intestinal sterol exporters, leaving less than 1% to 5% of dietary phytosterols being absorbed. A small percentage of this phytosterol and cholesterol pool is converted to bile acids, while the remainder is eliminated via specific canalicular sterol transporters and secreted into the bile. Sir William Osler was among the first to make the connection between nonhepatic infections and cholestasis and coined the phrase toxemic jaundice. The mechanism appears to involve the release of inflammatory cytokines from Kupffer cells in response to endotoxin, which in turn act on receptors on the sinusoidal membranes of the hepatocyte. During sepsis, the liver also plays an important role in the acute-phase response, which functions to prioritize the functions of the liver and restore homeostasis to the body. Those cytokines, however, also suppress the function and expression of critical hepatobiliary transporters. Longer-term exposure to endotoxin and inflammatory cytokines results in activation of the mitogen-activated protein kinase family, which leads to marked alteration in the expression of a wide array of hepatic transporters, prolonging cholestasis. It is likely that the enhanced susceptibility to inflammationassociated cholestasis in infants is related to hepatic immaturity, which is even more apparent in those born prematurely. Treatment for this form of cholestasis involves proper attention to sepsis and gut integrity. After the use of parenteral nutrition, sepsis, including catheterrelated sepsis, is the second most important risk factor for cholestasis. Discharge on home parenteral nutrition utilizing fish oil is generally not feasible as this product is still only available through studies or compassionate use. Table 95-3 Characteristics and Composition of Structurally Different Parenteral Lipid Emulsions Emulsion % Fat (g/100 mL) (Manufacturer) Intralipid20%(FreseniusKabi,Bad Homburg,Germany) Lipofundin20%(B.
Discount dapoxetine 60 mg amex
A relatively greater medullary flow in neonatal kidneys may delay establishing the corticomedullary gradient erectile dysfunction doctor in delhi order 90mg dapoxetine. As the animal matures, secondary fornices and outpouchings of the renal pelvis come to extend well towards the renal cortex so that urine in the pelvis will bathe a greater part of the papilla. Ruminants have particularly well-developed renal pelvic fornices in their outer medulla. Therefore the outer medulla may play an important role in the reabsorption and recycling of urea in these animals. In summary, the low urinary concentrating capacity of newborn mammals is related to a variety of anatomic and functional factors. The loops of Henle are relatively short, the transport properties of the thick ascending limb of Henle are immature, and the number of loops of Henle from more superficial nephrons that penetrate deeper into the cortex and outer medulla is low. Renal blood flow to deeper juxtamedullary nephrons is proportionally greater in the newborn than in the adult. Enhanced prostaglandin production has the potential to reduce salt, water, and urea transport at critical sites and to increase medullary blood flow. These factors may all contribute to the smaller medullary gradient and the lower medullary urea content found in the newborn. This latter anatomic difference may contribute to a low concentrating ability during maturation because urine bathing the papillae may enhance urine and papillary osmolality. Aquaporin-1 may also limit neonatal concentrating ability because the amount of this protein is decreased in the human kidney at birth and increases gradually to approach adult levels at a time when the young kidney concentrates urine nearly as well as the adult. Less likely to play a role is aquaporin-2 because this protein is not only present in utero at 20 weeks of gestation but also must be functional as evidenced by the response of the isolated human fetal medullary collecting tubule of similar gestational age to vasopressin. In so doing, they were forced to develop mechanisms that could separate water from solute to preserve needed solute, eliminate imbibed excess water, and avoid fatal dilution of body fluids. It was considerably later in evolution when creatures had to develop a renal concentrating system to retain water as they traveled from one water environment to another. In terms of absolute volume, this capacity is considerably more limited in the infant, although the young subject can excrete 15%, and perhaps more, of the filtered load. Our ability to dilute urine and remove excess water is more efficient than our ability to concentrate urine and retain needed water. For example, suppose a 70-kg subject has a serum osmolality of 300 mOsm/kg H2O and a daily renal solute excretory load of 600 mOsm. If urine osmolality is 300 mOsm/kg H2O and the 600 mOsm solute load is excreted in 2 L of water, the subject is in water balance because urine is otonic to plasma and the kidney has neither to concentrate nor to dilute urine to maintain a normal serum sodium level. If the subject is water deprived, urine osmolality can increase to a maximum of approximately 1200 mOsm/kg H2O. At this urine concentration, 500 mL of water is needed to excrete the 600-mOsm solute load. Stated another way, of the 2 L of water/day needed to excrete this solute isotonically, a maximum of approximately 1500 mL of water/day can be retained to maintain normal serum osmolality; however, 600 mOsm cannot be concentrated in a volume of less than 500 mL. If the subject is water loaded, excess water can be excreted by reducing urine osmolality to a minimum of approximately 50 mOsm/kg H2O. In this case, the kidney can excrete the 600 mOsm of solute in a urine volume of 12 L and remove 10 L of "pure" water in the process to maintain a normal serum sodium level. In this example, renal diluting capacity (10 L water) is nearly seven-fold the concentrating capacity (1. This translates to a 24-fold increase in urine osmolality and urine volume when the urine changes from maximally dilute (osmolality, 50 mOsm/kg H2O; volume, 12,000 mL) to maximally concentrated (osmolality, 1200 mOsm/kg H2O; volume, 500 mL). Renal excretory solute loads in children usually range from 10 to 40 mOsm/100 calories expended. Urine volume required to excrete this solute varies with diet and availability of water. Extra water is eliminated by insensible losses and urine output, the latter allowing removal of the renal excretory solute load. Solute reabsorption continues in the thick ascending limb, distal nephron, collecting tubule, and collecting duct. As a consequence, fluid traversing the distal nephron and entering the medulla becomes progressively dilute. Because water remains in the tubule lumen, urea concentration is reduced, and a major urea concentration difference between collecting duct fluid and interstitium will fail to develop. The overall effect is that urea tends to be eliminated from, rather than recycled in, the medullary system. Interstitial as well as urinary urea concentrations decrease; whereas total urea excretion actually increases (but in a larger volume of water). Reduced tubule permeability to water and continued reabsorption of solute in more distal parts of the nephron might be expected to increase interstitial solute concentrations. However, interstitial solute concentrations are actually reduced compared with the antidiuretic state. As a result, reabsorption of water in medullary collecting ducts is actually greater, not less, during water diuresis. Perhaps as much as half the water delivered to collecting ducts back-diffuses into the interstitium, but NaCl is sufficiently reabsorbed along this segment so that the urine actually becomes more dilute. Full retrograde pelvic reflux is not typical of the antidiuretic state, but exposure of medullary structures to urine occurs much more often with the high flow rates associated with dilute urine. Investigators have noted a lack of clear correlation between concentrating ability and size and complexity of pelvic extensions, but a correlation exists between the size of pelvic extensions and the need to excrete a water load. Animals living in arid areas, with little water at their disposal, exhibit a high urinary concentrating ability, but have difficulty excreting a water load rapidly enough to avoid water intoxication and possible death. Animals that tolerate dehydration but periodically need water must be able to eliminate water reasonably rapidly and tend to have large pelvic extensions. Experimental evidence shows that during antidiuresis, water exchanges across the pelvic epithelium and hypotonic fluid can 1500 mOsm/kg H2O or mM 1000 500 osm P <0. Refluxes were then mechanically induced for 20 minutes in experimental kidney (green bar). Fluid along the proximal tubule is reabsorbed isotonically and does not directly add to urinary dilution. However, the amount of fluid reabsorbed at this site determines, to a major extent, the volume of dilute urine that can later be formed. A drop in filtration rate or an increase in proximal tubular reabsorption allows less fluid to arrive at the diluting site and therefore will limit the actual amount of water excretion. Some segment must be capable of reabsorbing solute in excess of water to allow luminal fluid to become dilute. This process occurs along the entire length of the ascending limb of Henle, especially along its thick portion. Any problem in solute reabsorption along this site will effectively prevent excretion of dilute urine. After urine passes into the distal nephron, in which solute reabsorption continues, water must remain largely in the lumen. Vasopressin determines the degree to which water will be reabsorbed because the water permeability of collecting duct epithelium depends on the presence of this hormone. It becomes apparent, then, that to dilute urine, three fundamental conditions must be met. First, a sufficient amount of filtrate must escape reabsorption along the proximal tubule and reach the diluting segment (ascending loop of Henle) to deliver a sufficient amount of potential pure water. Second, this segment must be able to reclaim NaCl and separate reabsorbed solute from water so that urine becomes dilute (water stays in the lumen for excretion). Accordingly, urinary dilution results from the active reabsorption of NaCl along the thick ascending limb of Henle and the continued reabsorption of solute along more distal nephron segments in concert with a disproportionate reduction in reabsorption of water. In this study, fractional delivery of sodium to the distal nephron was high, indicating decreased proximal tubular salt reabsorption. However, reabsorption of salt along diluting segments of the distal nephron increased, indicating that enhanced distal reabsorption compensated for decreased proximal reabsorption. In general, the youngest infants tended to have high rates of delivery of sodium to the distal nephron, but they also had high rates of distal tubular sodium reabsorption. The primary limitation in neonatal water excretion, therefore, falls largely on the low rates of filtration.
