
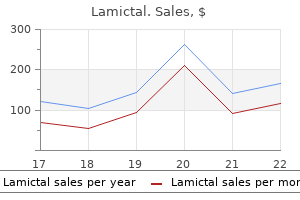
Order lamictal 25mg without a prescription
Liquefying posterior subcapsular cataract consisting mostly of globular and granular debris medicine guide order lamictal australia. Abnormal basement membrane material accumulates over the anterior surface of the lens and in other tissues of the body. The condition tends to occur in families with some concordance among identical twins. All races are affected with higher prevalence rates found in Scandinavian, Saudi Arabian, Navajo, and Australian aborigines. Erosions occur in its midzone, leaving a central disk of mild opacification and peeling edges. White dandruff-like material is also seen on the central disk, zonular fibers, anterior hyaloid membrane, pupillary and anterior iris, trabeculum, cornea (infrequently), and the ciliary processes. Subluxation of the lens may occur spontaneously in up to 5% of the patients affected. Iridodonesis, which is usually a subtle sign of subluxation, may be absent because the iris is relatively immobile as a result of deposits of pseudoexfoliative material in its stroma and muscle or because of posterior synechiae to the midzone of the lens. Zonular weakness is reflected in a higher frequency of surgical zonular dehiscences and lens subluxation, with a fivefold higher frequency of vitreous loss during extracapsular cataract extraction. The variation in fiber size and periodicity suggests abnormal fibril aggregation and cross-linking. By light microscopy, there is a splitting of the outer layers of the lens capsule. Morphologically, the lens epithelial cells undergo metaplasia to myofibroblastic cells, forming a plaque under the anterior lens capsule. Large, white, anterior subcapsular cataract after severe contusive trauma with chronic uveitis. Basement membrane (bm) produced by these fibroblast-like cells is primarily on the outer capsular side of the cell. Profuse intracellular actin and intermediate filaments (asterisk) are oriented along the opposite side of the cell. The lens capsule has some elasticity and usually flaps outward, perhaps from zonular traction, thereby preventing closure of the rupture. If the capsular penetration is small and quickly sealed by a capsular flap, fibrin, or overlying iris, a localized nonprogressive opacity may result. Mature anterior subcapsular plaque, almost completely collagenized, with a new layer of cuboidal lens epithelial cells (arrows) separating the plaque from the cataractous lens cortex in a 49-year-old diabetic patient with a chronic corneal ulcer. The capsule has flapped back on itself (arrows), and the extruded cortex shows advanced globular degeneration. This 18 month old child fell on one of his toys, but the lens capsule was not perforated. Yellowish Soemmerring ring of remaining cataractous equatorial lens material after surgery for a traumatic cataract at age 15 years. Soemmerring ring cataract after a perforating corneal wound paracentrally (arrowhead), associated with a complete perforation of the lens. Partial petaliform contusion cataract has a feathery exaggeration of the sutural pattern, after edema and permanent injury to the sutural ends of the lens fibers. Slit-beam localization shows that the injury occurred during early formation of the adult nucleus. Injury by electric shock from high-power lines, especially when they directly contact the head region, can also produce anterior subcapsular cataracts with a stellate suture-like pattern, and a central fibrous plaque after an initial diffuse vacuolar pattern. In adults, slowly growing tumors of the ciliary body or iris, whether benign or malignant, may present with focal cataracts, progressing to diffuse involvement. Following extracapsular cataract surgery, variable amounts of lens cortical tissue may remain in the equatorial region, the area of the lens that is least surgically accessible. It is estimated that up to 50% of patients will have visually significant opacification of the posterior capsule 3 to 5 years after surgery and that children and young adults are even more susceptible to this proliferative process. The minimal cataractogenic dose has been considered to be ~500 cGy but under some circumstances may be as low as 200 cGy. Most ultraviolet light is absorbed by the cornea, but it is generally accepted that ultraviolet A and B light can be cataractogenic from the usual daily doses, when combined with aging and dietary or other deficiencies of antioxidants. Lasers can cause cataracts when they are focused on the lens or from inadvertent heat transfer through the iris. The original proposed mechanism was that the sugar alcohol sorbitol, an end-product of glucose reduction by aldose reductase, accumulated to exert an osmotic effect in the lens cells. More recent research is focusing on the stress that hyperglycemia places on antioxidant pathways in the lens. The glycosylation of proteins, especially the crystallins, can cause oxidation of sulfhydryl groups, with abnormal cross-linking and aggregation of proteins. There are no histologic features that distinguish diabetes-associated cataracts with age-related cataracts. There is a genetic abnormality on chromosome 9 affecting galactose 1-phosphate uridyltransferase that normally clears galactose. Bilateral cataracts and early retardation may not be recognized until 1 to 2 months of age. Contraction of the collagen has thrown the posterior capsule into deep wrinkles (arrow). Pathology of the Lens the psychotrophic drug phenothiazide (chlorpromazine) produces a type of anterior polar stellate cataract, with deposition of a melanin-like pigment in the anterior subcapsular lens, although the exact location of deposition has not been established. Phenothiazide is also associated with skin, corneal, and conjunctival pigmentation. Typically, iron deposition is related to the presence of an ironcontaining intraocular foreign body or long-standing vitreous hemorrhage. Inflammation may occur in the setting of trauma, infection, systemic disease, or from those elusive remaining causes for idiopathic uveitis. The primary inflammation may be physically distant in the cornea (anterior subcapsular cataracts) or the retina (posterior subcapsular cataract) but the lens remains vulnerable. It is likely that many factors are related to cataract development including the influence of inflammatory cytokines on cell permeability, antioxidant level, and adhesion to surrounding structures (synechiae). However, in the setting of extensive traumatic disruption of the nuclear fibers begin to swell; the central lens is sometimes surrounded by zonular opacities. The lens opacities are potentially reversible with appropriate dietary restriction. Intracellular edema and mitochondrial swelling have been observed in affected lenses. Posterior subcapsular cataracts may be a toxic effect of topical, oral, and perhaps inhaled corticosteroids. Intravitreally injected drugs, such as antibiotics that have retinal toxicity, are usually cataractogenic as well. Another intravitreal therapeutic chemical, perfluoropropane gas (C3F8), induced cataracts in 67% of phakic eyes when the gas was used in the repair of complex retinal detachments. Some granular material is just visible within the lens capsule and angle of the anterior chamber. It has been reported in ~25% of eyes removed for sympathetic uveitis, with histopathologic confirmation in either the exciting or the sympathizing eye, or both. Experimental evidence strongly supports the possibility of a mixed immunologic response to lens antigens in this process. Secondary vitreous, also formed from peripheral neuroectodermal cells, comes in contact with and attaches to the posterior lens capsule particularly in the posterior equatorial region (ligamentum capsulare). Insults of various types at any time during lens development can result in lens opacities. These insults may include genetic mutations in structural proteins, enzymes, or infections. Developmental opacities are less likely to be progressive than those that develop later in life. There is an intimate interdependence of the lens and the retina during development because of cross-stimulation by vital cytokines. The coloboma is a fault of the neuroectoderm and therefore does not affect the lens directly. The outer epithelial cells of the vesicle form a basement membrane comprising the lens capsule. The remaining growth of the lens is limited to the equatorial region (germinal center) that throughout life will produce anucleate lens fibers that join in the anterior and posterior visual axis to form sutures. Initially the sutures are visible as an anterior upright Y suture and a posterior inverted Y suture.
Safe 25 mg lamictal
Nolle B medications qid cheap lamictal 100 mg free shipping, et al: Anticytoplasmic autoantibodies: their immunodiagnostic value in Wegener granulomatosis. Zhang X, et al: Clinical and pathological manifestations of patients with antineutrophil cytoplasmic autoantibodies directed against proteinase 3 or myeloperoxidase. Goldstein I, Wexler D: Bilateral atrophy of the optic nerves in periarteritis nodosoa. Hayasaka S, Uchida M, Setogawa T: Polyarteritis nodosa presenting as orbital apex syndrome. Clinical and pathologic investigations of intermittent choroidal vascular insufficiency in a case of periarteritis nodosa. The differential diagnosis for orbital inflammatory disease includes infectious and noninfectious causes (Table 232. A detailed history and accurate examination is essential in reaching the correct diagnosis and appropriate prompt treatment. Modes of presentation, inciting factors, and treatment options differ for each of these groups, although diagnostic modalities are largely the same. Bacteria are the most common cause of orbital infection, with a wide spectrum of bacteria associated with disease. Clinical circumstances often provide the necessary clues to determine the offending organism and to allow the initiation of treatment pending culture results, but investigation should not delay immediate management where an acute orbital infection is suspected on clinical grounds. Bacterial orbital cellulitis leading to proptosis, severe conjunctival chemosis, and exposure keratopathy. Systemic Complications of Orbital Infection Cavernous sinus thrombosis11 Superior orbital fissure syndrome Meningitis in 1. A history of fever, upper respiratory tract infection, lacrimal outflow obstruction, sinusitis, or trauma should carefully be elicited. Preseptal infection may present with lid edema and redness, the ocular examination otherwise being normal (Chandler stage 1, Table 232. The presence of a demarcation line corresponding to the arcus marginalis, conjunctival chemosis, proptosis, ophthalmoplegia, or loss of vision are, however, all features of orbital (postseptal) infection, although early postseptal extension may be associated with more subtle signs. Ancillary investigations, including a white blood cell count with differential, cultures (pus and blood), and orbital ultrasonography may not be contributory, and initiation of treatment for suspected postseptal disease should on no account be delayed for the sake of such investigations. Anatomical Factors Predisposing the Orbit to Infection the paranasal sinuses are related to the orbit inferiorly, medially and superiorly the orbit is separated from the ethmoid sinuses by the paper-thin bone of the lamina papyracea Veins in the midface, including the inferior and superior ophthalmic veins, lack valves, permitting direct posterior spread of infectious organisms Bacteriology 2962 orbital foreign body, results from trauma to the periorbital area or sinuses. In the pediatric age group, a- or nonhemolytic streptococci, group A b-hemolytic streptococci, Staphylococcus aureus and Haemophilus influenzae, were the most commonly isolated organisms among a cohort of 41 children with postseptal cellulitis described by Nageswaran et al between 1996 and 2006. A previously healthy 4-year-old boy presented with periorbital swelling and a preceding upper respiratory tract infection. At presentation the swelling was confined to the preseptal tissues, and the visual acuity and eye movements were normal. A diagnosis of preseptal cellulitis was made, and parenteral flucloxacillin and ceftriaxone were initiated. His general condition deteriorated over the following 36 h (a), with increased lid edema, inability to open the eyelids and a spiking pyrexia (b). Discrete Stages of Orbital Cellulitis* Stage 1 Features & pathophysiology Inflammatory, preseptal edema of the eyelids. Eyelid edema results from impaired venous and lymphatic drainage by the infected sinus. Diffuse postseptal orbital edema and infiltration by bacterial and inflammatory cells. Bilateral proptosis, severe pain, and signs of meningeal inflammation, resulting from extension of the abscess posteriorly and the formation of cavernous sinus thrombosis. Botryomycosis is a chronic bacterial granulomatous disease often involving the skin and subcutaneous tissue, caused by an encapsulated form of Staphylococcus that is particularly resistant to conventional medical therapy. Early involvement of both the pediatrician and the otorhinolaryngologist is essential. For children with mild preseptal disease and no constitutional malaise, out-patient management with oral antibiosis and daily review is appropriate. Sinusitis is managed with the appropriate antibiotic, but endoscopic sinus drainage should be performed if the orbital cellulitis fails to respond to intravenous antibiotics. In the study by Nageswaran et al, 12 of of the 41 children responded to antibiotic alone; the remainder (71%) underwent surgical drainage, of which over half also required ethmoidectomy. Although historically the presence of a subperiosteal abscess was an indication for urgent drainage, current indications for medical treatment include normal visual function, age less than 9 years, medial location, and no intracranial or frontal sinus involvement. An obstruction may be the result of chronic infection, tumor, or trauma54 and chronicity leads to an expansion of the cavity and thinning of the bony sinus walls. Expansion into the orbit or contiguous inflammation may result in orbital findings. Specifically, sphenoidal sinus involvement may compress the optic nerve and cause visual loss or visual field loss. Orbital apex involvement or extension of the infectious process intracranially as meningitis, abscess, or cavernous sinus thrombosis are particularly severe manifestations of orbital infection. Identification of the anatomic location and the extent of infection define the severity of the disease, the prognosis, and the appropriate course of therapy. Loss of vision or ophthalmoplegia mandates a search for orbital apex or cavernous sinus involvement. Aerobes reduce the tissue pressure of oxygen, which is toxic to anaerobic organisms, and anaerobes produce beta-lactamase thereby protecting aerobes against the effect of certain antibiotics. Harris has proposed that these factors may underscore the clinical observation that subperiosteal abscesses have a better prognosis in children under 9 years of age than older children, in whom drainage cultures are usually negative. Imaging (b and c) identified a huge superior orbital abscess that was compressing and deforming the globe. Infectious Processes of the Orbit lying infection elsewhere (for example, an upper respiratory tract infection), and a full ear, nose, and throat history. Accurate clinical examination will provide key information regarding the position (pre- or postseptal) and severity (inflammatory orbital edema or subperiosteal abscess) of suspected periorbital or orbital infection. Both preseptal and postseptal infections may present with local pain, swelling, heat, and redness, and fever. Postseptal infections tend to be characterized by systemic malaise, conjunctival chemosis, ophthalmoplegia, proptosis, and in severe cases, visual loss, suggesting high intraorbital pressure, abscess, or cavernous sinus thrombosis (Table 232. A peripheral demarcation line corresponding to the arcus marginalis is suggestive of a postseptal infection. However, suspected postseptal infection requires immediate treatment with a high dose, broad spectrum intravenous antibiotic. The urgency of treatment cannot be overstated, as any delay may lead to irreversible visual failure in severe cases. Where there is a high incidence of community-acquired methicillin resistant staphylococcus infection, initial treatment might include vancomycin, cefotaxime, and either metronidazole or clindamycin. A nasal decongestant, such as oxymetazoline, should also be given, since this may facilitate drainage of the sinuses and an adjacent subperiosteal orbital abscess. The periorbita is elevated until the anterior extent of the abscess is reached and the contents are evacuated. These transcutaneous approaches give good access to the subperiosteal space but, where the possibility of a scar is of particular concern, a transconjunctival or transcaruncular approach might be considered where such an approach provides reasonable access to the medial, inferior, or lateral orbit. An intraorbital abscess (Chandler stage 4) is rare and is usually secondary to ocular surgery, penetrating orbital injury, or septic hematogenous emboli.
Discount 100mg lamictal amex
However medications varicose veins buy lamictal 100mg line, B lymphocytes predominate within the aqueous humor and at the iris-ciliary body junction. Juvenile Rheumatoid Arthritis Uveitis in children is rare, except for those with juvenile rheumatoid arthritis, who are negative for the circulating autoantibody rheumatoid factor. It is usually a chronic bilateral nongranulomatous anterior uveitis of variable severity, small keratic precipitates, anterior synechiae and anterior vitreous cells. The iris may show infiltration by plasma cells, occasionally containing Russell bodies. This facilitates sequestering of circulating antigenantibody complexes and results in recurrence and chronic inflammation. No fibrinoid necrosis or scleral inflammation are seen, as they are in adult rheumatoid scleritis. Cystoid macular edema is often found, and to a lesser extent, retinal vasculitis and subretinal neovascularization occur. The physiopathology of Birdshot chorioretinopathy implies an autoimmune process affecting the choroid and the retina. This would again suggest a genetic susceptibility associated with environmental factors. Heterochromia is secondary to stromal iris atrophy that can have a patchy distribution. The involved eye can actually be darker if the stromal atrophy unmasks the pigmented epithelium. Characteristically, there are no posterior synechiae but isolated anterior synechiae can occur. Lymphocytes (a mixture of interleukin-2 receptor-negative helper and suppressor T-cells and B lymphocytes) and plasma cells infiltrate the iris and the ciliary body. Hyalinization of iris arterioles contributes to their fragility and vascular occlusion. Based on these findings, a vascular cause to this disorder has been suggested but no evidence for active vascular inflammation has been found. Findings of abnormal melanin production along with membranous degeneration of nerve fibers lead some authors to suggest abnormal adrenergic innervation, either primary or secondary to the inflammation. Fluorescein angiography shows early hypofluorescence of the patches, followed by hyperfluorescence in the late venous phase. Occasionally, retinal venous vasculitis occurs that is topographically independent of the choroidal lesions. The process usually begins in the peripapillary region and extends by recurrences in an irregular fashion to the midperiphery. Retinal vasculitis, papillitis, hyalitis, and neovascularization have occasionally been observed. Defects in Bruchs membrane may occur, allowing subretinal neovascularization and fibrosis to extend into the choroid. The reason that septic emboli occur more frequently in the retina than in the choroid is unknown. Diffuse inflammation shows numerous bacteria and inflammatory cells with necrosis and hemorrhage of the involved tissues. During the course of bacteremia, any causative bacteria can lodge in eye and produce endophthalmitis. Certain organisms clearly have a propensity to invade the eye from the blood stream. In large tuberculomas, caseation necrosis is present with zonal granulation surrounding the coagulative necrosis. Miliary choroidal tuberculosis causes a multifocal, discrete, sarcoid-like inflammation, but with caseating necrosis affecting the centers of the epithelioid granulomas. Leprosy (Mycobacterium leprae) this disease affects 10 million people living between the tropics of Cancer and Capricorn. In lepromatous leprosy, ocular involvement includes the cornea, sclera, and iris; iridocyclitis can be either insidious or acute and exudative. The iris often develops striking white globular bodies enmeshed in the stroma (leprotic pearls). In lepromatous leprosy, histopathologic examination reveals granulomatous inflammation occurring with characteristic formation of lepromas. In tuberculoid leprosy, lesions are akin to noncaseat- Metastatic Bacterial Endophthalmitis Several distinct clinical forms of metastatic bacterial endophthalmitis can be empirically designated as focal (anterior or posterior), diffuse (anterior or posterior), and panophthalmitis. Focal intraocular inflammation appears to be concentrated in one or a few discrete foci with the appearance of whitish nodules or plaques in the iris, ciliary body, retina, or choroid. Anterior diffuse inflammation is characterized by severe generalized signs of inflammation involving the anterior segment; corneal edema, hypopyon, or fibrinous clot in the anterior chamber is typical. Posterior diffuse inflammation is characterized by an intense inflammatory reaction in the vitreous. Histopathologic examination reveals focal inflammation with bacteria and inflammatory cells occluding the lumen of vessels and infiltrating the surrounding tissue. Tuberculoma of the choroid in a 22-year-old man with known active pulmonary tuberculosis. The active lesion is smaller and is now surrounded by an accumulation of pigment epithelium. Discrete tubercular or sarcoidal inflammation is present with nodules of varying size. Syphilis (Treponema pallidum) Ocular involvement may occur in both congenital and acquired syphilis. Iritis may occur either as roseola in the initial stages of secondary syphilis, with a hyperemic, bright red spot in the middle third of the iris that lasts several days and resolves, or as yellow to brown papules at the pupillary margin or ciliary border. Retinal periphlebitis and juxtapapillary chorioretinitis heal with severe scarring. In syphilitic chorioretinitis, chronic granulomas and inflammation are characterized by lymphocytes, epithelioid and plasma cells, and treponemas (Treponema pallidum). The most common manifestations are rash and arthritis and neurologic and cardiac signs and symptoms. Histopathologic study reveals dense sheets of Pneumocystis organisms infiltrating the choroid, choriocapillaris, and choroidal vessels. An amorphous, foamy, acellular, eosinophilic infiltrate may be present within the choroidal vessels. Vitritis, optic neuritis, and round, yellow-white chorioretinal lesions surrounding the optic disk. Herpetic uveitis is a common complication of herpes keratitis, but it may also occur without keratitis. With herpetic infection, granulomatous inflammation of the iris is histologically found to consist of lymphocytes, macrophages, plasma cells, and fibrin. The salt-and-pepper fundus appearance is due to alternating areas of pigment epithelium hyperpigmentation and hypopigmentation. It causes various ocular inflammations, including conjunctivitis, episcleritis, keratitis, uveitis, and optic neuritis. Acute bilateral severe anterior uveitis, and acute punctate retinochoroiditis with panuveitis have been described. The infectious mechanism could occur through reactivation of an old primary local infection or through infectious emboli in the choriocapillaris.
Buy lamictal 50 mg without prescription
The lesion rapidly erodes ad medicine discount lamictal 25mg otc, leaving a smooth base and indurated borders that have a characteristically cartilaginous consistency when palpated. Extragenital chancres may be more painful and may follow a more chronic course than do genital chancres. In secondary syphilis, a maculopapular, papulosquamous, pustular, follicular, or nodular lesion can occur following an average 8-week incubation period. The eyelid manifestations of tertiary syphilis include the typical granulomatous lesion known as the gumma. Diffuse gummatous ulcerations have been reported in association with untreated late congenital syphilis. Treponemal serologic tests are positive in ~90% of cases of syphilis and remain positive regardless of disease activity, whereas non-treponemal tests are indicative of disease activity and can become negative with treatment. Furthermore, falsepositive non-treponemal tests may result from a number of medical conditions. Parenteral Penicillin is the treatment of choice for all stages of acquired syphilis. Primary, secondary, and early latent syphilis is treated with Benzathine Penicillin G: 2. Late latent and benign tertiary syphilis is treated with Benzathine Penicillin G: 7. Clinical appearance of cutaneous malakoplakia shows a hyperkeratotic, dome-shaped, umbilicated mass on the right medial canthal region. Primary herpetic blepharoconjunctivitis begins as a vesicular eruption with surrounding erythema on the skin of the eyelids. Corneal involvement is most commonly seen as a punctate epithelial keratitis but may appear as a dendrite, geographic ulcer, or stromal infiltrate. Indirect immunofluorescent staining is a quick and reliable technique in confirming the diagnosis. The Herpetic Eye Disease Study found a 19% recurrence rate of ocular herpes with Acyclovir prophylaxis compared to 32% with placebo over an 18-month period. The latent virus is activated by a change or depression in cell-mediated immunity. In zoster ophthalmicus, the activated virus moves down the ophthalmic division of cranial nerve V and manifests as erythematous or maculopapular cutaneous eruptions in the respective dermatomal distribution. Scarring may occur because of the deeper involvement of the dermis in herpes zoster, compared to varicella lesions. Cicatrization can lead to lid margin abnormalities such as entropion, ectropion, madorosis, trichiasis, punctal and canalicular stenosis, lid retraction, and necrosis with subsequent exposure keratitis. Elevated immunoglobulin E, abnormal cell-mediated immunity, and dendritic cell function have been associated with eczema herpeticum. Involvement of the nasociliary branch of the ophthalmic division of the trigeminal nerve is often associated with ocular complications from herpes zoster. This patient illustrates the healing phase of the rash during the second week when crusts have started to form and the erythema is subsiding. Transmission from sexual contact is more common in adults Eyelid lesions appear as multiple, round, waxy umbilicated skin papules Incision and expression of the viral bead with a curette is usually curative. Although uncommon, lid involvement is characterized by nongrouped vesicular lesions resting on an erythematous base. Individuals with lid vesicles should be examined for conjunctival or corneal lesions and anterior uveitis. The conjunctival lesions consist of small limbal or perilimbal pock-like elevations or tarsal and bulbar conjunctival ulceration that heals without sequelae. Eyelid lesions should be treated with topical antibiotic ointment to prevent bacterial superinfection. A biphasic incidence profile has been reported with peaks in young children and young adults. The diagnosis is based on recognition of the characteristic lesions and histopathologic confirmation. Incision with scalpel blade, followed by expression of the viral bead using a chalazion curette, is usually curative. Recalcitrant and disseminated disease in immunocompromised individuals may require topical and intravenous Cidofovir. Clinical appearance of molluscum contagiosum of the left upper eyelid margin shows a dome-shaped nodule with smooth contour and central umbilication. Vaccinia lesions of the eyelid are seen in various stages of evolution from vesicles to umbilicated pustules. Because of the virtual impossibility of contracting smallpox, the production of smallpox vaccine for general use was discontinued in 1982. Conjunctival disease manifests as follicular or papillary conjunctivitis with occasional ulcerations and membrane or pseudomembrane formation. Punctate, dendritiform, or geographic corneal epithelial keratitis, interstitial keratitis, and corneal ulceration may complicate blepharoconjunctival involvement. Late sequelae include madarosis, scarring and punctual stenosis, symblepharon or corneal scarring. Topical antiviral agents (Trifluridine or Vidarabine) are recommended for prophylaxis after direct ocular contact with the vaccinia vaccine, for treatment of conjunctival or corneal involvement, and can be considered as preventative measure with isolated eyelid involvement. It is most prevalent in the southeastern United States and the Ohio and Mississippi river basins. Primary, but often subclinical, pulmonary infection occurs after inhalation of the conidia. The fungus then spreads hematogenously to involve various organs, but most frequently, skin, bone, and the internal genitalia are involved. Although lid involvement was previously reported to occur in 25% of patients with systemic disease, Bartley73 found eyelid involvement in only 1 of 79 patients (1. The diagnosis is established by microscopic examination of potassium hydroxide-treated preparations of drainage from skin lesions. Hematogenous dissemination occurs in the setting of immune system compromise, and most often spreads to the central nervous system, although the skin, liver, kidneys and lymph nodes can be involved. Less commonly, lesions can present as violaceous papules, vesicles, crusted plaques, or subcutaneous nodules. Confirmation of the clinical diagnosis is based on culture of the organism from skin lesions, cerebrospinal fluid, blood, or urine. Of the available serodiagnostic tests that can indicate the presence of cryptococcal infections, the latex agglutination test is the most valuable. Presents as single or multiple nodules with or without superficial ulceration, or as localized eyelid edema Coccidioidin skin testing valuable in establishing the diagnosis, confirmed when organism is identified on culture or tissue biopsy specimen Treatment consists of oral azoles. Although worldwide in distribution, it is found most often in Central and South America. Three forms occur, the cutaneouslymphatic form, the pulmonary form, and the disseminated form. Cutaneous inoculation usually occurs from a thorn or splinter in a finger or hand.
Order lamictal in india
However 300 medications for nclex generic lamictal 100mg without a prescription, in one patient studied, postmortem viable tumor in the optic nerve was demonstrated despite a full course of orbital irradiation. Occasionally, the metastasis is isolated and discrete, and resection for cure can be attempted. In children, metastatic disease to the eye and its adnexa almost exclusively involves the orbit. Also, metastases commonly do not arise from carcinomas, such as in adults, but from sarcomas. Metastatic neuroblastoma to the orbit, presenting with bilateral eyelid ecchymoses. In Huh and associates193 series of 70 patients, no serious side effects were observed. However, the orbit is as likely to respond to systemic therapies as is the primary tumor or other areas of dissemination. Thus, patients with metastatic orbital disease from estrogen receptor-positive breast carcinoma responsive to antiestrogens, prostate carcinoma responsive to orchiectomy or diethylstilbestrol, and small-cell carcinoma of the lung responsive to chemotherapy should all be treated aggressively with these modalities. These patients frequently enjoy improvement and temporary control of their disease. It is unclear whether the metastases arise in the orbital soft tissue or in the bone with contiguous spread. Neuroblastoma can also be associated with the paraneoplastic syndrome of opsoclonus and myoclonus. The disease has also been seen to arise primarily in the soft tissues or bone of the orbit. Prophylaxis consists of intrathecal injection of methotrexate and reinforcement of chemotherapy. Prognosis was poor and 2 years after diagnosis of the ocular lesions, only 1 of the children studied remains alive. In addition to arising primarily in the orbit of infants, teratomas can secondarily involve the orbit by direct extension from surrounding structures. Most of these primary lesions are addressed elsewhere in the text, and what follows is a discussion of these lesions as orbital diseases. Rootman9 found that secondary neoplasias represented onethird of all cases of orbital neoplasias. Shields and associates12 found that secondary tumors represent 11% of orbital lesions and that 29% of these represented clinically detectable orbital extension of uveal melanoma. The next most common secondary tumor was orbital extension of conjunctival melanoma. Shields and associates12 described 2% of all orbital tumors to be lymphoplasmacytic lesions and leukemia. Most of leukemia patients had involvement of the fundus with concurrent invasion of the optic nerve and did not present as a primary orbital mass. Four children had an initial orbital lesion with a rapidly progressing exophthalmos; all were diagnosed with myeloid sarcoma. In addition, secondary orbital tumors arising from the sinuses, eyelids, and globe are the most common settings in which patients require exenteration. Therefore, aggressive and complete excision must be accomplished to prevent a recurrence. Osteoma was the second most common benign lesion to involve the orbit and was studied by Johnson and associates. Orbital extension is a rare event that can give rise to ocular signs and symptoms; in such a case treatment is mandatory. Osteomas frequently enlarge most during rapid skeletal growth, and therefore they are an important consideration in children and adolescents. Some consider that these occur secondarily in patients who have had orbital trauma or sinus infections. Others believe that they represent a developmental lesion occurring at the site of fusion of membranous and cartilaginous bone. The lesion represents compact bone (without fibrovascular stroma) and is managed by simple excision. Dinesh and associates219 investigated 62 patients with primary bone tumors of the orbits found that osteoma along with fibrous dysplasia were the most common encountered entities. The sinus epithelium continues to secrete mucus, filling the normal aerated space and exerting pressure on the surrounding bony structures. It has also been reported in association with malignancy, however, most likely secondary to occlusion of the sinus ostia. More than 50% of patients with sinus and nasal tumors can have signs and symptoms related to the eye or orbit. The maxillary and sphenoidal sinuses are present at birth, and all the sinuses develop throughout childhood until they reach their final size in adolescence. Each sinus communicates with the nasal pharynx by a bony osteum, and each is directly adjacent to the orbit. The primary mode of extension of sinus tumors to the orbit is via direct extension. This can be accomplished by bone erosion, extension along normal neurovascular bundles, and extension through preexisting bone canals. In the case of the maxillary sinus, which is the most common origin of these secondary orbital tumors, only thin bone separates the inferior orbital fissure from the mucosa of the sinus. Benign lesions include inverting papilloma, osteomas, juvenile angiofibroma,214 and unusual neuroectodermal tumors. Nasoangiofibroma commonly invades the pterygopalatine fossa, nasal cavity, sphenoid sinus and nasopharynx. Orbital involvement was noticed in six of 19 patients (32%) with juvenile angiofibroma; in five of these patients the tumor invaded the orbit via the inferior orbital fissure. These papillomas typically arise in the lateral nasal wall or in the mucosa of the ethmoidal sinus. Clinical presentation of sinonasal tumors cannot be distinguished from inflammatory disease and include: nasal obstruction, rhinorrhea, and sinus pressure226; therefore, many patients present having had disease for longer than 6 months. Because the tumors often do not invade the orbit in the retrobulbar space, these patients may present with nonaxial displacement of the globe; i. Other signs include proptosis, strabismus, hypesthesia, and a mass on nasal examination (Table 239. When comparing metastatic to secondary orbital tumors, Rootman234 found that in metastatic carcinomas, the disease was not painful and that proptosis was axial in most cases (75%). This was in contradistinction to secondary malignancy in which pain and paresthesias were present in 60% of cases, and nonaxial displacement occurred in 48%. Carcinomas arising from the floor of the maxillary sinus are less likely to involve the orbit than are those from the roof of the sinus. Tumors involving the floor can spread to the pterygoid region and present with pain in the teeth. Further extension of these tumors to the base of the skull can cause multiple cranial nerve palsies. Approximately 10% of all orbital mass lesions consist of secondary tumors originating from the nose and paranasal sinuses. The patient was diagnosed with right ethmoid mucocele and was referred to endonasal surgical drainage. The optic canal forms a part of the wall of the sphenoid sinus; therefore tumors arising in this location can occasionally invade the optic nerve. Harbison and associates reviewed 42 cases of sphenoid sinus carcinoma and found that five patients (12%) had optic nerve and chiasmal invasion. These patients more commonly present with nasal congestion and epistaxis than do patients with antral carcinoma. Despite its lower incidence, Mohan and associates238,239 found these tumors invading the orbit as frequently as antral carcinoma. Overall survival was poor despite combined surgery, chemotherapy and radiation with 52% 5-year survival. Frontal sinus malignancies are rare but can involve the frontal lobe and the structures around the sella turcica at an early stage.
Order lamictal 100mg overnight delivery
Lesions that grow rapidly and double in size within days are more likely to be inflammatory conditions such as chalazion or pyogenic granuloma than melanoma medicine runny nose purchase lamictal 100 mg without prescription. Malignant pigmented lesions can be clinically distinguished from benign pigmented lesions because malignant lesions exhibit disorganized and chaotic pigment and color patterns whereas benign lesions tend to have order and symmetry in their coloration, regular borders, and uniform surface characteristics. Benign lesions that are occasionally confused with melanoma include seborrheic keratosis, compound nevus of Spitz, junctional nevus, lentigo, hemangioma, blue nevus, and tattoo spots. This is particularly true in patients whose lesions change in size, color, or shape. A rapidly growing nodular melanoma with a Breslow thickness of at least 12 mm that started on the lower eyelid margin in the skin parallel to the lash line and then rapidly grew onto the surface of the globe and diffusely involved the bulbar and palpebral conjunctiva in a period of less than 4 weeks. An amelanotic lesion in the lower eyelid that was initially mistakenly diagnosed as a chalazion and on examination of the final excisional biopsy specimen was discovered to be invasive melanoma. Melanocytic Lesions of the Eyelid and Ocular Adnexa Excisional biopsy is almost always preferred over other biopsy techniques; however, if the lesion is large and involves multiple areas of the conjunctiva or the entire lower eyelid margin, an incisional biopsy of the most worrisome area is a reasonable alternative. Several studies have disproved concerns that incisional biopsy of a melanoma could promote seeding or dissemination of melanoma cells. The biopsy method chosen must yield a specimen that provides information about tumor thickness. For conjunctival melanomas, special care is required in specimen handling and processing of the primary tumor specimen. In addition, most conjunctival melanoma specimens are quite small and thin compared to cutaneous melanoma specimens. These factors together frequently lead to tangential cutting of conjunctival melanoma specimens. Controversy exists regarding the role of frozen sections for determination of tumor thickness and resection margin status for melanoma. At present, the consensus seems to be that frozen-section diagnosis of melanoma is not as accurate as diagnosis made using paraffin-embedded sections. Uniform classification and staging of melanoma are of paramount importance: useful comparisons of treatment regimens and results from different centers can only be made if patient populations are similar with respect to tumor load, distribution of disease, and potential for a poor outcome. Curling-up of the edges of the surgical specimen led to tangential cutting and inability to determine the depth of invasion of the melanoma. The Breslow thickness can be determined accurately and is measured from the epithelial surface to the deepest area of invasion of tumor. From Esmaili B et al: Surgical specimen handling for conjunctival melanoma: implications for tumor thickness determination and sentinel lymph node biopsy. En bloc excision of an invasive melanoma of the eyelid and conjunctiva with involvement of the canaliculi and the palpebral and bulbar conjunctiva. Such specimens are presented to the pathology lab in total and over a drawing of the eye and eyelid to clearly outline the margins of interest and orientation for the pathologist. The goal of surgical treatment is to remove all melanoma cells and thus achieve local control and possibly increase the probability of cure. In the past, normal skin margins as wide as 5 cm were advocated in an effort to remove all occult foci of melanoma cells. M0 = no distant metastasis; M1a = distant skin, subcutaneous, or nodal metastases; M1b = lung metastases; M1c = all other visceral metastases or any distant metastases with elevated serum lactic dehydrogenase level. Melanocytic Lesions of the Eyelid and Ocular Adnexa adequate for primary melanomas no more than 1 mm thick. For melanomas thicker than 2 mm, another study suggested that survival was poor if the excision margin was less than 2 cm but that increasing the margin beyond 3 cm did not offer a further advantage. For melanomas in the periocular region, adjacent vital structures and cosmetic considerations generally limit the margins of excision. One recent study of 44 patients with eyelid melanoma treated by 23 oculoplastic surgeons concluded that most eyelid melanomas (~60%) are discovered early and have a Breslow thickness of less than 2 mm at the time of diagnosis. This study also demonstrated that the majority of oculoplastic surgeons aimed for margins of excision of ~5 mm. This conservative margin led to good local control in the majority of patients (75%), and local and regional recurrences were limited to patients who had tumors that were greater than 2 mm thick. Although this study was based on a relatively small number of patients, it suggested that a 5-mm excision margin may be appropriate for tumors less than 2 mm thick but may not be acceptable for tumors with Breslow thickness of 2 mm or greater. The results further suggested that the size of the excision margins, while important for local control in thicker tumors, did not have a significant effect on the rate of regional nodal or distant metastases. Adjuvant Radiation Therapy Radiation therapy is generally not used as definitive treatment for eyelid melanoma. However, adjuvant radiation therapy is very useful in patients with eyelid melanoma, especially given the limitations on resection margins and the desire to preserve vital structures. Adjuvant Topical Chemotherapy the use of topical chemotherapy for ocular adnexal melanomas is mostly limited to conjunctival melanomas. At the time of this report, 2 years after completion of radiation therapy, the patient remains free of evidence of local recurrence in the orbit. Given the rarity of ocular adnexal melanomas, large-scale natural-history or population studies of these tumors are scarce. Indeed the current standard management for ocular adnexal melanomas at most centers is to observe the regional lymph nodes until clinically obvious nodal metastasis is discovered. Larger volumes are avoided because they could lead to spread of the radioactive material into the subconjunctival space or nonspecific drainage from areas with a different pattern of lymphatic drainage than the primary tumor site. Multiple images of the ipsilateral head and neck region are obtained in the nuclear medicine department beginning within a few minutes after radionuclide injection. The area of technetium injection in the eye region is seen, as are three sentinel lymph nodes draining the primary tumor. From Amato M et al: Feasibility of preoperative lymphoscintigraphy for identification of sentinel lymph nodes in patients with conjunctival and periocular skin malignancies. A skin incision suitable to permit exploration of the lymphatic basins at risk is made, and these basins are explored. Postoperative adjuvant radiation therapy to the regional nodes is recommended to ensure durable regional control. Use of serial sectioning and immunohistochemistry should decrease this type of error, although the technology is still not perfect. The parotid nodes are also smaller than other nodes and often located in a bed of fibroadipose tissue, making their dissection more challenging. The assumption is that each time a conjunctival melanoma recurs locally, there is a risk of spread through the lymphatics to the regional lymph nodes. At the time of a recurrence, the lymphatic drainage pattern may be less reliable because of previous surgery. Choroidal metastasis in the left eye of a patient who had a right orbital exenteration 4 years prior to this presentation for conjunctival melanoma of the right eye. She was also found to have multiple other sites of metastasis, including the brain, kidneys, lung, and liver. The estimated rate of distant-organ metastasis for eyelid skin melanoma in a series from our Tertiary Cancer Center was 50% with a mean follow-up time of 9. An estimate of association based on a histologic study of 234 primary cutaneous melanomas. Esmaeli B, Wang B, Deavers M, et al: Prognostic factors for survival in malignant melanoma of the eyelid skin. Tuomala Tuomaala S, Kivela T: Metastatic pattern and survival in disseminated conjunctival melanoma: implications for sentinel lymph node biopsy. Esmaeli B, De Martelaere S, Ozkan Y, et al: Surgical specimen handling for conjunctival melanoma: implications for tumor thickness determination and sentinel lymph node biopsy.
Cheap lamictal 200 mg visa
Interestingly medications with sulfur buy lamictal in united states online, immunohistochemical analysis has been suggestive of a T-cell disorder. The primary differential considerations are infectious processes, other vasculitides, and central facial lymphomas. Both entities are uncommon benign disorder involving cutaneous lesions in the head and neck region and vascular proliferation. Excision of the lesions is the first treatment modality; however, surgical excision is complicated by bleeding and the lack of distinction between abnormal and normal tissue. Benjamin I, Taylor H, Spindler J: Orbital and conjunctival involvement in multiple myeloma: report of a case. Nikoskelainen E, Dellaporta A, Rice T, et al: Orbital involvement by plasmacytoma: a report of two cases. Laroche L, Laroche L, Pavlakis E, Saraux H: Immunologic characterization of an ocular adnexal lymphoid T tumor by monoclonal antibodies. Uchiyama T, Yodoi J, Sagawa F, et al: Adult T-cell leukemia: clinical and hematologic features of 16 cases. Dalla-Favera R, Bregni M, Erickson J, et al: Human c-myc oncogene is located on the region of chromosome 8 that is translocated in Burkitt lymphoma cells. Kimura T, Yoshimura S, Ishikawa E: On the unusual granulation combined with hyperplastic changes of the lymphatic tissues. Rosai J, Gold J, Landy R: the histiocytoid hemangiomas: a unifying concept embracing several previously described entities of the skin, soft tissue, large vessels, bone, and heart. On the unusual granulation combined with hyperplastic changes of lymphatic tissues. Angiolymphoid hyperplasia with Eosinophilia: a case report of orbital involvement. Orbital involvement with angiolymphoid hyperplasia with eosinophilia- a benign condition for the practicing ophthalmologist to be aware of. A rapidly fatal case of T-Cell lymphoma presenting as idiopathic orbital inflammation. Albert Patients with cancer typically survive their disease due to advances in early diagnosis and treatment. The presence of orbital metastases invariably implies advanced disease, therefore usually carry poor prognosis. Orbital and ocular adnexa metastases are rare in comparison with other secondary sites; however, along with secondary tumors comprise the most common malignancies to involve the eye and orbit. Identifying orbital metastases is important prognostically, as their presence is associated with very poor survival. The choroid is the most common site for uveal metastasis with approximately one-third of patients having no history of primary cancer at the time of ocular diagnosis. Clinical examination may show orbital or ocular adnexal mass, redness or swelling, proptosis, globe displacement or ptosis. Both the ophthalmologist and the internist should be able to identify symptoms and signs associated with metastatic orbital lesions, be familiar with common sites of origin and appropriate management strategies. Prompt recognition of this condition may help in the detection of a previously unrecognized systemic malignancy or allow early treatment. In many cases, treatment can only be palliative; however, in other cases, using modern combined-modality therapies, patient survival can be prolonged. The incidence and prevalence of this condition must be considered in two different ways: first, how many individuals with carcinomas will experience orbital metastases and second, what percentage of orbital disease is caused by metastatic lesions The percentage of patients with known systemic malignancies who have clinically documented metastases to the eye and its adnexa is not as high as the incidence of identification of tumor foci in autopsy studies of patients who have succumbed to their malignancies. Eliassi-Rad and associates29 examined the frequency of intraocular metastases in patients who had died of cancer. The incidence of eye or orbital involvement in patients with known malignancies is reported to be between 4. Suffice it to say that orbital lesions are likely to occur almost as frequently as intraocular metastases. It has been estimated that 25 000 patients per year who die of systemic malignancies also have ocular involvement. With increased clinical awareness and sophistication, as well as more sensitive diagnostic modalities, increasing numbers of patients with metastatic orbital lesions will be identified. The incidence of metastatic tumors as the cause of orbital disease ranges in various series from 1% to 12%, with most investigators reporting an incidence of 3%. In a recent survey12 his group reported a higher incidence of orbital metastases of 7%, 91 of 1264 patients with orbital mass lesions were diagnosed with orbital metastatic disease, with breast carcinoma being the most common primary comprising 4% of all patients (44 cases). In a biopsy series of 300 patients with expanding orbital lesions, Silva41 reported seven cases (2. There seems to be a trend toward decreased incidence of orbital metastases presumably due to better treatment modalities, this is despite the fact that the overall incidence of cancer has increased. The most accurate work by Fahmy and associates25 investigated the incidence of orbital metastases in the ophthalmic region in Denmark between 1969 and 1998 and compared it to the incidence between 1944 and 1968. They found that while the pattern of anatomical location of metastases has not changed, the incidence has fallen significantly. Breast cancer in women, lung cancer in men and skin melanoma were the most prevalent primary tumors in their series. If one extrapolates from autopsy studies of ocular metastases, it is likely that subclinical disease frequently goes unrecognized. Generally, orbital disease is uncommon and is caused by metastatic tumors in only a relatively small percentage of cases with most surveys report 3% of all orbital tumors and up to 12% of all orbital masses to be secondary to metastatic disease. Despite this relatively low incidence, it is essential that all ophthalmologists will be familiar with this entity and the spectrum of disease for which it is responsible. Familiarity aids in prompt diagnosis and treatment, affording patients improved quality of life and possibly an increased rate of survival. In addition, a small amount of blood flow reaches the orbit via branches (facial, maxillary, and temporal) of the external carotid artery. After seeding through the vascular system, tumor emboli settle in the microvasculature of the different ocular tissues. Areas of increased vasculature (particularly the choroid in the posterior pole of the globe) receive the most emboli and are frequently involved with metastatic disease. In reviewing the literature, Goldberg and associates38 found that ~40% of tumors involved the lateral orbit, and only 12% involved the inferior orbit. In this series, 30% occurred in the superior orbit and 20% occurred in the medial orbit. Shields and associates1 reported 60% of all metastases to involve the anterior orbit (posterior sclera to eyelids) with a similar percentage showing diffuse orbital involvement. Orbital involvement by metastasis can be diffused or localized, with a tendency of similar patterns for various primary tumors. Initial tumor emboli can lodge in muscle, fat, or bone or can involve the orbit diffusely. Therefore, it is presumed that all metastatic tumors reach the eye and its adnexa via the blood stream. It follows that all tumor emboli that are to reach the eye must have passed through the pulmonary circulation and seeded the lungs with tumor emboli; tumor cells subsequently travel in the carotid system to reach the orbit via the ophthalmic artery. However, in one study, 15% of patients with ocular metastases had no demonstrable pulmonary metastases at the time of autopsy. In the latter route tumor emboli reach the cranial venous sinuses traveling up to the ophthalmic and vortex veins. Metastatic melanoma involving the eye or orbit may appear as solitary or multiple nodules. There seems to be bone erosion, and the mass is centered posterior to the lacrimal gland fossa. Histopathology was consistent with the diagnosis of metastatic prostate carcinoma. Courtesy of Dr Alan A McNab, Royal Victorian Eye and Ear Hospital, Department of Ophthalmology, University of Melbourne, Melbourne, Australia. Note the tumor is well circumscribed, cannot be separated from the lateral rectus muscle and molding around normal orbital structure (right globe).

100mg lamictal mastercard
Neisseria gonorrhea or meningiditis strains typically cause a hyperacute conjunctivitis medicine game generic lamictal 50mg online, with copious purulence, and the organism can even penetrate into the globe through a nonulcerated cornea. Chlamydia is an obligate intracellular parasite that is responsible for several forms of conjunctivitis, including trachoma, adult inclusion conjunctivitis, neonatal inclusion conjunctivitis, and lymphogranuloma venereum. Adult inclusion conjunctivitis is a sexually transmitted infection, characterized by a follicular conjuncitivitis that is either unilateral or bilateral, and often has associated lymph node enlargement (preauricular or submandibular). Neonatal inclusion conjunctivitis is a follicular conjunctivitis resulting from the organism being transmitted to the newborn through the birth canal. Lymphogranuloma venereum is a sexually transmitted chlamydial disease that occurs in tropical regions (also called tropical bubo). It is characterized by genital infection with ulceration and subsequent painful lymph node enlargement with lymphadenitis as the organism multiplies within the lymph node. Trachoma is the most common chlamydial eye disease, and is the leading cause of infectious blindness in underdeveloped countries. The sequelae of conjunctival scarring and trichiasis can lead to blinding corneal opacification. The severity of trachoma as graded by MacCallan,15 is based on the maturity of conjunctival follicles and the presence of conjunctival scarring. Examination of conjunctival epithelial cells at this stage show cytoplasmic perinuclear inclusions. Histopathology of the entropion in trachoma shows contraction of a subepithelial fibrous membrane. Noninfectious causes of conjunctivitis includes acute or chronic inflammations due to mechanical causes. Allergic/vernal conjunctivitis is characterized by a follicular reaction of the palpebral conjunctiva, with possible limbal involvement (gelatinous follicles circumferentially surrounding the cornea). An allergic response to an antigen can result in an elevated conjunctival nodule called a phlyctenule, consisting of lymphocytes, histiocytes, and plasma cells. Note the acanthosis and development of epidermal-like rete pegs in the conjunctival mucosa at the lid margin. Mechanical causes of conjunctivitis include floppy eyelid, ectropion, ocular prostheses, or contact lens wear. Floppy eyelid is a condition sometimes associated with obesity, whereby the eyelid tarsus demonstrates laxity and ease in everting, exposing the conjunctiva to mechanical irritation during sleep. The patient presents with a papillary conjunctivitis that may be bilateral or unilateral, and involves predominantly the upper eyelid. Ocular prostheses or contact lenses can be a cause of chronic giant papillary conjunctivitis, from the mechanical irritation of the prosthesis rubbing on the eyelids, or a chronic reaction to lens proteins deposited on contact lenses. Histologically, both lesions show an accumulation of basophilic and amorphous or finely granular degenerated collagen interspersed with coiled or fragmented fibers resembling abnormal elastic tissue (elastase-resistant elastic stain-positive material). The pathogenesis appears to be related to actinic exposure; however, abnormalities of the p53 protein have also been demonstrated. All patients with conjunctival amyloid should be evaluated for possible plasma cell dyscrasias. Conjunctival biopsy samples may demonstrate ultrastructural abnormalities in several lysosomal storage diseases before clinical signs appear. In cystinosis, water-soluble cystine crystals are present in the subepithelial connective tissue of the conjunctiva. Because these crystals dissolve in aqueous solutions, the conjunctival biopsy must be fixed in absolute alcohol or processed by frozen section. Lastly, diseases with metabolic abnormalities of calcium and phosphate can be associated with calcareous deposits in the superficial conjunctival stroma. Patients with sarcoidosis may have clinically identifiable conjunctival nodules that, at histopathologic examination, demonstrate noncaseating granulomas. Biopsies taken from areas of conjunctiva without clinically apparent nodules, result in a much lower diagnostic yield. Subepithelial fibrosis, goblet cell loss, and keratinization may follow, leading to symblepharon formation. Dermatologic manifestations are noted in 21% and oral mucosa lesions in 50% of patients. The bullae may undergo spontaneous regression but often leave a scar, with loss of goblet cells and symblepharon formation. The condition was described initially in descendents of native American and black ancestors from northeastern North Carolina, but has since been documented in patients from Texas and Georgia. The average age of incidence is decades lower in climates located closer to the equator. Histopathologically, they are composed of fibrovascular fronds covered by acanthotic squamous epithelium. Epidermal inclusion cyst (a) A discrete clear-fluid filledlesion of the bulbar conjunctiva. The intracytoplasmic mucin vacuoles stain positively with the alcian blue or mucicarmine stain. Subepithelial and compound nevi are similar in their clinical and histologic features. Subepithelial and compound nevi typically elevate the conjunctival surface, whereas junctional nevi such as those in primary acquired melanosis characteristically do not thicken the conjunctiva. The malignant potential of nevi also varies in that junctional and compound nevi have a low malignant potential whereas the subepithelial nevus usually remains benign. Acquired melanosis manifests in adults as stippled brown conjunctival pigmentation. The brown pigmentation of the basal layers of the epithelium is related to cytoplasmic melanin. At histopathologic examination of the acquired melanosis lesion, few to many melanocytic cells may be found in the junctional area of epithelium. However, if these cells appear markedly atypical or there is evidence of superficial invasion into the substantia propria, the diagnosis of malignant melanoma must be considered. This is especially true when epithelioid cells are noted or basilar hyperplasia is not prominent. Other adverse factors include involvement of the palpebral, caruncular, or forniceal conjunctiva and invasion of the episclera, sclera, or cornea. Note also the pagetoid spread of melanoma cells highlighted in the epithelium (arrows Immunohistochemistry has confirmed that the spindle-shaped cells have an endothelial origin. Mucosa-associated lymphoid tissue lymphoma has been described in the conjunctiva on the basis of microscopy, immunophenotyping, and gene rearrangement analysis involving oncogenes bcl-1, bcl-2, and c-myc. In one reported study, however, there was light chain restriction in three patients without evidence of oncogene rearrangement. Sebaceous carcinoma of the upper and lower eyelids with diffuse pagetoid spread-like conjunctiva and cornea. Malignant lymphoma of the conjunctiva has a better prognosis than lymphoma of the orbit and eyelid. The ground substance, composed of glycoprotein and mucoprotein, coats each collagen fibril. Corneal transparency is maintained by the uniform size and parallel array of collagen fibrils, avascularity, regularity of the epithelial surface, and deturgescence. Anomalies of Corneal Size and Shape Microcornea Microcornea is characterized by <10 mm in greatest diameter at birth. Autosomal dominant, recessive, and X-linked modes of inheritance have been described. When megalocornea is associated with enlarged anterior segment structures, the condition is called anterior megalophthalmos. Iris: Iridocorneal adhesions (vascularized iris strands extend from the anterior iris surface to the central posterior cornea) 4. Lens: Anterior polar cataract, lenticulocorneal adhesion Cornea plana See section on Anterior Segment Dysgenesis.
