

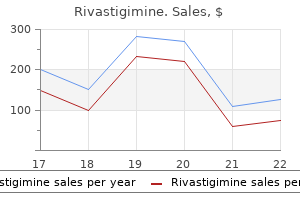
Buy 1.5 mg rivastigimine with mastercard
The findings are usually transient and segmental symptoms miscarriage rivastigimine 1.5mg without prescription, returning to normal after an acute attack. A high degree of clinical suspicion is needed, particularly in patients using angiotensinconverting enzyme inhibitors and a variety of other medications, in the setting of typical imaging findings. Duodenal diverticula are relatively common and have been found in up to 5% of the population undergoing barium studies. Jejunoileal diverticula are less common but usually multiple and localized to the proximal jejunum. They are frequently associated with disorders of intestinal motility such as scleroderma and visceral neuropathies. Complications are more common in jejunoileal diverticula than duodenal diverticula and, similar to their colonic counterpart, include bleeding, intestinal obstruction, and diverticulitis. It is a true diverticulum that contains all layers of the intestinal wall and has its own blood supply. It results from incomplete absorption of the omphalomesenteric duct and is frequently associated with heterotopic gastric or pancreatic mucosa in up to 50% of cases, with gastric heterotopia being most common. It is typically located in the distal ileum approximately 2 feet from the ileocecal valve. Although usually asymptomatic, approximately 2% of patients can present with complications, more common in children than adults. Computed tomography diagnosis relies on the identification of a blind-ending, tubular, round, or oval structure in the right lower quadrant or periumbilical region, with surrounding inflammation. The diverticulum can be associated with mural thickening and hyperenhancement, with focal calcifications at the base (enteroliths), and adjacent mesenteric fat stranding and fluid collections. In some instances the diverticulum will extend Celiac Disease Celiac disease in now recognized as a common but largely underdiagnosed disease, with typical diagnostic delay of more than 10 years from the onset of symptoms. It is a chronic autoimmune disorder induced in genetically susceptible individuals after ingestion of gluten proteins. The small bowel mucosa is primarily affected, resulting in progressive villus inflammation and destruction, with resulting induction of crypt hyperplasia. It may be asymptomatic or characterized by diverse symptoms of malabsorption with varying severity. Characteristic findings include duodenitis with dilution, slow transit, and flocculation of oral contrast, small bowel dilation, transient small bowel intussusception, villous atrophy and reversal of the fold pattern, with jejunization of the ileum, as reflected by a decrease in normal jejunal folds in contrast to the increasing fold pattern in the ileum. Whipple Disease Whipple disease is a rare multisystemic bacterial infection caused by the Whipple bacillus (Tropheryma whipplei), involving the small bowel (particularly the jejunum), lymph nodes, joints, and central nervous system. Barium studies can demonstrate to better extent the thickened, irregular folds and tiny nodules in the jejunum and, to a lesser degree, the ileum, due to accumulation of the Whipple bacilli and periodic acid-Schiffpositive macrophages in the submucosa and lamina propria. Whipple disease is an infectious condition, and these patients often demonstrate significant response to treatment with antibiotics. Bowel angioedema was suggested because of the imaging appearance in combination with use of an angiotensin-converting enzyme inhibitor and a history of prior episodes of facial angioedema. The identification of a normal appendix can be very helpful because patients will often present with right lower quadrant pain. It can cause bowel wall thickness of 1 cm or more, but it will often extend for less than 15 cm in length. Other Inflammatory Conditions of the Small Bowel There are numerous additional inflammatory conditions of the small bowel that will present with nonspecific bowel wall thickening, including eosinophilic gastroenteritis, amyloidosis, Behзet syndrome, and primary lymphangiectasia. Differentiation will depend on the clinical history, distribution pattern, and often biopsy. This section will review the pathophysiology and pertinent imaging features of nontraumatic emergencies that affect the colon and the appendix. Initially the appendiceal lumen becomes obstructed by fecal material (appendicolith or fecalith), undigested material such as vegetables or seeds, hypertrophied Peyer patches, or neoplasm, and progressive accumulation of secretions leads to intraluminal distention and increased intramural pressure. The initial periumbilical abdominal pain represents referred pain from visceral innervation due to appendiceal luminal distention, and localized right lower quadrant pain is secondary to inflammation of the parietal peritoneum. Ongoing luminal distention and bacterial overgrowth result in lymphatic and venous obstruction leading to mucosal ischemia. Plain abdominal radiographs have limited utility in the diagnosis of acute appendicitis. However, appendicoliths may be seen on abdominal radiographs and, in the appropriate clinical setting, are suggestive of acute appendicitis. In addition, free intra-abdominal air and bowel obstruction may readily be excluded on plain abdominal radiographs. In cases in which positive oral contrast agents are administered, opacification of the appendiceal lumen with oral contrast effectively excludes a diagnosis of appendicitis. However, the converse does not hold true, and a lack of appendiceal opacification with oral contrast material does not definitively indicate a diagnosis of acute appendicitis because this is often the case with normal appendices. Diverticular disease is the most common pathologic process that involves the colon, with the sigmoid colon most commonly affected in up to 90% of the population. Initially the neck of a colonic diverticulum becomes obstructed by stool, undigested food particles such as seeds, or inflammation, eventually resulting in microscopic or macroscopic perforation and inflammation, contamination, and infection of the pericolic fat. Patients with acute diverticulitis typically present with left lower quadrant pain and fever. Less common signs and symptoms include nausea, vomiting, constipation, and urinary symptoms. Importantly, the location of the abdominal pain varies depending on the segment of colon that is affected. On imaging, acute diverticulitis may yield abnormalities on abdominal radiographs, including pneumoperitoneum, bowel obstruction, or the presence of a focal region of increased soft tissue density related to the presence of an abscess. In pregnancy, intravenous gadolinium should not be administered for this application and the utility of oral contrast is a subject of ongoing investigation. Appendectomy is the treatment of choice in simple acute appendicitis, and laparoscopic appendectomy is increasingly common. Antibiotic treatment for small abscesses is feasible, whereas image-guided percutaneous drainage may be performed for larger abscesses. Acute Colonic Diverticulitis Acute diverticulitis results from the obstruction and subsequent perforation of a colonic diverticulum. Complications, including diverticular perforation with frank abscess formation, fistulas. A pericolic abscess appears as a hypoattenuating, pericolic collection with peripheral enhancement, often containing air or an air-fluid level. Acute diverticulitis represents the most common cause of vesicocolonic fistulas, which often occur along the left posterolateral aspect of the bladder in cases of sigmoid diverticulitis and may be suspected based on the presence of intravesicular air and focal bladder wall thickening adjacent to an inflamed diverticulum. Treatment options in cases of acute diverticulitis range from conservative management with antibiotics and bowel rest to emergent surgery in cases of complications. An important differential diagnostic consideration in patients with focal colonic wall thickening includes colon carcinoma, which may have similar imaging findings to that of acute diverticulitis. Marked wall thickening out of proportion to the degree of pericolic inflammation, obliteration of the expected mural enhancement pattern of the colon, the presence of mesenteric lymphadenopathy, and acute bowel obstruction are imaging findings that are suggestive of colonic carcinoma. In contradistinction, the presence of fluid within the root of the sigmoid mesentery, visualization of an offending diverticulum, preservation of the expected mural enhancement pattern, and a relatively long segment of circumferential colonic wall thickening favor the diagnosis of acute diverticulitis. Presenting symptoms typically include acute onset of crampy abdominal pain and tenderness and watery or bloody diarrhea. Additional signs and symptoms include fever, rash, nausea, vomiting, headache, malaise, and weight loss. Patients with infectious colitis may be found to have electrolyte imbalances and leukocytosis. Bacterial causes of infectious colitis include Salmonella, Shigella, Campylobacter, Yersinia, Staphylococcus, E. Viral organisms known to cause colitis include herpes, cytomegalovirus, Norwalk virus, and Rotavirus, and associated fungal organisms include Histoplasma and Mucor. Finally, parasitic infections known to cause colitis include Entamoeba histolytica, Schistosoma, Strongyloides, Trichuris, and Anisakis, all of which are more commonly seen in underdeveloped countries. Some of the more commonly encountered causes of infectious colitis include Campylobacter jejuni, Yersinia enterocolitica, Salmonella typhi, and Clostridium difficile.
Purchase discount rivastigimine
Patients with preoperatively identified disease in the lateral part of the neck are generally cured with total thyroidectomy and neck dissection medications drugs prescription drugs cheap rivastigimine 3 mg. Thyroid and neck surgery should not be considered in the setting of distant metastatic disease. Food and Drug Administration approval for use in patients with advanced medullary thyroid cancer. Preoperative localization of parathyroid glands offers little in surgical planning. In primary hyperparathyroidism, a drop in intraoperative parathyroid hormone levels to less than 50% of the highest preexcisional levels predicts a 97% cure rate. All four glands should routinely be explored in multiple endocrine neoplasia syndromes. A lateral approach to the posterior aspect of the thyroid may facilitate access in revision parathyroid surgery. The presence of hypercalcemia and a palpable neck mass are suggestive of parathyroid carcinoma. During surgery parathyroid carcinoma should be carefully dissected from the ipsilateral thyroid lobe. There is evidence of distant disease, but biopsypositive nodes are present in the central part of the neck. Select from the list below the initial surgical therapy most appropriate for the following patients. From the following imaging techniques, select the most appropriate initial investigation(s) for localization of a hyperfunctioning parathyroid gland. A is the percentage of thyroid cancers that are follicular carcinoma; B is the mortality from thyroid cancer. From the following options, identify those features that are an indication for sternotomy when resection of a substernal goiter is planned. The following responses relate to the anatomy and embryology of the thyroid and parathyroid glands. Ventral to the recurrent laryngeal nerve (a) this is the point of origin of the thyroid in the embryo. For Questions 59 through 63, select the correct thyroidectomy surgical technique(s) from the following list. Which technique(s) have been associated with reduced rates of recurrent nerve injury? Which technique(s) are oncologically sound management of the thyroid gland in the cancer setting? Should be excised with preservation of the laryngeal framework and treated with postoperative external beam radiation therapy. Which technique(s) have been associated with increased rates of recurrent nerve injury? Should be excised with preservation of the laryngeal framework and treated with postoperative radioactive iodine. Should be managed with complete resection with negative margins so that uncontrolled disease in the central part of the neck is avoided. Should remain under observation until nodular disease is identified in the thyroid gland. Patients with medullary thyroid cancer that is unresectable or distantly metastatic and who have evidence of disease progression A. The prognosis of patients with unresectable medullary cancer is best assessed with the use of A. In patients with differentiated thyroid cancer that presents with lateral neck node metastases, the levels that should routinely be included in a therapeutic lateral neck dissection are A. Unifocal T2 lateralized well-differentiated thyroid cancer, in order to protect the contralateral nerve B. In regions of the world where there is little access to thyroid hormone replacement D. In patients with differentiated thyroid cancer metastatic to the lateral side of the neck, which preoperative investigation should be considered routine? Which of the following side effects is associated with the administration of radioactive iodine? From the mastoid tip, parallel with the trapezius, to the inferior part of the neck, then within a skin crease at the level of the cricoid cartilage. From the mastoid tip to the cricoid cartilage with a "lazy S" extension to the clavicle. In two parallel skin creases two fingerbreadths below the mandible and two fingerbreadths above the clavicle. Access to level V during a therapeutic neck dissection for thyroid cancer without overt nodal disease in the posterior triangle A. Is obtained by extending the incision to the anterior border of the trapezius laterally. Is obtained by dissecting posterolaterally under the sternomastoid muscle and retracting the nodal tissue from behind the muscle. Requires division of the accessory nerve to ensure a comprehensive nodal dissection. In patients with papillary thyroid cancer and without evidence of central neck metastases at presentation, management of the neck with observation rather than elective central neck dissection results in what percentage of cases requiring further central neck surgery in the subsequent 10 years? When treatment options are considered in patients with T4 differentiated thyroid cancer with distant metastases, what percentage will still be alive after 5 years if adequate surgical resection of the primary tumor is performed? Elective central neck dissection in differentiated thyroid cancers has been shown to result in A. The disease that presents most commonly to surgeons as metastatic disease to the thyroid is A. Extrathyroidal extension that is not evident in the operating room but that is identified microscopically on histopathological examination A. Which statement about radioactive iodine avidity in thyroid cancers of follicular cell origin is true? Which of the following areas is a common site for nodal metastases from thyroid cancers? Papillary thyroid metastasis to the Delphian nodes has been shown to be associated with A. Factors that have been shown to predict the risk of postthyroidectomy hematoma include the A. During follow-up of low-risk differentiated thyroid cancers, serial thyroglobulin monitoring A. Which treatment modality is most effective for managing recurrent nodal disease in differentiated thyroid cancer? Which of the following factors is not an independent predictor of survival in differentiated thyroid cancer? Which of the following features is suggestive of malignancy in a parathyroid lesion? The next step in managing a patient with normal clinical examination results and a rising thyroglobulin level after surgery for thyroid cancer is A. Which of the following statements about targeted therapy in medullary thyroid cancers is true? The most important differential diagnosis in patients with suspected anaplastic thyroid cancer is A. B Core Knowledge · the incidence of thyroid cancer is rising in the United States and around the world. In the event of stable distant disease and progressive local disease, aggressive surgery in the central area of the neck may prevent complications such as asphyxia and provide meaningful quality of life. Disease in the central part of the neck should be approached with central neck dissection and a low threshold for lateral neck dissection if lymphadenopathy suggestive of cancer is encountered. However, if the disease is incurable, a tradeoff must be made between preventing complications from disease and causing complications with surgery.
Discount 1.5 mg rivastigimine overnight delivery
The child is asked to lift both arms above the shoulder and place the palms behind the head Feel for effusion of the knee Ask the child to bend and then straighten your knee and feel for crepitus Apply passive flexion (90°) with internal rotation of hip and then external rotation Observe the spine from behind Ask the child: Can you bend and touch your toes? These tests are further detailed in the Chapter on Developmental Dysplasia of the Hip section 8 medications order rivastigimine with paypal. The Barlow-Ortolani maneuvers are useful during the neonatal period but are not as reliable in older children. Beyond 36 months of age, secondary contractures of the capsule, ligaments and adductor muscles cause limitation of hip abduction. A 3-Year-Old Boy with Intoeing Gait and Frequent Falls History It is fairly common for children in this age group to trip and fall frequently but this could also be the first indication of an underlying disorder such as a neuromuscular disorder or cerebral palsy. One should look for other features of development delay such as retention of primitive reflexes and cognitive delay. In most toddlers, the intoeing gait is first noticed by grandparents, neighbors or staff at the nursery/playgroup. Parents are usually aware of whether the problem is unilateral or bilateral and whether it is improving. Intoeing gait that is bilaterally symmetrical indicates a physiological normal variant in this age group. The parent is then asked to walk the child around the waiting area or a quiet corridor. By the age of about 30 months, most children have relatively symmetric gait with greater time spent in stance phase (approximately 60%). Intoeing gait occurs principally at three levels, namely (1) the femur, (2) tibia and (3) foot. The relative alignment of the lower limb in the axial plane is called torsional profile and must be assessed in every child. The degree of internal and external rotation of the hip indicates the amount of femoral anteversion. Femoral version is the angle made by the proximal femur in relation to the distal femur. It reduces over the first 2 years of life to the normal adult anteversion of 1015°. Tibial torsion (rotation of the tibia along its axis) is internal at birth and becomes external over the first 23 years of life. Physiological foot deformities such as metatarsus adductus can also cause intoeing gait. A 20-Month-Old Girl Presents with Bowed Legs (Genu Varum) History It is important to establish when the deformity was first noticed and whether there has been any progression over a period of time. The birth and developmental history are typically normal, though in cases of skeletal dysplasia there may be short stature and growth retardation. History of similar complaints in family members may be significant in this context. Clinical features of rickets such as expansion of the long ends of bones (wrists) may be present. The spine, hips and arms are examined to rule out the possibility of skeletal dysplasias such as spondyloepiphyseal dysplasia. In the age group of 47 years, Perthes disease must be considered in the differential diagnosis of a painful limp. History Children develop a mature, reproducible gait pattern at around 7 years of age. The onset, duration, progression and severity of the pain/limp provide important clues as to the diagnosis. In transient synovitis, the child typically has been limping for a day or two, though they may stop walking altogether for a brief period. Bone or joint infection has a sudden onset with rapid progression associated with systemic symptoms and highgrade fever (> 38. Children with transient synovitis usually walk into the examination room but may have a slight limp, whereas a child with septic arthritis will be carried or brought in a wheelchair. The limb is usually in an attitude of slight flexion, abduction and external rotation at the hip thus maintaining the hip capsule in maximal relaxation. Restriction of internal rotation of the hip is an early and sensitive sign of hip pathology. But, a flatfoot may be first sign of intrinsic foot pathology such as tarsal coalition or neurological disorders (spinal dysraphism). If pain is present, the nature and severity of pain helps differentiate mechanical problems from sinister pathology. Children in this age group (47 years) frequently suffer from bilateral calf pain in the evenings. This has been termed growing pains, though the exact cause is yet to be fully understood. The clinical evaluation must focus on ruling out less common but serious causes which may require emergent treatment. Referred pain from the hip must be considered in every child presenting with knee pain. Anterior knee pain has typically been present for several months without any antecedent history of trauma. Night pain should raise the rare possibility of an osteogenic sarcoma or other bone tumors which occur around the knee. Mechanical symptoms such as locking and of the knee following trauma point to tears of the menisci or cruciate ligament. The hindfeet are normally in slight valgus at rest and move into varus on tiptoeing. In the presence of any bony pathology such as tarsal coalition or if there is a neuromuscular disorder, the hindfoot (heel) remains in valgus due to stiffness in the subtalar joint or due to a fixed valgus hindfoot deformity. Passive range of movement in the ankle and subtalar joints is within normal limits. The metatarsophalangeal joint of the big toe is dorsiflexed which also restores the arch (Jack test). Examination of the spine is essential since children with unilateral foot deformity may have otherwise asymptomatic intraspinal lesions such as a cord tumor or spinal dysraphism. The leg may be externally rotated when lying down and an external foot progression angle may be present when walking. Small amounts of effusion in the knee can be appreciated by squeezing the suprapatellar pouch and looking for fullness over the medial aspect of the knee. The medial, lateral and patellofemoral joints are palpated for crepitus and tenderness. A 12-Year-Old Boy with Left Knee Pain and Limp for 2 Months Knee pain is common in the adolescent age group. Evaluation of the locomotor system in a child could be a screening examination or a focused assessment based on the clinical scenario. Detailed history and systematic physical examination of the affected joint(s) are crucial in generating a differential diagnosis. There are a number of abnormal gait patterns in children, knowledge of which can direct the examination towards the affected joint. The pediatric Gait, Arms, Legs, and Spine is a quick and useful assessment tool in the evaluation of school-going children. Pediatric regional examination of the musculoskeletal system: a practice- and consensus-based approach. Over the last few years, the incidence of osteomyelitis has decreased in developed countries, but we still continue to deal with both childhood and adult osteomyelitis in India. Osteomyelitis also can occur after open fractures due to direct contamination from the surroundings. In diseases like sickle cell anemia, there occur vascular infarcts along the shaft of the bone with resultant avascular segments which act as good media for bacterial growth. Although avascularity itself is not an infection, there can be seeding and this can result in diaphyseal osteomyelitis which is typically seen in sickle cell disease. In older children, Streptococcus pyogenes, Streptococcus pneumoniae and Kingella kingae are increasingly seen. Also, they seem to have a recent history of varicella infection though the exact reason for this association is not known. It occurs usually in day care centers and crиches and is preceded by an upper respiratory tract infection.

Rivastigimine 1.5 mg with mastercard
United Nations General Assembly defines a "child" as a person below the age of 18 years medicine 031 6 mg rivastigimine visa. These rights are binding to the nations; children are not mere passive holders of these rights. Despite constitutional provisions for protection of children in India, the ground reality for their health, education, early childhood care, and protection is not satisfactory. National Policy and Charter for Children, 2001 for India ensures that every child enjoys his/her rights as described in the Convention on Rights of the Children. The Juvenile Justice Care and Protection of the Child Act, 2000 of India aims to target children in need of care and protection; and juveniles in conflict with law. Vulnerable Children Child Line this is a national helpline for children in distress. It operates through a national toll free number 1098 and responds to the urgent and emergency needs of children such as medical assistance, shelter, protection from abuse and exploitation, assistance in child missing cases, repatriation, sponsorship, etc. Indicators are markers of health status, service performance or resource availability defined to enable the monitoring of objectives, targets and performance. It comprises of four intervention areas including family planning, maternal and newborn care, immunization, and treatment of sick children. In this chapter, however, we shall concentrate on indicators primarily related to child health. Perinatal mortality and neonatal mortality reflect the health and care of women during pregnancy and perinatal period, whereas infant mortality has been described as one of the most sensitive indices of health and quality of living of a population. South-East Asia accounts for 28% of all child deaths; another 40% under-5 deaths occur in Africa. More than 10 million children are still dying every year across the globe before they are 5 years of age in addition to 3 million stillbirths. While prematurity, infections, and asphyxia together contribute to almost 85% of neonatal deaths; conditions responsible for most of postneonatal under-5 deaths include pneumonia, diarrhea, malaria, and measles. About 35% of deaths in children have one or more of the three underlying risk factors: underweight, micronutrient deficiency, and suboptimal breastfeeding. This is irrespective of the fact that some of those infants who died in this year might have been born in the last few months of the previous year. It also reflects income and education of parents, the prevalence of malnutrition and disease, availability of clean water, efficacy of health services, and health and status of women. It is an appropriate indicator of cumulative exposure to risk of death during the first 5 years of life. Under-5 Infant mortality rate of a nation is a well accepted long-standing indicator of wellbeing of her children. Developed countries have shown greater reduction in infant mortality as compared to child mortality; while in the developing countries, the situation is reverse. There is a wide variation in morbidity and mortality pattern of different regions in India. To establish the relative public health importance of the different possible determinants of death 2. To select place and program interventions Measurement of cause specific mortality can serve: 1. To investigate the circumstances surrounding the deaths of children for devising effective action to decrease child mortality 4. To investigate reason for differing rates of infant and child mortality among geographical areas and 5. To evaluate the effectiveness of specific public health interventions in controlled settings To measure cumulative deficient growth associated with long-term factors including: i) chronic insufficient dietary intake, ii) frequent infection, iii) poor feeding practices over a sustained period, and possibly, iv) low socioeconomic status of the household To define the overall magnitude of malnutrition and its changes over time. Wasting could be due to: i) inadequate food intake, ii) illness or infection, or iii) current poor feeding practices Classified as acceptable, poor, serious and critical for the mean weight for height Z-score of Greater than -0. Computed serially, it helps to monitor change in the status of vitamin A in the body Contd. Type of indicator Name of indicator Goiter prevalence rate Definition Proportion of children 611 years (preferably 810 years) of age with goiter of any grade Uses A total goiter rate (goiter grades 1 and 2) of 5% or more in primary children aged 810 years is a signal for a public health problem. When ultrasonography is used to provide a more precise measurement of thyroid volume the indicator becomes significant in monitoring iodine control programs where thyroid volumes are expected to decrease over time 1. Monitoring the impact of neonatal control programs Measles deaths Indicators for treatment of sick children Oral rehydration therapy Care seeking for pneumonia Annual number of deaths due to measles in children under 5 years of age. It can be estimated by the following formula: [infants surviving to 1 year of age] Ч [1- (vaccine efficacy Ч coverage by first birthday) Ч case fatality rate due to measles] Percentage of children under-5 with diarrhea in the preceding 2 weeks who received oral rehydration therapy and continued feeding Percentage of children aged 0-59 months with suspected pneumonia (cough and dyspnea) who sought care from a health provider Useful for: 1. Monitoring the effectiveness of management as well as control measures against measles and 2. To identify areas in need of special attention the indicator should be presented geographically by: 1. Majority of neonatal deaths are accounted for by low birthweight, infections, birth asphyxia, sepsis, and congenital anomalies; whereas postneonatal mortality occurs primarily due to infections (diarrhea, respiratory infections, vaccine-preventable diseases) and malnutrition. Low birthweight (< 2,500 g) as a result of maternal malnutrition, decreased spacing between births, large family size, and a high fertility rate is one of the prime factor resulting in high infant mortality. Non-practicing of exclusive breastfeeding, noncompliance with immunization on account of illiteracy, ignorance, cultural and social beliefs pose the greatest risk of deaths to the infant. Infant Mortality Rate Number of infant dying between birth and exactly 1 year of age expressed per 1,000 livebirths, per year. Neonatal Mortality Rate the number of deaths among livebirths during the first 28 days of life per 1,000 livebirths, per year. Early Neonatal Mortality Rate the number of child deaths less than 7 days of life expressed as per 1,000 livebirths in that reference year. Late Neonatal Mortality Rate the number of child deaths between 7 and 28 completed days of life expressed as per 1,000 livebirths in that reference year. Postneonatal Mortality Rate the number of child deaths of 29 days to less than 1 year of age expressed as per 1,000 livebirths in the reference year. Perinatal Mortality Rate the number of deaths of fetus after 28 completed weeks of gestation plus the number of early neonatal deaths per 1,000 total births, per year. Stillbirth Rate the number of stillbirths per 1,000 births (live and stillbirths) during the reference year. Pediatrics as such is a preventive medicine and prevention starts not after birth but before birth, in utero, and even before pregnancy when prospective mothers are counseled. On a national level, the child health policy needs to be followed politically, emotionally and with national commitment to the rights of children. The greatest risk is within first 24-hour after birth when 2545% of all neonatal deaths occur. Major causes of neonatal deaths in this region are prematurity or low birthweight, infections and asphyxia. Other important causes of mortality are congenital anomalies, neonatal tetanus and diarrhea. Neonatal mortality is a measure of the intensity with which endogenous factors (birthweight, birth injuries) affect life. The high concentration of infant deaths in the early neonatal period with endogenous factors suggests the need to improve the antenatal and postnatal services to expectant mothers. However, neonatal mortality is the most difficult part of infant mortality to alter, because of the endogenous factors which are not sensitive to improvements in environmental conditions. Indices related to neonatal and perinatal mortality are calculated as follows: Neonatal mortality rate It is the number of neonatal deaths in relation to 1,000 livebirths per year. State of the World Children, 2015; *Neonatal and Perinatal Mortality, Country, Regional and Global estimates 2007. Perinatal mortality rate Number of deaths occurring in the perinatal period (includes stillbirths plus the deaths occurring in the first 7 days after birth) in a given year to the total number of births (live and still) in the same year. For the purpose of inclusion in this rate, the stillbirth or livebirths should be either (i) > 1,000 g in weight; (ii) > 28 weeks in gestation; or if (i) and (ii) are not available, should measure 35 cm or more in length at birth. In recent times, stunting has been singled out as key indicator for assessing child nutrition and its consequences. Similarly, exclusive breastfeeding is another important indicator estimated to prevent almost 13% of under-5 mortality.

Diseases
- Eisenmenger syndrome
- Cerebral palsy
- Complex 1 mitochondrial respiratory chain deficiency
- Polycystic kidney disease, type 2
- Neuropathy, hereditary sensory, type II
- Hemi 3 syndrome
Discount rivastigimine 1.5mg
Imaging studies show ductal dilatation symptoms ulcerative colitis generic 4.5mg rivastigimine, pneumobilia, and possibly stones in the common bile duct. There is a lowsignal-intensity focus (arrow) at the junction of the cystic duct and common hepatic duct. Imaging surveillance of patients with recurrent pyogenic cholangitis focuses on the detection of complications: abscess formation, intrahepatic bilomas, portal vein thrombosis, and cholangiocarcinoma. These foci represent hyperemia and are caused by infection of the obstructed biliary tree (ascending cholangitis). Recurrent Pyogenic Cholangitis Recurrent pyogenic cholangitis is a type of infectious cholangitis that occurs most commonly in people from Southeast Asia. Chronic infection with the parasites Ascaris lumbricoides or Clonorchis sinensis and malnutrition are predisposing factors, by promoting the calcium formation of pigmented stones. Bacterial superinfection ensues, and affected patients present with recurrent episodes of ascending cholangitis. Recurrent inflammation leads to the development of chronic complications such as fibrosis with strictures, parenchymal disruption and cirrhosis, hepatic abscesses, portal hypertension, and cholangiocarcinoma. Initially there is an obstruction of the lymphatic supply, which causes an increase in capillary pressure and massive edema of the ovaries. Risk factors include pregnancy, dermoid cyst, hemorrhagic cyst, and ovarian hyperstimulation syndrome. Some studies have hypothesized that the right ovary is more susceptible to torsion due to the fact that the sigmoid colon forms a protective barrier on the left side. The clinical presentation of ovarian torsion is nonspecific, and the condition is generally included in the differential diagnosis of acute abdominal and pelvic pain. Symptoms include nausea, vomiting, sharp right or left lower abdominal pain, and tenderness. Patients may complain of constant or intermittent abdominal pain depending on whether there is complete torsion or a torsion/detorsion of the adnexa. Ultrasound (transvaginal and transabdominal) is the primary modality used for the evaluation of patients with adnexal torsion. In addition, there is associated free fluid within the cul-de-sac in almost 90% of cases. In addition to evaluating the symptomatic side, an examination of the contralateral side is recommended for comparison. On color Doppler imaging the classic appearance is the complete absence of arterial flow, but this is present in only a minority of cases. Lee and colleagues described a finding, which incorporates both the gray-scale and color Doppler ultrasonographic features, that is known as the twisted pedicle or the whirlpool sign. B, Spectral Doppler images of the right adnexa demonstrate dampening of the venous waveforms, which is consistent with a torsion-detorsion of the right ovary. The most common organism is Chlamydia trachomatis; others include Neisseria gonorrhoeae, Haemophilus influenzae, Gardnerella vaginalis, enteric gram-negative rods. Tubo-ovarian abscesses are often polymicrobial and may involve both anaerobic and coliform bacteria. Viruses, including herpes simplex virus 2 and cytomegalovirus, have also been found to sometimes be implicated in the process. Additional signs of lower genital tract infection that increase specificity of diagnosis include cervical friability, vaginal or cervical discharge, fever, elevated erythrocyte sedimentation rate or C-reactive protein level, or laboratory evidence of presence of C. Salpingitis represents the next level of disease progression, with involvement of one or both fallopian tubes. Findings on imaging may be subtle and limited to thickening and hyperemia of the tubal walls. Tubo-ovarian complex and tubo-ovarian abscess occur when the infection extends beyond the fallopian tube to involve the ovary and regional pelvic structures. In addition to the imaging findings associated with salpingitis or pyosalpinx, tubo-ovarian complex demonstrates an adherent adjacent ovary, which is no longer freely mobile under transvaginal transducer probe pressure. The term abscess is a misnomer because in most cases of tubo-ovarian abscess the fluid and debris are predominantly contained within a distended but anatomically intact space (the fallopian tube) and do not represent the organization of infectious fluid and debris seen in a typical abscess. Following resolution of the acute infection, a hydrosalpinx may form in which the fallopian tube remains distended with sterile watery fluid following proteolysis of pus. Patients typically present with diffuse abdominal pain, abdominal distention, ascites, moderate to large pleural effusions, and hemoconcentration. There is also free fluid, which may be simple ascites but can be higher in attenuation due to a ruptured hemorrhagic cyst. Differential considerations for pelvic pain in a pregnant woman include normal early intrauterine pregnancy, spontaneous abortion, and ectopic pregnancy. Ectopic pregnancy is the leading cause of first-trimester pregnancy-related mortality. The overall incidence of ectopic pregnancies was 2% in 1992 and has since increased to approximately 4. Early diagnosis and treatment are crucial because the risk for rupture increases as the ectopic pregnancy enlarges. C, Right adnexal mass with a yolk sac (arrow) is visualized, consistent with an ectopic pregnancy with hemoperitoneum. In a normal intrauterine pregnancy, the first ultrasonographic sign is the intradecidual sign, typically seen at 4 menstrual weeks. At 5 weeks, a double-decidual sac sign can be visualized that manifests as two concentric hyperechoic rings surrounding an anechoic gestational sac. The double-decidual sac sign must be differentiated from a pseudogestational sac, which is a focal intrauterine fluid collection surrounded by decidual reaction located centrally in the endometrial cavity. Fetal cardiac activity is typically seen at 5 to 6 weeks, when the gestational sac measures 18 to 20 mm or when the fetal pole measures at least 5 mm. On imaging, ectopic pregnancies have varying appearances depending on the location. Locations of ectopic pregnancies include tubal, interstitial, ovarian, scar, cervical, intra-abdominal, and heterotopic. Tubal pregnancies account for a majority (approximately 95%) of ectopic pregnancies and occur in the ampulla (75% to 80%), isthmus (10%), and fimbria (5%). Another sign of tubal ectopic pregnancy is the "ring of fire" seen as peripheral hypervascularity in color Doppler evaluation of the extraovarian adnexal mass, related to high-velocity, low-impedance flow. Although this can be seen in tubal ectopic pregnancies, the ring of fire is not specific because it can also be seen in corpus luteum cysts. Additional intrauterine findings include the previously mentioned pseudogestational sac and decidual cysts. Decidual cysts are thin-walled, simple cysts located at the junction of the myometrium and endometrium and tend to be multiple. Interstitial ectopic pregnancies are rare, accounting for 2% to 4% of all ectopic pregnancies. They occur when the blastocyst implants in the intramyometrial segment of the fallopian tube. Interstitial ectopic pregnancies carry higher mortality and morbidity rates because of later presentation in pregnancy and the potential for massive hemorrhage given the close proximity of the uterine artery. The most common predisposing condition is the bell clapper deformity, which is a congenital anomaly in which the testicle and epididymis are nearly completely surrounded by the tunica vaginalis, leaving the support structures and epididymis prone to twisting. The rate of testicular salvage is inversely proportional to the duration of ischemia, and delays in appropriate treatment increase the risk for infarction. In cases where there has been detorsion, increased testicular blood flow from postischemic hyperemia can be seen and can be misinterpreted as epididymo-orchitis. Patient was found to have a complete testicular torsion, and orchiectomy was necessary. Epididymo-orchitis the most common cause of acute scrotal pain is epididymo-orchitis, which accounts for 75% of all scrotal inflammatory processes. Epididymo-orchitis most commonly results from bacterial seeding or ascending infection of the genitourinary tract. Because the route of spread is ascending from the genitourinary tract, the tail of the epididymis is initially affected with spread of infection through the tail into the testicle, resulting in orchitis. The contralateral epididymis and testis can be used as direct comparison of size, echogenicity, and vascularity. Accurately differentiating between acute testicular torsion and epididymo-orchitis has important therapeutic implications, and it is imperative to prevent potential complications in both diagnoses.
Discount rivastigimine 4.5 mg without prescription
Cetuximab plus radiation therapy was superior to cisplatin plus radiation therapy in terms of the larynx preservation rate symptoms 4 days post ovulation order rivastigimine with visa, although overall survival rates did not differ between the two arms. Patients with low levels of dihydropyrimidine dehydrogenase are at increased risk of severe toxicity when treated with A. In the Intergroup Study for patients with locally advanced (M0) head and neck cancer conducted by Adelstein and colleagues, treatment with concurrent radiation plus cisplatin was associated with A. An increased incidence of acute toxic effects (including mucositis and nausea/vomiting). Which of the following targeted agents has received regulatory approval by the Food and Drug Administration of the United States for the treatment of head and neck cancer? A 31-year-old woman has undergone resection of an adenoid cystic carcinoma of the submandibular salivary gland. With two more cycles of induction chemotherapy if there was less than a complete response, and then to repeat the response assessment to guide subsequent locoregional therapy. Which of the following strategies has been shown to reduce the risk of second primary tumors in patients with head and neck cancer? The available data from randomized prospective clinical trials of standard cisplatin-based chemoradiation therapy for head and neck cancer indicates that the incidence of early treatment-related death is approximately A. Which of the following was not a finding of the Head and Neck Contracts Program Trial? A significantly improved disease-free survival rate was seen in the neoadjuvant therapy arm. A higher objective response rate but no significant difference in the median overall survival rate B. An improved median overall survival rate but increased treatment-related mortality C. A higher objective response rate and significantly improved median overall survival and improved median progression-free survival rates D. An improved median progression-free survival rate but no significant improvement in the overall survival rate 88. Which of the following toxic effects are most typically associated with cetuximab monotherapy? In a subset analysis of patients who had received at least one prior cytotoxic regimen for recurrent or metastatic disease, the objective response rate was higher in the cisplatin plus cetuximab arm. In a subset analysis of patients who had received at least one prior cytotoxic regimen for recurrent or metastatic disease, the overall survival rate was higher in the cisplatin plus cetuximab arm. In the cetuximab plus cisplatin group, the objective response rate was higher among patients who experienced skin toxic effects. Cetuximab plus radiation therapy is appropriate because the study by Bonner and colleagues showed improved outcomes for patients with renal insufficiency with this regimen. In the study of radiation therapy plus concurrent cetuximab by Bonner and colleagues, cetuximab adverse events included a A. Identified patients with high-risk features in surgical pathological specimens in a retrospective analysis. Treatment was complicated by diarrhea and mucositis that required hospitalization but now have resolved. In planning a second cycle, dose modification in which of the following drugs would be most appropriate? In the Southwest Oncology Group study by Forastiere and colleagues that randomly assigned 277 patients with advanced head and neck cancer to three different treatment regimens, A. A significantly improved overall survival rate but only a trend toward improved 2-year locoregional control. Improved 2-year locoregional control and a significantly improved overall survival rate. A trend toward an improved survival rate but no increase in incidence of grade 3 toxic effects. Premedication with steroids before infusion is required to reduce the risk of an anaphylactic reaction with which of the following chemotherapeutic agents? He has no significant medical comorbidities and wishes to be maximally aggressive to improve his chance of durable disease-free survival. For his situation, which of the following concurrent chemotherapy regimens is best supported by data from prospective randomized clinical trials? Core Knowledge · Chemotherapy may be given before definitive radiation therapy (induction chemotherapy), during radiation therapy (concurrent chemoradiation therapy), or after radiation therapy (adjuvant chemoradiation therapy) in selected patients. Cetuximab, a novel chimeric antibody directed against the epidermal growth factor receptor, is the only molecularly targeted agent that is currently approved for the treatment of head and neck cancer. Taxanes are metabolized by the liver and not administered in patients with significant liver dysfunction. A small risk of a severe allergic-type hypersensitivity reaction also exists during the first exposure to cetuximab. There was a higher objective response rate, improved median overall survival rate, and improved progression-free survival rate. However, the application of concurrent cisplatin with postoperative radiation therapy intensifies acute toxic effects. Chemoradiation after surgery for high-risk head and neck cancer patients: how strong is the evidence? Randomized trial of radiation therapy versus concomitant chemotherapy and radiation therapy for advanced-stage oropharynx carcinoma. Final results of the 9401 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. A randomized prospective comparison of methotrexate with a combination of methotrexate, bleomycin, and cisplatin in head and neck cancer. Imaging is a useful adjunct for accurate mapping of the superficial extent of mucosal cancer in the upper aerodigestive tract. Imaging features of many clinical entities such as neurogenic and vascular tumors are typical enough to allow accurate diagnosis without examination of tissue. Imaging provides little additional benefit in pretreatment assessment of the clinically negative neck if surgical treatment is planned. Prominent soft tissue of the nasopharynx is a normal feature in children and adolescents. Retropharyngeal nodes are normally located in the infrahyoid neck between the scalene muscles and common carotid artery. Tonsil cancers can spread to the buccal space by tracking along the pharyngobasilar fascia. Subtle invasion of the prevertebral fascia from posterior pharyngeal wall carcinoma is difficult to detect on imaging. Imaging is of limited value in evaluation of submucosal skip areas of involvement in hypopharyngeal carcinoma. Carotid artery encasement is likely if a tumor is noted to encircle at least 180 degrees of the carotid. Imaging can help assess the extent of planned surgical resection in early stage supraglottic squamous cell carcinoma. The majority of patients with early stage glottic squamous cell carcinoma do not need imaging before endoscopic resection. The hyoepiglottic ligament separates the preepiglottic from the paraglottic spaces. The hyoepiglottic ligament is an effective barrier to tumor spread from the preepiglottic space to the base of the tongue. Involvement of the preepiglottic space is more common with tumors of the suprahyoid epiglottis than with those of its infrahyoid portion. Cartilage involvement and extralaryngeal spread is more frequent with glottic than with supraglottic squamous cell carcinoma. Cartilage invasion should be suspected in all glottic T1 lesions that involve the anterior commissure. Radiographic imaging is unreliable in detecting early invasion of the laryngeal cartilage framework. Imaging of the mandible is not necessary for surgical planning of a posteriorly based cancer of the oral tongue. Clinical examination is the most sensitive modality for detection of early cortical invasion of the mandible from a primary tumor of the floor of the mouth.
Generic rivastigimine 1.5 mg amex
Osteosarcomas of the head and neck require radiation therapy after resection to achieve better local control than surgery alone medicine 93 2264 buy 1.5 mg rivastigimine with mastercard. Primary intraosseous squamous cell carcinoma develops from the usual carcinogenic factors associated with mucosal squamous cell carcinoma. Primary intraosseous squamous cell carcinoma develops from odontogenic epithelial remnants. Fibrous dysplasia has three radiographic patterns: cystic, sclerotic, and mixed radiolucent and radiopaque. Ossifying fibromas are well demarcated and/or encapsulated compared with fibrous dysplasia. Aneurysmal bone cysts are expansile, osteolytic, multiloculated, blood-filled spaces with fibrous septa. Odontogenic fibroma i, iii, iv, vii i, iii, iv, v i, iii, iv, v, vii ii, vi All of the above 66. Is an autosomal dominant disease with multiple odontogenic keratocysts and skeletal abnormalities. Has no genetic linkage but has multiple odontogenic keratocysts and skeletal abnormalities. Contain ghost cells, occur in the anterior jaw, and are mixed radiolucent and radiopaque. Contain ghost cells, occur in the posterior jaw, and are mixed radiolucent and radiopaque. B Core Knowledge · Odontogenic cysts are cysts derived from odontogenic epithelium and may be classified as either inflammatory or developmental. Radiographically, they appear as unilocular radiolucencies surrounding the crown of an unerupted tooth. Treatment generally entails enucleation and curettage with regular long-term follow-up because these tumors are associated with a reasonable risk of recurrence or secondary tumors in the setting of basal cell nevus syndrome. Most ameloblastomas are multicystic and have a greater tendency for recurrence compared with unicystic lesions. Rarely, ameloblastomas have malignant potential and are classified as malignant ameloblastoma or ameloblastic carcinoma. Unicystic ameloblastomas may be treated conservatively with enucleation and curettage, but multicystic ameloblastomas are best managed with wide surgical resection and at least 1-cm bone margins. They are unilocular or multilocular and, in general, have a mixed radiolucent and radiopaque appearance. Treatment entails local resection, although enucleation may be adequate for smaller tumors. They appear as unilocular radiolucencies involving the crown and root of an unerupted tooth. In general, they appear as unilocular radiolucencies, and half contain some amount of radiopaque material. Most lesions are unilocular and have a mixed radiolucent and radiopaque appearance. It can occur in a single bone (monostotic) or in multiple locations (polyostotic). Surgery is generally reserved for correcting cosmetic deformities or functional deficits. They are generally unilocular or multilocular radiolucencies in the posterior region of the mandible. The anterior limit of dissection of the temporoparietal fascia is marked by the course of the frontal branch of the facial nerve (approximately 1. The temporoparietal fascia flap and the temporalis flap share the same blood supply. The temporoparietal fascia flap is not a good choice for use in contaminated fields because it is very thin and not resistant to infection. The Allen test is not a reliable test in determining adequate blood supply to the hand after harvest of a radial forearm free flap. Up to 60% of the radius diameter can be harvested in an osteocutaneous radial forearm free flap. Both the palmaris longus tendon and the lateral antecubital sensory nerve can be harvested with a radial forearm free flap. Hypoesthesia/anesthesia of the anatomical snuffbox is an unavoidable sequela of harvesting a radial forearm free flap because of sacrifice of the sensory branches of the radial nerve. Occlusion of the superficial femoral artery is a contraindication to harvesting of the anterolateral thigh flap. The most common cutaneous perforators for the anterolateral thigh flap are within 3 cm of the midpoint between the anterosuperior iliac spine and the superolateral corner of the patella. Bilobed flaps are a good option when the surrounding skin is not mobile enough to achieve primary closure of a surgical defect. Transposition flap design enables the surgeon to bring tissue from some distance away from the defect. The main blood supply to the pectoralis major is located medial to the tendon of pectoralis minor. A proximal (cephalad) skin island flap will permit a greater arc of rotation of the pectoralis major myocutaneous flap. When the pectoralis major flap is harvested, the nerves to the muscle should be identified and divided. The pectoralis major muscle flap shares a common blood supply with the deltopectoral flap. The superior trapezius flap and the lower trapezius island flap have the same blood supply. Radical neck dissection is a contraindication to use of the superior trapezius flap. In oral cavity tumors, the need for a thorough level I dissection might preclude the use of a submental island flap based on the ipsilateral side. The primary blood supply to the temporalis muscle is from the superficial temporal artery. In facial reanimation, it is important to divide the nerve to the temporalis muscle. The deltopectoral flap receives its blood supply from the internal mammary artery. The abdominal skin around the umbilicus has the most reliable blood supply for the musculocutaneous rectus abdominis flap. The deep superior epigastric artery is larger than the deep inferior epigastric artery. The most consistent cutaneous perforators are located at the junction of the proximal third and mid third of the skin on the lateral side of the calf. Cutaneous perforators travel through posterior intermuscular septa or through the soleus muscle. During insetting, the peroneal artery should be placed on the lingual surface of the neomandible. Leaving 6 to 7 cm of fibula proximally reduces the risk of injury to the posterior tibial artery. The scapular tip free flap is based on the angular branch of the thoracodorsal artery. Regardless of the extent of the flap, the parascapular flap base should be centered over the triangular space (between the teres major, minor, and long head of the triceps). Up to 10 cm of lateral scapular border can be harvested based on the angular branch. Latissimus dorsi, scapular tip, and serratus flaps cannot be raised based on one pedicle. The parascapular flap can be raised as a fasciocutaneous flap without disrupting any of the shoulder musculature. Donor site defects as wide as 7 cm can be closed primarily after harvesting of a musculocutaneous latissimus dorsi flap. The ascending branch of the deep circumflex iliac artery supplies the internal oblique muscle. When an iliac crest flap is harvested, the external oblique muscle is harvested with the bone. The skin paddle for the iliac crest can be extended from the anterosuperior iliac spine to approximately 9 cm posteriorly. The main blood supply to the gracilis is from the adductor artery, a branch of the profunda femoris.
Buy generic rivastigimine 4.5mg on-line
A burst component may complicate the injury and when present treatment carpal tunnel buy rivastigimine 6 mg free shipping, is best evaluated on sagittal images, which permit accurate measurement of any canal compromise. Fracture Dislocations Fracture dislocations result from complex forces that disrupt all three spinal columns. These are highly unstable injuries closely associated with severe neurologic deficits. Both injuries result from flexion at the anterior abdominal wall with dorsal distraction. When the injury is osseous, a Chance fracture results; when it is ligamentous, a flexion-distraction injury results. D, Lateral radiograph shows horizontal fracture line through the pedicle (dashed line). Serial axial images (E to G) show an asymmetric injury with right "dissolving pedicle" and left "naked facet" signs. Certain conditions, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, result in unusually brittle spines. In these patients, even minor trauma, such as a fall from standing, can result in devastating hyperextension injury. Osteoporosis and poorly defined disk spaces in the ankylosed spine contribute to diagnostic difficulty. Lateral radiographs can reveal anterior disk space widening or distraction of anterior vertebral body fracture fragments. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. Imaging Severe comminution, translation, and/or rotation are hallmarks of these grossly unstable injuries, and multiplanar reconstructions are essential in their analysis. Hyperextension Injuries An important variant of spinal fracture dislocation, the hyperextension fracture constitutes less than 3% of all thoracolumbar spine fractures. Severe hyperextension forces cause distraction of the spine with subluxation and canal compromise. In the normal nonfused spine, chapter 7 Nontraumatic Spine Emergencies Thomas Ptak Infection of the vertebral column represents up to 20% of all osteomyelitis and is the most common infection of the axial skeleton. It is not uncommon for symptoms to be present for 6 to 8 weeks before being diagnosed. If ignored or misdiagnosed, infection of the spine can have a chronic, destructive, and significantly debilitating course. Infection is commonly spread hematogenously, although direct extension from adjacent infection such as pneumonia or pyelonephritis is also possible. In 60% to 70% of patients the most common infectious agents encountered are gram-positive cocci, especially skin flora such as Staphylococcus (in about 60% of positive cultures), and less commonly Streptococcus with Peptostreptococcus, Escherichia coli, and Proteus. Although often implied by examination findings, a definitive infectious source is identified in less than 50% of patients with pyogenic spinal osteomyelitis. In unusual circumstances, such as immunodeficiency or patients from underdeveloped countries, one should consider atypical agents such as fungi or Mycobacteria. Patients at risk include older adults, intravenous drug abusers, those with chronic illness, and those with a recent history of surgery, especially of the back or genitourinary system. Insidious onset of diffuse back pain (in 90%) and fever (in 50% to 70%) should suggest spinal infection. A history of recent back or genitourinary surgery, intravenous drug use, or infection of the soft tissue or respiratory or genitourinary system should increase the likelihood of spinal infection. Infection involves the vertebral body in 95% of cases, with the posterior elements being involved in less than 5%. Although neurologic symptoms such as radiculopathy may be present, they are uncommon and often present later in the course as the infection spreads from the disk and vertebra to the epidural, subarticular, and external foraminal spaces. Weight loss may also be present, but this constitutional symptom is less helpful in that it may also be associated with both inflammatory and neoplastic disease. When thinking about where to look for infectious involvement of the vertebrae, it is helpful to consider the pathophysiologic manifestations. The nucleus pulposus of the disk receives nutrients typically by diffusion from the subchondral vascular bed of the vertebral end plate. In addition, the outer annulus fibrosis has a direct capillary supply via spinal canal arteries, also contributing nutrients across the concentric fibrous layers of the annulus. The bloodborne organism is able to establish itself at the more vascular outer free margin of the disk and at the end plate in the capillaries of the subchondral vascular bed. From here the organism can spread contiguously into the more avascular central disk and into the adjacent bony vertebrae. Using this model, it is understandable that the earliest changes of infection should appear at the disk margin closest to the vascular source anteriorly and anterolaterally, as well as anywhere along the disk-margin interface. Advanced infection is characterized by an abnormal intervertebral disk and abnormal adjacent vertebral end plates. Both are directed at identifying bony changes that may indicate infection of the vertebral bodies. Plain film has limited sensitivity because of many overlying confluent shadows and other technical difficulties in obtaining an image. Gross findings such as vertebral sclerosis, vertebral collapse with acute angulation of the spine. Contrast administration may produce enhancement of the actively inflamed tissue with nonenhancing areas of central liquifactive debris in early abscess formation, if present. Attention should also be directed to adjacent organ systems such as the kidneys or lungs to provide clues to the origin of infection. Typical findings suspicious for acute or active infectious involvement of the bone include focal or regional 165 166 Section ii Spine emergencieS Table 7-1 Common Locations and Characteristics of Spinal Infections Infection Vertebral osteomyelitis Spinal epidural abscess Diskitis Characteristics Elderly and debilitated Male predominance Hematogenous gram-positive cocci Adult postdiscectomy most common Rare in pediatrics; often accompanies chronic infections. Also note involvement of the superior end plate of the T6 vertebra, not appreciated on the plain film. It is crucial to include fat suppression in the evaluation because abnormal signal indicating infection on T2-weighted and postcontrast T1-weighted sequences may be confused with hyperintense signal produced in the normal fat planes of the epidural space, marrow compartment, and in the interstitial spaces of spinal ligaments. Precontrast T1-weighted images are customarily performed without fat suppression so that anatomic detail is preserved (and to save time), with T2-weighted sagittal and postcontrast T1-weighted images being fat suppressed in all planes. Fat suppression allows increased sensitivity in detecting infectious deposits by ensuring that hyperintense regions identified indicate areas of edema and enhancing inflammation and are not due to the normal soft tissue fat planes and interstitial fat encountered in the spine. Chemical fat suppression is typically employed but is prone to inhomogeneity due to off-resonance excitation resulting from local susceptibility effects and static field inhomogeneity. More homogeneous suppression is attained, and the signal-to-noise ratio of water and edema with respect to the surrounding tissue is optimized. Starting with a T2-weighted, fat-suppressed, large field-of-view image may be helpful and efficient for determining the extent and involvement of inflammation. Once inflammation is identified, further evaluation can be carried out with more focused T1-weighted precontrast and postcontrast imaging in additional planes optimized to best show the lesion(s) identified. Inflammation and/or enhancement identified adjacent to or within potential spaces should include additional orthogonal views (typically axial if sagittal was already used to survey the region) along the full length of the soft tissue space involved to ensure identification of the full extent of involvement. Enhancement adjacent to the central spinal canal should lead to a careful evaluation of the extradural space to identify any infection or abscess formation. This evaluation can be carried out using two orthogonal planes through the region of interest. Evaluation of the bony structures is especially important, particularly in areas of adjacent soft tissue swelling or enhancement. Again, fat-suppressed T1-weighted imaging in the optimal plane for visualization is imperative. T2-weighted imaging may show hyperintensity in the marrow space adjacent to the soft tissue inflammation, and with the addition of fat suppression this will make certain that marrow edema from infection/ inflammation is not confused with marrow space fat signal. Precontrast T1 weighting with fat-suppressed imaging should show the normally hypointense densely calcified bony cortex as very hypointense, but inflamed edematous cortical mantle may appear relatively hyperintense or nearly isointense to adjacent marrow signal, making it indistinguishable from adjacent marrow. On postcontrast T1-weighted imaging, areas of infectious involvement of the bony cortex will enhance, producing a hyperintense disruption in the normally sharply defined, thin hypointense signal of the normal bony cortical stripe. As discussed earlier, one might expect diskitis to begin in the periphery at the outer annulus or along the diskend plate margin; these are the regions of vascular supply and are the most likely points of origin for a blood-borne infection.
