

Order venlafaxine uk
Hiersch L et al: Effectiveness of medical treatment with methotrexate for interstitial pregnancy anxiety love buy venlafaxine 75 mg overnight delivery. Tanaka Y et al: Three-dimensional sonography in the differential diagnosis of interstitial, angular, and intrauterine pregnancies in a septate uterus. Sagiv R et al: Interstitial pregnancy management and subsequent pregnancy outcome. Cucinella G et al: Laparoscopic management of interstitial pregnancy: the "purse-string" technique. Tamarit G et al: Combined use of uterine artery embolization and local methotrexate injection in interstitial ectopic pregnancies with poor prognosis. Because an interstitial ectopic is covered by myometrium, it can grow to a larger size and present later than a tubal ectopic. Close interval follow-up should be done if there is any question regarding the diagnosis. The oval gestational sac, which contains a yolk sac, is clearly implanted in the cervix, not the uterine cavity. Chukus A et al: Uncommon implantation sites ectopic pregnancy: thinking beyond the complex adnexal mass. This can be seen after treatment and is also the appearance during miscarriage, in contradistinction to the closed appearance in a cervical ectopic. The sac is implanted above the internal os, differentiating it from a cervical ectopic. Cok T et al: Transvaginal ultrasound-guided local methotrexate administration as the first-line treatment for cesarean scar pregnancy: Follow-up of 18 cases. The developing gestational sac is in the right lower quadrant, adjacent to the ascending colon. Dabiri T et al: Advanced extrauterine pregnancy at 33 weeks with a healthy newborn. The uterus was empty, and the patient had adnexal pain out of proportion to what would be expected for a corpus luteum. The intrauterine fluid collection (calipers) is flat in shape and has pointed edges most consistent with blood, although such collections may mimic an intrauterine pregnancy. Treatment for a heterotopic gestation is focused on preserving the intrauterine pregnancy. A 2nd smaller sac is present in the interstitial portion of the left fallopian tube. The high-signal fluid in the uterus is the intrauterine pregnancy, which was preserved. This type of medical treatment is especially useful for nontubal heterotopic pregnancies as these are challenging to manage surgically. In an embryo of this size (7 mm), this is diagnostic of embryonic demise and no additional follow-up is required. Doppler should be used sparingly in early pregnancy, but in this case, color Doppler was used appropriately to illustrate absence of cardiac pulsation. There are often multiple findings in failed pregnancies; in this case, note the hydropic chorionic villi and the perigestational hemorrhage. This is an ectopic (thus, nonviable) pregnancy, and if it is not recognized as such, the patient is placed at great risk. There was concern for gestational trophoblastic disease, but pathology only revealed retained products of conception. The fetus is in the cervix, the external os is open, and the gestational sac is elongated and flattened. Abnormal Sac Location Abnormal Sac Location (Left) 3D coronal reconstruction shows an interstitial ectopic pregnancy implanted away from the uterine cavity with surrounding myometrium becoming imperceptible. A short interval followup study showed embryonic demise and D&C revealed partial mole. Chorionic bump is associated with partial mole more frequently than with complete mole as occurred in this patient. Choriocarcinoma 60 Abnormal Gestational Sac and Contents First Trimester Abnormal Embryo or Fetus Abnormal Embryo or Fetus (Left) There is a focal protrusion from the abdominal wall in this 12week fetus (1 of a pair of dichorionic twins). Normal bowel herniation is into the cord, and bowel should be back in the abdomen by this gestational age. The exposed brain is subject to direct trauma with the end result of anencephaly, which is lethal. The bladder can mimic a cystic adnexal mass on a single image but should be anterior to the uterus on real-time imaging. Unless suspicious features are present to suggest a malignant lesion, follow-up in the 2nd trimester at the time of fetal anatomy scan should show a significant decrease in size. In this case, an adjacent thinwalled hemorrhagic cyst is also present, with layering reticular echoes consistent with blood products. At times, the echogenic Rokitansky nodules appear to layer dependently in the otherwise cystic dermoid fluid. Teratoma (Dermoid) Teratoma (Dermoid) (Left) Occasionally, an echogenic, solid-appearing dermoid can be seen in the same ovary as the thick-walled corpus luteum cyst. Teratoma (Dermoid) Endometrioma (Left) this ovarian cyst has diffuse low-level internal echoes with a punctate echogenicity in the cyst wall, characteristic of an endometrioma. Theca Lutein Cysts 64 Adnexal Mass in Pregnancy First Trimester Pedunculated Fibroid Ectopic Pregnancy (Left) this 7-cm complex cystic adnexal mass is actually a degenerated pedunculated fibroid. Hydrosalpinx Stool-Filled Colon (Left) this composite shows features of a hydrosalpinx in longitudinal (top) and crosssectional (bottom) views. You should always try to elongate any cystic mass to see if it has a tubular configuration; note it is blind-ending and there are incomplete septa. Pelvic Kidney Cystadenoma (Left) Occasionally, unusual incidental adnexal masses can be identified at the time of the anatomy ultrasound. In this 8-cm serous tumor with a borderline component, there are subtle soft tissue nodules. If there is low suspicion for epithelial ovarian cancer, some masses can be followed until after delivery. The cranial neuropore closes at day 24, while the caudal neuropore closes at day 25. The prosencephalon (green) gives rise to the forebrain, the mesencephalon (purple) to the midbrain, and the rhombencephalon (light blue) to the hindbrain. The abdominal wall has closed, the yolk sac has detached, and the umbilical cord has formed. The torso is relatively small, the limb buds have not yet developed, but as shown above, the neural tube within it has already developed the precursors to the forebrain, midbrain, and hindbrain. This is a normal finding with high-resolution modern equipment and should not be mistaken for holoprosencephaly or other brain malformation. The mesencephalon elongates, while the rhombencephalon gives rise to the secondary vesicles, metencephalon, and myelencephalon. At this point, several flexures develop in the neural tube so that it adapts to the contour of the developing cranium. The choroid plexus echogenicity and shape on an axial image gives rise to the butterfly sign in which the choroid forms the butterfly wings. The intracranial translucency (the future 4th ventricle) is seen between the brainstem and the choroid plexus of the 4th ventricle. Intracranial translucency assessment may be used for early detection of open neural tube defects. The ocular globes are visible within the bony orbits and the oral cavity is visible between the bright echoes of the maxilla and mandible. The latter marks the anatomic location at which the width of the lateral ventricle should be measured. Although not a standard image in a 2nd-trimester scan, this is as easy to obtain as a profile view of the face. The cisterna magna cannot be measured in this plane as it is artificially deepened by the extension into the foramen magnum. It is a box-shaped, anechoic space in the midline between the frontal horns of the lateral ventricles.
37.5mg venlafaxine free shipping
Here anxiety panic attacks safe venlafaxine 37.5mg, each embryo is within a separate amniotic sac surrounded by a single chorionic sac with a single placenta. The cords are closely inserted on a single placenta, and both embryos are within a single amniotic sac. The amnion has only of a single layer of epithelial cells, a basement membrane, and a collagen layer. Both cords insert into the placenta and are widely separated on the placental disc. Note the long course of unprotected vessels running in the membranes prior to reaching the placenta. In twins, velamentous cord insertion increases the risk for discordant growth, and it is a proxy marker for unequal placental sharing in monochorionic placentas. The donor is oligemic and growth restricted, and the recipient is plethoric and volume overloaded. The linear structure to the right of the image is an intrauterine contraceptive device that, even though well positioned, failed to prevent pregnancy in this case. The broad-based triangle of chorion where the sacs abut each other creates the twin peak sign. Dichorionic Diamniotic Twins Multiple Gestations (Left) Transvaginal ultrasound shows 2 embryos, each one is fully surrounded by its own thick, echogenic chorion. Note how thin the amnion is in comparison to the chorion (which forms the twin peak and thick membrane). The fetuses are separated by a thick membrane, which abuts the anterior placenta in the configuration of the twin peak. The thin membrane in monochorionic diamniotic twinning is composed of only the 2 amnions. If chorionicity is unknown late in pregnancy, evaluation of fetal gender and number of placentas becomes more important. One of the 2 yolk sacs was visible in this plane, which nicely demonstrates delicate amniotic sacs surrounded by the echogenic fluid of the extraembryonic coelomic space. The amnion has only of a single layer of epithelial cells with a basement membrane and a collagen layer. Note the "T" junction of the diamniotic membranes as opposed to the dichorionic "twin peak" or lambda sign. Cord inserts on the membranes, and vessels run along the membranes to reach the placenta. Variations in the direction and degree of shunting result in alterations of cord Doppler waveforms. It can be difficult to exclude conjoined twinning in early monoamniotic twins as the embryos are often very close to each other. The cranial end of the superior embryo was irregular in shape, and we were suspicious for exencephaly vs. Prefumo F et al: the natural history of monoamniotic twin pregnancies: a case series and systematic review of the literature. This case illustrates how elevated maternal serum -fetoprotein in twins is not always simply attributable to the presence of more than 1 fetus. Cord entanglement in relation to demise in monoamniotic twins is controversial, and recent studies suggest that it is does not play as large a role as previously thought. Also note that entanglement occurred even though the cord insertion sites are quite far apart on the placental surface. At 11 months, there was a 5-lb weight difference, but both boys are healthy & developmentally normal. Discordant Twin Growth Multiple Gestations (Left) Color Doppler imaging is very helpful for evaluation of the placental cord insertion site. This is associated with a high risk of intrauterine demise; a Csection was performed. The combination of oligohydramnios (< 2 cm) and polyhydramnios (> 8 cm) is diagnostic. The membrane was no longer visible because it was "shrinkwrapped" around the donor twin, which was unable to move at all while the recipient twin was very active. Unfortunately, her membranes ruptured a week after treatment, and she delivered live, preterm infants. The cord Doppler is also abnormal with absent end diastolic flow and pulsatile umbilical vein flow. In this case, the donor (A) shows either absent or reversed end diastolic flow and pulsatile umbilical vein flow. These deep placental anastomoses manifest as "nose-to-nose" vessels on the placental surface. The vascular equator is devoid of intertwin communications as a result of "dichorionization. Abnormal circulation with selective perfusion of the lower extremities impairs development of the heart, torso, and head. The normal twin is the pump for the abnormal one and is at risk of high-output cardiac failure. Monoamniotic twins may be very close to each other and appear to be hugging, but they will not have contiguous skin covering. Stahr N et al: In utero and postnatal imaging findings of parasitic conjoined twins (ischiopagus parasiticus tetrapus). As is so often the case, there are multiple anomalies; in this instance, bladder outlet obstruction. There was a single shared liver with a single umbilical vein, which bypassed the liver, entered 1 heart, and then connected to the other heart by a large anomalous vessel. These twins would have been excellent candidates for separation, but the pregnancy ended in spontaneous intrauterine demise within weeks of this scan. With 1 yolk sac and no membrane there was concern that A and B were a monoamniotic pair. Birthweight, gestational age, and perinatal mortality and morbidity in triplets, quadruplets, and quintuplets. At 28 weeks, fetuses B and C died for unknown reasons; cord entanglement had not been seen. High-order multiples are at risk for poor placentation and abnormal placental cord insertion. The unprotected umbilical artery runs in the membranes and is within 2 cm of the internal os. Recent studies indicate that cerclage is potentially harmful in multiple gestations and should be avoided. It was urgently resected at birth in an attempt to treat respiratory compromise, but the infant expired from pulmonary hypoplasia attributed to thoracic compression by this very large mass. The mass was distinct from the urinary tract and did not appear associated with the bowel. Note the resemblance to a twin reversed arterial perfusion sequence fetus (another form of asymmetric monochorionic twinning). Many authors consider the presence of a neural axis an essential characteristic of fetus-in-fetu and a key point of differentiation from a mature teratoma. Fetus-in-fetu often presents in this way as the fetus is suspended within the fluidfilled amniotic sac. The incidence for live born neonates with T21 is reported as 1:700 while the first-trimester prevalence is 1:300. The prevalence of aneuploidy is highest in the first trimester since many are lost or terminated subsequently. Current guidelines for screening for aneuploidy utilize ultrasound, noninvasive genetic screening, & invasive diagnostic testing techniques. Combined First- & Second-Trimester Screening With integrated screening, the patient is given a single risk assessment at the completion of the first- & second-trimester tests. However, integrated screening is not popular because patients are not told their first-trimester results & cannot have early invasive testing. With stepwise sequential screening, the first screen results are shared with the patient, & if screen positive, she is offered invasive testing. With contingent sequential screening, only women with intermediate increased risk go on to secondtrimester screening. Women who screen negative have only a second-trimester ultrasound, & those who screen positive are offered invasive genetic testing. Imaging Techniques & Normal Anatomy First-trimester screening is performed by certified sonographers.
Buy 75 mg venlafaxine with amex
Tumor extends into the left foramen transversarium and along the vertebral artery anxiety rash venlafaxine 37.5mg on line. Tumor extends into adjacent soft tissues and epidural space through small perforations in bone cortex. Note the relatively low T2 signal intensity characteristic of cellular neoplasms ("small round blue cell"). There is vertebral body destruction and epidural extension resulting in approximately 50% narrowing of the epidural space. The leading differential consideration was neuroblastoma in this pathology-proven Ewing sarcoma. Radiological and subjective clinical results after at least one year of treatment. The location is typical for occult sacral meningocele, now designated extradural arachnoid cyst. Note mild upward mass effect on the terminal thecal sac, which normally terminates at S2/3. There is remodeling and expansion of the adjacent vertebral body and overlying posterior elements. Grammatikopoulou I et al: Immature malignant sacrococcygeal teratoma: case report and review of the literature. Usui N et al: Outcomes of prenatally diagnosed sacrococcygeal teratomas: the results of a Japanese nationwide survey. Draper H et al: Long-term functional results following resection of neonatal sacrococcygeal teratoma. The fat fills much of the central spinal canal and narrows the thecal sac, particularly within the thoracic spine. Note also the preponderance of epidural fat combining with compression fractures that narrow the spinal canal and produce diffuse spinal stenosis. The latter is subdivided into low- & high-risk categories, depending on clinical course, treatment response, & involvement of lungs, liver, spleen, & hematopoietic system. The natural history of these spinal lesions in the absence of systemic disease or spinal deformity is such that aggressive surgical management is usually not indicated; only follow-up is necessary to monitor recovery and spinal balance. Large soft tissue masses are common during the early phase of involvement but regress with evolution of lesions. Although many patients show substantial regeneration of vertebral height, this patient demonstrates vertebra plana despite treatment. In this case of extramedullary hematopoiesis, there is marrow expansion from severe anemia and paraspinal masses as extramedullary hematopoietic elements. The marrow of the vertebral bodies is diffusely hypointense due to hyperplastic hematopoietic elements. Note the intradural location and close relationship with the dorsal conus neural placode. A T1-hyperintense epidermoid cyst or subacute (methemoglobin) hemorrhage would not demonstrate this suppression, confirming the lipoma diagnosis. Note that there is very subtle remodeling and enlargement of the osseous spinal canal at the lipoma level. Vitamin E capsule placed at skin opening marks clinically detected dermal sinus ostium that prompted imaging. Within the fatty component is the angiomatous component of the lesion, which exhibits hypointense signal. Spinal angiolipomas are benign uncommon neoplasms composed of varying proportions of mature lipocytes and abnormal vascular elements. These are tumors containing angiomatous & lipomatous tissue, predominantly located in the midthoracic region. The dilatation is centered within the central canal and confined to the conus only. The cystic dilatation is centered within the central canal and confined to the conus only, helping to make the diagnosis of variant ventriculus terminalis. Despite the loculated appearance of large syringes, the individual fluid spaces are contiguous and drainable using a single shunt catheter. Kemp J et al: Holocord syringomyelia secondary to tethered spinal cord associated with anterior sacral meningocele and tailgut cyst: case report and review of literature. Nagoshi N et al: Factors contributing to improvement of syringomyelia after foramen magnum decompression for Chiari type I malformation. Aghakhani N et al: Long-term follow-up of Chiari-related syringomyelia in adults: analysis of 157 surgically treated cases. The hypointense syringopleural shunt catheter is visible, extending into the syrinx cavity. Note intramedullary edema without frank syringomyelia, representing a "presyrinx state. This patient presented with typical acute onset of weakness and areflexia of the distal extremities. Barbay M et al: Clinically silent posterior reversible encephalopathy in Guillain-Barre syndrome. Mohsen H et al: Acute disseminated encephalomyelitis following infectious mononucleosis in a toddler. The pathological substrate is an intraparenchymal/ perivascular cellular influx into the cord breakdown of the blood-cord barrier variable demyelination and neuronal injury. Idiopathic acute transverse myelitis is reported to make up 16-17% of transverse myelopathies. There is conus enlargement secondary to edema but no central fluid signal to indicate syringohydromyelia. Malignant transformation, while common in recurrent adult low-grade gliomas, is unusual in pediatric low-grade intramedullary spinal cord tumors. Glial fibrillary acidic protein- immunoreactivity is reported to significantly correlate with grade of spinal cord astrocytoma compared to that in normal control tissues. Cranial and rostral cysts as well as hemorrhagic products are associated with this mass. There are 2 areas of enhancing solid and a superior component cyst extending cephalad into brainstem with medullary expansion. Spinal ependymomas are less common than cerebral ependymomas and exhibit a better prognosis, which may relate to a distinct pattern of genetic alterations, different from intracerebral ependymomas. Bydon M et al: Multiple primary intramedullary ependymomas: a case report and review of the literature. There is extensive cord edema, seen at the superior margin as a flame-shaped termination. The large myelomeningocele lumbosacral sac has not been surgically repaired, and it protrudes dorsally through a large posterior dysraphic defect. The attenuated elongated spinal cord typically inserts into the surgical closure, with detection of small terminal syrinx. The low-lying spinal cord and cauda equina nerve roots adhere to a large fatty mass that extends through dysraphic posterior elements. May L et al: Lack of uniformity in the clinical assessment of children with lipomyelomeningocele: a review of the literature and recommendations for the future. A skin dimple with capillary angioma and hairy tuft (cutaneous marker) indicates sinus opening. Note that terminal cord central canal is dilated, probably representing syringohydromyelia rather than ventriculus terminalis because of low-lying cord and the presence of dermal sinus. De Vloo P et al: Spinal dermal sinuses and dermal sinus-like stalks analysis of 14 cases with suggestions for embryologic mechanisms resulting in dermal sinus-like stalks. This mild dysraphic defect represents the point of spinal entry for the dorsal dermal sinus. The spinal cord termination within the lipomatous mass is low lying and reflects radiographic cord tethering. This finding represents a subtle posterior dysraphism that facilitates passage of the dermal sinus tract into the spinal canal. This is a typical location for an acquired epidermoid cyst following prior lumbar puncture.
Generic 150mg venlafaxine with mastercard
Prognostic value of blood pressure in patients with high vascular risk in the Ongoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial study anxiety symptoms or something else cheap 75 mg venlafaxine mastercard. Chlorthalidone versus hydrochlorothiazide as the preferred diuretic: Is there a verdict yet Risk of incident diabetes with intensivedose compared with moderate-dose statin therapy: A meta-analysis. Also, alkali therapy improves protein nutrition by suppressing protein catabolism and protects against hyperkalemia. Whether metabolic acidosis needs to be present for benefit to be derived from alkali supplementation is not clear. On the natural tendency to progressive loss of remaining kidney function in patients with impaired renal function. Therapeutic approaches in lowering albuminuria: Travels along the renin-angiotensin-aldosterone-system pathway. Aldosterone blockade and the mineralocorticoid receptor in the management of chronic kidney disease: Current concepts and emerging treatment paradigms. Allopurinol treatment and its effect on renal function in gout: A controlled study. Starting dose is a risk factor for allopurinol hypersensitivity syndrome: A proposed safe starting dose of allopurinol. Allopurinol is the most common cause of Stevens-Johnson syndrome and toxic epidermal necrolysis in Europe and Israel. Although every effort has been made to ensure that this chapter reflects current recommendations, the reader is advised to check for any relevant guideline updates. A detailed medical history covering issues, including other medical conditions, family history of kidney disease, prescribed medication, and illicit drug use, may suggest an underlying cause. The physical examination findings are not usually helpful, although skin pigmentation, scratch marks, left ventricular hypertrophy, and hypertensive fundal changes favor a chronic presentation. Blood tests for other conditions can be helpful if the findings indicate evidence of an acute illness that may be the cause of kidney failure, such as systemic vasculitis or multiple myeloma. Patients with grossly abnormal biochemical values-for example, blood urea nitrogen higher than 140 mg/dl, serum creatinine above 13. There is some evidence that early diagnosis with appropriate management may slow the rate of decline of kidney function and reduce cardiovascular risk. Where appropriate, urine tests for Bence-Jones protein (immunoglobulin light chains) may be required because this is not detected by standard proteinuria or albuminuria testing. Small kidneys with reduced cortical thickness, showing increased echogenicity, scarring, or multiple cysts, suggest a chronic process. Diffuse brown pigmentation as seen here suggests chronic kidney disease rather than acute kidney injury. Furthermore, some kidney diseases may recur after transplantation (see Chapter 108), and an accurate diagnosis may therefore influence later management. In such patients, investigation should not be pursued relentlessly because the implications for treatment are often minimal. Attempting to obtain biopsy material from small kidneys is associated with risk, and even if a biopsy is performed, histologic assessment may simply show nonspecific chronic scarring rather than diagnostic features that explain the cause of kidney damage. Whether or not proteinuria is detected by dipstick, further measurement of urinary protein excretion should be conducted. Proteinuria is an important diagnostic and prognostic marker, and its presence indicates a higher risk for both progression of kidney disease and cardiovascular complications. However, often the best guide to future change in kidney function is the previous pattern of decline, highlighting the importance of considering results of previous blood and urine testing during the initial assessment. They may be caused by reversible factors, such as intravascular depletion or high meat intake, so repeat testing may be required. Furthermore, because an arteriovenous fistula takes several weeks to mature, patients presenting late start hemodialysis with central venous catheters. Catheters are prone to infectious complications and inevitably damage central veins, leading to thromboses and stenoses, which may manifest at a later stage when venous return from one or the other arm is increased by the subsequent construction of an arteriovenous fistula (see Chapter 91). Such criteria are not absolute but should provide a guide to the primary care physician as to which patients are likely to benefit from specialist care. Late referral is often avoidable, although in some cases, patients may have had a truly silent illness or an acute presentation of a disease with rapid decline in kidney function. However, in light of growing evidence about the adverse effects of hypotension, the paradigm has moved toward less-intensive and individualized blood pressure control. Lifestyle modifications, including maintenance of a healthy weight, reductions in salt and alcohol intake, and regular exercise, should be encouraged (see Chapter 35). Although current recommendations are based on office blood pressure recordings, recent studies suggest that readings obtained from home and ambulatory monitoring correlate better with cardiovascular and kidney outcomes. Salt substitutes containing potassium should be avoided because of the risk for hyperkalemia. The causes are multifactorial but include anorexia, acidosis, insulin resistance, inflammation, oxidative stress, and urinary protein loss. Biochemical indicators may demonstrate a decrease in serum albumin, transferrin, and cholesterol. Serum creatinine concentrations, which in part reflect muscle mass, may stop rising despite a progressive loss of kidney function, because of compromised nutritional status. In light of this, recommendations to restrict protein intake have been controversial. Although there is evidence that reduced protein intake may slow progression of decline of kidney function, many patients develop protein-calorie malnutrition on a low-protein diet. When this recommendation is followed, detailed dietary assessment and supervision are needed to ensure that malnutrition is prevented. Anemia may have multiple adverse effects, including worsening cardiac dysfunction by increasing cardiac output and exacerbating left ventricular hypertrophy, exacerbating the decline of kidney function, and reducing cognition and concentration. Anemia Hyperphosphatemia, together with a deficiency of 1,25dihydroxyvitamin D3, contribute to secondary hyperparathyroidism and ultimately to the development of renal bone disease. Phosphate-binding drugs may be required, and their choice is discussed in Chapter 85. Acidosis aggravates hyperkalemia, inhibits protein anabolism, and accelerates calcium loss from bone where the hydrogen ions are buffered. Neutrophil activation is defective, and although serum immunoglobulin levels are normal, antibody responses to immunization may be poor. This should happen as early as possible to maximize the chances of seroconversion. The aim is to create an environment in which patients can become informed and proactive in their care. The potential risk of nephrogenic systemic fibrosis from gadolinium-based contrast media and measures to reduce it are discussed in Chapter 5. As discussed earlier, the need for temporary cessation of all medications should be considered during periods of severe intercurrent illness. Clinicians should always consider whether acceleration of loss of kidney function is a result of relapse of the underlying disease or of a superimposed problem such as acute interstitial nephritis (see Chapter 62), obstructive uropathy (see Chapter 60), or renal vein thrombosis. Although dialysis may offer longer survival, those choosing conservative management may have as many hospital free-days as those who choose hemodialysis. If hemodialysis is the preferred option, an arteriovenous fistula should be constructed, remembering that it may take 8 to 12 weeks for veins to become adequately arterialized before needling can be attempted (see Chapter 91). Similar plans need to be made for preemptive insertion of a peritoneal dialysis catheter to allow time for healing and training before any acute need for commencement of dialysis (see Chapter 96). Peritoneal dialysis catheters can be inserted and completely buried subcutaneously some time before patients require dialysis, then superficialized for use once clinical circumstances dictate. Early kidney transplantation may be associated with improved long-term outcome,35 so patients should be assessed for their suitability and, when feasible, activated on the waiting list before dialysis is commenced. This maximizes the chances of the potential recipient remaining in reasonable health. The availability of a living donor should be explored to increase the chances of preemptive transplantation before the patient begins dialysis. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Late referral for end-stage renal disease: A region-wide survey in the south west of England. Outcomes of early versus late nephrology referral in chronic kidney disease: A systematic review. Association of low blood pressure with increased mortality in patients with moderate to severe chronic kidney disease.
Buy venlafaxine with american express
The left renal vein is then secured with large bulldog clamps 2 cm apart and cut between anxiety symptoms talking fast cheap 37.5mg venlafaxine overnight delivery, leaving a cuff of 1 cm on either side to repair when the procedure is completed. The retroaortic left renal vein is usually not perpendicular to the aorta, as is the normal left renal vein. Abdominal wall Lesser omentum Hepatic portal vein and proper hepatic artery in right margin of lesser omentum Omental bursa (lesser sac) Stomach Middle colic artery Transverse mesocolon T12 Omental (epiploic) foramen (of Winslow) Celiac trunk Splenic vessels Renal vessels L1 L2 L3 Pancreas Superior mesenteric artery Lumbar vessels Inferior (horizontal, or 3rd) part of duodenum Abdominal aorta Transverse colon Greater omentum Small intestine L4 L5 S1 S2 Parietal peritoneum (of posterior abdominal wall) Mesentery of small intestine B. The groin incisions are made transversely or horizontally depending on the complexity of the femoral reconstruction. The shorter abdominal incision is adequate because dissection of the aorta from its bifurcation to the renal arteries is the goal. These tunnels are created on top of the iliac vessels with blind finger dissection from the groins to the aorta. An infraureteral tunnel is created to prevent stenosis or pressure on the urterer after scarring around the graft occurs. The tunnels are usually marked with an umbilical tape, and the limbs are pulled through the tunnels at the appropriate time. The renal vein can be difficult to identify because of the hematoma and the tissue staining, making the entire retroperitoneum the same deep-maroon, purple color. Occasionally, clamping the aorta at the diaphragmatic hiatus is necessary to gain proximal control. This technique can be an especially helpful maneuver in the trauma victim with a central hematoma. The left lobe of the liver is taken down, and the anterior portion of the crus of the diaphragm is incised. With the liver retracted to the right and the stomach retracted left, blunt finger dissection on both sides of the aorta allows pressure with a sponge stick or occlusion with a straight aortic clamp. Abdominal aortic aneurysm (infrarenal) Aortic arch Aneurysm opened Celiac artery Renal arteries Prosthetic graft sewn into position Graft Aneurysm Incision lines for opening aneurysm Common iliac arteries Aneurysm wall Indications for surgery include aneurysm diameter twice normal aorta, rapid enlargement, or symptomatic aneurysm. Completion of aortic repair with tube graft and relationships of supraceliacaorta,stomach,andcrusofstomach. Wahlberg E, Olofsson P, Goldstone J; Emergency vascular surgery: a practical guide. This chapter briefly addresses clinical presentations of acute and chronic mesenteric ischemia that most often require surgery and considers the various options to achieve optimal exposure. Patients present with the sudden, acute onset of epigastric pain not associated with rebound tenderness. The other primary cause of acute mesenteric ischemia is sudden thrombosis of one or more dominant mesenteric blood vessels. Although these patients frequently have symptoms similar to those with embolic events, prodromal symptoms such as postprandial abdominal pain ("intestinal angina") and a history of atherosclerotic complications (peripheral vascular disease, myocardial infarction) are often elicited. Chronic mesenteric ischemia is almost always caused by atherosclerosis of the mesenteric vessels; the classic symptoms are postprandial abdominal pain, weight loss, and food avoidance ("food fear"). In most cases, two of the three major visceral vessels (celiac axis, superior and inferior mesenteric arteries) must be significantly narrowed or occluded for symptoms to occur. Arteriographic findings of multiple arterial plaques at the vessel origins confirm the diagnosis. Less common, nonatherosclerotic causes of chronic mesenteric ischemia include fibromuscular dysplasia, median arcuate ligament syndrome, and vasculitis. The diagnosis of acute or chronic mesenteric ischemia requires both knowledge of the multiple clinical presentations and supporting findings from arterial imaging studies. Computed tomography angiography has an increasing role in diagnosis, with conventional angiography often reserved for potential therapeutic intervention such as fibrinolysis or angioplasty. The artery divides most often into three major branches within 2 cm of its origin: the common hepatic, splenic, and left gastric arteries. These arterial branches and their tributaries provide the blood supply for the stomach, liver, spleen, portions of the pancreas, and proximal duodenum. The common hepatic artery gives rise to the superior pancreaticoduodenal arteries, cystic artery, and right gastric artery in addition to its left and right hepatic arteries. In approximately 18% of cases, the right hepatic artery is "replaced" and originates from the superior mesenteric artery. The splenic artery gives off the dorsal pancreatic artery, left gastroepiploic artery, and short gastric arteries before completing its tortuous course toward the spleen. The left gastric artery supplies the gastric cardia and fundus before anastomosing with the right gastric artery. A "replaced" left hepatic artery originates from the left gastric artery in approximately 12% of cases. It travels behind the neck of the pancreas, in front of the uncinate process and over the third portion of the duodenum. Anatomy of celiac axis Left hepatic artery Right hepatic artery Common hepatic artery Left gastric artery Splenic artery B. Normal celiac axis angiogram Proper hepatic artery Right gastric artery Left gastric artery Proper hepatic artery Right gastric artery Common hepatic artery Splenic branches of splenic artery C. Superior mesenteric artery as it courses below the inferior border of the pancreas Gastroduodenal artery Celiac trunk Celiac trunk Splenic artery Superior mesenteric artery D. When performing a surgical procedure for chronic mesenteric ischemia, it is generally wise to revascularize the celiac axis as well. The optimal procedure depends on the disease process, indication for operation, patient anatomy, comorbidities, and surgeon experience. An upper midline incision provides adequate exposure in most patients, whereas bilateral subcostal incisions may be advantageous in patients with previous midline incisions or large abdominal girth. This portion of the aorta is often the last to be involved in patients with extensive atherosclerosis and is the preferred site of proximal anastomosis for a bypass graft. Care is taken to avoid excessive force when using self-retaining retraction systems, to prevent damage to liver parenchyma as the left lobe is folded toward the right. The right crus of the diaphragm is divided by electrocautery and the underlying median arcuate ligament incised, often through dense lymphatic and neural tissue. The posterior peritoneum may then be incised and the supraceliac aorta visualized and evaluated for its suitability for proximal anastomosis. Dissection in an inferior direction will expose the origin of the celiac axis and its primary branches. If bypass to the celiac axis is planned, adequate exposure will be available for graft anastomosis to either the common hepatic artery or the cut end of the main celiac trunk. The main vessel is exposed by incising the peritoneum directly above it at the root of the mesentery. The vessel usually is easily identified, but care must be taken to avoid injury to parallel veins and often-sizable arterial branches. Incision of the triangular ligament of the liver, which will be greatly retracted to the right in preparation for supraceliac aortic exposure Superior mesenteric artery Superior mesenteric artery Duodenum Bifurcated graft D. If a retrograde bypass is planned, the infrarenal aorta or left iliac arteries are exposed directly by either retracting the duodenum to the right and incising the retroperitoneum or medially reflecting the left colon. Retrograde bypass is less favored because of extensive atherosclerotic involvement of the distal aortoiliac segment and potential kinking of grafts. Specific indications for retrograde bypass include a "hostile" upper abdomen or severe heart disease, which makes supraceliac aortic occlusion undesirable. Incising the left lateral peritoneal reflection from the diaphragm to the pelvis allows mobilization of the descending colon. As discussed next, rotating the patient to a lateral position with the right side down facilitates this exposure. In addition to affording excellent and continuous aortic exposure, the retroperitoneal route is particularly useful in patients with an ostomy or prior abdominal surgery and dense intraperitoneal adhesions. The patient is positioned with the left side up, rotated about 60 degrees from the supine position. Care is taken to position the "break" of the operating room table equidistant between the rib cage and pelvis and properly pad both the torso and the left arm, which is secured on a special arm holder and positioned crossing the chest. Depending on how high an exposure is needed, the left flank incision is made along the 9th, 10th, or 11th rib. The selected rib is carefully dissected free from the intercostal neurovascular bundle on its underside. The peritoneal envelop is identified laterally and posteriorly and the dissection carried out as previously described for transperitoneal medial visceral rotation. In patients with suspected acute ischemia, the surgeon may need to enter the peritoneal cavity at the conclusion of the procedure to assess bowel viability.
Sweet Sedge (Calamus). Venlafaxine.
- How does Calamus work?
- Ulcers, gas, upset stomach, appetite stimulation, arthritis, strokes, and skin disorders.
- Are there any interactions with medications?
- Dosing considerations for Calamus.
- Are there safety concerns?
- What is Calamus?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96757
Venlafaxine 75 mg online
Drugs that alter the ion flux affect the resting transmembrane potential difference anxiety symptoms high blood pressure discount venlafaxine 37.5mg mastercard. The larger this difference, the further the neuron is from its firing threshold and the less likely that it will fire (ie, initiate an action potential). The smaller the transmembrane potential difference, the more likely it is that the neuron will reach this threshold and fire. Somatic afferent neurons transmit sensory information about normal status (eg, proprioception) or pathologic states (eg, heat and mechanical damage) to the spinal cord and brain. Drugs can selectively modulate the activity of afferent or efferent pathways: those that excite afferent nociceptive neurons produce pain; those that inhibit afferent nociceptive neurons are analgesic. Those that excite efferent, or neuromuscular, junctions produce tetanus; those that inhibit these junctions cause paralysis. Neuromuscular junction (motor endplate) (longitudinal section) Schwann cell Axon terminal in synaptic trough Axoplasm Myelin sheath Sarcolemma Sarcoplasm Muscle cell nucleus Myofibrils B. Synaptic trough (cross section) Schwann cell Sarcolemma Axoplasm Axolemma Mitochondria Synaptic vesicles Synaptic cleft Folds of sarcolemma Sarcoplasm D. Acetylcholine release (in response to an action potential in presynaptic neuron) Axon terminal C. Acetylcholine synthesis Choline Acetate Acetylcholine Synaptic vesicles Axolemma Basement membrane Sarcolemma E. The axon-muscle interface forms at a synaptic trough, which has extensive foldings that increase the surface area of exposure to a neurotransmitter (B). Ion flux then increases and the postsynaptic membrane depolarizes (E), which triggers an action potential that leads to muscle contraction. Information is transmitted across this gap via chemical transmitters (neurotransmission). Neurotransmitters are commonly stored in presynaptic vesicles; arrival of an action potential stimulates a Ca2+-dependent neurotransmitter release into the synapse. The neurotransmitter crosses the gap and binds to highly selective receptor molecules on the postsynaptic cell, thereby modifying the activity of the postsynaptic cell. Unwanted effects are bradycardia, prolonged paralysis, and malignant hyperthermia. Sympathetic neurons mediate fight or flight responses (pupil dilation, bronchodilation, increased heart rate). Parasympathetic neurons usually mediate the opposite response and control daily functions such as peristalsis, saliva flow, and near vision accommodation. The response is rapid and widespread and includes pupil dilation (mydriasis) for better vision, and increased heart rate, bronchodilation, and vasodilation of blood vessels supplying skeletal muscles for increased energy supply. Simultaneously, parasympathetic activity is depressed, and functions not needed immediately for survival are dampened. The release of the hormone epinephrine (also called adrenaline) from the adrenal (suprarenal) gland is part of the fight or flight response. The closely related neurotransmitter norepinephrine (noradrenaline) elicits nearly the same effects but does so locally. Activation of these responses by a real threat elicits a beneficial, magnified, short-term response; prolonged activation (stress) has harmful effects. Most available sympathomimetics-ie, drugs or other chemicals that mimic fight or flight responses-target a subset of fight or flight responses. For example, phenylephrine, a common component of decongestants, produces vasodilation of nasal blood vessels but has relatively little effect on the heart. Some substances are sympathomimetic because they amplify epinephrine or norepinephrine release. Examples include ephedrine (the active ingredient of ephedra, or Ma-huang, which is banned in the United States because of adverse effects), amphetamines (synthesized in the 1930s as an alternative to ephedra), and tyramine (present in fermented foods). Knowing the identity and synaptic distribution of neurotransmitters can offer insight into the therapeutic action or adverse effects of a drug, which can often be predicted. Norepinephrine, or noradrenaline, is the neurotransmitter at most postganglionic sympathetic synapses. Drugs that mimic or potentiate norepinephrine produce sympathetic effects that resemble fight or flight responses such as increased heart rate. Acute angle closure results in marked increase in intraocular pressure with conjunctival hyperemia, corneal edema, and fixed middilated pupil. Superior cervical sympathetic ganglion Preganglionic sympathetic Postganglionic sympathetic Preganglionic parasympathetic Postganglionic parasympathetic Canal of Schlemm Episcleral vein Cornea Sphincter Dilator Pupil -Adrenergic antagonists and -adrenergic agonists decrease aqueous inflow. Parasympathetic activity opens pores in the trabecular meshwork and enhances outflow of aqueous humor into the canal of Schlemm. Sympathetic activity on the ciliary epithelium increases the secretion of aqueous humor. Cholinergic agonists such as pilocarpine, which enhance aqueous humor outflow, and adrenergic antagonists such as timolol, which decrease aqueous humor inflow, ameliorate symptoms of glaucoma. The receptors were named on the basis of selective actions of nicotine and muscarine (from the mushroom Amanita muscaria). Muscarinic antagonists such as atropine (derived from Atropa belladonna) and scopolamine have the opposite effects. Nicotinic agonists such as succinylcholine stimulate, and nicotinic antagonists such as pancuronium inhibit, skeletal muscle contraction. Clinical Manifestations Regional distribution of muscle weakness 95% 60% 30% 10% Ptosis and weakness of smile are common early signs. Improvement after edrophonium chloride In early stages, patient may feel fine in the morning but develops diplopia and speech slurs later in the day. The same adrenergic agonist (eg, epinephrine, norepinephrine, or drug) can produce various effects depending on the G protein coupling in a cell. Effects of receptor activation include muscle contraction (1, 2) and relaxation (1, 2, 2), increased heart rate and force (1), and lipolysis and thermogenesis (3). Sympathetic effects can be produced by drugs that either enhance sympathetic tone (sympathomimetics such as adrenoceptor agonists) or depress parasympathetic tone (cholinergic receptor antagonists). Parasympathetic effects can be produced by drugs that either enhance parasympathetic tone or depress sympathetic tone. Drugs enhancing neurotransmitter action by activating receptors are known as direct acting; drugs enhancing neurotransmitter action by some other means, eg, by inhibiting enzymes that degrade the neurotransmitter, are known as indirect acting. The therapeutic and adverse effects of a drug are sometimes a function of intended use. Also, drugs that have different therapeutic targets can share a similar side effect. Drug treatment of these disorders developed partly as the result of serendipity and, more recently, targeted drug discovery efforts. For example, it is now recognized that clinical depression and clinical anxiety are biochemically distinct from normally experienced feelings of sadness or apprehen sion. Schizophrenia is now known to consist of what are known as positive and negative symptoms. Neuronal atrophy is implicated in conditions in which it was not previously suspected. Such abuse can adversely affect the availabil ity of these drugs (such as opioids for relief of severe pain) to patients in need. There is something special and inherently compelling about drugs that affect behavior or cognitive processes. X (vagus) optic stalk (sensory and motor) Opening of right telencephalic vesicle Hindbrain (myelencephalon) Lamina terminalis 78. The neural tube develops bulges, bends, and crevices that form mature brain structures and ventricles. Three major bulges appear by approximately day 28 of gestation: the forebrain (prosencephalon), midbrain (mesencephalon), and hindbrain (rhombencephalon). At approximately day 36, the pos terior (caudal) portion of the forebrain develops into the dien cephalon; the anterior part develops into the telencephalon (eventually cerebral hemispheres). The cerebral cortex has a specific outline by 6 months but develops sulci and gyri only in the 3 months before birth. The developing brain is affected, espe cially in the first trimester, to injuries caused by various chemi cals such as drugs. Efforts aimed to identify these substances and design drugs that will facilitate or enhance their actions are ongoing.
Venlafaxine 75 mg with visa
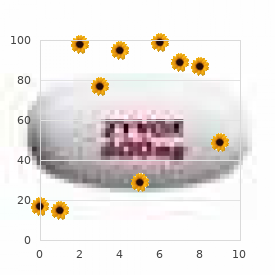
With a few exceptions anxiety symptoms arm pain generic 150 mg venlafaxine mastercard, most major anatomic anomalies are associated with aneuploidy. Trisomy 21 Trisomy 18 Trisomy 13 Normal Normal Turner Syndrome (45,X) Mild or if hydrops or if hydrops Anomalies, Markers, & Aneuploidy Incidence Isolated Markers nuchal fold 6 mm Small or absent nasal bone Echogenic bowel Short humerus Short femur Pelviectasis Intracardiac echogenic focus Choroid plexus cyst Single umbilical artery Anomalies Cystic hygroma Holoprosencephaly Cardiac defect Omphalocele Diaphragmatic hernia Duodenal atresia Bladder outlet obstruction Mild ventriculomegaly 1/6,000 1/16,000 7-9/1,000 1/5,800 1/3,500-4,000 1/10,000 1-2/1,000 7-15/1,000 50-75% 40-60% 5-30% 40-70% 30-40% 20-25% 20-30% 20-25% 5% Turner > T21 > T18 > T13 T13 > T18 T21, T18, T13, abnormal 22, 8, 9 T21 T18 > T13 T18, T13, T21, Turner T21 T13, T18 T21 > T18, T13 0. The 11- to 14-week scan: the diagnosis of fetal abnormalities from the Diploma in Fetal Medicine series, 1999. The unfused amnion can be seen separate from the fetal skin & should not be mistaken for fetal skin. In addition, the image is adequately magnified to include only the fetal head, neck, & upper chest. The A peak here is normal, but there is an additional small retrograde peak, secondary to inclusion of flow in the inferior vena cava. Findings are classic for holoprosencephaly, a hallmark anomaly seen in trisomy 13. Physiologic bowel herniation occurs at the cord base & resolves by 12 weeks; therefore, the diagnosis of gastroschisis can be made at 13 weeks. The presence of anteriorly displaced bony palate is usually from bilateral cleft lip & palate. The nuchal fold (calipers) is increased, & there is a small ventricular septal defect. Maternal serum screen results were also suspicious for T21 and amniocentesis in the 2nd trimester was performed, diagnostic for T21. This finding is considered both a marker for aneuploidy and potential progressive hydronephrosis. Abele H et al: First trimester ultrasound screening for Down syndrome based on maternal age, fetal nuchal translucency and different combinations of the additional markers nasal bone, tricuspid and ductus venosus flow. Trisomy 21 Aneuploidy (Left) 3D ultrasound of the back of the neck shows nuchal fold thickening in a 2nd trimester fetus with T21. Amniocentesis, in this case, ruled out the other diagnoses and was diagnostic for T21. Even as an isolated finding, most lowrisk patients become high risk when the nasal bone is small or absent, and genetic counseling is recommended for this finding. T21 can present with fetal anasarca and hydrops from lymphatic malformation or cardiac failure. Thoracentesis revealed chylothorax, a lymphatic defect, and placement of a shunt reversed the hydrops. Fetuses with T21 are at increased risk for leukemia, most commonly transient abnormal myelopoiesis, which presents as hepatosplenomegaly and has an excellent prognosis. Red Doppler signal is from fluid traveling toward the transducer, out of the duodenum. On the reconstructed 3D image, there is 5th finger clinodactyly, a soft marker which can be seen with T21. The middle phalanx is short, leading to curvature of the tip of the little finger toward the ring finger. As an isolated finding in a low-risk patient, clinodactyly is considered idiopathic and sometimes seen in multiple other normal family members. Fetal tongue is enlarged and was seen extending outside the mouth for the duration of the exam. A persistent gap was seen between the 1st and 2nd toe in this fetus with multiple other anomalies and T21. Subtle extremity findings including sandal gap and clinodactyly are more often seen in normal fetuses than T21. On the sagittal view through the head, chest, and upper abdomen, an omphalocele and ventriculomegaly are seen. Not one hallmark anomaly is associated with T18; however, the diagnosis should be suspected in fetuses with multiple anomalies in different organ systems. The hand is held clenched with overlapping fingers, and the index finger typically overlaps the other clenched fingers. Trisomy 18 Aneuploidy (Left) Axial view through the calvarium in this midgestation fetus with T18 shows narrow frontal bones and lateral calvarial bulging, giving the head a strawberry shape. The presence of several abnormalities, some subtle, led to amniocentesis in this low-risk patient. Approximately 1/2 of pregnancies that do not terminate result in a liveborn child. Posterior fossa anomalies are associated with aneuploidy and T18 is the most common association. There is only 1 bone in the forearm, and the radius is missing (note the humerus). The hind foot is convex (like the bottom of a rocking chair) and the toes are upturned. Chorionic villus sampling was performed on the same day, and the diagnosis of T18 was made early in the pregnancy. Although a hallmark finding for Turner syndrome (cystic hygroma) and a hallmark finding for T13 (holoprosencephaly) are seen, this fetus has T18 (a diagnosis without a hallmark anomaly). The patient chose to have chorionic villus sampling on the same day and the results showed trisomy 13 (T13). Other anomalies were seen in this case, including outflow tract anomalies of the heart. Patients may better appreciate facial anomalies when 3D images are reviewed with them. Six digits can be counted beginning with the thumb, with the extra digit on the ulnar side. There is a premaxillary protrusion of tissue caused by dysplastic anterior palate and soft tissue from bilateral cleft lip and palate. The subtle bilateral cleft lip soft tissue defect is seen best on the axial image. The coronal surface-rendered image shows the mass-like protruding palate typical of bilateral cleft lip and palate. The falx is absent and soft tissue seen anterior to the calvarium is from a proboscis. A spectrum of facial features is associated with holoprosencephaly; however, proboscis and hypotelorism/cyclopia are classic findings. Although this was a near-term infant, notice the extremely immature appearance of the cerebral cortex, without discernible gyri and sulci. Over 90% of Turner syndrome cases will have abnormal findings in the 1st trimester. Most, but not all, fetuses with Turner syndrome diagnosed prenatally will suffer in utero fetal demise. Christiansen M et al: Nuchal translucency distributions for different chromosomal anomalies in a large unselected population cohort. Turner Syndrome (45,X) Aneuploidy (Left) In this fetus with Turner syndrome and oligohydramnios, the lateral neck cystic hygroma mimics pockets of amniotic fluid. If necessary, cystic hygroma fluid can be aspirated and sent for genetic analysis. The renal parenchyma is echogenic, suggesting parenchymal dysplasia, and the inferior poles are joined via an isthmus. Lymphatic malformation and aortic anomalies are hallmark findings with Turner syndrome. The head is significantly larger than the abdomen, although, both were smaller than expected for gestational age. There is also bilateral syndactyly of the 3rd and 4th digits, a common feature in triploidy. Fleischer J et al: Digynic triploidy: utility and challenges of noninvasive prenatal testing. Triploidy karyotype occurs in 1% of all conceptions and 10% of spontaneous abortions.
Buy venlafaxine 150mg free shipping
Mediastinal involvement occurs in ~ 2/3 of pediatric patients with Hodgkin lymphoma anxiety brain discount venlafaxine. While this is a normal finding in infants due to the thymus, it is not normal in older children or adolescents & indicates the presence of an anterior mediastinal mass. This mediastinal mass can be distinguished from the thymus due to its lobular contour & patient age. Approximately 80% of pediatric patients with Hodgkin lymphoma present with painless cervical adenopathy. There are 3 potential patterns of lung involvement in lymphoma: Pulmonary nodules, reticular interstitial pattern, & airspace consolidation. Pulmonary involvement in non-Hodgkin lymphoma is uncommon, occurring in 5% of patients. Nonseminomatous germ cell tumors can metastasize to the lymph nodes, lung, & liver. This is larger than typically seen for normal thymus, & the right hemidiaphragm is mildly depressed. The mass is mostly fluid density but shows a nodule inferiorly that contains fat & calcium. Germ cell tumors of the heart & pericardium occur less frequently than in the anterior mediastinum. There is mild splaying of the left 8th9th ribs as compared to the right intercostal space at this level. When an elongated paraspinal mass is identified on a chest radiograph in a young child, it should be considered a neuroblastic tumor until proven otherwise. The mass involves > 1/3 of the spinal canal diameter & lifts the aorta off of the spine, partially encasing it. Also note the poorly defined, hypoenhancing foci in the liver, consistent with distant metastases. The suspected 6th rib fracture was also confirmed by visualization of callus formation. Also present are healing posterior rib fractures with subtle rib broadening with callus. Multiple fractures of varying ages are highly concerning for nonaccidental trauma. Associated rib fractures are less frequent in pediatric patients (as compared to adults) due to the pliability of the rib cage. A small round lucent focus in the left lower lobe is consistent with a laceration. Scattered patchy & groundglass opacities are also present in the right middle & bilateral lower lobes, consistent with contusions. Also note the widened mediastinum & prominent paraspinal soft tissue density behind the heart. Note how the large mediastinal hematoma causes rightward deviation of the nasogastric tube. The regional fat is slightly increased in attenuation from mediastinal hemorrhage. Subsequent bronchoscopy demonstrated an aspirated peanut in the left main bronchus. Other findings include left upper lobe contusions, a right pneumothorax, & subcutaneous emphysema. Note the asymmetric geographic areas of air-space opacity & volume loss that mostly involve the right lung. Despite the lung window settings, numerous fat-containing lesions can be seen throughout the kidneys, typical of renal angiomyolipomas. Note the peribronchovascular distribution of cysts reflecting the bronchiolocentric nature of the disease. Narayanan S et al: Relevance of chest radiography in pediatric inpatients with asthma. Ober C et al: the genetics of asthma and allergic disease: a 21st century perspective. Bisgaard H et al: Long-term studies of the natural history of asthma in childhood. There is resulting airspace opacity as well as volume loss causing elevation of the right hemidiaphragm & slight mediastinal shift. The left lower lobe is relatively hyperlucent due to airtrapping, & there are widespread patchy airspace opacities due to aspiration. In the correct clinical setting, static lung volumes on inspiratory & expiratory or bilateral decubitus chest radiographs are very suggestive of air-trapping due to foreign body aspiration. Depending on the degree of bronchial occlusion, a foreign body may cause atelectasis, hyperexpansion, or a changing picture over time. Note the signet ring sign (or pearl ring sign) in the right upper lobe with the dilated bronchus forming the ring & the adjacent artery forming the attached jewel. Mucus impacted in the dilated bronchi is referred to as a finger-in-glove appearance. Evaluation of the more distal branches & adjacent parenchyma (for alveolar hemorrhage & extravasation) may help localize the source of bleeding. Notice the narrowing of the trachea with soft tissue swelling around the metallic foreign body. Acute chest syndrome is defined as a new pulmonary opacity in a symptomatic patient with sickle cell disease. Perfusion defects in sickle cell disease may represent acute or chronic infarction. The vertebral bodies have an abnormal Hshaped configuration typical of sickle cell disease. Other bone findings in sickle cell disease include sclerotic bone infarcts & enlargement of the ribs due to marrow expansion. The left-to-right (blue line) & anterior-to-posterior (sagittal yellow line) diameters are measured, & the ratio is calculated as X/Y. Note the small left postoperative pleural effusion & passive left lower lobe atelectasis. There is complete opacification of the right hemithorax with mass effect on the mediastinum. A heterogeneous mass in the left upper hemithorax is partly cystic & extends into the soft tissues of the left lower neck. Some lesions shows abnormal fatty deposition compared to normal (for this age) vertebral marrow, while other lesions show increased fluid signal intensity. Situs Evaluation of situs involves the designation of an individual as normal (situs solitus), reversed (situs inversus), or some other combination (situs ambiguous). The tracheobronchial branching in situs solitus includes a trilobed lung & main bronchus that sits posteriorly &/or superiorly to the pulmonary artery (eparterial bronchus) on the right & a bilobed lung with a main bronchus sitting below the pulmonary artery on the left (hyparterial bronchus). In the heart, be aware of symmetric atria & appendages in patients with heterotaxy as these may represent 2 right atria or 2 left atria in right or left isomerism. It is usually not difficult to differentiate the ventricles based on the prominence of the trabeculations. The right ventricle may more confidently be identified by the presence of a moderator band (muscular fibers connecting the free wall of the right ventricle to the interventricular septum). Also, pay attention to the tracheobronchial branching relative to the pulmonary arteries: It may be abnormal bilateral left-sided branching (hyparterial bronchi) or bilateral right-sided branching (eparterial bronchi). These include pig bronchus, congenital stenosis, & bilateral right- or left-sided tracheobronchial branching seen with heterotaxy syndromes. More common than congenital airway anomalies is airway compression from cardiomegaly & enlarged or anomalous vasculature.
