
Buy aygestin toronto
The embryos are then transferred back into the uterine cavity via in vitro fertilization menstruation 1800s buy aygestin 5mg visa. When the initial infertility evaluation reveals no cause, the problem often involves abnormalities in sperm transport, the presence of antisperm antibodies, or problems with penetration and fertilization of the egg. When no cause for infertility is identified after in-depth testing, studies show that most therapies for unexplained infertility have no higher success rates than no treatment at all. The eventual pregnancy rate for couples with unexplained infertility who receive no treatment approaches 60% over 3 to 5 years. Other options include use of donor sperm, gestational surrogacy, adoption, or acceptance of childlessness. About 85% to 90% of infertility cases can be treated with drug therapy or surgery. Clomid is generally administered orally to women with absent or infrequent ovulation, starting on day 3 or 5 of the follicular phase of the menstrual cycle for approximately 5 days. Letrozole (Femara) is an aromatase inhibitor that decreases the conversion of androgens (testosterone and androstenedione) to estrogens (estradiol and estrone) (Table 26-5). They are administered via intramuscular injection during the follicular phase of the menstrual cycle. Monitoring decreases the risk of both multiple gestations and ovarian hyperstimulation. Progesterone is often used to promote endometrial receptivity beginning after embryo transfer and lasting through the first trimester. Any remaining embryos are saved using cryopreservation techniques for future cycles, embryo donation, or research. Following ovulation induction, multiple eggs are removed from the ovaries by placing a vaginal probe into the vagina. A fine needle is guided toward the ovary while the physician visualizes the follicles on ultrasound. Fluid around the follicles is then collected through a needle connected to a test tube. Effectiveness Clomiphene citrate is successful in inducing ovulation in 80% of correctly selected patients, but <50% will become pregnant. If pregnancy does not occur after three to six cycles of Clomid where ovulation is achieved, then more aggressive therapies are needed. Gonadotropins have an 80% to 90% ovulation success rate and a 10% to 40% pregnancy success rate per cycle depending on the diagnosis (recall fecundity is only 20% to 25% in the general population). Gonadotropins carry a much higher risk of ovarian hyperstimulation (1% to 3%) and multiple gestation pregnancy (20%) than do Clomid and Femara. Side Effects and Complications the potential side effects of Clomid are related to its antiestrogen effects: hot flashes, abdominal distension and bloating, and emotional lability. These side effects are mostly mild and disappear after discontinuation of the medication. Although there is some controversy about the risk of teratogenesis with aromatase inhibitors, care should be taken to rule out pregnancy prior to induction of ovulation for this off-label indication. Multiple gestation pregnancies occur in 8% of Clomid-induced pregnancies and in 20% of pregnancies from gonadotropins. This completely iatrogenic disorder can range from ovarian enlargement and minimal symptoms to significant ovarian enlargement, torsion, or rupture. This may be complicated by ascites, pleural effusions, hemoconcentration, hypercoagulability, electrolyte disturbances, renal failure, and even death. This technique is usually performed when a patient has a known inherited genetic disease, is a carrier of a chromosomal translocation that has resulted in recurrent miscarriages, has an affected child, or is of advanced maternal age with increased risk of aneuploidy. Effectiveness the success rate of these advanced reproductive technologies varies from center to center. Success rates depend on maternal age, diagnosis, the number and quality of oocytes, sperm, and embryos. The most favorable rates are seen among women younger than 35 years, those without hydrosalpinges, and women with adequate ovarian reserve. The most recent published statistics show a live birth rate of 48% in women younger than 35 years and 39% in women aged 35 to 37 years when fresh non-donor embryos are transferred. Again, keep in mind that the normal fecundity rate in a couple without infertility is approximately 20% to 25% per month. This compares with a multiple-infant birth rate of slightly more than 3% in the general U. Guidelines have been established regarding the number of embryos to transfer in various clinical scenarios with the intent of minimizing the risk for multiple gestations. These factors are diagnosed by history and laparoscopy and treated surgically to improve fertility rates. Synechiae, submucosal fibroids, and polyps can be resected; endometritis is treated with antibiotics. Female infertility may also be due to cervical factors, such as cervical stenosis from surgical or mechanical dilation. Male factor infertility may be idiopathic or due to improper coital practices; sexual dysfunction; endocrine disorders; or abnormalities in spermatogenesis, sperm volume, density, or mobility. Male factor infertility is diagnosed by semen analysis and endocrine evaluation if indicated. Over 25% of couples find no explanation for infertility after their initial assessment. When this occurs, further assessment may be done to search for problems with sperm transport, ability to penetrate and fertilize the egg, and antisperm antibodies. Most therapies for unexplained infertility have not been shown to have higher success rates than no treatment. Couples with unexplained infertility who choose no treatment will conceive up to 60% of the time over 3 to 5 year. The primary complications of fertility drugs include ovarian hyperstimulation and multiple gestation pregnancy. Her husband is 33 years old, has had a semen analysis, which was reported as normal. On further history, the patient reports that her periods have been quiet irregular over the last year and that she has not had period in the last 3 months. You have the patient and her husband come back to clinic and gently give them the diagnosis. They have many questions of what this means in terms of their ability to achieve a pregnancy. The patient has no significant medical history and does not take any medications other than prenatal vitamins. Her husband is also in good health, is 30 year of age, and has two children from a previous marriage. When you asked the patient how long they have been trying to achieve a pregnancy, they tell you 6 months. Continue trying appropriately timed intercourse for 6 more months, and if no pregnancy is achieved, come back to see you d. The couple comes back to you after appropriately timed intercourse, not having achieved a pregnancy. Have 6 more months of timed intercourse, and if no pregnancy is achieved, come back to see you b. However, after six cycles with ovulation while on Clomid, a pregnancy had not been achieved. The finding of endometriosis is not typically associated with any type of amenorrhea or oligomenorrhea or any of the other symptoms described. Although Kallmann syndrome is associated with amenorrhea, it is primary amenorrhea rather than secondary amenorrhea. This patient reports a lifelong history of regular menses except for the past year. Similarly, although pregnancy could explain the lack of menses for the past 3 months, pregnancy is not associated with hot flashes, vaginal dryness, or decreased libido. This woman, although young, presents with classic menopausal symptoms associated with low estrogen levels, including hot flashes, night sweats, decreased libido, and vaginal dryness. Answer D: There are several available tests for the assessment of ovarian reserve. Measurement of the day 3 estradiol level assesses ovarian reserve by looking for elevated basal rates of estradiol caused by premature follicle recruitment in women with poor ovarian reserve.
Juniperus virginiana (Eastern Red Cedar). Aygestin.
- What is Eastern Red Cedar?
- Cough, bronchitis, rheumatism, venereal warts, and skin rash.
- Are there safety concerns?
- Are there any interactions with medications?
- Dosing considerations for Eastern Red Cedar.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97062
Buy aygestin 5 mg fast delivery
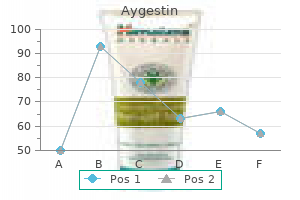
Contractions during labor will increase by 20 to 30 mm Hg in early labor and by 40 to 60 mm Hg as labor progresses menstruation after miscarriage buy aygestin 5 mg overnight delivery. The most commonly used measurement of uterine contractions is the Montevideo unit, which is an average of the variation of the intrauterine pressure from the baseline multiplied by the number of contractions in a 10minute period. Some institutions use the Alexandria unit, which multiplies the Montevideo units by the length of each contraction as well. Note that each deceleration returns to baseline before the completion of the contraction. Fetal blood is obtained by making a small nick in the fetal scalp and drawing up a small amount of fetal blood into capillary tubes. Care must be taken to avoid contamination of the blood sample with amniotic fluid, which is basic and will elevate the results falsely. Although this tool is used less frequently now that technology has improved fetal monitoring, it can still provide additional information on fetal well-being. Interestingly, it is almost never used in the United States any longer, but still used in 5% or more of fetuses in the United Kingdom. After making a small stab incision in the fetal scalp, the blood is drawn off through a capillary tube. Another modality for assessing fetal status that is still experimental at this point is fetal pulse oximetry. Using technology similar to the monitors placed on ears, fingers, and toes, the fetal pulse oximeter is placed intrauterine along the fetal cheek and measures fetal oxygen saturation. Because fetal variability and decelerations have a poor predictive value of fetal hypoxemia and acidemia, it is theorized that the fetal pulse oximeter would be useful in such patients. A large, multicenter trial demonstrated that many of these fetuses with nonreassuring tracings do have normal pulse oximeter readings. However, the use of the pulse oximeter did not have an effect on either the cesarean delivery rate or fetal outcomes. Although initial studies were promising, with lower cesarean rates and lower rates of neonatal acidemia, a recent, large trial in the United States showed no benefit of either reducing cesareans or reducing neonatal acidemia at delivery. To assess the progress of labor, it is important to understand the cardinal movements or mechanisms of labor. When the fetal presenting part enters the pelvis, it is said to have undergone engagement. The head will then undergo descent into the pelvis, followed by flexion, which allows the smallest diameter to present to the pelvis. As the vertex passes beneath and beyond the pubic symphysis, it will extend to deliver. Once the head delivers, external rotation occurs and the shoulders may be delivered. Stage 1 begins with the onset of labor and lasts until dilation and effacement of the cervix are completed. Stage 3 begins after delivery of the infant and ends with delivery of the placenta. Stage 1 the first stage of labor ranges from the onset of labor until complete dilation of the cervix has occurred. An average first stage of labor lasts approximately 10 to 12 hours in a nulliparous patient and 6 to 8 hours in a multiparous patient. The range of what is considered within normal limits is quite wide, from 6 hours up to 20 hours in a nulliparous patient and from 2 to 12 hours in a multiparous patient. The active phase follows the latent phase and extends until complete dilation, and is defined by the period of time when the slope of cervical change against time is at its maximum. A third phase has been delegated just prior to complete dilation called deceleration or transition phase. Historically, the values of the length of the first stage were primarily derived from studies of labor by Dr. This minimal expectation was approximately the fifth percentile of women undergoing labor, and the median rates of dilation range from 2. However, studies over the last decade reveal longer first and second stages of labor and variation by maternal race/ethnicity, age, and body habitus; thus, longer norms have been created and the new threshold for active labor of 6 cm. The three "Ps"-powers, passenger, and pelvis-can all affect the transit time during the active phase of labor. The "powers" are determined by the strength and frequency of uterine contractions. The size and position of the infant affect the duration of the active phase, as do the size and shape of the maternal pelvis. If there is no change in either cervical dilation or station for 2 hours in the setting of adequate Montevideo units during the active phase of labor, this is deemed active phase arrest and is an extremely common indication for cesarean. However, in the past decade, several studies have indicated that if clinicians exhibited more patience in this setting by waiting up to 4 or more hours to make this diagnosis, then more than half of these women will go on to deliver vaginally. Although the issue deserves more research, in a setting with continuous fetal monitoring and no worrisome signs from either the mother or the fetus, it appears reasonable to manage such pregnancies expectantly to allow for the possibility of vaginal birth. Stage 2 is considered prolonged if its duration is longer than 3 hours in a nulliparous patient, although at least an extra hour is allowed in patients who have epidurals. In multiparous women, stage 2 is prolonged if its duration is longer than 2 hours without an epidural and at least 3 hours with an epidural. In multiparous women without an epidural, it is rare for stage 2 to last longer than 60 minutes unless there is fetal macrosomia, persistent occiput posterior or transverse position, compound presentation, or asynclitism. However, epidurals can have a profound effect on the length of the second stage in both nulliparous and multiparous women. One reason for the effect on the second stage is that often women will have little urge to push, little sensation, and even a strong motor block and so have less ability to push. Often, such patients are given an hour or two without pushing at the beginning of the second stage; this is called "laboring down" or "passive descent. Traditionally, it was perceived that a prolonged second stage of labor may lead to worse neonatal outcomes. However, recent studies of the length of the second stage of labor have not actually demonstrated a difference in neonatal outcomes with prolonged second stage of labor in the setting of fetal heart rate monitoring. There also remains a concern that prolonged second stage of labor will lead to higher rates of maternal urinary incontinence and pelvic relaxation, but to date, no large, prospective studies have been performed. Monitoring Repetitive early and variable decelerations are common during the second stage. The clinician can be reassured if these decelerations resolve quickly after each contraction and there is no loss of variability in the tracing. Repetitive late decelerations, bradycardias, and loss of variability are all signs of nonreassuring fetal status. If a prolonged deceleration is felt to be the result of uterine hypertonus (a single contraction lasting 2 minutes or longer) or tachysystole (greater than five contractions in a 10-minute period), which can be diagnosed by palpation or examination of the tocometer, the patient can be given a dose of terbutaline to help relax the uterus. If a nonreassuring pattern does not resolve with these interventions, the fetal position and station should be assessed to determine whether an operative vaginal delivery can be performed. If fetal station is above 0 station (though many clinicians will require the fetus to be +2 station or lower) or the position cannot be determined, cesarean delivery is the mode of choice. More recently, it has been recognized that uterine tachysystole, even in the setting of no fetal heart rate decelerations, can lead to higher rates of complications. If uterine tachysystole with a Category I tracing occurs spontaneously, it deserves close follow-up. Vaginal Delivery As the fetus begins crowning, the delivering clinician should be dressed with eye protection, sterile gown, and sterile gloves (for self-protection as much as for prevention of maternal/fetal infection) and have two clamps, scissors, and suction bulb. Historically, when meconium was suspected or confirmed many units used a DeLee suction trap to aspirate meconium from the neonatal airway after the head is delivered and prior to delivery of the rest of the body before breaths can be taken. However, after a large, prospective, randomized trial was conducted and demonstrated no benefit from such suctioning, the routine use of the DeLee for meconium is no longer recommended. Near completion of the delivery of the fetal head by the modified Ritgen maneuver. Moderate upward pressure is applied to the fetal chin by the posterior hand covered with a sterile towel while the suboccipital region of the fetal head is held against the symphysis. Various approaches can be taken to vaginal delivery, but most clinicians would agree that a smooth, controlled delivery leads to less perineal trauma. Thus, one hand is commonly used to support or massage the perineum, while the other hand is used to flex the head to keep it from extending too quickly and causing periurethral or labial lacerations.
Discount 5mg aygestin overnight delivery
Answer E: Chorioamnionitis/Triple I is the most common precursor of neonatal sepsis womens health toning station purchase aygestin master card, which has a high rate of fetal mortality. The most common maternal complications include dysfunctional labor and need for cesarean section, uterine atony, and postpartum hemorrhage. Classically, this mild infection presents with a low-grade fever and a red macular rash giving the "slapped cheek" appearance and usually resolves with minimal intervention. Approximately one-third to one-half of pregnant women have IgG to the virus and are immune from a prior infection. Among pregnant women who do not have immunity, the incidence of acute parvovirus infection during pregnancy is around 3%. Answer A: Acute parvovirus infections during pregnancy may be transmitted through the placenta to the fetus. First-trimester infections have been associated with miscarriage, but midtrimester and later infections are associated with fetal anemia and hydrops. If studies indicate an acute parvovirus infection (positive IgM and positive or negative IgG) beyond 20 weeks of gestation, then the fetus should undergo serial ultrasounds, up to 8 to 10 weeks after maternal infection. Small studies have shown a benefit of fetal transfusion for fetal anemia leading to hydrops; however, these studies also reported fetal deaths from complications related to transfusion, so this procedure is likely to be reserved for the most severe cases. Parvovirus can also lead to pancytopenia in the fetus, and this has important clinical implications because fetal thrombocytopenia can increase the risk of exsanguination and fetal death during attempts at intrauterine transfusion. It is also important to note that this mechanism for fetal anemia is different from that of Rh alloimmunization, which leads to fetal anemia via hemolysis. Transmission occurs in utero (one-third), generally late in pregnancy or during labor and delivery (two-third). In resource-poor nations, breastfeeding is encouraged because of increased risk of neonatal mortality from diarrheal diseases, pneumonia, and other infectious diseases. Standard precautions and good hand washing behavior should always be encouraged because they may not lower the risk of transmission but would not increase the risk either. In this chapter, a variety of the other common medical complications of pregnancy are discussed. Pregnancy affects every physiologic system in the body as well as many disease states. Disease management in pregnancy requires consideration of any potential fetal effects of treatment or imaging modalities. Additionally, progesterone decreases gastric motility and relaxes the esophageal sphincter that can contribute to nausea and vomiting in pregnancy. Despite nausea and vomiting in early pregnancy, patients are usually able to maintain adequate nutrition. However, some women can become significantly dehydrated and potentially develop electrolyte abnormalities. The diagnosis of hyperemesis gravidarum is made when a woman has persistent vomiting, weight loss of greater than 5% of prepregnancy body weight, and ketonuria. Persistent nausea and vomiting during pregnancy can be treated with vitamin B6 and doxylamine (Unisom). Ginger and supplementation with vitamin B12 have been shown to be effective and can be used as adjuncts to antiemetic therapy. First-line antiemetic therapy is usually with promethazine, followed by the addition of metoclopromide, prochlorperazine, and Tigan. If symptoms persist to dehydration, patients should be rehydrated and electrolyte abnormalities corrected. In the acute setting, antiemetics should be given intravenously, intramuscularly, or as suppositories because oral medications may be vomited prior to systemic absorption. Long-term management of hyperemesis includes maintaining hydration, adequate nutrition, and symptomatic relief from the nausea and vomiting. Once they are rehydrated, they can use the antiemetic to control nausea so that they are able to maintain oral intake. In addition, because hypoglycemia may contribute to nausea, frequent small meals can help to maintain more stable blood glucose and decrease nausea. In these cases, treatment with corticosteroids has been shown to decrease symptoms. Other alternative treatments shown to decrease nausea include acupuncture, acupressure, hypnotherapy, and nerve stimulation. A small percentage of patients for whom the treatment fails will require feeding tubes or even parenteral nutrition for the course of the pregnancy. As long as hydration and adequate nutrition are maintained, pregnancy outcomes are usually good. Seizures have implications for fetal and maternal health, and concerns during these pregnancies include risk of fetal malformations, miscarriage, perinatal death, and increased seizure frequency. The combination of these factors is thought to contribute to increased seizure frequency in 17% to 33% of pregnancies. There are a variety of possible etiologies proposed for the increase in seizure frequency seen in some pregnancies. In addition, renal function increases during pregnancy with a 50% rise in creatinine clearance that affects the metabolism of carbamazepine, primidone, and the benzodiazepines. Hormonal changes, added stress, and decreased sleep during pregnancy likely lower seizure threshold and have been shown to increase seizure frequency in nonpregnant patients. Increased levels of estrogen and progesterone may both have direct effects on seizure activity during pregnancy. Thus, rising estrogen levels in pregnancy that peak in the third trimester may have some impact on the observed increase in seizure frequency. It has been observed that women with seizure disorders have fewer seizures during the luteal phase of the menstrual cycle. Sleep deprivation and stress may also play a role in increased seizures in pregnancy. The best predictor of seizure frequency in pregnancy appears to be the amount of seizures in the year prior to pregnancy. Since then, unique malformations and syndromes have been ascribed to phenytoin, phenobarbital, primidone, valproate, carbamazepine, and trimethadione. Ideally, a patient is started on or transitioned to a single medication with the lowest risk of malformation (lamotrigine, levetiracetam, and oxacarbemazepine) preconception. Specific increases in congenital abnormalities seen in infants born to epileptic mothers include a fourfold increase in cleft lip and palate, and a three- to fourfold increase in cardiac anomalies. Lamotrigine has the lowest risk at 0% to 2%, and baseline risk of women with epilepsy is 1% to 3%. Recent studies in teratogenesis-particularly in the fetal hydantoin syndrome-point to a genetic predilection for the generation of epoxides. Specifically, children whose enzyme activity of epoxide hydrolase is onethird less than normal have an increased rate of fetal hydantoin syndrome. Anomalies have also been observed in children exposed to carbamazepine with low epoxide hydrolase activity. Because there is particular evidence that high peak plasma levels of valproic acid may be more teratogenic than constant steady-state levels, it should be dosed three to four times per day rather than the standard twice per day dosing. However, epileptic patients should be counseled that they are still at a greater risk (4% to 6% vs. Therefore, patients should be advised to take supplemental folate prior to conception, particularly those using either valproic acid or carbamazepine. The decision to perform an amniocentesis routinely for -fetoprotein and acetylcholinesterase is controversial. All care providers-obstetricians, neurology, nursing, anesthesia, and pediatrics-should be informed about an epileptic patient in labor and delivery. Because trauma and hypoxia from a seizure can put both the mother and the fetus at risk, treatment of seizures should be discussed a priori with the group of practitioners caring for the patient. One difference is that the drug of choice in patients with a known seizure disorder is usually phenytoin compared with magnesium used in preeclamptic patients. There have been reports of increased risk of spontaneous hemorrhage in newborns because of the inhibition of vitamin K-dependent clotting factors. Although the risk is small, conservative management is to overcome this theoretical vitamin K deficiency by aggressive supplementation with vitamin K toward the end of pregnancy. Upon delivery, clotting studies can be performed on the cord blood and vitamin K administered to the infant.
Order on line aygestin
Similar to the imperforate hymen menopause 10 years after hysterectomy purchase cheap aygestin line, diagnosis is usually made at the time of puberty in adolescents who present with primary amenorrhea and cyclic pelvic pain accompanied by menstrual symptoms. On physical examination, patients typically have normal external female genitalia, and a short vagina that appears to end in a blind pouch. The transverse vaginal septa are usually less than 1 cm thick and may have a central perforation. It occurs when the lower vagina fails to develop and is replaced by fibrous tissue. Physical examination reveals the absence of an introitus and the presence of a vaginal dimple. Surgical correction can be achieved by incising the fibrous tissue, and dissecting it until the normal upper vagina is identified. Any accumulated blood or materials can be evacuated, and the normal upper vaginal mucosa is then brought down to the introitus and sutured to the hymenal ring. These patients typically have normal external genitalia, normal secondary sexual characteristics (breast development, axillary, and pubic hair), and normal ovarian function. In motivated patients, a vagina can be created using serial vaginal dilators pressed into the perineal body (Frank and Ingram procedures). If this nonsurgical approach fails, a variety of vaginal, laparoscopic, and abdominal procedures are available to create a neovagina. A transverse incision is then made at the vaginal dimple and the fibrous tissue in the location of the normal vagina. Once the mold is removed, dilators must still be used for several months to maintain vaginal patency. Although normal sexual intercourse is possible after these surgical and nonsurgical procedures, the patient will be unable to carry a pregnancy. This classification system allows gynecologists, dermatologists, and pathologists to use a shared terminology for these disorders. These lesions often require histologic examination (Table 13-1) to identify and treat the disorder and to differentiate the lesion from vulvar and vaginal intraepithelial neoplasia and cancer (Chapter 27). The etiology is unknown, but it may be autoimmune related with secondary genetic and hormonal influences. Classic changes involve white hypopigmented plaques on the vulva, perineum, and perianal areas. Can scar Symptoms Often asymptomatic; May report itching, pain, dysuria, dyspareunia; Chronic waxing and waning course Treatment Options High-potency topical steroid ointment (clobetasol or halobetasol 0. Can have narrowed introitus with inflamed vagina from erosions; may have vaginal adhesions or occlusion. Does not scar Red moist lesions; often nonspecific with poor margins and slight scaling. May find more classic psoriasis with welldemarcated heavy Pruritus with mild inflammation to severe erosions. Lichen planus is an uncommon inflammatory skin condition that can affect the nails, scalp, and skin mucosa. Patients may also complain of pruritis, burning, irritation, and painful intercourse. This inflammatory dermatosis results in chronic eruption of shiny purple papules with white striae on the vulva. Similar lesions are often found on the flexor surfaces, and mucous membrane of the oral cavity. It generally occurs in women in their 50s or 60s, and it is associated with a 3% to 5% risk of vulvar skin cancer. Vulvar psoriasis may be a feature of psoriasis-a very common skin rash that affects up to 2% of the population. There are several different types, but the usual form appears as silvery-red scaly patches over the elbows and knees. Vulvar psoriasis can occur as part of more general disease but in some people, it affects only the vulva. This disorder may begin with something that simply rubs, irritates, or scratches the skin, such as clothing. Or, intense pruritis may develop secondary to atopic dermatitis, psoriasis, neuropathic pain, or psychologic disorders. The constant scratching causes an inflammatory reaction with subsequent skin thickening. The appearance depends on whether the patient rubs the area (lichenfication) or scratches the area (excoriations). They may also report dysuria, dyspareunia, and vulvar pain, and feel that the skin of their vulva is tender, bumpy, irritated, or thickened. Physical Examination these disorders range in appearance from erythematous plaques to hyperkeratotic white plaques to erosions and ulcers (Table 13-1). Occasionally, petechiae and/or ecchymoses are present as a result of trauma from scratching. Colpoposcopy and directed biopsy can also be used to evaluate and identify vulvar and vaginal lesions. Vulvovaginal irritation and pruritis may be seen in yeast, folliculitis, trichomoniasis, contact dermatitis, and drug reactions. The differential diagnosis also includes premalignant and malignant disease such as vulvar and vaginal intraepithelial neoplasia, squamous cell carcinoma, and Paget disease of the vulva. Patients should avoid tight-fitting clothes; pantyhose; panty liners; scented soaps and detergents; bubble baths; washcloths; and feminine sprays, douches, and powders. They should use mild, unscented detergents and soaps such as Dove or Cetaphil, and take morning and evening tub baths without additives. In general, there is no role for topical estrogens or testosterone in the treatment of these disorders; however, low-dose vaginal estrogen is an effective treatment for concomitant genital urinary syndrome of menopause. Similarly, surgical management is generally not indicated in treatment of these disorders. Cysts can originate from occlusion of pilosebaceous ducts, sebaceous ducts, and apocrine sweat glands. Treatment of benign cystic and solid tumors is needed only if the lesions become symptomatic or infected. These cysts usually result from occlusion of a pilosebaceous duct or a blocked hair follicle. They are lined with squamous epithelium and contain tissue that would normally be exfoliated. These solitary lesions are normally small and asymptomatic; however, if these become superinfected and developed into abscesses, incision and drainage or complete excision is the treatment. As with any cyst, these can become superinfected with local flora and require treatment with incision and drainage. Fox-Fordyce disease is an infrequently occurring chronic pruritic papular eruption that localizes to areas, where apocrine glands are found. Hidradenitis suppurativa is a skin disease that most commonly affects areas bearing apocrine sweat glands or sebaceous glands, such as the underarms, breasts, inner thighs, groin, and buttocks. Initial treatment for hidradenitis includes antimicrobial skin washes and antibiotic ointments. As in the axillary region, if these cysts become infected and form multiple abscesses, excision or incision and drainage are the treatments of choice. When conservative measures fail, persistent or recurrent paraurethral cysts can be treated with simple marsupialization or excision. They are mucus-secreting glands with ducts that open just external to the hymenal ring. If the cyst remains small (1 to 2 cm) and is asymptomatic, it can be left untreated and will often resolve on its own or with sitz baths. These abscesses are the result of polymicrobial infections, but they are also occasionally associated with sexually transmitted infections. These abscesses can become quite large, causing exquisite pain and tenderness and associated cellulitis.
Cheap aygestin 5 mg online
This might be the case menstrual gas pains buy cheap aygestin on line, for instance, during extended periods of fasting when the liver starts to produce ketone bodies, or after a bout of intense exercise when skeletal muscle releases lactate into the circulation. In case the period of fasting is not overly long, or the physical exercise is less exhaustive, the changes in circulating substrate levels are subtle and predominantly driven by a drop in the insulin/glucagon ratio. Under these catabolic conditions adipose tissue becomes the main source of circulating fatty acids and cardiac metabolism shifts toward the oxidation of even more fatty acids, while glucose oxidation becomes less. Next to these relatively acute changes in circulating substrate levels, sometimes the heart is also faced with more chronic changes in its nutritional environment for instance under hyperlipidemic or diabetic conditions. Under these conditions there appears to be ample time for the heart to adapt to these longstanding alterations in nutritional environment. However, it seems that this happens at the expense of its omnivorous capacity, that is, the heart loses some of its flexibility to readily switch to other substrates [2]. In addition to changes at the supply side (nutritional environment), from the demand side the need for substrates of the cardiac tissue is largely dependent on the workload of the heart. Chronic increases in cardiac workload also occur in case of, for instance, hypertension, when the heart is forced to generate a higher pressure to maintain cardiac output. Moreover, longstanding hypertension also evokes remodeling of the heart (hypertrophy, dilation). As with chronic changes in the nutritional milieu, cardiac remodeling due to chronic changes in cardiac workload has been shown to lead to adaptations in the substrate preference of the heart and limit the capacity of the heart to use alternative substrates. In the present chapter the focus will first be on the effect of relatively short-term variations in nutritional environment on cardiac substrate handling and on cardiac function and phenotype. Thereafter the more long-term effects of metabolic derangements, associated with obesity and diabetes, and the effects of dietary interventions on the heart are being discussed. Various hormones controlling plasma nutrient levels show a circadian rhythm, the most wellknown being cortisol, the plasma levels of which peak in the late night/early morning hours, thereby priming us for our daytime activities. Importantly, recent studies indicate that in addition to the master clock in the brain, almost all tissues, including liver, adipose tissue, skeletal muscle and heart, possess an autonomous circadian rhythm. By transcriptomic analysis it was demonstrated that the expression of about 13% of the genes in the murine heart, including many metabolic genes, is subject to a circadian rhythm [3]. Under in vivo conditions, however, it is impossible to discern if these changes are secondary to changes in neurohumoral factors that are under control of the central clock, or if they are intrinsic to the heart itself. By using isolated adult cardiomyocytes, deprived of potential changes in levels of neurohumoral factors, it was demonstrated that gene expression still follows a circadian rhythm, thereby providing unequivocal evidence for the existence of a functional, intrinsic circadian clock within cardiomyocytes [4]. It is commonly acknowledged that the evolutionary advantage of the existence of central and peripheral clocks is that it allows the organism and its tissues, to anticipate the upcoming changes. For the heart this mainly refers to anticipation of the daily increase in physical activity during the active time of the day (light phase for man, dark phase for rodents) and the associated feeding/fasting cycles. Studies in rats indicate that increases in cardiac energy demand during the active phase are largely met by increases in carbohydrate oxidation, with only modest effects on fatty acid oxidation [5]. Paradoxically, at the end of the sleep-phase plasma fatty acid levels peak [6,7], while cardiac fatty acid oxidation capacity remains relatively constant during the active phase [5]. The heart seems to cope with this situation by increasing triglyceride synthesis [8]. This rise in nocturnal fatty acids has been directly linked to the development of insulin resistance. It would be interesting to test if the rise in plasma fatty acid levels during the sleep phase also leads to an enhanced accumulation of triglycerides in the myocardium, possibly predisposing to lipotoxicity. It is important to realize when studying the role of circadian rhythms on cardiac metabolism and function that the feeding pattern (ad libitum or time-restricted) of laboratory animals is clearly important. Notwithstanding these limitations it has been convincingly shown that in various cardiac disease conditions the rhythmic expression of genes across the day, also those involved in cardiac metabolism, becomes dampened [5], thereby limiting the ability of the heart to anticipate changes in nutritional environment. At the same time, several elegant studies in which genes that are components of the circadian clock have been knocked out at the whole body level or in a tissue specific manner, demonstrated the importance of a functional clock in controlling overall energy homeostasis and, consequently, the risk of becoming obese or diabetic (reviewed in [9]). Recently, it was shown that cardiac-specific disruption of the circadian clock by knockout of Bmal1, leads to changes in cardiac metabolism that were manifested during fasting in particular [10,11]. In addition, disruption of the cardiac circadian clock was associated with the development of dilated cardiomyopathy, thereby revealing the importance of the intrinsic clock in maintaining proper function of the heart. It has even been argued that entrainment of peripheral clocks is the result of feeding and fasting primarily. Generally speaking, the early postprandial phase is characterized by high glucose (and insulin) levels, while during the fasting-phase plasma fatty acid (and glucagon) levels rise. Cardiac metabolism largely follows these changes being somewhat more dependent on glucose oxidation in the fed state, and more dependent on fatty acid oxidation in the fasted state. It should be noted that more prolonged fasting also leads to a rise in the levels of circulating ketone bodies, produced by the liver, which act as a preferred substrate for the heart [12]. The role of ketogenesis is often ignored, but may be significant in mice, possibly owing to their high metabolic rate. Accordingly, this response allows the heart to match its substrate preference to the prevailing nutritional environment as imposed by fasting. The combined effect is a further increase in cardiac fatty acid oxidation at the expense of glucose oxidation. It is well established that changes in nutritional environment directly influence cardiac function and affect the susceptibility of the heart for challenges like (transient) ischemia. With respect to the circadian rhythm it was already observed that hearts, extirpated from rats during the sleep phase and perfused ex vivo, generated less force than hearts isolated during the active phase. Notably, this intervention did not affect cardiac systolic function, but diastolic function was significantly reduced in these persons. In other studies the effect of prior fasting on ischemia tolerance of the heart has been investigated. However, the outcome is inconclusive, with some reporting reduced ischemia tolerance [21] and others reporting enhanced ischemia tolerance in response to prior fasting [22,23]. It is tempting to speculate, that the observation, that the frequency of ischemic attacks in man is higher in the early morning hours is somehow related to the nutritional environment prevailing at the end of the sleep phase. As far as the heart is concerned many of the health benefits are secondary to improved skeletal muscle performance, decreased adiposity, and increased insulin sensitivity. At the same time the physical exercise also asks for adaptation of the heart itself, due to changes in circulating hormone levels, nutrient levels, and cardiac workload. As far as hormones are concerned it is important to realize that next to changes in wellknown humoral factors, like the rise in adrenaline, more recent findings indicate that exercising skeletal muscle also releases factors acting as hormones, so-called myokines, that may influence cardiac metabolism and function in the short term and cardiac remodeling in the long term. Exercise dramatically increases the workload and, hence, the energy demand of the heart, which must be met by increasing mitochondrial oxidative metabolism. As exercise is associated with rapid mobilization of fatty acids from adipose tissue, resulting in an up to fourfold rise in circulating fatty acid levels with moderate exercise [26], it is likely that the heart in situ will respond to this by increasing fatty acid oxidation as well. The more acute changes in cardiac substrate metabolism during exercise involve multiple steps, some of which are related to the change in nutritional environment (higher circulating fatty acid levels), while others are driven by the increase in cardiac high-energy phosphate demand. From a molecular/biochemical perspective the effects are largely mediated by the phosphorylation of enzymes and the allosteric modulation of enzyme activity. Intriguingly, studies with ex vivo perfused hearts of normal, untrained rats have shown that a sudden increase in workload as induced by administration of adrenaline is largely met by first increasing the oxidation from glucose derived from intracellular glycogen stores, followed by a more gradual increase in the oxidation of exogenous glucose. The oxidation of fatty acids remains fairly constant under these ex vivo conditions, whereby nutrient levels remain constant [27]. It is still unclear if these ex vivo observations can be translated to the in vivo situation. Repeated exercise results in remodeling of the heart (physiologic hypertrophy), which also extends to cardiac metabolism. An enhanced glucose uptake and metabolism results in increased mitochondrial acetyl-CoA and citrate levels. As a consequence, malonyl-CoA levels will drop, allowing increased entry of fatty acids into the mitochondria for subsequent b-oxidation. The factors mentioned earlier closely interact to increase oxidative capacity, on the one hand, and nutrient and oxygen supply, on the other (for recent reviews see [32,33]).
Order 5 mg aygestin with amex
For example womens health zone natural remedies health buy aygestin visa, proteins are made by the linkage of amino acids through peptide bonds, which depend on the reactivity between amino and carboxyl groups. Further chemical and physical interactions, such as electrostatic attraction or repulsion, and hydrophobicity of amino acid side groups, bend and twist the protein into its final three-dimensional shape. Some of these same forces may in certain cases create a larger protein from several subunits. Without the correct chemical and physical properties, proteins would not assume a proper shape; this is extremely important in physiology because the shape of a protein is critically linked with its function. The resulting change in three-dimensional structure of the protein may enhance or reduce the ability of the protein to bind its ligand. Sucrose (b); Glucose (a); Glycogen (c); Fructose (a); Starch (c) the other reactions in which larger molecules are formed occur via dehydration reactions. Thus, the structure of this membrane increases the ability of mitochondria to carry out their major function. The general principle that structure is a determinant of-and has coevolved with-function is also evident at the molecular (protein) level. Proteins and ligands interact due to a variety of forces and molecular features, including complementary shapes. In addition, however, chemical or physical properties of molecules often strongly influence their ability to interact or bind with each other. The fundamental property of physics that opposite charges attract one another means that a ligand with the correct electrical charges will be more likely to bind to this protein than another ligand without those charges. If the gene were only composed of the triplet exon code words, the gene would be 300 nucleotides in length because a triplet of three nucleotides codes for one amino acid. However, because of the presence of intron segments in most genes, which account for 75% to 90% of the nucleotides in a gene, the gene would be between 1200 and 3000 nucleotides long; moreover, it would also contain termination codons. Thus, the exact size of a gene cannot be determined by knowing the number of amino acids in the protein for which the gene codes. The reason for a lack of insulin effect could be either a decrease in the number of available binding sites insulin can bind to or a decrease in the affinity of the binding sites for insulin so that less insulin is bound. A third possibility, which does not involve insulin binding, would be a defect in the way the binding site triggers a cell response once it has bound insulin. The maximum rate at which the end product E can be formed is 5 molecules per second, the rate of the slowest (rate-limiting) reaction in the pathway. Glucose, which is the major source of energy for the brain, must now be synthesized from other types of molecules. Most of this newly formed glucose comes from the breakdown of proteins to amino acids and their conversion to glucose. The metabolites of the fatty acid portion of triglyceride cannot be converted to glucose. Ammonia is formed in most cells during the oxidative deamination of amino acids and then travels to the liver via the blood. Segregation of function on different surfaces of the cell, and the ability to secrete chemicals. Because ions are charged, both the chemical and the electrical gradients determine their rate and direction of diffusion. The two one-way fluxes will be much larger in B than in A, but the net flux has the same magnitude in both cases, although it is oriented in opposite directions. The net transport will be out of the cell in the direction from the higher-affinity site on the intracellular surface to the loweraffinity site on the extracellular surface. More molecules will be bound to the transporter on the higher-affinity side of the membrane, and therefore more will move out of the cell than into it, until the concentration in the extracellular fluid becomes great enough that the number of molecules bound to transporters at the extracellular surface is equal to the number bound at the intracellular surface. The solution with the greatest osmolarity will have the lowest water concentration. Solution B is isoosmotic because it has the same osmolarity as intracellular fluid. Initially, the osmolarity of compartment 1 is (2 3 200) 1 100 5 500 mOsm and that of 2 is (2 3 100) 1 300 5 500 mOsm. The two solutions therefore have the same osmolarity, and there is no difference in water concentration across the membrane. Because the membrane is permeable to urea, this substance will undergo net diffusion until it reaches the same concentration (200 mM) on the two sides of the membrane. In other words, in the steady state, it will not affect the volumes of the compartments. In contrast, the higher initial NaCl concentration in compartment 1 than in compartment 2 will cause, by osmosis, the movement of water from compartment 2 to compartment 1 until the concentration of NaCl in both is 150 mM. Note that the same volume change would have occurred if there were no urea present in either compartment. It is only the concentration of nonpenetrating solutes (NaCl in this case) that determines the volume change, regardless of the concentration of any penetrating solutes that are present. Solution C will cause cells to shrink because it has a higher concentration of nonpenetrating solute than the intracellular fluid. Solution A is isotonic because it has the same concentration of nonpenetrating solutes as intracellular fluid (300 mOsm). Solution A is also hyperosmotic because its total osmolarity is greater than 300 mOsm, as is also true for solutions B and C. Solution B is hypotonic because its concentration of nonpenetrating solutes is less than 300 mOsm. Solution C is hypertonic because its concentration of nonpenetrating solutes is greater than 300 mOsm. Solution D is hypotonic (less than 300 mOsm of nonpenetrating solutes) and also hypoosmotic (having a total osmolarity of less than 300 mOsm). If the intracellular concentration of sodium ions were increased, the sodium ion concentration gradient across the membrane would be decreased, and this would decrease the secondary active transport of Ca 21 out of the cell. This would lead to an increase in cytosolic Ca 21 concentration, which would trigger increased exocytosis. Also, the regulated changes in aquaporin numbers in the epithelial cells of the kidneys help maintain water homeostasis by controlling the rate at which water is lost in the urine; this is particularly important in situations such as dehydration. The general principle that controlled exchange of materials occurs between compartments and across cellular membranes is apparent from the many diverse types of mechanisms by which solutes may cross plasma membranes. The control arises from such mechanisms as gates in ion channels that may open or close depending on cell requirements, and the just-mentioned glucose transporters and aquaporins, the concentrations of which can increase or decrease in plasma membranes under different conditions. The general principle that physiological processes are dictated by the laws of chemistry and physics is evident from the relationship between the chemical nature. Electrochemical gradients aid in the diffusion of charged molecules (ions) through membrane channels because of the basic physical principle that like charges repel and opposite charges attract each other. Finally, molecular movement (and therefore potential interactions between molecules) is directly related to heat energy; solutes move through solution at faster rates at higher temperatures. The intracellular concentration of nonpenetrating solute is typically about 300 mOsm, so solution A will produce no change in cell volume. Lipid-soluble messengers cross the plasma membrane and act primarily on cytosolic and nuclear receptors. Not in most cells, because there are other physiological mechanisms by which signals impinging on the cell can increase cytosolic Ca21 concentration. These include (a) second-messengerinduced release of Ca21 from the endoplasmic reticulum and (b) voltage-sensitive Ca21 channels. When the voltage-gated K1 channels eventually close, the K1 leak channels once again determine the resting membrane potential. It would repolarize more slowly because repolarization depends on net K1 diffusion from the cell, and the concentration gradient driving this diffusion is lower. Therefore, the drug would remove the slowing effect of these nerves on the heart, allowing the heart to speed up. We know that the drug is not blocking cholinergic nicotinic receptors because the skeletal muscles are not affected. Therefore, we can also predict that this passive inward movement was being exactly balanced by active transport of Cl2 out of the cells. Without acetylcholinesterase, more acetylcholine would remain bound to the receptors, and all the actions normally caused by acetylcholine would be accentuated. Consequently, there would be significant narrowing of the pupils, airway constriction, stomach cramping and diarrhea, sweating, salivation, slowing of the heart, and decrease in blood pressure. On the other hand, in skeletal muscles, which must repolarize after excitation in order to be excited again, there would be weakness, fatigue, and finally inability to contract.
Syndromes
- Low blood pressure
- Pyloric stenosis (narrowing)
- Malnutrition
- Hypokalemic periodic paralysis
- Graft failure, which means that the new cells do not settle into the body and start producing stem cells
- Be withdrawn, easily upset, or confused
- Zinc
- Headache and pain if you also have a sinus infection
- Brain tumor
- Amount swallowed
Purchase aygestin 5 mg free shipping
The rule of biomedical waste is prescribed by the Ministry of Environment and Forest women's health clinic darnall hospital aygestin 5mg low price, Government of India and applied on 28th July 1998 to those who generate, collect, receive, stor, dispose, treat or handle the source in however. Soiled wastes such as dressings, bandages, plaster casts, material contaminated with blood, tubes, and catheters. Incineration Chemical disinfection Autoclaving Microwave irradiation Controlled tripping/sanitary landfill/deep burial. If color is changed, it indicates these bags are properly disinfected and then can be discarded into yellow bags to be sent for incineration. After that mix it properly and wait for 114 Step by Step Technical Manual of Blood Components Preparation 30 minutes. With the help of this equipment sterilization is done for killing the fungi, bacteria, and viruses. There are several methods of sterilization such as steam heating, dry heating, ethylene oxide gas method, cold sterilization by cidex, automatic decontamination system (cidematic) and radiation technique. Steam storing period: In the outside chamber which is made of 304 graded stainless steel allows the super heated steam to enter from boiler. Sterilization period: the super heated steam enters in the inner chamber where the material is stored. A special type of indicator which is rapped on the material before sterilization, changes the color. Exhaust period: After 20 minutes of operation the steam present in the inner chamber is allowed to exhaust outside from the chamber and the pressure falls to zero. Drying period: After the exhaust period, the inner chamber is kept into vacuum line for the residual steam to come out and then the sterilized item Sterilization 117 becomes dry. Autoclaves have two chambers for boiler to produce steam and another one for sterilization. Between the two chambers, the glass wool is laminated to prevent temperature of outside to move in. The freon gas is highly compressed and allows expanding in the cooling chamber (by Joule-Thompson effect). The temperature of the inner chamber is made uniform with the help of a blower fan. Temperature controller measured and compared the temperature of the chamber with set point. If the temperature is low than the set point, the controller start the compressor to make temperature high. The temperature sensor which is set in inner chamber will provide signal to the controller to control display and record the temperature. Starter will start or off the control as per received signal from the temperature controller. Compressor delivered the compressed gas to the cooling chamber and also collect the noncompressed gas from cooling chamber. Cooling chamber, here the compressed gas goes to an adiabatic expansion and temperature fall. Temperature controller receives the signal from sensor and advice starter to start or off the compressor. Always keep packed cells blood in Remedy-Display board circuit is horizontal position to be checked. Guide to the preparation, use and quality assurance of blood components, 7th edition. Cardiac metabolism therefore comprises all processes involved in the biochemical conversion of molecules within the cell utilizing energy substrates. In addition, cardiac metabolism comprises all biochemical processes of the cell aimed at the generation of building blocks for cell maintenance, biosynthesis, and cellular growth. As simple as this illustration, which stems originally from Heinrich Taegtmeyer, appears as complex is its meaning [4]. However, the scheme finally encompasses myocardial metabolism as potential target for treating contractile dysfunction [5]. Considering that metabolic processes also influence biosynthesis, it becomes clear that metabolism is a prime target of investigations for nearly all physiologic and pathologic states of the heart, may it be ischemia/reperfusion, diabetes, hypertrophy, and acute and chronic heart failure [6]. In order to develop an understanding for these interrelations and to obtain basic knowledge about the methods and tools used for the investigation of (cardiac) metabolism, we have compiled this book. It reflects a selection of chapters geared toward the transfer of principles in cardiometabolic research. The book does not claim to be complete, but its content should make the reader quickly understand most of the specific topics he or she intends to specialize in and to be better able to put the personal investigations into perspective. In Chapter 2, Jan Glatz and Miranda Nabben begin with illustrating basics in metabolically relevant biochemistry. They show that metabolism is tightly coupled to all major types of biomolecules as virtually every biomolecule can be used as a substrate or pathway component in metabolism. Furthermore, the properties of biomolecules influence their transport as well as their import into the cell or into cellular substructures, such as mitochondria. Fatty acids as lipophilic compounds are not readily soluble in the aqueous blood and cytoplasm. Carbohydrates, nucleic acids, and amino acids are more hydrophilic and may not cross membranes without help. Thus, it is important to be aware of the properties of biomolecules and their biochemistry. This chapter introduces the reader to the biochemical properties of the major classes of molecules and illustrates their behavior. In Chapter 3, Bernd Niemann and Susanne Rohrbach address metabolically relevant cell biology and illustrate the roles of intracellular organelles for cardiac metabolism. In this chapter, the roles of all major cellular organelles with respect to cardiac metabolism are described. The reader may find that both fatty acid oxidation and phospholipid ether biosynthesis may be peroxisomal processes and that the endoplasmatic/ sarcoplasmatic reticulum has a major role in calcium homeostasis which influences cardiac contractility as well as metabolic enzyme activities. While the role of ribosomes seems to be better known, the importance of transport systems and vesicle pools may have been less recognized and their role in glucose and fatty acid uptake, fission and fusion of mitochondria is highlighted. Finally, the authors elegantly explain the different modes of cell death known as apoptosis, autophagy, necrosis, and necroptosis. In Chapter 4, together with Christina Werner, we address principle metabolic pathways and metabolic cycles as they relate to energy production and building-block generation in the heart. This chapter covers the important biochemical parts of substrate use in cardiac metabolism. The contents of this chapter represent another fundamental component of cardiac metabolism, as it demonstrates how glucose and fatty acids as the main substrates are metabolized. Here, the connection between different pathways is illustrated and the importance of the citric acid cycle for the generation of reducing equivalents as well as for building blocks for biosynthetic processes becomes readily visible. Furthermore, anaplerosis as mechanism to "refill" exploited moieties within metabolic cycles is introduced and the interrelation of hexosamine biosynthetic pathway, pentose phosphate pathway, and glycolysis is presented as well as the influence of fatty acid oxidation on glucose use and vice versa. Understanding of the principles explained in this chapter is essential to follow the metabolic path of substrates in an organism. Louis Hue, Luc Bertrand, and Christophe Beauloye then address the principles of how the 1. Cardiac metabolism must never stop and needs to be adjusted to substrate availability, hormonal regulation, and workload. The authors elegantly describe how metabolic pathways are organized and controlled.
Order aygestin 5 mg fast delivery
IgM antibodies are primarily involved in immune defense mechanisms found in the surface or lining of the gastrointestinal menstrual acne cheap aygestin 5 mg online, respiratory, and genitourinary tracts. All antibodies of a given class have an Fc portion that is identical in amino acid sequence. Edema (swelling), which occurs during inflammation, has important adaptive value in helping defend against infection or injury. Toll-like receptors are the major defense against specific pathogens and therefore have an important function in adaptive immunity. If an individual failed to develop a thymus because of a genetic defect, what would happen to the immune responses mediated by antibodies and those mediated by cytotoxic T cells Which antigen binds to which immunoglobulin is determined entirely by the structure of the ligand and the structures of the variable ends of each immunoglobulin molecule. The structure of the constant ends of immunoglobulins is also important in their function, because it is this structure that is recognized by phagocytes when the immunoglobulin is a circulating antibody attached to a pathogen. By establishing a population of memory cells, each subsequent infection can be defended against more efficiently and quickly. The first exposure to antigen elicited a response from about 2 units to 10 units (fivefold), whereas the second exposure elicited a response from about 2 units up to nearly 10,000 (5000-fold). Testosterone acts locally within the testes (paracrine) and reaches other targets through the blood (endocrine). As that fluid flows through the lymph nodes, lymphocytes are exposed to antigens from the invading pathogen, thus activating the adaptive immune response. Via another developmental pathway, myeloid cells also differentiate into mast cells and dendritic cells. This personalized adaptive learning tool serves as a guide to your reading by helping you discover which aspects of immune defenses you have mastered, and which will require more attention. A fascinating view inside real human bodies that also incorporates animations to help you understand the immune system. P hysiology is one of the pillars of the health-related professions, including nursing, occupational health, physical therapy, dentistry, and medicine. In fact, the term pathophysiology- the changes in function associated with disease-highlights the intertwining of physiology and medicine. You need a thorough understanding of the general principles of physiology to properly diagnose and treat diseases and disorders. We are aware that many users of this textbook may not be planning a career in the health professions. However, teachers of physiology can attest to the use of clinical examples as an effective approach to highlight and reinforce the understanding of the functions and interactions of the organ systems of the body. This chapter uses clinical cases to allow you to continue to explore the material you learned from this book and, at the same time, review some of the general principles of physiology that were first introduced in Chapter 1. You have been introduced to the educational power of clinical cases at the end of each chapter of this book. The true art of medicine is the ability of clinicians to recall these basic principles and put them together in the evaluation of the patient. As you read these sections, you should consider the relationships among disease, integrative physiology, and homeostasis, the last of which has been a theme throughout this textbook. Some of the conditions and physiological interactions described in this chapter are not explicitly described in the book and may be new to you. Interspersed at key points in the chapter are several places where you will be asked to "Reflect and Review. We encourage you to answer these questions as the case unfolds by, if necessary, referring back to the appropriate section of the book. Furthermore, we have annotated each case with figure and table numbers to facilitate review of material covered in previous chapters. In some cases, the figures and tables from previous chapters do not specifically answer the question but provide an opportunity to review the control system in question to allow the student to propose potential answers. We hope that the cases in this chapter will motivate you to synthesize and integrate information from throughout the book and perhaps even go beyond what you have learned. In fact, you may enjoy consulting other sources to answer some of the more challenging questions or learn more about specific aspects of each case that interests you. Finally, when she is asked to gaze to the far right, her right eye does not move as far as does her left eye and she says she has double vision (diplopia). She has lost 30 pounds of body weight over this period despite having a voracious appetite and increased food intake. She states that she has double vision when looking to the side but does not have any loss of vision when using only one eye or the other. What might be causing her hypertension, tachycardia (increased heart rate), and tachypnea (increased respiratory rate) Which hypothalamic, anterior pituitary gland, and ovarian hormones control the menstrual cycle Her systolic/diastolic blood pressure is 140/60 mmHg (normal for a young, healthy woman is about 110/70 mmHg). Before she became ill, her resting Her patellar tendon (knee-jerk) reflexes are hyperactive. Reflect and Review #5 What are the neural pathways involved in the knee-jerk reflex When increased thyroid hormone causes significant symptoms, it is part of a condition called hyperthyroidism or thyrotoxicosis. There are two circulating thyroid hormones-thyroxine (T4) and triiodothyronine (T3). Whereas T4 is the main secretory product of the thyroid gland, T3 is actually more potent and is actively produced in target tissues by the removal of one iodine molecule from T4. Nonetheless, for practical reasons, T4 is the form of thyroid hormone that is routinely measured in clinical situations. The 684 Chapter 19 *In actuality, these measurements are performed in serum or plasma derived from blood. There are several reasons why the thyroid gland in this patient could be producing too much thyroid hormone, leading to thyrotoxicosis. Measurement of free T4 is helpful because most of the circulating thyroid hormone in the blood is bound to plasma proteins, so measuring the serum T4 that is not bound to plasma proteins proves that there is an increase in the amount of biologically active T4. Notice that the eye symptoms are caused by autoimmune response rather than by the increase in thyroid hormones. Serum calcium and parathyroid hormone were measured because weakness is a common finding in primary hyperparathyroidism (Chapter 11, Section F). A normal prolactin concentration indicated that she does not have hyperprolactinemia, which can cause abnormalities in the menstrual cycle and visual disturbances (see Chapter 17 Clinical Case Study). Up to 10% of women will develop hyperthyroidism or hypothyroidism by the age of 60 to 65. Thyroid hormone has a wide range of effects throughout the body; therefore, an understanding of all the organ systems is extremely useful in understanding the symptoms of thyroid disease. The resultant increase in heat production by our patient explains the warmness and moistness of her skin and her heat intolerance. It also explains why, despite eating more, she is losing weight because she is burning more fuel than she is ingesting. The nervousness, irritability, and emotional swings are likely due to effects of thyroid hormone on the central nervous system, although the exact cellular mechanism of this is not well understood. The symptoms also appear to be due to an increased sensitivity within the central nervous system to circulating catecholamines. Despite this, there appears to be an increase in the speed of muscle contraction and relaxation, contributing to the hyperactive reflexes observed in our patient. The normal fasting blood glucose rules out diabetes mellitus as a cause of her muscle weakness. The enlarged thyroid with increased metabolic activity explains why a bruit was heard over the thyroid gland.
Aygestin 5mg with mastercard
Heat is also lost via the expired air (insensible loss) menopause 34 symptoms order aygestin paypal, and some people actually begin to pant under such conditions. The rapid, shallow breathing increases airflow and heat loss without causing hyperventilation. They achieve these effects in part through opposite actions on key metabolic organs such as the liver. In the liver, insulin stimulates glycogen synthesis and inhibits gluconeogenesis, whereas glucagon stimulates glycogen breakdown and gluconeogenesis. Insulin and glucagon are always present in plasma; it is the ratio of the two hormones that determines the net effect that will be to either decrease (insulin) or increase (glucagon) the concentration of plasma glucose. Neural and endocrine signals arising from the gastrointestinal tract and adipocytes appear to be very important regulators of appetite. Other factors, such as plasma glucose and insulin concentrations, body temperature, and behavioral mechanisms also play a role. As described in the chapter, the first law of thermodynamics states that energy can neither be created nor destroyed but can be transformed from one type to another. This is demonstrated by the production of heat within cells during the breakdown of organic molecules such as glucose. Maintaining body temperature in a homeostatic range also depends upon the properties of heat; for example, heat flows from a region of higher temperature to one of lower temperature. Core temperature is generally kept fairly constant, but skin temperature can vary. Lipoprotein lipase cleaves plasma triglycerides, so its blockade would decrease the rate at which these molecules were cleared from plasma and would decrease the availability of the fatty acids in them for the synthesis of intracellular triglycerides. However, this would only reduce but not eliminate such synthesis, because the adiposetissue cells could still synthesize their own fatty acids from glucose. Bile salts are formed from cholesterol, and losses of these bile salts in the feces will be replaced by the synthesis of new ones from cholesterol. The luteal phase of the ovary, when progesterone production is maximal, occurs after ovulation but before the end of the menstrual cycle. This stimulates the maturation of a small number of follicles for the next menstrual cycle. It is homologous to but not the same peptide as human placental lactogen, which is produced by the placenta. The decrease in estrogen leads to an increase in pituitary gland gonadotropin release (loss of negative feedback). The other two are due to increased plasma progesterone and so do not occur until after ovulation and formation of the corpus luteum. When test-tube fertilization is performed, special techniques are used to induce capacitation. The placenta produces progesterone entirely on its own, whereas estriol secretion requires participation of the fetus, specifically, the fetal adrenal cortex. Prostaglandin antagonists, oxytocin antagonists, and drugs that lower cytosolic Ca21 concentration. You might not have thought of the last category because Ca21 is not mentioned in this context in the chapter, but as in all muscle, Ca21 is the immediate cause of contraction in the myometrium. This person would have normal male external genitals and testes, although the testes might not have descended fully, but would also have some degree of development of uterine tubes, a uterus, and a vagina. These two hormones are already increased in menopause, and the problem is that the ovaries are unable to respond to them with estrogen secretion. The male and female genitalia arise from the same primordial cluster of cells in the embryo. The reproductive structures diverge in early embryonic development to form organs suited for their function. For the male, it is the production of sperm and the development of a penis that evolved to fit into the vagina of the female. In the female, it is to produce ova and to receive sperm to allow fertilization of the ova. So even though they started the same, through differentiation, the male and female tracts develop into complementary structures suited for their functions. The adaptation to pregnancy is one of the best examples of integration of multiple organ systems. This allows the increase in cardiac output and perfusion of the rapidly growing placenta as well as increase in blood flow to , for example, the maternal kidneys to enable the excretion of the additional waste products produced by the fetus. As a test of your knowledge, you should be able to explain the mechanism of these and other adaptations to pregnancy listed in Table 17. The Sertoli cells are essential for spermatogenesis, and so is testosterone produced by the Leydig cells. The person with Leydig cell destruction, but not the person with Sertoli cell destruction, would also have other symptoms of testosterone deficiency. The androgens act on the hypothalamus and anterior pituitary gland to inhibit the secretion of the gonadotropins. You would also expect to find that the testes and penis were small if the deficiency occurred before puberty. The result is inadequate secretion of gonadotropins and therefore inadequate stimulation of the ovaries. In addition to the loss of regular menstrual cycles, the woman may suffer some degree of masculinization of the secondary sex characteristics because of the combined effects of androgen excess and estrogen deficiency. They are sometimes given in viral diseases to eliminate or prevent secondary infections caused by bacteria, however. The drug may reduce but would not eliminate the action of complement, because this system destroys cells directly (via the membrane attack complex) as well as by facilitating phagocytosis. In each case, the respective variable is decreased or increased beyond its usual homeostatic range. Although these changes are adaptive to fight infection, they may come with a cost, as does any challenge to homeostasis. For example, elevated concentrations of cortisol may temporarily result in hyperglycemia, water retention, and potentiated actions of catecholamines on cardiovascular function. Other responses to infection, such as fever, accelerate the rate of chemical reactions in all cells (increase metabolism) and, if fever is sufficiently high, may damage neuronal function. The absence of cytotoxic T cells would eliminate responses mediated by these cells. The absence of helper T cells would impair antibody-mediated responses because most B cells require cytokines from helper T cells to become activated. Neutrophil deficiency would impair nonspecific (innate) inflammatory responses to bacteria. Small variations in reference ranges occur due to several factors, including method of measurement. C-1 Glossary Index Page numbers followed by t or f indicate tables and figures respectively. Myriad physiologic changes occur in a pregnant woman, affecting every organ system. An infant delivered prior to 23 to 24 weeks is considered to be previable, delivered between 24 and 37 weeks is considered preterm, and between 37 and 42 weeks is considered term. For example, a woman who has given birth to one set of twins would be a G1 P1, because a multiple gestation is considered to be just one pregnancy. A more specific designation of pregnancy outcomes divides parity into term and preterm deliveries and also adds the number of abortuses and the number of living children. Abortuses include all pregnancy losses prior to 20 weeks, both therapeutic and spontaneous, as well as ectopic pregnancies. For example, a woman who has given birth to one set of preterm twins, one term infant, and had two miscarriages would be a G4 P1-1-2-3. The prefixes nulli-, primi-, and multi- are used with respect to gravidity and parity to refer to having 0, 1, or more than 1, respectively. For example, a woman who has been pregnant twice, one ectopic pregnancy and one fullterm birth, would be multigravid and primiparous. Unfortunately, this terminology often gets misused, with individuals referring to women with a first pregnancy as primiparous, rather than nulliparous.
Buy generic aygestin 5 mg on line
Translation and Posttranslational Modifications Although alterations in gene expression have the potential of providing mechanistic insight menstrual flooding buy generic aygestin canada, it is important to recall that the activity of the encoded protein holds a greater potential to directly impact metabolic fluxes. The activity of a protein is influenced not only by its level of expression (which is dependent on rates of protein synthesis and degradation), but also through modulation of substrate availability, allosteric effector levels, and covalent modifications (both irreversible. Comparable to transcription-based studies, diurnal variations in protein expression have been investigated through the use of both hypothesis generating and testing approaches. For example, proteomic studies have recently revealed that approximately 8% of cardiac proteins exhibit a time-of-day-dependent oscillation in the murine heart [37]. Interestingly, proteomic analysis of the murine heart revealed that a large proportion of proteins exhibiting diurnal variations are directly involved in metabolism. Identified proteins included a surprisingly large number of nuclear-encoded mitochondrial enzymes, which play important roles in oxidative metabolism. These include enzymes involved in alcohol metabolism, fatty acid b-oxidation, and oxidative phosphorylation [37]. Previous studies suggest that the turnover of mitochondria in the heart is relatively long, with an estimated half-life of 30 days [39]. The recent proteomic studies identifying a subset of mitochondrial proteins exhibiting a diurnal variation suggest that even though cardiac mitochondria have a half-life well in excess of 24 h, mitochondrial function and oxidative metabolism potentially exhibit time-of-day-dependent oscillations. To date, no studies have directly investigated day-night differences in cardiac mitochondrial function. Phosphorylation status of components of signaling axes known to directly influence myocardial metabolism have also been investigated. Indeed, whole body insulin sensitivity peaks in both rodents and humans at the beginning of the active period [8,9]. In the latter case, it is important to note that protein degradation is essential for protein turnover, particularly in the 24 h timeframe. As highlighted earlier, evidence exists in support of the concept that the intrinsic metabolic properties of the heart fluctuate in a time-of-day-dependent manner. This includes persistence of day-night differences in: (1) metabolic fluxes of ex vivo perfused hearts; (2) responsiveness of the heart to stimuli/ stresses. Observations such as these have led to questions focused on identification of the mechanism(s) responsible for diurnal rhythms in these metabolism-related parameters. For example, cortisol is a steroid hormone that alters cellular function through transcriptional mechanisms, and exhibits a marked diurnal variation in both rodents and humans, peaking at the beginning of the awake phase [50,51]. However, recent studies have highlighted a mechanism that is intrinsic to the cardiomyocyte as a critical mediator of diurnal variations in cardiac metabolism. Circadian clocks are cell autonomous molecular mechanisms that enable the cell/organ to temporally partition biological processes [5,6]. In doing so, circadian clocks confer the selective advantage of anticipation, allowing preparation prior to the onset of a predicted stimulus/stress. In other words, circadian clocks orchestrate biological processes, such that temporal synchronization between the stimulus and responsiveness is achieved in an appropriate manner. The mammalian circadian clock is comprised of at least 15 transcription factors, whose levels/activities oscillate over the course of the day, with a periodicity of approximately 24 h [6]. Upon heterodimerization, these transcriptional regulators bind to E-boxes in target genes, resulting in induction [52,53]. One cellular process that appears to be under direct circadian clock control is metabolism. The Cardiomyocyte Circadian Clock Circadian clocks are ubiquitous in nature, having been identified in all mammalian cells investigated to date. Circadian clocks can be divided into two main categories, namely central versus peripheral circadian clocks. However, it is important to note that this synchrony is easily disrupted through behaviors such as eating, which can dissociate central and peripheral oscillators. Consistent with its ubiquitous nature, genetic disruption of the circadian clock in murine models in a germline fashion impacts a plethora of processes, ranging from behaviors 132 9. Such a phenotype makes use of germline models of clock disruption difficult for investigation of the role of a cell autonomous clock on a specific biological process. This includes determining of the influence of the cardiomyocyte circadian clock on cardiac metabolism. Accordingly, two novel models of cardiomyocyte-specific circadian clock disruption have been developed to investigate the impact that this molecular mechanism has on cardiac metabolism. Given its transcriptional nature, an initial tactic for identification of those metabolic processes that are regulated by the cardiomyocyte circadian clock included gene expression microarray studies. As discussed earlier, net triglyceride synthesis exhibits a marked diurnal variation in wild-type hearts. It is apparent that cardiac metabolism is a "moving target," and as such, choice of the time-of-day at which an experiment is performed markedly impacts the results observed. Failure to appreciate/account for these oscillations during experimental design can lead to erroneous conclusions. Within this subsection, experimental considerations in light of diurnal variations in metabolic processes will be discussed. Accordingly, laboratory rodents tend to be less active during the light phase, and are more active during the dark phase. The majority of animal model-based research is performed with the goal of improving knowledge regarding underlying mechanisms responsible for human health and disease. Yet, for the sake of convenience, many rodent-based studies are performed during the light phase, which is equivalent to observing human subjects during the middle of the night. This can become increasingly problematic when interventions are performed in laboratory rodents and/or data are correlated to findings in humans. Simple interventions, such as dietary manipulations (including fasting), exercise, and pharmacological interventions are often performed, without consideration of time-of-day. For example, mice are routinely fasted overnight prior to investigation, an intervention that is equivalent to fasting a human subject throughout a day. The effects of distinct diets on metabolic parameters are commonly investigated during the light phase, a time at which food intake reaches a natural trough in rodents, thereby minimizing identification of mechanisms contributing to perturbations during food consumption. Many rodent-based studies exercise mice during the light phase, which is equivalent to forcing a human subject to be physically active in the middle of the night. Finally, both human and rodent studies indicate that sensitivity to many pharmacological agents exhibits a time-of-day-dependence (termed chronopharmacology). Collectively, failure to consider the nocturnal nature of rodent models will likely limit translational capacity. When assessing cardiac metabolism, it is important to appreciate that many of these metabolic processes oscillate in a time-of-day-dependent manner. Many investigations attempt to circumvent this issue, by performing all studies at the same time-of-day. However, choice of the time-of-day at which metabolic studies are performed markedly impacts the results obtained and conclusions drawn. Consider a hypothetical study designed to investigate the mechanisms responsible for high fat diet-induced perturbations in cardiac metabolism in rodents. The latter induce changes in gene and protein expression, which persist when cardiac metabolism is assessed during the light phase. However, circulating fatty acid levels return to control levels during the light phase [33]. Such observations could lead to the erroneous conclusion that circulating fatty acids are not important for perturbations in cardiac metabolism following high fat feeding. Similarly, if the impact of putative glucose oxidation inhibitor was assessed during the light phase, it is possible that an erroneous null result could be obtained, as cardiac glucose oxidation is already depressed at this time of day. Aberrant oscillations in cardiac metabolism are likely to be more common than currently appreciated. Such a term has been utilized to highlight an inability of the myocardium to respond to both acute and chronic interventions. It is likely that the heart exhibits metabolic inflexibility over the course of the day during these disease states, although studies directly interrogating this issue have not been reported to date. Consistent with this hypothesis, the circadian clock in the heart is altered in various animal models of cardiac disease, including pressure overload and streptozotocin-induced diabetes mellitus [63,64]. It is also noteworthy that many genetically modified mouse models are likely models of disrupted metabolic rhythms. Overexpression or knockout of a gene that normally exhibits a diurnal variation in the heart essentially locks expression at the peak or trough. If such a gene plays an important role in metabolism, this in turn has the potential to temporally suspend a metabolic process. These rhythms likely play a critical role in synchronization of metabolic pathways with time-of-daydependent fluctuations in energetic demand, nutrient availability, and presence of pro-oxidants.
