

Purchase fml forte once a day
Recently allergy symptoms negative test results cheap 5ml fml forte with amex, several small endemic foci were reported in southern rural communities where eating raw fish is common [15]. The egg-positive rates, which are regarded as average prevalence of clonorchiasis in the general population in the surveyed year, have been decreasing slowly. Hong and Fang [1] explained that the slow decrease is due mainly to frequent treatment failure or reinfection after treatment. In Guangdong, China, where fish farming is common, the prevalence of human clonorchiasis is about 14%, and it may reach 80% in rural endemic areas [8]. A recent analysis of data from three parasitic disease surveys conducted in Hengxian County, China, in the last 22 years showed substantial increases in the patterns of clonorchiasis prevalence and infection intensity and decrease in trends of prevalence of soil-transmitting helminths [21]. Another recent study in Guangdong, China, reported that incidence rates of clonorchiasis showed a direct increasing trend by years with temperature change [22]. The distribution of clonorchiasis is determined not only by the distribution of snail intermediate hosts but also by the fish-consuming custom of residents in the endemic community. Fishing and eating of raw fish is an old popular tradition that has remained habitual and constant for thousands of years in endemic areas. The eating habit has resulted in persistent transmission of the liver fluke to humans [23,24]. There are several well-known risk factors that are associated with the transmission of clonorchiasis such as poor educational level of local residents, lack of sanitation, habit of eating raw or undercooked freshwater fish, development of freshwater aquaculture, and lack of systematic control activities in many endemic areas. In particular, freshwater aquaculture has rapidly expanded, with a resulting increase in fish contamination that has resulted from a lack of quarantine measures for fish products [25]. The reason for its increase among adult men reflects behavioral patterns of fishing as an occupation or recreation. That finding suggests that host immunity is not so efficient to prevent reinfection or superinfection in humans. Early diagnosis and treatment is important to prevent serious complications of clonorchiasis in humans. Detection of eggs or adult worms in feces, bile, or duodenal fluids is a definite diagnosis. However, since detection of worms from a human body needs invasive procedures, the gold standard diagnosis of C. The images of the liver and bile ducts can be used as a good practical alternative diagnostic method of clonorchiasis. Although most of the positive images are acceptable for diagnosis, their sensitivity and specificity are lower than those of the fecal examination. This is mainly because those images recognize the tissue changes caused by the worms but not the worms itself. Clonorchis sinensis 709 and diffuse dilatation of the peripheral intrahepatic bile ducts [31]. The remaining ductal dilatation with thick wall after chemotherapy further reduces the image specificity [11]. In endemic areas, it is recommended to make diagnosis of clonorchiasis by any feasible method and to treat positives more actively. In heavily endemic areas of China, using mass chemotherapy with praziquantel, it was reported that four selective annual treatments for egg-positive subjects reduced the egg-positive rates from 54. In general, thorough cooking of fish, proper diagnosis, health education, and praziquantel treatment are major requirements for its control. Unfortunately, control of snail intermediate hosts by molluscicides was not considered feasible because of widespread distribution of snails, low prevalence of fluke infection among snails even in endemic communities, hazards to surrounding ecology, and economic considerations [26]. Currently, fish farming and neighboring environmental ponds that are routinely contaminated by untreated sewage have resulted in the establishment of infection in fish populations at large. This phenomenon along with the involvement of animal reservoir hosts will make control of the liver fluke infection even more challenging. Animals are used as basic research models of helminths to study their life cycle in the laboratory as well as to study pathology, immunology, diagnosis, or treatment. In vitro cultivation of helminths or cell culture models, especially the secondary cell line, is a valuable tool that may help us in determining its virulence potential. The recovery rates suggest that rats and hamsters are highly susceptible; guinea pigs, rabbits, and dogs are moderately susceptible but mice are not. Rats, mice, guinea pigs, and rabbits were recognized to be resistant to reinfection after chemotherapy [34]. Mice are the most commonly used laboratory animal model in biomedical research, but they are not susceptible to C. Many strains of mice have been developed for diverse research purposes, and the susceptibility was different in the strains [36]. On the other hand, there have been reports that rats are resistant (to some degree) to reinfection by C. The significant increase in the levels of bile IgA antibodies and serum IgE antibodies in resistant reinfected rats might play a role in the development of resistance to reinfection by C. Meanwhile, hamsters, dogs, and humans are susceptible to primary and also reinfection or superinfection, and the infection is accumulated in those hosts. The resistance of the rats was mainly modulated by the local immune response in the infected tissue [39]. The host immunity provokes the host resistant to reinfection or superinfection in rats but not in humans. In this perspective, glycolytic enzymes are crucial molecules for trematode survival and have been targeted for drug development. On the other hand, there have been several reports on in vivo study to evaluate other chemotherapeutic agents than praziquantel to treat clonorchiasis. Those studies investigated cure rates, reduction of worm burdens, and morphological damage of C. One clinical trial in China reported a cure rate of 44% with a 400 mg single dose of tribendimidine and of 58% after therapy for 3 days [51]. The chemotherapy study using experimental animals should evaluate cure rates or worm reduction rates after medication. Rats or rabbits are commonly used for this purpose because they are susceptible and because C. The induced pathological changes of the infected bile duct start to present different clinical symptoms, although severity of the pathology depends upon intensity and chronicity of the infection. In extreme cases, liver enlargement, thickening of the bile ducts, fibrosis, and some destruction of liver parenchyma are evident. However, unlike Fasciola, Clonorchis does not invade liver tissues and therefore, does not cause extensive liver necrosis [8]. Several well-documented epidemiological, histopathological, and experimental studies of C. In this regard, it was reported that bile acids and conjugated bile salts favored the survival of newly excysted juvenile C. These studies helped define the best conditions for in vitro maintenance of the organism for long durations in different inorganic solutions and nutrient media under laboratory conditions. In vitro cultivation in any nutrient media could not foster adult worms from larvae. Clonorchis sinensis 713 For the biliary hyperplasia, several in vitro experiments provided strong evidence that C. There has been a well-established body of knowledge about these highly reactive free radicals that can damage biologically relevant molecules of cells. Consequently, oxidative stress arising as a result of an imbalance between free radical production and antioxidant defenses is associated with damage to a wide range of molecular species including lipids, proteins, and nucleic acids [73,74]. Since its host specificity is low, most of the laboratory mammals except for mice are susceptible, and rats or rabbits are commonly used for common experimental infection. It is recommended to develop other animal models such as murine model for experimental studies on immunology and oncology of C. The involvement of the cysteine proteases of Clonorchis sinensis metacercariae in excystment. Infection status of freshwater fish with metacercariae of Clonorchis sinensis in Korea.
Purchase fml forte now
Effect of ticlopidine on the longterm patency of saphenousvein bypass grafts in the legs allergy treatment rash order genuine fml forte on-line. Etude de la Ticlopidine apres Pontage FemoroPoplite and the Association Universitaire de Recherche en Chirurgie. Metaanalysis of results from eight randomized, placebocontrolled trials on the effect of cilostazol on patients with intermittent claudication. Effects of aspirin on coronary reocclusion and recurrent ischemia after thrombolysis: a metaanalysis. I: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in vari ous categories of patients. Prescribing pat terns of antiplatelet agents are highly variable after lower extremity endovascular procedures. Antiplatelet and anticoagulant drugs for pre vention of restenosis/reocclusion following peripheral endovascular treatment. Potential use of a low molecularweight heparin to prevent restenosis in patients with extensive wall damage following peripheral angioplasty. Lowmolecularweight heparin for prevention of restenosis after femoropopliteal percutaneous trans luminal angioplasty: a randomized controlled trial. Functional and clinical outcomes of nitinol stenting with and without abciximab for complex superficial femoral artery disease: a randomized trial. Adjunctive abciximab improves patency and functional outcome in endovascular treatment of femoro popliteal occlusions: initial experience. Lowdose aspirin combined with dipyridamole versus anticoagulants after femoropopliteal percutaneous transluminal angioplasty. Cilostazol reduces restenosis after endovascular therapy in patients with femoropopliteal lesions. A better effect of cilostazol for reducing instent restenosis after femoropopliteal artery stent placement in comparison with ticlopidine. Bivalirudin versus heparin dur ing coronary angioplasty for unstable or postinfarction angina: final report rea nalysis of the Bivalirudin Angioplasty Study. Clinical experience with the use of bivalirudin in a large population undergoing endovascular abdominal aortic aneurysm repair. Heparin versus bivalirudin for carotid artery stenting using proximal endovascular clamping for neuroprotection: results from a prospective randomized study. ChaPter 83 Chronic Venous Insufficiency Karthik Gujja1, Cristina Sanina2, and Jose M. Varicose veins are a common mani festation of chronic venous insufficiency and affect approximately 25% of adults in the Western hemisphere, where prevalence varies greatly by geographic area. These reported ranges reflect differences in the population distribution of risk factors, accuracy in the application of diagnostic criteria, and the quality and availability of medical diagnostic and treatment resources. Various risk factors are responsible for these incidences: older age, pregnancy (especially multiple), family history of venous disease, female gender, obesity, and occupations that result in significant orthostasis from prolonged standing [2]. Historically, the treatment has been surgery, with high ligation and stripping, combined with phlebectomies. However, the operation can occa sionally be associated with significant postoperative morbidity, including bleeding, groin infection, thrombophlebitis, and saphen ous nerve damage. Conventional surgery is expensive as it is often performed in hospital using general or regional anesthesia. Performed as officebased procedures using tumescent local anes thesia, the new minimally invasive techniques have been shown in numerous studies to obliterate the affected vein, eliminate reflux, and improve symptoms safely and effectively [3]. The Tampere study investigated a large cohort of 3284 men and 3590 women with varicose veins and showed a prevalence of 18% and 42%, respectively. The overall prevalence of varicose veins at ages 40, 50, and 60 years was 22%, 35%, and 41%, respectively [8]. Pregnancy Multiparity has been shown to be a major predisposing factor for development of varicose veins and part of its increase in prevalence has been attributed to female gender. In the Tampere study, the prevalence of varicose veins in women with 0, 1, 2, 3, and 4 or more pregnancies was 32%, 38%, 43%, 48%, and 59%, respectively [8]. The exact mechanism of pregnancyinduced venous insufficiency is not fully understood. Pressure of the gravid uterus on the pelvic vasculature is associated with lower extremity venous hypertension, venous distention, and valve rupture. The saphenous veins have been shown to contain estrogen and progesterone receptors that may enable the estradiolrich hormonal state of pregnancy to exert a similar effect. Hereditary A positive family history of varicose veins is associated with a sig nificantly increased risk of development of varicose veins. A study conducted in Japan showed that 42% of women with varicose veins reported a positive family history compared with 14% without the disease [10]. Various genetic predispositions have been linked to development of varicose veins. Lifestyle Sedentary work and prolonged standing at work are independent risk factors for development of venous insufficiency [12]. In the Tampere study, the prevalence of varicose veins in standing versus sitting workers was 36% and 27%, respectively. The Edinburgh Vein Study has also shown predisposition of varicose veins in patients whose work involved prolonged standing. It has been assumed that subcutaneous dep osition of adipose and fibrous tissue disrupts the cutaneous venous network, impairs drainage, and promotes stasis. The characteristic serpiginous appearance of varicose veins reflects segments of dilatation interspersed between segments of normal vein [14]. Venous stasis this concept suggests that stagnant accumulation of blood in tortu ous, nonfunctioning, dilated skin veins results in subsequent tissue anoxia and cell death leading to skin changes and ulceration. Venous hypertension this concept has been attributed to muscle pump dysfunction and venous ulceration. It has been hypothesized that venous hydro static pressure is equal in the deep and superficial venous systems both at rest and in the erect position. During calf muscle contrac tion, the pressure in the deep veins increases more than in the superficial veins. However, valve closure prevents the pressure from being transmitted to the superficial veins. Fibrin cuff Pericapillary fibrin cuff has been associated with restriction of oxygen diffusion across the vessel wall leading to edema and der matosclerotic skin changes. Pericapillary fibrin cuffs may act as a barrier, a marker for endothelial cell damage, or as part of an overall mechanism of macromolecular leakage and trapping [20]. It contends that reflux is mainly transmitted to the superficial veins through perforators. Studies by Raju and Fredericks have shown that this effect explains and correlates with most venous ulceration cases. Because of stasis and venous pressure changes, margination of the white cells occurs resulting in capillary plugging with further tissue hypoxia and damage. These cells also activate free radicals and cytokine (interleukin1, tumor necrosis factor) release, resulting in tissue damage and apoptosis [22]. Unifying concepts of leukocyte trapping and venous hypertension have also been proposed [16]. There are two universally accepted theories: (i) primary valvular incompetence and (ii) primary congenital vein wall weakness. Primary valvular incompetence is the oldest theory and was pos tulated by Sir William Harvey in 1628. It states that varicose veins develop as a sequela of central valvular incompetence related to paucity or atrophy of its valves.
Discount 5 ml fml forte
The prognostic value of renal resistance during hypothermic machine perfusion of deceased donor kidneys allergy symptoms 5 month old buy discount fml forte 5 ml online. Use of two biomarkers of renal ischemia to assess machine-perfused non-heart-beating donor kidneys. Glutathione-S-transferase as predictor of functional outcome in transplantation of machinepreserved non-heart-beating donor kidneys. The value of machine perfusion perfusate biomarkers for predicting kidney transplant outcome. Nomogram for predicting the likelihood of delayed graft function in adult cadaveric renal transplant recipients. A comparison of hypothermic machine perfusion versus static cold storage in an experimental model of renal ischemia reperfusion injury. An in vivo autotransplant model of renal preservation: cold storage versus machine perfusion in the prevention of ischemia/reperfusion injury. Perfusion storage reduces apoptosis in a porcine kidney model of donation after cardiac death. Flow cessation triggers endothelial dysfunction during organ cold storage conditions: strategies for pharmacologic intervention. Room temperature pulsatile perfusion of renal allografts with Lifor compared with hypothermic machine pump solution. Addition of a water-soluble propofol formulation to preservation solution in experimental kidney transplantation. Gaseous hydrogen sulfide protects against myocardial ischemia-reperfusion injury in mice partially independent from hypometabolism. Effects of hydrogen sulphide in an experimental model of renal ischaemia-reperfusion injury. Detrimental effects of prolonged warm renal ischaemia-reperfusion injury are abrogated by supplemental hydrogen sulphide: an analysis using real-time intravital microscopy and polymerase chain reaction. Hydrogen sulphide ameliorates ischaemia-reperfusion injury in an experimental model of non-heartbeating donor kidney transplantation. Transfection and transgene expression in a human kidney during ex vivo warm perfusion. Machine perfusion in organ transplantation: a tool for ex-vivo graft conditioning with mesenchymal stem cells. Administered mesenchymal stem cells enhance recovery from ischemia/reperfusion-induced acute renal failure in rats. Donor-derived mesenchymal stem cells combined with low-dose tacrolimus prevent acute rejection after renal transplantation: a clinical pilot study. Subnormothermic machine perfusion for preservation of porcine kidneys in a donation after circulatory death model. Static normothermic preservation of renal allografts using a novel nonphosphate buffered preservation solution. A pilot study assessing the feasibility of a short period of normothermic preservation in an experimental model of non-heart beating donor kidneys. Oxygen consumption during oxygenated hypothermic perfusion as a measure of donor organ viability. Supplementation with a new therapeutic oxygen carrier reduces chronic fibrosis and organ dysfunction in kidney static preservation. Benefits of active oxygenation during hypothermic machine perfusion of kidneys in a preclinical model of deceased after cardiac death donors. Role of oxygenation in hypothermic machine perfusion of kidneys from heart beating donors. Improved kidney graft function after preservation using a novel hypothermic machine perfusion device. Evaluation of a novel system for hypothermic oxygenated pulsatile perfusion preservation. However, the boundaries of kidney transplantation are increasingly being extended and there is more reliance on the use of so-called marginal donors to accommodate the increasing demand. Hypothermic temperatures act to inhibit the enzymatic processes and prevent injury. There is a two- to threefold decrease in metabolism for every 10 C reduction in temperature. The damage caused by hypothermic conditions is evident upon reperfusion when normal circulation is restored to the organ. Large data series have shown that the cold ischemic time is an independent risk factor for graft failure. Nonetheless, he pursued the idea of keeping organs alive and functioning at warmer temperatures. With the help of Charles Lindbergh, an engineer and pilot, he developed the first organ perfusion device, in 1935. The system was capable of maintaining a sterile, pulsating circulation of fluid through a living organ. It was made up of three glass chambers, an organ chamber at the top, a pressure equalizing chamber in the middle, and fluid chamber on the bottom. A mixture of oxygen, carbon dioxide, and nitrogen was pulsated by compressed air into the perfusate through the equalizing chamber and into the organ. They perfused a variety of organs such as the thyroid, suprarenal gland, ovary, spleen, heart, and kidney from adult fowls and cats. The organs were perfused with a nutrient fluid designed to culture the organs which often contained blood, serum, or solutions containing proteinsplit products such as hemin, cysteine, insulin, thyroxine, glutathione, vitamin A, and ascorbic acid. This perfusion system allowed the organs to be studied in an ex vivo environment to acquire knowledge on the metabolic processes and nutrient requirements of individual organs. Nonetheless, his research pioneered the development of the extracorporeal perfusion systems that are widely used today in cardiac surgery and indeed for the last decade, to perfuse isolated organs at normothermic temperatures ex vivo. Several groups identified a need for alternative techniques of preservation to allow more marginal organs to be used and to improve their outcome. Kidneys were perfused at a subnormal temperature of 32 C and mean arterial pressure of approximately 35 mmHg with an acellular culture-like medium solution. In 2006, our group (Hosgood & Nicholson) reported the use of an adapted pediatric cardiopulmonary bypass system incorporating a centrifugal pump, a membrane oxygenator, venous reservoir, and heat exchanger. Kidneys were perfused at a near physiological pressure (75 mmHg) and temperature (36 C) with a packed red cell based solution. There are other isolated reports of systems that have adapted or modified hypothermic perfusion technology,30 or used custom-made devices with roller pumps and dialysis circuits31,32 to obtain optimal renal function. There is one commercially available system; "The Kidney Assist" made by a Dutch company "Organ Assist. It is a pressure-controlled device which includes a rotary pump to deliver a pulsatile flow. A hollow fiber oxygenator is also included in the system to oxygenate the blood based solution. Despite the availability of this system there are no current reports of its application in kidney transplantation. When administered intravenously they caused side effects such as anaphylaxis, hypotension, reduced platelet count, and complement activation. Historically, other artificial hemoglobin based oxygen carriers have also been used as preservation mediums. A more stable pyridoxalated hemoglobin-polyoxyethylene solution has proved to be more successful and Brasile et al. However, due to the complexity of manufacturing, the cost is considerable, which may limit their adaptation. Other novel solutions such as Lifor, an artificial preservation medium containing a nonprotein oxygen carrier, nutrients, and a growth factor have also been used for preservation at more normothermic temperatures. Studies in the heart have shown an advantage compared to a standard cardioplegia solution. However, with the development of improved atraumatic centrifugal pumps and equipment used in cardiac bypass surgery, hemolysis is less of a problem. Modern pumps reduce the risk of stress and hemolysis and the membrane oxygenators enable filtration and highly efficient oxygenation.
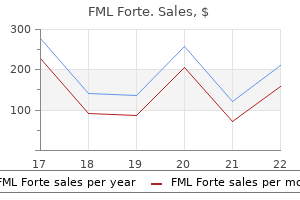
| Comparative prices of FML Forte | ||
| # | Retailer | Average price |
| 1 | Verizon Wireless | 805 |
| 2 | Albertsons | 114 |
| 3 | CVS Caremark | 974 |
| 4 | PetSmart | 947 |
| 5 | Ingles Markets | 726 |
| 6 | Darden Restaurants | 253 |
| 7 | HSN | 685 |
| 8 | Lowe's | 808 |
| 9 | Dillard's | 258 |
| 10 | ShopRite | 986 |
Purchase fml forte without a prescription
The ratio of peak systolic pressure distal to the lesion over peak systolic aortic pressure at the renal artery level is called renal: aorta pressure ratio allergy map cheapest fml forte. Furthermore, repeating pressure gradients after each balloon angioplasty provides an objective tool to indicate when the lesion has been adequately dilated and the webs are suffi ciently disrupted to allow normal blood flow and pressure. The translesional pressure gradient can be measured across the stenosis, comparing aortic pressure with pressure in the renal artery after the stenosis. Fortunately, several recent clinical trials provide more evidence about this choice. This was defined as a composite of death from cardiovascular or renal causes, stroke, myocardial infarction, hospitalization for congestive heart failure, progressive renal insufficiency, or the need for permanent renal replacement therapy. There was no significant difference in the occurrence of the primary composite endpoint, or any of its individual components, between the stent group and medical therapyonly group, and no difference in allcause mortal ity. Systolic blood pressure was modestly lower in the stent group than in the medical therapyonly group (-2. Renal artery stenting was performed in 33 patients who displayed a serum creatinine >1. However, as stated earlier, when compared with a contemporary group of individuals managed medically, there is no evidence that stenting improves kidney function more than medical therapy alone. This observation is confounded significantly though by significant age differences between the medical therapy and revascularized sub jects. In general terms these cohorts demonstrated that 75% of subjects undergoing revasculari zation had no further episodes after treatment [36,37]. There have been efforts in developing predictors that can identify subgroups of patients who will benefit from revascularization. On the other hand, a renal resistance index of more than 80 by duplex Doppler ultrasound was reported to be an indicator of unresponsiveness to revascularization [42]; yet again the finding was not replicated in subsequent studies [43,44]. There are unfortunately few comparative data between different regi mens of medical therapy. Clearly, antiatherosclerotic therapies are indicated, such as lipidlowering agents, especially statins. Lifestyle modification is also impor tant such as smoking cessation, exercise, and weight reduction. Smoking is not only a cardiovascular risk factor, it is also a risk factor for chronic kidney disease and can increase the risk of nephropathy progression [48]. All patients with cardiovascular dis ease or cardiovascular disease equivalents are highrisk for adverse cardiovascular events. We believe that the strongest rationale for revascularization in the athero sclerotic patient is for those infrequent individuals with severe renal stenosis and advanced chronic kidney disease who are faced with the choice of an attempt at revascularization or instituting renal replace ment therapy in the near future. However, this is not an evidence based recommendation but is grounded in clinical experience. This type of lesion involves the ostium of renal artery at its origin from the aorta. Radial or brachial artery access site should be considered for ante grade approach if the takeoff of the renal artery is sharply down ward angulated or in the presence of severe bilateral aortoiliac disease and/or tortuosity. In the presence of an aortic aneurysm, the angulation of the renal artery could favor upper or lower extremity access. Similarly, if a renal artery has been covered by a stent during an aortic procedure, careful selection of access and willingness to change access sites may be the difference between a successful and unsuccessful procedure. Renal artery angiography Abdominal aortography prior to stenting should be performed to identify the local anatomy, including the severity and location of aortic pathology, location of the renal ostia, the extent of the ostial stenosis, the angulation of the renal artery takeoff from the abdomi nal aorta, accessory renal arteries, and the presence of aneurysms and calcification. A shallow left anterior oblique projection is often the best angle view for identifying both the right and left renal ostia. Prior to the first selective renal angiog raphy, active aspiration of 10 mL blood via a Yconnector or passive backbleeding can be performed to clean debris from the guiding catheter to reduce the risk of embolism. Engagement of guide catheter Anticoagulation should be started after sheath insertion. Indirect engagement of the renal artery ostium using the guide catheter is preferred over direct engagement of the renal ostium because of the higher risk of renal artery complications associated with direct engagement. Indirect engagement of the renal ostium can be achieved through two kinds of approaches: the "exchange technique" or the "no touch" technique. For the exchange technique, after renal angiography a 4Fr diag nostic catheter is inserted through the sheath and used to engage the renal ostium gently. The soft small diagnostic catheter carries a lower risk of atheroembolization and dissection than the stiffer guiding catheter. After engagement of the diagnostic catheter in the renal artery ostium, a guidewire, 0. The guide is then advanced over the wire and diagnostic catheter, after which the diagnostic catheter is removed leaving the guidewire in place. Then the guidewire is retracted to allow the guide catheter to assume its angled shape. The tip of the guidewire is against the aor tic wall above the renal artery ostium. The opening of the guide catheter is then adjusted gently to align the opening of the guide catheter with the ostium of renal artery. Hydrophilic wires should generally be avoided because of the higher risk of renal parenchymal perforation. A 6Fr guiding catheter is most often used and its shape should reflect the angle between renal artery and the aorta with considera tion of other characteristics of local anatomy. When this is done great care should be taken for symptoms of pending arterial rupture or dissection, heralded as back pain, at which time the balloon is gently deflated. In ath erosclerotic stenoses, predilatation is achieved through a balloon with a slightly smaller diameter than the reference vessel. Percutaneous renal stenting the atherosclerotic renal artery often recoils after angioplasty resulting in restenosis, so stenting is a better approach to maintain the patency of the artery. Balloon expandable stents are sized 1:1 with the reference vessel diameter, not the poststenotic dilated seg ment. Stent length should be as short as possible while being long enough to completely cover the entire lesion. Using the shortest stent possible that allows complete lesion coverage can be helpful because the renal artery displaces dynamically during the respiro phasic cycle and longer stents are subject to greater stress and potentially fracture risk. The stent should be positioned with 1 mm protruding into the aorta, in order to completely cover the arterial ostium. It uses a dualballoon delivery system, with a locator balloon stopping at the ostium for visually confirming the right position. Further inflation of the locator balloon results in flaring of the proximal stent end and full ostial coverage. After proper positioning of the stent, the balloon is inflated to its nominal diameter to achieve a 1: 1 ratio with the diameter of the reference vessel. Inadequate stent expansion results in high rates of restenosis; thus, it is important to further dilate the stent if it appears to be underdeployed initially. Larger balloons with higher inflation pressure can be utilized to further dilate an underex panded stent. Specifically, when the patient experi ences back pain during balloon inflation, this can be the only warning sign before main renal artery rupture or perforation. Should this complication occur, placement of a covered stent is clearly indicated if the perforation of the renal artery is not promptly sealed with balloon inflation. A final selective angiogram should be performed to assess the stent position, exclude dissection, perfora tion and spasm, and the renal parenchymal blush to exclude atheroembolism. The "kissing balloon technique" can be utilized for the renal arteries with same origin without a common trunk or in the pres ence of a short main trunk. The first utilizes a single guiding catheter through which two wires and two balloons are introduced by femoral access route. However, this technique is limited by the relatively large diameter of the stents and their delivery balloons, making this impractical for lesions of the main renal arteries that require stents of 5 mm diameter or larger.
Cheap fml forte 5ml with amex
The RovA dimer is given in red; the stars illustrate the amino acid substitution that renders the RovA protein less susceptible to the Lon protease allergy symptoms red ears purchase fml forte 5ml on line. Coinfection studies with O:3 wild and mutant strains demonstrated that small variations within the O:3 genome improved colonization/survival in swine but had only a minor effect on the colonization in mice. Besides, they first observed yersiniae dissemination to brain in experimental infection. More surprising were the pathomorphological changes not established in tonsils with the virulent strain but with sodA mutant strain. Together, these showed the potential of sodA mutant to be a candidate for immunization. Infected macrophages displayed general features of apoptosis such as membrane blebbing (apoptotic body formation) and nuclear and cellular shrinkage. Specifically, two chromosomal genes, inv and ail, and one plasmidial gene, yadA, of Y. This protein is thought to be expressed in the cell wall of the bacteria when they reach the small intestine and is required for the initial steps of host colonization and penetration into the intestinal epithelium cells. Like Inv, Ail is chromosomally encoded and also mediates the binding and invasion of epithelial cells. YadA can bind to collagen, fibronectin, and laminin and mediate adhesion to epithelial cells and macrophages. Beyond adhesion, YadA can act as an autoagglutinin, has antiphagocytic properties, and serum resistance. Besides inv, ail, ystA, and virF, other chromosomal and plasmidial encoded genes are responsible for the expression of virulence determinants in Y. It controls the synthesis of cytokines, acute-phase proteins, and adhesion molecules and mediates cellular survival by prevention of apoptosis. These pathogens generate a number of proteins that help evade host innate immune response and replicate inside the host. Use of mouse models revealed the interaction between the host and the extracellular lifestyle of the pathogen. Comparative studies employing minipig and mouse models uncovered that O:3 strains utilize serotype- and host-specific colonization strategies in fattening pigs. Cell models are useful for investigating different stages of yersinia infection: adhesion and invasion, and evasion of host innate and adaptive immune mechanisms. Intestinal carriage of Yersinia pseudotuberculosis by wild birds and mammals in Japan. Ecology and geographic distribution of Yersinia enterocolitica among livestock and wildlife in China. Strategies used by Yersinia enterocolitica to evade killing by the host: Thinking beyond Yops. Immunohistochemical and electron microscopic study of interaction of Yersinia enterocolitica serotype O8 with intestinal mucosa during experimental enteritis. Yersinia pseudotuberculosis inhibits Fc receptor-mediated phagocytosis in J774 cells. Inhibition of phagocytosis in Yersinia pseudotuberculosis: A virulence plasmid-encoded ability involving the Yop2b protein. Role of YadA in resistance of Yersinia enterocolitica to phagocytosis by human polymorphonuclear leukocytes. Differential contribution of Yersinia enterocolitica virulence factors to evasion of microbicidal action of neutrophils. Role of Yops in inhibition of phagocytosis and killing of opsonized Yersinia enterocolitica by human granulocytes. Yersinia signals macrophages to undergo apoptosis and YopJ is necessary for this cell death. Role of plasmid-encoded antigens of Yersinia enterocolitica in humoral immunity against secondary Y. Rational live oral carrier vaccine design by mutating virulence-associated genes of Yersinia enterocolitica. Phospholipase A of Yersinia enterocolitica contributes to pathogenesis in a mouse model. Yersinia-induced apoptosis in vivo aids in the establishment of a systemic infection of mice. Contribution of the major secreted yops of Yersinia enterocolitica O:8 to pathogenicity in the mouse infection model. Requirement of the Yersinia pseudotuberculosis effectors YopH and YopE in colonization and persistence in intestinal and lymph tissues. Chromosome-mediated resistance of Yersinia enterocolitica serotype O9 to intracellular killing by mouse peritoneal macrophages. Experimental infection of mice with Yersinia enterocolitica serotype O9 by oral and parenteral routes: spreading and enterotropism of virulent yersiniae. Presence of Yersinia enterocolitica in tissues of orally-inoculated pigs and the tonsils and feces of pigs at slaughter. Experimental infection of newborn piglets with Yersinia enterocolitica: An animal model of enteritis. Unique virulence properties of Yersinia enterocolitica O:3-An emerging zoonotic pathogen using pigs as preferred reservoir host. Essential role of invasin for colonization and persistence of Yersinia enterocolitica in its natural reservoir host, the pig. Yersinia enterocolitica infection and tcaAdependent killing of Caenorhabditis elegans. Transcriptional analysis of long-term adaptation of Yersinia enterocolitica to low-temperature growth. Comparative analysis of the Photorhabdus luminescens and the Yersinia enterocolitica genomes: Uncovering candidate genes involved in insect pathogenicity. Analysis of the class-specific immune response to Yersinia enterocolitica virulence-associated antigens in oro-gastrically infected rabbits. Experimental Yersinia enterocolitica infection in rodents: A model for human yersiniosis. Arthritis after experimental infection with Yersinia enterocolitica O:3 in rabbits. An enterotoxin-negative strain of Yersinia enterocolitica serotype O:3 is capable of producing diarrhea in mice. Invasiveness of Yersinia enterocolitica lacking the virulence plasmid: An in-vivo study. Clinical, morphological, and biochemical alterations in acute intestinal yersiniosis. Effect of acute Yersinia enterocolitica infection on in vivo and in vitro small intestinal solute and fluid absorption in the rabbit. Role of Yersinia enterocolitica Yst toxin in experimental infection of young rabbits. Proper expression of the O-antigen of lipopolysaccharide is essential for the virulence of Yersinia enterocolitica O:8 in experimental oral infection of rabbits. Contribution of the Mn-cofactored superoxide dismutase (SodA) to the virulence of Yersinia enterocolitica serotype O8. Comparison of the course of infection of virulent Yersinia enterocolitica serotype O:8 with an isogenic sodA mutant in the peroral rabbit model. Evidence for two genetic loci in Yersinia enterocolitica that can promote invasion of epithelial cells. The Yersinia enterocolitica inv gene product is an outer membrane protein that shares epitopes with Yersinia pseudotuberculosis invasin. The ail gene of Yersinia enterocolitica has a role in the ability of the organism to survive serum killing. Digoxigenin-labelled inv- and ail-probes for the detection and identification of pathogenic Yersinia enterocolitica in clinical specimens and naturally contaminated pig samples.
Buy genuine fml forte online
Being a facultative anaerobe allergy symptoms 10 purchase 5ml fml forte mastercard, Aeromonas is oxidase and catalase positive (best tested on media without a fermentable sugar, such as MacConkey agar). Aeromonas 239 Other morphological features include the possession of a single polar flagellum (especially motile strains, although some species may form peritrichous or lateral flagella or no flagella in solid media) and pili (fimbriae, which are surface appendages that facilitate attachment to host cells), which are either short rigid (S/R type) or long wavy flexible (L/W type). Direct mucocutaneous contact with or exposure of open wound to environmental mud or water offers another way for aeromonads to enter human hosts (extraintestinal infections). In Aeromonas gastroenteritis, after enduring the detrimental effects of gastric acidity, ingested bacteria settle in the small or large intestine, and release enterotoxigenic molecules (leading to enteritis), or invade the gastrointestinal epithelium (causing dysentery or colitis). Aeromonad infections often occur in the community settings, as well as in health-care facility settings. While all people are susceptible to Aeromonas-associated gastroenteritis, young children (<5 years of age) and older adults (>60 years of age) are particularly vulnerable. Additional risk factors for Aeromonas infections include traumas and near-drowning events related to recreational activities. The secretory form of Aeromonas gastroenteritis is most common and manifests with low-grade fever and abdominal pain, and watery diarrhea, with mild to moderate dehydration. The watery diarrhea is generally a self-limiting illness, lasting a few days to a few weeks. The dysenteric form of Aeromonas gastroenteritis is less common and shows cramping abdominal pain and mucus (leukocytes) and blood in stools (similar to shigellosis). The chronic form of Aeromonas gastroenteritis lasts for more than 2 months and is frequently associated with A. With the spread of gastrointestinal infections, appendicitis, peritonitis, pancreatitis, and acute cholangitis may emerge [19]. Application of leeches (which may harbor aeromonads symbiotically) to tissue flaps or replantation areas during plastic or reconstructive surgery to relieve venous congestion may be a potential cause of Aeromonas infections. Most (90%) of the Aeromonas species from humans produce -hemolysis on sheep blood agar, with the exception of A. Identification at the genus level is achieved by positive oxidase test, fermentation of d-glucose, motility (most Aeromonas species are motile apart from A. However, phenotypic identification to species level may require additional work involving the use of selective and differential media [33]. A number of selective media (supplemented with ampicillin and/or inhibitors such as bile salts, brilliant green, and sodium lauryl sulfate) have been used for recovery of Aeromonas species. Aeromonas isolates surviving the selective process can be further distinguished via differentiation media. A combination of selective and differential media enables to classify clinical Aeromonas isolates into the A. Prevention of Aeromonas infections should focus on avoiding physical contact with marine microorganisms or wild water or incidental ingestion of contaminated food or water, and eating uncooked seafood. Additionally, mice undergoing streptomycin pretreatment allow transient Aeromonas colonization and enable determination of the colonization rates of different isolates. Furthermore, intraperitoneal injection of immunocompromised mice or gastric lavage of neonatal mice offer alternative approach for investigating of Aeromonas pathogenicity relating to Aeromonas-induced gastroenteritis as well as extraintestinal infections [54,55]. Rats (Rattus norvegicus) undergoing clindamycin pretreatment develop a self-limited, loose stool (evidence of enteritis) after oral feeding with A. Zebrafish succumbing to Aeromonas infection often displays clinical signs typical of hemorrhagic septicemia [57]. Aeromonas isolate is considered virulent when relative survival is >60%, whereas Aeromonas isolate is considered avirulent when relative survival is <40%. Other animal models used to study Aeromonas strains include crayfish (Pacifastacus leniusculus), mealworm larvae (Tenebrio molitor), leech, and blue gourami. Using Caco-2 cells, it was shown that c-jun and c-fos are upregulated upon incubation with virulent Aeromonas isolates and thus provide a predictive indicator of Aeromonas virulence [61]. Besides causing diseases in fish and other animals, Aeromonas species are also responsible for opportunistic foodborne or wound-related infections in humans, including gastroenteritis and extraintestinal infections. Pathogenic Aeromonas species are known to generate a number of virulence factors that aid their invasion of host cells and sabotage host immune surveillance. Nonetheless, despite our concerted efforts in the past, an effective vaccine against Aeromonas infections is still unavailable. Markers of pathogenicity islands in strains of Aeromonas species of clinical and environmental origin. Pan-genome analysis of Aeromonas hydrophila, Aeromonas veronii and Aeromonas caviae indicates phylogenomic diversity and greater pathogenic potential for Aeromonas hydrophila. A foodborne outbreak of Aeromonas hydrophila in a college, Xingyi City, Guizhou, China, 2012. Phylogenetic diversity of Aeromonas from "alheira," a traditional Portuguese meat product. Inactivation kinetics of various chemical disinfectants on Aeromonas hydrophila planktonic cells and biofilms. Skin and soft tissue infections following marine injuries and exposures in travelers. Aeromonas stool isolates from individuals with or without diarrhea in southern Taiwan: predominance of Aeromonas veronii. Spontaneous bacterial peritonitis caused by Aeromonas caviae in a patient with cirrhosis. Aeromonas hydrophila as a causative organism in peritoneal dialysis-related peritonitis: case report and review of the literature. Aeromonas pneumonia in a trauma patient requiring extracorporeal membrane oxygenation for severe acute respiratory distress syndrome: case report and literature review. Surgical site infection due to Aeromonas species: report of nine cases and literature review. Ciprofloxacin-resistant Aeromonas hydrophila infection following leech therapy: a case report and review of the literature. Development of diagnostic and vaccine markers through cloning, expression, and regulation of putative virulence-protein-encoding genes of Aeromonas hydrophila. Detection and characterization of antimicrobial resistance and putative virulence genes in Aeromonas veronii biovar Sobria isolated from gilthead sea bream (Sparus aurata L. Complexity of -lactamases among clinical Aeromonas isolates and its clinical implications. The genus Aeromonas: biochemical characteristics, atypical reactions, and phenotypic identification schemes. Characterization and virulence potential of phenotypically diverse Aeromonas veronii isolates recovered from moribund freshwater ornamental fishes of Kerala, India. Development of cross-priming amplification assays for rapid and sensitive detection of Aeromonas hydrophila. Development of highly sensitive electrochemical genosensor based on multiwalled carbon nanotubes-chitosan-bismuth and lead sulfide nanoparticles for the detection of pathogenic Aeromonas. Molecular basis of sulfonamide and trimethoprim resistance in fish-pathogenic Aeromonas isolates. Phylogenetic diversity, antibiotic resistance and virulence traits of Aeromonas spp. A mouse model for characterization of gastrointestinal colonization rates among environmental Aeromonas isolates. Gastrointestinal colonization rates for human clinical isolates of Aeromonas veronii using a mousemodel. Re-examination of Rattus norvegicus as an animal model for Aeromonas-associated enteritis in man. Tetrahymena: an alternative model host for evaluating virulence of Aeromonas strains.
Best 5 ml fml forte
Necropsies revealed pulmonary hemorrhage with necrosis allergy juniper best 5 ml fml forte, and flukes as long as 8 mm were recovered from intrathoracic tissues. Interestingly, while eggs from worms encased in a cyst were passed in the feces, those from worms in the pleural cavity were only found on the lung surface and pleural cavity. Humans usually acquire Paragonimus infection through consumption of raw or undercooked crustaceans or meat from a paratenic host, with serious consequence. Clearly, continued application of rapid, sensitive, and specific laboratory diagnostic procedures and prompt implementation of appropriate treatment regimens are critical for limiting the harmful effects of human paragonimiasis. North American paragonimiasis (caused by Paragonimus kellicotti) in the context of global paragonimiasis. A molecular perspective on the genera Paragonimus Braun, Euparagonimus Chen and Pagumogonimus Chen. A new species of Paragonimus (Trematoda: Troglotrematidae) from a cat infected with metacercariae from mountain crabs Larnaudia larnaudii. A rare case of paragonimiasis miyazaki with lung involvement diagnosed 7 years after infection: a case report and literature review. Morphological and molecular characterization of Paragonimus westermani in northeastern India. Detection of Paragonimus mexicanus (Trematoda) metacercariae in crabs from Oaxaca, Mexico. Presence of three distinct genotypes within the Paragonimus westermani complex in northeastern India. Pleuropulmonary infection by Paragonimus westermani in the United States: a rare cause of eosinophilic pneumonia after ingestion of live crabs. Systems biology studies of adult Paragonimus lung flukes facilitate the identification of immunodominant parasite antigens. Paragonimus heterotremus Chen and Hsia (1964), in Vietnam: a molecular identification and relationships of isolates from different hosts and geographical origins. Molecular identification of a case of Paragonimus pseudoheterotremus infection in Thailand. Molecular variation in the Paragonimus heterotremus complex in Thailand and Myanmar. Discovery of Paragonimus westermani in Vietnam and its molecular phylogenetic status in P. The mitochondrial genome of Paragonimus westermani (Kerbert, 1878), the Indian isolate of the lung fluke representative of the family Paragonimidae (Trematoda). Molecular discrimination between individual metacercariae of Paragonimus heterotremus and P. Application of multiplex pcr for species discrimination using individual metacercariae of Paragonimus occurring in Thailand. Application of a real-time fluorescence resonance energy transfer polymerase chain reaction assay with melting curve analysis for the detection of Paragonimus heterotremus eggs in the feces of experimentally infected cats. Artemether and tribendimidine lack activity in experimental treatment of Paragonimus westermani in the dog. Effectiveness of mefloquine against Clonorchis sinensis in rats and Paragonimus westermani in dogs. Experimental infection with Paragonimus heterotremus metacercariae in laboratory animals in Manipur, India. Experimental chemotherapy on the animals infected with Paragonimus westermani or P. Molecular characterization of the North American lung fluke Paragonimus kellicotti in Missouri and its development in Mongolian gerbils. The ribbon-like adult worm (so called tapeworm) resides in the intestines of carnivores or omnivores, causing intestinal taeniasis, whereas the cyst-like larva (metacestode) occurs in the internal organs of herbivores or omnivores, causing cysticercosis or neurocysticercosis (representing different forms of taeniasis). Indeed, as the only definitive host for these three species, human infection with the adult worms leads to intestinal parasitism, which is largely asymptomatic. A more recent description of cysticercosis was made by Johannes Udalric Rumler in 1555; however, the connection between tapeworm and cysticercosis was not established until the middle of the 19th century. Members of the family Taeniidae are characterized by their terrestrial life cycle, which includes three developmental stages (eggs, larva, and adult) and involves a carnivorous/omnivorous definitive host for adult worm, and a herbivorous/omnivorous intermediate host for larva (metacestode). Of the two wellrecognized genera (Echinococcus and Taenia) within the family Taeniidae, the genus Echinococcus is monophyletic, with a notable similarity in morphology, developmental processes, and genetic makeup, and is separated into nine species: E. On the other hand, the genus Taenia is a highly diverse, paraphyletic group with 45 species identified to date, including T. Recent examination of nuclear and mitochondrial genes enables further clarification of the genetic relationships among the representative members of the Taenia genus. Similar topologies were also observed in mitochondrial genomic analyses using 12 complete proteincoding genes. The scolex (holdfast organ) often possesses suckers (acetabula), rostellum, and spiny hooks. The strobila (up to 22 m long depending on the species) is composed of a chain of segments called proglottids, each of which contains a set of male and female reproductive organs (thus hermaphroditic). The reproductive organs are made up of tubular unbranched uterus (filled with eggs), ovary, genital pore, testes, and vitelline gland, with testes and ovary opening into a common genital pore located on the side. Being an acoelomate animal, the adult worm has no body cavity or digestive system, and relies entirely on its penetrable tegument to absorb nutrients. As body growth starts from the neck region, immature proglottids are found near the neck, mature proglottids in the middle, and gravid (oldest) proglottids at the posterior end. Being highly resistant to desiccation and sewage treatment, these eggs can survive on pastures for weeks. Upon ingestion by intermediate host, the eggs hatch and develop into infective cysticerci in selective organs. Typically, the life cycle begins when vegetation, feed, or water contaminated with taeniid eggs (or gravid proglottids) are consumed by a herbivorous/omnivorous intermediate host. Once inside, the embryonated eggs hatch into motile oncospheres within the duodenum and penetrate the intestinal wall, enter the bloodstream, and differentiate into metacestodes within 70 days (either cysticercoid, cysticercus, or a hydatid cyst) in selective internal organs (liver, lungs, brains, and muscles, etc. When raw or undercooked pork and beef containing the fluid-filled cysticerci are eaten by a carnivorous/omnivorous final host, the cyst (bladder) is digested away, the inverted scolex evaginates under stimuli from the digestive enzymes of the host, the scolex then embeds itself into the intestinal wall, and the neck buds off segments to form the strobila. In addition, humans may function as aberrant intermediate host after accidental ingestion of embryonated eggs, either through autoinfection or consumption of contaminated food, leading to neurocysticercosis, which demonstrates a predilection for brain tissue and other soft muscle tissues [8]. This parasite is found in places where beef is eaten, and is relatively common in Africa, the Middle East, the Philippines, Eastern Europe, and Latin America. While the adult worm is found in the small intestine of humans, pea-sized, fluid-filled cyst (cysticercus) is present in liver, serosa, and lungs of pigs and in the liver of cattle. Geographically, the parasite is essentially restricted to Taiwan, Korea, Indonesia, Nepal, Thailand, and China, in addition to Japan, the Philippines, and Vietnam [9,10]. In more severe cases (racemose neurocysticercosis), lesions as large as 6 cm in diameter, lobulated, and may occur in subarachnoid space and fissures. Clinical presentations may include severe headaches, dizziness, epilepsy, seizures, dementia, hypertension, lesions in the brain, blindness, tumorlike growths, hydrocephalus, paraplegy, meningitis, convulsions, and even death. Other rare clinical signs include ileus, pancreatitis, cholecystitis, and cholangitis. Nevertheless, in severe cases, damage and bleeding in the stomach and intestine may be observed. However, this approach lacks desired sensitivity and specificity given that the eggs from different Taenia species are morphologically indistinguishable [12]. In addition, application of, X-rays facilitates detection of calcified cysticerci in the subcutaneous and muscle tissues.

Discount fml forte 5 ml on-line
Likewise allergy symptoms year round order fml forte online now, when A/J mice were orally infected with spores of the Sterne strain,190 a systemic infection with commensal enteric organisms was seen. Interestingly, the effects were partially attenuated by the co administration of antibiotics. When viable bacteria were inoculated, the recruitment of high numbers of neutrophils masked the effect on other cells. The authors concluded that Hbl and Nhe cannot complement each other in spite of the coexpression of these factors. In contrast to murine gastrointestinal anthrax, which produced intestinal hemorrhage, edema, systemic dissemination, and death, mouse infection with B. Additionally, the infected mice showed a higher ratio of intestinal goblet cells and the presence of mononuclear cell infiltrates in the spleen. This study established relevant immune readouts to assess gastrointestinal infection with B. Evaluation of the composition of the indigenous gut flora and examination of whether spores and vegetative cells were able to persist in the gut were carried out. Experiments included administration of irradiated spores, untreated spores, heat-activated spores, and vegetative cells of a known-to-cause food-poisoning B. However, culture-dependent approaches did not reveal changes during the passage of B. Using in vitro assays and commercial kits for detection of toxins, no enterotoxins were detected in the intestinal tract. In addition, in those infectious conditions, only spores were able to resist the gastrointestinal passage. The use of in vitro and in vivo models allowed for establishing key steps and mechanisms involved in infection and foodborne outbreaks. Further insights were obtained with in vivo invertebrate and vertebrate models that elucidated many aspects of the pathogenesis in a more complex cellular context. The recent advances in the field of in vivo expression technologies herald further gains in our understanding of the control and treatment of foodborne pathologies associated with Bacillus spp. Rolny is a Research Scientist at the Biological Sciences Department (Facultad de Ciencias Exactas, Universidad Nacional de La Plata, Argentina), and Pablo F. Bacillus taxonomy in the genomic era finds phenotypes to be essential though often misleading. Bacillus anthracis, Bacillus cereus, and Bacillus thuringiensis-one species on the basis of genetic evidence. The Bacillus cereus group: novel aspects of population structure and genome dynamics. Pathogenic potential of Bacillus cereus strains as revealed by phenotypic analysis. Two cases of gastrointestinal anthrax with an unusual presentation from Kermanshah (western Iran). A case of pneumonia caused by Bacillus anthracis secondary to gastrointestinal anthrax. Inhalational, gastrointestinal, and cutaneous anthrax in children: a systematic review of cases: 1900 to 2005. Gastrointestinal anthrax after an animal-hide drumming event-New Hampshire and Massachusetts, 2009. Fatal pneumonia among metalworkers due to inhalation exposure to Bacillus cereus containing Bacillus anthracis toxin genes. Characterization of Bacillus cereus isolates associated with fatal pneumonias: strains are closely related to Bacillus anthracis and harbor B. Biodiversity of psychrotrophic bacteria of the Bacillus cereus group collected on farm and in egg product industry. Cutting edge: resistance to Bacillus anthracis infection mediated by a lethal toxin sensitive allele of Nalp1b/Nlrp1b. Capsule synthesis by Bacillus anthracis is required for dissemination in murine inhalation anthrax. Comparison of biological effect of the two different enterotoxin complexes isolated from three different strains of Bacillus cereus. Sphingomyelinase is part of the "enterotoxin complex" produced by Bacillus cereus. The cell envelope-bound metalloprotease (camelysin) from Bacillus cereus is a possible pathogenic factor. Identification of emetic toxin producing Bacillus cereus strains by a novel molecular assay. Evidence for non-ribosomal peptide synthetase production of cereulide (the emetic toxin) in Bacillus cereus. Disassembly of F-actin cytoskeleton after interaction of Bacillus cereus with fully differentiated human intestinal Caco-2 cells. Interaction between Bacillus cereus and cultured human enterocytes: effect of calcium, cell differentiation, and bacterial extracellular factors. Amylosin from Bacillus amyloliquefaciens, a K+ and Na+ channel-forming toxic peptide containing a polyene structure. The peptide toxin amylosin of Bacillus amyloliquefaciens from moisturedamaged buildings is immunotoxic, induces potassium efflux from mammalian cells, and has antimicrobial activity. Effect of Bacillus cereus exocellular factors on human intestinal epithelial cells. Rapid Ped-2E9 cell-based cytotoxicity analysis and genotyping of Bacillus species. Characterisation of a non-haemolytic enterotoxin complex from Bacillus cereus isolated after a foodborne outbreak. The Bacillus cereus Hbl and Nhe tripartite enterotoxin components assemble sequentially on the surface of target cells and are not interchangeable. Bacillus cereus enterotoxins act as major virulence factors and exhibit distinct cytotoxicity to different human cell lines. Putative virulence factor expression by clinical and food isolates of Bacillus spp. Inhibition of cytotoxicity by the Nhe cytotoxin of Bacillus cereus through the interaction of dodecyl maltoside with the NheB component. CytK toxin of Bacillus cereus forms pores in planar lipid bilayers and is cytotoxic to intestinal epithelia. Concerted action of sphingomyelinase and nonhemolytic enterotoxin in pathogenic Bacillus cereus. Bacillus cereus Nhe is a poreforming toxin with structural and functional properties similar to the ClyA (HlyE, SheA) family of haemolysins, able to induce osmotic lysis in epithelia. Sub-emetic toxicity of Bacillus cereus toxin cereulide on cultured human enterocytelike Caco-2 cells. Toxicological profile of cereulide, the Bacillus cereus emetic toxin, in functional assays with human, animal and bacterial cells. In vitro assay for human toxicity of cereulide, the emetic mitochondrial toxin produced by food poisoning Bacillus cereus. An improved method for detecting cytostatic toxin (emetic toxin) of Bacillus cereus and its application to food samples. Differential cytotoxicity of Bacillus anthracis and Bacillus cereus culture filtrates. Pathogenesis of human enterovirulent bacteria: lessons from cultured, fully differentiated human colon cancer cell lines. Enterotoxigenic profiles of food-poisoning and food-borne Bacillus cereus strains. Determination of the toxic potential of Bacillus cereus isolates by quantitative enterotoxin analyses. Monoclonal antibodies neutralize Bacillus cereus Nhe enterotoxin by inhibiting ordered binding of its three exoprotein components. Cytotoxicity of the Bacillus cereus Nhe enterotoxin requires specific binding order of its three exoprotein components.
