
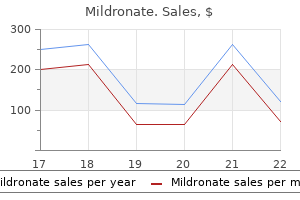
Buy mildronate 500mg fast delivery
In contrast to the spinal claudicatory syndrome medicine garden discount mildronate 500mg visa, warming up and progressive mobilization make the pain better. There is a notable absence of systemic symptoms such as fatigue, malaise, or fever, and, more importantly, there are limited or no features of radicular compression. Some patients complain of vague and intermittent pains in the upper or posterior legs, but sciatica is not a component and the straight-leg raising tests do not elicit pain. The sitting posi tion is usually comfortable, although stiffness and discom fort are accentuated when the erect posture is resumed. The usual clinical features are intractable low back and leg pain and paresthesia, all positionally sensitive, in combination with neurologic abnormalities referable to lumbar spinal roots. In our few patients, multiple previ ous myelograms with lipid contrast agent (a problem of the past), disc rupture, operative procedures, infections, and subarachnoid bleeding have been causal. Some cases have followed spinal anesthesia and even epidural anes thesia by a period of months or years. The presumption is that the dura had been breached, and often, there were clinical signs of aseptic meningitis soon after the proce dure. In the absence of such an acute reaction, the later diagnosis of arachnoiditis rests on less-certain grounds. Lysis of adhesions under an operating microscope and administration of intrathecal steroids have been of limited value, although some experienced surgeons claim otherwise. Epidural injection of steroids is occasionally helpful according to some of our orthopedic surgeon colleagues. In the typical instance, osteoarthritic degeneration of the facet joint gives rise to a focal parasagittal lumbar back pain, with tenderness over the joint. The pain can be severe, worse at night, and prevent sleep if no comfortable position can be found. The diagnosis is confirmed when the pain is relieved for a vari able period by injection of the joint with local anesthetic. Often one is uncertain whether it was the analgesic effect on the joint or the infiltration of the region around the nerve root that relieved the pain. Two controlled studies have provided evidence of the inefficacy, both in the short and long term, of corticosteroid injections into the facet joints (Carette et al, 1991; Lilius et al). Notwithstanding these reports, we have found the injec tion of analgesics and steroids in and around the facet to be a useful temporizing measure in some patients. Some patients have discovered that they may obtain temporary relief from facet pain by forcefully twisting or stretching the back and creating an audible pop at the affected joint, comparable to chiropractic manipulation. Over time, they acquire a laxity of the supporting structures of the joint, which may actually perpetuate the problem. If the diagnosis is established by local injection, pain centers offer radiofrequency ablation of the small recur rent sensory nerves that innervate the j oint as a means of permanent relief. Some writers have used the term facet syndrome to describe a painful state from facetal hypertrophy that gives rise to a lumbar monoradiculopathy indistinguish able from that caused by a ruptured disc or spondylosis. At operation, the spinal root is compressed against the floor of the intervertebral canal by overgrowth of an infe rior or superior facet. Foraminotomy and facetectomy, after exploration of the root from the dural sac to the pedicle, have relieved the pain in many operated cases. At first, the symptoms are vague (tired back, "catches" up and down the back, sore back), and the diagnosis may be overlooked for many years. Although the pain is recurrent, limitation of move ment is constant and progressive and comes to dominate the clinical picture. Early in the course of disease there is only "morning stiffness" or an increase in stiffness after periods of inactivity similar to lumbar osteoarthritis but unusual for the affected age group. In advanced stages, a cauda equina compression syndrome may compli inflammatory reaction and proliferation of connective tissue (Matthews). Limitation of chest expansion, tender ness over the sternum, decreased motion and tendency to progressive flexion of the hips, and the characteristic immobility and flexion deformity of the spine ("poker spine") may be present early in the course of the disease. The radiologic hallmarks are destruction and sub sequent obliteration of the sacroiliac joints, followed by bony bridging of the vertebral bodies to produce the characteristic "bamboo spine. The term is also applied to thickening of the arachnoidal sheaths around roots (normal roots have essentially no epineurium). Axial T2-weighted image at the L3 vertebral level showing lateral displacement of nerve roots by acquired arachnoid cysts. The great risk in this disease is fracture dislocation of the spine from relatively minor trauma, particularly flexion extension injuries. Occasionally, ankylosing spondylitis is complicated by destructive vertebral lesions. This complication should be suspected whenever the pain returns after a period of quiescence or becomes localized. The cause of these lesions is not known, but they may represent a response to nonunion of fractures, taking the form of an excessive production of fibrous inflammatory tissue. When it is severe, ankylosing spondylitis may involve both hips, greatly accentuating the back deformity and disability. Rheumatoid arthritis of the spine may be confined to the cervical region and creates risk of fracture-dislocation; it is considered further on in this chapter. The primary lesion may be small and asymp tomatic, and the first manifestation of the tumor may be pain in the back caused by metastatic deposits. The pain is constant and dull; it is often unrelieved by rest and is generally worse at night, interrupting sleep. A fracture of a vertebral body in an otherwise healthy young or middle-aged person should alert the physician to the possibility of an underlying metastasis. At the time of onset of the back pain, there may be no radiographic changes on plain radiographs; when such changes do appear, they usually take the form of destructive lesions in one or several vertebral bodies with little or no involvement of the disc space, even in the face of a com pression fracture. Infection of the vertebral col umn, osteomyelitis, is usu ally caused by staphylococci and less often by coliforms and mycobacteria. The patient complains of subacute or chronic pain in the back, which is exacerbated by move ment but not materially relieved by rest. Motion becomes limited, and there is percussion-induced tenderness over the spine in the involved segments and pain with jarring of the spine, as occurs when the heels strike the floor. A paravertebral mass is often found, indicating an abscess, which may, in the case of tuberculosis, drain spontaneously at sites quite remote from the vertebral column. However, if the posterior stomach w all is involved, particularly if there is retroperitoneal extension, the pain may be felt in the thoracic spine, centrally or to one s1de, or in both locations. The back pain tends to reflect the tempor charac teristics of the pain from the affected organ;. Diseases of the pancreas are apt to cause pain in the back, being more to the right of the spine if the head of the pancreas is involved and to the left if the body and tail are implicated. A tumor in the iliopsoas region often produces a urillateral lumbar ache with radia tion toward the groin and labia or testicle; there may also be signs of involvement of the upper lumbar pinal roo. An aneurysm of the abdominal aorta may mduce pam localized to an analogous region of the spine. The sudden appearance of lumbar pain in a patient receiving antic ag ulants should arouse suspicion of retroperitoneal bleedmg; this pain may also be referred to the groin. Infl ammatory diseases and neoplasms of the colon cause pain that may be felt in the lower abdomen, the In the postoperative setting or following trauma, a disc infec tion can occur by direct microbial seeding. It should be remembered that the intervertebral disc is an avascular structure, and therefore blood-borne pathogens first infect the bone and then secondarily spread to the adjacent disc. This is not the case in the neonatal period when the discs are directly perfused, for which reason neonates are sub ject to hematogenously seeded disci tis. We have also encountered a number of patients with bacterial endocarditis who complained of severe midline thoracic and lumbar back pain but had no evident infec tion of the spine. Tuberculous spinal infection and the resultant kyphotic deformity (Pott disease) represent a special condition that is common in developing countries (see Chaps. Special emphasis is placed Spinal Epidural Abscess on this condition, which usually necessitates urgent sur gical treatment. Most often this is caused by staphylococcal infection, which is carried in the bloodstream from a septic focus. Another important avenue of infection is the intravenous self-administration of drugs and use of contaminated needles. Rarely, the infection is introduced in the course of a lumbar puncture, epidural injection, or laminectomy for disc excision.
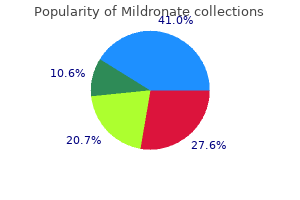
Buy mildronate us
They compared the results of ten sor imaging to a patient who had been in a minimally conscious state for 6 years without improvement and to 20 normal individuals treatment dvt purchase 250 mg mildronate with amex. Their findings are subject to several interpretations, but axonal growth in the parietal lobes offers a potential explanation for the few instances in which recovery from severe injury does occur. When combined with the findings of Laureys and colleagues, a case can be made for the posterior parietal regions as necessary for integrated consciousness. This further raise the possibility that certain islands of limited awareness may be dissociated from global brain function. Additional terms that have been used to describe this syndrome of preserved autonomic and respiratory function without cognition include apallic syndrome and neocortical death. It is difficult to predict which comatose patients will later fall permanently into the vegetative or minimally conscious categories (see Chap. Plum and Posner reported that of 45 patients with signs of the vegetative state at 1 week after onset, 13 had awakened and 5 of these had satisfactory outcomes. After being vegetative for close to 2 weeks, only 1 recovered to a level of moder ate disability; after 2 weeks, the prognosis was uniformly poor. As a rough guide to prognosis spe cifically in head injury, Braakman and colleagues found that among a large group of comatose patients, 59 per cent regained consciousness within 6 h, but of those in a vegetative state at 3 months, none became independent. At no time before 3 or 6 months was it possible to distin guish patients who would remain in a vegetative state from those who would die. Further comments regarding recovery are made in the next section on the minimally conscious state. Adams and coworkers have proposed that this reflects differences in the state of thalamic neurons in the two situations. They suggested that after acute hypoxia, neurons subjected to ischemic necrosis are liable to be permanently lost; by contrast, in trauma, the loss of thalamic neurons is more frequently secondary to transsynaptic degeneration fol lowing diffuse axonal injury, allowing a greater potential for recovery. Here, there is pres ervation of the ability to carry out basic motor behaviors that demonstrate a degree of awareness, at least at some times. The minimally conscious state is found as either a transitional or permanent condition and is sometimes difficult to separate from akinetic mutism discussed fur ther on. The causes and pathologic changes underlying the minimally conscious state are identical to those of the vegetative state, including the frequent finding of tha lamic and multiple cerebral lesions, and the distinction between them is one of degree. It is useful to maintain a critical view of reports of remarkable recuperation after months or years of pro longed coma or the vegetative state. When the details of such cases become known, it is evident that recovery might reasonably have been expected. There are, how ever, numerous reported instances of partial recovery in patients-particularly children and young adults-who display vegetative features for several weeks or, as Andrews and Childs and Mercer describe, even several months after injury. Such observations cast doubt on unqualified claims of success with certain therapies, such as sensory stimulation. Nevertheless, the occur rence of very late recovery in adults must be acknowl edged (see Andrews; Higashi et al; and Rosenberg et al, 1977) and a relation of awakening to the recovery of connections to the parietal lobes has already been mentioned. Cases of improvement from the "minimally conscious state" are more plausible than those from the vegetative state. More recent reports, for example by Estraneo and colleagues and by Luate and coworkers, may be more instructive but still not entirely directive. Of course, the assignation of a poor prognosis by the application of these terms to an individual patient often leads to the withdrawal of care, and the self-fulfilling poor prognosis. This is a much discussed problem that has not been satisfactorily but it emphasizes that simply labeling patients with certain diagnoses has implications for accurately assessing the natural history of some diseases. Among the interesting recent therapeutic observa tions, one observation has come from Schiff and col leagues, who were able to improve function by stimulat ing the medial (interlaminar) thalamic nuclei through implanted electrodes in a patient who had been initially vegetative and made a natural transition to a minimally conscious state after traumatic brain injury. Longer peri ods of eye opening and increased responses to execute commands, such as bringing a cup to his mouth, were observed, including, for the first time since his injury, intelligible verbalization. The authors point out that this individual had preserved language cortex and connec tions between thalamus and cortex. It cannot go without comment that the degree of disability that families find acceptable varies greatly and leads to difficult decisions regarding the continuation of medical care. The knowledgeable, sympathetic, and flex ible physician is in the best position to offer perspective and guide these matters as discussed at the end of this chapter. The term pseudocoma as a synonym for this state is best avoided, because it is used by some physicians to connote the unconsciousness of the hysteric or malingerer, the dissociative state, or catatonia. The locked-in syndrome is most often caused by a lesion of the ventral pons (basis pontis) as a result of occlusion of the basilar artery. Such an infarction spares both the somatosensory pathways, and the ascending neuronal systems responsible for arousal and wakefulness, as well as certain midbrain elements that allow the eyelids to be raised in wakefulness; the lesion essentially interrupts the corti. Aki netic Mutism One could logically refer to the locked-in state as akinetic mutism insofar as the patient is akinetic (motionless) and mute, but this is not the sense in which the term was orig inally used by Cairns and colleagues, who described a patient who appeared to be awake but was unresponsive (actually their patient was able to answer in whispered monosyllables). Following each of several drainings of a third ventricular cyst, the patient would become aware and responsive but would have no memory for any of the events that had taken place when she was in the akinetic mute state. This state of apparent vigilance in an imper ceptive and unresponsive patient has been referred to by French authors as coma vigile, but the same term has been applied to the vegetative state. The term akinetic mutism has been applied to yet another group of patients who are silent and inert as a result of bilateral lesions usually of the anterior parts of the frontal lobes, leaving intact the motor and sensory pathways; the patient is profoundly apathetic, lacking to an extreme degree the psychic drive or impulse to action (abulia). Catatonia the patient with catatonia appears unresponsive, in a state that simulates stupor, light coma, or akinetic mutism. There are no signs of structural brain disease, such as pupillary or reflex abnormalities. Peculiar motor mannerisms or repetitive motions, seen in a number of these patients, may give the impression of seizures; choreiform jerking has also been reported, but the latter sign should also suggest the possibility of seizure activity. Because there is considerable imprecision in the use of terms by which various states of reduced con sciousness are designated, the physician would be bet ter advised to supplement designations such as coma and akinetic mutism by simple descriptions indicating whether the patient appears awake or asleep, drowsy or alert, aware or unaware of his surroundings, and responsive or unresponsive to a variety of stimuli. This requires that the patient be observed more frequently or over a longer period than the several minutes usually devoted to this portion of the neurologic examination. The aforementioned findings of apparent limited respon siveness reflected with functional imaging only further emphasizes the care with which these clinical diagnoses should be determined. Mollaret and Goulon referred to this condition as coma depasse (a state beyond coma). A Harvard Medical School committee, in 1968, called it brain death and estab lished a set of clinical criteria by which it could be recog nized (Beecher et al). The concept that a person is dead if the brain is dead and that death of the brain may precede the cessation of cardiac function has posed a number of important ethical, legal, and social problems, as well as medical ones. All aspects of brain death have since been the subject of close study by several professional committees, which for the most part have confirmed the 1968 guidelines for determin ing that the brain is dead. The American Academy of neurology published guidelines on this subject in 1995 and affirmed them with some refinements in 2010. The monograph by Wijdicks is a thorough modern source on the subject of brain death and also addresses the subject from an international perspective. The philosophical underpinnings of the equating of brain death to death, giving it the same status as cessa tion of cardiorespiratory death, a utilitarian approach, are complex. The ethical and moral dimensions of brain death are complex and subject to differing interpretations in various societies, religions, and cultures. One justification for equating brain death with somatic death is the general inevitability of cardiorespiratory failure in patients who fulfill the standard criteria. This tenet has exceptions, the most striking of which is a well-studied case of 20-year survival in a boy who had meningitis reported by Reptinger and colleagues, and other cases of long survival have been described with varying degrees of documentation. The central considerations in the diagnosis of brain death are (1) absence of all cerebral functions; (2) absence of all brainstem functions, including spontaneous respi ration; and (3) irreversibility of the state. Following from the last of these criteria, it is necessary to demonstrate an irrefutable cause of the underlying catastrophic brain damage. In the diagnosis of brain death, the absence of cere bral function is demonstrated by the presence of deep coma and total lack of spontaneous movement and of motor and vocal responses to all visual, auditory, and cutaneous stimulation. Spinal reflexes may persist, and the toes often flex slowly in response to plantar stimula tion; but a well-developed Babinski sign is unusual in our experience (although its presence does not exclude the diagnosis of brain death). Extensor or flexor postur ing is seen from time to time as a transitional phenom enon just before or after brain death becomes evident, and the status of these movements in the diagnosis is ambiguous, but the physician should proceed cautiously in declaring a patient dead in the presence of posturing and should consider conducting the examination again at a later time.
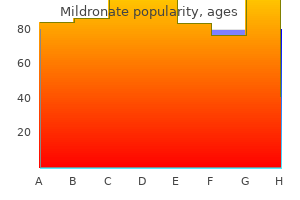
Buy mildronate 500mg free shipping
All the medical facts should be reviewed and the clinical and laboratory examinations repeated if some time has elapsed since they were last done medicine clip art purchase cheap mildronate. Tumors in the hilum of the lung or mediastinum; in the retropharyngeal, retroperitoneal, and paravertebral spaces; or in the uterus, testicle, kidney, or prostate pose a special difficulty in diagnosis, often being undetected for many months. More than once, we have seen a patient for months before a kidney or pancreatic tumor became apparent. Neurofibroma causing pain in an unusual site, such as one side of the rectum or vagina, is another type of tumor that may defy diagnosis for a long time. Truly neurogenic pain is almost invariably accompanied by alterations in cutaneous sensation and other neurologic signs, the finding of which facilitates diagnosis; however, the appearance of the neurologic signs may be delayed for example, in brachial neuritis. Because of the complexity and difficulty in diagnosis and treatment of chronic pain, most medical centers have found it advisable to establish pain clinics. Here a staff of internists, anesthesiologists, neurologists, neurosur geons, and psychiatrists can review each patient in terms of drug dependence, neurologic disease, and psychiatric problems. Intractable pain may also be the leading symptom of both somatization and conversion reactions. Experienced physicians are familiar with the patient who has under gone multiple surgical procedures to address painful complaints (so-called Briquet disease). The question of ruptured disc is often raised, and laminectomy and spinal fusion may be performed (sometimes more than once) on the basis of dubious radiologic findings. Long delay in the settlement of litigation, allegedly to determine the seriousness of the injury, only enhances the symptoms and prolongs the disability. The medical and legal professions have no certain approach to such problems and often work at cross-purposes. We have found that a frank, objective appraisal of the injury, an assessment of any psychiatric problem, and encouragement to settle the legal claims as quickly as possible work in the best interests of all con cerned. The possibility of drug addiction as a motivation for visiting the physician and reporting severe pain should be addressed. It is impossible to assess pain in addicted individuals, for their complaints are woven into their need for medication. Temperament and mood should be evaluated carefully; the physician must remember that the depressed patient often denies feeling dysphoric and may even occasionally smile. Under the title of of narcotics may be required early in the course of ill ness-for example, to treat the pain of visceral and bone cancer. The same measured strategy is appropriate in the treatment of neuropathic pain and of pain of unclear origin except that one generally stops short of ablative procedures that irrevocably damage nerves or parts of the central nervous system. The field of pain relief has been changed by the intro duction of analgesic procedures that block nerves, alter neural conduction, or administer conventional medica tions in new ways. These have become the province of pain clinics and hospital pain services usually led by departments of anesthesiology. In addition, a number of special procedures or unique medications are highly effective for pain relief but are unique to specific situa tions. These include certain forms of headache and limb pain (temporal arteritis and polymyalgia rheumatica treated with corticosteroids, or migraine relief with "trip tan" drugs); trigeminal neuralgia, which may be relieved by microvascular decompression of a branch of the basi lar artery or by controlled damage of the gasserian gan glion; and painful dystonic disorders that are relieved by the inj ection of botulinum toxin. Special procedures that have been devised to treat various forms of spinal back pain fall into the same category. The following discussion provides some guidance for the physician who is asked to undertake or participate in the treatment of chronic pain or of neuropathic pain. When pinched on the affected side, the patient, after a delay, became agitated, moaned, and seemed distressed but made no effort to fend off the painful stimulus with the other hand or to withdraw from it. In contrast, if the good side was pinched, the patient reacted normally and moved the normal hand at once to the site of the stimulus to remove it. The motor responses seemed no longer to be guided by sensory information from one side of the body. There are also two varieties of rare individuals who from birth are totally indifferent to pain coupled with anhidrosis ("congenital insensitivity to pain") or are incapable of feeling pain ("universal analgesia"). The former have been found by Indo and colleagues to have a mutation in the a neural tyrosine kinase receptor, a nerve growth factor receptor; those in the second group suffer from either a congenital lack of pain neurons in dorsal root ganglia, or to a mutation in the sodium chan nel discussed earlier. A similar loss of pain sensibility is encountered in the Riley-Day syndrome (congenital dys autonomia, see Chap. The analgesic effects of these types of drugs are additive, which is not the case when narcotics are com bined with diazepam or phenothiazine. Antidepressants and antiepileptic drugs, as discussed further on, may have a beneficial effect on pain even in the absence of overt depression. This is true particularly in cases of neuropathic pain (painful polyneuropathy and some types of radicular pain). Should the foregoing measures prove to be ineffec tive, one must tum to narcotic agents. Methadone and levorphanol are sometimes useful drugs with which to begin, because of their effectiveness by mouth and the relatively slow development of tolerance. Some pain clinics prefer the use of shorter-acting drugs such as oxycodone, given more frequently through the day. The oral route should be used whenever possible, as it is more comfortable for the patient than the parenteral route. Also, the oral route is associated with fewer side effects except for nausea and vomiting, which tend to be worse than with parenteral administration. Should the latter become necessary, one must be aware of the ratios of oral-to-parenteral dosages required to produce rare and unusual condition wherein the patient, although capable of distinguishing the different types of pain stimuli from one another and from touch, is said to make none of the usual emotional, motor, or verbal responses to pain. The patient seems totally unaware of the pain ful or hurtful nature of stimuli delivered to any part of the body, whether on one side or the other. The current interpretation of asymbolia for pain is that it represents a particular type of agnosia (analgognosia) or apractagno sia (see Chap. Pre-frontal lobe lesions from stroke, trauma, tumor, or in former times frontal lobotomy, can produce a version of this syndrome. Initially, of course, attention is directed to the underlying disease with the idea of eliminating the source of the pain by appropriate medi cal, surgical, or radiotherapeutic measures. When the primary disease is not treatable, the physician should, if time and the circumstances permit, attempt to use the milder measures for pain relief first-for example, non narcotic analgesics and antidepressants or anti-epileptic drugs before resorting to narcotics, local nerve blocks or contemplating surgical approaches for pain relief. Can be used intramuscularly Fewer gastrointestinal or platelet effects than aspirin Gastrointestinal side effects common Potent nonnarcotic with similar side effects but less respiratory depression Nausea common Usually available combined with acetaminophen or aspirin Oral slow-release preparation Shorter acting than morphine sulfate Longer acting than morphine sulfate; absorbed well orally Delayed sedation because of long half-life Poorly absorbed orally; normeperidine is a toxic metabolite Parenteral and transcutaneous ("patch") use Side effects of drowsiness, ataxia, nystagmus Codeine Oxycodone Morphine Morphine, sustained release Hydromorphone Levorphanol Methadone Meperidine Fentanyl Antiepileptic and related drugs 30-60 10 q4h 1-2 q4h 2 q6-8h 10 q6-8h 25 to 100 100 200-300 300-2,700 25-100 150-200 q4h 5-10 q4-6h 60 q4h 90 q12h 2-4 q4h 4 q6-8h 20 q6-8h 300 q4h apply q72h q6-8h q6h q8h q8h q4-6h 10-25). Lg Phenytoin Carbamazepine Gabapentin Pregabalin Special Agents Mexiletine Ketarnine Heart block Dysphoria, confusion equivalent analgesia. If oral medication fails to control the pain, the par enteral administration of codeine or more potent opioids becomes necessary. One may begin with methadone, dihydromorphine (Dilaudid), or levorphanol, given at intervals of 4 to end, the need to use larger doses. Most physicians now realize that the fear of creating narcotic dependence and the expected phenomenon of increasing tolerance must be balanced against the overriding need to relieve pain. The most pernicious aspect of addiction, that of compul sive drug-seeking behavior with its attendant sociopathic behaviors, occurs only rarely in this setting and usually in patients with a previous history of addiction or alco holism, with depression as the primary problem, or with certain characterologic disorders that have been loosely referred to as "addiction proneness. Guidelines for the use of orally and parenterally administered opioids for cancer-related pain are contained in the article of Cherny and Foley and in the publication of the U. Department of Health and Human Services, which unfortunately, is no longer easily obtained. The approach outlined above conforms to our under standing about pain-control mechanisms. Morphine and meperidine 6 h because of their relatively long dura tion of action (particularly in comparison to meperi dine). Alternatively, one may first resort to the use of transdermal patches of drugs such as fentanyl, which provide relief for 24 to 72 h and which we have found particularly useful in the treatment of pain from brachial or lumbosacral plexus invasion by tumor and of painful neuropathies such as those caused by diabetes and sys temic amyloidosis. Should long-continued injections of opiates become necessary, the optimal dose for the relief of pain should be established and the drug then given at regular inter vals around the clock, rather than "as needed. For many years it was widely believed that the drug should be given in the smallest possible doses, spaced as far apart as possible, and repeated only when severe pain reasserted itself. Opioids not only act directly on the central pain-conducting sensory sys tems but also exert a powerful action on the affective component of pain. If these are not feasible, opioid medications are required and are effective, but they must be prescribed in adequate doses.
Purchase genuine mildronate online
In this way medicine used to stop contractions cheap mildronate american express, localization may be viewed as the product of genetic patterns of structure, which mature during development, and their synaptic formations, which per mit the development of complex circuits during lifelong learning and experience. It is worthwhile to point out that these broadened concepts of cerebral function, which apply to all mental activities, contradicts both the historical notion that there is a functional equivalence of all cerebral regions and also the more recently developed one that assumes strict localization of any given activity. From these remarks, it follows that subdivision of the cerebrum into frontal, temporal, parietal, and occipital lobes is somewhat of an abstraction in terms of land marks and cerebral function. Some of these delineations were made long before our first glimmer of know ledge about the function of the cerebrum. Even when neuro histologists began parceling the neocortex, they found that their areas did not fall neatly within zones bounded by sulci and fissures. Therefore, when the terms frontal, parietal, temporal, and occipital are used, it is largely to provide the clinician with familiar and manageable ana tomic landmarks for localization. Invariably, an ensemble of areas, a "network" of the variety described earlier, is activated to perform even seemingly simple tasks such as recalling a name, visualizing or identifying an object, or carrying out a commanded task. The fact that multiple areas of the cortex are entrained may seem at odds with the classic view of lesional neurology, but as already stated, the dis crepancy is one of epistemology in that normal function does not equate with abnormal function as exposed by a focal lesion. A lesion in the cerebrum merely exposes the site at which damage results in the greatest loss of that particular function but does not reveal the much wider area that is essential for the full normal operation of that function. Imaging studies similarly demonstrate that cer tain regions of the cortex are necessary to fully conduct particular behaviors, but they are not sufficient for their enactment. Although this parceling was severely criticized by Bailey and von Bonin (and the data upon which Brodmann based his system were never published), it is still used by physiologists and clinicians, who find that the Brodmann areas do indeed approximate certain functional zones of the cerebral cor tex. Also, the cortex has been shown to differ in its various parts by virtue of connections with other areas of the cortex and with the thalamic nuclei and other lower centers. Hence, one must regard the cortex as a heterogeneous array of many anatomic systems, each with highly organized intercortical and dience phalic connections. Unfolded, it has a surface extent of about 4,000 cm2, about the size of a full sheet of newsprint (right and left pages). Contained in the cortex are many billions of neurons (estimated at 10 to 30 billion) and five times this number of support ing glial cells. Because nerve cells look alike and presumably function alike, the remarkable diversity in human intelligence, store of knowledge, and behavior must depend on the potential for almost infinite varia tions in neuronal interconnectivity. Most of the human cerebral cortex is phyloge netically recent, hence the term neocortex. Approximate distribution of functional zones on lateral (A) and medial (B) aspects of the cerebral cortex. These latter features distinguish the neocortex from the older and less uni form allocortex ("other cortex"), which comprises mainly the hippocampus and olfactory cortex. Concerning the detailed histology of the neocortex, six layers (lami nae) can be distinguished-from the pial surface to the underlying white matter they are as follows: the molecular (or plexiform), external granular, external pyramidal, internal granular, ganglionic (or internal pyramidal), and multiform (or fusiform) layers (illus trated in. Two cell types-relatively large pyramidal cells and smaller, more numerous rounded (granular) cells-predominate in the neocortex, and varia tions in its lamination are largely determined by variations in the size and density of these neuronal types. Many variations in lamination have been described by cortical mapmakers, but two main types of neocortex are recognized: (1) the homol:t pical cortex, in which the j six-layered arrangement is readily discerned, and (2) the heterotypical cortex, in which the layers are less distinct. The association cortex-the large areas (75 percent of the surface) that are not obviously committed to primary motor or sensory functions-is generally of this latter type. The precentral cortex (Brodmann areas 4 and 6, mainly motor region) is domi nated by pyramidal rather than granular cells, especially in layer V (hence the term agranular). Beyond these morphologic distinctions, the intrinsic organization of the neocortex follows a pattern elucidated by Lorente de N6. He described vertical chains of neu rons arranged in cylindrical modules or col umns, each containing 100 to 300 neurons and heavily interconnected up and down between cortical layers and to a lesser extent, horizontally. Their impulses are then transmitted by internuncial neurons (intemeurons) to adjacent superficial and deep layers and then to appropriate efferent neurons in layer V. Neurons of layer V (projection efferents) send axons to subcortical structures and the spinal cord. In the macaque brain, each pyramidal neuron in layer V has about 60,000 synapses, and one afferent axon may syn apse with dendrites of as many as 5,000 neurons; these figures convey some idea of the wealth and complexity of cortical connections. These columnar ensembles of neurons, on both the sensory and motor sides, function as the elementary working units of the cortex. Whereas certain regions of the cerebrum are com mitted to special perceptual, motor, sensory, mnemonic, and linguistic activities, the underlying intricacy of the anatomy and psychophysical mechanisms in each region are just beginning to be envisioned. The lateral geniculate occipital organization in relation to vision and recognition of form, stemming from the work of Hubel and Wiesel, may be taken as an example. The six basic cell layers are indi cated on the left, and the fiber layers on the right (see text). Lying between the main unimodal receptive areas for vision, audition, and somesthetic perception are zones of integration called heteromodal cortices. Here neurons respond to more than one sensory modality or neurons responsive to one sense are inter spersed with neurons responsive to another. The integration of cortical with subcortical structures is reflected in volitional or commanded movements. A simple movement of the hand, for example, requires acti vation of the premotor cortex (also called accessory motor cortex), which projects to the striatum and cerebellum and back to the motor cortex via a complex thalamic circuitry before the direct and indirect corticospinal pathways can activate certain combinations of spinal motor neurons, as described in Chaps. Interregional connections of the cerebrum are required for all natural sensorimotor functions; moreover, as indi cated above, their destruction disinhibits or "releases" other areas. Thus, destruction of the premotor areas, leaving the precentral and parietal lobes intact, results in release of sensorimotor automatisms such as groping, grasping, and sucking. Temporal lesions lead to a visually activated reaction to every observed object and its oral exploration, and limbic sexual mechanisms are rendered hyperactive. Extensive white matter lesions may virtually isolate certain cortical zones and result in a functional state that is the equiva lent of destruction of the overlying cortical region. An example is the isolation of the perisylvian language areas from the rest of the cortex, as occurs with anoxic-ischemic infarction of border zones between major cerebral arteries (see "Disconnection Syndromes" further on). Four fundamental types of cerebral cortex and their clistribution in the cerebrum. The primary visual cortex has a preponderance of small neurons; hence, it was historically called "granular. The visual pattern is transferred from the visual cortex and association areas to the angular gyrus, which arouses the auditory pattern in the Wernicke area. The auditory pattern is transmitted to the Broca area through the arcuate fasciculus, where the articulatory form is aroused and transferred to the contiguous face area of the motor cortex. With destruction of the left visual cortex and splenium (or intervening white matter), the words perceived in the right visual cortex cannot cross over to the language areas and the patient cannot read. They are not, strictly speaking, parts of the motor cortex in the sense that electrical stimulation evokes no direct movement (the prefrontal cortex is said to be inexcitable). Yet these areas are involved in the initiation of planned action and executive control of all mental operations, including emotional expression. The frontal agranular cortex (areas 4 and 6) and more specifically, pyramidal cells of layer V of the pre- and postcentral convolutions provide most of the cerebral efferent motor system that forms the pyramidal, or cor ticospinal, tract. In addition, there are several parallel fiber systems that pass from frontal cortex to the caudate and putamen, subthalamic and red nuclei, brainstem reticular forma tion, substantia nigra, and inferior olive, as well as to the ventrolateral, mediodorsal, and dorsolateral nuclei of the thalamus. Areas 8 and 6 are connected with the ocular and other brainstem motor nuclei and with identical areas of the other cerebral hemisphere through the corpus callosum. A tract, the ironto-occipital fasciculus, con nects the frontal with the occipital lobe and the uncinate bundle connects the orbital part of the frontal lobe with the temporal lobe. The granular frontal cortex has a rich system of con nections both with lower levels of the brain (medial and ventral nuclei and pulvinar of the thalamus) and with than in any other primate (9 percent in the macaque). Several systems of neurons are located here, and they subserve different functions. The supplementary motor cortex, a portion of area 6, shares most of these connections. As pointed out in earlier chap ters, all motor activity requires sensory guidance, and this comes from the somesthetic, visual, and auditory cortices and from the cerebellum via the ventral tier of thalamic nuclei. Area 44 of the dominant hemisphere (Broca area) and the contiguous part of area 4 are "cen ters" of motor speech and related functions of the lips, tongue, larynx, and pharynx. Left-sided lesions cause a distinctive articulatory and language syndrome, and bilateral lesions in these areas cause paralysis of articula tion, phonation, and deglutition. The medial-orbital gyri and anterior parts of the cingulate and insular gyri, which are the frontal components of the limbic system, take part in the control of respiration, blood pressure, peristalsis, and other autonomic functions. As to its limbic connec tions, the frontal lobe is unique among cerebrocortical areas in that electrical stimulation of the orbitofrontal cortex and cingulate gyrus has manifest effects on respi ratory, circulatory, and other vegetative functions. These parts of the frontal cortex also receive major afferent projections from other parts of the limbic system, pre sumably to mediate the emotional responses to sensory experiences; they, in project to other parts of the limbic and paralirnbic cortices (hippocampus, parahip pocampus, anterior pole of the temporal lobe), amygdala, and midbrain reticular formation.
Cheap 250 mg mildronate with mastercard
The differential effect of drugs on tremor and bradykinesia suggest that they must have separate mechanisms medicine mountain scout ranch buy mildronate master card. A lesion of the nucleus interpositus or den tate nucleus causes an ipsilateral tremor of ataxic type, as one might expect, associated with other manifestations of cerebellar ataxia. In addition, such a lesion gives rise to a "simple tremor," which is the term that Carpenter applied to a "resting" or parkinsonian tremor. He found that the latter was most prominent during the early postoperative period and was less enduring than ataxic tremor. Characteristic athetoid-dystonic deformities of the hand in a patient with tardive dyskinesia. The use of drugs in treating this movement disorder has met with variable success. Selective injection of the palatal muscles with botulinum toxin, while technically demanding, affords modest relief; it is particularly helpful in eliminating the annoying ear clicking. Montalban and colleagues, came to a similar conclusion, namely that unilateral asterixis is usually attributable to an acute thalamic stroke on the contralateral side, but there was an interesting variety of other localizations including the frontal lobe (anterior cerebral artery infarc tion), midbrain, and cerebellum in a few cases each. Our experience is limited to those arising from thalamic and overlying parietal lesions. Many drugs may unmask uni lateral asterixis that has its basis in an underlying lesion of the anterior thalamus. Myoclonus specifies the very rapid, shock-like contractions of a group of muscles, irregular in rhythm and amplitude, and, with few exceptions, asynchronous and asymmetrical in distribution. If such contractions occur singly or are repeated in a restricted group of muscles, such as those of an arm or leg, the phe nomenon is termed segmental myoclonus, whereas wide spread, lightning-like, arrhythmic repeated contractions are referred to as polymyoclonus. The discussion that fol lows makes evident that each of the three phenomena has a distinctive pathophysiology and clinical implications. It is most easily elicited by forcefully dorsiflexing the ankle; a series of rhythmic jerks of small to moderate amplitude result. A common and benign example of myoclonus, famil iar to many persons, is the "sleep-start" that consists of a jerking of the body, particularly the torso, while falling asleep or occasionally, just prior to waking (see Chap. This movement will be vigorous enough to cause tongue biting and be mistaken for a convulsion. Epilepsia partialis continua is a special type of rhyth mic epileptic activity in which one group of muscles usually of the face, arm, or leg-is continuously (day and night) involved in a series of rhythmic monophasic con tractions. The disorder appears to be cerebral in origin, but in most cases its precise anatomic and physiologic basis cannot be determined (see Chap. It consists of arrhythmic lapses of sustained posture that allow gravity or the inherent elasticity of muscles to produce a movement, which the patient then corrects, sometimes with overshoot. This confirmed that asterixis differs physi ologically from both tremor and myoclonus, with which it was formerly confused; it has incorrectly been referred to as a "negative tremor. Flexion movements of the hands may then occur arrhythmically once or several times a minute. The same lapses in sus tained muscle contraction can be provoked in any muscle group-including, for example, the protruded tongue, the closed eyelids, or the flexed trunk muscles. Sometimes, asterixis can be elicited best by asking the patient to place his hand flat on a table and raise the index finger. This sign was first observed in patients with hepatic encephalopathy but was later noted with hypercapnia, uremia, and other metabolic and toxic encephalopathies. Asterixis may also be evoked by phenytoin and other anticonvulsants, usually indicating that these drugs are present in excessive concentrations. Similar rapid lapsing movements of the head or arms sometimes appear dur ing drowsiness in normal persons ("nodding off"). Unilateral asterixis occurs in an arm and leg on the side opposite an anterior thalamic infarction or small hemorrhage, after stereotaxic thalamotomy; and with an upper midbrain lesion, usually as a transient phenom enon after stroke. One-sided or focal myoclonic jerks are the dominant feature of a particular form of childhood epilepsy-so-called benign epilepsy with rolandic spikes (Chap. Myoclonus may be associated with atypi cal petit mal and akinetic seizures in the Lennox-Gastaut syndrome (absence or petit mal variants); the patient often falls during the brief lapse of postural mechanisms that follows a single myoclonic contraction. These types of special "myoclonic epilepsies" are discussed further below and in Chap. Focal simple myoclonus is also one of the notable fea tures of degenerative neurologic conditions, particularly corticobasal ganglionic degeneration; it is generally seen in a limb that is made rigid by this process. As a result, an arm may suddenly flex, the head may jerk backward or forward, or the trunk may curve or straighten. In this and other forms of myoclonus, the muscle contraction is brief (20 to 50 ms)-i. The speed of the myoclonic contraction is the same whether it involves a part of a muscle, a whole muscle, or a group of muscles. Some of the patients register little complaint, accept ing the constant intrusions of motor activity with sto icism; they generally lead relatively normal, active lives. Occasionally there is hint of a mild cer ebellar ataxia and, in one family studied by R. Adams, essential tremor was present as well, both in family mem bers with polymyoclonus and in those without. Both the tremor and myoclonus were dramatically suppressed by the ingestion of alcohol. In a Mayo Clinic series reported by Aigner and Mulder, 19 of 94 cases of polymyoclonus were of this "essential" type. Several of the sleep-related syndromes that involve repetitive leg movements include an element of myoc lonus. In a few patients, mainly older ones with severe "restless legs syndrome," the myoclonus and dyskinesias may become troublesome in the daytime as well. It was probably in the course of this description that the term myoclonus was used for the first time. Muscles were involved diffusely, particularly those of the lower face and proximal segments of the limbs, and the myoclonus persisted for many years, being absent only during sleep. Over the years, the term paramyoclonus multiplex, or polymyoclonus has been applied to all varieties of myo clonic disorder (and other motor phenomena as well), to the point where it has nearly lost its specific connotation. Polymyoclonus may occur in pure or "essential" form as a benign, often familial, nonprogressive disease or as part of a more complex progressive syndrome that may prove disabling and fatal. More importantly, there are several acquired forms that are associated with various neurologic diseases as discussed below. The myoclonus takes the form of irregular twitches of one or another part of the body, involving groups of muscles, single muscles, or even a Myoclonic epilepsy constitutes an important syndrome of multiple etiologies. A relatively benign idiopathic form, juvenile myoclonic epilepsy, has been mentioned and is discussed extensively in Chap. A more seri ous type of myoclonic epilepsy, which in the beginning may be marked by polymyoclonus as an isolated phe nomenon, is eventually associated with dementia and other signs of progressive neurologic disease (familial variety of Unverricht and Lundborg). An outstanding feature of the latter is a remarkable sensitivity of the myoclonus to stimuli of all sorts. If a limb is passively or actively displaced, the resulting myoclonic jerk may lead, through a series of progressively larger and more or less synchronous jerks, to a generalized convulsive seizure. In late childhood this type of stimulus-sensitive myoclonus is usually a manifestation of the juvenile form of lipid storage disease, which, in addition to myoclonus, is char acterized by seizures, retinal degeneration, dementia, rigidity, pseudobulbar paralysis, and, in the late stages, by quadriplegia in flexion. Another form of stimulus-sensitive (reflex) myoclo nus, inherited as an autosomal recessive trait, begins in late childhood or adolescence and is associated with neu ronal inclusions (Lafora bodies thus Lafora-body disease) in the cerebral and cerebellar cortex and in brainstem nuclei. Unlike Lafora-body disease, the Baltic variety of myoclonic epilepsy has a favorable prognosis, particularly if the seizures are treated with valproic acid. Under the title of cherry-red-spot myoclonus syn drome, Rapin and associates have drawn attention to a familial (autosomal recessive) form of diffuse, incapaci tating intention myoclonus associated with visual loss and ataxia. The earliest sign is a cherry-red spot in the macula that may fade in the chronic stages of the illness. The specific enzyme defect appears to be a deficiency of lysosomal alpha-neu roaminidase (sialidase), resulting in the excretion of large amounts of sialylated oligosaccharides in the urine. This has been referred to as type 1 sialidosis to distinguish it from a second type, in which patients are of short stature (as a result of chondrodystrophy) and often have a defi ciency of beta-galactosidase in tissues and body fluids. In patients with sialidosis, a mucopolysaccharide-like material is stored in liver cells, but neurons show only a nonspecific accumulation of lipofuscin. A similar clinical syndrome of myoclonic epilepsy is seen in a variant form of neuroaxonal dystrophy and in the late childhood-early adult neuronopathic form of Gaucher disease, in which it is associated with supranuclear gaze palsies and cerebel lar ataxia (Chap.
Cheap mildronate 500 mg on line
The superficial temporal and other scalp arteries are frequently thickened and tender and with out pulsation treatment spinal stenosis discount mildronate 250mg online. Jaw claudication and ischemic nodules on the scalp, with ulceration of the overlying skin, have been described in severe cases. Many of the patients feel generally unwell and have lost weight; some have a low-grade fever and anemia. As many as 50 percent of patients have generalized ach 55, "Polymyalgia ing of proximal limb muscles, reflecting the presence of polymyalgia rheumatica (see Chap. This may be preceded by several episodes of amaurosis fugax (transient monocular blindness). Ophthalmoplegia may also occur but is less frequent, and its cause, whether neural or muscular, is not settled. Masticatory claudication is a specific but not particularly sensitive symptom of cranial arteritis. For this reason, the earliest suspicion of cra nial arteritis should lead to the administration of corti costeroids and then to biopsy of the appropriate scalp artery. Microscopic examination discloses an intense granulomatous or "giant cell" arteritis. Arteriography of the external carotid artery branches is probably the most sensitive test but is seldom used, because of its relatively higher risk. Ultrasonographic examination of the temporal arteries may display a dark halo and irregularly thickened vessel walls. This technique has not yet been incorporated into the routine evaluation because its sensitivity has not been established; our own experience suggests that it may miss cases, but it could be useful in choosing the site for biopsy of the temporal artery. Assuming the supine posi tion almost immediately relieves the cranial pain and eliminates vomiting, but a blood-patch procedure may be required in persistent cases. In a limited number of cases, success has been obtained by the use of intravenous caffeine injections. In practice, factors such as sleep deprivation are at least as important in triggering perimenstrual headaches. The headache can be expected to improve within a day or two of beginning treatment; failure to do so brings the diag nosis into question. The management of migraine during pregnancy poses special problems because one wants to restrict exposure of the fetus to medications. It can be stated that beta-adrenergic compounds and tricyclic antide pressants may be used safely in the small proportion of women whose headaches persist or intensify during pregnancy. From a limited registry of patients who were given sumatriptan during pregnancy, and from several small trials s ummarized by Fox and colleagues, no tera togenic effects or adverse effects on pregnancy arose, but serotonin agonist drugs should be used advisedly until their safety is further confirmed. For those women who use antiepileptic drugs as a means of headache preven tion, it is recommended that the drugs be stopped prior to pregnancy or as soon as it is known that pregnancy has begun. Most typical is a feeling of occipital pressure that is greatly worsened by lying down, but many patients have-in addition, or only-headaches of migraine or tension type. Indeed, some of them respond to medica tions such as propranolol and ergot compounds. None of the proposed mechanisms for pain in pseudotumor cerebri seems to be adequate as an explanation, particu larly the idea that cerebral vessels are displaced or com pressed, as neither has been demonstrated. It is worth noting that facial pain may also be a feature of the illness, albeit rare. Chapter 30 has a more complete description of the clinical features and treatment. After successful treatment for pseudotumor, some patients have persistent headaches that have the flavor of migraine. Pain is usually felt in the front of the head, sometimes occipitally, and may be unilateral or bilateral. As a rule, it follows the initiating action within a second or two and lasts a few seconds to a few minutes. The pain is often described as having a bursting quality and may be of such severity as to cause the patient to cradle his head in his hands, thereby simulating the headache of acute subarachnoid hemorrhage. Most often this syndrome is a benign idiopathic state that recurs over a period of several months to a year or two and then disappears. Bilateral jugular compression may induce an attack, possibly because of traction on the walls of large veins and dural sinuses. In a few instances, we have observed this type of headache after lumbar puncture or after a hemorrhage from an arteriovenous malformation. Patients with cough or strain headache will only occasionally be found to have serious intracranial disease; when present, it has been traced to lesions of the posterior fossa and foramen magnum, arteriovenous malformation, subdural hematoma, Chiari malformation, basilar impres sion, or tumor. Far more common, of course, are the temporal and maxillary pains that are caused by dental or sinus disease, which may also be worsened by coughing. All manner of headache has been attributed to Chiari type 1 malformation (with tonsils descended at least 3 mm below the lip of the foramen magnum) with little justifica tion. However, some instances of exertional and Valsalva induced suboccipital pain can be attributed to this disease. Some patients report radiating pain across the base of the neck and shoulders with straining and headache. In the survey by Pascual and colleagues of 50 patients with Chiari type 1 malformations, the incidence of migraine and tension-type headache was found to be appropriate to the population at large and only the degree of tonsil lar descent correlated with the presence of exertional headache. It follows that suboccipital decompressive operations should be undertaken only selectively. Athletes and runners in general seem to suffer exertional headaches quite often in our experience, and the episodes usually have migrainous features. Indomethacin is usually effective in controlling exer tional headaches; this has been confirmed in controlled trials. In a few of our patients, lumbar puncture appeared to immediately resolve the problem in some inexplicable way. The latter headaches were of such abruptness and severity as to suggest a ruptured aneurysm but the neurologic examination was negative in every instance, as was arteriography in 7 patients who were subjected to this procedure. In 18 patients who were followed for a period of 2 to 7 years, no other neurologic symptoms developed. Characteristically, the headache occurred on several consecutive occasions and then disappeared. Of course, so-called orgasmic headache is not always benign; a hypertensive hemorrhage, rupture of an aneurysm or vascular malformation, carotid artery dissection, or myocardial infarction may occur during the exertion of sexual intercourse. There are several reports regarding such pains as a "warning leak" of rupture and even reports suggesting that acute severe headaches occur as a consequence of unruptured aneurysms (although subsequent studies suggest that this is infrequent). It was in relation to an exceptional case of this nature that the term thunderclap was intro duced by Day and Raskin. Patients in our services have offered colorful descriptions, such as "being kicked in the back of the head. To this list we would add diffuse idiopathic arterial spasm (Call Fleming syndrome; see "Diffuse and Focal Cerebral Vasospasm" in Chap. Recurrent thunderclap pain may be particularly indicative of mul tifocal or diffuse vasospasm, as pointed out by Chen and colleagues, who found this vasculopathy in 39 percent of their patients with recurrent thunderclap pain. The diagnosis is clarified after lumbar puncture and cerebral imaging exclude bleeding and aneurysm, and the pain resolves in hours or less. Wijdicks and colleagues confirmed that thunderclap headache is usually a benign condition; among 71 patients followed for more than 3 years they found no serious cerebrovascular lesions. For this reason, these idiopathic thunderclap headaches have been presumed to be a form of migraine ("crash migraine"). This opinion is based in part on a history of preceding or of subsequent headaches and migrainous episodes in affected individuals; however, in our experi ence not all of such patients have had migraine in the past. E ryth rocyan otic Headache An intense, generalized, throbbing headache may occur in conjunction with flushing of the face and hands and numbness of the fingers (erythromelalgia). This condition, called erythrocyanotic, has been reported in a number of unusual settings: (1) in mastocytosis (infiltra tion of tissues by mast cells, which elaborate histamine, heparin, and serotonin); (2) with carcinoid tumors; (3) with serotonin-secreting tumors; (4) with some tumors of the pancreatic islets; and (5) with pheochromocytoma. Seventy-five percent of patients with pheochromocytoma reportedly have vascular-type headaches coincident with paroxysms of hypertension and release of catecholamines (Lance and Hinterberger) but the flushing phenomenon has been rare in our experience.
Buy 500 mg mildronate with amex
In walk ing medications may be administered in which of the following ways purchase mildronate master card, the knee is slightly flexed, and weight bearing on the painful leg is brief and cautious on the ball of the foot, giving a limp. The signs of more severe spinal root compression are impairment of sensation, loss or diminution of ten don reflexes, and muscle weakness, as summ a rized in Table 11-1. Generally, disc herniation compresses the root on one side, at the level just below the herniation (see below). In a few patients, foot drop (L5 root) or weakness of plantar flexion (Sl root) is a main feature of disc protrusion, and some of these patients have little associated pain. The reflex changes noted below have little relationship to the severity of the pain or sensory loss. Furthermore, compression of the fourth, or sometimes fifth, lumbar root may occur without any change in the tendon reflexes. Bilaterality of symptoms and signs is rare, as is sphincteric paralysis, but they occur with large central protrusions that compress the cauda equina. As emphasized earlier, herniations of the interverte bral lumbar discs occur most often between the fifth lum bar and first sacral vertebrae (compressing the traversing Sl or exiting L5 root;. Pain is elicited by the straight-leg raising test or one of its vari ants, and protective nocifensive reflexes come into play, limiting further elevation of the leg. Weakness, if present, involves the extensors of the big toe and foot and the foot invertors (a distinguishing feature of foot drop originating in pero neal nerve damage). The ankle j erk may be diminished (more often it is normal), but the knee jerk is hardly ever altered. With lesions of the first sacral root (51), the pain is felt in the midgluteal region, mid-posterior part of the thigh, posterior region of the calf to the heel, outer plantar sur face of the foot, and fourth and fifth toes. Mechanisms of compression of the fifth lumbar and first sacral roots by herniated lumbosacral discs. Paresthesia and sensory loss are mainly in the lower part of the leg and outer toes, and weakness, if present, involves the plantar flexor muscles of the foot and toes, abductors of the toes, and hamstring muscles. Walking on the toes is more difficult and uncomfortable than walking on the heels because of weakness of the plantar flexors. The less-frequent lesions of the third (L3) and fourth (L4) lumbar roots give rise to pain in the anterior part of the thigh and knee and anteromedial part of the leg (fourth lumbar), with corresponding sensory impair ment in these dermatomal distributions. Third lumbar (L3) motor root lesions may weaken the quadriceps, thigh adductor, and iliopsoas; lA root lesions weaken the anterior tibial innervated muscles, sometimes with a mild foot drop. First lumbar (Ll) root pain is pro jected to the groin, and L2, to the lateral hip. Some patients have a distinctive syndrome asso ciated with extreme lateral disc protrusions, particu larly those situated within the proximal portion of the intervertebral spinal foramina. Unremitting radicular pain without back pain and a tendency to worsen with extension of the back and torsion toward the side of the herniation are characteristic. Both of these configurations may confound clinical and radio logic diagnosis and make surgery more difficult. Rarer still, and often clinically obscure, are protru sions of Anomalies of the lumbosacral roots may lead to errors in localization (see descriptions by Postacchini et al). The combined rupture of two or more discs occurs occa sionally and complicates the clinical picture. When both the L5 and Sl roots are compressed by a large herniated disc, the signs of the Sl lesion usually predominate. Herniation may occur directly into the adjacent ver tebral body, giving rise to a Schmorl nodule. In such cases there are no signs of nerve root involvement although back pain may be present, sometimes recurrent and referred to the thigh. Trauma, particularly hard falls on the heels or buttocks, is an important caus ative factor. Deep boring spine pain; root pain circling the body or projected to the abdomen or thorax (some times simulating visceral disease); paresthesias below the level of the lesion; loss of sensation; both deep and superficial; and paraparesis or paraplegia are the usual clinical manifestations. Diagnosis When all components of the lumbar disc syndrome are present, the diagnosis can be made with reasonable confidence. Furthermore, the above descriptions of single root compression refer mainly to signs and symptoms of typical posterolat eral disc protrusion. Very large of neurological deficits, imaging generally need not be undertaken until the pain has persisted for several weeks (see Chou and colleagues). This, of course, may not be necessary if the pain is manageable and surgery is not contemplated (see further on). The posteriorly protruding disc material indents and elevates the anterior thecal sac and narrows the spinal canal. The disc space at this level is narrowed and the disc is less hyperintense than normal because of desiccation and the extruded component. Axial view showing the focal right paracentral posterior disc herniation (large arrow) protruding into the canal and compressing the traversing nerve root (the right can be seen laterally to the disc (small arrows). Loss or marked asymmetry of the H reflex is another useful indication of S1 radiculopa thy, but this simply corroborates the loss of an Achilles reflex. The finding of denervation potentials in the para spinal muscles (indicating root rather than peripheral nerve lesions) and in muscles that conform to a root dis tribution is also helpful, but again, some weeks must have elapsed from the onset of root pain for these findings to be present. An entirely normal study should lead to reconsideration of the diagnosis, particularly if surgery was planned for relief of a compressive radiculopathy. In 27 percent, there was a focal or asymmetrical extension of the disc beyond the margin of the interspace (protrusion), and in only 1 percent was there more extreme extension of the disc (extrusion or sequestration). However, the time-honored tenet of prolonged bed rest has been questioned by the results of several randomized studies (Vroomen et al). It would appear that the main benefit is simply that time has passed and the expected resolution of pain has taken its course in many patients. In a few patients with severe sciatica we have been impressed with the tem porary relief afforded by administration of oral dexa methasone (4 mg every 8 h) for several days, although this approach has not been studied systematically and several of our colleagues decry it. The treatment of nerve root compression with repeated epidural injections of corticosteroids has enjoyed periods of popularity, but controlled studies have failed to confirm sustained efficacy (White et al; Cuckler et al), and it is not without compli cations including the rare but widely publicized outbreak of fungal meningitis from contaminated steroids. As with many similar studies, Carette and colleagues (1997) found only short-term improvement with epidural steroid injection and the ultimate need for surgery was not altered. Nevertheless, some pain specialists have not discarded this form of treatment in view of success in selected patients, even if short-lived. Surgical Treatment of Lumbar Disc Disease An indication for emergency surgery is an acute compression of the cauda equina by massive disc extrusion, causing bilateral sensorimotor loss and sphincteric paralysis. Although not the recommended course, it should be pointed out that there have been instances in which even a dramatic syndrome of cauda equina compression had resolved spontaneously after several weeks. If the pain and neurologic findings have not subsided in response to conservative management or the patient has suffered frequent disabling acute episodes, surgi cal treatment must be considered. In the first study, a large proportion of patients assigned to treat ment with physical therapy and pain medications had enough pain that they required surgery within several months. In addition, patients assigned initially to surgery by microdiscectomy had considerably faster relief of back and sciatic pain, but at the end of a year, both groups had minimal disability and similar degrees of minor pain. The implications of this study are that avoiding surgery initially does not have adverse consequences but if more rapid pain relief and mobilization are the aims, surgery is preferable. In the second cited study there was even greater crossover between conservative and surgically assigned groups and there was a slightly more favorable outcome in those who underwent early surgery. The surgical procedure most often indicated for lumbar disc disease is one of the variants of a hemilami nectomy with excision of the disc fragment introduced almost a century ago by Mixter and Barr. Questions relating to the relative merits of limited ("microscopic"), or minimally invasive excision of the lamina are often raised by patients and no clear answer can be given except that individual surgeons excel at one or another technique and the outcomes are similar. Rerupture occurs in approximately 5 percent of operated cases according to Shannon and Paul. Spinal fusion of the involved segments is indicated in cases in which there is instability, usually related to extensive or prior surgery or to an anatomic abnormality. Our practice would be to avoid surgery in such cases, but to endorse physical therapy. Compression of the cauda equina by epidural masses, as described further on, most often begins with back pain or sciatica.
Buy mildronate 500 mg without a prescription
If the dementia is slight and circumstances are suitable medicine of the wolf 250mg mildronate visa, patients should remain at home for the first years, continuing to engage in those accustomed activities of which they are capable. They should be spared responsibility and guarded against injury that might result from imprudent action, such as leaving a stove turned on or driving and getting lost-or worse. If they are still at work, plans for occupational retirement should be carried out. In more advanced stages of the disease, when mental and physical enfeeble ment become pronounced, a skilled nursing facility or supervised home care should be arranged. The value of centrally acting cholinergic agents and glutamate antagonists in the treatment of Alzheimer disease is modest but clear and should be weighed against the need for blood testing and side effects. These medications, however, offer psychologic benefit to the patient and family; Chap. Undesirable restlessness, nocturnal wandering, and belligerency may be reduced by administration of one of the antipsychotic or benzodiazepine drugs (see Chaps. Although randomized trials of these drugs have failed to show benefit in extreme circum stances, partly as a result of poor tolerance, there are few other options. Emotional lability and paranoid tenden cies may be managed by the judicious use of quetiapine, olanzapine, risperidone, or haloperidol. Some patients are helped by short-acting sedatives such as lorazepam without any worsening of the mental condition, but all these drugs must be given with caution and some may be particularly problematic in patients with combined parkinsonism and dementia syndromes. Visiting nurses, social agencies, live-in healthcare aides, day care settings, and respite care to relieve fami lies from the constant burden of caring for the patient should all be used to advantage. Some of the inevitable practical problems accompanying the dissolution of per sonal life caused by dementia can be ameliorated by judicious use of powers of attorney or guardianship and similar legal vehicles. Mishkin M, Delacour J: An analysis of short-term visual memory in the monkey I Exp Psycho/ A nim Behav Proc 1:326, 1975. J Sander D, Winbeck K, Eigen T, et al: Disturbance of venous flow patterns in patients with transient global amnesia. Lund and Manchester Groups, The: Consensus statement: Oinical and neuropathological criteria for fronto-temporal dementia. Together: A n Investigation Into the Genetic and Environmental Causes of Variation in Personality. Suthana N, Haneef Z, Stem J, et al: Memory enhancement and deep-brain stimulation of the entorhinal area. Victor M, Agamanolis D: Amnesia due to lesions confined to the hippocampus: A clinical-pathologic study. The long-standing controversy about cerebral functions, whether they are diffusely represented in the cerebrum with all parts roughly equivalent, or localized to certain lobes or regions, has been resolved to the satisfaction of most neurologists. Clinicians have demonstrated beyond doubt that particular functions are assignable to certain cortical regions. For example, the pre- and postrolandic zones control motor and sensory activities, respectively, the striate occipital zones control visual perception, the superior temporal gyri are auditory, and so on. Beyond these broad correlations, however, there is a notable lack of precision in the cortical localization of most of the behavioral and mental operations described in Chaps. In particular, of the higher order functions, such as attention, vigilance, apperception, and analytic and synthetic thinking, none has a precise and predictable anatomy; or, more accurately, the neural systems on which they depend are widely distributed among several regions. Does it refer to the physiologic func tion of a circumscribed group of neurons in the cerebral cortex, indicated clinically by a loss of that function when the neurons in question are destroyed This is the way in which neurologists have assigned functions to particular areas of the cerebral cortex. However, from what we know of the rich connectivity of all parts of the special ized cortical centers, one must assume that this is only partly the case. Most who ponder this subject believe that the organization of cerebral function is based on discrete networks of closely interconnected afferent and efferent neurons in several regions of the brain. These ensembles must be linked by both regional and more widespread systems of fibers. This is especially apparent in the dis cussion of the anatomy of complex cognitive properties such as intelligence, as described in Chap. Thus, many basic functions are anchored in one cortical region and a lesion there causes loss of a particular ability. But it is apparent from physiologic studies such as functional imaging and electromagnetic stimulation that widely distributed networks are engaged, which nonetheless encompasses the region that can be ablated and eliminate the function in question. These aspects of cerebral localization-brought out so clearly in the writings of Wernicke, Dejerine, and Liepmann, have been elaborated by Luria (1966 and 1969) and the Russian school of physiologists and psy chologists and extended by Geschwind (1965). In keeping with the model of interconnected networks, they viewed function not as the direct property of a particular, highly specialized region of the cerebrum but as the product of complex, diffusely distributed activity by which sensory stimuli are analyzed and integrated at various levels of the nervous system and then united, through a system of temporarily acquired connections, into a working mosaic adapted to accomplish a particular task To some extent, this model has been corroborated by functional imaging studies, which show increased metabolic activity in sev eral cortical regions during almost every form of human behavior, including willed motor acts, language tasks, and those coinciding with perceptive and apperceptive sensory experiences. Within such a functional system, the initial and final points (the task and the effect) remain unchanged, but the intermediate links (the means of performance of a given task) may be modified within wide limits and will never be exactly the same on two consecutive occasions. Thus, when a certain act is called for by a spoken command, the dominant temporal lobe must receive the message and transmit it to the premo tor areas. Or it may be initiated by the intention of the individual, in which case the first measurable cerebral activity (a "readiness potential") occurs anterior to the premotor cortex. The motor cortex is also always under the dynamic control of the proprioceptive, visual, and vestibular systems. Thus, a lesion that affects any one of several elements in the act may cause loss of a skilled ability, either the motor centers themselves or their con nections with the other elements. Another theoretical scheme of cerebral function identifies cortices of similar overall structure and divides the cerebral mantle into three longitudinally oriented zones, the triune brain articulated by Paul Maclean. A central vegetative neuronal system (allocortex and hypothalamus) provides the mechanisms for all internal functions, the milieu interieur of Bernard and Cannon. This ostensibly metaphoric concept of central nervous sys tem function, first proposed by Broca, was elaborated by Yakovlev and has been adopted more recently by Benson and by Mesulam (1998). Such a model retains to a large degree the cytoarchitectural similarities among areas that serve similar functions. Most of the popular notions relating to the function of the frontal lobes are oversimplified. In the frontal lobe, are presumed to reside the mechanisms that govern per sonality, character, motivation, and our unique capacities for abstract thinking, introspection, and planning. These qualities and traits do not lend themselves to easy defini tion and study and certainly not to discrete localization. Except for the more posterior frontal mechanisms subserving motility, motor speech, and certain behaviors relating to impulse (conation), neurologists recognize that the other features of frontal lobe disease are more abstruse. Blood is supplied to the medial parts of the frontal lobes by the anterior cerebral artery and to the convexity and deep regions, by the superior (rolandic) division of the middle cerebral artery. The underlying deep white matter is supplied by a series of small penetrating arter ies, called lenticulostriate vessels that originate directly from the initial portion (stem) of the middle cerebral artery, as detailed in Chap. These are combined with sucking, grasping, and groping reflexes and other obligate behaviors. In the emotional sphere, frontal lobe lesions may cause anhedonia (lack of pleasure), apathy, loss of self-control, disinhibited social behavior, and euphoria, as described further on. Electrical stimulation of the motor cortex elicits contraction of corresponding muscle groups on the opposite side of the body; focal seizure activity has a similar effect. Stimulation of Brodmann area 4 produces movement of discrete muscle groups or, if sufficiently refined, of individual muscles. Repertoires of larger coor dinated movements are evoked by stimulation of area 6, the premotor and supplementary motor cortices. Lesions in the posterior part of the frontal lobe cause spastic paralysis of the contralateral face, arm, and leg. Motor impulses from the frontal lobe are conducted by the direct corticospinal tract and by tracts that descend from the motor, premotor, supplementary motor, and anterior parietal cortex to the spinal cord, either directly or via the red and reticular nuclei in the brainstem. Lesions of the more anterior and medial parts of the motor cortex result in less paralysis and more spastic ity, as well as a release of sucking, groping, and grasp ing reflexes, the actual mechanisms for which probably reside in the parietal lobe and which, as conceptualized by Denny-Brown, are tropisms or automatisms that are normally inhibited by the frontal cortex. When the lesions of the motor parts of the frontal lobe are bilateral, there is a tetraparesis in which the weakness is not only more severe but also more extensive than in unilateral lesions, affecting both spinal and cranial muscles (pseu dobulbar palsy). On the basis of blood flow studies, Roland and colleagues and Fuster suggest that an important function of the supplementary motor area is the ordering of motor tasks or the recall of memorized motor sequences, further evidence of the executive functions of the frontal lobes. Some insight into organization in supplementary motor cortex is given by seizures originating there; they give rise to curious postures such as a fencing position or flail ing of the opposite arm. Thus, aside from the overt abnormalities of motor, speech, and cerebral cortex, often referred to as the frontal eye field 22-1).
