
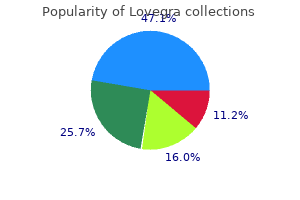
Buy genuine lovegra line
The epiphyseal plate is a region of transition from cartilage to bone pregnancy jewelry lovegra 100mg without a prescription, and functions as a growth zone where the bones elongate. The red- stained regions are calcified at this age, whereas the elbow, wrist, knee, and ankle joints appear translucent because they are still cartilaginous. This region, farthest from the marrow cavity, consists of typical hyaline cartilage with resting chondrocytes, not yet showing any sign of transformation into bone. A little closer to the marrow cavity, chondrocytes multiply and arrange themselves into longitudinal columns of flattened lacunae. Next, the chondrocytes cease to multiply and begin to hypertrophy (enlarge), much like they do in the primary ossification center of the fetus. Minerals are deposited in the matrix between the columns of lacunae and calcify the cartilage. Within each column, the walls between the lacunae break down and the chondrocytes die. This converts each column into a longitudinal channel (clear spaces in the figure), which is immediately invaded by blood vessels and marrow from the marrow cavity. Osteoblasts line up along the walls of these channels and begin depositing concentric lamellae of matrix, while osteoclasts dissolve the temporarily calcified cartilage. But around the perimeter of the marrow cavity, continuing ossification converts this spongy bone to compact bone. Osteoblasts lining the aforementioned channels deposit layer after layer of bone matrix, so the channel grows narrower and narrower. By adulthood, these will disappear and the epiphyses will fuse with the diaphyses. Chondrocyte multiplication in zone 2 and hypertrophy in zone 3 continually push the zone of reserve cartilage (1) toward the ends of the bone, so the bone elongates. In the lower limbs, this process causes a person to grow in height, while bones of the upper limbs grow proportionately. Cartilage growth from within, by the multiplication of chondrocytes and deposition of new matrix in the interior, is called interstitial21 growth. The most common form of dwarfism results from a failure of cartilage growth in the long bones (see Deeper Insight 7. In the late teens to early twenties, all the cartilage of the epiphyseal plate is depleted. The junctional region where they meet is filled with spongy bone, and the site of the original epiphyseal plate is marked with a line of slightly denser spongy bone called the epiphyseal line (see figs. When the epiphyseal plate is depleted, we say that the epiphyses have "closed" because no gap between the epiphysis and diaphysis is visible on an X-ray. Once the epiphyses have all closed in the lower limbs, a person can grow no taller. This micrograph shows the transition from cartilage to bone in the growth zone of a long bone. Bone Widening and Thickening Bones also continually grow in diameter and thickness. This involves a process called appositional growth,22 the deposition of new tissue at the surface. In bone, however, osteocytes embedded in calcified matrix have little room to spare for the deposition of more matrix internally. Osteoblasts in the inner layer of periosteum deposit osteoid tissue on the bone surface, calcify it, and become trapped in it as osteocytes-much like the process in figure 7. They lay down matrix in layers parallel to the surface, not in 22 cylindrical osteons like those deeper in the bone. This process produces the surface layers of bone called circumferential lamellae, described earlier. This is achieved by osteoclasts of the endosteum dissolving tissue on the inner bone surface. Thus, flat bones develop by intramembranous ossificaton alone, whereas long bones develop by a combination of the intramembranous and endochondral methods. Bone Remodeling In addition to their growth, bones are continually remodeled throughout life by the absorption of old bone and deposition of new. It repairs microfractures, releases minerals into the blood, and reshapes bones in response to use and disuse. As its name implies, achondroplastic dwarfism results from a failure of cartilage growth-specifically, failure of the chondrocytes in zones 2 and 3 of the metaphysis to multiply and enlarge. This is different from pituitary dwarfism, in which a deficiency of growth hormone stunts the growth of all of the bones, and a person has short stature but normal proportions throughout the skeletal system. Two people of normal height with no family history of dwarfism can therefore have a child with achondroplastic dwarfism. The mutant allele is dominant, so the offspring of a heterozygous achondroplastic dwarf have at least a 50% chance of exhibiting dwarfism, depending on the genotype of the other parent. Persons homozygous for the trait (those who inherit it from both parents) are usually stillborn or die soon after birth. Wolff observed that these stress lines were very similar to the ones that engineers knew of in mechanical cranes. The effect of stress on bone development is quite evident in tennis players, in whom the bones of the racket arm are more robust than those of the other arm. Long bones of the limbs are thickest at about midshaft, because this is where they are subjected to the greatest stress. Bone remodeling comes about through the collaborative action of osteoblasts and osteoclasts. If a bone is little used, osteoclasts remove matrix and get rid of unnecessary mass. If a bone is heavily used, or a stress is consistently applied to a particular region of a bone, osteoblasts deposit new osseous tissue and thicken the bone. Consequently, the comparatively smooth bones of an infant or toddler develop a variety of surface bumps, ridges, and spines (described in chapter 8) as the child begins to walk. On average, bones have a greater density and mass in athletes and people engaged in heavy manual labor than they do in sedentary people. Anthropologists who study ancient skeletal remains use evidence of this sort to help distinguish between members of different social classes, such as distinguishing aristocrats from laborers. The orderly remodeling of bone depends on a precise balance between deposition and resorption, between osteoblasts and osteoclasts. If one process outpaces the other, or both processes occur too rapidly, various bone deformities, developmental abnormalities, and other disorders occur, such as osteitis deformans (Paget disease), osteogenesis imperfecta (brittle bone disease), and osteoporosis (see table 7. Describe how a cartilage model is transformed into a long bone in endochondral ossification. Even after a bone is fully formed, it remains a metabolically active organ with many roles to play. Not only is it involved in its own maintenance, growth, and remodeling, but it also exerts a profound influence on the rest of the body by exchanging minerals with the tissue fluid. Disturbances of calcium homeostasis in the skeleton can disrupt the functioning of other organ systems, especially the nervous and muscular systems. For reasons explained later, such disturbances can even cause death by suffocation. A calcified mass in an otherwise soft organ such as the lungs is called a calculus. They have surface receptors for calcium and respond to falling levels of calcium in the tissue fluid. Hydrogen pumps in the ruffled border of the osteoclast secrete hydrogen ions into the tissue fluid, and chloride ions follow by electrical attraction. The space between the osteoclast and the bone thus becomes filled with concentrated hydrochloric acid with a pH of about 4. The osteoclast also secretes an acid-tolerant enzyme (protease) that digests the collagen of the bone matrix. When orthodontic appliances (braces) are used to reposition teeth, a tooth moves because osteoclasts dissolve bone ahead of the tooth (where the appliance creates greater pressure of the tooth against the bone) and osteoblasts deposit bone in the low-pressure zone behind it.
Buy lovegra online from canada
Squamous suture Squamous part Mastoid part the Temporal Bones If you palpate your skull just above and anterior to the ear-that is menopause jewelry safe lovegra 100mg, the temporal region-you can feel the temporal bone, which forms the lower wall and part of the floor of the cranial cavity (fig. The temporal bone derives its name from the fact that people often develop their first gray hairs on the temples with the passage of time. The squamous9 part (which you just palpated) is Petrous part Zygomatic relatively flat and vertical. It bears two prominent features: meatus (a) the zygomatic process, which extends anteriorMastoid process ly to form part of the zygomatic arch (cheekbone); Styloid process and (b) the mandibular fossa, a depression where (b) Medial surface the mandible articulates with the cranium. The lateral surface faces the scalp borders the opening of the external acoustic and external ear; the medial surface faces the brain. The petrous12 part can be seen in the cranial floor, where styloid process provides attachment for muscles of the it resembles a little mountain range separating the middle tongue, pharynx, and hyoid bone. The internal acoustic bears a heavy mastoid process, which you can palpate as meatus, an opening on its posteromedial surface, allows a prominent lump behind the earlobe. It is filled with small passage of a nerve that carries signals for hearing and balair sinuses that communicate with the middle-ear cavity. On the inferior surface these sinuses are subject to infection and inflammation of the petrous part are two prominent foramina named (mastoiditis), which can erode the bone and spread to the for the major blood vessels that pass through them (see brain. The notch is so close to the inner ear that one can sometimes hear perforated at its anterior end by the stylomastoid foramen, the pulsing of its blood when the ear is resting on a pillow which is a passage for the facial nerve, and at its posterior or the heart is beating hard. Its most conspicuous feature, the foramen magnum, admits the spinal cord to the cranial cavity; the dura matter is attached to the rim of this foramen. Since the cranium cannot expand, swelling puts pressure on the brain and results in even more tissue damage. Severe swelling can force the brainstem out through the foramen magnum, usually with fatal consequences. The occipital bone continues anterior to this as a thick median plate, the basilar part. At the anterolateral edge of each condyle is a hypoglossal13 canal, named for the hypoglossal nerve that passes through it to innervate the muscles of the tongue. Internally, the occipital bone displays impressions left by large venous sinuses that drain blood from the brain (see fig. Just before 13 reaching the foramen magnum, it branches into right and left grooves that wrap around the occipital bone like outstretched arms before terminating at the jugular foramina. A ridge, the superior nuchal line, can be traced horizontally from this protuberance toward the mastoid process (see fig. It defines the superior limit of the neck and provides attachment to the skull for several neck and back muscles. It forms the boundary where, in palpating the upper neck, you feel the transition from muscle to bone. By pulling down on the occipital bone, some of these muscles help to keep the head erect. The deeper inferior nuchal line provides attachment for some of the deep neck muscles. This inconspicuous ridge cannot be palpated on the living body but is visible on an isolated skull. The greater wings form about half of the middle cranial fossa (the temporal bone forming the rest) and are perforated by several foramina to be discussed shortly. The greater wing also forms part of the lateral surface of the cranium just anterior to the temporal bone (see fig. The lesser wing forms the posterior wall of the orbit and contains the optic canal, which permits passage of the optic nerve and ophthalmic artery (see fig. Superiorly, a pair of bony spines of the lesser wing called the anterior clinoid processes appears to guard the optic foramina. A gash in the posterior wall of the orbit, the superior orbital fissure, angles upward lateral to the optic canal. In life, the dura mater stretches over the sella turcica and attaches to the anterior clinoid processes. A stalk penetrates the dura to connect the pituitary gland to the base of the brain. Lateral to the sella turcica, the sphenoid is perforated by several foramina (see fig. The foramen spinosum, about the diameter of a pencil lead, provides passage for an artery of the meninges. In an inferior view of the skull, the sphenoid can be seen just anterior to the basilar part of the occipital bone. The vertical perpendicular plate, a thin median plate of bone that forms the superior two-thirds of the nasal septum (see fig. On each side of the crista is an elongated depressed area perforated with numerous holes, the cribriform (olfactory) foramina. A pair of olfactory bulbs of the brain, concerned with the sense of smell, rests in these depressions, and the foramina allow passage for olfactory nerves from the nasal cavity to the bulbs (see Deeper Insight 8. The labyrinth is named for the fact that internally, it has a maze of air spaces called the ethmoidal cells. The lateral surface of the labyrinth is a smooth, slightly concave orbital plate seen on the medial wall of the orbit (see fig. These project into the nasal fossa from its lateral wall toward the septum (see figs. By filling space and creating turbulence in the flow of inhaled air, they ensure that the air contacts the mucous membranes that cover these bones, which cleanse, humidify, and warm the inhaled air before it reaches the lungs. The superior concha and adjacent part of the nasal septum also bear the sensory cells of smell. Usually, all that can be seen of the ethmoid is the perpendicular plate, by looking into the nasal cavity (see fig. The force of a blow can drive bone fragments through the cribriform plate into the meninges or brain tissue. Such injuries are often evidenced by leakage of cerebrospinal fluid into the nasal cavity, and may be followed by the spread of infection from the nasal cavity to the brain. Blows to the head can also shear off the olfactory nerves that pass through the ethmoid bone and cause anosmia, an irreversible loss of the sense of smell and a great reduction in the sense of taste (most of which depends on smell). Facial Bones Facial bones do not enclose the brain but lie anterior to the cranial cavity. They support the orbital, nasal, and oral cavities, shape the face, and provide attachment for the muscles of facial expression and mastication. There are 14 facial bones: 2 maxillae 2 palatine bones 2 zygomatic bones 2 lacrimal bones 2 nasal bones 2 inferior nasal conchae 1 vomer 1 mandible 23 concha = conch (large marine snail) Key Ethmoid bone: Crista galli Cribriform plate Cribriform foramina Sella turcica Cartilage Frontal bone Frontal sinus Nasal bone Nasal conchae: Superior Sphenoid sinus Occipital bone Sphenoid bone Anterior nasal spine Palatine bone Lacrimal bone Maxilla Incisive foramen Lip Incisor Middle Inferior Nasal cartilages Ethmoid b. They form the upper jaw and meet each other at a median intermaxillary suture (see figs. Small points of maxillary bone called alveolar processes grow into the spaces between the bases of the teeth. If a tooth is lost or extracted so that chewing no longer puts stress on the maxilla, the alveolar processes are resorbed and the alveolus fills in with new bone, leaving a smooth area on the maxilla. Just below the orbit, it exhibits an infraorbital foramen, which provides passage for a blood vessel to the face and a nerve that receives sensations from the nasal region and cheek. The maxilla forms part of the floor of the orbit, where it exhibits a gash called the inferior orbital fissure that angles downward and medially (fig. The inferior and superior orbital fissures form a sideways V whose apex lies near the optic canal. The inferior orbital fissure is a passage for blood vessels and sensory nerves from the face. Its function is to separate the nasal cavity from the oral cavity, enabling us (and other mammals) to continue breathing while chewing. The high metabolic rate of humans requires rapid digestion of food, which in turn is aided by prolonged and thorough mastication into small, easily digested particles. This would be difficult if such prolonged mastication required an interruption of airflow. The palate consists of a bony hard palate anteriorly and a fleshy soft palate posteriorly. Just behind the incisors (front teeth) is a median pit, the incisive fossa, which is a passage for an artery to the palate and a nerve to the lower part of the nasal septum and the six front teeth of the maxilla. The palatine processes normally meet at the intermaxillary suture at about 12 weeks of gestation.

Discount lovegra online
History and Discovery During the clinical development of lamotrigine as a treatment for intractable seizures menstruation no bleeding buy lovegra master card, improved mood in lamotrigine-treated patients was anecdotally reported (Jawad et al. In 1993, the addition of lamotrigine to an existing antiepileptic drug regimen was evaluated in a small study of 81 patients with epilepsy (Smith et al. Lamotrigine-treated patients reported significantly higher levels of happiness and an improvement in perceived internal locus of control. There was no correlation between perceived happiness and changes in seizure frequency or severity. Thus, the investigators preliminarily concluded that lamotrigine may have an effect on mood independent of its antiepileptic effect. Lamotrigine has not been shown to inhibit the reuptake of norepinephrine, dopamine, or serotonin. Lamotrigine inhibits usedependent sodium channels, allowing continued normal depolarizations while suppressing paroxysmal burst firing encountered in seizures and hypoxic insult. Pharmacokinetics and Disposition Oral lamotrigine is rapidly absorbed with negligible first-pass metabolism. Lamotrigine is approximately 55% bound to plasma proteins and is unlikely to significantly interact with drugs that are highly protein bound. The clearance of lamotrigine is reduced in the setting of renal insufficiency and hepatic disease. During pregnancy, clinically significant perturbations in lamotrigine levels can occur. The rate of lamotrigine clearance increases during each trimester, reaching a peak of 330% of baseline clearance by week 32 gestational age (Pennell et al. The American Academy of Neurology recommends active monitoring of lamotrigine levels during pregnancy (Harden et al. Mechanism of Action the mechanism by which lamotrigine achieves its therapeutic effect in the treatment of bipolar disorder is unknown. In addition to sodium channel inhibition, lamotrigine antagonizes N-type calcium channels (Stefani et al. These genetic findings, coupled with the action of lamotrigine on sodium and calcium channels, suggest that channelopathies may be involved in the pathophysiology of bipolar disorder. Presynaptic inhibition of voltage- and usesensitive sodium channels, calcium channels, and potassium channels (Grunze et al. In addition, lamotrigine may increase brain levels of N-acetylaspartate, a mechanism believed to enhance neuronal viability, as deficits in N-acetylaspartate contribute to excessive glutamatergic tone and subsequent cell death (Croarkin et al. Lamotrigine is also indicated for adjunctive antiepileptic therapy in adults and pediatric patients (2 years of age) with partial seizures, with generalized seizures secondary to Lennox-Gastaut syndrome, or with primary and generalized tonic-clonic seizures, as well as for antiepileptic monotherapy in patients (16 years of age) with partial seizures (GlaxoSmithKline 2015). Inadequate data are available to recommend use of lamotrigine in unipolar depression. Other conditions in which lamotrigine has shown promising results in clinical trials include management of rapid-cycling bipolar disorder, borderline personality disorder, schizophrenia, and menstrually entrained mood cyclicity. Maintenance Therapy in Bipolar I Disorder Two large randomized, double-blind, parallel-group, placebo-controlled multicenter studies led to the approval of lamotrigine as a maintenance therapy in bipolar I disorder (Bowden et al. Both of these paired studies included a screening phase of up to 2 weeks; an 8- to 16-week open-label phase during which lamotrigine was initiated as an adjunctive agent or as monotherapy and other psychotropic drugs were discontinued; and an 18-month double-blind phase during which patients received lamotrigine, lithium, or placebo as maintenance monotherapy. The primary efficacy variable in both studies was time to intervention for any mood episode. Both lamotrigine and lithium were superior to placebo in delaying the time to intervention for any mood episode (P=0. Lamotrigine, but not lithium, was superior to placebo in prolonging the time to a depressive episode (P=0. Lithium, but not lamotrigine, was superior to placebo in prolonging the time to a manic, hypomanic, or mixed episode (P=0. In a post hoc analysis of these two studies, both lithium and lamotrigine were more effective than placebo in prolonging the time to any mood relapse and manic or hypomanic relapse, but only lamotrigine was superior to placebo in delaying depressive relapse (Goodwin et al. An open-label study conducted in a clinical setting did not find a significant difference between lithium and lamotrigine in preventing any mood, manic or hypomanic, or depressive relapse (Licht et al. In the interpretation of maintenance-phase data, it is important to distinguish between efficacy in relapse prevention and true prophylactic efficacy (Ghaemi et al. Mood episodes of the same polarity as the index episode that occur during the initial 2 months following recovery are generally regarded as relapses, and therefore are considered as being still part of the acute recovery period. Alternatively, mood episodes that occur beyond this time frame, during the period of remission, are regarded as recurrences. When all subjects who experienced a relapse to a mood episode of the same polarity as the index episode within 90 days of randomization were excluded, both lamotrigine and lithium were found to be more effective than placebo in delaying the time to intervention for a mood episode (P=0. Similar results were found when patients who relapsed to a mood episode of the same polarity as the index episode within 180 days of randomization were excluded, suggesting that lamotrigine and lithium possess true maintenance efficacy. Acute Monotherapy and Adjunctive Therapy of Bipolar Depression Monotherapy of Bipolar Depression A series of double-blind, placebo-controlled multicenter studies of lamotrigine was completed to replicate and extend preliminary open-label prospective findings suggesting moderate to marked efficacy in bipolar depression (Calabrese et al. The first study in this series evaluated the efficacy and safety of two dosages of lamotrigine compared with placebo in the acute treatment of a major depressive episode in 195 patients with bipolar I disorder (Calabrese et al. Outpatients received lamotrigine (50 or 200 mg/day) or placebo as monotherapy for 7 weeks. However, the advantage of lamotrigine over placebo was larger in more severely depressed patients. The Guidelines for the Biological Treatment of Bipolar Disorders: Update 2010 from the World Federation of Societies of Biological Psychiatry recommended use of lamotrigine for acute bipolar depression on the basis of the overall positive results of the meta-analysis by Geddes et al. Although negative controlled studies outweigh positive studies of lamotrigine administered as monotherapy for bipolar depression, the negative findings in individual trials may be more a reflection of the patient composition than of a property of the drug itself, given the lack of a comparator arm to determine assay sensitivity and the relatively high rates of placebo response (Grunze et al. In an effort to identify the symptomatic dimensions that may be responsive or unresponsive to lamotrigine, Mitchell et al. Lamotrigine was unlikely to provide benefits for weight gain, insomnia, anergia, or anxiety (Mitchell et al. Overall response and remission rates were comparable between the active agents, although differences did emerge in regard to tolerability profiles. The incidence of adverse events involving suicidal and self-injurious behavior was higher among patients taking lamotrigine (3. However, significant differences in mean change from baseline to endpoint for clinically relevant laboratory and physiological parameters favored treatment with lamotrigine, including measures such as hemoglobin A1c, prolactin, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglycerides, and body weight. After 16 weeks, all responders in both groups were followed for 68 weeks or until a relapse or recurrence of a depressive or manic episode occurred.
Buy lovegra canada
A number of unforeseen methodological limitations in this trial complicated interpretation of its results women's health clinic oakville buy 100mg lovegra fast delivery. Among patients who received divalproex for treatment of the index manic episode in an open treatment period prior to randomization, divalproex was superior to placebo on rates of early termination due to any mood episode (29% vs. Divalproex was also compared with olanzapine in a 47week blinded maintenance trial (Tohen et al. There are no data regarding the optimal maintenance valproic acid concentration in bipolar disorder. Although a number of studies have examined the efficacy of carbamazepine in the maintenance treatment of bipolar disorder, most of these studies yielded results that were difficult to reliably interpret on methodological grounds (Dardennes et al. Atypical Antipsychotics Olanzapine was comparable to divalproex in a 47-week comparison trial (Tohen et al. Olanzapine received an indication for maintenance treatment in bipolar disorder based on superiority over placebo in prevention of manic and depressive episodes over 48 weeks (Tohen et al. The combination of olanzapine and lithium or divalproex was superior to placebo and lithium or divalproex in relapse prevention over 18 months in patients who had initially responded to the active combination acutely (Tohen et al. However, patients in the combination therapy group had twice the weight gain of patients in the monotherapy group. Aripiprazole was superior to placebo in preventing manic relapse over a 6month follow-up period in patients with bipolar disorder who were initially stabilized on aripiprazole monotherapy for an acute manic or mixed episode (Keck et al. By contrast, no significant difference between aripiprazole and placebo was found for rates of depressive relapse. However, the overall low rate of depressive relapse in this trial may have been due to the inclusion of patients whose index episodes were manic or mixed rather than depressive. Two 104-week adjunctive placebo-controlled trials found quetiapine in combination with lithium or divalproex to be superior to placebo with lithium or divalproex in prolonging time to recurrence of a mood episode (Suppes et al. The quetiapine combination groups also had lower proportions of patients experiencing a mood event. In a 6-month maintenance trial, ziprasidone was superior to placebo in combination with lithium or divalproex in prolonging time to intervention for a mood episode and in proportion of patients requiring an intervention during the length of the trial (Bowden et al. In two randomized controlled trials, risperidone (long-acting injectable formulation) was found to be superior to placebo in prevention of relapse, both as monotherapy and as adjunctive therapy (Quiroz et al. Evidence from one placebo-controlled trial suggests that paliperidone extended release may be efficacious as a maintenance treatment in patients with bipolar disorder (Berwaerts et al. Psychotherapy Most patients with bipolar disorder experience a common cluster of psychological problems stemming directly from the illness. A number of specific psychosocial interventions as adjuncts to mood stabilizer therapy have been shown to improve the long-term outcome of bipolar disorder (reviewed in Rizvi and Zaretsky 2007). The best-studied interventions include educational, interpersonal, family, and cognitive-behavioral therapies. Randomized controlled trials conducted over 1- to 2-year follow-up periods support the efficacy of cognitive-behavioral therapy (Lam et al. Family-focused, interpersonal, and social rhythm therapies were all associated with delaying time to depressive episode relapse compared with brief treatment (Miklowitz et al. Conclusion There have been substantial advances in the pharmacological treatment of bipolar disorder in the past two decades. A number of medications have demonstrated efficacy in the treatment of acute mania in placebo-controlled trials, either as monotherapy or as an adjunct to mood stabilizers. In addition, available data indicate that combination therapy with an antipsychotic and a mood stabilizer is more rapidly effective, with better overall response rates in acute mania, than either mood stabilizers or antipsychotics alone. The treatment of bipolar depression remains one of the least-studied aspects of the illness. The "mood stabilizer first" strategy and the combined use of mood stabilizers and antidepressants in moderate to severe bipolar depression are common approaches. Most patients with bipolar disorder require treatment with more than one medication during the course of their illness. Recent studies suggest that for some patients, the use of combinations of antidepressants and mood stabilizers as maintenance treatment may be important to prevent depressive relapse. The role and efficacy of different types of psychotherapy at different phases of illness management in bipolar disorder are now becoming clearly established. These components of treatment are important in educating patients and families, improving insight and treatment adherence, enhancing coping skills, and dealing with the sequelae of mood symptoms and episodes -and, it is hoped, improving functioning and outcome. Bringing these treatments to patients with bipolar disorder is both the challenge and the reward of helping people manage this illness. Report of the Veterans Administration and National Institute of Mental Health Collaborative Study Group. Over the past two decades, there has been substantial progress in the treatment of anxiety and related disorders. In this chapter, we review the main findings from double-blind and some open-label trials in each disorder.
Diseases
- Pseudohermaphroditism
- Short stature hyperkaliemia acidosis
- Olivopontocerebellar atrophy deafness
- Kostmann syndrome
- Congenital heart block
- Cantu Sanchez Corona Garcia syndrome
- Aerosinusitis
- Mesodermal defects lower type
Order lovegra 100 mg with amex
It is now known that a number of important intracellular proteins are able to alter the function of glutamate receptors (see diagram) menstruation reddit 100 mg lovegra visa. Reprinted from Schizophrenia Working Group of the Psychiatric Genomics Consortium: "Biological Insights From 108 Schizophrenia-Associated Genetic Loci. History and Discovery After noting the sedating properties of lithium in animals, Cade first described the successful treatment of mania with lithium salts (Cade 1949). Pharmaceutical companies were reluctant to produce this inexpensive drug that they could not patent (Kline 1973). Lithium is a highly cost-effective treatment for bipolar disorder (Chisholm et al. A growing number of medications with proven efficacy in bipolar disorder have become available since the introduction of lithium, including anticonvulsants and second-generation (atypical) antipsychotics. In contrast to many of these medications, lithium is available generically and is relatively affordable. Substitution of or competition with other cations may contribute to its effects (Baldessarini 1996; Ward et al. Pharmacological Profile Lithium is minimally protein bound, does not undergo biotransformation, and is renally eliminated (Kilts 2000). Pharmacokinetics and Disposition Lithium is available in multiple preparations, including lithium carbonate tablets and capsules, lithium citrate, and slow-release formulations (Jefferson et al. Lithium is absorbed from the gastrointestinal tract and is renally excreted unchanged within approximately 24 hours (Baldessarini 1996; Baldessarini and Tarazi 2001). Lithium is not protein bound and is evenly distributed in total body water space (Jermain et al. Lithium excretion is controlled by osmotic factors and is a function of renal sufficiency (Birch et al. Multiple theories, based on animal models and on limited studies in humans, have been proposed. Neurotransmitter Effects Lithium brings about changes in several of the major neurotransmitter systems in the brain, with the overall effect being stimulation of inhibitory transmission and inhibition of excitatory signals (Malhi et al. Chronic administration of lithium in mice increases and stabilizes glutamate uptake. Lithium enhances norepinephrine and serotonin function in the central nervous system, which could explain its antidepressant effects (Price et al. Inositol Depletion There has been much focus on the role of the inositol cycle in the clinical effects of lithium. Lithium is a noncompetitive inhibitor of inositol monophosphatase, depleting free inositol within 5 days of treatment initiation (Berridge et al. Depletion of free inositol can lead to effects on neurotransmitter and intracellular second-messenger systems linked to the inositol cycle. For example, adrenergic, serotonergic, and cholinergic receptor subtypes are coupled to the cycle via G proteins, and the cycle in turn regulates protein kinase C action, which appears to be influenced by lithium treatment in mania (Hahn et al. Wnt signaling triggers a cascade of events that leads to stimulation of protein kinase C activity (Grahame-Smith 1998; Williams and Harwood 2000). Patients treated with lithium have larger cortical and hippocampal volumes (Hajek et al. Indications and Efficacy Bipolar Disorder Acute Mania Cade (1949) first published data on the efficacy of lithium in mania more than 60 years ago. As we approach the end of the second decade of the twentyfirst century, lithium remains one of the most efficacious treatments for bipolar disorder. Lithium has been shown in studies to be more efficacious than placebo in the treatment of acute mania (Bowden et al. A review of response rates in randomized trials of medication treatment indicated that lithium was at least somewhat efficacious in the treatment of mania, with a response rate of 70% (87 of 124 patients) (Keck et al. Early studies with lithium established its antimanic efficacy relative to first-generation (typical) antipsychotics (Garfinkel et al. However, a later meta-analysis concluded that lithium was more effective than chlorpromazine in acute mania (Poolsup et al. A review of studies by Goodwin and Zis (1979) found lithium to be efficacious in at least 70% of patients, as defined by remission or marked improvement. In a 3-week double-blind study of lithium, haloperidol, and their combination for acute mania, patients who received haloperidol or haloperidol plus lithium had more significant improvement compared with those who received lithium alone (Garfinkel et al. Lithium has also been studied in comparison with second-generation antipsychotic medications (Berk et al. However, many of these trials were focused on assessing the efficacy of the antipsychotic in a noninferiority approach rather than on demonstrating significant differences between the medications. For example, in a direct comparison with lithium, olanzapine produced greater improvement in manic symptoms over 4 weeks, but it also produced more weight gain (Niufan et al. By and large, antipsychotics appear to work faster than lithium but carry higher risks for weight gain and other metabolic effects (Fountoulakis et al. In a recent study, the addition of lithium to therapy with extended-release quetiapine was found to be more efficacious than add-on placebo. However, the high proportion of enrolled subjects that did not meet all eligibility criteria for the study may have contributed to the negative findings (Sachs et al. In one study, adjunctive gabapentin added to lithium was found to be effective in treating acute mania (Astaneh and Rezaei 2012). Double-blind randomized studies suggest that carbamazepine and lithium are equally effective in the treatment of acute mania (Fountoulakis et al. A meta-analysis of available randomized controlled trials likewise showed that lithium and valproate were equally effective in acute mania (Poolsup et al. In a meta-analysis examining the efficacy of lithium, valproate, and carbamazepine in mania, no significant differences in efficacy were found among the three agents (Emilien et al. The presence of neurological abnormalities may predict a better response to anticonvulsants than to lithium in mania. One study found that patients with electroencephalogram abnormalities are more likely to respond to valproate than to lithium (Reeves et al. Mixed mania-the co-occurrence of mania with depression-may predict a poorer response to lithium. To further investigate the relation between co-occurring depressive symptoms and treatment response in acute mania, Swann et al. They found that the presence of depressive symptoms during an acute manic episode was associated with a poorer response to lithium and a better response to divalproex. Lithium plus topiramate showed no superiority to lithium plus placebo in acute mania (Mirsepassi et al. Psychotic Mania Lithium is equally effective in psychotic and nonpsychotic mania, and early improvement in psychotic symptoms was found to predict higher remission and response rates (de Sousa et al. Bipolar Depression Lithium is considered a first-line treatment for acute bipolar depression (Compton and Nemeroff 2000). Goodwin and Jamison (1990) analyzed placebo-controlled trials in bipolar depression and found that 79% of bipolar patients had either a complete or a partial response to lithium. Placebocontrolled trials showing the efficacy of lithium in bipolar depression include those by Baron et al. These studies generally were small (involving between 3 and 40 patients [Goodwin et al. A recent meta-analytic summary of the above-listed short studies showed a significant advantage for lithium over placebo in bipolar disorder versus unipolar depression (Selle et al. In this study, which used new clinical trials methodology, participants in the lithium group were not given a secondgeneration antipsychotic, and those in the quetiapine group were not given lithium; however, other adjunctive treatments were provided in accordance with best-practice guidelines (Nierenberg et al. Both groups showed improvement, with 20% achieving sustained response over the study period, and no differences in outcome were detected between the lithium and quetiapine groups (Nierenberg et al.
Generic lovegra 100mg mastercard
Even more gradual initiation strategies may be necessary to alleviate adverse effects women's health center uvm 100mg lovegra free shipping. Thus, starting with 50 mg (half of a chewable 100-mg tablet) at bedtime and increasing by 50 mg every few days can result in a bettertolerated initiation. However, if there is no hint of therapeutic response at moderate dosages, it is unlikely that pushing to very high dosages would be beneficial. Limited data suggest that this formulation has enhanced tolerability (Chung et al. Licarbazepine is 40% bound to plasma proteins, has a moderate volume of distribution (about 0. Elimination is mainly through the kidneys, unchanged or glucuronidated (Zaccara et al. Oxcarbazepine is metabolized to the active monohydroxy derivative as a racemic mixture with a higher (4:1) ratio of the S-enantiomer compared with the R-enantiomer. Despite the aggressive titration schedule, adverse effects were of mostly mild to moderate intensity (Grunze et al. However, these agents have such a diversity of biochemical effects that linking these mechanisms to their varying clinical actions presents a considerable challenge. High rates of placebo response and poor study recruitment (leading to premature study termination) may have contributed to failure in the second study (Grunze et al. Unfortunately, most of these studies are limited by their use of small samples of heterogeneous (both bipolar and unipolar) patients with highly treatment-resistant depression. However, subgroup differences may exist, such that lithium may be more effective in patients with "classical" bipolar disorder. However, this advantage was offset by more early discontinuations in the lithium group, so that similar proportions (about one-third) of patients completed 2 years with no episode. Of the 85 patients who had responded during acute treatment and were randomly assigned to one of the three dosage groups, at least 50% did not show any clinical worsening, although there was no significant difference between dosage groups (Grunze et al. Side Effects and Toxicology Baseline evaluation of patients with bipolar disorder includes not only psychosocial assessment but also a general medical evaluation in view of the risk of medical processes, which could confound diagnosis or influence management decisions, and the risk of adverse effects, which may occur with treatment. Assessment commonly includes history; physical examination; complete blood count with differential and platelets; renal, hepatic, and thyroid function; toxicology; pregnancy tests; and other chemistries and electrocardiogram as clinically indicated (American Psychiatric Association 2002). Such evaluation provides baseline values for parameters that influence decisions about choice of medication and intensity of clinical and laboratory monitoring. For example, mild leukopenia and benign rash occur in up to 1 in 10 patients, with the slight possibility that these usually benign phenomena are heralding malignant aplastic anemia and Stevens-Johnson syndrome, seen in about 1 in 100,000 patients (Kramlinger et al. In the instance of benign leukopenia, the addition of lithium can increase the neutrophil count back toward normal (Kramlinger and Post 1990), but this strategy is not likely to be helpful for the suppression of red cells or platelets, which is likely to indicate a more problematic process. Given the risk of serious rash, patients should be alerted to seek medical attention immediately if a rash develops. In particular, rash in patients presenting with systemic illness or involvement of the eyes, mouth, or bladder (dysuria) constitutes a medical emergency: carbamazepine should be immediately discontinued, and the patient should be assessed emergently (Scaparrotta et al. Data from controlled trials of anticonvulsant medications compared with placebo found a 1. Because of the risk of rare hepatitis, patients should be advised to seek medical evaluation immediately if they develop malaise or abdominal pain or other marked gastrointestinal symptoms. A baseline electrocardiogram is worth considering if there is a positive cardiac history. Most of the serious hematological reactions occur within the first 3 months of therapy (Tohen et al. Patients who have abnormal or marginal indices at any point merit careful scheduled and clinically indicated monitoring. Weight gain and obesity are important clinical concerns in the management of bipolar disorder. Medications and the hyperphagia, hypersomnia, and anergy commonly seen in bipolar depression can contribute to this important obstacle to optimal outcomes. In some cases, hyponatremia can be effectively counteracted with the addition of lithium or the antibiotic demeclocycline (Ringel and Brick 1986). Folate supplementation may attenuate the risk of spina bifida, and fetal ultrasound studies may allow early detection. However, clinically significant hyponatremia is less common than asymptomatic hyponatremia (Reinstein et al. Italic type indicates that serum concentrations of the medication may decrease to a clinically significant extent not only with carbamazepine but also with oxcarbazepine, hindering efficacy of the agent. The combination is generally well tolerated, with merely additive (as opposed to synergistic or antagonistic) neurotoxicity (McGinness et al. Pharmacokinetic interactions between these drugs do not occur because lithium has no hepatic metabolism. The risk of fatal hepatitis is of great concern in infants treated with combinations of valproate with other anticonvulsants (Scheffner et al. Interactions With Antidepressants Antidepressants are commonly combined with mood stabilizers in the treatment of bipolar disorder. These observations are consistent with the finding that verapamil and diltiazem but not nifedipine inhibit the hepatic oxidative metabolism of various drugs (Hunt et al.
Buy 100mg lovegra overnight delivery
These compounds are especially useful for patients who cannot sleep well because of acute allergic reactions or itching women's health boot camp workout order genuine lovegra on line. Because sedative antihistamines lack abuse potential, they also may be a good choice for individuals with substance use disorders. Doxepin (as Sinequan) (3 and 6 mg) reduces wake after sleep onset and prolongs total sleep time (Markov and Doghramji 2010). Several other selective H1 receptor blockers and H1 receptor reverse agonists are also under development for use as hypnotics. In animals, melatonin has been implicated in the circadian regulation of sleep and in the seasonal control of reproduction. Studies suggest that melatonin administration may have some therapeutic effects in various disturbances of circadian rhythmicity, such as those related to jet lag (Arendt et al. In humans, the production of melatonin during the dark period declines with age; this effect parallels declines in sleep quantity and quality (van Coevorden et al. These findings appear to suggest that deficiencies in nocturnal melatonin secretion might contribute to disrupted sleep in the elderly; thus, melatonin may be particularly beneficial for insomnia in this population. Indeed, some studies reported favorable effects with supplementary administration of melatonin in elderly persons with disturbances in sleep maintenance (Garfinkel et al. However, several studies reported contradictory findings indicating no significant relation between physiological melatonin secretion levels and sleep-maintenance parameters (Hughes et al. It is also unclear whether the hypnotic effect from a physiological or pharmacological dose represents a direct effect on sleep, an indirect effect on circadian timing that subsequently gates the release of sleep, or both. Finally, very few double-blind, placebo-controlled studies have been done, and most current reports are confounded by strong placebo effects in the context of a melatonin fad. Melatonin might be an effective hypnotic in some indications, but better-controlled studies are needed to establish its efficacy in specific indications. The purity of the products sold in health food stores is also a problem, and the long-term effects of melatonin administration in humans are unknown. A prolonged-release formulation of melatonin (marketed under the trade name Circadin) was approved by the European Commission in June 2007 as monotherapy (2 mg) for the short-term treatment of primary insomnia characterized by poor-quality sleep in patients 55 years and older (Lemoine et al. Melatonin receptors in the retina likely play an important role in retinal physiology, including circadian regulation (Sengupta et al. Ramelteon is currently the only nonscheduled prescription drug for the treatment of insomnia available in the United States. It has no appreciable affinity for receptors that bind neuropeptides, cytokines, serotonin, dopamine, norepinephrine, acetylcholine, and opiates. It also does not interfere with the activity of any known enzymes in standard panels. No published studies have reported comparative data on whether ramelteon is more or less safe or effective than melatonin, a much less expensive drug widely available in the United States without a prescription. Although significant decline in melatonin levels during aging has been reported by many investigators (Srinivasan et al. Melatonin receptor agonists can produce improvements in sleep timing similar to those produced by melatonin. Synthetic melatonin receptor agonists may also be useful in patients who experience insomnia due to shift work or jet lag, as well as delayed sleep phase syndrome or advanced sleep phase syndrome; beneficial effects of melatonin were reported in these conditions. Orexin (Hypocretin) Receptor Antagonists Orexin A (or hypocretin 1) and orexin B (or hypocretin 2) are newly discovered hypothalamic neuropeptides that play critical roles in the promotion and maintenance of wakefulness and in the pathophysiology of narcolepsy with cataplexy (Nishino 2011; Sakurai et al. In humans, chronic loss of orexin neurons is associated with narcolepsy with cataplexy. Orexin neurons are presumed to be most active during wakefulness and least active during sleep. The recommended dosage is 10 mg/day (a maximum of 20 mg once daily), to be taken orally once every night within 30 minutes of bedtime and with at least 7 hours remaining until the planned wake time. Suvorexant has demonstrated efficacy in both inducing and maintaining sleep (Jacobson et al. Adverse effects include next-day sleepiness and fatigue and issues with driving, as well as unusual dreams (Merck & Co 2014). Sleep paralysis and hypnagogic/hypnopompic hallucinations also have been reported to occur. Administration of suvorexant with a high-fat meal had no clinically significant effects on systemic drug exposure but delayed Tmax by 1. The main circulating compounds are the unchanged drug and a hydroxyl metabolite, which is not expected to be pharmacologically active. Suvorexant is primarily eliminated in the feces, with about 66% of a radiolabeled dose recovered in the feces (vs. There are as yet no published studies comparing suvorexant with other medications used for insomnia. Because insomnia is a very heterogeneous disease condition, it is likely that many patients will benefit from this new agent, and large amounts of clinical data should soon be available. General Considerations in the Pharmacological Treatment of Insomnia the International Classification of Sleep Disorders is the classification system most commonly used by sleep medicine specialists. Insomnia is a subjective complaint of insufficient, inadequate, or nonrestorative sleep (Buysse and Reynolds 1990). Inadequate sleep causes disturbances in daytime functioning, such as fatigue, mood problems, and impaired performance. Estimates of its prevalence depend on the definition criteria used and the population studied. The current use of hypnotics in the general population is estimated to range between 3. Insomnia is a symptom that must be explored clinically before treatment is initiated. Sleep disturbances often indicate a larger psychiatric problem, such as depression. As mentioned earlier, insomnia is a common complaint in older populations, especially in institutional settings. Insomnia Classifications Based on Duration A useful initial approach to the patient with insomnia is to consider the duration of the complaint. The duration of the insomnia not only suggests its cause but also provides some guidance on how best to use hypnotics in its treatment. Chronic insomnia disorder requires a report of a sleep initiation or sleep maintenance problem, an adequate opportunity and circumstances to sleep, and daytime consequences as the result of the insomnia symptoms. To meet diagnostic criteria for chronic insomnia disorder, the patient should have symptoms at least three times per week over a duration of 3 or more months. Because insomnia is a component of many psychiatric and medical conditions, a diagnosis of chronic insomnia disorder should be considered only when the insomnia is very prominent and requires further evaluation and treatment. Chronic insomnia (several months or even years) should first be evaluated with a sleep log of a 2-week period. Most commonly, some degree of sleepstate misperception is present, and patients with chronic insomnia may greatly exaggerate the complaint. In rare cases, insomnia began in childhood and has persisted into adulthood (idiopathic insomnia). In chronic insomnia, improved sleep hygiene and various behavioral techniques that aim to reduce negative conditioning. Pharmacotherapy is most appropriate for patients whose sleep disturbance is clearly causing some daytime dysfunction. If the clinician decides to prescribe medication, it is always helpful to start with the lowest dose of hypnotic possible to reduce the risk of tolerance and dependence; in addition, it is recommended that daily use be avoided if possible. To qualify for this diagnosis, the insomnia must be an independent focus for the patient and/or require separate clinical attention. Short-term insomnia disorder often resolves when the stressor does, or when the patient develops adequate coping mechanisms or adapts to the stressor (American Academy of Sleep Medicine 2014).

Purchase lovegra 100mg on-line
Men breast cancer quick facts generic 100 mg lovegra visa, on the other hand, have only one X chromosome and normally express any allele found there (fig. Ironically, even though color blindness is far more common among men than women, a man can inherit it only from his mother. Even if one parent transmits the recessive allele to her, the chances are high that she will inherit a normal allele from her other parent. There are so few functional genes on the Y chromosome-concerned mainly with development of the testes-that virtually all sex-linked traits are associated with the X chromosome. A polygenic trait such as eye color is determined by the contributions of genes at multiple loci. Another well-known example of pleiotropy is sickle-cell disease, detailed in section 18. In alkaptonuria, a single mutation leads to darkening of the skin, dark patches in the sclera ("white") of the eye, and darkening of the urine as it stands and oxidizes. Left: A female who inherits a recessive allele (c) for color blindness from one parent may not exhibit the trait, because she is likely to inherit the dominant allele (C) for normal vision from her other parent. For example, a dominant allele causes polydactyly,19 the presence of extra fingers or toes. We might predict that since it is dominant, anyone who inherited the allele would exhibit this trait. Penetrance is the percentage of a population with a given genotype that actually exhibits the predicted phenotype. If 80% of people with the polydactyly allele actually exhibit extra digits, the allele has 80% penetrance. Another reason the connection between genotype and phenotype is not inevitable is that environmental factors play an important role in the expression of all genes. Brown eyes, for example, require not only genes for the enzymes that synthesize the pigment melanin, but also the dietary raw material, phenylalanine, from which the melanin is made (fig. No gene can produce a phenotypic effect without nutritional and other environmental input, and no nutrients can produce a body or specific phenotype without genetic instructions that tell cells what to do with them. Just as you need both a recipe and ingredients to make a cake, it takes both heredity and environment to make a phenotype. The truth is that dominance and recessiveness have little to do with how common an allele is. We also saw earlier that people with cleft chins are in a minority, even though the allele for that is dominant. Epigenetics We have long thought of heredity as involving only the genes passed from parent to offspring. There is a growing awareness, however, of nongenetic changes that can occur in one generation and be inherited by the next. These are the subject of a new, astonishing, and fast-growing field called epigenetics20-heritable changes beyond the level of the genome. There is speculation that epigenetic changes can persist over multiple generations. If so, some aspects of your phenotype and health could stem even from what your grandparents ate, whether they smoked, and other environmental influences in their generation. Things you do or experience today might affect even your children or grandchildren through epigenetic changes. We must now view heredity as entailing more than just the genes passed from one generation to the next. A man can inherit color blindness only from his mother, whereas a woman must inherit it from both her father and mother to show the trait. Brown eye color requires phenylalanine from the diet (environment) and two genetically coded (hereditary) enzymes to convert phenylalanine to melanin, the eye pigment. This means the tumor is slow-growing and contained in a fibrous capsule so it will not metastasize, and in most cases it is relatively easy to treat. Oncology is a medical specialty that deals with both benign and malignant tumors, but only malignancies are called cancer. Energy-hungry tumors often stimulate such ingrowth of blood vessels-a phenomenon called tumor angiogenesis. Cancers are named for the tissue of origin: carcinomas originate in epithelial tissue; lymphomas in the lymph nodes; melanomas in pigment cells (melanocytes) of the epidermis; leukemias in blood-forming tissues such as bone marrow; and sarcomas in bone, other connective tissue, or muscle. About 90% of malignancies are carcinomas, probably because epithelial cells have a high rate of mitosis, making them especially subject to mutation, and because epithelia are more exposed than other tissues to carcinogens (environmental cancer-causing agents). Most cases are due to mutations arising anew in the affected individual, not to genes received from a parent. Oncologists are especially interested in two families of cancer genes called oncogenes and tumor-suppressor genes. An oncogene is analogous to a stuck accelerator on a car-it causes cell division to accelerate out of control, sometimes by inducing the excessive secretion of growth factors that stimulate mitosis, or the production of excessive growthfactor receptors. An oncogene called ras underlies about one-quarter of human cancers, and erbB2 is a common factor in breast and ovarian cancer. Consequently, mutations that destroy their protective "braking" function can lead to cancer. It takes time for so many mutations to accumulate, which is why cancer is more common in the elderly than in the young. Mortality usually results not from the original (primary) tumor, but from metastasis. A lively area of cancer research today is the development of drugs to starve tumors by blocking tumor angiogenesis. Primary tumor 1 Malignant cell penetrates blood or lymphatic vessel 2 Malignant cells travel to new sites 3 Traveling cells escape vessel 4 Escaped malignant cells multiply and establish metastatic tumors at new sites Secondary (metastatic) tumor 3. The process by which malignant cells escape from a primary tumor, travel in the blood or lymph, and seed the growth of new (metastatic) tumors in other localities. How alternative splicing partially explains why the diversity of human proteins vastly exceeds the number of human genes 7. Posttranslational modification of proteins, where it occurs, and how new proteins destined for extracellular use are packaged and released from a cell 9. How gene expression can be turned on or off according to the functions of different kinds of cells or physiological needs that change over time, such as a temporary need for breast milk 10. The structure of a metaphase chromosome and how many chromosomes are in a typical cell 6. The four stages of the cell cycle, what occurs in each stage, and which stages occur during interphase 5. How mitosis can be either stimulated or inhibited according to the need for tissue maintenance or growth 8. The definition of gene; how genes relate to the amino acid sequence of proteins; why it cannot be said that every gene codes for protein structure; and why not every protein is encoded by its own unique gene 2. The normal functions of a liver cell- synthesizing proteins, detoxifying wastes, storing glycogen, and so forth-are done during its a. Two genetically identical strands of a metaphase chromosome, joined at the centromere, are its a. An allele that is not phenotypically expressed in the presence of an alternative allele of the same gene is said to be a. Mutagens sometimes cause no harm to cells for all of the following reasons except a. At the checkpoints of the cell cycle, proteins called cyclins bind to and activate reactions that enable the cell to proceed to the next stage of the cycle. The pattern of nitrogenous bases that represents the 20 amino acids of a protein is called the. Briefly explain why each of the following statements is false, or reword it to make it true. Proteins destined to be exported from a cell are made by ribosomes on the surface of the Golgi complex. Steroids, carbohydrates, and phospholipids are encoded by different types of genes than are proteins. All mutations result in the production of defective proteins and are therefore harmful.
