
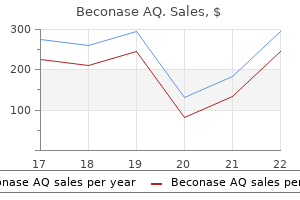
Buy discount beconase aq 200mdi line
Stimulated seizures initially resemble partial seizures allergy forecast tulsa order beconase aq overnight, which evolve during the protocol into secondary generalization. It has been hypothesized that the subtle and slow but cumulative neuronal loss and cellular/molecular alterations in neuronal circuits induced during the kindling protocol are a relevant model of epileptogenesis, which could better mimic human epileptogenesis than chemical status epilepticus models. However, kindling is a costly and time-consuming procedure with long periods of handling and stimulation, and whether it is completely relevant to some specific forms of human epilepsy remains contentious [38]. Short repetitive seizures can be also induced with chemical agents [4], for example fluorothyl, which can increase long-term seizure susceptibility and induce some cognitive deficits in rodents. Models of Post-Status Epilepticus Epilepsy Chemical these models are based on the administration of convulsive agents to induce an initial precipitating injury (status epilepticus) that is followed by a latent period of epileptogenesis leading to recurrent pharmacoresistant seizures originating from limbic structures and cognitive deficits [32, 33]. Systemic injections of kainic acid or pilocarpine in rodents are the most widely used models in epilepsy research today. The most used model of post-traumatic epilepsy is the fluid percussion injury, in which a mallet strikes a fluid column that transfers the mechanical energy to an adapter placed on the exposed dura of the animal. A single manipulation is in general sufficient to cause post-traumatic epilepsy, and the initial frontal-parietal injury can expand also to the hippocampus showing features of temporal lobe epilepsy. Other models are the weight drop, which induces diffuse injury, and the controlled cortical impact, which makes use of a computer-controlled pneumatic device, allowing precision in injury location, administration of force and cortical displacement. A limitation of animal models of post-traumatic epilepsy is that only a relatively small proportion of animals develop seizures, and they usually show long latent periods and low seizure frequency. Arterial occlusion by ligation or photo-thrombosis without subsequent hypoxia in adult rodents is used to model post-stroke epilepsy. Although phenotypes and neuropathology approximate human conditions, cellular and molecular mechanisms are not clear yet. Brain Tumor-Associated Epilepsy and Injections of Pathologic Organisms In these models, suspensions of tumor cells (cell lines or primary cell cultures from human tumors) are injected stereotactically into the rodent brain and can lead to spontaneous seizures [43]. Most investigations have studied highgrade tumors, in particular glioblastoma, although human epilepsy develops more frequently with low-grade malignancies. Among the proposed mechanisms of epileptogenesis there are increased intracranial pressure, de-afferentation of cortical structures and modification of glial properties. However, other types of tumors besides high-grade malignant glioma models should be modeled. Similarly, inoculations of pathogenic organisms can model other acquired epilepsies, for example in neurocysticercosis [44] or malaria [45]. Hypoxia models are generated by reducing O2 to less than 10% for a few minutes/tens of minutes, which induces acute seizures and leads in adulthood to the development of spontaneous seizures and cognitive/behavioral deficits, without evidence of cell death or gliosis. This procedure leads to acute seizures and to a more robust form of epilepsy in adulthood, cognitive impairments and, unlike the pure hypoxia model, damage to different brain areas. Thus, this model produces more severe phenotypes, Conclusions the perfect model should mimic the clinical etiology (constructive validity), show the same pathophysiological and behavioral features (face validity) and respond to the same therapies (predictive validity). However, as implied by the definition of "model", there is no single model that can fully reproduce all the features of a human disease. Each model has similarities and differences from human disease, and the choice of a model depends on the particular aspect under study and on the scale of the study (low- to high-throughput). Simpler model organisms are increasingly used for screening a larger number of experimental conditions or drugs. A comparative approach can reveal aspects of epilepsy that are common in animals and thus probably shared and clinically important in humans. Close collaborations between basic scientists and clinicians are fundamental to identify which feature(s) of the pathology can be actually modeled in the different models. Infants are most susceptible to developing epileptic seizures during the neonatal period. Diagnosing neonatal seizures on clinical grounds alone is difficult because clinical manifestations are highly variable and often subtle [3]. In addition, epileptic events may be difficult to differentiate from non-epileptic movements seen in sick preterm or term babies [4]. More than half of all seizures are subclinical in the neonatal period and only electrographically evident [3, 5]. Treatment of electroclinical seizures with antiseizure medication may control clinical events, but electrographic seizures can persist (known as uncoupling or electro clinical dissociation) [6, 7]. The seizures often resolve once the underlying etiology is corrected, and so the rapid identification and treatment of the etiology is imperative. This, however, is not always easy to achieve since neonatal seizures are difficult to recognize because of their variable presentation, the need to differentiate seizures from normal neonatal movements, and co-occurring medical circumstances affecting infant survival. It is necessary, therefore, to approach the diagnosis of neonatal seizures in a consistent and organized manner. However, hypoglycemia, stroke, direct drug effect, or pyridoxine dependency can also present at this time. Over the next 72 hours to a week, causes include familial neonatal seizures, cerebral dysgenesis, cerebral infarction, hypoparathyroidism, cerebral venous thrombosis, intracerebral hemorrhage, kernicterus, urea cycle disturbances, or other metabolic disorders. Epilepsy Syndromes with Onset in the Neonatal Period Once the clinician has diagnosed neonatal epileptic seizures, the next step is to decide whether they are acute reactive seizures or part of an epileptic syndrome. Acute reactive seizures are more common, but sometimes seizure may be the first presentation of an epilepsy syndrome. In such situations, it is important to identify the syndrome and its etiology (genetic, inflammatory, metabolic, post-infectious vs. Seizure onset usually is within the first 2 days of life, but rarely within the first 6 hours. For preterm babies, vascular etiologies are the most common cause of seizures [11]. Biotinidase deficiency is a rare autosomal recessively inherited disorder affecting the recycling of biotin, an essential B vitamin that presents with intractable neonatal seizures. Glycine encephalopathy (neonatal nonketotic hyperglycinemia) typically presents with seizures on the second or third day of life. Serine deficiency, disorders of creatine biosynthesis, and phenylketonuria should also be considered as rare causes of neonatal seizures. Events of Non-Epileptic Origin Neonatal seizures must be differentiated from non-epileptic behaviors of the newborn (Table 6. When examining infants experiencing electroclinical seizures, the clinical event cannot usually be suppressed by restraint or 54 Chapter 6: Approach to the Diagnosis of Neonatal Seizures Table 6. Etiology Several, may be physiological Several, including immaturity, Undine syndrome, etc. Differential diagnosis of epileptic seizures in infancy including the neonatal period. Non-epileptic movements can often be provoked with stimulation and are typically suppressed by touching or by repositioning during the event. While stabilizing the infant, the movement should be evaluated to determine whether it is an electroclinical seizure, and then etiology should be established. The clinical evaluation should include: (1) detailed perinatal and family histories, and (2) a thorough physical examination noting head circumference, any neurocutaneous stigmata, and dysmorphic features. Antiseizure drugs should be considered complementary to treatments directed at the etiology. Rapid identification of the underlying etiology is imperative for appropriate treatment because seizures typically resolve once the neurological/metabolic disruption of the causal event is corrected. It is easily available, readily applied, and an easily interpreted method of assessment of brain function. The relative value of each neurophysiological technique is also dependent upon the availability of hardware and of professional staff trained and experienced in interpreting generated data.
Buy cheap beconase aq line
Long-term outcomes are often good allergy shots duration buy cheap beconase aq, though persistent fatigue, myalgia, and cognitive deficits have been reported. Nipah Virus Nipah virus is a paramyxovirus endemic among the giant fruit bats (Pteropus species) in South and South-East Asia and in east African coastal regions. In 1998, it caused a fatal outbreak of encephalitis among pig farmers in Malaysia, when pigs contracted the virus by consuming fruits partially eaten by fruit bats. The disease continues to cause small annual outbreaks in Bangladesh and North-East India, probably related to the local practice of consuming raw, contaminated, date palm juice. In the Malaysian outbreak, more than 60% of patients required mechanical ventilatory support and mortality was about 40%. Terminal events were often heralded by severe hypertension, tachycardia, and hyperthermia, and then irreversible shock. Nipah immunoglobulin M (IgM) serology is positive in almost all patients by day 12 of the illness, and that of immunoglobulin G (IgG) by day 26. In a nonrandomized, historical-controlled trial, ribavirin was found to reduce mortality by about 30%, though supportive treatment is equally, if not more, important [10,11]. Interestingly, myoclonus was absent in the reports of Nipah encephalitis in Bangladesh, though this could be due to reporting bias. Focal discharges are seen in about half of the patients and bitemporal periodic complexes in a quarter. Almost all patients with periodic complexes were comatose in the initial Malaysian outbreak and none survived [11,12]. About 24% had intermittent diffuse slow waves, 18% intermittent focal slow waves, and 6% showed focal slow waves and focal discharges [12]. The ominous bitemporal periodic complexes in acute infection are not seen in relapsing patients. It was first discovered in Queensland, Australia, in 1994, when it caused infection in horses and encephalitis in horse-handlers. Sporadic cases of human infections are still reported, though the transmissions from bats to horses and from horses to humans are not efficient. In a report of four patients, two recovered with no residual neurological deficit; one had relapse Hendra encephalitis 13 months after the initial acute infection. She presented with focal neurological deficits, altered conscious state, and seizures, and ultimately died [15]. These patients present with recurrence of fever, headache, focal neurological deficits, and seizures. Segmental myoclonus, prominent during acute infection, has not been seen in relapsing patients. There are more than 60 different serotypes of enteroviruses, and humans are the only host. Transmission is facilitated during warm weather; therefore, the incidence of infection is 669 Section V: Symptomatic Epilepsies of Acquired Origin high in warm countries all year round. A few serotypes predominate in a particular locality, and these cause cyclical outbreaks depending on a variety of factors, including the availability of new, susceptible hosts- usually young children. Some serotypes are more likely to cause central nervous system infection, and among these, enterovirus 71 is probably the most important as it has caused large, multiple outbreaks in the United States, Europe, Australia, and East and South-East Asia since its discovery in California in 1969. The largest outbreak occurred in Taiwan in 1998 when the virus caused a massive epidemic affecting over a million people. Clinically, enterovirus 71 affects mainly children, and those under 5 years of age are more severely affected. There is no proven antiviral therapy for enterovirus 71, though various agents have been tried, such as steroids and intravenous immunoglobulin. Other seizures and opsomyoclonus have been documented, though there are few details in the current literature. The overall outlook is good; in children without pulmonary edema or hemorrhage, mortality is close to zero. The outlook for children with pulmonary edema and/or hemorrhage is poor, however, with a mortality rate of about 80%. Remote symptomatic epilepsy is not documented in survivors of enterovirus 71 infection [16]. The rash may be florid, and may even become confluent, with associated flushing around the face, neck, and chest and islands of pale, normal skin. Leukopenia and thrombocytopenia are common, and so are bruises on the skin and subcutaneous bleeding after venipuncture. However, thrombocytopenia and vascular leakage may worsen suddenly, and hemorrhagic complications and shock arise rapidly. This is termed dengue hemorrhagic fever, and it is an indication of impending shock. Therefore, intensive observation and prophylactic replenishment of lost intravascular fluid are indicated. If not treated, the patient may progress into dengue shock syndrome, which may be heralded by intense abdominal pain, persistent vomiting, restlessness, lethargy, or hypothermia with sweating. Other uncommon, but often severe, manifestations of dengue infection include severe hemorrhage, hepatic damage, cardiomyopathy, and encephalopathy/encephalitis. Since dengue virus is closely related to other flaviviruses, the serologic test may be falsely positive in Japanese encephalitis, West Nile fever, or St. Neurological involvement in dengue infection is well documented, though whether the virus causes encephalopathy or encephalitis is still debated. Patients with neurological involvement present with confusion, altered conscious state, limb weakness, and seizures. Dengue Virus Dengue virus, a flavivirus, causes one of the most important viral infections in humans, affecting over 50 million individuals yearly, with 500 000 hospital admissions. The virus is pandemic in South and South-East Asia and South America, as well as affecting northern Australia and sub-Saharan Africa. The infection is asymptomatic in the majority of patients, especially among children. The mode of transmission is not clear, though the virus is secreted in saliva and urine. The primary infection is symptomatic in 93% of children, and the symptoms include fever, irritability, rhinorrhea, cough, diarrhea, and rash. Primary infection in immunocompetent adults or older children is rare, and may result in infectious mononucleosis-like illness, with fever, lymphadenopathy, hepatitis, or encephalitis.
Buy beconase aq 200mdi otc
Soya beans have a high content of phytoestrogens when does allergy medicine kick in buy beconase aq in india, particularly isoflavones, and are an important component of the diet in Asian countries. The high consumption of soya in these countries may be responsible for the lower incidences of osteoporosis, breast cancer, and menopausal symptoms compared to those in Western countries. Flavonoid glycosides are complex molecules found in fruits and vegetables and are converted to flavonoids by the glycosidases produced by bacteria in the colon. The flavonoids released include quercetin, rutin, myricetin, and morin which protect against the mutagenic and carcinogenic effects of other dietary components. Butyrate can also up-regulate the transcription of enzymes such as glutathione-S-transferases which can detoxify a number of carcinogens thereby helping to reduce the risk of cancer. Protection against exogenous pathogens It has long been known that germ-free animals such as mice and rats are considerably more susceptible to infection by intestinal pathogens, which implies that the gut microbiota plays a crucial role in protecting its host from such infections. The means by which this is achieved can be broadly classified into two categories: (1) Direct interactions between the gut microbiota and pathogens and (2) enhancement of host defense mechanisms by the gut microbiota. The mechanisms involved include production of antimicrobial compounds that kill or inhibit the growth of pathogens, alteration of the local environment so that it is no longer conducive to the growth of pathogens, consumption of important nutrients thereby preventing the growth of pathogens, preventing the expression of virulence genes by the pathogen, and preventing adhesion of the pathogen to its usual site within the host. Alteration of the local environment can be achieved by a number of microbial activities. Oxygen consumption by facultative anaerobes creates atmospheric conditions unsuitable for virulence gene expression by Sh. The low pH of the colon of breast-fed infants resulting from acid production by Bifidobacterium spp. Butyrate production by many gut bacteria inhibits virulence gene expression in Salmonella spp. The fucose released from mucins by many species inhibits virulence gene expression in enteropathogenic E. The mucus layer on the surface of the gut epithelium is an important host defense mechanism because it prevents microbes reaching the underlying epithelium. Recently this mucus layer has been shown to have a high content of bacteriophages which are maintained there by interactions between mucin and proteins on the phage capsids. The concentration of phages in mucus appears to be four times greater than in the luminal contents. The phages prey on any bacteria that adhere to the mucus layer and so reduce the likelihood of them reaching the epithelial surface. This symbiosis benefits the phages because it enables more frequent interactions with their bacterial hosts and benefits humans by protecting against bacterial infection of the epithelium. Development and maturation of the intestinal mucosa and immune system the key role played by the microbiota in the development and maturation of the intestinal mucosa and immune system has been demonstrated by studies in germ-free animals. Some of the abnormalities, such as decreased mucus production, can be rectified by simply administering bacterial components such as lipopolysaccharide or peptidoglycan. However, our understanding of the mechanisms by which the absence of microbes induces these deficiencies, or how their presence can correct them, is limited. Hence, the number of intraepithelial lymphocytes expands greatly, germinal centers with antibody-producing cells appear in follicles and in the lamina propria, the levels of circulating antibodies increase, and increased quantities of IgA are secreted into the gut lumen. Many studies have shown that the gut microbiota stimulates the secretory IgA system and B lymphocyte function in general. In mice, for example, bacterial colonization soon after birth induces the development of IgAsecreting cells in the small intestine. Furthermore, during weaning, with its associated increase in diversity of the gut microbiota, the number of IgA-secreting plasma cells characteristically increases. Another change associated with weaning in mice is a dramatic increase in the production of a potent antimicrobial peptide, angiogenin-4, by Paneth cells. In contrast, germ-free mice never produce high levels of angiogenin-4 which implies that its expression is under the control of the gut microbiota. The deficiency can be reversed by inoculation of the germ-free mice with the gut microbiota. Infections caused by individual members of the microbiota of the gastrointestinal tract: Hel. In developing countries, most children are infected before the age of 10 whereas in developed countries infection in children is unusual but becomes more common in adulthood. Two researchers in Australia, Barry Marshall and Robin Warren, thought differently. They had noticed the association between what was then known as "pyloric campylobacter" and gastritis and were convinced that there was a causal relationship between the two. The organism should be found in all cases of the disease and should be present in the lesions of the disease. Inoculation of the pure culture into a susceptible animal should result in a similar disease. It should be possible to recover the organism from the lesions of the diseased animal. Marshall and Warren had evidence to satisfy the first two of these postulates, but not the last two. Then, in 1984, Marshall decided to use himself as a guinea pig to obtain evidence that satisfied postulates 3 and 4. Firstly, he had biopsies taken from a number of regions of his stomach to establish that he had no inflammation or abnormalities and was not colonized by Hel. After 5 days, he started to have bloating and fullness after his evening meal, his appetite decreased and he started to vomit clear watery liquid each morning. Biopsy samples from his stomach revealed severe gastritis, many polymorphonuclear cells and the presence of helical bacteria adhering to the epithelial cells. In 2005 Barry Marshall and Robin Warren were awarded the Nobel prize in Physiology or Medicine "for their discovery of the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease. Secondly, its outer membrane covers the flagella and so masks these important antigenic constituents, which again, helps it to avoid provoking an immune response. As well as these immune-evasion mechanisms, the organism has a number of additional virulence factors and these are listed in Table 9. An obvious possibility is that the organism is more effective at competing for iron than mammalian cells and therefore deprives its human host of this essential element. If not treated, the disease progresses to chronic gastritis which may affect the whole stomach (pangastritis) or be predominant in the antrum or corpus regions. Patients with diffuse gastritis have severely impaired acid secretion and this allows Hel. The progression from gastritis to carcinoma occurs over many years so that most patients with gastric cancer are middle aged or older. However, factors such as smoking and diet increase the risk of developing the disease. Eighteen of the studies involved Western populations and nine involved Eastern (Iran and China) populations. Recently it has been reclassified as Clostridioides difficile and as a member of the Peptostreptococcaceae family. It is no longer regarded as being a species within the genus Clostridium but it remains a member of the class Clostridia within the phylum Firmicutes. Major risk factors for colonization by the organism are antibiotic administration (particularly ampicillin, amoxicillin, cephalosporins, clindamycin, and fluoroquinolones) and hospitalization and this can result in either asymptomatic carriage of the organism or clinical disease. Disease ranges in severity from mild diarrhea to life-threatening pseudomembranous colitis, the symptoms of which include diarrhea, abdominal pain, fever, nausea, vomiting, and leukocytosis.
Purchase beconase aq visa
Disorders of potassium homeostasis also very occasionally result in seizures and will be also briefly mentioned allergy shots exercise cheap beconase aq generic. Where seizures are precipitated, this is often within the context of an encephalopathy, and associated with other neurological signs such as drowsiness, confusion, headache, and stupor. Encephalopathy is typical of disorders of sodium and osmolality, hypercalcaemia, and hypermagnesaemia. Although periodic epileptiform discharges, triphasic waves, and other epileptic abnormalities are described in some relatively specific encephalopathic situations, they are uncommon. The seizures themselves can be generalized or less often focal (the latter particularly in non-ketotic hyperglycaemia). The seizures in electrolyte disturbance are generally successfully resolved by reversing the disturbance and do not recur in the longer term unless permanent cerebral damage is caused. Sodium is the predominant extracellular cation and the main determinant of serum osmolality and extracellular fluid volume. The effects of the disturbance on brain function are responsible for the morbidity and mortality in hyponatraemia. Aetiology Hyponatraemia is the reflection of excessive total body water relative to total body sodium content. Depending on the plasma osmolality, hyponatraemia can be hypovolemic, euvolemic, or hypervolemic. Hypovolemic hyponatraemia occurs most commonly in: gastrointestinal losses (diarrhoea or vomiting), other losses (for instance with burns), renal losses (for instance with diuretic therapy, mineralocorticoid deficiency, osmotic diuresis, salt-losing nephropathies). Euvolemic hyponatraemia occurs most commonly in: Addison disease, hypothyroidism, the syndrome of inappropriate antidiuretic hormone secretion, drug therapy (notably thiazide diuretics, mannitol, sorbitol, glycine, oxcarbazepine, eslicarbazepine and carbamazepine, tolbutamide, oxytocin, desmopressin, antidepressants), and primary polydipsia (especially psychogenic polydipsia). Hypervolemic hyponatraemia occurs most commonly in: cirrhosis, heart failure, acute and chronic kidney disease, and nephrotic syndrome. In epilepsy practice, chronic hyponatraemia due to carbamazepine, eslicarbazepine or oxcarbazepine therapy is by far the most common cause of hyponatraemia. Psychogenic polydipsia is also a notable cause of hyponatraemia encountered in neurological clinics and is a risk factor for the aggravation of habitual seizures in patients with epilepsy [5]. The mechanism by which carboxamides (carbamazepine, oxcarbazepine or eslicarbazepine) induce hyponatraemia in not fully understood, and may include central and peripheral targets. These drugs may cause an altered sensitivity to serum osmolality by the hypothalamic osmoreceptors and an increased sensitivity of the renal tubules to antidiuretic hormone [11]. Hyponatraemia Hyponatraemia is usually defined as a reduction in plasma sodium concentration below 136 mmol/l [3] although different institutional laboratories have slightly differing values based on the population means of that institution. Slightly low values are of no significance, but different authorities consider values 830 Chapter 113: Electrolyte and Sugar Disturbances Table 113. Other factors also influence the occurrence of seizures and the levels at which seizures occur such as the rate of change of electrolyte values, the cause of the disturbance, and the clinical setting. When plasma osmolality is reduced, the equilibrium is maintained by either intracellular solutes passing out or water from extracellular space passing in and diluting the intracellular solutes [12]. If the solute extrusion is not adequate, water will continue to enter the brain to maintain equilibrium resulting in increased intracranial pressure and cerebral oedema leading to seizures, coma, or death. After this the brain water content progressively decreases without any change in the brain electrolyte content [13]. This is explained by loss of organic osmolytes, which are intracellular, osmotically active solutes that normally contribute substantially to the osmolality of cell water and that do not adversely affect cell functions when their concentrations change. If brain electrolytes were lost without loss of brain organic osmolytes, the increase in brain water content would be much greater [14]. The changes described above can result in acute brain swelling and thus tentorial herniation, and these pose significant risks in acute hyponatraemia. The adaptive processes result in the movement of water from the interstitial space to the cerebrospinal fluid and then the systemic circulation, and the egress of osmolytes from cerebral cells. If the decline in sodium is slow, these adaptive processes prevent oedema, but in acute hyponatraemia and where levels are very low, these processes are overwhelmed [3]. The same processes apply (in reverse) on rehydration and again if this is too fast, the osmotic demyelination syndrome occurs resulting in permanent cerebral damage. In vitro experiments have shown that low osmolarity and decreased Na+ concentration increases neuronal excitability. Furthermore in acute hyponatraemia, cerebral oedema can cause a decrease in cerebral perfusion pressure. The hypo-osmolar ionic disturbances can increase cellular excitability and facilitate epileptic activity [15]. The rapid correction of serum sodium in chronic hyponatraemia can precipitate the osmotic demyelination syndrome, which can be associated with seizures in 1% of patients [16]. This is precipitated because the process of recovery of osmolytes during correction is slower than during loss [17]. Clinical Features the major symptoms of hyponatraemia relate to central nervous system dysfunction, and are much more common in rapid falls in serum sodium or when the levels fall to very low concentrations. Symptoms include headache, confusion, seizures, weakness, restlessness, nausea, and vomiting. Seizures in hyponatraemia are most commonly encountered in acute hyponatraemia, where the sodium decreases over less than 48 hr, and this reflects the rapidity with which the brain adapts to the reduced osmolality. In one early study, patients with acute hyponatraemia (defined as less than 12 hr duration) had a 29% incidence of seizures and a 50% mortality rate, largely attributable to hyponatraemia, whereas patients with chronic hyponatraemia (3 or more days in duration) had a 4% incidence of seizures and a 6% mortality rate with no deaths attributable to hyponatraemia [19]. In a study amongst patients without epilepsy, 5% of patients with hyponatraemia <125mEq/l had seizures [20]. Children are at particular risk from cerebral oedema in hyponatraemia as their brain-to-skull ratio is larger [1], and hyponatraemia should be suspected in any child with acute seizures and especially so in those less than 6 months of age. Gender is also a factor with women said to have a 25-fold higher risk of permanent neurological damage or death from hyponatraemia than men [1], and women are also more likely to develop postoperative hyponatraemia than men. There are few general surveys of the frequency of seizures in hyponatraemia, but in one retrospective hospital series of patients without a prior history of epilepsy, 363 patients were recorded to have sodium levels below 125 mEq/ l of whom eleven had seizures thought to be secondary to the hyponatraemia. Seizures were the only neurological manifestation in those whose sodium levels were >115 mEq/l [21]. Hyponatraemia induced by drugs can result in seizures (especially thiazides and psychotropic drugs)[22,23]. However, the extent to which in epilepsy practice, the hyponatraemia induced by carbamazepine, oxcarbazepine and eslicarbazepine increases seizure frequency (if at all) is not known. It has to be said that it would be difficult to identify a small effect on seizure frequency due to hyponatraemia. Seizures are occasionally the presenting feature in hyponatraemia and can be partial or generalized. Seizures may sometimes occur iatrogenically due to the too-rapid correction of hyponatraemia. Seizures can also be part of a more widespread osmotic demyelination syndrome (previously sometimes known as central pontine or extrapontine myelinolysis) also due to too rapid a correction, with severe neurologic symptoms such as quadriplegia, pseudobulbar palsy, coma, and even death [1,26,27]. The risk of the osmotic demyelination syndrome is also greater in patients with coexisting comorbidities such as liver disease or alcoholism. Treatment the usual approach to hyponatraemia is the replacement of water and sodium in hypovolemic hyponatraemia with normal saline, fluid restriction and sometimes a diuretic in hypervolemic hyponatraemia, and by the treatment of the cause in euvolemic hyponatraemia. If the hyponatraemia is severe (<110 mmol/l; effective osmolality <238 mOsm/kg) active therapy is usually needed. Too rapid a correction of even mild hyponatraemia carries the risk of precipitating the osmotic demyelination syndrome. Hypertonic (3%) saline (containing 513 mEq Na/l) may be occasionally used, under the close supervision of a metabolic team, if seizures are recurrent or intractable. In all cases, the rise of sodium should not exceed 10 mEq/l over the first 24 hr to avoid the osmotic demyelination syndrome. Hypernatraemia Hypernatraemia is defined as a serum sodium level exceeding 145 mmol/l, and is much less common than hyponatraemia.

Generic beconase aq 200mdi otc
Frequency of Epilepsy after Neurosurgery the frequency of epilepsy in certain conditions is well known allergy forecast killeen buy beconase aq line. For example, de novo epilepsy after operative treatment of intracranial abscess is around 70%, but this would probably occur independent of the surgical technique used. It is therefore difficult to assess the real influence of surgical technique and surgical intervention on de novo epilepsy in most conditions. In the shunted cases, in this series, epilepsy was associated with a blocked shunt or haematoma [3]. Likewise the incidence of seizures after endoscopic ventriculostomy is low and usually associated with adverse events; recent papers put it at 1% [4]. Similar figures are quoted for epilepsy after operations involving the insertion of deep brain stimulating electrodes as used, for example, in movement disorder treatment with lesioning or stimulators. In a study of 716 patients undergoing posterior fossa surgery, five patients had seizures within the first 24 hours (0. The causes of these seizures were mixed and included metabolic acidosis and hypernatraemia in the first 24 hours, and between two days and fourteen days seizures were associated with shunting for hydrocephalus and remote supratentorial haemorrhage [5]. Seizures following posterior fossa surgery have been associated with the occurrence of air embolus in the sitting position, a practice now rare [6]. In a study of early postoperative seizures (within three weeks of surgery) among 128 patients with chronic subdural haematomata, the incidence was 5. In the mixed-density group, in which there was more active bleeding, epilepsy was most likely. In 118 craniotomies reported from Canada, performed for a miscellany of reasons, there were 87 patients who had not experienced seizures before surgery and 11 of these had seizures within the first week after operation (12. Late-onset seizures were reported in 8% of patients undergoing craniotomy for astrocytic tumours [10]. In a series of 107 children undergoing craniotomy for a variety of causes, half of whom were receiving prophylactic anticonvulsants, 13 patients (12%) developed epilepsy within 12 months [10]. In another study involving 538 patients, epilepsy after operation occurred in 23 patients (4. Among 72 palliative craniotomies for glioblastoma multiforme, there 535 Section V: Symptomatic Epilepsies of Acquired Origin were 17 patients (23. It is interesting to compare the incidence of epilepsy in treatment modalities for the same condition which involve an intracranial approach with those which involve some other approach. In patients with precocious puberty and a hypothalamic hamartoma, but no epilepsy, where the hamartomas are usually pedunculated, surgery is rare, though in these cases there is no postoperative epilepsy and the surgery is mostly extracerebral [12]. The treatment of subarachnoid haemorrhage provides an interesting study in de novo epilepsy after neurosurgery. The International Study of Unruptured Intracranial Aneurysms quoted a pre-treatment incidence of 4. However, these studies suggest that treatment increases the likelihood of epilepsy and that there is an increased risk, probably about 5%, with open intervention [16]. Pathophysiology this is a broad and complex topic, bearing in mind the wide range of neurosurgical procedures both in terms of their underlying pathology, the severity of the intervention, and the region of the brain involved. There are few specific studies of these matters, and some of these have already been alluded to . A combination of the severity of the underlying disease and anaesthetic conditions may produce a metabolic derangement such as hypoxia or electrolyte imbalance which could cause generalised convulsions. There may also be a secondary effect whereby acute cerebral oedema is produced, itself significantly lowering the threshold for seizures. This is mirrored by the ability of chemicals, such as ferric chloride or penicillin, to produce an epileptic focus when applied to the cerebral cortex of experimental animals. Another analogous clinical situation is the epileptogenic properties of the ring of haemoglobin breakdown products on the periphery of cavernomas. Studies of post-traumatic epilepsy with modern imaging techniques have shown the relationship between cortical damage, in particular cortical contusions, and posttraumatic epilepsy. There is a similar mechanism with cerebral abscesses, which are surrounded by intense gliosis and have a 75% incidence of epilepsy. It is therefore clear that the underlying pathology will be one of the major factors which determine whether a patient will develop de novo epilepsy after neurosurgery. Finally, it is evident from clinical experience that there are genetic and other factors which influence the development of epilepsy. For example, the same or similar size meningiomas in the same location may cause raised pressure in one patient, neurological deficit in another, and seizures in a third. Again, series of patients operated upon for arteriovenous malformation show that the overall incidence of seizures before and after surgery is the same, some patients having lost their preoperative seizures and others having gained them after surgery. The influence of these factors is at present impossible to assess in any individual patient. The avoidance of conditions which provoke seizures such as haemorrhage and infection will reduce the incidence of epilepsy. Meticulous handling of tissue and minimal retraction will discourage gliosis and avoid damage to passing vessels which can produce distant lesions. Subpial dissection eliminates islands of gliotic tissue and also protects the adjacent underlying cortex and vessels from damage, and therefore should be used wherever possible. Risk Factors for Epilepsy in Disease As already suggested there are some, as yet undefined, genetic factors which determine whether epilepsy develops in an individual patient. Outside of this, the location of the lesion and the nature of the lesion, particularly if it is destructive, will be potent factors in determining whether epilepsy develops. Although it might be thought that progressive lesions would be more likely to be associated with epilepsy than stationary ones, it must be remembered that even static lesions can slowly mature and produce lesions. The account above of the 536 Chapter 75: De Novo Epilepsy after Neurosurgery frequency of epilepsy illustrates how this varies with various conditions and increases with the complexity of the lesion. Types of Epilepsy Accounts of this in the literature are sparse, but correspond to general principles and personal experience. The seizures which occur soon after the procedure, say within 48 hours, are likely to be generalised seizures because they are likely to relate to generalised brain dysfunction such as cerebral oedema. By contrast, later seizures relating to localised brain dysfunction are likely to be complex partial seizures. The literature on cerebral tumours suggests that late postoperative seizures are more likely to be partial seizures and may be more difficult to control. Principles of Management Management of the underlying condition is important and in some circumstances further surgery may be needed. One of the clearest predictors of success in surgery for drug-resistant epilepsy is the presence of a discrete, resectable lesion and this has also been noted in surgery for gliomas where one author reports that complete resection is less likely to be followed by seizures. The majority of lesions encountered in this circumstance are of natural origin such as cortical dysplasia or benign tumours, but even these are sometimes not completely removed when they could be. However, there are other conditions, such as cerebral abscess, where the primary treatment may not be surgical or the surgical management may not involve resection. Drug Treatment this is a complex matter and individual advice about drug regimes is not appropriate to a review of this nature. Suffice it to say that most would agree that initially monotherapy is preferred to polytherapy. For generalised seizures, the first choice is probably sodium valproate or, if unsuccessful, lamotrigine, and for complex partial seizures, carbamazepine, or if unsuccessful, valproate or phenytoin. More detailed advice can be found in Dulac and colleagues [2] and an account of the clinical evidence for the use of various drugs is given by Glauser and colleagues [6]. Because of the many other considerations such as age, sex, co-existent disease, and so on, it is clearly essential for the non-specialist practitioner to seek advice in any individual case. Likewise the treatment of status epilepticus, which might arise in the immediate postoperative period, requires careful and expert management. They concluded that patients older than 2 years should not receive perioperative prophylaxis and in those younger than 2 years, further study was required [23].

Mint oil (Japanese Mint). Beconase AQ.
- Dosing considerations for Japanese Mint.
- Irritable bowel syndrome, itching, hives, mouth inflammation, rheumatic conditions, common cold, cough, fever, tendency to infection, nausea, sore throat, diarrhea, headaches, toothaches, cramps, earache, tumors, sores, cancer, cardiac complaints, sensitivity to weather changes, intestinal gas (flatulence), inflammation of the airways such as bronchitis, muscular pain (myalgia), ailments associated with nerve pain, and other uses.
- Are there safety concerns?
- How does Japanese Mint work?
- What is Japanese Mint?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96610
Buy on line beconase aq
The mucosa is folded into ridges known as rugae which enable the vagina to expand allergy symptoms cough phlegm order beconase aq 200mdi online. Migrating lymphocytes and Langerhans cells are also present throughout the mucosa. Non-keratinized, stratified, squamous epithelium Mucus layer the anatomy and physiology of many regions of the reproductive system are dependent on the sexual maturity of the individual and vary during the reproductive cycle the epithelium is constantly undergoing remodeling during the female reproductive cycle and this involves the proliferation, maturation, and desquamation of cells. Various phases within this cycle are recognized- follicular, luteal, ovulation, and menstruation. Cross section through the wall of the vagina showing the typical stratified, squamous, non-keratinized epithelium and the mucus layer that coats the epithelium. The cultured cells form multi-layered structures similar to those seen in vaginal biopsies from healthy individuals. Diagram showing the changes that occur during the female reproductive cycle with respect to: (1) the development of an oocyte in the ovary, (2) body temperature, (3) hormone levels, and (4) the endometrium (the mucosa lining the inside of the uterus). Note that these are average values; duration and values may differ between different females or in different cycles of the same individual. Diagram illustrating the difference in thickness of the vaginal mucosa in pre-menopausal (left image) and postmenopausal (right image) females. The vagi nal mucosa is much thicker in pre-menopausal individuals than in post-menopausal individuals. This marks the boundary between the squamouslined ectocervix and the columnar-lined endocervix. The ectocervix is covered by a stratified, squamous, nonkeratinized epithelium similar to that present in the vagina. This type of epithelium extends into the cervical canal for a distance which varies depending on the age of the individual. Unlike the mucosa of the uterus, the cervical epithelium is not shed during menstruation. For example, the quantity of mucus secreted increases tenfold when the level of estrogen peaks at mid-cycle. Following ovulation, the increased level of progesterone causes less mucus to be produced and it becomes more viscous so that it forms a plug which seals the canal. Consequently, the environments within these organs are markedly dependent on the sexual maturity of the individual. These environmental fluctuations will, in turn, affect the composition of the resident microbial communities. The environments within the various regions of the vulva are also likely to be affected by hormonal fluctuations although less is known about this. The mons pubis and the labia majora have the innate and acquired defense mechanisms typically present in skin whereas the labia minora, clitoris, and vestibule have defense mechanisms similar to those found at other mucosal surfaces. The partial pressure of oxygen in the vagina of healthy individuals during menstruation is approximately 4 mm Hg which is 2% of that present in air and 10% of that found in tissue cells. However, oxygen levels in the vagina vary during the menstrual cycle, with lower levels being found in mid-cycle. The vaginal ecosystem, therefore, can be regarded as predominantly microaerophilic. For example, the insertion of a contraceptive diaphragm results in an increase in the partial pressure of oxygen to approximately 82% of that present in air. Also, the insertion of a tampon increases the oxygen content of the vagina to a level similar to that found in air-the concentration then decreases slowly and returns to normal after approximately 8 hours. This could have a profound effect on the vaginal microbiota and may encourage the growth of aerobes and facultative organisms such as Staph. The pH of the vagina correlates strongly with the sexual maturity of the individual (Table 7. In neonates the estrogen level is high due to a corresponding high level in the mother. This results in neonates having a thick vaginal epithelium with a high glycogen content and a low pH (approximately 4. The estrogen level then declines until, after approximately 3 weeks, the vaginal epithelium becomes thinner and the glycogen content lower. At the onset of menstrual flow the pH is almost neutral, it then falls during and after menstruation and reaches a minimum (<4) at mid-cycle. Pregnancy does not appear to affect the pH of the vagina which remains less than 4. Vaginal fluid is a source of a wide variety of nutrients Vaginal fluid is the main source of host-derived nutrients for the vaginal microbiota and this is produced by women of reproductive age at a rate of approximately 6 g per day with approximately 0. Consequently, it is an important source of a wide variety of nutrients and contains approximately 48 mg/g of carbohydrates, 4 mg/g of proteins, and 0. Importantly, it contains hemoglobin which could be a valuable source of iron for vaginal microbes. Although there is a plentiful and varied supply of nutrients available to microbes colonizing the vagina, certain features of the environment are unfavorable to many organisms, for example the low pH and low oxygen content. Furthermore, the range of antimicrobial mechanisms described later exert a selective effect and influence the composition of the vaginal microbiota. Like the vagina, it is predominantly a microaerophilic environment with the lowest oxygen levels (approximately 8% of that found in air) during the proliferative phase of the reproductive cycle. The pH of the cervix is generally higher than that of the vagina and ranges from 5. Both the amount of mucus produced and its water content gradually increase until mid-cycle and then decrease. For example, the immunoglobulin content is highest during the follicular phase than during the luteal phase whereas the albumin content decreases significantly prior to , and during, ovulation then increases. A large variety of proteins (approximately 200) have been identified in cervical mucus and one study has reported that 38 of these are present at all stages of the menstrual cycle. The presence of polysaccharides was revealed by staining with fluorescent wheat germ agglutinin which stains polysaccharides blue. The main nutrient sources for microbial colonizers vary with the exact location within the vulva but include vaginal secretions (see Table 7. The anatomy and physiology of the vulva depend on the degree of sexual maturity and will vary during the menstrual cycle. Consequently, the environmental determinants operating in the vulva will fluctuate in a similar manner. Other factors that affect the vulval environment, particularly with respect to the moisture content and pH, include the type of underwear worn, panty-liner use (type used, frequency of use, length of use), use of genital deodorants, and the frequency and type of hygiene practices employed. However, several studies have now demonstrated the presence of microbes in the uterus of non-pregnant and pregnant females. It is, of course, very important to maintain these upper regions devoid of pathobionts and exogenous pathogens in order to protect any fertilized ovum from infection. The cervix is the main potential entry route for microbes and has a variety of antimicrobial defense mechanisms to prevent ingress of microbes from the heavily colonized lower genital tract (Table 7. The thick layer of mucus coating the cervical epithelium is a physical barrier to microbes and hinders their access to the underlying epithelium. The carbohydrate moieties on the mucins present in mucus act as receptors for many of the adhesins present on microbes and so trap them within the mucus layer. Mucus was stained for IgA (green) and IgG (red) and also with wheat germ agglutinin (blue) to show the presence of mucus polysaccharides. The mucus also contains a variety of antimicrobial peptides secreted by the underlying epithelium and these are able to kill entrapped bacteria or inhibit their growth. Any microbes that do eventually arrive at, and adhere to , the underlying epithelium do not remain there for long as they will be regularly removed by desquamation. Unlike at other body sites, however, the effectiveness of many of these defense mechanisms varies markedly during the menstrual cycle. For example, the quantity of mucus secreted increases tenfold at mid-cycle while its viscosity reaches a minimum just before ovulation. Furthermore, the concentrations of many of the antimicrobial compounds in cervical mucus vary throughout the cycle (Table 7.
Syndromes
- Unpleasant taste when biting down on or near the area
- Problems with digestion or absorption
- Fluids through a vein (IV)
- Fluid buildup in the nose
- Shoulder impingement syndrome, to make more room for the shoulder to move around
- Get physical activity and enough rest.
Purchase cheap beconase aq on line
The neurological disorder may also develop without clinically apparent crises at any age allergy forecast last week generic 200mdi beconase aq free shipping. Significant behavioural problems, including anxiety, are frequently reported [30]. Over 150 different mutations of the three known genes E1, E1 and E2 cause the classic or intermediate clinical phenotype [31]. The pathogenesis is due to the neurotoxicity of leucine and of its transamination product 2-ketoisocaproic acid, and to energy deprivation due to inhibition of Krebs cycle by accumulation of branched-chain ketoacids [33]. Patients with maple syrup urine disease rarely exhibit seizures without first presenting with coma or hypoglycaemia. Isolated 3-methylcrotonyl-CoA carboxylase deficiency shows a variable phenotype ranging from severe neonatal onset with infantile spasms and hypsarrhythmia, other seizure types, and hypotonia, to asymptomatic adult forms. Elevated excretion of 3-methylcrotonylglycine and 3-hydroxyisovaleric acid is present. In organic acidurias, myoclonic jerks and other types of seizures are often observed in the acute systemic decompensation, but as in propionic acidaemia, they can also occur during the long-term course of disease [35]. Clinical findings include mild psychomotor delay in the first years of life, followed by progressive cerebellar ataxia, dysarthria, mental deterioration, pyramidal and extrapyramidal signs, seizures and macrocephaly. The severe neonatal or early infantile onset form is characterized by severe generalized hypotonia, irritability, developmental delay, generalized, mostly tonic, seizures, lethargy, cardiomyopathy and dysmorphic features including a flat face with broad nasal bridge and ear abnormalities. Patients with a mild phenotype exhibit 266 Chapter 35: Organic Acid and Amino Acid Metabolism Disorders psychomotor retardation, macrocephaly, and hypotonia [42]. Typical neuroradiological findings include enlargement of the lateral ventricles, subependymal cysts, and delayed myelination [43]. The biochemical marker of this disorder is a persistently elevated urinary excretion of D-2-hydroxyglutaric acid with mildly increased urinary 2-ketoglutarate, succinate, fumarate, lactate, and L-2-hydroxyglutaric acid. The most constant clinical features are developmental delay, hypotonia, and intellectual disability. Seizures, ataxia, behavioural problems and hyporeflexia are reported in nearly half of patients. Magnetic resonance imaging typically reveals bilaterally increased T2-weighted signal in the globi pallidi, with variable involvement of the white matter and dentate nuclei in the cerebellum. In contrast to other organic acidurias or other metabolic disorders, in this defect metabolic acute decompensation or intermittent vomiting, ataxia and altered mental status are not reported. In contrast to the progressive course of inherited metabolic diseases, ataxia is not progressive and has been reported to improve with age. The inclusion of selective ion monitoring mass spectrometry for 4-hydroxybutyric acid in organic acid analyses has increased the number of diagnoses. Dicarboxylic aciduria, with elevations of glutaric, adipic and suberic acids, occurs secondarily to the inhibition of mitochondrial -oxidation and these elevations may mislead the investigator, but the accumulation of 4-hydroxybutyric aciduria is specific to succinic semialdehyde dehydrogenase deficiency. This drug has been widely used in succinic semialdehyde dehydrogenase deficiency but its long-term clinical efficacy appears to be marginal [44,45]. Valproate is contraindicated as it may inhibit any residual succinic semialdehyde dehydrogenase enzyme activity. Disorders of Phenylalanine and Biogenic Amine Metabolism Diagnostic assessment should also consider diseases that are usually tested in newborn screening programmes as false negatives are possible, and not all countries have implemented neonatal screening programmes. Untreated phenylketonuria subjects constantly exhibit delayed developmental skills and a mousy odour is detectable in the urine; infantile spasms with hypsarrhythmia, often with progressive microcephaly, begin after the first few months of life in one-third of infants. However, neurotransmitters are involved in a wide spectrum of neurological diseases. Note the widespread areas of white matter abnormality, manifested as high signal intensity lesions. Rare disorders of monoamine metabolism are aromatic Lamino acid decarboxylase deficiency and tyrosine hydroxylase deficiency. Seizures may be difficult to differentiate from oculogyric crises and paroxysmal dystonia. Typically, the patients initially receive a diagnosis of cerebral palsy, epilepsy, or hyperekplexia. In both defects neuroimaging is generally unremarkable or can show progressive cerebral atrophy in the advanced stages [46,47]. Disorders of Biotin Metabolism Multiple Carboxylase Deficiency (Biotinidase and Holocarboxylase Synthetase Deficiency) Seizures and developmental delay are often combined in inborn errors of metabolism but usually do not cluster to produce specific syndromes. In some metabolic defects, however, highly specific symptoms can be excellent clues to diagnosis. In multiple carboxylase deficiency (holocarboxylase synthetase deficiency and biotinidase deficiency) characteristic manifestations are cutaneous symptoms, such as skin rash and alopecia, seizures, ataxia, hypotonia, impaired consciousness and metabolic acidosis [3]. In biotinidase deficiency, low doses of biotin stop seizures and, if started early, can prevent brain damage [48]. Biotinidase deficiency is a metabolic disorder characterized by the inability to recycle biotin and hence multiple carboxylase deficiency. Age at onset of symptoms varies from 1 week to 2 years, with median and mean ages of 3 and 5. Neurological manifestations are major features, with seizures occurring in over 50% of patients often as the presenting and only manifestation, which makes testing for biotinidase deficiency warranted in any patient with unexplained seizures. In some patients, they only occur during fever or intermittently only in some periods. Ataxia is also a prominent feature and may also be intermittent; hypotonia is being observed in over half of patients and development may be delayed. Other common initial symptoms include seborrhoeic or atopic dermatitis, partial or complete alopecia and conjunctivitis. Most untreated patients experience a progressive encephalopathy with psychomotor regression and bulbar symptoms; 75% of the patients have ketolactic acidosis at some time with lethargy leading to coma and eventually death. Breathing problems such as hyperventilation, stridor or apnoea, sensorineural hearing loss and visual loss associated with optic atrophy have been reported [4,3,49]. Early diagnosis and treatment with biotin may result in complete control of epilepsy. Metabolic abnormalities in biotinidase deficiency include lactic acidaemia and characteristic organic aciduria that consists of 3-methylcrotonylglycine, 3-hydroxyisovaleric acid, 3hydroxypropionic acid and 2-methylcitric acid, although some patients have been reported not to have organic aciduria. Samples with biotinidase activity show a characteristic purple colour upon addition of developing reagents after incubation with biotinyl p-aminobenzoate, whereas those with little or no activity remain straw-coloured. Positive screening tests can be confirmed by a quantitative assay of enzyme activity using additional samples of serum. All affected children showed, a few hours after birth, or in the first days of life, intractable seizures and 268 Chapter 35: Organic Acid and Amino Acid Metabolism Disorders hypotonia with progressive microcephaly. It is important to recognize these disorders early, before irreversible consequences occur, since a specific therapy may be effective. Metabolic acidosis with ketosis (elevated anion gap, urine pH below 5 and positive acetest) is suggestive of organic acidurias such as methylmalonic aciduria, propionic aciduria and isovaleric acidaemia, and can also be a clue to the large number of rarer and less known organic acidurias. A positive family history (parental consanguinity and other family members having neurological disorders) together with clinical or radiological features can suggest an inborn error of metabolism or even a specific defect. Unexplained seizures in infants should prompt careful routine metabolic screening in the blood and urine with plasma amino acids and urinary organic acid analysis (Table 35. In neonates, lumbar puncture should be performed immediately to rule out infection, non-ketotic hyperglycinaemia or disorders of biogenic amine metabolism. Confirmatory tests include skin biopsy for enzyme assays on fibroblasts and molecular studies of causative genes. Extraneurologic findings can be the clue for a specific diagnostic approach in view of the relevant associated signs: (1) Disorder of the respiratory rhythm: hyperpnoea and apnoea can result from metabolic acidosis (organic aciduria), brainstem lesions, or the direct action of a toxic metabolite (hyperammonaemia in propionic and methylmalonic acidaemia and urea cycle disorders) on the respiratory centre. An early progressive head enlargement is characteristic of a few disorders (glutaric aciduria type I, Canavan disease). In 3-phosphoglycerate dehydrogenase deficiency (serine deficiency) congenital microcephaly and intractable seizures are almost always present. The list of genetically determined metabolic diseases that produce seizures in infancy is quite long (Table 35.
Purchase beconase aq online
Various stimuli may be involved including light allergy treatment and medicare order beconase aq toronto, noise, contact and self stimulations [14]. At the other end of the spectrum, epilepsy is common in older patients, at the same age range as Alzheimer-like mental deterioration. Subclinical event: posterior high voltage slow wave with superimposed fast activity followed by electrodecrement. Recently, reports have stated the possible role of genetic changes in ion channels and neurotransmitter functions. Eye elevation and deviation to the right side associated to chewing and smacking movements associated to a rhythmic high voltage irregular spike wave activity in occipital areas for 16 seconds. These cytoskeletal proteins are known to be involved in neurological disorders, in particular, Alzheimer neuropathology. Some genes in the genome are categorized as haploinsufficient, as loss-of-function variants of one allele result in a recognizable phenotype. It has been argued that haploinsufficient genes are also sensitive to three copies and are thus good candidates for contributing to some of the phenotypes in full or partial trisomies. It is noteworthy that the 4-week period of spasm cessation required to achieve a primary clinical response to treatment in this study suggests that the effect seen might be sustained, but this needs to be confirmed at the 18-month follow-up. There is no contraindication reported to date for the classical antiepileptic compounds. There is also a higher incidence of acute leukemia than in the general population, which requires specific treatment. Stafstrom Definitions, Genetics, and Epidemiology Fragile X syndrome is the most frequent cause of inherited intellectual disability and the second most common cause of intellectual disability after Down syndrome. It is also the most common known single gene mutation implicated in autism spectrum disorder. Onefourth to one-third of patients with X-linked mental retardation have fragile X syndrome. It is named for the presence of an unstable site on the long arm of chromosome X [3,4]. Males with premutations are generally normal intellectually and phenotypically though some have mild cognitive impairment. About one-third of carrier females are impaired mentally or have social or emotional dysfunction. Some females with premutations have a syndrome of premature ovarian insufficiency [8]. Most commercial laboratories employ both methods, as recommended by the American College of Medical Genetics [10]. Other indications for genetic testing include: (1) individuals seeking reproductive counseling who have a family history of fragile X syndrome or a family history of undiagnosed intellectual disability, (2) fetuses of known carrier mothers, (3) affected individuals or their relatives in context of positive cytogenetic fragile X test (older, less accurate than current testing) who are seeking counseling related to risk of carrier status among themselves or their relatives, (4) women with reproductive or fertility problems associated with elevated follicle stimulating hormone levels, especially those with a family history of premature ovarian failure, fragile X syndrome, or undiagnosed intellectual disability, and (5) men or women with late-onset intention tremor and cerebellar ataxia of unknown origin, especially with family history of movement disorders, fragile X syndrome, or undiagnosed intellectual disability [11]. Clinical Features, Pathology, and Physiology Clinical features of fragile X syndrome vary widely, and include cognitive, behavioral, and morphologic signs and symptoms. Phenotypically, individuals with fragile X syndrome may have a long, narrow face with prominent ears and forehead, protruding mandible, high arched palate, macroorchidism (after puberty), and hyperextensible joints. Neurobehavioral symptoms may include moderate to severe intellectual disability, hyperactivity, social anxiety, sensory hypersensitivity, autism spectrum disorder, gaze avoidance, socialization difficulties, stereotyped movements and behaviors such as hand flapping and rocking, poor motor coordination, delayed speech development, and echolalia. Heterozygous females typically present with only learning disabilities or difficulty with emotional regulation. In addition to the clinical features of the disorder itself, concurrent medical problems that occur more frequently in individuals with fragile X syndrome include strabismus, otitis media, sinusitis, gastroesophageal reflux disease, and seizures [12]. Anatomically, macroscopic brain structure is usually normal in fragile X syndrome, but brains of some affected individuals have an abnormally large caudate nucleus or decreased volume of specific structures. Similar neuroanatomical findings are also seen in autism spectrum disorder [15], which is present in as many as half of individuals with fragile X syndrome [16,17]. All of the anatomic structures that reveal volumetric abnormalities in fragile X syndrome are involved in social cognition [18]. Microscopically, in fragile X syndrome, dendritic spines are abnormally long, thin, and tortuous [19], hallmarks of dendritic immaturity associated with aberrant synaptic plasticity [20]. During a critical developmental period, thalamocortical synapses are disrupted in Fmr1 knock-out mice [22]. Fmr1 knock-out mice display aberrant forms of synaptic plasticity including increased long-term depression and decreased long-term potentiation [20,23,24]. ImGluR(v) is a cation-mediated, voltage-activated non-inactivating current that enhances depolarization of the dendrite (thin arrows) and modulates cellular excitability. A family of proteins called Homer acts as scaffolds, anchoring mGluR to other postsynaptic structural proteins. The interaction of the Homer family of scaffolding proteins that regulates mGlu5 localization to synapses has been implicated in contributing to the pathophysiology of fragile X syndrome and other neurodevelopmental disorders. Mice with an mGluR5 knockin mutation, interrupting binding of mGluR5 to Homer, were found to mimic many phenotypes seen in human fragile X syndrome mice including protein synthesis rates, neocortical hyperexcitability and audiogenic seizures [29]. In Fmr1 knockout mice, the abnormal phenotype (including audiogenic seizure susceptibility) can be rescued by selective restitution of the wildtype pattern of Homer proteins [30]. These interneurons have dampened inhibitory control over their excitatory targets, potentially contributing to epilepsy in fragile X syndrome [39]. In a survey of 1394 children with full-mutation fragile X syndrome, seizures were found in 14% of males and 6% of females [48]. The presence of seizures corresponded to a much higher likelihood of autism spectrum disorder. The peak age of seizure onset is 2 years, with most seizures beginning between 6 months and 4 years of age [44]. Among individuals with fragile X syndrome, this type of epilepsy has a good prognosis Table 59. The Fragile X Clinical and Research Consortium database, which gathered data from children and adults with fragile X syndrome at nine specialty clinics between 2005 and 2011, showed a seizure prevalence of 10% with a male predominance [46]. Seizures occur more frequently in fragile X syndrome than in the general population, but not more frequently than in males with developmental delays of unknown cause. In addition to individuals with full mutations, there is an increased frequency of seizures in male premutation carriers and an even higher incidence if there is comorbid autism spectrum disorder [47]. Interestingly, the severity of epilepsy does not correlate with the number of triplet repeats. However, one study showed that fragile X subjects with severe epilepsy had more pronounced facial dysmorphisms; it is unclear if this association is coincidental or causal [45]. In a study on 16 patients with fragile X syndrome and epilepsy, 12 exhibited focal seizures. The two syndromes have a different genetic basis, cognitive profile, and associated clinical features. Furthermore, not all authors have reported a benign course for seizures in fragile X syndrome; in one study, one-half of affected individuals continued to have seizures after age 20 and overall, seizures improved in only about 50% of patients [43]. A recent preliminary study of a small cohort of full mutation patients found a 15. A retrospective analysis of 90 males with fragile X syndrome who had Autism Diagnostic Observation Schedule testing demonstrated a trend towards more seizures in those with fragile X syndrome plus autism spectrum disorder (28%) compared with fragile X syndrome only (12%) [53]. The National Fragile X Survey of males over age 12 years old with full mutation fragile X syndrome showed that seizures were more prevalent when patients had autism spectrum disorder, anxiety disorder, or both [54]. The Fragile X Clinical and Research Consortium database showed a seizure prevalence of 16% in fragile X syndrome patients with autism spectrum disorder versus a seizure prevalence of 10% in patients with fragile X syndrome without autism [46]. Fmr1 knock-out mice have increased susceptibility to audiogenic and kindled seizures [55,57]. However, it is not understood why Fmr1 knock-out mice have a propensity for audiogenic seizures, since humans with fragile X syndrome do not tend to seize in response to auditory stimuli. Many of the pathophysiological features in fragile X syndrome that have been invoked to explain the cognitive deficits may contribute to the hyperexcitability underlying seizures as well. The involvement of mGluR5 receptor activation in both processes is indicated by the reduction of longterm depression, seizures, and behavioral abnormalities when these receptors are blocked or knocked out [58,59].
Order beconase aq with american express
The optimum durations of intravenous and total antibiotic courses remain to be clarified and some reports have used shorter courses [10] allergy forecast denton tx order generic beconase aq line. Some have advocated administration of antimicrobial agents directly into the abscess cavity through the drainage catheter, but there are limited data on the risks and benefits of this approach and it is not routinely recommended [56]. It should be noted that certain antibiotics can be neurotoxic and cause seizures and encephalopathy [57]. Suppurative Intracranial Disorders Combined medical and surgical treatment is usual. Medical treatment alone can be successful in those with small lesions and in the early cerebritis stage. A main aim of surgical intervention is to identify the pathogen(s) and guide antibiotic treatment. Current practice favors burr hole aspiration, usually with the use of stereotaxy or image guidance. Aspiration removes pus, decompresses, and provides material for analysis and culture. The more invasive craniotomy with resection is considered in the case of impending brain herniation, periventricular abscess location, abscess location in superficial non-eloquent cortex and in those with slow or limited response to antibiotic treatment. A meta analysis of five studies of treatment of brain abscess in superficial non-eloquent areas reported that abscess resection compared to abscess aspiration had lower postoperative residual abscess rate, lower re-operation rate, higher rate of improvement in neurological status within 1 month but not 3 months after surgery, shorter duration of postoperative antibiotics and average length of hospital stay, but no difference in mortality [55]. Brouwer and van de Beek [10] argue that no clear conclusion could be drawn because of the quality of the studies, their retrospective nature, and publication bias. Because of the risk of recurrence, regular imaging is recommended until resolution, with continuing surveillance over the next year. However, appropriate and adequate antimicrobial cover is essential if corticosteroids are given, and steroids should only be commenced under the guidance of the neurosurgeons. Although the use of hyperbaric oxygen has been reported, its role is not clear [10]. There are other mechanisms for drug interaction other than enzyme inhibition and induction. Caution is required with co-medication in any clinical setting and potential interactions should always be considered. Epilepsy Surgery Epilepsy surgery may also be considered in any focal epilepsy associated with a focal lesion if the lesion is shown to be the source of seizures and is resectable without significant risk of deficit. Epilepsy surgery can be successful in cases with intractable epilepsy secondary to previous intracranial sepsis. Patients with temporal lobe epilepsy may have a previous history of meningitis or encephalitis leading to concern whether more diffuse damage precludes epilepsy surgery. In a series from the Mayo Clinic [61], 39 of 383 patients who underwent anterior temporal lobectomy for temporal lobe epilepsy had a remote history of meningitis or encephalitis. There was a non-significant trend for worse outcome in the meningitis/ encephalitis group compared to those without (Class 1 outcomes 61. Management of Acute Symptomatic Seizures Antiepileptic Drug Treatment In bacterial meningitis, it is advisable to treat acute symptomatic seizures. Those that can be given intravenously and orally (with loading where appropriate for early efficacy) include phenytoin, phenobarbital, valproate, levetiracetam, and lacosamide. The latter two have a better profile in relation to interactions and are well tolerated. For those with acute symptomatic seizures, gradual withdrawal over weeks to months, depending on the case, is also usually advised after recovery. As appropriate, patients should be counseled not to drive for a period dependent on assessment of individual risk and advised of local driving regulations. The effect of enzyme inhibition on the half-life of the other drug on the other hand. Conversely, carbapenem antibiotics, in particular meropenem, can Acknowledgments the authors would like to acknowledge Dr. John PhilpottHoward, for his comments on the chapter published in the first edition and Dr Amanda Fife, Consultant in Medical Microbiology, for her comments and additions to the revised edition. Daniel Walsh for his comments on surgical treatment in the first and revised edition of the chapter, and Dr. Fitch M, Van der Beek D (2007) Emergency diagnosis and treatment of adult meningitis. Tikhomirov E, Santamaria M, Esteves K (1997) Meningococcal disease: public health burden and control. Cranial extradural empyema in the era of computed tomography: a review of 82 cases. Ford H, Wright J (1994) Bacterial meningitis in Swaziland: an 18-month prospective study of its impact. Jit M (2010) the risk of sequelae due to pneumococcal meningitis in high-incomecountries: a systematic review and meta-analysis. Preux P, Druet-Cabanac M (2005) Epidemiology and etiology of epilepsy on sub-Saharan Africa. Sellner J, Trinka E (2013) Clinical characteristics, risk factors and pre-surgical evaluation of post-infectious epilepsy. Carpenter J, Stapleton S, Holliman R (2007) Retrospective analysis of 49 cases of brain abscess and review of the literature. Tseng J-H, Tseng M-Y (2006) Brain abscess in 142 patients: factors influencing outcome and mortality. Koszewski W (1991) Epilepsy following brain abscess: the evaluation of possible risk factors with emphasis on new concept of epileptic focus formation. Garfield J (1960) Management of supratentorial intracranial abscess: a review of 200 cases. Van de Beek D, de Gans J, Mclntyre P, Prasad K (2007) Corticosteroids in acute bacterial meningitis. De Gans J, van de Beek D (2002) Dexamethasone in adults with bacterial meningitis. Age of meningitis or encephalitis is independently predictive of outcome from anterior temporal lobectomy. Newton There are now five recognised species of Plasmodium that naturally infect humans, but only P. Falciparum malaria is the most severe form of malaria and is responsible for most of the neurological complications, since the infected erythrocytes adhere to the endothelium of the brain. Epidemiology of Malaria It is estimated that over 1 billion persons live in areas with exposure to malaria-carrying mosquitoes. The World Health Organization estimated that in 2015 there were 214 million clinical episodes of malaria, with about 438 000 deaths [1]. The incidence fell by 37% from 2000 to 2015, with 88% of cases occurring in Africa, mainly in young children living in sub-Saharan Africa. There are differences in the clinical presentation between African children and non-immune individuals, i. Malaria retinopathy is a pathognomonic feature in African children [3], and is documented in non-immune individuals. The petechial haemorrhages consist of normal erythrocytes surrounding a ruptured cerebral vessel, appear more common in the white matter, and are associated with sequestration. The ring haemorrhage is unique to malaria, since it consists of infected erythrocytes, pigment, and monocytes surrounding a layer of uninfected erythrocytes and gliosis, encircling a central thrombosed vessel. These are circumscribed cellular reactions scattered throughout the brain, and may represent the residue of ring haemorrhages. The infected erythrocytes adhere to the post capillary venules via parasite-derived proteins exported to the erythrocyte surface that attach to ligands upregulated in the endothelium. This sequestration stimulates mediators such as cytokines and nitric oxide, causing microvascular obstruction leading to a reduction in the perfusion of brain tissue. However, frank ischaemia is rarely documented in falciparum malaria, since most patients recover without any evident sequelae. Manifestations of Falciparum Malaria the manifestations of severe falciparum malaria include coma, seizures, severe anaemia, metabolic acidosis, and, in non-immune individuals, renal impairment and pulmonary oedema.
