
Buy 50 mg azathioprine overnight delivery
Elongation of the trachea during neck extension in children: implications of the safety of endotracheal tubes spasms vs seizures buy cheap azathioprine 50mg. Movement of the distal end of the endotracheal tube during flexion and extension of the neck. The wonderful world of the windpipe: a review of central airway anatomy and pathology. Correlation between the bronchial subepithelial layer and whole airway wall thickness in patients with asthma. This bonus information about the airway can be aptly used for formulating an anesthetic plan. The main goal of this chapter is to introduce airway practitioners to normal airway anatomy, as visualized on radiography (plain film or digital radiograph) and cross-sectional imaging. The technology behind the different imaging modalities, as well as their technical differences, is briefly reviewed, with the main emphasis placed on evaluation of the airway using available radiologic studies, which most patients already have as part of their often-extensive medical workup. Familiarity with the normal anatomy and its variants is often more useful than an exhaustive list of esoteric diagnoses. Therefore our clinical examples focus on the pathologic processes involving the airway that are most relevant to anesthesiologists and include a short discussion of some common abnormalities. The macroscopic airway can be regarded as a tubular conduit for air inhaled from the nares to the tracheobronchial tree. The integrity of the airway with its natural contrast is usually referenced with respect to extrinsic compression, luminal encroachment, or airway displacement. Segmentation of the airway into the head, neck, and chest compartments is artificial but usually done, conforming to the different medical disciplines addressing the pathologies affecting these anatomic regions and for ease of discussion. This is especially important when selecting a study that will best depict the anatomic structures and pathologic processes of the airway that are of clinical interest. Computed Tomography After the discovery of x-rays, it became apparent that images of the internal structures of the human body could yield important diagnostic information. However, the usefulness of the x-rays is limited by the projection of a three-dimensional object onto a two-dimensional display. With x-rays and radiographs, the details of internal objects are masked by the shadows of overlying and underlying structures. Thus the goal of diagnostic imaging is to bring forth the organ or area of interest in detail and eliminate the unwanted information. The patient is enclosed in a gantry, and a fan-shaped x-ray source rotates around him or her. The radiation counted by the detectors is analyzed using mathematical equations to localize and characterize the tissues within the imaged section based on density and attenuation measurements. The gantry must then "unwind" to prepare for the next slice while the table with the patient moves forward or backward a distance predetermined by slice thickness. An intrinsic limitation of this technique is the time necessary for movement of the mechanical parts. Volumetric information also makes it possible to identify small lesions more accurately and allows better three-dimensional reconstruction. This is especially important when scanning uncooperative patients and trauma victims. Imaging Modalities A brief description of the different imaging modalities is presented here, starting with plain x-ray films and more currently, digital radiographs. This will enable the reader to develop a good foundation for understanding how different imaging modalities are used in modern diagnostic imaging. Conventional Radiograph (Plain Film, X-Ray) and Digital Radiograph Wilhelm Conrad Roentgen, a German physicist, discovered x-rays on November 8, 1895, while studying the behavior of cathode rays (electrons) in high-energy cathode ray tubes. By serendipity, he noted that a mysterious ray that escaped the cathode ray tube struck a small piece of paper coated with fluorescent barium platinocyanide on a workbench 3 feet away, causing a faint fluorescent glow. Different objects placed between the cathode ray tube and the fluorescent screen changed the brightness of the fluorescence, indicating that the mysterious ray penetrated objects differently. When Roentgen held his hand between the tube and the screen and saw the outline of the bony skeleton of his hand, he quickly realized the significance of his discovery. Other types of electromagnetic radiation include radio waves, radiant heat, and visible light. In diagnostic radiology, the predominant energy source used for imaging is ionizing radiation, such as alpha particles, beta particles, gamma rays, and x-rays. The science of electromagnetic waves and x-ray generation is very complex and exceeds the scope of this chapter. In principle, x-rays are produced by energy conversion as a fast stream of electrons is suddenly decelerated in an x-ray tube. The final image is dependent on the degree of attenuation of the beam by matter. Attenuation, the reduction in the intensity of the beam as it traverses matter of different constituents, is caused by the absorption or deflection of photons from the beam. The transmitted beam determines the final image, which is represented in shades of gray. An example would be bone, a high-density material that attenuates much of the x-ray beam; images of bone on radiographs are very bright or white. The conventional plain film, or x-ray, is obtained using screen film cassette technology in which the film is processed using several chemical "washes" or chemical reactions to produce a two-dimensional image of the body part under examination on a large field of view film. Instead, imaging is based on the resonance of the atomic nuclei of certain elements such as sodium, phosphorus, and hydrogen in response to radio waves of the same frequency produced in a static magnetic field environment. Every water molecule contains two hydrogen atoms, and larger molecules, such as lipids and proteins, contain many hydrogen atoms. When radio waves are applied, protons are knocked out of natural alignment, and when the radio wave is stopped, the protons return to their original state of equilibrium, realigning to the steady magnetic field and emitting energy, which is translated into weak radio signals. The time it takes for the protons to realign is referred to as a relaxation time and is dependent on the tissue composition and cellular environment. The relaxation times, T1 and T2, for each tissue type are expressed as constants at a given magnetic field strength. Imaging that optimizes T1 or T2 characteristics is referred to as T1-weighted or T2-weighted imaging. Tissue response to pathologic processes usually includes an increase in bound water, or edema, which lengthens the T2 relaxation time and appears as a bright focus on T2-weighted images. One must also remove pagers, telephones, computers, credit cards, and analog watches because the strong magnetic field can cause malfunction or permanent damage. Patients must be carefully screened for implantable pacemakers, intracranial aneurysm clips, implants. In addition to the risk of ferromagnetic objects acting as a projectile externally, producing unwanted movement internally, or causing equipment malfunction, there is also the risk of heating, which can cause severe thermal injuries to the patient. Basics of Radiograph Interpretation the aim of this chapter is to review imaging of the airway. There is, however, useful information from imaging studies of other parts of the body. For example, imaging of the brain can give information regarding intracranial pathology such as masses and mass effect, including brain herniation, hemorrhage, and hydrocephalus. Abdominal imaging provides information regarding the presence or absence of ileus, pneumoperitoneum, and mass effect. To illustrate the usefulness of radiography in evaluating the airway, we focus our discussion on the interpretation of plain films or digital radiographs of the cervical spine, chest, and neck. They are also the most relevant to anesthesiologists because a composite of these studies gives a picture of the entire airway. Although these radiologic studies are usually obtained for reasons other than airway evaluation, it is in this group of patients who are "normal" or "cleared for surgery" that one may glean important observations about the airway. With a dedicated study of the neck or cervical spine, multidimensional reconstructions from those studies allow an excellent view of the airway, usually from the nares to tracheal bifurcation. The following sections address the basics of imaging interpretation with respect to the airway anatomy and pathology. Cervical Spine Radiography Radiologic Anatomy the cervical spine articulates with the occiput cranially and the thoracic vertebrae caudally. The bony elements, muscles, ligaments, and intervertebral discs support and provide protection to the spinal cord. On a lateral radiograph of the cervical spine, one can appreciate the bony morphology of the vertebrae and the disc spaces and assess the alignment of the vertebral column very quickly. This indirectly provides information regarding the integrity of the ligaments, which are crucial in maintaining alignment of the cervical spine. Individual ligaments and muscle groups, however, all have the same or similar attenuation and cannot be differentiated from one another on a radiograph.
Buy azathioprine without prescription
The posterior vertebral body-line is more reliable than the anterior vertebral body-line spasms and pain under right rib cage generic 50mg azathioprine visa, which is often encumbered by the presence of anterior osteophytes, and must be intact. The spinolaminar line is uninterrupted, and the interlaminar and interspinous distances are uniform. The spinolaminar line is the dense cortical line representing the junction of the posterior laminae with the posterior spinous process as seen on lateral radiographs. Lateral (A), anteroposterior (B), open-mouth odontoid (C), and oblique (D) views of the cervical spine. It is defined as the space between the posterior surface of the anterior arch of C1 and the anterior surface of the dens. In atlantoaxial subluxation, the dens is invariably displaced posteriorly, which causes narrowing of the spinal canal and potential impingement of the spinal cord. Congenital occipitalization of C1 with the occiput not only limits head extension but also adds stress to the atlantoaxial joint. It has been proposed that a shorter atlanto-occipital distance decreases the effectiveness of head extension and contributes to difficult intubation. Congenital anomalies of the dens, such as hypoplasia, can result in a loss of the buttressing action of the dens during extension and subsequent compression of neural elements. Conditions that are associated with odontoid hypoplasia are Morquio, Klippel-Feil, and Down syndromes; neurofibromatosis; dwarfism; spondyloepiphyseal dysplasia; osteogenesis imperfecta; and congenital scoliosis. Physiologic anterior displacement of C2 on C3 and of C3 on C4 occurs in 24% and 14%, respectively, of children up to the age of 8 years. In a neutral position, the spinolaminar line of C2 lies upon, or up to 1 mm anterior or posterior to , the imaginary posterior spinal line. The basion (straight arrow) is the midpoint of the anterior border of the foramen magnum; the dotted line is an imaginary line extending from it. Head extension is limited by the abutment of the occiput to the posterior tubercle of C1. Similarly, in extension, the posterior translation of the C2 body is mirrored by similar posterior displacement of the spinolaminar line of C2 with respect to the posterior spinal line. In traumatic spondylolisthesis, which is rare in children but more common in adults, the C2 body would translate anteriorly in flexion and posteriorly in extension, and the posterior spinal line would be maintained because of intact ligaments. However, flexion and extension films are not advisable when traumatic spondylolisthesis is suspected. Inflammatory arthropathies involving the atlantoaxial joint with subluxation are classically illustrated in rheumatoid arthritis and ankylosing spondylitis. The underlying cause of atlantoaxial subluxation is quite different in these two entities. T2-weighted sagittal magnetic resonance cervical spine study demonstrates physiologic anterior displacement of C2 on C3 in a child. Also seen are normal soft tissue masses encroaching on the airway from adenoids (a), palatine tonsils (b), and lingual tonsils at the base of the tongue (c). In rheumatoid arthritis, there is bone erosion, synovial overgrowth, and destruction of the ligaments. Whether this condition is referred to as "cranial settling,"14 superior migration of the odontoid process, or basilar invagination, the end result is the same. In response to the effective foreshortening of the spine secondary to the superior migration of the dens, there is acquired rotational malalignment between the spine and larynx. The effective neck length can be affected by superior migration of the dens, severe spondylosis with loss of disc space, or iatrogenic causes secondary to surgery. The soft tissues of the pharynx become more redundant attributable to the relative shortening of the neck, which further obscures the view of the larynx. The presence of a rotated airway is suspected when the frontal view of the cervical spine demonstrates a deviated tracheal air column. Historically, bone landmarks other than the spine, appreciated on a lateral cervical spine x-ray study, have been used to preoperatively predict difficult laryngoscopy and endotracheal intubation based on anatomic factors. Combined with a clinical examination, anatomic measurements and findings assessed by radiography can help to alert the anesthesiologist to a potentially difficult airway. Acute cervical spine injury is often the indication for ordering a cervical spine examination. The hypertrophic bone changes associated with this condition are well depicted on x-ray studies. Large anterior osteophytes that project forward may cause dysphagia and difficult intubation. The spinal canal and neural foramina are assessed for stenosis, and, when present, precautions can be taken when hyperextending the neck and positioning the patient to avoid exacerbation of baseline neurologic symptomatology. Ossification of the anterior longitudinal ligament and diffuse idiopathic skeletal hyperostosis have been reported as causes of difficult intubation. Muscles acting on the hyoid bone elevate the larynx and provide the primary protection from aspiration. The largest cartilage in the neck is the thyroid cartilage, which along with the cricoid cartilage, acts as a protective shield for the inner larynx. The cricoid cartilage is the only complete cartilaginous ring in the respiratory system. Normal air-filled structures seen on lateral plain film are the nasopharynx, oropharynx, and hypopharynx. Any sizable soft tissue pathology results in deviation or effacement of the airway. The tongue constitutes the bulk of the soft tissue in the oral cavity and the oropharynx. In children, and sometimes in adults, prominent lymphatic tissues, such as adenoids and palatine tonsils, may encroach on the nasopharyngeal and oropharyngeal airway. The small linear dark line at the level of mid-C2 is the subdental synchondrosis (arrow). Lateral cervical spine radiograph reveals large anterior osteophytes (arrow) that indent the airway and oropharynx. The epiglottis is an elastic fibrocartilage in the shape of a flattened teardrop or leaf that tapers inferiorly and attaches to the thyroid cartilage. During the first several years of life, the larynx changes its position in the neck. However, the position of these structures in the normal population varies by at least one vertebral body level. This anterior mucosal recess is between the posterior third of the thyroid cartilage and the aryepiglottic fold. The extreme lower aspect of the pyriform sinus is situated between the mucosa-covered arytenoids and the mucosa-covered thyroid cartilage at the level of the true vocal cords. The soft tissues dorsal to the airway, the prevertebral soft tissue, are adherent to the anterior surface of the atlas and the axis and are the normal soft tissue structures of the posterior pharynx extending from the clivus to the nasopharynx and hypopharynx. Lateral radiograph of the cervical spine demonstrates a compression fracture of the C5 vertebra (arrow). Note the change in the level of the hyoid bone and the vocal cords with flexion and extension of the neck. The ligaments of the cervicocranium critical to maintaining stability throughout this region are directly involved in the range of motion of the cervicocranium and anteriorly contribute to the prevertebral soft tissue shadow. Superimposed on these deep structures are the pharyngeal constrictor muscles and the mucosa of the posterior pharyngeal wall. The cervicocranial prevertebral soft tissue contour should normally be slightly posteriorly concave rostral to the anterior tubercle of C1, anteriorly convex in front of the anterior tubercle, and posteriorly concave caudal to the anterior tubercle, depending on the amount of adenoidal tissue and on the amount of air in the pharynx. Adenoidal tissue appears as a homogeneous, smoothly lobulated mass of varying size and configuration. The anterior surface of the adenoid is demarcated by air anteriorly and inferiorly.
Discount azathioprine 50mg mastercard
In other words xanax muscle relaxer azathioprine 50mg free shipping, environmentally altered gene expression was not inherited stably through multiple generations in the absence of the environmental factor. If this phenomenon does exist in humans even though it has not yet been detected, we would need to consider that our actions, as well as our genes, might affect the traits we pass on to future generations. Paternally imprinted genes are silenced 600 Chapter 17 Gene Regulation in Eukaryotes when inherited from the father, while maternally imprinted genes are silenced when inherited from the mother. During meiosis, the old methylation marks are erased and new sex-specific methylation patterns are established. Explain how the primary transcript of a single eukaryotic gene can produce different proteins. Describe results that could be obtained from ribosome profiling that would indicate the existence of a regulatory mechanism operating at the level of translational initiation. Thus far we have discussed mechanisms that influence the frequency of transcription initiation, but many other systems exist that regulate posttranscriptional events. It is impossible to discuss all of these mechanisms in a single chapter, so we focus here on a few of the key decision points. We mentioned at the beginning of this chapter that sexspecific courting behaviors of male Drosophila are under the control of the fruitless (fru) gene. In their brains, male flies produce a male-specific form of the fru gene product, Fru-M, a zinc-finger transcription factor. Although Fru-F appears not to have a function, Fru-M elicits a program of gene expression that controls both the male mating dance and its orientation toward females. Male flies with fru mutations that block production of Fru-M still do the mating dance, but court males and females indiscriminately. However, female flies with fru mutations that cause them to express Fru-M acquire male sexual behaviors; they display the male dating dance and also specifically court females. Thus, Fru-M is redundant for the mating dance behavior in males, and Fru-M is required absolutely for males to orient that dance only toward females. Researchers are now trying to identify the transcriptional targets of Fru-M that ultimately dictate these behaviors. In females, Tra protein (with Tra2) blocks the use of one exon, causing the fru transcript to be spliced so as to encode Fru-F. The spliceosomes that assemble at the splice junction sites of primary transcripts can contain more than 100 proteins. Some of the spliceosome components are crucial -specific splicing Fru-M protein sexual behavior 17. In this section we first describe two of the eukaryotic translational regulation mechanisms that control assembly of initiation factors at the 5 cap. Intriguingly, this mechanism is partially responsible for circadian oscillations in the amounts of certain proteins at different times of day. On the other hand, if females make a different, normally male-specific protein called Msl-2, they will die. In this way, scientists can turn down the expression of any gene of interest and investigate any possible phenotypic consequences of this loss of function. Antenna Sensillae Foreleg Chemosensory axons Sex comb in male Brain Regions determining courtship behaviors More Kenyon fibers in female mushroom body mutations influence somatic sex determination came from a combination of genetic experiments (studying, for example, whether one mutation is epistatic to another) and molecular biology experiments (in which investigators cloned and analyzed mutant and normal genes). Through such studies, Drosophila geneticists dissected various stages of sex determination to delineate the following complex regulatory network. However, the underlying molecular mechanism of sex determination is different in humans and flies. In flies, maleness is the default state brought about by the presence of only one X chromosome instead of two as in females. The reason is that two X chromosomes are required to activate transcription of the Sxl gene in early Drosophila embryogenesis. We focus here mainly on the first-mentioned pathway: the determination of somatic sexual characteristics. An understanding of this pathway emerged from analyses of mutations that affect particular sexual characteristics in one sex or the other. Only in cells with two X chromosomes is the concentration of activators sufficient for Sxl transcription to occur. As embryogenesis progresses, the transcription factors that activate Sxl transcription from Pe disappear, and Sxl is transcribed instead from the maintenance promoter (Pm). In females, however, the Sxl protein previously produced by transcription from the establishment promoter Pe influences the splicing of the primary transcript initiated at the maintenance promoter Pm. The result is a feedback loop that maintains Sxl protein in females but not in males. But females with mutations in Sxl incorrectly make Msl-2 protein (as well as other dosage-compensation factors), and this causes each X-linked gene to be transcribed at twice the frequency at which it is transcribed in normal females. Because females have two X chromosomes rather than the one X in males, hypertranscription of the genes from the two X chromosomes proves lethal. The reason is that males, which do not normally express the Sxl gene, do not miss its functional product, but females, which depend on the Sxl protein for sex determination, do. The N-terminal parts of the Dsx-F and Dsx-M proteins are the same, but the C-terminal parts of the proteins are different. At the yp1 gene enhancer, Dsx-F acts as a transcriptional activator, whereas Dsx-M acts as a transcriptional repressor. In conjunction with the protein encoded by the intersex (ix) gene, Dsx-F primarily represses the transcription of genes whose expression would generate the somatic sexual characteristics of males. However, it also activates the transcription of genes that promote somatic femaleness. Dsx-M, which works independently of the Intersex protein, does the opposite; it is primarily a transcriptional activator of maleness genes, and it also represses femaleness genes. For example, both bind to an enhancer upstream of the promoter for the yp1 gene, which encodes a yolk protein; females make this protein in their fat body organs and then transfer it to developing eggs. The binding of Dsx-F stimulates transcription of the yp1 gene in females; the binding of Dsx-M to the same enhancer helps inactivate yp1 transcription in males. Mutations in dsx affect both sexes because in both males and females, the production of Dsx proteins represses certain genes specific to the development of the opposite sex. You have also learned about technologies that allow scientists to analyze individual genes and whole genomes at the molecular level. In the previous two chapters, we discussed how genes and their products are regulated, allowing a single-celled organism to respond to its environment and a multicellular organism to form different organs. In Chapter 18, you will see that genes can be inserted into or removed from the genomes of model organisms at will-any gene, indeed any base pair, in the genome can be changed at the whim of a molecular geneticist. Genome manipulation is the basis for gene therapies that hold promise for curing some human diseases. In Chapter 19, we will explore how scientists use the genetics of model organisms to dissect biological pathways. In particular, the analysis of mutants that develop aberrantly from a fertilized egg to a multicellular organism has helped uncover many details of this remarkable process. Finally, in Chapter 20, you will see how new technologies for studying genomes are revolutionizing our understanding and treatment of cancer, the most important of all genetic diseases. One of the genes whose transcription is activated by retinoic acid binding to the receptor is myoD. This means oligonucleotide 1 will cause termination of translation of the protein in either orientation, wherever it is inserted. Thus, oligonucleotide 2 will only add amino acids to the protein, and it will not change the reading frame of the protein. Insertion of the oligonucleotide can disrupt the function of a domain in which it inserts, although this will not necessarily be the case. Answer this question involves the concept of domains within proteins and the use of the genetic code to understand the effects of oligonucleotide insertions. Assume that the disease illustrated with the following pedigree is due to the phenotypic manifestation of a rare recessive allele of an autosomal gene that is paternally imprinted. Alleles of paternally imprinted genes are expressed only if they are inherited from the mother. Neither parent in generation I displays the disease, but two out of their three children do.
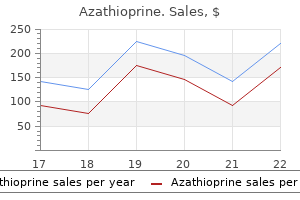
| Comparative prices of Azathioprine | ||
| # | Retailer | Average price |
| 1 | Darden Restaurants | 785 |
| 2 | WinCo Foods | 343 |
| 3 | RadioShack | 204 |
| 4 | Costco | 585 |
| 5 | AT&T Wireless | 505 |
| 6 | Aldi | 791 |
| 7 | A&P | 685 |
| 8 | Advance Auto Parts | 409 |
Buy on line azathioprine
Double-access-port endotracheal tube for selective lung ventilation in pediatric patients spasms before falling asleep buy azathioprine 50 mg. Pro: one-lung ventilation is best accomplished with the Univent endotracheal tube. The relationship among bronchial blocker cuff inflation volume, proximal airway pressure, and seal of the bronchial blocker cuff. Students may be able to witness a surgical cricothyrotomy, and possibly to assist in the performance of an elective tracheostomy, but most anesthesiologists have successfully avoided incorporating these procedures into their practice. As reported by Caplan and colleagues, and Cheney and comrades, the two major categories of anesthesia-related events or mechanisms causing death or brain damage between 1975 and 2000 were respiratory and cardiovascular difficulties, which together made up 68% of damaging events. In an analysis of claims against the National Health System in England between 1995 and 2007,4 airway and respiratory claims accounted for 12% of anesthesia-related claims, 53% of deaths, 27% of costs, and 10 of the 50 most expensive claims in the dataset. This algorithm describes emergency and nonemergency pathways for managing the airway if intubation fails and suggest that equipment suitable for "emergency surgical airway access". Definitions and Classifications Cricothyrotomy and Percutaneous Dilational Cricothyrotomy Cricothyrotomy is a technique for providing an opening in the space between the anterior inferior border of the thyroid cartilage and the anterior superior border of the cricoid cartilage for the purpose of gaining access to the airway. This area is considered to be the most accessible part of the respiratory tree below the glottis. Based on the urgency of the clinical situation, the procedure can be performed emergently or electively. The second category includes techniques requiring the introduction of a guidewire that is inserted through a needle or catheter and followed by dilation of the cricothyroid space. After an initial skin incision, sharp dissection is carried out to the thyroid isthmus, which is divided. An airway catheter is also introduced over the dilator threaded over the guidewire. The third category is surgical cricothyrotomy, which involves the use of a scalpel and other surgical instruments to create an opening between the skin and the cricothyroid space. Tracheostomy and Percutaneous Dilational Tracheostomy Open Tracheostomy Surgical tracheostomy, as described by Chevalier Jackson,18 is a surgical procedure that provides an airway through the cervical trachea. It remains the standard against which all other procedures with the same aim must be compared in terms of success and complications rates. Emergency situations were traditionally considered absolute contraindications to the use of percutaneous tracheostomy, but in the past few years, some reports have supported its safety and feasibility in selected emergent cases. It involves making a very small skin incision, introducing a needle into the trachea, and dilating the opening with sequentially larger dilators to allow insertion of a tracheostomy tube of the selected size. As originally described, this procedure was performed blind, but it is increasingly performed under continuous endoscopic guidance. Other modifications of the Ciaglia technique include the use of lower tracheal ring interspaces (originally performed in the interspace between the cricoid cartilage and the first tracheal ring) and the use of a single, curved dilator to replace the original multiple dilators. Of the percutaneous approaches described, the Ciaglia technique with continuous endoscopic visualization and use of a single dilator is considered by many to be the safest and is the most widely used in North America. The Griggs guidewire/dilating forceps technique involves placing a guidewire through an initial puncture site. The procedure as originally described is performed blind and subject to complications such as false passage and subcutaneous emphysema. Concurrent endoscopic visualization reduces these risks, although bleeding may be a problem because of tearing of adjacent structures, such as the thyroid isthmus, when inserting and opening the forceps. The Fantoni technique is based on retrograde dilation of an initial tracheal puncture. A guidewire is then passed through the needle and directed toward the oral cavity. Dilation is carried out by means of a conic cannula inserted over the guidewire through the oral cavity. The tracheostomy tube is ultimately brought out in a retrograde fashion through the cervical trachea and skin. This technique is used primarily in Italy, where it originated; however, it has found little applicability in North America because it is lengthy to perform and involves potential loss of the airway as a result of the many airway manipulations necessary to perform the procedure and secure the cannula in its final position. There are a number of different terms and acronyms used in the literature to describe this same technique. Terms such as percutaneous (or simply "trans-"), laryngeal (versus tracheal), and insufflation or oxygenation (versus ventilation) may all be appropriate. Appropriate equipment for cricothyrotomy should be available throughout the hospital or as part of an emergency airway kit. Continuing medical education is essential to maintain skills in performing emergent invasive airway access, and standardized simulation alone may not be sufficient for optimal training. Individual skills, availability of devices, and training in specific techniques may deviate from standard guidelines, making sitespecific guidelines necessary. A "threatened airway" protocol has been proposed for implementing an escalation-based model at McGovern Medical School at the University of Texas Health Science Center at Houston. Four main features constitute the cornerstones of management of a patient with a threatened airway: identification of the airway emergency and escalation of the approach to management, choice of appropriate sedation or anesthesia technique, optimal positioning, and articulation of plans for intervention. The otolaryngologist plays a critical role in airway management by contributing a skill set that is different from but complementary to that of the anesthesiologist. Circumstances may range from well-controlled elective situations to last-ditch attempts to establish an airway when all else has failed. It covers the cricothyroid space and is located in the anterior neck between the thyroid cartilage superiorly and the cricoid cartilage inferiorly. The cricothyroid space can be readily identified by palpating a slight dip or indentation in the skin immediately below the laryngeal prominence. The thicker and stronger conus elasticus narrows above and broadens below, connecting the thyroid to the cricoid cartilage. It lies subcutaneously in the midline and is often crossed horizontally in its upper third by the superior cricothyroid vessels. The two lateral parts are thinner, lie close to the laryngeal mucosa, and extend from the superior border of the cricoid cartilage to the inferior margin of the true vocal cords. Lateral to the membrane are venous branches from the inferior thyroid and anterior jugular veins. Because the vocal cords usually lie 1 cm above the cricothyroid space, they are not commonly injured, even during emergency cricothyrotomy. The anterior cricothyroid space is trapezoidal and has a cross-sectional area of approximately 2. The mean distance between the anterior borders of the inferior thyroid cartilage and the superior cricoid cartilage is 9 mm (range, 5 to 12 mm), whereas the width of the anterior cricothyroid space ranges from 27 to 32 mm. The cricothyroid space is not much larger than 7 mm in its vertical dimension, and that space may be narrowed further by contraction of the cricothyroid muscle. The vertical distance between the undersurface of the true vocal cords and the lower anterior edge of the thyroid cartilage is between 5 and 11 mm. Although the arteries always lie deep to the pretracheal fascia and are easily avoided during a skin incision, veins may be found in the pretracheal fascia and between the pretracheal and superficial cervical fascia. The importance of these landmarks is emphasized because it is disastrous to place a cricothyrotomy tube into the thyrohyoid space instead of the cricothyroid space. When the normal anatomy is distorted, identification of these landmarks is difficult. From cephalad to caudad, the thyroid notch, inferior border of the thyroid cartilage, superior border of the cricoid cartilage, and sternal notch are marked. From cephalad to caudad, the hyoid bone, thyroid cartilage, and cricoid cartilage are marked. Cricothyrotomy can also be used as an alternative to tracheostomy in patients with recent sternotomy who require invasive airway access because the incision does not communicate with the mediastinal tissue planes. Emergency cricothyrotomy has largely replaced emergency tracheostomy in the emergency department because of its simplicity, rapidity, and minimal morbidity; additionally, percutaneous techniques are replacing surgical approaches. Patients who have been intubated translaryngeally for more than 3 days (7 days according to many investigators) should not undergo cricothyrotomy because of the propensity to develop subglottic stenosis. Those with preexisting laryngeal diseases, such as cancer, acute or chronic inflammation, or epiglottitis, have a higher morbidity rate when cricothyrotomy is performed.
Buy genuine azathioprine on line
What would you predict about the progeny of two mice muscle relaxant drugs methocarbamol buy discount azathioprine on-line, both of which carried one copy of the A transgene What would you predict about the progeny of two mice, both of which were heterozygous for the C gene knockout A single transgenic copy of either gene promotes tumor growth, so the transgenes have dominant effects. A predisposition to cancer is particularly obvious when both wild-type copies of gene C are knocked out. The fact that the two transgenic oncogenes have synergistic effects is consistent with the idea that the generation of cancer involves the accumulation of mutations in more than one gene. Recall the two-hit idea that cancerous properties arise only when both copies of a tumor-suppressor gene become inactivated. Homozygotes for the knockout would have no functional copies and therefore would develop cancer relatively early in life. Heterozygotes for the knockout would be born with one remaining copy of C+, but these heterozygotes would eventually begin to die of cancer after a second hit inactivates that copy in one or more cells. Note that this latter result indicates that inheritance of a single knockout allele predisposes to cancer in a dominant fashion at the level of the organism. Homozygous knockout mice survive past birth because mutations must accumulate in several oncogenes and tumor-suppressor genes to produce cancer, not just in this one tumor-suppressor gene. Note that this tumorsuppressor gene cannot be necessary for the survival of cells. One-quarter of the progeny would not inherit any copy of the transgene, so they would develop no or very few tumors over their normal life spans. Onehalf the progeny inherit one copy of the transgene, so they would develop tumors at about the same rate as their parents (the blue line in experiment 1). One-quarter of the progeny would not inherit any copy of the knockout, so they would survive normally. One-half would inherit one copy of the knockout, so their survivability should resemble the blue line in experiment 2. The remaining one-quarter would be homozygotes for the transgene, so they would die at a rate similar to that shown by the green line in experiment 2. Propose a hypothesis to explain how the high expression of p53 saves the cells from transformation by T antigen. Each mutation alters an amino acid that is crucial for the activity of one functional domain of the p53 protein. By supplying excess p53 from the strong promoter, there is now enough p53 protein in the cell to bind to all the T antigen and still have enough unbound p53 to regulate the cell cycle. Mutants 1 and 2 are expressing large amounts of altered p53 protein, but they no longer are affected by T antigen. Mutations 1 and 2 could therefore be loss-of-function mutations that block the ability of p53 to bind T antigen. Another possibility is that mutant proteins 1 and 2 cannot function in cell cycle control but can bind sufficient T antigen to allow the endogenous p53 to function. Mutant 3 cannot rescue cells from the oncogenic effect of T antigen, so this mutation must affect a functional domain other than those that bind T antigen or that allow p53 to serve as a transcription factor for cell-cycle genes. As one of several possibilities, p53 has a domain that specifically helps it regulate apoptotic (but not cell-cycle) genes. Disruption of this domain might have no effect in normally growing cells that do not need to undergo apoptosis. Characterize the differences between tumor cells and normal cells in terms of the following properties. In cancer cells, how might each of these properties contribute to tumor progression The incidence of colon cancer in the United States is 30 times higher than it is in India. Differences in diet and/or genetic differences between the two populations may contribute to these statistics. Some germ-line mutations predispose individuals to cancer, yet often environmental factors (chemicals, exposure to radiation) are considered major risks for developing cancer. In many of these mice, skin tumors develop at the site of exposure, but only months after the chemical is no longer detectable. An extended family from Morocco in which the disease presents itself in a large percentage of family members at a very early age has come to your attention. Normally, human blood has millions of different types of B cells making millions of different kinds of antibody molecules. In the blood of patients with cancers called B cell lymphomas, almost all of the antibody molecules are all of one type, but this single type of antibody is different in different lymphoma patients. Based on this information, provide a brief description of the genesis of B cell lymphomas, focusing on the cells that are overproliferating. Molecules outside and inside the cell regulate the cell cycle, making it start or stop. What is an example of a molecule inside the cell that is involved in cell-cycle regulation The addition of ubiquitin to a protein targets that protein to be degraded by another protein complex called the proteasome. Based on the information you have been given, what evidence, if any, suggests an inherited contribution to the development of this disease You decide to take a medical history of all of the 33 people indicated in the pedigree and discover that a very large percentage drink a special coffee on a daily basis, while the others do not. Could the drinking of this special coffee 708 Chapter 20 the Genetics of Cancer a. Based on the answer you have just given for Problem 11, propose a mechanism that would allow sister chromatids to separate during anaphase. How might your proposed mechanism also explain the checkpoint operating in M phase that prevents sister chromatid separation until all the chromosomes have connected properly to the mitotic spindle Describe how you would use replica plating of mutagenized, haploid yeast cells to identify temperature-sensitive (ts) mutations in essential genes needed for yeast growth and survival. Among the many ts mutations you found in part (a), how would you distinguish mutations in genes needed for cell-cycle progression from those in genes needed for other aspects of the life of yeasts If you had a large collection of yeast cell-cycle mutants, how would you determine which of the mutations are in the same gene and which are in different genes What do these observations tell you about when during the cell cycle the protein product of the gene in question normally functions Why do you think that this particular translocation that fuses the bcr and abl genes happens independently in the somatic cells of many different people Karyotype analysis shows that the leukemic cells of this patient are heterozygous for a reciprocal translocation involving chromosomes 9 and 22. However, none of the normal, nonleukemic cells of this patient contain the translocation. The translocation results in the inactivation (loss of function) of a tumor-suppressor gene. The normal function of the affected tumor-suppressor gene or proto-oncogene at the translocation breakpoint could potentially block the function of the cyclin proteins that drive the cell cycle forward. Two rare events must have occurred to disrupt both copies of the tumor-suppressor gene or Problems 709 proto-oncogene at the translocation breakpoint in the leukemic cells. A possible treatment of the leukemia would involve a drug that would turn on the expression of the tumor-suppressor gene or oncogene at the translocation breakpoint in the leukemic cells. Describe a molecular test to determine if chemotherapy given to the patient described in Problem 19 would be completely successful. Be as specific as possible in describing the reagents you would need for the test, how you would perform it, and what the different results would show. When it is unphosphorylated, the transcription factor is inactive and stays in the cytoplasm. When it is phosphorylated by kinase A, the transcription factor moves into the nucleus and helps turn on the transcription of a mitosis factor gene whose product stimulates cells to divide. The following list contains the names of the genes encoding the corresponding proteins. What would you expect to be the effect when kinase A adds a phosphate group to the phosphatase Is the phosphatase gene likely to be a proto-oncogene or a tumor-suppressor gene or neither
Order azathioprine 50 mg line
Association of advanced airway device with chest compression fraction during out-ofhospital cardiopulmonary arrest muscle relaxer kick in 50mg azathioprine amex. Difficult Airway Society guidelines for management of the unanticipated difficult intubation. Fiberoptic tracheal intubation through the laryngeal mask in an awake patient with cervical spine injury. Use of the laryngeal mask in a patient with an unstable fracture of the cervical spine. Use of the laryngeal mask prior to definitive intubation in a difficult airway: a case report. Larynxmaske versus Intubation bei erschwerten Intubationsbedingungen beim Franceschetti-Zwahlen-Klein-Syndrom (Treacher-Collins-Syndrom). Laryngeal mask airway for management of a difficult airway and extracorporeal shock wave lithotripsy. Gum elastic bougie-guided insertion of the ProSeal laryngeal mask airway is superior to the digital and introducer tool techniques. Tracheal intubation via the Classic and Proseal laryngeal mask airways: a manikin study using the Aintree Intubating Catheter. Comparison of the reinforced laryngeal mask airway and tracheal intubation for adenotonsillectomy. Comparison of reinforced laryngeal mask airway vs endotracheal intubation in tonsillectomy. Application of a laryngeal mask to a fiberoptic bronchoscope-aided tracheal intubation. The use of readily available equipment in a simple method for intraoperative monitoring of recurrent laryngeal nerve function during thyroid surgery: initial experience with more than 300 cases. Fibreoptic bronchoscopy under general anaesthesia using the laryngeal mask airway. The laryngeal mask airway: a new standard for airway evaluation in thoracic surgery. The laryngeal mask may be a useful device for fiberoptic airway endoscopy in pediatric anesthesia. Laryngeal mask airway and fiberoptic endoscopy in an infant with Schwartz-Jampel syndrome. Anaesthesia and tracheobronchial stenting for central airway obstruction in adults. Self-positioning followed by induction of anaesthesia and insertion of a laryngeal mask airway versus endotracheal intubation and subsequent 348. Laryngeal mask airway classic as a rescue device after accidental extubation in a neonate in prone position. The use of a laryngeal mask airway for emergent airway management in a prone child. Emergency airway management with a laryngeal mask airway in a patient placed in the prone position. An unusual case of airway rescue in the prone position with the ProSeal laryngeal mask airway. Premolar loss following insertion of a Classic Laryngeal Mask Airway in a patient in the prone position. Use of the laryngeal mask airway for respiratory distress in the intensive care unit. Comparison of hemodynamic and metabolic stress responses caused by endotracheal tube and Proseal laryngeal mask airway in laparoscopic cholecystectomy. I-gel: A comparative evaluation of respiratory mechanics in laparoscopic cholecystectomy. The ProSeal laryngeal mask airway and the laryngeal tube Suction for ventilation in gynaecological patients undergoing laparoscopic surgery. Laryngeal mask airway indications: new frontiers for second-generation supraglottic airways. ProSeal versus the Classic laryngeal mask airway for positive pressure ventilation during laparoscopic cholecystectomy. The laryngeal mask airway is effective (and probably safe) in selected healthy parturients for elective Cesarean section: a prospective study of 1067 cases. Survey of accepted practice following failed intubation for emergency caesarean delivery. Laryngeal mask airway in pediatric practice: a prospective study of skill acquisition by anesthesia residents. Analysis of 1500 laryngeal mask uses by one anaesthetist in adults undergoing routine anaesthesia. Jaw thrusting as a clinical test to assess the adequate depth of anaesthesia for insertion of the laryngeal mask. Topical lignocaine and thiopentone for the insertion of a laryngeal mask airway; a comparison with propofol. Cp50 of propofol for laryngeal mask airway insertion using predicted concentrations with and without nitrous oxide. Cricoid pressure impedes placement of the laryngeal mask airway and subsequent tracheal intubation through the mask. Gum-elastic bougie-guided insertion of the ProSeal laryngeal mask airway: a new technique. Gum elastic bougie-guided insertion of the ProSeal laryngeal mask airway is superior to the digital and introducer tool techniques in patients with simulated difficult laryngoscopy using a rigid neck collar. Techniques for the insertion of the ProSeal laryngeal mask airway: comparison of the Foley airway stylet tool with the introducer tool in a prospective, randomized study. Use of the Laryngeal Mask Airway in patients positioned prone for short surgical cases in an ambulatory surgery unit in the United States. The proseal laryngeal mask airway in prone patients: a retrospective audit of 245 patients. Incidence of and risk factors for difficult ventilation via a supraglottic airway device in a population of 14,480 patients from South-East Asia. A proposal for a new scoring system to predict difficult ventilation through a supraglottic airway. Malpositioning of supraglottic airway devices: preventive and corrective strategies. Prospective clinical and fiberoptic evaluation of the Supreme laryngeal mask airway. Randomized crossover comparison of the proseal with the classic laryngeal mask airway in unparalysed anaesthetized patients. Fewer sore throats and a better seal: why routine manometry for laryngeal mask airways must become the standard of care. Complications with supraglottic airways: something to worry about or much ado about nothing Comparison of laryngeal mask airway Supreme and laryngeal mask airway Pro-Seal for controlled ventilation during general anaesthesia in adult patients: systematic review with meta-analysis. Obtaining proficiency and retaining the skills necessary to efficiently use an alternative noninvasive airway device may prove to be crucial in a life-threatening situation such as "cannot ventilate, cannot intubate" scenario. The unique value of the device is that it permits ventilation of the lungs regardless of whether it is positioned in the esophagus or in the trachea. Proximally, both lumens are opened and linked by short tubes with universal 15-mm connectors. This design allows ventilation through the perforations of the pharyngeal lumen, when the Combitube is positioned in the esophagus and through the opened distal end of the tracheoesophageal lumen, when it is positioned in the trachea. Printed ring marks proximal to the oropharyngeal balloon indicate the appropriate depth of insertion. There are several different packaging options available, including a sturdy plastic case with the Combitube, syringes, suction catheter, and an elbow connector, a soft pack with the same contents, or simply the Combitube itself. The distal esophageal balloon is then inflated with 10 mL of air, via the white pilot balloon, using the smaller 20-mL syringe. With blind insertion, the Combitube will most likely be placed into the esophagus in more than 95% of cases. Air passes into the pharynx and then through the glottis into the trachea because the mouth, nose, and esophagus are blocked by the balloons. Auscultation of breath sounds in the absence of gastric insufflation confirms adequate ventilation when the Combitube is in the esophagus.
Discount azathioprine online american express
Some available methods of delivery for drugs that affect the airway are: inhalation spasms knee order azathioprine 50 mg mastercard, topical application, oral, and parenteral routes. Inhalation delivery is particularly useful for drugs with an effect on the airway. This route tends to provide optimal delivery of the drug to the lungs and airways (especially useful if these are the target tissues) but requires a dedicated device for administration, which may not always be available. For drugs that are in liquid or powder form, this would require the use of an actuator to agitate the drug and create the aerosol. Second, an ideal delivery device would assist in driving the drug airway from the site of aerosol formation. For example, many inhaler devices use a propellant gas to carry the aerosol particles and aid delivery to the airway. Inhalation of aerosols has the detriment of requiring a great deal of patient education and cooperation for successful use, but it is one of the most widely used forms of drug delivery to the airway. This is an option available for liquid medications and involves driving a gas (usually oxygen or air) through the liquid to draw it into droplets that are carried by the flowing gas for inhalation. It is, however, a very frequently used modality because it requires far less patient cooperation, allows for delivery of oxygen to patients that require it (as many conceivably do when presenting with airway pathology), and is relatively easy to use interchangeably in patients with or without airway instrumentation in place. Topical administration is more typically used for delivering drug to the upper airway and can be in the form of liquids, creams, gels, or powders. The anatomic difficulty of topically applying a drug to the lower airway limits its use in this regard. An example of topical administration of drug in airway management is the practice of directly applying local anesthetic to the oropharynx and palate in preparation for awake intubation. Oral administration of drugs that affect the airway is used infrequently but is most used when inhalation delivery is problematic or impossible. Additionally, this route can be used when an urgent need for airway effect is needed with inefficient action or delivery of drug by other routes. Parenteral administration is most frequently used in emergency situations for drugs that are intended to affect the airway, but the effect of parenteral drugs used for sedation and anesthesia and their effects on the airway are readily seen on a daily basis. The secondary airway effects of these drug types will be discussed later in the chapter. Similarly, the lower airway can be affected with changes in lung volumes and functional residual capacity. The upper airway is most susceptible to anatomic change and loss of patency because of the complex muscle arrangements that coordinate function such as passage of air, swallowing, and speech. This concept will present itself in various forms when various drug classes are considered with their effects on neuromuscular function and upper airway patency. Anatomy and Physiology of the Airway Airway anatomy has already been covered in great detail in Chapter 1, and airway physiology has been covered extensively in Chapter 5; however, a brief review of key elements that are relevant to the administration and effect of drugs that are frequently used with airway effect is warranted. Neuromuscular Function the upper airway is primarily comprised of skeletal muscles that are innervated by motor neurons. This is not to say that the muscles are always and completely under voluntary control. In fact, the complex relationships between muscles for contraction and relaxation to maintain patency of the airway are controlled by the respiratory centers and to some extent by the arousal centers and reticular activating system. Additionally, there are reflex arcs that exist in response to mechanical and chemical stimuli that create coordinated contractions of the upper airway musculature to protect the airway. It also, however, has reflex activity that serves to protect the airway in the presence of noxious stimuli12,13 and prevent the aspiration of unwanted material into the lungs. Hypoxia and hypercarbia also serve to increase the respiratory drive, triggering the upper airway muscles, diaphragm, and accessory muscles of the lung to increase airway patency and function. Autonomic Nervous System Airway dynamics are controlled by the surrounding musculature, which provide either dilating or constricting effects. Environmental stresses such as exercise increase sympathetic nervous activity, which dilates the upper and lower airways. Adrenergic receptors are present in the lower airway; however, no sympathetic nerves actually innervate the smooth muscle fibers of the airway-they are influenced by the Anatomy Anatomic considerations include age, body habitus, and posture. As individuals age, the cartilaginous structures of the airway continue to grow and increase in rigidity. Obesity, particularly in the cervical region, can restrict range of movement as well as decrease the volume of the upper airway. Airway sensitivity, resistance, patency, and anatomy can be affected and must be considered when selecting a pharmacologic agent. Throughout the remainder of the chapter, drug action will be discussed in the context of modulation of airway patency, protection, reactivity, and resistance. These are the primary modifiable qualities of the airway that are commonly encountered by the clinician and should be considered when choosing a therapeutic regimen for a patient needing airway management. The effect of parasympathetic activity is of muscarinic activation, which leads to bronchoconstriction, increase in mucus production and secretion, and pulmonary vasodilation. Airway Patency Patency of the upper airway is of great concern and is the most modifiable airway parameter affected by pharmacologic agents. Centrally or locally effective agents may affect upper airway patency, and the changes involve both motor output and sensory feedback. As with all agents, the effects may be directly initiated or indirectly caused by action at another site. Upper airway patency may also be diminished by physical factors, such as malignancy, mass, or inflammation. These types of obstructions may not be amenable to pharmacologic treatment, but they undoubtedly affect a drug regimen that may be used during airway management. Airway Protection Protection of the airway was described earlier and associated with arousal and reflex pathways. Lower airway reflexes prevent aspiration of particulate matter or liquids into the lungs that would impede oxygen delivery and gas exchange. The loss of these reflexes can be dangerous to a patient, and potentially lifethreatening complications may ensue. As a result, protection of the airway must be a serious concern when it is pharmacologically eliminated from normal functionality. As a reflex arc mediated afferently by the glossopharyngeal nerve and efferently by the vagus nerve, the principal function of the pharyngeal reflex is to prevent aspiration. Pharmacologic agents can directly or indirectly suppress this reflex, facilitating airway instrumentation in a sedated or even awake patient. Inadvertent suppression of the reflex must also be carefully considered as an unprotected airway can lead to aspiration of gastric contents. Airway Reactivity and Resistance Upper airway resistance is almost entirely related to patency and was discussed earlier. Increases in resistance and reactivity Voluntary Regulation of Airway Patency Upper airway patency is somewhat dependent on arousal,17 with the reticular activating system playing a role in the contraction of musculature and maintenance of patency. Sleep tends to have a counter-effect by typically increasing airway resistance,18 whereas general anesthesia blunts response of the sympathetic nervous system to external stimuli such as pain. Voluntary activities that involve coordination of muscular activity include speech and swallowing. The use of the term voluntary is not to indicate that the muscles of the oropharynx are under voluntary control individually but that the central processing and output of that coordinated activity is under voluntary control. An exception to this rule in the upper airway seems to be with the tongue; its movements are largely under voluntary control to facilitate speech and swallowing. Reactivity and resistance can be adversely affected by disease processes, such as infection and inflammation; noxious external stimuli, such as aspirated gastric contents; and pharmacologic agents, such as some volatile anesthetics. Airway reactivity will be discussed in much further detail at the end of this chapter. Those effects may be directly on the structures of the airway, or they may be mediated by indirect action. In some instances, there are both direct and indirect effects that combine to create an overall observed effect. This section will address various classes of these anesthetic drugs and review their effects on the airway. They are a very appropriate example of a drug being used specifically for an airway effect when used for preparation for awake endotracheal intubation or when used intravenously to blunt afferent sensory input from the airway during airway instrumentation or manipulation. Generally, the effect of local anesthetics on the airway is that of blockade of afferent nervous input for reflex activity.
Discount azathioprine 50 mg otc
A recombinant P element containing a transgene will not subsequently mobilize and move around the genome in flies of this stable line because laboratory strains of Drosophila do not contain P elements muscle relaxant review generic 50mg azathioprine fast delivery, so no transposase will be present. Researchers inject this plasmid, along with a helper plasmid containing the P element transposase gene, into w- host embryos where transposition occurs in some germ-line cells. When adults with these germ cells are mated with w- flies, some progeny will have red eyes and an integrated transgene. Researchers infect plants with Agrobacterium tumefaciens bacteria containing two plasmid constructs. Investigators select for single cells or seeds with a transgene insertion by growing cells or seeds in the presence of herbicide. Discuss examples of how transgenic organisms serve to produce proteins needed for human health. Explain the use of transgenic animals to model gain-of-function genetic diseases in humans. These examples of methods used for constructing transgenic organisms show how scientists can take advantage of natural processes to alter genomes. Studies with transgenic model organisms enable researchers to understand better the functions of particular genes and their regulation and to model certain human diseases in animals. Transgenes Assign Genes to Phenotypes In many genetic investigations, the available information may not allow scientists to pinpoint the gene responsible for a particular phenotype. The construction of transgenic organisms often allows investigators to resolve ambiguities. Therefore, the malformed eyes are due to the loss of gene B, not to the loss of gene A. For example, if homozygous m-/m- flies carrying a wild-type gene A transgene have malformed eyes, but m-/m- flies carrying a wild-type gene B transgene have normal eyes, you would conclude that the loss of gene B is the cause of the mutant phenotype; in other words, m = gene B. Here, we remind you that the function of these reporter constructs can be monitored only when they are introduced into eukaryotic organisms as transgenes. Bacteria are unable to perform many important posttranslational operations, including proper folding or cleavage of certain polypeptides, or modifications such as glycosylation and phosphorylation. To circumvent such problems, drug companies can sometimes use transgenic mammalian or plant cells that grow suspended in liquid culture. However, cell cultures produce only low yields of recombinant proteins, and growing the cells is expensive. The use of transgenic animals and plants to produce protein drugs is sometimes called pharming, a combination of the words farming and pharmaceutical. Pharming technology is still in its infancy; so far (in 2016), only one "pharmed" drug is available to patients, but many more are in development. The method used most commonly for the production of human protein drugs in transgenic animals is protein expression in the mammary glands, because proteins secreted into the milk can be purified at a high yield. Individual transgenic animals produced by pronuclear injection will have variable numbers of transgene copies, and the transgene array will be present at different random genomic locations. These variations result in large differences in the human protein yield among individual injected animals. One way to enhance the value of a rare, highproducing animal is by reproductive cloning: using somatic cell nuclei of transgenic adults to generate other animals with the identical genomes. Not surprisingly, the same pharmaceutical companies that are developing the technology to produce drugs in transgenic animals are funding the development of animal cloning technology. The Tools of Genetics Box entitled Cloning by Somatic Cell Nuclear Transfer describes the most commonly used reproductive cloning technology. Vaccine production in transgenic plants Like transgenic animals, plants carrying transgenes can be used for the production of human protein drugs. Transgenic plants have particular advantages for making vaccines, antigens of a disease-causing agent that stimulate an immune response to that particular foreign substance. Vaccine proteins produced by transgenic crop plants such as tobacco, sunflower, spinach, potatoes, rice, soybeans, corn, or tomatoes could be stored in the leaves or seeds. Edible vaccines could be especially advantageous for less-developed countries: No refrigeration is required for seed transport, plants could be grown on site, and no needles, syringes, or medical professionals would be necessary. Despite the theoretical promise of producing vaccines in transgenic plants, trials to date have had only partial success, and many problems need to be overcome before any of these vaccines can be marketed. One major difficulty is controlling the dose of the antigen: Individual plants can vary in the amount of antigen they produce, and too little antigen will result in an ineffective vaccine. Cloning in this sense refers to reproductive cloning, in which the genome of a single somatic cell from one individual now becomes the genome of every somatic cell in a different individual. Researchers create reproductive clones through a protocol known as somatic cell nuclear transfer. After several days of growth, the researchers implant the manipulated embryo into the uterus of a surrogate mother. A could be thought of as having three different mothers: the somatic nuclear donor, the oocyte donor, and the surrogate who provided the womb. It is also possible to clone male animals if the somatic cell nucleus comes from a male. Even though all of the nuclear chromosomes in all of the cells of the clone are derived only from the somatic nuclear donor, the cloned animal and this donor are not perfectly identical in all respects, for several reasons: (1) the mitochondrial genomes of the clone come from the oocyte donor, not the nuclear donor. Few people could afford the high costs of the cloning procedure, and furthermore, some ill-informed clients were disappointed to find that the clone they received was not in fact exactly the pet they knew. Research on cloned animals enables scientists to better understand basic processes such as gene imprinting. Drug companies are investing in reproductive cloning technology with an eye toward being able to generate large numbers of high-producing transgenic animals. Dolly was cloned by scientists in Scotland, in part with funding from a pharmaceutical company. Cloned animal Before Dolly died in 2003, she gave birth to five progeny who live on. Finally, several endangered species have been cloned for the purpose of their preservation. Even if the scientific problems can be overcome, drug companies will encounter many regulatory hurdles before making these plant-produced vaccines available to humans. Because the regulations are less strict, considerable recent attention has been placed instead on feeding transgenic vaccine-making plants to domestic animals, so as to protect them from various diseases caused by pathogenic organisms. The improvements conferred by the transgenes include enhanced nutritional value; increased shelf life; increased yield or plant size; and resistance to stress, herbicides, or infestations by plant viruses or insects. We discuss here two of the most commercially important transgenic crops that are currently in wide use. More than 90% of the soybeans grown in the United States are transgenic plants resistant to glyphosate, the active ingredient in the herbicide called Roundup. Farmers spray fields of herbicide-resistant soybeans with Roundup to kill weeds with no harm to the soybeans, thus saving much labor and time. This protein is made naturally by the bacterium Bacillus thuringiensis to protect itself from being eaten by the caterpillars. Bt protein is lethal to insect larvae that ingest it, but not to other animals, including humans. Because the engineered corn manufactures its own natural insecticide, farmers can avoid using costly chemical pesticides that damage farmworkers and the environment. More than 10 billion acres of land around the world is used to grow Bt-expressing crops, not only corn but also canola, cotton, corn, papaya, potato, rice, soybean, squash, sugar beet, tomato, wheat, and eggplant. Atlantic salmon normally take three years to grow to their full size of about 9 pounds; their growth hormone gene is shut off during the coldest months when food is scarce, and so they grow only about eight months of the year. Transgenic Animals Model Human Gain-of-Function Genetic Diseases Animal models of human genetic diseases have for decades been an important tool for scientists trying to understand disease biochemistry so as to design and test new drugs and other treatments. The idea of an animal model for a monogenic human disease is simple-to generate an animal with a corresponding mutation and a similar disease phenotype. You should note that because transgenes are added to otherwise wild-type genomes, transgenic animals made by the techniques just described can serve as models only for dominant, gain-of-function mutations. Mice are mammals, and similar versions of most human genes are present in their genome. But for the study of human neurological disorders, unfortunately, mice cannot replicate the complex effects of some gene mutations on brain functions and behavior. Instead, scientists have recently begun to model human diseases in transgenic laboratory monkeys-rhesus macaques. The first transgenic primate model for a human neurological disorder was for Huntington disease.
