
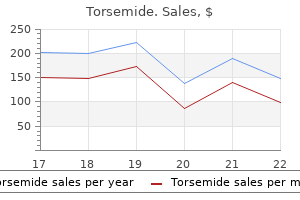
Purchase torsemide pills in toronto
These agents may be administered by continuous infusion in the intensive care setting for improving chest wall compliance and eliminating ventilator dyssynchrony arrhythmia when sleeping discount 20mg torsemide free shipping. Thus, its use should be reserved to nonambulatory patients with severe spasticity. Hepatotoxicity has been reported with chronic use, requiring frequent liver function tests and use of the lowest possible oral dose. Several agents, many of limited efficacy, have been used to treat spasticity involving the -motor neurons originating in the brainstem and spinal cord. A number of other agents used as muscle relaxants seem to rely on sedative properties and blockade of nociceptive pathways; this group includes carisoprodol (which is metabolized to meprobamate; see Chapter 19); metaxalone; methocarbamol; and orphenadrine. Responses are monitored from compound action potentials or muscle tension developed in the adductor pollicis (thumb) muscle. Responses to repetitive or tetanic stimuli are most useful for evaluation of blockade of transmission. Rates of onset of blockade and recovery are more rapid in the airway musculature (jaw, larynx, and diaphragm) than in the thumb. Hence, tracheal intubation can be performed before onset of complete block at the adductor pollicis, whereas partial recovery of function of this muscle allows sufficient recovery of respiration for extubation. Preventing Trauma During Electroshock Therapy Electroconvulsive therapy of psychiatric disorders occasionally is complicated by trauma to the patient; the seizures induced may cause dislocations or fractures. Inasmuch as the muscular component of the convulsion is not essential for benefit from the procedure, neuromuscular blocking agents, usually succinylcholine, and a short-acting barbiturate, usually methohexital, are employed. Control of Muscle Spasms and Rigidity Botulinum toxins and dantrolene act peripherally to reduce muscle contraction; a variety of other agents act centrally to reduce skeletal muscle tone and spasm. Originally approved for the treatment of the ocular conditions of strabismus and blepharospasm and for hemifacial spasms, botulinum toxins have been used to treat spasms and dystonias and spasms associated with the lower esophageal sphincter and anal fissures. Botulinum toxin treatments also have become a popular cosmetic procedure for those seeking a wrinkle-free face. Like the bloom of youth, the reduction of wrinkles is temporary; unlike the bloom of youth, the effect of botulinum toxin can be renewed by readministration. In addition, many other drugs affect transmission at the neuromuscular junction and thus can affect the choice and dosage of neuromuscular blocking agent used. Similarly, on completion of the surgical procedure, many anesthesiologists employ neostigmine or edrophonium to reverse and decrease the duration of competitive neuromuscular blockade. A muscarinic antagonist (atropine or glycopyrrolate) is used concomitantly to prevent stimulation of muscarinic receptors and thereby to avoid slowing of the heart rate. Anti-ChE agents will not reverse depolarizing neuromuscular blockade and, in fact, can enhance it. Many inhalational anesthetics exert a stabilizing effect on the postjunctional membrane and therefore potentiate the activity of competitive blocking agents. Consequently, when such blocking drugs are used for muscle relaxation as adjuncts to these anesthetics, their doses should be reduced. The rank order of potentiation is desflurane > sevoflurane > isoflurane > halothane > nitrous oxide-barbiturate-opioid or propofol anesthesia (Naguib et al. The blockade is antagonized by Ca2+ salts but only inconsistently by anti-ChE agents (see Chapter 58). The tetracyclines also can produce neuromuscular blockade, possibly by chelation of Ca2+. Additional antibiotics that have neuromuscular blocking action, through both presynaptic and postsynaptic actions, include polymyxin B, colistin, clindamycin, and lincomycin. Ca2+ channel blockers enhance neuromuscular blockade produced by both competitive and depolarizing antagonists. When neuromuscular blocking agents are administered to patients receiving these agents, dose adjustments should be considered. Miscellaneous drugs that may have significant interactions with either competitive or depolarizing neuromuscular blocking agents include trimethaphan, lithium, opioid analgesics, procaine, lidocaine, quinidine, phenelzine, carbamazepine, phenytoin, propranolol, dantrolene, azathioprine, tamoxifen, magnesium salts, corticosteroids, digitalis glycosides, chloroquine, catecholamines, and diuretics. Adverse Effects the important untoward responses of the neuromuscular blocking agents include prolonged apnea, cardiovascular collapse, those resulting from histamine release, and, rarely, anaphylaxis. Related factors may include alterations in body temperature; electrolyte imbalance, particularly of K+; 184 low plasma butyrylcholinesterase levels, resulting in a reduction in the rate of destruction of succinylcholine; the presence of latent myasthenia gravis or of malignant disease such as small cell carcinoma of the lung with Eaton-Lambert myasthenic syndrome; reduced blood flow to skeletal muscles, causing delayed removal of the blocking drugs; and decreased elimination of the muscle relaxants secondary to hepatic dysfunction (cisatracurium, rocuronium, vecuronium) or reduced renal function (pancuronium). Great care should be taken when administering neuromuscular blockers to dehydrated or severely ill patients. Depolarizing agents can cause rapid release of K+ from intracellular sites; this may be a factor in production of the prolonged apnea in patients who receive these drugs while in electrolyte imbalance. Succinylcholine-induced hyperkalemia is a life-threatening complication of that drug. Malignant hyperthermia is a potentially life-threatening event triggered by the administration of certain anesthetics and neuromuscular blocking agents. Uncontrolled release of Ca2+ from the sarcoplasmic reticulum of skeletal muscle is the initiating event. Susceptibility to malignant hyperthermia, an autosomal dominant trait, is associated with certain congenital myopathies, such as central core disease. In the majority of cases, however, no clinical signs are visible in the absence of anesthetic intervention. Treatment entails intravenous administration of dantrolene, which blocks Ca2+ release from the sarcoplasmic reticulum of skeletal muscle (see previous discussion, Control of Muscle Spasms and Rigidity). Rapid cooling, inhalation of 100% O2, and control of acidosis should be considered adjunct therapy in malignant hyperthermia. Treatment of respiratory paralysis arising from an adverse reaction or overdose of a neuromuscular blocking agent should be by positive-pressure artificial respiration with O2 and maintenance of a patent airway until recovery of normal respiration is ensured. With the competitive blocking agents, this may be hastened by the administration of neostigmine methylsulfate (0. In the case of overdose, a muscarinic cholinergic antagonist (atropine or glycopyrrolate) may be added to prevent undue slowing of the heart (see Synergisms and Antagonisms). Because the neuromuscular junction is not fully developed at birth, additional care must be taken in administration of neuromuscular blocking agents to infants and children. Succinylcholine is not safe for routine use in pediatric patients, and its use must be reserved for extreme emergency situations where immediate securing of the airway is necessary and other options for neuromuscular blockade are not available. Competitive blocking agents, however, are commonly used in pediatric patients; generally, dosage is similar to adults but both rate of block onset and clearance are faster. Atracurium is an exception: the dosage and duration of action are not significantly different between children older than 2 years and adults, and the same dose (0. Vecuronium, cisatracurium, rocuronium, and mivacurium are also commonly administered to children for short procedures where only a single intubating dose is required. There are normal changes at the neuromuscular junction in elderly patients that may affect pharmacodynamics of neuromuscular blocking agents. With aging, the distance between the terminus of the motor neuron and the end plate increases, the end-plate invaginations become flatter, the amount of transmitter per synaptic vesicle decreases, the vesicle release probability is lower, and the density of receptors at the end plate decreases. The end result of these changes is decreased efficiency of neuromuscular transmission. General physiological changes in aging patients, including decreases in body water and muscle, increases in total body fat, and decreases in renal and hepatic function, also contribute to the action of neuromuscular blockers. The dosing of succinylcholine is not significantly altered in the geriatric population. Among the competitive blocking agents, initial dose requirements are unchanged, however, the onset of blockade is delayed in an age-related manner, and block is prolonged. For compounds such as atracurium that are not dependent on hepatic or renal blood flow for their elimination, pharmacodynamics and kinetics are largely unaltered. Succinylcholine, mivacurium, and atracurium cause histamine release, but to a lesser extent than tubocurarine unless administered rapidly. The amino steroids pancuronium, vecuronium, pipecuronium, and rocuronium have even less tendency to release histamine after intradermal or systemic injection (Basta, 1992; Watkins, 1994). Histamine release typically is a direct action of the muscle relaxant on the mast cell rather than anaphylaxis mediated by immunoglobulin E.
Torsemide 10 mg amex
Membrane transporters (T) play roles in pharmacokinetic pathways (drug absorption arrhythmia beta blockers order torsemide 20 mg without prescription, distribution, metabolism, and excretion), thereby setting systemic drug levels. Inhibition of these transporters by drugs may cause cholestasis or hyperbilirubinemia. Membrane transporters (red ovals with arrows) work in concert with phase 1 and phase 2 drug-metabolizing enzymes in the hepatocyte to mediate the uptake and efflux of drugs and their metabolites. The left panel of each case provides a representation of the mechanism; the right panel shows the resulting effect on drug levels. The diagram also may represent an increase in the concentration of the endogenous compound in the target organ owing to drug-inhibited efflux of the endogenous compound. Uptake and efflux transporters determine the plasma and tissue concentrations of endogenous compounds and xenobiotics, thereby influencing the systemic or site-specific toxicity of drugs. Basic Mechanisms of Membrane Transport Transporters Versus Channels Both channels and transporters facilitate the membrane permeation of inorganic ions and organic compounds. In general, channels have two primary states, open and closed, that are stochastic phenomena. Only in the open state do channels appear to act as pores for the selected ions flowing down an electrochemical gradient. By contrast, a transporter forms an intermediate complex with the substrate (solute), and a subsequent conformational change in the transporter induces translocation of the substrate to the other side of the membrane. As a consequence, the kinetics of solute movement differ between transporters and channels. Typical turnover rate constants of channels are 106 to 108 s-1; those of transporters are, at most, 101 to 103 s-1. Black squares represent the ion that supplies the driving force for transport (size is proportional to the concentration of the ion). The basic mechanisms involved in solute transport across biological membranes include passive diffusion, facilitated diffusion, and active transport. Active transport can be further subdivided into primary and secondary active transport. Primary Active Transport Passive Diffusion Simple diffusion of a solute across the plasma membrane consists of three processes: partition from the aqueous to the lipid phase, diffusion across the lipid bilayer, and repartition into the aqueous phase on the opposite side. Passive diffusion of any solute (including drugs) occurs down an electrochemical potential gradient of the solute. In secondary active transport, the transport across a biological membrane of a solute S1 against its concentration gradient is energetically driven by the transport of another solute S2 in accordance with its electrochemical gradient. Depending on the transport direction of the solute, secondary active transporters are classified as either symporters or antiporters. This is an example of antiport, or exchange transport, in which the transporter moves S2 and S1 in opposite directions. Secondary Active Transport Facilitated Diffusion Diffusion of ions and organic compounds across the plasma membrane may be facilitated by a membrane transporter. Facilitated diffusion is a form of transporter-mediated membrane transport that does not require energy input. Just as in passive diffusion, the transport of ionized and nonionized compounds across the plasma membrane occurs down their electrochemical potential gradients. Therefore, steady state will be achieved when the electrochemical potentials of a compound on both sides of the membrane become equal. Active Transport Active transport is the form of membrane transport that requires the input of energy. It is the transport of solutes against their electrochemical gradients, leading to the concentration of solutes on one side of the plasma membrane and the creation of potential energy in the electrochemical gradient formed. Active transport plays an important role in the uptake and efflux of drugs and other solutes. Symport describes movement of driving ion and transported solute in the same direction. Antiport occurs when the driving ion and the transported solute move in opposite directions, as when the Kinetics of Transport the flux of a substrate (rate of transport) across a biological membrane via a transporter-mediated process is characterized by saturability. Km is an approximation of the dissociation constant of the substrate from the intermediate complex. The Km and Vmax values can be determined by examining the flux at different substrate concentrations. Emerging crystals structures are adding to our ideas of the mechanisms of transport via these proteins. Transporter-mediated membrane transport of a substrate is also characterized by inhibition by other compounds. The manner of inhibition can be categorized as one of three types: competitive, noncompetitive, and uncompetitive. Competitive inhibition occurs when substrates and inhibitors share a common binding site on the transporter, resulting in an increase in the apparent Km value in the presence of inhibitor. Noncompetitive inhibition assumes that the inhibitor has an allosteric effect on the transporter, does not inhibit the formation of an intermediate complex of substrate and transporter, but does inhibit the subsequent translocation process. C, left panel) and the Eadie-Hofstee transformation of the transport data (v/C vs. The blue lines depict transport in the presence of a competitive inhibitor (surmountable inhibition; achieves same Vmax). The red lines depict the system in the presence of a noncompetitive inhibitor that effectively reduces the number of transporting sites but leaves the Km of the functional sites unchanged. Involvement of multiple transporters with different Km values gives an Eadie-Hofstee plot that is curved and can be resolved into multiple components. Algebraically, the Eadie-Hofstee plot of kinetic data is equivalent to the Scatchard plot of equilibrium binding data (see Chapter 3). In general terms, the transporter undergoes a reversible conformational change between the two sides of the membrane during the translocation process. The transport cycle would be as follows: the substrate accesses the substrate binding site on one side of the membrane; substrate binding induces structural changes in the carrier protein, reorienting the opening of the binding site to the opposite side. The substrate dissociates from the transport site, allowing another substrate to be bound and transported in the opposite direction. Such a mechanism requires that binding of different substrates (the "outbound" and "inbound" substrates) that is mutually exclusive; that is, there is a single reorienting binding site. Vectorial transport is important for the absorption of nutrients and bile acids in the intestine in the intestinal absorption of drugs (from lumen to blood). Vectorial transport also plays a major role in hepatobiliary and urinary excretion of drugs from the blood to the lumen. In addition, efflux of drugs from the brain via brain endothelial cells and brain choroid plexus epithelial cells involves vectorial transport. Transepithelial or transendothelial flux of drugs requires distinct transporters at the two surfaces of the epithelial or endothelial barrier. A typical configuration involves a primary or secondary active transporter at one membrane and a passive transporter at the other. In this way, common substrates of coordinated transporters are transferred efficiently across the epithelial barrier. In the liver, a number of transporters with different substrate specificities are localized on the sinusoidal membrane (facing blood). These transporters are involved in the uptake of bile acids, amphipathic organic anions, and hydrophilic organic cations into the hepatocytes. In addition to conferring multidrug resistance, an important pharmacological aspect of these transporters is xenobiotic export from healthy tissues. The following examples illustrate the importance of vectorial transport in determining drug exposure in the circulating blood and liver and the role of transporters in drug-drug interactions. The rate-limiting process in renal tubular secretion is likely the uptake process at the basolateral surface. Bosentan Bosentan is an endothelin antagonist used to treat pulmonary arterial hypertension. Transporter-mediated hepatic uptake can be a determinant of elimination of bosentan, and inhibition of its hepatic uptake by cyclosporine, rifampicin, and sildenafil can affect its pharmacokinetics. Transporters in the liver and kidney have important roles in removal of drugs from the blood and hence in metabolism and excretion. These transporters mediate uptake by either facilitated or secondary active mechanisms.
Diseases
- X-linked mental retardation type Gustavson
- Placental abruption
- Epidermolysis bullosa herpetiformis, Dowling Meara
- Aase Smith syndrome
- Say Carpenter syndrome
- Reperfusion injury
- Dyskinesia
- Genu valgum, st. Helena familial
Order torsemide 10 mg with visa
If fertility is not desired blood pressure log sheet printable purchase 10 mg torsemide fast delivery, a hysterectomy with ovarian preservation can be the primary treatment of a molar pregnancy. Chemoprophylaxis with a one-time dose of single-agent chemotherapy can be considered. In these patients, data have shown the rates of persistent disease have gone from about 50% to 15%. Chemoprophylaxis in lower-risk patients can also be considered if they are seen as potentially noncompliant. A single dose of either methotrexate or dactinomycin immediately prior to the surgical procedure can be considered for prophylaxis against embolism of tumor cells from surgical manipulation. If there are cerebral metastases, craniotomy to prevent herniation from mass or hemorrhage may be indicated. Consideration of intrathecal methotrexate or whole brain irradiation to 30 Gy is important. This is a relatively chemoresistant tumor, so if the disease is found to be advanced, surgery with adjuvant chemotherapy is likely the best option. The only prognostic factor identified regarding survival, is time from the last pregnancy. If this time is less than 4 years, patients usually do well; if it is greater than 4 years, this is usually universally fatal. Mechanical ventilation is contraindicated due to a high risk of trauma and iatrogenic hemorrhage, l 196 2. If cerebral metastases are identified, vigilance for cerebral hemorrhage, edema, and herniation should be maintained. A hysterectomy or local uterine resection may be considered in addition to chemotherapy if there is persistent disease. Hysterectomy with ovarian preservation may be offered if this is the sole site of resistant disease. Hysterectomy with ovarian preservation may be indicated if this appears to be the sole site of resistant disease. If no major toxicity was encountered, the weekly dose was escalated by 5 mg/m2 at 3-week intervals until a maximum dose of 50 mg/m2 each week was achieved. If no major toxicity was encountered, the weekly dose was escalated by 5 mg/m2 at 2-week intervals until a maximum dose of 50 mg/m2 per week was achieved; 74% had a complete response. Primary chemotherapy should then consist of actinomycin D in these intermediate and high-risk patients (8). Surgical failure occurred in 59% of women and was found more commonly in the age extremes. The role of repeat uterine evacuation in the management of persistent gestational trophoblastic disease. Hormonal contraception and trophoblastic sequelae after hydatidiform mole (a Gynecologic Oncology Group study). Weekly intramuscular methotrexate for nonmetastatic gestational trophoblastic disease. Rapid escalation of weekly intramuscular methotrexate for nonmetastatic gestational trophoblastic disease: a Gynecologic Oncology Group study. In premenopausal women, oophorectomy reduces the risk of developing breast cancer by 60%. Interval salpingectomy followed by oophorectomy (a staged procedure) can be considered if patients are highly concerned of early surgical menopause. This suggests the genetic assessment of all women diagnosed with high-grade serous carcinoma will improve detection rates and capture mutation carriers otherwise missed by referral based on family history alone (5). Pregenetic screening, counseling, and testing can be offered to those considering children. Immunohistochemistry can be a first-line approach on the pathological specimen and provide baseline mutation information on the tumor itself. Progestin-based contraception should be used to decrease malignant transformation of reproductive organs. Because of incomplete penetrance, 15% to 20% of these procedures may be unnecessary, but this risk reduction option can be discussed. For breast cancer, the risk is 25% to 50% at age 38 to 50 years; for thyroid cancer 30% to 68%. Breast cancer at any age and more than one relative with breast cancer less than 50 years old, more than one relative with invasive ovarian cancer, more than two relatives with breast and/or pancreatic cancer at any age, or from a population at increased risk. Minor criteria Autism spectrum disorder Colon cancer Esophageal glycogenic acanthoses (3) Lipomas (3) Intellectual disability. A baseline test should be obtained at 8 to 10 years old with follow-up interval based on findings but at least by age 18, then every 2 to 3 years, or with symptoms. Magnetic resonance cholangiopancreatography or endoscopic ultrasound should be obtained every 1 to 2 years starting at age 30 to 35. Mutations in 12 genes for inherited ovarian, fallopian tube, and peritoneal carcinoma identified by massively parallel sequencing. Superior to the arcuate line, the internal oblique aponeurosis splits to envelop the rectus abdominis muscle. Inferior to the arcuate line, the internal oblique and transversus abdominis aponeuroses merge and pass superficial. A small evagination of peritoneum (canal of Nuck) accompanies the round ligament through the inguinal ring. Utero-ovarian: these contain the utero-ovarian vessels between the ovary and the uterus. Uterosacral: located posterior to the cervix, they originate from thickening of the endopelvic fascia. There are two branches of the external iliac artery and vein: the deep circumflex iliac and the inferior epigastric. It is a sensory nerve to the medial thigh, and motor innervation to the cremaster muscle. This is bounded superiorly by the inguinal ligament, the sartorius muscle laterally to medially, and the adductor longus muscle medially to laterally. The base of the triangle consists of the iliacus, iliopsoas, and pectineus muscles, laterally to medially. The femoral nerve consists of the anterior femoral cutaneous branch and the medial femoral cutaneous branches from the L1, L2, and L3 nerve roots. The lateral femoral cutaneous nerve runs on top of the iliopsoas muscle and originates from L1. The ilioinguinal nerve also runs through the triangle and originates in the L1 root. The femoral vein receives branches from the superficial circumflex, external pudendal, and superficial epigastric veins. These enter the femoral vein near the saphenous vein, or sometimes drain into the saphenous prior to entry into the femoral vein. The internal pudendal artery (a branch of the anterior division of the internal iliac) divides to form the perineal, clitoral, and inferior rectal arteries.
Order torsemide 20mg line
The fraction of total drug in plasma that is bound is determined by the drug concentration arteria bologna 8 marzo cheap torsemide 10mg free shipping, the affinity of binding sites for the drug, and the concentration of available binding sites. For most drugs, the therapeutic range of plasma concentrations is limited; thus, the extent of binding and the unbound fraction are relatively constant. The extent of plasma protein binding also may be affected by disease-related factors. Changes in protein binding caused by disease states and drugdrug interactions are clinically relevant mainly for a small subset of so-called high-clearance drugs of narrow therapeutic index that are administered intravenously, such as lidocaine. When changes in plasma protein binding occur in patients, unbound drug rapidly equilibrates throughout the body and only a transient significant change in unbound plasma concentration will occur. Only drugs that show an almost-instantaneous relationship between free plasma concentration and effect. Thus, unbound plasma drug concentrations will exhibit significant changes only when either drug input or clearance of unbound drug occurs as a consequence of metabolism or active transport. A more common problem resulting from competition of drugs for plasma protein-binding sites is misinterpretation of measured concentrations of drugs in plasma because most assays do not distinguish free drug from bound drug. Competition for plasma protein-binding sites may cause one drug to elevate the concentration of one bound less avidly. Binding of a drug to plasma proteins limits its concentration in tissues and at its site of action because only unbound drug is in equilibrium across membranes. Accordingly, after distribution equilibrium is achieved, the concentration of unbound drug in intracellular water is the same as that in plasma except when carrier-mediated active transport is involved. Rectal Administration Approximately 50% of the drug that is absorbed from the rectum will bypass the liver, thereby reducing hepatic first-pass metabolism. However, rectal absorption can be irregular and incomplete, and certain drugs can cause irritation of the rectal mucosa. Novel Methods of Drug Delivery Drug-eluting stents and other devices are being used to target drugs locally to maximize efficacy and minimize systemic exposure. Recent advances in drug delivery include the use of biocompatible polymers and nanoparticles for drug delivery (Yohan and Chithrani, 2014). Bioequivalence Drug products are considered to be pharmaceutical equivalents if they contain the same active ingredients and are identical in strength or concentration, dosage form, and route of administration. Two pharmaceutically equivalent drug products are considered to be bioequivalent when the rates and extents of bioavailability of the active ingredient in the two products are not significantly different under suitable and identical test conditions. Generic versus brand name prescribing is further discussed in connection with drug nomenclature and the choice of drug name in writing prescription orders (see Appendix I). Courts have not always found generic and brand name drugs to be legally equivalent (see Chapter 1). Curves depict the distribution of the barbiturate anesthetic thiopental into different body compartments following a single rapid intravenous dose. The rate of accumulation in the various body compartments depends on regional blood flow; the extent of accumulation reflects the differing capacities of the compartments and the steady but slow effect of elimination to reduce the amount of drug available. Emergence from the anesthetic influence of this single dose of thiopental relies on redistribution, not on metabolism. The drug will partition out of tissue depots as metabolism and elimination take their course. Depletion of compartments will follow the same order as accumulation, as a function of their perfusion. Tissue Binding Many drugs accumulate in tissues at higher concentrations than those in the extracellular fluids and blood. Tissue binding of drugs usually occurs with cellular constituents such as proteins, phospholipids, or nuclear proteins and generally is reversible. A large fraction of drug in the body may be bound in this fashion and serve as a reservoir that prolongs drug action in that same tissue or at a distant site reached through the circulation. Local destruction of the bone medulla also may result in reduced blood flow and prolongation of the reservoir effect as the toxic agent becomes sealed off from the circulation; this may further enhance the direct local damage to the bone. A vicious cycle results, whereby the greater the exposure to the toxic agent, the slower is its rate of elimination. The adsorption of drug onto the bone crystal surface and incorporation into the crystal lattice have therapeutic advantages for the treatment of osteoporosis. In obese persons, the fat content of the body may be as high as 50%, and even in lean individuals, fat constitutes 10% of body weight; hence, fat may serve as a reservoir for lipid-soluble drugs. Redistribution Bone the tetracycline antibiotics (and other divalent metal-ion chelating agents) and heavy metals may accumulate in bone by adsorption onto the bone crystal surface and eventual incorporation into the crystal lattice. Bone Termination of drug effect after withdrawal of a drug usually is by metabolism and excretion but also may result from redistribution of the drug from its site of action into other tissues or sites. Redistribution is a factor in terminating drug effect primarily when a highly lipid-soluble drug that acts on the brain or cardiovascular system is administered rapidly by intravenous injection or inhalation. Subsequently, the plasma and brain concentrations decrease as thiopental redistributes to other tissues, such as muscle and, finally, adipose tissue. The concentration of the drug in brain follows that of the plasma because there is little binding of the drug to brain constituents. Thus, both the onset and the termination of thiopental anesthesia are relatively rapid, and both are related directly to the concentration of drug in the brain. Prodrugs; Pharmacogenomics Prodrugs are pharmacologically inactive compounds that are converted to their active forms by metabolism. This approach can maximize the amount of the active species that reaches its site of action. Inactive prodrugs are converted rapidly to biologically active metabolites, often by the hydrolysis of an ester or amide linkage. Enalapril, for instance, is relatively inactive until converted by esterase activity to the diacid enalaprilat (see Chapters 6 and 26). For a number of therapeutic areas, clinical pharmacogenomics, the study of the impact of genetic variations or genotypes of individuals on their drug response or drug metabolism, allows for improved treatment of individuals or groups (Ramamoorthy et al. Lipid solubility, extent of plasma binding, and degree of ionization of weak acids and bases are important general determinants in drug transfer across the placenta. The placenta functions as a selective barrier to protect the fetus against the harmful effects of drugs. The view that the placenta is an absolute barrier to drugs is inaccurate, in part because a number of influx transporters are also present. The Food and Drug Administration categorizes the relative safety of drugs that may be used in pregnant women (see Appendix I). Excretion of Drugs Drugs are eliminated from the body either unchanged or as metabolites. Excretory organs, the lung excluded, eliminate polar compounds more efficiently than substances with high lipid solubility. Thus, lipid-soluble drugs are not readily eliminated until they are metabolized to more polar compounds. Substances excreted in the feces are principally unabsorbed orally ingested drugs or drug metabolites either excreted in the bile or secreted directly into the intestinal tract and not reabsorbed. Excretion of drugs in breast milk is important not because of the amounts eliminated (which are small) but because the excreted drugs may affect the nursing infant (also small, and with poorly developed capacity to metabolize xenobiotics). Excretion from the lung is important mainly for the elimination of anesthetic gases (see Chapter 21). Metabolism of Drugs A Few Principles of Metabolism and Elimination the many therapeutic agents that are lipophilic do not pass readily into the aqueous environment of the urine. The metabolism of drugs and other xenobiotics into more hydrophilic metabolites is essential for their renal elimination from the body, as well as for termination of their biological and pharmacological activity. From the point of view of pharmacokinetics, the following are the three essential aspects of drug metabolism: First-order kinetics. For most drugs in their therapeutic concentration ranges, the amount of drug metabolized per unit time is proportional to the plasma concentration of the drug (Cp) and the fraction of drug removed by metabolism is constant. For some drugs, such as ethanol and phenytoin, metabolic capacity is saturated at the concentrations usually employed, and drug metabolism becomes zero order; that is, a constant amount of drug is metabolized per unit time. Zero-order kinetics can also occur at high (toxic) concentrations as drug-metabolizing capacity becomes saturated. The major drug-metabolizing systems are inducible, broad-spectrum enzymes with some predictable genetic variations. In general, drug-metabolizing reactions generate more polar, inactive metabolites that are readily excreted from the body.
Generic 20 mg torsemide fast delivery
Diphenoxylate hydrochloride is available only in combination with atropine sulfate arteria vesicalis medialis purchase torsemide 20mg with mastercard. The recommended daily dosage of diphenoxylate for the treatment of diarrhea in adults is 20 mg in divided doses. Difenoxin a metabolite of diphenoxylate and is marketed in a fixed dose with atropine for the management of diarrhea. Muscle rigidity, while possible after all narcotics, appears to be more common after the high doses used in anesthetic induction. As with analgesia, respiratory depression after small doses is of shorter duration than with morphine but of similar duration after large doses or long infusions. Delayed respiratory depression also can be seen after the use of fentanyl or sufentanil, possibly owing to enterohepatic circulation. Fentanyl and its derivatives decrease heart rate through vagal activation and may modestly decrease blood pressure. However, these drugs do not release histamine, and direct depressant effects on the myocardium are minimal. For this reason, high doses of fentanyl or sufentanil are commonly used as the primary anesthetic for patients undergoing cardiovascular surgery or for patients with poor cardiac function. In controlling chronic diarrhea, loperamide is as effective as diphenoxylate and little tolerance develops to its constipating effect. Loperamide is poorly absorbed after oral administration and, in addition, apparently does not penetrate well into the brain due to the exporting activity of P-glycoprotein, which is widely expressed in the brain endothelium. Loperamide is unlikely to be abused parenterally because of its low solubility; large doses of loperamide given to human volunteers do not elicit pleasurable effects typical of opioids. After systemic delivery, fentanyl is about 100 times more potent than morphine; sufentanil is about 1000 times more potent than morphine. The time to peak analgesic effect after intravenous administration of fentanyl and sufentanil (~5 min) is notably less than that for morphine and meperidine (~15 min). However, with larger doses or prolonged infusions, the effects of these drugs become more lasting, with durations of action becoming similar to those of longer-acting opioids. Transbuccal absorption by the use of buccal tablets and lollipop-like lozenges permits rapid absorption and has found use in the management of acute incident pain and for the relief of breakthrough cancer pain. Fentanyl should only be used in opioid-tolerant patients, defined as consuming more than 60 mg of oral morphine equivalent. Epidural use of fentanyl and sufentanil for postoperative or labor analgesia is popular. A combination of epidural opioids with local anesthetics permits 374 reduction in the dosage of both components. Illicit use (self-administration by chewing) of fentanyl patches can be deadly, and practitioners must be aware of this potential and keep careful control of fentanyl stocks. Remifentanil Therapeutic Uses the pharmacological properties of remifentanil are similar to those of fentanyl and sufentanil. Remifentanil produces similar incidences of nausea, vomiting, and dose-dependent muscle rigidity. Remifentanil has a more rapid onset of analgesic action than fentanyl or sufentanil. Remifentanil hydrochloride is useful for short, painful procedures that require intense analgesia and blunting of stress responses; the drug is routinely given by continuous intravenous infusion because of its short duration of action. In this situation, either a longer-acting opioid or another analgesic modality should be combined with remifentanil for prolonged analgesia, or another opioid should be used. Remifentanil is not used intraspinally (epidural or intrathecal administration) because of its formulation with glycine, an inhibitory neurotransmitter in the dorsal horn of the spinal cord (Stroumpos et al. The primary use of methadone hydrochloride is detoxification and maintenance treatment of opioid addiction within certified treatment programs. Care must be taken when increasing the dosage because of the prolonged t1/2 of the drug and its tendency to accumulate over a period of several days with repeated dosing. Despite its longer plasma t1/2, the duration of the analgesic action of single doses is essentially the same as that of morphine. With repeated use, cumulative effects are seen, so either lower dosages or longer intervals between doses become possible. Because of its oral bioavailability and long t1/2, methadone has been widely implemented as a replacement modality to treat heroin addiction. Thus, addicts who receive daily subcutaneous or oral therapy develop partial tolerance to the nauseant, anorectic, miotic, sedative, respiratory-depressant, and cardiovascular effects of methadone. Many former heroin users treated with oral methadone show virtually no overt behavioral effects. Development of physical dependence during the long-term administration of methadone can be demonstrated following abrupt drug withdrawal or by administration of an opioid antagonist. Likewise, subcutaneous administration of methadone to former opioid addicts produces euphoria equal in duration to that caused by morphine, and its overall abuse potential is comparable with that of morphine. Miotic and respiratory-depressant effects can be detected for more than 24 h after a single dose; on repeated administration, marked sedation is seen in some patients. Effects on cough, bowel motility, biliary tone, and the secretion of pituitary hormones are qualitatively similar to those of morphine. Rifampin and phenytoin accelerate the metabolism of methadone and can precipitate withdrawal symptoms. In the treatment of mild-to-moderate pain, tramadol is as effective as morphine or meperidine. Tramadol is as effective as meperidine in the treatment of labor pain and may cause less neonatal respiratory depression (Grond and Sablotzki, 2004). The major metabolites, pyrrolidine and pyrroline, result from N-demethylation and cyclization and are excreted in the urine and the bile along with small amounts of unchanged drug. The amount of methadone excreted in the urine is increased when the urine is acidified. Methadone appears to be firmly bound to protein in various tissues, including brain. The primary O-demethylated metabolite of tramadol is two to four times more potent than the parent drug and may account for part of the analgesic effect. Tramadol is supplied as a racemate that is more effective than either enantiomer alone. The maximum recommended daily dose is 400 mg (300 mg in patients > 75 years old and for extended-release formulations; 200 mg is given for patients with low creatinine clearance). Side effects of tramadol include nausea, vomiting, dizzi- ness, dry mouth, sedation, and headache. Respiratory depression appears to be less than with equianalgesic doses of morphine, and the degree of constipation is less than that seen after equivalent doses of codeine. Tramadol can cause seizures and possibly exacerbate seizures in patients with predisposing factors. Precipitation of withdrawal necessitates that tramadol be tapered prior to discontinuation. Nalbuphine depresses respiration as much as equianalgesic doses of morphine; however, nalbuphine exhibits a ceiling effect such that increases in dosage beyond 30 mg produce no further respiratory depression or analgesia.
Cheap 10 mg torsemide with mastercard
Quality of Life Quality of life is a widely used term that conveys an overall sense of well-being that encompasses aspects of happiness and satisfaction with life in general pulse pressure stroke buy discount torsemide 20mg on line. It is one of the most important factors when considering systemic treatment in patients with incurable disease. In patients with advanced incurable cancer, treatment should aim to improve quality of life by palliating troublesome symptoms and prolong life if possible. Quality of life is also becoming increasingly important for patients with potentially curable cancer. Treatments are becoming increasingly effective and therefore more 59 Chapter 6: Systemic Therapy in Gynaecological Cancers patients are cured with many more experiencing longer remission periods. For example, an uncommon side effect of paclitaxel is chronic, disabling neuropathic pain. Although the importance of curing the cancer greatly outweighs the concerns of long-term adverse effects, long-term effects are becoming more prevalent and should be considered when planning treatment and ongoing care. Nowadays, quality of life is assessed as an integral part of clinical trials and several tools have been developed to measure quality of life. Surgery and Systemic Therapy Surgery is the standard of care for the majority of gynaecological cancers and forms an integral part of the management plan for ovarian, fallopian tube, primary peritoneal and uterine cancers. When chemotherapy is indicated after surgical treatment, it should be commenced as soon as possible to prevent regrowth of any residual cancer cells. Surgical planning and systemic therapy has become particularly important in the treatment of advanced epithelial ovarian, fallopian tube and primary peritoneal cancers. However, in a 60 substantial proportion of patients complete debulking is not achieved. This may be due to extensive preoperative disease with severe morbidity associated with poor nutritional state, hypoalbuminaemia, ascites, pleural effusions and risk of thromboembolism. In such patients, adjuvant chemotherapy is frequently delayed due to significant postoperative morbidity. Myelosuppression is a common side effect of chemotherapy, and rapid deterioration with life-threatening sepsis can occur with neutropenia. Although most patients have had recovery in their bone-marrow function by the time their surgery is planned, the medical team should confirm this prior to proceeding with elective surgery. A haematology consultation may be advisable if there are significant abnormalities that have not resolved spontaneously. Chapter 6: Systemic Therapy in Gynaecological Cancers Bevacizumab is an anti-angiogenic agent that may be indicated in selected patients with advanced-stage epithelial ovarian, fallopian tube and primary peritoneal cancers. Patients taking bevacizumab require careful surgical planning because it has been associated with multiple surgical complications, including delayed wound healing, wound dehiscence, surgical site bleeding, bowel perforation, venous thromboembolic disease and wound infection. Where elective surgery is planned, bevacizumab must be withheld for a minimum of 28 days prior to surgery and reintroduced into the chemotherapy regime at least 28 days after surgery, and only after the surgical incisions have fully healed. Patients who require emergency surgery while taking bevacizumab pose significant management challenges. If emergency surgery is necessary, then re-anastomosis of bowel must be avoided in these patients. The objective is to determine if a particular drug has antitumour activity against the tumour type in question. Summary Systemic therapies include cytotoxic chemotherapy, biological agents and hormonal therapies. Surgeons and anaesthetists must be familiar with these risks in order to provide optimal surgical management. Clinical Trials the process of developing a new drug is complex and takes many years for a new idea or concept to become a successful treatment option. When a new drug is being developed, it initially undergoes preclinical testing in the laboratory on human tumour cell lines and if they show promise further testing is conducted in animal models. This process itself can take several years and when the new drug is finally available for use in humans, rigorous testing through clinical trials are conducted in humans to evaluate efficacy, toxicity and response rates. The primary objective is to determine the maximum tolerated dose as defined by acceptable toxicity. The secondary objectives are to study pharmacokinetics and to describe any tumour response. There are important conceptual differences between the two classification systems. Collection and analysis of this data is paramount in assessing the effectiveness of the screening programme. A number of other terminologies have been used to describe these lesions, including incipient, precancerous, pre-neoplasia, or commonly intraepithelial neoplasia, as well as at times epithelial dysplasia or preinvasive neoplasia. Classification the terminology used to classify preinvasive disease of the cervix has been modified to reflect changes in our understanding of underlying biology and disease management. Protection against cervical cancer incidence offered by cervical screening ranges approximately from 60% to 85%. It has been suggested that an overall coverage of 80% can potentially decrease associated mortality rates by 95%. Although cytological screening may be less effective against cervical adenocarcinoma (which account for 15% of cervical cancers), it does have a substantial impact even in this subgroup. Sensitivity and specificity of cervical cytology have been reported to range between 30% to 87% and 86% to 100%, respectively. The current programme is as follows: First cervical cytology test by age 25 (women are invited 6 months prior to their 25th birthday). While most experts agree that cervical screening is effective, discussion continues over the most appropriate screening interval. Any gain in protection has to be considered against the considerable cost of the screening programme. The ideal age for starting routine cervical screening has been a matter of debate for some time. This is reflected by variances in practices across the countries of the United Kingdom. Screening has not been shown to reduce the incidence of, or mortality from, cervical cancer in women under the age of 25. Most women diagnosed with invasive cancer after the age of 50 have not participated fully in the cervical screening programme. It is a ubiquitous organism, and consequently both men and women are likely to contract this infection at some point, most commonly at around the time of coitarche. The virus is also responsible for other anogenital preinvasive diseases and cancers. A catch-up programme was also implemented for older girls up to 18 years of age from 2009 to 2011. Depending on the combination of the cytology result and colposcopic assessment, the following management options are usually considered: Conservative management with repeat cytology at prescribed interval Punch biopsies of small areas of a lesion, to aid in diagnosis and to facilitate management planning Excisional biopsy of abnormal transformation zone. When excision is used, the specimen should be removed as a single sample wherever possible. Removing the transformation zone in multiple fragments can increase the difficulties in histopathological assessment and if microinvasive disease is present, it may be difficult to stage or define completeness of excision. A punch biopsy may be inadequate for diagnosis in cases of abnormal high-grade glandular cytology. The endocervical excision margin must be shown to be clear of disease after treatment. If not, or if there is uncertainty, then a repeat procedure should be performed to obtain this. Subsequent colposcopy for screening abnormality should follow national guidelines. This type, like other forms of lower genital tract preinvasive disease, is more frequent among immunocompromised women. The recurrence rates at follow-up tend to be higher than for excision, but cosmesis is usually good.
Chicory Extract (Inulin). Torsemide.
- Weight loss.
- Lowering high levels of a kind of fat called triglycerides.
- Are there safety concerns?
- Dosing considerations for Inulin.
- What other names is Inulin known by?
- High cholesterol levels.
- What is Inulin?
- How does Inulin work?
- Constipation.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97001
Purchase 10mg torsemide amex
Oxycodone is available as single-ingredient medication in immediate-release and controlled-release formulations arteria buccinatoria cheap torsemide 20mg on line. At present, oxycodone is one of the most commonly abused pharmaceutical drugs in the U. It is used orally for relief of moderate-to-severe pain and is employed in a liquid formulation as a cough suppressant. Oxymorphone is extensively metabolized in liver and excreted as the 3- and 6-glucuronides. These effects include respiratory depression, nausea, vomiting, dizziness, mental clouding, dysphoria, pruritus, constipation, increased pressure in the biliary tract, urinary retention, hypotension, and, rarely, delirium. Increased sensitivity to pain may occur after analgesia has worn off, and removal of opiate receptor occupancy (abstinence, antagonism) may lead to a highly aversive state of withdrawal. In neonates or when the blood-brain barrier is compromised, lipophilic opioids may give more predictable clinical results than morphine. In adults, the duration of the analgesia produced by morphine increases progressively with age; however, the degree of analgesia that is obtained with a given dose changes little. However, as the pain subsides, the patient may exhibit sedation and even respiratory depression as the stimulatory effects of pain are diminished. All opioid analgesics are metabolized by the liver and should be used with caution in patients with hepatic disease. Renal disease also significantly alters the pharmacokinetics of morphine, codeine, dihydrocodeine, and meperidine. Although single doses of morphine are well tolerated, the active metabolite, morphine-6-glucuronide, may accumulate with continued dosing, and symptoms of opioid overdose may result. This metabolite also may accumulate during repeated administration of codeine to patients with impaired renal function. When repeated doses of meperidine are given to such patients, the accumulation of normeperidine may cause tremor and seizures. Similarly, the repeated administration of propoxyphene 372 may lead to naloxone-insensitive cardiac toxicity caused by accumulation of the metabolite norpropoxyphene. There is a growing body of data that examines gender differences in the responses to pain and analgesics (Mogil, 2012). Females have the majority of chronic pain syndromes, and surveys examining sex differences in acute pain models report either no sex difference or greater sensitivity in females. Data on sex differences in opiate analgesia have thus far been inconsistent (Loyd and Murphy, 2014). Morphine and related opioids must be used cautiously in patients with compromised respiratory function. Although many patients with such conditions seem to be functioning within normal limits, they are already using compensatory mechanisms, such as increased respiratory rate. The respiratory-depressant effects of opioids and the related capacity to elevate intracranial pressure must be considered in the presence of head injury or an already-elevated intracranial pressure. While head injury per se does not constitute an absolute contraindication to the use of opioids, the possibility of exaggerated depression of respiration and the potential need to control ventilation of the patient must be considered. Finally, because opioids may produce mental clouding and side effects such as miosis and vomiting, which are important signs in following the clinical course of patients with head injuries, the advisability of their use must be weighed carefully against these risks. Reduced blood volume causes patients to be considerably more susceptible to the vasodilating effects of morphine and related drugs, and these agents must be used cautiously in patients with hypotension from any cause. Morphine causes histamine release, which can cause bronchoconstriction and vasodilation. Morphine can precipitate or exacerbate asthmatic attacks and should be avoided in patients with a history of asthma. Other receptor agonists associated with a lower incidence of histamine release, such as the fentanyl derivatives, may be better choices for such patients. The effects usually are manifested as urticaria and fixed eruptions; contact dermatitis in nurses and pharmaceutical workers also occurs. Wheals at the site of injection of morphine, codeine, and related drugs are likely secondary to histamine release. Anaphylactoid reactions have been reported after intravenous administration of codeine and morphine, but such reactions are rare. In addicts who use intravenous heroin, such reactions may contribute to sudden death, episodes of pulmonary edema, and other complications. Compared to morphine, this agent is about seven times more potent and may produce less nausea and vomiting. Meperidine causes pupillary constriction, increases the sensitivity of the labyrinthine apparatus, and has effects on the secretion of pituitary hormones similar to those of morphine. Meperidine has well-known local anesthetic properties, particularly noted after epidural administration. The effects of meperidine on the cardiovascular system generally resemble those of morphine, including the release of histamine following parenteral administration. Intramuscular administration of therapeutic doses of meperidine does not affect heart rate significantly, but intravenous administration frequently produces a marked increase in heart rate. As with other opioids, clinical doses of meperidine slow gastric emptying sufficiently to delay absorption of other drugs significantly. Administered before an oxytocic, meperidine does not exert any antagonistic effect. Therapeutic doses given during active labor do not delay the birth process; in fact, frequency, duration, and amplitude of uterine contraction may be increased. The peak plasma concentration usually occurs at about 45 min, but the range is wide. Metabolites are the N-demethyl product, normeperidine, and the hydrolysis product, meperidinate, both of which may be conjugated. The onset of analgesic effect is faster (within 10 min) after subcutaneous or intramuscular administration, and the effect reaches a peak in about 1 h, corresponding closely to peak concentrations in plasma. Peak respiratory depression is observed within 1 h of intramuscular administration, and there is a return toward normal starting at about 2 h. In terms of total analgesic effect, meperidine is about one-third as effective when given orally as when administered parenterally. Single doses of meperidine can be effective in the treatment of postanesthetic shivering. Meperidine crosses the placental barrier, and even in reasonable analgesic doses causes a significant increase in the percentage of babies who show delayed respiration, decreased respiratory minute volume, or decreased O2 saturation or who require resuscitation. Fetal and maternal respiratory depression induced by meperidine can be treated with naloxone. The overall incidence of untoward effects is similar to those observed after equianalgesic doses of morphine, except that constipation and urinary retention and nausea may be less common. Patients who experience nausea and vomiting with morphine may not do so with meperidine; the converse also may be true. In patients or addicts who are tolerant to the depressant effects of meperidine, large doses repeated at short intervals may produce an excitatory syndrome that includes hallucinations, tremors, muscle twitches, dilated pupils, hyperactive reflexes, and convulsions. As a result of these properties, meperidine is not recommended for the treatment of chronic pain because of concerns over metabolite toxicity. The more prominent is an excitatory reaction ("serotonin syndrome") with delirium, hyperthermia, headache, hyper- or hypotension, rigidity, convulsions, coma, and death. Chlorpromazine increases the respiratory-depressant effects of meperidine, as do tricyclic antidepressants (but not diazepam). Concurrent administration of drugs such as promethazine or chlorpromazine also may greatly enhance meperidine-induced sedation without slowing clearance of the drug.
Discount torsemide 10mg line
Therapeutic Uses For epithelial ovarian blood pressure monitor reviews torsemide 20 mg with visa, fallopian tube and primary peritoneal cancers, carboplatin is used in combination with paclitaxel or as a single agent, in the adjuvant and neoadjuvant setting. It is also used in combination or as monotherapy for recurrent platinum-sensitive disease. Its further use in gynaecological cancers includes treatment of uterine cancers in the adjuvant and metastatic setting either as a single agent or in combination with paclitaxel. Cisplatin is given weekly concurrently with radiotherapy for the treatment of cervical, vaginal and vulval cancers. Carboplatin, paclitaxel and bevacizumab is used to treat metastatic cervical cancer. Both drugs are usually administered every 3 weeks, but cisplatin is given weekly (at a lower dose) when used concurrently with radiotherapy. Both are renally excreted and therefore dose modification is often not needed if liver function is impaired. For separation to occur, the microtubule structure must undergo polymerisation followed by depolymerisation. Both paclitaxel and docetaxel promote microtubule assembly and then stabilise the microtubule structure, preventing it from undergoing depolymerisation. This prevents chromosome separation and the cell is unable to divide and will undergo programmed cell death. Docetaxel is given every three 53 Chapter 6: Systemic Therapy in Gynaecological Cancers weeks, whereas paclitaxel can be given either weekly or every 3 weeks. Adverse Effects Both agents are administered with high-dose steroids and antihistamines to prevent hypersensitivity reactions. Although desensitisation programmes have been shown to be successful in some patients, they are time-consuming and may lead to treatment delay. Docetaxel tends to cause more myelosuppression than paclitaxel, whereas paclitaxel tends to cause more peripheral neurotoxicity. This effect is thought to be due to its effect on -tubulin, a neuro-transport protein found in peripheral nerves. Although the neuropathy can be temporary and improves following treatment completion, many patients can develop long-term loss of sensation in their fingers and toes. Cardiotoxicity is dosedependent and lifetime dose is generally aimed to be less than 450 mg/m2. In patients with cardiac disease or previous mediastinal radiotherapy, a lower maximum lifetime dose is advised. It is also a vesicant, which means that it can cause tissue inflammation, blistering and necrosis if it extravasates (leaks from the vein into surrounding tissues). Therapeutic Uses Paclitaxel is frequently used in combination with carboplatin in the treatment of epithelial ovarian, fallopian tube and primary peritoneal cancers. Paclitaxel alone (monotherapy) is used in platinum-refractory disease and also has activity in uterine cancers. Doxorubicin is mainly used as a single agent in relapsed uterine cancers and in metastatic leiomyosarcoma of the uterus. This converts the drug into a slow-release preparation, which alters its activity and side-effect profile. Doxorubicin is generally Chapter 6: Systemic Therapy in Gynaecological Cancers Administration Topotecan is given intravenously once daily over five consecutive days in three weekly cycles. Etoposide can be given orally or intravenously and dosing depends on the route of administration and the indication. Adverse Effects Both drugs can cause myelosuppression, alopecia, diarrhoea and liver toxicity. Rarely etoposide can cause myocardial infarction, cardiac arrhythmias and acute leukaemia. It can also be given orally for relapsed epithelial ovarian, fallopian tube and primary peritoneal cancers, however response rates can be variable as the bioavailability is different in different patients. Administration Bleomycin is most commonly given intravenously but can also be given intramuscularly. Adverse Effects the most significant side effect of bleomycin is pulmonary toxicity. Bleomycin pneumonitis is dose- and agerelated, with smokers and patients on oxygen therapy most at risk. Biological Agents Basic Principles Cancer research is continually identifying novel mechanisms by which cancers can be targeted to prevent their growth and spread. Adverse Effects the most significant side effect of gemcitabine is myelosuppression, predominantly affecting the production of platelets and granulocytes. Administration Bevacizumab is given intravenously and dosed according to body weight. Cases of myelodysplastic syndrome, acute myeloid leukaemia and pneumonitis have also been reported, and although relatively rare they can be fatal. Niraparib also causes myelosuppression in particular thrombocytopenia and anaemia. Adverse Effects Bevacizumab increases the risk of hypertension, arterial and venous thromboembolic events, haemorrhage, gastrointestinal perforation, fistulae formation and also delays wound healing. Due to these effects bevacizumab should be avoided 28 days before and after surgery, and not re-commenced until the wound has fully healed. Therapeutic Uses It is used as maintenance treatment following first-line combination chemotherapy for high-risk epithelial ovarian, fallopian tube and primary peritoneal cancers including stages 3 and 4 disease with macroscopic residual disease of >1 cm after debulking surgery. It is also used in the first-line treatment of metastatic cervical cancer in combination with carboplatin and paclitaxel. Hormonal Therapies Basic Principles Some types of cancer express hormone receptors (oestrogen and progesterone receptors). These can act as growth factors in the presence of the hormone activating the hormone receptor resulting in cancer cell growth and multiplication. By reducing the hormone circulating in the body or by blocking the receptor, cancer growth can be prevented. In premenopausal women the main site of oestrogen synthesis is the ovary, whereas in postmenopausal women oestrogen synthesis occurs in the adipose tissue through the action of the enzyme aromatase. This prevents the activation of oestrogen-dependent genes, thus preventing oestrogen-dependent cell growth. Administration 56 Olaparib is given orally at a dose of 400 mg twice a day as maintenance therapy after platinum-based Dosing Tamoxifen is given orally at a daily dose of 20 mg. Chapter 6: Systemic Therapy in Gynaecological Cancers Adverse Effects Common adverse effects include hot flushes, vaginal discharge and irregular vaginal bleeding. It is also associated with an increased risk of endometrial pathology, including a small increased risk of endometrial cancer. They also inhibit oestrogen-mediated cell proliferation, as progesterone can inhibit oestrogen receptor gene expression and increase oestrogen receptor degradation. Administration Medroxyprogesterone acetate is usually given orally at a dose of 200 mg once a day. Therapeutic Uses Tamoxifen is generally limited to use in asymptomatic patients with low volume, relapsed epithelial ovarian, fallopian tube and primary peritoneal cancers. Adverse Effects Common side effects include weight gain, hot flushes, peripheral oedema, irregular menstruation and deranged liver function. Progestogens can also increase the risk of thromboembolic events including venous thromboembolism, myocardial infarction and stroke. By inhibiting the action of the P450 aromatase enzyme in adipose tissue circulating levels of oestrogen are reduced, which prevents oestrogen-dependent cancer growth. Therapeutic Uses Progestogens are used in the treatment of metastatic endometrial cancers where response rates of up to 30% are seen. Administration Anastrazole is given orally at a dose of 1 mg per day and letrozole is also taken orally at 2.
Buy cheap torsemide 10mg line
In the past arteria facial order torsemide with amex, surgeons used the paramedian incision to minimise the complications of midline incision (that injures the weakest part of the abdominal wall). The use of modern suture materials and mass closure have more recently minimised this need, and this approach is rarely used. Recent advances in minimal access surgery have largely replaced the transverse incision, as the majority of procedures that were previously performed through these incisions are now carried out laparoscopically. Although transverse incisions are relatively uncommon in modern practice of gynaecological oncology surgery, they are still used in obstetrics, benign gynaecology and in cases of endometrial or cervical cancer surgery with large uterine size where intact removal of the uterus is not feasible with laparoscopy and morcellation is contraindicated. A modification of the suprapubic transverse incision, the Maylard incision, provides better access when necessary as the rectus muscle is divided and the inferior epigastric vessels are ligated. Extraperitoneal pelvic and para-aortic lymph node dissections are now commonly performed laparoscopically. Laparoscopic Incisions the choice of laparoscopic surgical approach is preferable in certain tumour sites such as cervical and endometrial cancer. Minimal access surgery has been associated with improved recovery, reduced pain, smaller scars and wound complications and better visualisation of the operative field for some cancers, without compromise to the surgical and oncological outcomes (Box 8. There is no agreement on which approach is superior; however surgeons should be able to use either of these if needed. The majority of surgeons use 5 mm ancillary suprapubic and left lateral ports and an additional 5 mm right lateral port for the assistant when operating in the pelvis. Some surgeons prefer to use two operative ports on the left side, while some use a right and left lateral incision for small procedures. The monopolar current (red arrows) runs from the active electrode through the patient and grounds to the return electrode (blue square) on the patient. The current flows (red arrows) only through the tissue that is held between the jaws of the grasper that includes both the active and the passive electrode. Principles of Energy Devices Traditional surgical and haemostatic techniques relied predominantly on the use of scalpel, scissors and haemostatic sutures. These surgical techniques have been largely complimented or replaced by advanced haemostasis and dissecting techniques that use different energy sources. Minimal access surgery relies almost exclusively on energy sources, with increasing use in open surgery. An electrosurgical unit produces the current which flows at high density into the small surface tip (needle, scissors, etc. In cutting mode, the waveform uses high-frequency, lowvoltage current and cuts with desiccation. With 84 coagulation and fulguration, a low-frequency, high-voltage waveform is required and heating occurs by direct tissue contact. New technologies have feedback sealing properties and integrated dissection capabilities. They use a function of time, pressure and heat generation for sealing and/or cutting. These devices are precise cutting and haemostatic instruments with minimal smoke and tissue charring. The laser may be used for Chapter 8: Surgical Principles in Gynaecological Oncology cutting, while coagulation properties are limited to small vessels. Laser energy is not commonly used in gynaecological oncology surgery but it is a useful tool in the surgical treatment of endometriosis. Complications of Energy Devices Complications related to the use of diathermy can occur. Advanced training of surgeons in the principles of energy sources, the risks and potential complications, as well as advances in the technology have now substantially reduced untoward events. Although novel technologies have introduced energy feedback to alarm for possible problems with the equipment, the surgeons should be aware of these complications. This should be considered when there is a problem with the energy source rather than increasing the power to reach the necessary strength. Direct coupling occurs when the active electrode is in close proximity to , or touching another metal instrument. Current will flow through the pathway of least resistance, and potentially damage adjacent structures that are in direct contact with the secondary instrument. Capacitive coupling occurs in laparoscopic surgery when current is transferred from an insulated instrument to an uninsulated instrument or tissue through capacitance. Capacitance happens when there is storage of electrical charge, and arises in tissue or metal instruments running parallel to , but not directly in contact with the active electrode. This current may seek an alternative path, and create a high-density current that may transfer to adjacent tissues or other conductive instruments without direct contact. Thermal injury occurs predominantly with the use of monopolar diathermy that produces very high tissue heating. The tissue damage extends far from the point of the contact of the electrode to the tissue. Although thermal spread and tissue damage is much more controlled with bipolar diathermy, the two jaws of the instrument become very hot and care should be taken to protect the surrounding tissues. Unintended activation of the instrument while handling sensitive structures can occur. Unrecognised thermal injuries of the bowel and urinary tract are some of the most common complications. Attention to detail, and cooling the tissue and instruments with irrigation and wash may be necessary. When using the laser, care should be taken to ensure that the beam does not affect tissue in front or behind the target. The staff using the laser should be specially trained and wear protective eyewear. Careful consideration is needed in placement of the primary and accessory ports due to the change in surface anatomical landmarks that arise in obesity. Port placement therefore needs to be perpendicular or directed cranially in relation to the skin at the umbilicus to prevent tunnelling through subcutaneous tissue. If the abdominal pannus is very large, then the umbilicus may hang lower than the pelvis. Laparoscopic Surgery Laparoscopic surgery should be considered in all cases of early-stage endometrial and cervical cancer when the uterus is not grossly enlarged. Cochrane review of laparoscopic versus open hysterectomy for early-stage endometrial cancer demonstrated no statistically significant difference in the risk of death or disease recurrence between women who underwent laparoscopy and those who underwent laparotomy. In addition, a meta-analysis (a) (b) reported that the rate of severe postoperative adverse events was significantly lower in the laparoscopy group compared with the laparotomy group. There are no randomised controlled trials in regards to open versus laparoscopic surgery for earlystage cervical cancer in regards to survival, although retrospective studies suggest that the laparoscopic approach is safe. The design is also ergonomically superior to laparoscopic surgery as the surgeon operates sitting down, although the surgery can take longer to perform. Due to higher costs, the use of the robot will depend on individual institutional needs and expertise. Fertility Sparing Approaches In some situations, women may present with malignancy before they have completed their family. Where fertility is desired, careful consideration, counselling and an up-to-date view of the latest literature are necessary. Summary this article has highlighted general surgical principals in gynaecology oncology. This encompasses a broad range of tools in order to achieve the goal of ensuring that the patient is optimised for surgery; the surgical procedure is carefully planned and completed and postoperative recovery is successful. The prevention and early recognition of any complication should be prioritised in the high-risk setting. Most gynaecological oncologists now offer laparoscopic surgery as a standard of care in the surgical management of endometrial and cervical cancers. The survival outcomes in endometrial and cervical cancers appear similar after laparoscopic surgery and laparotomy.
Buy cheapest torsemide
The major adverse effects of clonidine are dry mouth and sedation arteria jejunales torsemide 20 mg low price, which may diminish in intensity after several weeks of therapy. These effects of clonidine frequently are related to dose, and their incidence may be lower with transdermal administration of clonidine. Withdrawal reactions follow abrupt discontinuation of long-term therapy with clonidine in some hypertensive patients (see Chapter 28). Cardiovascular System Apraclonidine Apraclonidine is a relatively selective 2 receptor agonist that is used topically to reduce intraocular pressure with minimal systemic effects. This agent does not cross the blood-brain barrier and is more useful than clonidine for ophthalmic therapy. Apraclonidine is useful as short-term adjunctive therapy in patients with glaucoma whose intraocular pressure is not well controlled by other pharmacological agents. The drug also is used to control or prevent elevations in intraocular pressure that occur in patients after laser trabeculoplasty or iridotomy (see Chapter 69). Heart rate often is reflexly slowed; with large doses, cardiac arrhythmias may occur. Cardiac output is not enhanced by therapeutic doses, and cerebral blood flow does not change much. The l-isomer is slightly more potent than the d-isomer in its cardiovascular actions. Other Smooth Muscles Brimonidine Brimonidine is a clonidine derivative and 2-selective agonist that is administered ocularly to lower intraocular pressure in patients with ocular hypertension or open-angle glaucoma. In general, smooth muscles respond to amphetamine as they do to other sympathomimetic amines. The contractile effect on the sphincter of the urinary bladder is particularly marked, and for this reason amphetamine has been used in treating enuresis and incontinence. If enteric activity is pronounced, amphetamine may cause relaxation and delay the movement of intestinal contents; if the gut already is relaxed, the opposite effect may occur. The response of the human uterus varies, but there usually is an increase in tone. Like clonidine, guanfacine lowers blood pressure by activation of brainstem receptors with resultant suppression of sympathetic activity. The psychic effects depend on the dose and the mental state and personality of the individual. Performance of simple mental tasks is improved, but, although more work may be accomplished, the number of errors may increase. Prolonged use or large doses are nearly always followed by depression and fatigue. Many individuals given amphetamine experience headache, palpitation, dizziness, vasomotor disturbances, agitation, confusion, dysphoria, apprehension, delirium, or fatigue. In general, amphetamine prolongs the duration of adequate performance before fatigue appears, and the effects of fatigue are at least partly reversed, most strikingly when performance has been reduced by fatigue and lack of sleep. Such improvement may be partly due to alteration of unfavorable attitudes toward the task. However, amphetamine reduces the frequency of attention lapses that impair performance after prolonged sleep deprivation and thus improves execution of tasks requiring sustained attention. When the drug is discontinued after long use, the pattern of sleep may take as long as 2 months to return to normal. Amphetamine and some other sympathomimetic amines have a small analgesic effect that is not sufficiently pronounced to be therapeutically useful. Amphetamine stimulates the respiratory center, increasing the rate and depth of respiration. In normal individuals, usual doses of the drug do not appreciably increase respiratory rate or minute volume. Nevertheless, when respiration is depressed by centrally acting drugs, amphetamine may stimulate respiration. Amphetamine and similar drugs have been used for the treat- ment of obesity, although the wisdom of this use is at best questionable. Weight loss in obese humans treated with amphetamine is almost entirely due to reduced food intake and only in small measure to increased metabolism. The site of action probably is in the lateral hypothalamic feeding center; injection of amphetamine into this area, but not into the ventromedial region, suppresses food intake. Hence, continuous weight reduction usually is not observed in obese individuals without dietary restriction. These mechanisms include amphetamine-induced exchange diffusion, reverse transport, channel-like transport phenomena, and effects resulting from the weakly basic properties of amphetamine. Amphetamine analogues affect monoamine transporters through phosphorylation, transporter trafficking, and the production of reactive oxygen and nitrogen species. These mechanisms may have potential implications for neurotoxicity as well as dopaminergic neurodegenerative diseases (discussed further in the chapter). These effects can be prevented in experimental animals by inhibiting tyrosine hydroxylase and thus catecholamine synthesis. With still higher doses of amphetamine, disturbances of perception and overt psychotic behavior occur. The acute toxic effects of amphetamine usually are extensions of its therapeutic actions and as a rule result from overdosage. Confusion, aggressiveness, changes in libido, anxiety, delirium, paranoid hallucinations, panic states, and suicidal or homicidal tendencies occur, especially in mentally ill patients. However, these psychotic effects can be elicited in any individual if sufficient quantities of amphetamine are ingested for a prolonged period. Cardiovascular effects are common and include headache, chilliness, pallor or flushing, palpitation, cardiac arrhythmias, anginal pain, hypertension or hypotension, and circulatory collapse. Fatal poisoning usually terminates in convulsions and coma, and cerebral hemorrhages are the main pathological findings. Toxic manifestations occasionally occur as an idiosyncratic reaction after as little as 2 mg but are rare with doses less than 15 mg. Treatment of acute amphetamine intoxication may include acidification of the urine by administration of ammonium chloride; this enhances the rate of elimination. Severe hypertension may require administration of sodium nitroprusside or an adrenergic receptor antagonist. Chronic intoxication with amphetamine causes symptoms similar to those of acute overdosage, but abnormal mental conditions are more common. A psychotic reaction with vivid hallucinations and paranoid delusions, often mistaken for schizophrenia, is the most common serious effect. Recovery usually is rapid after withdrawal of the drug, but occasionally the condition becomes chronic. In these persons, amphetamine may act as a precipitating factor hastening the onset of incipient schizophrenia. The abuse of amphetamine as a means of overcoming sleepiness and of increasing energy and alertness should be discouraged. Amphetamine use is inadvisable in patients with anorexia, insomnia, asthenia, psychopathic personality, or a history of homicidal or suicidal tendencies. Tolerance almost invariably develops to the anorexigenic effect of amphetamines and often is seen also in the need for increasing doses to maintain improvement of mood in psychiatric patients. Tolerance is striking in individuals who are dependent on the drug; a daily intake of 1. Development of tolerance is not invariable, and cases of narcolepsy have been treated for years without requiring an increase in the initially effective dose.
