
Buy epivir-hbv 150 mg cheap
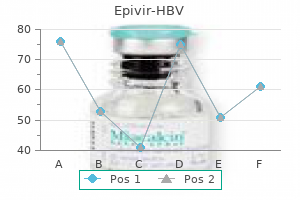
Lymphocytes Lymphocytes are critical for the development of asthma and are found in the airways of asthmatic subjects in proportion to disease severity (Chapter 11) symptoms esophageal cancer purchase epivir-hbv 100mg online. However, the exact interpretation of this has undergone a substantial change in recent years. A wide range of different T cell subtypes have been described associated with asthma in its different forms. By operating together, these three epithelial-derived cytokines have the potential to bridge innate and adaptive immunity to sustain the Th2 response toward a more chronic state characteristic of asthma. These different leukocyte subsets generate cytokines that influence different cell types and the attendant inflammatory response, driving allergic airway inflammation and airway hyperresponsiveness. The recent recognition of a new, innate type 2 immune effector leukocyte has brought renewed focus on the origins of the T2 response, especially in nonallergic eosinophilic asthma. They exist in naturally occurring (thymus-derived or nTreg) or inducible (iTreg) forms. Th17 cells are a distinct T cell lineage that does not share developmental pathways with either Th1 or Th2 cells. Th17 cells regulate both neutrophilic and macrophage inflammation in autoimmune disease and especially psoriasis and have been implicated in asthma and its corticosteroid insensitivity. These failed resolution mechanisms could contribute to the persistence of airway inflammation in severe asthma. Apoptosis, or programmed cell death of eosinophils, is intended to limit tissue inflammation and injury. However, the number of apoptotic eosinophils is significantly reduced in the bronchial mucosa of asthmatic compared with normal subjects, and these values are inversely correlated with the disease severity. Thus part of the chronicity of asthma may be caused by reduced downregulation of eosinophilic inflammation. Tregs are identified through their coexpression of the transcription factor Neutrophils the role of neutrophils in asthma is still undefined but of increasing interest, with studies indicating that neutrophils may play a role in select asthmatic subtypes (Chapter 17). Treg cell development and suppression is fundamental in protecting normal airways against allergen sensitization. Treg cells are also induced in response to allergen-specific immunotherapy and promote the production of the "blocking" antibody class IgG4. Solid arrows indicate stimulatory signals; blunt arrows indicate inhibitory signals. Neutrophil accumulation in the airway is also a hallmark of patients who die suddenly from asthma, during viral exacerbations. Neutrophils have potent proinflammatory functions, with the release of various cytokines. This upregulation of innate immune receptors may occur in response to increases in airway endotoxin, bacterial colonization, or respiratory viruses. Epithelial Cells the airway epithelium is a highly specialized physicochemical barrier preventing the ingress of inhaled environmental agents into the lung tissue (Chapter 19). In addition to its physical barrier function, the epithelium coordinates the recruitment, activation, and differentiation of immune and inflammatory cells, particularly in response to exogenous stimuli (pollutants, allergens, viruses), which have the potential to cause epithelial damage. Inflammatory cell infiltration is targeted to sites of epithelial damage by the upregulated expression of adhesion molecules. In asthma these soluble mediators support mast cell, eosinophil, and basophil survival as well as isotype switching of B cells to IgE. Loosening of columnar cell tight junctions, and in extreme circumstances, shedding of columnar epithelial cells (Creola bodies), is a characteristic feature of asthma, as is the associated marked goblet cell metaplasia and mucus hypersecretion. There is evidence of reduced tight-junction assembly,106 oxidant stress and increased markers of apoptosis in asthmatic epithelium, and reduced antioxidant enzyme activity, such as superoxide dismutase and glutathione peroxidase. Injury can also be induced by environmental agents, such as exogenous pollutants or oxidants, allergens with intrinsic protease activity, such as Der p 1 and Der p 9, and respiratory viruses. These further disrupt epithelial tight junctions, leading to a more porous epithelium. A downstream consequence of environmental stress on this susceptible epithelium is an initiation and secondary amplification of inflammatory cell influx. The airway epithelium in asthma is similar to a chronic wound: more susceptible to environmental injury and exhibiting reduced repair. Reduced ability to proliferate creates a "chronic wound" scenario in the airways with increased growth factor release. Increased expression of p21(waf) cyclin-dependent kinase inhibitor in asthmatic bronchial epithelium. The extent of epithelial damage in asthma correlates with disease severity and with increased expression of the epidermal growth factor receptor, a key regulator of epithelial function. These findings suggest that the epithelium in asthma has an inadequate or prolonged repair mechanism that contributes to airway remodeling. Cell-cell communication between the epithelium and the subepithelial fibroblasts has been examined in a number of coculture systems. Epithelial cells from asthmatic but not normal or atopic normal children grown as monolayers exhibit reduced capacity for wound closure after scrape injury, resulting partly from reduced generation of fibronectin. Threshold response (a, sensitivity), slope of dose-response (b, reactivity), and maximal response (c, plateau) can be obtained in normal subjects and patients with mild asthma. The degree of loss in lung function has been shown to be related to the duration of asthma. Rapid "decliners" may be one subphenotype that differentiates from more classic asthma. The presence of irreversible airflow obstruction correlates with the number of airway neutrophils (measured in induced sputum) and with neutrophil activation, as measured by sputum myeloperoxidase. If irreversible airflow obstruction is caused by persistent airway inflammation, early treatment with effective therapy. In asthma, remodeling is a multifactorial process leading to structural changes that involve complex interactions among cytokines, growth factors, and cell adhesion molecules, leading to variable combinations of proliferation of microvessels, nerves, and smooth muscle; mucous metaplasia; and deposition of matrix such as collagens and proteoglycans. The end result is an airway with thicker walls that may be either more or less responsive to external stimuli, along with reduced airway caliber. Compared with postmortem tissue from nonasthmatic controls, total wall area in cartilaginous and membranous airways of all sizes is increased, including "small airways" with an internal perimeter of less than 2 mm. In postmortem tissue the area of the submucosa occupied by vessels was greater in asthmatic than nonasthmatic participants, but the number of vessels per unit area was similar in the two groups, indicating that angiogenesis was a feature of asthma, but that this was appropriate for the overall increase in submucosal area. Perhaps the most characteristic pathologic feature in bronchial biopsy specimens in atopic asthma is deposition of excess connective tissue beneath the airway epithelium. In asthmatic patients who are also smokers, the irreversible component of the airflow obstruction may be a result of smoking. Some asthmatic patients with irreversible airflow obstruction have never smoked, however, and the irreversible airflow obstruction results from persistent asthma. An Australian study found a greater decline in lung function in asthmatic than in normal subjects (50 versus 35 mL/year) followed for 18 years, as well as variability in the asthmatic population, with much greater rates of decline in some patients. Directly below the lamina reticularis is a population of subepithelial mesenchymal cells with ultrastructural features of myofibroblasts. These cells correspond to the attenuated fibroblast sheath described in the basement membrane zone in rat trachea and to similar cell populations in small airways and in the pulmonary interstitium. There are increased numbers of myofibroblasts in bronchoscopic biopsy specimens from asthma and a correlation between cell number and depth of the lamina reticularis. This differentiation also selects a more contractile phenotype than myofibroblasts matured from normal airway fibroblasts, suggesting a link to the increased airway smooth muscle. Increased airway smooth muscle mass may be related to a combination of airway infiltration of myofibroblasts, neighboring airway smooth muscle cells in the bundle, or circulating hematopoietic progenitor cells. The fibrotic process in asthma may also extend to the deeper layers of the airway wall. Other bronchoscopy-based studies in adults and children with asthma have focused on airway smooth muscle and vascularity, showing disease severity-related differences. Also, goblet cell hyperplasia in the airway epithelium, with an accompanying increase in stored mucin, occurs even in mild and moderate asthma, but mucus plugging becomes lifethreatening in severe asthma. The potential for bidirectional communication between epithelial and mesenchymal cells has been demonstrated using three-dimensional in vitro coculture systems. When guinea pig tracheal epithelial cells are cultured on an amniotic membrane with tracheal fibroblasts cultured beneath, they differentiate into a pseudostratified layer that closely resembles the tracheal epithelium in vivo. Morishima and coworkers122 used this model to examine the consequences of epithelial injury induced by mechanical scraping.
Order epivir-hbv on line
Human studies using more advanced technologies strongly suggest environmental influences treatment resistant anxiety order line epivir-hbv, often collectively referred to as the exposome, are more important than heritable traits in shaping the immune system and in protecting against development of allergic disease. For example, plasma metabolomics has revealed shared maternal/ fetal metabolites,216,217 and a link between labor-induced mediators and immune dysfunction in neonates who develop food allergy was recently demonstrated. The utility of measuring cord blood serum IgE for predicting subsequent development of atopic disease is generally thought to be a poor predictor, although this remains controversial. Mechanism for poor T-independent response remains unclear but likely secondary to decreased memory B cells, immaturity of toll-like receptors, and diminished marginal-zone B cells in infants. Cord blood V24-V11 natural killer T cells display a Th2-chemokine receptor profile and cytokine responses. Cord serum immunoglobulin E as a risk factor for allergic symptoms and sensitization in children and young adults. In comparison, tTreg cell maturation was significantly delayed in age-matched atopic children. IgG Some studies show higher allergen-specific IgG1 and IgG4 subclasses in young children developing allergic disease, although significance is not clear. Effector T Cell Responses100,199 Proliferation Several studies report higher frequency and magnitude of proliferative responses to allergens compared with aged-matched nonallergic children. Cytokine responses Early (presymptomatic) increase in allergen-specific Th2 cytokine production (often detected by 6 months of age in children who develop subsequent allergic disease). Regulatory Function85,155,219,220 Percentage Reduced proportion of Treg of Treg cells in high-risk neonates cells Neonatal Foxp3 expression Suppressive capacity Reduced Foxp3 expression c Trends for lower percentage of Treg cells at birth (inconclusive) Trends for lower Foxp3 expression at birthc Trends for reduced suppressive capacityc Reduced suppressive capacityc Regulatory Function85,155,219,220 Percentage of Preliminary studies suggest reduced thymic Treg, Foxp3 Treg and expression, and suppressive function in children with Foxp3 atopy, but more studies are needed. Other Adaptive Immune Cells As the hallmark of the allergic response, production of IgE by classswitched B cells is the most well-recognized immunologic difference in allergic individuals, with early studies showing the steadily increasing titers of specific IgE to allergens in allergic children. Against a genomic background, environmental exposures affect molecular and microbial systems, variation of which can be measured by using omics technologies and statistical modeling with the assistance of high-performance computing to address clinical and biological questions. Maturation of key aspects of innate and adaptive immune function is incomplete at birth, resulting in susceptibility to a variety of diseases, including infections and allergic sensitization. The degree of impairment of immune competence during early life is highly variable; however, children with an atopic family history cluster toward the "slow development" end of the population spectrum, displaying reduced functionality at birth and taking longer to attain adult-equivalent levels of immune competence. Microbial products are arguably the most powerful immunostimulants in the early environment and likely play a key role in the maturation of innate and adaptive immune responses, which together may prevent inappropriate allergic Th2 responses. These observations suggest that dysregulated inflammatory responses may have a role in abnormal T cell development. However, a consensus on the trajectory of innate immune function and potential biomarkers of allergic disease risk is currently lacking. Independent studies from different continents have reported increased microbial diversity in farm compared with rural nonfarm household environments, or between unique agrarian cultures. This relationship is understudied in humans but is critical to determine rational approaches to improving health via modulation of the microbial environment. The role of other innate cells in the pathogenesis of allergic disease is less clear. The most critical periods for immune maturation and allergen sensitization occur simultaneously, beginning in utero and during the first 2 years of life. As mentioned previously, the hygiene hypothesis posits that environmental and exogenous exposures modulate the maturing immune system and can direct the development of allergic immune responses. Neonates born to mothers on European farms were found to have increased proinflammatory. Most work in this area has focused on bacterial exposures, particularly the airborne environment. In fact, endotoxin levels are reported to be elevated in farm households compared with rural nonfarm households. The immune system reaches into every organ, where it influences local development, and similarly, each developing tissue system will have a unique influence on the development of its local immune network to best suit its needs. Allergic diseases are manifest in specific tissues, generally in those where environmental allergens are encountered and initially processed, such as the airways (asthma, allergic rhinitis), skin (eczema), and gut (food allergy), although the consequences of these conditions can often be seen elsewhere. Thus the developmental aspects of these local tissues and how their immunomodulatory properties evolve in both health and disease need to be better understood, as well as how they are modified by modern environmental changes. This must include a better understanding of other interrelated organ systems, including the bone marrow (as a primary source of immune progenitor populations) and lymphoid organs. Further, the role of even earlier events in the developing placenta and the maternal-fetal interface are likely important antecedents in the pathogenesis of disease, contributing to the perinatal differences in immune function that can lead to clinical disease within the first months of life. Although addressed in more detail in other chapters, it is useful briefly to consider events in the tissues where allergens are encountered, because they are highly relevant to the development of specific allergic diseases of the airways, skin, and gastrointestinal tract. As predisposing events in the development of asthma, the growing list of maternal exposures shown to decrease fetal lung growth includes tobacco smoke, air pollution, household chemicals and cleaning agents, infections, and maternal diet and nutrition. There is also growing interest in the defects in epithelial integrity now seen frequently with rising rates of eczema, which may increase the permeability to allergens and risk of sensitization through the (less tolerogenic) cutaneous route. Although barrier dysfunction in eczema may also result from many environmental factors, this highlights that cutaneous gene pathways are important predisposing factors for systemic atopic disease. As discussed earlier, events in the developing gut are important in understanding the rising rates of food allergy. The normal development of oral tolerance is an antigen-driven process and may logically depend on regular exposure to foods and other antigens during a critical early developmental window. These processes are also likely to depend on other conducive exposures, such as favorable gut colonization,285 breast milk,286 and other nutritional immunomodulatory factors. A range of factors (microbial contact, diet, cigarette smoke, other airborne pollutants) are known to modify fetal immune function and increase the risk of subsequent allergic disease. The early postnatal period also represents a critical period for environmental influences. Notably, most factors are now known to exert effects on immune programming by epigenetically activating or silencing immune-related genes. These pathways provide a mechanism through which modern environmental changes may be inducing inappropriate gene expression patterns that promote allergic disease. Although evidence shows direct immune effects, environmentally induced changes in the milieu of local tissues may have further, indirect effects on local immune networks as they are "conditioned" within that local tissue. Clinicians must understand how factors driving the rise in various immune-mediated diseases can be modified toward prevention strategies. It is hoped that this early period of life will provide unique "windows of opportunity" for modulating these responses before they become persistent. A sound understanding of all the developing elements of the immune system and their interaction with endogenous and exogenous environmental stimuli is essential. As past experience has taught, our understanding of immune development will clearly evolve with investigative capacity. As history has also shown, this will almost certainly mean modifying, extending, or even dismantling past ideas as the field progresses. At the crossroads between tolerance and aggression: revisiting the "layered immune system" hypothesis. Maternal alloantigens promote the development of tolerogenic fetal regulatory T cells in utero. An exposome perspective: Early-life events and immune development in a changing world. Prenatal lipopolysaccharide-exposure prevents allergic sensitisation and airway inflammation, but not airway responsiveness in a murine model of experimental asthma. Fish oil supplementation in pregnancy modifies neonatal allergen-specific immune responses and clinical outcomes in infants at high risk of atopy: a randomised controlled trial. The mechanism or mechanisms driving atopic asthma initiation: the infant respiratory microbiome moves to center stage. Allergic children show clear developmental differences in several cellular compartments (innate responses, adaptive effector responses, regulatory functions) that contribute to the production of allergen-specific IgE. Local inflammatory events and variations in the specific tissue milieu are important for shaping local immune responses and determining the predisposition for tissue-specific disease. This may explain the heterogeneity in allergic manifestations between and within individuals. Firm evidence now shows that environmental exposures during critical stages of development can alter gene expression and disease. Mounting evidence also shows that immune development does not evolve in a simple linear fashion from immaturity to maturity but rather in distinct functional waves that serve different purposes at different developmental stages. In fetal life, active immune regulatory mechanisms are dominant, challenging notions that fetal immune quiescence is the result of immature adaptive responses. Transcriptional and epigenetic control of T helper cell specification: molecular mechanisms underlying commitment and plasticity.
Buy generic epivir-hbv 150mg
Nasal responses in asthmatic and nonasthmatic subjects following exposure to diesel exhaust particles medicine youkai watch generic epivir-hbv 150mg on line. Nasal challenge with diesel exhaust particles can induce sensitization to a neoallergen in the human mucosa. Diesel exhaust exposure and nasal response to attenuated influenza in normal and allergic volunteers. Diesel exhaust enhances virus- and poly(I:C)-induced Toll-like receptor 3 expression and signaling in respiratory epithelial cells. Nrf2 expression modifies influenza A entry and replication in nasal epithelial cells. Association of indoor nitrogen dioxide with respiratory symptoms and pulmonary function in children. Effect of domestic concentrations of nitrogen dioxide on airway responses to inhaled allergen in asthmatic patients. Airway response of asthmatic subjects to inhaled allergen after exposure to pollutants. Nitrogen dioxide exposure enhances asthmatic reaction to inhaled allergen in subjects with asthma. Nitrogen dioxide increases eosinophil activation in the early-phase response to nasal allergen provocation. Association of low-level ozone and fine particles with respiratory symptoms in children with asthma. Particulate and ozone pollutant effects on the respiratory function of children in southwest Mexico City. Age-related association of fine particles and ozone with severe acute asthma in New York City. Global incidences of out-ofhospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Short-term effects of air pollution on out-of-hospital cardiac arrest in Stockholm. Sputum phagocytes from healthy individuals are functional and activated: a flow cytometric comparison with cells in bronchoalveolar lavage and peripheral blood. Effects of cyclo-oxygenase inhibition on ozone-induced respiratory inflammation and lung function changes. Ozone-induced release of cytokines and fibronectin by alveolar macrophages and airway epithelial cells. Induction of interleukin-8 by ozone is mediated by tyrosine kinase and protein kinase A, but not by protein kinase C. In vitro ozone exposure increases release of arachidonic acid products from a human bronchial epithelial cell line. Effects of ozone exposure on nuclear factor-kappaB activation and tumor necrosis factor-alpha expression in human nasal epithelial cells. Comparative airway inflammatory response of normal volunteers to ozone and lipopolysaccharide challenge. Effects of air pollutants on innate immunity: the role of Toll-like receptors and nucleotide-binding oligomerization domain-like receptors. Atopic asthmatic subjects but not atopic subjects without asthma have enhanced inflammatory response to ozone. Ozone exposure increases eosinophilic airway response induced by previous allergen challenge. Increased specific airway reactivity of persons with mild allergic asthma after 7. Increase in markers of airway inflammation after ozone exposure can be observed also in stable treated asthmatics with minimal functional response to ozone. Airway cells from atopic asthmatics exposed to ozone display an enhanced innate immune gene profile. The influence of childhood traffic-related air pollution exposure on asthma, allergy and sensitization: a systematic review and a meta-analysis of birth cohort studies. Traffic-related air pollution and development of allergic sensitization in children during the first 8 years of life. Perinatal exposure to traffic-related air pollution and atopy at 1 year of age in a multi-center Canadian birth cohort study. Parental smoking and development of allergic sensitization from birth to adolescence. Maternal and cord blood miR-223 expression associates with prenatal tobacco smoke exposure and low regulatory T-cell numbers. Genome-wide analysis of Foxp3 target genes in developing and mature regulatory T cells. Effect of glutathione-S-transferase M1 and P1 genotypes on xenobiotic enhancement of allergic responses: randomised, placebo-controlled crossover study. Outdoor air pollution, genetic susceptibility, and asthma management: opportunities for intervention to reduce the burden of asthma. Genetic ancestry influences asthma susceptibility and lung function among Latinos. Intrauterine and early postnatal exposure to outdoor air pollution and lung function at preschool age. Effects of prenatal community violence and ambient air pollution on childhood wheeze in an urban population. Traffic-related air pollution and lung function in children at 8 years of age: a birth cohort study. Early-life exposure to traffic-related air pollution and lung function in adolescence. Traffic-related air pollution and the development of asthma and allergies during the first 8 years of life. Traffic-related air pollution and asthma onset in children: a prospective cohort study with individual exposure measurement. Early-life ozone exposure associated with asthma without sensitization in Latino children. Timing and Duration of Traffic-related Air Pollution Exposure and the Risk for Childhood Wheeze and Asthma. Exposure to air pollution and development of asthma and rhinoconjunctivitis throughout childhood and adolescence: a population-based birth cohort study. Glutathione S-transferases M1 and P1 prevent aggravation of allergic responses by secondhand smoke. The glutathione-S-transferase Mu 1 null genotype modulates ozone-induced airway inflammation in human subjects. Cyclooxygenase metabolites play a different role in ozone-induced pulmonary function decline in asthmatics compared to normals. Protective effect of sodium cromoglycate on lipopolysaccharide-induced bronchial obstruction in asthmatics. Budesonide reduces neutrophilic but not functional airway response to ozone in mild asthmatics. Antioxidant supplementation and lung functions among children with asthma exposed to high levels of air pollutants. Effect of antioxidant supplementation on ozone-induced lung injury in human subjects. Dietary antioxidants and ozone-induced bronchial hyperresponsiveness in adults with asthma. Antioxidant enzyme induction: a new protective approach against the adverse effects of diesel exhaust particles. Ozone enhancement of lower airway allergic inflammation is prevented by gamma-tocopherol. Vitamin E, gamma-tocopherol, reduces airway neutrophil recruitment after inhaled endotoxin challenge in rats and in healthy volunteers. Gamma tocopherol-enriched supplement reduces sputum eosinophilia and endotoxin-induced sputum neutrophilia in volunteers with asthma. Air quality and outpatient visits for asthma in adults during the 2008 Summer Olympic Games in Beijing. Impact of changes in transportation and commuting behaviors during the 1996 Summer Olympic Games in Atlanta on air quality and childhood asthma. Effect of air-pollution control on death rates in Dublin, Ireland: an intervention study.
Cheap epivir-hbv 100 mg on-line
An important concept that has emerged in recent years about the biology of lymphocytes medicine journals impact factor order epivir-hbv online, both belonging to the innate and adaptive arms, is the plasticity of their phenotype and function influenced by the microenvironment. Cross-presentation, dendritic cell subsets, and the generation of immunity to cellular antigens. Integrin function in T-cell homing to lymphoid and nonlymphoid sites: getting there and staying there. Opposing signals from the Bcl6 transcription factor and the interleukin-2 receptor generate T helper 1 central and effector memory cells. Development of spontaneous airway changes consistent with human asthma in mice lacking T-bet. Transcription factors T-bet and Runx3 cooperate to activate Ifng and silence Il4 in T helper type 1 cells. Repression of interleukin-4 in T helper type 1 cells by Runx/Cbf beta binding to the Il4 silencer. Modulation of chromatin structure regulates cytokine gene expression during T cell differntiation. Conditional deletion of Gata3 shows its essential function in T(H)1-T(H)2 responses. The development of inflammatory T(H)-17 cells requires interferon-regulatory factor 4. Activated T cells and eosinophilia in bronchoalveolar lavages from subjects with asthma correlated with disease severity. Advances in mucous cell metaplasia: a plug for mucus as a therapeutic focus in chronic airway disease. Interleukin-13 induces tissue fibrosis by selectively stimulating and activating transforming growth factor beta(1). The association of atopy with a gain-of-function mutation in the alpha subunit of the interleukin-4 receptor. Migration matters: regulatory T-cell compartmentalization determines suppressive activity in vivo. The transcription factor T-bet controls regulatory T cell homeostasis and function during type 1 inflammation. Proteomic analyses of human regulatory T cells reveal adaptations in signaling pathways that protect cellular identity. Regulatory T cell-derived interleukin-10 limits inflammation at environmental interfaces. Early infection with respiratory syncytial virus impairs regulatory T cell function and increases susceptibility to allergic asthma. Reovirus infection triggers inflammatory responses to dietary antigens and development of celiac disease. Lymphokine-mediated regulation of the proliferative response of clones of T helper 1 and T helper 2 cells. T helper 1 cells and interferon gamma regulate allergic airway inflammation and mucus production. Differences in airway cytokine profile in severe asthma compared to moderate asthma. Identification of T helper type 1-like, Foxp3+ regulatory T cells in human autoimmune disease. Intracellular cytokine expression in whole blood preparations from normals and patients with atopic dermatitis. House dust mite-specific T cells in the skin of subjects with atopic dermatitis: frequency and lymphokine profile in the allergen patch test. Natural killer T cells are not the predominant T cell in asthma and likely modulate, not cause, asthma. Invariant natural killer T cells recognize a fungal glycosphingolipid that can induce airway hyperreactivity. Lipoxin A4 regulates natural killer cell and type 2 innate lymphoid cell activation in asthma. The expanding family of innate lymphoid cells: regulators and effectors of immunity and tissue remodeling. Nfil3 is crucial for development of innate lymphoid cells and host protection against intestinal pathogens. Innate production of T(H)2 cytokines by adipose tissue-associated c-Kit(+)Sca-1(+) lymphoid cells. Innate lymphoid cells promote lung-tissue homeostasis after infection with influenza virus. Chitin activates parallel immune modules that direct distinct inflammatory responses via innate lymphoid type 2 and gammadelta T cells. Thymic stromal lymphopoietin is induced by respiratory syncytial virus-infected airway epithelial cells and promotes a type 2 response to infection. An interleukin-33-mast cell-interleukin-2 axis suppresses papain-induced allergic inflammation by promoting regulatory T cell numbers. Allergen-experienced group 2 innate lymphoid cells acquire memory-like properties and enhance allergic lung inflammation. Adaptation of innate lymphoid cells to a micronutrient deficiency promotes type 2 barrier immunity. Once differentiated, which specific T cell subset is fixed with regard to its phenotype and function Which of the following lymphocytes can develop into memory cells after activation In addition to influenza, rhinovirus infection is a major cause of asthma morbidity, including triggering asthma exacerbations. This finding is intriguing because of the association between Alternaria sensitization and exposure with severe asthma, including fatal exacerbations. It is important to note that methods to detect cytokine production by various cell types in vivo do not account for the levels of cytokine produced by individual cells. Similar to asthma models in mice, models of atopic dermatitis exist that show some features of the disease, including eosinophilic infiltration, epidermal hyperplasia, dermal thickening, and systemic IgE production. Retinoic-acid-receptor-re lated orphan nuclear receptor alpha is required for natural helper cell development and allergic inflammation. Prostaglandin D activates group 2 innate lymphoid cells through chemoattractant receptor-homologous molecule expressed on T2 cells. Sex differences in asthma: a key role of androgen-signaling in group 2 innate lymphoid cells. The neuropeptide neuromedin U stimulates innate lymphoid cells and type 2 inflammation. Innate lymphoid cells mediate influenza-induced airway hyper-reactivity independently of adaptive immunity. Group 2 innate lymphoid cells mediate ozone-induced airway inflammation and hyperresponsiveness in mice. Enhanced innate type 2 immune response in peripheral blood from patients with asthma. Type 2 innate lymphoid cells: a novel biomarker of eosinophilic airway inflammation in patients with mild to moderate asthma. Increased numbers of activated group 2 innate lymphoid cells in the airways of patients with severe asthma and persistent airway eosinophilia. Allergen-induced increases in sputum levels of group 2 innate lymphoid cells in subjects with asthma. Testosterone attenuates group 2 innate lymphoid cell-mediated airway inflammation. Group 2 innate lymphoid cells are elevated and activated in chronic rhinosinusitis with nasal polyps. In situ mapping of innate lymphoid cells in human skin: evidence for remarkable differences between normal and inflamed skin. Increased frequencies of basophils, type 2 innate lymphoid cells and Th2 cells in skin of patients with atopic dermatitis but not psoriasis. Seasonal increases in peripheral innate lymphoid type 2 cells are inhibited by subcutaneous grass pollen immunotherapy. Group 2 innate lymphoid cells are recruited to the nasal mucosa in patients with aspirin-exacerbated respiratory disease.
Best purchase epivir-hbv
Prevention of allergic respiratory disease in infants: current aspects and future perspectives treatment 32 100 mg epivir-hbv with visa. Association of bacteria and viruses with wheezy episodes in young children: prospective birth cohort study. Wheeze in preschool age is associated with pulmonary bacterial infection and resolves after antibiotic therapy. Influence of gastrointestinal commensal bacteria on the immune responses that mediate allergy and asthma. The Asthma Predictive Index: a very useful tool for predicting asthma in young children. Validation of the Asthma Predictive Index and comparison with simpler clinical prediction rules. Ciclesonide in wheezy preschool children with a positive asthma predictive index or atopy. Atopic characteristics of children with recurrent wheezing at high risk for the development of childhood asthma. Optimum predictors of childhood asthma: persistent wheeze or the Asthma Predictive Index Psychological and lifestyle risk factors for asthma exacerbations and morbidity in children. Lung function measurement in the assessment of childhood asthma: recent important developments. The relationship of the bronchodilator response phenotype to poor asthma control in children with normal spirometry. Value of the bronchodilator response in assessing controller naive asthmatic children. Relating small airways to asthma control by using impulse oscillometry in children. Nonspecific bronchial reactivity in asthmatic children depends on severity but not on age. Lung function, bronchial responsiveness, and asthma in a community cohort of 6-year-old children. Antibiotics in fetal and early life and subsequent childhood asthma: nationwide population based study with sibling analysis. Early administration of azithromycin and prevention of severe lower respiratory tract illnesses in preschool children with a history of such illnesses: a randomized clinical trial. A simple tool to identify infants at high risk of mild to severe childhood asthma: the persistent asthma predictive score. Predicting the long-term prognosis of children with symptoms suggestive of asthma at preschool age. Predicting asthma in preschool children at high risk presenting in primary care: development of a clinical asthma prediction score. Severity of obstructive airways disease by age 2 years predicts asthma at 10 years of age. Cross-sectional and longitudinal association of the secretoglobin 1A1 gene A38G polymorphism with asthma phenotype in the Perth Infant Asthma Follow-up cohort. Antioxidant gene polymorphisms and susceptibility to a rapid decline in lung function in smokers. Asthma and atopy are associated with chromosome 17q21 markers in Chinese children. Epigenome-wide association study of asthma and wheeze in childhood and adolescence. What is a feature of atypical wheezing that should alert the physician to consider a diagnosis other than asthma In general, the preschool asthma population tends to be characterized by which of the following clinical features Asthma severity is defined as the intrinsic intensity of the disease process and is most easily assessed in a child who is not currently on long-term controller therapy. Asthma control is described as the degree to which the symptoms of asthma are alleviated by treatment and the goals of therapy are met. Both asthma severity and asthma control are evaluated in the context of two domains: impairment (current asthma symptom burden and pulmonary function) and risk (future asthma morbidity in terms of exacerbations and side effects from medications)1: 1. A stepwise approach to achieve and attain asthma control, in which the dose, type and number of medications, and frequency of administration are increased or decreased based on asthma symptoms and lung function, has been recommended by expert panels. During the development of these pharmacologic guidelines, educators have struggled with terminology that would be suitable for the diverse set of individuals who often care for children with asthma who may have dissimilar levels of training and personal experiences. Tiotropium by mist inhaler is an add-on treatment for patients with a history of exacerbations; it is not indicated in children <12 years. Quick-relief or reliever medications describe medications that produce rapid reversal of acute airflow obstruction and bronchoconstriction (also termed rescue medications). Giving daily longterm controller therapy only during specific exposures or seasons can also be considered. For example, in children who experience asthmatic episodes primarily related to viral infections, stepping up therapy targeted to high-risk times of the year (school attendance) or social situations (daycare settings) may be appropriate. It is also recommended that patient education and environmental control be discussed at every step of severity, and close follow up should be provided every 1 to 6 months, because asthma is a chronic disease. For example, use of long-term controller medications should be considered in a young child who does not have symptoms on a consistent basis but has required at least two courses of systemic corticosteroids for exacerbations in the last 6 months, or who has wheezed at least four times in the past year and has risk factors for the development of asthma (parental asthma or personal atopy). However, based on the limited data available on treatment in young children, many of these recommendations are extrapolated from studies performed in older children and adults. Through ongoing studies focused on pediatric pharmacology, more comprehensive phenotypic characterization, and advances in pharmacogenetics, it is anticipated that more specific therapeutic regimens (targeted at primary, secondary, and tertiary prevention) will become available in the future. Recent work has indicated that bacterial infections, either alone or in combination with viral infections, may also be a risk factor for asthma exacerbations. Children requiring higher steps of care for more moderate to severe disease may benefit from the administration of omalizumab before the return to school and continued during the fall of the year when rhinovirus infections are more prevalent. Recent studies in children16 and adults17,18 with persistent asthma have been promising regarding this approach to asthma therapy. Once optimal control has been achieved, step down of therapy should be considered after 3 months of control. Once the degree of symptomatology and risk moves the child into one of the persistent disease severity categories, the options for both step-up and step-down care become more variable, because adequate asthma control is perceived differently among individuals. Additional features relevant to the proper selection of a long-term controller medication include the age of the patient, the pharmacologicprofile,thedosinginterval,thedeliverysystem,therisk/ benefit ratio, and the cost effectiveness of each medication by itself and in various combinations. However, the risk-benefit ratio is complicated, resulting in part from difficulties in distinguishing statistically significant research findings from clinically relevant adverse effects. A step-up short-term or "yellow zone" approach in the preschool age group, in high-risk children 12 to 53 months of age with severe episodic disease, found no difference in the rate of exacerbations or symptoms between daily low-dose budesonide and intermittent high-dose budesonide during respiratory tract illnesses over the course of 1 year10 (Table 50. In this study, children who received beta-agonists only had higher rates of exacerbations than children that received beclomethasone whenever they used albuterol or received daily low-dose beclomethasone. Notably, there was not a significant difference in exacerbations between children treated with daily vs. Montelukast modestly improved lung function and response to allergen and exercise challenges when used as monotherapy in school-age children. Children who do not have these characteristics appear to respond to either treatment equally. However, in a recent real-world practice study, a small but significant proportion of young children started on montelukast experienced neuropsychiatric side effects leading to medication discontinuation. When administered in a single dose, salmeterol has a delayed (10 to 15 minute) onset of action compared with albuterol (5 minutes), but the duration of significant bronchodilation is much longer (12 to 18 hours vs. Thus use of long-acting 2-agonists as monotherapy is contraindicated for long-term control of persistent asthma. Studies in adults have demonstrated a modest reduction in asthma exacerbations (21%). Recently published studies in children were not powered to assess an exacerbation endpoint but demonstrated improvements in lung function. Theophylline, a methylxanthine, has been shown to be effective as monotherapy for the attenuation of persistent asthma in children related to its effects as a bronchodilator, antiallergic, and antiinflammatorycompound.
Clivers. Epivir-HBV.
- How does Clivers work?
- Dosing considerations for Clivers.
- What is Clivers?
- Fluid retention, painful urination, psoriasis, enlarged lymph nodes, skin ulcers, breast lumps, and skin rashes.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96196
Buy epivir-hbv 100mg online
The decision whether to include such a nonendemic extract in an allergen immunotherapy formulation depends on several factors medicine - buy epivir-hbv 100 mg free shipping, one of which is whether related plants provide adequate coverage. At a time of constricting availability of particular pollen and fungal extracts, this issue becomes crucial. Initially, because pollen cross-allergenicity data were limited, plant systematics had been used to infer the likelihood of cross-reactivity. The validity of this process depends on two premises: first, that more closely related plants will share greater similarities and antigens; second, that the accepted botanical classification reflects phylogeny, that two plants in the same genus evolved from a common ancestor, two in the same family from a more distant ancestor, and so on. Cross-reactivity with groups of related allergenic plants will be commented on in the sections on Representative Pollens and Representative Fungi. The subtleties of outdoor sampling, interpretation, and the importance of submicronic allergic-laden particles have been well described. Gravimetric Samplers the earliest samplers were crude devices that relied on gravity to deposit particles on sticky surfaces. The Durham sampler is a greased microscope slide mounted horizontally on a stand, with a roof, or rain shield, above. Petrie dishes with the appropriate agar medium have been used outside and indoors for mold studies, with the advantage of the growth medium allowing identification of viable spores via distinctive colony characteristics. Disadvantages of gravimetric samplers are that they can only be quantified in terms of surface area (cm2) and do not give an estimate of particle burden in a volume of air. Gravimetric samplers are no longer considered adequate for generation of meaningful data. Aerobiology of Outdoor Allergens 433 Volumetric Samplers Such devices sample volumes of air over a given time interval with results reported in particles per cubic meter per 24 hours. The rods are lowered into the ambient air from the spinning armature by centrifugal force. It has a fixed surface area determined by the exposed length and width of the rod, and that sweeps a given length of air (circumference of the circle) for a fixed length of time. The formula for calculating the concentration of pollen per volume per 24 hours is C = N/V, where N is the number counted and V is the volume of air sampled. Hirst-type slit-suction devices use vacuum pumps to move air continuously through an aperture to impact on tape on a rotating 7-day drum. Alternatively, a microscope slide can advance under the aperture in a Kramer-Collins sampler or the Burkard pollen and spore trap equipped for a 24-hour lid assembly. However, to provide a representative estimate, a minimum of three longitudinal transects is recommended so that approximately 10% of the area impacted by pollen is counted. Agar plates between the separate stages can be used to identify fungi by culture growth characteristics. Liquid impingers have been used primarily for airborne bacteria detection; particles are pulled into a fluid media and may be cultured or filtered and observed microscopically. High-volume suction devices operating at 600 L/min are fitted with fiberglass or Gore-Tex-membrane filters that can be scanned microscopically, or eluted and stained with allergen-specific antibodies. Most of these groups have at least a few members incriminated in airborne allergy. The angiosperms have traditionally been divided into monocots and dicots, although it appears that the phylogeny is much more complicated and will not be discussed here. The most important monocot group for aeroallergen purposes is the grass family Poaceae. In the allergy literature the dicots have historically been treated as trees and weeds. However, numerous botanical families have both trees and smaller herbaceous plants. Because cross-reactivity makes more sense in terms of plant systematics, in the following discussion plants will be addressed in taxonomic groupings. Gymnosperms the most important family of the order Pinales (Coniferales) is Cupressaceae. This family contains many members that have been implicated in severe pollinosis (Table 27. Exposure is not only from forest stands, but also from the ubiquitous use of Juniperus species in home landscaping. In Texas and parts of Oklahoma, mountain cedar (Juniperus ashei) counts may easily exceed 20,000 grains/m3, pollinating from mid-December through January. The pine family consists of pines (Pinus), spruces (Picea), hemlocks (Tsuga), and firs (Abies, Pseudotsuga). The pollens of this family are produced in copious amounts, but they are weak allergens and uncommon inducers of hay fever. Weak cross-allergenicity reported between both these families and angiosperms is most likely related to panallergenic calmodulins. Automated Samplers A number of real-time automated pollen counters based on diverse technologies are under development. More refinement is needed before automated counters can be used reliably as a replacement for routine manual pollen monitoring. Though not used routinely, high-volume particulate air samplers can capture sufficient pollen to measure the content of allergen molecules within airborne pollen grains. This stain permanently stains the exine, the outer wall of the pollen grain, a pink to red color, without staining the majority of fungal spores. Pollen and fungal spore identification is based on gestalt, or pattern recognition. Certain characteristics help in determination: number of associated grains or spores, color, size, shape, presence of pollen apertures such as pores and furrows, presence of attachment scars, and surface sculpturing. Ascospores are generally formed in groups of eight spores in the ascus and are often found clustered in eights on samplers. Basidiospores have small attachment scars and commonly develop in groups of four, although the spores are released singly and are usually not observed to be in quartets on samplers. Monocots (Class Liliopsida) the grass family, Poaceae, is a huge botanical group with several subfamilies and numerous tribes (Table 27. The fescue subfamily Pooideae, including the temperate climate pasture grasses and most cereal grains, is the most prominent in pollinosis in temperate regions. These grasses have wide distribution throughout the United States and Western Europe. With only minor exceptions, members of the fescue subfamily have strongly cross-reactive major pollen allergens. Buffalo, salt, and grama grasses are native prairie grasses related to Bermuda grass and are cross-reactive, but less potent than Bermuda. Notably, pollen allergens of Panicoideae and Chloridoideae grasses show distinct patterns of IgE reactivity with only limited cross-reactivity with each other, and with allergens of temperate grasses. Included within the superorder containing the grasses are the rush, sedge, and cattail families, which produce airborne pollen but are not considered significant inducers of pollinosis. At least thirteen grass allergen groups have been characterized for temperate grass pollens, as well as additional food allergens among the cereal grains. These plants are known for their vascular stems, flowers, fruit, seeds and pollen, which have features of three furrows or pores (colpi). The superorder Caryophyllanae contains ubiquitous and allergenically important chenopod and amaranth weeds of the family Amaranthaceae, as well as the lesser docks and sorrels of family Polygonaceae. These latter weeds pollinate earlier than many other weeds, coinciding with the grass pollen season. Sheep sorrel (Rumex acetosella) is considered a moderate hay fever inducer; curly or yellow dock (R.
Syndromes
- Is it worse at night? Are you able to sleep?
- Fainting or feeling light-headed
- Rich pastries and baked goods
- Antithyroglobulin antibody
- Bring an extra supply with you in case your return is delayed.
- A latex condom should be used during ALL sexual contact, even if the infected person does not have any sores or blisters at that time. However, you may still get genital herpes when using a condom.
- Exposure to smoke
- Enlarged muscles of the calves, buttocks, and shoulders (around age 4 or 5). These muscles are eventually replaced by fat and connective tissue (pseudohypertrophy).
Buy discount epivir-hbv 150mg on-line
Bhlbb5 symptoms anxiety order 100 mg epivir-hbv overnight delivery, a transcription factor, appears to modulate itch through a direct inhibitor mechanism that is dependent upon stimulation of pain fibers in the dorsal root ganglia. As such, the loss of stimulation of Bhlbb5 fibers after damage to sensory nerve fibers can lead to chronic scratching conditions such as trigeminal trophic syndrome. More recent data have shown that inflammatory Th2 cytokines can both sensitize and stimulate itch-specific type C fibers through Jak1 signaling. The trophic effects of efferent sensory nerves in cutaneous inflammation, wound healing, and various homeostatic functions are also recognized. For example, sensory nerves release neuropeptides, which lead to vasodilation and increased vasopermeability. The interplay between the hair follicle, hair follicle stem cells, and the immune system has recently come into focus. T regulatory cells play a critical role in the maintenance of the hair follicle stem cell population. For example, after the depletion of Langerhans cells, the hair follicle releases chemokines which attract precursor Langerhans cells which then populate the epidermis. Nerve fibers (yellow-green) are stained with antibody that recognizes a general nerve marker, protein gene product 9. Fine nerve fibers reside just beneath and traverse into the epidermis, which is marked by the dermalepidermal junction basement membrane (orange-red) that is stained with type 4 collagen antibody. Sensory and postganglionic autonomic nerve fibers are codistributed by large cutaneous branches of musculocutaneous nerves that arise segmentally from spinal nerves or, on the face, from branches of the trigeminal cranial nerve. The main subcutaneous nerve trunks branch to form a deep nerve plexus at the subcutaneous-dermal junction and a superficial nerve plexus in the papillary dermis. As many as 1000/cm2 sensory nerve fibers innervating nonfacial skin travel as individual, continuous axons bundled within peripheral nerves that extend from a single dorsal root ganglion of the spinal column. Consistent with their functional classification, autonomic nerves innervate involuntary vascular smooth muscle, arrector pili muscles of hair follicles, sweat glands, and sebaceous glands. Nerve impulse conduction velocity, fiber diameter, sensitivity to anesthetics, and function. Autonomic activities in skin appear to be mediated by unmyelinated postganglionic C fibers, although other C fibers also have an important role in sensory function. All three subclasses of autonomic C fibers innervate the microcirculation; adrenergic fibers mediate vasoconstriction, and cholinergic fibers mediate vasodilation and sweating. Innate immunity of the skin can be roughly divided into constitutive innate immunity, involving an anatomic and physiologic barrier, and inducible innate immunity, involving an acute inflammation and cellular infiltration barrier. Neither constitutive nor inducible innate immunity of the skin demonstrates acquired specificity or memory for an invading pathogen. However, new evidence has emerged that the innate immune system can prime the adaptive immune system. The immune protection provided by these two functional barriers is essentially unchanged regardless of the number of previous encounters with a particular pathogen. The normal flora of the skin includes various bacteria (primarily coryneforms and staphylococci) and some fungi (primarily Malassezia). These microorganisms assist the host by competing with other, more pathogenic organisms for resident status. Specific skin microbes and their metabolic byproducts modulate diseases, including atopic dermatitis, cutaneous T cell lymphoma, and melanoma and nonmelanoma skin cancers. Interlocking cornified keratinocytes form a relatively impenetrable surface, and the outward growth and shedding of cornified keratinocytes help to eliminate superficially bound pathogens. Similarly, some epidermal lipids, such as sphingosine and keratinocyte- and sebumderived fatty acids, exhibit antibacterial activity through their ability to reduce skin surface pH. Lactic acid excreted in eccrine sweat also lowers the skin surface pH level, and normal body temperature inhibits the growth of some pathogens. Important among these events is the induced expression of inflammatory cytokines, chemokines, mediators. Keratinocytes and other epithelial cells such as those in the gut express specific cytokines and growth factors that likely represent novel members of the innate immune system. Disruption of the constitutive skin barrier allows significant penetration of commensal microorganisms or pathogens. Innate immunity molecules with broad specificity and relatively targeted activity against intruding microbes prevent dissemination of infection and, when necessary, guide acquired immunity. These pathogen-targeted molecules can be broadly divided into soluble molecules. Important pathogen-targeted, inducible, soluble, innate immunity molecules of the skin include inducible antimicrobial polypeptides, complement-activating and opsonin proteins, and complement proteins. Several antimicrobial polypeptides are distinct features of epithelial surfaces and are produced by keratinocytes in skin. Cutaneous immunity is divided into constitutive innate immunity, inducible innate immunity, and acquired immunity. On disruption of the skin barrier (upper left), an inflammatory response ensues that is marked by the early release of primary cytokines. Vasodilation and increased vasopermeability, which are characteristic of an inflammatory response, result. Subsequent inducible events such as increased antimicrobial polypeptide expression and complement activation contribute to the early neutralization of invading pathogens. Pathogenrecognition receptors constitutively expressed on a wide variety of cell types (red and green shapes indicating neutrophils and a single macrophage and Langerhans cell) also contribute to pathogen clearance and help direct the acquired immune response. Subsequent antigen presentation in the skin can activate these T cells to perform their programmed function. Clearance of and heightened immunity against the invading pathogen followed by resolution of the inflammatory response with concurrent wound healing is the desired outcome; however, disease can also develop. Plasmacytoid dendritic cells secrete large amounts of type 1 interferons in response to a viral infection. Unlike the antimicrobial peptides, the protective activities of type 1 interferons are apparently related to antiviral effects on host cells rather than direct toxicity for pathogens. The complement-activating (opsonin) molecules of the innate immune system include members of the acute phase proteins. The collectins and ficolins recognize unique carbohydrates on bacteria, fungi, and viruses and mark them for destruction. Initial availability of the C3 complement component and other complement proteins is provided by the minor but significant quantities produced by resident cells of the skin. These complement proteins are rapidly supplemented by an influx of additional complement proteins from blood after vasodilation and increased vascular permeability resulting from the acute inflammatory response. Pathogen-targeted molecules, such as antimicrobial peptides and complement-related proteins, represent soluble components of the inducible innate immunity barrier that counter pathogen invasion in skin. Different pathogens and antigens lead to different patterns of host gene expression and influence the degree and composition of immune cell infiltration. Effective elimination of pathogens that are not easily phagocytosed, such as fungi and parasites, may require mechanisms that target excretion of toxic leukocyte products directly onto the pathogen. Although eosinophils are less phagocytic than neutrophils, they produce reactive oxygen species at the plasma membrane surface, not intracellularly,139 and they can readily degranulate and deposit toxic cationic proteins onto the surface of parasites. Specific cell types other than neutrophils and monocytes or increased numbers of a particular cell type can preferentially enter skin in circumstances of chronic inflammation or disease (Table 32. Overall, the acute inflammatory response leads to resident cell activation and increased accessibility of blood components and leukocytes to the site of pathogenic incursion. Acquired Immunity Acquired (adaptive) immunity mounts a specific response to a stimulus and demonstrates memory. Th17 cells play a key role in defense against fungal infections, extracellular bacterial infections, and autoimmunity. B cells recognize relatively intact antigens, unlike T cells, whose activation involves antigenic peptide recognition. Thymus-dependent protein antigens do not induce antibody responses in the absence of T cells; this is different from thymus-independent polysaccharide and lipid antigens, which induce antibody production with little or no help from T cells. Antigen recognition occurs through surface immunoglobulins, all with identical specificity on a given B cell.
Buy cheap epivir-hbv 150mg online
The mast cell stabilizing component of these drugs benefits patients most if treatment is started before the height of symptom onset medicine 6 year course buy epivir-hbv visa. Patients usually note rapid onset of relief of itch upon drop instillation, because most dual action medications have high H1 receptor affinity. Drug dosing varies from one to four times per day, and efficacy is judged best by symptom relief. Nonsteroidal drugs inhibit cyclooxygenase resulting in decreased formation of prostaglandins and thromboxanes, but not leukotrienes. Therefore these compounds are useful in controlling itching and some inflammation but may not control the infiltration of inflammatory cells. In extreme cases, use of a low-potency topical steroid four times a day should be considered. All patients receiving topical steroids should have their intraocular pressure measured every 3 months and be evaluated for cataract annually. There is no retrograde passage of nasal steroids up through the lacrimal sac, so any ocular effect is considered to be secondary to systemic absorption. A metaanalysis of grass pollen allergen sublingual immunotherapy tablets for seasonal allergic rhinoconjunctivitis provides evidence of a small benefit. Hogan, in 1953, was the first to describe the findings of chronic conjunctivitis and keratitis in patients with atopic dermatitis. The onset of disease is usually in the second through fifth decade, although the majority of patients with atopic dermatitis are diagnosed by age 5 years. Atopic keratoconjunctivitis is thought to consist of both type 1 and type 4 hypersensitivity mechanisms. Evidence of the pathologic process comes from histologic and immunohistochemical analysis of conjunctival biopsy specimens and from tear fluid analysis for mediators and cells. The skin and conjunctiva are more likely to be colonized with enterotoxin-producing Staphylococcus aureus bacteria than normal. Conjunctival inflammatory cell density showed a negative correlation with tear stability and corneal sensitivity and a positive correlation with the vital staining scores. These eosinophils are found to have increased numbers of activation markers on their surface. Fibroblast number is increased, and there is an increased amount of collagen compared with normal individuals. Furthermore, a complex immune cell profile implicates more than these mast cells alone, but the details of the initiation and perpetuation of these cellular responses remains unclear. Allergic and Immunologic Diseases of the Eye 611 same surface problems but has been shown to improve vision in some. This cataract often has the configuration of a multilobed opacity resembling a "milk splash. Other symptoms, in decreasing order of frequency, include watering, mucous discharge, redness, blurring of vision, photophobia, and pain. The skin of the lids may become leather-like, developing cicatricial ectropion (turning outward of the lid from skin scarring) and lagophthalmos (incomplete closure of eyelids). Lateral canthal ulceration and cracking as well as lash loss (madarosis) may also be present. The conjunctiva of the tarsal surfaces can manifest a papillary reaction and possibly pale white edema. Subepithelial fibrosis is present in many, fornix foreshortening in some, and symblepharon (scar of conjunctival surface of lid to conjunctiva of the globe) in a few. Persistent epithelial defects, scarring, microbial ulceration, and neovascularization are the main corneal causes for decreased vision (Table 38. Penetrating keratoplasty is at risk of the Patient Evaluation, Diagnosis, and Differential Diagnosis. The patient typically describes severe, persistent, periocular itching associated with dermatitis. There is usually a family history of atopic disease in one or both parents and commonly other atopic manifestations in the patient, such as asthma (65%) or allergic rhinitis (65%). The approach to treatment is multifaceted and includes environmental controls as well as topical and systemic medications. However, the patient must remove environmental irritants in both the home and the employment or school setting. The topical application of a vasoconstrictor-antihistamine combination may bring transient relief of symptoms but is unlikely to alter the immunopathologic process or its sequelae. The potent topical antihistamines offer much greater H1 receptor antagonism than overthe-counter antihistamines. The topical administration of steroids such as prednisolone acetate eight times per day for 7 to 10 days is clearly beneficial in controlling symptoms and signs. These agents, of course, must be used judiciously, because the chronic nature of the disease may encourage overuse. The patient must be instructed that steroid use must be transient only and must be carefully monitored for efficacy as well as warned of the potential for causing cataract and glaucoma. Nonsteroid medications have been shown to be effective in reducing itching, tearing, and photophobia. Topical mast cell stabilizers one to four times daily are recommended year-round in patients with perennial symptoms. If an exacerbation occurs and the patient is not taking a mast cell stabilizing agent topically, its use should be initiated one to four times daily concurrent with a short burst of topical steroids (for 7 to 10 days). Mast cell stabilizers alone such as cromolyn, nedocromil, lodoxamide, or mast cell stabilizer antihistamine combinations such as olopatadine, azelastine, epinastine, and ketotifen, may be helpful. Trichiasis or lid position abnormalities, if contributing in any way to corneal compromise, must be corrected. The ocular surface inflammation, lid malposition, and lid margin keratinization may contribute to the development of limbal stem cell deficiency. It may be extremely difficult to achieve reepithelization in these defects, and surgical approaches have been attempted. Care should be taken in using these to achieve viral eradication without sustained use and subsequent epithelial toxicity. An excellent review of the history and description of this disease was published by Kumar in 2008. The onset of disease is generally before age 10 years and lasts 2 to 10 years, usually resolving during late puberty. The epithelium contains large numbers of mast cells and eosinophils, neither of which are found in normal individuals. Associated foreign body sensation, ptosis, thick mucous discharge, and blepharospasm occur. The conjunctiva develops a papillary response, principally of the limbus or upper tarsus. Limbal papillae tend to be gelatinous and confluent, and they occur more commonly in African and West Indian patients. The forniceal conjunctiva usually does not show foreshortening or symblepharon formation. If, at this point, inadequate or no treatment is rendered, a plaque containing fibrin and mucus deposits over the epithelial defect. This so-called shield ulcer usually has its lower border in the upper half of the visual axis. The peripheral cornea may show a waxing and waning, superficial stromal, gray-white deposition termed pseudogerontoxon. Allergic and Immunologic Diseases of the Eye 613 Patient Evaluation, Diagnosis, and Differential Diagnosis. These patients have intense photophobia, ptosis, and the characteristic finding of giant papillae. Tear fluid analysis and cytology, conjunctival scraping for cytology, and biopsy are rarely needed to assist in establishing the diagnosis. As with any atopic condition, avoidance of allergens is important, although many afflicted are skin test negative.
Epivir-hbv 100 mg amex
A systematic review and meta-analysis: tailoring asthma treatment on eosinophilic markers (exhaled nitric oxide or sputum eosinophils) 5ht3 medications cheap epivir-hbv 150mg visa. Fractional exhaled nitric oxide for the management of asthma in adults: a systematic review. The efficacy of proton pump inhibitors for the treatment of asthma in adults: a meta-analysis. Dietary restriction and exercise improve airway inflammation and clinical outcomes in overweight and obese asthma: a randomized trial. Dysfunctional breathing: a review of the literature and proposal for classification. Among the following exposures, which one is not a potential trigger of asthma symptoms The dose, class, and frequency of medications needed to achieve control are increased (stepup) according to greater levels of asthma severity (features of impairment and risk). The importance of bronchospasm and airway smooth muscle contraction, in the pathophysiology of asthma and its symptoms, has long been recognized, both as an essential component of the disease and as a target of treatment. Asthma is a heterogeneous disease with multiple phenotypes, which are based upon shared features, such as disease onset, allergic sensitization, altered pulmonary physiology, and markers of severity such as exacerbations and responsiveness to treatment. Efforts are ongoing to establish endotypes, or underlying molecular mechanisms of asthma phenotypes, but this goal has yet to be fully achieved. The recognition of asthma phenotypes has begun to explain why some patients do not achieve disease control with current treatments and what may be the specific characteristics of their underlying disease leading to variations of the clinical picture. These limitations to achieve disease control in asthma are undergoing a needed paradigm shift with the availabilities of an increasing array of biologics, which have targeted specificity to pathways of inflammation. Experiences with biologics have found the efficacy of various treatments to be more apparent in subpopulations of patients with asthma. Although a personalized approach is not in practice at present, its eventual incorporation is essential for the next advancement in care and will be considered in this chapter. Although these phenotypic features do not necessarily point to specific underlying disease mechanisms, such as endotypes, or even predict responses to treatment, broad-based "types" of asthma include allergic asthma, nonallergic asthma (formerly intrinsic asthma), late-onset asthma, and asthma with fixed airflow obstruction. Allergic asthma is associated with IgE sensitization, begins in early childhood, and often persists into adulthood. An identification of the inflammatory fingerprint in an asthma patient has become important in selecting immune modulators for use in patients unresponsive to standard medications. Late-onset asthma begins in adulthood, is more common in women, and often coexists with sinusitis and nasal polyps. Recognition of these subjects is important, because the primary treatment is different when the predominance of disease is asthma (antiinflammatory) vs. If the dominant pattern of disease is asthma, there is usually eosinophilia and allergic sensitization. Less well understood, or characterized, is nonallergic asthma, often referred to as low T2 or non-T2 disease. Clinically, asthma in these patients is similar to other phenotypes, but the underlying inflammatory processes are not associated with eosinophils, allergic sensitization is infrequent, and responsiveness to corticosteroid-based treatments is less predictable. Severe or Refractory Asthma the past decade has seen considerable interest focus on patients with severe or treatment-refractory asthma. Attention to this group is justified as they experience the greatest disease burden, morbidity, and health care costs. In younger patients with a family history of asthma or allergic diseases or the absence of a smoking history, the presence of these symptoms is strong clinical evidence for asthma. However, in the presence of normal lung functions, demonstrating airflow reversibility can be difficult to achieve. The importance of verifying the diagnosis of asthma by measures of lung function before beginning long-term care has been reported by Aaron et al. A primary reason for mistaken diagnosis of asthma was an absence of pulmonary function measurements during the initial evaluation and verification of airflow obstruction. Serious exacerbations: at least one hospitalization, intensive care unit stay, or mechanical ventilation in the previous year 4. For every patient, an assessment of control should include both measures of symptoms (impairment) and risk for future adverse outcomes (risks). There are also additional aspects to consider when asthma control is not achieved, including the proper use of inhalers and medication adherence. Finally, measurement of lung function, both with the initial diagnosis of asthma and at least yearly, is a necessary monitor of disease control and indicator for future risks, which is greater with impaired lung function. Collectively, these outcomes are important to the patient and serve to reflect a more comprehensive control of disease, reduce disease morbidity, and influence health care costs. Risk domains include exacerbations, progressive loss of lung function, and medication side effects. Although linkages exist between these two major domains of control, the actions of different treatments, such as bronchodilators, antiinflammatories, and biologics, may have a more selective or specific influence on these individual clinical outcomes. Considerable heterogeneity occurs among patients, or groups of patients, with asthma, as reflected in the level of symptoms, altered airway function, frequency of exacerbations, and responses to treatment, to reflect individual patterns of underlying disease. An assessment of existing asthma control is necessary to initiate treatment and as a marker for effectiveness of the treatment. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness, and cough that vary over time and in intensity, together with variable expiratory airflow limitation. History of Variable Respiratory Symptoms Wheeze, shortness of breath, chest tightness, and cough Descriptors may vary between cultures and by age;. Confirmed Variable Expiratory Airflow Limitation Documented excessive variability in lung function* the greater the variations, or the more occasions excess variation is seen, the more confident (one or more of the tests listed) the diagnosis. Medication side effects can range in intensity from none to very troublesome and worrisome. Scores range from 5 to 25: 20 to 25 is rated well controlled, 16 to 19 is not well controlled, and 5 to 15 is very poorly controlled. Patients in the not well controlled or very poorly controlled categories require reassessment and an escalation of treatment in an attempt to achieve wellcontrolled status and thus disease stabilization. In contrast, for patients in the well controlled category, it may be possible, after a period of disease stabilization, to safely reduce the level of treatment. Approaches to step-down care are less well established than experiences with step-up care. Although guidelines provide evidence-based direction in treatment, patient needs and individual circumstances should always be considered. Asthma symptoms and control are variable for most patients, and providing instructions on how to recognize a loss of asthma control and directions on strategies, or steps, to regain control are important for successful and effective care. This aspect of self-management is especially important for patients with a history of frequent asthma exacerbations or for those individuals with moderate to severe asthma, in whom such events are more likely to occur. Action plans include information on key management elements for the individual patient: long-term medications, including dosages and frequency of use, and quick-relief medications. Traditionally, the action plan includes three levels of asthma symptoms: "I feel good" (green zone), "I do not feel good" (yellow zone), and "I feel awful" (red zone). In developing an action plan for an individual patient, it is essential to review the features of these levels of control. In addition, it is critical that the patient has instructions on what steps or actions to take when loss of disease control occurs, and what to do if the recommended interventions do not improve asthma control. Prevent asthma symptoms every day: Peak Flow My Personal Best Take my long-term-control medicines (above) every day. Before exercise, take puffs of Avoid things that make my asthma worse like: I do not feel good. Call 9-1-1 if you have trouble walking or talking due to shortness of breath or lips or fingernails are gray or blue. Patients with asthma should have knowledge of their allergic sensitizations to environmental allergens and what steps may reduce this exposure, if possible. It is important to determine not only existing sensitization but also, by historical correlation, if possible, the significance and contribution of specific allergens to ongoing symptoms. Equally important is the need to avoid cigarette smoke exposure, especially from personal smoking. Upper airway diseases, allergic rhinitis, or sinusitis commonly coexist with asthma. The use of biologics in treatment of sinusitis with polyps has been found to be associated with improved asthma control. The role and contribution of obesity to asthma pathogenesis, pathophysiology, and treatment selection need to be clarified, in addition to the effects of weight loss on asthma control30; there is evidence that weight loss after bariatric surgery can improve asthma control in some patients with obesity. Influenza vaccination, however, is suggested in all asthma patients but primarily to prevent the development of influenza, not necessarily to prevent exacerbations.
