
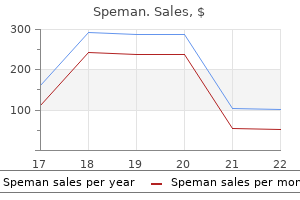
Cheap speman 60 pills overnight delivery
Positive diagnostic injections may identify candidates for future interventions such as radiofrequency or thermochemical ablation 9 mens health 9 order speman 60pills visa. Randomized, double-blind, placebo-controlled trials are necessary in order to evaluate its efficacy in managing pelvic/perineal pain. For this reason, it is recommended that a 22-gauge needle is entered first for protection. There are also a number of factors the operator must be aware of during the procedure (Table 37. For example, patients with a history of coccygectomy, arthritis, and radiation to the lower pelvis are at increased risk for calcification of the sacrococcygeal ligament. Side Effects and Complications Patients should be followed up the next day to assess for complications and the necessity of pain relief due to local anesthetic. Injectate spread into unintended areas during the procedure may lead to motor, sexual, and bowel/bladder dysfunction. Ganglion impar block with botulinum toxin type a for chronic perineal pain -a case report. A case report on the treatment of intractable anal pain from metastatic carcinoma of the cervix. Magnetic resonance neurographyguided nerve blocks for the diagnosis and treatment of chronic pelvic pain syndrome. Blockade of ganglion impar through sacrococcygeal junction for cancer-related pelvic pain. Sacral postherpetic neuralgia and successful treatment using a paramedial approach to the ganglion impar. Transsacrococcygeal approach to ganglion impar block for management of chronic perineal pain: a prospective observational study. Thermocoagulation of the ganglion impar of Walther: description of a modified approach. Would pulsed radiofrequency applied to different anatomical regions have effective results for chronic pain treatment Radiofrequency thermocoagulation of ganglion impar in the management of coccydynia: preliminary results. Transsacrococcygeal approach to ganglion impar for pelvic cancer pain: a report of 3 cases. Thermocoagulation of the ganglion impar or ganglion of Walther: description of a modified approach. Ganglion impar block for sympathetically mediated pain in a patient with a rectourethral fistula. Neurolytic block of ganglion of Walther for the management of chronic pelvic pain. Blockade of the ganglion impar (walther), using ultrasound and a loss of resistance technique. Celiac Plexus Blocks and Splanchnic Nerve Blocks Vijay Babu, Karthik Kura, and Karina Gritsenko 38 Introduction Chronic abdominal pain is commonly seen in medical practices and is a major health-related issue. It has been shown to be present in 75% of adolescents and 50% of adults, leading to frequent visits to healthcare professionals [1]. Medical management and surgery occasionally may not be adequate to treat chronic abdominal pain. Celiac plexus blocks and splanchnic nerve blocks have successfully been used to treat a variety of painful conditions of the abdominal viscera with availability of the most significant literature on nonspinal blocks related to celiac plexus block. A Cochrane review described pancreatic cancer as the fifth leading cause of cancer-related mortality in the United States, with an estimated 33,370 deaths attributable to the disease in 2007 alone [3]. Celiac plexus block (also known as solar plexus block, celiac ganglion block, or splanchnic plexus block) is the largest of the three great plexuses in the chest and abdomen, with the other two being the cardiac and hypogastric plexV. Although celiac plexus and splanchnic nerves are often used interchangeably secondary to their anatomic proximity, they are in fact distinct structures. A Cochrane review [3] also concluded that a celiac plexus block causes fewer adverse effects than opioids; thus, it is important for patients. History the percutaneous approach to blocking the splanchnic nerves and the celiac plexus was initially devised for surgical anesthesia by Kappis in 1914 [8]. He continued to develop the technique and eventually published a case series in 1918 [9]. Subsequently, Popper, in a 1948 publication [12], introduced the use of splanchnic nerve block as a diagnostic tool to differentiate between somatic and visceral components of abdominal pain. Ethanol-induced neurolysis of the celiac plexus and splanchnic nerves for long-term pain relief was described by Jones in a 1957 publication [13]. As imaging guidance for celiac plexus nerve blocks emerged, the limitations of the utility of fluoroscopically guided celiac plexus blocks were recognized since fluoroscopy did not accurately depict the needle tip in relation to the retroperitoneal structures [4]. Recently, An [21] described an alternate method for retrocrural approach during celiac plexus using a bent-tip needle. Pathophysiology the pain that originates from the upper abdominal viscera is carried by special visceral afferent fibers that relay through splanchnic nerves and the celiac plexus [22, 23]. Abdominal viscera may be affected by an abnormal distention of the organ wall or viscus, tension or torsion on mesenteric vessels, and ischemia [5]. Such visceral pain may be seen with chronic benign disorders, however, more commonly with gastrointestinal malignancies such as hepatic metastasis, an intestinal tract tumor, and pancreatic cancer. Of all the visceral pain conditions seen by interventional pain physicians, pancreatic cancer is the most common which is the fifth leading cause of cancer-related mortality in the United States [3]. They included a total of seven randomized controlled trials of pain relief from pancreatic cancer by treatment with medical management alone to celiac plexus block with medical management. Sympathetic trunk Spinal sensory (dorsal root) ganglion Dorsal (posterior) root Thoracic part of spinal cord Intermediolateral cell column Ganglion of sympathetic trunk Spinal nerve to vessels and glands of skin Ventral (anterior) root Meningeal branch to spinal meninges and spinal perivascular Stretch plexuses (usually arises from (distention) spinal nerve) Abdominopelvic (greater, lesser, and least) thoracic splanchnic nerves Pain Vagus nerve (X) White ramus communicans Gray ramus communicans Ganglion of sympathetic trunk Celiac ganglion Ganglion of sympathetic trunk Enteric plexuses of gut Superior mesenteric ganglion Sympathetic Preganglionic fibers Postganglionic Parasympathetic fibers Preganglionic Postganglionic Afferent fibers. Preganglionic fibers from T5 to T12 leave the ventral roots of the spinal cord to join with white rami communicans. Preganglionic nerves from T10 to T11 join together to form the lesser splanchnic nerve and subsequently converge to form the celiac plexus. The least splanchnic nerve arises from the T12 sympathetic ganglion and courses through anteriorly to join the celiac plexus. The celiac plexus is located anterior to the aorta at the level of the L1 vertebral body and anterior to the crura of the diaphragm. However, the needle tip should be positioned cephalad to the celiac artery to achieve a wider spread of either local anesthetic or a neurolytic solution [38, 39]. The needle is then withdrawn and redirected at a steeper angle (60 degrees from midline) so the needle tip is walked off the L1 vertebral body. The needles, however, are aimed more cephalad to the anterolateral margin of the T12 vertebral body, being careful to hug the vertebral body. Although no longer commercially available, phenol has the benefit of minimal pain on injection. Alternatives to ethyl alcohol and phenol for neurolysis have been described using cryoablation [44] and with a reverse phase polymer [45], but these are not commonly utilized.
Discount speman on line
The testis prostate 3 3 buy speman 60 pills with mastercard, with its tunica vaginalis, is then delivered through the incision by blunt and sharp dissection, and the inguinal incision is closed. Sometimes, a testicular prosthesis is inserted and fixed in the scrotum before the inguinal incision is closed. Muscles are split and peritoneum reflected medially to expose the spermatic vessels; the vein is identified and ligated. Usual preop diagnosis: Varicocele causing infertility Groin dissection, or inguinofemoral lymphadenectomy (lymph node dissection), is the most critical of the inguinal operations. In these patients, consider causes of increased intraabdominal pressure during H&P. Local anesthesia is acceptable for simple herniorrhaphy, although discomfort may be elicited if the peritoneum is manipulated. Most inguinal procedures are done on an outpatient basis, and the anesthetic should be planned appropriately. Castorina S, Luca T, Privitera G, El-Bernawi H: An evidence-based approach for laparoscopic inguinal hernia repair: lessons learned from over 1,000 repairs. If the tumor can be resected with a safe margin of at least 2 cm, partial penectomy is usually enough. A tourniquet is placed at the base of the penis, which is amputated at least 2 cm proximal to the tumor. The corpora cavernosa are sutured, and the tourniquet is released, followed by inspection for bleeding. The edges of the urethra are sutured to the ventral skin, and the lateral and dorsal skin edges are approximated over the ends of the corpora cavernosa. Usual preop diagnosis: Squamous cell carcinoma of the penile skin Insertion of penile prosthesis is performed for impotence. Sacral anesthesia (saddle block) is sufficient; lumbar epidural anesthesia may be less reliable than spinal or caudal at blocking sacral fibers. Usual preop diagnosis: Metastatic prostate cancer Vasovasostomy is the reestablishment of the continuity of the vas deferens and restoration of fertility following a previously performed vasectomy. The site of previous vasectomy is identified and excised and the two ends of the vas deferens anastomosed. It is bilateral and requires the use of either the operating microscope or magnifying loupes. The wall of the hydrocele is excised and the edges sutured around the epididymis to prevent recurrence. Variant procedure or approach: Aspiration used as a temporizing approach because recurrence is almost 100%. Usual preop diagnosis: Hydrocele Spermatocelectomy: A spermatocele is a cyst of the epididymis, usually excised with the part of the epididymis from which it arises. Variant procedure: Aspiration as a temporizing maneuver until the operation can be performed. Usual preop diagnosis: Spermatocele or epididymal cyst Insertion of testicular prosthesis: A small incision is made in the scrotal skin, and a pouch is created by blunt dissection in dartos fascia. The prosthesis is placed in the pouch and fixed to the dartos fascia to prevent prosthesis migration. Usual preop diagnosis: Absent testis, either congenital or following orchiectomy Reduction of testicular torsion is an emergency operation that must be performed within 6 h of occurrence to prevent irreversible ischemic damage to the testis. Through a small scrotal incision, the testis is reduced and fixed to the dartos fascia to prevent retorsion. Many of these procedures are done on an outpatient basis, and the anesthetic should be appropriately planned to facilitate early discharge. A transverse or longitudinal perineal incision is made and carried down to the urethra, which is dissected free from surrounding tissues. The strictured area is excised and end-to-end anastomosis is performed over a catheter. Repair of a long urethral stricture may require placement of a patch from the scrotum, foreskin, or buccal mucosa. Usual preop diagnosis: Urethral stricture, usually posttraumatic Urethrectomy: Partial or total urethrectomy is done through a longitudinal perineal incision. The urethra is dissected free of surrounding tissues and followed proximally and distally from the membranous urethra to the external urethral meatus. In total urethrectomy, a tubularized skin graft is interposed between membranous urethra and perineal skin. Usual preop diagnosis: Urethral carcinoma Insertion of artificial urinary sphincter, performed for incontinence, consists of a perineal incision, through which a cuff is inserted around the bulbar urethra. A suprapubic incision is made to place the reservoir and pump, which inflates and deflates the cuff. Usual preop diagnosis: Urinary incontinence Transperineal prostate seed implantation (brachytherapy): High doses of radiation can be delivered to the prostate by implanting radioactive seeds directly into the prostate gland. Using a transrectal ultrasound probe, radioactive seeds (iodine 125 or palladium 103) are implanted into the prostate. The patient is placed in lithotomy position, and a rectal ultrasound probe, with a perineal grid attached, is introduced to image the prostate. This procedure is done by a combined team of radiation oncologists and urologists. Lumbar epidural anesthesia may be less reliable at providing sacral anesthesia and offers no advantages over the above techniques for shorter procedures, although caudal anesthesia may be an acceptable alternative. They include the following: Repair of vesicovaginal fistulas: the vaginal approach is usually recommended for small and distally located vesicovaginal fistulas; otherwise, a transabdominal repair is performed (see Open Bladder Operations, p. An incision is made in the anterior vaginal wall around the fistula, which is excised. Bladder and vaginal walls are separated and closed with interposition of tissues or flaps to separate the incisions and prevent recurrence. Variant approach: Transabdominal repair of vesicovaginal fistula (see Open Bladder Operations, p. Usual preop diagnosis: Vesicovaginal fistula Operations to correct stress urinary incontinence: Many procedures have been designed to correct female urinary incontinence. They fall into two basic groups: (a) operations to correct hypermobility of the urethra and (b) operations to correct nonfunctioning urethra. The operation most commonly used by urologists to correct hypermobility is the Stamey procedure. The operation is performed through two small suprapubic incisions, one on each side of the midline, and an anterior vaginal incision. A nylon suture is placed in a loop from either side of the bladder neck and not around it. Cystoscopy is used to ensure proper placement and to prevent the suture from transversing the bladder. When the sutures are pulled up and tied over the anterior rectus sheath, they pull the bladder neck up to its original position behind the symphysis pubis and restore the acute posterior ureterovesical angle. A variant of this procedure is the Raz bladder neck suspension, where bolsters are not used. Operations to correct a nonfunctioning urethra include submucosal collagen injection at the bladder neck or construction of a sling. Rectus fascia, fascia lata of the thigh, or the vaginal wall can be used to construct a sling around the urethra. Sling operations are the most common procedures done for correction of stress incontinence. Many modifications have been made with reference to the placement of anchorage of the sling; therefore, there are a large number of procedures with different names utilizing the same principle.
Purchase speman online
Once they have passed through the foramen transversarium of C1 prostate oncology york cheap 60pills speman visa, the vertebral arteries travel across the posterior arch of C1 crossing the medial posterior aspect of the atlanto-occipital joint and through the suboccipital triangle before entering the foramen magnum. This diagonal course across the posteromedial aspect of the atlanto-occipital joint provides an important landmark for performing atlanto-occipital injections. Although this is the classic description, the vertebral arteries can be asymmetric [26] and have tortuous and unpredictable anatomical variance between the vertebral artery, and the bony structures suggest that no reliable placement of a needle may be expected to be completely safe, and transarterial or intra- Nerves the C1 nerve root (suboccipital nerve) exits between the skull and the C1 vertebrae. It provides motor innervation to the suboccipital muscles and interconnects with fibers of the C2 and C3 nerves. Its course often covers a 22 Atlanto-Occipital and Atlanto-Axial Joint Injections 417 arterial injections are always a potential disastrous complication. Of note, the vertebral artery is covered during its entire course with a large plexus of veins. Barring intravascular spread of contrast, medication can be incrementally injected with intermittent aspiration via extension tubing under close scrutiny for neurovascular compromise or change in neurologic status. Technical Aspects Injections may be performed either under fluoroscopy or under ultrasound guidance. Atlanto-Occipital: Ultrasound-Guided Technique the patient is placed comfortably in the prone position with a small roll or towel placed under the chin to accentuate cervical flexion. The cervical level can be identified by scanning inferiorly from the base of the occiput. The ultrasound probe is placed in the transverse position in the midline starting at the inion. The posterior arch of C1 does not have a spinous process, and the first bifid spinous process is C2. Scanning laterally off midline, it will be possible to visualize the vertebral artery as it passes through the transverse processes. By moving the transducer cranial/caudal, the vertebral artery should be traced from medial to lateral, and inferior to superior, until it is seen to move diagonally and medially near the atlantooccipital joint. To perform an atlanto-occipital joint injection, the needle should be directed toward the superior-posterior-lateral aspect of the joint to avoid the vertebral artery medially. Power Doppler can be used to help identify the vertebral artery as it wraps around the C1 lateral arch. As an added safety feature, once the anatomy has been identified using ultrasound, an injection of contrast under live fluoroscopy may provide Atlanto-Occipital Injection Under Fluoroscopic Guidance the patient is placed in the prone position with a small roll or towel placed under the chin to accentuate cervical flexion. Although both atlanto-occipital and atlanto-axial injection can be performed under ultrasound guidance, fluoroscopic guidance is most commonly utilized to identify the vertebral bodies of C1 and C2 by identifying the characteristic odontoid process of C2. It is important to visualize the vertebrae of C1 and C2 midline, accounting for any rotation. After negative aspiration, injection of contrast under fluoroscopy is recommended to assure correct placement of the needle. If the needle tip is directed too medially, it may cause inadvertent puncture of the vertebral artery or the dural sleeve. The injectate may consist of either local anesthetic alone or local anesthetic with a corticosteroid. Due to the potential for arterial injection of medication, the present authors recommend that, if a steroid is intended for use, soluble drugs such as dexamethasone should be used to the exclusion of insoluble. If a local anesthetic alone is selected for injection, there does not appear to be any advantage conferred by using high concentrations (0. In fact, there is no data to support using any local anesthetic more potent or longer acting than 1. Therefore, this is the drug of choice by the present authors when injecting the atlanto-axial or atlanto-occipital joints with or without ultrasound guidance. Atlanto-Axial Injection Under Fluoroscopic Guidance the patient is similarly positioned and prepared as above. It is critically important to adjust the C-arm and clearly visualize the atlanto-axial joint. The target for atlanto-axial joint injection is the space between the exiting C2 root and the vertebral artery. Once the image is optimized under anterior-posterior fluoroscopic guidance, a needle should be directed toward the junction of the middle and lateral thirds of the posterior aspect of the joint to avoid the C2 nerve root medially or the vertebral artery laterally. A lateral radiograph should be obtained to determine appropriate needle placement within the atlanto-axial joint. After negative aspiration, injection of contrast under live fluoroscopy is recommended to assure correct needle placement. Barring intravascular spread of contrast, medication can be incrementally injected with intermittent 22 Atlanto-Occipital and Atlanto-Axial Joint Injections 419. Atlanto-Axial: Ultrasound-Guided Technique the patient is placed comfortably in the prone position with a small roll or towel placed under the chin to accentuate cervical flexion. Both high- or low-frequency transducers can be used for this procedure depending on body habitus. The ultrasound transducer is placed in the transverse position midline to visualize the occiput. The C2 spinous process is the first and most superior cervical vertebrae with a bifid spinous process. When the C2 spinous process and lamina are identified, the transducer is moved laterally to identify the exiting C2 nerve root. Moving the ultrasound probe further laterally, the vertebral artery can be identified. The target for an atlanto-axial joint injection is the space between the exiting C2 root and the vertebral artery. As a further assurance of correct needle tip placement, an injection of contrast under live fluoroscopy may be undertaken to assure correct placement of medication. The volume of injectate and consistency of the injectate should be less than 1 mL as previously discussed. Inadvertent intravascular injection of local anesthetic can lead to anesthetic toxicity, presenting first with signs and symptoms of anesthetic toxicity to the central nervous system including a metallic a taste in the mouth and ringing in the ears. This may be followed by the development of ataxia, dizziness, or seizures depending upon the dose of local anesthetic injected and the rate of vascular absorption. Higher doses or rapid absorption centrally of local anesthetic can lead to cardiovascular system toxicity after the initial central nervous system manifestations. Injection of insoluble (particulate) steroids may lead to embolic infarction of the central nervous system. Subarachnoid administration of local anesthetic in this region can result in an immediate total spinal anesthetic. These injections are contraindicated in patients with cervical joint hypermobility or joint instability or in those who are taking antiplatelet drugs or other anticoagulation medications. Injection of contrast under fluoroscopy is recommended to assure needle placement prior to injection of medication. Cervicogenic headaches may have atlanto-occipital and atlanto-axial osteoarthritis and ligament pathology as potential etiologies. These abnormalities might be revealed by x-ray but may also only be detected from provocative and anesthetic injections. Though effective for a group of patients, these injections have increased levels of inherent risk and should only be performed by highly experienced physicians. Because of the highly vascular nature of this region, only small volumes of local anesthetic should be injected after meticulous evaluation of contrast flow patterns. The literature is limited in defining role, safety, and therapeutic outcome of these injections. There is no defined evidence that short- or long-term relief can be expected with this block. Currently there is scant evidence of efficacy of heat radiofrequency techniques of nerve supply of these joints. Andrea Trescot, Hans Hansen, and Laxmaiah Manchikanti for their contributions to the understanding and treatment of cervicogenic headache. Side Effects and Complications Complications associated with atlanto-occipital/atlanto-axial injection are primarily related to the close proximity of the target structures to the foramen magnum and the vertebral arteries.
| Comparative prices of Speman | ||
| # | Retailer | Average price |
| 1 | H-E-B | 604 |
| 2 | Big Lots | 711 |
| 3 | Staples | 413 |
| 4 | Price Chopper Supermkts | 160 |
| 5 | Neiman Marcus | 235 |
| 6 | Ahold USA / Royal Ahold | 162 |
Effective 60pills speman
Based on a comprehensive review of the literature and assessment of all factors prostate cancer jokes purchase cheap speman on line, Manchikanti et al. There is good evidence for the risk of a thromboembolic phenomenon in patients who stop antithrombotic therapy. There is fair evidence that excessive bleeding, including epidural hematoma formation, may occur with interventional techniques when antithrombotic therapy is continued. The risk of thromboembolic phenomenon is higher than the risk of epidural hematomas when antiplatelet therapy is stopped prior to interventional techniques. There is fair evidence to continue phosphodiesterase inhibitors (dipyridamole [Persantine], cilostazol [Pletal], and Aggrenox [aspirin and dipyridamole]) and that anatomic conditions such as spondylosis, ankylosing spondylitis, and spinal stenosis and procedures involving the cervical spine, multiple attempts, and large bore needles increase the risk of epidural hematoma; and rapid assessment and surgical or nonsurgical intervention to manage patients with epidural hematoma can avoid permanent neurological complications. The risks of a thromboembolic phenomenon and bleeding with hematoma formation must be considered equally. In this regard, the simultaneous use of multiple agents that possess anticoagulant properties. The new oral anticoagulants dabigatran etexilate (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis) are increasingly used to replace warfarin for their predictable pharmacokinetic and pharmacodynamic profiles. However, there is limited evidence on how to manage bleeding in patients taking them, and no specific antidote is known to reverse their anticoagulant effect. Advantages of these new anticoagulants include that monitoring of coagulation function is not routinely necessary which may be useful of course in emergencies. It is excreted renally unchanged, greater than 80%, and through bile, 5% to 10%, with plasma protein binding of 35%. For low-risk, paravertebral, or caudal interventional techniques, it may be stopped for 1 day in patients with normal renal function. It is excreted renally with 50% inactive, to a total of 66%, and through feces, 33%, with plasma protein binding of 95%. Excretion is through the kidneys with 25% to 30% renally and 56% through feces with plasma protein binding of 87%. There is limited evidence in reference to newer antithrombotic agents dabigatran (Pradaxa) rivaroxaban (Xarelto), and Edoxaban (Savaysa) to discontinue usage to avoid bleeding and epidural hematomas during interventional techniques and to continue to avoid cerebrovascular and cardiovascular thromboembolic events. Assessment of practice patterns of perioperative management of antiplatelet and anticoagulant therapy in interventional pain management. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. A systematic review and meta-analysis on the hazards of discontinuing or not adhering to aspirin among 50,279 patients at risk for coronary artery disease. Incidence of death and acute myocardial infarction associated with stopping clopidogrel after acute coronary syndrome. Interventional pain management is a specialty that utilizes minimally invasive procedures to diagnose and treat chronic pain in patients undergoing exogenous anticoagulants and antithrombotics. The risk of major bleeding is very small, but the consequences can be catastrophic. Based on multiple reviews and guidelines, there is good evidence for the risk of a thromboembolic phenomenon in patients who stop antithrombotic therapy. There is fair evidence that the risk of a thromboembolic phenomenon is higher than the risk of epidural hematomas when antiplatelet therapy is stopped prior to interventional techniques. There is fair evidence for continuing phosphodiesterase inhibitors (dipyridamole [Persantine], cilostazol [Pletal], and Aggrenox [aspirin and dipyridamole]). There is limited evidence for stopping antiplatelet therapy with platelet aggregation inhibitors to avoid bleeding and epidural hematomas and/or to continue antiplatelet therapy with clopidogrel (Plavix), ticlopidine (Ticlid), or prasugrel (Effient) during interventional techniques to avoid cerebrovascular and cardiovascular thromboembolic fatalities. Aspirin for the prevention of cardiovascular events in patients with peripheral artery disease: a meta-analysis of randomized trials. Clopidogrel use and long-term clinical outcomes after drug-eluting stent implantation. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. Effectiveness and safety of combined antiplatelet and anticoagulant therapy: a critical review of the evidence from randomized controlled trials. A randomised controlled trial of triple antiplatelet therapy (aspirin, clopidogrel and dipyridamole) in the secondary prevention of stroke: safety, tolerability and feasibility. Aspirin combined with clopidogrel (Plavix) decreases cardiovascular events in patients with acute coronary syndrome. Preoperative antiplatelet therapy does not increase the risk of spinal hematoma associated with regional anesthesia. Does preoperative antiplatelet therapy increase the risk of hemorrhagic complications associated with regional anesthesia Neuraxial blockade and thromboembolism prophylaxis/antithrombotic therapy: revised recommendations of the German Society of Anaesthesiology and Intensive Care. Regional anesthesia and anticoagulant drugs: a survey of current Italian practice. Hemostasis-altering drugs and techniques for regional anesthesia and analgesia: safety recommendations. Recommendations of the task force on perioperative coagulation of the Austrian Society for anesthesiology and intensive care medicine. Vandermeulen E, Singelyn F, Vercauteren M, et al; Belgian Association for Regional Anesthesia Working Party on Anticoagulants and Central Nerve Blocks. Belgian guidelines concerning central neural blockade in patients with drug-induced alteration of coagulation: an update. Risk assessment of hemorrhagic complications associated with nonsteroidal antiinflammatory medications in ambulatory pain clinic patients undergoing epidural steroid injection. Anticoagulation and neuraxial block: historical perspective, anesthetic implications, and risk management. A review of neuraxial epidural morbidity: experience of more than 8,000 cases at a single teaching hospital. Relation of the site of acute myocardial infarction to the most severe coronary arterial stenosis at prior angiography. Pathology of fatal perioperative myocardial infarction: implications regarding physiopathology and prevention. The pathophysiology of perioperative myocardial infarction: facts and perspectives. Activation markers of coagulation and fibrinolysis: alterations and predictive value in acute coronary syndrome. Optimal timing of discontinuation of clopidogrel and risk of blood transfusion after coronary surgery. Bridging therapy in the perioperative management of patients with drug-eluting stents. Conflicting clinical environment about the management of antithrombotic agents during the periendoscopic period in Japan. Clopidogrel is not associated with major bleeding complications during peripheral arterial surgery. Evaluation of safety of endoscopic biopsy without cessation of antithrombotic agents in Japan. Perioperative management of patients receiving oral anticoagulants: a systematic review. Regional anaesthesia in the patient receiving antithrombotic and antiplatelet therapy. Nordic guidelines for neuraxial blocks in disturbed haemostasis from the Scandinavian Society of Anaesthesiology and intensive care medicine. Gogarten W, Vandermeulen E, Van Aken H, et al; European Society of Anaesthesiology. Practical management of bleeding due to the anticoagulants dabigatran, rivaroxaban, and apixaban. Management of patients with recently implanted coronary stents on dual antiplatelet therapy who need to undergo major surgery. Focused clinical review: periprocedural management of antiplatelet therapy in patients with coronary stents. Antiplatelet drugs: a review of their pharmacology and management in the perioperative period.
Cheap 60pills speman visa
Of note androgen hormone melatonin buy speman overnight, the outer diameters of the artery in the foramen and a 22 g needle are quite similar. If paresthesia is observed, the needle must be withdrawn approximately a millimeter or so, and contrast is injected. After negative aspiration for blood and cerebrospinal fluid and also negative vascular and intrathecal/subdural contrast spread, inject the medication. Multiple causes described for chronic thoracic and chest wall pain include disc herniation, discogenic pain, post-thoracic laminectomy syndrome, and spinal stenosis. Thoracic epidural injections are administered with two approaches, namely, interlaminar and transforaminal, with both approaches associated with certain benefits and risks. Thoracic epidural injections are indicated in patients with chronic low back and lower extremity pain who have failed to respond to conservative modalities of treatments. Anatomically, the angulation is mild from T1 to T4 and T9 to T12, whereas angulation is more marked downward from T5 to T8, influencing the ease of entry into the epidural space, with increased technical difficulty between T5 and T8. Asymptomatic versus symptomatic herniated thoracic discs: their frequency and characteristics as detected by computed tomography after myelography. Safeguards to prevent neurologic complications after epidural steroid injections: analysis of evidence and lack of applicability of controversial policies. The complications related to needle placement include infection, hematoma formation, abscess formation, subdural injection, intracranial air injection, nerve damage, intravascular injection, vascular injury, spinal cord ischemia, paralysis, pneumothorax, and cerebral vascular or pulmonary embolus. Multiple precautions must be exercised with application of risk reduction strategies in performing transforaminal epidural injections. Acknowledgments this book chapter is modified and updated from a previous book chapter, "Thoracic Interlaminar Epidural Steroid Injections" by Kenneth P. Immediate complications and pain relief associated with 296 fluoroscopically guided thoracic foraminal nerve blocks. Thoracic interlaminar epidural injections in managing chronic thoracic pain: a randomized, double-blind, controlled trial with a 2-year follow-up. Spinal cord stimulation for treatment of pain in a patient with post thoracotomy pain syndrome. Comparative study of the azygous venous system in man, monkey, dog, cat, rat and rabbit. The dorsomedian connective tissue band in the lumbar epidural space of humans: an anatomical study using epiduroscopy in autopsy cases. Assessing the superiority of saline versus air for use in the epidural loss-of-resistance technique: a literature review. Accidental subdural injection during attempted lumbar epidural block may present as a failed or inadequate block: radiographic evidence. Needle position analysis in cases of paralysis from transforaminal epidurals: consider alternative approaches to traditional techniques. Valor de la aspiracion liquada en al espacio peridural en la anesthesia peridural. Effects of steroids and lipopolysaccharide on spontaneous resorption of herniated intervertebral discs. Local corticosteroid application blocks transmission in normal nociceptive C-fibers. The effect of epidural injection of betamethasone or bupivacaine in a rat model of lumbar radiculopathy. Foundations of pain medicine and interventional pain management: a comprehensive review. The prolonged analgesic effect of epidural ropivacaine in a rat model of neuropathic pain. Do corticosteroids produce additional benefit in nerve root infiltration for lumbar disc herniation. Efficacy of epidural injections in managing chronic spinal pain: a best evidence synthesis. Digital subtraction angiography does not reliably prevent paraplegia associated with lumbar transforaminal epidural steroid injection. Incidence of neurologic complications related to thoracic epidural catheterization. Prevention and management of complications resulting from common spinal injections. Adverse effects of fluoroscopically guided interlaminar thoracic epidural steroid injections. Regional anaesthesia and antithrombotic agents: recommendations of the European Society of anaesthesiology. Falco 13 Introduction Chronic neck pain is common in the general population and is associated with significant economic, societal, and health impact, similar to low back pain, and is the number 4 cause of disability in the United States [1]. Neck and upper extremity pain with headaches have been shown to be caused by intervertebral discs, cervical facet joints, ligaments, fascia, muscles, and nerve root dura which are capable of transmitting pain [2]. Among the multiple treatments described in managing neck and upper extremity pain of disc and nerve irritation without involveL. History In 1933, Dogliotti [5] introduced the technique of cervical epidural injection describing the loss of resistance technique as a sudden loss of resistance to injection when the needle bevel was passed from the ligamentum flavum into the epidural space. In the same year, Gutierrez [6] described the hanging drop technique to identify epidural space. While it is difficult to ascertain the history of cervical transforaminal injections with any accuracy [19], it appears that the first report of the use of cervical transforaminal injections was by Morvan et al. Even then, the literature on cervical transforaminal injections, either for diagnostic or therapeutic purposes, is sparse. Compression accounts for numbness, paresthesia, weakness, and hyporeflexia by blocking conduction in nerves and causing ischemia, but radicular pain may have other explanations in addition to compression. Pain compression both contribute caused by mechanical forces superimposed to lumbar pain on chemically activated nociceptors Disc Rupture and Nuclear Herniation. Reprinted with permission Central stenosis Thickened ligamentum flavum Lateral recess stenosis Forminal stenosis 212 Table 13. The fact that so many structures, spinal and otherwise, are packed into such a small cylinder, connecting the head to the thorax, makes the entire neck an outstanding feat of efficient design as shown in. These are some of the smallest but most distinct vertebrae of any vertebral region.
60 pills speman sale
Any particulate matter (including particulate steroid) has the potential to occlude the distal arterioles of these spinal end arteries prostate cancer vitamin e order speman 60pills on line, creating extensive cord infarction in the downstream spinal tissue. It is crucial for the spinal injectionist to have a detailed understanding of spinal anatomy. The spinal column is a complex structure consisting of multiple bones, ligaments, and intervertebral discs, which are functionally integrated to facilitate upright locomotion and to provide protection for the spinal cord. The image appearing on the fluoroscopic monitor is a composite representation of the overlapping tissue densities that lie between the x-ray tube and the image intensifier. The prototypical vertebra is composed of an anterior cylindrical block of bone called the vertebral body which is connected to the posterior neural arch by the pedicles. The sacrum is a triangular block of bone that is adapted in part to transmit weight from the upper body to the lower extremities through the sacroiliac joints. The spinal cord begins within the skull, exits the foramen magnum, and ends with the filum terminale at approximately L1/L2, giving rise to 31 pairs of spinal nerves. Schultz Posterior spinal arteries Anterior spinal artery Anterior segmental medullary artery Anterior radicular artery Posterior radicular artery Branch to vertebral body and dura mater Spinal branch Dorsal branch of posterior intercostal artery Posterior intercostal artery Paravertebral anastomoses Prevertebral anastomoses Thoracic (descending) aorta Section through thoracic level: anterosuperior view Sulcal (central) branches to right side of spinal cord Posterior radicular artery Anterior segmental medullary artery Pial arterial plexus Anterior and posterior radicular arteries Anterior spinal artery Right posterior spinal artery Peripheral branches from pial plexus Sulcal (central) branches to left side of spinal cord Left posterior spinal artery Posterior radicular artery Arterial distribution: schema Anterior segmental medullary artery Pial arterial plexus Note: All spinal nerve roots have associated radicular or segmental medullary arteries. All rights reserved) 7 Anatomy of the Spine for the Interventionalist Crura of diaphragm Posterior longitudinal ligament Psoas 87 Dura Pedicle Aorta Cauda equina Internal vertebral plexus of veins in extradural space Ligamenta flava Interspinous ligament Supraspinous ligament Quadratus lumborum Vein Erector spinae muscles Lumbar artery Intervertebral foramen Intervertebral disc Vertebra Skin Lamina. The intervertebral discs fill the spaces between adjacent vertebral bodies from C2 to the sacrum with a central semiliquid nucleus pulposus surrounded by a circumferential annulus fibrosus. The spinal cord receives its blood supply from three longitudinal arteries including a single anterior spinal artery and two posterior spinal arteries and a variable number of intraforaminal segmental arteries that pose direct routes of injection into the spinal cord. Cervical transforaminal epidural injections are associated with extremely high risk. In contrast, the arteries can be avoided in the majority of the patients with alternate techniques. Acknowledgments this book chapter is modified and updated from a previous book chapter, "Spinal Anatomy for the Interventionalist" by David M. Engel A, King W, MacVicar J, Standards Division of the International Spine Intervention Society. The effectiveness and risks of fluoroscopically guided cervical transforaminal injections. Anatomic dissection that demonstrates the path of the C8 radicular artery (arrowheads) as it follows the inferior aspect of the C8 spinal nerve through the intervertebral foramen to join with the anterior spinal artery. This specific vessel is larger than a 22-gauge needle (shown for scale) of steroids: a systematic review with comprehensive analysis of the published data. Latchaw 8 Introduction the role of this chapter is to demonstrate and discuss pertinent imaging findings, both normal and pathological, that will aid the spinal interventionalist in providing therapy to the patient. Important points regarding the imaging characteristics of both normal and abnormal conditions are discussed in the legends to the many illustrations. Inserts have been added that stress the important findings to observe when treating a given condition and the advantages and disadvantages of the modalities used to image the spine. Because of this, references for a given topic have been chosen that discuss findings on imaging that insure the specificity of the diagnosis or that will affect treatment. Because the cortex is seen as a signal void, subtle cortical fractures may be missed. The axial view (b) demonstrates a small disc protrusion in the midline, having obtuse margination with the rest of the disc, typical of a protrusion. There is a small annular fissure (arrow) through which the nucleus pulposus projects through the annulus. Part of this extrusion has a higher water content (arrow), indicating its recent herniation. The axial view (b) demonstrates another component extending into the lateral recess at the disc space level, posteriorly displacing the right L4 nerve root (arrow). Considerations are a nerve sheath tumor such as a schwannoma and an extruded or free disc fragment. The enhanced fat-suppressed axial T1 image (c) shows peripheral enhancement (arrow), typical of the inflammatory component around a disc fragment. A schwannoma would enhance homogeneously unless there was central cyst formation, which the unenhanced sequences do not demonstrate. The axial T2 image (e) shows that this mass (arrow) is epidural in location, displacing the thecal sac to the right. An enhanced axial image (f) demonstrates the classic peripheral ring of enhancement typically seen surrounding a disc fragment (arrow). While the location on the sagittal image (d) might have suggested a meningioma or schwannoma, both of these possible tumors would have been intradural and shown homogenous enhancement, plus a schwannoma would have been hyperintense on the T2 images. The fissure is usually asymptomatic, although some believe that there may be irritating substances secreted through it during its initial formation 8 Radiology of the Spine for the Interventionalist 95. The root courses in the foramen superior to the disc plane, and so the sagittal view (b) is needed to determine if the root is compressed by this disc extrusion, which it is (arrow), or if the root courses above the disc extrusion extruded disc, a schwannoma, and some other type of intraspinal tumor. The enhanced fat-suppressed T1 image (b) demonstrates peripheral enhancement of the left lateral recess mass (arrow), typical of a disc fragment, with the thecal sac being the "second mass," displaced to the right anteroposterior slippage, may be predisposed due to congenital spinal stenosis. While osteomyelitis/discitis can produce edema in the bone, there was no edema in the disc and no disc enhancement (not shown), typical of such a process. The axial T2-weighted image (c) shows a bulging disc with an annular fissure and moderate facet hypertrophy, producing a mild degree of central canal spinal stenosis 8 Radiology of the Spine for the Interventionalist 97. The sagittal view (b) demonstrates a grade 2 spondylolisthesis (arrow) secondary to the severe facet disease. The left neural foramen is deformed by the slippage (c), and the exiting left L4 root (arrow) is compressed between the osteophytic facets and the degenerated disc. The sagittal T2 sequence (a) shows the central canal throughout the lumbar spine to be congenitally narrow.
Order speman australia
On the other hand prostate cancer 7 out of 12 speman 60 pills fast delivery, rheumatoid arthritis is an autoimmune systemic inflammatory disease affecting the synovium of the shoulder joint. Although shoulder involvement typically occurs late in the course of the disease, shoulder involvement is fairly common in rheumatoid arthritis. This is usually chronic in nature, associated with periodic exacerbations secondary to inflammation. The earliest changes include narrowing of the articular cartilage and inferior glenoid fossa irregularities. However, in advanced disease, a large spur may be evident along with flattening of the humeral head and obliteration of the articular cartilage at the inferior glenoid. However, oftentimes, correlation with symptomatology and clinical examination may not always be evident. Interventional Technical Aspects Landmark Approach the value of physical therapy and trial of nonsteroidal antiinflammatory drugs should not be underestimated. However, after failed conservative management, intra-articular injection with glucocorticoids or a series of injections with sodium hyaluronate may provide some relief from shoulder pain. With the advent of fluoroscopy and ultrasound, this increases the success rate and strongly recommended in patients who are obese. Injection of the glenohumeral joint can be done from an anterior and posterior approach. The patient is usually sitting comfortably with the arm resting at the side and the shoulder externally rotated. Anatomic landmarks include the head of the humerus, coracoid process, and the acromion. Glenohumeral Joint this is the most mobile joint in the body representing the articulation of the humerus and the glenoid fossa. This joint is stabilized by ligaments (joint capsule, labrum, and glenohumeral ligaments) and muscles that include the rotator cuff (supraspinatus, infraspinatus, teres minor, and subscapularis). Note the contrast flow into the joint cavity along the glenoid fossa Standard sterile technique must be followed at all times to decrease the chances of infection which can be catastrophic. Anterior Approach the needle is inserted 1 cm lateral to the coracoid process just medial to the head of the humerus. If the needle gets contact against bone, it should be redirected in a different angle. After standard aseptic technique, a needle is introduced through the skin with an in-plane technique from the lateral shoulder with a medial trajectory. The target for the needle position is the posterior humeral head near the posterior labrum. Care is made to avoid injuring the labrum or the articular surface of the humerus. Elbow Joint Introduction Elbow pain may be attributed to pain generators originating from the joint itself and surrounding structures such as muscle and ligaments or to referred pain from the neck or the shoulder. Fluoroscopic-Guided Glenohumeral Joint Injection the patient is positioned supine on the table. The final target for the needle can be within the joint or along the superior-medial portion of the humeral head. Injection of contrast should demonstrate easy flow throughout the joint capsule which may also outline the biceps tendon sheath. After confirmation of needle placement, medication should also be injected without much resistance. Pathophysiology Elbow pain involves pathologic alteration in the musculotendinous origins of the extensor or flexor tendons at the lateral and medial epicondyles. The affected structure reveals edema and fibroblast proliferation in the subtendinous space, tendinopathy with hypervascularity, and spur formation with a sharp longitudinal ridge on the medial and lateral epicondyles [28]. Ultrasound-Guided Glenohumeral Joint Injection the patient is positioned lateral recumbent with the affected shoulder up. Scanning of the posterior shoulder is performed with the transducer in a transverse oblique plane to demonstrate Evidence Base In a review by Stephens et al. The common source of pain is the epicondyles that can easily be palpated on the medial and lateral sides of the distal humerus. Also, the elbow joint is surrounded by multiple bursae, and swelling may occur, causing pain. Ulnar and median nerves course thought the elbow joint that may be impinged causing entrapment syndrome. Examination of the elbow joint requires assessment of the range of motion (flexion, extension, pronation, and supination). Palpation of the lateral and medial epicondyles to determine tendinopathies and determine the presence of effusion and focal tenderness and olecranon bursa for swelling and thickening would allow diagnosis of elbow joint pathology. Repetitive movements of the elbow that exceed tissue capacity may be a cause of epicondylitis in both lateral and medial epicondyles. Gouty arthritis may involve the olecranon bursa and may be the initial presentation of gout. Since the elbow is a non-weight-bearing joint, degenerative changes are usually rare [30]. Narrowing or loss of joint space and osteophytic changes are consistent with osteoarthritis. However, radiographic imaging is rarely necessary besides traumatic injury of the elbow. Palpation of surface landmarks includes the soft tissue at the center of the triangle formed by the olecranon, head of the radius, and lateral epicondyle. As with any injection, aspiration is important to note the needle is not in a blood vessel. The injection should be slow and smooth without any resistance upon injection under constant pressure. Females are commonly affected than males with approximately 3 to 1 ratio [31, 32]. Interventional Technical Aspects Identification of the flexor carpi radialis and palmaris tendon on the wrist is necessary. Using a 25-gauge needle, make a skin wheal with lidocaine just medial to the palmaris longus tendon and approximately 1 cm proximal to the wrist crease. Aspirate to check for intravascular placement before injection of glucocorticoid, and it should be smooth with minimal to no resistance. Acquired or congenital structural changes of the carpal tunnel may result in the impingement of the median nerve. The lowest carpal tunnel pressure is seen when the wrist is in a neutral or slightly flexed position, and it increases proportionately with deviation from this posture as seen with computer use [35, 37, 38]. Ultrasound-Guided Carpal Tunnel Injection Ultrasound-guided injection is usually done to avoid direct trauma to the median nerve. A high-frequency linear probe is positioned in a transverse position across the carpal tunnel. The needle tip should pierce the transverse carpal ligament to enter the carpal tunnel. Easy flow of injectate should demonstrate hydrodissection of the median nerve away from the flexor tendons at the needle target site near the median nerve. In conclusion, a thorough history and physical examination are warranted prior to any type of intra-articular injections. A good grasp on anatomy and utilization of different imaging modalities improve outcome and success rate of such injections. Evidence Base Two good-quality randomized controlled trials have shown that corticosteroid injections were clinically more effective than placebo and oral corticosteroid in a 4-week period [39, 40].
Cheap speman 60pills online
They found that not only did the injections decrease the overall pain score by up to 50% but the patients also had significantly decreased number of paroxysmal pain attacks by over 60% by the end Myofascial Pain Syndrome Myofascial pain is pain arising from a group of muscles or their related fascia prostate 59 60pills speman fast delivery, and the areas of pain from where most of the symptoms originate are called the myofascial trigger points. For most sufferers of myofascial pain, the symptoms go away without intervention within a few weeks. Myofascial pain is very widespread; in one study, it was estimated that up to about 44 million Americans are affected. Other reports and studies showed that among patients with pain symptoms, up to 55% had myofascial trigger points. These patients were treated with trigger point injections of 20 to 60 units of botulinum toxin: one patient responded with significantly reduced pain and increased activity level within 1 week, while the other patient responded within 1 month. Despite the apparent success in treating myofascial pain syndromes in patients with concurrent sympathetic disease as described above, a review of the current literature shows that the overall evidence for botulinum toxin injections for myofascial pain syndromes is equivocal at this point. For example, one study that compared the botulinum toxin injections and saline injections into trigger points showed that the group that received the botulinum toxin injections had improved pain compared to 632 M. However, as promising as these studies seem, further larger-scale studies are required to make a definitive statement on the role of botulinum toxin on trigeminal neuralgia. Other Pain Syndromes There are other pain syndromes in which botulinum toxin shows promise. A series of five or six injections of about 20 to 30 units of botulinum toxin can be injected into the pelvic muscles for pain relief as well as for bowel control. They found that about 80% of patients reported improvement in their pain scores after their first injections and that 58% percent of the patients continued to have improvement of their pain scores on their second follow-up visits. A few patients did have adverse side effects, such as urinary incontinence, but the all of the adverse effects reversed with time. Patients with cervical dystonia have also benefited from botulinum toxin injections. As cervical dystonia patients not only have abnormal posturing of their necks but also chronic pain of the cervical region, botulinum toxin has been a welcome modality of treatment for those patients. Patients suffering from arthritic joint pains may also benefit from regular injections of botulinum toxin directly into the joints. Myofascial pain syndrome and its trigger points may also benefit from botulinum toxin injections; however, there is still a paucity of evidence to support regular botulinum toxin injections. Trigeminal neuralgia is a debilitating condition that requires treatments with medications and/or surgical interventions; botulinum toxin is a promising alternative therapy to patients with this disease. Patients with other pain syndromes such as pelvic pain and cervical dystonia may benefit from injections with botulinum toxin; however, because of the novelty of this treatment modality, further studies need to be performed to show significant benefits for patients with such syndromes. Historical notes on botulism, clostridium botulinum, botulinum toxin, and the idea of the therapeutic use of the toxin. Antinociceptive effect of botulinum toxin type a in rat model of carrageenan and capsaicin induced pain. Botulinum neurotoxin type a counteracts neuropathic pain and facilitates functional recovery after peripheral nerve injury in animal models. The applications of this promising medication are sprouting within various fields of chronic pain management. Further research into this fascinating therapy can only provide deeper understanding and more options for our treatment arsenal for chronic pain patients who are often resorting to dolorology as a last resort. Although closely associated with food poisoning from the ancient times, botulinum toxin was only utilized for its therapeutic purposes during the second half of the twentieth century. Botulinum toxin binds to the neuromuscular junction and prevents the release of acetylcholine into the synapse causing flaccid paralysis. Onabotulinumtoxin A for treatment of chronic migraine: pooled results from the doubleblind, randomized, placebo-controlled phases of the preempt clinical program. Intra-articular botulinum toxin type A: a new approach to treat arthritis joint pain. Repeat injections of intra-articular botulinum toxin A for the treatment of chronic arthritis joint pain. Botulinum toxin A (Botox) for treatment of proximal myofascial pain in complex regional pain syndrome: two cases. Botulinum toxin treatment of myofascial pain: a critical review of the literature. Candido 42 Introduction this chapter will review some of the basic techniques in the conduct of upper extremity joint injection and the main indications for specific intra-articular injections. The utilization of different approaches such as landmark, fluoroscopy, and ultrasound will be described and illustrated in this chapter. The choice of injectable medication that includes glucocorticoid with or without local anesthetic, the frequency of injection, and potential complications will likewise be addressed. Being equipped with the knowledge of anatomy and real-time needle guidance improves the success of joint injections and cannot be overemphasized. Needle and Syringe Size the best strategy is to use one needle and syringe size for the injections to allow the operator to get used to resistance offered by injecting through the same syringe and needle size. This will help recognize higher resistance afforded by injecting through a tendon substance. One may opt to use a larger needle such as 20 gauge if using a high viscosity material like hyaluronate. Too big of a syringe may create too much vacuum, and the opposite holds true for small syringes. However, small-volume tendon sheath injection can best be accomplished with tuberculin-sized syringe. Sterile Preparation General Technique When performing joint injections, a multitude of factors such as needle, syringe size, skin sterilization, and local anesthesia should be taken into account. Patients who are under anticoagulation on therapeutic dosages can still undergo these injections safely. Ultrasonography and fluoroscopy may be of value to ensure proper needle placement and improve accuracy [1]. Cleaning the injection site with iodine disinfectant and chlorhexidine prep kit is both acceptable [2, 3]. If the initial attempt was unsuccessful, it is advised to palpate and sterilize after identification of the different injection site. The commonly used preparations are methylprednisolone (Depo-Medrol) and triamcinolone acetonide (Kenalog). Another point of discussion was the practice of mixing glucocorticoid with lidocaine as a diluent. The lidocaine serves its role as a pain reliever as well as providing immediate relief. Also, with the dilution, there is decreased propensity to develop steroid-induced atrophy, irritation, and postinjection flare. Methylparaben, a bacteriostatic agent in local anesthetic, was found to be the culprit for precipitation of steroid crystals and therefore is usually avoided. There is an absence of definitive data regarding the dose of glucocorticoid and volume of injection to be used. Again, based on habits alone, 40 mg of steroid injection is used for large joints such as shoulders and knees; 30 mg for the wrist, ankle, and elbow; and 10 mg for small spaces such as tendon sheaths and metacarpophalangeal joints. The frequency of injection is likewise controversial due to theoretical mechanism for possible cartilage and tendon damage. Studies have demonstrated the capacity of glucocorticoids to inhibit the production of collagenases and other metalloproteases which may mediate cartilage destruction induced by rheumatoid arthritis or osteoarthritis [5, 6]. This normally occurs once the operator encounters a higher resistance flow during injection and is very crucial to be recognized and abort the injection. Once the perineurium is violated, moderate pain may ensue, accompanied by burning sensation. Minor complications such as skin atrophy, hypopigmentation, and dystrophic calcification around the joint capsule may occur. Systemic effect of steroids can manifest as ecchymoses, menstrual irregularity, cataract formation, hyperglycemia, osteoporosis, osteonecrosis, and suppression of hypothalamic-pituitary axis. Longer intervals between injections and good glycemic control especially in diabetic patients are advocated. Complications Complications following joint injections are rare besides the inherent risk of infection, tissue trauma, and bleeding.
