
Buy detrol 4mg low price
Overall symptoms pulmonary embolism cost of detrol, these disorders have a poor prognosis, but corticosteroids and other immunosuppressive agents have improved the survival rate (Biller and Grau, 2004). Infections and Stroke Intracranial vasculitis and stroke can result from meningovascular syphilis; prodromal manifestations are common before stroke. Other neurological manifestations in patients with secondary syphilis include headaches, meningismus, mental status changes, and cranial nerve abnormalities. Luetic aneurysms of the ascending aorta can extend to involve the origin of the great vessels and lead to stroke. Worldwide, an estimated 1 billion people are infected with Mycobacterium tuberculosis. The exudative basilar inflammation entraps the cranial nerves at the base of the brain, most frequently the third, fourth, and sixth cranial nerves. Fungal arteritis may result in aneurysms, pseudoaneurysms, thrombus formation, and cerebral infarction. Complications of acute purulent meningitis include intracranial arteritis and thrombophlebitis of the major venous sinuses and cortical veins. Intracranial arterial stenoses have been associated with a complicated clinical course. Varicella-zoster may cause a virus-induced necrotizing arteritis similar to granulomatous angiitis. Large-artery cerebrovascular occlusions have been found in association with meningoencephalitis caused by free living amebae. Other infectious agents known to produce cerebral infarcts include Mycoplasma pneumoniae, aspergillus, coxsackie 9 virus, California encephalitis virus, mumps paramyxovirus, hepatitis C virus, Borrelia burgdorferi, Rickettsia typhi group, cat-scratch disease, Trichinella infection, and the larval stage (cysticercus) of Taenia solium. Cerebrovascular involvement in neurocysticercosis is usually ischemic and is caused by chronic meningitis, arteritis, or endarteritis of small vessels. Unilateral or bilateral carotid artery occlusion can complicate necrotizing fasciitis of the parapharyngeal space. Infection with Chlamydia pneumoniae accelerates the process of atherosclerosis in animal studies; treatment with azithromycin has been shown to reduce the degree of atherosclerotic lesions in a rabbit model. The risk for intracerebral hemorrhage, especially among young women, has led to removal from the American market of phenylpropanolamine. Ephedra, also called ma-huang, widely used in weight-loss products, has been associated with high blood pressure, heart attacks, and strokes. Stroke in young athletes may also be the result of anabolic-androgen steroid abuse and recombinant erythropoietin ("blood doping") administration. Affected patients are mainly of Mediterranean or East Asian origin and may have a history of iritis, uveitis, and oral, genital, and mucocutaneous ulcerations. Cerebrovascular complications include strokes, carotid aneurysm formation, and cerebral venous thrombosis. Cogan syndrome is a rare condition characterized by nonsyphilitic interstitial keratitis, vestibular dysfunction, and deafness. The angiitic form of sarcoidosis primarily affects the eyes, meninges, and cerebral arteries and veins. Kohlmeier-Degos disease or malignant atrophic papulosis is a multisystem occlusive vasculopathy characterized by cutaneous, gastrointestinal, and neurological manifestations; it may be complicated by ischemic or hemorrhagic strokes. Cerebral vasculitis may also complicate the course of children with acute poststreptococcal glomerulonephritis. The disease, prevalent in young women of Asian, Mexican, or Native American ancestry, develops insidiously, causing stenosis, occlusion, aneurysmal dilatation, or coarctation of the involved vessels. In the acute or "prepulseless" phase, nonspecific systemic manifestations are present. Patients have rashes, erythema nodosum, fever, myalgias, arthritis, pleuritis, carotidynia, and elevated erythrocyte sedimentation rate. Months or years later, the second or occlusive phase develops and is characterized by multiple arterial occlusions. Patients may have cervical bruits, absent carotid or radial pulses, asymmetrical blood pressure recordings, and arterial hypertension. Surgical treatment (angioplasty or bypass) of severely stenotic vessels may be required. Cranial (giant cell or temporal) arteritis is a polysymptomatic systemic large-vessel arteritis with a predilection to involve carotid artery branches (see Chapter 103). Thromboangiitis obliterans, also known as Buerger disease, is a rare segmental, inflammatory, obliterative angiopathy of unknown cause. It is suspected in young men who smoke and have a history of superficial migratory thrombophlebitis presenting with distal limb ischemia accompanied by digital gangrene. Migraine and Stroke Migraine (see Chapters 20 and 103) affects women more often than men and may start during childhood or adolescence. Epidemiological studies suggest a nonrandom association of both headache and migraine with stroke, particularly among young women. The risk of intracerebral hemorrhage is not increased in persons who have migraines. The International Headache Society Classification and Diagnostic Criteria require that to establish a diagnosis of migrainous infarction, one or more migrainous aura symptoms must be present and not fully reversed within 7 days from onset, and must be associated with neuroimaging confirmation of ischemic infarction. This definition implies that a firm diagnosis of migraine with aura has been made in the past. Also, the clinical manifestations judged to be the result of a migrainous infarction must be those typical of previous attacks for that individual, and finally, other causes of infarction, including those related to migraine therapy need to be excluded by appropriate investigations. Headache accompanies a number of embolic or thrombotic causes of stroke, including cervicocephalic arterial dissections. Symptomatic migraine attacks are more frequent than migraine-induced ischemic insults. The usual scenario of migrainous infarction is one of recurrent episodes of gradual buildup of unilateral throbbing headaches, associated with stereotyped visual phenomena occurring in both visual fields simultaneously, in one of which the vision loss becomes permanent. Migrainous infarctions have been subdivided as definite when all the International Headache Society criteria are fulfilled and possible when some but not all criteria are fulfilled. The Notch 3 mutation has been thought to be one of the most common human mutations. Pathologically, there is a characteristic granular osmiophilic material in arterial walls, including dermal arteries. Three specific enzyme deficiencies responsible for homocystinuria have been identified: cystathionine-synthetase, homocysteine methyltransferase, and methylene tetrahydrofolate reductase. The accumulation of homocysteine in the blood leads to endothelial injury and premature atherosclerosis. Patients with homocystinuria may display a marfanoid habitus, malar flush, livedo reticularis, ectopia lentis, myopia, glaucoma, optic atrophy, psychiatric abnormalities, mental retardation, spasticity, seizures, osteoporosis, and a propensity for intracranial arterial or venous thrombosis. Raised levels of plasma homocysteine may be an independent risk factor for cerebrovascular disease, coronary artery disease, and peripheral arterial occlusive disease. Elevated levels of homocysteine can be effectively reduced with the administration of folic acid, occasionally requiring the addition of pyridoxine (vitamin B6) and vitamin B12. However, the treatment of high-normal homocysteine levels with folic acid and B-complex vitamins has not been associated with decreased stroke or coronary risk (Lonn et al. Other agents that may reduce homocysteine include choline, betaine, estrogen, and acetylcysteine. Fabry disease is an X-linked disorder of glycosphingolipid metabolism characterized by deficient lysosomal -galactosidase activity. As a result, deposits of ceramide trihexosidase accumulate in endothelial and smooth muscle cells. Patients have a painful peripheral neuropathy, renal disease, hypertension, cardiomegaly, autonomic dysfunction, and corneal opacifications. Characteristic dark red or blue lesions that do not blanch on pressure, called angiokeratoma corporis diffusum, are found between the umbilicus and knees. Marfan syndrome is an autosomal dominant inherited connective tissue disease associated with qualitative and quantitative defects of fibrillin. This disorder is characterized by a variety of skeletal, ocular, and cardiovascular findings. Patients with Marfan syndrome may display arachnodactyly, extreme limb length, joint laxity, pectus excavatum or carinatum, subluxation of the lens, and aortic valvular insufficiency. Marfan syndrome is associated with a high incidence of dilatation of the aortic root. Other cardiovascular abnormalities include coarctation of the aorta, mitral valve prolapse, and mitral annulus calcification with regurgitation.
Order 4 mg detrol with mastercard
Clinically affected patients present with subacute or insidious onset of upper motor neuron signs and gait instability medicine plus discount detrol online american express. Muscle aching and paresthesias may be present, but the sensory examination is largely normal. Partial recovery after discontinuation of Lathyrus intake is possible, but interestingly, there are reports of deterioration without further exposure many years later. Peyote Peyote (Lophophora williamsii) is a small cactus native to the southwestern United States and Mexico, but it can be cultivated anywhere. The principal agent is mescaline, which has actions similar to those of the hallucinogenic indoles. A peyote button, the top portion of the cactus, contains about 45 mg of mescaline; approximately six to nine buttons are sufficient to be hallucinogenic. Dizziness, drowsiness, ataxia, paresthesias, sympathomimetic symptoms, nausea, and vomiting are frequent accompanying clinical features. MorningGlory the active agents in morning glory (Ipomoea tricolor) seeds are various amides of lysergic acid. Acute clinical effects may also include mydriasis, nausea, vomiting, and diarrhea. MedicinalHerbs Treatment of illness with herbal remedies, either purchased over the counter at health food stores or procured from practitioners of traditional medicine, may lead to undesired toxicity. The labels, if present, may not fully represent the myriad of compounds contained within. Potentially harmful ingredients may be included as contaminants or intentionally added to increase a desired effect. Common MushroomPoisoning Of the more than 5000 varieties of mushrooms, approximately 100 are known to be toxic to humans. The common mushrooms associated with neurological morbidity are listed in Table 86. This can be further supplemented by specific treatments such as infusion of pyridoxine (gyromitrin poisoning), atropine (muscarine poisoning), or physostigmine (ibotenic acid and muscimol poisoning) as needed. The algae are consumed by small herbivorous fish that in turn are eaten by carnivorous ones. As a result, predatory fish such as barracuda, eel, sea bass, grouper, red snapper, and amberjack are likely to be more toxic, although practically any reef fish eaten in significant quantity can cause ciguatera. Outbreaks can also occur in residents of temperate areas after a return from travel or from consumption of imported fish. A number of toxins are responsible for ciguatera, including ciguatoxins and maitotoxin. Ciguatoxins are a group of lipidsoluble molecules that act on tetrodotoxin-sensitive voltagegated Na+ channels in nerve and muscle, leading to increased Na+ permeability at rest and membrane depolarization. It is a water-soluble compound that increases Ca2+ influx through voltage-independent Na+ channels. Symptoms are typically dose-dependent, with more severe poisonings occurring after consumption of the toxin-rich head, liver, and viscera of contaminated fish. Abdominal pain, nausea, vomiting, and diarrhea first appear within hours of ingestion. Patients develop centrifugal spread of paresthesias, involving the oral cavity, pharynx, limbs, trunk, genitalia, and perineum. Particularly characteristic is cold allodynia and a paradoxical temperature reversal when cold is perceived as burning, tingling, or unbearably hot. Headache, weakness, fatigue, arthralgia, myalgia, metallic taste, and pruritus are common. Symptoms may be worsened by alcohol consumption, exercise, sexual intercourse, or diets. Some patients are referred to psychiatrists by clinicians unfamiliar with the disease. Cold allodynia in the distal limbs is a common finding on neurological examination (Schnorf et al. George Vancouver recognized paralytic shellfish poisoning in the Pacific Northwest toward the end of the eighteenth century. Most marine toxins originate from micro-organisms, typically unicellular flagellated algae (dinoflagellates). The proliferation of toxin-producing algae depends on environmental and seasonal factors. During periods of intense algal proliferation ("blooms"), high concentrations of toxins accumulate in fish or shellfish, which then act as transvectors for human disease. Outbreaks may also lead to widespread mortality of fish, shellfish, or marine mammals. One of the algal blooms familiar to residents of the United States is the so-called red tide, which refers to the reddish brown discoloration of sea water. They are often stable to heat, acid, and normal food preparation procedures, making them particularly dangerous to unsuspecting consumers. Many of these toxins affect the Na+ channels in peripheral nerves, causing disorders that range from mild sensory symptoms to life-threatening weakness. The diagnosis depends on a history of ingestion and recognition of the appropriate clinical features. Whenever possible, the contaminated food should be retrieved and tested, as assays for many toxins are available. Most neurological symptoms remit in approximately 1 week, although some degree of paresthesias, asthenia, weakness, and headache may persist for months to years. Diagnosis is based on history of ingestion and the characteristic gastrointestinal, cardiovascular, and neurological disturbances. Clustering of cases in people who consumed the same fish helps with the diagnosis, though there is variation in individual susceptibility. Nerve conduction studies may show slowing of both sensory and motor conduction velocities, with prolongation of the absolute refractory, relative refractory, and supernormal periods. Intravenous mannitol (20%; 1 g/kg at 500 mL/h) has been used for treatment of acute ciguatera poisoning. The efficacy of mannitol is supported only by uncontrolled case series that report dramatic neurological improvement, especially if mannitol is given soon after symptom onset. One small controlled trial in 50 patients found no difference in outcome between mannitol and saline placebo (Schnorf et al. Supportive care during acute disease may include fluid replacement, control of bradycardia, and symptomatic treatment of anxiety, headache, and pain. Calcium gluconate, anticonvulsants, and corticosteroids have been tried with varying results. Gabapentin, pregabalin, amitriptyline, or other tricyclic antidepressants may provide partial relief of neuropathic pain. Fatality rates are high in severely affected individuals due to respiratory insufficiency, cardiac dysfunction, and hypotension (Chowdhury et al. Patients who survive the acute period of intoxication (approximately the first 24 hours) often recover without neurological sequelae. All of them are primarily associated with ingestion of bivalve mollusks (clams, mussels, scallops, oysters), filter feeders that can accumulate toxic microalgae. Rarely, poisoning is seen after consumption of other seafood such as predator crabs that may have eaten contaminated shellfish. Outbreaks are more frequent during the summer months, especially during periods of red tides, but they may occur in any month and in the absence of red tides. Mortality rates range from 1% to 12%, with higher rates in areas without advanced life support capabilities. Paresthesias develop and initially involve the perioral areas, oral cavity, face, and neck. Other symptoms may include headache, gait ataxia, and limb incoordination, as well as brainstem symptoms such as dysarthria, dysphagia, ophthalmoplegia, and pupillary abnormality. Despite the name of this syndrome, muscle paralysis does not develop in every patient. If present, weakness may involve muscles of the face, jaw, swallowing, respiration, and the upper and lower limbs. Spontaneous recovery begins after 12 hours and is usually complete within a few days. Initial diagnosis depends largely on recognizing the history and clinical features.
Order on line detrol
Efficacy of bevacizumab plus irinotecan in children with recurrent low-grade gliomas-a Pediatric Brain Tumor Consortium study treatment 02 discount detrol 2mg without prescription. Mutations of the human homolog of Drosophila patched in the nevoid basal cell carcinoma syndrome. Focal midbrain glioma: long term survival in a cohort of 16 patients and the implications for management. Management of cystic craniopharyngiomas with phosphorous-32 intracavitary irradiation. Medulloblastoma metastatic to the suprasellar region at diagnosis: a report of six cases with clinicopathologic correlation. Prognostic factors in infants and very young children with intracranial ependymomas. High-dose carboplatin, thiotepa and etoposide with autologous stem cell rescue for patients with previously irradiated recurrent medulloblastoma. Efficacy and safety of radical resection of primary and recurrent craniopharyngiomas in 86 children. Prognostic relevance of localization and grading in intracranial ependymomas of childhood. Atypical teratoid or rhabdoid tumors: improved outcome with high dose chemotherapy. The treatment of high grade gliomas and diffuse intrinsic pontine tumors of childhood and adolescence: a historical-and futuristic-perspective. Visual outcomes in children with neurofibromatosis type 1-associated optic pathway glioma following chemotherapy: a multicenter retrospective analysis. Inhibitors of histone deactelases as potential therapeutics for high-risk medulloblastoma and atypical teratoid/rhabdoid tumors. Riskadapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma- 96): long term follow Primary Nervous System Tumors in Infants and Children Hilden, J. Central nervous system atypical teratoid/rhabdoid tumor: results of therapy in children enrolled in a registry. A multi-institutional retrospective study of intracranial ependymoma in children: identification of risk factors. Intramedullary lowgrade astrocytomas: long-term outcome following radical surgery. Prognostic implications of atypical histologic features in choroid plexus papilloma. Craniopharyngiomas in children and adults: systematic analysis of 121 cases with long-term follow-up. Epidemiological survey of central nervous system germ cell tumors in Canadian children. The clinical, metabolic and endocrine features and the quality of life in adults with childhood-onset craniopharyngioma compared with adultonset craniopharyngioma. Radiological findings following postsurgical intratumoral bleomycin injection for cystic craniopharyngioma. Trilateral retinoblastoma: a meta-analysis of hereditary retinoblastoma associated with primary ectopic intracranial retinoblastoma. Histone deacetylase inhibition decreases proliferation and potentiates the effect of ionizing radiation in atypical teratoid/rhabdoid tumor cells. Sonic hedgehog signaling is required for expansion of granule neuron precursors and patterning of the mouse cerebellum. Molecular genetics of supratentorial primitive neuroectodermal tumors and pineoblastoma. Pediatric and adult sonic hedgehog medulloblastomas are clinically and molecularly distinct. Long-term results of radiotherapy for intracranial germinoma: a multi-institutional retrospective review of 126 patients. Successful treatment of disseminated central nervous system malignant rhabdoid tumor. Neurocognitive outcomes in pediatric and adolescent patients with central nervous system germinoma treated with a strategy of chemotherapy followed by reduced-dose and volume irradiation. Prognostic factors for progression of childhood optic pathway glioma: a systematic review. Standardrisk medulloblastoma treated by adjuvant chemotherapy followed by reduced-dose craniospinal radiation therapy: a French Society of Pediatric Oncology study. Spontaneous regression of optic gliomas: thirteen cases documented by serial neuroimaging. Intracranial ependymomas: an analysis of prognostic factors and patterns of failure. Health related quality of life and psychological outcome in patients treated for craniopharyngioma in childhood. Prediction of central nervous system embryonal tumour outcome based on gene expression. Supratentorial gangliogliomas: histopathologic grading and tumor recurrence in 184 patients with median follow-up of 8 years. Central neurocytoma: histologic atypia, proliferation potential, and clinical outcome. Acute neurotoxicity in children with B-precursor acute lymphoid leukemia: an association with intermediate-dose intravenous methotrexate and intrathecal triple therapy-a Pediatric Oncology Group study. The efficacy of stereotactic radiosurgery in the management of intracranial ependymoma. The impact of radiotherapy fields in the treatment of patients with choroid plexus carcinoma. Proton versus photon radiotherapy for common pediatric brain tumors: comparison of models of dose characteristics and their relationship to cognitive function. Does chemotherapy affect the visual outcome in children with optic pathway glioma Neurocognitive consequences of risk-adapted therapy for childhood medulloblastoma. Early diagnosis of subependymal giant cell astrocytoma in children with tuberous sclerosis. Myxopapillary ependymoma of the conus medullaris and filum terminale in the pediatric age group. Phase 2 study of temozolomide in children and adolescents with recurrent Primary Nervous System Tumors in Infants and Children Portwine, C. Absence of germline and somatic p53 alterations in children with sporadic brain tumors. Pediatric oligodendrogliomas: a study of molecular alterations on 1p and 19q using fluorescence in situ hybridization. Recurrence patterns across medulloblastoma subgroups: an integrated clinical and molecular analysis. Bithalamic involvement predicts poor outcome among children with thalamic glial tumors. Dysembryoplastic neuroepithelial tumor: an epidemiologic study from a single institution. Choriod plexus carcinomas are characterized by complex chromosomal alterations related to patient age and prognosis. Surgical outcomes and seizure control rates after resection of dysembryoplastic neuroepithelial tumors. Atypical tentorial meningioma 30 years after radiotherapy for a pituitary adenoma. Prospective clinical trials of intracranial low-grade glioma in adults and children. Optic pathway hypothalamic gliomas in children under three years of age: the role of chemotherapy. Microarray analysis of pediatric ependymoma identifies a cluster of 112 candidate genes including four transcripts at 22q12.
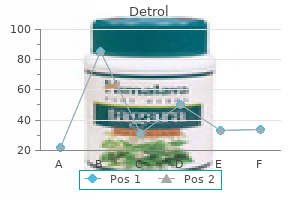
| Comparative prices of Detrol | ||
| # | Retailer | Average price |
| 1 | Rite Aid | 657 |
| 2 | Foot Locker | 204 |
| 3 | Hy-Vee | 168 |
| 4 | Burger King Holdings | 496 |
| 5 | PetSmart | 488 |
Purchase detrol 4mg on line
Two healthy young siblings developed ischemic stroke within "a few minutes" and "a few hours" of smoking the synthetic cannabinoid agonist Spice (Freeman et al medications hyponatremia buy detrol from india. CognitiveEffects Chronically altered mentation in drug users might be related to ethanol, infection. Determining whether the drugs themselves cause lasting cognitive or behavioral abnormality has been difficult; intoxication or withdrawal effects can persist for uncertain durations, and baseline cognitive performance prior to drug use is seldom available. A meta-analysis of studies addressing "neuropsychological consequences of chronic opioid use" (including prescription analgesics and methadone maintenance therapy) identified significant impairments in verbal working memory, verbal fluency, and "cognitive impulsivity," but the authors stressed methodological problems in the studies reviewed (Baldacchino et al. Structural and functional imaging studies have demonstrated reduced cerebral gray matter density and decreased white matter fractional anisotropy in heroin users (Bora et al. The effects are partially reversible, but regeneration can lead to aberrant pathways. Cocaine is not neurotoxic to axon terminals, but cognitive impairment is described. High doses of cocaine decrease hippocampal neurogenesis and impair working memory in rats (Sudai et al. Lasting cognitive impairment and structural alterations in frontostriatal systems are described in heavy cocaine users (Ersche et al. Cocaine-treated rats demonstrate abnormal dendritic spines on neurons in the nucleus accumbans, and in both rodents and humans, diffusion tensor imaging shows abnormal fractional anisotropy in cerebral white matter (Moeller et al. Reduced resting state functional connectivity between amygdala and prefrontal cortex predicted relapse in abstinent cocaine addicts (McHugh et al. Reduced frontal gray matter volume and increased striatal volume are described in users of either cocaine or amphetamine (Crunelle et al. A meta-analysis of neuroimaging studies in "stimulantdependent individuals" found consistent reduction of prefrontal gray matter," which was plausibly linked to impaired "self-regulation and self-awareness. Clinical, imaging, and animal studies provide persuasive evidence that marijuana use, especially during adolescence, causes lasting behavioral and cognitive alteration (Bolla et al. In the New Zealand Dunedin cohort study, which followed individuals from birth to age 38 years, heavy marijuana use by adolescents and young adults was associated with neuropsychological decline across multiple domains of functioning. Functional imaging during testing of executive function found abnormal patterns of activation after several weeks of abstinence (Bolla et al. Epidemiological studies offer compelling evidence that marijuana is a significant risk factor for schizophrenia (Le Bec et al. Sedative drugs cause reversible dementia in the elderly and delayed learning in small children. Severe axonal sensorimotor polyneuropathy affects sniffers of glue containing n-hexane. Rhabdomyolysis, myoglobinuria, and renal failure have followed use of heroin, psychostimulants, and phencyclidine (as well as ethanol) (Adrish et al. Myeloneuropathy indistinguishable from cobalamin deficiency and combined systems disease affects sniffers of nitrous oxide. The mechanism is inactivation of the cobalamin-dependent enzyme methionine synthetase. Such practice is associated with dementia, ataxia, dystonia, quadriparesis, blindness, and death as a result of a spongiform leukoencephalopathy most often affecting the posterior cerebrum and internal capsule. Irreversible extrapyramidal symptoms, including bradykinesia and dystonia, are described in users of methcathinone, a result of exposure to potassium permanganate used in preparing the drug (Steppins et al. Blindness occurred in a heroin user whose preparation contained large quantities of quinine. Cocaine users develop extrapyramidal symptoms progressing from repetitive stereotypic behavior ("punding") to choreoathetosis and dystonia. Marijuana inhibits follicle stimulating and luteinizing hormones, causing reversible erectile dysfunction in men and menstrual irregularity in women. Sensorineural hearing loss has followed overdose with either heroin or methadone (Aulet et al. Hallucinogen users not only experience flashbacks, but the visual phenomena-geometric shapes, objects in the peripheral field, flashes of color, enhanced color sensitivity, trailing and stroboscopic perception of moving objects, after images, halos, and macro/micropsia-can persist for years ("hallucinogen-persisting perception disorder") (Hermle et al. Complications attributable to levamisole in cocaine users include leukopenia and vasculitis. As of 2014, leukoencephalopathy, a recognized complication of levamisole, had not been documented in a cocaine user (Hofmaier et al. FetalEffects Adverse effects of in utero exposure to drugs are difficult to disentangle from inadequate prenatal care, concomitant ethanol or tobacco, malnutrition, and home environment. Fetal exposure to prescription opioids is associated with decreased gestational size, respiratory distress, and later, cognitive impairment (Broussard et al. In utero exposure to methamphetamine is significantly associated with restricted fetal growth, depressed arousal in neonates, and in older children, lower verbal memory, spatial memory, working memory, attention, and visual-motor integration. Lasting metabolic and structural changes affect frontostriatal circuitry (Roussotte et al. Neuropsychological testing has shown subtle abnormalities in executive functioning, and diffusion tensor imaging shows frontal white matter abnormalities (Bandstra et al. A 10-year prospective study controlling for such confounders as additional drugs and environmental influences concluded that first trimester exposure to cocaine conferred risk for reduced height, weight, and head circumference and for lower sociability and increased withdrawn behavior (Richardson et al. Adolescents exposed prenatally to cocaine had thinner prefrontal gray matter than controls (Liu et al. A systematic review of 27 studies concluded that prenatal cocaine exposure "increases the risk for small but significantly less favorable adolescent functioning," including variably, behavior, language, and memory. Eight studies reported morphological abnormalities of brain structure (BuckinghamHowes et al. Human and animal studies offer evidence that in utero exposure to marijuana carries risk for later cognitive impairment (Dinieri and Hurd, 2012). Long-term cohort studies have demonstrated impaired performance on tasks of attention and visual memory as well as greater impulsivity and smaller head size, persisting into adolescence (Fried et al. In animals, prenatal exposure disrupts cortical development by interfering with cytoskeletal dynamics critical for axonal connectivity between neurons (Tortoriello et al. Opioid overdose with gluteal compartment syndrome and acute peripheral neuropathy. Neuropsychological consequences of chronic opioid use: A quantitative review and meta-analysis. Mixed kappa/mu partial opioid agonists as potential treatments for cocaine dependence. Changes in oxycodone and heroin exposures in the National Poison Data System after introduction of extended-release oxycodone with abusedeterrent characteristics. Phenomenon of new drugs on the Internet: the case of ketamine derivative methoxetamine. Effects of repeated cocaine exposure on habit learning and reversal by N-acetylcysteine. Reduced frontal brain volume in non-treatment-seeking cocaine-dependent individuals: Exploring the role of impulsivity, depression, and smoking. The global epidemiology and burden of psychostimulant dependence: Findings from the Global Burden of Disease Study 2010. Reduction in cerebral perfusion after heroin administration: a resting state arterial spin labeling study. Association of frontal gray matter volume and cerebral perfusion in heroin addiction: A multimodal neuroimaging study. Sustained effects of ecstasy on the human brain: a prospective neuroimaging study in novel users. Abnormal structure of frontostriatal brain systems is associated with aspects of impulsivity and compulsivity in cocaine dependence. Meta-analysis of structural brain abnormalities associated with stimulant drug dependence and neuroimaging of addiction vulnerability and resilience. Prescription opioid related misuse, harms, diversion and interventions in Canada: a review. The role of guanfacine as a therapeutic agent to address stress-related pathophysiology in cocaine-dependent individuals.
Order detrol 1 mg online
A low resting blood pressure and orthostatic hypotension is common following cervical and high thoracic injuries medicine you can order online purchase generic detrol pills. It is possible that there is excessive pooling of blood in the viscera and organs secondary to a lack of a reflex vasoconstrictor activity from an ineffective baroreceptor response. Furthermore, with the absence of muscular activity in the lower extremity, there is less recirculation of blood in the venous pool. Additional explanations include reduced plasma volumes from hyponatremia and a cardiac deconditioned patient. Pressors should be used with invasive monitoring such as an arterial line and central venous catheters to allow for accurate readings. It can counteract hypotension and bradycardia by increasing heart rate and contractility, thus increasing cardiac output. With a lack of -adrenergic activity, it can potentially cause reflex bradycardia due to increased end-systolic volume. Patients being treated with phenylephrine may have a difficult time with fluid resuscitation because of the increased partition coefficient of intravascular volume. Norepinephrine is a more logical choice than phenylephrine because of its combined - and -adrenergic agonist properties. Norepinephrine has some inotropic activity to counteract hypotension and bradycardia. Epinephrine is used in refractory cases because of its potent effects in causing renal, splanchnic, and peripheral ischemia. Milrinone and dobutamine can be used to promote cardiac output, but their vasodilatory effects make them less than ideal agents for treating hypotension. The innervation of the diaphragm from the phrenic nerve is supplied by C3, C4, and C5. Patients with injuries between C3 and C5 may need initial ventilatory support, but as inflammation subsides in the cord, they may regain ventilatory strength and have effective recruitment of accessory muscles. The authors attributed hypoxemia (Pao2 <80 mm Hg) to a ventilation/perfusion mismatch. Thus, additional complications such as retained secretions, atelectasis, and pneumonia occur. Complicating factors in the treatment of respiratory problems stem from pulmonary and fat emboli, which can contribute to poor respiratory function. Pulmonary edema can occur from fluid overload; other less common causes include cardiogenic failure and pulmonary sources such as acute respiratory distress syndrome, infection, and trauma. Aggressive measures taken by the respiratory therapist have been shown to decrease the incidence of pneumonia and bronchoscopy use in the acute period. Some clinicians have even advocated early fiberoptic bronchoscopy and bronchial lavage to promote clearance of secretions (McMichan et al. Intrapulmonary percussive ventilation is a device that delivers high-frequency pulsations to loosen secretions and provide aerosolized medications to the lungs. Manually assisted coughing with a provider or via a device can clear bronchopulmonary secretions. Although suctioning is widely used and a mainstay of treatment, it can complicate matters by causing hypoxia, hypotension, infection, tracheal mucus drainage, vagus nerve Spinal Cord Trauma 893 stimulation, and increased mucus production. Pneumonia is a common complication related to the use of mechanical ventilation, with a risk of 1% to 3% per day of mechanical ventilation (Ball, 2001). The culprits of ventilatorassociated pneumonia occurring within the first 4 days are usually Haemophilus influenzae and Staphylococcus pneumoniae. Only when Pseudomonas aeruginosa is suspected should double coverage with antipseudomonal -lactam agents and aminoglycosides be considered. Prevention of aspiration and monitoring for its effects are essential for optimal care. Patients on tube feeds require monitoring of their gastric residual content after feeding. Respiratory failure is defined as a Pco2 over 50 mm Hg or Po2 less than 50 mm Hg on room air, or the requirement of ventilatory support in the setting of a high cervical injury. Patients with injuries in the high cervical cord may suffer neurological deterioration in subsequent days as the injury ascends superiorly in the cord. There is no standard protocol in providing ventilatory support to this group of patients, but simple principles can be used. Patients with high cervical injuries will typically need full ventilatory support with controlled mechanical ventilation. They do not require controlled ventilatory settings that promote ventilator dyssynchrony. Instead, they can benefit from pressure support modes to reduce ventilation/perfusion mismatches. Typically, tidal volume averages no higher than 6 to 8 mL/kg are used to avoid barotrauma, but one study suggested that tidal volumes as high as 20 mL/kg are needed to avoid atelectasis and prevent prolonged weaning times (Peterson et al. Regardless, tidal volumes can be increased in a manner to resolve atelectasis on chest X-ray. Patients requiring long-term ventilatory support may need a tracheostomy to avoid subglottic stenosis and sinusitis. Tracheostomy is easier to tolerate, facilitates improved pulmonary hygiene, produces less dead space and less airway resistance, and creates more favorable conditions for weaning. In the event anterior cervical surgery is performed, a time period of 2 weeks between surgery and tracheostomy placement is suggested. MedicalManagement Secondary injuries that occur in the spinal cord lead to deleterious and unwanted permanent damage. Steroids have been studied extensively as pharmacotherapy to hinder unwanted sequelae. Early animal models suggested benefit in impeding secondary injury, and this has translated into clinical studies in humans to assess steroid efficacy and safety. There have been at least four prospective randomized trials studying steroid effects, with great controversy in interpretation of the methods and results from these studies. One group received 100 mg of methylprednisolone followed by 25 mg every 6 hours for 10 days. Patients were followed up to 1 year after treatment, and results failed to show any significant difference between the two arms despite lacking a placebo. Patients receiving methylprednisolone before 8 hours after injury were separated from patients receiving treatment after 8 hours following their injury. Furthermore, they pointed out that patients treated with methylprednisolone after 8 hours did significantly worse than the placebo group. The original author performed an ad hoc subgroup analysis to support his conclusions (Bracken et al. Although the entire patient sample consisted of 487 patients, this study showed encouraging results from a subgroup of patients receiving treatment within 8 hours of injury. Since that time, there have been many critical analyses of the methods, statistical analysis, and scientific interpretation of the study. One of the most critical arguments stems from the lack of functional measures for assessing outcome. Independent chart analysis shows that the placebo group treated within 8 hours of injury had similar recovery patterns to the corresponding methylprednisolone group for the first 6 weeks. Most clinicians feel that incomplete injuries that show functional improvement at 6 months continue an ongoing trend of recovery. Chart analysis also showed that the placebo group treated within 8 hours of injury did worse than the group treated with placebo 8 hours after injury. In addition, the placebo group treated after 8 hours from the onset of injury had similar results to the methylprednisolone group treated within 8 hours of the injury. The study lacked any information regarding the timing or type of surgical interventions that were performed for these patients. Statistical tools have been criticized as being excessive, confusing, and difficult to replicate by professional statisticians. Furthermore, data from this study have never been made available for independent review. An added treatment arm received 48 hours of tirilazad, a medication with antioxidant properties. The authors noted neurological improvement at the 6-week and 6-month postinjury period for the 48-hour methylprednisolone group if medication was given between 3 and 8 hours post injury.
Order detrol 1mg without prescription
Parvovirus B19 infections have been described as the cause or trigger of various autoimmune disorders that include necrotizing vasculitis resembling polyarteritis or Wegener granulomatosis and in association with meningoencephalitis in immune reconstitution inflammatory syndromes (Nolan et al symptoms in early pregnancy purchase detrol on line amex. Neurological manifestations have included encephalitis, chorea, stroke, optic neuropathy abnormal pupillary reflexes, brachial plexitis, and autonomic, sensory, or motor neuropathies and recurrent paresthesias. They can be subgrouped into the polioviruses, coxsackieviruses A and B, echoviruses, and the newer sequentially numbered enteroviruses. Collectively, the enteroviruses are the leading identified causes of viral meningitis, accounting for over 80% of cases in some series. Other severe neurological syndromes including encephalitis, brainstem encephalitis and acute anterior poliomyelitis are also associated with several of these agents. Poliovirus Poliovirus is transmitted by fecal-oral contact and, during epidemics, also by pharyngeal spread. All can cause paralytic disease through destruction of motor neurons in the spinal cord and brainstem. Countries reporting cases included Somalia (193), Pakistan (93), Nigeria (53), Syria (24), Kenya (14), Afghanistan (14), Ethiopia (9) and Cameroon (4). Clinically apparent infection with poliovirus results in aseptic meningitis (8% of cases) or paralytic illness (1% of all cases). A 7- to 14-day incubation period is followed by headache, fever, signs of meningeal irritation, drowsiness, and seizures in infants. Asymmetrical flaccid weakness of limbs, diaphragm, or cranial nerve-innervated muscles develops within days and progresses, on average, for 3 to 5 days. Approximately one-quarter of polio patients develop an exacerbation of existing or new progressive lower motor neuron weakness 30 to 40 years after acute polio ("the postpolio syndrome"). Atrophy, fasciculations, and electromyographic evidence of active denervation are found in involved muscle groups. Diagnosis depends on the documentation of antecedent poliomyelitis and the exclusion of other new causes of lower motor neuron syndromes. Electrophysiology suggests that new weakness likely results from ongoing denervation that exceeds compensatory reinnervation. The exact cause of the syndrome remains uncertain; both immunemediated processes and chronic persistent viral infection have been speculated to be potential triggers. No specific therapy has been shown to be of proven benefit, although patients may respond to a carefully designed program of physical therapy and the use of orthoses and assistive devices (Gonzalez et al. Treatment of poliomyelitis is supportive, with particular attention to ventilatory assistance. Mortality from paralytic poliomyelitis is less than 10%, but bulbar forms have a poorer prognosis, and mortality may approach 50%. There have been no cases of polio caused by wild-type viruses in the United States since 1979, and none in the Western Hemisphere since 1991. For this reason, the Advisory Committee on Immunization Practices recommended in 2000 that the inactivated (Salk, intramuscular) polio vaccine replace the live attenuated (Sabin, oral) vaccine in the United States for the entire primary immunization series in the first year of life, as well as the booster dose prior to school entry. In areas of the world in which poliovirus is still endemic, primary immunization is still carried out with trivalent live attenuated (Sabin, oral) vaccine, because the mucosal immunity conferred outweighs the small risk of reversion to virulence. Inactivated polio vaccine should always be used for vaccination of persons with immunodeficiency diseases, in whom the risk of vaccine-associated paralytic polio from the live attenuated vaccine strain is high. Vaccine-related cases of paralytic polio have included infants with unrecognized immunodeficiency who have received their first oral polio vaccine dose and immunocompromised patients who have been in contact with recipients of live attenuated oral polio vaccine. In neonates, encephalitis is generally part of an overwhelming sepsis-like illness with up to 10% mortality. Infection of hypogammaglobulinemic patients commonly leads to progressive meningoencephalitis. Certain strains have also been associated with an acute motor neuron disease in association with epidemic hemorrhagic conjunctivitis. Nonpolio enteroviruses are the most common cause of viral meningitis in adult and pediatric populations (Kupila et al. Outbreaks tend to cluster in the late summer and early fall and may be associated with Viral Encephalitis and Meningitis 1135. In June 2003, an outbreak of human monkeypox transmitted from infected exotic pets was identified in the midwestern United States. The index animal source was imported wild rodents from Africa, where the disease is endemic (Reed et al. Human monkeypox was first identified in Zaire, now the Democratic Republic of Congo, in 1970 toward the end of smallpox eradication efforts in Africa. In western and central African countries, it continues to produce sporadic cases clinically similar to smallpox. The 37 confirmed human infections in the June 2003 outbreak represented the first time human monkeypox infection was documented in the Western Hemisphere (Reed et al. Cidofovir, other selective antipoxvirus drugs, and vaccinia immune globulin are investigational treatments. Smallpox vaccine protects against monkeypox both by preventing disease and by decreasing disease severity (Sejvar et al. For both monkeypox and smallpox, vaccination within 3 days of exposure lessens the severity of symptoms in the majority of individuals. Ultimately, the cases resulted in an importation ban and limitations on movement and sale of African rodents in the United States and restrictions on wild release of these species and prairie dog pets. Smallpox and Smallpox Vaccination There are two forms of smallpox, variola major and variola minor, with differing outcomes. Mortality from variola major has been estimated at 30%, and from variola minor approximately 1%. Neurological complications of acute smallpox are uncommon but include stupor, coma, seizure, headache, hemiparesis, incontinence, or flaccid paralysis (Boos and Davis, 2003). The world was declared free of smallpox infection in 1980, but the United States reinstated vaccination against smallpox among military personnel in 2002 and among selected civilian groups in January 2003. Vaccination against smallpox is by inoculation with a preparation of vaccinia, a relatively benign orthopoxvirus. Historically, routine smallpox vaccinations have been 90% effective in preventing smallpox and more than 99% effective in preventing fatalities (Sejvar et al. After primary vaccination, reported rates vary from 1 in 4000 to 1 in 80,000, and after revaccination, from 1 in 50,000 to 1 in 450,000. It is hoped that newer vaccines produced in cell culture will provide desired immunity with fewer complications (Johnson, 2003; Sejvar, 2011). Evidence regarding safety of vaccination of individuals with known neurological illness has been limited (summarized in Abrahams and Kaufman, 2004). In neonates, meningoencephalitis is generally a component of an overwhelming sepsis-like illness with up to 10% mortality. These are highly contagious viruses for which there is no specific antiviral treatment, underscoring the importance of surveillance, public health measures, and sanitation in limiting disease. The most common neuroinvasive infections include a relatively benign aseptic meningitis, and a severe brainstem encephalitis (rhombencephalitis). No specific therapy is available although patients with severe neurological illness have been treated with intravenous immunoglobulin. Arboviruses the term arbovirus (arthropod-borne virus) is a general term for viruses transmitted to humans by mosquito and tick (arthropod) vectors. Arboviruses exist in nature in complex cycles involving birds and mammals that serve as viral reservoirs and amplifying hosts. When transmitted to humans, arboviruses can cause fever, headache, meningitis, encephalitis, and myelitis. Arboviruses are divided between four taxonomic families: togaviruses (alphaviruses), flaviviridae (flaviviruses), reoviruses, and bunyaviruses. Considered together, arboviruses represent the leading cause of encephalitis worldwide. Key features of arboviral infections occurring in North America are summarized in Table 78. In New York in 1999, a reported 59 people were hospitalized with encephalitis or meningitis in late summer, with seven resultant fatalities (Nash et al. Transmission occurs overwhelmingly as the result of the bite of an infected mosquito; however, person-to-person transmission through organ transplantation, blood and blood product transfusion, and intrauterine spread can occur.
Purchase 2 mg detrol fast delivery
Other associated symptoms include priapism medicine man detrol 1mg on line, salivation, sweating, bronchospasm, and bronchorrhea. Treatment begins with careful monitoring of respiration and vital signs and intensive care support if necessary. Muscle spasms may also be treated with slow infusion of calcium gluconate or methocarbamol. Antivenom may be beneficial if administered early, but there are no vigorous clinical trial data. Scorpions Although only a few of the approximately 1,400 scorpion species are of neurological importance, bites by poisonous scorpions are generally more dangerous than spider bites. Scorpion envenomation is second only to snakebites as a public health problem in the tropics and North Africa. In Mexico alone, 100,000 to 200,000 scorpion bites occur annually, resulting in 400 to 1,000 fatalities. In the United States on average, approximately 14,700 scorpion bites with no fatalities are reported annually (Langley, 2008). Small children in particular are prone to developing neurological effects, and as Effects of Toxins and Physical Agents on the Nervous System 1249 many as 80% of bites are symptomatic. Presenting symptoms are highly variable, from local pain (which may be secondary to serotonin found in scorpion stings) to a general state of intoxication. Paresthesias are common and usually experienced around the site of the bite but also may be felt diffusely. Muscle fasciculations, spasms, limb flailing, dysconjugate roving or rotary ocular movements, dysphagia, and other cranial nerve signs are sometimes seen. Symptom control, cardiovascular and respiratory support, and antivenom administration are the mainstays of treatment. Scorpion antivenom appeared to be effective in a small randomized control trial in children with neurotoxicity (Boyer et al. Generalization of this result is uncertain owing to geographical differences in the venom and in the quality and safety of the antivenom. TickParalysis Tick paralysis is caused by tick bites, most notably by Dermacentor and Ixodes species. Most cases in North America appear in the Pacific Northwest, Rocky Mountains, and southeastern United States. Continuing attachment of the tick for 1 or more days is necessary before clinical symptoms appear. Other areas where a tick may go undetected for days are the ear and nose canals and the genital areas. Weakness typically starts in the legs and spreads to the arms and eventually to the bulbar and respiratory muscles. Examination shows limb weakness (most prominent in the legs), hypoactive or unobtainable stretch reflexes, and normal or mildly impaired sensation. Respiratory muscle weakness, if present, manifests as rapid shallow breathing and diminished forced vital capacity. There are reports of atypical presentations such as cranial neuropathy, encephalopathy, autonomic dysfunction, and brachial plexopathy. Electrodiagnostic findings are likely to be nonspecific during the acute phase of the disease, although only limited data are available. One study reported low-amplitude compound muscle action potentials with normal conduction velocities and sensory nerve conduction studies (Vedanarayanan et al. There is a case report of unilateral conduction block at the lower trunk of the brachial plexus from a tick bite in the ipsilateral axilla (Krishnan et al. Approximately 75% of cases occur in children younger than age 6 as a result of accidental ingestion. Adult poisoning may happen when toxic plants or mushrooms are mistaken for edible species. Another category arises with intentional consumption by those seeking drug-induced mood effects from plants such as Jimson weed. Plant identification is difficult and should be left to a trained botanist or mycologist. Common names of plants are inadequate, and botanical names should be used whenever possible. Even without a definitive identification, the history of ingestion and recognition of a characteristic syndrome are often sufficient for a tentative diagnosis. Initial treatment is usually empirical, consisting of gastric lavage or catharsis and supportive measures. With the exception of anticholinergic poisoning, there are few specific antidotes. Omitted are plants that do not have direct toxicity on the nervous system, such as those containing cardiac glycosides, coumarin, oxalates, taxines, andromedotoxin, colchicine, and phytotoxins. Secondary neurological disturbances may result from these toxins because some can cause electrolyte abnormalities, cardiovascular dysfunction, or coagulopathy. Intoxication is not uncommon, with the majority occurring among young people who intentionally ingest the plant for its psychic effects. The chief active ingredient is the alkaloid hyoscyamine, with lesser amounts of atropine and scopolamine. Symptoms of anticholinergic toxicity appear within 30 to 60 minutes after ingestion and often continue for 24 to 48 hours because of delayed gastric motility. The clinical picture can include hyperthermia, delirium, hallucinations, seizures, and coma. Autonomic disturbances such as mydriasis, cycloplegia, tachycardia, dry mouth, and urinary retention are often present. Treatment includes gastrointestinal decontamination with or without the induction of emesis. Supportive measures and symptom relief should be provided, but physostigmine should be reserved for severe or lifethreatening intoxications. PoisonHemlock the dangers of ingesting poison hemlock (Conium maculata) have been known since ancient times. The Old Testament describes rhabdomyolysis in Israelites who ate quail fed on hemlock (coturnism). The highest concentration of toxin is in the root of this plant that may be mistaken for wild carrots. In severe cases, a depressant phase may then ensue, presumably secondary to acetylcholine receptor depolarization blockade. WaterHemlock Water hemlock (Cicuta maculata) is a highly toxic plant found primarily in wet, swampy areas and is sometimes mistakenly ingested as wild parsnips or artichokes. Symptoms consist of initial gastrointestinal effects (abdominal pain, salivation, and diarrhea) followed by generalized convulsions, obtundation, and coma. Mortality is secondary to refractory status epilepticus; seizures are treated with standard protocols. Mayapple (Podophyllum peltatum), widely used in Chinese herbal medicine, is potentially neurotoxic. ExcitatoryAminoAcids Various Lathyrus species, including Lathyrus sativus (chickling pea), Lathrus clymenum (Spanish vetch), and Lathrus cicera (flat-podded pea), are responsible for lathyrism. These hardy plants are an important part of the diet of people in the Indian subcontinent, Africa, China, and some parts of Europe. Epidemics of lathyrism often coincide with periods of famine or war, probably a result of excessive dietary dependency on these legumes. More commonly used is a mouse bioassay employed to monitor commercial shellfish production in many parts of the world. A mouse unit is the minimum amount needed to produce death of a mouse in 15 minutes. Nerve conduction studies may show reduced amplitude of the sensory and motor-evoked responses and prolonged latencies with slowed nerve conduction velocities. Puffer fish (family Tetraodontidae) have a worldwide distribution in both fresh and salt waters but are most commonly found in Japan and China.
Cheap detrol 4 mg otc
Surgery and cardiac catheterization can disrupt the endothelium and lead to thrombosis treatment upper respiratory infection purchase discount detrol. An abnormal heart valve can serve as a nidus for bacterial or fungal vegetations that may cause cardioembolic stroke. Chronic hypoxemia in severe cases of congenital heart disease may lead to polycythemia, and the increased blood viscosity may promote thrombosis. Aortic coarctation may be complicated by infective endarteritis or ischemic or hemorrhagic strokes, including brain aneurysms. Hematological Any hematological disorder that disrupts coagulation can place a child at risk for hemorrhagic stroke. Newborns have lower levels of coagulation factors and have a drop in the vitamin K-dependent factors in the first days of life. Bleeding due to vitamin K deficiency was more common before intramuscular or oral administration to neonates became widespread; Cornelissen and colleagues (1996) found that administering vitamin K lowered the incidence of vitamin K deficiency bleeding from 7 to 1. However, late-onset vitamin K deficiency bleeding can occur in children with undiagnosed cholestatic jaundice who received oral vitamin K and are exclusively breastfed, because they cannot absorb the vitamin, and breast milk is low in vitamin K (Ijland et al. Schulte and colleagues (2014) reported a rise in late-presentation vitamin K deficiency bleeding in Tennessee because parents were refusing vitamin K, believing it was unnecessary or that the vitamin K injection included "toxins. Intracranial hemorrhage is the most common cause of death from bleeding in patients with hemophilia; the site of intracranial hemorrhage can be epidural, subdural, or intraparenchymal. A deficiency or imbalance of factors involved in regulating coagulation may place the child at risk for thrombosis. Pediatric ischemic stroke has been associated with iron-deficiency anemia (Maguire et al. Abnormalities of blood cells or blood cell concentration may place the child at risk for hemorrhagic or ischemic stroke. Low platelet count due to autoimmune thrombocytopenia or bone marrow suppression leads to hemorrhage. Several authors have noted the presence of multiple prothrombotic abnormalities in some children with ischemic stroke (Kenet et al. Children with congenital heart disease or leukemia may be at higher risk for developing thrombotic complications during hospitalization if they also have a prothrombotic abnormality. Subdural hemorrhages, subarachnoid hemorrhages, and ischemic infarctions occur in head injury. Ascertaining the cause of the trauma is important; at one pediatric trauma center, the mortality rate for nonaccidental trauma was 9. Bony abnormalities of the vertebrae or abnormalities of vessel walls due to collagen-vascular disease or metabolic disease may predispose to cervicocephalic arterial dissection after mild trauma. Arterial dissection may be idiopathic in otherwise apparently normal children (Rafay et al. A prothrombotic state associated with trauma can promote thrombosis and worsen outcome; trauma patients who go into disseminated intravascular coagulation have worse outcomes than those who do not. In neonates, compression of the sagittal sinus due to head position has been associated with cerebral sinovenous thrombosis; changing head position or minimizing compression with a specialized pillow may improve venous flow (Tan et al. VascularMalformations/Vasculopathy/Migraine As discussed previously, vascular malformations may present with intracerebral hemorrhage, and resulting vasospasm may lead to ischemic infarction. Arterial abnormalities such as large-artery stenosis are common in otherwise healthy children with arterial ischemic stroke (Ganesan et al. At least 10% of hemorrhagic strokes and most subarachnoid hemorrhages in children are caused by ruptured aneurysms (Jordan et al. Moyamoya is a rare, chronic, progressive steno-occlusive intracranial vasculopathy involving the distal supraclinoid internal carotid artery and the proximal anterior and middle cerebral arteries, and is associated with the formation of an abnormal vascular network at the base of the brain resembling a "puff of smoke" on angiography. Moyamoya disease has a high prevalence in Japan, Korea, and China but has been reported worldwide (Han et al. Children usually present with recurrent transient ischemic attacks or strokes, headaches, seizures, or movement disorders. Adults may present with intracranial hemorrhage, including subarachnoid hemorrhage, subependymal hemorrhage, or intraventricular hemorrhage. There are more frequently reported cases of less virulent vasculopathies in children, often occurring after varicella infection, which respond to aspirin alone and do not require immune suppression (Chabrier et al. Childhood stroke can be a first manifestation of Takayasu arteritis, an inflammatory largevessel vasculitis that affects the aorta and its branches (Brunner et al. A growing body of literature exists examining the role of inflammatory factors in stroke in children and in adults. Although true migrainous infarctions are rare, migraine is associated with a twofold increased risk of ischemic stroke. While migraine has been associated with childhood stroke in large studies (Gioia et al. Infection the consequences of bacterial meningitis are disseminated intravascular coagulopathy and vascular inflammation, and subsequent arterial or venous thrombosis and infarction. Other cerebrovascular complications of meningitis include vasculitis, vasospasm, intracranial aneurysm formation, and rarely subarachnoid hemorrhage. Group B streptococcal meningitis is an important cause of stroke in neonates and transmitted vertically from the mother or horizontally by nursery staff. During the first 2 months of life, infants are susceptible to bacteria found in maternal flora or in the local environment, including group B Streptococcus, Gram-negative enteric bacilli, and Listeria monocytogenes. After 2 months of age, Streptococcus pneumoniae and Neisseria meningitides are the most common causes of bacterial meningitis. The institution of Haemophilus influenzae type b vaccination at 2 months of age has led to a dramatic drop in H. Tuberculosis leads to meningitis in 1% to 2% of cases, which may cause vasculitis and infarction (Starke, 1999). Even minor recent infection has been identified as a risk factor for stroke, and may act by inducing an inflammatory prothrombotic state or by causing vascular injury (Hills et al. In some cases, arteriopathy is associated with recent upper respiratory infection (Amlie-Lefond et al. Drugs/Toxins Abuse of illicit drugs is an important cause of ischemic and hemorrhagic strokes in young patients. Maternal use of cocaine may lead to vasospasm and cerebral infarction in the fetus, and use of cocaine by children may lead to intracranial hemorrhage or ischemic stroke. Other drugs such as amphetamines, which lead to sudden increases in blood pressure or vasospasm, also raise the risk of infarction. Homocystinuria may lead to infarction, presumably through elevated homocysteine levels and subsequent vascular injury. Studies vary on the degree of associated risk, and carriers do not always have elevated homocysteine levels at the time of infarction. Fabry disease is an X-linked lysosomal storage disease that causes a deficiency of -galactosidase and resultant accumulation of glycolipids in the endothelial wall. Male patients experience paresthesias of the hands and feet and cardiac abnormalities that can begin in childhood; hypohidrosis and renal dysfunction tend to occur later in the course of the disease (Ries et al. Both male and female heterozygotes are susceptible to cerebral thrombosis, possibly because of an increase in vasoreactivity in damaged vessels or endothelial and leukocyte activation. Males may be more severely affected but rarely show cerebrovascular involvement before age 23 (Schiffmann, 2001). The hyperlipidemias can cause atherosclerotic vascular changes in children similar to those in older adults. One study found that both arterial ischemic stroke and sinovenous thrombosis are more common in boys, with male predominance particularly in cases of stroke caused by traumaassociated arterial dissection (Golomb et al. However, a recent population-based study in England did not find male gender to be a risk factor (Mallick et al. Higher testosterone levels have been associated with increased risk of stroke in boys (Normann et al. Black children appear to be at an increased risk for both ischemic and hemorrhagic stroke which cannot be fully explained by sickle cell disease. Asian ethnicity has been associated with stroke risk in the United Kingdom but not in the United States; differences in the ethnic makeup of the Asian populations between countries may explain some of the difference (Fullerton et al. A study of mortality from childhood stroke in England and Wales from 1921 to 2000 found that boys had a higher mortality rate (Mallick et al. Black children have had higher stroke mortality than white children in the United States.
