
Purchase luvox 100mg without a prescription
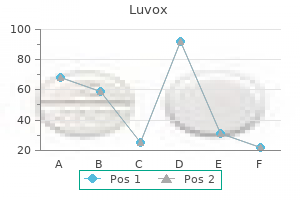
Lack of a high affinity transport system for dopamine in the median eminence and posterior pituitary anxiety bible verses discount 50mg luvox fast delivery. Dopamine transporter immunohistochemistry in median eminence, amygdala, and other areas of the rat brain. Noradrenergic innervation of the rat hypothalamus: Experimental biochemical and electron microscopic studies. Hypothalamic tanycytesmasters and servants of metabolic, neuroendocrine, and neurogenic functions. Central and peripheral catecholamine innervation of the rat intermediate and posterior pituitary lobes. Increase in pituitary dopaminergic receptors after monosodium glutamate treatment. Dopamine in hypophysial portal plasma of the rat during the estrous cycle and throughout pregnancy. Studies on the mechanism of the dopamine-mediated inhibition of prolactin secretion. Dopamine levels in hypophysial stalk blood in the rat are sufficient to inhibit prolactin secretion in vivo. Dopamine in hypophysial stalk blood of the rhesus monkey and its role in regulating prolactin secretion. Concentrations of dopamine and noradrenaline in hypophysial portal blood in the sheep and the rat. Circadian clocks generate self-sustaining, cell-autonomous oscillations with a time period of approximately 24 h. The features of a circadian clock in all organisms include its persistence under constant conditions, an oscillation that is temperature compensated, and an entrainment to external input. The neural circuitry that regulates the circadian rhythms includes the retina, suprachiasmatic nucleus, and the pineal gland. These structures operate under bidirectional neural and hormonal control to and from various organs and affect multiple physiological and endocrine functions. Stress is a state of threatened homeostasis caused by extrinsic adverse forces (stressors) and is counteracted by an intricate repertoire of physiologic and behavioral responses aiming at maintaining/reestablishing the optimal body equilibrium. Obesity and its opposite disorder anorexia are pervasive problems of humans in modern times. There is clearly a need for better understanding of the mechanisms that regulate appetite versus energy expenditure because the balance of the two processes ultimately determine body weight. Within the brain, the hypothalamus serves as a relay station that receives information on the state of energy fluxes by pancreatic, adipose, stomach and intestinal hormones and coordinates endocrine, autonomic, and behavioral responses that regulate feeding behavior and appetite around an optimal set point. More than any other physiological functions, each species has developed specific patterns of reproductive cycles, sexual behavior, as well as length of gestation and lactation, that are best suited for its social structure and living environment. The neuroendocrine system controls and coordinates both the physiological and the behavioral aspects of reproduction. Throughout the 24-h day, the clock regulates many physiological, endocrine, and mental processes, including sleep, body temperature, metabolism, blood pressure, hormone release and alertness. Circadian rhythms are endogenously generated ~24-h biological rhythms that are organized in two levels: a molecular level represented by the clock genes, and a systemic regulatory level represented by the neuroendocrine networks. The circadian oscillation is synchronized by external environmental cycles, primarily the light/dark cycle of the geophysical day and night. External rhythmic events that can synchronize biological rhythms are called zeitgebers or synchronizers. The importance of the circadian rhythm for multiple organisms, from flies to man, was recognized by the granting of the 2017 Noble Prize in Physiology and Medicine to three U. In subsequent years, various proteins that regulate the circadian rhythms in mammals have been isolated and characterized. Although an in-depth discussion on the molecular mechanisms that govern circadian rhythms is beyond the scope of this chapter, the interested reader can find excellent information in two comprehensive reviews [1,2]. The short background information presented below is largely based on those reviews. The molecular mechanism of the endogenous circadian clock in mammals comprises feedback loops of cyclic gene products that apply negative and positive transcriptional regulation of "clock" genes and proteins. The clock genes cycle in opposite phases and define the daily variations in physiological functions that shape the circadian rhythm. Several kinases and phosphatases that regulate the speed, precision, and functions of the circadian clock also contribute to circadian oscillations. Every day, the normal sleep-wake cycle is regulated by the intrinsic clocks that increase the release of melatonin, the "sleep" hormone, in the evening and elevate the serum levels of cortisol, the "stress and alertness" hormone, upon awakening in the morning. The explosion in the use of melatonin to regulate sleep in otherwise healthy individuals has led to the spending of more than $400 million by U. Most commercial products are offered at dosages that can cause blood melatonin levels to rise much above the endogenously produced levels in the body. For melatonin to be helpful, the correct dosage, method, and the time of day it is taken must be appropriate to the sleep problem. Taking it at the "wrong" time of the day may reset the biological clock in an undesirable direction [3]. These changes are driven by interactions between central neural and neuroendocrine control mechanisms, intrinsic peripheral clocks in different organs, local cytokines, and circulating hormones. Short-term misalignments between the internal clock and the external environment, as occur following a jetlag, can impose acute disruptive effects on the sleep-wake rhythm. Prolonged or 24:00 Midnight Melatonin Secretion starts Highest body temperature 21:00 20:00 23:00 22:00 1:00 Deepest sleep 2:00 3:00 4:00 Lowest body temperature Highest blood pressure 19:00 18:00 P. Shown are circadian changes in physiological, hormonal, and behavioral parameters. Mammals have peripheral clocks with the capacity to generate endogenous rhythms in nearly all organs and tissues. Under normal conditions, the various peripheral clocks are entrained to the light-dark cycle by an integrated input from the master clock and its associated neuroendocrine networks. Some peripheral clocks can be synchronized by feeding rhythms as the dominant signals. In addition, modulating functions are provided by some hypothalamic nuclei, the striatum, and several circulating hormones. Cones are active at higher light levels (photopic vision), are capable of color vision, and are responsible for high spatial acuity. Ganglion cells collect electrical messages of the visual signals from the two layers of neurons and serve as the final neuronal output of the retina [5]. The mammalian retina is not only a light-sensing tissue that conveys photic information to the brain, but it also has an intrinsic circadian system. The retinal cells and pigment epithelium have circadian oscillators that are integrated through neural synapses, electrical coupling (gap junctions), and released neurochemicals. Ganglion cells produce the photopigment melanopsin, which plays a non-image-forming role in the setting of the circadian rhythms. The retina produces its own melatonin that acts as an important local endogenous circadian signal. These mice had a significant disruption in their circadian rhythm, contrast sensitivity and visual acuity, all of which were rescued by the delivery of D1R or D4R agonists. There is also evidence for functional dopaminergic systems in circadian-driven brain sites in primates [12]. In both baboons and humans, in situ hybridization has revealed differential expression of D1R and D5R in several hypothalamic nuclei. Dietary tryptophan is absorbed into the bloodstream from the gut and is circulated through the body. Serotonin is the final product of the indoleamine pathway in many brain and peripheral locations, where it functions as a neurotransmitter and/ or a hormone. The indoleamine biosynthetic pathway leading to the production of melatonin from tryptophan via serotonin as an intermediate.
Discount 50mg luvox mastercard
Also anxiety 3000 purchase cheap luvox on line, other features, such as corpora amylacea near a blood vessel are visualized. In the image of the subiculum (Sub), a somewhat larger blood vessel is seen surrounded by corpora amylacea indicated by white (C) resp. A second abnormality is the presence of dysmorphic neurons with abnormal size and morphology of axons and dendrites, as well as increased accumulation of neurofilament proteins. The vast majority of these tumors are so-called "diffuse gliomas" as they show very extensive ("diffuse") growth into the surrounding brain parenchyma. With surgical resection, irradiation, and/or chemotherapy it is impossible to eliminate all glioma cells without serious damage to the brain tissue. As a consequence, so far, patients with a diffuse glioma have a poor prognosis, a situation which strongly contributes to the fact that brain tumor patients experience more years of life lost than patients with any other type of cancer [43, 44]. During brain surgery, however, it is extremely difficult for the neurosurgeon to determine the boundary of the tumor, i. If the neurosurgeon could have histopathological information on the tumor boundaries during brain surgery, then recognition of these tumor boundaries, and with that the surgical resection, could be significantly improved. These cells are specialized in the synthesis of melanin pigments inside membrane-bound organelles, the melanosomes. Along with hemoglobin and carotenoids, melanin is the main pigment responsible for the color variations of our skin and hair. During evolution, human ancestors living in equatorial Africa were probably characterized by light pigmentation of the body, which was, however, covered by dark hair. Folate deficiency has been linked to pregnancy complications and severe fetal abnormalities in neural tube development. In support of this hypothesis, in comparison to lightly pigmented individuals, darkly skinned people show a more acidic pH of the stratum corneum, which is further acidified by the slow and delayed degradation/extrusion of melanin. It has been also theorized that the melanocytes of darkly skinned people secrete paracrine mediators able to stimulate epidermal differentiation and the production of lipids positively involved in the constitution of the skin barrier, thus efficiently improving barrier competence in dark skin. Moreover, a pigmented epidermis displays enhanced antimicrobial defense, a property strictly co-regulated and interconnected with permeability barrier homeostasis. Differentiated melanocytes display a low growth rate and elevated resistance to apoptosis as a result of their high intrinsic expression of the antiapoptotic protein Bcl-2. Differences in ethnic color are rather related to the type and quantity of produced melanin and to its transfer, distribution pattern, and degradation into neighboring keratinocytes. There are two main types of melanin synthesized through the multistep process of melanogenesis: red/yellow pheomelanin and brown/black or dark eumelanin, which are both produced in different ratios. In light-skinned people, the predominant melanin type is usually pheomelanin, the melanosomes are smaller and less condensed, and they are transferred to keratinocytes grouped in membranebound clusters containing four to eight melanosomes. Melanin synthesis occurs within specialized membrane-bound organelles, the melanosomes, through four stages of maturation. Melanin arrangement inside melanosomes guarantees the protection of other cell compartments from oxidative stress produced during pigment synthesis and, at the same time, condensates melanin for its transfer to kertinocytes. They are deprived of tyrosinase activity and are transferred along dendrites and then to the surrounding keratinocytes. In dark-skinned people (left panel, a), melanosomes are large, abundant, and transferred to keratinocytes as singly packaged organelles. In light-skinned individuals (right panel, b), melanosomes are small, less matured, and transferred to keratinocytes as clusters in membrane-bound organelles, encompassing more melanosomes. The cooperation of these three enzymes leads to the production of two main melanin-type biopolymers: red-yellow pheomelanin and brownblack eumelanin. Melanogenic enzyme functionality and substrate obtainability drive the type of melanins produced. They are hence oxidized and polymerize, producing pheomelanins via benzothiazine intermediates. Pheomelanin, which is higher in people with fair skin and red hair, generates an increased amount of free radicals, thus inducing more harmful effects. Several genes involved in melanin synthesis and melanosome formation, as well as in pigment trafficking inside melanocytes and melanin transfer to keratinocytes, decisively influence the variations in pigmentation observed among human populations. Multiple genes are known to directly or indirectly impact pigmentation, and mutations of many of these genes may lead to pigmentary disorders, either as hyper- or hypopigmentation. Melanosome intracellular movement occurs both antero- and retrogradely, toward microtubule proteins belonging to the kinesin and dynein/dynein-associated protein superfamilies, respectively. While maturing, melanosomes acquire the structural and enzymatic components necessary to produce melanin. Two major melanin forms are synthesized within melanosomes: red-yellow pheomelanin and brown-black eumelanin. Based on in vitro and ultrastructural studies, different models of melanosome intercellular transfer, which are not incompatible with each other, have been hypothesized: (i) Exocytosis of naked melanin (also referred to as melanocore) into the extracellular areas through the fusion of the melanocyte plasma- and melanosome membranes. The pigment particles are then taken up by the surrounding keratinocytes via phagocytosis. Subsequent fusion of lysosomes and dissolution of the melanosome membrane lead to the formation of phagolysosomes. The latter are then gradually degraded in vesicles containing melanin granules spread in the cytoplasm of keratinocytes. Filopodial phagocytosis, in which melanocyte filopodia containing melanosomes are phagocitosed by keratinocytes, has been also reported. Melanosome transfer by the fusion model has been also suggested to occur via melanocyte filopodia united with keratinocyte plasma membrane to form a tubular structure of actin filaments. The expression of specific receptors on keratinocytes, but not on melanocytes, positively controls melanosome internalization. The cleavage discloses tethered ligands that bind the receptor, thus inducing its activation. Binding to their specific receptors, keratinocytederived mediators activate intracellular signaling pathways controlling the growth, survival, differentiation, and pigment synthesis of melanocytic cells. Differently, the action of an antagonist, for example, Agouti signaling protein, may lead to the synthesis of pheomelanin. Melanocyte-fibroblast interactions Dermal fibroblasts play an active role in modulating melanocyte homeostasis through the secretion of growth factors and cytokines, which act both in a synergistic and sometimes overlapping fashion with respect to the keratinocyte-mediated signaling network. Additionally, some paracrine messengers released by fibroblasts can indirectly target melanocyte functions, inducing the production of biofactors able to either block or stimulate melanocyte activities in keratinocytes. Similar to growth factors and cytokines synthesized by keratinocytes, in this intricate epithelial-mesenchymal interaction, some fibroblastic bioactive messengers act as melanocyte activators, others as inhibitors. This site-specific fibroblast-derived factor exerts a dual action: on the one hand, it suppresses melanocyte growth and melanin synthesis, and on the other, it acts on keratinocytes, decreasing the expression of the proteinase-activated receptor 2 actively involved in the process of melanosome transfer. However, contradictory effects are reported in the literature, showing both positive and negative regulatory abilities of vascular endothelial cells on the process of pigmentation. All these influences create an intricate and finely balanced signaling crosstalk, in which melanocytes exert a central and dynamic role in controlling the equilibrium and protection of the skin in its entirety. On the other hand, the network of bioactive messengers acts bidirectionally to and from the melanocytes toward the other dermal and epidermal cells. As a result, this mutual interaction confers on the whole cutaneous microenvironment the ability to strongly influence melanocytes themselves and therefore to contribute to both constitutive pigmentation and, whenever altered, to the onset and persistence of pigmentary disorders. Dynamic interplays among extracellular matrix proteins, cells, and bioactive mediators are also critical regulators of melanocyte activities and cutaneous pigmentation. Consequently, the uncontrolled propagation of growth factors and cytokines among the epidermis and dermis may inappropriately activate melanocytes. Re-appraisal of current theories for the development and loss of epidermal pigmentation in hominins and modern humans. Basis for the gain and subsequent dilution of epidermal pigmentation during human evolution: the barrier and metabolic conservation hypotheses revisited. The patterns of melanosome distribution in keratinocytes of human skin as one determining factor of skin colour.
Buy generic luvox 100 mg online
The use of botanical extracts as topical skin-lightening agents for the improvement of skin pigmentation disorders anxiety free buy discount luvox 100 mg on-line. Leucoderma after use of a skin-lightening cream containing kojic dipalmitate, liquorice root extract and Mitracarpus scaber extract. Depigmentation of oral mucosa as the earliest possible manifestation of oral submucous fibrosis in Sri Lankan preschool children. Guttate hypomelanosis 167 did not observe a decreased number or melanosomes in the melanocytes, but rather a decreased number of melanosomes in keratinocytes, suggesting an error in melanosome uptake from keratinocytes as opposed to decreased melanosome production. Patterns that were described by the authors as "amoeboid," "feathery," "petaloid," and "nebuloid," as well as combinations of these patterns, were the most frequently observed. These include vitiligo (early stages), pityriasis versicolor, pityriasis alba, hypopigmented flat warts, and post-inflammation hypomelanosis. Patients reported a better outcome and higher repigmentation on the tacrolimus-treated side compared to the placebo treated side after 6 months of treatment. Possible adverse events included irritation and transient post-inflammatory hyperpigmentation. No specific dermoscopic features can be identified besides a "nebuloid/cloudy"-type appearance. Assessment was performed with colorimetry, digital photography, and digital dermoscopy at weeks 0, 4, 8, 12, and 16. However, it is strongly recommended that a well-trained health care professional perform the treatment, as there is always the possibility of scarring if lesions are overtreated. The condition was later described by other investigators as well, and they assigned several terminologies to it, including "cutis trunci variata," "Creole dyschromia," and "idiopathic multiple large macule hypomelanosis. Overall, the dermis appears normal, while a decrease in melanin content in the epidermis, compared with that in normal adjacent skin, may be present. A distinction can be made from other hypopigmented macular diseases of the skin based on very subtle differences. The hands of the patients are never affected by the condition, while lesions on the face are considered extremely uncommon. This theory was considered because the condition is commonly seen in members of the same family; however, there are very few scientific data to support it. There are no specific dermoscopic characteristics, and lesions present as asymmetrical, ill-defined whitish macules. Progressive macular hypopigmentation can be differentiated from several of these conditions due to the lack of pruritus and desquamation. In addition, in cases of post-inflammatory hypopigmentation, a positive history for an inflammatory dermatosis precedes the appearance of lesions. Patients received the treatments for 14 weeks, followed by a 12-week follow-up period to evaluate repigmentation rates. The antimicrobial combination regimen showed strong superiority to the anti-inflammatory combination regimen (photometric measurements p = 0. Prognosis the prognosis of the condition remains uncertain, with various authors reporting mixed data. Idiopathic guttate hypomelanosis: A review of its etiology, pathogenesis, findings, and treatments. Clinical features of idiopathic guttate hypomelanosis in 646 subjects and association with other aspects of photoaging. Comprehensive understanding of idiopathic guttate hypomelanosis: Clinical and histopathological correlation. Idiopathic guttate hypomelanosis-like lesions in patients with mycosis fungoides: A new adverse effect of phototherapy. Melanocyte abnormalities and senescence in the pathogenesis of idiopathic guttate hypomelanosis. Hypopigmented macules of photodamaged skin and their treatment with topical tretinoin. Treatment of idiopathic guttate hypomelanosis with liquid nitrogen: Light and electron microscopic studies. Dermoscopic evaluation of idiopathic guttate hypomelanosis: A preliminary observation. Topical tacrolimus significantly promotes repigmentation in idiopathic guttate hypomelanosis: A double-blind, randomized, placebo-controlled study. Activation of melanocytes in idiopathic guttate hypomelanosis after 5-fluorouracil infusion using a tattoo machine: Preliminary analysis of a randomized, split-body, single blinded, placebo controlled clinical trial. Evaluation of placental extracts as an adjuvant therapy to phenol in treatment of idiopathic guttate hypomelanolsis. The effect of fractional carbon dioxide lasers on idiopathic guttate hypomelanosis: A preliminary study. Treatment of idiopathic guttate hypomelanosis with fractional carbon dioxide lasers. Non-ablative fractional photothermolysis in treatment of idiopathic guttate hypomelanosis. Treatment of idiopathic guttate hypomelanosis by localized superficial dermabrasion. Progressive macular hypomelanosis of the trunk: Primary acquired hypopigmentation. Propionibacterium acnes and the pathogenesis of progressive macular hypomelanosis. Progressive macular hypomelanosis is associated with a putative Propionibacterium species. The use of lymecycline and benzoyl peroxide for the treatment of progressive macular hypomelanosis: A prospective study. Ultrastructural findings in progressive macular hypomelanosis indicate decreased melanin production. Clinical, pathologic, and ultrastructural studies of progressive macular hypomelanosis. Progressive macular hypomelanosis: An epidemiological study and therapeutic response to phototherapy. Progressive macular hypomelanosis showing excellent response to oral isotretinoin. Unsuccessful treatment of progressive macular hypomelanosis with oral isotretinoin. When capacity is breached, patients must be transferred safely to other treatment facilities. Sustained capacity: the maximum capacity that a burn center can sustain over a longer time without lowering treatment quality. Burn capacity of a health system: the total capacity of burns that can be treated in a national health system. This capacity should be known; it should take into account the various requirements of burn treatment, such as the number of victims needing intensive care. The average capacity utilization over the year is part of resource planning for a health system. Time to establish surge capacity: how much time a burn center needs to rise to maximum surge capacity. Such teams can be formed only when burn experts are numerous enough and not already engaged in other aspects of disaster response. Technical relief: the general "civil defense" functions required to support disaster response. In Germany, these functions are provided by the Bundesanstalt Technisches Hilfswerk and include lighting, debris removal, search and rescue, flood mitigation, electricity, water supply, sewage disposal, catering, command center support, communications, logistics, equipment repair, and transportation of supplies. The Historical Record Even with the best preparation, a disaster remains a disaster for a certain period; the goal is to minimize that period. Although retrospectively correcting problems is impossible, lessons learned from the past should be applied to the future. Communication in the hospital also was problematic: Mobile phones had no reception, there was no time to read electronic texts, and land lines were not mobile.
Generic 50mg luvox with amex
Burns needing treatment for shock or intubation should be classified for urgent treatment anxiety eating buy generic luvox 50mg on line. Because of the need to resuscitate as soon as possible, resuscitation should begin here! Tags are used not only to indicate triage category but also to provide each patient with a unique number. The tags must not be removed until all the following have occurred: hospital arrival, identifying the patient, and registering the tag number and treatment data. If the number of patients exceeds the surge capacity of the local burn center but can be handled by the national system of burn centers, then initial care must occur in local trauma centers or burn centers. If the number of victims exceeds national resources, international resources must be evaluated to determine which patients are to be treated in burn centers nationally and which could be evacuated internationally. The preferred approach is one-on-one interviews and small-group sessions, after which the psychosocial specialist decides whether debriefing should be offered. Although minimum standards are rather clear, quality control is sometimes lacking. Klein and associates reported that the most common complications during air transport were loss of venous access and inability to secure an airway. Central disaster management must conduct a general survey of treatment centers to identify survivors and space available in the home area. Patients should be transported if they are stable and the situation in the home area is suitable. Regular follow-ups, surgical interventions, rehabilitation, and psychosocial support must be initiated. These should be long-lasting measures to give the patient a point of care that she or he trusts. The primary shortage in burn beds will be followed by a secondary shortage in rehabilitation centers. Follow-ups must be planned far into the future; projects should be established and funded. Care-physical, psychological, and social- should be given not only to the victims but also to their relatives. Staff in mass casualties have a higher risk of illness than the average population. Contributing factors include the need to make triage decisions, bad information, lack of routine, lack of resources, inability to provide help, and contact with aggressive news media. The formula is not suitable for resuscitation of burned children (weighing <40 kg body weight); for children, a weightbased formula should be used along with a maintenance fluid. Mass casualty events and disasters make it difficult to provide fluid resuscitation at the right time and in sufficient quantities. This mainly reflects concerns about disturbed gastric emptying and impaired peristalsis after the burn injury, exacerbated by the side effects of opioid analgesics. It is a small packet containing glucose, sodium, potassium, chloride, and buffer, with a slightly hypertonic osmolarity of 331 mmol/L when dissolved in water. It was first developed to treat the massive loss of volume and electrolytes in cholera, dysentery, and so on. If patient is intubated and ventilation is disturbed: Check tubus position; exclude pneumothorax; consider thoracic escharotomies and fasciotomies. If perfusion of extremities is disturbed or pressure is high: Check the need for escharotomy and fasciotomy. Delivering small bottles of liquid O2 is logistically difficult; the available capacity is strained by the weight, space, and the need to refill bottles. If electrical power is present, oxygen generators can deliver oxygen with a concentration of 93% or more. With a booster system to provide enough pressure, oxygen generators can be used to refill oxygen tanks. It therefore may require concomitant administration of glycopyrrolate or atropine. S (+) ketamine, with less psychomimetic effect, can be administered at half the dose of the racemate. Acute surgery of wounds on upper and lower limbs and reduction of open fractures can be done under peripheral single-shot regional anesthetic techniques if the region where the block must be performed is clean and not burned. The availability of ventilators and anesthesia machines depends on the scale of disaster. If field hospitals are required, providers must be familiar with the equipment available therein. They are used in the forward deployed medical units in the army but also in civil units like the German Red Cross "ziviles Feldlazarett. For ventilation in a controlled mode, however, they have to be connected to a ventilator. Therefore, training with the devices is difficult and requires connection to the safety and monitoring systems of standard anesthesia machines. Recently, field-deployable versions of standard anesthesia machines were developed and introduced. They are of a robust and lightweight design, are able to operate under extreme temperatures, have extended battery capacities, require little maintenance, and are able to ventilate in different modern ventilation modes. Burn disasters immediately deplete the available stocks and lead to urgent requests to the local blood center. Triaging mass casualties, especially in burn disasters, results in the dissemination of patients to different trauma centers, so that multiple hospital blood banks are involved. High-volume and high-priority requests concentrate in a spiraling sequence in one blood center, which is greatly strained to coordinate the distribution to its hospital blood banks. Supplies are usually sufficient to meet the urgent first requests, but many blood centers hold an average of blood products to meet the regular demand of 1 week or less. Burn disasters are characterized by the urgent need for platelet products and erythrocyte concentrates in the early phase. More often, a blood center acts without information about the disaster and the estimated need for blood products. Initial wound debridement should be thorough and aggressive and should use a surgical antiseptic such as chlorhexidine gluconate solution. Blood supply is mentioned as scarce in the first and prolonged phases of disaster response. Hospitals and burn centers often learn first of an incident through the media or other unofficial channels. When patients arrive tagged or telling certain stories, it indicates a mass casualty event. Measures to establish hospital preparedness should be taken, including checking supplies and the local situation and not allowing staff to go home after shifts until the situation is cleared. Crisis communication is the exchange of information among public authorities, organizations, news media, and affected individuals and groups-before, during, and after a crisis. Satellite Telephone Satellite phones are independent of local infrastructure and can be helpful in cases of uncertain or overloaded infrastructure. However, even a call made from a satellite phone will not go through if the telephone system at the receiving end is not functioning. Electronic News Media these are important in disasters, especially when locales must be evacuated and when staff are needed. Sequential failure of various communication methods was described in many disasters such as Enschede,60,61 London, and Madrid. Information should originate from a desire to be as correct and as complete as possible. The central incident command should appoint spokespersons to provide regular, scheduled press conferences and bulletins.
Diseases
- Vasopressin-resistant diabetes insipidus
- Sternal cleft
- Deafness, isolated, due to mitochondrial transmission
- Thymic epithelial tumor
- Cleft palate
- Eosinophilic cystitis
- MPS III-C
Order 100mg luvox otc
Side-limited illumination can be achieved by placing a miniature mirror at the waveguide end (Zorzos et al anxiety symptoms out of the blue order luvox with visa. Multi-site illumination using a single waveguide is produced by etching multiple apertures and manipulating the coupling strategy. The temporal resolution of the latter approach is inherently higher, but available light power is divided between multiple targets, limiting the number of targets that can be illuminated at a given input power. All strategies based on fiber bundles require surface mounting, cortical excavation, and/or considerable volume of compressed/displaced neuronal tissue. These two approaches for controlling multiple targets represent some of the possibilities for patterned illumination (Emiliani et al. Consequentially, optical fibers tethered to a behaving animal may suffer from decreased transmission efficiency, irreversible physical damage (breakage), restriction of animal movement, or all three. While mechanical compliance can be improved using a rotary joint (optical "commutator"; Gradinaru et al. Compared to optical waveguides, electrical wires provide many more degrees of freedom. In this manner, instead of delivering light from a remote light source via rigid fibers, electricity can be delivered from a remote power source via highly flexible lightweight wires. Moving the light source from the bench to the head is one conceptual leap; the natural next step is to insert the light source into the brain of the animal. In 2013, advances in micromachining techniques enabled the production of miniature light sources, i. Semiconductors typically used include aluminum nitride (AlN), gallium nitride (GaN), indium nitride (InN) and their alloys. Even though the light output at this "sub-threshold" domain (dashed box) is minuscule, it may affect low-light applications. Temperature can be easily controlled on the bench, but is more challenging to stabilize in miniature implanted devices. Nevertheless, experiments with mice implanted chronically with multi-site diode-probe arrays (Stark et al. The only way to circumvent these shortcomings is to remove the tether and provide power to head-mounted light sources by 324 Handbook of Neurophotonics Implant-brain mechanical interaction. A metal tube ("cannula") can be fixed to the skull, through which an optical fiber is inserted at the beginning of every experiment (Aravanis et al. A mating sleeve ("ferrule") can be used to connect two fibers, one fixed inside the brain, the other coupled to an on-bench light source, thus reducing the tissue damage caused by repeated insertions (Sparta et al. A microdrive capable of independently maneuvering multiple devices (optical fibers, diode-tetrode, etc. Instead of a stationary implant secured to the skull, an entire device can be implanted within the parenchyma, permitting movement with the brain rather than with the skull (Jeong et al. A potentially promising third direction for wireless devices is based on biological energy harvesting. Yet, understanding how this happens requires more than simply measuring the end result; neuronal activity must be registered. Electrical recordings enjoy a ground-truth status since they are inherent to neural communication, and indeed, many of the classical electrical recording techniques have been used alongside a separate optical stimulation device. Combining electrical recordings with optical stimulation in an implantable device requires more than a compact mechanical design and an efficient optical interface. The proximity of the light sources and the recording electrodes gives rise to two distinct types of artifacts which resemble spontaneous neural activity (local field potentials and spikes) and hinders the interpretation of the recorded data. First, when light directly hits a metal electrode, a "light artifact" generated by the photovoltaic (Bequerel) effect may arise (Han et al. Optrode constructed by gluing a 200 m diameter optical fiber to a 125 m diameter tungsten electrode (Gradinaru et al. Dual-core fiber, with a hollow core for extracellular recordings produced near a light-propagating optical core (LeChasseur et al. Multi-core, all-polymer flexible fiber, produced with integrating electrode material (Canales et al. Concentric electrode and fiber, produced by coating the tapered tip of an optical fiber with gold film (Zhang et al. This design is of special interest as it allows the same spot to be illuminated by different wavelengths, enabling, for instance, activating and silencing the same cell (Kampasi et al. Multi-electrode (Utah-like) array, containing multiple coaxial optrodes (Kwon et al. Combining optical manipulations with electrophysiologi- cal recordings can give rise to two distinct types of artifacts. Direct illumination (blue line, applied voltage) of metal electrodes can induce large potentials on the recording electrodes (black line, recorded signal; Han et al. Optical Stimulation of Neural Circuits in Freely Moving Animals 327 and Goldschlager, 1996). In essence, pacemakers are wireless stimulators that can operate in a metronomical fashion or in response to an event sensed by the device itself. An equivalent opto-electrical implant, capable of sensing and blocking epileptic seizures (Krook-Magnuson et al. An optical neural interface: in vivo control of rodent motor cortex with integrated fiberoptic and optogenetic technology. Novel interfaces for light directed neuronal stimulation: advances and challenges. Optical dissection of brain circuits with patterned illumination through the phase modulation of light. Photostimulation using caged glutamate reveals functional circuitry in living brain slices. Targeted optogenetic stimulation and recording of neurons in vivo using celltype-specific expression of channelrhodopsin-2. Conformal piezoelectric energy harvesting and storage from motions of the heart, lung, and diaphragm. Imaging large-scale neural activity with cellular resolution in awake, mobile mice. Targeting and readout strategies for fast optical neural control in vitro and in vivo. Spatio-temporal control of neural activity in vivo using fluorescence microendoscopy. Wireless optofluidic systems for programmable in vivo pharmacology and optogenetics. Fiberless multicolor neural optoelectrode with micro-optic assembly of laser diodes, gradientindex lenses and dielectric waveguides, Scientific Reports 6(1), 30961. Optopatcher-an electrode holder for simultaneous intracellular patch-clamp recording and optical manipulation. Review of diverse optical fibers used in biomedical research and clinical practice. Injectable, cellular-scale optoelectronics with applications for wireless optogenetics. Design, fabrication, and packaging of an integrated, wirelessly-powered optrode array for optogenetics application. A microprobe for parallel optical and electrical recordings from single neurons in vivo. Optogenetic manipulation of neural activity in freely moving Caenorhabditis elegans. Remote control of behavior through genetically targeted photostimulation of neurons. Wirelessly powered, fully internal optogenetics for brain, spinal and peripheral circuits in mice. Light activation of channelrhodopsin-2 in excitable cells of Caenorhabditis elegans triggers rapid behavioral responses. A coaxial optrode as multifunction write-read probe for optogenetic studies in non-human primates.
Luvox 50mg without a prescription
However anxiety symptoms yawning order luvox us, presacral neurectomy is an effective additional procedure to conservative surgery to reduce endometriosis-associated midline pain [9]. Among others, the most accepted are an abnormal chronic inflammation and reduced ovarian reserve that affect ovulation and distorted anatomy due to adhesions that affect the tubo-ovarian relationship. It has nonspecific symptoms such as pain and swelling Mode of surgery 61 of infertility, including a male factor, before planning any surgery for endometriosis. However, others authors report that reproductive outcomes have not been shown to be improved by the excision of deeply infiltrating endometriosis. Laparoscopic surgery with histological examination is the gold standard for diagnosis and treatment simultaneously. Both laparoscopy and laparotomy are equally effective for management of endometriosis-associated pain, but laparoscopy has the advantage of less pain, shorter hospital stay, rapid recovery, and better cosmetic outcome. Laparoscopy has the advantage of magnification, especially of difficult to access spaces during surgery. However, it is a compromise on the tactile differentiation of various structures during surgery. Operative rather than diagnostic laparoscopy is more effective in increasing ongoing pregnancy rates, even in mild to moderate endometriosis [19]. Both ablation and excision of peritoneal endometriotic implants to reduce endometriosis-associated pain should be considered [20]. Laparoscopic surgery has a limitation in treatment of moderate to severe endometriosis because of obliteration of surgical planes, deeper implants, and dense adhesions which require expert surgical skills. This system has three stages correlating to three levels of incremental complexity of surgery required. This scale would help triage women to appropriate levels of surgical expertise for laparoscopic surgery. In recurrent endometriosis with infertility, cyst aspiration is recommended when the ovarian reserve is poor. However, the need for conversion to laparotomy, if required, should always be included in the consent for surgery in cases of dense and extensive adhesions that make delineation of anatomy difficult or in cases of suspected or actual inadvertent injury in the case of surgery. Robotic surgery Traditional laparoscopy has gained popularity for the management of this disease but has limitations in the surgical treatment of the most difficult cases of endometriosis. As both experience and technology expand, it has been suggested that the robotic surgery platform enables more complex dissections and may be the ideal modality of the surgical management of deeply infiltrating endometriosis [24]. The aim is to vaporize the endometriotic cyst lining until hemosiderin pigment stained tissue is no longer visible and there is change of color of implants from red to yellowish white [28]. Electrocoagulation using monopolar or bipolar energy sources can be used to ablate endometriotic lesions. However, when using electrocoagulation, the ovary should be cooled frequently with irrigation fluid as tissue damage is deeper [29]. Electrocoagulation using different techniques and electrodes leads to different voltage levels. Tissue damage with electrocoagulation techniques is usually deeper than with laser or plasma energy. The impact of energy on superficial tissue may be visible due to change of color; however, damage to deeper tissue is difficult to assess. Uncontrolled use can lead to damage to primordial follicles and destruction of structure and function of healthy ovarian tissue. Cystectomy scores better than drainage and coagulation for endometriosis-associated pain [25]. Both ablation and excision of peritoneal endometriosis is beneficial in reducing endometriosis-associated pain [26]. It should be used for short coagulation time to minimize damage to ovarian tissue. Argon beam coagulation-Effect on tissue is similar to monopolar coagulation, but it has benefit of using it over the wider superficial areas. Based on no difference in pregnancy rate, some advise cystectomy while others advise caution with cystectomy because of harmful effects on ovarian reserve as a result of stripping of the cyst wall carrying healthy ovarian tissue. Anatomical consideration-Ovaries and endometriotic cysts are usually adherent to pelvic side walls and ovarian fossa where the ureter might be involved. Blood supply of the ovary is from the ovarian artery and ascending branch of the uterine artery in the ovarian ligament. Thus, large intraovarian vessels are found on anterolateral aspect of the ovary at the hilum near the insertion of the meso-ovarium. Method of cystectomy [30] Cyst wall is retrieved through laparoscopy ports and rarely through posterior colpotomy. Ovarian suspension and anti-adhesive measures should be used to prevent postoperative adhesion formation. Icodexrin (4%) derivative of maltodextrin, which is a colloid osmotic agent, can be used for peritoneal lavage during laparoscopy/ laparotomy. It remains in the peritoneal cavity for 4 days and helps in prevention of adhesion formation by hydrofloatation of peritoneal organs, thus keeping them apart during the probable time of adhesion formation in the postoperative period [32]. In case of suspicion of malignancy, peritoneal washings and biopsy from the suspected area should be taken before mobilizing ovary. If the cyst ruptures during separation, extend the opening in the cyst wall to expose cyst cavity. Turn cyst inside out to facilitate further removal of cyst wall and achieve hemostasis. When ovary is nonadherent, incision should be made on thinnest part of endometrioma on antimesenteric border. Vasopressin and saline injections in cyst capsule can be done to reduce blood loss during cystectomy. If cleavage plane is not identified, send cyst wall for histology, and use ablation method, rather than stripping of ovarian stroma. Careful dissection plane and precise spot bipolar coagulation is the key to achieve hemostasis. After removal of large cyst, reconstruction of ovary may be needed using monofilament suture. If fertility is desired [34] Offer excision/ablation and adhesiolysis to women with endometriosis not involving bowel, bladder, and ureter to increase the pregnancy rates. Cystectomy is associated with reduced ovarian reserve, and the same should be discussed with the patient before surgery, especially in cases of bilateral endometriomas and recurrent surgeries. If fertility is not desired [34] Consider excision rather than ablation of endometriosis lesions. If hysterectomy is indicated, excise all visible endometriotic lesions with hysterectomy. Likewise, postoperative hormonal therapy in the first 6 months does not improve the surgical outcome of pain relief. Postoperative additional hormonal therapy does not improve spontaneous pregnancy rates and should not be given. Nonetheless, hormonal therapy prescribed after surgery is helpful for contraception or secondary prevention. Secondary prevention is described as interventions aimed to prevent the recurrence of endometriosis and associated symptoms such as pain, more than 6 months after surgery [36]. Contraceptives are also recommended for secondary prevention of endometriomas [37]. In women undergoing surgical menopause for endometriosis, combined estrogen/progesterone therapy or tibolone may be given until the age of natural menopause [38]. However, the risk of reactivation of disease or malignant transformation of the same and the side effects of hormone replacement therapy should be considered and discussed with the patient [39]. Somigliana E, Vigano P, Filippi F, Papaleo E, Benaglia L, Candiani M, Vercellini P. Kondo, W, Bourdel N, Tamburro S, Cavoli D, Jardon K, Rabischong B, Botchorishvili R, Pouly J, Mage G, Canis M. Minimally invasive surgery when treating endometriosis has a positive effect on health and on quality of work life of affected women. Prospective evaluation of laparoscopic appendectomy in women with chronic right lower quadrant pain.
Purchase generic luvox on line
Two models have been developed using the retardance and optic axis orientation information (Ugryumova et al anxiety videos buy luvox line. The through-plane orientation and tissue birefringence are extracted by fitting the retardance measurements. Another method has been developed based on the measurements of the optical axis orientation corresponding to different incident angles (Liu et al. This method improves the contrast of the image while preserving the lateral resolution. Due to the distortions introduced by histology protocols, a non-linear approach is needed. To compare the neuronal content, we manually segmented neurons from each modality. The type, shape, and size of neurons vary dramatically throughout the human brain, which influences the optical properties of the brain tissue. Even though the diameter of the neurons covers a large range, the shape of the neurons, a triangular cell body with an apical dendrite, is plainly visible on both images. This pigment gives the neurons a black hue that is visible to the naked eye on a gross sample, as well on a Nissl staining of these areas. Finally, one of the largest neurons found in the brain are the Purkinje cells of the cerebellum, second only to the Betz cells found in primary motor cortex. Purkinje cells have a spherical cell body, and are packed in the narrow intermediate layer of the cerebellar cortex. These neurons have a single long axon in the granular layer, an extended dendritic tree in the molecular layer, which is organized in a 2D plane perpendicular to the long axis of the folium. The gap left by the vessels in the Nissl stained images is much larger than their size seen on the blockface. For some stains, such as Gallyas, studying both the white matter and gray matter with the same protocol is challenging. As a result, the white matter is darkly stained and does not allow visualization of the fiber organization. This allows us to probe the overall architecture (cyto- or myelo-) of the human cortex and the structures of subcortical regions. In contrast, histology and immunohistochemistry can make use of a wide variety of stains (dyes) and antibodies to differentiate neurons not only based on size and shape, but also on their neurotransmitter production. If we can quantify spatial distributions in the optical scattering coefficient, we would then obtain spatial maps indicating the relative cell density and myelin content. Thus, it may be possible to develop models to fit the depth dependent optical attenuation and retardance to disentangle the relative cell density and myelin content. Fitting this signal model to the depth profile of the experimental data, it is possible to estimate local values for the scattering coefficient, achieving our first step in quantifying the relative cell density and myelin content. In addition, this fitting will also reveal information about the tissue back-scattering coefficient. The ratio of the back-scattering coefficient to the overall scattering coefficient reveals information about the anisotropy of the scattering direction, in that a larger/smaller ratio indicates more/less isotropic scattering. When the ratio of back-scattering to scattering becomes small, it indicates that the optical scattering is preferentially along the optic axis and typically results from larger scattering particles. Thus, it is possible to derive some information about the relative sizes of the scattering particles within the tissue. Future work will integrate such model fitting of the tissue scattering and back-scattering coefficients with polarization measurements of tissue birefringence in order to quantify the relative spatial distributions of cell density and myelin content. This system has enabled us to produce stunning images, but is lacking several key advances critical for imaging of larger volumes of tissue. At this rate, it would take over ten years to image the approximately 1200 cm3 of the whole human brain. Two principal advances can be made to the optical acquisition system to reduce this to approximately ten weeks. This alone would reduce the projected greater than 3,600 days for imaging the whole human brain, down to 18 days. However, this projection ignores the dead time due to sample translation and sectioning. To volumetrically image the entire blockface of the whole human brain requires cutting slices at least 11 cm wide. This cannot be done with a vibratome, but can be done with a microtome, as is used in histology to section coronally a whole human brain (Amunts et al. The challenge is that these hardening methods increase optical scattering in the tissue. Those morphological and quantitative characterizations of these layers will provide useful information to investigate the cortical boundaries among different brain regions. The optical properties of scattering and birefringence originate from the underlying cellular and molecular content, such as size, cellular density, myelin content, and structural alignment. Thus, important pathological processes such as neuron loss may be observed as a decrease in scattering or increase of light penetration, whereas deposit or aggregation of proteins may manifest as highly scattering spots. Another example is the degradation of myelin that may be correlated with a decrease in birefringence in multiple sclerosis and traumatic brain injury. The neuropathological progression also leads to a morphometric change in brain structures such as cortical thinning in specific layers (Du et al. Assayag, Osnath, Kate Grieve, Bertrand Devaux, Fabrice Harms, Johan Pallud, Fabrice Chretien, Albert-Claude Boccara, and Pascale Varlet. Bolmont, Tristan, Arno Bouwens, Christophe Pache, Mitko Dimitrov, Corinne Berclaz, Martin Villiger, Bettina M. Vergleichende Lokalisationslehre Der Grosshirnrinde in Ihren Prinzipien Dargestellt Auf Grund Des Zellenbaues. Nakaji, Haruo, Nobuo Kouyama, Yoshihiro Muragaki, Yoriko Kawakami, and Hiroshi Iseki. Kadiri, Kannan Umadevi Venkataraju, Karsten Bahlmann, Jason Sutin, Julian Taranda, Ignacio Arganda-Carreras, Yongsoo Kim, H. Human Brain Imaging by Optical Coherence Tomography 437 Wang, Hui, Christophe Lenglet, and Taner Akkin. Zilles, Karl, Gottfried Schlaug, Massimo Matelli, Giuseppe Luppino, Axel Schleicher, Meishu Qu, Andreas Dabringhaus, Rudiger Seitz, and Per E. As the oxygen reserve in the brain is limited, and anaerobic metabolism of neurons is low, adequate perfusion of blood is crucial for the proper function and viability of these cells. The adequate perfusion of blood is regulated by the healthy brain in order to prevent situations where blood flow is higher or lower than needed for proper function (Czosnyka et al. The authors conclude that non-invasive monitoring of autoregulation may provide an accurate means to predict impaired autoregulation.
Buy luvox 50mg on line
Shown are follicles and enclosed oocytes at different stages of development from primordial to antral follicles anxiety yellow stool buy cheap luvox. Following ovulation, the oocyte is released into the body cavity and the empty follicle is transformed into a corpus luteum. A single report described a moderate expression of the long and short D2R isoforms in pig oviducts and uterus [88]. In the human placenta, D2R expression was seen in the cytotrophoblasts, syncytial trophoblasts, vascular endothelial cells, and fibroblasts in the chorionic villi [89]. In the rat placenta, expression of D1R and D2R was evident in the spongiotrophoblast and giant cells of the junctional zone [90]. Sources and significance of plasma levels of catechols and their metabolites in humans. Tyrosine hydroxylase and dopamine transporter expression in lactotrophs from postlactating rats: Involvement in dopamine-induced apoptosis. Tyrosine hydroxylase in the stalk-median eminence and posterior pituitary is inactivated only during the plateau phase of the preovulatory prolactin surge. Dopamine, vesicular transporters, and dopamine receptor expression in rat major salivary glands. Expression of tyrosine hydroxylase in lymphocytes and effect of endogenous catecholamines on lymphocyte function. Mast cells express tyrosine hydroxylase and store dopamine in a serglycindependent manner. Bone marrowderived mesenchymal stem cells increase dopamine synthesis in the injured striatum. Acute wounding alters the beta2adrenergic signaling and catecholamine synthetic pathways in keratinocytes. Tyrosine hydroxylase isoenzyme I is present in human melanosomes: A possible novel function in pigmentation. Uptake of L-3,4-dihydroxyphenylalanine and dopamine formation in cultured renal epithelial cells. Molecular modeling and quantitative structure-activity relationship analysis demonstrate a molecular basis for sulfotransferase substrate specificity. D2 dopamine receptor antagonist raclopride induces non-canonical autophagy in cardiac myocytes. Dopamine D1 receptor augmentation of D3 receptor action in rat aortic or mesenteric vascular smooth muscles. Pharmacological characterization and autoradiographic localization of dopamine receptors in the portal vein. Type 1A dopamine receptor expression in the heart is not altered in spontaneously hypertensive rats. Influence of bradykinin B2 receptor and dopamine D2 receptor on the oxidative stress, inflammatory response, and apoptotic process in human endothelial cells. Renal dopaminergic system: Pathophysiological implications and clinical perspectives. Dopamine receptor expression and function in human normal adrenal gland and adrenal tumors. Dopamine activates amiloride-sensitive sodium channels in alveolar type I cells in lung slice preparations. Differential expression of a(2a), A(1)-adenosine and D(2)-dopamine receptor genes in rat peripheral arterial chemoreceptors during postnatal development. Evidence for the presence of both D-1 and D-2 dopamine receptors in human esophagus. Organization of the enteric nervous system in the human colon demonstrated by wholemount immunohistochemistry with special reference to the submucous plexus. Physiological modulation of intestinal motility by enteric dopaminergic neurons and the D2 receptor: Analysis of dopamine receptor expression, location, development, and function in wild-type and knock-out mice. The analysis of quantitative expression of somatostatin and dopamine receptors in gastro-enteropancreatic tumours opens new therapeutic strategies. Dopamine, vesicular transporters and dopamine receptor expression and localization in rat thymus and spleen. The dopaminergic system in peripheral blood lymphocytes: From physiology to pharmacology and potential applications to neuropsychiatric disorders. Dopamine in the immune system: Dopamine receptors in immune cells, potent effects, endogenous production and involvement in immune and neuropsychiatric diseases. Dopamine D2-like receptor agonists accelerate barrier repair and inhibit the epidermal hyperplasia induced by barrier disruption. Expression profile of genes associated with the dopamine pathway in vitiligo skin biopsies and blood sera. Activation of dopamine D1 receptors in dermal fibroblasts restores vascular endothelial growth factor-A production by these cells and subsequent angiogenesis in diabetic cutaneous wound tissues. Autoradiographic localization of the dopaminergic agonist 3H-dihydroergotoxine within the male reproductive system. Localization of peripheral dopamine D1 and D2 receptors in rat and human seminal vesicles. Existence of postsynaptic dopamine D2 receptor as an enhancer of contractile response in vas deferens. Evidence for a dopamine intrinsic direct role in the regulation of the ovary reproductive function: In vitro study on rabbit corpora lutea. Molecular cloning, expression and variation analyses of the dopamine D2 receptor gene in pig breeds in China. Expression and therapeutic targeting of dopamine receptor-1 (D1R) in breast cancer. The neurogenic niche in the carotid body and its applicability to antiparkinsonian cell therapy. The kidney is a vital organ with considerable cellular complexity and functional diversity. Shown are the three major parts (pelvis, medulla, and cortex), location of a nephron, the pyramid structure composed of the collecting ducts, the ureter, and the renal vein and arteries. The remainder of the structures of the urinary system serve as the conduits for the transport, storage, and release of urine. Embryonic development of the kidney depends on time-related reciprocal inductive signals between mesenchymal and epithelial progenitor tissues [1,2]. The urinary system is a component of the "urogenital system," and is anatomically associated with genital development. The early patterning of the kidney region depends on interactions between the Pax/Eya/Six genes, with essential roles also played by lim1, Odd1, and Wnt genes. Ureteric bud outgrowth and branching morphogenesis are controlled by the Ret/Gdnf pathway, which is under positive and negative regulation by a variety of factors. After birth, the kidneys continue to mature, and by 2 years of age, they are similar to the adult kidneys in their capacity for regulating body water and for ensuring waste elimination. During childhood, the kidneys grow in size and reach a near-adult size of 10 cm in diameter by 12 years of age; the bladder also continues to grow up to this age. The kidneys in humans are located in the abdominal cavity on each side of the spine. Blood enters the kidneys through the renal arteries, which are branches of the abdominal aorta, and leaves via the renal veins, which drain into the inferior vena cava. Despite their relatively small size, the kidneys receive as much as 20% of the cardiac output, at a flow rate of about 1 L/min. This disproportionally large blood flow enables the kidneys to carry out a massive filtration endeavor that generates up to 180 L of filtrate each day. Once filtered, processed and concentrated, urine is moved from the kidney through the ureters into the bladder, where it is stored until being emptied upon the relaxation of the urethral sphincter. The renal hilum serves as the entry and exit site for all structures that service the kidneys: blood vessels, nerves, lymphatics, and ureters.
