
60caps ashwagandha with amex
In these cases anxiety symptoms flushed face purchase 60caps ashwagandha, death may result from laryngeal spasm and asphyxia during submersion. Early animal studies in anaesthetized dogs showed that spontaneous respiratory efforts continued for around 60 s after immersion. Recent Chinese bronchoscopic studies in anaesthetized dogs whose lungs were filled with seawater showed that the bronchi fill with bronchoalveolar fluid, causing increasing blood lactate dehydrogenase-L and alkaline phosphatase levels. There is a rapid fall in cardiac output, while pulmonary capillary wedge pressure, central venous pressure, and pulmonary vascular resistance increase. Reduction in the dynamic compliance of the lungs is similar, following inspiration of all types of solutions. However, aspiration of large volumes of hypertonic seawater draws fluid into the lung from the circulation by osmosis, resulting in fluidfilled, nonventilated, but perfused alveoli incapable of normal gas exchange while aspiration. Conversely, aspiration of large amounts of hypotonic freshwater may cause sufficient absorption of fluid into the circulation from the alveoli to cause both acute hypervolaemia and haemolysis. Within 1 h, pulmonary oedema develops, resulting in a decrease in circulating blood volume. Early studies suggested that 85% of human drowning victims aspirated 22 ml/kg of water or less, but it has been estimated that about 10% of body weight of water may be absorbed from the lungs during freshwater drowning. However, in hypothermic conditions, brain activity may be restored after up to 60 min of submersion apnoea. Continuous aspiration of cold water results in rapid core cooling, while the circulation is intact. Such victims may survive with little or no neurological deficit after long submersion with extreme hypoxia. Worldwide, fatal drowning is generally more prevalent in indigenous races than in others. Despite discouraging data from animal studies, recent reports suggest that in hypothermic submersion-associated cardiac arrest, adrenaline and vasopressin may help to achieve the vasopressor response needed to restore spontaneous circulation prior to rewarming. This treatment could obviate prolonged mechanical cardiopulmonary resuscitation, or the use of extracorporeal circulation. It has proved effective in restoring spontaneous circulation, but one patient died of multiorgan failure 15 h later. In warm-water drowning there appears to be no statistically significant correlation between duration of submersion and survival. Swimmers in difficulty may be able to shout for help but, contrary to public opinion, those who are drowning do not. Most drowning victims adopt a characteristic vertical position in the water-legs hanging vertically, head tilted back for quick exhalation and inhalation before bobbing underwater, with no time or sufficient breath to call for help. Clinical features Prognostic indicators None of the recent developments in assessment, treatment, or equipment has improved survival rates among submersion victims. The key to a successful outcome and return to productive, full life is early bystander cardiopulmonary resuscitation, early and aggressive advanced life support methods. However, up to 25% of drowning victims presenting to the hospital emergency department will die and a further 6% suffer neurological sequelae. The prognosis cannot Causes of drowning Drowning occurs in many different situations: after accidental immersion in people with little or no swimming ability, with head and neck injury, following cardiac and neurological emergencies. Neurological status Victims who are alert when medical help arrives have a survival rate approaching 100%, whereas the prognosis in those who are comatose with fixed, dilated pupils is poor. Among victims with impaired consciousness, 87% will survive without neurological defects and 2% with minor defects, while 11% will die. Those with no spontaneous limb movements and abnormal brain stem function 24 h after the accident have a poor neurological outcome. Pupil reactivity at the time of arrival differentiates survivors from fatalities but could not differentiate between those with minor or incapacitating neurological deficits. Children who show no spontaneous movements and have abnormal brainstem function 24 h after submersion injury are likely to suffer severe neurological deficits or death. Although the cause and pathophysiological changes of pulmonary insufficiency vary depending on the type and volume of fluid aspirated, serum electrolyte and haemoglobin concentrations (or haematocrit) do not predict survival. Mortality is high in victims with circulatory arrest on admission, but those in sinus rhythm with reactive pupils, who are neurologically responsive at the scene of immersion, have good outcomes. Those who are asystolic on arrival at hospital and remain comatose for more than 3 h have a poor prognosis unless they are hypothermic. Treatment Victims of submersion injury must be treated immediately for ventilatory insufficiency, hypoxia, and the resulting acidosis. A successful outcome depends on early effective resuscitation at the scene and on competent intensive life support. In-water resuscitation is effective within 5 mins of the shore, or longer, if the victim shows signs of increased activity after the initial breaths of the shore. Immediate Laying victims on their side for assessment of the airway and breathing will assist drainage of any excess water from the airways and lungs. If necessary, on-site cardiopulmonary resuscitation should be started as soon as possible using supplemental oxygen if available, preferably in the highest concentration An oropharyngeal airway, endotracheal tube, or laryngeal mask airway should be inserted in comatose victims, if suitably skilled personnel are present. Respiratory and cardiopulmonary arrest may occur after an apparently successful rescue, mandating close, uninterrupted monitoring, and the early administration of oxygen to all immersion victims. At the hospital On arrival at the hospital, after a clear airway and cardio-circulatory support have been established, arterial blood gas tensions and pH should be measured. The pH of the blood will indicate whether there is a residual metabolic acidosis after a substantial period of hypoxia. Mechanical ventilation may be necessary with positive endexpiratory pressure, or continuous positive airway pressure to maintain arterial oxygen pressure above 10 kPa with an inspired oxygen fraction below 0. After both freshwater and seawater aspiration, large volumes of intravenous colloid are usually needed while circulating blood volume and cardiac output are estimated. A central venous catheter or pulmonary artery catheter helps to assess the effective circulating blood volume to guide fluid therapy. Failure of response to intravascular replacement with 20 ml/kg of colloid is an indication for starting inotropes. Steroid and prophylactic antibiotic therapy do not appear to increase the chance of survival. Inpatient treatment Extracorporeal membrane oxygenation has been proved to be effective after drowning. A 3-year-old drowned girl in refractory cardiorespiratory arrest was successfully resuscitated using cardiopulmonary bypass, and then extracorporeal membrane oxygenation for 4 days. Despite a prolonged period in a vegetative state, she later made an almost complete neurological recovery. If adult respiratory distress syndrome occurs, it is usually within 6 h of admission.
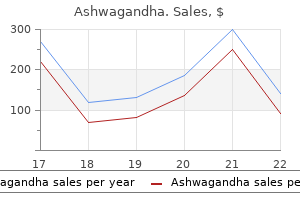
Glycine hispida (Soy). Ashwagandha.
- Reducing the duration of diarrhea in infants.
- What other names is Soy known by?
- Preventing thyroid cancer, endometrial cancer, lung cancer, prostate cancer, improving memory, reducing breast pain, weight loss, asthma, high blood pressure, premenstrual syndrome (PMS), and other conditions.
- Reducing protein in the urine of people with kidney disease.
- Dosing considerations for Soy.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96936
Generic 60 caps ashwagandha with visa
Effects of two forms of combined oral contraceptives on carbohydrate metabolism in adolescents with polycystic ovary syndrome anxiety symptoms guilt order genuine ashwagandha on line. Metformin therapy in obese adolescents with polycystic ovary syndrome and impaired glucose tolerance: amelioration of exaggerated adrenal response to adrenocorticotropin with reduction of insulinaemia/insulin resistance. Metformin or oral contraceptives for adolescents with polycystic ovarian syndrome: a meta-analysis. Pioglitazone and metformin in obese women with polycystic ovary syndrome not optimally responsive to metformin. Psychological aspects of hyperandrogenic states in the late adolescent and young women. The incidence of oligomenorrhea and the other manifestations are variable in different phenotypes. In fact, the increase of body weight and fat tissues, especially in the form of abdominal obesity, is associated with an abnormality of sex-steroid balance. The mechanisms that may mediate Adipokines In obesity, many genes were dysregulated in adipocytes of obese compared with nonobese individuals [35]. Obesity in polycystic ovary syndrome and infertility Chapter 3 25 Leptin Leptin is a 16 kDa protein that is secreted almost exclusively by the adipocytes and is produced by the obese (ob) gene. It may serve as a link between fat tissues and the brain, since by acting at the level of the hypothalamus, leptin decreases food intake and increases energy expenditure [37]. Leptin receptors have been demonstrated in the hypothalamus and pituitary as well as in theca cells, granulosa cells, oocytes, endometrial cells, and preimplantation embryos [14]. Leptin levels have been found to be positively correlated with insulin resistance in such women, although some contradictory findings have been reported. Similarly, in some but not all studies, following treatment with insulin-sensitizing agents, leptin concentrations in blood had decreased. In vivo and in vitro experiments in animals have shown that high levels of leptin, representing hyperleptinemia of obesity, may inhibit folliculogenesis [41,42]. Leptin may have a role in regulation of embryo implantation and endometrial receptivity, and it has been suggested that obesity-related perturbations of the leptin system can possibly interfere with embryo implantation, therefore causing infertility [14]. Besides, a direct role of low levels of adiponectin on folliculogenesis is possible. It was found that human theca cells express adiponectin and adiponectin receptors (AdipoR1 and AdipoR2), while granulosa cells express AdipoR1 and AdipoR2, but not adiponectin. Adiponectin, in contrast to leptin, is downregulated in obesity and may have both antiinflammatory and insulin-sensitizing effects. Of late, bariatric surgery has also gained ground in recent years in the case of infertile women with excessive obesity. Diet Lifestyle Bariatric surgery Lifestyle modifications are based on diet and exercise and aim at the restoration of the disturbed reproductive function. A steady decrease of intraabdominal fat is associated with restoration of ovulation [65]. Although energy-restricted diet is the key factor, information regarding the specific type of exercise that is more effective is limited. It has been suggested that the addition of aerobic resistance exercise to an energyrestricted diet did not further improve reproductive outcomes [66]. However, sibutramine has been withdrawn from the market in the majority of the European countries and therefore it is not recommended. Evidence from studies suggests that diets with reduced glycemic load may provide a better control of hyperinsulinemia and the metabolic consequences as well as menstrual cyclicity [68]. However, a recent metaanalysis has not provided clear evidence that lifestyle intervention can have an impact on glucose tolerance, although it improves free androgen index, but there were no studies investigating the effect of this intervention on live birth, miscarriages, or menstrual regularity [69]. This might be a hindrance to the women who are very anxious to get pregnant quickly. Evidence has been provided that ghrelin may affect reproductive function in animals and humans. Plasma ghrelin concentrations have been shown to be lower in obese when compared with normal subjects. These include visfatin, vaspin, apelin, retinolbinding protein 4, kisspeptin, copeptin, irisin, and zonulin [58]. However, for some of these substances, data are limited, and further research is needed. Although the basis of such treatment is the administration of different drugs, in obese women diet and lifestyle changes are considered the first-line approach [60]. In the case of noncompliance, various treatments or interventions, Obesity in polycystic ovary syndrome and infertility Chapter 3 27 conceptus or it is more reasonable to postpone conception until the end of the effort to lose weight. However, taking into account that obesity can adversely affect human reproduction by increasing perinatal and maternal risks, it is advisable for the women to reduce their weight before attempting to conceive [70]. Obese women during pregnancy carry a greater risk for congenital anomalies, miscarriage, gestational diabetes, and hypertension either after spontaneous or after assisted conception [71,72]. Although bariatric surgery may have a positive impact on pregnancy complications related to obesity, new risks may arise related to nutritional deficiencies, anemia, and changes in maternal glucose metabolism [79]. Clomiphene citrate Clomiphene citrate is an antiestrogenic compound that belongs to the selective estrogen receptor modulators. The protocol for ovulation induction involves the administration of clomiphene at a starting dose of 50 mg/day immediately after a spontaneous period or withdrawal bleeding induced by the administration of progesterone. Nevertheless, in properly selected patients, cumulative pregnancy rates as high as 63% at 6 months and 97% at 10 months have been reported [85,86]. In cases of clomiphene failure or clomiphene resistance, a second-line treatment is used. Clomiphene resistance is attributed to several hormonal and clinical characteristics of the women. Especially, women with less-reduced insulin sensitivity had a higher possibility of ovulating on clomiphene treatment [90], while obesity had a negative impact on the treatment outcome with clomiphene [91]. Such women may need higher dosages of clomiphene even up to 250 mg/day, although the evidence is limited to retrospective data [92]. These compounds inhibit the action of the enzyme aromatase, which converts androgens into estrogens. Consequently, the reduced production of estrogens and the reduced circulating levels of these steroids lead to the attenuation of the negative feedback and the increase in the secretion of gonadotrophins from the pituitary. Letrozole is one of the third-generation aromatase inhibitors used more extensively than others for the treatment of infertility. It should be noted, however, that letrozole is still considered an "offlabel" medication for infertility treatment due to possible teratogenic effects in pregnancy, although this has been debated [83,102]. It is advisable, therefore, to discuss with the patients the possible risks and benefits. Both protocols are equally effective in terms of pregnancy rate, although with the step-up protocol higher monofollicular development and lower hyperstimulation are achieved [105]. The treatment is monitored only by ultrasound scans of the ovaries, while estradiol measurement is not required. In the same study, significantly higher doses of gonadotrophins were required in the group of the obese than in the group of the lean women, a finding that was confirmed in a subsequent study [110]. However, due to a rather complicated prediction model based on a mathematical equation, such an approach has not been proven reliably effective. Obesity in polycystic ovary syndrome and infertility Chapter 3 29 Retrospective data have shown high ovulation and pregnancy rates [116]. Ovarian drilling can be also performed by fertiloscopy, which provides as good results as laparoscopy, but experience is needed because the risk of complications is greater [124]. Metformin is the main representative and has been used more extensively than other compounds with similar actions.
Generic ashwagandha 60caps with visa
Withdrawal symptoms can last two to three days and can include insomnia anxiety coach cost of ashwagandha, anxiety, nausea, hallucina tions, and nightmares. Hallucinogen Abuse Hallucinogens, also called psychedelic drugs, com monly produce hallucinations. These drugs cause a heightened and distorted response to visual, auditory, and tactile stimuli and induce the affected individual to see flat objects take on shape, stationary objects to move, and colors to become more vivid. It is a colorless, tasteless, and odorless synthetic substance primarily produced in illegal laboratories. It can be added to the food or drink of an unsuspecting vic tim or to chewing gum, hard candy, postage stamps, or stickers. Delusions, hallucinations, and abnormal thought processes can cause temporary or permanent mental changes. Some hallucinations are called "trips" since the drug user may feel that they have travelled outside their bodies or have gone to foreign, mysterious locations. It appears that this drug is abused to escape reality rather than to help cope with reality. The person might attempt to fly or exhibit episodes of violence and self-destruction. Flashbacks (recurrence of a trip) can occur months after the drug was taken because it is stored in fat tissue and might be released at a later time. Native Americans use this cactus as part of their traditional religious ceremonies. Narcotic Abuse Narcotics are depressants that are primarily prescribed as analgesics or painkillers. Demerol, methadone, morphine, heroin, and opium are classified as narcotics and are commonly abused. Narcotics lower blood pressure and slow nerve and muscle action and the rate of the heart and breathing. Physical and psychological dependence and tolerance rapidly develop with the use of narcotics. Overdose symptoms include slurred speech, confusion, staggering, coma, and respiratory arrest. References to opium smoking are common in Oriental history, and some people in Asian countries still smoke opium. Users in the Western coun tries, including the United States, prefer opium deriv atives such as morphine and heroin. Glimpse of the Future Nasal Spray for Overdoses study testing the effectiveness of a nasal spray treatment for victims of drug overdoses is being conducted in the United States. This drug is used at present time to treat overdoses, most commonly those caused by morphine, heroin, and oxycodone. The drug rapidly goes into the bloodstream and effects change within a few seconds to a couple minutes. The hope of the study is that a quicker response might save more lives and that friends and families will be more likely to call 911 and get help for overdose victims if they see the officers as being lifesavers. The results of the study, if positive, might influence other law enforcement departments to use this treatment for overdose victims, hopefully saving more lives. Heroin use usually gives a rush, or intense feeling of well-being, followed by a sleepy, drowsy state. Symptoms of withdrawal include sweating, shaking, diarrhea, vomiting, and sharp pain and cramps in the stomach and legs. Inhalant Abuse Inhalants are chemicals that produce a vapor that can be inhaled and that produce a mind-altering effect. Young people are more likely to abuse inhalants than adults and often treat the use of inhalants as a game or a way to get a cheap high. Inhalants include over 1,000 legal substances, including glue, spray paint, hair spray, nail polish, lighter fluid, and gasoline. These substances commonly contain harmful hydrocarbons and an oily base that, when inhaled, coats the inner lining of the lungs. Inhalant abuse refers to intentionally breathing the vapors of a substance to get high. Bagging is the most dangerous because it entails placing a plastic bag over the head to get a longer effect, thereby increasing the risk of accidental suffocation. Using inhalants over a period of time can result in permanent brain, heart, kidney, and liver damage. Some products, such as paint and gasoline, contain lead and can result in death from lead poisoning. Inhalant abuse is the third most common substance abused by individuals aged 12 to 14 years, surpassed only by alcohol and tobacco. Symptoms of inhalant abuse include spots or sores around the mouth, a glassyeyed look, fumes on the breath or clothing, anxiety, and loss of appetite. Anabolic Steroid Abuse Anabolic steroids are the synthetic derivatives of testos terone, the male sex hormone. They are widely abused by athletes and others trying to promote growth of skeletal muscle and increase lean body mass. From the fitness craze of the 1980s, the use of anabolic steroids has increased significantly in young males and even in females who want to develop athletic, lean bodies. They are up 78% over the last decade, which puts them ahead of car accidents on the accidental injury causes list. Some accidental overdoses and poisonings could certainly be avoided if individuals were more careful about reading labels on medications and not mixing them with alcohol or other prescription medications without consulting with their health care provider. Some of the overdoses are attributed to suicide, but far more are due strictly to misuse or overuse of prescription or over-the-counter medications. Many of these overdoses occur in those addicted to pain medications such as oxycodone. The overuse and abuse of prescription medications is rampant in the United States. Pain medications, such as the opiate drugs, are the most common ones that are abused. However, other over-the-counter drugs such as loperamide, decongestants, cough suppressants, and antihistamines are also abused. These drugs are generally considered to be safe, but should only be taken as prescribed by the health care provider and/or as noted on the label. The old adage "Read the Label," certainly applies when trying to prevent overdoses, but the individuals also need to "follow the instructions" after reading the label. Source: Associated Press (2016) and Davidson (2016) Copyright 2019 Cengage Learning. They do pro duce increases in muscle strength, lean body mass, and improved performance over periods of time, but the long-term effects are dangerous. The side effects include shrinking of the testes, reduced sperm count, infertility, and baldness in males; and growth of facial hair, changes in menstruation, enlargement of the cli toris, and a deepened voice in females. A spectrum of behaviors is exhibited by people on anabolic steroids: these behaviors range from being somewhat more assertive, to being frankly aggressive, to displaying what is described as "roid rage. Adolescents or preteen children can experience accelerated puberty changes and growth cessation from premature skeletal maturation. These disorders affect the cognitive abilities-the abilities to think, remember, and make judgments by the affected indi vidual. Dementia is common in the elderly; it was called senility in the past and thought to be caused by aging. Dementia is a progressive deterioration of mental abilities due to physical changes in the brain. We now know that dementia is not part of the normal aging process but, rather, is caused by a variety of medical conditions. Factors important in determining whether dementia will occur in an individual include nutritional status, family history, chronic diseases, and general state of health. An affected individual might lose items, get lost when driving even in familiar areas, get confused in conversations, and lose the ability to perform common tasks such as balancing a checkbook. Symptoms often develop gradually and show a progressive deterioration of cognitive or mental abilities, including severe memory loss, disorientation, impaired judgment, and the inability to learn new thorough medical, physical, and neurologic examination. The American Psychiatric Association has established two criteria to support the diagnosis of dementia. The second is the loss of one of the following functions: language, motor activity, recognition, and executive function (unable to plan, organize, or think abstractly). These include correcting drug doses, ensuring that prescribed medications are being taken correctly, withdrawing misused drugs, treating depression and other medical conditions, and ensuring proper nutrition and hydration.
Generic ashwagandha 60caps fast delivery
In addition anxiety symptoms breathing problems discount 60 caps ashwagandha mastercard, this young age group more frequently delivered babies of birthweight between 1500 and 2500 g. In this study of 16,512 consecutive nulliparous women, the incidences of stillbirth and index values of fetal condition at birth were not significantly different between age groups [27]. Younger maternal age has also been shown to be associated with increased risk of fetal death and anemia during pregnancy. The risk of preeclampsia, cesarean section, instrumental vaginal delivery, and postpartum hemorrhage is lower in teenage pregnancy [28]. Obesity confers an increased risk of adverse fetal and pregnancy outcomes, including gestational diabetes, fetal macrosomia, and delivery by cesarean section and preeclampsia. In addition to an increased risk of premature mortality, childhood/adolescent obesity is also associated with an increased risk of later diabetes, stroke, coronary heart disease, and hypertension. A retrospective study of 230,000 Norwegian adolescents was followed-up on average for 34. In case of diseases of the circulatory system in men, ischemic heart disease was the dominant cause of death, whereas in women the death was due to cerebrovascular disease. Parents should be encouraged to integrate healthy lifestyle behaviors into the family unit, thereby decreasing the risk of obesity in their children and improving their own physical and mental health. The long-term impact of maternal weight loss was elegantly demonstrated by the reported impressive reduction in childhood/adolescent obesity in children of mothers who underwent bariatric surgery. An accompanying improvement in cardiometabolic risk factors also occurred that was sustained into adolescence and adulthood [33]. Obesity prevention programs in kindergartens and schools based on exercise therapy and dietary intervention have failed in preventing childhood obesity. This may suggest that public health restrictions on advertising and marketing of sweetened drinks are a meaningful approach to the fight against childhood obesity. Lifestyle interventions A Cochrane review [34] regarding treatment in obese children included 64 randomized controlled trials with 5230 participants. Metaanalysis indicated a reduction in overweight at 6 and 12 months in response to lifestyle interventions. Dietary modification and exercise programs are effective in the treatment of already-obese children. Management principles Prevention Prevention programs should address parental weight status and smoking habits, both of which are modifiable risk factors. Reductions in weight preconception may result in Drugs the Cochrane review also concluded that consideration should be given to the use of drugs such as orlistat or sibutramine as an adjunct to lifestyle interventions in obese adolescents. Surgery Gastric banding in obese adolescents is an effective intervention leading to substantial and durable reduction in obesity and to better health. The prevalence of amenorrhea and/or oligomenorrhea decreased significantly in the weight-loss group. Lifestyle modification with calorie restriction and increased exercise should be considered as first-line treatment of the comorbidities of obesity and insulin resistance. Progestins protect the endometrium against hyperplasia induced by unopposed estrogen stimulation. Metformin increases insulin sensitivity by the liver, increases peripheral glucose uptake, decreases fatty acid oxidation, and decreases glucose absorption from the gut. Metformin therapy in adolescents seems to be associated with several benefits, including an improvement in glucose tolerance, a decrease in testosterone levels [41], and an improvement in menstrual cyclicity; some report between 90% and 100% resumption of menses in Obesity in adolescence Chapter 2 21 adolescents [42]. These studies were all relatively small, and, in most, significant weight loss occurred, making the data difficult to interpret the effect of metformin independent of weight loss. This has not yet been substantiated by metaanalysis of randomized controlled trials. The dose should be titrated upward over a period of 1 month due to gastrointestinal side effects. Metformin was superior for weight reduction and associated with decreased dysglycemia. These medications have not been well studied in adolescence and remain off-label in this age group due to lack of evidence on efficacy and safety. In particular, a clear focus on lifestyle and prevention measures should be adopted for all age groups from preconception to early childhood, adolescence, and adulthood. Population-based prevention strategies for childhood obesity: report of a who forum and technical meeting. Consensus views arising from the 53rd study group: obesity and reproductive health. Modelling the relationship between obesity and mental health in children and adolescents: findings from the Health Survey for England 2007. Conclusion Obesity in childhood and adolescence is a global epidemic with health implications. There are geographic and ethnic variations in the prevalence of adolescent obesity, but it is an international problem. All efforts should be made to control this epidemic and therefore to avoid or reduce the health-care burden of chronic illness on health-care systems as well as to reduce the personal cost, including premature mortality. Obesity-related lipid profile and altered insulin incretion in adolescents with polycystic ovary syndrome. Clinical, ultrasound and biochemical features of polycystic ovary syndrome in adolescents: implications for diagnosis. Maternal youth and pregnancy outcomes: middle school versus high school age groups compared with women beyond the teen years. Does young maternal age increase the risk of adverse obstetric, fetal and neonatal outcomes: a cohort study. Joint effect of obesity and teenage pregnancy on the risk of preeclampsia: a population-based study. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Body mass index in adolescence in relation to cause-specific mortality: a follow-up of 230,000 Norwegian adolescents. Effect on dietary weight loss on menstrual regularity in obese young adult women with polycystic ovary syndrome. The impact of metformin, oral contraceptives, and lifestyle modification on polycystic ovary syndrome in obese adolescent women in two randomised, placebo-controlled clinical trials. Cyproterone acetate/ethinyl estradiol for acne and hirsutism: time to revise prescribing policy. Treatment with metformin would be expected to improve insulin sensitivity and the metabolic and reproductive functions. Nevertheless, metformin administration over a period of 6 months in the context of a diet and lifestyle changes program was not better than placebo regarding body-weight reduction [134]. A more recent study, however, has shown that with metformin, the weight loss was greater than that with lifestyle changes, although there was a high dropout rate [136]. Understanding variation in prevalence estimates of polycystic ovary syndrome: a systematic review and meta-analysis. Body mass index and ovarian function are associated with endocrine and metabolic abnormalities in women with hyperandrogenic syndrome. Abdominal fat quantity and distribution in women with polycystic ovary syndrome and extent of its relation to insulin resistance. A prospective study of the prevalence of the polycystic ovary syndrome in unselected Caucasian women from Spain. Differences in clinical and endocrine features between obese and non-obese subjects with polycystic ovary syndrome: an analysis of 263 consecutive cases. Characteristics of obesity in polycystic ovary syndrome: etiology, treatment, and genetics. The independent effects of polycystic ovary syndrome and obesity on serum concentrations of gonadotrophins and sex steroids in premenopausal women.

Purchase ashwagandha us
After the surgery anxiety symptoms palpitations buy cheap ashwagandha 60caps, oral contraceptives may have a reduced efficacy due to malabsorption. Oral progestogen-only preparations do not seem to increase the cardiovascular risk on preoperative obese patients. Due to possible absorption problems, a reduction of efficacy will have to be expected. Barrier method Barrier methods, including male and female condoms, cervical caps, and diaphragms, are an effective method of contraception if used correctly. Above that condoms offer an additional protection against sexually transmitted diseases. American Society for Metabolic and Bariatric Surgery position statement on the impact of obesity and obesity treatment on fertility and fertility therapy endorsed by the American College of Obstetricians and Gynecologists and the Obesity Society. Intrauterine devices and endometrial cancer risk: a pooled analysis of the Epidemiology of Endometrial Cancer Consortium. Longacting reversible contraception: the effective and appropriate use of long-acting reversible contraception. The levonorgestrel-releasing intrauterine system: safety, efficacy, and patient acceptability. Differentiation of Kyleena, Jaydess and Mirena intrauterine delivery systems (levonorgestrel). Menstrual concerns and intrauterine contraception among adolescent bariatric surgery patients. Levonorgestrel-releasing and copper intrauterine devices and the risk of breast cancer. Long-acting reversible contraception: the effective and appropriate use of long-acting reversible contraception. The contraceptive efficacy of Implanons: a review of clinical trials and marketing experience. Effects of progestin-only long-acting contraception on metabolic markers in obese women. Progestogen-only contraceptives and the risk of acute myocardial infarction: a meta-analysis. Follicular development and ovulation in extremely obese women receiving depo-medroxyprogesterone acetate subcutaneously. Multinational comparative clinical evaluation of two long-acting injectable contraceptive steroids: norethisterone oenanthate and medroxyprogesterone acetate. Pharmacokinetics of a combined oral contraceptive in obese and normal-weight women. Metabolism and pharmacokinetics of contraceptive steroids in obese women: a review. The gut wall metabolism of ethinyloestradiol and its contribution to the pre-systemic metabolism of ethinyloestradiol in humans. Sex hormone levels and intestinal absorption of estradiol and D-norgestrel in women following bypass surgery for morbid obesity. Plasma concentrations of etonogestrel in women using oral desogestrel before and after Roux-en-Y gastric bypass surgery: a pharmacokinetic study. Long-term (7 years) follow-up of Roux-en-Y gastric bypass on obese adolescent patients (,18 years). These obesity-related characteristics should be taken into account regarding the efficacy, health risks, side effects, and benefits of contraceptive methods [11]. Obesity can lead to the following consequences, and they must be considered by the clinician and the woman when deciding upon the optimal method of contraception: 1. Increased risk of eclampsia, preterm birth, cesarean delivery, postpartum hemorrhage, and thromboembolic events during pregnancy and in the postpartum period [2]. The beneficial protective effect on endometrial carcinoma and reduction of heavy menstrual bleeding in general do not outweigh the risks. In addition, it should be kept in mind that although effectiveness studies are controversial, pharmacokinetic studies as explained earlier give indirect evidence of lower plasma values that may have a negative impact on efficacy. Their principal mode of action is through the local inflammatory and spermicidal effect of copper ions. The most frequently used are ParaGard, Flexi T, Multiload, T-Safe, and GyneFix [13]. In clinical trials, there is so far no evidence that the side-effect profile would be any different. Additional health benefits Obese women have a higher risk of endometrial carcinoma. Contraindications G Health risks No major health risks are reported except for rare complications in the context of use. The risk of complications during placement is minimal and includes uterine perforation (0. There is no evidence of increased risk of expulsion and perforation, although insertion maybe sometimes challenging. There are no metabolic impacts especially related to diabetes or metabolic syndrome. Severe uterine distortion-Anatomic abnormalities, including bicornuate uterus, cervical stenosis, or fibroids, severely distort the uterine cavity because of increased difficulty with insertion and increased risk of expulsion [11,13]. As obese women have a higher likelihood of heavy menstrual bleeding, there is a theoretical possibility that blood loss during menstruation may be higher than in Long-term contraceptive care in obese and superobese women Chapter 7 69 Practical issues in obese women Visualizing the cervix and determining the size and direction of the uterus can be challenging in severely obese women during insertion of the device. Optimizing equipment by selecting a large speculum or removing the tip of a condom and placing it over the blades of the speculum can help with the visualization of the cervix. Another limitation is the nonacceptance of intrauterine contraception (foreign body in the uterus) by the woman. However, two analyses of a large Finnish cohort suggest a small increased risk (up to 1. Taking into account the different results and the type of studies (observational studies), it can be concluded that the use of a progestogen-only method is either not, or to a minor degree (expressed as absolute risk), accompanied by an increased risk for breast cancer [13,14]. Taking into account the possible association between obesity and breast cancer risk, this remains an issue for future studies among progestogen-only users. Serum concentrations of progestin can lead to partial inhibition of ovarian follicular development and ovulation. Contraindications include those for intrauterine contraceptives and current/active breast cancer (category 4) or (category 3) for women with a personal history of breast cancer in the past 5 years with no active disease [12,13]. The matrices are inert or biologically degradable rods or capsules that release the respective steroid continuously over a lengthy period of time. The hormone implants consist of one or several small flexible rods or a capsule inserted under the skin of the upper arm. Health benefits Reduction in heavy menstrual bleeding and dysmenorrhea in patients without organic pathology and bleeding due to bleeding diathesis, including anticoagulation therapy. The efficacy regarding reduction of bleeding intensity in women with fibroids and adenomyosis is yet unclear and under investigation [11]. Amenorrhea can be expected up to 45% in women 6 months after insertion and up to 50% after 12 months. The concentration falls over time at a rate that depends on body weight, due the increased volume of distribution, effects on plasma protein binding, and altered clearance in individuals with obesity. No pregnancies occurred during the period of prolonged use, leading to an estimated failure rate of 0 (97. Nonetheless, there remains some controversy about the practical use of the implant with respect to efficacy. The implant has minimal clinically nonrelevant impact on fasting glucose and insulin in obese women. In women with diabetes, HbA1c did not change in implant users, neither did the daily insulin requirement [44].
Buy discount ashwagandha line
Public education and risk communication the novel and largely unpredictable effects of biological weapons are likely to increase the uncertainty surrounding a bioterrorism incident anxiety attacks symptoms purchase ashwagandha 60caps on-line. Public education and effective risk communication are essential in order to bolster public confidence and improve cooperation with the authorities. Clinicians and public health personnel should have access to up-to-date information. The general public should be provided with nontechnical descriptions of the diseases and simple instructions on how to act in an emergency situation. Risk communication associated with a bioterrorist event can be divided into five stages: prior to the event, on suspicion of an event, on confirmation of the event, during the event, and following the event. Since the authorities may possess very little factual information, the public might suspect that information is being withheld, resulting in hostility. Thus, it is important that the public messages be reassuring while sharing uncertainties. This can be exacerbated by rumours Postexposure prophylaxis Postexposure prophylaxis is appropriate for some, but not all, bioterrorism agents. A variety of problems should be anticipated during an outbreak, including atypical presentations of cases and varying responses to treatment and prophylaxis. Discovery of new exposure foci and reports of disease in apparently unexposed people could cause disquiet and mistrust. There might be inadequate isolation of patients and a breakdown of the implementation of quarantine. Untried new treatments might be proposed by unauthorized professionals or lay people. Following a bioterrorist incident, residual public fear and anxiety is likely to persist. Inevitably, there will be questions about the extent to which the authorities were able to control the incident, criticism of actions taken or not taken, and general recriminations. Public messages should be broadcast about the lessons learned from the incident and actions that will be taken to address deficiencies. It is essential that the authorities maintain transparency in order to strengthen public trust. Likely future developments the threat of bioterrorism is likely to increase, demanding greater resources to deter attacks and improve surveillance, vaccines, and medications. Reducing the motivation for terror and banning internationally the use of biological weapons should be promoted at all levels. Sensible preparedness for bioterrorist incidents is a deterrent in itself and ensures that public health systems and society will deal effectively with an incident. Such measures will also improve general emergency preparedness and the control of infectious diseases. Decontamination Decontamination is relevant, mainly for anthrax and smallpox, in the environment of an aerosol attack and at places where patients were treated. Bedding and clothing of patients should be sterilized or disposed of where indicated. Low humidity and temperature prolong survival of the smallpox virus in the environment, and on scab material; it can remain viable for months. Sensitive detection of Francisella tularensis directly from whole blood by use of the GeneXpert System. Rapid Detection of Bacillus anthracis bloodstream infections by use of a novel assay in the GeneXpert System. Risk communication, the West Nile virus epidemic, and bioterrorism: responding to the communication challenges posed by the intentional or unintentional release of a pathogen in an urban setting. Legal and ethical aspects Bioterrorism preparedness requires the necessary legislation to enable the public health authorities to carry out measures with adequate legal backing. Laws that are of particular importance relate to closing buildings, taking over hospitals, ordering isolation and quarantine, and active surveillance of presumed infected individuals and their contacts. Ethical issues might arise in the triage of patients for admission to overburdened hospital wards and intensive care units. Areas of uncertainty or controversy Bioterrorism incidents have so far been very rare, and preparedeness is based on an assumption that the potential risk is both real and severe. There are some concerns that the investment of large resources in bioterrorism preparedness could come at the expense of other essential public health activities. Research should be encouraged to assess the risks, costs, and benefits of the preparedness activities, in order to strike a reasonable balance. New surveillance systems, particular those based on syndromic surveillance, might be insufficiently specific and too much of a burden on the health services to be sustainable for long. Uncertainty remains about the efficacy of vaccines and antimicrobial therapy in the event of an outbreak. Simultaneous immunodetection of anthrax, plague, and tularemia from blood cultures by use of multiplexed suspension arrays. Implementing a negative-pressure isolation ward for a surge in airborne infectious patients. Comparison of MagPix assays and Enzyme-Linked Immunosorbent Assay for detection of hemorrhagic fever viruses. Rapid detection of viable Bacillus anthracis spores in environmental samples by using engineered reporter phages. A bivalent Anthrax-Plague vaccine that can protect against two Tier-1 bioterror pathogens, Bacillus anthracis and Yersinia pestis. Burkholderia pseudomallei and Burkholderia mallei vaccines: Are we close to clinical trials Less commonly, symptoms may arise only after prolonged exposure, as occurs with many heavy metals. It must be stressed that exposure does not necessarily equate with poisoning as uptake of the agent involved is required but, even if this occurs, poisoning does not necessarily result as the amount absorbed may be too small. Poisoning may be accidental or deliberate; it is usually accidental in small children, but in adults it is almost invariably deliberate. Diagnosis is based on the history, circumstantial evidence (if available), the presence of typical features, and, occasionally, on the results of toxicological and other investigations. Biochemical abnormalities due to disturbed metabolic processes are common in severely poisoned patients. These may be of diagnostic value, but mostly their recognition and treatment are important in management. Plasma electrolyte abnormalities, particularly hypo- or hyperkalaemia, are observed and are most often due to redistribution of potassium across cell membranes. Management Initial management involves the treatment of any potentially lifethreatening conditions, such as airway compromise, breathing difficulties, haemodynamic instability, and clinically significant arrhythmias. There is no evidence that the use of methods to reduce absorption from the gastrointestinal tract- such as activated charcoal, gastric lavage, syrup of ipecacuanha, cathartics, or whole-bowel irrigation- improves the clinical outcome in poisoned patients. However, activated charcoal and gastric lavage may be considered in patients who have ingested life-threatening amounts of a toxic agent up to 1 h previously. Antidotes exert their beneficial effects by a variety of mechanisms, including forming an inert complex with the poison, accelerating detoxification of the poison, reducing the rate of conversion of the poison to a more toxic compound, competing with the poison for essential receptor sites, blocking essential receptors through which the toxic effects are mediated, and bypassing the effect of the poison. There are, however, only a small number of poisons for which there is a specific antidote, and few antidotes are employed regularly in clinical practice; these include acetylcysteine, naloxone, and flumazenil. To increase poison elimination, treatment with multiple-dose activated charcoal (in patients who have ingested carbamazepine, dapsone, phenobarbitol, quinine, or theophylline), urine alkalinization Clinical assessment Assessment of a poisoned patient involves taking an appropriate history and performing a physical examination (including an assessment of the level of consciousness, ventilation, and circulation). Most countries have a poisons information service, which provides advice to medical staff Advice should always be sought if unfamiliar poisons are encountered or if there is clinical uncertainty about optimal management. Epidemiology Poisoning, either accidental or deliberate, is a common presentation in all countries throughout the world. Before the 1950s, hospital admissions from self-harm, now the most frequent cause of poisoning presentation to healthcare, was extremely rare worldwide. Patients who have suffered toxic exposures present to healthcare facilities in a variety of ways, including to primary care physicians, hospital emergency departments, and hospital outpatients; rarely, patients are discovered dead. Collecting statistics on poisoning is, therefore, a complex issue and there is currently no universally agreed system for documenting and comparing rates of poisoning in different countries. Most statistics refer to hospital admissions (as opposed to hospital presentations in emergency departments) or poisoning-related deaths.
Syndromes
- IgG subclass measurements
- Throat pain - severe
- Tell your doctor if you are using quick-relief medicines twice a week or more. Your asthma may not be under control and your doctor may need to change your dose of daily control drugs.
- Bleeding does not stop after usual treatments
- Male hormones (such as testosterone) taken or encountered by the mother during pregnancy.
- Testicular torsion
- For a closing wedge osteotomy, the surgeon may remove a wedge of your shinbone from underneath the healthy side of your knee.
- Infection or bleeding
- Liver function tests
Discount ashwagandha 60caps amex
In this chapter anxiety symptoms weak legs ashwagandha 60 caps discount, we will focus on the common potential gynecological causes of chronic pelvic pain. The female-specific obesity ranges are a waist circumference greater than 88 cm (35 in. Unfortunately, the most appropriate tool to assess and identify obesity has not been agreed upon. The relationship between chronic pelvic pain and obesity is poorly researched, with no identifiable studies specifically addressing these two entities. Therefore most of the information regarding obesity and chronic pelvic pain are extrapolated from studies of other chronic pain syndromes. Obesity and pain physiology Pain is felt when nociceptors are stimulated, transmitting impulses via the spinal cord, thalamus, and limbic system, and to the cerebral cortex of the brain where it is perceived [15]. Along the entire pathway, from the offending area to the cerebral cortex where pain is interpreted, various chemical mediators are released that can interact with and manipulate the pain signal. Appetite and hunger are also under signaling peptide control and some of the most well-known regulators of body habitus homeostasis demonstrate an involvement with inflammation and pain signal modulation. Use sedating analgesics cautiously in patients with preexisting or at risk of breathing disorders Consider comorbidities with analgesic selection. Antidepressants such as amitriptyline may be appropriate in patients with concomitant depression. Use sedating analgesics cautiously in patients with preexisting or at risk of breathing disorders Consider awake cystoscopy in high-risk patients Adenomyosis Abdominal myofascial syndrome Associated with pelvic organ prolapse and obesity Palpation abdominal and pelvic floor muscles are obscured by subcutaneous fat Pelvic assessment is impeded by subpar positioning and instruments Analgesia doses may need adjusting, Ghrelin is a neuropeptide hormone secreted from the stomach to increase hunger and is involved in glucose metabolism. It also increases the production of nitric oxide synthase which in turn modulates -opioid receptors to produce an antinociceptive effect [19]. The result is an increased level of inflammation and heightened susceptibility to pain in obesity due to a reduction of the protective antinociceptive and antiinflammatory effects of ghrelin. It stimulates glucocorticosteroid production, gluconeogenesis, and glycogen storage. It further contributes toward obesity through its interactions with leptin, ghrelin, and insulin-like growth factor. The orexinergic system consists of neuropeptides, orexin A, and orexin B that stimulate the appetite and can reduce the perception of pain [26]. In times of stress, such as acute or chronic pain, the orexin system is stimulated. This reaction is part of the fight or flight response to inhibit the transmission of pain signals and improve physical performance [27]. Via the orexinergic system, chronic pain can stimulate the appetite and contribute to weight gain. As a result of these associations, obesity is increasingly being considered a proinflammatory state [17]. Obesity also appears to contribute to the risk of developing neuropathic pain disorders. Finally, the prevalence of obesity is demonstrably higher among chronic pain sufferers [37]. This can lead to weight gain and deconditioning, which further hinders physical activity [38]. This vicious cycle of decreased activity, weight gain, and decondition can be difficult to break. Alternately, excessive weight may cause structural changes in the body that can result in an increased risk of developing chronic pain [39]. Quality-of-life surveys show that weight loss can significantly improve bodily pain scores [40,41]. The genetics of obesity and chronic pain It is generally well established that genetics play a contributing role in the obesity epidemic [42]. Twin studies from the United Kingdom and Australia agree that there is likely a hereditable component to chronic pelvic pain [47,48]. No studies have been conducted to investigate any genetic associations between obesity and chronic pelvic pain; however, there is a growing body of research demonstrating a genetic link between obesity and pain. A systematic review of twin studies and lower back pain demonstrates a strong genetic association with obesity [49]. Another suggested shared etiological pathway for the development of both chronic pain and obesity may be due to glucocorticoid receptor gene polymorphisms [53]. Many of the comorbidities of chronic pain or obesity are also implicated including type 2 diabetes, metabolic syndrome, anxiety, depression, hypertension, atherosclerosis, cardiovascular disease, and inflammatory autoimmune disorders [53]. The impact of obesity on the assessment of chronic pelvic pain the assessment of chronic pelvic pain usually requires a physical examination of the abdomen, bimanual palpation to assess the pelvic organs and the location of any tenderness, and speculum inspection of the vaginal walls and cervix. Rectal examination, pelvic floor assessment, and mobility assessments can also be performed as necessary. A thorough pelvic examination is essential in distinguishing between different etiologies and will also include an assessment for central sensitization which frequently accompanies chronic pelvic pain syndromes [74]. However, the presence of extra adiposity around the abdomen, pelvis, buttocks, and thighs will increase the difficulty and limit the effectiveness of pelvic examinations. Achieving a comfortable position for the patient, the ability to identify pelvic organs, and the visibility of vaginal structures are all increasingly hampered by increasing thickness of subcutaneous tissue. A study of physician attitudes toward the assessment of obese patients highlights these issues. The lack of appropriate equipment, such as larger instruments and bariatric examination couches, can contribute to the problem. Women with chronic pelvic pain and obesity and of low socioeconomic status all appear to have similar pitfalls and barriers to overcome. Access to healthcare services, the relationship with their primary care provider and gynecologist, trust in healthcare professionals, communication with healthcare professionals, frequent comorbidities, and fear of negative labels are prevalent in all three groups [71,76]. It stands to reason that these factors may compound and present even higher barriers to women in overlapping groups. The reliance on imaging in the assessment of chronic pelvic pain in the obese population is increasing due to the difficulties with clinical examination. Ultrasound is the most widely used imaging modality as it is readily available and relatively inexpensive. However, a greater depth of insonation and adjusting for the reduced signal amplitude produced by the attenuation of the ultrasound beam by fat is required for obese individuals. This helps to mitigate the effects of obesity on the quality of the image produced [77]. This can be done by reducing mean array emission frequency to improve penetration or by using filters such as harmonic or compound imaging to increase the signal-to-background noise ratio [78]. Care must be taken to avoid awkward positions which can result in muscular strain injuries [77]. The psychological impact of obesity and chronic pelvic pain There is at least a moderate link between psychiatric disorders, mainly anxiety and depression, and both obesity and chronic pelvic pain. One explanation may be "body image"-the way a person perceives their own physical appearance. Obesity is at least modestly associated with body image distortion and body image dissatisfaction [55]. Chronic pain sufferers also demonstrate an element of body image distortion [61,62]. Nevertheless, there are currently very few studies assessing the psychological effect of having both chronic pelvic pain and obesity. Further insights into the connection between obesity, chronic pelvic pain, and psychopathology may be provided by reviewing the greater medical literature on chronic pain syndromes. Weight loss treatment enhances the quality of life and improves pain management in chronic pain sufferers [40,41,68].

Buy ashwagandha overnight delivery
They respond to specific signals and chemokines that draw them not to the paracortex but to the lymph node follicles anxiety upper back pain buy discount ashwagandha on-line. B cells differ from T cells in that their receptors can recognize free, unprocessed antigen. A B cell typically meets its antigen in a lymph node follicle, or B-cell follicle. Small, soluble antigens can make their way directly into the follicle, whereas larger antigens are relayed to the follicular dendritic cells by subcapsular macrophages and non-antigen-specific B cells (see Chapter 14). Some activated B cells differentiate directly into antibody-producing cells (plasma cells), but others re-enter the follicle to establish a germinal center. A follicle that develops a germinal center is referred to as a secondary follicle; a follicle without a germinal center is referred to as a primary follicle. Some of these cells travel to the medulla of the lymph node and release antibodies into the bloodstream; others exit through the efferent lymphatics and take up long-term residence in the bone marrow, where they will continue to release antibodies into circulation. Germinal centers are established within 4 to 7 days of the initial infection, but remain active for 3 weeks or more (Chapter 11). Lymph nodes swell visibly and sometimes painfully during those first few days after infection as immune cells migrate into the node and T and B cells proliferate. Memory T and B cells either take up residence in secondary lymphoid tissues or exit the lymph node and circulate to and among other tissues, including those that first encountered the pathogen. Memory T cells that reside in secondary lymphoid organs are referred to as central memory cells and are distinct in phenotype and 160 functional potential from effector memory T cells that circulate among tissues. A third population, tissue-resident memory cells, settle in peripheral tissues for the long term and appear to be the first cells to respond when an individual is re-infected with a pathogen. Memory cell phenotype, locale, and activation requirements are very active areas of investigation and will be discussed in more detail in Chapters 10 and 11. Key Concepts: the lymph nodes organize the immune response to antigens that enter through lymphatic vessels. T cells and B cells are compartmentalized in different microenvironments in secondary lymphoid tissue. T cells are found in the paracortex of the lymph nodes, while B cells are organized in follicles in the cortex. If they do not, they exit via the efferent lymphatics and continue browsing in other lymph nodes. Those that do not exit the lymph node via the efferent lymphatics to browse another secondary lymphoid tissue. Activated B cells undergo further maturation into high-affinity, antibody-producing cells in specialized microenvironments called germinal centers, substructures that develop within B-cell follicles. Some memory cells remain in lymphoid tissue, some circulate, and some take up residence in other tissues, ready to respond quickly to a returning pathogen. Whereas lymph nodes are specialized for encounters between lymphocytes and antigen drained from local tissues, the spleen specializes in trapping and responding to blood-borne antigens; thus, it is particularly important in the response to systemic infections. Instead, bloodborne antigens and lymphocytes are carried into the spleen through the splenic artery and out via the splenic vein. Experiments with radioactively labeled lymphocytes show that more recirculating lymphocytes pass daily through the spleen than through all the lymph nodes combined. The splenic artery pierces the capsule and divides into progressively smaller arterioles, ending in vascular sinusoids that drain back into the splenic vein. The spleen is surrounded by a capsule that extends into the interior, dividing the spleen into lobes, all of which function similarly. The splenic red pulp consists of a network of sinusoids populated by red blood cells, macrophages, and some lymphocytes. It is the site where old and defective red blood cells are destroyed and removed; many of the macrophages within the red pulp contain engulfed red blood cells or iron-containing pigments from degraded hemoglobin. It is also the site where pathogens first gain access to the lymphoid-rich regions of the spleen, known as the white pulp. As in lymph nodes, germinal centers are generated within these follicles during an immune response. The spleen also maintains a fibroblastic reticular network that provides tracts for T-cell and B-cell migration. These cells are the first line of defense against blood-borne pathogens, trapping antigens that enter via the splenic artery. Interestingly, mouse and human marginal zone anatomy differ, as does the phenotype and behavior of their marginal zone B cells. The basis for and significance of this species-specific difference are under investigation. The events that initiate the adaptive immune response in the spleen are analogous to those that occur in the lymph node. As in the lymph node, germinal center B cells can become memory cells or plasma cells, which circulate to a variety of tissues including the bone marrow. Although fewer adverse effects are experienced by adults, splenectomy can still lead to an increased vulnerability to blood-borne bacterial infections, underscoring the role the spleen plays in our immune response to pathogens that enter the circulation. Because the spleen also serves other functions in iron metabolism, platelet storage, and hematopoiesis, these are also compromised if it is removed. Key Concepts: the spleen organizes the first immune response to blood-borne pathogens. The spleen is compartmentalized into the white pulp, which contains B and T lymphocytes, and the red pulp, which contains circulating red blood cells. The periarteriolar lymphoid sheath of the white pulp includes B-cell follicles and T-cell zones. The splenic marginal zone, a specialized region of macrophages and B cells, forms a boundary between the red and the white pulp and plays an important role in trapping and responding to blood-borne antigens. Barrier Organs Also Have Secondary Lymphoid Tissue Lymph nodes and the spleen are not the only organs with secondary lymphoid microenvironments. T-cell zones and lymphoid follicles are also found in barrier tissues, which 163 include the skin and mucosal membranes of the digestive, respiratory, and urogenital tracts. Our mucosal membranes are lined with a single epithelial layer, while our skin is protected by many layers of epithelial cells. Together, skin and mucosal membranes represent a surface area of over 400 m2 (nearly the size of a basketball court) and are the major sites of entry for most pathogens. Each of these tissues plays an important role in our innate immune defenses and recruits many different cell types to the effort. The epithelial cell layers provide more than just physical protection; they also respond actively to pathogens by secreting cytokines, chemokines, and even antimicrobial compounds. Many different types of immune cells reside in the deeper layers of barrier tissues and generate B-cell follicles. B cells that develop in these follicles tend to secrete IgA, which has the ability to cross epithelial barriers and interact with microbes in the lumen of our mucosal tracts. Innate and adaptive immune cells in barrier organs not only organize our first response to invading pathogens, but they also play a critical role in maintaining tolerance to the diverse and abundant commensal microbes that contribute positively to our health. The single layer of epithelial cells includes specialized cells, called M cells, that convey antigens from the intestinal lumen to the inner layers (lamina propria) of the intestinal wall. Here they trigger the formation of B-cell follicles, which generate antibody-producing plasma cells. The antibodies pass back into the intestinal lumen and bind to pathogens, protecting the intestinal wall from inflammation and invasion. Other cells, including macrophages, dendritic cells, and intraepithelial lymphocytes, sample antigens from the lumen and, with the help of regulatory T cells, work to distinguish between beneficial commensal bacteria and more dangerous pathogens. Antigen-presenting cells and lymphocytes can travel to local lymph nodes, where they trigger a more systemic immune response to antigens. Key Concepts: Barrier immune organs, which include the skin and mucosal tissues, contain secondary lymphoid tissue and mount an important first defense against pathogens that penetrate our epithelial layers. Epithelial cells play an active role and initiate the response of innate and adaptive immune cells, which can organize into B-cell follicles. Barrier immune systems also help us maintain tolerance to commensal microbes that coexist at our surfaces.
Purchase 60 caps ashwagandha
First anxiety from weed purchase ashwagandha, the death of infected macrophages prevents further spread of intracellular bacteria, such as Salmonella and Listeria, that replicate in these cells. Local Inflammation Is Triggered by Innate Immune Responses 320 When the outer barriers of the innate immune system-skin and other epithelial layers-are damaged, the resulting innate responses to infection or tissue injury can induce a complex cascade of events known as the inflammatory response. Inflammation may be acute (short-term effects contributing to combating infection, followed by healing)-for example, in response to local tissue damage-or it may be chronic (long term, not resolved), contributing to conditions such as arthritis, inflammatory bowel disease, cardiovascular disease, and type 2 diabetes. The hallmarks of a localized inflammatory response were first described by the Roman physician Celsus in the first century A. Today we know that these symptoms reflect an increase in vascular diameter (vasodilation), resulting in a rise of blood volume in the area. Vascular permeability also increases, leading to leakage of fluid from the blood vessels, resulting in an accumulation of fluid (edema) that swells the tissue. Within a few hours, leukocytes also enter the tissue from the local blood vessels. These hallmark features of inflammatory responses result from the activation of innate immune responses in the vicinity of the infection or wound. Bacterial entry through wounds activates initial innate immune mechanisms, including activation of phagocytosis by resident cells, such as macrophages and dendritic cells. Recognition of bacteria by cellular pattern receptors initiates production of cytokines, chemokines and other mediators, triggering changes in vascular endothelial cells that lead to an influx from the blood of fluid (containing antimicrobial substances) and phagocytes (first neutrophils and then monocytes) to the site of infection. These and subsequent events cause the redness, swelling, heat, and pain that are characteristic of local inflammatory responses. The recruitment of various leukocyte populations from the blood into the site of infection or damage is a critical early component of inflammatory responses. Fluid enters the tissue, delivering antimicrobial molecules such as complement components and causing swelling. Cells flowing through the local capillaries are induced by chemokines and cell adhesion molecule interactions to adhere to vascular endothelial cells in the inflamed region and pass through the walls of capillaries and into the tissue spaces, a process called extravasation that will be described in Chapter 14. Neutrophils are the first to be recruited to a site of infection, where they enhance local innate responses, followed by monocytes that differentiate into macrophages; the macrophages participate in clearance of pathogens and cellular debris and help initiate wound healing. Key early components of inflammatory responses are increased vascular permeability, allowing soluble innate mediators to reach the infected or damaged site, and the recruitment through the action of chemokines of neutrophils and monocytes from the blood into the site. This mechanism of cell-mediated cytotoxicity is also carried out by cytotoxic T cells, as a part of the adaptive response that occurs days later (see Chapter 12). These early innate responses control the infection for the days to week it takes for the adaptive response (antibodies and cytotoxic T cells) to be generated. Members of one group serve as activating receptors (of which more than 20 have been described in humans and mice) that have specificity for various cell surface ligands that serve as indicators of infection, cancer, or stress. As illustrated by these conditions, and by the many known roles (cited throughout this chapter) of innate and inflammatory mechanisms in protecting us against pathogens, these responses are essential to keeping us healthy. Some disorders show that innate and inflammatory responses can also be harmful, in that overproduction of various normally beneficial mediators and uncontrolled local or systemic responses can cause illness and even death. Therefore it is important that the occurrence and extent of innate and inflammatory responses be carefully regulated to optimize the beneficial responses and minimize the harmful responses. The adverse effects of mutations in genes encoding essential components of innate and inflammatory processes highlight the critical roles of these proteins in keeping us healthy. Since 2003, when the first mutations in innate immune components that predispose individuals to recurrent bacterial infections were discovered, a number of mutations interfering with the generation of protective innate immune responses have been identified. Proteins in which genetic mutations have been identified that result in defective functions and are associated with greater 329 susceptibility to viral diseases are shown in red. These devastating syndromes include many signs of systemic inflammation, including fever, rashes, arthritis, pain, and inflammation affecting the nervous system, with adverse effects on vision and hearing. Novel primary immunodeficiencies revealed by the investigation of paediatric infectious diseases. However, this does not always occur-a variety of conditions result from excessive or chronic innate and inflammatory responses. Several hundred thousand cases of sepsis occur annually in the United States, with mortality rates ranging from 20% to 50%, but sepsis can lead to septic shock- circulatory and respiratory collapse that has a 90% mortality rate. Sepsis results from septicemia, infections of the blood, in particular those involving gram-negative bacteria such as Salmonella and E. They, in turn, systemically activate vascular endothelial cells, inducing them to produce cytokines, chemokines, adhesion molecules, and clotting factors that amplify the inflammatory response. Enzymes and reactive oxidative species released by activated neutrophils and other cells damage the vasculature. These effects on the blood vessels are particularly damaging to the kidneys and lungs, which are highly vascularized. Thus the systemic inflammatory response triggered by septicemia can lead to circulatory and respiratory failure, resulting in septic shock and death. Much still needs to be learned about sepsis and septic shock to enable the development of effective treatments. While not as immediately dangerous as septic shock, chronic inflammatory responses resulting from ongoing activation of innate immune responses can have adverse consequences for our health. For example, a toxin from Helicobacter pylori bacteria damages the stomach by disrupting the junctions between gastric epithelial cells and also induces chronic inflammation that has been implicated in peptic ulcers and stomach cancer. Other examples of harmful sterile (noninfectious) inflammatory responses discussed earlier-including gout, asbestosis, silicosis, and aseptic osteolysis-are induced, respectively, by crystals of monosodium urate, 331 asbestos, and silica, and by metal alloy particles from artificial joint prostheses. Additional examples of chronic inflammatory conditions will be presented in Chapter 15. Key Concept: Infection of the blood can cause sepsis and the systemic expression of proinflammatory cytokines. Left unchecked, systemic inflammation leads to septic shock, a highly fatal condition. Innate and Inflammatory Responses Are Regulated Both Positively and Negatively Innate immune responses play essential roles in eliminating infections, but they also can be harmful when not adequately controlled. It is therefore not surprising that many regulatory processes have evolved that either enhance or inhibit innate and inflammatory responses. These mechanisms control the induction, type, and duration of these responses, in most cases resulting in the elimination of an infection without damaging tissues or causing illness. Positive Regulatory Mechanisms Innate and inflammatory responses are increased by a variety of mechanisms to enhance their protective functions. Negative Regulatory Mechanisms On the other side of the equation, as uncontrolled innate and inflammatory responses can have adverse consequences, many negative feedback mechanisms are activated to limit these responses. The activation of these and other intracellular negative feedback mechanisms can lead cells to become less responsive, limiting the extent of the innate immune response. Each of these cytokines induces production of a soluble version of its receptor or a receptor-like protein that binds the circulating cytokine molecules, preventing the cytokines from acting on other cells. One example may explain how influenza virus infection causes increased susceptibility to bacterial infections that cause pneumonia. Key Concept: As innate and inflammatory responses can be harmful as well as helpful, they are highly regulated by positive and negative feedback pathways that generally keep the responses at the appropriate level. Pathogens Have Evolved Mechanisms to Evade Innate and Inflammatory Responses Many pathogens have evolved mechanisms that allow them to evade elimination by the immune system by inhibiting various innate and inflammatory signaling pathways and effector mechanisms that would otherwise clear them from the body. Most bacteria, viruses, and fungi replicate at high rates and, through mutation, may generate variants that are not recognized or eliminated by innate immune effector mechanisms. Other pathogens have evolved complex mechanisms that block normally effective innate clearance mechanisms. A strategy employed especially by viruses is to acquire genes from their hosts that function as inhibitors of innate and inflammatory responses. However, innate immunity is not sufficient to protect us fully from infectious diseases, in part because many pathogens have features that allow them to evade innate immune responses, as discussed above. Hence the antigen-specific responses generated by our powerful adaptive immune system are usually needed to resolve infections successfully. While our B and T lymphocytes are the key producers of adaptive response effector mechanisms-antibodies and cell-mediated immunity (see Chapter 12)-it is becoming increasingly clear that our innate immune system plays important roles in helping to initiate and regulate adaptive immune responses so that they will be optimally effective. In addition, the adaptive immune system has coopted several mechanisms by which the innate immune system eliminates pathogens, modifying them to enable antibodies to clear pathogens.
Purchase ashwagandha on line amex
Other transcriptional regulators regulate myeloid versus lymphoid cell lineage choices anxiety relief techniques order ashwagandha 60caps with mastercard. For instance, Ikaros is required for lymphoid but not myeloid development; animals survive in its absence but cannot mount a full immune response. Activity of Notch1, one of four Notch family members, induces lymphoid progenitors to develop into T rather than B lymphocytes (see Chapter 8). Distinguishing Blood Cells Historically, investigators classified cells on the basis of their appearance under a microscope, often with the help of dyes. Their observations were especially helpful in distinguishing myeloid from lymphoid lineages, granulocytes from macrophages, and neutrophils from basophils and eosinophils. The pH-sensitive stains hematoxylin and eosin (H&E) are still commonly used in combination to distinguish cell types in blood smears and tissues. The basic dye hematoxylin binds basophilic nucleic acids, staining them blue, and the acidic dye eosin (named for Eos, the goddess of dawn) binds eosinophilic proteins in granules and cytoplasm, staining them pink. Microscopists drew astute inferences about cell function by detailed examination of stained and unstained cells. Fluorescence microscopy enhanced our ability to identify more molecular details, and in the 1980s, inspired the development of the flow cytometer. This invention revolutionized the study of immunology by allowing us to rapidly measure the presence of multiple surface and internal proteins on individual cells. In vivo cell imaging techniques now permit us to penetrate the complexities of the immune response in time and space. Together with our ever-increasing ability to edit animal and cell genomes, these technologies have revealed an unanticipated 123 diversity of hematopoietic cell types, functions, and interactions. While our understanding of the cell subtypes is impressive, it is by no means complete. Table 2-1 lists the major myeloid and lymphoid cell types, as well as their life spans and representation in our blood. As progenitors differentiate, they progressively lose their ability to self-renew as well as their ability to give rise to other cell lineages. Hematopoietic cells can be distinguished visually using hematoxylin and eosin stains or fluorescent markers. Flow cytometry takes advantage of monoclonal antibodies to distinguish individual cells on the basis of the many surface and internal proteins they express. Cells of the Myeloid Lineage Are the First Responders to Infection Myeloid lineage cells include all red blood cells, granulocytes, monocytes, and macrophages. The white blood cells within this lineage are innate immune cells that respond rapidly to the invasion of a pathogen and communicate the presence of an insult to cells of the lymphoid lineage (below). As we will see in Chapter 15, they also contribute to inflammatory diseases (asthma and allergy). All granulocytes have multilobed nuclei that make them visually distinctive and easily distinguishable from lymphocytes, whose nuclei are round. These granules contain a variety of proteins with distinct functions: some damage pathogens directly; some regulate trafficking and activity of other white blood cells, including lymphocytes; and some contribute to the remodeling of tissues at the site of infection. Note differences in the shape of the nucleus and in the number, color, and shape of the cytoplasmic granules. After differentiation in the bone marrow, neutrophils are released into the peripheral blood and circulate for 7 to 10 hours before migrating into the tissues, where they have a life span of only a few days. In response to many types of infection, innate immune cells generate inflammatory molecules. This transient increase in the number of circulating neutrophils is called leukocytosis and is used medically as an indication of infection. Neutrophils swarm in large numbers to the site of infection in response to inflammatory molecules (Video 2-4v). Once in the infected tissue, they phagocytose (engulf) bacteria and secrete a range of proteins that have antimicrobial effects and tissue-remodeling potential. Neutrophils are the main cellular components of pus, where they accumulate at the end of their short lives. Once considered a simple and "disposable" effector cell, neutrophils are now thought to play a regulatory role in shaping the adaptive immune response. Eosinophils contain granules that stain a brilliant pink in standard H&E staining protocols. They are thought to be important in coordinating our defense against multicellular parasitic organisms, including helminths (parasitic worms). Eosinophils cluster around invading worms, and damage their membranes by releasing the contents of their eosinophilic granules. They are most abundant in the small intestines, where their role is still being investigated. In areas where parasites are less of a health problem, eosinophils are better appreciated as contributors to asthma and allergy symptoms. Like neutrophils, eosinophils may also secrete cytokines that regulate B and T lymphocytes, thereby influencing the adaptive immune response. Like eosinophils, basophils are thought to play a role in our response to parasites, particularly helminths (parasitic worms). When they bind circulating antibody/antigen complexes basophils release the contents of their granules. Histamine, one of the best known compounds in basophilic granules, increases blood vessel permeability and smooth muscle activity, and allows immune cells access to a site of infection. Basophils also release cytokines that can recruit other immune cells, including eosinophils and lymphocytes. In areas where parasitic worm infection is less prevalent, histamines are best appreciated as a cause of allergy symptoms. They mature only after they leave the blood for a wide variety of tissues, including the skin, connective 126 tissues of various organs, and mucosal epithelial tissue of the respiratory, genitourinary, and digestive tracts. Like circulating basophils, these cells have large numbers of cytoplasmic granules that contain histamine and other pharmacologically active substances. Basophils and mast cells share many features, and basophils were once considered the bloodborne version of mast cells. However, recent data suggest that basophils and mast cells have distinct origins and functions. Note that macrophages are five- to tenfold larger than monocytes and contain more organelles, especially lysosomes. They become activated after making contact with a pathogen at the site of infection. They communicate this encounter to T lymphocytes in the lymph nodes by displaying peptides from the pathogen to lymphocytes, a process called antigen presentation (discussed in Chapter 7). They upregulate costimulatory molecules required for optimal activation of helper T cells. Macrophages are superb phagocytes and are especially efficient at removing both pathogen and damaged host cells from a site of infection. Monocytes regulate inflammatory responses at sites of tissue damage and infection. The functions of these subpopulations are under investigation; some will be described in more detail in coming chapters. They also provide a reservoir for tissue-resident monocytes in the absence of infection, and may quell rather than initiate immune responses. These inflammatory macrophages are expert phagocytes and typically participate in the innate immune response. Interestingly, recent work indicates that most tissue-resident macrophages actually arise early in life from embryonic cells rather than from circulating, activated monocytes. These resident macrophages, which include Kupffer cells in the liver, microglia in the brain, and alveolar macrophages in the lungs, have the ability to self-renew and form a committed part of the tissue microenvironment.
