
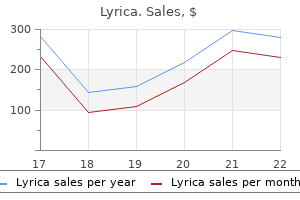
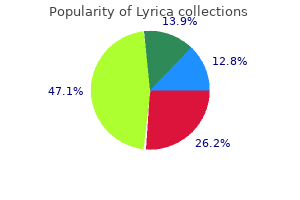
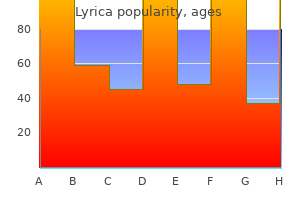
Generic 75mg lyrica with amex
Unfortunately mental conditions characterized excessive irrational buy lyrica 150 mg overnight delivery, once the kidney disease is moderate to severe in nature, renal pathologic examination may not always be helpful in determining the cause due to underlying fibrosis and sampling error. Hyponatremia and Hypernatremia the kidney plays an essential role in excreting water by producing a dilute urine (<1/6 serum osmolality) or retaining water by producing a concentrated urine (three to four times serum osmolality). Hyperkalemia the kidney plays the most critical role in the regulation of potassium balance. The degree of acidosis is usually mild to moderate with serum bicarbonate concentration ranging from 12 to 22 mEq/L. This stabilization of serum phosphorus is attributed to increased tubular excretion of phosphorus as a result of increased parathyroid hormone secretion. Serum calcium is usually in the normal range, but varies reciprocally with serum phosphorus. Because of derangements in divalent ion metabolism, bone disease with increased tendency to fractures and disordered soft tissue structures can be observed. The elevated parathyroid values are usually induced by hypocalcemia, although increased serum phosphorus concentrations independent of serum calcium values can also play a role. The increased parathyroid hormone levels can induce damage to bone and soft tissue structures, but also may affect cardiac function and production of red blood cells. Anemia the kidney is the source of erythropoietin, the hormone that regulates bone marrow production of red blood cells. Thus, with the development of renal impairment, there is a fall in red blood cell production. However, this relationship is not invariable, and many patients have only mild reductions in hemoglobin and hematocrit. The metabolic acidosis results from acid excretion falling below acid production, leading to positive proton balance. Uremic symptoms include nausea, vomiting, anorexia, metallic taste, pericarditis, peripheral neuropathy, central nervous system changes including difficulty with concentration, and seizures. Salt retention is a critical factor in the development of hypertension and can promote congestive heart failure. These patients should be carefully monitored for progression of renal disease every 6 months and should be aggressively treated for underlying diseases such as diabetes and hypertension within recommended guidelines. Again, it is rare at this stage for any significant clinical abnormalities other than hypertension to be present. At this stage, patients may develop hypertension, mild abnormalities in serum phosphorus, and normocytic-normochromic anemia. These patients need to be followed more closely, and it is recommended that patients in stage 3B be followed by a nephrologist every few months. Anemia is common and the patient may begin to note reductions in appetite and have a decrease in muscle mass. However, there is great variability in the appearance of symptoms or laboratory derangements. Patients who are transplant candidates should be referred to a transplant center for evaluation. Patients in stage 0 should be screened and treated for other comorbid conditions, such as diabetes mellitus, hypertension, and cardiovascular disease. Significant elevations in parathyroid hormone levels can cause bone pain, ruptured tendons, or other disorders of soft tissue. Hyperkalemia, if severe, can lead to arrhythmias or heart block and muscle weakness. Metabolic acidosis can contribute to fatigue and weight loss, development of bone disease, and increased mortality. Sexual dysfunction characterized by reduced libido and reduced fertility are common with moderate to severe renal failure. Understanding the methods to accomplish the former requires knowledge of those factors that are integral to progression of the disease. These adaptive mechanisms probably induce damage by causing endothelial cell damage with detachment of epithelial cells allowing enhanced flux of water and solutes that might cause narrowing of capillary lumens. It also produces strain on mesangial cells, causing them to produce cytokines and extracellular matrix with resultant expansion of the mesangium and glomerulosclerosis. Proteinuria Although proteinuria has traditionally been a marker of glomerular injury, with greater amounts of urinary protein excretion being associated with more severe injury, recent studies indicate that proteinuria can induce mesangial and tubular damage and is associated with increased cardiovascular disease, independent of traditional risk factors. It has been postulated that the tubulointerstitial disease can produce atrophy of tubules or obstruction, destroying individual nephrons. Even when tubular inflammation is treated, progressive scarring can continue unabated. Thus, treatments designed to reduce interstitial fibrosis may be important for preventing progression of disease. Hyperlipidemia Hyperlipidemia is frequently observed in disorders associated with nephrotic-range proteinuria, but it is also noted in a large percentage of the general population without renal disease. Thus, loading with cholesterol augments renal injury and treatment with cholesterol-lowering drugs slows the rate of progression. The mechanisms underlying the effects of lipids are not well understood, but possible explanations include mesangial lipid deposition leading to glomerular injury or tubular injury. A few studies performed in human subjects have demonstrated benefit from lipid lowering on the progression of renal injury, although they are not conclusive. Because patients with chronic renal failure have a high prevalence of cardiovascular disease, it is reasonable to initiate therapy with statin drugs to lower serum cholesterol and lipid levels. Measures Designed to Reduce the Rate of Progression of Renal Failure Control of Systemic and Intraglomerular Hypertension Experimental and human studies demonstrate that control of systemic hypertension can slow the rate of progression of renal disease substantially. Recent evidence indicates that target blood pressure levels should be lower than those recommended for the general population without adverse side effects. Control of hypertension with the use of myriad agents can benefit the patient with renal failure. However, as indicated previously, reduction in intraglomerular hypertension is the most important factor underlying the benefits of blood pressure control. Patients who do not tolerate these drugs might benefit from administration of non-dihydropyridine calcium channel blockers. If these complications occur, a dose reduction or even discontinuation might be required. The deposits can then induce an inflammatory response producing interstitial fibrosis and tubular atrophy. Some have indicated that the deposits may form before detectable elevations in serum phosphorus concentrations. The benefits of protein restriction in preventing progression are unclear, but it has been suggested that reducing protein intake to 0. In patients with substantial proteinuria, the quantity of protein recommended will have to be adjusted to prevent hypoalbuminemia. Reducing protein intake will have the added benefit of decreasing acid, potassium, and phosphate production. The increased prostanoids produce renal vasodilatation and a rise in intraglomerular pressure, factors that augment progression of disease. Recent studies also indicate that a reduction in the interstitial pH of the kidney can be observed even in the absence of a depressed serum bicarbonate concentration. Because iron stores need to be repleted for anemia to be successfully treated, they should be monitored closely. Because of the vagaries of ferritin measurements, we use serum iron and iron binding capacity with the goal of maintaining saturation above 20% and near 30%. Given the recent concern about vascular complications with erythropoietin therapy, the clinician must be vigilant in preventing hemoglobin values from exceeding 12 mg/dL. Some experts recommend raising serum bicarbonate to levels above 22 mEq/L, whereas others recommend complete normalization of serum bicarbonate. Divalent Ion Metabolism Serum phosphorus is controlled by administration of phosphate binders usually starting with calcium citrate (Citracal) or acetate (PhosLo). If these are not successful or if patients have elevated serum calcium levels, then sevelamer (Renagel) or lanthanum (Fosrenol) can be used alone or in combination with calcium binders. Suppression of parathyroid hormone secretion can be achieved by administration of various vitamin-D analogs in combination with calcimimetic agents such as cinacalcet (Sensipar). If levels are below 30 ng/mL, ergocalciferol or cholecalciferol should be given at sufficient doses to maintain it above this level.
Diseases
- Fronto-facio-nasal dysplasia
- Leukemia
- Night blindness
- Cowpox
- Optic atrophy opthalmoplegia ptosis deafness myopia
- Ohdo Madokoro Sonoda syndrome
- Graphite pneumoconiosis
- Short limb dwarf oedema iris coloboma
- Nicolaides Baraitser syndrome
- Prader Willi syndrome
Discount lyrica 150mg with visa
The process is known as a furuncle (boil) when the infection extends beyond the hair follicle xkcd mental illness cheap lyrica 150mg online. These lesions occur most frequently in the moist areas of the body and in areas subject to friction and perspiration. Host factors known to predispose one to folliculitis include obesity, blood dyscrasias, defects in neutrophil function, immune deficiency states. Pseudomonas species such as aeruginosa or cepacia are associated with hot-tub folliculitis, which involves numerous hair follicles. Successful treatment of folliculitis depends on correcting the predisposing factors that promote the development of this condition. For patients with localized disease, topical wound care including antibiotics such as mupirocin (Bactroban) is effective. Patients with furunculosis or multiple lesions with surrounding erythema of more than 2. This not only determines which type of Staphylococcus is causing the infection, but illustrates to the patient the importance of self-inoculation. Localization of purulent fluid necessitates surgical drainage and local wound care. The administration of oral or parenteral antibiotic therapy should not be used routinely after incision and drainage of localized abscesses. They should be administered only when clinically indicated, and antibiotic therapy should be based on culture and sensitivity testing. These organisms secrete hemolysins and streptolysins O and S, which are cardiotoxic, leukocytic, and responsible for the characteristic hemolysis. Gangrene results when the cutaneous blood vessels thrombose, a finding that is often associated with intense local pain. The involved skin is initially erythematous and indurated and quickly evolves to hemorrhagic blebs with focal necrotic zones. The potential for extensive tissue loss and mortality exists, especially if treatment is delayed. This condition may initially begin as a benign process with scant indication of its impending severity. The initial lesion is typically an erythematous, tender pustule or abscess with a small area of necrosis. The benign appearance of this lesion belies the widespread and aggressive tissue destruction that has occurred beneath it. Direct inspection through skin incisions reveals extensive gangrene of the superficial tissues and fat that rarely involves the underlying fascia and muscles. These lesions characteristically exude a thin, brown, malodorous discharge, which manifests mixed flora with abundant polymorphonuclear leukocytes with 925 Cellulitis Cellulitis is an acute infection of the skin and underlying soft tissues. It commonly begins as a hot, red, edematous, sharply defined eruption and may progress to lymphangitis, lymphadenitis, or in severe cases, necrotizing fasciitis and gangrene. Cellulitis usually occurs in local skin trauma caused by insect bites, abrasions, surgical wounds, contusions, or other cutaneous lacerations. Cellulitis is 20-fold e more common in patients with chronic venous stasis or lymphedema. Recurrent cellulitis may occur in patients at the exact site of saphenous donor site surgery. Initial presentation is that of a rapidly expanding, tender, erythematous, indurated area of skin. An ascending lymphangitis may be present, especially in cellulitis involving an extremity often associated with regional lymphadenopathy. Systemic signs and symptoms can eventually evolve and when present, mandate hospitalization and treatment with systemic antibiotics. If fever, septicemia, or other signs of advancement to deeper tissues are present, the patient should be admitted to the hospital for blood and wound cultures, parenteral antibiotics (see Table 1), and observation. If a prompt response is not observed after parenteral antibiotic treatment, surgical exploration of the involved area may be indicated to establish an etiologic diagnosis and rule out the presence of necrotic or gangrenous tissue. Immunosuppressed patients or patients with recurrent cellulitis should be extensively examined to exclude chronic sources of infection, and these patients should be treated with parenteral antibiotics until the cellulitis resolves, followed by 5 to 7 days of oral antibiotics. It is often associated with local crepitus and systemic signs of toxemia, which are caused by the anaerobic, gas-forming bacilli of the Clostridium species. This infection most often occurs after abdominal operations on the gastrointestinal tract; penetrating trauma, such as gunshot wounds, and frostbite can also expose muscle, fascia, and subcutaneous tissues to these organisms. Common to all these conditions is an environment containing tissue necrosis, low oxygen tension, and sufficient amounts of amino acids and calcium to allow germination of clostridial spores and production of the lethal toxin. Crepitus, which is caused by the accumulation of gas in the tissue produced by facultative or obligate anaerobes, can be palpated in 25% of patients, and it mandates immediate surgical attention. Predisposing factors include perirectal abscess and ischiorectal abscess, both of which may track to the deeper structures of the pelvis, leading to abscess formation and subsequent septicemia. This infection can occur after amputation and is usually associated with diabetes mellitus (75% of cases) or peripheral vascular disease (50% of cases). Synergistic necrotizing cellulitis is commonly caused by mixed flora originating in the gastrointestinal tract. Coliforms are the most prevalent aerobes (Escherichia coli, Klebsiella, Proteus), and anaerobic flora include Bacteroides, Peptostreptococcus, Clostridium, and Fusobacterium. The primary treatment modality is aggressive dbridement of nonviable skin and subcutaneous e tissues. This may involve several operations and dressing changes under general anesthesia, which should be performed until all necrotic tissue is removed. Rotation or free myocutaneous flaps and split-thickness skin grafting may cover areas of tissue loss when necessary. If the perineum is involved, fecal diversion by colostomy may be necessary to facilitate healing. Empiric parenteral antibiotics effective against polymicrobial gram-positive and gram-negative aerobic and anaerobic flora are also a mainstay of therapy. However, antibiotic coverage must be modified as soon as culture and susceptibility testing reveal specific offending organisms (Table 2) to reduce the emergence of resistant organisms. Clostridia are gram-positive, spore-forming, obligate anaerobes that are widely found in soil contaminated with animal excreta. They have also been isolated in the human gastrointestinal tract and skin, most importantly in the perineum and oropharynx. Clostridium perfringens is the most common isolate (in 80% of cases) and is among the fastest growing clostridial species, having a generation time under ideal conditions of approximately 16 minutes. This organism produces collagenases and proteases that cause widespread tissue destruction and produces toxin, which is associated with the high mortality rate of clostridial myonecrosis. The toxin, a phospholipase C, causes platelet-neutrophil complexes, vascular obstruction, and extensive compromised vascular perfusion, leading to necrosis of the muscle and overlying fascia, skin, and subcutaneous tissues. Historically, clostridial myonecrosis was a disease associated with battle injuries, but 60% of current cases occur after trauma: 50% after automobile accidents and the remainder after crush injuries, industrial accidents, and gunshot wounds. Mortality can be the result of a failure to recognize that clostridial infection is underway, which leads to a delay in the dbridement of devitalized tise sues. Patients often complain of a sudden onset of pain at the site of trauma or surgical wound, which increases rapidly in severity and extends beyond the original borders of the wound. The skin initially exhibits tense edema, but its pale appearance progresses to a magenta hue. A Gram stain examination of wound discharge reveals abundant gram-positive rods with a paucity of leukocytes. The diagnosis of gas gangrene is based on the appearance of the muscle on direct visualization by surgical exposure, because many changes are not apparent when inspected through a small traumatic wound. As the disease process continues, the muscle becomes frankly gangrenous, black, and extremely friable. Despite profound hypotension and impending organ failure, these patients may be remarkably alert and extremely sensitive to their surroundings. They feel their impending doom and often panic just before slipping into toxic delirium and eventually into coma.
Order lyrica 150mg without a prescription
In the wrestler with frequent outbreaks mental illness stigma quotes order lyrica online pills, chronic suppressive therapy may be recommended. The primary infection results in varicella, also known as chickenpox, a widespread vesicular eruption usually seen in the pediatric population. The ensuing unilateral dermatomal distribution of blisters, often preceded by neuralgic pain, is known as herpes zoster or shingles. Herpes zoster is especially common in patients older than 50 years, but it may be seen at any age. Herpes zoster is no longer considered a marker for underlying cancer, and evaluation for occult malignancy in an otherwise asymptomatic patient is not indicated. A single recurrence of herpes zoster, usually in the same dermatome, may occur but this is uncommon in immunocompetent individuals. The most common dermatomes involved with herpes zoster are in the thoracolumbar (T3-L2) and trigeminal (V1) regions. Skin lesions typically evolve from papules to vesicles and pustules, and then to crusted erosions, before healing approximately 2 to 4 weeks after onset. Pain that continues for more than 3 months after the skin lesions resolve is referred to as postherpetic neuralgia, one of the most common and debilitating complications of this infection. Prompt initiation of a systemic antiviral agent (Table 2) and evaluation by an ophthalmologist are recommended. Disseminated zoster, with more than a few lesions outside the primary and immediately adjacent dermatomes, can indicate visceral involvement and its associated complications. Nevertheless, they experience asymptomatic shedding and unknowingly transmit the disease to sexual partners. Interrupting this cycle of transmission has become a major focus among health care providers who work with these patients. A combination of patient education and appropriate use of systemic antiviral agents may be gradually having some impact on this epidemic. Recommendations for patients with genital herpes include avoiding sex with uninfected partners when active lesions or prodromal symptoms are present and routinely using latex condoms to minimize transmission during periods of asymptomatic shedding. Chronic suppressive doses of oral antiviral agents (Table 1), including acyclovir (Zovirax), valacyclovir (Valtrex), and famciclovir (Famvir), significantly reduce the frequency of clinical recurrences as well as the rate of asymptomatic shedding and may be recommended together with these other practices to reduce the risk of transmission. However, they also code for type-specific proteins that can be used to differentiate them. Current tests based on detecting type-specific viral glycoprotein G (gG-based, type-specific assays) are accurate and should be requested for this purpose. The diagnosis can be supported by demonstration of increased IgG antibody titers between the acute and convalescent phases. Single or multiple warty growths can persist for weeks or months in areas of skin previously involved by typical lesions of varicella or herpes zoster. Tissue biopsy and viral cultures, with further testing for antiviral resistance, may aid in assessment. Herpes Zoster Diagnosis Diagnosis of herpes zoster is often made on clinical grounds alone. With atypical presentations, however, the diagnosis is best confirmed by either an antigen detection method or viral culture. Samples submitted for viral culture should be obtained from vesicular fluid because dried or crusted lesions are unlikely to yield positive results. Viral cultures are required if there is a need to assess possible antiviral resistance. The doses outlined in Table 1 for either episodic or chronic suppressive therapy can be used as a guideline in these cases. Acyclovir became available more than 25 years ago and continues to be widely used. Inside an infected host cell, acyclovir must be phosphorylated-first by a virally encoded enzyme (thymidine kinase) and then by host-cell enzymes-to the active form of the drug, acyclovir triphosphate. Valacyclovir is an oral prodrug of acyclovir and has a much higher bioavailability. After ingestion, valacyclovir is rapidly metabolized to acyclovir, and the subsequent mechanism of action is as just described. Famciclovir is an oral prodrug of penciclovir (Denavir), designed for greater bioavailability. Similar to acyclovir, penciclovir must first be phosphorylated by viral thymidine kinase and then by cellular enzymes to penciclovir triphosphate. Famciclovir has greater bioavailability and a longer intracellular half-life than acyclovir. If taken as recommended, acyclovir, valacyclovir, and famciclovir are generally comparable in their safety and effectiveness. Dosing for all three should be adjusted in the presence of renal insufficiency (see Table 5). Although antiviral therapy does not decrease the incidence of postherpetic neuralgia, all three agents decrease the time for lesion healing and shorten the overall duration of pain if initiated within 48 to 72 hours after the onset of herpes zoster. Several days after exposure, a prodrome of low-grade fever, malaise, abdominal pain, or respiratory symptoms can develop, followed by the appearance of papulovesicles on the palate, tongue, or buccal mucosa. Since 1997, outbreaks of hand-foot-and-mouth disease caused by enterovirus 71 have been reported in Asia and Australia. Although hand-foot-and-mouth disease associated with Coxsackie A16 infection is typically a mild illness, hand-foot-and-mouth disease caused by enterovirus 71 has shown a higher incidence of neurologic involvement, including fatal cases of encephalitis. An atypical hand-foot-and-mouth disease with more widespread cutaneous involvement has been reported as associated with Coxsackievirus A6. Parvovirus B19 Cutaneous manifestations of parvovirus B19 infection include the childhood exanthem known as erythema infectiosum (fifth disease) and, less commonly, petechial or purpuric eruptions. The virus is transmitted primarily via respiratory secretions and, to a much lesser extent, through blood or blood products. The host cells er na famciclovir appear to be more effective than acyclovir for this purpose, presumably because of easier dosing. An otherwise healthy person younger than 50 years who has discrete involvement on the trunk and mild to moderate pain might benefit minimally or not at all from this intervention, especially if it is initiated after 72 hours of lesion onset. However, patients who are older than 50 years, are immunosuppressed, have involvement in the ophthalmic distribution, or have more-extensive lesions or severe pain should receive systemic antiviral therapy, even if the 72-hour deadline has expired. The addition of systemic corticosteroids to the antiviral regimen remains controversial. There is evidence to suggest this can lessen the severity of the acute episode but does not decrease the incidence or duration of postherpetic neuralgia. Corticosteroids may be of benefit in herpes zoster complicated by facial paralysis or cranial polyneuropathy. Corticosteroids should not be used without concomitant systemic antiviral therapy. In patients 60 years of age or older, the live-attenuated herpes zoster vaccine (Zostavax) was shown to substantially reduce the incidence of both herpes zoster and postherpetic neuralgia. Advisory Committee on Immunization Practices recommends that all immunocompetent persons 60 years of age or older receive a single dose of this vaccine. Despite widespread use of these antiviral agents, antiviral resistance is rarely a problem in the immunocompetent population. The basis for the resistance is most commonly a mutation in the gene coding for thymidine kinase. Molluscum contagiosum are benign umbilicated papules caused by infection with the Molluscipoxvirus, a member of the poxvirus family. Lesions are limited to the mucocutaneous surface and typically appear in clusters on the face, trunk, and skin fold areas in children and on thighs, lower abdomen, and suprapubic areas in sexually active adults. Large numbers of lesions in an extensive distribution may be seen in the immunosuppressed population. Transmission routinely occurs by skin-to-skin contact with an infected host, but transmission from contaminated fomites has been reported. Diagnosis is usually based on clinical examination, but histopathology of atypical lesions may be used for confirmation.
Purchase lyrica 75 mg on-line
These studies demonstrated lower mortality in patients who received timely antimicrobial treatment mental disorders vietnam veterans purchase lyrica cheap online. The first study showed that if the first dose was given within 8 hours of arrival, mortality was reduced. The second study demonstrated that a 4-hour interval was associated with better outcomes. Treatment should be given for a minimum of 5 days; the patient should be afebrile for 48 to 72 hours and clinically stable. Several reviews have demonstrated that influenza vaccination not only prevents pneumonia but also decreases hospitalizations, decreases cerebrovascular events, and decreases deaths from all causes. Pneumococcal polysaccharide vaccine (Pneumovax 23) is recommended for all persons older than 65 years and persons with certain underlying illnesses. Studies have documented moderate effectiveness for preventing invasive pneumococcal disease (bacteremia and meningitis). The overall efficacy in patients older than 65 years is reported to be between 44% and 75%. The diagnosis is suspected if a patient has a new or progressive infiltrate along with new-onset fever, purulent sputum (>25 neutrophils per low-power field), leukocytosis, and decreased oxygenation. Unfortunately, the clinical parameters are overly sensitive; therefore, other diagnostic tests are desirable. The microbiological approach favors quantitation or semiquantitation of lower respiratory secretions. The diagnostic threshold used to differentiate colonization versus true infection varies by specimen collection. A major reservation to this approach is the possibility of false-negative results, which can result if a patient has been started on an antimicrobial agent before the specimens are collected. Whenever possible, select antimicrobial therapy based on local microbiology and epidemiology. Vaccination should be offered year-round for pneumococcal vaccine and during the fall and winter months for influenza vaccine. Some investigators consider time of onset an important factor in terms of outcomes and pathogens. The stomach and sinuses, blood, and contaminated aerosols are much less common sources. De-escalation of therapy is strongly recommended when culture results become available. Discontinue antimicrobial therapy if results of cultures and other clinical parameters do not confirm pneumonia. For patients on a ventilator, keep the head of the bed at 30 to 45 degrees to prevent aspiration (except when contraindicated). Glucose control to maintain level lower than 180 mg/dL results in lower mortality without increasing the risk of severe hypoglycemia. Use agents such as oral chlorhexidine (Peridex) to reduce oropharyngeal colonization. Modified from American Thoracic Society; Infectious Diseases Society of America: Guidelines for the management of adults with hospital-acquired, ventilatorassociated, and healthcare-associated pneumonia. If Legionella suspected, the combination regimen should include either a macrolide. It is presumed that those patients acquired infection in the endemic areas and subsequently presented outside of these geographic locations. The clinical manifestations of blastomycosis can be diverse, and therefore this infection should be suspected within the appropriate clinical context in persons with a history of residence or travel to such endemic areas. In addition, the incidence and prevalence of blastomycosis has been difficult to establish because suitable serologic or skin-prick assays (demonstrating acceptable sensitivity and/or specificity) to confirm infection are lacking. Although most cases of blastomycosis are concentrated in these regions, it should be remembered that persons can acquire infection with Blastomyces spp. Inquiring about residence or travel to these areas is important to help establish the diagnosis. Risk factors for acquiring blastomycosis have been defined by case reports, case series, and a small number of case-control studies and have not been conclusively established. Exposure while in endemic regions to soil, decaying wood, or to dust clouds generated by soil disruption is important; however, specific outdoor occupations or activities have not been confirmed. In one study from Mississippi, African-American race and prior history of pneumonia were independent risk factors for blastomycosis; however, neither environmental nor socioeconomic risk factors were detected. These findings were in contrast to previously noted studies where race and gender were not identified as specific risk factors for acquisition of blastomycosis. One study in Canada noted an increased incidence among the aboriginal population of Manitoba. Thus, it remains unclear if certain ethnic groups are at increased risk for disease or simply reflect differences in exposure. Immunosuppression may also be an important risk factor, particularly for the tendency to develop severe disease. In such cases, it is speculated that humans and their pet dogs have a simultaneous exposure to the same source of fungus and therefore develop synchronous infection. This hypothesis, however, remains to be confirmed, and in a more recent study, canine blastomycosis was not deemed to predict human disease among the human owners. Additional studies are required to establish the relationship between blastomycosis in humans and disease in their pet dogs. The most common mode of transmission is presumed to be by inhalation of aerosolized conidia from the environment. There are, however, reports of cutaneous blastomycosis occuring after accidental cutaneous inoculation, for example in the laboratory setting during autopsy or after dog bites. The median incubation period, established by reviewing the results of point-source outbreaks, ranges from 30 to 45 days. Following inhalation of conidia into the lungs, the fungus is phagocytosed by alveolar macrophages. It is speculated that a process similar to infection with Mycobacterium tuberculosis then occurs. The patient with intact immunologic responses can contain the process without progression to clinical disease. Alternatively, the patient can develop a symptomatic pneumonia and then mount a suitable immunologic response and recover. Impaired immunity favors the development of progressive pulmonary disease with or without extrapulmonary manifestations. It has also been suggested that reactivation of disease can occur at pulmonary or extrapulmonary sites. Most primary infections (at least 50%) are asymptomatic or mild and usually go unrecognized, resolving spontaneously. In others, a symptomatic pneumonia can develop; recovery can occur either spontaneously or with therapy, without further progression. Blastomycosis has been termed "the great mimic," because its clinical manifestations are nonspecific and can be similar to those of many different clinical entities. Children demonstrate a similar spectrum of manifestations as in adults (excluding prostatic disease). The most common symptoms include cough, headache, chest pain, weight loss, fever, abdominal pain, and night sweats. It is postulated that children experience disseminated infection more frequently than do adults. Although there are few published reports of blastomycosis in pregnancy, disease has been observed in pregnant women, with presumed subsequent intrauterine and perinatal transmission. In immunocompromised hosts, it appears that a significant percentage developed rapidly progressive pulmonary disease, leading to respiratory failure and death. For those who are immunocompromised, the reported mortality rate range is 30% to 40%, with death occurring within the first few weeks of disease onset.
Cobalamin (Vitamin B12). Lyrica.
- Reducing a condition related to heart disease called "hyperhomocysteinemia" when taken with folic acid and vitamin B6.
- Are there safety concerns?
- Dosing considerations for Vitamin B12.
- Treatment and prevention of vitamin B12 deficiency, and diseases caused by low vitamin B12 levels.
- How does Vitamin B12 work?
- Improving thinking and memory in people aged 65 and older, when used in combination with vitamin B6 and folic acid.
- Sleep disorders.
- Are there any interactions with medications?
- What is Vitamin B12?
- What other names is Vitamin B12 known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96890
Lyrica 75mg cheap
The neoplasms include nevus sebaceus mental disorders vs diseases purchase lyrica 150 mg line, plexiform neurofibromas, and leukoplakia or erythroplakia. Scars, epitomized by the persistent scarring seen in dystrophic epidermolysis bullosa, and nonhealing wounds. By recognizing these risk factors, predispositions, special populations, and associations, the practitioner can identify premalignant lesions in at-risk patients and recommend appropriate follow-up evaluation and treatment. This approach is essential for prevention and early detection of various types of cancers of cutaneous and mucosal surfaces. Lesions that progress, become symptomatic, become locally destructive or disfiguring, do not respond to appropriate treatment, or change their clinical appearance or behavior should be evaluated for malignancy. Lesions that persist after treatment or show rapid progression should raise suspicion for malignant degeneration. Suspicion should be elevated if mucosal lesions are ulcerated, and biopsy is recommended. Treatment Limited mechanical removal of discrete lesions is possible with curettage. Liquid nitrogen applied with a cotton-tipped applicator or spraying device is a common and effective treatment for cutaneous and mucosal lesions. Lesions can be treated until they appear white or frozen; treatment is for 8 to 10 seconds on the lip and other delicate tissues. Some lesions may require two or three such treatments separated by 4 to 12 weeks before resolution. Because this modality is nonselective, normal and atypical cells are affected equally. Treatment of individual lesions with chemical peeling agents such as glycolic acid 20%. These nonselective agents can also be applied to a wider field of involvement for broader effect. More delicate mucosal tissues should be treated once or twice daily for 1 to 3 weeks. Because this is a selective chemical treatment, affected cells are targeted, and a more vigorous response should lead to more significant improvement. Inflammatory response is individual, and for patients who are not tolerating treatment well, application can be reduced to once to three times weekly. Other topical chemotherapeutic field treatments include diclofenac sodium 3% gel (Solaraze) applied once or twice daily for 8 to 12 weeks. The inflammatory response is attenuated and therefore may be better tolerated by patients. Imiquimod 5% cream (Aldara) may be applied daily for 3 to 6 weeks or twice daily for 3 days per week for 4 to 8 weeks. Another regimen is application once or twice per week for 4 to 8 months, used continuously or in alternating 1-month cycles. The daily dosing schedule and treatment course should be decreased by about one half for mucosal surfaces. Photodynamic treatment is another selective treatment for individual lesions or field treatment. Some are rather firm and indurated with a hard scale; others are thin and friable, with a more delicate scale or without scale, appearing shiny and atrophic. Clinical diagnosis is facilitated by light palpation of sun-exposed sites with the fingertips because the characteristic, gritty, sandpaper-like scale can be very prominent. Involvement can range from multiple or few discrete lesions to an ill-defined zone or field. The disseminated superficial type favors sun-exposed sites and manifests as numerous, small, annular papules. The linear type may be generalized or segmental and often manifests very early in life. Only the punctate keratotic papules seen in porokeratosis palmaris, plantaris et disseminate have no clinically evident cornoid lamellae. Malignant transformation occurs mostly commonly in the linear type, followed by the Mibelli type. It is rare in the disseminated type and has not been reported in the punctate type. Treatment Treatment modalities include those described for actinic keratoses and surgical excision may be beneficial. As for actinic keratoses, treatment of arsenical keratoses includes cryotherapy, topical chemotherapy, photodynamic therapy, and retinoids. Carcinoma may develop after 10 to 20 years and evolve from precancerous keratoses or on any skin surface. Observation may be reasonable for certain lesions with clinically benign appearance and behavior, and spontaneous resolution may occur. Lesions of nonmucosal sites, including the plantar feet, can be treated by freezing with liquid nitrogen for 10 to 30 seconds for two cycles. The advantage is painless application, but individual responses are unpredictable. Hyperkeratotic lesions, such as those on the plantar surface, require more aggressive use of these modalities. Imiquimod (Aldara)1 applied daily can be beneficial, but it may require 6 months of treatment. Constant use of occlusive tapes such as duct tape has demonstrated efficacy and may be combined with any treatments. Between liquid nitrogen treatments or as adjunctive therapy, use of keratolytics such as topical salicylic acid products. Oral cimetidine (Tagamet)1 30 to 40 mg/kg/day may be a helpful adjunctive therapy. In those demonstrating sensitivity, cure rates of 60% to 80% can be achieved with intralesional candidal (Candida albicans skin test antigen [Candin])1 or mumps antigen (mumps skin test antigen)1 injections. For treatment of lesions in the anogenital region, liquid nitrogen may be used less aggressively. Imiquimod 5% cream (Aldara) applied twice daily for 3 days of the week for 10 to 16 weeks is about 50% effective. Before application, scale should be removed with acetone, chemical peel, or microdermabrasion. Alternatively, the patient can apply 5-fluorouracil cream or solution for 5 days or any topical retinoid (tretinoin [Retin-A],1 adapalene [Differin],1 or tazarotene [Tazorac]1) for 1 month. Topical (tretinoin, adapalene, or tazarotene) and oral (acitretin [Soriatane]1) retinoids can decrease development of actinic keratoses and nonmelanoma skin cancer in at-risk individuals. Efficacy is relatively mild, but any topical retinoid can be used each night indefinitely as tolerated by the patient. Oral retinoids can be used daily or every other day at the lowest dose (acitretin 10 mg) producing clinical improvement. The clinically benign appearance and behavior change may signal malignant degeneration. Dermatologists reserve the term bowenoid papulosis for discrete, fleshy, red-brown papules with a better prognosis that are seen in younger patients. Progressive verrucous leukoplakia may appear as benign leukoplakia early-hyperplastic, thin, white plaques of the mucosal surface. This leads to flat verrucous papules on the extremities, face, and neck, which may be numerous and may coalesce. Dysplastic nevi are clinically and histologically atypical and therefore likely represent a higher risk. They have a "fried egg" appearance, with a papular center on a macular base, and they are 5 to 12 mm in diameter, larger than common nevi. They often cover most of an extremity, the trunk, the scalp, or even the entire dorsal surface in the neonate. Often, satellites or smaller nevi are seen beyond the border of the primary lesion.
Lyrica 150 mg cheap
Significant injuries should be treated more like crush injuries mental disorders that cause hallucinations 150mg lyrica with amex, as the extent of the internal injuries is difficult to assess. Cutaneous burns due to electrical injury can be treated similarly to thermal burns. During the initial evaluation of electrical injury, patients should undergo electrocardiography and cardiac monitoring, and obtaining serum levels of myoglobin, creatine kinase, and troponin, as well as coagulation studies, should be considered, in addition to liver and pancreas enzyme levels in patients with intra-abdominal injuries. In cases of multiple victims of a lightning strike, a reverse triage process occurs whereby care is provided first to the patients who appear to be in cardiac arrest, as cardiopulmonary resuscitation and defibrillation may save their lives if applied early enough. Therapy (or Treatment) First Aid and Office Management the initial management for burn injuries consists of stopping further injury by removing the heat source and providing cooling. Hot liquid or scald injuries especially require prompt removal of overlying clothing, as the clothing will trap the heat, which will continue the burning damage. After the heat source is removed, copious cool water should be used to irrigate the injured area, and any constricting jewelry should be removed immediately. Early wound cooling decreases the temperature of the injured area quickly to halt the burning process, but irrigation has been shown to be beneficial even after the wound has returned to a normal temperature. It is unclear why cool water irrigation improves burn outcomes; heat removal and edema prevention appear to play a role, but they also appear to lead to alterations in gene expression that decrease injury and improve healing. After cooling the injured area, the initial treatment is to cover the wounds with a clean, thin cloth or sterile sheets while the patient awaits further care. Debride any ruptured blister tissue, clean the wounds with mild soap and water or dilute antiseptic solution, and dress the wound. Wound dressings may include topical antibiotic cream or ointment, silver impregnated nylon or bismuth tribromophenate, and petrolatum impregnated gauze (Xeroform). Silver sulfadiazine cream 1% (Silvadene) is also commonly used, but avoid use on the face as it can lead to pigmented scarring. The management of intact blisters is controversial; however, if a blister appears fragile or likely to rupture, unroof and debride the wound before dressing the wound. If the blister is in thicker skin or appears stable, most recommendations are to aspirate the blister fluid and dress the wound. Some silver products and occlusive bandages may be left in place for several days; most traditional dressings need to be changed daily, or more frequently if needed. Burns are painful injuries and often require early, aggressive pain control, such as with nonsteroidal anti-inflammatory medications, opioid medications, and acetaminophen. It is important to remember to provide additional analgesia as needed for dressing changes and wound care. Pruritus and neuropathic pain may occur as the wound heals, these are often treated with adjunct pain medications such as gabapentin (Neurontin),1 and diphenhydramine (Benadryl). Prophylactic antibiotics should not be used for burn management, as they have been shown to be harmful. If possible, identify the mechanisms and circumstances surrounding the injury, including agents involved, duration of exposure, and situation, including possibility of inhalation injury or enclosed space involvement. The social history may play an important role in disposition and management decisions. Patients who were in an enclosed space or structure fire or who were otherwise exposed to high levels of smoke or toxins should be assessed for carbon monoxide and cyanide injuries. Lactate, troponin, and carboxyhemoglobin levels should be checked in patients at risk for carbon monoxide or cyanide exposure. A patient at risk for cyanide exposure who has a decreased level of consciousness, hypotension, or a lactate level greater than 9 should receive 5 g (or 70 mg/kg to a maximum of 5 g) of hydroxocobalamin (Cyanokit) intravenously. If the patient is in cardiac arrest or does not improve with the initial dose, a total of 10 g should be given. A patient with carbon monoxide exposure should have a carboxyhemoglobin level obtained and be placed on 100% oxygen as soon as possible, typically delivered via a non-rebreather face mask. Carbon monoxide binds tightly to hemoglobin, and by increasing the oxygen concentration in the lungs and blood, the half-life of carboxyhemoglobin is greatly reduced. With oxygen levels typically delivered by non-rebreather face mask, the half-life of carboxyhemoglobin is 74 minutes. This leads to the recommendation that after 6 hours on 100% oxygen, if the patient is asymptomatic, treatment can be stopped. Patients with carbon monoxide poisoning may experience delayed neurologic sequelae. Hyperbaric oxygen therapy may reduce the risk of delayed neurologic sequelae in appropriately selected patients. If possible, consult with a physician capable of providing hyperbaric oxygen therapy or with a poison control center for patients with carboxyhemoglobin levels greater than 10, symptoms consistent with carbon monoxide exposure, or pregnant patients (Table 3). Patients with inhalation injuries can develop rapidly progressing airway swelling. The initial evaluation of burn patients should include assessment for perioral injury, singed facial or nasal hair, and soot or swelling in the oral or hypopharyngeal cavities. These findings, other indications of airway swelling, or difficulty breathing should prompt early placement of a definitive airway. Because patients with extensive wounds can be at risk of developing hypothermia during this phase, it is important to raise the ambient temperature in the resuscitation room or use warm blankets to maintain normothermia. Because children have a proportionally larger head and torso, diagrams have been adapted for use in pediatric populations. Head Neck Anterior trunk Posterior trunk Right buttock Left buttock Genitalia Right upper arm Left upper arm Right lower arm Left lower arm Right hand Left hand Right thigh Left thigh Right leg Left leg Right foot Left foot 19 2 13 13 2. In addition to monitoring of respiratory and circulatory status, a Foley catheter should be placed to monitor urinary output and for intermittent assessment of bladder pressure to evaluate for the development of intra-abdominal compartment syndrome. Because burned tissue increases insensible fluid losses, burn victims have increased fluid requirements. Various formulas are available for calculating approximate fluid requirements, but all require careful monitoring of the results and progress of fluid resuscitation. Patients who receive more than 250 mL/kg in the first 24 hours are at increased risk of developing fluid-related complications. The American Burn Association Consensus Statement formula is used to guide initial fluid management. Burns that warrant a discussion with a burn center for possible transfer or outpatient follow-up include burns in children; patients with comorbid conditions that will impact healing; and patients with special social, emotional, psychological, or rehabilitative needs. Unfortunately, ensuring adequate urine output does not necessarily guarantee adequate fluid resuscitation. In addition to using urine output as an indicator of resuscitation adequacy, other modes of monitoring can be used to help guide fluid resuscitation (hemodynamic monitoring, echocardiography, gastric tonometry, or other devices). Whether they lead to any increased improvement or survivability is not clear, however. Severely burned patients who are treated at specialized centers have better outcomes. It is recommended that hospitals and clinics have agreements with burn centers for the management of complicated patients and patients who meet criteria for burn center transfer. Complications Pain management for burns may require multiple modalities because the type of pain varies, depending on where the patient is in the cycle of treatment and healing. There are three types of pain that need to be treated during the care of a burn patient: background pain, breakthrough pain, and long-term pain. Background pain is present from the onset of the injury, and the pain is typically intensified during procedures. Depending on the severity of the injury, initial pain and background pain may be treated with acetaminophen, nonsteroidal anti-inflammatory drugs. Procedural pain may require bolus dosing of opioids or other adjunctive medications such as ketamine1 (0. Long-term pain may respond to medications such as gabapentin, clonidine, or others. Psychosocial recovery from burns is impacted by the preexisting conditions and the resilience of the patient. Risk factors for burn injury include poverty, a history of abuse or neglect, substance abuse, serious mental illness, and risk for suicide or assault. Psychiatric recovery is negatively affected by posttraumatic stress disorder, depression, learning disorders, substance abuse, stigma, and disability. Pediatric patients often have fewer comorbid medical conditions, which can speed their recovery and limit disability, and they tend to heal more quickly, but their injuries may have a significant impact on their body image development, self-confidence, and interpersonal relationship building.
Order 75 mg lyrica amex
The use of a hot tub or whirlpool bath mental disorders 2 cheap lyrica 150 mg free shipping, especially after exercise or work, may be of palliative benefit. Job and recreational activities must be assessed and modified if necessary to avoid overuse of affected joints. Sexual counseling may be needed, especially in some patients with severe knee, hip, or back involvement. Opioids may be needed occasionally for intense pain, but the benefits are limited owing to the common gastrointestinal adverse events and the potential for addiction. The clinical results demonstrated no significant difference in efficacy among the three treatment groups. Critical analysis of this comparative study, however, discloses a short duration of the treatment trial (4 weeks) and a relatively low antiinflammatory dosage (up to 2400 mg) of ibuprofen. Compounds currently available include salsalate, choline magnesium trisalicylate, and magnesium salicylate. These agents are weak prostaglandin (cyclooxygenase) inhibitors, thus avoiding the anticlotting effect and potential adverse effect on the gastrointestinal tract and kidneys. Side effects are relatively uncommon and minor with nonacetylated salicylates when administered in a dosage of 1 to 1. The prodrug effect might partially spare the gastrointestinal tract and also produces less suppression of renal prostaglandins. Concomitant prophylactic use of misoprostol (Cytotec) has been recommended to protect gastric mucosa in patients with a previous history of peptic ulcer or gastrointestinal bleeding. Unfortunately, misoprostol causes cramps and diarrhea in a relatively high percentage of patients. A gastroprotective agent, such as a proton pump inhibitor, will reduce the risk of gastrointestinal adverse effects. Analgesic agents (non-narcotic) currently available include acetaminophen (Tylenol) and tramadol (Ultram). Adverse effects are rare, but caution must be exercised in patients who have preexisting renal or liver conditions. Tramadol can be given in 50-, 100-, 200-, or 300-mg tablets up to two to three times daily for pain relief (do not exceed 400 mg of immediate-release tablets per day or 300 mg of extended-release tablets per day). These drugs are generally well tolerated, and nausea, vomiting, and dizziness are the most common adverse effects. Duloxetine (Cymbalta) 60 mg daily was introduced as a compound for pain caused by fibromyalgia syndrome. Duloxetine has minor adverse effects, the most common of which is nausea that usually subsides when the medication is continued for a period of approximately 6 to 10 days. In large, controlled clinical trials, nausea occurred in up to 24% of patients taking duloxetine versus 8% of the placebo group. Discontinuing the drug brings about clearing of the renal dysfunction within 1 to 2 weeks. Patients who have a history of elevated blood pressure should be cautioned to have their blood pressure checked every 2 to 3 months. In view of this problem it should not be used in patients who have uncontrolled narrow-angle glaucoma. Duloxetine may increase the risk of bleeding; therefore patients should be cautioned about taking the medication with aspirin or other possible anticoagulants. A trial assessing the effect of celecoxib on cardiovascular events found a slightly higher risk of cardiovascular events but chiefly only at higher doses (400 mg/day or greater). Celecoxib can be used with low-dose aspirin (81 mg) daily and anticoagulants including warfarin (Coumadin). This form of treatment is considered an adjunct to a conventional management program. A painful knee effusion is the most common indication for arthrocentesis followed by a local corticosteroid injection. The remote potential deleterious effect of instability developing in the knee can be avoided by giving injections at infrequent intervals and prescribing a strict postinjection rest regimen. Specific instructions are given to the patient to refrain from weight-bearing activity for 3 days, except getting up for meals and going to the bathroom. The patient is advised to reduce loading of the injected knee by using a cane or crutches with a three-point gait during weight bearing for 2 to 3 weeks after the procedure. This rest regimen delays escape of the steroid suspension from the joint cavity and promotes a longer duration of response to the injection. When a strict postinjection rest program was imposed, these patients obtained substantial improvement in the duration of the effect, and some achieved indefinite "cures. Diagnosis is confirmed by radiographic findings of chondrocalcinosis and polarized microscopic identification of the specific crystals in the fluid. Treatment, including aspiration and administration of intraarticular steroids, is usually successful in controlling the acute synovitis. The mechanism of action of hyaluronate is termed viscosupplementation, an effort to restore normal viscoelastic properties to the pathologically altered synovial fluid. Other possible beneficial effects include protection of the chondrocytes, antiinflammatory effects, and improvement of the mechanics of joint motion. Table 1 lists the more common hyaluronans that are available for injecting knee osteoarthritis. All the hyaluronans are highly purified natural preparations except Hylan G-F20, which is cross-linked with added formaldehyde and vinyl sulfone in an effort to increase retention in the joint cavity. This preparation would be especially useful in the rare patient who is allergic to avian products. Hyaluronan therapy has been studied in other specific joints including the hip, shoulder, ankle, and first carpometacarpal joints. Drawbacks of intraarticular hyaluronan include difficulty injecting and limited response in patients with extreme obesity and severe advanced osteoarthritis of the knee (grade 4 Kellgren classification). Re-treatment with intraarticular hyaluronic acid 1 year after the first series is safe and effective in patients whose initial course of therapy was successful. A new hyaluronan preparation (Monovisc) has been developed, containing 4 or 5 times the amount of hyaluronan used in the usual knee injection, which is given in a series of 3 or 4 weekly injections. The response and results have not been compared directly in a clinical trial to date. The approach, if effective, would simplify the procedure, especially for "needle shy" patients. The authors of a recent double-blind, shamcontrolled evaluation concluded that "most, if not all" of the effects of tidal irrigation seem to be attributable to a placebo effect. Associated abnormalities such as ligamentous and meniscal tears can be observed in conjunction with osteoarthritis. It has been suggested that the beneficial action of hydroxychloroquine is due to its inhibitory effects on lysosomal enzymes and the secretion of interleukin-1. Other novel therapeutic approaches that are under study but lack conclusive significant data at this time include insulin-like growth factors, transforming growth factor-, and glucosamine, a proteoglycan component and a growth factor for cartilage. In ongoing studies, an antinerve growth factor antibody, fully humanized, effectively reduces pain and improves function in subjects with knee osteoarthritis. Undesirable effects so far are minor, including a rare, transient, mild peripheral neuritis. A subsequent report described relatively successful treatment of 23 patients who had chondral defects of the knee and were given autologous chondrocyte transplantation combined with periosteal grafting. However, if the thumb base joint (trapeziometacarpal, first carpometacarpal) is involved, abduction splinting or local injection may be necessary for relief of pain. When a digital node is inflamed, local instillation of a few drops of a corticosteroid suspension often provides prompt relief. If symptoms persist, a cautious trial with one of the topical analgesic pepper plant creams (capsaicin) such as Zostrix may be worthwhile. The topical cream is safe, and a local burning or transient stinging sensation during application is the only troublesome adverse effect. Gene Therapy Gene therapy is an exciting new technology that holds promise for the future but requires considerable further investigation and refinement. Techniques to introduce gene transfer in conjunction with autologous cultured chondrocytes are being explored. Glucosamine and Chondroitin Sulfate Glucosamine7 and chondroitin7 sulfate are over-the-counter nutraceuticals (dietary supplements) that have considerable anecdotal data touting their symptom-modifying effects.
Lyrica 75 mg on-line
Large amounts of glucose given rapidly to nondiabetic patients may cause a transient reactive hypoglycemia and hyperkalemia and may accentuate damage in ischemic cerebrovascular and cardiac tissue mental disorder treatment cheap 150 mg lyrica with mastercard. If focal neurologic signs are present, it may be prudent to withhold glucose, because hypoglycemia causes focal signs in less than 10% of cases. Thiamine Deficiency Encephalopathy Thiamine is administered to avoid precipitating thiamine deficiency encephalopathy (Wernicke-Korsakoff syndrome) in alcohol abusers and in malnourished patients. Thiamine 100 mg intravenously should be administered around the time of the glucose administration but not necessarily before the glucose. The clinician should be prepared to manage the anaphylaxis that sometimes is caused by thiamine, although it is extremely rare. All the extracted components are returned to the blood except the plasma, which is replaced with a colloid protein solution. It can be as effective as hemodialysis or hemoperfusion for removing toxins that have high protein binding, and it may be useful for toxins not filtered by hemodialysis and hemoperfusion. Plasmapheresis has been anecdotally used in treating intoxications with the following agents: paraquat (removed 10%), propranolol (removed 30%), quinine (removed 10%), L-thyroxine (removed 30%), and salicylate (removed 10%). It has been shown to remove less than 10% of digoxin, phenobarbital, prednisolone, and tobramycin. Complications include infection; allergic reactions including anaphylaxis; hemorrhagic disorders; thrombocytopenia; embolus and thrombus; hypervolemia and hypovolemia; dysrhythmias; syncope; tetany; paresthesia; pneumothorax; acute respiratory distress syndrome; and seizures. Supportive Care, Observation, and Therapy for Complications Altered Mental Status If airway protective reflexes are absent, endotracheal intubation is indicated for a comatose patient or a patient with altered mental status. If respirations are ineffective, ventilation should be instituted, and if hypoxemia persists, supplemental oxygen is indicated. It also affects endogenous opioid peptides (endorphins and enkephalins), which accounts for the variable responses reported in patients with intoxications from ethanol, benzodiazepines, clonidine (Catapres), captopril (Capoten), and valproic acid (Depakote) and in patients with spinal cord injuries. There is a high sensitivity for predicting a response if pinpoint pupils and circumstantial evidence of opioid abuse. In older children and adults, the dose is 2 mg every 2 minutes for five doses up to a total of 10 mg. Naloxone can also be administered into an endotracheal tube if intravenous access is unavailable. If opioid abuse is suspected, restraints should be in place before the administration of naloxone, and it is recommended that the initial dose be 0. Naloxone may unmask concomitant sympatho-mimetic intoxication as well as withdrawal. Larger doses of naloxone may be required for more poorly antagonized synthetic opioid drugs: buprenorphine (Buprenex), codeine, dextromethorphan, fentanyl and its derivatives, pentazocine (Talwin), propoxyphene (Darvon), diphenoxylate, nalbuphine (Nubain), and long-acting opioids such as methadone (Dolophine). Indications for a continuous infusion include a second dose for recurrent respiratory depression, exposure to poorly antagonized opioids, a large overdose, and decreased opioid metabolism, as with impaired liver function. A continuous infusion has been advocated because many opioids outlast the short half-life of naloxone (30 to 60 minutes). Although naloxone is safe and effective, there are rare reports of complications (less than 1%) of pulmonary edema, seizures, hypertension, cardiac arrest, and sudden death. Agents Whose Roles Are Not Clarified Nalmefene (Revex), a long-acting parenteral opioid antagonist that the Food and Drug Administration has approved, is undergoing investigation, but its role in the treatment of comatose patients and patients with opioid overdose is not clear. It is 16 times more potent than naloxone, and its duration of action is up to 8 hours (half-life 10. It has been demonstrated to be safe and effective for reversing benzodiazepine-induced sedation. It should not be used routinely in comatose patients and is not an essential ingredient of the coma therapeutic regimen. It is contraindicated in cases of co-ingestion of cyclic antidepressant intoxication, stimulant overdose, and long-term benzodiazepine use (may precipitate life-threatening withdrawal) if benzodiazepines are used to control seizures. There is a concern about the potential for seizures and cardiac dysrhythmias that may occur in these settings. If aspiration pneumonia (history of loss of consciousness, unarousable state, vomiting) or noncardiac pulmonary edema is suspected, a chest radiograph is needed. Table 7 lists appropriate testing on the basis of clinical toxicologic presentation. Electrolyte, Acid-Base, and Osmolality Disturbances Electrolyte and acid-base disturbances should be evaluated and corrected. The potassium is usually not used in the calculation because it may be hemolyzed and is an intracellular cation. It is important to recognize anion gap toxins, such as salicylates, methanol, and ethylene glycol, because they have specific antidotes, and hemodialysis is effective in management of cases of overdose with these agents. Table 9 lists other blood chemistry derangements that suggest certain intoxications. Serum osmolality is a measure of the number of molecules of solute per kilogram of solvent, or mOsm/kg water. The osmolarity is molecules of solute per liter of solution, or mOsm/L water at a specified temperature. Osmolarity is usually the calculated value and osmolality is usually a measured value. The freezing point serum osmolarity measurement specimen and the serum electrolyte specimens for calculation should be drawn simultaneously. The serum osmolal gap is defined as the difference between the measured osmolality determined by the freezing point method and the calculated osmolarity. This gap estimate is normally within 10 mOsm of the simultaneously measured serum osmolality. Ethanol, if present, may be included in the equation to eliminate its influence on the osmolal gap (the ethanol concentration divided by 4. Metabolic disorders such as hyperglycemia, uremia, and dehydration increase the osmolarity but usually do not cause gaps greater than 10 mOsm/kg. A gap greater than 10 mOsm/mL suggests that unidentified osmolal-acting substances are present: acetone, ethanol, ethylene glycol, glycerin, isopropyl alcohol, isoniazid, ethanol, mannitol, methanol, and trichloroethane. Alcohols and glycols should be sought when the degree of obtundation exceeds that expected from the blood ethanol concentration or when other clinical conditions exist: visual loss (methanol), metabolic acidosis (methanol and ethylene glycol), or renal failure (ethylene glycol). A falsely elevated osmolar gap can be produced by other low molecular weight un-ionized substances (dextran, diuretics, sorbitol, ketones), hyperlipidemia, and unmeasured electrolytes. Studies have found that the anion gap may be relatively insensitive for determining the presence of toxins. Lactic acidosis can be produced by intoxications of the following: carbon monoxide, cyanide, hydrogen sulfide, hypoxia, ibuprofen, iron, isoniazid, phenformin, salicylates, seizures, theophylline. Note: this equation is often not considered very reliable in predicting the actual measured blood concentration of these alcohols or glycols. Note: A normal osmolal gap may be reported in the presence of toxic alcohol or glycol poisoning, if the parent compound is already metabolized. This situation can occur when the osmolar gap is measured after a significant time has elapsed since the ingestion. In cases of alcohol and glycol intoxication, an early osmolar gap is a result of the relatively nontoxic parent drug and delayed Toxicologic Studies Routine blood and urine screening is of little practical value in the initial care of the poisoned patient. Specific toxicologic analyses and quantitative levels of certain drugs may be extremely helpful. One should always ask oneself the following questions: (a) How will the result of the test alter the management Owing to long turnaround time, lack of availability, factors contributing to unreliability, and the risk of serious morbidity without supportive clinical management, toxicology screening is estimated to affect management in less than 15% of cases of drug overdoses or poisonings. Toxicology screening may look specifically for only 40 to 50 drugs out of more than 10,000 possible drugs or toxins and more than several million chemicals. To detect many different drugs, toxic screens usually include methods with broad specificity, and sensitivity may be poor for some drugs, resulting in falsenegative or false-positive findings. On the other hand, some drugs present in therapeutic amounts may be detected on the screen, even though they are causing no clinical symptoms. Because many agents are not sought or detected during a toxicologic screening, a negative result does not always rule out poisonings. The specificity of toxicologic tests is dependent on the method and the laboratory. The presence of other drugs, drug metabolites, disease states, or incorrect sampling may cause erroneous results.
75 mg lyrica for sale
Clusters of tense blisters on an erythematous base often quickly evolve into erosions or ulcerations with associated crusting mental health therapy eau claire wi generic lyrica 150 mg on-line. Lesions can develop at any mucocutaneous site but are typically found in the perioral or anogenital regions. Following viral replication in the skin or mucosa, intact viral nucleocapsids travel via sensory neurons to the corresponding dorsal root ganglia to establish latency. The virus travels back along the sensory neurons to the mucocutaneous surface to replicate and induce active or subclinical infection. In the case of subclinical infection, no active skin lesions are evident, but infectious particles are present, a state known as asymptomatic shedding. Because most primary infections, whether oral or genital, are asymptomatic, the first evidence of disease often represents a recurrent or initial nonprimary infection. Symptomatic primary disease usually takes the form of gingivostomatitis with or without additional lesions on the cutaneous perioral surfaces. In recurrent episodes, clusters of blisters erupt along the vermillion border of the lips, and subsequent erosions and crusting persist for several days up to 2 weeks. In men, a viral folliculitis of the beard area (herpetic sycosis) may be mistaken for a bacterial process because it is often pustular. The presence of a prodrome and recurrence in the same site are clues to the correct diagnosis. Exposure to ultraviolet light is a common trigger factor for herpes labialis, as is fever or intercurrent infection. Genital Herpes Simplex Virus Infection When symptomatic, primary genital herpes often involves bilaterally distributed lesions in the anogenital area with associated fever, inguinal adenopathy, and dysuria or urinary retention. Nonprimary infections are usually less severe and have fewer constitutional symptoms. Often, there is a prodrome of tingling or burning followed by the development of localized vesicles that can quickly rupture, leaving nonspecific erosions or ulcerations. The lesions may be anywhere within the anogenital region but tend to recur close to the same area in subsequent episodes. The time between exposure and development of primary disease is estimated to be from 3 to 14 days. However, more often the first clinical indication of disease is a recurrence, which can occur weeks to years after the initial infection. This method is sensitive when specimens are obtained from lesions that have not yet become too dry or crusted, usually during the first 2 to 3 days after onset. An adequate sample, obtained by unroofing the blister and swabbing the base, increases the likelihood of an accurate result. Antigen detection tests can remain positive even after lesions have dried, as long as the specimen includes epithelial cells and not just debris. For this method, a scraping from the lesion is usually smeared on a glass slide to be sent to the laboratory. The Tzanck smear (cytologic detection) is both insensitive and nonspecific but may be of use in some clinical settings. Because of the extensive and inflammatory nature of the process and the possible secondary bacterial infection, the underlying viral etiology may be obscured. Herpes gladiatorum is a problem seen most commonly in athletes who participate in close contact sports such as wrestling. Typically transmitted from active herpes labialis or asymptomatic shedding in oral secretions of an infected opponent, herpes gladiatorum often affects the head, neck, or shoulders and may be recurrent. Because molluscum contagiosum tends to be self-limited, treatment is not always recommended, but it can reduce the risk of autoinoculation and transmission to others. Treatment modalities are primarily aimed at destroying the lesions, similar to those used for verruca vulgaris (Table 6). In the case of sexual transmission, evaluation for other sexually transmitted diseases may be indicated. Transmission to humans is by direct contact with infected animals or recently vaccinated animals and is usually seen several days and up to 2 weeks after exposure. Preexisting skin trauma or other disruption of the normal cutaneous barrier enhances the risk of transmission. Lesions evolve through several clinical stages over a period of 3 to 5 weeks, ranging from solid red nodules to vesicular, exudative, or wartlike tumors. As with other poxvirus infections, lesions of orf often demonstrate central umbilication. Orf virus infection can resemble skin lesions associated with potentially life-threatening zoonotic infections such as tularemia, cutaneous anthrax, and erysipeloid. In general, the lesions of orf are self-limited, resolving within 4 to 6 weeks, and treatment is not routinely required. However, immunocompromised persons can develop more progressive and destructive lesions requiring therapeutic intervention such as topical cidofovir1,6 or imiquimod (Aldara). A child with erythema infectiosum typically develops a lowgrade fever and nonspecific upper respiratory symptoms approximately 2 days before the onset of rash. The rash has been described as having a slapped-cheeks appearance, with prominent redness over the malar eminences. This is followed by a pink-to-red lacy or reticular eruption over the trunk and extensor surfaces of the arms and legs. The rash usually lasts a week to 10 days but can transiently recur over months in response to precipitating factors such as sunlight, exercise, and bathing. Diagnosis of erythema infectiosum is usually made on clinical grounds, and treatment is ed ic in. By the time the rash appears and the diagnosis has been made, the child is no longer infectious. Much less commonly parvovirus B19 infection may manifest as a papular-purpuric eruption with edema, erythema, and patecchiae in a "gloves and socks" distribution on the hands and feet. Infection with parvovirus B19 in older adolescents and adults often manifests with arthralgias or arthritis rather than a rash. In certain patient populations, parvovirus B19 infections may be associated with complications including transient aplastic crisis, chronic anemia, and hydrops fetalis. In these less-typical presentations, serology (anti-B19 IgM or documented seroconversion) may be needed for diagnosis. Autoinoculation is possible by scratching the lesions, often leading to a linear pattern. The cellular proliferation gives rise to thick, hyperkeratotic lesions generally known as warts. Most warts are asymptomatic, though patients often present with complaints of a "bump. They usually occur in a linear arrangement related to local trauma, such as shaving. They are usually flesh colored, covered with callus, and can be painful, especially when located on pressure points. Filiform warts are slender, finger-like growths most commonly seen on the face, especially around the eyelids, nose, and mouth. This is a slow-growing variant of squamous cell carcinoma that occurs in the oral mucosa, anogenital region, or plantar surface. Cutaneous warts are divided into common warts, plantar warts, flat warts, and genital warts. Two-thirds of untreated common warts spontaneously regress within 2 years, but previously infected individuals have a higher rate of developing new warts than those who were never infected. Epidemiology It is estimated that 10% of the general population has cutaneous warts, and warts are one of the most common reasons for dermatologic visits. As a result, warts are seen with greater frequency among groups of people in close contact, such as schoolchildren. It is found in the basal layer of the epidermis but replicates in the superficial, well-differentiated layer of the skin. The lesions may be single or multiple and may range in size from miniscule to several centimeters in diameter. Common warts (verrucae vulgaris) are white to flesh-colored, rough, hyperkeratotic, raised, and firm, usually found on the extremities. They are small, 1 to 3 mm in diameter, flat, sharply demarcated growths that appear in large numbers on the face, arms, or legs. Plantar and palmar warts (verrucae plantaris and verrucae palmaris) are hard, thickened, callus-like lesions that disrupt skin lines on the soles or palms.
