
600 mg biltricide amex
Letters to the Editor ombrello glass treatment generic biltricide 600 mg fast delivery, as well as full journal articles, are often sources of individual case reports or a case series. Some publications commonly present review articles and may include meta-analyses of data. For instance, proceedings from conferences are often reviewed by staff from marketing, clinical research and other departments outside drug safety. As usual, any suspect reports from these sources should be forwarded to the drug safety department for appropriate review, evaluation, and possible regulatory reporting. Such searches should be conducted regularly with a frequency appropriate to the drug and any special situations, but in general not less frequently than once a month. If in doubt, cases satisfying the usual minimum criteria should be reported to regulators. Under regulation, there is in principle no difference between published reports on identifiable patients with attributed reactions, and spontaneous or clinical study reports. Thus, the usual considerations on seriousness and expectedness apply with regard to expedited and periodic reporting. Publications addressing product safety fall into a number of broad categories including individual case reports or case series, letters to the editor, retrospective database reviews. In addition to individual case reports, many articles contain information on identifiable patients in various forms. Also, it may be very difficult or impossible to determine whether the same cases are already represented in the company or regulatory safety database (as a result of prior direct reporting). The following is recommended: o In accord with most current guidelines and regulations, appropriate types of reports of adverse drug reactions. Published line listings from registries, studies and drug information centers infrequently provide sufficient details to form the basis of individual patient case reports to authorities. To assure that all recipients of the report can properly evaluate the relationship of the event to the suspect drug and reach their own conclusions about attribution, all concomitant medications should be entered in the database and recorded on any report. Another issue reviewers of literature cases face is what to do about the list of references usually cited within an article, some of which may relate to cases similar to those that are the subject of the publication under review. This problem is magnified for review articles, in which few if any identifiable cases are discussed but extensive references are given to articles that might be relevant. Many of those references will already be known to the company (or regulator); some of the cases discussed within those ``secondary' references may have been reported through other sources, and many if not all the cases may reflect years-old experiences. Routinely checking or tracking down all such sources is clearly unrealistic, especially if some of the reference articles are in different languages which require translation. Of course, when faced with a major safety issue all such sources should be sought and would probably be found with a literature search anyway. There are often multiple manufacturers and/or marketers of the same drug, operating independently or through contractual arrangements. All manufacturers, including generic companies, have the responsibility to review the literature and report appropriate information to regulators. This has the potential to greatly increase the number of duplicate reports in databases of both regulators and manufacturers, since information is often shared in many directions, between and among companies and regulators. Most regulations for expedited reporting of clinical trial and spontaneous reports stipulate that the regulatory clock begins with the first awareness of a valid case by anyone in a company anywhere in the world. Special considerations might apply under some circumstances, such as in the following not unusual scenario: initial awareness comes from a printout by a literature search service or from an abstract that does not provide sufficient individual patient and other details to satisfy the minimum criteria for a case; a copy of the full paper or abstract is ordered; the original paper is in a language unfamiliar to the company. For reports uncovered by foreign affiliates of a multinational company in a journal published in their local language, the situation is a bit more straightforward; that affiliate will still have to provide, say, an appropriate translation, typically in English, to the central safety department of the corporation. Journals may be circulated to staff in a number of different departments and in a number of different countries. A published report may thus become known to individuals within a company soon after a journal is received. However, individual members of a safety department with responsibility for managing such a report may or may not be the first to become aware of an article on safety or an individual case. Journals are often read for many 46 reasons and identification of a case report may depend on the skills of the reader. In many companies, there is a formal process for screening the literature for safety information, which may be under the responsibility of someone within the company library, within the safety department, or through an outside contractor, for example. Although others outside the safety department may come upon a relevant article, they may not bring it to the attention of the safety people, knowing that such an automatic search process is in effect. The drug safety unit of a company also requires adequate time to process the case(s) and conduct appropriate evaluation. Recognizing the difficulties involved, the general recommendations on reporting timelines are as follows: o Companies should establish processes for timely access to and review of the literature to permit expedited reporting of relevant cases within the usual timeframe (15 calendar days from recognition of a valid case). However, especially when the case(s) represent new information, attempts to obtain any needed follow-up should still be made promptly and the case(s) dutifully reported to regulators as necessary. When is translation required, to what extent, and into what language(s) should it be done In general, for most countries other than those whose language is that of the journal, the internationally accepted standard is that translations can be in English; however, as noted, several regulators might require translation into the local language for some or all literature reports. Because experience suggests that literature reports are often sufficiently complete and detailed enough to permit evaluation, the need for follow-up may not be as important. However, caution is always appropriate to be aware of fraudulent or fictitious reports. Additionally, the lag time between the event and publication has often resulted in the original medical records having been archived and less available than for more recent cases, making it less likely that an author will respond to requests for information; authors may be much less likely than other reporters to cooperate since they believe and often reply that all the pertinent and important information is in the publication; and, there appears to be less urgency in follow-up, since, by the time a case appears in the published literature, considerable time is likely to have elapsed since its occurrence. In either case, the publication details should be added to the case record along with any additional important medical details relevant to the case; the new information should be handled as for any other follow-up report for regulatory reporting purposes, including on an expedited basis if appropriate. It would be highly unusual for such publications to provide information beyond what was already reported. Thus, the fact that the study results have been published should not, per se, be the subject of a follow-up report to the original case submission or study-report regulatory filings. In addition to the regulatory standards against which companies and regulators manage literature safety information, there have been attempts to set publication standards for authors and editors on content guidelines for adverse experiences and on informing companies or regulators of cases on a timely basis (the Morges recommendations). Editors of journals often do not require that adverse reaction reports be submitted to the manufacturer or regulator at or before the time of submission of a manuscript for publication. Similarly, authors all too frequently fail to report cases in a timely way, either because they are not accustomed to spontaneous reporting or prefer to wait and only publish the case or case series. Changes to these unfortunate practices would help both companies and regulators fulfill their obligations and responsibilities and would ultimately help to improve the quality of case reports as a result of interactions between the authors and knowledgeable company representatives. Minimum information requirements for single and multiple case reports were defined, i. The guidelines developed in Morges are accessible on the Drug Information Association web site: <dia@diahome. Additionally, when the report is sent to companies prior to publication, they can provide comments and information that the author will often find very useful in his/ her interpretation of individual cases as well as in placing such cases in perspective relative to the overall safety experience. Furthermore, advanced notice to a company or regulator of a proposed publication can prepare these parties for disseminating any necessary information to the public or professionals. The Internet Introduction the Internet, in particular the ``world wide web' ( ), is a rapidly growing medium for communication and transmission of information (e-mail and web sites). It represents a network of millions of computers throughout the world that have the ability to interconnect on a full-time or part-time basis. It is expected to transform the healthcare landscape by offering unprecedented access to information, and it will empower 15 See Appendix 1. However, the ability to search for and obtain comprehensive information on a particular subject may be difficult depending on the choice of search engine(s), data classification and selection of search-term(s). Many websites have prescribing information for healthcare professionals and an area for posing and answering questions. From a pharmacovigilance perspective it is important to distinguish between (1) the collection (receipt) of safety data or correspondence over the Internet by companies or regulators from healthcare professionals or consumers. These two different uses of the medium do not necessarily carry the same responsibilities and processes. Some Practical Issues Several considerations bear on the possible use of the Internet for pharmacovigilance and drug safety applications. The Internet is also playing an ever increasing role in drug development, marketing and sales of 16 17 Poste, G. The Internet, Adverse Events and Safety, International Journal of Pharmaceutical Medicine, 12:83-86, 1998. Without the requisite information, it may not be possible to satisfy the minimum criteria for a valid safety case report in terms of an ``identifiable' reporter or patient. There is also the risk that information may by accessed by unintended parties and that the information may be deliberately altered. While these actions are not unique to the Internet, they are facilitated with such a medium and precautionary measures are advisable.
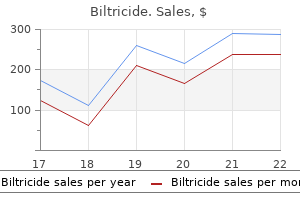
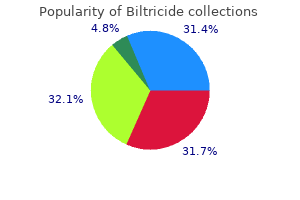
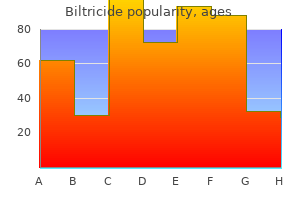
Sansho (Chinese Prickly Ash). Biltricide.
- Pain, vomiting, diarrhea, abdominal pain, snakebite, skin diseases, and other conditions.
- How does Chinese Prickly Ash work?
- Are there safety concerns?
- Are there any interactions with medications?
- What is Chinese Prickly Ash?
- Dosing considerations for Chinese Prickly Ash.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97065
Purchase biltricide without prescription
This is followed by neovascularisation and fibrous tissue proliferatiion which ultimately forms a retrolental mass treatment kidney infection buy biltricide 600 mg amex. Spindle cell theory proposed recently postulates the induction of retinal and vitreal neovascularization by spindle cell insult in a premature retina. Clinical features In anaemia, retinal changes are liable to occur when haemoglobin level falls by 50 percent and are consistently present when it is below 35 percent (5 gm%). Anaemic retinopathy is characterised by pale arterioles and a pale general background of the fundus. Superficial retinal and preretinal (subhyaloid) haemorrhages may be seen in posterior half of the fundus. Leukaemic retinopathy It is characterised by pale and orange fundus background with dilated and tortuous veins. In later stages, greyish white lines may be seen along the course of the veins (due to perivascular leukaemic infiltration). It is characterised by formation of a demarcation line seen at the edge of vessels, dividing the vascular from the avascular retina. It is characterised by a ridge with extraretinal fibrovascular proliferation into the vitreous. This stage is further subdivided into mild, moderate and severe, depending on the amount of fibrovascular proliferation. It occurs as a result of exudation from incompetent blood vessels or traction from the fibrous (cicatricial) tissue. A circle drawn on the posterior pole, with the optic disc as the centre and twice the discmacula distance as the radius, constitutes zone I. A circle is drawn with the optic disc as the centre and disc to nasal ora serrata as the radius. Extent of involvement is denoted by the clock hours of retinal involvement in the particular zone. Associated with it is the engorgment and dilatation of iris vessels, which result in poor pharmacological dilatation of pupil. Since spontaneous regression of disease occurs in 80 to 90% of cases, so only a weekly examination is recommended. Stage 3, threshold disease should be treated by cryo or laser to prevent progression and to achieve regression. Differential diagnosis Advanced retrolental fibroplasia needs to be differentiated from other causes of leukocoria (see page 282). The first examination by indirect ophthalmosocpy should be done between 6 and 7 weeks post-natal age or 34 weeks post-conceptual age (whichever is earlier). The further line of action will depend upon the overall status of the eye as below: I. In early stages it is characterised by large areas of intra and subretinal yellowish exudates and haemorrhages associated with overlying dilated and tortuous retinal blood vessels and a number of small aneurysms near the posterior pole and around the disc. It may present with visual loss, strabismus or leukocoria (whitish pupillary reflex) and thus needs to be differentiated from retinoblastoma. The condition usually progresses to produce exudative retinal detachment and a retrolental mass. In late stages complicated cataract, uveitis and secondary glaucoma occur, which eventually end in phthisis bulbi. Treatment Photocoagulation or cryotherapy may check progression of the disease if applied in the early stage. However, once the retina is detached the treatment becomes increasingly difficult and success rate declines to 33 percent. Ocular ischaemic syndrome refers to a rare condition resulting from chronic ocular hypoperfusion secondary to carotid artery stenosis. Risk factors include male gender, old age (60-90 years), smoking, for carotid stances hypertension, diabetes mellitus and hyperlipidaemia. Ocular ischaemic syndrome is usually unilateral (80%), affecting elderly males more commonly than females. Symptoms include: Loss of vision, which usually progresses gradually over several weeks or months. Anterior chamber my reveal faint aqueous flare with few, if any, cell (ischaemic pseudoiritis). Neovascular glaucoma is a frequent sequelae to anterior segment neovascularization. Fundus examination may reveal: - Venous dilatation with irregular caliber but no or only mild tortuosity. Other rare conditions to be excluded include hyperlipidaemic ophthalmopathy and aortic arch disease caused by Takayasu arteritis, aortoarteritis, atherosclerosis and syphilis. Treatment of ocular ischaemic syndrome includes: Treatment of neovascular glaucoma (see page 234). Treatment of carotid stenosis is medical (antiplatelet therapy, oral anticoagulants) and surgical (carotid endarterectomy). These lesions are beyond the scope of this chapter, only a common retinal dystrophy (retinitis pigmentosa), a few peripheral retinal degenerations some of the vitreoretinal degenerations are described here. Optic disc becomes pale and waxy in later stages and ultimately consecutive optic atrophy occurs. As the disease progresses, scotoma increases anteriorly and posteriorly and ultimately this primary pigmentary retinal dystrophy is a hereditary disorder predominantly affecting the rods more than the cones. Inheritance Most common mode is autosomal recessive, followed by autosomal dominant. It is the characteristic feature and may present several years before the visible changes in the retina appear. Light threshold of the peripheral retina is increased; though the process of dark adaptation itself is not affected until very late. It comprises retinitis pigmentosa, vestibulo-cerebellar ataxia, congenital deafness and mental deficiency. It is characterised by all the clinical features of typical retinitis pigmentosa, except that there are no visible pigmentary changes in the fundus. In this condition all the clinical features are similar to typical retinitis pigmentosa except that pigmentary changes are confined to an area, immediately around the macula. It is characterised by the presence of innumerable discrete white dots scattered over the fundus without pigmentary changes. These include myopia, primary open angle glaucoma, microphthalmos, conical cornea and posterior subcapsular cataract. It is characterised by retinitis pigmentosa, obesity, hypogenitalism, polydactyly and mental deficiency. It comprises retinitis pigmentosa, progressive infantile deafness, dwarfism, mental retardation, nystagmus and ataxia. It is most unsatisfactory; rather we can say that till date there is no effective treatment for the disease. Measures to stop progression, which have been tried from time to time, without any breakthrough include: vasodilators, placental extracts, transplantation of rectus muscles into suprachoroidal space, light exclusion therapy, ultrasonic therapy and acupuncture therapy. Rehabilitation of the patient should be carried out as per his socio-economic background. It is characterised by white arborizing lines arranged in a lattice pattern along with areas of retinal thinning and abnormal pigmentation. The typical lesion is spindle-shaped, located between the ora serrata and the equator with its long axis being circumferentially oriented. It more frequently involves the temporal than the nasal, and superior than the inferior halves of the fundus. The term retinoschisis refers to splitting of the sensory retina into two layers at the level of the inner nuclear and outer plexiform layers. The latter, also called as senile retinoschisis, may rarely act as predisposing factor for primary retinal detachment. Acquired retinoschisis is characterised by thin, transparent, immobile, shallow elevation of the inner retinal layers which typically produces absolute field defects-the fact which helps in differentiating it from the shallow retinal detachment which produces a relative scotoma. These are small, localised areas of irregular pigmentation, usually seen in the equatorial region. It is characterised by diffuse areas of retinal thinning and depigmentation of underlying choroid. Peripheral retinal degernerations: A, Lattice degeneration, B,Snail track degeneration: C, Acquired retinoschisis; D, white-with-pressure; E, Focal pigment clumps; F, Diffuse chorioretinal degeneration; and G, Peripheral cystoid degeneration.
Order biltricide visa
Also treatment quietus tinnitus purchase cheap biltricide, exceptionally difficult births or prematurity are found more often in patients with idiopathic insomnia than are expected by chance. Most sleep disturbances in childhood are associated with behavioral-psychologic issues, not with idiopathic insomnia. Age of Onset: Typically starts at birth, although in some mild forms, childhood sleep is marginally adequate. Familial Pattern: There is evidence for a genetic disposition in some but not all patients with idiopathic insomnia. Idiopathic insomnia is diagnosed when the history of a serious sleep disturbance can be traced to early childhood, markedly predating the occurrence of other sleep-disturbing factors, and when, in the opinion of the diagnostician, the imbalances in the sleep-wake system play a paramount role. Whereas the short sleeper awakens refreshed and shows no detrimental daytime effects secondary to short sleep, patients with idiopathic insomnia clearly need more sleep than they can obtain, leading them to develop strategies to increase daytime vigilance and deal with chronic fatigue. The innate predisposition toward poor sleep that is often seen in patients with physiologic insomnia is less serious but clearly lies on a continuum with the sleep disturbances shown in idiopathic insomnia. Psychophysiologic insomnia is diagnosed if the inherent predisposition toward poor sleep is mild and needs the stress of maladaptive conditioning before bona fide insomnia develops, whereas idiopathic insomnia is relatively chronic and stable from early childhood on. Psychologically, most patients with idiopathic insomnia are remarkably healthy, given their chronic lack of sleep. If mental abnormalities are found, they clearly develop after insomnia has been established for years, if not decades. Also, idiopathic insomnia is relentless, continuing almost unvaried through both poor and good periods of emotional adaptation. Pathology: In some cases, biochemical abnormalities have been demonstrated, such as inadequate production of serotonin. A complaint of insomnia, combined with a complaint of decreased functioning during wakefulness, is present. The insomnia is long-standing, typically beginning in early childhood, if not at birth. The insomnia is relentless and does not vary through periods of both poor and good emotional adaptation. Complications: Patients often make excessive use of hypnotics or alcohol to induce sleep. Patients may use excessive caffeine and stimulants to maintain wakefulness after chronically inadequate sleep. Polysomnographic Features: Idiopathic insomnia ranges from mild to severe, and includes some of the worst forms of insomnia ever recorded in a sleep laboratory. Somnograms are often difficult to score because sleep spindles may be poorly formed and the characteristics of different sleep stages may be intermixed. Typically, idiopathic insomniacs show long periods of rapid eye movement sleep that are devoid of any eye movements. Paradoxically, idiopathic insomniacs may show fewer body movements per unit of sleep time than do normal sleepers or other insomniacs. Many show a reversed first-night effect, sleeping best on the first night in the laboratory. Other Laboratory Test Features: Patients with idiopathic insomnia may have nonspecific abnormalities on the electroencephalogram, rare biochemical abnormalities, etc. Specific effects of sedative/hypnotic drugs in the treatment of incapacitating chronic insomnia. The loss of muscle tone varies in severity and ranges from a mild sensation of weakness with head droop, facial sagging, jaw drop, slurred speech, and buckling of the knees to complete postural collapse, with a fall to the ground. Cataplexy is always precipitated by emotion that usually has a pleasant or exciting component, such as laughter, elation, pride, anger, or surprise. The body area affected by cataplexy can be localized or can include all skeletalmuscle groups. The waist, lower or upper limbs, neck, mouth, or eyelids may be regionally affected. Sometimes strong emotion may provoke another episode of cataplexy in succession and is termed status cataplecticus. The use of tricyclic antidepressant medications such as protriptyline hydrochloride or imipramine hydrochloride almost always ameliorates cataplexy. The frequency of cataplexy shows wide interpersonal variation, from rare events during a year-long period in some patients, to countless attacks in a single day in others. Patients may learn to avoid conditions inducing cataplexy and may have a decrease in the frequency of cataplectic events over time. Associated Features: Sleep paralysis, hypnagogic hallucinations, automatic behavior, and nocturnal sleep disruption commonly occur in patients with narcolepsy. Hypnagogic hallucinations are vivid perceptual experiences occurring at sleep onset, often with realistic awareness of the presence of someone or something, and include visual, tactile, kinetic, and auditory phenomena. Hallucinatory experiences, such as being caught in a fire, being about to be attacked, or flying through the air, are commonly reported. Sleep paralysis is a transient, generalized inability to move or to speak during the transition between sleep and wakefulness. The patient usually regains muscular control within a short time (one to several minutes). Sleep paralysis is a frightening experience, particularly when initially experienced, and often is accompanied by a sensation of inability to breathe. Episodes often occur with hypnagogic hallucinations, and thus the frightful emotional experience is intensified. These two symptoms are defined as auxiliary symptoms and, along with cataplexy and excessive sleepiness, comprise the narcolepsy tetrad. Narcoleptic patients may report lapses of memory and automatic behavior without awareness of sleepiness, and show inappropriate activity and poor adjustment to abrupt environmental demands. The excessive sleepiness of narcolepsy is characterized by repeated episodes of naps or lapses into sleep of short duration (usually less than one hour). The narcoleptic patient typically sleeps for 10 to 20 minutes and awakens refreshed but within the next two to three hours begins to feel sleepy again, and the pattern repeats itself. Sleep usually occurs in situations in which tiredness is common, such as traveling in transport; attending a monotonous meeting that requires no active participation; or listening to a play, concert, movie, or lecture. The patients often can tolerate the sleepiness if, with much effort and attention, they make a strong attempt to stay awake. There may be sudden and irresistible sleep attacks in situations where sleep normally never occurs, including: during an examination; at interactive business talks; while eating, walking, or driving; and when actively conversing. Sleep attacks usually occur on a background of drowsiness that is a common daily feature. It is characterized by sudden loss of bilateral muscle tone provoked by strong emotion. The duration of cataplexy is usually short, ranging from a few seconds to several Course: Cataplexy, hypnagogic hallucinations, and sleep paralysis decrease in frequency over time; however, excessive daytime sleepiness seems to be lifelong. In others, the excessive sleepiness can worsen over the years and may be associated with the development of periodic limb movement disorder or sleep apnea syndrome, both of which are more common in patients with narcolepsy than in the general population. Because other disorders can occur in patients with narcolepsy, their presence can make it difficult to confirm the diagnosis of narcolepsy. Age of Onset: Narcolepsy most commonly begins in the second decade, with a peak incidence around 14 years of age. Excessive sleepiness is usually the first symptom to appear, with cataplexy appearing either simultaneously or with a delay of 1 to 30 years. Familial Pattern: First-degree relatives of a narcoleptic proband are at about a 20-40 times greater risk of developing narcolepsy-cataplexy than are individuals in the general population. Pathology: No positive brain histopathologic abnormalities on light microscopy have been reported. Complications: Accidents due to sleepiness and cataplexy can occur in almost any situation but commonly occur while driving, operating dangerous equipment, in the home, or at regular employment. Serious social consequences can result because of the sleepiness and can lead to marital disharmony or loss of employment. Education difficulties commonly occur in adolescence, and advanced education opportunities may be lost.
Order biltricide with a mastercard
Narcolepsy 4d medications order biltricide 600mg without a prescription, recurrent hypersomnia, idiopathic hypersomnia, and posttraumatic hypersomnia are primarily disorders of excessive sleepiness. Obstructive sleep apnea syndrome, central sleep apnea syndrome, central alveolar hypoventilation syndrome, and periodic limb movement disorder are disorders that can produce a complaint of either insomnia or excessive sleepiness. The term intrinsic implies that the primary cause of the disorder is an abnormality in physiology or pathology within the body. For some disorders, however, external factors are clearly important in either precipitating or exacerbating the disorder. The following examples are given to help explain the rationale in organizing the disorders under the group heading of intrinsic. Post-traumatic hypersomnia is an example of an intrinsic disorder that could not exist without the occurrence of an external event that produced a head injury. Obstructive sleep apnea syndrome can be induced by an external factor, such as alcohol ingestion, but the development of the syndrome would not be possible without the internal factor of upper airway obstruction; a predisposition to develop the disorder must also be present. Some of the extrinsic sleep disorders may depend upon factors within the body important for the expression of the sleep disturbance; external factors are essential, however, for the continuation of the sleep disturbance and, if they are not present, the sleep disturbance does not occur. For example, although an adjustment sleep disorder is due to psychologically stressful factors and, therefore, could be considered to be internally generated, an external event is the cause and, if the factor is removed, the sleep disorder resolves. If the sleep disorder continues after removal of the external factor, an intrinsic sleep disorder, such as psychophysiologic insomnia, has developed. Essential Features: Psychophysiologic insomnia is a disorder of somatized tension and learned sleep-preventing associations that results in a complaint of insomnia and associated decreased functioning during wakefulness. Psychophysiologic insomnia is an objectively verifiable insomnia that develops as a consequence of two mutually reinforcing factors: (a) somatized tension and (b) learned sleep-preventing associations. Individuals who have psychophysiologic insomnia typically react to stress with somatized tension and agitation. The meaning of stressful events (other than insomnia) is typically denied and repressed but manifests itself as increased physiologic arousal. Learned sleep-preventing associations not only exacerbate the state of high somatized tension but also directly interfere with sleep. These associations can be learned in response to either internal cognitions or external stimuli. Learned internal associations consist mainly of a marked overconcern with the inability to sleep. A vicious cycle then develops: the more one strives to sleep, the more agitated one becomes, and the less able one is to fall asleep. Patients in whom this internal factor (trying too hard to sleep) is a driving force for insomnia often find that they fall asleep easily when not trying to do so. Conditioned external factors causing insomnia often develop from the continued association of sleeplessness with situations and behaviors that are related to sleep. Thus, simply lying in a bedroom in which one has frequently spent sleepless nights may cause conditioned arousal, as may behaviors that lead up to the frustration of not sleeping, such as brushing teeth or turning off the bedroom lights. Patients with externally conditioned arousal often report that they sleep better away from their own bedroom and away from their usual routines. Because conditioning factors are not subjectively experienced, most patients with conditioned arousal have no idea why they sleep so poorly. Both internal and external associations are frequently learned during a bout of insomnia caused by other precipitating factors, such as depression, pain, disturbed sleep environment, or shift work. Psychophysiologic insomnia then persists long after the precipitating factors have been removed. Consequently, this type of insomnia remains rather fixed over time, although occasional periods of better or worse sleep may occur either "out of the blue" or in response to life events such as vacations or stress. Associated Features: As in all insomnias, chronically poor sleepers tend to note decreased feelings of well-being during the day. There is a deterioration of mood and motivation; decreased attention, vigilance, energy, and concentration; and an increase in fatigue and malaise but no objective sleepiness. Although patients with psychopathologic insomnia have little overt psychopathology, they tend to be guarded, with denial and repression often being their main defenses. They typically are sensation avoiders, claiming that they do not want to aggravate their insomnia by deviating from their daily routine. They do show an increased incidence of stress-related psychophysiologic problems, such as tension headaches or cold hands and feet. Course: When not treated, psychophysiologic insomnia may last for years or decades. In some cases, it may gradually worsen over time because a vicious cycle of insomnia develops. Predisposing Factors: Many patients were marginal, light sleepers even before developing psychophysiologic insomnia. One might speculate that in these patients an occasional, naturally occurring, poor night of sleep will reinforce the learned sleep-preventing associations so that the associations cannot be extinguished over time. Differential Diagnosis: the diagnosis of psychophysiologic insomnia lies on a continuum with a number of other diagnostic categories. Inadequate Sleep Hygiene: Inadequate sleep hygiene is the preferred diagnosis when negligence of good sleep hygiene is directly causing the insomnia, which resolves after correction of the sleep hygiene. Psychophysiologic insomnia is the preferred diagnosis to the extent that the insomnia has become independent of the precipitating factors. The discrimination, then, is often made on the basis of other "vegetative signs" of depression, such as loss of appetite, loss of libido, marked diurnal fluctuations in mood (morning being worst), digestive upsets (typically constipation), etc. Finally, it is important that the diagnostician sense that chronic depression, though covert, was a first event rather than a reaction to the frustrations of poor sleep and resulting fatigue. Psychophysiologic insomnia is also often confused with dysthymic-personality disease. In dysthymic personalities, depressive features are often seen before the insomnia develops. Generalized Anxiety Disorder: Generalized anxiety disorder is the preferred diagnosis when symptoms of anxiety pervade all of waking life and to the extent that general adaptive functioning is significantly impaired. Psychophysiologic insomnia is the preferred diagnosis when the symptoms focus on insomnia, the consequences of which are present during wakefulness. Although patients with psychophysiologic insomnia typically were marginal sleepers during childhood and adolescence, they typically "got by," except for occasional poor nights around especially exciting or stressful events. The patient with idiopathic insomnia, on the other hand, slept consistently poorly during childhood. Prevalence: In sleep disorders centers, about 15% of all insomniacs are diagnosed with psychophysiologic insomnia. Learned sleep-preventing associations, while paramount in psychophysiologic insomnia, also tend to play an important role in most other forms of chronic insomnia. Age of Onset: Rare in childhood or adolescence, psychophysiologic insomnia typically starts in young adulthood (20s or 30s) and gradually exacerbates until help is sought typically in middle adulthood. Sex Ratio: the complaint of insomnia leading to a diagnosis of psychophysiologic insomnia is more frequently found in females. Familial Pattern: A predisposition toward light marginal sleep seems to "run in families" and may have a genetic basis. Complications: Frequently found are the excessive use of hypnotics or alcohol, plus either administration of tranquilizers during the day to combat the somatized tension, or excessive use of caffeine or abuse of stimulants to combat excessive fatigue. The chronic pattern of failure to attain good sleep may occasionally generalize to other areas of psychologic functions, leading to a passive, defeatist attitude. Polysomnographic Features: the usual features indicating objective insomnia, such as increased sleep latency, increased wakefulness after sleep onset, and decreased sleep efficiency, are found. There may be increased muscle tension and increased electroencephalographic alpha production. If these patients sleep better in the laboratory than at home, they typically are aware of this circumstance and reveal embarrassment about it when interviewed after the polysomnographic evaluation. Other Laboratory Test Features: Psychologic testing will show the profile described previously: malaise, guardedness, sensation avoidance, repression, and denial. A complaint of insomnia is present and is combined with a complaint of decreased functioning during wakefulness. Indications of learned sleep-preventing associations are found and include the following: 1. Trying too hard to sleep, suggested by an inability to fall asleep when desired, but ease of falling asleep during other relatively monotonous pursuits, such as watching television or reading.
Generic 600mg biltricide with visa
However medications side effects prescription drugs cheap 600 mg biltricide mastercard, treatment can improve quality of life by controlling the symptoms and complications of this disease. Pancreaticoduodenectomy, the "Whipple procedure", involves the resection of all of the duodenum with a short section of the jejenum, the pancreatic head, cholecystectomy and excision of the common bile duct and a distal gastrectomy followed by reconstruction. In a total pancreatectomy, the entire pancreas, as well as the duodenum, common bile duct, gallbladder, spleen, and nearby lymph nodes are removed. In Western countries and Japan, different classification systems for staging of pancreatic cancer have evolved, resulting in difficulties in assessing the efficacy of different therapies. Both to overcome the barriers inherent in international classification systems and to achieve a universal prospective data acquisition, a uniform International Documentation System for Exocrine Pancreatic Cancer has been developed by an international group of pancreatologists [13]. Palliative treatment is required for the treatment of jaundice, gastric outlet obstruction and pain. Adjuvant chemotherapy (5-fluorouracil and folinic acid), but not adjuvant radiotherapy, appears to confer a slight survival benefit. Despite substantial evidence for hormone-dependence of pancreatic cancer, there are no data currently confirming a role for estrogens, androgens, cholecystokinin or their antagonists in clinical treatment of exocrine pancreatic cancer [2]. Survival is poor and the majority of pancreatic cancer patients die within one year of diagnosis, although five-year survival rates can reach >30% for lesions of less than 2 cm, negative lymph nodes and clear surgical margins. Definition Melanoma is a malignant proliferation of melanocytes, the pigment-forming cells of the skin, which is the site of most (>95%) disease. Epidemiology There are about 133,000 new cases of melanoma worldwide each year, of which almost 80% are in North America, Europe, Australia and New Zealand. Malignant melanoma of the skin occurs predominantly in white-skinned populations ("Caucasians") living in countries where there is high intensity ultraviolet radiation but this malignancy afflicts to some degree all ethnic groups. Assessed in relation to skin colour, melanoma incidence falls dramatically as skin pigmentation increases and the disease is very rare in dark skinned people. The highest incidence of melanoma occurs in Australia where the population is predominantly white, there is an average of six hours of bright sunlight every day of the year and there is an essentially outdoors lifestyle. The lifetime risk of developing melanoma in Australia is 4-5% in men and 3-4% in women. In Africa and South America, the sole of the foot, where the skin is not pigmented, is the most frequent site affected in the context of a low incidence. Asian peoples have a low risk of melanoma despite their paler skins; naevi in Asian people, though common, are predominantly of the acral-lentiginous type which have low malignant potential. Marked increases in incidence and mortality are being observed in both sexes in many countries. Mortality rates are slightly higher in men than in women, with Australia and New Zealand registering rates of 4. Etiology It is estimated that 80% of melanoma is caused by ultraviolet damage [2] to sensitive skin, i. Ultraviolet radiation is particularly hazardous when it involves sporadic intense exposure and sunburn. Most damage caused by sunlight occurs in childhood and adolescence, making this the most important target group for prevention programmes. Established but rare risk factors include congenital naevi, immunosuppression and excessive use of solaria. While melanoma may occur anywhere on the skin, the majority of melanoma in men is Melanoma 253. New South Wales Central Cancer Registry, Australia on the back, while in women the majority is on the legs. This difference in site incidence is not completely explained by differential exposure to ultraviolet light. Detection Melanoma is usually asymptomatic but a person with melanoma sometimes complains of an intermittent itch. A melanoma often arises from a pre-existing pigmented lesion of the skin (a mole or "naevus") but these tumours can also develop in unblemished skin. The common predisposing skin lesions are dysplastic naevi, junctional and dermal naevi and blue naevi. However, the risk for melanoma development from mature dermal, junctional and blue naevi is quite small, estimated at approximately 1 in 200,000. Congenital naevi are also known precursors of melanoma but the risk for malignant change is related specifically to the size of the naevus. Naevi greater than 20 mm in diameter and, in particular, the large bathing trunk naevi have a high risk of malignant degeneration. These are naevi that are larger than six mm in diameter, have irregular pigmentation, an ill-defined margin and often exist in multiples. Of particular risk is the dysplastic naevus syndrome (familial atypical mole syndrome). The clinical features of melanoma are asymmetry (A), a coastline border (B), multiple colours and quite often some areas of blue/black pigmentation (C), and a diameter greater than six mm (D). Surface microscopy [4] (dermoscopy, epiluminescence microscopy) has developed as an aid to the clinical diagnosis of melanoma. In this technique, the skin surface is rendered translucent by the application of oil and a hand-held instrument providing magnification of at least ten times is used to view the internal details of the tumour. Many additional characteristics, such as pseudopods, radial streaming, blue/grey veil, peripheral black dots and multiple colours are visible and have been used in diagnostic systems now readily accessible to the clinician with an interest in cutaneous diagnosis. Pathology and genetics Melanocytes occur primarily in the skin (where more than 95% of cases of melanoma occurs) but are also found in the mucous membranes of the mouth, nose, anus and vagina and, to a lesser extent, the intestine; melanocytes are also present in the conjunctiva, the retina and the meninges. The morphological classification system for melanoma defines four types: superficial spreading melanoma, nodular melanoma, acral-lentiginous melanoma, and lentigo maligna melanoma. However, this classification has been superseded by a system based on the histopathological parameters of the excised lesion. The majority of cases of melanoma is attributable to sporadic, excessive exposure to ultraviolet radiation which may clinically manifest as sunburn. The patient shows atypical cutaneous naevi, usually exceeding 5mm in diameter, with variable pigmentation and ill defined borders. Management Treatment of primary melanoma is essentially surgical and is related specifically to the tumour thickness measurement. The primary tumour is excised with a margin of normal skin, the excision being based on the tumour thickness measurement [10]. As the primary melanoma becomes thicker (deeper), the risk for metastatic spread rises and thus survival outcomes are related specifically to the tumour thickness measurement. Melanoma metastasizes via the lymphatic system and also via the systemic circulation. Approximately 50% of melanomas metastasize first to the lymph nodes, thus making the management of lymph node metastases an important part of the treatment. The standard management for lymph nodes in patients with primary melanoma is an observation policy and therapeutic node dissection if lymph nodes become involved. However, selective lymphadenectomy [11] is under clinical trial at the present time. While it is clear that the genetic make-up of the melanoma-prone population is very important, few melanomas can be ascribed to specific genetic defects in these populations. While 10% of melanoma patients have a first degree relative affected, less than 3% of melanomas in Australia (where the incidence of melanoma is high) can be ascribed to an inherited gene defect [3]. This lymph node is then removed for histopathological examination; only patients with positive lymph nodes are subjected to full lymph node dissection. However, pending completion of an international trial, the survival benefit of this technique is unknown. As the thickness of the melanoma increases and as the number of lymph nodes involved rises, the risk of systemic metastases becomes greater. Melanoma metastasizes widely, with the lungs, liver and brain being the most common sites. Vitiligo (a skin condition characterized by failure to form melanin) is a favourable prognostic sign in metastatic melanoma. At the present time, only a small proportion of people (<5%) live more than two years once systemic metastases become evident [12]. However, no highly effective single agent or combination has yet been developed and metastatic melanoma is characterized by drug resistance [13]. Spontaneous regression of melanoma, as a result of natural and induced immune rejection, is seen in about 0. Steiner A, Pehamberger H, Wolff K (1987) In vivo epiluminescence microscopy of pigmented skin lesions. In Eastern Europe (Belarus, Ukraine, Russia), several hundred children developed thyroid cancer following the Chernobyl accident.
Biltricide 600mg amex
Spirometric studies and other pulmonary tests usually demonstrate normal lung functioning treatment hypercalcemia buy biltricide 600 mg visa. A lesion of the medullary chemoreceptors controlling ventilation is postulated in the idiopathic form. A central nervous system lesion affecting brain-stem function, such as poliomyelitis or brain-stem infarction, may be found in patients with the acquired form. Complications: Severe hypoxemia and hypercapnia may result in the development of cardiac arrhythmias. Polysomnographic Features: Periods of decreased tidal volume lasting up to several minutes, with sustained arterial oxygen desaturation, are usually observed. Carbon-dioxide levels show an increase during the episodes of hypoventilation, with some improvement following the termination of the respiratory event. Sleep may be characterized by frequent awakenings and arousals associated with body movements. Associated Features: Obstructive or central sleep apneas may occur intermittently or repetitively on the episodes of hypoventilation but do not form the predominant respiratory pattern during sleep. The clinical signs of hypoxia can be quite subtle in children, who may not look distressed. Children do not develop inspiratory retractions, nasal flaring, or other signs of increased respiratory effort in response to the hypoxia. As a result, hypoxia may progress for quite some time without notice until the child appears to deteriorate suddenly, with a cardiopulmonary arrest or severe decompensation. Other Laboratory Test Features: Patients with normal awake pulmonary function tests may demonstrate a marked decrease in ventilatory response to inhalation of carbon dioxide. Brain imaging may be necessary to detect structural lesions that can account for the impaired respiratory control. No associated lesions are present in the idiopathic form of alveolar hypoventilation syndrome. Rarely, phrenic-nerve conduction tests and electromyography, or muscle biopsy of the respiratory musculature, may be indicated. Electrocardiography, chest radiography, and echocardiography may show evidence of pulmonary hypertension. Elevated hematocrit and hemoglobin levels indicate polycythemia from chronic hypoxia. Course: the course of central alveolar hypoventilation can be variable but often is slowly progressive, eventually leading to severe respiratory impairment and cardiac failure. Children who initially present with hypoventilation during both sleep and wakefulness often will be able to sustain adequate spontaneous ventilation during wakefulness later in life. Predisposing Factors: the use of central nervous system depressants, such as alcohol, anxiolytics, and hypnotics, may further worsen or precipitate central Differential Diagnosis: Patients with central alveolar hypoventilation syndrome must be distinguished from patients with peripheral neurologic, muscular, skeletal, orthopedic, or pulmonary lesions. Cardiac disease and hypothyroidism need to be considered in the differential diagnosis. The patient is usually unaware of the clinical features observed by others such as hypoventilation during sleep. No primary lung disease, skeletal malformations, or peripheral neuromuscular disorders that affect ventilation are present. Episodes of shallow breathing greater than 10 seconds in duration associated with arterial oxygen desaturation, and one or more of the following: a. The term periodic limb movement disorder is preferred because the movements can occur in the upper limbs. Essential Features: Periodic limb movement disorder is characterized by periodic episodes of repetitive and highly stereotyped limb movements that occur during sleep. The movements usually occur in the legs and consist of extension of the big toe in combination with partial flexion of the ankle, knee, and sometimes hip. The movements are often associated with a partial arousal or awakening; however, the patient is usually unaware of the limb movements or the frequent sleep disruption. Patients who are unaware of the sleep interruptions may have symptoms of excessive sleepiness. The clinical significance of the movements needs to be decided on an individual basis. Periodic limb movements may be an incidental finding, and medication that reduces the number of limb movements can produce little or no change in sleep duration or sleep efficiency. It is possible that a centrally mediated event can give rise to both the periodic movements and the related sleep disturbance. It is necessary to integrate the clinical history and the polysomnographic findings to assess the role of this phenomenon in a sleep disorder. Most of the major sleep episode is free of respiratory disturbance but it can be associated with mild oxygen desaturation or mild cardiac arrhythmias. Moderate: Usually associated with moderate sleepiness or mild insomnia, as defined on page 23. There may be moderate oxygen desaturation, cardiac arrhythmias, and evidence of pulmonary hypertension. Most of the habitual sleep period is associated with respiratory disturbance, with severe oxygen desaturation or severe cardiac arrhythmias. Associated Features: the disorder can produce anxiety and depression related to the chronicity of the sleep disturbance. Periodic limb movement disorder appears to increase in prevalence with advancing age. Periodic limb movements can accompany narcolepsy and the obstructive sleep apnea syndrome. Periodic limb movement disorder can be associated with, or evoked by, a variety of medical conditions. Episodes of limb movements can develop in patients with chronic uremia and other metabolic disorders. The use of tricyclic antidepressants and monoamine oxidase inhibitors can induce or aggravate this disorder, as does withdrawal from a variety of drugs, such as anticonvulsants, benzodiazepines, barbiturates, and other hypnotic agents. Limb movements associated with ingestion or withdrawal from drugs should be distinguished from the disorder in the drug-free patient. It appears to be rare in children and progresses with advancing age to become a common finding in up to 34% of patients over the age of 60 years. Age of Onset: Appears to be most prevalent in middle adulthood and is rarely seen in children. Contractions occurring during drowsiness, before the onset of stage 1 sleep, are not counted as part of the sleep disorder. The periodic leg movements may be associated with a K-complex with an electroencephalographic arousal or an awakening. Periodic limb movements can occur in discrete episodes that last from a few minutes to several hours or may be present throughout the entire recording. The numbers of movements that occur in each leg are added together, as long as they occur in episodes of at least four movements; isolated movements are not counted. Complications: Periodic limb movement disorder can result in fragmented, restless sleep and complaints of insomnia or excessive sleepiness. Some patients with severe periodic limb movement disorder can also have the movements during wakefulness. Differential Diagnosis: Sleep starts may need to be differentiated from periodic limb movements; the appearance of sleep starts during drowsiness, prior to sleep onset, is the main distinguishing feature. Sleep starts do not recur during sleep stages nor do they occur with a regular periodicity. Leg movements seen in association with disorders that produce frequent sleep fragmentations, such as sleep apnea, may resemble periodic limb movements but disappear upon treatment of the primary condition. The patient occasionally will be asymptomatic, and the movements are noticed by an observer. Repetitive highly stereotyped limb muscle movements are present; in the leg, these movements are characterized by extension of the big toe in combination with partial flexion of the ankle, knee, and sometimes hip. The patient has no evidence of a medical or mental disorder that can account for the primary complaint.
Syndromes
- Apply cool washcloths to the forehead and neck. Sponge the rest of the body with lukewarm (not cold) water. Cold water or alcohol may make the fever worse.
- The type of spider
- Antibiotics
- Heart attack
- Tobacco smoke or other irritants
- Do you smoke?
- Biopsy of the lining of the uterus
Buy 600 mg biltricide otc
Staphylococcus aureus medications bad for liver discount biltricide on line, found in moist areas, that is, axillae, groin, perineum Propionibacterium acnes, found in hair follicles and sebaceous glands Corynebacterium spp, found on the skin surface, and Candida spp, found in the female genital tract. Fungi Aspergillus is a fungal organism found on plants and in soil, dust and building materials. This is a disease that has been linked to redevelopment and renovations especially in healthcare facilities. For additional information refer to the Renovation, Repairs and Redevelopment Risk Management online module. Aspergillosis symptoms and transmission Aspergillosis symptoms range from allergic reactions, like wheezing and coughing, to invasive symptoms resulting from infected bodily organs and compromised immune systems. There is no harm for healthy people as the immune system can get rid of the spores. However, inhalation by compromised people from a dusty environment can lead to infection. This means the risk is greatest for immunocompromised patients, including bone marrow or solid organ transplant patients, leukemia patients, or cystic fibrosis patients. Invasive aspergillosis is very serious and requires early treatment with antifungals. The main purpose of a virus is to deliver its genome into the host cell to allow its expression by the host cell. B,measles, rubella, herpes, and varicella zoster Bacteria Gram-positive bacteria Gram-positive organisms are characterised by having a thick cell wall made of peptidoglycan, and stain blue when challenged with the Gram stain technique. Gram-negative bacteria Gram-negative organisms have a thinner cell wall and an additional outer layer made up of polysaccharides that stain red when challenged with the Gram stain. Spaulding classification the Spaulding classification is a system that provides a general framework for healthcare workers to classify the level of reprocessing required for individual items. This classification system should be risk based and consistent with relevant national and international standards for reprocessing reusable medical devices, instruments and equipment (Rutala, & Weber, 2008). Respiratory equipment An example of reprocessing reusable medical equipment is the cleaning and disinfection of anaesthetic and respiratory equipment. The process required to clean and disinfect this equipment is shown in the table below. Cycle temperatures required Rinsing 40o C to 50o C Washing Disinfecting Final rinsing 50o C to 60o C 70o C to 95o C 80o C to 90o C Disinfection Disinfection is the process that inactivates non-spore forming infectious agents, using either thermal or chemical means. Disinfection is not a sterilisation process and must not be used on critical items as described by the Spaulding classification. Significantly different process are used for the disinfection of flexible and rigid scopes, and accessories used for invasive endoscopic procedures must be treated separately as critical items as described in the Spaulding classification. Sterilisation Sterilisation is a process used to render an item free from all forms of viable microorganisms Critical items require preparation prior to sterilisation including cleaning and drying, a visual inspection for damage, an inspection to ensure the item is functioning correctly and prepackaging. The most widely used methods of sterilisation used in healthcare facilities are steam sterilisation, dry heat sterilisation and peracetic acid. Monitoring Physical monitoring of any method of sterilisation requires certain parameters are met as per the following table. It detects air entrapment and evaluates the removal of residual air from the chamber and load. Using biological/enzymatic monitoring indicators the table shown here is a guide showing test organisms appropriate to the method of sterilisation. Australian Guidelines for the Prevention and Control of Infection in Healthcare,(current edition). Gastroenterological Society of Australia and Gastroenterological Nurses College of Australia. In addition, some jurisdictions and organisations have included an additional sub-category to reflect a high risk for certain vaccine preventable infections i. Source: Australian Technical Advisory Group on Immunisation: the Australian Immunisation handbook. Assess the risk to both the person and clients based on the type of clinical area/procedures involved. Access link here Queensland Health Guideline for Vaccination of Healthcare Workers June 2016. An outbreak can be defined as: "when there are more cases of infection with the same organism than would normally be expected in one area or period of time". Implement and reinforce infection control strategies to contain/ prevent further cases 2. Communication to key stakeholders and the development of an outbreak control team 4. Identify and monitor existing and new cases, contact tracing and data collection 6. Appropriate selection and use of chemical agents for environmental cleaning and disinfection should be risk assessed for correct and safe use. Ensure that solutions used for environmental cleaning are compatible with items or surfaces, receive adequate contact time with surfaces and are prepared correctly. Disinfectants to be used in healthcare settings for environmental cleaning may vary according to national/state/territory recommendations and also between acute and nonacute patient care areas. When using disinfectants, ensure staff, patients and items are not harmed by exposure to the disinfectant agents. Monitoring of cases and the resolution of the outbreak the development of surveillance lists, case lists, checklists and reporting formats should include appropriate data required by the outbreak management team and state/territory health authorities. Australian Government, Communicable Diseases Information, Access link here Victorian Department of Health and Human Services. Access link here Australian Commission on Safety and Quality in Health Care (2018). Clostridium difficile infection in Australia, Access link here Gravel,D, Garden M, Taylor G, Miller M,Simor A, McGeer A, Hutchinson J, Moore D, Kelly S, Mulvey and Canadian Nosocomial Infection Surveillance Program (2009). Guidelines for Management of Occupational Exposures to Blood and Body Fluids, 2017. Updated July 2003, Access link here Australian Guidelines for the Prevention and Control of Infection in Healthcare, (current edition). In Reducing Harm to Patients from Health Care Associated Infection: the Role of Surveillance. Small scale short duration, maintenance or renovation activities that create minimal dust. Work that generates a moderate to high level of dust or work that cannot be completed in a single work shift. Major maintenance, demolition/ excavation/ construction projects that require consecutive work shifts to complete.
Order biltricide overnight delivery
Inadequate sleep hygiene is the preferred diagnostic term because it suggests various habits and activities of daily living that may promote a sleep difficulty medicine to stop diarrhea order biltricide now. Extrinsic Sleep Disorders the extrinsic sleep disorders include those disorders that originate or develop from causes outside of the body. External factors are integral in producing these sleep disorders, and removal of the external factors leads to resolution of the sleep disorder. This is not to say that internal factors are not important in the development or maintenance of the sleep disorder, just as external factors can be important in the development or maintenance of an intrinsic sleep disorder. However, the internal factors would not, by themselves, have produced the sleep disorder without presence of an external factor. Many of the extrinsic sleep disorders listed here were not previously described in the Diagnostic Classification of Sleep and Arousal Disorders. Inadequate sleep hygiene applies to a sleep disorder that develops out of normal behavioral practices that for another person usually would not cause a sleep disturbance. For example, an irregular bedtime or waketime that might not be important in one person may be instrumental in producing insomnia in another. Although environmental factors can produce a disorder of inadequate sleep hygiene, the diagnosis of an environmental sleep disorder is only made when the 72 Essential Features: Inadequate sleep hygiene is a sleep disorder due to the performance of daily living activities that are inconsistent with the maintenance of goodquality sleep and full daytime alertness. Although an exhaustive list of these practices is not feasible, the specific behaviors can be classified into two general categories: practices that produce increased arousal and practices that are inconsistent with the principles of sleep organization. Arousal may be produced by commonly used substances such as caffeine and cigarettes. Alcohol ingestion may also interfere with sleep by producing arousal during the sleep period, which results in sleep-maintenance difficulties. Stress and excitement, such as vigorous exercise close to bedtime, intense mental work late at night, party-going in the evening, and watching the clock during an awakening in the middle of the night, may also lead to arousal. Arousal due to environmental factors may result from the neglect of caretaking activities, such as not regulating ambient temperature within a comfortable range, allowing nocturnal prodding by pets, and failing to prevent early morning light in the bedroom. Sleep may become disrupted or variable when too much time is spent in bed; when there is excessive daily variation in bedtime, arising time, and amount of sleep; and when naps are taken during the day. Although clinicians usually have no trouble identifying grossly excessive time in bed and nightly variability of retiring and arising times, the influence of more subtle changes may go undetected. For example, just as the daily quota of sleep varies in noncomplaining individuals, so too does time in bed. Because a single regular daytime nap does not necessarily interfere with nocturnal sleep, judgment is required to determine if the frequency, duration, proximity to nocturnal sleep, or variable timing of naps suggests an impact on sleep. Prevalence: the prevalence of this disorder in the general population is not known, although it is believed to be a fairly common primary cause or contributing factor of sleep disturbance. It is the rare case of insomnia that does not necessitate some attention to shaping the sleep schedule or prescribing certain arousing practices. Inadequate sleep hygiene may not reach sufficient salience to independently produce insomnia; however, these practices may produce nightly variability, lower the threshold to arousal, and have other effects that render the individual more susceptible to developing insomnia as a result of some other factor. In many cases, it is a confluence of factors that produce a clinically significant insomnia. For example, a habitual sleep-wake schedule and level of coffee consumption in and of themselves may have caused no sleep problem, but the addition of other factors to these preexisting conditions could produce an insomnia. At this stage, each factor may be understood as making an independent contribution to the sleep disturbance. When sufficiently strong or habitual, these inadequate sleep hygiene practices may precipitate insomnia. For example, consuming excessive amounts of caffeine or taking naps at different times of the day becomes part of the behavioral repertoire over time. Although adaptation to these changes is possible at first, with time and increasing intensity of these practices, they begin to have an effect on sleep. The importance of assessing the contribution of inadequate sleep hygiene in maintaining a preexisting sleep disturbance cannot be overemphasized. Once insomnia is present, individuals attempt to cope by taking such actions as going to sleep earlier, staying in bed later, napping, lying down to rest during the day, and drinking coffee. These strategies are attempts to obtain more sleep or minimize the fatigue, performance decrements, and sleepiness that result from insomnia. Although these alterations may lead to increased sleep and reduced daytime decrements, they also lead to increased variability of the timing of sleep and weaken the self-sustaining properties of a regular sleep-wake cycle. Therefore, sleep hygiene should be evaluated in the context of every insomnia to determine how much of a contribution it is making to sustaining the sleep disturbance. Pathology: Mental status examination and psychologic testing reveal little or no psychopathology. Complications: Caffeine addiction, alcoholism, and conditioned insomnia are all complications of inadequate sleep hygiene. In addition, chronic sleep loss and frequent or irregular timing of daytime naps may produce excessive sleepiness and the need for daytime naps. Polysomnographic Features: the usual polysomnographic features associated with sleep disturbance, such as prolonged sleep latency, fragmented sleep, early morning awakening, and reduced sleep efficiency, are present. Recording in the sleep laboratory environment may correct some inadequate sleep hygiene practices; therefore, there may be some attenuation of the severity of the problem. Differential Diagnosis: Psychophysiologic insomnia, environmental sleep disorder, mental disorders, hypnotic-dependent sleep disorder, alcohol-dependent Predisposing Factors: Individuals who are intolerant of any debilitating daytime consequences of sleep loss will resort more quickly to practices that defy good sleep hygiene principles. For example, those people who accept the sleep loss and compromised performance and mood that result from a night or two of poor sleep can ride out the sleep disturbance without restructuring their sleep schedule, taking naps, or increasing daytime caffeine or nighttime alcohol consumption. On the other hand, those individuals who are so distressed by fatigue, sleepiness, moodiness, and reduced performance that they will not put up with a period of incapacity due to sleep loss will institute countermeasures designed to limit these problems. Frequent periods (two to three times per week) of extended amounts of time spent in bed 4. Routine use of products containing alcohol, tobacco, or caffeine in the period preceding bedtime 5. Allowing the bedroom to be too bright, too stuffy, too cluttered, too hot, too cold, or in some way not conducive to sleep 10. Performing activities demanding high levels of concentration shortly before bed 11. No other sleep disorder either produces difficulty in initiating or maintaining sleep or causes excessive sleepiness. Environmental sleep disorder is the preferred term because it may connote either an insomnia or excessive sleepiness that may arise from a variety of environmental factors. Essential Features: Environmental sleep disorder is a sleep disturbance due to a disturbing environmental factor that causes a complaint of either insomnia or excessive sleepiness. This category covers those environmental conditions that invariably result in a disorder of either insomnia or excessive sleepiness. The onset, time course, and termination of the sleep complaint are tied directly to a causative environmental condition. Amelioration or removal of the environmental condition brings about either an immediate or gradual reduction of the sleep problem. A variety of physically measurable environmental factors can result in insomnia or excessive sleepiness. Sleep-disturbing circumstances include heat, cold, noise, light, movements of a bedpartner, and the necessity of remaining alert in a situation of danger or when having to provide attention to an infant or invalid. A variety of medical procedures and an imposed abnormal sleep-wake schedule often associated with hospitalization also may result in a sleep disorder. The sensitivity of the patient to such environmental circumstances is often more critical than is the level of noxious stimulation. Sensitivity to environmental disturbances in nocturnal sleepers increases toward morning. Older individuals are generally more sensitive to environmental factors than are younger ones, although substantial variability in sensitivity may be noted within a particular age group. Three conditions must be present to make a diagnosis of environmental sleep disorder: (1) the sleep problem is temporally associated with the introduction of a Minimal Criteria: A plus B. Mental status examination and psychologic evaluation reveal no psychiatric explanation for the sleep complaint. Polysomnographic Features: Laboratory polysomnography, particularly in those patients with an insomnia complaint, should reveal a total sleep time that is longer than is reported as typical for the home environment. Patients with environment-induced excessive sleepiness show mild to moderate sleepiness during a scheduled series of polysomnographically monitored daytime naps (multiple sleep latency test). Polysomnography reveals no evidence of other sleep disorders such as periodic limb movement disorder or sleep-related breathing disorder. Differential Diagnosis: Inadequate sleep hygiene, insufficient sleep syndrome, psychophysiologic insomnia, psychiatric sleep disorders, irregular sleep-wake pattern, obstructive sleep apnea syndrome, central sleep apnea syndrome, narcolepsy, idiopathic hypersomnia, delayed sleep-phase syndrome.
600 mg biltricide with mastercard
The jerks can occur in any part of the body but most often involve the arms or legs treatment notes order 600 mg biltricide mastercard, sometimes being most prominent in distal muscle groups. The pattern of movements tends to vary between affected individuals and can consist of flexion and extension or abduction and adduction. Neonatal seizures are usually seen in the context of perinatal disorders such as asphyxia, infection, or metabolic abnormalities. Infantile spasms are most often seen after the first month of life but sometimes occur earlier. Benign infantile myoclonus of Lombroso and Fejerman usually occurs after the third month of life and only occurs during wakefulness. Periodic limb movement disorder can occur in infants but typically begins in older age groups. Fragmentary myoclonus consists of similar brief twitchlike muscle jerks, which occur in adults and are often associated with excessive daytime sleepiness. The findings do not meet the diagnostic criteria for other sleep disorders that produce muscle jerking during sleep. Severity Criteria: Mild: Muscle activity that produces muscle fasciculations only. The division into mental and medical categories is somewhat arbitrary and is used here to highlight the less usual association with medical disorders. The first is a listing of the mental disorders that are more commonly seen and associated with disturbed sleep or wakefulness. The second subsection indicates the importance of neurologic disorders and their effect upon sleep and wake states. The third subsection is a listing of disorders that fall into other medical specialty areas but are insufficient in number to warrant separate subsections. Only those medical disorders that are commonly seen in the practice of sleepdisorders medicine are listed here or described in the text. A large number of medical and mental disorders are associated with disturbances of sleep and wakefulness, but an exhaustive list is not provided here. As additional important associations with medical disorders become recognized, they will be added to this list if considered appropriate. Acute psychotic decompensation or the waxing phase of chronic schizophrenia is often associated with significant sleep disruption and is generally characterized by severe difficulty in initiating sleep. Extreme anxiety and preoccupation with delusional material and hallucinatory phenomena may result in motor hyperactivity. A partial or complete inversion of the day-night cycle or reversion to a polyphasic sleep pattern may be seen. Some patients with chronic or remitted disease may have normal sleep efficiency but show persistent abnormalities in sleep architecture such as a deficit in slow-wave sleep. Sleep Disorders Associated with Mental Disorders Although most mental disorders can have an associated sleep disturbance, the psychoses, mood disorders, anxiety disorders, panic disorder, and alcoholism are presented here because they are commonly seen in patients presenting with sleep complaints and need to be considered in differential diagnoses. Panic disorder, one of the anxiety disorders, has a separate text because this disorder can produce only a sleep complaint. Included under the general mental disorder heading in each text is a listing of the disorders to which the text applies. Course: Reduced sleep efficiency may precede psychotic decompensation and may accompany the acute exacerbation of psychotic symptoms. Patients with residual schizophrenia, as compared to patients in the waxing phase of the illness, may have an associated higher sleep efficiency. The use of adequate antipsychotic medication may increase sleep efficiency and may normalize sleep-wake cycles. Predisposing Factors: Any medical illness or psychosocial situation that increases stress and anxiety may be a predisposing factor. Prevalence: Most psychotic patients experience some degree of sleep disruption during exacerbations of their illness. Sex Ratio: Both sexes are equally likely to have sleep disturbance during an exacerbation of their illness. Familial Pattern: To date, there are no studies of the familial pattern of sleep disorders among patients with psychosis. Psychoses (292-299) Synonyms and Key Words: Schizophrenia (295), schizophreniform disorder (295. Complications: Severe sleep disruption may complicate schizophrenia to the degree that patients can become suicidal. Polysomnographic Features: the sleep patterns of psychotic patients vary widely, with some patients showing almost normal sleep patterns. A comparison with delusional and nondelusional depressives and with healthy controls. Other Laboratory Test Features: Recent research suggests that elevations in central norepinephrine levels may be associated with psychotic relapse and reduced sleep efficiency. Differential Diagnosis: Sleep disturbance due to the psychoses must be distinguished from: 1. Insomnia and hypersomnia due to disorders of organic etiology such as periodic limb movement disorder or the sleep apnea syndromes 3. Sleep disturbance due to post-traumatic stress disorder with paranoia Mood Disorders (296, 300, 301, 311) Diagnostic Criteria: Psychoses Associated with Sleep Disturbance (292-299) A. The patient has a clinical diagnosis of schizophrenia, schizophreniform disorder, or other functional psychosis. Polysomnographic monitoring demonstrates an increased sleep latency, reduced sleep efficiency, an increased number and duration of awakenings, and often a reversed first-night effect. If a psychosis is not associated with a sleep symptom, state and code the psychosis on axis C. Typically insomnia and, occasionally, excessive sleepiness, are features of mood disorders. Mood disorders include bipolar disorder, cyclothymia, major depressive disorder, or dysthymia. Patients with bipolar disorders may show cycling between periods of depression, normal mood, mania, or hypomania. Patients with major depression only, have depressive episodes; therefore, their disorder is described as unipolar. Some patients may show a seasonal pattern, with episodes frequently occurring during the winter months; this finding is more common in patients with bipolar disorders. Another group within the mood disorders is secondary depression, which is defined as depression occurring in connection with other mental or medical disorders; the sleep findings here are usually different from those associated with other mood disorders. A major, and usually recurrent, disturbance in mood, either of a depressive or manic nature, typically occurs. Although such mood episodes may develop within the context of a life stress, many episodes have no obvious precipitating factors. The sleep disturbance associated with mood disorders is comprised of two patterns of insomnia that are a part of the diagnostic criteria of the mental disorders. In depression, the insomnia is characterized by difficulty in falling asleep, which is inversely related to age, sleep maintenance disturbance, and "early morning" (premature) awakening; in mania, sleep-onset insomnia occurs and the sleep duration is short. The most characteristic feature of the insomnia seen in major depression is the repeated awakenings, leading to the so-called "early morning" (or premature) awakening that foreshortens sleep. Waking up too early and not being able to return to sleep is the cardinal complaint. A complaint of excessive sleepiness or frequent napping is most commonly associated with milder bipolar depression; some dysthymic patients also exhibit these features. Most depressed patients complain of nocturnal restlessness and tired feelings, whereas patients with hypomania or mania, despite abbreviated sleep, do not complain about the lack of sleep and feel refreshed. Despite the "achy," "washed-out" feelings associated with the profound insomnia, most depressed patients are not objectively sleepy during the day. This finding probably relates to their high degree of psychophysiologic arousal, making it difficult for them to sleep at any time.
Discount biltricide master card
One area in which modern computer technology can facilitate work in pharmocovigilance is assistance in narrative preparation medications prescribed for migraines purchase generic biltricide from india, which is a resource intensive activity. If done correctly, computer-assistance can have many advantages; it obviously can save time for the preparer to have a first draft produced at the press of a button. Advances in automated (computerized) translation into different languages might also be tried to facilitate case review by all concerned parties. The use of such techniques is optimized when as much information for the narrative as possible is extracted directly from the database fields and any extra annotations within or between the data fields are minimized and standardized across cases. No doubt regulatory authorities would also find use of computer-assisted narrative preparation an advantage for summarizing and communicating clinical details of spontaneous cases that are received directly by the agencies. No matter how a narrative is prepared, there is always the need to reconcile the information between its contents and the data base fields from which it is derived (part of a quality assurance process). Computer-assisted narratives have the additional advantage that they obviate the manual reconciliation step, thereby allowing more focus by the reviewer on case evaluation. An effective computer-assisted narrative program will automatically account for phrases or sections not relevant to a particular patient. For purposes of clarity and improved understanding, extra information beyond the data stored in the database might be added to a narrative. However: Any alteration to the basic data included within a narrative should be made first and foremost to the underlying database. It is important to ensure consistency between the data field in the safety or clinical trial data base and the information in the narrative. It was also adopted by the Ministry of Health in Japan in April 1997 and is undergoing implementation over a transition period. The results are summarized later in this chapter and presented in full in Appendix 11. The experience gained over the past several years has led to the recognition of several problem areas that were not foreseen and for which the process might benefit from change or enhancement. For example, are individual case line-listings necessary or desirable for hundreds or thousands of cases However, a method is needed to tie together (bridge) such multiple reports for ease of understanding. A proposal is made for a simplified ``Addendum Report' to cover the desired new data (1 December 2000 to 28 February 2001 in the example). In addition to these four broad concepts, there are several related details for which proposals are made. The aims of any solutions to the current difficulties are that they be practical and achievable with the focus on safety assessment rather than on merely satisfying sometimes divergent or arbitrary regulatory requirements. Focus is placed on suitable solutions for report content, format and frequency which undoubtedly should depend on the stage a drug has reached in its life cycle - whether the product is new with a rapidly evolving safety profile, has an established profile which has changed little over several years, or lies somewhere in between. Each company 145 was asked to respond on behalf of their entire corporation by obtaining data from their affiliates, if appropriate. Responses were received from 29 companies (48%), 6 based in Europe, 12 in Japan, and 11 in the U. Further breakdown of the types of reports, including licenserenewal reports, is found in Table 3. As shown, some companies prepare over 200 different reports per year; the numbers for Japanese companies were surprisingly low and may reflect the fact that they dealt only with local reports. Mean number products [range] 221 [100-308] 10 [4-27] 99 [3-250] 86 [3-308] Table 2. The details in Appendix 11 should be consulted for a more extensive perspective on the many issues and ideas raised by the survey respondents. Individual Case Histories: Line Listings and Summary Tabulations (including discussion of individual cases as necessary) 7. Conclusion Some reports may require supplemental information (usually as appendices) to satisfy specific local regulatory requirements. More streamlined inclusion and presentation criteria for the data are desirable under such circumstances. There can be considerable variations in listedness over 5 years depending on when the classification is made. Especially for many older products, clinical trial exposure may be minimal over a 5 year period and in any event will be far exceeded by market exposure. It is proposed that: Clinical trial data should only be included if the data suggest a signal or are relevant to any suspected changes in the benefit-risk relationship for the product. It must be emphasized that companies must still review and analyze all the case histories received in the time period to search for safety signals. When the line listing is omitted, presentation and analysis of the case reports through the summary tabulation(s) becomes especially im2 In principle, company-generated line listings may become moot in the future for those regulators able and willing to receive individual case reports electronically, especially on an ongoing basis. However, it is uncertain when such a situation will prevail and furthermore there will presumably always be some authorities requiring that line listings be submitted. There is no magic number that qualifies as defining a very large, unwieldy volume for a line listing; 200 is chosen arbitrarily as a reasonable cut-off. Clearly, for any event involving a signal or key safety issue, all relevant cases should be line-listed independent of any cut-off number. However, care must be taken to ensure that medically important distinctions are not overlooked by using terms at too high a level. Also, it is important that when possible, diagnoses rather than (or in addition to) signs and symptoms be identified in summary tabulations. Presentation and assessment in terms of listedness (rather than by serious vs non-serious) under each system organ class may be the most meaningful approach. A large number of clinical or non-clinical studies may have been conducted during a five-year reporting period. Similarly, a comprehensive literature search for an active drug could potentially produce several hundred papers. The inclusion and discussion of literature reports should be selective and focus on publications relevant to safety findings, independent of listedness. The key question, of course, is how to define little or no new information or findings. The following criteria are suggested, all of which ought to be considered: (1) No serious unlisted cases have been received, there are very few serious listed cases. As usual, a list of any completed studies that focussed on safety should be mentioned. It is not uncommon for local regulators to request changes to safety information in a data sheet. Therefore, it is incumbent on the company to use its judgment on whether local label alterations constitute ``regulatory actions for safety reasons. While the example is for an annual report, the same format could be used for 6 month and 5 year reports as well. Please note that the example purposely does not technically satisfy all the suggested criteria but is included to illustrate how a special situation can be handled. Proposals Relating to Frequency and Timing of Reporting As already discussed, there are circumstances in which the usual reporting schedule as designated by many regulators does not or cannot readily apply. In order to avoid the need for a company to prepare a separate one-year report when the product is still under a 6-monthly reporting cycle, a need has been expressed by regulators for some other way to tie together (``bridge') the two 6-month reports (thus, a Summary Bridging Report). One possible practical approach to help overcome the difficulty associated in general with timing and frequency of reporting for new drugs would be to continue with a six-monthly or annual schedule indefinitely, especially if new indications or formulations are likely to be introduced over the years. However, whether such an approach is suitable will depend on the number and types of products a company sells, business processes, resources, and other factors. For example, it may be used to cover four six-month reports in lieu of a separate two-year report, or five separate annual reports for a new, cumulative 5-year report, including reports for license renewal in Europe. The bridging report would obviously cross reference the covered individual reports and, although some of them may have been previously submitted as part of a shorter reporting cycle, the actual reports should be appended. The submission of a summary bridging report should not by itself indicate a need for a new review of the data. The summary bridging report itself, however, is not the tool for such interim (addendum) reporting. It may not be appropriate to structure this chronologically but according to issues and the most recent measures taken to manage them. Exposure data - an estimate of the total number of patients exposed in the time period covered by the bridging report (including from clinical trials if appropriate). Overall Safety Evaluation and Conclusion - mention only key unresolved issues and possible measures to address the problem. Until then, an expedient approach is needed to manage the inconsistencies in harmonization without adding an undue burden for both companies and regulators in the preparation and review of extra reports.
