
Innopran xl 40mg mastercard
Respiratory Distress Respiratory distress is a common complaint necessitating prehospital medical intervention pulse pressure wave qrs complex order innopran xl 80mg overnight delivery. Unfortunately, dyspnea, the perception of respiratory distress, can be influenced by a variety of factors and patient complaint alone is insufficient to identify the underlying cause or its severity. Early stabilization of respiratory function regardless of the underlying pathology is important to avoid significant morbidity and mortality. For example, chronic mitral regurgitation is well tolerated until it becomes severe whereas acute mitral regurgitation is a medical emergency the acuity of onset of the condition is helpful for determining the cause. Patients rarely injure themselves in locations where access and maintenance of spinal precautions is easy. Balancing the risk of worsening or causing injury must be weighed against the necessity of moving the patient to a suitable transport platform. It is important to note that transporting a patient as carefully as practical is very unlikely to generate enough force to cause an injury that is not already present. Spinal immobilization techniques have received increased scrutiny over the past decade. The hard-cervical collar is no longer considered the "magic bullet" of cervical spine immobilization. Hard spinal boards are also falling out of favor with many emergency services around the world. Regardless of the jurisdiction, if "hard" immobilization devices are used, there is a shift toward using them for as short a period of time as possible. Depending on the expected transport time from the scene there may be a role for early application of Philadelphia- or Aspen-style collars with transport in a vacuum mat. The main advantage of cervical spine collars is that they alert the receiving hospital that this patient might have c-spine injury and needs according attention. It is possible that this can be achieved with a soft collar, avoiding some of the risks of prolonged hard collar immobilization. This is particularly relevant for the older patient with fragile skin or for the patient requiring prolonged transfer. Trauma Abdominal Psychogenic Metabolic/endocrine Infectious Hematologic Adapted from Braithwaite S, Perina D. From the moment of injury all care should be focused on maximizing the survival of remaining neuronal tissue. Specific parameters outlined in Chapter 66 are followed with particular emphasis on minimizing secondary injury. Much like percutaneous interventions for heart attacks, interventional neuroradiology is able to drastically change the clinical trajectory of a "brain attack. Thus, early diagnosis, activation of neuroradiology, and timely transport become essential to achieving optimal clinical outcomes. Recent major studies were halted early due to evidence of benefit for those patients who received thrombectomy. As such, transporting these patients to a center that can provide clot retrieval is important. To maximize the speed of diagnosis, mobile stroke units have been developed that contain a portable computed tomography scanner and capacity for "teleradiology" to make a radiologic diagnosis in the field. While these platforms have been launched with significant enthusiasm, they remain the exception across the developed world, and potentially of questionable cost-benefit. Accordingly, the prehospital management of trauma patients has the potential to start the process of recovery from the point of injury. It is essential that anesthesiologists working in receiving hospitals understand the capacity, unique challenges, and limitations of providing care in the prehospital environment so they can be prepared to continue with ongoing care. Understanding what can (and cannot) be done in the prehospital environment minimizes duplication and stagnation of care in-hospital, and is essential to avoiding the therapeutic vacuum. Routinely, higherlevel responses are dispatched to the most acutely sick or injured patients. This number varies from region to region and can be reached via landline or cellular networks (911 in the United States, 999 in the United Kingdom, 000 in Australia, and 112 from cellular telephones worldwide). Once activated, trained nonmedical dispatchers utilize a standardized script to determine urgency and location, and provide bystander advice and support. Alternatively, the system may be activated for a partner emergency service such as police or fire to respond to an incident, or all three emergency services may be required at an incident site. First responders are therefore often required to provide emergency medical management and, where appropriate, supportive care during transport to hospital. In the prehospital environment, first responders may be required to assess, treat, and safely transport people with a range of underlying disorders. Patients may be drug affected, head injured, delirious, or suffering from a wide range of medical or neurosurgical disorders. Prehospital providers may need to treat patients with altered mental status in their own home, at a motor vehicle accident scene, or in any number of complex environments. As with any scene, providing a safe environment for the providers as well as for the patient is of utmost importance. When the need arises, pharmacologic sedation may be utilized to facilitate safe transport to a healthcare facility. Providers are expected to assess and treat any easily reversible causes of altered mental status such as hypoglycemia or hypoxia, but many precipitants are outside the scope of a field diagnosis. For first responders and others who deliver trauma care in the prehospital environment, there are many hazards that need to be considered and addressed to ensure as safe an environment as possible-for themselves and their patient. Some examples of hazards that need to be considered and/or addressed are included in Table 67. The priority on arrival at the scene is to ensure safety for self, the crew, bystanders, and then the patient. It is also important to rapidly assess the number and nature of injured, so a further triage can occur. If the number or severity of injured exceeds the capacity of the on-scene crew, then additional resources should be requested. Prehospital Trauma Trauma remains a significant burden of disease globally and is the greatest cause of death for those under 40 years of age. The focus of the prehospital primary survey is to perform a rapid initial assessment identifying, assessing, and treating life-threatening injuries. It differs from the in-hospital primary survey in that there is the inherent imperative to secure and package the patient for transport at the same time as assessing and treating. In some circles providers have looked to dichotomize the clinical approach in the field between the two extreme positions of "stay and play" and "scoop and run. Proponents of scoop and run argue that the time to definitive care is what makes the difference, hence the patient should be moved as quickly as possible to a trauma center-with only the barest of essential lifesaving interventions performed at the scene. Depending on the expected transport time, this philosophy may be entirely appropriate for many trauma patients. Any interventions performed in this context would be for immediate lifesaving interventions only. By providing maximal appropriate treatment in the field, the intent is to minimize the clinical insult of the injury or illness. The rationale for stay and play is that if the patient needs advanced trauma care from the moment of injury, then that care should be delivered to them early on. In reality, it is not as simple as merely transporting a one-person trauma resuscitation bay to the patient. Despite ever-increasing standards of prehospital resuscitation and more easily available diagnostic equipment, reduced sterility and limited diagnostics and monitoring remain an issue for prehospital teams. As such, each treatment needs to be considered in relation to its potential benefits weighed against the possible harm in delayed primary transfer. In recognition of this tension, many high-performing teams have developed focused, standard operating procedures to maximize their chance of first attempt success and minimize the time taken to perform tasks. The strongest clinical prehospital team is one that possesses complementary and overlapping skills. Current medications, collateral medical history, and photos of the accident scene are all tasks that are expected to be undertaken whenever possible. Effort is made in most systems to deliver patients to the appropriate clinical location wherever possible. Other acute subspecialty centers include stroke, extracorporeal membrane oxygenation, trauma, pediatrics, and burns.
Purchase discount innopran xl on-line
Learning curve in concurrent application of laparoscopic and robotic-assisted hysterectomy with lymphadenectomy in endometrial cancer prehypertension for years order innopran xl master card. Learning curve analysis of the first 100 robotic-assisted laparoscopic hysterectomies performed by a single surgeon. Robotically assisted vs laparoscopic hysterectomy among women with benign gynecologic disease. Outcomes of roboticassisted laparoscopic hysterectomy stratified by body mass index. A comparison of operative outcomes between standard and robotic laparoscopic surgery for endometrial cancer: a systematic review and meta-analysis. Robotic versus laparoscopic right colectomy: an updated systematic review and meta-analysis. Laparoscopic versus robotic colectomy: a national surgical quality improvement project analysis. Robotic cholecystectomy versus conventional laparoscopic cholecystectomy: a meta-analysis. Robotic single-site versus multiport laparoscopic cholecystectomy: a case-matched analysis of short- and long-term costs. Robotic-assisted versus laparoscopic cholecystectomy: outcome and cost analyses of a case-matched control study. A comparative study of outcomes between single-site robotic and multi-port laparoscopic cholecystectomy: an experience from a tertiary care center. Robotic single-port laparoscopic cholecystectomy is safe but faces technical challenges. Laparoscopic vs open hepatic resection for benign and malignant tumors: an updated meta-analysis. Robotic liver surgery for minor hepatic resections: a comparison with laparoscopic and open standard procedures. Robotics in hepatobiliary surgery-initial experience, first reported case series from India. Laparoscopic versus robotic surgery for hepatocellular carcinoma: the first 46 consecutive cases. The University of Pennsylvania curriculum for training otorhinolaryngology residents in transoral robotic surgery. Transoral robotic surgery: a multicenter study to assess feasibility, safety, and surgical margins. A flexible, single-arm robotic surgical system for transoral resection of the tonsil and lateral pharyngeal wall: next-generation robotic head and neck surgery. Robotic surgery in oral and maxillofacial, craniofacial and head and neck surgery: a systematic review of the literature. Transoral robotic surgery of the oropharynx: clinical and anatomic considerations. Two-year survival analysis of 50 consecutive head and neck cancer patients treated with transoral robotic surgery in a single European centre. Endoscopic coronary artery bypass grafting with the aid of robotic assisted instruments. Robotically assisted totally endoscopic atrial septal defect repair: insights from operative times, learning curves, and clinical outcome. Robotic techniques improve quality of life in patients undergoing atrial septal defect repair. Totally endoscopic robotic-assisted repair of patent ductus arteriosus and vascular ring in children. Integrated coronary revascularization: percutaneous coronary intervention plus robotic totally endoscopic coronary artery bypass. Results of the prospective multicenter trial of robotically assisted totally endoscopic coronary artery bypass grafting. Technical aids to performing thoracoscopic robotically-assisted internal mammary artery harvesting. Totally endoscopic robotic-guided pulmonary veins ablation: an alternative method for the treatment of atrial fibrillation. Initial experience with robotic navigation for catheter ablation of paroxysmal and persistent atrial fibrillation. The first series of completely robotic esophagectomies with three-field lymphadenectomy: initial experience. Robotassisted lobectomy for early-stage lung cancer: report of 100 consecutive cases. A systematic review and metaanalysis on pulmonary resections by robotic video-assisted thoracic surgery. Comparison of robotic and video-assisted thoracic surgery for lung cancer: a propensitymatched analysis. A comparison of three approaches for the treatment of early-stage thymomas: robot-assisted thoracic surgery, video-assisted thoracic surgery, and median sternotomy. Short-term outcomes of robot-assisted minimally invasive esophagectomy for esophageal cancer: a propensity score matched analysis. Patients should not be excluded on the basis of arbitrary limits, such as age, body mass index, or American Society of Anesthesiologists physical status classification system. Effective preoperative assessment is required to evaluate and prepare patients and is essential for the delivery of safe, high-quality, and efficient ambulatory surgical care. Of prime importance, provider experience and careful attention to detail are required to deliver high-quality rapid recovery with minimal side effects. Spinal anesthesia may extend the range of patients and procedures suitable for ambulatory surgery, but it requires the use of small doses of bupivacaine combined with opioids or shortacting local anesthetics to avoid prolonged recovery. Sedative techniques can facilitate a wide variety of procedures performed in the hospital, office, or remote settings. However, sedation is no safer than general anesthesia and requires the same standards of personnel, monitoring, and perioperative care as for patients undergoing general or regional anesthesia. Multimodal analgesia, using combinations of local or regional anesthesia, acetaminophen, and nonsteroidal antiinflammatory drugs, provides effective relief of pain. The reduced need for opioids decreases the incidence and intensity of adverse effects. Multimodal regimens are required for patients and procedures known to be associated with increased risk for perioperative nausea and vomiting. Patients should be discharged with written instructions concerning aftercare, return to normal activities, follow-up evaluation, and a contact telephone number. Ambulatory surgery remains very popular with patients with infrequent rates of adverse events and complications. Introduction Ambulatory surgery has its origins in Glasgow, Scotland, where, between 1898 and 1908, James Henderson Nicoll performed almost 9000 ambulatory surgical procedures on children, nearly half of whom were younger than 3 years of age. A few years later, Ralph Milton Waters opened his Downtown Anesthesia Clinic in Sioux City, Iowa, allowing adult patients to return home within a few hours of difficult dental extractions, abscess drainage, or reduction of minor fractures. Ambulatory surgery has expanded far beyond the performance of simple procedures on healthy patients. The availability of improved anesthetic and analgesic drugs minimizes the anesthetic side effects and facilitates the recovery process, as do the increasing availability of minimally invasive surgical techniques. Equally important has been a philosophical change that challenged outdated and conservative practices, demanding unnecessary postoperative inpatient admission. Ambulatory surgery now accounts for approximately 80% of the elective surgeries in the United States. Since 2010 in the United Kingdom, a higher level of funding has been available for an increasing number of procedures when performed on an ambulatory basis,9 in order to incentivize best practice and finance any necessary pathway redesign. Quality standards are set and enforced by government regulation, licensing, or accreditation. Some have been purpose designed, and others have evolved by adapting existing facilities. The facilities delivering ambulatory care services also vary by country, but they can be broadly categorized into four models of care, each with its own advantages and disadvantages.
Generic innopran xl 80mg mastercard
Lithium-sulfur dioxide batteries carry a theoretic risk of sulfur dioxide discharge arteria lienalis discount innopran xl online mastercard. Similarly, an objection exists to the use of mercury cells (now banned in the United States). Fire Hazards Although fires in hyperbaric chambers are rare, they are usually lethal. The effects of fire at elevated ambient pressure are so devastating and so fast that fire extinguisher systems may not be effective. Minimization of these risks involves the following: Controlling chamber O2 concentrations (irrelevant in a monoplace chamber) Minimizing the use of combustible materials within the chamber Eliminating sources of heat and spark Having a chamber fire-extinguisher system the geometric increase in burning rate with increases in O2 concentrations mandates careful monitoring of chamber O2, as already noted. At increased ambient pressure, burning occurs more rapidly, even when O2 concentration is 21%. Cotton garments are recommended because of their reduced risk of static electricity. Elimination of hair grease and humidification of the O2 within the head tent can reduce the risk of hair ignition. Cigarette lighters, matches, and other sources of ignition should be excluded from the chamber. Plugging and unplugging electrical cables during hyperbaric treatments is a source of sparking that can be eliminated by taping all electrical plugs onto receptacles before compression. Electrical systems used in monoplace chambers must comply with specific codes, which stipulate the types of switches, grounding, and insulation that can be used. The following issues are pertinent: Whether a sufficient elevation in PaO2 can be obtained Whether the patient can equilibrate middle ear pressure Optimization of reversible obstructive lung disease and the presence of pulmonary bullae or blebs Whether the patient is susceptible to claustrophobia the calculation of predicted PaO2 in the hyperbaric chamber was described previously. The ability to vent the middle ears may be assessed before treatment by observing directly the tympanic membrane with an otoscope while the patient holds his or her nose or performs a Valsalva maneuver. Intubation was performed after succinylcholine and topical anesthesia of the airway. These investigators suggested using intravenous instead of inhaled general anesthesia because of the problems of pollution of the chamber environment. Inhaled anesthesia of any type can pollute the enclosed chamber atmosphere with anesthetic gases, which may exert pharmacologic effects on medical personnel inside the chamber, particularly at high ambient pressures. Russell and associates270 reported nitrous oxide concentrations in chamber air of 2500 ppm; ventilation of the chamber with air at a high rate (3500 L/min of air) was required to reduce the concentration to 25 to 75 ppm. Lung lavage is performed by flooding one lung with normal saline via a double-lumen endotracheal tube. Protein washout is performed by cyclic filling and emptying with 400 L to 500 mL saline volumes until the effluent clears. Depicted is a patient under general anesthesia with propofol/opioid receiving manual chest percussion during the emptying phase. After 2 to 4 hours of anesthesia, most subjects emerged rapidly from the anesthetic; however, the majority subsequently experienced nausea and vomiting, which was often severe. A potential problem associated with nitrous oxide anesthesia at high ambient pressures is the possibility that tissues could become supersaturated during decompression, thus allowing nitrous oxide bubbles to form during decompression. This complication was not observed by Russell and associates,270 who used an empiric staged decompression schedule with a decompression stop for 30 minutes at 1. Bubble formation can occur without decompression if the patient breathes one gas while surrounded by an atmosphere of another gas that is more diffusible. This phenomenon can occur even at normal atmospheric pressure if a person breathes nitrous oxide-O2 while surrounded by helium. Another risk of hyperbaric nitrous oxide is the dilutional effect of large volumes of dissolved gas entering the lungs during decompression, causing dilutional hypoxia. This situation can be prevented by administration of an O2-enriched breathing mix for several minutes before decompression. The effect of a volatile anesthetic on a patient is proportional not to the alveolar concentration but to the partial pressure of the anesthetic. Because of the effect of increased gas density on this flow ratio, in practice the delivered partial pressure depends somewhat on ambient pressure. McDowell276 reported the following relationship for rotameter flow: Flowactual = Flowread 1 P Intravenous Anesthesia. Intravenous anesthetics behave similarly and are unlikely to be affected within the usual clinical range of ambient pressure (see Chapter 23). Regional anesthesia is likely to be both safe and effective in a hyperbaric environment by avoiding the requirement for mechanical ventilation. Ischemic preconditioning is the application of a brief period of ischemia, which activates endogenous protective mechanisms to reduce the damage from subsequent ischemic insults. Ischemic preconditioning was first described in canine myocardium and subsequently was shown to also exist in the brain. The etiology of cerebral injuries is probably multifactorial, including cerebral microemboli, global cerebral hypoperfusion, inflammation, cerebral temperature modulation, and genetic susceptibility. Summary Environmental exposures can cause specific types of clinical conditions that require targeted therapy. Experience with compressed air and diving has led to new treatments using hyperbaric oxygen. Planning and design of monitoring capabilities will enable optimal control of hemodynamics and oxygenation. Patient safety in this environment can be achieved with careful attention to detail that includes patient selection and monitoring, and chamber procedures. Optimized treatment schedules will evolve from studies of mechanism of action and further clinical trials. Advances in prevention and treatment of O2 toxicity may allow more prolonged therapy than can currently be safely administered, and a more aggressive approach to ischemic and infectious syndromes. Stroke Several studies of middle cerebral artery occlusion in rats have demonstrated beneficial effects of hyperbaric oxygen. Proceedings of the Ninth International Symposium on Underwater and Hyperbaric Physiology. Navy diving manual, rev 6, Diving medicine and recompression chamber operations, vol 5. Mechanics of breathing with helium-oxygen and neon-oxygen breathing mixtures in deep saturation diving. Changes of peripheral venous tone and central transmural venous pressure during immersion in a thermoneutral bath. Circum-rescue collapse: collapse, sometimes fatal, associated with rescue of immersion victims. Swimming-induced pulmonary edema: pathophysiology and risk reduction with sildenafil. A new definition of drowning: towards documentation and prevention of a global public health problem. Recommended guidelines for uniform reporting of data from drowning: the "Utstein style". Near-drowning and drowning classification: a proposal to stratify mortality based on the analysis of 1,831 cases. Predicting outcome of drowning at the scene: a systematic review and meta-analyses. The hemodynamic and cardiovascular effects of near-drowning in hypotonic, isotonic, or hypertonic solutions. Drowning in fresh or salt water: respective influence on respiratory function in a matched cohort study. Drowning and near-drowning on Australian beaches patrolled by life-savers: a 10-year study, 1973-1983. Incidence and Consequences of Near-Drowning-Related PneumoniaA Descriptive Series from Martinique, French West Indies. Molecular and cellular pathways as a target of therapeutic hypothermia: pharmacological aspect. Experimental hypothermia; respiratory and blood pH changes in relation to cardiac function. The effect of acute hypothermia and serum potassium concentration on potassium cardiotoxicity in anesthetized rats.
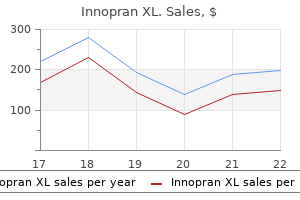
| Comparative prices of Innopran XL | ||
| # | Retailer | Average price |
| 1 | Alimentation Couche-Tard | 354 |
| 2 | AT&T Wireless | 469 |
| 3 | OfficeMax | 677 |
| 4 | Verizon Wireless | 112 |
| 5 | Ruddick Corp. | 189 |
| 6 | Neiman Marcus | 490 |
Cheap innopran xl 40 mg free shipping
Lesions in both globus pallidus and white matter are associated with poor long-term outcome hypertension and alcohol buy 80 mg innopran xl free shipping. Carboxyhemoglobin half-life in carbon monoxide-poisoned patients treated with 100% oxygen at atmospheric pressure. However, it may also occur iatrogenically in several clinical circumstances, such as during cardiopulmonary bypass or as a result of inadvertent injection of air during a diagnostic arteriogram or hemodialysis. Additionally, large amounts of gas may enter the venous system, for example during neurosurgical procedures with the patient in the sitting position, accidental disconnection of hemodialysis access equipment, major back surgery, total hip replacement, cesarean section, laparoscopy, intrauterine laser surgery, arthroscopy (from air escaping from a faulty air-powered instrument), and hydrogen peroxide irrigation or oral ingestion (due to elaboration of gaseous oxygen from tissue and blood catalase). This reduction in blood flow is abolished when there is neutropenia; thus it has been concluded that leukocytes are a major component of the pathophysiology. The gas bubbles in these situations occur because of a decrease in ambient pressure at a rate sufficient to induce local inert gas supersaturation, resulting in formation of bubbles in situ from tissue stores. Fluid resuscitation will replenish intravascular volume, relieve hemoconcentration, and facilitate microcirculatory flow,183 principles that have been confirmed by both animal184 and human observations. The decision to administer recompression treatment should be based entirely on clinical evaluation. Neither the presence nor absence of intravascular gas predicts response to hyperbaric treatment. The pathophysiology is unknown but local hypoxia has been speculated as a possible cause. Size may vary from a small, portable 2-person chamber used for transporting patients in the field to one 20 feet or more in diameter, in which up to 12 or more patients may be comfortably treated, in addition to tenders (attendants). Because of immediate access to the patient by accompanying nursing personnel or physicians, monitoring and resuscitative procedures are straightforward. However, multiplace chambers take up a significant amount of space and are expensive. The chamber wall in most types is manufactured of Plexiglas, facilitating close visual observation of the patient. The advantage of monoplace chambers is their relatively low cost and ease of installation. Chamber operation can often be implemented by connecting the O2 inlet to the hospital supply. Operation is relatively simple, but the patient inside is not directly accessible. Monitoring is somewhat more remote, and emergency airway management is not possible. Monitors are usually kept outside the chamber because of electrical safety considerations. A personnel lock and a transfer lock allow physicians, nurses, or other personnel, in addition to medications, food, and blood samples, to be moved into and out of the chamber without repeated compression and decompression of the patient. Through-hull penetrators in the door on the left can be seen and allow monitoring, intravenous fluid administration, and control of a ventilator inside the chamber. Exhaust gas may be either vented outside the chamber or recirculated through a carbon dioxide scrubber. Development of a pneumothorax during treatment, particularly a tension pneumothorax, can be fatal because pleural decompression with a needle or chest tube cannot be performed before decompression; however, this complication is extremely rare. Moreover, intermittent periods of air breathing, to decrease the risk of O2 toxicity during some types of treatment schedules (see later), requires installation of an additional gas delivery system. Nevertheless, monoplace technology now permits intravenous fluid administration from outside the chamber, invasive intravascular monitoring, mechanical ventilation, and utilization of pleural drainage systems incorporating regulated suction. During the 30-minute period at 6 atmospheres absolute, air or 40% to 50% oxygen (O2) can be administered. This table was originally designed for the treatment of decompression sickness but is now the most commonly used table for gas embolism as well. The shaded areas represent 100% O2 breathing; the white areas represent air breathing periods. Generally, this schedule is used for repetitive treatment of chronic conditions. The patient breathes 100% O2, except for two 5-minute air breaks to reduce pulmonary and central nervous system O2 toxicity. Periods of O2 breathing are interspersed with 5- or 15-minute periods of air breathing to decrease O2 toxicity (see later). Incomplete relief of signs or symptoms can be treated with repeated applications of U. Because saturation treatment results in a much larger degree of nitrogen uptake in both the patient and the tender, decompression must occur much more slowly, usually over 24 to 36 hours. Because hyperbaric chambers used for saturation treatments require additional hardware. This treatment schedule has been designed to maximize PaO2 (and hence tissue bactericidal activity resulting from O2) without an undue risk of hyperoxic seizures. At this lower ambient pressure, the risk of O2 toxicity is minimal and treatments are well tolerated by most patients. At high O2 partial pressures, scavenging mechanisms can be overcome by increased rates of free radical production. Pulmonary toxicity in the conscious patient is heralded by symptoms of tracheobronchial irritation, namely, cough and burning chest pain. Although these algorithms may be useful as an approximate guide to safe O2 exposures in populations, interindividual variability is such that they cannot be relied on to predict accurately the development of pulmonary O2 toxicity for a specific patient. The figure illustrates the value of intermittent O2 (20 minutes O2, 5 minutes air) versus continuous O2 administration in the prevention of pulmonary O2 toxicity. Propensity to pulmonary O2 toxicity engendered by these drugs appears to diminish a few weeks after their discontinuation. Some physicians then routinely administer an anticonvulsant such as phenobarbital, phenytoin, or a benzodiazepine. It is recommended that the chamber should not be decompressed while the patient is actively convulsing because airway closure and failure to exhale during this period may cause pulmonary barotrauma. There is no evidence that hyperoxic seizures are more common in patients with preexisting seizure disorders. A subacute or chronic ocular effect is a change in the refractive index of the lens that results in myopia. However, some patients may be left with residual myopia, particularly older patients. Inert Gas Uptake Breathing air at high ambient pressure can result in nitrogen narcosis, a dose-dependent decrement in cerebral performance due to the anesthetic properties of nitrogen. Barotrauma As the ambient pressure is altered, the pressure within gas-containing spaces in the body must equilibrate with the ambient pressure or undergo a change in volume. Volume change can easily occur in compliant compartments such as the gastrointestinal tract, but if the free flow of gas into and out of containing spaces surrounded by a rigid shell. Indeed, the most common side effect of hyperbaric chamber use for patients is difficulty with middle ear pressure equilibration. Patients who have previously had irradiation of the head and neck and acute respiratory tract infections are at particular risk. Despite the common occurrence of middle ear or sinus squeeze on compression, symptoms on decompression, as a result of the inability of gas to exit through the eustachian tubes or sinus ostia ("reverse squeeze"), are rare. Although a pneumothorax should diminish in size and resorb more quickly after compression, continuing leakage of air from the lung could result in tension pneumothorax during decompression. Equilibration may be facilitated by application of a topical nasal vasoconstrictor. For patients who cannot equalize despite these measures or for obtunded or intubated patients, myringotomy or tympanostomy tubes may be required. Caution must be exercised when using certain commercially available pleural suction regulators, which can exert high negative pleural pressures during chamber compression. Patient Monitoring Despite the changes in the acoustic properties of compressed air, blood pressure measurement may be performed without difficulty with a standard sphygmomanometer and stethoscope. Aneroid pressure gauges are preferred to mercury to avoid contamination of the closed environment. If pressure bags are used to drive continuous flow systems, they must be repressurized during compression and vented before or during decompression. Pulmonary artery catheter balloon ports should also be left open to the chamber during compression and decompression.
Buy innopran xl australia
When the usual 30% oxygen concentration is too low prehypertension innopran xl 80 mg with mastercard, one trick is to titrate in additional oxygen by nasal cannula. The recipient must be able to undergo a very prolonged anesthetic and be free of serious comorbidities. Each procedure is unique with respect to indications, as well as with respect to the nature and the extent of the graft. In the case of the donor, although anesthetic principles similar to conventional organ procurement apply, because of the surgical complexity and time involved, harvesting of the facial graft should ordinarily be performed before harvesting other organs. Recipient patients who do not have a tracheostomy may first require awake fiberoptic oral intubation, followed by a tracheostomy. Largebore catheters are placed to facilitate fluid resuscitation, whereas a central line may be useful to monitor central venous pressure. Blood and fluid management is no different from that during other long surgical procedures involving microvascular free flaps. Connie Culp before (A) and after (B) the two stages of her face transplant at Cleveland Clinic. Finally, there may be periods when muscle relaxation must be avoided to allow nerve identification using electrical stimulation. Acknowledgment this article is a consolidation of two chapters in the 8th edition, Chapter 85 Anesthesia for Ear, Nose, and Throat Surgery by D. The editors and publisher would like to thank the authors for their contributions to the prior edition of this work. American Society of Anesthesiologists Task Force on Management of the Difficult Airway. On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Bilateral adductor vocal cord paresis following endotracheal intubation for general anaesthesia. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. The mechanism of recurrent laryngeal nerve injury during thyroid surgery: the application of intraoperative neuromonitoring. American Society of Anesthesiologists Task Force on Management of the Difficult Airway: Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Difficult airway management practice patterns among anesthesiologists practicing in the United States: have we made any progress Unanticipated difficult airway in anesthetized patients: prospective validation of a management algorithm. Difficult airway management algorithm in emergency medicine: do not struggle against the patient, just skip to next step. The airway approach algorithm: a decision tree for organizing preoperative airway information. An evidence-based approach to airway management: is there a role for clinical practice guidelines A survey of tracheal intubation difficulty in the operating room: a prospective observational study. Predicting difficult airways using the intubation difficulty scale: a study comparing obese and non-obese patients. Determination of the utility of the intubation difficulty scale for use with indirect laryngoscopes. Eschmann introducer through laryngeal mask airway: a cadaveric trial of an alternate means of rescue intubation. A comparison of the use of Trachlight and Eschmann multiple-use introducer in simulated difficult intubation. Use of the endotracheal tube introducer as an adjunct for oral tracheal intubation in the prehospital setting. Frequent use of alternative airway techniques makes difficult intubations less and easier. Case reports: iatrogenic bronchial rupture following the use of endotracheal tube introducers. Gum elastic bougie-guided insertion of the ProSeal laryngeal mask airway is superior to the digital and introducer tool techniques in patients with simulated difficult laryngoscopy using a rigid neck collar. Macintosh direct laryngoscope for intubation of morbidly obese patients: a randomized trial. GlideScope videolaryngoscopy versus direct laryngoscopy for endotracheal intubation: a systematic review and meta-analysis. A comparison of GlideScope videolaryngoscopy with direct laryngoscopy for nasotracheal intubation in children. Comparison of video laryngoscopes with direct laryngoscopy for tracheal intubation: some clarification needed. Evaluation of the GlideScope Direct: a new video laryngoscope for teaching direct laryngoscopy. A retrospective study of the performance of video laryngoscopy in an obstetric unit. GlideScope vs flexible fibreoptic scope for elective intubation in obese patients. Update on dexmedetomidine: use in nonintubated patients requiring sedation for surgical procedures. Awake intubation using the GlideScope video laryngoscope: initial experience in four cases. Comparison of the Magill forceps and the Boedeker (curved) intubation forceps for removal of a foreign body in a manikin. Epiglottitis in the United States: national trends, variances, prognosis, and management. Review of transoral laser microsurgery for cancer of the upper aerodigestive tract. Update on the etiology, diagnosis, and treatment of vocal fold nodules, polyps, and cysts. Airway management in pediatric patients undergoing suspension laryngoscopic surgery for severe laryngeal obstruction caused by papillomatosis. Anesthesia management in pediatric patients with laryngeal papillomatosis undergoing suspension laryngoscopic surgery and a review of the literature. Percutaneous transtracheal jet ventilation for paediatric endoscopic laser treatment of laryngeal and subglottic lesions. Postoperative management of the airway with a Ravussin cricothyroid cannula in head and neck surgery. Fires of endotracheal tubes of three different materials during carbon dioxide laser surgery. The Hunsaker MonJet tube with jet ventilation is effective for microlaryngeal surgery. Transtracheal high frequency jet ventilation for endoscopic airway surgery: a multicentre study. Transtracheal jet ventilation in 50 patients with severe airway compromise and stridor. Comparison of superimposed highfrequency jet ventilation with conventional jet ventilation for laryngeal surgery. Comparison of local anaesthesia with dexmedetomidine sedation and general anaesthesia during septoplasty. Topical nasal anesthesia for transnasal fiberoptic laryngoscopy: a prospective, double-blind, cross-over study. Thunderclap headache and reversible segmental cerebral vasoconstriction associated with use of oxymetazoline nasal spray. Comparison of total intravenous anesthesia using propofol and inhalational anesthesia using isoflurane for controlled hypotension in functional endoscopic sinus surgery. Intravenous anesthesia provides optimal surgical conditions during microscopic and endoscopic sinus surgery. Visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy: what about the costs Practice advisory for the prevention and management of operating room fires: an updated report by the American Society of Anesthesiologists task force on operating room fires. Perioperative management of obstructive sleep apnea: a survey of Veterans Affairs health care providers.
Buy genuine innopran xl line
Case reports and series have shown promising results with decreased pain and analgesic requirements pulse pressure locations buy cheap innopran xl 80mg on-line. Intrathecal Medications If intractable pain persists despite optimized oral or intravenous therapy, a single shot or tunneled intrathecal catheter trial can be performed and an implantable drug delivery system should be considered. Continuous intrathecal infusions minimize fluctuation of drug levels in cerebrospinal fluid and allow for significant analgesia and use of spinal adjuncts (local anesthetic, ziconitide) in addition to opioids with significantly lessened dose-limiting side effects. In summary, perioperative pain syndromes of the urogenital system and those related to pain from malignant or nonmalignant disease require prompt attention, a comprehensive assessment, and consideration of multimodal early intervention including treatment with nonopioid or opioid medications, neuraxial and regional nerve blocks, and neuromodulation or surgery when appropriate. Surgical, radiographic and endoscopic anatomy of the retroperitoneum, kidneys, and ureters. Transurethral prostatectomy syndrome and other complications of urological procedures. Ventricular tachycardia during extracorporeal shock wave lithotripsy for renal stone disease. Radical cystectomy, radical nephrectomy and retroperitoneal lymph node dissection. The renal excretion of hydrogen ion in renal tubular acidosis, I: quantitative assessment of the response to ammonium chloride as an acid load. Mechanisms of renal excretion of drugs (with special reference to drugs used by anesthesiologists). An approach to pain management in end stage renal disease: considerations for general management and intradialytic symptoms. Renal effects of enflurane and halothane in patients with abnormal renal function. Biotransformation and hepato-renal function in volunteers after exposure to desflurane (I-653). Serum and urinary inorganic fluride levels after prolonged inhalation of sevoflurane in man. Clinical characteristics and biotransformation of sevoflurane in healthy human volunteers. Effect of halothane on renal hemodynamics during normovolemia and hemorrhagic hypovolemia. Comparison of the effects of isoflurane and desflurane on cardiovascular dynamics and regional blood flow in the chronically instrumented dog. Binding of thiopental to plasma proteins: effects on distribution in the brain and heart. The pharmacodynamics and pharmacokinetics of vecuronium in patients anesthetized with isoflurane with normal renal function or with renal failure. Interaction of cyclosporin and its solvent, Cremophor, with atracurium and vecuronium: studies in the cat. Pharmacokinetics of mivacurium in normal patients and in those with hepatic or renal failure. Attenuation of furosemide diuretic effect by indomethacin: pharmacokinetics evaluation. Comparative pharmacology of calcium antagonists: nifedipine, verapamil and diltiazem. Blood levels of the metabolites of glyceryl trinitrate and pentaerythritol tetranitrate after administration of a two-step preparation. Risks and outcomes of acute renal failure following surgical repair of ruptured abdominal aortic aneurysms. Outcome in patients who require renal support after surgery for ruptured abdominal aortic aneurysm. Does the administration of mannitol prevent renal failure in open abdominal aortic aneurysm surgery Meta-analysis: low dose dopamine increases urine output but does not prevent renal dysfunction or death. Atrial natriuretic peptide for management of kidney injury: a systematic review and meta analysis. Fenoldopam to prevent acute kidney injury after major surgery-a systematic review and metaanalysis. Review of prostate anatomy and embryology and the etiology of benign prostatic hyperplasia. Benign prostatic hyperplasia: etiology, pathophysiology, epidemiology, and natural history. Benign Prostatic Hyperplasia: Diagnosis and Treatment, Clinical Practice Guideline. Surgical and anaesthetic considerations in transurethral resection of the prostate. Clinical and experimental evaluation of different irrigating fluids for transurethral surgery. Perioperative myocardial ischaemia in patients undergoing transurethral surgery: a pilot study comparing general with spinal anaesthesia. Routine cross-matching is not necessary for a transurethral resection of the prostate. Baerwald J, et al: Irrigation fluid absorption during transurethral resection of the prostate: spinal vs. Morbidity, mortality and early outcome of transurethral resection of the prostate: a prospective multicenter evaluation of 10,654 patients. Comparison of perioperative mental function after general anaesthesia and spinal anaesthesia with intravenous sedation. Dilutional hyponatremic shock: another concept of the transurethral prostatic resection reaction. Fluid absorption and circulating endotoxins during transurethral resection of the prostate. Ammonia toxicity resulting from glycine absorption during a transurethral resection of prostate. Factors influencing the mortality and morbidity of transurethral prostatectomy: a study of 2015 cases. Gender and body mass index as risk factors for bladder perforation during primary transurethral resection of bladder tumors. Body temperature changes during prostatic resection as related to the temperature of the irrigating solution. The effect of warm irrigation on blood loss during transurethral prostatectomy under spinal anesthesia. Holmium laser enucleation of the prostate technique for benign prostatic hyperplasia. Comparison of standard transurethral resection, transurethral vapour resection and holmium laser enucleation of the prostate for managing benign prostatic hyperplasia of >40g. Transurethral holmium laser enucleation of the prostate versus transurethral electrocautery resection of the prostate: a randomized prospective trial in 200 patients. Holmium laser enucleation versus transurethral resection of the prostate: results from a 2-center, prospective, randomized trial in patients with obstructive benign prostatic hyperplasia. A randomized trial comparing holmium laser enucleation of the prostate with transurethral resection of the prostate for the treatment of bladder outlet obstruction secondary to benign prostatic hyperplasia in large glands (40 to 200 grams). Outcomes and complications after 532 nm laser prostatectomy in anticoagulated patients with benign prostatic hyperplasia. High-power potassiumtitanyl-phosphate photoselective laser vaporization of prostate for treatment of benign prostatic hyperplasia in men with large prostates.
Order genuine innopran xl
Preterminal events include decreased level of consciousness arteria dorsalis pedis buy innopran xl 80 mg online, which can progress to seizure and coma, disseminated intravascular coagulation, hepatic necrosis, renal failure, and gastrointestinal hemorrhage. A total of three patients brought from West Africa to the United States experienced multiorgan failure requiring mechanical ventilation and renal replacement therapy. Advanced life-sustaining therapy was managed at Emory University Hospital, Serious Communicable Disease Unit; at the University of Nebraska Medical Center-Nebraska Medicine, Nebraska Biocontainment Unit; and at Texas Health Presbyterian Hospital Dallas. More important than the unique physical structure of the units located in the United States and Europe within which patients with highly communicable diseases receive care is the culture of safety and preparedness, including the critical importance of training healthcare workers to care not only for the patient, but for themselves as well. Given that blood viral titers can exceed 108 virus particles per milliliter, it is not surprising that even highly trained healthcare workers have become infected. In all situations, patients become infected and, in some cases, die as a result of lack of appropriate training and a lack of the critical knowledge specific to the pathophysiology of each disease as well as the logistics of caring for patients while protecting oneself. The "dirty side" on the map is where patients are treated and gear is considered contaminated. At a minimum, providers should be wearing a facemask when entering the room of a patient with suspected influenza, including perioperative areas such as the preoperative holding area or postanesthesia care unit. When moving a suspected influenza patient on droplet precautions from one area of the hospital to another, having the patient wear a facemask during transport is prudent. This would of course include transport to and from the operating room if deemed medically safe and appropriate. We should only perform procedures on patients with suspected or confirmed disease that are critical to optimizing care. Some of the issues to address to minimize complications associated with intubation include ensuring availability of all medications that may be required and access to all likely equipment that might be needed to secure the airway. Finally, all healthcare staff must be instructed to review and understand the guidelines for personal protection appropriate for each pathogen. It is highly recommended that the addition of a powered air purifying respirator be included when providers are doing any medical procedure with high risk of aerosolization. For this reason, the entire doffing process should be strictly supervised by a doffing partner. Report of the mission dispatched by the Secretary general to investigate allegations of the use of chemical weapons in the conflict between the islamic republics of Iran and Iraq. An organized, comprehensive, and security-enabled strategic response to the Haiti Earthquake: a description of pre-deployment readiness preparation and preliminary experience from an academic anesthesiology department with no preexisting international disaster response program. Surgery under extreme conditions in the aftermath of the 2010 Haiti earthquake: the importance of regional anesthesia. Airway management of tetanus after the Haitian earthquake: new aspects of old observations. Business continuity after catastrophic medical events: the Joplin medical business continuity report. Anesthesia for Indian Ocean tsunami-affected patients at a southern Thailand provincial hospital. Use of death counts from vital statistics to calculate excess deaths in Puerto Rico following Hurricane Maria. Differential and persistent risk of excess mortality from Hurricane Maria in Puerto Rico: a time-series analysis. The initial response to the Boston marathon bombing: lessons learned to prepare for the next disaster. The dark morning: the experiences and lessons learned from the Tokyo subway sarin attack. Centers for Disease Control and Prevention; Department of Health and Human Services, National Institute for Occupational Safety and Health. Lessons learned: critical care management of patients with Ebola in the United States. Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: a modelling study. Ebola virus disease in West Africa-the first 9 months of the epidemic and forward projections. Clinical presentation, biochemical, and haematological parameters and their association with outcome in patients with Ebola virus disease: an observational cohort study. Critical care for multiple organ failure secondary to ebola virus disease in the United States. Safety considerations in the laboratory testing of specimens suspected or known to contain Ebola virus. Some ophthalmic surgeries (cataract, glaucoma, simple vitrectomy) are short procedures, but high in volume. A working knowledge of the anatomy and physiology of the eye is essential in providing safe anesthesia care. This includes the effect of anesthetic drugs and interventions on intraocular pressure and systemic effects of ophthalmologic medications. Orbital blocks, particularly retrobulbar blocks, can have severe complications, including retrobulbar hemorrhage, and retrograde spread of local anesthetic into the subarachnoid space causing brainstem anesthesia, loss of consciousness, and respiratory arrest. Routine preoperative laboratory testing is not necessary for cataract surgery and has not been shown to reduce adverse perioperative events. Strabismus surgery is an independent risk factor for postoperative vomiting in pediatric patients. Succinylcholine can be used in unfasted patients who have an open-globe injury that requires emergent vision-saving surgery under general anesthesia. Prevention of prolonged postoperative anesthesia care unit stay and unanticipated hospital admission requires careful patient evaluation, optimization of underlying medical conditions, adequate pain control, prevention of postoperative nausea and vomiting, and maintenance of hemodynamic stability. Overview of Ophthalmic Anesthesia Vision is one of the most important functions of the human body. Anesthesia providers specialized in ophthalmic anesthesia play an important role in helping patients undergo surgery comfortably and safely. The majority of ophthalmic surgeries are short in duration and primarily 2194 performed in ambulatory surgical centers. Patients who undergo ophthalmic surgery can be as young as preterm infants to nonagenarians. Ophthalmic procedures are generally considered low risk because they do not cause significant physiological perturbations, and do not involve a large volume of blood loss or significant postoperative pain. Adequate preoperative evaluation and optimization are important in the prevention of same day cancellation and unplanned hospital admission. Fast-track surgery has been successfully implemented in ophthalmic surgery to facilitate early discharge home and to allow patients to resume normal activities of daily living. Perioperative surgical home is a patientcentric, team-based model of care to improve population health, reduce costs, and satisfy patients. Patient satisfaction has become a standard indicator of value in health care, including anesthesia care. The wall of the globe has three layers: the sclera, the uveal tract, and the retina. It is the tough, fibrous white of the eye, and it is continuous with the cornea anteriorly. The tissue where the cornea and sclera meet is the limbus, which contains stem cells responsible for regeneration of the epithelium. The middle layer, the uveal tract, has three structures: the choroid, the iris, and the ciliary body. The pigmented iris controls light entry with muscle fibers that change the size of the pupil. Sympathetic stimulation dilates the pupil by causing iris dilator muscles to contract, whereas parasympathetic stimulation causes meiosis, or pupillary constriction by causing the iris sphincter muscles to contract. Uveitis is an inflammatory condition of these structures (iris, choroid, and ciliary body). The innermost eye layer is the retina, which is a membrane consisting of highly specialized nerve tissue continuous with the optic nerve. Light stimulates retinal photoreceptors to produce neural signals that the optic nerve carries to the brain.
Order innopran xl with visa
A single injection of opioid combined with a small dose of local anesthetic in the subarachnoid space is quick to perform blood pressure medication pros and cons discount generic innopran xl uk, provides rapid analgesia, and dissipates when no longer needed. A single spinal injection for labor analgesia can be utilized in a parturient who is unable to hold still to facilitate placement of an epidural but is usually reserved for when the duration of labor can be reasonably estimated, such as in multiparous parturients with advanced dilation or in the second stage of labor. Continuous spinal analgesia with a spinal catheter can be considered in the case of accidental dural puncture or in the high-risk parturient. A catheter-over-needle system provides the option for a 23-gauge intrathecal catheter placed over a 27-gauge pencil-point spinal needle. It is most commonly placed utilizing the "needle-through-needle" technique, which involves identification of the epidural space through a lossof-resistance technique followed by insertion of a long, pencil-point spinal needle (25-27 gauge) into the intrathecal space. After the epidural space is located with the epidural needle, a pencil-point spinal needle is inserted utilizing the "needle-through-needle" technique and the dura is punctured. A perfect labor analgesic recipe provides excellent analgesia without motor blockade or other maternal or fetal effects. Low concentrations of local anesthetics (alone or in combination with opioids) are used to maximize sensory blockade and minimize motor blockade and maternal hypotension from sympathetic blockade. Ropivacaine and levobupivacaine were synthesized to reduce cardiotoxicity that occurs with inadvertent intravascular bolus doses of bupivacaine. However, with the dilute concentrations of local anesthetic currently used for labor analgesia, cardiotoxicity is uncommon. The addition of fentanyl to bupivacaine has been shown to reduce local anesthetic requirements while still providing similar pain relief. The most troublesome complication that limits the dose of epidural fentanyl and sufentanil is pruritus. The search for the perfect labor epidural drug combination has led to the use of other adjuvant drugs that can reduce the dose of required local anesthetic. Epinephrine is a nonselective adrenergic agonist activating 1-, 2-, 1-, and 2-adrenergic receptors. Activation of 1-receptors in the epidural vasculature causes vasoconstriction that delays the vascular uptake of local anesthetic and opioid. Intrathecal or epidural neostigmine produces analgesia by increasing acetylcholine stimulation of spinal muscarinic and nicotinic receptors. A randomized controlled trial compared bupivacaine use in laboring patients when neostigmine versus fentanyl was added and found no difference in bupivacaine requirements. The continuous infusion is commonly utilized because it allows the maintenance of a steady anesthesia level without frequent, time-consuming manual boluses by the anesthesia provider. Relative contraindications may include systemic infection, preexisting neurologic disease, severe cardiac valvular stenosis, and pharmacologic anticoagulation. The decision to place neuraxial anesthesia should be individualized for the patient and the risks and benefits should be considered. It controls pain of the first stage of labor only and is more effective than placebo or intramuscular meperidine. More commonly, side effects of transient fetal bradycardia and maternal local anesthetic toxicity have been reported. It has become safer with more superficial injection ensured by a needle guide and more dilute solutions of local anesthetic. The pudendal nerve is derived from sacral nerve roots (S2S4) and can be blocked with local anesthetic using a transvaginal or transperitoneal approach to treat pain during the second stage of labor and for episiotomy repair. Although a pudendal nerve block provides some relief during second stage, it is not as effective as a subarachnoid block with fentanyl and bupivacaine. Anesthesia Considerations for Operative Delivery Low-dose epidural analgesia can be inadequate for assisted vaginal delivery with forceps or vacuum. In this setting, a higher concentration local anesthetic can be administered through an indwelling epidural catheter. Supplementation of an indwelling epidural catheter with 5 to 10 mL of 1% to 2% lidocaine or 2% to 3% 2-chloroprocaine is usually adequate, depending on whether vacuum or forceps are being used. Although maternal mortality substantially decreased during the first half of the twentieth century, the maternal mortality ratio has not declined in over 25 years and appears to have recently been increasing in the United States. However, it appears that the risks associated with general anesthesia have decreased significantly over time to the point where it is difficult to say that avoiding general anesthesia prevents maternal mortality. Use of neuraxial anesthesia for cesarean delivery minimizes exposure of the neonate to maternal anesthetic medications, avoids airway manipulation, improves postoperative pain, and allows the mother to see the child almost immediately after birth. All pregnant women should undergo a preoperative evaluation, regardless of planned delivery mode or type of anesthetic technique, with appropriate risk and benefit counseling. The current status of the fetus and obstetric management plan also should be taken into consideration when formulating the anesthetic plan. In addition, appropriate equipment and medications should always remain readily available to safely provide general anesthesia for an emergent or unanticipated situation. Although the rates of significant maternal aspiration of gastric contents with induction of general anesthesia are difficult to determine, the mortality from such an event is estimated at 5% to 15% based on retrospective data. At present, most cesarean deliveries in developed countries are performed with neuraxial techniques. Compared with an epidural, a single injection spinal is often faster and technically easier to perform, allows adequate operating conditions in a shorter time, provides a denser block, is more cost effective, and is less likely to fail (failure rate <1%). On occasion, a continuous spinal catheter may be used for anesthesia for cesarean delivery. As previously discussed, a spinal catheter may be placed in the case of an inadvertent dural puncture but can be placed intentionally for cesarean delivery in high-risk obstetric patients. The chance of significant maternal hypotension is greater with spinal anesthesia than with epidural anesthesia. Left uterine displacement with appropriate administration of fluids and use of vasopressor medications can minimize the associated hypotension. Intravenous administration of crystalloid or colloid can reduce the degree of hypotension after spinal anesthesia for cesarean delivery. Of note, fluid co-loading is thought to have limited efficacy in consistently preventing postspinal hypotension and is typically utilized in combination with a vasopressor. Historically, ephedrine was considered the vasopressor of choice to manage hypotension caused by neuraxial anesthesia in pregnancy; however, prophylactic or therapeutic phenylephrine in boluses or as an infusion is not only effective in reducing hypotension but also has less transfer to the fetus and results in less fetal acidosis than ephedrine. There is increasing interest in norepinephrine as an alternative vasopressor for treating spinal hypotension. Compared to phenylephrine, norepinephrine had similar efficacy for maintaining arterial blood pressure during spinal anesthesia for cesarean delivery and was associated with a greater heart rate and cardiac output. Although various local anesthetics can be used for spinal blockade, hyperbaric bupivacaine 10 to 12 mg is frequently used to achieve an adequate (T4) level block. Neither patient height nor weight affect block extension,169 although dosing may require adjustment at extremes of the height spectrum. Lipid soluble opioids (such as fentanyl or sufentanil) may be added to enhance neuraxial blockade by reducing local anesthetic dose and decreasing stimulation from surgical traction of the viscera. Typical epidural local anesthetic volumes required for cesarean delivery range between 10 and 20 mL, depending on whether the epidural is already in use. The administration of epidural local anesthetic should occur in divided doses to ensure that the catheter has not migrated into the intravascular or intrathecal space. Block quality can be improved with addition of epinephrine 1:200,000, fentanyl 50 to 100 g, or sufentanil 10 to 20 g. Epidural clonidine 50 to 100 g can be useful in patients with preexisting chronic pain or severe hypertension if the benefit is judged to outweigh the risk for hypotension, bradycardia, and sedation. Epidural morphine 2 to 5 mg is frequently administered to improve postoperative pain. This technique allows for the rapid onset of a dense reliable block while allowing the block time or height to be extended with use of the epidural catheter. In addition, it allows for a controlled airway, controlled ventilation, and in some scenarios such as massive hemorrhage, improved hemodynamic control and perhaps decreased maternal psychological stress in comparison to neuraxial anesthesia. Appropriate equipment preparation, knowledge of patient comorbidities, airway examination, and familiarity with the difficult airway algorithm are necessary preparation for delivering a safe general anesthetic. Clear, concise communication among all members of the perioperative team is especially critical in urgent or emergent situations to maximize patient safety and minimize procedural complications. A catheter-based technique allows for the ability to titrate the local anesthetic to the proper block height and provide additional local anesthetic administration during the case. For patients who do not already have a catheter in place, this technique may be chosen if the procedure is anticipated to take additional time, or if maternal comorbidities would favor a more gradual, controlled onset of epidural anesthesia. Achieving surgical block conditions takes longer with an epidural than spinal technique but can be rapid enough for use in many urgent situations if already in place and used for maternal analgesia.
