
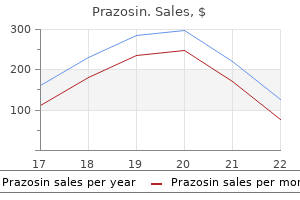
Cheap prazosin american express
Introduction Risk assessment and management is an essential skill for any healthcare provider cholesterol levels breastfeeding trusted 2.5 mg prazosin. Questions regarding risk of harm to self and others arise in multiple domains, from outpatient clinics to acute psychiatric inpatient units or forensic facilities. Practitioners from all disciplines are often called upon to provide expertize in this arena, despite different levels of training or experience with such questions. Most commonly, clinicians must assess and manage the risk of violence or harm to others or oneself. The role of the healthcare provider in the assessment and management of risk is paramount. Substance abuse or dependence A diagnosis of substance abuse or dependence is the second most validated predictor of violence, both independently and when combined with other mental health factors. Social stressors Relationship instability, unemployment, poor social supports, a history of victimization, and homelessness have all been shown to increase the risk for violence. Demographics Patients who exhibit violence at younger ages have an elevated risk of violence. Similarly, men are more likely to commit violent acts than women, though gender-related differences in rates of violence are less pronounced among persons with a mental disorder. The availability of the potential victim should be considered, as should access to firearms or other weapons. As these situations do not often present in a clear-cut manner with obvious answers, a structured approach to risk assessment is essential. However, in the past 30 years, we have improved our awareness of the epidemiological risk factors for violence. Additionally, there has been an appropriate shift from an emphasis on the prediction of violence toward the assessment of risk for violence. J Of note, most violent individuals are not psychotic and most psychotic individuals are not violent. Personality disorders: Antisocial and borderline personality disorders have been shown to elevate the risk for violence. People who meet the criteria for psychopathy, typically assessed via the Hare Psychopathy Checklist, Revised, are at a relatively high risk for engaging in violent, threatening, and other behaviors. Cognitive disorders: People with cognitive disorders, especially those with a history of head injury, have an elevated risk of violence. Additionally, in an elderly population, there is an increased representation of cognitive disorders in those who commit violent acts. Clinical characteristics: Impulsivity, active symptoms of major mental illness, lack of insight and self care, confusion, low intelligence, and negative attitudes elevate the risk of violence. Acute findings in a mental status examination associated with violence include hostility, suspicion, agitation, thought disturbance, command hallucinations, and anger. Then, when a more detailed violence inquiry is required, guided clinical assessment techniques should be considered. Intersection of multiple risk factors Once comorbid substance abuse and personality disorder are taken into account, the contribution of psychosis to violence in the community diminishes dramatically. Additionally, violence is significantly correlated with various sociodemographic and environmental factors, wherein the contribution of mental illness is relatively small. Violence Risk Assessment Tools There are numerous instruments designed to assess risk of violence in psychiatric and correctional populations. Tools that employ structured clinical judgment are currently considered the gold standard. The following table lists some of the most common peerreviewed and validated instruments used and their methods of assessment (Table 1). Nonmental health variables can be significant Do not focus exclusively on mental health concerns. Nonmental health variables contribute more significantly to the overall rate of violence than do mental health variables. Risk Assessment for Suicide and Violence Risk Factors for Suicide 61 Additionally, substance abuse is a significant risk factor for violence among all the populations studied. Symptomatology is more relevant than diagnosis Imminent risk of violence may be mediated and predicated by acute psychiatric symptoms, whereas long-term risk is associated best with historical variables. Previous history of suicide attempts As with violence risk, a history of prior suicide attempts is the single biggest risk factor for suicide. Clinical Pitfalls Overgeneralization Most literature on violence risk assessment has originated from forensic settings and, therefore, much of it may not apply to general psychiatric or primary care settings. It is important to contextualize the risk to the population that needs assessment. Failing to get collateral Consultation with knowledgeable third parties is an important adjunct tool in the assessment of violence. Gender: Research has consistently shown that men are at a higher risk for completed suicides by a factor of approximately 4:1. Age: Risk increases with age for men, with elderly men in the highest age risk group. Marital status: Married persons are at a lower risk than those who are single, divorced, or widowed. Residence: There are relatively higher rates of suicide among those who live alone, have moved recently, live in urban (vs. Clinicians who ignore this responsibility expose themselves to the risk of legal action. Overall, however, in terms of individual risk assessment, suicide is relatively infrequent, and therefore difficult to predict. Therefore, an effective assessment of suicide risk is essential for care providers across all disciplines, not just those in mental health. A vast majority of people who commit suicide are suffering from a diagnosed mental illness. Psychiatric disorders associated with suicide include mood disorders (bipolar affective and major depressive disorders), substance abuse, anxiety disorders, impulse control disorders, personality disorders, and psychotic disorders. J Specific research in people with schizophrenia who commit suicide suggests that young white males with good premorbid history and good intellectual functioning and who are in the early course of their illness are at an elevated risk. J Other risk factors include depressive symptoms, active hallucinations, insight, and comorbid chronic physical illness. Clinical characteristics: Current symptoms of depression with hopelessness are important indicators of increased risk. Anxiety, sleep difficulties, and anhedonia have also been shown to place people at an increased risk. Other well-studied markers include agitation, fear of mental 62 Risk Assessment for Suicide and Violence disintegration, poor adherence, and recent loss. Social stressors the acute disruption of a major interpersonal relationship, social isolation, and imprisonment are risk factors. Intersection of multiple risk factors Patients with more than one psychiatric illness are at a higher risk of suicide. Clinicians should document the data supporting the assigned level of risk, the level of care required, and treatment plans to reduce suicide risk. Structured approaches to suicide risk assessment have been developed, but there is no empirically determined cutoff score on any of these measures demonstrated to predict in an absolute sense who will attempt or commit suicide. Several common approaches are the following: Suicide Risk Assessment Tools Unfortunately, no model of suicide assessment has been proven to be more effective than others. Identify and assess the factors that actively influence risk with an eye toward what can be modified. Protective factors: What are the protective factors such as family or social support Collateral information: Wherever possible, communicate with family, friends, or other providers. Risk should be considered imminent if the patient expresses the intention to die, has a cogent plan, and has lethal means available. However, there is no empirically determined cutoff score on any of these measures demonstrated to predict in an absolute sense who will attempt or commit suicide. Clinical Pearls Always ask about suicide specifically Physicians are sometimes reluctant to ask patients about suicide, fearing that the question may lead to suicidal thinking and precipitate suicidal acts. Get collateral Routinely contact and interview several family members and close friends, inquiring specifically on examples of morbid preoccupations and suicidal thoughts. If a patient refuses to allow consent to contact others, then take this into consideration in the risk assessment process. This is an essential component of the suicide risk assessment and should not be neglected. Furthermore, it combines actuarial and clinical approaches, and involving the patient in the process as much as possible.
Generic 2.5 mg prazosin otc
Multicultural factors also play a critical role in scientific and clinical assessment in developmental neuropsychology kind of cholesterol in eggs order 5 mg prazosin amex. For example, ethnicity itself does not cause variability in cognitive test performance, although cognitive differences do exist between ethnic groups. Rather, ethnicity appears to be a marker for a number of contributing environmental and cultural factors that impact neuropsychological performance. Such factors include quality of education, disease burden, 528 Encyclopedia of the Neurological Sciences, Volume 3 doi:10. Clarification of the interplay between neuropsychological functioning and environmental influences on neural circuitry continues to be a focus of research. Understanding these moderating variables can aid in treatment development by promoting or abating pertinent environmental factors. Individual moderating factors affecting neuropsychological outcome include age of onset, type of syndrome, etiology, and response to pharmacological agents. Researchers in developmental neuropsychology strive to understand the influence of neurochemistry and neuroanatomy on eventual cognitive and behavioral outcomes, how moderating factors in the environment support or alter neuropsychological functioning, how developmental stage at time of injury impacts outcome, and the efficacy of diverse interventions for neuropsychological disorders. In terms of structural correlates of neuropsychological abilities, the epilepsy literature is an example that has linked neuropsychological deficits directly to anatomical, functional, and metabolic markers of cerebral functioning. Alterations in the expected developmental course are particularly important for identifying etiological factors of disorders. Dysfunction in areas of executive functioning, emotion regulation, attention, working memory, and temporal processing has not only been linked to learning disabilities, but also to childhood psychiatric disorders. There has been a recent surge in research examining the efficacy of treatment interventions for neuropsychological disorders in childhood. The first examines the applicability of neuropsychological results to inform treatment decisions. Second, research determining which neuropsychological factors impede treatment and to what extent will advance the efficacy of individualized treatment plans. Third, attention has been directed toward how to best incorporate brain imaging into treatment plans as a means of monitoring intervention success and aiding in overall diagnostic practices. Additional relevant information includes family history of medical and psychiatric disorders. Neuropsychological Clinical Assessment the neuropsychological clinical evaluation involves a comprehensive assessment of psychological and emotional functioning. Finally, as part of the evaluation process, the clinical developmental neuropsychologist highlights specific diagnoses and what the impact of the diagnoses may be in both the short and long term, recognizing that re-evaluation may best serve to monitor the developmental course. Recommendations for treatment, remediation, or accommodations are included in the report. Impact on academic achievement of learning and behavior problems is discussed, and accommodations are recommended for parents and the school. Strengths in particular serve as the focus in determining which intervention strategies may be most productive. Treatment Interventions the underlying neural substrates of developmental neuropsychological disorders are yet to be fully understood, making treatment decisions particularly difficult. However, the field of developmental neuropsychology utilizes a variety of modes through which the treatment and interventions are provided. Although these interventions are nascent in nature, they provide hope for establishing even more effective treatment models. The goals of neuropsychological treatment interventions are to assist with recovery of function or compensation for deficits. Methods for attaining these goals include pharmacological intervention and cognitive remediation. Pharmacological interventions may be effective in treating behavioral symptoms of a variety of neuropsychological disorders. However, difficulty surrounding pharmacological treatment decisions exists due to scant research on effects of childhood pharmacological interventions. Continued research in childhood pharmacology is needed to weigh the risks and benefits, as well as short- and long-term effects, and to determine how medications affect the developing brain. As future research unlocks the ambiguities of brain disorders, scientists can better determine appropriate pharmacological treatment and possibly develop drugs that target specific neuropsychological or cognitive abilities. Cognitive rehabilitation is a therapy employed to train the brain to adapt or compensate for the neuropsychological deficits. It can be difficult to target abilities for cognitive rehabilitation in children due to the complexity of childhood brain injuries and the tendency for childhood deficits to be diffused rather than focal. Therefore, further research is needed to understand the overall effectiveness of cognitive remediation and the optimal frequency and duration of treatment. Across all treatment modalities, neuroimaging techniques may be useful in identifying pathological changes in the brain, ruling out structural abnormalities, assessing secondary effects of a lesion or disease, determining changes that occur over time, and relating treatment to outcome. Before writing the report, an interpretive feedback session with the parents and consultation with the referral source is an opportunity to gather additional information. Scores based on normative data ideally will take into account demographic information such as age, ethnicity, and gender. The use of neuroimaging along with multiple treatment modalities has a potential synergistic effect for improved neuropsychological outcome. Overall, the goal of intervention is to improve adaptive functioning, which includes not only improved cognitive abilities but also improved ability to maintain social relationships, improved academic performance, and decreased psychological distress. Future Directions In recent years, the field of developmental neuropsychology has quickly advanced in terms of clinical and scientific understanding of neuropsychological disorders. However, many questions remain, and the challenges facing developmental neuropsychology as it progresses forward as a science and clinical practice involve normative samples, research, and treatment applicability. Current sets of normative data for standardized child testing measures are often based on rather homogeneous groups and only stratified by age. Such limited representativeness across normative samples leads to inappropriate comparisons between children in a clinical setting and limited generalizability of research studies. There is a need for normative data that are developed with large sample sizes, across a number of ethnic groups, and stratified by age, handedness, gender, and education level. Additionally, minimal clinical normative sample groups for between- and within-group comparisons of various disorders complicate interpretation of functioning. Of particular concern are overdependence on case studies, small sample sizes, exploratory analyses, and homogeneity of samples. Future research needs to focus on the recovery of function, treatment outcome, reliability and validity of testing instruments, and clinical significance of findings. Better understanding of these areas will lead to better pharmacological treatment, assessment, and interventions. Researchers and practitioners must recognize the moderating variables affecting treatment outcome and their potential impact on the treatment intervention. Reed J and Warner-Rogers J (2008) Child Neuropsychology: Concepts, Theory, and Practice. Definition Neuropsychology is the study of the relationship between brain function and behavior. Pierre Flourens, a French physiologist, argued against the ideas of phrenology, using his work with animals to discredit the idea. Flourens removed regions of the brain and studied the subsequent behavioral changes. He found that the amount of damage in the brain determines the extent of loss of function, which led him to conclude that there were no areas of specific function in the brain. Despite the fact that phrenology has been discredited, the theory that specific mental functions can be localized in the brain has remained important to this day. The prominence of this theory relates directly to the work of Pierre Paul Broca and Carl Wernicke. In 1861, Broca published his findings of a patient who had lost his ability to speak but could understand language. In 1876, Carl Wernicke published a paper describing another type of aphasia in which patients lose their ability to comprehend language, but have the ability to speak. By the early twentieth century, localization of function was a widely accepted concept in the field. However, not all scientists accepted this view, including the American experimental psychologist Karl Lashley. Unable to reconcile either view, other neuroscientists began to develop more integrated theories of brain function.
| Comparative prices of Prazosin | ||
| # | Retailer | Average price |
| 1 | The Home Depot | 340 |
| 2 | Dollar General | 683 |
| 3 | 7-Eleven | 201 |
| 4 | Verizon Wireless | 813 |
| 5 | Sports Authority | 323 |
Prazosin 5 mg for sale
Postictal paralysis usually lasts between 10 s and 30 min and only rarely continues for hours or days cholesterol test fasting guidelines order prazosin with amex. Postictal Signs Mediated by the Autonomic Nervous System Major seizures, particularly secondary generalized convulsions, can produce massive activation of sympathetic outputs with catecholamine release and parasympathetic suppression. Autonomic dysfunction may persist into the postictal period resulting in tachycardia and systemic hypertension. Postictal Headache Visual and Somatosensory Repetitive or prolonged occipital seizures can produce transient postictal visual loss including cortical blindness and visual field deficits. Postictal somatosensory impairments with focal and hemisensory deficits (including hemineglect) are also well documented but infrequently reported. Severe migraine-type postictal headaches often last several hours or even days and usually respond to acute treatment with triptan medications. Severe muscle contractions Encyclopedia of the Neurological Sciences, Volume 3 doi:10. Neuronal depolarization during seizures may activate the trigeminal vascular system and trigger migraine due to increases in calcitonin gene-related peptide and substance P. Seizures may trigger the glutamate-mediated cellular hyperexcitability associated with cortical spreading depression in migraine. Patients may develop new transient depressive symptoms during the postictal period or may have exacerbation of interictal depressive symptoms. The onset of depressive symptoms is usually delayed by several hours or even several days following seizures, lasts a median of 1 day, and may emerge from postictal delirium. Ligand-binding positron emission tomography studies show relative increases in focal opioid receptor availability following temporal lobe seizures which may be linked to affective changes. Postictal Neuropsychological and Behavioral Manifestations Postictal Amnesia Transient memory impairment is common following seizures and usually evolves out of more general postictal confusion. Postictal amnesia not only is particularly common following temporal lobe seizures (and seizures propagating into medial temporal areas) but also may occur due to disordered attention with frontal lobe seizures. Postictal amnesia is particularly severe in patients with underlying injuries and seizures involving bilateral medial temporal structures. Severe status epilepticus can cause acute neuronal injury, marked by elevations in neuron-specific enolase, and can produce severe prolonged and even permanent amnesia. Postictal Delirium Postictal delirium may last from seconds to many hours depending on the severity and duration of seizures. Early postictal hypoactive forms of delirium are associated with confusion and withdrawn behavior and can evolve into a hyperactive delirium with agitated, poorly controlled behaviors. Some patients who appear to have prolonged postictal delirium, in fact, have nonconvulsive status epilepticus, a continued ictal state. Postictal Psychosis Postictal psychosis often emerges immediately out of postictal delirium but may occur after a latent period of lucidity (mean 20 h). Postictal psychosis is often manifested as delusions with affective symptoms such as religious or persecutory delusions, heightened emotionality, and pressured speech. Patients often have other signs of brain injury such as Postictal Blood Chemistry and Cerebrospinal Fluid Changes Complex partial and generalized seizures can disrupt hypothalamic regulation and produce postictal elevations in serum Postictal Manifestations 955 prolactin, luteinizing hormone, and follicle-stimulating hormone. Seizures trigger increases in adenosine, an inhibitory neuromodulator, which contributes to the cessation of seizures and may contribute to a postictal refractory period. Additionally, severe seizures can produce inflammation and neuronal injury resulting in postictal cytokine and neuronspecific enolase increases. Epileptic Seizures Further Reading Devinsky O (2008) Postictal psychosis: Common, dangerous, and treatable. Kanemoto K, Kawasaki J, and Kawai I (1996) Postictal psychosis: A comparison with acute interictal and chronic psychoses. It is characterized primarily by new progressive weakness, fatigue, and pain after a period of prolonged stability. This poliomyelitis results in flaccid paralysis and in some cases, diaphragmatic paralysis and respiratory failure as well. Polio-related disability is typically static in nature after the initial polio attack, although minor gradual changes in strength and function can occur slowly over decades. Fortunately, polio vaccines have virtually eliminated polio in most countries in the world. Although a few countries continue to have endemic poliovirus, massive epidemics of infections such as those of the early 1900s, which left millions of people permanently disabled or dead, are no longer seen. Today, there are approximately 20 million polio survivors worldwide, including more than one million in the United States. Data from the United States suggest that nearly half of the survivors have residual paralysis resulting in functional impairment. This is experienced as lack of energy and endurance, and sometimes as a sudden onset of generalized exhaustion after minimal physical activity. Other impairments as described above are less frequently seen, but can be quite disabling. It is also distinct from slowly progressive minor strength and functional decline that some polio survivors experience. A period of partial or complete functional recovery after acute paralytic poliomyelitis, followed by an interval, usually 415 years of stable neuromuscular function. Gradual onset of progressive and persistent new muscle weakness or decreased endurance, with or without generalized fatigue, muscle atrophy, or muscle and joint pain. Onset may follow trauma, surgery, or a period of inactivity and can also be sudden. Exclusion of other neuromuscular, medical, and orthopedic problems that could explain symptoms. With years of overwork, these surviving motor nerves may lose their ability to meet the metabolic demands of serving all the muscle fibers. Terminal axon sprouts die back, and the muscle fibers they once served become denervated. Superimposed on this loss, anterior horn cells die out with normal aging, further reducing the motor neuron pool and the muscle fibers they serve. When there are too few muscle fibers to provide necessary motor power, new muscle weakness and atrophy may manifest. Some have suggested hormone deficiencies or environmental toxins as pathogenic, but there has not been any scientific evidence to-date to support these theories. Specific pathophysiology underlying the symptoms of fatigue and pain is not well understood, including the relationship of these symptoms to initial polio infection. Palliative care physicians can also provide patients and families with pain and symptom management and support in adjusting with life change. Studies of prednisone (anti-inflammatory agent) and insulinlike growth factor 1 (nerve growth factor believed to promote new axon sprouting) have not shown clinical benefit and are not currently recommended. Studies of intravenous immune globulin are ongoing, and conflicting results about its impact on strength and pain remain to be clarified. Progressive muscle weakness and atrophy are generally believed to be associated with motor unit dysfunction. It is also important to provide supportive counseling for those for whom the experience of new symptoms and need for assistive devices may cause distressing recollections of the initial experience with polio. These factors include weight gain, smoking, excess alcohol use, and muscle overuse. In addition, exercises to maintain muscle and joint flexibility (stretching and range of motion) can reduce the risk of contractures and pain. Aerobic exercises (low-resistance dynamic activity using large muscle groups, with cardiopulmonary training effect) can reduce the risk of secondary diseases, psychological distress, poor sleep quality, and loss of bone density. Balance exercises (improving unipedal stance and functional reach) can reduce the risk of falls. In some neuromuscular diseases, nondepolarizing neuromuscular blockers used during anesthesia carry a risk of severe effects such as malignant hyperthermia. Activity modification, energy conservation techniques, and the use of lower extremity orthoses or mobility devices can help mitigate fatigue. Energy conservation techniques include modifying timing or pacing of activities, incorporating frequent rest breaks into exercise or work regimens, utilizing new techniques for daily activities, and utilizing adaptive technology. Physical and occupational therapists can offer individualized guidance regarding these strategies. They can also perform home and workplace evaluations and recommend environmental modifications to mitigate fatigue and maximize energy and endurance.
Buy cheap prazosin 2.5 mg line
However cholesterol medication for ibs order prazosin 2.5mg visa, anatomical studies have shown that each of these feedforward projections is reciprocated by a feedback projection. Functional Subsystems A further possible relation between anatomical structure and physiological maps is indicated by the hypothesis that there are separate neural pathways for processing information about different visual properties, such as motion, depth, color, and shape. Physiological and anatomical studies in monkey brain indicate that this segregation of neural pathways begins in the retina, and different compartments within early visual areas project to different high-level areas. In the following sections, the processing that leads to the perception of motion, depth, color, and form in the human brain is discussed. Motion Objects in the world move relative to each other and to the viewer in a nearly ceaseless pattern of change. Motion processing encompasses different kinds of information, such as the derivation of the speed and direction of a moving target, the motion boundaries associated with an object, or the structure of an object determined from its coherent motion. Given the range of functions that motion processing subserves, this may not be surprising. Indeed, converging evidence suggests that some aspects of motion processing are localized in dedicated modules in the human brain. Several elegant studies have used the perceptual illusion of the motion after-effect In addition, it has been shown that the activation of this area is enhanced when subjects attend to or track motion. Another intriguing aspect of motion cue is related to the perception of biological motion, or the motion of people and animals. Humans can perceive biological motion from impoverished visual displays in which points of light are attached to the joints of a person moving in an otherwise dark room. From these sparse displays, people can discriminate the type of motion (running, dancing, etc. Color appearance results from neural processing of these cone signals within the retina and brain. One emphasizes regions in cortex that may play a special role in color perception and the second emphasizes a stream of color processing stages beginning in the retina and extending into the cortex. Human neuropsychological studies suggest that damage to a cortical region on the ventral surface of the occipital lobe, in the collateral sulcus, interferes with normal color processing. They measured the difference in activity caused by achromatic and colored stimuli. The area showing a significant change of activity was located in the collateral sulcus and is the same area implicated in achromatopsia. Although the area associated with color signal tends to correspond with the foveal representation, some researchers refer to the area as V4, whereas others suggest that the color-responsive area is beyond V4 and that it should be called V8. Other results from several laboratories show that opponent color signals can be measured in a sequence of visual areas, including early visual areas. For example, for certain stimuli, the most powerful responses in area V1 are caused by lights that excite opponent color mechanisms. Moreover, moving stimuli, seen only by opponent color mechanisms, evoke powerful activations in motion-selective areas located in the lateral portion of the parietooccipital sulcus. Further research should reveal the processing stages and mechanism underlying color perception. Depth Compared to the work that has been performed on motion and form processing, there are fewer studies concerning the processing of depth, surfaces, and three-dimensional (3D) structure. Like the processing of visual motion, the analysis of depth can involve both low-level cues, such as disparity, derived from the retinal images and high-level inferred attributes, such as the surfaces corresponding to retinal points with different disparities. Moreover, studies using eventrelated potentials recorded from electrodes placed directly on the cortical surface of patients before surgery found objectspecific waveforms that show stronger activation for a variety of objects In ventral cortex there is a consistent relationship between eccentricity maps and object selectivity. These experiments suggest that the entire object-selective region may be organized along an eccentricity axis that could be relevant to the way in which humans perceive different object categories. Note that the face area overlaps with foveal representations and the place area overlaps with peripheral representations. Object-, face-, and place-selective regions are depicted on the inflated brain of one subject. The brain was inflated using specialized software to enable visualization of regions buried inside sulci. These regions were also selectively activated when subjects perceived simple shapes that were created via illusory contours, color contrast, stereo cues, texture boundaries, grayscale photographs of objects, or line drawings. Thus, these regions may constitute a neural substrate for the convergence of multimodal object representations. However, evidence from lesion studies demonstrates that damage to the fusiform and occipitotemporal junction results in a variety of recognition deficits. In addition, studies in humans have shown that electric stimulation of similar regions interferes with recognition processes or, in some cases, can create an illusory percept of an object or a face. Together, these findings suggest that these regions may be necessary (and perhaps even sufficient) for object recognition. The following question arises: How many categoryselective regions of cortex exist in the human visual pathway Selectively activated focal regions of cortex were reported for other categories as well, including animals, tools, letter strings, and even body parts. The critical question is whether these lower responses reflect a critical involvement of these stimuli in the representation or recognition of other objects. What is the basis of the functional organization in the ventral processing stream Conclusions By virtue of physiological and anatomical study, a number of important observations have been made about the functions of the occipital lobe. Second, several of these stages contain a retinotopic representation of the visual field. However, ascending through the processing stages the retinotopic mapping becomes coarser, whereas the functional properties of these areas become more complex. This is consistent with the idea that processing of visual information requires both local processing in lower visual areas and more complex operations extracting global attributes in high-level stages. Although a hierarchical model for the processing of color, object recognition, and motion exists with discrete areas responding to specific modalities, a more distributed network of cells is also operative to allow for finer resolution of the visual world. Kanwisher N, Downing P, Epstein R, and Kourtzi K (2000) Functional neuroimaging in visual recognition. A single midline caudal central subnucleus innervates both the levator palpebrae superioris muscles. Distinct rootlets enter the interpeduncular fossa and merge into one root or trunk, which travels through the subarachnoid space between the posterior cerebral and superior cerebellar arteries. The oculomotor nerve pierces the dura and passes into the cavernous sinus, traveling along the lateral wall, together with the first and second divisions of the trigeminal nerve and the fourth cranial nerve. On entering the superior orbital fissure, the oculomotor nerve fibers separate into superior and inferior divisions and enter the orbit. The inferior division sends fibers to the inferior and medial recti, inferior oblique, and ciliary ganglion. The superior division delivers fibers to the superior rectus and levator palpebrae superioris. Disruption may occur at any location along the path of the nerve and subsequent paresis may occur in any muscle or combination of muscles innervated by the oculomotor nerve. The third nerve may be affected in isolation or there may be associated neurological symptoms and signs that facilitate localization. Aberrant regeneration should not be a component of microvascular ischemia and should also prompt investigation for another etiology. A complete pupil-sparing third nerve palsy is characterized by the same findings, except in conjunction with a normal pupillary examination. Partial third nerve palsies are common and are represented by weakness of any combination of oculomotor innervated muscles. The presence or absence of aberrant regeneration should be evaluated at the time of initial third nerve paresis presentation and at each subsequent examination. Aberrant regeneration represents anomalous axonal innervation and clinically manifests as cocontraction of individual third nerve-innervated muscles, such as elevation of the eyelid or constriction of the pupil on adduction or depression of the eye. Temporal lobe uncal herniation from elevated intracranial pressure due to intracranial, subdural, or epidural hemorrhage must be ruled out in cases of severe head trauma and lethargy or in any patient in an intensive care setting who develops sudden unilateral pupillary dilation. Given the proximity of the pituitary gland to the cavernous sinus and the location of the oculomotor nerve in the dural cavernous sinus wall directly lateral to the pituitary gland, a pituitary adenoma with or without pituitary apoplexy or a parasellar tumor such as craniopharingioma or meningioma may lead to unilateral or bilateral third nerve dysfunction. Aberrant regeneration often occurs following the acute stage of the third nerve palsy.
Buy prazosin master card
Other muscle attachments such as the temporal arch cholesterol test validity proven 2.5mg prazosin, formed by the zygomatic and temporal bones, as well the temporal lines of the parietal bones, and the gonial angle of the mandible, anchor muscles that assist in the movements associated with chewing and speaking. This discussion reviews the more firmly established relationships between sleep and epilepsy and sleep disorders in people with epilepsy. Sleep activated additional epileptic foci in some patients who had only one focus during wakefulness. Among the earliest findings was that nearly two-thirds of seizures occurred between 8 p. These findings suggested that peaks in seizures occur in response to falling asleep and awakening. Secondary generalization of focal seizures is more common during sleep than wake, and frontal lobe seizures tend not to secondarily generalize during sleep. Circadian influences appear to affect timing of focal seizures, varying by the type and location of the epileptic generator. Seizures of mesial temporal origin may be particularly vulnerable to these effects, with a peak time of occurrence from 3 to 7 p. Effects of Sleep Deprivation on Epilepsy the effect of sleep deprivation on epilepsy has been the subject of extensive investigation. Sleep deprivation has long been recognized as a seizure precipitant, reported in one-third of patients with epilepsy. In people with focal epilepsy, the odds of a seizure increase with progressive sleep loss, suggesting that modest amounts of sleep loss can precipitate seizures. For most seizure types, sleep and sleep-deprived recordings produce similar activation rates. Whether a lesser degree of sleep loss produces comparable results remains unknown. Sleep Organization in Epilepsy A variety of sleep architectural abnormalities have been reported in people with epilepsy. Despite 190 Sleep and Epilepsy frequent self-reported drowsiness and sedation in people with epilepsy, surprisingly few studies have objectively measured this common complaint. Primary sleep disorders also affect vigilance, sleep quality, and quality of life in people with epilepsy. In older patients with epilepsy, the presence of sleep apnea is associated with worsening seizure control or late-onset seizures. A score of 0 or less is very unlikely to be seen in epilepsy, whereas patients scoring 3 or greater generally have epilepsy. Conclusions Over a century of work has confirmed crucial links between sleep and epilepsy. Sleep deprivation and unrecognized or untreated sleep disorders increase the likelihood of daytime sleepiness and seizures. These observations underscore the importance of the routine assessment of sleep and wake complaints in all people with epilepsy. Differentiating Nocturnal Seizures from Parasomnias and Other Paroxysmal Events the differential diagnosis of abnormal motor activity in sleep is illustrated in Table 3. Frontal lobe seizures are often misdiagnosed as sleep terrors, sleepwalking, or nightmares (Table 3). Steriade M, Conteras D, and Amzica F (1994) Synchronized sleep oscillations and their paroxysmal developments. Zucconi M, Oldani A, Ferini-Strambi L, Bizzozero D, and Smirne S (1997) Nocturnal paroxysmal arousals with motor behaviors during sleep: Frontal lobe epilepsy or parasomnia Definition Sleep is a normal, physiological state in which alertness is reduced in a readily reversible manner. Sleep and wakefulness are cyclical and relate to subcortical centers that regulate the circadian rhythm. Since 1975, this technique has yielded rich descriptions of heretofore unsuspected physiological dysfunction in sleep and led to the creation of the new field of sleep disorders medicine. Sleep Disorders: Clarification and Diagnosis In a classification scheme proposed by the American Sleep Disorders Association in 1990, sleep disorders were subdivided into four major categories. This scheme groups most of the known sleep symptoms and signs into syndromes that correspond to the International Classification of Diseases nomenclature. It is beyond the scope of this entry to give an account of all the coded sleep disorders. However, there are general concepts and guidelines that must be taken into consideration for a correct diagnosis and treatment of the most serious and common sleep disorders. Evaluation of Sleep Complaints Until recently, sleep was neither observed nor objectively measured so that physicians were literally groping in the dark in their diagnostic efforts. Sleep laboratory studies indicate that there are two kinds of errors in subjective reporting: overestimation of time spent awake in insomnia and underestimation of the physiologically significant respiratory disturbances that occur in sleep. Insomnia patients perceive their 1 or 2 h of sleep loss as 3 or 4 h, whereas the apneic patient is completely unaware of the hundreds of sleep arousals that occur when cyanotic with a low oxygen saturation. This irony is compounded by the insomniac, who is often anxious and may put great pressure on the physician for a prompt, uncritical, and even potentially dangerous therapeutic response, whereas the apneic patient, perhaps urgently needing a tracheotomy, sits lethargically and uncomplainingly. Documentation can be accomplished in several direct and simple ways before referral for sleep laboratory evaluation. A sleep log can be kept for at least 2 and preferably 4 weeks following an initial visit. On a single sheet, each line of which represents 24 h, the times of retiring, falling asleep, arousals, awakening, and arising are recorded. Dated entries corresponding to the lines indicate subjective state and behavioral data for the intervening waking periods. Another source of documentation is actigraphy, which provides data regarding normal and abnormal sleep in its natural habitat. Because movement distinguishes wakefulness from sleep and even punctuates sleep in a predictable pattern, simple actigraphic monitoring provides useful data about circadian and ultradian rhythm control. The Nightcap is sensitive to most of the parameters relevant to the diagnosis and treatment of insomnia. Sleep laboratory studies still provide the only definitive means of documenting the diagnostic signs of the major sleep disorders. If narcolepsy, nocturnal myoclonus, or sleep apnea cannot be ruled out by the simple means described previously, referral to a sleep laboratory is indicated. Because so much has been made of the value of sleep laboratory evaluations, it is worthwhile to note some of their limitations. Adaptation effects have already been mentioned: It is common, especially for anxious subjects, to sleep poorly for one, two, or even three nights in an unfamiliar place, so little confidence can be placed in studies of insomnia lasting less than four successive nights. Therefore, sleep laboratory evaluation, which is an expensive and disruptive procedure, may not provide definitive diagnosis, especially for the most common problems. The Insomnias the insomnias can be subdivided into initial, midterm, and terminal insomnias, according to difficulties falling asleep, maintaining sleep throughout the night, and awakening early in the morning, respectively. All of these variants can present at the same time and in the same subject, as in the case of insomnia due to an anxiety disorder (initial and midterm insomnia) or depression (sleep maintenance and early awakening problems). The insomnias can also be classified according to the duration of symptoms as transient, short-term, intermediate-term, and persistent or chronic insomnias. Although a short-term (less than 2 weeks) pharmacological trial with sleeping pills is indicated for transient and short-term insomnias, a more thorough investigation is needed for intermediate-term cases and for the chronic insomnias, for which sleeping pills can only be a short-term add-on treatment to the etiological therapeutic plan. Most experts maintain that although the short-acting hypnotic benzodiazepines are clearly safer than the older barbiturates, they should not be used for consecutive periods longer than 2 or 3 weeks because they can provide only symptomatic relief and subjects habituate rapidly to them and may experience rebound insomnias when they are stopped. Insomnias that are related to chronic anxiety disorders are thus problematic because their treatment usually requires longer-term trials. Some of the new nonbenzodiazepine agents, such as zolpidem or eszopiclone, minimize the effects of withdrawal and allow longer and safer periods of treatment, especially in persistent insomnias of the elderly. Melatonin agonists, at least in some countries, are among the drugs used for initial insomnia. Melatonin, short or long acting, may help children and the elderly sleep or readjust jet lag and phasedelayed syndrome, among the most common circadian disorders due to misalignment of the sleep period with the working and relational society clock. The first two symptoms are mandatory for the diagnosis and distinguish this syndrome from other hypersomnias. Narcoleptic patients usually have disrupted nocturnal sleep with multiple arousals sometimes related to breathing disorders but often due to periodic limb movements. Most recently, sodium oxybate (g hydroxybutyrate) has been 196 Sleep Disorders considered as the first-line treatment for both cataplexy and poor-quality nocturnal sleep. Less common forms of hypersomnia include the idiopathic and recurrent hypersomnias. Among the latter, gabapentin and pregabalin, an a2d-ligand, have been promoted as firstline drugs, especially when sensory symptoms prevail over motor expressivity. Bruxism, noisy grinding or clenching of the teeth during sleep, and rhythmic movement disorder, such as head banging and body rocking, are other types of sleep-related movement disorders that may endanger sleep continuity through repetitive arousals.
Syndromes
- Ringing in the ears
- Proton pump inhibitors (for people with gastroesophageal reflux)
- Salmon patches are small, pink, flat spots. They are small blood vessels (capillaries) that are visible through the skin. They are most common on the forehead, eyelids, upper lip, between the eyebrows, and on the back of the neck. Salmon patches may be more noticeable when the infant cries or during temperature changes.
- Dizziness for the first time
- Cancer treating drugs, or other medicines (see list below)
- Tear test
- Pens, pocketknives, and eyeglasses may fly across the room.
- A small amount of electric current will then be delivered to your head to cause seizure activity in the brain. It lasts for about 40 seconds. You will receive medicine to prevent the seizure from spreading throughout your body. As a result, there will be only slight movement of your hands or feet during the procedure.
- Excessive bruising
Discount prazosin master card
Clinical manifestations include severe and persistent headache cholesterol eating chart order prazosin 2.5mg overnight delivery, motor deficits, visual abnormalities, seizures, altered mental status, vertigo, speech disturbances, sensory impairment, and ataxia. In acute or subacute transverse myelitis, there is a diffuse necrotic reaction believed to be the result of a hypersensitivity reaction to ova in sensitized persons. Schistosomainduced vascular inflammation leading to infarction of the spinal cord is another possible mechanism. Schistosomal myelopathy occurs predominantly in young adult males living in rural areas. Most patients present with a short history, with symptoms developing over a few days to a few weeks. Occasionally, symptoms develop acutely within 24 h (myelitic form) or evolve gradually over many months. Common presenting features are low back pain often radiating into the saddle area and lower limbs. The weakness may typically progress over days or weeks to severe flaccid paraparesis or paraplegia. When higher levels of the spinal cord are affected, an altered sensory level on the trunk may be identified. The knee and ankle reflexes are commonly abolished, but brisk reflexes may be found in cases of transverse myelitis. Species determination is aided by evaluating the location and size of the spine protruding from the egg. An enzyme-linked immunotransfer blot assay is useful for species-specific diagnosis. Conversion to seropositivity usually occurs within 3 months of initial infection but can be delayed for a couple of weeks after the onset of symptoms of neuroschistosomiasis. Of course, serological evidence of schistosomiasis does not prove that specific neurological symptoms are due to schistosomal infection. Ultrasonography is useful for evaluating the portal and urinary tracts of affected individuals. Spinal Schistosomiasis Spinal cord schistosomiasis is less common than the cerebral form and is due almost exclusively to S. In endemic areas, spinal cord schistosomiasis is a significant cause of nontraumatic paraplegia and is probably underreported. As with brain infection, ova may be present in the spinal cord without clinical symptoms. Schistosomal myelopathy is the result of ectopic schistosome ova migration with subsequent host reactions and tissue damage. The two main pathological processes are granuloma formation and necrotic or transverse myelitis. The most common site for intramedullary granulomas is the lower thoracic and lumbosacral spinal cord. Granulomas may be present on the surface of the spinal cord and roots of the cauda equina. Histological examination reveals granulomas in which ova may be identified, with perivascular cuffing or vasculitis, venous thrombosis, and hemorrhages. Granulomas are occasionally found at higher levels of the thoracic cord or in the lower cervical cord, but the T11 to L1 region is the most 98 Schistosomiasis Histopathology can reveal species-specific eggs with surrounding granulomatous reactions consisting of giant cells and surrounding lymphomononuclear infiltrates and eosinophils. Treatment Praziquantel is a safe, effective, and broad-spectrum oral schistosomicidal agent, and it is the drug of choice for the treatment of all forms of chronic schistosomiasis. The duration of therapy for neuroschistosomiasis, however, is not fully delineated. Durations of therapy varying from 1 to 14 days have been used with fairly good success, and 5-day courses have been recommended. Corticosteroids are not used for routine schistosomal infections but have been used for patients with neuroschistosomiasis. No randomized studies have been done to test the efficacy or dosing of steroids, but anecdotal reports suggest that they are quickly effective in blunting the immune response to the infection and in resolving neurological symptoms. Steroids should be used before the initiation of praziquantel therapy for acute neuroschistosomiasis associated with eosinophilic toxicity in early infections. In addition, patients not improving with medical management might benefit from granuloma removal when the spine is involved. Artemisinin derivatives hold potential for hindering the establishment and development of infection in contaminated individuals. Population-based treatments can decrease the load of parasites being released into the environment. Effective vaccines against schistosomiasis are not likely to be available in the near future. Caumes E and Vidailhet M (2010) Acute neuroschistosomiasis: A cerebral vasculitis to treat with corticosteroids not praziquantel. Prognosis In general, medical management is adequate with more than two-thirds of nonneuroschistosomiasis patients fully resolving the infection and arresting disease progression. Similarly, neurological infection can resolve, but residual myelopathy persists in a majority of spine-affected patients. Multidisciplinary rehabilitation strategies are especially important for patients with transverse myelitis. Introduction Psychosis is a heterogeneous term that is generally defined as a significant break with normal reality or functioning. Tactile, gustatory, or olfactory hallucinations are more common in psychosis secondary to a neurological condition. Hallucinations that occur only at the time of sleep onset or upon awakening are common, and are generally not considered to be clinically significant psychotic symptoms, unless they are frequent and negatively impact functioning. Delusions are fixed false beliefs that persist even in the presence of evidence to the contrary, and are not shared by members of a defined religion or subculture. They are problematic not solely for their presence or absence, but rather the extent to which they are preoccupying, distressing, and affect daily functioning. Disorganized thinking or speech, often referred to as formal thought disorder, represents a collection of deficits in the ability to produce logical and linear communication. It commonly manifests as a tangential thought process, where the associations between concepts become loosened, as measured by speech or writing. It often manifests in bizarre postures or movements and can be evident in extremely cluttered clothing or living environment. Differential Diagnosis the differential diagnosis for isolated psychotic symptoms is large (Table 1), and any new onset of significant psychotic symptoms demands a careful and thorough work up. Magnetic resonance imaging is recommended in cases of first psychotic presentation when motor signs, impaired levels of consciousness, or personality changes are seen. Primary Psychosis Persistent psychotic symptoms that are not secondary to a discrete condition or lesion are considered to be one of the several primary psychotic syndromes. Schizophrenia and Schizophreniform Disorder Schizophrenia is the prototypical disease of chronic primary psychosis. According to the World Health Organization, schizophrenia is one of the leading causes of functional impairment worldwide. There is growing evidence that certain drugs of abuse increase the risk for developing schizophrenia, especially when used heavily during adolescence. Onset of schizophrenia typically occurs in adolescence or early adulthood, with women having a slightly later age of onset than men. Families of people with schizophrenia tend to have higher rates of schizotypal and schizoid personality traits. Causal theories of schizophrenia revolve around several different neurotransmitter systems. The strongest body of evidence implicates dopamine transmission in the mesolimbic and mesocortical systems. Source: Reproduced with permission from Rose D (2010) Primary psychotic disorders. This psychotic symptom must generally coincide with at least one other psychotic symptom or any of the negative symptoms, which include affective flattening, alogia (poverty of speech), and avolition (lack of drive or motivation). Negative symptoms do not include anhedonia as part of the formal diagnosis of schizophrenia, though loss of pleasure is often associated with the negative symptoms. If the above criteria are met and the total time of disturbance has been less than 6 months, then the proper diagnosis is schizophreniform disorder. If, however, signs of disturbance in social and occupational functioning have been present for at least six months, 1 month of which must be the same time period accounting for Criterion A, then the diagnosis is schizophrenia.
Order 5mg prazosin with amex
Immunoglobulin and complement deposits have been found intracellular and adjacent to the internal elastic lamina in arterial biopsies good cholesterol definition 5 mg prazosin otc. If the temporal artery appears abnormal on physical examination, only a small 2 cm in length specimen needs to be removed for biopsy. It is important to remember that the inflammatory involvement of affected arteries is often intermittent rather than continuous. Temporal artery biopsy should ideally be performed before treatment is initiated, although evidence of arteritis in biopsies has been found even after more than 2 weeks of corticosteroid therapy. The pain in shoulder and pelvic girdles usually radiates distally toward the elbows and knees. The musculoskeletal pain is worse with movement of the affected area and commonly interferes with daily activities. Systemic manifestations can include fever, malaise or fatigue, anorexia, and weight loss which may be present for months and may be an early finding. On examination, active and sometimes passive movements of the shoulders are limited due to pain. The presence of synovitis in proximal joints and periarticular structures has been found in magnetic resonance 922 Encyclopedia of the Neurological Sciences, Volume 3 doi:10. Mononeuropathies may involve the median nerve at the wrist (carpal tunnel syndrome), peroneal, phrenic, or sciatic nerve. Also having the typical laboratory findings and rapid response to small doses of corticosteroids significantly contributes to the diagnosis. Mild to moderate normochromic or hypochromic anemia may be found in about two-thirds of the patients. Some may have mildly abnormal liver function test (increased alkaline phosphatase), thrombocytosis, eosinophilia, or hypergammaglobulinemia. The positive histopathological findings are characteristic of a panarteritis and giant cell granulomatous formation, with disrupted internal elastic lamina. The adventicia is usually invaded by mononuclear, and occasionally polymorphonuclear, inflammatory cells. It is always important to rule out any underlying infection, malignancy, or inflammatory arthritis. After diagnosis and treatment of neoplasia, musculoskeletal symptoms may completely resolve. The absence of improvement of symptoms should make the physician question the diagnosis. It is important to remember that reducing the dose of corticosteroids too quickly may result in flare-up of symptoms, and some patients cannot tolerate the outlined dose-reduction regimen. Relapses are more common in the first 18 months of treatment or after the prednisone dosage is reduced to less than 7. When symptoms recur and the acute phase proteins are normal, the possibility of other co-morbid conditions being responsible for the symptoms must be considered. Long-term treatment with corticosteroids requires the assessment of comorbid conditions and side effects. Out of all the drugs studied up to now, methotrexate seems to show the best evidence. Hazleman B (2000) Laboratory investigations useful in the evaluation of polymyalgia rheumatica and giant cell arteritis. However, in recent decades, great strides have been made in understanding some of its clinical pathology. Sleep does not represent a single state or distinct steps but rather a continuum through which the brain gradually passes and returns many times during a night. Data from these are collected, analyzed, and used to differentiate stages of sleep. Because clinical polysomnography is designed to measure not only sleep staging but also many other aspects of physiological parameters occurring during sleep, other parameters are also recorded. This is generally measured by using an oximeter, which passes specific wavelengths of light through the finger, toe, or other tissue, and records the intensity of light reaching the probe. This directly correlates with the percentage of oxygen saturation of hemoglobin in the blood. Less commonly, and for specific clinical situations, other measurements are utilized to precisely quantitate the volume of airflow moving in and out of the lungs, the airway pressure generated by the chest and abdominal movement, movement of the limbs, or measurements of penile erections during sleep. The list is not limited to these, however, and for specific purposes nearly every physiological parameter that can be assessed during wakefulness that is not measured in a painful or disruptive manner might be recorded during sleep. Clinical Focus Evaluation of sleep and clinical abnormalities during sleep has expanded dramatically in recent decades. Technology the modern sleep laboratory relies heavily on rapidly evolving advances in technology. In addition to the physiological parameters indicated previously, video recording and visual monitoring of the patient are also important observation techniques. Recording is done under infrared lighting so the patient can sleep in full darkness and yet events of interest can be analyzed. The accuracy of such home monitoring data is often less reliable than recordings in the laboratory. Indications the most common indication for clinical polysomnographic monitoring is suspected sleep apnea. The oximeter channel shows the percent oxygen saturation (and, toward the right side of the epoch, is seen falling as a consequence of the apnea). Toward the right edge of the epoch, the airflow resumes, associated with a body movement. They are manifested by specific respiratory pauses or breathing changes during sleep. Symptoms most commonly noted include loud snoring, fragmented nocturnal sleep, excessive daytime sleepiness, and sometimes partner observations of the patient having breathing pauses during sleep. The severity of sleep apnea is characterized by calculating variations of the Respiratory Disturbance Index (the number of breathing pauses per hour of sleep), the severity of oxygen desaturation, and the fragmentation and disruption of sleep. Once apnea is identified, various treatment options exist, including surgery on the airway, devices to maintain airway patency, patient positional therapy if apnea is confirmed to have a strong body position relationship, and weight loss if obesity is a major contributing factor. All these disorders need to be accompanied by the basic monitoring of sleep in order to correlate with sleep stages and identify the impact on sleep disruption. Correlation with Other Assessment Tools the previously mentioned examples demonstrate the vital role of clinical polysomnography in the diagnosis of multiple sleep disorders. Much of the modern polysomnography is dependent on advances in technology during the past few decades. The first sleep disorders clinic was established at Stanford University, California, in 1970. M1 and M2 are theoretically silent reference electrodes corresponding to the left and right mastoid processes, respectively. M1 and M2 are also sometimes referred to as A1 and A2, respectively, referring to auricle rather than mastoid process. The electrodes are applied to the surface of the scalp with an adhesive paste, conductive medium, or, more preferably, collodion. The addition of occipital electrodes facilitates the appreciation of background a-activity associated with the waking state, and its attenuation with eye opening and transition into sleep. Recording of endoesophageal pH can allow the appreciation of episodes of esophageal reflux and resulting disruption of sleep. In the clinical setting, calibrated or uncalibrated inductance plethysmography is the most commonly used sensor for qualitatively detecting respiratory effort. Inductive plethysmography utilizes piezo crystals embedded into bands or belts that are placed around the thoracic and abdominal regions of the patient. The crystals emit changes in voltages corresponding to movement of the abdominal and thoracic areas during breathing. Esophageal manometry quantitatively measures effort of breathing by monitoring pressure changes with the use of an endoesophageal balloon. Airflow the pneumotachograph is a device that measures airflow quantitatively by detecting flow of respiratory gases and comparing it to the pressure drop against a small resistive field. This is considered the gold standard for measuring airflow but, because the pneumotachograph is large and uncomfortable, qualitative measure of airflow, especially in the clinical setting, is a more widely accepted alternative. Qualitative measures of airflow include monitoring of changes in airway pressure and temperature at the nose and mouth of the patient. A nasal air pressure transducer measures pressure changes of the nasal airway between inspiration and expiration, providing an estimate of airflow.
Cheap prazosin 2.5 mg on line
In addition ideal cholesterol to hdl ratio cheap prazosin uk, Trk activation can lead to local signaling events in neurons, to modulate synaptic plasticity and acute remodeling of dendritic structures. The transmembrane receptor p75 is a member of the tumor necrosis factor receptor family, and encodes an intracellular death domain. P75 binds to all mature neurotrophins, and can modulate Trk signaling via direct actions and through effects on signal transduction. These are transported retrogradely to the cell body and culminate in changes in gene expression. Local delivery of neurotrophins at the cell bodies of neurons can also promote survival. Specifically, distinct mitogen activated protein-kinase species are activated by Trks at the cell body as compared with those activated by retrograde Trk signaling. Neurotrophins can be anterogradely transported to axons and released from a neuron following depolarization. Trk receptors are present on the dendritic spines of postsynaptic neurons, and activation leads to an enhanced synaptic activity. Vertebrate Nervous System, Development of the Further Reading Ascano M, Bodmer D, and Kuruvilla R (2012) Endocytic trafficking of neurotrophines in neural development. Hamburger V and Levi-Montalcini R (1949) Proliferation, differentiation and degeneration in the spinal ganglia of the chick embryo under normal and experimental conditions. Signaling Location the biological actions of neurotrophins also differ depending on the location at which a neuron is stimulated. In many fishes the case is clear, where the two nerves are joined only by simple contact, and in the camelion not at all, as is said. Reproduced from Brewster D (1855) Memoirs of the Life, Writings, and Discoveries of Sir Isaac Newton, vol. Brewster D (1855) Memoirs of the Life, Writings, and Discoveries of Sir Isaac Newton, vol. As the major addicting component of tobacco, it is linked to millions of deaths from cardiovascular and pulmonary disease. As a stimulator of functionally important acetylcholine receptors, nicotine has played an important role in the history of neuroscience. It has multiple effects on behavior and these include locomotion, mood, cognition, and pain, as well as addiction. Differentiation of cholinergic receptors into subclasses based on the actions of the plant alkaloids muscarine and nicotine played an essential role in the development of concepts of neurotransmission in the central and peripheral nervous systems. Drugs that act on these muscarinic and nicotinic receptors play a critical role in clinical medicine. In addition, nicotinic receptors appear to be involved in a variety of neurodevelopmental and degenerative processes. The use of new molecular and pharmacological approaches to further differentiate cholinergic receptor subtypes and develop more selective drugs may lead to the development of more effective therapies in the future. However, it is now clear that both pre- and postsynaptic nicotinic receptors of various subtypes exist in the central nervous system and are important for motor function, pain, and cognition. The neuromuscular nicotinic receptor is the most extensively studied member of the superfamily of receptors. Many different approaches have been used to study nicotinic receptors, particularly recently using molecular approaches such as constructing transgenetic and knockout mice and inducing mutations in the genes for the receptors. Such approaches allow scientists to understand the relationships between the structure and function of the receptor. Structure Five subunits, labeled alpha, beta, gamma, delta, and epsilon, form allosteric membrane proteins that compose the structure of the ligand-gated ion channel as various subtypes in welldefined combinations. A dozen or so subunits have been characterized in different amounts in different brain regions and in different species. Physical loops constituting intracellular and transmembrane components have been identified. Nicotinic receptors can also be broadly classed as those containing a b2 subunit that binds nicotine with high affinity and those like a7 that bind bungarotoxin, a snake venom toxin. The most common nicotinic receptor subtypes in the central nervous system are a4b2, a3b4, and a7. However, more than 30 nicotinic receptor subtypes have been identified in the brain. The study of nicotinicbinding sites in the central nervous system was assisted by the use of radioactively labeled nicotine and acetylcholine (with selective blocking of muscarinic sites). Although the distribution of nicotinic receptors in the central nervous system remains to be fully elucidated, a4 and b2 units are distributed widely, whereas a3, a7, and b4 are less abundant and are more often located in subcortical structures. Numerous genes for the subunits have been identified on various different chromosomes including 2, 8, 11, 15, 17, and 20. History the work of Otto Loewi at the turn of the twentieth century laid the foundation not only for the identification of neurotransmitters as chemical entities but also for the conception of their mechanism in the brain through their effects on proteins that were labeled neurotransmitter receptors. The classic distinction between muscarinic and nicotinic receptors has been enriched by the understanding that muscarinic receptors are linked through G proteins to second messenger systems and tend to have slower action compared to nicotinic receptors. A variety of agents can block the often inhibitory consequences of the muscarinic receptor activity. Nicotinic receptors, however, are composed of a structurally related family of ion channels that are predominantly excitatory and active over a short period of time. Historically, nicotinic receptors were first characterized at the neuromuscular junction by taking advantage of the large numbers of receptors found in a variety of species with modified organs associated, for example, with creating electrical discharges as a mechanism for organism defense The nicotinic receptors at the neuromuscular junction have been studied extensively in relation to human diseases such as myasthenia gravis. Here, autoimmune phenomena contribute to receptor dysfunction and the resulting muscle weakness. Early studies in the central nervous system focused on the identification of muscarinic receptors. Five kinds of muscarinic receptors have been cloned, with the M1 receptor being more common in telencephalic areas. The identification of nicotinic receptors in the brain was delayed because Function Many nicotinic receptors appear to modulate neurotransmitter release through excitatory mechanisms. Such presynaptic action affects the release of acetylcholine, dopamine, noradrenaline, serotonin, g-aminobutyric acid, and glutamate. In some circuits such autoreceptor action provides a feedback loop to reduce the release of acetylcholine. The different subunits are structured in different patterns that have different functional effects. The molecular structure Encyclopedia of the Neurological Sciences, Volume 3 doi:10. Complex systems of tubes, vestibules, and pores compose the receptor and determine its interactions with drugs, naturally occurring neurotransmitters, and ions. Other species such as snails have specific receptors and binding proteins on glial and other cells. The elucidation of the functional properties has been enhanced by the ability to express receptor combinations in cell lines. Nicotinic receptors have also been found to have binding sites in addition to the principal binding sites for the native neurotransmitter. A variety of modulatory sites have been proposed, perhaps the most interesting of which is a noncompetitive activator site or so-called allosteric modulating site. Nicotine receptors are located throughout the brain including in the cortex, hippocampus, basal ganglia, thalamus, cerebellum, basal forebrain, and brainstem, as well as the retina and cochlea. From a systems perspective, nicotinic receptors have a role in directly stimulating not only pre- and postsynaptic neurons but also other functions. For example, nicotinic receptors are located in the blood vessels and can modulate blood flow. A considerable amount of knowledge has been gained by studying nicotinic receptors in association with smoking (and other forms of drug abuse). Interestingly, exposure to nicotine by inhaling cigarette smoke increases the number of receptor-binding sites. In humans and animals models mecamylamine and other nicotinic receptor antagonists can alter cognition and a variety of behaviors. The effects of nicotine on effects in human beings in vivo are complex and include peripheral and central effects. Clinical Relevance An understanding of the effects of nicotine on the brain has led to attempts to treat nicotine addiction as well as several neurological and psychiatric diseases. Various nicotinic chewing gums, patches, and other formulations can be used to diminish smoking behavior, particularly if associated with behavioral management.
Discount prazosin online visa
Skin potential abnormalities with a loss of skin potentials in the lower extremity have also been described cholesterol lowering foods in malayalam buy 5mg prazosin overnight delivery. The heart rate response to deep breathing and the Valsalva ratio are usually normal and often large. Patients with prominent venous pooling may have an excessive reduction in pulse pressure. Our own early experience based on both preliminary as well as a prospective study lead to the same conclusion. Over time, function improves although patients will continue to complain of some symptoms (albeit less). Management Management is based on a detailed history, examination, and a medical evaluation including cardiological and autonomic laboratory evaluation. The cardiological evaluation includes an electrocardiogram, a 24 h Holter monitor, and a decision as to whether cardiac electrophysiological studies should be undertaken. The neurological evaluation comprises a neurological history, examination, and tests seeking evidence for an autonomic neuropathy. The autonomic laboratory evaluation comprises an autonomic reflex screen and thermoregulatory sweat test. The clinician should document the severity of orthostatic intolerance and seek evidence of autonomic neuropathy, or history of vasovagal syncope. For patients with bronchospasm, a b-selective lipophilic agent such as metoprolol can be used in a low dose Midodrine appears to work best in terms of absorption, predictable duration of action, and lack of central nervous system side effects. If this fails to control the storms, clonidine, which is administered at a dose of 0. This concern is based on findings of reduced cardiac distensibility and atrophy, which responds well to a program of exercise (endurance training). Vertigo and Dizziness Further Reading El-Sayed H and Hainsworth R (1996) Salt supplementation increases plasma volume and orthostatic tolerance in patients with unexplained syncope. Introduction the neurological state of a woman can change during pregnancy or during the postpartum period. The focus of this article is the more common neurological symptoms or disorders that develop in the mother during pregnancy, including eclampsia-induced seizures, depression, stress, and cognitive changes. Many, but not all, of these symptoms resolve themselves after delivery and are specific to the period of pregnancy. Pregnancy is characterized by enormous increases in the production of hormones, such as chorionic gonadotropins, placental lactogen, progesterone, and estrogen, and these hormones can act on the central nervous system to have neurological effects. Indeed, there appears to be a relationship between many neurological syndromes and the altered maternal hormone levels. Estrogen has been shown to have effects on cognitive function such as learning and memory, with reports demonstrating differences across the menstrual cycle and after menopause, as well as during pregnancy. Thus, it is not surprising that the dramatic changes in hormone levels during gestation have neurological consequences for the mother. The management of neurological diseases during pregnancy often needs to be adjusted to ensure that the fetus (as well as the mother) is not harmed. Several neurological syndromes that can change in frequency in association with pregnancy are described here, along with a summary of how these syndromes may be managed differently during pregnancy than at other times. Seizures and Pregnancy Hormones of Pregnancy To understand the relationship between maternal hormone levels and the neurology of pregnancy, it is first necessary to have an understanding of the major hormones of pregnancy and their changes during gestation. This high level of progesterone can have both direct effects in the brain as well as serve as a precursor for the synthesis of neuroactive steroids, such as dihydro- or tetrahydroprogesterone, which affect numerous neurotransmitter receptors. Although progesterone is the major hormone of pregnancy, estrogen levels also increase during pregnancy. The increase in estrogen levels also begins to occur at approximately day 50 of pregnancy, and levels increase thereafter during gestation. The major source of estrogen synthesis during pregnancy is the fetus and placenta, acting in cooperation. It should be noted that the major estrogen produced by the fetus and placenta is estriol, which is less potent than 17b-estradiol, the major hormone produced by the ovaries during the menstrual cycle. Numerous neurological conditions and certain aspects of cognitive function are affected by the hormones of reproduction. In addition to elevated blood pressure, preeclampsia is characterized by proteinuria, edema, headache, visual disturbances, epigastric pain, or vomiting. In addition, preeclampsia can progress to eclampsia in approximately 1 in 75 women, in which seizures can occur without any warning. The cerebral changes that occur in women undergoing eclampsia-induced seizures can include cerebral edema, hemorrhage, cerebral venous thrombosis, hypoxic-ischemic damage, microinfarcts, and coagulopathy. However, in those women in whom eclampsia has developed and in whom seizures have occurred, it may be necessary to manage the seizures with anticonvulsants such as phenytoin or magnesium sulfate or, if necessary, a benzodiazepine. Along with eclampsia, seizures associated with epilepsy can pose a serious risk to the mother and potentially the fetus. The management of epilepsy during pregnancy is greatly complicated by an increased risk to the fetus of congenital malformations that may result from antiepileptic drugs. However, because uncontrolled seizures are usually not a viable alternative, and seizure risk and threshold can change during pregnancy, it is generally necessary to treat pregnant women with epilepsy with antiepileptic medications. Several alternative courses of action are recommended, depending on the individual. If possible, women of child-bearing potential should avoid taking certain anticonvulsants that have a high risk of inducing fetal malformations. Often, a pregnant woman is maintained on the same regimen of medication that she had been on before the pregnancy, but drug levels in the blood 968 Encyclopedia of the Neurological Sciences, Volume 3 doi:10. Polytherapy should be avoided as it appears to pose the greatest risk of malformation to the fetus. It has been proposed that sex steroid hormones may be a factor underlying this sexual dimorphism. Migraine and Pregnancy the occurrence of headaches such as migraines is sexually dimorphic, with women experiencing more chronic headache than men. In women, migraine frequency is altered depending on the levels of hormones, particularly the changes in estrogen and progesterone concentrations that occur across the menstrual cycle, during pregnancy, menopause, or following oral contraceptive use. Although migraine headaches may worsen during the first trimester of pregnancy, their frequency generally decreases during the second and third trimesters. Moreover, migraine itself is not a risk factor for pregnancy or fetal complications. For those women who suffer migraines during pregnancy, it is often recommended that they rely on nonpharmacological treatments. If medication is necessary, acetaminophen or codeine can be used or, if these are not effective, ibuprofen or naproxen sodium can be taken for short periods. Several recent studies following women who took sumatriptan during pregnancy suggested that there was no or at most extremely little difference in pregnancy outcome compared with women who had not taken sumatriptan. The one adverse outcome associated with sumatriptan use was a slight, nonsignificant increase in preterm delivery and smaller birthweight. There did not appear to be an increase in congenital malformations caused by sumatriptan during pregnancy. Maternal Depression Most studies on maternal depression involve the examination of postpartum depression, which is generally attributed to the precipitous postpartum decline in progesterone. However, depression can be a symptom that develops during the progression of pregnancy. Moreover, a relationship between prepartum and postpartum depression was noted, suggesting that mood during pregnancy may be useful for predicting postpartum mood. The mechanisms of depression are under intense investigation, and it is becoming increasingly clear that imbalances in the synthesis, release, or degradation of several neurotransmitters in the brain, including serotonin, dopamine, norepinephrine, and glutamate, may contribute to depression. Depression can also be related to hormone levels, and indeed postpartum depression is linked to changes in progesterone and possibly estrogen. Moreover, depression in nonpregnant women tends to be mitigated by estrogen treatment. Nevertheless, this relationship between hormones and prepartum depression has not been investigated. Meningioma and Pregnancy Meningiomas are tumors that arise from the cells forming the arachnoid membrane around the central nervous system.
Purchase 5 mg prazosin otc
Paramount in the evaluation of ptosis is determining that the eyelid disorder is not a manifestation of a life-threatening neurological condition high cholesterol simple definition buy 2.5 mg prazosin otc. A third nerve palsy may present with variable combinations of ptosis, ocular motility disturbances, and anisocoria. Given that the levator palpebrae superioris is the primary eyelid retractor, ptosis from a third nerve palsy is often pronounced and levator function is markedly impaired. When seen in combination with ocular motility disturbances and pupillary abnormalities, this degree of ptosis usually warrants urgent neuroimaging. Myasthenia gravis may cause variable ptosis, often associated with ocular misalignment and other muscle weakness. Though isolated ocular myasthenia is common, many cases eventually generalize and can ultimately lead to systemic compromise, including respiratory failure. Testing the eyelids for fatigability or improvement of ptosis with rest or ice may help confirm the diagnosis, but single-fiber electromyelogram, acetylcholine receptor antibody assay, and edrophonium testing are usually considered more definitive. Myogenic causes of ptosis include oculopharyngeal muscular dystrophy, oculopharyngodistal myopathy, myotonic dystrophy, and chronic progressive external ophthalmoplegia. Patients with these disorders often have a family history of ptosis and symptoms are usually progressive and relatively symmetrical. Although both eyelids are often affected, there may be asymmetry, and levator function is usually well preserved. Levator function is preserved and treatment is directed at the cause of the mechanical ptosis. Acute intervention is usually needed for direct muscular injury as seen in penetrating trauma, but close observation is usually all that is necessary when the ptosis is caused by edema or contusion to the lid muscles. Congenital ptosis is a particularly challenging problem because a variety of anatomical variations may be encountered, and there is the potential for amblyopia if the ptosis is left untreated. Many syndromic disorders may have associated eyelid abnormalities, and thus a thorough systemic evaluation is required in any child presenting with ptosis. A careful evaluation of eyelid function, pupil size, and ocular motility should always be performed in any patient presenting with ptosis. After underlying neurological or myogenic conditions are addressed, attention may be turned to the eyelid itself if ptosis persists. With markedly diminished or absent levator function, as is seen in myogenic and neurogenic ptosis, a sling procedure may be used to suspend the upper lid from the frontalis muscle in the forehead. In such cases, the frontalis muscle may provide some degree of voluntary lid control. When levator function is preserved, the levator or its abnormal aponeurosis may be shortened or reinserted to its appropriate anatomical location on the tarsal plate. The pulvinar is an association nucleus located in the posterolateral portion of the thalamus. It has reciprocal projections with large areas of the cerebral cortex and is thought to play a role in the integration of visual, auditory, and general sensory information. In 1967, Richardson reported the results of stereotactic lesioning of the anteromedial pulvinar in six patients with cancer pain. Work performed in his laboratory on cats suggested that the primary sensory input to the pulvinar traveled through the dorsal and anterolateral portions of the spinal cord. It was proposed that pain impulses ascending in these columns entered the pulvinar by way of the mesencephalic reticular formation, and that pulvinotomy alleviated chronic pain by interrupting the paleospinal pathway without affecting acute pain sensations mediated by the neospinothalamic system. In general, the results for treating cancer pain were superior to those for neuropathic pain. However, there was a clear tendency for pain to return with time, particularly in patients with noncancer pain and a normal life expectancy. Postoperatively, 19 patients were immediately pain free and 12 had worthwhile pain improvement. There seem to be few side effects from lesioning the pulvinar, and major alterations in sensory or cognitive function are rare. Pulvinotomy has also been used to treat a small number of patients with tremor, dyskinesias, and hypertonia. Some results were favorable, but other lesion sites in the thalamus and basal ganglia proved to be more effective. A relatively large thermal lesion is made with an electrode and a radio frequency lesion generator. Electrical stimulation is used before a lesion is made to ascertain that the nearby somatosensory thalamic nuclei will not be damaged, but most authors have failed to note a specific response associated with stimulation of the pulvinar. Enthusiasm for stereotactic pulvinotomy has waned as better pain control measures have evolved and the poor longterm success rates of the procedure have become apparent. Pulvinotomy is unwarranted for other types of chronic pain or for movement disorders. The pupillary reaction to light can be used as an indicator of the status of the afferent visual system. If there is a disease affecting the retina or the optic nerve, there will be less stimulation of the visual pathways and the pupils will respond as if the light were dimmer. The diminished pupillary response under these conditions is called an afferent pupillary defect. However, a decrease in the response to direct stimulation is not diagnostic because an efferent defect will cause a similar decrease in pupillary response even with normal optic nerve and retina function. As the pupillary light reaction can be evoked with even small changes in light stimulation, mild and moderate bilateral afferent defects are clinically difficult to detect. Even severe losses are frequently missed because clinicians are more practiced in detecting the presence versus the absence of pupillary constriction rather than variations in the speed and amplitude of constriction. Thus, a poor but present reaction that is equal in both eyes is often not appreciated as being abnormal. The pupillary light reflex is typically absent only with virtually total loss of afferent input from the anterior visual pathways. This may come from marked obstruction within the eye keeping the light from reaching the retina or from severe retinal or optic nerve damage. Thus, the etiology of total bilateral afferent defects is typically not difficult to diagnose. One must keep in mind that damage to the optic chiasm can also cause bilateral blindness and can be missed if appropriate studies are not ordered. Compared to bilateral afferent defects, unilateral or bilateral asymmetric afferent deficits are much easier to detect through use of the swinging flashlight test. The test should be performed in a dark room with the patient looking at a distant fixation target. It is critical that the timing of the stimulation is the same for both eyes and that the angular displacement of the stimulus from the line of sight is the same for each eye. It is also critical that light be moved rapidly and directly from one eye to the other. The longer it takes to move the stimulus from one eye to the other, the more the pupils will dilate during that movement and prevent a more accurate assessment of asymmetry. As the light alternates between the eyes, normal subjects may have no significant change in size because the light stimulus is the same for each eye. Close observation may reveal a small initial constriction often followed by a small redilation. This can be done using photographic neutral density filters or crossed polarized filters. Just as there are more afferent fibers from the contralateral eye in an optic tract, there are more fibers from the contralateral eye synapsing on each pretectal nucleus. The eye that is stimulated with more light will become relatively more light adapted and therefore less sensitive to the light, and the pupil will be less reactive. If one is not careful in performing the swinging flashlight test, it is easy to pay more attention to the pupil one initially considered to be abnormal and less attention to the presumed normal one. Insight into the anatomy of the pupillary light reflex has been obtained through the use of pupillometry. When a light is shone into one eye of a normal subject, both pupils respond by becoming smaller.
