
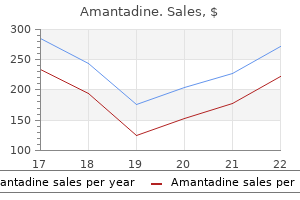
Cheap 100 mg amantadine
The key change is an increase in the serum of IgA1 O-glycoforms that contain less galactose hiv infection time period purchase amantadine pills in toronto. These high-molecular-weight immune complexes are prone to mesangial deposition, resulting ultimately in mesangial cell proliferation, release of proinflammatory mediators, and glomerular injury. There is increasing evidence, predominantly from in vitro models, that circulating IgA immune complexes containing poorly galactosylated polymeric IgA1 are key drivers for all of these processes. IgA1 contains a 17-amino-acid hinge region that undergoes co/posttranslational modification by the addition of 6 O-glycan chains. These mediators, along with the direct effects of exposure to IgA immune complexes, cause podocyte injury, a process fundamental to segmental glomerular scarring (S), and proximal tubule cell activation, which drives tubulointerstitial scarring (T). Approximately 25% to 30% of any cohort will require kidney replacement therapy within 20 to 25 years of presentation. Many studies have identified clinical, laboratory, and histopathologic features at presentation that mark a poor prognosis (Table 20. Although the various prognostic factors listed may be informative for populations of patients, they do not as yet possess the specificity to identify an individual prognosis with complete confidence. This could be mediated through production of autoantibodies with specificity for the poorly galactosylated IgA1 hinge region. There are a number of patients who will continue to experience proteinuria in excess of 0. In these patients, current evidence regarding additional therapy is controversial. Overall results are equivocal, and reports showing positive outcomes have been criticized for inadequate trial design and the presence of multiple confounding factors. There was no difference in kidney disease progression for patients who received immunosuppression in addition to optimized intensive supportive therapy, compared with patients receiving optimized intensive supportive therapy alone. Tonsillectomy reduces the frequency of acute episodes of visible hematuria when tonsillitis is the provoking factor, and tonsillectomy has its advocates, especially in Japan, as a treatment to reduce kidney disease progression. A kidney biopsy, including electron microscopy, is key to distinguishing between these two extremes. This may be the consequence of significant preexisting chronic damage at the time of a crescentic transformation, thereby reducing the chances of a response to immunosuppression. Most cases occur in the winter, spring, and autumn months, which may be because of its association with preceding upper respiratory tract infections. Both diseases share similar kidney biopsy findings, and they also share changes in the complement of serum IgA1 O-glycoforms. There is a similar association between mucosal infection and presentation of disease. Kidney involvement typically manifests as transient asymptomatic microscopic hematuria and/or proteinuria. More severe complications, such as nephrotic syndrome or rapidly progressive deterioration of kidney function, occur less frequently and are more common in adults than in children. Confirmation of the clinical diagnosis requires histologic evidence of IgA deposition in affected tissue, often the skin or kidney. IgA immune complex deposition can be seen using immunofluorescence staining, but detection of IgA in the skin is unreliable. If a tissue diagnosis is required, a kidney biopsy should be performed in the presence of nephritis. Regimens include pulsed methylprednisolone followed by a 3-month course of oral prednisolone. There is currently no conclusive evidence that other immunosuppressive agents, including cyclophosphamide or azathioprine, or other interventions, such as plasmapheresis, have any beneficial effect on outcome. Kidney transplant traditionally is delayed for 12 months from date of presentation. An "evidence-based" survey of therapeutic options for IgA nephropathy: assessment and criticism. These women are at increased risk of developing hypertension and proteinuria during pregnancy. The Oxford classification of IgA nephropathy: rationale, clinicopathological correlations, and classification. Thurman the complement system is a group of proteins that provide an important part of the immune defense against infection. Many components of the complement system circulate as inactive proteins in the plasma. Activation of the complement system generates peptide fragments that serve as ligands for several receptors and completes a multimeric complex (C5b-9) that forms pores in membranes resulting in cell lysis. As with all components of the immune system, proper function of the complement system helps with the effective elimination of invasive pathogens while causing minimal inflammation or injury to host tissues. However, uncontrolled activation of the complement system can cause tissue injury, and there is clear evidence that the complement cascade is activated in many autoimmune and inflammatory diseases. The kidney is particularly susceptible to complement-mediated injury, and the complement system has been implicated in the pathogenesis of multiple kidney diseases. It is also evident that acquired and congenital defects in the complement system are important risk factors for several diseases. These diseases are clinically and histologically distinct yet share similar risk factors. Our understanding of the pathogenesis of these diseases has been significantly advanced by recent discoveries. All three pathways result in the cleavage of C3, forming C3b that can be covalently fixed to tissue surfaces. Leukocytes also express receptors for C3b and the C3b inactivation fragments (iC3b and C3d). Several features of the alternative pathway are notable and may explain the link between activation of this pathway and kidney disease. Tissue-bound C3b can combine with a protein called factor B to form an alternative pathway activating enzyme (C3bBb). This spontaneous "tickover" process continuously generates C3b that can also bind to surfaces and be amplified through the alternative pathway. Complement activation is controlled by a group of regulatory proteins expressed on the surface of cells or that circulate in plasma. These regulatory proteins provide a shield that protects the host from complement-mediated injury. Full activation of the complement cascade generates several proinflammatory fragments: C3a, C3b, C5a, C5b-9 (shown in red font). Of these regulators, defects in factor I, factor H, and membrane cofactor protein are associated with kidney disease. The cleavage of C3 by any of the activation pathways causes deposition of C3b on tissue surfaces. C3b is part of the alternative pathway C3-convertase, and this enzyme generates additional C3b unless the convertase decays or C3b is inactivated by the plasma protease factor I, generating iC3b. Factor H is a cofactor for inactivation of C3b in the fluid phase and on cell surfaces. Specific activating proteins can trigger complement activation on a particular cell or surface, but the degree of activation is also determined by the local expression of complement regulatory proteins. Impaired regulation may lower the threshold for activation within a particular tissue, and local impairments of regulation may even be sufficient to permit spontaneous activation. Endothelial cells and podocytes each express several of the complement regulatory proteins, and ordinarily there is little evident complement activation within the glomerular capillary wall. Other proteins regulate complement activation by reducing the half-life of the activating enzymes through a process termed decay acceleration. Several additional proteins also control the complement system through other mechanisms. Gain-of-function mutations have also been identified in the genes for C3 and factor B.
Buy amantadine 100 mg on-line
Glomeruli can appear shrunken and ischemic anti viral bronchitis discount amantadine 100 mg on line, with wrinkling of the basement membrane corresponding to the injured glomerular capillaries. Obstruction of the microcirculation due to thrombi can lead to acute cortical ischemia with cortical necrosis, which is irreversible, and whose entity correlates with the degree of chronic kidney damage. Immunofluorescence is negative for immunoglobulin and complement factors and positive for fibrinogen within blood vessels. Endothelium of arterioles and small arteries can be positive for complement activation products. The brain is the next most frequently involved organ (70%), followed by the heart, intestine, lungs, and pancreas in about 20% of patients. Diplopia or cortical blindness, hemiparesis, and hemiplegia have also been reported. Heart failure due to cardiac involvement and fluid overload can be present and severe, leading to sudden death. Stool must be checked for intestinal bleeding, and an abdominal ultrasound looking at the integrity of intestinal walls should be performed. Some patients (about 5%) present with fulminant multivisceral involvement, with kidney failure, seizures, intestinal bleeding, heart failure, pulmonary hemorrhage, hepatic cytolysis, and pancreatitis. This is particularly true in patients with reduced circulating C3 levels or a family history of kidney failure, sudden unexplained death, coagulopathies, hypertension, or glomerulopathies. The age of onset, circulating C3 levels, and clinical features can be useful indicators of which complement gene or abnormality to screen first. Concomitant coagulopathy or pulmonary hypertension suggests thrombomodulin mutations. Children older than 7 years with a low C3 level suggests anti-factor H antibodies. Every effort should be made to manage them in a setting with expertise in emergent dialysis. Infusion of platelets is contraindicated, unless there is a hemorrhagic event or a high-risk procedure is necessary. Before 2010, the use of intensive and early plasma exchange was advocated to replenish missing or malfunctioning factors and to curb the complement alternative pathway dysregulation. This approach was accompanied by significant side effects, especially in children, and it was only partially effective. The use of the monoclonal anti-C5 antibody eculizumab, which inhibits the terminal complement pathway, has dramatically changed the natural history of this disease from a dismal prognosis to a severe but manageable condition. When these criteria are established, a complete workup of complement proteins, alternative pathway genes, and anticomplement factor H autoantibodies must be performed. Because eculizumab blocks the terminal complement pathway, the drug makes patients more susceptible to infections by encapsulated bacteria-mainly Neisseria meningitidis. Therefore, when possible, all patients should receive antimenigococcal vaccination (both serotype A, C, Y, W and serotype B) 15 days before first infusion. In critically ill patients, treatment should start under antibiotic prophylaxis (with methylpenicillin or a macrolide), and vaccination should be performed when possible. Moreover, in immunocompromised patients, children, and individuals at increased risk. Therapy with eculizumab is not disease modifying, and treatment discontinuation entails a nonquantifiable risk of disease relapse. Of note, when anti-factor H autoantibodies are present, therapy with plasma exchange combined with immunosuppression (steroids plus azathioprine, mycophenolate mofetil, cyclophosphamide, or rituximab) is effective, though not standardized. The response to therapy can be monitored by measuring anti-factor H antibodies, which correlate closely with the risk of disease relapse. If plasma exchange therapy is not available, plasma infusion can be considered if the patient does not present with fluid overload, heart failure, or severe hypertension. This is currently the only disease-modifying definitive cure, but plasma exchange or eculizumab should be used at the time of transplantation to protect the transplanted liver from complement-mediated injury until it can replenish these proteins. Complement defects in patients with C3G, on the other hand, tend to affect complement regulation in the fluid phase. These differences are not absolute, however, and some of the mutations found in patients with C3G. It is not yet known why patients with similar defects in alternative pathway regulation manifest at different ages and with distinct clinical syndromes. It is possible that variations in other genes modify the exact location and nature of these diseases or that disease triggers or associated illnesses influence how the diseases manifest. Future work will hopefully answer these questions and improve our understanding of how best to predict, diagnose, and treat these kidney diseases. Genetics and outcome of atypical hemolytic uremic syndrome: a nationwide French series comparing children and adults. Complement genes strongly predict recurrence and graft outcome in adult renal transplant recipients with atypical hemolytic and uremic syndrome. Human C3 mutation reveals a mechanism of dense deposit disease pathogenesis and provides insights into complement activation and regulation. Acquired and genetic complement abnormalities play a critical role in dense deposit disease and other C3 glomerulopathies. Combined complement gene mutations in atypical hemolytic uremic syndrome influence clinical phenotype. Complement factor H-related hybrid protein deregulates complement in dense deposit disease. Heterozygous and homozygous factor h deficiencies associated with hemolytic uremic syndrome or membranoproliferative glomerulonephritis: report and genetic analysis of 16 cases. Clinical features of anti-factor H autoantibody-associated hemolytic uremic syndrome. Pregnancy-associated hemolytic uremic syndrome revisited in the era of complement gene mutations. Identification of a mutation in complement factor H-related protein 5 in patients of Cypriot origin with glomerulonephritis. Familial C3 glomerulonephritis associated with mutations in the gene for complement factor B. Revisiting post-infectious glomerulonephritis in the emerging era of C3 glomerulopathy. An international consensus approach to the management of atypical hemolytic uremic syndrome in children. Clinical features and outcomes of 98 children and adults with dense deposit disease. Recurrent dense deposit disease after renal transplantation: an emerging role for complementary therapies. Activation of the alternative pathway of complement by monoclonal lambda light chains in membranoproliferative glomerulonephritis. Dense deposit disease: clinicopathologic study of 32 pediatric and adult patients. Primary glomerulonephritis with isolated C3 deposits: a new entity which shares common genetic risk factors with haemolytic uraemic syndrome. Heterogeneous pattern of renal disease associated with homozygous factor H deficiency. Epidemiology, clinical presentation, and pathophysiology of atypical and recurrent hemolytic uremic syndrome. In cases of ongoing active infection, other clinical manifestations related to the specific infectious disease are common. Sites of infection can include the upper and lower respiratory tract, skin/soft tissue, bone, teeth/oral mucosa, heart, deep abscesses, shunts, and indwelling catheters. Adults more commonly present with kidney failure and with complications of hypervolemia, including decompensated heart failure. In these cases, coexistence of the glomerular disease and the infection is common, and classic clinical findings such as low complement levels may be absent. Diabetes is the most commonly recognized comorbidity and is associated with poor outcomes. The presentation and outcomes in children are often different from those in adults (Table 22. The urinary sediment is usually active, with dysmorphic red cells, red blood cell casts, and leukocyturia. Hypocomplementemia is very common, with decreased C3 in up to 90% of cases and to a lesser extent depleted levels of C4. There is usually a "latent" period between the resolution of the streptococcal infection and the acute onset of the nephritic syndrome.
Purchase generic amantadine from india
For a 3-hour glucose tolerance test antiviral medication for cats discount amantadine 100mg on-line, the patient must ingest a minimum of 150 g/day of glucose for the 3 days preceding the test. If two or more values are abnormal, the diagnosis of gestational diabetes may be made. Studies indicate that screening may be omitted for selected individuals who are very low risk by selection criteria (see Box 224. This anti-insulin effect is sufficient to tip borderline patients into a diabetic state or prompt readjustments in the insulin dosage used by patients with insulin-dependent diabetes. Screening for gestational diabetes mellitus by a model based on risk indicators: a prospective study. A comparison of glyburide and insulin in women with gestational diabetes mellitus. Different strategies for diagnosing gestational diabetes to improve maternal and infant health. Gestational Diabetes Screening: the International Association of the Diabetes and Pregnancy Study Groups Compared With Carpenter-Coustan Screening. Jelly beans as an alternative to a fifty-gram glucose beverage for gestational diabetes screening. Physical activity interventions in pregnancy and risk of gestational diabetes mellitus: a systematic review and meta-analysis. Fetal-dental caries, cardiac defects, and ophthalmic problems (vision correction often necessary). Description: Fetal alcohol syndrome is characterized by malformations found in infants born to mothers who have consumed alcohol during pregnancy. Abnormalities include structural malformations (predominantly facial), growth restriction, and neurologic abnormalities including mental retardation. Prevalence: Estimates vary from 6 of 10,000 births to 2 of 1000 births and globally as high as 23 of 1000 births. Intrauterine exposure to alcohol is a leading cause of preventable birth defects and developmental disabilities. Some cardiac anomalies may be detected while in utero; absence does not exclude effects. There does not appear to be a lower limit of safety nor are the effects confined to one part of pregnancy. The severity of the effects appears to be proportional to the amount and duration of exposure. Clinically identifiable effects are generally not seen with sporadic exposures of less than 1 oz of alcohol per day, although absolute safety cannot be assured even at this dose. Pathologic Findings Reduced brain volume affecting the frontal lobe, striatum and caudate nucleus, thalamus, and cerebellum; thinning of the corpus callosum; and abnormal functioning of the amygdala. For the fetus-evaluation, special education and support, surveillance for dental caries (more common in these children), and cardiac and ophthalmic problems. No safe level of exposure has been demonstrated, although sporadic use of less than 1 oz of alcohol per day has not been associated with the syndrome. Alcohol use among pregnant and nonpregnant women of childbearing age - United States, 1991-2005. Possible Complications: Higher rate of spontaneous miscarriage in heavy users of alcohol. Expected Outcome: Infants affected by fetal alcohol syndrome vary from mildly to profoundly mentally retarded. Systematic review of effects of lowmoderate prenatal alcohol exposure on pregnancy outcome. Alcohol abuse and other substance use disorders: ethical issues in obstetric and gynecologic practice. They are abnormalities of pregnancy that arise entirely from abnormal placental proliferation. They are classified as being either complete, in which no fetus is present, or incomplete (partial), in which both fetus (generally abnormal) and molar tissues are present. Clotting function studies and blood cross-matching are advisable before the evacuation of a large uterus. Chorionic gonadotropin levels often exceed 100,000 ImU/mL for invasive mole or choriocarcinoma. Edematous trophoblastic fragments may be vaginally passed through a partially dilated cervical os, alerting the clinician to the diagnosis. Specific Measures: the treatment of molar pregnancies is surgical: evacuation of the uterine contents. Because of the large size of some molar pregnancies and a tendency toward uterine atony, concomitant oxytocin administration is advisable and blood for transfusion must be immediately available, should it be needed. Oxytocin or methylergonovine maleate (Methergine) is used to help contract the uterus during surgical evacuation. Primary or recurrent malignant trophoblastic disease is generally treated with chemotherapy (methotrexate, actinomycin D, chlorambucil, or cyclophosphamide [Cytoxan], singly or in combination). Possible Complications: Gestational trophoblastic neoplasia is notable for the possibility of malignant transformation, although fewer than 10% of patients develop malignant changes. In general, the larger or more advanced the molar pregnancy, the greater the risk of pulmonary complications, bleeding, trophoblastic emboli, or fluid overload during evacuation. Expected Outcome: Approximately 80% of molar pregnancies follow a benign course after an initial therapy. The theca lutein cysts often found in molar pregnancies may take several months to regress after evacuation of the uterine contents. Fewer than 5% of patients will require hysterectomy to achieve a cure for choriocarcinoma. Methotrexate with citrovorum factor rescue for nonmetastatic gestational trophoblastic neoplasms. These patients have no higher rate of abortions, stillbirths, congenital anomalies, prematurity, or other complications of pregnancy with future gestations. The placenta from any subsequent pregnancies should be sent for histologic evaluation. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Despite concerns directed elsewhere during pregnancy, the practitioner must watch for this common problem and address it when present. Prevention/Avoidance: Good dental hygiene (daily brushing and flossing), periodic evaluation and cleaning. Expected Outcome: Generally improves after delivery if hormonal change is the cause; can recur if dental hygiene is not maintained. Oral health in women during preconception and pregnancy: implications for birth outcomes and infant oral health. Evaluation of the incidence of preterm low birth weight in patients undergoing periodontal therapy. Periodontal therapy reduces the rate of preterm low birth weight in women with pregnancy-associated gingivitis. The relationship between periodontal disease, bacterial vaginosis, and preterm birth. Infection, abscess, or sources of sepsis require prompt treatment, regardless of the stage of pregnancy. Should we treat periodontal disease during gestation to improve pregnancy outcomes Precautions: Watch for possible overgrowth of vaginal fungal flora if penicillin is used.
Discount 100mg amantadine with amex
Potassium-sparing diuretics hiv infection rates heterosexual vs homosexual buy amantadine 100mg fast delivery, such as triamterene and amiloride, and mineralocorticoid-receptor antagonists, such as spironolactone and eplerenone, reduce urinary K+ and Mg++ excretion when it might otherwise increase with either thiazide or loop diuretic therapy. In certain instances, significant K+ retention occurs with K+-sparing diuretics that hyperkalemia ensues. The administration of trimethoprim-sulfamethoxazole (Bactrim) or heparin therapy, inclusive of subcutaneous heparin regimens, can also reduce urinary K+ excretion and therein lead to the development of hyperkalemia. Electrolyte changes are the most common side effects with diuretics and ostensibly most noticeable with the more potent loop diuretics, but the strength of a diuretic is likely not as critical as might be its duration of action. For example, thiazide-type diuretics, such as chlorthalidone and metolazone, while less potent than a loop diuretic, can still cause significant hypokalemia and hypomagnesemia owing to their long-lived duration of action. Not all thiazide diuretics are the same in their likelihood to lead to hyponatremia. Acetazolamide use under these circumstances is often empiric with limited information as to dose-response relationships. Metabolic alkalosis can also lessen the natriuretic response to a loop diuretic, a factor of some particular relevance to the diuretic-resistant patient. It may take several days for acid-base balance to be restored after discontinuation of a K+-sparing diuretic. All diuretics, including loop diuretics, cause these lipid changes, with the possible exception of indapamide. Several long-term studies with thiazide diuretics have shown cholesterol levels return to their respective baseline at 1 year. All K+-sparing diuretics also diminish the heightened Mg++ excretion that arises from thiazide or loop diuretic use. Cellular Mg++ depletion occurs in 20% to 50% of patients in the course of thiazide therapy, particularly with long-acting thiazide-type diuretics such as chlorthalidone, and can be present notwithstanding an otherwise normal serum Mg++. Hypomagnesemia-related symptoms include depression and muscle weakness, as well as nystagmus, tetany, and positive Chvostek and Trousseau signs. Refractory hypokalemia, as well as hypocalcemia, and an array of atrial/ventricular arrhythmias can occur, with torsades de pointes being a particularly troubling finding. Many of these abnormalities and, in particular, refractory hypokalemia and hypocalcemia correct quickly with small amounts of Mg++ replacement. Loop diuretics are direct inhibitors of the Na+/K+/2Cl- cotransport system, which also exists in the marginal and dark cells of the stria vascularis and are responsible for endolymph secretion. The ototoxicity of these agents may be due to variations in the ionic composition and endolymph volume. Loop diuretic-induced ototoxicity usually occurs within 20 minutes of infusion and is typically reversible, although permanent deafness has been reported, particularly with ethacrynic acid. Ototoxicity is clearly related to both the rate of infusion and the peak serum concentrations of a diuretic and appears to be a more likely occurrence with furosemide than bumetanide. In general, ototoxicity can be minimized by slow continuous infusion (<4 mg/min) rather than bolus injection and use of divided oral dose regimens. Patients with kidney failure and those receiving concomitant aminoglycoside therapy are at greatest risk of developing ototoxicity with furosemide. It is unclear as to the level of association of these items to hyperuricemia stemming from diuretic therapy. This phenomenon may be abrupt in its development or more insidious, occurring months after therapy is begun with a thiazide diuretic or, less commonly, with furosemide. Hyperglycemia/glucose intolerance has been linked to diuretic-induced hypokalemia, which inhibits insulin secretion by cells. Diuretic-associated glucose intolerance appears to be dose dependent, less frequent with loop diuretics, and in many cases reversible upon withdrawal of the agent. Co-administration of thiazides increases the efficacy of loop diuretics even in patients with advanced renal failure. Decongestive treatment of acute decompensated heart failure: cardiorenal implications of ultrafiltration and diuretics. Renal effects of conivaptan, furosemide, and the combination in patients with chronic heart failure. Co-administration of albumin and furosemide in patients with the nephrotic syndrome. Thiazide and thiazide-like diuretics: an opportunity to reduce blood pressure in patients with advanced kidney disease. Diuretic combinations in refractory oedema states: pharmacokinetic-pharmacodynamic relationships. Intravenous high-dose furosemide and hypertonic saline solutions for refractory heart failure and ascites. Thiazide diuretics, potassium, and the development of diabetes: a quantitative review. The chemical structure of ethacrynic acid differs from that of the other loop diuretics and makes it a nontoxic replacement in patients having experienced diuretic-related allergic complications. By causing hypokalemia and/or hypomagnesemia, diuretics in general increase digitalis toxicity. Plasma lithium (Li+) concentrations can increase with diuretic therapy if significant volume contraction occurs; however, this is a variable and somewhat unpredictable phenomenon. Li+ levels should be carefully monitored in those patients receiving Li+ in conjunction with diuretics. Triamterene can also induce crystal formations that are brown, spherical, and assume a Maltese cross appearance under polarized light with crystal formation prevented with alkalization of urine to a pH of 7. Effects of albumin/furosemide mixtures on responses to furosemide in hypoalbuminemic patients. Approximately 98% of this total is intracellular, primarily in skeletal muscle, and to a lesser extent in the liver. The second regulates potassium shifts between the extracellular and intracellular fluid compartments. To stay in potassium balance, it is necessary to increase potassium excretion when dietary potassium increases and decrease potassium excretion when dietary potassium decreases. Normally the kidneys excrete 90% to 95% of dietary potassium, with the remaining 5% to 10% excreted by the gut. Potassium excretion by the kidney is a relatively slow process, taking 6 to 12 hours to eliminate an acute load. Plasma potassium is freely filtered across the glomerular capillary into the proximal tubule. It is subsequently completely reabsorbed by the proximal tubule and loop of Henle. In the distal tubule and the collecting duct, potassium is secreted into the tubular lumen. For practical purposes, urinary excretion of potassium reflects potassium secretion into the lumen of the distal tubule and collecting duct. Thus any factor that stimulates potassium secretion increases urinary potassium excretion; conversely, any factor that inhibits potassium secretion decreases urinary potassium excretion. Conversely, medical conditions associated with increased aldosterone levels (primary hyperaldosteronism, secondary hyperaldosteronism due to diuretics or vomiting) increase potassium loss in the urine. Although there is profound secondary hyperaldosteronism in congestive heart failure and cirrhosis, each of these conditions may be associated with hyperkalemia because of decreased delivery of sodium to the distal nephron. Many diuretics increase renal potassium excretion by a number of mechanisms, including high distal sodium delivery, high urine flow rate, metabolic alkalosis, and hyperaldosteronism due to volume depletion. Poorly controlled diabetes commonly increases urinary potassium excretion due to osmotic diuresis with high urinary flow rate and high distal delivery of sodium. Reabsorption of sodium in the collecting duct occurs through selective sodium channels. This creates an electronegative charge within the tubular lumen relative to the tubular epithelial cell. Therefore drugs that block the sodium channel in the collecting duct decrease potassium secretion. Conversely, in Liddle syndrome, a rare genetic disorder in which the sodium channel is constitutively open, avid sodium reabsorption results in excessive potassium secretion.
Buy amantadine 100 mg low price
As individual nephrons may have different thresholds for glucose reabsorption depending on morphologic features antiviral influenza order genuine amantadine, the Tm reflects the average. These include molecules that are too large for filtration and those that are protein bound. This process is facilitated by an array of organic ion KidneyDevelopment Norman D. Establishment of the metanephric kidney is preceded by formation of two other mesenchyme-derived kidney-like structures-the pronephros and the mesonephros. Both are transient kidney-like paired structures that do not contribute to the permanent kidney. The pronephros is the more anterior of these structures and degenerates in mammals. The more posterior structure, the mesonephros, gives rise to male reproductive organs including the rete testis, efferent ducts, epididymis, vas deferens, seminal vesicle, and prostate. Metanephric mesenchyme is the tissue source of all epithelial cell types comprising the mature nephron. Reciprocal inductive interactions between the metanephric mesenchyme and the ureteric bud result in (1) nephrogenesis, defined as formation of the glomerulus and all tubules proximal to the collecting ducts, and (2) branching morphogenesis, defined as growth and branching of the ureteric bud and subsequent formation of the renal collecting system, which is constituted by the cortical and medullary collecting ducts, the renal calyces, and the renal pelvis. Failure to induce ureteric bud outgrowth results in renal agenesis, while outgrowth of more than one ureteric bud can result in kidney malformations including a double collecting system and duplication of the ureter. The position at which the ureteric bud arises from the wolffian duct relative to the metanephric mesenchyme is critical to the nature of the interactions between the ureteric bud and the metanephric mesenchyme. Ectopic positioning of the ureteric bud is associated with renal tissue malformation (dysplasia), which may result from abnormal ureteric bud-metanephric mesenchyme interactions. Ectopic positioning of the ureteric bud is also thought to contribute to the integrity of the ureterovesical junction. Branching of the ureteric bud occurs immediately following invasion of the metanephric mesenchyme by the ureteric bud. The number of ureteric bud branches is a major determinant of final nephron number, since ureteric bud branch tips induce discrete subsets of metanephric mesenchyme cells to undergo nephrogenesis. Concomitant with formation of these branches, new nephrons are induced by reciprocal inductive interactions between newly formed ureteric branch tips and surrounding metanephric mesenchyme. Thereafter, collecting duct development occurs by extension of peripheral branch segments, and new nephrons form predominantly around the tips of terminal collecting duct branches. Between the 22nd and 34th week of gestation, the peripheral (cortical) and central (medullary) domains of the developing kidney are established. The renal cortex, which represents 70% of total kidney volume at birth, becomes organized as a relatively compact, circumferential rim of tissue surrounding the periphery of the kidney. The renal medulla, which represents 30% of total kidney volume at birth, has a modified cone shape with a broad base contiguous with cortical tissue. The apex of the cone is formed by convergence of collecting ducts in the inner medulla and is termed the papilla. Distinct morphologic differences emerge between collecting ducts located in the medulla and those located in the renal cortex. Medullary collecting ducts are organized into elongated, relatively unbranched linear arrays, which converge centrally in a region devoid of glomeruli. In contrast, collecting ducts located in the renal cortex continue to induce metanephric mesenchyme. The most central segments of the collecting duct system, formed from the first five generations of ureteric bud branching, undergo remodeling by increased growth and dilatation of these tubules to form the pelvis and calyces. Cells adjacent to the invading ureteric bud are induced to undergo a mesenchymal to epithelial transformation. An internal cavity forms within the pretubular aggregate, at which point the structure is called a renal vesicle. Multipotential precursors residing in renal vesicles give rise to all the epithelial cell types of the nephron. Nephron segmentation into glomerular and tubular domains is initiated by the sequential formation of two clefts in the renal vesicle. Creation of a lower cleft, termed the vascular cleft, precedes formation of the comma-shaped body. The middle limb gives rise to the proximal convoluted tubule and the upper limb to the descending and ascending limbs of the loops of Henle and the distal convoluted tubule. Epithelial cells lining the inner wall of this cup will comprise the visceral glomerular epithelium, or podocyte layer. The glomerular capillary tuft is formed via recruitment and proliferation of endothelial and mesangial cell precursors. Subsequent development of the glomerular capillary tuft involves extensive branching of capillaries and formation of endothelial fenestrae. Mesangial cells, in turn, populate the core of the tuft and provide structural support to capillary loops through the deposition of extracellular matrix. The full complement of glomeruli in the fetal human kidney is attained by 32 to 34 weeks when nephrogenesis ceases. Subsequent glomerular development involves hypertrophy, and glomeruli reach adult size by 3 1 2 years of age. These malformations are the most frequently detected abnormalities during intrauterine life (0. Over 200 distinct syndromes feature some type of kidney and urinary tract malformation (Table 2. Renal dysplasia is a polymorphic disorder characterized at the microscopic level by abnormal differentiation of mesenchymal and epithelial elements, decreased nephron number, loss of the demarcating zone between the cortex and the medulla, and metaplastic transformation of mesenchyme to cartilage and bone. Dysplastic kidneys range in size from large distended kidneys with multiple large cysts to small kidneys, with or without cysts. A small dysplastic kidney without macroscopic cysts, imaged by ultrasound, is classified as hypoplastic/dysplastic in the absence of a pathologic examination, which distinguishes between simple hypoplasia and dysplasia. In probands with bilateral renal agenesis or bilateral renal dysgenesis and without evidence of a genetic syndrome or a family history, 9% of first-degree relatives have some type of malformation in the kidney and/or lower urinary tract apparent on ultrasound. Fetal urine production begins at 9 weeks of gestation and makes a significant contribution to amniotic fluid volume by the onset of the second trimester. Thus, a decrease in amniotic fluid volume, termed oligohydramnios, at or beyond the 20th week of gestation is a surrogate marker of fetal kidney dysfunction. When two kidneys exist, oligohydramnios is observed in bilateral renal agenesis or severe dysgenesis, bilateral ureteric obstruction, or obstruction of the bladder outlet or urethra. When a solitary kidney exists, oligohydramnios is caused by renal dysgenesis or obstruction of urinary outflow. Poor postnatal outcome is highly suggested by the presence of severe oligohydramnios and small, hyperechogenic kidneys. Other genetic causes include autosomaldominant and autosomal-recessive forms of polycystic kidney disease. Newborns with an antenatal history of hyperechoic kidneys should be studied with a renal ultrasound to further define the phenotype. In the absence of such findings, a careful physical examination and pelvic ultrasound should be performed to rule out genital abnormalities. A diagnosis of unilateral renal agenesis is supported by compensatory hypertrophy in the normally positioned kidney. Thus imaging of the existing kidney and lower urinary tract is important and should consist of a kidney ultrasound. Management of affected patients involves determining the functional status of the existing kidney; if serum creatinine is normal, the long-term prognosis is excellent. However, some studies suggest that some patients ultimately will develop proteinuria and hypertension; accordingly, it is reasonable to propose that individuals with a single functioning kidney should have blood pressure measured, urine tested for protein, periodically continuing into adulthood, and monitoring of comorbidities including body weight. However, a large dysplastic kidney may exist in at least two clinical circumstances. Second, larger dysplastic kidneys are a feature of somatic overgrowth syndromes including Beckwith-Wiedemann syndrome and Simpson-Golabi-Behmel syndrome. During the antenatal period, a unilateral dysplastic kidney is likely to be discovered as an incidental finding. This may also be the case for bilateral renal dysplasia unless it is associated with oligohydramnios. After birth, bilateral renal dysplasia is associated with a variable degree of decreased kidney function proportional to the severity of the dysplasia.
Deer Balls (Puff Ball). Amantadine.
- Dosing considerations for Puff Ball.
- What is Puff Ball?
- Are there safety concerns?
- Nosebleeds and skin disorders.
- How does Puff Ball work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96087
Order 100 mg amantadine overnight delivery
Newer mechanical ventilators have a setting that will automatically adjust gas flows to make this adjustment hiv infection risk percentage discount amantadine on line. If pressure support is concomitantly used, it should generally be reduced to 5 to 8 cm H2O. Blood gas measurements can be checked after a minimum of 15 to 30 min at each setting. The goal is to try to ensure a Vt of 4 to 6 mL/kg and an f of less than 30 with acceptable Pao2 and Paco2. The -piece attaches directly to the tracheal tube or tracheostomy tube and has corrugated tubing on the other two limbs. Sufficient gas flow must be given in the proximal limb to prevent the mist from being completely drawn back at the distal limb during inspiration; this ensures that the patient is receiving the desired oxygen concentration. The patient is observed closely during this period; obvious new signs of fatigue, chest retractions, tachypnea, tachycardia, arrhythmias, or hypertension or hypotension should terminate the trial. If the patient can also protect and clear the airway, the tracheal tube can be removed. If the patient has been intubated for a prolonged period or has severe underlying lung disease, sequential -piece trials may be necessary. Periodic trials of 10 to 30 min are initiated and progressively increased, typically by 5 to 10 min per trial as long as the patient appears comfortable, maintains acceptable arterial saturation, and does not become hypercarbic. Improvement in the latter parameter will show as a decrease in venous admixture and an improvement in arterial O2 tension. Constant levels of pressure can be attained only if a high-flow (inspiratory) gas source is provided. When the patient does not have an artificial airway, tightly fitting fullface masks, nasal masks, or nasal "pillows" can be used. Expiratory pressures greater than 15 cm H2O should only be administered by tracheal or tracheostomy tube. By compressing alveolar capillaries, overdistention of normal alveoli can also increase pulmonary vascular resistance and right ventricular afterload. Disruption of alveoli allows air to track interstitially along bronchi into the mediastinum (pneumomediastinum). E, result of excessive pressure when alveoli are overdistended and pulmonary compliance decreases. The need for excessive Fio2 is most easily avoided with an adequate cardiac output and hemoglobin concentration. The most commonly suggested endpoint is an arterial oxygen saturation of hemoglobin of greater than 88% to 90% on a nontoxic inspired oxygen concentration (50%). Many clinicians favor reducing the inspired oxygen concentration to 50% or less because of the potentially adverse effect of greater oxygen concentrations on the lung. Progressive reductions in cardiac output may be seen as mean airway pressure and mean intrathoracic pressure rise. The principal mechanism appears to be inhibition of return of venous blood to the heart from increased intrathoracic pressure. Other mechanisms may include reduced left ventricular filling from leftward displacement of the interventricular septum (when overdistention of alveoli and increased pulmonary vascular resistance lead to increased right ventricular volume). When this occurs, left ventricular compliance may be reduced, necessitating a higher filling pressure to achieve the same cardiac output. Circulatory depression is most often associated with end-expiratory pressures greater than 15 cm H2O. An aerosol mist is a gas or gas mixture containing a suspension of liquid particles. Aerosolized water may be administered to loosen inspissated secretions and facilitate their removal from the tracheobronchial tree. Aerosol mists are also used to administer bronchodilators, mucolytic agents, or vasoconstrictors (metered-dose inhalers are preferred for administration of bronchodilators). Aerosol mists with or without bronchodilators may induce cough as well as loosen secretions. Instillation of hypertonic saline has been used as a mucolytic and to induce cough. Additional effective measures include chest percussion or vibration therapy and postural drainage of the various lung lobes. Patients should be instructed to inhale maximally and to hold their breath for 2 to 3 s before exhalation. When thick, copious secretions are associated with atelectasis and hypoxemia, more aggressive measures may be indicated. Characteristics and outcomes of ventilated patients according to time to liberation from mechanical ventilation. Adoption of these guidelines, describing standards for basic monitoring during general anesthesia, was associated with a reduction in the number of patients suffering brain damage or death secondary to ventilation mishaps during general anesthesia. In manufacturing and in medicine, there is a natural tendency to assume that errors can be prevented by better education or better management of individual workers (ie, to look at errors as individual failures made by individual workers rather than as failures of a system or a process). To reduce errors, one changes the system or process to reduce unwanted variation so that random errors are less likely. Some of the first studies to evaluate safety of care focused on provision and sequelae of anesthesia. When spinal anesthesia was virtually abandoned in the United Kingdom (as a response to two patients developing subsequent paraplegia), Drs Robert Dripps and Leroy Vandam helped prevent spinal anesthesia from being abandoned in North America by carefully reporting outcomes of 10,098 patients who received this technique. They determined that only one patient (who proved to have a previously undiagnosed spinal meningioma) developed severe, long-term neurological sequelae. After halothane was introduced into clinical practice in 1954, concerns arose about whether it might be associated with an increased risk of hepatic injury. The National Halothane Study, a very early clinical outcomes study, was performed (long before the term outcomes research gained widespread use), demonstrating the remarkable safety of the then relatively new agent compared with the alternatives. It failed, however, to settle the question of whether "halothane hepatitis" actually existed. Adoption of standards for basic monitoring during general anesthesia (that included detection of carbon dioxide in exhaled gas) was associated with a reduction in the number of patients suffering brain damage or death secondary to ventilation mishaps. A fortunate associated result was that the cost of medical liability insurance coverage for American anesthesiologists also declined. It is not an objective that has been fulfilled or a reflection of a problem that has been solved. It must be sustained by research, training, and daily application in the workplace. That document highlighted many opportunities for improved quality and safety in the U. More recently, the Institute for Healthcare Improvement has been "motivating and building the will for change; identifying and testing new models of care in partnership with both patients and health care professionals; and ensuring the broadest possible adoption of best practices and effective innovations," as described on its web site. The quality and safety movement(s) in medicine have their origins in the work of Walter Shewhart and his associate W. Edwards Deming, who popularized the use of statistics and control charts in improving the reliability of a process. In medicine, reducing the error rate (for everything from accurate timing and delivery of prophylactic antibiotics to ensuring "correct side and site" surgery or regional anesthetic blocks) reduces preventable injuries to patients, eliminates the additional costs resulting from those errors, and improves quality. In other words, there is a tendency to look at errors as individual failures made by individual workers, rather than as failures of a system or a process. As was first stated by Arthur Jones and then popularized by Paul Batalden, "All organizations are perfectly designed to get the results they get! An outstanding example of this is aadoption of the "universal protocol" prior to invasive procedures. Adherence to this protocol ensures that the correct procedure is performed on the correct part of the correct patient by the correct physician, that the patient has given informed consent, that all needed equipment and images are available, and that (if needed) the correct prophylactic antibiotic was given at the correct time. A related example of a simple approach to improve safety and quality of a procedure is the use of a cognitive aid, such as a standardized checklist, as described in the popular press by Dr Atul Gawande. The importance of checklists is addressed elsewhere in this text, for example, in Chapter 2 in the context of developing a culture of safety in the operating room. By accurately describing the intended surgical procedure (at the time the patient is "posted" on the surgical schedule), the surgeon helps prevent the operating room nurses from making the critical error of not having the necessary instrumentation for the procedure, and helps ensure that the appropriate regional anesthetic will be performed. We have selected these examples of good communication because we are aware of adverse patient outcomes that have resulted from failure to transfer these specific points of information.
Syndromes
- Heart attack or stroke
- Confusion
- Neuroblastoma
- Male pattern baldness
- Activated charcoal
- Urine immunoelectrophoresis
- Liver, beef, and fish
- Enlargement of the heart
Generic amantadine 100 mg mastercard
However hiv infection treatment purchase amantadine pills in toronto, high-dose oral beta-lactam therapy provides the tissue antibiotic exposure thought to be required to eradicate the remaining pathogens at the infection site as the tissue perfusion improves. High-dose oral beta-lactam antibiotic therapy of osteoarticular infections has been associated with treatment success since 1978. One must also assume that the parent and child are compliant with the administration of each antibiotic dose, that the oral antibiotic will be absorbed from the gastrointestinal tract into the systemic circulation (no vomiting or diarrhea), and that the parents will seek medical care if the clinical course does not continue to improve for their child. From some of the first published cases of oral step-down therapy, failures caused by noncompliance have occurred. Antimicrobial Prophylaxis/Prevention of Symptomatic Infection this article provides a summary of recommendations for prophylaxis of infections, defined as providing therapy prior to the onset of clinical signs or symptoms of infection. Postexposure Antimicrobial Prophylaxis to Prevent Infection Given for a relatively short, specified period after exposure to specific pathogens/ organisms, where the risks of acquiring the infection are felt to justify antimicrobial treatment to eradicate the pathogen or prevent symptomatic infection in situations in which the child (healthy or with increased susceptibility to infection) is likely to have been inoculated/exposed (eg, asymptomatic child closely exposed to meningococcus; a neonate born to a mother with active genital herpes simplex virus). Given to a particular, defined population of children who are of relatively high risk of acquiring a severe infection from a single or multiple exposures (eg, a child postsplenectomy; a child with documented rheumatic heart disease to prevent subsequent streptococcal infection), with prophylaxis provided during the period of risk, potentially months or years. Prophylaxis of Symptomatic Disease in Children Who Have Asymptomatic Infection/ Latent Infection Antimicrobial Prophylaxis/Prevention of Symptomatic Infection B. Long-term Antimicrobial Prophylaxis to Prevent Symptomatic New Infection Where a child has a documented but asymptomatic infection and targeted antimicrobials are given to prevent the development of symptomatic disease (eg, latent tuberculosis infection or therapy of a stem cell transplant patient with documented cytomegalovirus viremia but no symptoms of infection or rejection; to prevent reactivation of herpes simplex virus). Treatment period is usually defined, particularly in situations in which the latent infection can be cured (tuberculosis), but other circumstances, such as reactivation of a latent virus, may require months or years of prophylaxis. Surgical/Procedure Prophylaxis 14 A child receives a surgical/invasive catheter procedure, planned or unplanned, in which the risk of infection postoperatively or post-procedure may justify prophylaxis to prevent an infection from occurring (eg, prophylaxis to prevent infection following spinal rod placement). Treatment is usually short-term, beginning just prior to the procedure and ending at the conclusion of the procedure, or within 24 to 48 hours. However, some "highest risk" conditions are currently recommended for prophylaxis: (1) prosthetic heart valve (or prosthetic material used to repair a valve); (2) previous endocarditis; (3) cyanotic congenital heart disease that is unrepaired (or palliatively repaired with shunts and conduits); (4) congenital heart disease that is repaired but with defects at the site of repair adjacent to prosthetic material; (5) completely repaired congenital heart disease using prosthetic material, for the first 6 months after repair; or (6) cardiac transplant patients with valvulopathy. Follow-up data in children suggest that following these new guidelines, no increase in endocarditis has been detected,10 but in adults in the United States11 and in the United Kingdom,12 some concern for increase in the number of cases of endocarditis has been documented since widespread prophylaxis was stopped. More recent data from California and New York do not support an increase in infective endocarditis with the current approach to prophylaxis. Antimicrobial Prophylaxis/Prevention of Symptomatic Infection None Doxycycline 4 mg/kg (up to 200 mg max), once. Amoxicillin prophylaxis is not well studied, and experts recommend a full 14-day course if amoxicillin is used. A single dose of ciprofloxacin should not present a significant risk of cartilage damage, but no prospective data exist in children for prophylaxis of meningococcal disease. Close contact can be considered as face-to-face exposure within 3 feet of a symptomatic person; direct contact with respiratory, nasal, or oral secretions; or sharing the same confined space in close proximity to an infected person for $1 h. Azithromycin and clarithromycin are better tolerated than erythromycin (see Chapter 5); azithromycin is preferred in exposed very young infants to reduce pyloric stenosis risk. Scenario 1: Previously uninfected child becomes exposed to a person with active disease. This regimen is to prevent infection in a compromised host after exposure, rather than to treat latent asymptomatic infection. Therapy (evidence grade) Comments 14 Antimicrobial Prophylaxis/Prevention of Symptomatic Infection 240 - Chapter 14. Some experts would evaluate at birth for exposure following presumed maternal primary infection and start preemptive therapy rather than wait 24 h. Reference 21 provides a management algorithm that determines the type of maternal infection and, thus, the appropriate evaluation and preemptive therapy of the neonate. Bites of squirrels, hamsters, guinea pigs, gerbils, chipmunks, rats, mice and other rodents, rabbits, hares, and pikas almost never require antirabies prophylaxis. For bites of bats, skunks, raccoons, foxes, most other carnivores, and woodchucks, immediate rabies immune globulin and immunization (regard as rabid unless geographic area is known to be free of rabies or until animal proven negative by laboratory tests). Not recommended for infants 0 to #3 mo unless situation judged critical because of limited data on use and variability of drug exposure in this age group. Therapy (evidence grade) Comments 14 Antimicrobial Prophylaxis/Prevention of Symptomatic Infection 242 - Chapter 14. Comments To prevent recurrent infections, also consider the risks and benefits of placing tympanostomy tubes to improve middle ear ventilation as an alternative to antibiotic prophylaxis. However, antimicrobial prophylaxis may alter the nasopharyngeal flora and foster colonization with resistant organisms, compromising long-term efficacy of the prophylactic drug. Although prophylactic administration of an antimicrobial agent limited to a period when a person is at high risk of otitis media has been suggested (eg, during acute viral respiratory tract infection), this method has not been evaluated critically. Alternatives to penicillin include sulfisoxazole or macrolides, including erythromycin, azithromycin, and clarithromycin. Antimicrobial Prophylaxis/Prevention of Symptomatic Infection Acute rheumatic fever For. Check for acyclovir resistance for those who relapse while on appropriate therapy. The virulence/pathogenicity of bacteria inoculated and the presence of foreign debris/devitalized tissue/surgical material in the wound are also considered risk factors for infection. For complicated appendicitis, antibiotics provided to treat ongoing infection, rather than prophylaxis. Cefazolin 30 mg/kg 14 Antimicrobial Prophylaxis/Prevention of Symptomatic Infection 248 - Chapter 14. This section focuses on reactions that may require close observation or laboratory monitoring because of their frequency or severity. This allows one to assign drug-attributable side effects for specific drugs, such as oseltamivir, used for influenza, when influenza and the antiviral may both cause nausea. Monitor all patients receiving aminoglycoside therapy for more than a few days for renal function with periodic determinations of blood urea nitrogen and creatinine to assess potential problems of drug accumulation with deteriorating renal function. Monitoring is especially important in patients with any degree of renal insufficiency. Renal toxicity may be related to the total exposure of the kidney to the aminoglycoside over time. With oncedaily administration regimens, peak values are 2 to 3 times greater, and trough values are usually very low. Nephrotoxicity is less common in adults with once-daily (as opposed to 3 times daily) dosing regimens, but data are generally lacking in children. Aminoglycosides potentiate botulinum toxin neuromuscular junction dysfunction and are to be avoided in young infants with infant botulism. The most feared reaction to penicillins, anaphylactic shock, is extremely rare, and no absolutely reliable means of predicting its occurrence exists. However, in certain situations, the benefits of penicillin or a beta-lactam may outweigh the risk of anaphylaxis, requiring that skin testing and desensitization be performed in a Adverse Reactions to Antimicrobial Agents 15 252 - Chapter 15. The commercially available skin testing material, benzylpenicilloyl polylysine (Pre-Pen, AllerQuest), contains the major determinants thought to be primarily responsible for urticarial reactions but does not contain the minor determinants that are more often associated with anaphylaxis. Diarrhea, oral or diaper-area candidiasis, morbilliform, and blotchy rashes are not uncommon. The kinds of non-urticarial rashes that may occur while a child is receiving amoxicillin are not known to predispose to anaphylaxis and may not actually be caused by amoxicillin itself; they do not represent a routine contraindication to subsequent use of amoxicillin or any other penicillins. Rarely, beta-lactams cause serious, life-threatening pseudomembranous enterocolitis due to suppression of normal bowel flora and overgrowth of toxin-producing strains of Clostridium difficile. Reversible neutropenia and thrombocytopenia may occur with any of the beta-lactams and seem to be related to dose and duration of therapy, but the neutropenia does not appear to carry the same risk of bacterial superinfection that is present with neutropenia in oncology patients. Third-generation cephalosporins cause profound alteration of normal flora on mucosal surfaces, and all 15 have caused pseudomembranous colitis on occasion. Ceftriaxone commonly causes loose stools, but it is rarely severe enough to require stopping therapy.

Discount 100mg amantadine mastercard
It is characterized by deposition of immune complexes and complement components in the glomerular capillary wall and attendant new basement membrane synthesis chicken pox antiviral cheap 100mg amantadine fast delivery. This histologic pattern is more properly called nephropathy than nephritis, because there is rarely any inflammatory response in the glomeruli or interstitium. In the remaining 20%, the disease is secondary to a variety of disorders (Table 19. In some, such as hepatitis B or thyroiditis, the specific antigen has been identified as part of the immune complex within the deposits in the glomeruli. In others, the association is less well defined, but the designation remains, because treatment of the underlying condition or removal of the putative agent results in resolution of the clinical and histologic features of the disease. Hence a careful history, laboratory evaluation, and review of histologic features must be pursued to rule out potential secondary causes. Ongoing vigilance is also necessary, because the causative agent may not be obvious for months or even years after presentation. Other factors impacting geographic variation include malaria in Africa and hepatitis B in East Asia. The other 30% to 40% of cases present with asymptomatic proteinuria, usually in the subnephrotic range (3. This pattern is particularly common in the elderly, and, unless a urinalysis is performed, these symptoms may be incorrectly labeled as signs of primary cardiac failure. This frequency is substantially lower than that previously reported in studies that used systematic screening for thromboembolic events. In the most extreme cases, this beading can become so dense that careful examination is required to distinguish it from a linear pattern. A classification system has been developed based on their specific location on electron microscopic examination. Unfortunately, the clinical and laboratory correlations with these stages are poor. In others cases, deposits appear as if there had been a continuous production of complexes with growth in size over time, producing lesions that are all at a similar stage and that can extend from the surface of the subepithelial space and penetrate all the way through the basement membrane. Additional diagnostic value may be obtained by staining kidney biopsies for IgG subclasses. This contrasted with positivity in only 37% of patients in partial remission and 10% of patients in complete remission. Generally, antibody levels decrease rapidly in the first 3 months of treatment and disappear over 6 to 9 months, followed by a remission of proteinuria over 12 to 24 months (or longer, as discussed later), independently of the type of immunosuppressive agent used. When taken in concert with follow-up of proteinuria, antibody testing may allow early intervention and earlier stopping of potent immunosuppressive agents. Investigations should include a complement profile, assays for antinuclear antibodies, rheumatoid factor, hepatitis B surface antigen and hepatitis C antibody, thyroid antibodies, and cryoglobulins. The evaluation should consist of most age-appropriate screening tests, including colon cancer screening, mammography, a prostate-specific antigen assay in men, and a chest radiograph (or in high-risk patients, a chest computed tomography). The cost-benefit ratio of this additional screening in the absence of symptoms remains unknown, but, given the dramatic difference in management and outcome, it seems prudent to perform these investigations. Spontaneous complete remissions, defined as a reduction in proteinuria to less than 0. A summary review of 11 large studies demonstrated a 10-year kidney survival rate of 65% to 85%, whereas a more recently pooled analysis of 32 reports indicated a 15-year kidney survival rate of 60%. Spontaneous complete remission rates have been reported in 20% to 30% of longterm (>10 years) follow-up studies, with 20% to 50% of these cases exhibiting at least one relapse. A complete remission and a lower relapse rate are more common in patients with persistent low-grade (subnephrotic) proteinuria and in women. In contrast, male gender, age greater than 50 years, high levels of proteinuria (more than 6 g/day), abnormal kidney function at presentation, tubulointerstitial disease, and focal and segmental lesions on biopsy are all associated with poorer kidney survival rates. The predictive value of the risk score was much greater than that of presence of nephrotic range proteinuria at presentation alone when proteinuria values during 6-month time frames were monitored. When proteinuria was consistently 4 g/ day, its overall accuracy was 71%; when 6 g/day, 79%; and when 8 g/day, 84% (Box 19. The advantages of the algorithm are that it only requires assessing kidney function and proteinuria, and the risk can be calculated repeatedly during the period of follow-up. Age, sex, degree of nephrosclerosis, and presence of hypertension are relevant but do not add to the predictive ability of this model. Importantly, proteinuria and serum creatinine may not accurately reflect disease activity. Patients may be judged to be at high risk and exposed to potentially toxic immunosuppressive therapy but could still develop a spontaneous remission. In addition, the observation period required to assess the risk of progression may delay treatment, resulting in significant residual kidney damage. Achieving a partial remission is associated with a significant slowing of the decline in kidney function at 10 years when compared with patients who do not experience remission. This dyslipidemia probably plays a role in the increased risk for cardiovascular disease in patients with prolonged high-grade proteinuria. Blood pressure reduction has been shown to reduce proteinuria and should be part of the management from the time of diagnosis. A majority of physicians use anticoagulation as primary prevention only in high-risk cases or reserve its use until after documentation of a thromboembolic event. In a series of more than 300 cases from three distinct geographic regions followed for more than 5 years, fewer than 8% developed a measurable decrease in kidney function. Immunosuppression is not recommended, as long as the patient remains in the low risk for progression category. In the majority of cases (70%), this will occur within the first year after diagnosis. There is evidence for a treatment benefit when corticosteroids are combined with a cytotoxic agent. Therapy consisted of 1 g of intravenous methylprednisolone on the first 3 days of months 1, 3, and 5, followed by 27 days of oral methylprednisolone at 0. This therapeutic regimen was found to be superior to either no treatment or methylprednisolone monotherapy, although in the latter study, the benefit was not significant after 4 years of follow-up. The original regimen was remarkably safe, and all adverse events were reversed after stopping the drugs. However, a substantial relapse rate of approximately 30% was seen within 2 years in both groups, regardless of whether they were treated with chlorambucil or cyclophosphamide. Fewer patients had to discontinue cyclophosphamide (5%) compared with chlorambucil (14%). Using this regimen versus conservative therapy, similar long-term results were reported in a trial from India. Regimens using longer term (1 year) cyclophosphamide and lower dose prednisone have also demonstrated an improved outcome, but in these studies the patients were compared with historical controls, and the total cumulative dose of cyclophosphamide far exceeded the total dose used in the Ponticelli protocol. Cyclosporine has shown results similar to the cytotoxic/ steroid regimen in terms of improving proteinuria in the medium risk for progression group. Complete or partial remission in proteinuria was seen in 70% of the cyclosporine group compared with 24% of the control group. The relapse rate (40% to 50% within 2 years of discontinuing the drug) was higher than that seen in the Italian trials. A study using a longer duration of cyclosporine treatment at a dose of 2 to 4 mg/kg per day for 12 months, followed by a reduction in the cyclosporine therapy in the range of 1. Acthar Gel), currently approved in the United States for remission of proteinuria in the nephrotic syndrome, reported similar encouraging results. Most patients were treated for a minimum of 6 months, with the longest treatment period being 14 months. Several prospective but nonrandomized pilot studies using rituximab monotherapy have demonstrated complete or partial remission in proteinuria in 60% to 80% of patients by the end of the trial. A recent study reported that only 18 of the 65 patients treated with rituximab (the majority treated with one single dose) that achieved complete or partial remission had a relapse of proteinuria from 7 to 116 months (median 42 months) after treatment. Lower antibody levels at baseline and full antibody depletion at 6 months after rituximab treatment were strong predictors of remission. A B-cell titrated protocol using a single dose of 375 mg/m2 rituximab has been proposed to be as effective as the four-dose protocol, at a lower cost. The response to rituximab is independent of patients receiving it as first- or second-line therapy.
Buy amantadine on line
Mortality rate comparison after switching from continuous to prolonged intermittent renal replacement for acute kidney injury in three intensive care units from different countries who hiv infection stages cheap 100 mg amantadine mastercard. Intermittent versus continuous renal replacement therapy for acute renal failure in adults. Hyperoncotic colloids and acute kidney injury: a meta-analysis of randomized trials. Shirali Medications are a mainstay of appropriate patient care, and new agents are being introduced into clinical practice at a rapid pace. Although most drugs are well tolerated, and therapeutic agents are often essential for medical care, kidney injury remains an unfortunate and relatively frequent adverse consequence. This bespeaks the fact that some individuals possess risk factors that predispose to drug-induced kidney toxicity. Not unexpectedly, the general population is regularly exposed to various diagnostic and therapeutic agents with nephrotoxic potential. Although most are prescribed, many other preparations are purchased over the counter. Drugs fall into the categories of diagnostic agents, therapeutic medications, alternative or complementary substances, and drugs of abuse, resulting in a variety of kidney syndromes (Table 35. As we learn more about drug-induced kidney disease, it appears that these factors explain much of the variability and heterogeneity noted among patients. Drug-related factors are the critical first step to the development of nephrotoxicity. Innate drug toxicity is important because the drug or its toxic metabolite may cause kidney injury by impairing renal hemodynamics, direct cellular injury, osmotic injury, or intratubular crystal deposition, to name a few conditions. Large doses, extended drug exposure, and nephrotoxic drug combinations further enhance nephrotoxicity. As renal blood flow approximates 25% of cardiac output, the kidney is significantly exposed to nephrotoxic drugs. Kidney injury is increased in the loop of Henle where high metabolic rates coexist with a relatively hypoxic environment. Increased drug/metabolite concentrations in the kidney medulla also contribute to direct toxicity. The kidney pathway of excretion for many therapeutic agents involves proximal tubular cells. Extensive drug trafficking through the cell via luminal and basolateral transporters can lead to cellular injury. Some drugs are endocytosed at the luminal membrane of cells, whereas other drugs are transported into the cell via basolateral ion transporters. Such drug transport can be associated with increased cellular concentrations that injure mitochondria, phospholipid membranes, lysosomes, and other organelles. Nonmodifiable factors such as older age and female sex increase nephrotoxic risk through reduced total body water leading to drug overdose. Pharmacogenetic differences likely explain much of the variable response of patients to drugs. Polymorphisms of genes encoding proteins involved in the metabolism and kidney elimination of drugs are correlated with nephrotoxic risk. Another important aspect of genetic makeup is a highly variable host immune response to drugs; one patient reacts with a heightened allergic response, whereas another has a limited reaction with no kidney lesion. Kidney susceptibility to drug injury is also enhanced by true and effective volume depletion, including nausea/ vomiting, diarrhea, and diuretic therapy, as well as heart failure, liver disease with ascites, and sepsis. This physiology enhances the nephrotoxicity of drugs that are excreted primarily by the kidney, drugs reabsorbed/secreted by the proximal tubule, and drugs that are insoluble in the urine. Finally, electrolyte and acid-base disturbances present in some patients also contribute to host susceptibility to drug injury. Recognizing that all drugs cannot be covered in this chapter, we describe drug-induced nephrotoxicity by drug category and highlight the clinical kidney syndrome and the segment of nephron injury by the drug within each category. It is defined by an absolute or percentage rise in serum creatinine from the baseline within 48 to 72 hours. In general, serum creatinine begins to rise within the first 24 hours after exposure, peaks between 2 and 5 days, and returns to baseline by 7 to 14 days. In the presence of reduced kidney function, the elimination (T1/2) of radiocontrast agents is increased. Thus, the kidney undergoes prolonged contrast exposure that increases the likelihood of kidney injury. First, vasoactive substances, such as adenosine and endothelin, mediate vasoconstriction of the afferent arterioles, thereby reducing renal blood flow and promoting kidney medullary ischemia. Second, renal epithelial cell necrosis also occurs with isoosmolar radiocontrast agents because their high viscosity causes sluggish blood flow through the peritubular capillaries and promotes hypoxic kidney injury. Lastly, radiocontrast causes direct renal tubular toxicity through hyperosmolar injury, which results in vacuolization of proximal tubular cells, and oxidative stress from free oxygen radicals with associated tubular cell apoptosis and necrosis. In addition, patient-specific risk factors include older age, volume depletion, congestive heart failure, diabetes mellitus, both hypertension and hypotension, and anemia. Emergent procedures increase risk because of reduced use of contrast prophylaxis and increased severity of patient illness. With regard to radiocontrast type, osmolality and viscosity are the two most important characteristics. As radiocontrast exposure is often predictable, measures to reduce kidney injury should be undertaken in patients at risk. Thus, sodium bicarbonate is not superior to isotonic saline, and either solution is acceptable for radiocontrast prophylaxis. Approximately half of the published randomized controlled trials demonstrate benefit, whereas several meta-analyses suggest either large benefit or no benefit. Beneficial studies are notable for early publication dates, small size, and low quality. Given its favorable safety profile, low cost, easy administration, and wide availability, clinicians could argue for continued use of the drug as prophylaxis. However, the Acetylcysteine for ContrastInduced Nephropathy Trial casts doubt on this conclusion. In contrast, the hemofiltration post-procedure alone offered no benefit beyond standard prophylaxis. Nephrotoxicity may be related to a direct effect on tubules, mediated by osmolarity or some other mechanism. However, when this disease develops, its consequences are often devastating, and therapeutic options are limited. Therapies such as extracorporeal photopheresis, sodium thiosulfate, and imatinib show promise; however, only early kidney transplant may offer stabilization or reversal of the fibrosing process. They are administered as a solution or tablets before the procedure and contain approximately 38 g of monobasic sodium phosphate and 9 g of dibasic sodium phosphate. The adverse events associated with phosphate-containing bowel preparations occur with excessive dosing or use in patients with underlying kidney disease. Tubular injury and atrophy with abundant calcium phosphate deposits in distal tubules and collecting ducts were features on kidney biopsy. Thus, oral sodium phosphate-based products should not be used in patients with underlying kidney disease, volume depletion, or electrolyte abnormalities. Patients with hypertension, heart failure, and diuretic therapy had an adjusted relative risk of 11. This is especially common in patients with hypertension, heart disease, and other salt-retentive disease states. A similar clinical syndrome marked by proteinuria (rarely nephrotic) and hypertension occurs in patients treated with antiangiogenesis agents such as bevacizumab and the tyrosine kinase inhibitors. One of their major adverse effects is nephrotoxicity, seen primarily with pamidronate and zoledronate. Depending on the particular bisphosphonate, glomerular and/or tubular injury may result. Pamidronate-induced kidney injury is dose related, where high dosage and long duration increase risk. The time to clinical presentation is shorter for interferon- as compared to other subtypes. Although proteinuria declines with cessation of interferon therapy, complete reversal is uncommon. The mechanism underlying interferon-associated glomerular injury is not entirely clear, but it may include direct binding to podocyte receptors and alteration of normal cellular proliferation. Cisplatin has the most nephrotoxic potential, although second- and thirdgeneration drugs such as carboplatin and oxaliplatin are also nephrotoxic at high doses.
