
Buy mircette 15mcg online
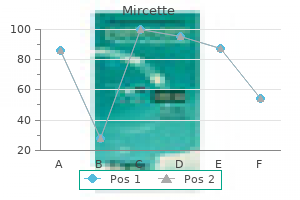
On plain radiographs birth control pills womens rights buy mircette cheap online, a "lateral capsular sign" shows avulsion of the midportion of the lateral capsular ligament with a small fragment of proximal lateraltibia. Casesofmildinstabilitymaybe treated nonoperatively similar to that for lesser-grade sprains. Atthetimeofinjury,thepatientexperiences sudden pain, which may be associated with a tearing sensationabouttheknee. Also, the patient may not be able to maintain a passively extended knee against gravity. In both cases, surgery is required to reestablish the continuity of the quadriceps mechanism. After postoperative immobilization for 8 to 10 weeks, patients gradually start protected range-ofmotion exercises and should use a cane or walker for sometime. Circulation and nerve function must be carefully evaluated before and after reduction. Whereas apatelladislocation involves the patellofemoral joint, a knee dislocation involves the tibiofemoral articulation. Striking the knee against the dashboard during an automobile accident is the most common cause of injury, but athletic injuries are also common causes. Classification of knee dislocations is based on the position of the tibia in relation to the femur. Lateral,medial,androtational dislocations may also occur, as may combination patterns such as anterolateral and posterolateral. Tear or thrombosis of popliteal artery is a frequent complication, requiring immediate repair or replacement. Tibial and common peroneal nerves may also be torn but usually do not require surgical repair. Four-compartment fasciotomy must be done at the first sign of compartment syndrome. Inanteriordislocations, stretching of the artery and vein is severe and often results in vascular injury. Obese children are more prone to this problem because of increasedloadontheirjoints. Ifthedefectislarge,thejointmaybecomeincongruous, leading to mechanical signs and symptoms. Whenradiographsare taken for other reasons, these defects are not unusual findings. A necroticappearing flap of cartilage is lifted from the diseased medial femoral condyle. The medial femoral condyle is most commonly involved, but osteonecrosis also may occur in the lateral femoral condyle and the tibial plateau (usuallymedial). Smallerlesions(<5cm2)typicallyhavea better clinical prognosis and may be satisfactorily treated with activity modification and use of assistive devices such as a cane. Progressive symptoms may necessitate drilling of the lesion, realignment osteotomy,ortotalkneereplacement. Complete fracture, displaced Type I tibial spine fracture the terms tibial spine, tibial eminence, and intercondylar eminence are used interchangeably to designate the nonarticular portion of the adjacent medial and lateral tibial plateaus to which the anterior cruciate ligament is attached anteriorly. Injuries that typically cause ruptures of the anterior cruciate ligament in adults often cause a fracture of the tibial spine in children 7 to 14 years of age. On the date of injury, the patient underwent debridement of the right tibia with application of an external fixator and retrograde nailing of the right femur, and intramedullary nailing of the left tibia. Nine days after injury, intramedullary nailing of the right tibia and open reduction and plating of the right calcaneus were done. Becausethis is an intra-articular fracture, anatomic reduction is required for return of knee function. Duringsurgery,allsoft tissue is removed from the fracture site and the tibial spine is replaced in its anatomic position and fixated with sutures or a screw. In the fetus, thin synovial membranes divide the knee joint into three compartments (medial,lateral,andpatellar). Inthefifthmonthoffetal development, these partitions usually degenerate and thekneejointbecomesonecavity. Most synovial folds contain a considerable amount of elastin and areolar tissue and are thus extensible and asymptomatic. Many are detected during routine arthroscopic procedures performedforotherreasons. Whenthekneeisextended, the patella protects the anterior aspect of the femoral condyles, but when the knee is flexed, the medial condyleismorevulnerable. With the tibia internally rotated, the examiner passively With flexion, plica sweeps across condyle. Arthrosopic resection of medial plica using motorized instrument After resection, preexisting condylar erosion (due to irritation by plica) can be seen. Examining fingers placed along the medial patellofemoral joint may feel a click, possiblysometenderness,orevenapopofapathologicplica. Typically, the prepatellar bursa, pes anserinus bursa, tibial collateral ligament bursa, and deep infrapatellar bursaareinvolved. Careful physical examination and routine laboratory studies, such as a white blood cell count and determination of the levels of inflammatorymarkers,arebothimportantpartsofthe assessment of a patient with an acute presentation of bursitis. The patient may present with lateral knee pain on activity, tightness of the iliotibial band, and occasionallypopping. Initial treatment options include iliotibial band stretching exercises, anti-inflammatory agents, ultrasound to the lateral femoral epicondyle, and corticosteroid injection. Rarely, in refractory cases, surgery can be done to release an area of tightness or debride any focal areas ofinflammation. Diffuse Villonodular Synovitis this condition typically occurs in adults between 20 and 40 years of age. A single joint of the lower limb, mostfrequentlytheknee,isthemostcommonsiteof involvement. Lateinthedisease,thepathologicchangesmaycause pressure indentation of bone and sometimes actual invasion of bone at the articular margins with subsequentbonedestruction. The predominant symptom is a chronic, slowly increasing swelling of the joint that is associated with mildaching. Because the course of the disease is usually benign, diagnosis and treatment are often delayed. Early on, radiographic examination may reveal an increase in joint fluid and a thickened synovial membrane. The cysts normally develop in the periphery of the middle third of the meniscus and in the adjacent soft tissues within the joint capsule. Rehabilitation must begin as soon as possible after injury, because disuse atrophy of the muscles occurs rapidly. Rehabilitation focuses on muscle strengthening, particularly strengthening of the extensor (quadriceps) muscles and the flexor (medial and lateral hamstring) muscles. The knee is flexed in an arc of motion between 30 and 90 degrees, avoiding full extension. Resistance is appliedinthepain-freeportionoftherangeofmotion, with the tibia internally and externally rotated to strengthenthehamstringmuscles. Use of a stationary bicycle, with the resistance set at zero, is effective and also improves the range of motion in the knee. Once the knee is pain free, the resistance can be increased for furthercardiovascularbenefits. Straight-legraises,flexion-to-extension exercises within the safe range of limited motion, cocontractions,hipflexionexercises,andlegcurlsarealso started to maintain muscle tone and strength. By 6 months, a program to achieve full extension should have begun with slow, progressive resistance exercises, such as light squatting with the thighs parallel with the floor. The patient should avoid running until the injured limb has regained at least 80% of the strength of the normallimb. Thisanatomicvariantrepresents a true synchondrosis (a joint whose surfaces are connected by a cartilaginous plate). Patient treated with 4 weeks of immobilization for suspected quadriceps strain/slight avulsion of bipartite fragment.
Syndromes
- Treatment of the physical, emotional, and social concerns
- Uncoordinated movements (ataxia)
- Stage III -- Treatment involves surgery, possibly followed by chemotherapy, hormone therapy, and biologic therapy.
- Divide that answer by your height in inches.
- Blood tests such as a complete blood count (CBC)
- If the person starts having convulsions, give convulsion first aid.
Order online mircette
Progressing from superficial to deep (posterior to anterior) within the fossa birth control for 8 days generic 15mcg mircette with amex, as in dissection, the nerves are encountered first, then the veins. The tibial nerve is the most superficial of the three main central components of the popliteal fossa. Five genicular branches of the popliteal artery supply the capsule and ligaments of the knee joint. They participate in the formation of the periarticular genicular anastomosis, a network of vessels surrounding the knee that provides collateral circulation capable of maintaining blood supply to the leg during full knee flexion, which may kink the popliteal artery. Muscular branches of the popliteal artery supply the hamstring, gastrocnemius, soleus, and plantaris muscles. The superior muscular branches of the popliteal artery have clinically important anastomoses with the terminal part of the profunda femoris and gluteal arteries. Throughout its course, the vein lies close to the popliteal artery, lying superficial to it and in the same fibrous sheath. The popliteal vein is initially posteromedial to the artery and lateral to the tibial nerve. Superiorly, the popliteal vein, which has several valves, becomes the femoral vein as it traverses the adductor hiatus. The deep popliteal lymph nodes surround the vessels and receive lymph from the joint capsule of the knee and the lymphatic vessels that accompany the deep veins of the leg. The many arteries making up the peri-articular anastomosis around the knee provide an important collateral circulation for bypassing the popliteal artery when the knee joint has been maintained too long in a fully flexed position or when the vessels are narrowed or occluded. While in the fossa, the tibial nerve gives branches to the soleus, gastrocnemius, plantaris, and popliteus muscles. The nerve leaves the fossa by passing superficial to the lateral head of the gastrocnemius and then passes over the posterior aspect of the head of the fibula. The nerve traverses most of the length of the posterior compartment of the thigh deep to the fascia lata; only its terminal branches enter the subcutaneous tissue as cutaneous nerves. The anterior (dorsiflexor or extensor) compartment contains four muscles (the fibularis tertius lies inferior to the level of this section). The posterior (plantarflexor or flexor) compartment, containing seven muscles, is subdivided by an intracompartmental transverse intermuscular septum into a superficial group of three (two of which are commonly tendinous/aponeurotic at this level) and a deep group of four. It forms a strong loop around the tendons of the fibularis tertius and the extensor digitorum longus muscles. These muscles pass and insert anterior to the transversely oriented axis of the ankle (talocrural) joint and, therefore, are dorsiflexors of the ankle joint, elevating the forefoot and depressing the heel. The long extensors also pass along and attach to the dorsal aspect of the digits and are thus extensors (elevators) of the toes. The latter is important to a smooth gait and is important to deceleration (braking) relative to running and walking downhill. During standing, the dorsiflexors reflexively pull the leg (and thus the center of gravity) anteriorly on the fixed foot when the body starts to lean (the center of gravity begins to shift too far) posteriorly. The central band inserts into the base of the middle phalanx, and the lateral slips converge to insert into the base of the distal phalanx. It may play a special proprioceptive role in sensing sudden inversion and then contracting reflexively to protect the anterior tibiofibular ligament, the most commonly sprained ligament of the body. These dissections demonstrate the continuation of the anterior and lateral leg muscles into the foot. The thinner portions of the deep fascia of the leg have been removed, leaving the thicker portions that make up the extensor and fibular retinacula, which retain the tendons as they cross the ankle. At the ankle, the vessels and the deep fibular nerve lie midway between the malleoli and between the tendons of the long dorsiflexors of the toes. This dissection shows the muscles of the anterolateral leg and dorsum of the foot. The common fibular nerve, coursing subcutaneously across the lateral aspect of the head and neck of the fibula, is the most commonly injured peripheral nerve. In this deeper dissection of the anterior compartment, the muscles and inferior extensor retinaculum are retracted to display the arteries and nerves. It is one of the two terminal branches of the common fibular nerve, arising between the fibularis longus muscle and the neck of the fibula. The deep fibular nerve then exits the compartment, continuing across the ankle joint to supply intrinsic muscles (extensors digitorum and hallucis brevis), and a small area of the skin of the foot. The smaller terminal branch of the popliteal artery, the anterior tibial artery, begins at the inferior border of the popliteus muscle. Here the tendons of the two muscles of the lateral compartment (fibularis longus and brevis) enter a common synovial sheath to accommodate their passage between the superior fibular retinaculum and the lateral malleolus, using the latter as a trochlea as they cross the ankle joint. Here it is subject to entrapment as it passes beneath the tendinous arch of the soleus muscle. These muscles have their fleshy bellies in the lateral compartment but are tendinous as they exit the compartment within the common synovial sheath deep to the superior fibular retinaculum. However, because the fibularis longus and brevis pass posterior to the transverse axis of the ankle (talocrural) joint, they contribute to plantarflexion at the ankle-unlike the postaxial muscles of the anterior compartment (including the fibularis tertius), which are dorsiflexors. In practice, the primary function of the evertors of the foot is not to elevate the lateral margin of the foot (the common description of eversion) but to depress or fix the medial margin of the foot in support of the toe off phase of walking and, especially, running and to resist inadvertent or excessive inversion of the foot (the position in which the ankle is most vulnerable to injury). When standing (and particularly when balancing on one foot), the fibularis muscles contract to resist medial sway (to recenter a line of gravity, which has shifted medially) by pulling laterally on the leg while depressing the medial margin of the foot. Because the nerve and blood vessels supplying the entire posterior compartment and the sole of the foot pass through the deep subcompartment, when swelling occurs it leads to a compartment syndrome that has serious consequences, such as muscular necrosis (tissue death) and paralysis. The retinaculum is subdivided deeply, forming separate compartments for each tendon of the deep muscle group, as well as for the tibial nerve and posterior tibial artery as they bend around the medial malleolus. The posterior compartment and the muscles within it are divided into superficial and deep subcompartments/muscle groups by the transverse intermuscular septum. The gastrocnemius and soleus share a common tendon, the calcaneal tendon, which attaches to the calcaneus. These muscles are strong and heavy because they lift, propel, and accelerate the weight of the body when walking, running, jumping, or standing on the toes. It then widens as it inserts on the posterior surface of the calcaneal tuberosity. Although they share a common tendon, the two muscles of the triceps surae are capable of acting alone, and often do so: "You stroll with the soleus but win the long jump with the gastrocnemius. A deep bursa of the calcaneal tendon (retrocalcaneal bursa), located between the tendon and the calcaneus, allows the tendon to glide over the bone. It is a fusiform, two-headed, two-joint muscle with the medial head slightly larger and extending more distally than its lateral partner. The gastrocnemius crosses and is capable of acting on both the knee and the ankle joints; however, it cannot exert its full power on both joints at the same time. The three heads of the triceps surae muscle attach distally to the calcaneus via the spiraling fibers of the calcaneal tendon. The transverse intermuscular septum has been split to reveal the deep muscles, vessels, and nerves. The popliteus acts on the knee joint, whereas the other muscles plantarflex the ankle with two continuing on to flex the toes. However, because of their smaller size and the close proximity of their tendons to the axis of the ankle joint, the "non-triceps" plantarflexors collectively produce only about 7% of the total force of plantarflexion, and in this the fibularis longus and brevis are most significant. The soleus has a continuous proximal attachment in the shape of an inverted U to the posterior aspects of the fibula and tibia, and a tendinous arch between them, the tendinous arch of soleus (L. The soleus can be palpated on each side of the gastrocnemius when the individual is standing on their tiptoes. The soleus may act with the gastrocnemius in plantarflexing the ankle joint; it cannot act on the knee joint and acts alone when the knee is flexed.
Buy genuine mircette
In addition to tracking known adverse outcomes of transfusion and resulting in development of mitigation strategies birth control for women chapel order mircette 15 mcg amex, an important additional benefit of fully implemented national and international hemovigilance networks will be early detection of novel infectious and non-infectious hazards of transfusion. A perspective on transfusion-related acute lung injury two years after the Canadian Consensus Conference. It is increasingly being recognized that this reaction does not always manifest with fever, and in approximately 85% of reactions, patients might experience only chills, cold sensation and discomfort in the absence of fever. Patients experiencing severe reactions, especially if repeated, might become apprehensive about future transfusions. The mild and moderate reactions cause the patient discomfort and increase the use of hospital resources. Sepsis due to the transfusion of bacterially contaminated blood product usually presents with a higher increase in fever and hypotension. In this case Gram stain and culturing of the patient and the unit will help exclude septic transfusion reactions. Immunosuppressed patients with malignancies commonly have intermittent temperature spikes due to infections that could be misinterpreted as febrile transfusion reactions. Furthermore, assigning the reaction to a particular unit of blood product might be difficult in patients receiving multiple consecutive transfusions. There is a significant variability in reported rates of these reactions between institutions, influenced by multiple factors, including premedication use, storage age of blood product and product preparation. Certain patient populations are considered to be at a higher risk of developing febrile reactions, including patients with hematologic malignancies, who are at risk of alloimmunization due to frequent transfusions and in whom existing clinical factors, such as inflammation, may increase the likelihood of febrile response to infused cytokines. The reported incidence for pre-storage leukoreduced platelet products (apheresis or whole blood derived) is 0. In some studies, more reactions are observed when 4 to 5 day old platelet concentrates are transfused, most likely related to an increase in cytokine levels in those products demonstrated after 3 days of storage. These cytokines induce the production of prostaglandin E2, which acts on the hypothalamus to increase body temperature. An immune-mediated mechanism that depends on donor cytokines is seen in patients with preformed white blood cell alloantibodies which stimulate transfused donor white blood cells to release cytokines. This type of reaction is prevented by both pre-storage and bedside leukocyte reduction. In this case, leukoreduction is effective only in preventing reactions mediated by antibody interaction with donor leukocytes but not platelets. The antibody interaction with donor platelets provides a possible explanation for febrile reactions in alloimmunized recipients of pre-storage leukocyte-reduced platelets. Passive transfer of pro-inflammatory cytokines accumulated in the plasma portion of the product during storage at room temperature results in fever in the recipient upon transfusion. Leukocyte-derived cytokines have been demonstrated in supernatant plasma of stored platelet products, and their levels correlate with the duration of storage and pre-storage number of leukocytes. Pre-storage leukocyte reduction is effective, although it does not eliminate these reactions completely, possibly due to platelet-derived mediators that are not removed by leukocyte reducing filters. Treatment: Transfusion should be discontinued immediately and antipyretics administered. The patient should be reassured that these are self-limited reactions that do not leave longterm consequences. Post-storage leukoreduction is not effective in preventing reactions to platelets that are mediated by accumulation of cytokines released from leukocytes during storage. Pre-storage leukoreduction is not effective in removing platelet-derived mediators, and some patients experience repeat reactions to even pre-storage leukoreduced blood products. Decreasing cytokine levels in platelet products can also be achieved by removal of stored supernatant plasma. Adding plasma removal step prior to platelet transfusion decreased the rate of febrile reactions to poststorage leukoreduced platelets from 20% to 0. However, the impact of additional centrifugation on function of stored platelets should be considered when evaluating this approach. Two prospective, randomized, controlled trials examined the effectiveness of acetaminophen and diphenhydramine in preventing transfusion reactions. In the first study, 51 patients with hematological malignancies experienced 12 febrile and three allergic reactions when transfused with 98 pre-storage leukoreduced apheresis platelets. The results of this study suggest that premedication is ineffective in preventing the febrile reactions in patients receiving pre-storage leukoreduced apheresis platelets. However, the subgroup analysis revealed that febrile reactions were less frequent in the treatment group compared to the placebo group (0. The utility of <3-day-old whole-blood platelets in reducing the incidence of febrile nonhemolytic transfusion reactions. A prospective, randomized, double-blind controlled trial of acetaminophen and diphenhydramine pretransfusion medication versus placebo for the prevention of transfusion reactions. Platelet washing to prevent recurrent febrile reactions to leucocyte-reduced transfusions. Acetaminophen and diphenhydramine as premedication for platelet transfusions: a prospective randomized double-blind placebo-controlled trial. On one end of the spectrum, typical mild allergic reactions consist of isolated, pruritic/urticarial lesions. On the other end of the spectrum is anaphylaxis, which is an acute, life threatening, systemic allergic reaction that is characterized most significantly by hypotension and/or respiratory compromise. The term anaphylactoid has been used historically to describe either systemic hypersensitivity reactions not mediated by IgE or moderate severity allergic reactions that involve allergic signs or symptoms other than cutaneous manifestations. Anaphylactic reactions occur in approximately 1 in 20,000 to 47,000 components transfused. Clinical investigations have shown no benefit of leukoreduction in the incidence of allergic reactions, and atopic disease in donors does not appear to contribute to allergic reactions. Recipient atopic susceptibility may be involved, as some patients experience recurrent reactions and show evidence of other allergic sensitization. Urticarial reactions consist of pruritic, localized, well-circumscribed, discrete wheals with erythematous, raised, serpiginous borders and blanched centers. There may be generalized erythema (flushing) of the skin or angioedema, which is localized, nonpitting and deep edema of the skin. Lower airway obstruction results in audible wheezing, a feeling of chest tightness, substernal pain, dyspnea, cyanosis, anxiety and/or a feeling of impending doom. In addition, there may be profound hypotension, possibly leading to loss of consciousness, tachycardia, cardiac arrhythmias or cardiac arrest. Severe gastrointestinal symptoms (abdominal cramps/pain, nausea, vomiting, diarrhea) may also be present. Diagnosis: Pruritus and urticaria are the hallmarks of allergic transfusion reactions, but some other symptoms that are consistent with allergic reactions overlap with other types of reactions. The differential diagnosis of allergic reactions includes reactions Transfusion Medicine and Hemostasis. Immediate hemolytic transfusion reactions usually have the presence of fever and absence of cutaneous manifestations. Hypotensive reactions have marked drops in blood pressure without cutaneous symptoms or other signs of anaphylaxis. Bacterial contamination is associated with hypotension and shock, but the presence of rigors and fever differentiate it from allergic reaction. Circulatory overload can be differentiated from an allergic reaction by the presence of pulmonary edema and hypervolemia with hypertension. Patients with a severe allergic reaction should be tested for IgA deficiency and the presence of anti-IgA. Reference laboratories can perform IgA tests which are more sensitive and can distinguish severe IgA deficiency from IgA concentrations that are present, but below the limit of detection of routine assays. Anti-IgA testing is currently only performed in reference laboratories, and a common diagnostic approach is to screen for anti-IgA antibodies only after severe IgA deficiency is diagnosed. Pathophysiology: Allergic reactions manifest clinically as type I hypersensitivity responses, which are typically mediated by IgE; however, the evidence for IgE involvement in allergic transfusion reactions is limited. In IgE-mediated hypersensitivity responses, IgE binds to mast cells and basophils by means of IgE Fc receptors. When an allergen, thought to be a protein in the plasma of the transfused blood component, binds the cell-associated IgE, the mast cell is activated and releases mediators (such as histamine, heparin, leukotrienes, platelet-activating factor, cytokines and chemokines).
Cheap 15mcg mircette visa
The Kleihauer-Betke test is performed on a maternal blood smear treated with acid and then stained so the fetal cells remain red and the maternal cells appear as ghosts birth control for women in late 40s cheap mircette online master card. The goal of blood bank prenatal testing is to identify the alloantibody (see Chapter 20) to determine the clinical significance of the alloantibody (Table 48. Fetal genotyping or phenotyping may be performed to determine the antigen status of the fetus. Antibody Titration: Antibody titers should be performed using a standard procedure. The critical titer varies between laboratories, but most institutions use 8 to 32 for anti-D. With the advent of non-invasive measurements of fetal anemia through Doppler assessment of the middle cerebral artery peak systolic velocity, the role of antibody titration, as well as more invasive techniques, such as amniocentesis and cordocentesis, is limited. Once the critical titer is reached no further titration studies are necessary and the pregnancy should be monitored by middle cerebral artery Doppler. In addition, if the mother had a previously affected fetus or infant, maternal antibody titers are not helpful and the fetus should be monitored for anemia by middle cerebral artery Doppler. Middle cerebral artery blood flow has 88% sensitivity and 82% specificity in predicting fetal anemia. Amniocentesis: Prior to the use of middle cerebral artery peak systolic velocity, serial amniocentesis was used to determine the severity of hemolysis. Serial measurements are used to follow the severity of disease; when values are unchanging or increasing then the disease is worsening. With advances of ultrasonography, allogeneic blood is directly infused into the umbilical cord vein. A combination of intravascular and intraperitoneal transfusions can also be used to prolong the interval between transfusions. Alternatively, the transfused volume is estimated by multiplying the estimated fetal weight by 0. Intravascular exchange transfusions can be performed instead of simple intravascular transfusions, but the simple transfusion is preferred due to the shorter procedure time and being technically easier. Multiply the result by the difference in post-transfusion (desired) and pre-transfusion (intial) Hct 3. Management of hyperbilirubinemia in the newborn infant 35 or more weeks gestation. Biomedical excellence for safer transfusion collaboration; Transfusion Medicine Resource Committee of the College of American Pathologists. Hematological morbidity and management in neonates with hemolytic disease due to red cell alloimmunization. Thus, these antibodies must be binding to a ubiquitous antigen or have nonspecific binding. In contrast to IgG alloantibodies, IgM molecules efficiently activate the complement cascade (starting with C1q) and can result in intravascular hemolysis. The degree of intravascular hemolysis is affected by antibody concentration, thermal amplitude and amount and inactivation by complement regulatory proteins, such as decay accelerating factor and others. The short time period may only be sufficient to activate the complement cascade to the C3b stage and not to the membrane attack complex stage. Clinical Manifestations: the presence of antierythrocyte autoantibodies does not always cause hemolysis and thus anemia. The plasma-phase autoantibody usually reacts as a panagglutinin in the indirect antiglobulin test. First line treatment is usually corticosteroids; other treatments include splenectomy, rituximab, intravenous immunoglobulin, and alternate immunosuppressive medications. Due to the presence of a strong autoantibody, both the direct and indirect antiglobulin tests (and thus the antibody screening tests and panels) will be positive as the autoantibody, reacting as a panagglutinin, will react with all tested cells. It is also helpful to recognize that the presence of a panagglutinin will create positive crossmatch results and thus the crossmatch will not be helpful in determining compatibility with underlying alloantibodies. The Johns Hopkins Hospital published their approach to patients with warm autoantibodies (Shirey et al. During analysis of subsequent samples if the serologic results were consistent with previous findings, then phenotype-matched products were provided. Twelve of the 20 patients studied could be fully phenotyped and eight patients could be partially phenotyped or phenotyping was indeterminate. The patients received between two to 39 products and none developed new alloantibodies during the study period of 13 months. Due to the presence of the warm, IgG autoantibody in these patients, it is typically not possible to indentify crossmatch compatible units. Arguments against this approach include: there is scant data to support this approach, and this practice increases the likelihood that an alloantibody will be induced to the antithetical antigen. The typical clinical manifestations are a moderate chronic hemolytic anemia, which is exacerbated in the cold, in a middle-aged or elderly person with a good prognosis. In severe cases, the IgM autoantibody can result in severe, life-threatening intravascular hemolysis. The specificity of the antibody associated with infectious mononucleosis is anti-i. In addition, a clonal lymphoproliferative disorder, usually characterized as lymphoplasmacytic lymphoma, has been identified through immunohistochemical staining of the bone marrow of these patients. Plasma free hemoglobin binds haptoglobin and thus free haptoglobin measurements are low. In the majority of cases the anemia is mild; thus cold avoidance is the sole treatment used to prevent exacerbations. Some suggest using a blood warmer, especially in severe cases, in addition to keeping the patient warm and transfusing the product slowly. However, the effect of plasma exchange is usually temporary and should therefore be combined with immunosuppressive therapy. Drug-Induced Hemolytic Anemia: Administration of a number of commonly used medications can lead to hemolysis typically occurring secondary to the mechanisms described below. Drug-induced hemolytic anemia may occur acutely as intravascular hemolysis soon after the patient receives the drug, or it may have a milder presentation as extravascular hemolysis sometimes months after drug administration. Some of the antibodies produced require the presence of the drug (drug dependent) for their detection and/or destruction, while others do not (drug-independent). If an eluate does not react during an antibody screen and the patient has recently received a drug, then it is important to test for drug-dependent antibodies. Patients who have an acute presentation of hemolysis after receiving a drug often have a history of prior administration of the same drug and therefore have previously formed antibodies. The disease has an excellent prognosis and treatment is usually to discontinue the medication. Drug-induced hemolytic anemia is most often associated with an IgG antibody with Rh specificity. The blue lines represent antigen-binding sites on the F(ab) region of the drug-induced antibody. Drugs (haptens) bind loosely, or firmly, to cell membranes and antibodies may be made to: (a) the drug (producing in-vitro reactions typical of a drug adsorption [penicillin-type] reaction); (b) membrane components, or mainly membrane components (producing in-vitro reactions typical of autoantibody); or (c) part-drug, part-membrane components (producing an in-vitro reaction typical of the so-called immune complex mechanism). From a blood bank and transfusion service perspective, it is imperative to consider drug-induced hemolytic anemias under the appropriate clinical circumstances.
Order generic mircette from india
Venous drainage by the superior mesenteric vein and inferior mesenteric vein corresponds to the pattern of the superior mesenteric artery and inferior mesenteric artery birth control kelnor cheap mircette 15 mcg amex. Lymph from the large intestine flows sequentially to epicolic nodes (on the gut), paracolic nodes (along mesenteric border), intermediate colic nodes (along the colic arteries), and then to the superior or inferior mesenteric nodes and the intestinal trunks. Innervation of the colon occurs by means of mixed peri-aterial plexuses extending from the superior and inferior mesenteric ganglia along the respective arteries. Individuals with a slender asthenic physique are likely to have a transverse colon that dips down toward or into the pelvis. The termination of the teniae coli, approximately 15 cm from the anus, indicates the rectosigmoid junction. The sigmoid colon usually has a long mesentery-the sigmoid mesocolon-and therefore has considerable freedom of movement, especially its middle part. The left ureter and the division of the left common iliac artery lie retroperitoneally, posterior to the apex of the root of the sigmoid mesocolon. The teniae coli also disappear as the longitudinal muscle in the wall of the colon broadens to form a complete layer in the rectum. The superior branch of the most superior sigmoid artery anastomoses with the descending branch of the left colic artery, thereby forming a part of the marginal artery. However, lymph from the left colic flexure may also drain to the superior mesenteric lymph nodes. The sympathetic nerve supply of the descending and sigmoid colon is from the lumbar part of the sympathetic trunk via lumbar (abdominopelvic) splanchnic nerves, the superior mesenteric plexus, and the peri-arterial plexuses following the inferior mesenteric artery and its branches. Esophageal varices commonly develop in persons who have developed alcoholic cirrhosis (fibrous scarring) of the liver (see the blue box "Cirrhosis of the Liver," p. This adhesion occurs because of the close relationship of the posterior wall of the stomach to the pancreas. Hiatal Hernia A hiatal (hiatus) hernia is a protrusion of part of the stomach into the mediastinum through the esophageal hiatus of the diaphragm. The hernias occur most often in people after middle age, possibly because of weakening of the muscular part of the diaphragm and widening of the esophageal hiatus. Although clinically there are several types of hiatal hernia, the two main types are paraesophageal hiatal hernia and sliding hiatal hernia (Skandalakis et al. In these cases, usually no regurgitation of gastric contents occurs because the cardial orifice is in its normal position. Some regurgitation of stomach contents into the esophagus is possible because the clamping action of the right crus of the diaphragm on the inferior end of the esophagus is weak. As a result, food does not pass easily from the stomach into the duodenum and the stomach becomes overly full, usually resulting in discomfort and vomiting. Following pancreatitis (inflammation of the pancreas), the posterior wall of the stomach may adhere to the part of the posterior wall of the omental bursa that covers Congenital Hypertrophic Pyloric Stenosis Congenital hypertrophic pyloric stenosis is a marked thickening of the smooth muscle (hypertrophy) in the pylorus that affects approximately 1 of every 150 male infants and 1 of every 750 female infants (Moore, Persaud, and Torchia, 2012). Proximally, the stomach may become secondarily dilated because of the pyloric stenosis (narrowing). Pyloric canal Pyloric stenosis Carcinoma of Stomach When the body or pyloric part of the stomach contains a malignant tumor, the mass may be palpable. The nodes along the splenic vessels can be excised by removing the spleen, gastrosplenic and splenorenal ligaments, and the body and tail of the pancreas. Involved nodes along the gastro-omental vessels can be removed by resecting the greater omentum; however, removal of the aortic and celiac nodes and those around the head of the pancreas is difficult. The bacteria erode the protective mucous lining of the stomach, inflaming the mucosa and making it vulnerable to the effects of the gastric acid and digestive enzymes (pepsin) produced by the stomach. In such cases, erosion of the splenic artery results in severe hemorrhage into the peritoneal cavity. Pain impulses from the stomach are carried by visceral afferent fibers that accompany sympathetic nerves. Partial gastrectomy (removal of part of the stomach) may be performed to remove a region of the stomach involved by a carcinoma, for example. Because the anastomoses of the arteries supplying the stomach provide good collateral circulation, one or more arteries may be ligated during this procedure without seriously affecting the blood supply to the part of the stomach remaining in place. When removing the pyloric antrum, for example, the greater omentum is incised parallel and inferior to the right gastro-omental artery, requiring ligation of all the omental branches of this artery. Partial gastrectomy to remove a carcinoma usually also requires removal of all involved regional lymph nodes. Posterior Anterior Celiac ganglion Vagal trunk Gastric Ulcers, Peptic Ulcers, Helicobacter pylori, and Vagotomy Gastric ulcers are open lesions of the mucosa of the stomach, whereas peptic ulcers are lesions of the mucosa of the pyloric canal or, more often, the duodenum. They often have gastric acid secretion rates that are markedly higher than normal between meals. Truncal (A), selective gastric (B), and selective proximal (C) vagotomy are shown. Visceral Referred Pain Pain is an unpleasant sensation associated with actual or potential tissue damage and mediated by specific nerve fibers to the brain, where its conscious appreciation may be modified. The brain interprets the pain as though the irritation occurred in the skin of the epigastric region, which is also supplied by the same sensory ganglia and spinal cord segments. Pain arising from the parietal peritoneum is of the somatic type and is usually severe. The anatomical basis for this localization of pain is that the parietal peritoneum is supplied by somatic sensory fibers through thoracic nerves, whereas a viscus such as the appendix is supplied by visceral afferent fibers in the lesser splanchnic nerve. Because the superior part of the duodenum closely relates to the liver, gallbladder, and pancreas, any of these structures may become adherent to the inflamed duodenum. Developmental Changes in Mesoduodenum During the early fetal period, the entire duodenum has a mesentery; however, most of it fuses with the posterior abdominal wall because of pressure from the overlying transverse colon. Place your hands on each side of the intestine and its mesentery and then follow the mesentery with your fingers to its root (its attachment to the posterior abdominal wall), untwisting the loop of intestine as necessary. Once the mesentery and intestine are straightened to match the direction of the root, the cranial end must be the orad end, and the caudal end the aborad end. If the ischemia is severe, necrosis (tissue death) of the involved segment results and ileus (obstruction of the intestine) of the paralytic type occurs. Brief Review of Embryological Rotation of Midgut An understanding of the rotation of the midgut clarifies the adult arrangement of the intestines. Pain arising from hindgut derivatives-the distal part of the transverse colon, descending colon, sigmoid colon, and rectum-localizes in the hypogastric region (see Table 2. It is attached to the umbilical vesicle (yolk sac) by the omphalo-enteric duct (yolk stalk). As the relative size of the liver and kidneys decreases, the midgut returns to the abdominal cavity as increased space becomes available. Although its mucosa is mostly ileal in type, it may also include areas of acid-producing gastric tissue, pancreatic tissue, or jejunal or colonic mucosa. An ileal diverticulum may become inflamed and produce pain mimicking that produced by appendicitis. Appendicitis Acute inflammation of the appendix, appendicitis, is a common cause of an acute abdomen (severe abdominal pain arising suddenly). Laparoscopic appendectomy has become a standard procedure selectively utilized for removing the appendix. One or two other small incisions ("portals") are required for surgical (instrument) access to the appendix and related vessels. When the cecum is high (subhepatic cecum), the appendix is in the right hypochondriac region (see Table 2. This condition, present in approximately 11% of individuals, may cause volvulus of the colon (L. In this anchoring procedure, a tenia coli of the cecum and proximal ascending colon is sutured to the abdominal wall. Appendicitis in young people is usually caused by hyperplasia of lymphatic follicles in the appendix that occludes the lumen. When secretions from the appendix cannot escape, the appendix swells, stretching the visceral peritoneum.
Schizonepeta tenuifolia (Schizonepeta). Mircette.
- Are there safety concerns?
- Dosing considerations for Schizonepeta.
- Eczema, common cold, fever, sore throat, psoriasis, heavy menstrual bleeding, and others conditions.
- What is Schizonepeta?
- How does Schizonepeta work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97048
Buy generic mircette on-line
However birth control zanesville ohio best 15 mcg mircette, their thickness relative to the size of the bodies they connect is most clearly related to the range of movement, and relative thickness is greatest in the cervical and lumbar regions. The uncovertebral "joints" are frequent sites of bone spur formation in later years, which may cause neck pain. The ligament extends longitudinally from the pelvic surface of the sacrum to the anterior tubercle of vertebra C1 and the occipital bone anterior to the foramen magnum are the superiormost parts, the anterior atlanto-axial and atlantooccipital ligaments. This ligament prevents hyperextension of the vertebral column, maintaining stability of the joints between the vertebral bodies. The posterior longitudinal ligament runs within the vertebral canal along the posterior aspect of the vertebral bodies. This ligament weakly resists hyperflexion of the vertebral column and helps prevent or redirect posterior herniation of the nucleus pulposus. As these nerves pass postero-inferiorly, they lie in grooves on the posterior surfaces of the medial parts of the transverse processes. These articulations are plane synovial joints between the superior and inferior articular processes (G. The joint capsule is attached to the margins of the articular surfaces of the articular processes of adjacent vertebrae. Accessory ligaments unite the laminae, transverse processes, and spinous processes and help stabilize the joints. The zygapophysial joints permit gliding movements between the articular processes; the shape and disposition of the articu- the laminae of adjacent vertebral arches are joined by broad, pale yellow bands of elastic tissue called the ligamenta flava (L. The flaval ligaments bind the lamina of the adjoining vertebrae together, forming alternating sections of the posterior wall of the vertebral canal. The ligamenta flava are long, thin, and broad in the cervical region, thicker in the thoracic region, and thickest in the lumbar region. Unlike the interspinous and supraspinous ligaments, the strong, broad nuchal ligament (L. The pedicles of the superior two vertebrae have been sawn through and the vertebral arches removed to reveal the posterior longitudinal ligament. Intertransverse, supraspinous, and interspinous ligaments are demonstrated in association with the vertebrae with intact vertebral arches. The medial branch gives rise to articular branches that are distributed to the zygapophysial joint at that level, and to the joint one level inferior to its exit. Thus, each zygapophysial joint receives articular rami from the medial branch of the posterior rami of two adjacent spinal nerves. The medial branches of both posterior rami have to be ablated to denervate a zygapophysial joint. Their design gives a wider range of movement than in the rest of the vertebral column. These joints permit nodding of the head, such as the flexion and extension of the head occurring when indicating approval (the "yes" movement). They are synovial joints of the condyloid type and have thin, loose joint capsules. The anterior membranes are composed of broad, densely woven fibers (especially centrally where they are continuous with the anterior longitudinal ligament). The atlanto-occipital membranes help prevent excessive movement of the atlanto-occipital joints. The articulated atlas and axis showing that the median atlanto-axial joint is formed as the anterior arch and transverse ligament of the atlas form a socket for the dens of the axis. Only the thicker, most anterior part of the anterior longitudinal ligament is included here to demonstrate its superior continuation as the anterior atlanto-axial membrane and anterior atlanto-occipital membrane. The posterior atlanto-occipital and atlanto-axial membranes span the gaps between the posterior arch of the atlas (C1) and the occipital bone (posterior margin of the foramen magnum) superiorly, and the laminae of the axis (C2) inferiorly. The vertebral arteries penetrate the atlanto-occipital membrane before traversing the foramen magnum. It runs superiorly from the body of C2 through the foramen magnum to attach to the central part of the floor of the cranial cavity, formed by the internal surface of the occipital bone. The sagittally oriented joint planes of the lumbar region are conducive to flexion and extension. Relative stability is also conferred on this part of the vertebral column through its connection to the sternum by the ribs and costal cartilages. This rotation of the upper trunk, in combination with the rotation permitted in the cervical region and that at the atlanto-axial joints, enables the torsion of the axial skeleton that occurs as one looks back over the shoulder. Contortionists, who begin their training during early childhood, become capable of extraordinary movements. They are assisted by gravity and the action of the anterolateral abdominal muscles. Although movements between adjacent vertebrae are relatively small, especially in the thoracic region, the summation of all the small movements produces a considerable range of movement of the vertebral column as a whole. Movements of the vertebral column are freer in the cervical and lumbar regions than elsewhere. The thoracic and sacral kyphoses (singular = kyphosis) are concave anteriorly, whereas the cervical and lumbar lordoses (singular = lordosis) are concave posteriorly. Lateral flexion (to the right or left in a frontal plane) is shown, also occurring mostly in the cervical and lumbar regions. Rotation around a longitudinal axis, which occurs primarily at the craniovertebral joints (augmented by the cervical region) and the thoracic region, is shown. The primary curvatures are retained throughout life as a consequence of differences in height between the anterior and posterior parts of the vertebrae. The cervical lordosis becomes fully evident when an infant begins to raise (extend) the head while prone and to hold the head erect while sitting. The lumbar lordosis becomes apparent when toddlers begin to assume the upright posture, standing and walking. When sitting, especially in the absence of back support for long periods of time, one usually "cycles" between back flexion (slumping) and extension (sitting up straight) to minimize stiffness and fatigue. This allows alternation between the active support provided by the extensor muscles of the back and the passive resistance to flexion provided by ligaments. In the thoracic and lumbar regions, each vertebra is encircled on three sides by paired intercostal or lumbar arteries that arise from the aorta. They emerge from foramina on the surfaces of the vertebral bodies (mostly the posterior aspect) and drain into the anterior external and especially the anterior internal vertebral venous plexuses, which may form large longitudinal sinuses. Two to four of these fine meningeal branches arise on each side at all vertebral levels. Close to their origin, the meningeal branches receive communicating branches from the nearby gray rami communicantes. They also supply the periosteum and especially the anuli fibrosi and anterior longitudinal ligament. As the nucleus dehydrates, the two parts of the disc appear to merge as the distinction between them becomes increasingly diminished. Overt or marked disc narrowing, especially when it is greater than that of more superiorly located discs, suggests pathology, not normal aging (Bogduk, 2012). Furthermore, the water content of their nuclei pulposi is high (approaching 90%), giving them great turgor (fullness). Flexion of the vertebral column produces compression anteriorly and stretching or tension posteriorly, squeezing the nucleus pulposus further posteriorly toward the thinnest part of the anulus fibrosus. The localized back pain of a herniated disc, which is usually acute pain, results from pressure on the longitudinal ligaments and periphery of the anulus fibrosus and from local inflammation caused by chemical irritation by substances from the ruptured nucleus pulposus. Chronic pain resulting from compression of the spinal nerve roots by the herniated disc is usually referred pain, perceived as coming from the area (dermatome) supplied by that nerve. The clinical picture varies considerably, but pain of acute onset in the lower back is a common presenting symptom. Because muscle spasm is associated with low back pain, the lumbar region of the vertebral column becomes tense and increasingly cramped as relative ischemia occurs, causing painful movement. Bone spurs (osteophytes) developing around the zygapophysial joints or the posterolateral margins during aging may narrow the foramina even more, causing shooting pains down the lower limbs. Any maneuver that stretches the sciatic nerve, such as flexing the thigh with the knee extended (straight leg-raising test), may produce or exacerbate (but in some individuals relieves) sciatic pain. Often these fractures are unstable (do not reunite) because the transverse ligament of the atlas becomes interposed between fragments (Crockard et al. This type of fracture heals more readily because the fragments retain their blood supply.
Purchase mircette online pills
The skin over the major weight-bearing areas of the sole-the heel birth control for dogs order genuine mircette on-line, lateral margin, and ball of the foot-is thick. The subcutaneous tissue in the sole is more fibrous than in other areas of the foot. The thick, central part of the plantar fascia forms the strong plantar aponeurosis, longitudinally arranged bundles of dense fibrous connective tissue investing the central plantar muscles. The plantar fascia holds the parts of the foot together, helps protect the sole from injury, and helps to support the longitudinal arches of the foot. The plantar aponeurosis arises posteriorly from the calcaneus and functions like a superficial ligament. Distally, the longitudinal bundles of collagen fibers of the aponeurosis Muscles of Foot Of the 20 individual muscles of the foot, 14 are located on the plantar aspect, 2 are on the dorsal aspect, and 4 are intermediate in position. The deep plantar fascia consists of the thick plantar aponeurosis and the thinner medial and lateral plantar fascia. The bones and muscles of the foot are surrounded by the deep dorsal and plantar fascia. Rather than producing actual movement, they are most active in fixing the foot or in increasing the pressure applied against the ground by various aspects of the sole or toes to maintain balance. Despite individual actions, the primary function of the intrinsic muscles of the sole of the foot is to resist flattening or maintain the arch of the foot. The medial plantar nerve courses within the medial compartment of the sole between the 1st and 2nd muscle layers. These thin, broad muscles form a fleshy mass on the lateral part of the dorsum of the foot, anterior to the lateral malleolus. The 1st layer consists of the abductors of the large and small toes and the short flexor of the toes. Also demonstrated are the neurovascular structures that course in a plane between the 1st and 2nd layers. Note that the plantar arteries enter and run in the plane between the 1st and the 2nd layers, with the lateral plantar artery passing from medial to lateral. The deep branches of the artery then pass from lateral to medial between the 3rd and the 4th layers. The arteries of the midfoot and forefoot resemble those of the hand in that (1) arches on the two aspects give rise to metatarsal (metacarpal) arteries, which in turn give rise to digital arteries; (2) the dorsal arteries are exhausted before reaching the distal ends of the toes or digits, so the plantar (palmar) digital arteries send branches dorsally to supply the distal dorsal aspects of the digits, including the nail beds; and (3) perforating branches extend between the metatarsals (metacarpals) forming anastomoses between the arches of each side. In addition to supplying the skin and fascia on the anteromedial aspect of the leg, the saphenous nerve passes anterior to the medial malleolus to the dorsum of the foot, where it supplies articular branches to the ankle joint and continues to supply skin along the medial side of the foot as far anteriorly as the head of the 1st metatarsal. After supplying the muscles of the anterior compartment of the leg, the deep fibular nerve passes deep to the extensor retinaculum and supplies the intrinsic muscles on the dorsum of the foot (extensors digitorum and hallucis longus) and the tarsal and tarsometatarsal joints. When it finally emerges as a cutaneous nerve, it is so far distal in the foot that only a small area of skin remains available for innervation: the web of skin between and contiguous sides of the 1st and 2nd toes. These branches supply the skin of the medial three and a half digits (including the dorsal skin and nail beds of their distal phalanges), and the skin of the sole proximal to them. Compared to the other terminal branch of the tibial nerve, the medial plantar nerve supplies more skin area but fewer muscles. The superficial branch divides, in turn, into two plantar digital nerves (one common and one proper) that supply the skin of the plantar aspects of the lateral one and a half digits, the dorsal skin and nail beds of their distal phalanges, and skin of the sole proximal to them. The deep branch of the lateral plantar nerve courses with the plantar arterial arch between the 3rd and the 4th muscle layers. The superficial and deep branches of the lateral plantar nerve supply all muscles of the sole not supplied by the medial plantar nerve. Compared to the medial plantar nerve, the lateral plantar nerve supplies less skin area but more individual muscles. Its distribution to both skin and muscles of the foot is comparable to that of the ulnar nerve in the hand (Chapter 6). The medial and lateral plantar nerves also provide innervation to the plantar aspects of all the joints of the foot. In these people, the skin normally innervated by the sural nerve is supplied by the medial and lateral sural cutaneous branches. The course and destination of the dorsal artery and its major continuation, the deep plantar artery, are comparable to the radial artery of the hand, which completes a deep arterial arch in the palm. The 1st dorsal metatarsal artery divides into branches that supply both sides of the great toe and the medial side of the 2nd toe. The anterior tibial artery becomes the dorsalis pedis artery when it crosses the talocrural joint. Perforating veins begin the one-way shunting of blood from superficial to deep veins, a pattern essential to operation of the musculovenous pump, proximal to the ankle joint. Dorsal digital veins continue proximally as dorsal metatarsal veins, which also receive branches from plantar digital veins. For the main part, superficial veins from a plantar venous network either drain around the medial border of the foot to converge with the medial part of the dorsal venous arch and network to form a medial marginal vein, which becomes the great saphenous vein, or drain around the lateral margin to converge with the lateral part of the dorsal venous arch and network to form the lateral marginal vein, which becomes the small saphenous vein. Perforating veins from the great and small saphenous veins then continuously shunt blood deeply as they ascend to take advantage of the musculovenous pump. The medial plantar artery is the smaller terminal branch of the posterior tibial artery. It gives rise to a deep branch (or branches) that supplies mainly muscles of the great toe. The lateral plantar artery arches medially across the foot with the deep branch of the lateral plantar nerve to form the deep plantar arch, which is completed by union with the deep plantar artery, a branch of the dorsalis pedis artery. The deep veins take the form of interanastomosing paired veins accompanying all arteries internal the lymphatics of the foot begin in subcutaneous plexuses. The collecting vessels consist of superficial and deep lymphatic vessels that follow the superficial veins and major vascular bundles, respectively. The deep lymphatic vessels from the foot follow the main blood vessels: fibular, anterior and posterior tibial, popliteal, and femoral veins. Lymphatic vessels from them follow the femoral vessels, carrying lymph to the deep inguinal lymph nodes. The deep veins accompany the arteries and their branches; they anastomose frequently and have numerous valves. The main superficial veins drain into the deep veins as they ascend the limb by means of perforating veins so that muscular compression can propel blood toward the heart against the pull of gravity. The distal great saphenous vein is accompanied by the saphenous nerve, and the small saphenous vein is accompanied by the sural nerve and its medial root (medial sural cutaneous nerve). The fibularis longus tendon can be palpated as far as the cuboid, and then it disappears as it turns into the sole. With toes actively extended, the small fleshy belly of the extensor digitorum brevis may be seen and palpated anterior to the lateral malleolus. Superficial lymphatic vessels from the medial foot drain are joined by those from the anteromedial leg in draining to the superficial inguinal lymph nodes via lymphatics that accompany the great saphenous vein. It may result from running and high-impact aerobics, especially when inappropriate footwear is worn. Point tenderness is located at the proximal attachment of the aponeurosis to the medial tubercle of the calcaneus and on the medial surface of this bone. The pain increases with passive extension of the great toe and may be further exacerbated by dorsiflexion of the ankle and/or weightbearing. Usually a bursa develops at the end of the spur that may also become inflamed and tender. Infections of Foot Foot infections are common, especially in seasons, climates, and cultures where shoes are less commonly worn. When possible, the incision is made on the medial side of the foot, passing superior to the abductor hallucis to allow visualization of critical neurovascular structures, while avoiding production of a painful scar in a weightbearing area. Contusion and tearing of muscle fibers and associated blood vessels result in a hematoma (clotted extravasated blood), producing edema anteromedial to the lateral malleolus. Most people who have not seen this inflamed muscle assume they have a severely sprained ankle. Because of the variations in the level of formation of the sural nerve, the surgeon may have to make incisions in both legs, and then select the better specimen. Some healthy adults (and even children) have congenitally non-palpable dorsalis pedis pulses; the variation is usually bilateral. Plantar Reflex the plantar reflex (L4, L5, S1, and S2 nerve roots) is a myotatic (deep tendon) reflex that is routinely tested during neurologic examinations. The lateral aspect of the sole of the foot is stroked with a blunt object, such as a tongue depressor, beginning at the heel and crossing to the base of the great toe.
Order mircette cheap online
This glistening lubricated surface allows the heart (attached only by its afferent and efferent vessels and related reflections of serous membrane) the free movement required for its "wringing-out" motions during contraction birth control that goes in your arm buy mircette 15mcg low price. The left side of the heart (left heart) receives well-oxygenated (arterial) blood from the lungs through the pulmonary veins and pumps it into the aorta for distribution to the body. The heart sounds are produced by the snapping shut of the oneway valves that normally keep blood from flowing backward during contractions of the heart. Epicardium, a thin external layer (mesothelium) formed by the visceral layer of serous pericardium. The walls of the heart consist mostly of myocardium, especially in the ventricles. When the ventricles contract, they produce a wringing motion because of the double helical orientation of the cardiac muscle fibers (Torrent-Guasp et al. Continued sequential contraction of the inner (apical) spiral elongates the heart, followed by widening as the myocardium briefly relaxes, increasing the volume of the chambers to draw blood from the atria. The helical (double spiral) arrangement of the myocardium (modified from Torrent-Guasp et al. A band of nearly horizontal fibers forms an outer basal spiral (dark brown) that comprises the outer wall of the right ventricle (right segment; rs) and external layer of the outer wall of the left ventricle (left segment; ls). Thus the septum, like the outer wall of the left ventricle, is also double layered. The isolated fibrous skeleton is composed of four fibrous rings (or two rings and two "coronets"), each encircling a valve; two trigones; and the membranous portions of the interatrial, interventricular, and atrioventricular septa. The ventricles dominate this surface (two thirds right ventricle, one third left ventricle). Diaphragmatic (inferior) surface, formed mainly by the left ventricle and partly by the right ventricle; it is related mainly to the central tendon of the diaphragm. Left pulmonary surface, formed mainly by the left ventricle; it forms the cardiac impression in the left lung. The pulmonary trunk, approximately 5 cm long and 3 cm wide, is the arterial continuation of the right ventricle and divides into right and left pulmonary arteries. All of the venous structures entering the right atrium (superior and inferior vena cavae and coronary sinus) open into the sinus venarum. Full understanding of the features of the right atrium requires an awareness of the development of the heart; see the blue box "Embryology of the Right Atrium," p. The interior of the right ventricle has irregular muscular elevations (trabeculae carneae). A thick muscular ridge, the supraventricular crest, separates the ridged muscular wall of the inflow part of the chamber from the smooth wall of the conus arteriosus, or outflow part. Because the fibrous ring maintains the caliber of the orifice, the attached valve cusps contact each other in the same way with each heartbeat. The septal papillary muscle arises from the interventricular septum, and its tendinous cords attach to the anterior and septal cusps of the tricuspid valve. The right atrium contracts when the right ventricle is empty and relaxed; thus blood is forced through this orifice into the right ventricle, pushing the cusps of the tricuspid valve aside like curtains. The wall of this vein and four of its tributaries were incorporated into the wall of the left atrium, in the same way that the sinus venosus was incorporated into the right atrium. For parts A and B, the heart was incised vertically along its left border and then transversely across the superior part of its base, passing between the superior and the inferior left pulmonary veins. Because arterial pressure is much higher in the systemic than in the pulmonary circulation, the left ventricle performs more work than the right ventricle. The anterior surface of the left ventricle has been incised parallel to the interventricular groove, with the right margin of the incision retracted to the right, revealing an anterior view of the chamber. The left atrioventricular orifice and mitral valve are located posteriorly, and the aortic vestibule leads superiorly and to the right to the aortic valve. Immediately superior to each semilunar cusp, the walls of the origins of the pulmonary trunk and aorta are slightly dilated, forming a sinus. It is located posterior to the left side of the sternum at the level of the 3rd intercostal space. The endocardium and some subendocardial tissue located immediately external to the endocardium receive oxygen and nutrients by diffusion or microvasculature directly from the chambers of the heart. Like the pulmonary valve, the aortic valve has three semilunar cusps: right, posterior, and left. The coronary arteries, the first branches of the aorta, supply the myocardium and epicardium. The coronary arteries supply both the atria and the ventricles; however, the atrial branches are usually small and not readily apparent in the cadaveric heart. Variations in the branching patterns and distribution of the coronary arteries are common. The branches of the coronary arteries are generally considered to be functional end arteries (arteries that supply regions of the myocardium lacking sufficient anastomoses from other large branches to maintain viability of the tissue should occlusion occur). Several small anterior cardiac veins begin over the anterior surface of the right ventricle, cross over the coronary sulcus, and usually end directly in the right atrium; sometimes they enter the small cardiac vein. Although called veins, they are valveless communications with the capillary beds of the myocardium and may carry blood from the heart chambers to the myocardium. Lymphatic vessels in the myocardium and subendocardial connective tissue pass to the subepicardial lymphatic plexus. Vessels from this plexus pass to the coronary sulcus and follow the coronary arteries. The potential for development of collateral circulation probably exists in most if not all hearts. The coronary sinus, the main vein of the heart, is a wide venous channel that runs from left to right in the posterior part of the coronary sulcus. The left posterior ventricular vein and left marginal vein also open into the coronary sinus. In the ordinary sequence of events in the cardiac cycle, the atrium and ventricle work together as one pump. The conducting system consists of nodal tissue that initiates the heartbeat and coordinates contractions of the four heart chambers, and highly specialized conducting fibers for conducting them rapidly to the different areas of the heart. The impulses are then propagated by the cardiac striated muscle cells so that the chamber walls contract simultaneously. Direct adrenergic stimulation from the sympathetic nerve fibers, as well as indirect suprarenal (adrenal) hormone stimulation, increases atrial and ventricular contractility. Most adrenergic receptors on coronary blood vessels are b2-receptors, which, when activated, cause relaxation (or perhaps inhibition) of vascular smooth muscle and, therefore, dilation of the arteries (Wilson-Pauwels et al. Parasympathetic stimulation slows the heart rate, reduces the force of the contraction, and constricts the coronary arteries, saving energy between periods of increased demand. This nerve network is most commonly described as lying on the anterior surface of the bifurcation of the trachea (a respiratory structure), since it is most commonly observed in dissection after removal of the ascending aorta and the bifurcation of the pulmonary trunk. The cardiac plexus is formed of both sympathetic and parasympathetic fibers en route to the heart, as well as visceral afferent fibers conveying reflexive and nociceptive fibers from the heart. Using this technique, intracardiac pressures can be recorded and blood samples may be removed. If a radiopaque contrast medium is injected, it can be followed through the heart and great vessels using serially exposed X-ray films.
Buy mircette on line
For example birth control pills kaiser cost discount mircette 15 mcg with visa, published data suggest that transfusion may increase cancer recurrence and/or metastasis, presumably due to decreased antitumor immunity. In each of these situations, an equally large number of reports show no statistically significant effects. However, humoral and cellular immunity represent distinct response pathways, which can be mutually antagonistic. In this way, enhanced antibody responses and cellular immunosuppression may simultaneously occur. Much of the animals data suffers the same problem; in particular, that the effects being observed may or may not be due to alterations in immunity (which is not itself tested). Thus, while secondary outcomes of transfusion may be real and reproducible, considerable scrutiny must be applied to determine whether the mechanism of such outcomes is due to effects on the immune system. Transfusion of red blood cells after prolonged storage produces harmful effects that are mediated by iron and inflammation. Patients with transfusion-requiring anemias may accumulate close to 10 g of iron each year. Hepcidin is the central regulator of systemic iron homeostasis and is insufficiently elevated in states of primary and secondary iron overload, thought to either cause or compound the degree of iron overload, respectively. The clinical manifestations, diagnosis, and management of iron overload are discussed below. The supply of iron to erythroid precursors in the bone marrow and to other tissues is largely maintained by daily recycling of iron from senescent erythrocytes. Iron absorption is tightly regulated to maintain iron balance because no physiological mechanism exists for iron elimination in humans and other animals. Pathophysiology: Due to this limitation in iron excretion, patients with transfusion-requiring anemias are subject to a significant iron load, often leading to parenchymal iron deposition and overload. Furthermore, diseases associated with iron overload in the absence of transfusion. It is known that hepcidin is regulated by iron, hypoxia, inflammation, and erythropoiesis. Primary iron overload diseases are associated with insufficient hepcidin, which leads to inappropriately high iron absorption. How tissue iron accumulates and results in toxicity has not been clearly delineated. Normally, iron circulates bound to transferrin (which is highly iron saturated in iron-overloaded patients) or ferritin (whose plasma levels generally reflect iron stores but also increase in chronic inflammatory states). Thus, excess iron leads to the generation of reactive oxygen species which have the potential to oxidize lipids, proteins, and nucleic acid, resulting in tissue damage in multiple organs. Since then, with the institution of iron chelation therapy, patients have a prolonged survival and a delayed onset of cardiac iron overload. Diagnosis: the diagnosis of iron overload requires clinical correlation of the signs and symptoms noted above with an estimation of total body iron accumulation/ stores. Estimating total body iron stores is imprecise and can be accomplished via direct and indirect methods. Direct measurements can be accomplished by liver biopsy with increased accuracy albeit as a consequence of an invasive procedure not without risk. Iron chelating agents directly bind iron, and the iron:chelator complex is excreted in the urine or feces. In most cases, compliance with iron chelation therapy significantly Iron Overload 451 reduces the complications of iron overload and leads to an improved quality of life. These different chelating agents exhibit differences in organ specific efficacy and their varying side effect profiles require different patient follow-up recommendations. Combination therapy or switching between chelators may be required in cases of inadequate response to individual chelators. Exchange transfusion may be used instead of simple transfusion which reduces the overall transfused iron burden (see Chapters 50 and 74). The changing role of liver biopsy in diagnosis and management of haemochromatosis. Iron overload in thalassemia and related conditions: therapeutic goals and assessment of response to chelation therapies. Examples of the broad spectrum of infections of current interest in the transfusion medicine community are found in Table 71. Septic transfusion reactions as a result of bacterial contamination, particularly of platelet products, are discussed in Chapter 65. These combined strategies result in much lower donor prevalences and incidences of transfusion transmissible pathogens than in the general population (Table 71. Thirty to 50% of infected persons aged 5 years will have signs and symptoms clinically suggestive of hepatitis, and 0. Approximately 25% of those chronically infected during childhood and 15% of those who become chronically infected later die prematurely from cirrhosis or liver cancer, but most remain asymptomatic until the onset of end-stage liver disease. Current residual risk estimates are 1:750,000 or less in an era of universal immunization. Hepatocellular carcinoma develops in cirrhotics an average of 30 years following infection. The solvent-detergent process used to make pathogen-reduced plasma fails to inactivate this nonenveloped virus and transmission has occurred, subsequently donor nucleic acid testing for source plasma has been implemented, and it is recommended that recipients of plasma derivatives be vaccinated. While usually self-limited, it can be lethal in pregnant women, their fetuses and patients with chronic liver disease. Transfusion transmission remains rare, but has been reported from endemic areas, and rarely in nonendemic regions, resulting from asymptomatic viremia. Subsequent transcription and translation of viral genes and processing of the proteins results in progeny viruses that bud from the plasma membrane and can infect other cells. This precautionary approach is underpinned by an unwillingness to accept the risk of a decrement in blood safety from known, unknown or unrecognized agents. Products stored for more than 7 days are less likely to transmit the viruses, as are those that have been leukoreduced. Incident infections are rare in repeat donors, an observation that has led to one-time testing of donors in some European countries. The residual risk of transfusion transmission is estimated to be 1:2,700,000 products transfused. This is age dependent, rising to over 90% in octogenarians and is also associated with race/ ethnicity and other socioeconomic and demographic correlates. These high rates mean that timely provision of components from seronegative donors for high-risk recipient populations can be challenging. Latency is established, and persists for life in cells of the monocyte/macrophage lineage, from which reactivation can occur. Transplacental infection after primary infection during pregnancy can result in fetal wastage, intrauterine growth retardation, deafness, mental retardation, blindness, and thrombocytopenic bleeding. Latently infected leukocytes are the primary vector of transfusion transmission and leukoreduction greatly decreases transmission. The expansion of routine leukoreduction has greatly decreased transfusion transmission, which is an argument for universal leukoreduction. Serological screening of blood donors is not done as the high population prevalence (90%) makes it impractical and donors with active infection (infectious mononucleosis) are usually symptomatic. The latter, and concern about transfusion transmission, are among reasons cited for maintenance of stringent deferrals of men having sex with other men.

Generic mircette 15 mcg on line
Because there is considerable variation from one side of the body to the other birth control kellymom cheap mircette 15 mcg on-line, each limb should be evaluated separately. The effects of muscle imbalance and presence of soft tissue contractures must be considered in the neurologic examination. Evaluation of the newborn should focus on determining which joints the child can control, and muscle strength can be assessed more accurately later. The lesion generally follows anatomic lines; thus, even in children with only mild involvement of the foot there may be significant weakness of the hip and the abductor muscles and increased tendency to late hip dislocation. If the hip has been dislocated early in fetal life (teratologic dislocation) and there are advanced adaptive changes of bone and soft tissue, reduction is not indicated. Contracted and/or spastic adductor muscles in conjunction with weak power of abductor muscles frequently lead to hip dislocation. If this imbalance is discovered early, intervention with physical therapy, bracing, or splinting can help prevent dislocation. Many patients have contracture of the iliotibial band, which maintains the hip flexed, abducted, and externally rotated. Early and intensive physical therapy should be instituted to avoid a fixed deformity. A major goal of treatment is the ability to extend the knee and take advantage of the normal locking mechanism. Congenital kyphosis is unique to myelodysplasia and is of such magnitude that it can be recognized at birth. The kyphosis usually involves the entire lumbar spine from the thoracolumbar junction down, including the sacrum, with its apex at L2 or L3; there is usually complete paralysis below the level of the lesion. In the newborn, the size of the cutaneous defect and the rigidity and magnitude of the curve may make skin closure extremely difficult. Cavovarus and equinovarus (clubfoot) should be corrected before the child learns to stand-before extensive adaptive and remodeling changes in both bone and soft tissue occur, making surgical intervention necessary. In the newborn period, calcaneovalgus with overpull of the anterior and paralysis of the posterior Although common in patients with myelodysplasia, spinal deformities are not usually a problem in the newborn period. However, congenital anomalies of the vertebrae occur in about 30% of affected children. Although the etiology is not certain, it has been noted that 14% to 18% of patients have mothers with diabetes or a strong family history of diabetes. Although partial sacral agenesis may not be noticeable, lumbar or complete sacral agenesis is a severe deformity. The posture of the lower limbs has been likened to that of the "sitting Buddha" and is characterized by flexion-abduction contractures of the hips and severe knee flexion, with popliteal webbing; the feet are in equinovarus and tucked under the buttocks. Inspection of the back reveals a bony prominence, which is the last vertebral segment, and often gross motion between this and the pelvis. Flexion-extension may occur at the junction of the spine and pelvis rather than at the hips. Scoliosis, hemivertebrae, spina bifida, and meningocele are common associated spinal anomalies. With low-level lesions, deformities of the foot and lower limb resemble those of resistant clubfoot or arthrogryposis. Children may be misdiagnosed for several years or until problems with toilet training call attention to the sacral anomalies. Although the clinical signs resemble those of arthrogryposis, patients with arthrogryposis have full sensation in the lower limbs, bowel and bladder control, and normal vertebral architecture. Motor paralysis is profound, with no voluntary or reflex activity, and it corresponds anatomically within one level to what might be expected from the vertebral loss. Even patients with the most severe involvement have sensation to the knees and spotty hypesthesia distally. Trophic ulceration of the feet is quite uncommon, suggesting at least protective sensation. Bladder dysfunction is a consistent finding in all patients, even those with a relatively minor hemisacral defect, but the patterns of urinary function vary. Patients exhibit individual mixtures of upper and/or lower motor neuron disorders; perineal electromyography is necessary to obtain the correct diagnosis. Severe constipation with absence of the normal sensation of rectal distention is a common bowel abnormality. The visceral anomalies are usually confined to the anogenital region (imperforate anus is the most common) and urinary tract. A lesion at the level of the lumbar spine results in the complete absence of all vertebral development below it, including the sacrum and coccyx. However, lesions of the sacrum are less consistent; and in about one third of patients the defect occurs on one side only. In lumbar or complete sacral agenesis there is usually no bony connection of the spine to the pelvis. Treatment measures vary with the level of involvement; and the management plan, based on the following broad concepts, must be highly individualized. If the sacropelvic ring is intact, the spinopelvic junction is usually stable and the patient can walk with minimal or no brace support. Patients with significant deformities of only the feet and legs require Lumbosacral agenesis vigorous correction, begun at birth, including serial plaster casts in conjunction with stretching and exercises to position the feet plantigrade and the knees in extension. Because of the high incidence of associated defects that may lead to serious renal impairment, recognition and treatment of urinary abnormalities are an important part of management. Delay in diagnosis and treatment may lead to upper tract deterioration and severely limit therapeutic options. The principal ones are the greater and lesser saphenous veins, which arise in the venous radicles in the feet and toes. There are also plantar digital veins, which drain into the dorsal metatarsalveins. In the thigh, the vein inclines anteriorly and lateralward; in the femoral triangle, it turns deeply through the saphenous opening to empty into the femoralvein. Intheleg,thegreatersaphenousveinhas tributaries from the heel of the foot, the front of the leg,andthecalf. Just before it turns through the saphenous opening, it receives the superficial external pudendal, superficial epigastric, and superficial circumflex iliac veins. They usually arise from the femoral nerve in the femoral triangle on the lateral surface of the femoral artery. Thisisdistributedto the skin of the distal third of the thigh on its medial surface. An infrapatellar branch curves downward below the patella, forming the patellar plexus with terminals of the medial and lateral femoral cutaneous nerves. The saphenous nerve continues distally along the medial surface of the leg, distributing from there and finally reaching the posterior half of the dorsum and the medialsideofthefoot. Thelateral sural cutaneous nerve(L5;S1,2)arisesin the popliteal space from the common peroneal nerve. Asthelateral dorsal cutaneous nerve of the foot, it is cutaneous to the lateral side of the foot, having previously given off lateral calcaneal branches to the ankle and heel. Thesuperficial peroneal nerve(L4,5;S1),abranchof the common peroneal nerve, descends to the distal third of the leg, where it almost immediately divides intotwoterminalbranches. It terminates in dorsal digital branches for the adjacent sides of the third and fourth and fourth and fifthtoes. Theterminal segment of the toes is supplied by dorsal terminals of theplantarnerves. Themedial plantar nerve(L4,5)providesaproper digital nerve to the medial side of the great toe and three common digital branches. Blood passes from superficial to deep through these communications, with valves in the communications determining the direction of drainage. It communicates with radicles of the greater saphenous veinandalso with deepveins of theleg. Itfrequently gives rise to a radicle, which communicates with the accessorysaphenousvein.
