
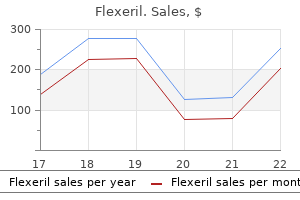
Flexeril 15 mg sale
The condition is usually reversible after discontinuation of the gold injections medicine 2355 discount flexeril 15mg with amex, but corticosteroids may be required to reverse the process. Although this pulmonary reaction is rare, it must not be confused with rheumatoid lung disease. Drug-induced chronic fibrotic reactions are probably nonimmunologic in nature, but their exact mechanism is unknown. Cytotoxic chemotherapeutic agents (azathioprine, bleomycin sulfate, busulfan, chlorambucil, cyclophosphamide, hydroxyurea, melphalan, mitomycin, nitrosoureas, and procarbazine hydrochloride) may induce pulmonary disease that is manifested clinically by the development of fever, nonproductive cough, and progressive dyspnea of gradual onset after treatment for 2 to 6 months or, rarely, years (233). It is essential to recognize this complication because such reactions may be fatal and could mimic other diseases, such as opportunistic infections. The chest radiograph reveals an interstitial or intra-alveolar pattern, especially at the lung bases. A decline in carbon monoxide diffusing capacity may even precede chest radiograph changes. Mononuclear cell infiltration of the interstitium may be seen early, followed by interstitial and alveolar fibrosis, which may progress to honeycombing. Even those who respond to treatment may be left with clinically significant pulmonary function abnormalities. Although an immunologic mechanism has been suspected in some cases (234), it is now generally believed that these drugs induce the formation of toxic oxygen radicals that produce lung injury. Noncardiogenic Pulmonary Edema Another acute pulmonary reaction without eosinophilia is drug-induced noncardiogenic pulmonary edema. Most of the drugs associated with this reaction are illegal, including cocaine, heroin, and methadone (235,236). Salicylate-induced noncardiogenic pulmonary edema may occur when the blood salicylate level is over 40 mg/dL (237). Hematologic Manifestations Many instances of drug-induced thrombocytopenia and hemolytic anemia have been unequivocally shown by in vitro methods to be mediated by immunologic mechanisms. The onset is usually abrupt, and recovery is expected within 1 to 2 weeks after drug withdrawal. Eosinophilia Eosinophilia may be present as the sole manifestation of drug hypersensitivity (240). Its recognition is useful because it may give early warning of hypersensitivity reactions that could produce permanent tissue damage or even death. However, most would agree that eosinophilia alone is not sufficient reason to discontinue treatment. In fact, some drugs, such as digitalis, may regularly produce eosinophilia, yet hypersensitivity reactions to this drug are rare. Drugs that may be associated with eosinophilia in the absence of clinical disease include gold salts, allopurinol, aminosalicylic acid, ampicillin, tricyclic antidepressants, capreomycin sulfate, carbamazepine, digitalis, phenytoin, 713 sulfonamides, vancomycin, and streptomycin. There does not appear to be a common chemical or pharmacologic feature of these agents to account for the development of eosinophilia. Drug-induced eosinophilia does not appear to progress to a chronic eosinophilia or hypereosinophilic syndrome. However, in the face of a rising eosinophil count, discontinuing the drug may prevent further problems. Thrombocytopenia Thrombocytopenia is a well-recognized complication of drug therapy. The usual clinical manifestations are widespread petechiae and ecchymoses and occasionally gastrointestinal bleeding, hemoptysis, hematuria, and vaginal bleeding. Bone marrow examination shows normal or increased numbers of normal-appearing megakaryocytes. With the exception of gold-induced immune thrombocytopenia, which may continue for months because of the persistence of the antigen in the reticuloendothelial system, prompt recovery within 2 weeks is expected on withdrawal of the drug (242). Readministration of the drug, even in minute doses, may produce an abrupt recrudescence of severe thrombocytopenia, often within a few hours. Although many drugs have been reported to cause immune thrombocytopenia, the most common offenders in clinical practice today are quinidine, the sulfonamides (antibacterials, sulfonylureas, and thiazide diuretics), gold salts, and heparin. The mechanism of drug-induced immune thrombocytopenia is thought to be the "innocent bystander" type. Some studies indicate that quinidine antibodies react with a platelet membrane glycoprotein in association with the drug (244). Because heparin has had more widespread clinical use, the incidence of heparin-induced thrombocytopenia is about 5% (245). A heparin714 dependent IgG antibody has been demonstrated in the serum of these patients. A low-molecular-weight heparinoid can be substituted for heparin in patients who previously developed heparin-induced thrombocytopenia (246). The diagnosis is often presumptive because the platelet count usually returns to normal within 2 weeks (longer if the drug is slowly excreted) after the drug is discontinued. Many in vitro tests are available at some centers to demonstrate drug-related platelet antibodies. A test dose of the offending drug is probably the most reliable means of diagnosis, but this involves significant risk and is seldom justified. Treatment involves stopping the suspected drug and observing the patient carefully over the next few weeks. Corticosteroids do not shorten the duration of thrombocytopenia but may hasten recovery because of their capillary protective effect. Platelet transfusions should not be given because transfused platelets are destroyed rapidly and may produce additional symptoms. Hemolytic Anemia Drug-induced immune hemolytic anemia may develop through three mechanisms: (1) immune complex type, (2) hapten or drug adsorption type, and (3) autoimmune induction (108). Another mechanism involves nonimmunologic adsorption of protein to the red blood cell membrane, which results in a positive Coombs test but seldom causes a hemolytic anemia. Hemolytic anemia after drug administration accounts for about 16% to 18% of acquired hemolytic anemias. The immune complex mechanism accounts for most cases of drug-induced immune hemolysis. The antidrug antibody binds to a complex of drug and a specific blood group antigen, for example, Kidd, Kell, Rh, or Ii, on the red blood cell membrane (247). Drugs implicated include quinidine, chlorpropamide, nitrofurantoin, probenecid, rifampin, and streptomycin. The serum antidrug antibody is often IgM, and the direct Coombs test is usually positive. Penicillin is the prototype of a drug that induces a hemolytic anemia by the hapten or drug absorption mechanism (248). Penicillin normally binds to proteins on the red blood cell membrane, and among patients who develop antibodies to the drug hapten on the red blood cell, a hemolytic anemia may occur. Anemia usually develops after 1 week of therapy, more rapidly in patients with preexisting penicillin antibodies. The antidrug antibody 715 is IgG, and the red blood cells are removed by splenic sequestration independent of complement. About 3% of patients receiving high-dose penicillin therapy develop positive Coombs test results, but only some of these patients actually develop hemolytic anemia. The anemia usually abates promptly, but mild hemolysis may persist for several weeks. Other drugs occasionally associated with hemolysis by this mechanism include cisplatin and tetracycline. A positive Coombs test develops in 11% to 36% of patients, depending on drug dosage, after 3 to 6 months of treatment (249). Hemolysis usually subsides within 1 to 2 weeks after the drug is stopped, but the Coombs test may remain positive for up to 2 years. Because only a small number of patients actually develop hemolysis, a positive Coombs test alone is not sufficient reason to discontinue the medication. Several other drugs have induced autoimmune hemolytic disease, including levodopa, mefenamic acid, procainamide, and tolmetin.
Buy flexeril with paypal
The length of time from reexposure to the drug to the onset of symptoms is 30 minutes to 8 hours (mean medications requiring central line order flexeril, 2. The lesions usually resolve within 2 to 3 weeks after drug withdrawal, leaving transient desquamation and residual hyperpigmentation. Drugs most commonly implicated vary depending on the country, the availability of drugs, and their pattern of use (166,167). In addition, some authors believe the location of lesions may be specific to the drug (168). Treatment is usually not required after the offending drug has been withdrawn because most fixed drug eruptions are mild and not associated with significant symptoms. Corticosteroids may decrease the severity of the reaction without changing the course of the dermatitis (159). The pustules are subcorneal or intraepidermal and appear on an erythematous, edematous base, and most commonly involve the trunk, upper extremities, and main skinfolds such as the neck, axilla, and groin. It is selflimited, with skin eruptions occurring soon after the medication is first administered (less than 2 days), followed by superficial desquamation and 700 spontaneous resolution in less than 15 days (171). It is a relatively common condition in young adults 20 to 40 years of age and is often recurrent in nature. Typically, the lesions begin as red, edematous papules that may resemble urticaria. Some lesions may develop concentric zones of color change, producing the pathognomonic "target" or "iris" lesions. The rash usually resolves in 2 to 4 weeks, leaving some residual postinflammatory hyperpigmentation but no scarring or atrophy. The vermilion border of the lips becomes denuded and develops serosanguinous crusts, a typical feature of this syndrome. Serious ocular complications include the development of keratitis sicca, corneal erosions, uveitis, and even bulbar perforation. Mucous membrane involvement of the nares, anorectal junction, vulvovaginal region, and urethral meatus is less common. The epithelium of the tracheobronchial tree and esophagus may be involved, leading to stricture formation. The pathogenesis of this disorder is uncertain; however, the histopathologic features are similar to graft-versus-host disease and suggest an immune mechanism. Deposition of C3, IgM, and fibrin can be found in the upper dermal blood vessels (179). Upregulation of intercellular adhesion molecule 1, an adhesion molecule that facilitates recruitment of inflammatory cells, has been found in the epidermis of patients with erythema multiforme (180). Corticosteroids hastened recovery, produced no major side effects, and were associated with 100% survival and full recovery with no significant residual complications. Generalized Exfoliative Dermatitis Exfoliative dermatitis is a serious and potentially life-threatening skin disease characterized by erythema and extensive scaling in which the superficial skin is shed over virtually the entire body. Fever, chills, and malaise are often prominent, and there is a large extrarenal fluid loss. Secondary infection frequently develops, and on occasion, a glomerulonephritis has developed. Laboratory tests and skin biopsy are helpful only to exclude other causes, such as psoriasis or cutaneous lymphoma. High-dose systemic corticosteroids and careful attention to fluid and electrolyte replacement are essential. Exfoliative dermatitis may occur as a complication of preexisting skin disorders. The drug-induced eruption may appear abruptly or may follow an apparently benign, drug-induced exanthematous eruption. The process may continue for weeks or months after withdrawal of the offending drug. Many drugs have been implicated in the development of exfoliative dermatitis, but the most frequently encountered are sulfonamides, penicillins, barbiturates, carbamazepine, phenytoin, phenylbutazone, allopurinol, and gold salts (193). The diagnosis is based on clinical grounds, the presence of erythema followed by scaling, and drug use compatible with this cutaneous reaction. The outcome is usually favorable if the causative agent is identified and then discontinued and 703 corticosteroids are initiated. However, an older study reported a 40% mortality rate, reminding us of the potential seriousness of this disorder (194). Photosensitivity Photosensitivity reactions are produced by the interaction of a drug present in the skin and light energy. Although direct sunlight (ultraviolet spectrum 2,800 to 4,500 nm or 280 to 450 mm) is usually required, filtered or artificial light may produce reactions. African Americans have a lower incidence of drug photosensitivity, presumably because of greater melanin protection. The eruption is limited to light-exposed areas, such as the face, the V area of the neck, the forearms, and the dorsa of the hands. Often, a triangular area on the neck is spared because of shielding by the mandible. Although symmetric involvement is usual, unilateral distribution may result from activities such as keeping an arm out of the window while driving a car. Photosensitivity may occur as a phototoxic nonimmunologic phenomenon and, less frequently, as a photoallergic immunologic reaction. Phototoxic reactions are nonimmunologic, occurring in a significant number of patients on first exposure when adequate light and drug concentrations are present. The drug absorbs light, and this oxidative energy is transferred to tissues, resulting in damage. Clinically, the reaction resembles an exaggerated sunburn developing within a few hours after exposure. Most phototoxic reactions are prevented if the light is filtered through ordinary window glass. Tetracycline, fluoroquinolones, and amiodarone are some of the many agents implicated in phototoxic reactions (195). Photoallergic reactions, in contrast, generally start with an eczematous phase and more closely resemble contact dermatitis. Such reactions occur in only a small number of patients exposed to the drug and light. The concentration of drug required to elicit the reaction can be very small, and there is cross-reactivity with immunochemically related substances. Flare-ups may occur at lightly covered or unexposed areas and at distant, previously exposed sites. The reaction may recur over a period of days or months 704 after light exposure, even without further drug administration. As a rule, longer ultraviolet light waves are involved, and window glass does not protect against a reaction. The photoallergic reaction may be detected by a positive photopatch test, which involves application of the suspected drug as an ordinary patch test for 24 hours, followed by exposure to a light source. Purpuric Eruptions Purpuric eruptions may occur as the sole expression of drug allergy, or they may be associated with other severe eruptions, notably erythema multiforme. Phenylbutazone has produced both thrombocytopenic and nonthrombocytopenic purpuras. The typical eruption is symmetric and appears around the feet and ankles or on the lower part of the legs, with subsequent spread upward. The eruption is composed of small, welldefined macules or patches of a reddish brown color. With time, the dermatitis turns brown or grayish brown, and pigmentation may persist for a relatively long period.
Diseases
- Central type neurofibromatosis
- Chromosome 12, 12p trisomy
- Hypergonadotropic ovarian failure, familial or sporadic
- Herpesvirus simiae B virus
- Craniofaciocardioskeletal syndrome
- Pulmonary surfactant protein B, deficiency of
- Adrenocortical carcinoma
- Basilar impression primary
- Osteochondrodysplasia thrombocytopenia hydrocephalus
- Blepharitis
Buy generic flexeril 15mg line
Malignant cardiac arrhythmias have been known to occur with overdoses medications 4 less canada flexeril 15 mg for sale, emphasizing the need to act expeditiously to counteract the toxic effect of these agents (13,65). Caution should be exercised using antihistamines in elderly patients or in those with liver dysfunction because of their slower clearance rates and increased susceptibility to overdose (13). Polypharmacy (comedication with five or more drugs) is a serious risk factor in the elderly, with strong anticholinergic antihistamines being a common cause of adverse drug events. Because first-generation H1-antihistamines are secreted in breast milk, caution should be exercised using these agents in lactating women (56,65). Patients taking rupatadine should be made aware that its blood levels are increased by grapefruit juice, whereas those taking fexofenadine advised that blood levels are reduced by grapefruit and orange juice (47). Sedation and other side effects associated with first-generation agents have been noted to occur, but generally at a rate similar to placebo (13). No longer available in the United States, terfenadine and astemizole were very occasionally associated with torsades de points. Newer second-generation antihistamines, such as fexofenadine and loratadine, have not been reported to cause cardiotoxicity (7). Cetirizine is considered a low-sedating antihistamine but is generally well tolerated by most patients, especially if dosed at bedtime. The newer second-generation antihistamines, desloratadine and levocetirizine, have thus far been demonstrated to be very safe and well tolerated. Rarer adverse effects of antihistamines include palpitation, arrhythmias, extrapyramidal symptoms, disturbed sleep, depression, convulsions, tremor, liver dysfunction, 1554 blood disorders, angle-closure glaucoma, and hypersensitivity reactions, such as anaphylaxis, angioedema, bronchospasm, photosensitivity, and other rashes (27). This phenomenon has been speculated to occur because of autoinduction of hepatic metabolism, resulting in an accelerated clearance rate of the antihistamine. However, studies have failed to confirm this hypothesis, and most reports of tolerance to antihistamines are now believed to be secondary to patient noncompliance because of intolerable drug side effects or breakthrough symptoms owing to severity of disease (2). Short-term studies evaluating tolerance to second-generation agents have found no change in their therapeutic efficacy after 6 to 8 weeks of regular use (2,13). Studies up to 12 weeks found no evidence that second-generation agents cause autoinduction of hepatic metabolism, leading to rapid excretion rates and drug tolerance. The clinical efficacy of these agents in the skin and treatment of allergic rhinitis does not decrease with chronic use (65). Tolerance of the sedative effects of antihistamines is more common than tachyphylaxis of their antihistaminic effects (27). The decongestants currently used in most preparations include phenylephrine hydrochloride or pseudoephedrine hydrochloride. These agents have saturated benzene rings without 3- or 4-hydroxyl groups, which is the reason for their weak -adrenergic effect, improved oral absorption, and duration of action. Pseudoephedrine, the most effective of the -adrenergic agonists, has been designated as a Schedule V over-the-counter drug product because of issues with individuals using this compound to manufacture methamphetamines; several studies have reported fewer visits to the emergency department for methamphetamine-related burn incidents caused by illicit lab fires since this law went into effect (68). Phenylephrine is a weaker adrenergic agonist available in many over-the-counter cough and cold formulations. Currently, questions remain regarding safety of these agents in 1555 children; in addition, their efficacy in clinical trials at the dose available in these preparations is unclear (69). These agents have a close structural resemblance to histamine, because most are simple modifications of the histamine molecule itself (71). H2-antagonists are weak bases with water-soluble hydrochloride salts and tend to be less lipophilic than H1-antagonists (7). Cimetidine was introduced to the United States in 1982 and has been proven safe and effective in the treatment of peptic ulcer disease (71). For example, ranitidine has a furan ring, whereas famotidine and nizatidine are composed of thiozole rings (71). H2-antagonists act primarily by competitive inhibition of the H2-receptors, with the exception of famotidine, which works noncompetitively (71). The four available agents all have potent H2-antagonistic properties; they vary in their pharmacokinetics and adverse effects, such as drug interactions. Numerous studies have been undertaken to examine the clinical utility of H2antagonists in allergic and immunologic diseases. Although several studies report these agents have promising immunologic changes in vitro, these findings have not been substantiated clinically (7,72). Generally, H2-antagonists have limited or no utility in treating allergen-induced and histamine-mediated diseases in man (72). One notable exception to this rule may be their use in combination with H1-antagonists in the treatment of chronic idiopathic urticaria although the evidence supporting this combination is low (46,73). H3-receptors also exist as receptors on nonhistaminergic neurons, regulating the release of neurotransmitters such as dopamine and noradrenaline. They both have demonstrated H3-receptor selectivity, but are available only for experimental use (12). There are some therapeutic agents available, such as betahistine, which act through the H3R and may be helpful in treating vertigo, although more rigorous research is necessary (75). Evidence is growing for the role of the H3R in cognitive function, sleep physiology, pain physiology, feeding behavior, and fear memory (76). It is of interest as a drug target for treating neurologic/neurodegenerative diseases such as Alzheimer and Parkinson diseases as well as other neuropsychiatric disorders such as drug addiction and Tourette syndrome (74). Ongoing clinical research suggests the efficacy of an H4R antagonist, which may be an available therapy in the near future for asthma and the pruritus of atopic dermatitis, which have been unresponsive to antihistamines targeting the H1R and H2R (77). In addition, the H4R antagonists may have a role in the eventual treatment of chronic inflammation, pain, itch, cancer, diabetes and related complications. Chemical modifications of these early agents have yielded the second-generation antihistamines, which are of equal antagonistic efficacy but with fewer side effects. Newer nonsedating antihistamines, which are metabolites or isomers of existing agents, are now under development. H2-receptor antagonists have been found extremely useful in the treatment of peptic ulcer disease. However, they have not proven to be very 1557 useful in the treatment of allergic and immunologic disorders in humans. Owing to better side effect profiles, newer, selective nonsedating H1-antagonists and dual-action antihistamines have provided therapeutic advantages over firstgeneration agents for long-term management of allergic diseases, including rhinitis, conjunctivitis, and urticaria. The role of histamine H1 and H4 receptors in allergic inflammation: the search for new antihistamines. Perspectives in drug development and clinical pharmacology: the discovery of histamine H1 and H2 antagonists. Histamine H4 receptor agonists have more activities than H4 agonism in antigen-specific human T-cell responses. Human basophil chemotaxis and activation are regulated via the histamine H4 receptor. In vitro pharmacology of clinically used central nervous system-active drugs as inverse H1 receptor agonists. Grapefruit juice alters the systemic bioavailability and cardiac repolarization of terfenadine in poor metabolizers of terfenadine. A double-blind, single-dose, crossover comparison of cetirizine, terfenadine, loratadine, astemizole, and 1559 chlorpheniramine versus placebo: suppressive effects on histamine-induced wheals and flares during 24 hours in normal subjects. Intracellular calcium release induced by histamine releasers and its inhibition by some antiallergic drugs. Azelastine hydrochloride: a review of pharmacology, pharmacokinetics, clinical efficacy and tolerability. Combined antagonism of leukotrienes and histamine produces predominant inhibition of allergeninduced early and late phase airway obstruction in asthmatics. Mast cell stabilization and antihistamine effects of olopatadine ophthalmic solution: a review of preclinical and clinical research. H1-antihistamines for chronic spontaneous urticaria: an abridged Cochrane Systematic Review. Repeated-dose effects of mequitazine, cetirizine and dexchlorpheniramine on driving and psychomotor performance. Antihistamines and related: H1 antagonists, sodium cromoglycate, leukotriene receptor antagonists. Handbook of Dermatology Treatments: A Practical Guide to Topical Treatments, Systemic Therapies and 1561 Procedural Dermatology. Effect of oral terfenadine on the bronchoconstrictor response to inhaled histamine and adenosine 5monophosphate in non-atopic asthma. An evidence-based review of the efficacy of antihistamines in relieving pruritus in atopic dermatitis. Fetal safety of drugs used in the treatment of allergic rhinitis: a critical review.
Buy cheap flexeril 15mg
Drugs and other agents involved in anaphylactic shock occurring during anaesthesia symptoms jaw pain and headache buy flexeril canada. A prospective study of the risk of an immediate adverse reaction to protamine sulfate during cardiopulmonary bypass surgery. IgE against ethylene oxidealtered human serum albumin in patients with anaphylactic reactions to dialysis. Plasma histamine but not anaphylatoxin levels correlate with generalized urticaria from infusions of anti-lymphocyte monoclonal antibodies. The incidence and management of infusion reactions to infliximab: a large center experience. Human serum sickness: a prospective analysis of 35 patients treated with equine anti-thymocyte globulin for bone marrow failure. Immunology of a serum sickness/vasculitis reaction secondary to streptokinase used for acute myocardial infarction. Serum sickness-like reactions to amoxicillin, cefaclor, cephalexin, and trimethoprim-sulfame-thoxazole. A prospective clinical and 746 immunologic analysis of patients with serum sickness. Etanercept-induced lupus erythematosus presenting as a unilateral pleural effusion. Complement system protein C4 and susceptibility to hydralazine-induced systemic lupus erythematosus. Antibodies to nuclear anti-gens in patients treated with procainamide or acetylprocainamide. Remission of procainamideinduced lupus erythematosus with N-acetylprocainamide therapy. Graft-versus-host reactions: clues to the etiopathology of a spectrum of immunological disease. The American College of Rheumatology 1990 criteria for the classification of vasculitis. A report from the Boston Collaborative Drug Surveillance Program on 15,438 consecutive inpatients, 1975 to 1982. Angio-oedema in relation to treatment with angiotensin converting enzyme inhibitors. Severe angioedema after long-term use of an angiotensin-converting enzyme inhibitor. Prevalence and relevance of allergic reactions in patients patch tested in North America-1984 to 1985. Clinical pattern of cutaneous drug eruption among children and adolescents in North India. Postcoital fixed drug eruption in a man sensitive to trimethoprim-sulphamethoxazole. The interaction between keratinocytes and T cells-an overview of the role of adhesion molecules and the characterization of epidermal T cells. Possible role of Fas/Fas ligand-mediated apoptosis in the pathogenesis of fixed drug eruption. Topical provocation in 31 cases of fixed drug eruption: change of causative drugs in 10 years. Acute generalized exanthematous pustulosis: pathogenesis, genetic background, clinical variants and therapy. Acute generalized exanthematous pustulosis: role of cytotoxic T cells in pustule formation. Erythema multiforme: a critical review of characteristics, diagnostic criteria, and causes. Cutaneous immunofluorescence study of erythema multiforme: correlation with light microscopic patterns and etiologic agents. Drug-induced, photosensitive, erythema multiforme-like eruption: possible role for cell adhesion molecules in a flare induced by Rhus dermatitis. Erythema multiforme: microvascular damage and infiltration of lymphocytes and basophils. Lymphocyte subsets and Langerhans cells/indeterminate cells in erythema multiforme. Adverse reactions during imatinib and lansoprazole treatment in gastrointestinal stromal tumors. Petechiae, ecchymoses, and necrosis of skin induced by coumarin congeners: rare, occasionally lethal complication of anticoagulant therapy. Toxic epidermal necrolysis treated with lowdose intravenous immunoglobulin: immunohistochemical study of Fas and Fas-ligand expression. Hypersensitivity to pancreatic extracts in parents of patients with cystic fibrosis. Dyspnoea, asthma, and bronchospasm in relation to treatment with angiotensin converting enzyme inhibitors. Low-dose amiodarone-induced pneumonitis: evidence of an immunologic pathogenetic mechanism. Fatal pulmonary failure complicating high-dose cytosine arabinoside therapy in acute leukemia. A Mechanism of cell destruction in individuals sensitized to foreign antigens and its implications in auto-immunity. Heparin-induced thrombocytopenia: studies with a new low molecular weight heparinoid, Org 10172. Current understanding of the mechanisms of idiosyncratic drug-induced agranulocytosis. Evidence for expression in human liver of halothane-induced neoantigens recognized by antibodies in sera from patients with halothane hepatitis. Enflurane metabolism produces covalently bound liver adducts recognized by antibodies from patients with halothane hepatitis. Acute interstitial nephritis with glomerulopathy due to nonsteroidal anti-inflammatory agents: a review of its clinical spectrum and effects of steroid therapy. Association of protamine IgE and IgG antibodies with life-threatening reactions to intravenous protamine. Sulfonamide-reactive lymphocytes detected at very low frequency in the peripheral blood of patients with drug-induced eruptions. A decade of penicillin related acute interstitial nephritis-more questions than answers. Toxic epidermal necrolysis and Stevens Johnson syndrome: our current understanding. Cross-reactivity between penicillins and cephalosporins: clinical and immunologic studies. Desensitization (induction of drug tolerance or drug provocation testing) to these immunoglobulin E (IgE)-mediated reactions renders mast cells specifically unresponsive to only the drug antigen used for desensitization. In many patients, successful desensitization is accompanied by a marked decrease or transient disappearance of the cutaneous wheal-and-flare response. Similar changes in skin test responses have been reported following successful desensitization to vancomycin (1), aminoglycosides (2), and carboplatin (3). Similar to acute desensitization for IgE-mediated reactions, these patients have had undeniable reactions to these drugs in the past.
Purchase discount flexeril online
Expiratory high-resolution computed tomography demonstrating bilateral focal air trapping (arrowheads) medicine cups flexeril 15 mg lowest price. It is characterized by a pattern of necrotizing granulomatous inflammation that destroys the walls of small bronchi and bronchioles (22). High-resolution computed tomography demonstrating extensive bilateral central bronchiectasis (arrows) and peripheral centrilobular nodules (arrowhead). Causative factors are numerous and include bacteria, fungi, avian proteins, wood dusts, and chemicals. Mosaic attenuation on inspiratory and air trapping on expiratory images are common. Highresolution computed tomography showing numerous centrilobular nodules (arrows). The radiologic and clinical findings resolved 5 days after initiating corticosteroid therapy. The radiographic differential diagnosis includes hydrostatic pulmonary edema, adult respiratory distress syndrome, and atypical viral or bacterial pneumonia. Computed tomography showing traction bronchiectasis (arrowhead) and honeycombing (arrows). High-resolution computed tomography showing peripheral small ground-glass opacities and centrilobular nodules in the upper lung zones (arrowheads). Chronic eosinophilic pneumonia is an idiopathic condition histologically characterized by filling of the airspaces with eosinophils and macrophages and associated mild interstitial pneumonia. The combination of peripheral unilateral or bilateral patchy consolidation and peripheral blood eosinophilia is virtually diagnostic for chronic eosinophilic pneumonia (29). High-resolution computed tomography demonstrating thickening of the interlobular septum (arrows) and ground-glass opacities (arrowheads). Cardiac involvement, including endocardial fibrosis and restrictive cardiomyopathy, is one of the major complications of this entity. Pulmonary involvement occurs in up to 40% of patients, and typically presents on radiography as interstitial, nonlobar opacities (26,30,31). The syndrome is most commonly seen in patients 30 to 50 years of age and has no gender predilection. Patients are typically asthmatic and present with eosinophilia, fever, and multisystem vasculitis. Findings of chest radiography are often abnormal, but nonspecific and most often consist of patchy nonsegmental areas of consolidation with no zonal predominance. The areas of consolidation may have 483 peripheral distribution and are often transient. A pleural effusion is present in approximately 30% of patients, usually due to cardiac involvement or eosinophilic pleuritis (32). Transverse thin-section computed tomography demonstrating extensive areas of airspace consolidation (arrows) and ground-glass attenuation (arrowhead) involving the periphery of the lungs. Computed tomography demonstrating irregular areas of consolidation (arrows) in a 57year-old woman with previous episodes of eosinophilic pneumonia. The ground-glass opacities and consolidation reflect the presence of chronic eosinophilic pneumonia (32). Numerous agents, including cytotoxic and noncytotoxic drugs, have the potential to cause pulmonary disturbances. The clinical and radiologic manifestation of these drugs generally reflects the underlying histopathologic processes. The prevalence of drug-induced pulmonary hypersensitivity or toxicity is increasing, and more than 100 drugs are now known to cause injury. The diagnosis of pulmonary drug hypersensitivity should be considered in any patient with drug therapy who presents with new progressive respiratory complaints. There is not a classic imaging finding, but it may mimic malignancy, presenting with pseudotumor. The accuracy of high-resolution computed tomography in diffuse infiltrative lung disease. Diffuse lung disease: pathologic basis for the high- resolution computed tomography findings. The secondary pulmonary lobule: a practical concept for interpretation of chest radiographs. Management of this disorder, which accounts for approximately 16 million patient visits per year, has changed dramatically in the past 50 years. This is due to new insights into the pathophysiology of sinusitis, advances in rhinoscopy (nasal endoscopy), improved radiographic imaging, and availability of antibiotics (1). Technical advances in endoscopic instrumentation have defined a new era in the office diagnosis and surgical management of sinusitis, permitting an unprecedented level of precision. Hirschman performed the first fiberoptic nasal examination using a modified cystoscope in 1901 (2). In the early 1950s, investigators at Johns Hopkins University designed a series of endoscopes with relatively small-diameter, wide-field, high-contrast optics, and adequately bright illumination. At this time Messerklinger of Graz began to use this technology for systematic nasal airway evaluation. He reported that primary inflammatory processes in the lateral nasal wall, particularly in the middle meatus, result in secondary disease in the maxillary and frontal sinuses (2). Messerklinger found that small anatomic variations or even minimal inflammatory activity in this area could result in significant disease of the adjacent sinuses as a result of impaired ventilation and drainage. With this observation, he used endoscopes to develop a surgical approach to relieve the obstruction in such a way that normal sinus physiology was preserved. This philosophy was markedly different from the ablative sinus procedures advocated in the past, such as Caldwell-Luc, in that cilia and sinus mucosal function were preserved. In contrast, the other sinuses exist as a single bony cavity on each side of the facial skeleton. The ethmoid and maxillary sinuses are present at birth and can be imaged in infancy. The frontal sinuses begin to develop anatomically by 12 months and can be evaluated radiographically at 4 to 6 years. Sphenoid sinuses begin to develop by the age of 3, but cannot be imaged until a child is 9 or 10 years of age. The point at which mucosal outpouching occurs persists as the sinus ostium, through which the sinus drains (3). Diagnostic rhinoscopy offers a wealth of information regarding the distribution of inflammatory foci within the sinonasal labyrinth and the associated anatomic variations that may impair physiologic sinus drainage. It is usually performed in an office setting with the aid of topical decongestants and topical anesthesia. It is essentially an extension of the physical examination that helps confirm the diagnosis, gain insight into the pathophysiologic factors at work, and guide medical or surgical therapy. The lateral nasal walls are each flanked by three turbinate bones, designated the superior, middle, and inferior turbinates. The region under each turbinate is known, respectively, as the superior, middle, and inferior meatus. This is an anatomically narrow space where, even minimal mucosal disease, can result in impairment of drainage from any of these sinuses. The sphenoid sinus drains into a region known as the sphenoethmoidal recess, which lies at the junction of the sphenoid and ethmoid bones in the posterior superior nasal cavity. The nasolacrimal duct courses anteriorly to the maxillary sinus ostium and drains into the inferior meatus. It is a T-shaped structure, of which the horizontal portion forms the cribriform plate of the skull base. The vertical part forms most of the lateral nasal wall and consists of the superior and middle turbinates, as well as the ethmoid sinus labyrinth. Within the middle meatus, a sickle-shaped projection of the ethmoid bone, known as the uncinate process, forms a boundary of a recess called the infundibulum, into which the maxillary sinus drains (4). A collection of anterior ethmoid air cells forms a bulla, which is suspended from the remainder of the ethmoid bone, and hangs just superiorly to the opening of the infundibulum into the meatus.
Buy flexeril
Carboplatin hypersensitivity: a 6-h 12-step protocol effective in 35 desensitizations in patients with 817 gynecologic malignancies and mast cell/IgE-mediated reactions treatment in spanish order generic flexeril on line. Joint Task Force on Practice Parameters; American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology. Hypersensitivity reactions to chemotherapy: outcomes and safety of rapid desensitization in 413 cases. Aspirin challenge and desensitization for aspirin-exacerbated respiratory disease: a practice paper. The relationship between historical aspirin-induced asthma and severity of asthma induced during oral aspirin challenges. Intravenous desensitization to allopurinol in a heart transplant patient with gout. Rapid desensitization for nonimmediate reactions in patients with cystic fibrosis. The incidence of antimicrobial allergies in hospitalized patients: implications regarding prescribing patterns and emerging bacterial resistance. Results of the National Institute of Allergy and Infectious Diseases collaborative clinical trial to test the predictive value of skin testing with major and minor penicillin derivatives in hospitalized adults. Incidence of allergic reactions associated with antibacterial use in a large, managed care organization. Nature and extent of penicillin sidereactions with particular reference to fatalities from anaphylactic shock. Brief communication: tolerability of meropenem in patients with IgE-mediated hypersensitivity to penicillins. An analysis of 51 episodes in two Dallas hospitals and 97 episodes reported in the English literature. Adverse drug reactions to a cephalosporins in hospitalized patients with a history of penicillin allergy. Risk of administering cephalosporin antibiotics to patients with histories of penicillin allergy. Adverse reactions associated with oral and parenteral use of cephalosporins: a retrospective population-based analysis. Amoxicillin-induced exanthema in patients with infectious mononucleosis: allergy or transient immunostimulation Serum sickness-like reactions to amoxicillin, cefaclor, cephalexin, and trimethoprim-sulfamethoxazole. Selection of treatment of cefaclorassociated urticarial, serum sickness-like reactions and erythema multiforme by emergency pediatricians: lack of a uniform standard of care. A report of near fatal ceftriaxone induced anaphylaxis in a child with review of literature. Anaphylactic shock associated with cefuroxime axetil: structure-activity relationships. Adverse drug reactions associated with ceftaroline use: a 2-center retrospective cohort. Immune-mediated and adverse drug reactions during treatment with the fifth generation cephalosporin, ceftaroline: drug allergy matters. Decrease of selective immunoglobulin E response to amoxicillin despite repeated administration of benzylpenicillin and penicillin V. Prevalence and characteristics of reported penicillin allergy in an urban outpatient adult population. Cross-reactivity between penicillins and cephalosporins: clinical and immunological studies. Safety and effectiveness of a preoperative allergy clinic in decreasing vancomycin use in patients with a history of penicillin allergy. Immediate allergic reactions to cephalosporins: evaluation of cross-reactivity with a panel of penicillins and cephalosporins. Cross-reactivity and tolerability of cephalosporins in patients with immediate hypersensitivity to penicillins. Is it safe to use carbapenems in patients with a history of allergy to penicillin Allergy test outcomes in patients selfreported as having penicillin allergy: two-year experience. Fatal and near-fatal anaphylaxis: factors that can worsen or contribute to fatal outcomes. Routine elective penicillin allergy skin testing in children and adolescents: study of sensitization. Incidence of resensitization after tolerating penicillin treatment in penicillin-allergic patients. Desensitization of patients allergic to penicillin using orally administered -lactam antibiotics. Acute and chronic desensitization of penicillin-allergic patients using oral penicillin. Long-term ticarcillin desensitization by the continuous oral administration of penicillin. Detection of human IgE to sulfamethoxazole by skin testing with sulfamethoxazoyl-poly-L-tyrosine. Diagnosis of sulfonamide hypersensitivity reactions by in vitro "rechallenge" with hydroxylamine metabolites. Desensitization to trimethoprimsulfamethoxazole in patients with acquired immunodeficiency syndrome and Pneumocystis carinii pneumonia. A 5-day course of oral desensitization to trimethoprim/sulfamethoxazole (T/S) is successful in patients with human immunodeficiency virus type-1 infection who were previously intolerant to T/S but had no sulfamethoxazole-specific IgE. Monitoring adverse drug reactions to sulfonamide antibiotics in human immunodeficiency virusinfected individuals. Indications for 5-aminosalicylate in inflammatory bowel disease: is the body of evidence complete Acute desensitization of a patient with cystic fibrosis allergic to both B-lactam and aminoglycoside antibiotics. Fluoroquinolone-associated anaphylaxis in spontaneous adverse drug reaction reports in Germany: differences in reporting rates between individual fluoroquinolones and occurrence after first-ever use. Drug provocation tests in patients with a history suggesting an immediate drug hypersensitivity reaction. Skin testing and drug challenge outcomes in antibiotic-allergic patients with immediate-type hypersensitivity. Apparent anaphylactoid reaction after treatment with a single dose of telithromycin. Amphotericin B: emergency challenge in a neutropenic, asthmatic patient with fungal sepsis. Amphotericin-induced stridor: a review of stridor, amphotericin preparations, and their immunoregulatory effects. Safety, tolerance and outcome of treatment with liposomal amphotericin B in paediatric patients with cancer or undergoing haematopoietic stem cell transplantation. Appearance of anaphylactic shock after long-term intravenous itraconazole treatment. Immediate cross-hypersensitivity between micafungin and caspofungin: a case report. Efficacy and safety of micafungin versus intravenous itraconazole as empirical antifungal therapy for febrile neutropenic patients with hematological malignancies: a randomized, controlled, prospective, multicenter study. Efavirenz severe hypersensitivity reaction: case report and rapid desensitization protocol development. Successful use of valciclovir in a case of recurrent urticaria associated with genital herpes.
Zibeth (Civet). Flexeril.
- Are there safety concerns?
- What is Civet?
- Pain relief and sleeplessness.
- Dosing considerations for Civet.
- How does Civet work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96707
Cheap flexeril 15 mg without a prescription
Fundamental principles of asthma management include (a) preventing death medications quiz buy cheap flexeril 15mg on line, disability, and school or work absenteeism/presenteeism, (b) trying to minimize or overcome the effects of airway remodeling and allergic inflammation, mast cell activation, smooth muscle contraction, and pulmonary physiologic abnormalities; and (c) using medications effectively and as safely as possible. It is expected that our treatment modalities will continue to improve and that more specific therapies, whether pharmacologic, allergen immunotherapy, immunologically targeted treatments or other innovative approaches, will be of help to patients. It is hoped that we can take advantage of pharmacogenomic patterns to provide optimal "personalized medicine" for patients with asthma and allergic-immunologic conditions. National Institutes of Health, National Heart, Lung, and Blood Institute, Expert Panel Report, National Asthma Education Program, Executive Summary. National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. Inflammatory subtypes in cough-variant asthma: Association with maintenance doses of inhaled corticosteroids. Evaluation of the left and right ventricular systolic and diastolic function in asthmatic children. In-hospital and long-term mortality in Takotsubo cardiomyopathy: a community hospital experience. Adolescents with asthma: consequences of transition from paediatric to adult healthcare. Results of a home-based environmental intervention among urban children with asthma. IgE anti-respiratory syncytial virus antibodies detected in serum of pediatric patients with asthma. Role of parainfluenza virusspecific IgE in pathogenesis of croup and wheezing subsequent to infection. The contributions of allergic sensitization and respiratory pathogens to asthma inception. Innate immune responses to rhinovirus are reduced by the high-affinity IgE receptor in allergic asthmatic children. Preseasonal treatment with either omalizumab or an inhaled corticosteroid boost to prevent fall asthma exacerbations. Infection with human rhinovirus 16 promotes enhanced IgE responsiveness in basophils of atopic asthmatics. Meta-analysis of the heritability of human traits based on fifty years of twin studies. The contribution of twin studies to the understanding of the aetiology of asthma and atopic diseases. The pivotal role of 5lipoxygenase products in the reaction of aspirin-sensitive asthmatic subjects to aspirin. The effect of aspirin desensitization on urinary leukotriene E4 concentrations in aspirin-sensitive asthma. Overexpression of leukotriene C4 synthase in bronchial biopsies from patients with aspirin-intolerant asthma. Spatio-temporal ozone variation in a case-crossover analysis of childhood asthma hospital visits in New York City. Increased ultrafine particles and carbon monoxide concentrations are associated with asthma exacerbation among urban children. Post-traumatic stress disorder, bronchodilator response, and incident asthma in World Trade Center rescue and recovery workers. Association between adverse childhood experiences in the home and pediatric asthma. In utero exposure to 25-hydroxyvitamin D and risk of childhood asthma, wheeze, and respiratory tract infections: a meta-analysis of birth cohort studies. Family history of asthma and atopy: in-depth analyses of the impact of asthma and wheeze in 7- and 81029 year old children. No evidence for effects of family environment on asthma: a retrospective study of Norwegian twins. Pulmonary effects of maternal smoking on the fetus and child: effects on lung development, respiratory morbidities, and life long lung health. A randomized trial of air cleaners and a health coach to improve indoor air quality for inner-city children with asthma and secondhand smoke exposure. Early-life determinants of asthma from birth to age 20 years: a German birth cohort study. Amish children living in northern Indiana have a very low prevalence of allergic sensitization. Not all farming environments protect against the development of asthma and wheeze in children. The eosinophilic leukocyte and the pathology of fatal bronchial asthma: evidence for pathologic heterogeneity. Airway responsiveness to mannitol in asthma is associated with chymase-positive mast cells and eosinophilic airway inflammation. Association between neutrophilic airway inflammation and airflow limitation in adults with asthma. Markers of vascular perturbation correlate with airway structural change in asthma. A morphologic study of the airway structure abnormalities in patients with asthma by high-resolution computed tomography. Triggering the induction of myofibroblast and fibrogenesis by airway epithelial shedding. Functional characteristics of bronchial epithelium obtained by brushing from asthmatic and normal subjects. Apoptosis, proliferation, and expression of Bcl-2, Fas, and Fas ligand in bronchial biopsies from asthmatics. Airway hyperresponsiveness in asthma: mechanisms, clinical significance, and treatment. Associations between asthma history, atopy and non-specific bronchial responsiveness in young adults. Elevated levels of eosinophil granule major basic protein in the sputum of patients with bronchial 1032 asthma. Elevated substance P content in induced sputum from patients with asthma and patients with chronic bronchitis. Neurokinin A is the predominant tachykinin in human bronchoalveolar lavage fluid in normal and asthmatic subjects. Management of asthma based on exhaled nitric oxide in addition to guideline-based treatment for innercity adolescents and young adults: a randomized controlled trial. Increased 8-isoprostane, a marker of oxidative stress, in exhaled condensate of asthma patients. Relationship between exhaled leukotriene and 8-isoprostane levels and asthma severity, asthma control 1033 level, and asthma control test score. Pharmacogenetics of the 5lipoxygenase biosynthetic pathway and variable clinical response to montelukast. Corticosteroid-resistant asthma is associated with classical antimicrobial activation of airway macrophages. Theophylline in maintenance treatment of chronic asthma: concentration-dependent additional effect to beta 2-agonist therapy. Tiotropium improves lung function, exacerbation rate, and asthma control, independent of baseline characteristics including age, degree of airway obstruction, and allergic status. Impact of coping and socioeconomic factors on quality of life in adults with asthma. Coping and social problem solving correlates of asthma control and quality of life. An Official American Thoracic Society Workshop Report: evaluation and management of asthma in the elderly. Health service use by African Americans and Caucasians with asthma in a managed care setting. Quantitative structural analysis of peripheral airways and arteries in sudden fatal asthma. Airway epithelial orchestration of innate immune function in response to virus infection: a focus on asthma.
Discount 15 mg flexeril fast delivery
Its role in allergic diseases is not well established because no purified allergens have been identified to date symptoms gallstones cheapest flexeril. The genera Acremonium and the more restrictive genera Cephalosporium play limited roles in allergic respiratory diseases. The genera Chrysonilia (formerly Monilia) and Neurospora have been chiefly linked to occupational lung diseases. High levels of basidiospores in the outdoor air have been linked to epidemic episodes of asthma. While several allergens have been identified, commercially available materials for skin testing are limited. Lastly, the genus Ustilago and other smut fungi (Sporisorium and Sphacelotheca) belong to the family Ustilaginaceae. Ustilago is a frequent plant pathogen of corn (corn smut), and positive intradermal skin tests to U. Fungal Allergens Unfortunately, the ability of clinicians to diagnose fungal allergy has been limited owing to the lack of standardized fungal extracts for skin testing and the continued use of archaic terminology. The use of microarrays with purified fungal allergens to assay for specific IgE antibodies in sera of individuals with respiratory disease demonstrates a high degree of IgE cross-reactivity between fungal allergens and the close phylogenetic relationships among fungi (115). In addition to IgE-binding allergens, fungal allergens and other fungal products can activate innate immune responses leading to asthma (116). Major allergens have been isolated from a number of fungi important in allergic diseases. Alt a 1 from Alternaria alternata is of unknown biological activity; cross-reactive allergens to it have been obtained from Stemphylium, Epicoccum, and other genera. Cla h 1 from Cladosporium herbarum is a major allergen, and when employed in skin testing reagents significantly increases positive responses. A large number of Aspergillus and Penicillium allergens have been purified which are often highly cross-reactive. Many of these have protease activity, such as vacuolar serine protease (Asp f 18, Pen c 18), metalloprotease (Asp f 5), alkaline serine protease (Asp f 13, Pen c 13), aspartyl protease (Asp f 10), enolase (Alt a 6, Cla h 6, Asp f 22), manganese superoxide dismutase (Asp f 6), glutathione-S-transferase (Alt a 13, Pen c 24), and various dehydrogenases (Alt a 10, Cla h 8, Cla h 3). Further advances in the isolation and characterization of fungal allergens will clarify their role in allergic diseases and improve diagnostics available to clinicians and epidemiologists. It dates back to 1921 when Kern described patients who had skin test reactivity to house dust extracts taken from their own residence (117). However, it was not until the 1960s, when several Dutch workers demonstrated that dust mites (specifically Dermatophagoides pteronyssinus) were the allergens in house dust and elaborated on those relationships (118). They are a subclass of arachnids that constitute several orders of Acarina, and belong to the family Pyroglyphidae. The primary dust mites found inside homes in North America and Europe are Dermatophagoides farinae and Dermatophagoides pteronyssinus. Other house dust mite species are Dermatophagoides microceras, Euroglyphus maynei, and the tropical Blomia tropicalis. A male house mite can have a life span of about 10 to 20 days while females can live up to 70 days. They can lay between 30 and 100 eggs over their life span and produce about 2,000 fecal particles making them a prolific contributor to allergy. Dust mites 264 feed off shed human skin, organic detritus, and other high protein debris in their environment. The major factors governing mite reproduction are ambient temperature and humidity. High altitudes are associated with low number of dust mites, presumably because of the reduced humidity (121). Dust mites typically are found in the greatest numbers in mattress dust, but 272 can certainly be found anywhere in the house that people routinely traffic, including rugs, bedding, and furniture. Housekeeping or the presence of household pets does not necessarily influence the mite load. The primary methods recommended to reduce dust mites include nylon or polyester-based impermeable mattress and pillow encasings, frequent washing of bedding, and maintenance of ambient humidity at less than 40% to 50%. Both the mite body and the feces contain allergen, though the major allergens are found in feces extracts. Studies show that many allergens cross-react between the two species although some are unique (124). These allergens have 80% to 85% homology among the mite species, with moderate levels of antigenic cross-reactivity measured by IgE antibodies. Studies of Der p 1, a 24-kDa glycoprotein, suggest that it is responsible for 75% of the IgE binding in mite feces (125). Using sequence data, the group 1 allergens have been identified as members of the cysteine protease family, and the possible importance of this function is addressed earlier in the chapter. Both allergens have been cloned and reveal over 85% to 90% sequence homology (126). Der p 3 and Der f 3 are found primarily in fecal material from the house dust mites. Der p 3 has been cloned (128), and enzymatic studies have demonstrated serine protease activities consistent with trypsin (129). In addition to group 1 and 2 allergens (Der p 1/Der f 1; Der p 2/Der f 2), it has also been recently proposed that group 23 allergens (Der p 23) are also deemed to be immunodominant in the hierarchy of IgE reactivity of dust mite allergens (135). There are other species of mites that are pests in areas of stored grain and can cause allergy, particularly in farm workers. Species include Acarus siro, Tyrophagus putrescentiae, Lepidoglyphus (Glycyphagus) domesticus, and Lepidoglyphus destructor. Spider mites (Panonychus ulmi and Tetranychus urticae) have been implicated in occupational allergy among apple farmers, and citrus red mite (Panonychus citri) among citrus farmers (136,137). People often believe that a short-haired or hairless animal is not allergenic, which is a common misconception. It is unknown whether this is because of the strength of the allergic reaction, the quantities in the air, or the size of the airborne particles. IgE to the major allergen, Fel d 1, is present in 80% of cat-sensitive individuals and has traditionally been thought to be the primary antigen responsible for allergic disease. Crystal structures of recombinant Fel d 1 also have a significant resemblance to uteroglobin, which is cytokine-like molecule with anti-inflammatory and immunomodulatory properties (140). Recently, two additional major allergens have been identified using molecular techniques. Fel d 3 (cystatin) has been identified, and appears to be a cysteine protease based on molecular modeling (141,142). Fel d 4 has been suggested as a major allergen, and 47% of patients have a significantly higher IgE titer against Fel d 4 than against Fel d 1. Fel d 4 is a lipocalin that has sequence homology with other known animal allergens (143). Cats have significant individual variation in the production of Fel d 1, with male cats generally producing greater amounts of allergen than females. These factors may explain why some patients are more allergic to certain cats than to others. Air sampling in rooms occupied by cats show abundant cell fragments <5 m in diameter. The small particle size may also explain why cat allergen can remain airborne in undisturbed conditions for extended periods. Further studies have indicated that it takes up to 24 weeks after removing a cat from inside the home to get back to the baseline quantity of Fel d 1 found in a home with no cat (145). It has been shown that repeated washing of the pet does help to reduce the release of cat allergens though the effect appears to last about 1 week necessitating frequent washing (146,147). Four of the allergens, Can f 1, Can f 2, Can f 4, and Can f 6, are lipocalins with dimeric structures (1).

Order 15 mg flexeril visa
The acute phase of otitis media occurs during the first 3 weeks of the illness symptoms nervous breakdown purchase cheap flexeril, the subacute phase between 4 and 8 weeks, and the chronic phase begins after 8 weeks. This condition results in the one of the most commonly performed surgeries in the United States: tympanostomy tube placement (118). Other risk factors include male sex, bottle feeding, day care attendance, allergy, race (Native American and Inuit), lower socioeconomic status, pacifier use, prone sleep position, winter season, and passive smoke exposure (118,123). Any of these manifestations can indicate an elevated intraocular pressure or the presence of uveitis or other threatening ocular conditions (see text). Eustachian Tube Anatomy and Physiology the nasopharynx and middle ear are connected by the eustachian tube. The production of middle ear effusions appears to be related to functional or anatomic abnormalities of this tube. Under normal conditions, the eustachian tube has three physiologic functions: (a) ventilation of the middle ear to equilibrate pressure and replenish oxygen; (b) protection of the middle ear from nasopharyngeal sound pressure and secretions; and (c) clearance of secretions produced in the middle ear into the nasopharynx. The eustachian tube of the infant and the young child differs markedly from that of the adult. These anatomic differences predispose infants and young children to middle ear disease. Usually, after the age of 7 years, these physical changes lessen the frequency of middle ear effusion (118). In the normal state, the middle ear is free of any significant amount of fluid and is filled with air. When the eustachian tube is blocked by either functional or anatomic defects, air cannot enter the middle ear, and the remaining air is absorbed. Also, there is an increased density of goblet cells in the epithelium of the eustachian tube. It is thought that many children with middle ear effusions, without a demonstrable cause of eustachian tube obstruction, have a growth-related inadequate action of the tensor veli palatini muscle. Another possibility is functional obstruction from persistent collapse of the tube owing to increased 1398 tubal compliance. Nasal obstruction, either from adenoid hypertrophy or from infectious or allergic inflammation, may be involved in the pathogenesis of middle ear effusion by the Toynbee phenomenon (124). Studies have reported that, when the nose is obstructed, there is an increased positive nasopharyngeal pressure followed by a negative nasopharyngeal pressure on swallowing. The increased positive nasopharyngeal pressure may predispose to insufflation of secretions into the middle ear, and the secondary negative pressure in the nasopharynx may further be a factor in the inadequate opening of the eustachian tube, thereby causing obstruction. Bacteria have been cultured in about 70% of middle 1399 ear effusions during tympanocentesis for otitis media in children (125). The predominant anaerobes are Grampositive cocci, pigmented Prevotella and Porphyromonas species, Bacterioides species, and Fusobacterium species. The predominant organisms isolated from chronic otitis media are Staphylococcus aureus, Pseudomonas aeruginosa, and anaerobic bacteria. In neonates, group B streptococci and Gram-negative organisms are common bacterial pathogens causing otitis media. Investigations suggest that the mucociliary transfer system is an important defense mechanism in clearing foreign particles from the middle ear and the eustachian tube (131). Goblet and secretory cells provide a mucous blanket to aid ciliated cells in transporting foreign particles toward the nasopharynx for phagocytosis by macrophages, or to the lymphatics and capillaries for clearance. Respiratory viral infections are associated with transient abnormalities in the structure and function of cilia (132). Primary ciliary dyskinesia, an autosomal recessive syndrome, has been linked to more than 20 different structural defects in cilia, which lead to ciliary dysfunction (133). Both of these conditions can lead to inefficient ciliary 1400 transport, which results in mucostatics and can contribute to eustachian tube obstruction and the development of middle ear effusion. Many investigators believe that allergic disorders play a prominent role, either as a cause or contributory factor; whereas others state that there is no convincing evidence that allergy leads to otitis media. In a series of 488 new patients referred to a pediatric allergy clinic, 49% had documented middle ear dysfunction (137). Twenty-three percent were considered allergic by history, physical examination, and allergy skin testing. Patients were blindly challenged with the pollen to which the patient was sensitive or to a control. Nasal function was determined by nasal rhinomanometry and eustachian tube function by the nine-step-deflation tympanometric test. The results from this and other studies (141) showed that eustachian tube dysfunction can be induced by allergen and histamine challenge (141), although no middle ear effusions occurred. Osur evaluated 15 children with ragweed allergy and measured eustachian tube dysfunction before, during, and after a ragweed season (142). These researchers evaluated 89 patients for allergy who 1401 required the placement of tympanostomy tubes because of persistent effusion. Significant levels of eosinophil cationic protein and eosinophils were found in the effusions, suggesting allergic inflammation in the middle ear (143). These investigators also determined that IgE in middle ear effusion is not a transudate but more likely reflects an active localized process in atopic patients (144) and that tryptase, a reflection of mast cell activity, is found in most ears of patients with chronic effusion who were atopic (145). The middle ear is usually one of many locations for infection in immunodeficient patients. Of the primary immunodeficiency conditions, otitis media is more common in the humoral or Bcell disorders, such as X-linked hypogammaglobulinemia, common variable immunodeficiency, and selective IgA deficiency. Otorrhea, discharge from the middle ear, may occur if spontaneous perforation of the tympanic membrane occurs. Classically, the tympanic membrane is erythemic and bulging without a light reflex or the ossicular landmarks visualized. Pneumatic testing fails to elicit any movement of the tympanic membrane on applying positive and negative pressures. Others may complain of stopped-up or popping ears or a feeling of fullness in the ear. Their teachers and parents detect the condition in many younger children because they are noted to be inattentive, loud talkers, and slow learners. When middle ear effusions become chronic, there may be significant diminution of language development and auditory learning, with resultant poor academic achievement. There is often retraction of the tympanic membrane, and the malleus may have a chalky appearance. As the disease progresses, the tympanic membrane takes on an opaque amber or bluish gray color. Mild retraction of the tympanic membrane may indicate only negative ear pressure without effusion. In more severe retraction, there is a prominent lateral process of the malleus with acute angulation of the malleus head. Tympanic membrane motility is generally poor when positive and negative pressures are applied by the pneumatic otoscopy. It is a tool for indirect measuring of the compliance or mobility of the tympanic membrane by applying varying ear canal pressure from 200 to 400 mm H2O. Eye examination may illustrate injected conjunctiva seen in patients with allergic conjunctivitis. Pale, boggy turbinates with profuse serous rhinorrhea are commonly found with allergic rhinitis. When chronic middle ear effusions are associated with the signs and symptoms of allergic disease, a standard allergic evaluation is indicated. A nasal smear for eosinophils, peripheral eosinophil count, and cutaneous tests for specific allergens may be of diagnostic importance. In patients with recurrent or chronic otitis media in whom middle ear disease is just one of many sites of infection, screening of the immune system should be considered. Laboratory studies, such as IgG, IgA, and IgM, naturally occurring antibodies such as isohemagglutinins, and specific antibody titers to antigens previously given in vaccines, such as tetanus, are useful in evaluation of humoral immune status. Measuring specific antibody levels before and after administration of a pneumococcal polyvalent vaccine is an effective mean of evaluating humoral immune function.
Discount 15 mg flexeril with mastercard
Effect of daily pollen challenge medications memory loss discount 15mg flexeril otc, environmental pollen exposure and placebo challenge on the nasal membrane. Minimal persistent inflammation is present at mucosal level in patients with asymptomatic rhinitis and mite allergy. Current concepts and therapeutic strategies for allergic rhinitis in school age children. Burden of allergic rhinitis: allergies in America, and Asia-Pacific adult surveys. Childhood environment and adult atopy: results from the European Community Respiratory Health Survey. Treatment of allergic rhinitis with intranasal corticosteroids in patients with mild asthma. Prevalence of allergic rhinitis and its impact on the use of emergency care services in a group of children and adolescents with moderate to severe persistent asthma. Further observations on the role of IgE-mediated hypersensitivity in recurrent otitis media with effusion. Economic impact of workplace productivity losses due to allergic rhinitis compared with select medical conditions in the United States from an employer perspective. Allergic rhinitis: burden of illness, quality of life, comorbidities, and control. Allergic rhinitis-a total genomescan for susceptibility genes suggests a locus on chromosome 4q24-q27. A genome-wide linkage analysis of orchard grass-sensitive childhood seasonal allergic rhinitis in Japanese families. Fine-scale mapping of type I allergy candidate loci suggests central susceptibility genes on chromosomes 3q, 4q and Xp. Genome-wide linkage analysis of allergic rhinoconjunctivitis in a Swedish population. Polymorphisms of histamine metabolizing enzymes and clinical manifestations of asthma and allergic rhinitis. Epigenetic modifications and improved regulatory T-cell function in subjects undergoing dual sublingual immunotherapy. Prenatal farm exposure is related to the expression of receptors of the innate immunity and to atopic sensitization in school aged children. Childhood allergic rhinitis predicts asthma incidence and persistence to middle age: a longitudinal study. Association of severity of chronic rhinosinusitis with degree of comorbid asthma control. Absence of nasal priming as measured by rhinitis symptom scores of ragweed allergic patients during seasonal exposure to ragweed pollen. Antigen presenting cells in the nasal mucosa of patients with allergic rhinitis during allergen provocation. Immunohistology of the nasal mucosa in seasonal allergic rhinitis: increases in activated 1316 eosinophils and epithelial mast cells. Basophil influx occurs after nasal antigen challenge: effects of topical corticosteroid pretreatment. The influx of inflammatory cells into nasal washings during the late response to antigen challenge: effect of systemic steroid pretreatment. Striking deposition of toxic eosinophil major basic protein in mucus: implications for chronic rhinosinusitis. Role of intradermal skin tests 1317 in the evaluation of clinically relevant respiratory allergy assessed using patient history and nasal challenges. Rebound congestion and rhinitis medicamentosa: nasal decongestants in clinical practice. The influence of female sex hormones on nasal reactivity in seasonal allergic rhinitis. Prevalence of asthma, aspirin intolerance, nasal polyposis and chronic obstructive pulmonary disease in a population-based study. Comprehensive algorithm for skull base dural lesion and cerebrospinal fluid fistula diagnosis. Management of invasive juvenile nasopharyngeal angiofibromas: the role of a multimodality approach. Nasal ciliary ultrastructure and function in patients with primary ciliary dyskinesia compared with that in normal subjects and in subjects with various respiratory diseases. Up-date on neuro-immune mechanisms involved in allergic and non-allergic rhinitis. Pathophysiological mechanisms for the respiratory syncytial virus-reactive airway disease link. Effect of experimental rhinovirus 39 infection on the nasal response to histamine and cold air challenges in allergic and nonallergic subjects. Upper respiratory tract complications of gastroesophageal reflux in adult and pediatric-age patients. Systematic review: ageing and gastro-esophageal reflux disease symptoms, oesophageal function and reflux oesophagitis. Follow-up study in local allergic rhinitis shows a consistent entity not evolving to systemic allergic rhinitis. Local IgE production and positive nasal provocation test in patients with persistent nonallergic rhinitis. Local allergic rhinitis: concept clinical manifestations, and diagnostic approach. Increasing prevalence of hay fever and atopy among children in Leipzig, East Germany. Long-term risk factors for developing asthma and allergic rhinitis: a 23-year followup study of 1323 college students. Increased prevalence of perennial allergic rhinitis in patients with obstructive sleep apnea. Soluble intercellular adhesion molecule-1 level in sera is elevated in perennial allergic rhinitis. Randomized placebocontrolled trial comparing fluticasone aqueous nasal spray in monotherapy, fluticasone plus cetirizine, fluticasone plus montelukast and cetirizine plus montelukast for seasonal allergic rhinitis. Steroids inhibit uptake and/or processing but not presentation of antigen by airway dendritic cells. Inhibition of mediator release in allergic rhinitis by pretreatment with topical glucocorticosteroids. Effect of short-term treatment with fluticasone propionate nasal spray on the response to nasal allergen challenge. Effect of topical applications of budesonide and azelastine on nasal symptoms, eosinophil count and mediator release in atopic patients after nasal allergen challenge during the pollen season. Evaluating approved medications to treat allergic rhinitis in the United States: an evidence-based review of efficacy for nasal symptoms by class. Safety update regarding intranasal corticosteroids for the treatment of allergic rhinitis. Bioavailability of fluticasone propionate and mometasone furoate aqueous nasal sprays. Beclomethasone dipropionate: absolute bioavailability, pharmacokinetics, and metabolism following intravenous, oral, intranasal, and inhaled administration in man. Safety, tolerability and exposure of ciclesonide nasal spray in healthy and asymptomatic subjects with seasonal allergic rhinitis. Once-daily treatment with beclomethasone dipropionate nasal aerosol does not affect hypothalamicpituitary-adrenal axis function. Effects of intranasal corticosteroids on adrenal, bone, and blood markers of systemic activity in allergic rhinitis. Safety considerations of intranasal corticosteroids for the treatment of allergic rhinitis. Evaluation of intraocular pressure and cataract formation following the long-term use of nasal corticosteroids. Absence of growth retardation in children with perennial allergic rhinitis after one year of treatment with mometasone furoate aqueous nasal spray.
