
Etoricoxib 120mg amex
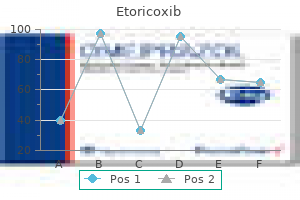
The blood flows into the corresponding venous channels either through the terminal capillary networks or through the shunts knee arthritis definition buy 60 mg etoricoxib visa. This countercurrent flow facilitates material exchange between the mother and fetus. The above two are separated by tissues Fetal blood flow 400 mL/min called placental membrane or barrier, consisting through the placenta of the following. In early pregnancy, it consists Pressure in the 60 mm Hg of (1) syncytiotrophoblast, (2) cytotrophoblast, umbilical artery (3) basement membrane, (4) stromal tissue, and Pressure in the 10 mm Hg (5) endothelium of the fetal capillary wall with umbilical vein its basement membrane. Sparse cytotrophoblast and distended fetal artery vein capillaries almost fill the villus. The thick "beta zones" of the terminal villi with the layers remaining thick in patches are for hormone synthesis. The aging process varies in degree and should be differentiated from the morbid process likely to affect the organ in some pathological states. These are called white infarcts which vary in size from few millimeters to a centimeter or more. Maternal properties Drug Molecular weight: Lower the molecular weight, more is the transfer Lipid solubility: Lipophilic substances diffuse readily concentration in the maternal blood Uterine blood flow Concentration gradient on either side of placental Ionization: Nonionized form crosses lipid membrane membranes freely C. Placental properties pH of blood: Lower pH favors ionization of many Lipid membrane of placenta enhances transfer drugs Total surface area of placental membrane Protein binding Functional integrity and thickness of placental barrier Spatial configuration (p. Immunoglobulin IgG is taken up by endocytosis from maternal circulation and is transferred to the fetus via exocytosis. Respiratory function: Although the fetal respiratory movements are observed as early as 11 weeks, there is no gaseous exchange. Intake of oxygen and output of carbon dioxide take place by simple diffusion across the fetal membrane. Partial pressure gradient is the driving force for exchange between the maternal and fetal circulations. Excretory function: Waste products from the fetus such as urea, uric acid, and creatinine are excreted in the maternal blood by simple diffusion. Nutritive function: the fetus obtains its nutrients from the maternal blood and when the diet is inadequate, then only depletion of maternal tissue storage occurs. Glucose which is the principal source of energy is transferred to the fetus by facilitated diffusion. Fetal glucose level is lower than that of the mother indicating rapid rate of fetal utilization of glucose. Lipids for fetal growth and development are transferred across the fetal membrane or synthesized in the fetus. Triglycerides and fatty acids are directly transported from the mother to the fetus in early pregnancy but probably are synthesized in the fetus later in pregnancy. Fetal proteins are synthesized from the transferred amino acids and the level is lower than in mother. Water and electrolytes such as sodium, potassium and chloride cross through the fetal membrane by simple diffusion, whereas calcium, phosphorus and iron cross by active transport (active transporter proteins) against a concentration gradient, since their levels are higher in fetal than in maternal blood. Water soluble vitamins are transferred by active transport, but the fat soluble vitamins are transferred slowly so that the latter remains at a low level in fetal blood. Chapter 3 the Placenta and Fetal Membranes 41 Hormones - Insulin, steroids from the adrenals, thyroid, chorionic gonadotrophin or placental lactogen cross the placenta at a very slow rate, so that their concentration in fetal plasma are appreciably lower than in maternal plasma. In general, substances of high molecular weight of more than 500 daltons are held up, but there are exceptions. Antibody and antigens in immunological quantities can traverse across the placental barrier in both directions. Maternal infections during pregnancy by virus (rubella, chickenpox, measles, mumps, poliomyelitis), bacteria (Treponema pallidum, Tubercle bacillus) or protozoa (Toxoplasma gondii, malaria parasites) may be transmitted to the fetus across the so-called placental barrier and affect the fetus in utero. Similarly, almost any drug used in pregnancy can cross the placental barrier and may have deleterious effect on the fetus. There is a shift of maternal response from cell-mediated (T helper 1) to humoral (T helper 2) immunity, which may be beneficial to pregnancy (see p. The cytokines thus derived, will regulate the invasion of extravillous trophoblast cells into the spiral arteries. The spiral arteries are thus converted to low resistance, high conductance uteroplacental arteries. The immunological response of implantation and that of organ transplantation are different and not comparable. Internally, it is attached to the amnion by loose areolar tissue and remnant of primitive mesenchyme. Externally, it is covered by vestiges of trophoblastic layer and the decidual cells of the fused decidua capsularis and parietalis which can be distinguished 42 Textbook of Obstetrics microscopically. Therefore human placenta is a discoid, deciduate, labyrinthine and hemochorial type (p. The outer surface consists of a layer of connective tissue and is apposed to the similar tissue on the inner aspect of the chorion from which it can be peeled off. The amnion can also be peeled off from the fetal surface of the placenta except at the insertion of the umbilical cord. Functions: (1) Contribute to the formation of liquor amnii; (2) Intact membranes prevent ascending uterine infection; (3) Facilitate dilatation of the cervix during labor; (4) Has got enzymatic activities for steroid hormonal metabolism; (5) Rich source of glycerophospholipids containing arachidonic acid - precursor of prostaglandin E2 and F2. Fluid accumulates slowly at first, but ultimately the fluid-filled cavity becomes large enough to obliterate the chorionic cavity; the amnion and the chorion come in loose contact by their mesenchymal layers. Production Transudation Removal of maternal serum across the placental Fetus swallows membranes every day. Chapter 3 the Placenta and Fetal Membranes 43 Initially, the cavity is located on the dorsal surface of the embryonic disk. Thus, the liquor amnii surrounds the fetus everywhere except at its attachment with the body stalk. The amnion is firmly attached to the umbilical cord up to its point of insertion to the placenta, but everywhere it can be separated from the underlying chorion. The presence of lanugo and epithelial scales in the meconium shows that the fluid is swallowed by the fetus and some of it passes from the gut into the fetal plasma (vide scheme). As the pregnancy continues post term, further reduction occurs to the extent of about 200 mL at 43 weeks. Color: In early pregnancy it is colorless, but near term it becomes pale straw colored due to the presence of exfoliated lanugo and epidermal cells from the fetal skin. Abnormal color: Deviation of the normal color of the liquor has got clinical significance. Meconium stained (green) is suggestive of fetal distress in presentations other than the breech or transverse. Depending upon the degree and duration of the distress, it may be thin or thick or pea soup (thick with flakes). But in late pregnancy, the composition is very much altered mainly due to contamination of fetal urinary metabolites. As pregnancy advances, there may be slight fall in the sodium and chloride concentration probably due to dilution by hypotonic fetal urine, whereas the potassium concentration remains unaltered. During pregnancy: (1) It acts as a shock absorber, protecting the fetus from possible extraneous injury; (2) Maintains an even temperature; (3) the fluid distends the amniotic sac and thereby allows for growth and free movement of the fetus and prevents adhesion between the fetal parts and amniotic sac; (4) Its nutritive value is negligible because of small amount of protein and salt content; however, water supply to the fetus is quite adequate. During labor: (1) the amnion and chorion are combined to form a hydrostatic wedge which helps in dilatation of the cervix; (2) During uterine contraction, it prevents marked interference with the placental circulation so long as the. Maternal abdomen is divided into quadrants taking the umbilicus, symphysis pubis and the fundus as the reference points. It is measured to diagnose the clinical condition of polyhydramnios or oligohydramnios respectively; (4) Rupture of the membranes with drainage of liquor is a helpful method in induction of labor (p. Initially, it is attached to the caudal end of the embryonic disk, but as a result of cephalocaudal folding of the embryo and simultaneous enlargement of the amniotic cavity the amnioectodermal junction converges on the ventral aspect of the fetus.
Diseases
- Venencie Powell Winkelmann syndrome
- Pili canulati
- Fibromatosis
- Young Hugues syndrome
- Glossopalatine ankylosis micrognathia ear anomalies
- Encephalo cranio cutaneous lipomatosis
Buy etoricoxib 120mg mastercard
More and more cases of placental abruption are being diagnosed in the recent years rheumatoid arthritis causes etoricoxib 60mg visa. Risk factors are: (a) high birth order pregnancies with gravida 5 and above - three times more common than in first birth (b) advancing age of the mother (c) poor socio-economic condition (d) malnutrition (e) smoking (vasospasm). Preeclampsia, gestational hypertension and essential hypertension, all are associated with placental abruption. The mechanism of the placental separation in preeclampsia is: Spasm of the vessels in the utero-placental bed (decidual spiral artery) anoxic endothelial damage rupture of vessels or extravasation of blood in the decidua basalis (retroplacental hematoma). Trauma: Traumatic separation of the placenta usually leads to its marginal separation with escape of blood outside. The trauma may be due to: (i) Attempted external cephalic version specially under anesthesia using great force (ii) Road traffic accidents or blow on the abdomen (iii) Needle puncture at amniocentesis. Sudden uterine decompression: Sudden decompression of the uterus leads to diminished surface area of the uterus adjacent to the placental attachment and results in separation of the placenta. This may occur following- (a) delivery of the first baby of twins (b) sudden escape of liquor amnii in hydramnios and (c) premature rupture of membranes. Short cord, either relative or absolute, can bring about placental separation during labor by mechanical pull. Supine hypotension syndrome: In this condition which occurs in pregnancy there is passive engorgement of the uterine and placental vessels resulting in rupture and extravasation of the blood. Sick placenta: Poor placentation, evidenced by abnormal uterine artery Doppler waveforms is associated with placental abruption. Folic acid deficiency even without evidence of overt megaloblastic erythropoiesis - this has been observed to be associated. Uterine factor: Placenta implanted over a septum (Septate Uterus) or a submucous fibroid. Torsion of the uterus leads to increased venous pressure and rupture of the veins with separation of the placenta. Cocaine abuse is associated with increased risk of transient hypertension, vasospasm and placental abruption. Prior abruption: Risk of recurrence for a woman with previous abruption varies between 5% and 17%. The collected blood (decidual hematoma) at the early phase, hardly produces any morbid pathological changes in the uterine wall or on the placenta. However, depending upon the extent of pathology, there may be degeneration and necrosis of the decidua basalis as well as the placenta adjacent to it. Rupture of the basal plate may also occur, thus communicating the hematoma with the intervillous space. The decidual hematoma may be small and self limited; the entity is evident only after the expulsion of the placenta (retroplacental hematoma). The features of retroplacental hematoma are: (a) Depression found on the maternal surface of the placenta with a clot which may be found firmly attached to the area (b) Areas of infarction with varying degree of organization. As the uterus remains distended by the conceptus, it fails to contract and therefore fails to compress the torn bleeding points. It has to be remembered that absence of rhythmic uterine contractions plays a significant role for the blood fig. Blood may dissect downwards in between the membranes and the uterine wall and ultimately escapes out through the cervix or may be kept concealed by the pressure of the fetal head on the lower uterine segment. Pre-placental: Between the placenta and the amniotic uid, within amnion and chorion (subamniotic). There is massive intravasation of blood into the uterine musculature upto the serous coat. Naked eye features: the uterus is of dark port wine color which may be patchy or diffuse. It tends to occur initially on the cornu before spreading to other areas, more specially over the placental site. Subperitoneal petechial hemorrhages are found under the uterine peritoneum and may extend into the broad ligament. Microscopic appearance: the uterine muscles over the affected area are necrosed and there is infiltration of blood and fluid in between the fig. The serosa may split on occasions, to allow the blood to enter the peritoneal cavity. The myometrial hematoma rarely interferes with uterine contractions following delivery. Thus, the presence of Couvelaire uterus as observed during cesarean section is not an indication per se for hysterectomy. The precise mechanism is not clear but may be due to intrarenal vasospasm as a consequence of massive hemorrhage. Shock proteinuria is probably due to renal anoxia which usually disappears 2 days after delivery, whereas proteinuria due to preeclampsia tends to last longer. There is overt hypofibrinogenemia (< 150 mg/dL) and elevated levels of fibrin degradation products and D-dimer (see p. Grade-3 (15%): (i) bleeding is moderate to severe or may be concealed (ii) uterine tenderness is marked (iii) shock is pronounced (iv) fetal death is the rule (v) associated coagulation defect or anuria may complicate. The clinical features of the revealed and mixed variety are given in tabulated form (Table 19. The differentiating points have been given previously in tabulated form (Table 19. In concealed variety-The following complications may occur either singly or in combination. However, a severe case may lead to (d) cortical necrosis and 298 Textbook of Obstetrics Table 19. Related with the visible blood loss May be absent Proportionate to the period of gestation. Can be identi ed easily Usually present Normal Low value proportionate to the blood loss Usually unchanged Mixed (concealed features Predominate) Abdominal acute intenses pain followed by slight vaginal bleeding. The pain becomes continuous Continuous, dark color (usually slight) or blood stained serous discharge * Shock may be pronounced which is out of proportion to the visible blood loss. Pallor is usually severe and out of proportion to the visible bleeding Frequent association May be disproportionately enlarged and globular. As such vaginal examination is withheld unless certain in the diagnosis Usually present With acute obstetrical-gynecological-surgical complications * Shock: Shock is often due to blood loss and hypovolemia or due to coagulopathy. Mild hemorrhage (< 15% of the blood volume loss) is generally not associated with any change of vital signs. Moderate hemorrhage (15-30% of the blood volume loss) is associated with tachycardia, hypotension, pulse pressure and mean arterial pressure whereas severe hemorrhage (loss > 30-40%) is associated with features of shock. The complicating factors that are responsible for increased maternal death varies from 2% to 8%. However, with better understanding in the management of shock, coagulation failure and renal failure, maternal death has been reduced markedly. Some cases who manage to survive may develop features of ischemic pituitary necrosis. In concealed type, however, the fetal death is appreciably high, ranging from 50% to 100%. With same degree of placental separation, the fetus is put to more risk in abruptio placentae than in placenta previa. This is due to the presence of preexisting placental pathology with poor functional reserve in the former, in contrast to an almost normal placental functions in the latter. Avoidance of trauma-specially forceful external cephalic version under anesthesia. To avoid sudden decompression of the uterus- in acute or chronic hydramnios, amniocentesis is preferable to artificial rupture of the membranes. To avoid supine hypotension the patient is advised to lie in the left lateral position in the later months of pregnancy. Routine administration of folic acid from the early pregnancy - of doubtful value. Management options are: (a) immediate delivery (b) management of complications if there is any (c) expectant management (rare).
Order 60 mg etoricoxib amex
Meanwhile arthritis treatment by homeopathy 120 mg etoricoxib, the cytotrophoblastic cells beyond the tips of the villus system penetrate into the overlying syncytium adjacent to the decidua. The cells become continuous with those of the neighboring villus system traversing through the syncytium. Thus, a thin outer cytotrophoblastic shell is formed which surrounds the entire blastocyst. The zone of the decidua immediately adjacent to the trophoblastic shell is called trophosphere which comprises of the compact layer of the decidua. Maternal blood vessels pass through all the layers to reach the intervillous space. The villi overlying the decidua basalis continue to grow and expand and are called chorion frondosum which subsequently forms the discoid placenta. The chorionic villi on the decidua capsularis gradually Chapter 2 Fundamentals of Reproduction 29 undergoes atrophy from pressure and become converted into chorion laeve by the 3rd month and lies intervening between the amnion and decidua on its outer surface. Remnant of decidual cells and of the trophoblast can however be distinguished microscopically. The bilaminar germ disc is connected with the trophoblast by mesenchymal condensation, called connecting stalk or body stalk which later on forms the umbilical cord. Its floor is formed by the ectoderm and the rest of its wall by primitive mesenchyme. Formation of trilaminar embryonic disk: Fourteen days after fertilization, proliferation of ectodermal cells in the midline, leads to formation of primitive streak. Cells within the streak spread laterally between the ectoderm and endoderm as intraembryonic mesoderm. This intraembryonic mesoderm becomes continuous with the extraembryonic mesoderm at the lateral border of the embryonic disk. Subsequently the amniotic cavity enlarges at the expense of the extraembryonic coelom. The extraembryonic mesenchyme covering the amnion now fuses with the lining of the chorion. During the embryonic stage which extends from the fourth to eighth week, individual differentiation of the germ layers and formation of the folds of the embryo occur. Most of the tissues and organs are developed during this period, the details of which are beyond the description of this book. However, the major structures which are developed from the three germinal layers are mentioned below. The human placenta is discoid, because of its shape; hemochorial, because of direct contact of the chorion with the maternal blood and deciduate, because some maternal tissue is shed at parturition. The placenta is attached to the uterine wall and establishes connection between the mother and fetus through the umbilical cord. The fact that maternal and fetal tissues come in direct contact without rejection suggests immunological acceptance of the fetal graft by the mother. The principal component is fetal which develops from the chorion frondosum and the maternal component consists of decidua basalis. When the interstitial implantation is completed on 11th day, the blastocyst is surrounded on all sides by lacunar spaces around cords of syncytial cells, called trabeculae. From the trabeculae develops the stem villi on 13th day which connect the chorionic plate with the basal plate. Primary, secondary and tertiary villi are successively developed from the stem villi. Arterio-capillary-venous system in the mesenchymal core of each villus is completed on 21st day. This ultimately makes connection with the intraembryonic vascular system through the body stalk. As the growth of the embryo proceeds, decidua capsularis becomes thinner beginning at 6th week and both the villi and the lacunar spaces in the abembryonic area get obliterated, converting the chorion into chorion laeve. This is, however, compensated by (a) exuberant growth and proliferation of the decidua basalis and (b) enormous and exuberant division and subdivision of the chorionic villi in the embryonic pole (chorion frondosum). Until the end of the 16th week, the placenta grows both in thickness and circumference due to growth of the chorionic villi with accompanying expansion of the intervillous space. Subsequently, there is little increase in thickness but it increases circumferentially till term. The human hemochorial placenta derived its name from hemo- (blood) that is in contact with the syncytiotrophoblasts of chorionic tissue. It feels spongy and weighs about 500 gm, the proportion to the weight of the baby being roughly 1: 6 at term and occupies about 30% of the uterine wall. Fetal surface: the fetal surface is covered by the smooth and glistening amnion with the umbilical cord attached at or near its center. Branches of the umbilical vessels are visible beneath the amnion as they radiate from the insertion of the cord. The amnion can be peeled off from the underlying chorion except at the insertion of the cord. A thin grayish, somewhat shaggy layer which is the remnant of the decidua basalis (compact and spongy layer) and has come away with the placenta, may be visible. Each fissure is occupied by the decidual septum which is derived from the basal plate. These are due to deposition of calcium in the degenerated areas and are of no clinical significance. The maternal portion of the placenta amounts to less than one-fifth of the total placenta. Only the decidua basalis and the blood in the intervillous space are of maternal origin. Margin: Peripheral margin of the placenta is limited by the fused basal and chorionic plates and is continuous with the chorion laeve and amnion. Essentially, the chorion and the placenta are one structure but the placenta is a specialized part of the chorion. Attachment: the placenta is usually attached to the upper part of the body of the uterus encroaching to the fundus adjacent to the anterior or posterior wall with equal frequency. The attachment to the uterine wall is effective due to anchoring villi connecting the chorionic plate with the basal plate and also by the fused decidua capsularis and vera with the chorion laeve at the margin. Separation: Placenta separates after the birth of the baby and the line of separation is through the decidua spongiosum. Between the two plates lies the intervillous space containing the stem villi with their branches, the space being filled with maternal blood. At places, placental or decidual septa project from the basal plate into the intervillous space but fail to reach the chorionic plate. It is lined internally on all sides by the syncytiotrophoblast and is filled with slow flowing maternal blood. With the progressive development - primary, secondary and tertiary villi are formed. Functional unit of the placenta is called a fetal cotyledon or placentome, which is derived from a major primary stem villus. Functional subunit is called a lobule, which is derived from a tertiary stem villi. Thus while some of the villi are anchoring the placenta to the decidua, the majority are free within the intervillous space and are called nutritive villi. Blood vessels within the branching villi do not anastomose with the neighboring one. In placenta at term, syncytiotrophoblast becomes relatively thin at places overlying the fetal capillaries and thicker at other areas containing extensive endoplasmic reticulum.
Etoricoxib 60mg overnight delivery
It has been estimated that for one maternal death at least 15 more suffer from severe morbidities arthritis vinegar treatment cheap 120 mg etoricoxib. Definition: Obstetric morbidity originates from any cause related to pregnancy or its management any time during antepartum, intrapartum and postpartum period usually up to 42 days after confinement. Indirect: these conditions are only expressions of aggravated previous existing diseases like malaria, hepatitis, tuberculosis, anemia, etc. Reproductive morbidity is used in a broader sense to include-(a) Obstetric morbidity, (b) Gynecological morbidity and (c) Contraceptive morbidity. The perinatal mortality rate is expressed in terms of such deaths per 1000 total births. The perinatal mortality rate closely reflects both the standards of medical care and effectiveness of social and public health measures. However, for international comparisons, only deaths of fetuses or infants weighing > 1000 g at birth should be included as in the developing countries many such deaths are under reported. Worldwide nearly four million newborns die within the first week of life and another three million are born dead. Perinatal deaths could be reduced by at least 50% worldwide if key interventions are applied for the newborn. The perinatal mortality is less than 10 per 1000 total births in the developed countries while it is much higher in the developing countries (60/1000 in India). The major health problem in the developing world arises from the synergistic effect of malnutrition, infection and unregulated fertility combined with lack of adequate obstetric care. The important causes of antepartum deaths are: (a) Chronic hypoxia (30%), (b) Pregnancy complications (30%), (c) Congenital malformations (15%), (d) Infection (5%) and (e) Unexplained (20%). Perinatal deaths increase due to hypoxia, intrauterine growth restriction, prematurity, congenital malformations and infection. Obstetric complications: (a) Antepartum hemorrhage particularly abruptio placenta is responsible for about 10% of perinatal deaths due to severe hypoxia, (b) Preeclampsia-eclampsia is associated with high perinatal loss either due to placental insufficiency or prematurity- spontaneous or induced (c) Rh isoimmunization (d) Cervical incompetence-Premature effacement and dilatation of cervix between 24 and 36 weeks is responsible for significant perinatal deaths from prematurity. Complications of labor: Dystocia from disproportion, malpresentation, abnormal uterine action, premature rupture of membranes may result in asphyxia, amnionitis and birth injuries contributing to perinatal deaths. Fetoplacental factors: Multiple pregnancy most often leads to preterm delivery and usual complications. Congenital malformation and chromosomal abnormalities are responsible for 15% of perinatal deaths, the lethal malformations are mostly related to nervous, cardiovascular or gastrointestinal system. Intrauterine growth restriction and low-birth-weight babies-Apart from preterm delivery, intrauterine nutritional deficiency may be responsible for such low weight babies which are more vulnerable to biochemical, neurological and respiratory complications resulting in high perinatal deaths of about 50% when the birth weight is less than 2 kg. Preterm labor and preterm rupture of the membranes are the known leading causes of prematurity. Unexplained: About 20% of stillbirths have no obvious fetal, placental, maternal or obstetric causes. As such, improvement of obstetric service only around delivery, will not minimize perinatal deaths appreciably. Simultaneous demographic and social changes help in reduction of perinatal mortality rate significantly. Termination of an affected fetus is a positive step in reduction of deaths due to congenital malformations (see p. Screening of high-risk patients those of poor socioeconomic status or high parity, extremes of age, and twins, etc. Skilled birth attendant - To minimize sepsis, at least three cleans are to be maintained (see p. Provision of referral neonatal service especially to look after the preterm babies. Continued study of perinatal mortality problems by demographic studies, regular clinically allied interdepartmental meetings and pathological research. Perinatal morbidity: It implies major illness of the neonate from birth to first 4 weeks of life. Important causes of morbidity are due to (a) Prematurity and low birth weight, (b) Birth asphyxia and birth trauma (c) Congenital malformations. Such deaths include antepartum deaths (macerated) and intrapartum deaths (fresh stillbirths). Stillbirths rate is the number of such deaths per 1000 total births (live and stillbirths) (Table 38. Causes: the causes of death within 7 days are almost always obstetrically related and as such stillbirths and neonatal deaths within 7 days are grouped together as perinatal deaths. However the progress fell short of the target in parts of South Asia and Subsaharan Africa. Beyond these strategic actions, good governance must also incorporate a human rights approach which includes accountability, participation, ownership, transparency, equity and non-discrimination. Lifetime risk of dying from pregnancy-related complications for a woman of developing country is 1 in 11, compared to 1 in 5000 in the industrialized country (see p. Maternal deaths are classified into- (a) Direct, (b) Indirect and (c) Fortuitous deaths (see p. Maternal Near Miss is a condition when a women who nearly died but survived from a severe health condition, during pregnancy, child birth or within 6 weeks of puerperium. Maternal morbidity (Obstetric morbidity) develops from any cause related to pregnancy, childbirth or puerperium. Nearly 15 more women suffer from severe morbidity, when there is one maternal death. Important causes of stillbirths are: Birth asphyxia and trauma (30%), pregnancy complications (30%) and others. Severe hypoxia in labor when associated with metabolic acidosis can cause fetal organ damage or fetal death. In between contractions the intraluminal pressure within the spiral artery (85 mm of Hg) is higher than the intramyometrial pressure (10 mm of Hg) to maintain the uteroplacental blood flow. During peak uterine contractions, myometrial pressure (120 mm of Hg) exceeds the arterial pressure (90 mm of Hg) causing temporary halting of O2 delivery to the fetus through the placenta. Depending upon the intensity and duration of contraction, fetal hypoxia may develop. Even in a normal labor, the baby is subjected to stress due to: (1) Uterine contractions temporarily curtailing the uteroplacental circulation. But in a compromised fetus and/or in a pathological state of labor, the fetal distress may appear abruptly. The term "Fetal distress" has been abandoned in favor of more appropriate term "Nonreassuring fetal status". The auscultation should be made for 60 sec particularly before and immediately following a uterine contraction. Pathogenesis: Hypoxia vagal response peristaltic activity and relaxation of the anal sphincter passage of meconium. The vicious circle is: Placental insufficiency oligohydramnios cord compression hypoxia thick meconium gasping breath meconium aspiration. Meconium staining of the liquor as observed following rupture of the membranes gives a crude idea of intrauterine fetal jeopardy. Intermittent auscultation is recommended to monitor the fetus for a woman in labor without any complications. The transducers are placed on the maternal abdomen, one over the fundus and the other at a site where the fetal heart sound is best audible. Frequency of uterine contractions and uterine pressure are recorded simultaneously by tocodynamometer. Intrauterine pressure could be simultaneously measured by passing a catheter inside the uterine cavity. Drawbacks: (i) Interpretation is affected by intra- and interobserver error (ii) Due to error of interpretation, cesarean section rate may be high (iii) Instruments are expensive and trained personnel are required to interpret a trace (iv) Mother has to be confined in bed. Absence of accelerations, reduced baseline variability of < 5 bpm for > 90 minutes denotes a hypoxic fetus.
Threonine. Etoricoxib.
- Familial spastic paraparesis and multiple sclerosis.
- Are there safety concerns?
- What is Threonine?
- How does Threonine work?
- Dosing considerations for Threonine.
- Spinal spasticity.
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97029
Buy 120 mg etoricoxib amex
Cytoplasmic volume is increased along with changes in the number arthritis pain wikipedia buy 120 mg etoricoxib fast delivery, distribution of mitochondria and Chapter 2 Fundamentals of Reproduction 23 in the Golgi apparatus. Completion of the arrested first meiotic division occurs with extrusion of first polar body, each containing haploid number of chromosomes (23, X). The ovum is picked up into the Fallopian tube and undergoes either degeneration or further maturation, if fertilization is to occur. Menstruation is unrelated with ovulation and anovular menstruation is quite common during adolescence, following childbirth and in women approaching menopause. It begins with sperm egg collision and ends with production of a mononucleated single cell called the zygote. Its objectives are: (1) To initiate the embryonic development of the egg and (2) To restore the chromosome number of the species. The pick up action might be muscular or by a kind of suction or by ciliary action or by a positive chemotaxis exerted by the tubal secretion. Fertilizable life span of oocyte ranges from 12 to 24 hours whereas that of sperm is 48 to 72 hours. The tubal transport is facilitated by muscular contraction and aspiration action of the uterine tube. Soon after the sperm fusion, penetration of other sperm is prevented by zona reaction (hardening) and oolemma block. The bigger one is called the female pronucleus and the smaller one is called second polar body which is pushed to the perivitelline space. Head and the neck of the spermatozoon become male pronucleus containing haploid number of chromosomes (23, X) or (23, Y). The zygote, thus formed, contains both the paternal and maternal genetic materials. In some instances, an antigen called fertilizin present on the cortex and its coat of the ovum, reacts with the antibody called antifertilizin liberated at the plasma membrane of the sperm head. Thus the union between the two gametes may be an immunological reaction (chemotaxis). The blastomeres continue to divide by binary division through 4, 8, 16 cell stage until a cluster of cells is formed and is called morula, resembling a mulberry. As the total volume of the cell mass is not increased and the zona pellucida remains intact, the morula after spending about 3 days in the uterine tube enters the uterine cavity through the narrow uterine ostium (1 mm) on the 4th day in the 16-64 cell stage. The transport is a slow process and is controlled by muscular contraction and movement of the cilia. The central cell of the morula is known as inner cell mass which forms the embryo proper and the peripheral cells are called outer cell mass which will form protective and nutritive membranes of the embryo. The fluid passes through the canaliculi of the zona pellucida which separates the cells of the morula and is now termed blastocyst. Zona hatching is the next step so that trophectoderm cells interact with endometrial cells and implantation occurs. The cells on the outer side of the morula (polar) become trophectoderm and the inner cells (apolar) become inner cell mass by the mediation of epithelial cadherin (E-cadherin) (protein). Trophectoderm differentiates into chorion (placenta) and the inner cell mass into the embryo. Pinopods are long finger like projections (microvilli) from the endometrial cell surface. These pinopods absorb the endometrial fluid which is secreted by the endometrial gland cells. This fluid, rich in glycogen and mucin provides nutrition to the blastocyst initially. Adhesion of blastocyst to the endometrium occurs through the adhesion molecules like integrin, selectin and cadherin (glycoproteins). With increasing lysis of the stromal cells, the blastocyst 26 Textbook of Obstetrics. Concurrently, the syncytial cells penetrate deeper into the stroma and erode the endothelium of the maternal capillaries. The syncytium by penetrating the vessels, not only becomes continuous with the endothelial lining but permits the maternal blood to enter into the lacunar system. Ultimately erosion of few maternal arteries with formation of blood space (lacunae) occurs. Further penetration is stopped probably by the maternal immunological factor and the original point of entry is sealed by fibrin clot and later by epithelium. This type of deeper penetration of the human blastocyst is called interstitial implantation and the blastocyst is covered on all sides by the endometrium (decidua). Occasionally, there may be increased blood flow into the lacunar spaces at the abembryonic pole. This results in disruption of the lacunae and extravasation of blood into the endometrial cavity. This corresponds approximately to 13th day after fertilization (at about the expected day of the following period). The cytotrophoblasts that line the villous stems are the villous cytotrophoblasts. Thus, it serves at least 3 important functions - invasion, nutrition and production of hormones for the maintenance of pregnancy. Decidual reaction: the increased structural and secretory activity of the endometrium that is brought about in response to progesterone following implantation is known as decidual reaction. Changes occur in all the components of the endometrium but most marked at the implantation site and first commence around maternal blood vessels. The fibrous connective tissues of the stroma become changed into epithelioid cells called decidual cells. The glands show marked dilatation and increased tortuosity with its lining epithelium showing evidences of active cell proliferation with increased secretory activity. There are areas of small interstitial hemorrhage and leukocytic infiltration specially at the implantation site. After the interstitial implantation of the blastocyst into the compact layer of the decidua, the different portions of the decidua are renamed as - (1) Decidua basalis or serotina - the portion of the decidua in contact with the base of the blastocyst (2) Decidua capsularis or reflexa - the thin superficial compact layer covering the blastocyst and (3) Decidua vera or parietalis - the rest of the decidua lining the uterine cavity outside the site of implantation. As the growing ovum bulges towards the uterine cavity, the space between the decidua capsularis and the decidua vera, called the decidual space is gradually narrowed down and by 4th month, it is completely obliterated by the fusion of the decidua capsularis with the decidua vera. At term, they become atrophied due to pressure and the two cannot be defined as a double layer. The decidua basalis, however, retains its characteristic appearance till term and becomes the maternal portion of the placenta. It consists of two embryonic layers - outer trophoblast and inner primitive mesenchyme which appears on 9th day. At the beginning of the 3rd week, the syncytiotrophoblast produces irregular finger like projections which are lined internally by the cytotrophoblast. These finger like buds are called primary stem villi - surrounded by lacunar spaces which will later form into intervillous spaces. After the appearance of the primitive mesenchyme and the development of the chorion, the primary stem villi are named chorionic villi. With the insinuation of the primary mesoderm into the central core of the villi structures, secondary villi are formed on 16th day. Later on mesodermal cells in the villi begin to differentiate into blood cells and blood vessels, thus forming villous capillary system. These vascularized villi are called tertiary villi which are completed on 21st day. Later on, this extra embryonic circulatory system establishes connection with the intraembryonic circulatory system through the body stalk. The former is probably the site for transfer and the latter, the site for synthesis. Stroma contains dilated vessels along with all the constituents and few Hofbauer cells. Hofbauer cells are round cells that are capable of phagocytosis and can trap maternal antibodies crossing through the placenta (immune suppressive). A mature placenta has a volume of about 500 mL of blood; 350 mL being occupied in the villi system and 150 mL lying in the intervillous space.
Order etoricoxib australia
An assistant is required to hold the left handle after its introduction (b) With axis-traction device: While applying the left blade rheumatoid arthritis levels purchase generic etoricoxib, the traction-rod already attached to the blade is held backwards. During introduction of the right blade, the traction-rod must be held forwards otherwise it will prevent locking of the blades. Traction: (a) Without axis-traction device: the direction of pull is first downwards and backwards, then (horizontal or straight pull) and finally upwards and forwards (b) With axis-traction device: the traction handle is to be attached to the traction rods. When the base of the occiput comes under the symphysis pubis, the traction-rods are to be removed. During application of the blades: the causes are: (1) Incompletely dilated cervix (2) unrotated or nonengaged head. Difficulty in locking: the causes are: (1) Application in unrotated head (2) improper insertion of the blade (not far enough in) (3) failure to depress the handle against the perineum and (4) entanglement of the cord or fetal parts inside the blades. Difficulty in traction: the causes of failure to deliver with traction are: (1) Undiagnosed occipitoposterior position (2) faulty cephalic application (3) wrong direction of traction (4) mild pelvic contraction and (5) Constriction ring. Slipping of the blades: the causes are: (1) the blades are not introduced far enough in (2) faulty application in occipitoposterior position. The blades should lie equidistant from the sinciput and occiput, otherwise the blades may slip during traction. Horizontal traction is given until the root of the nose is under the symphysis pubis. But the handles should be kept well forward to avoid grasping of the neck by the tips of the blade. Traction is made like that of occipitoanterior to bring the chin well below and then round the symphysis pubis. Its advantages over the widely used longcurved forceps are: (1) It can be used with advantages in unrotated vertex or face presentation (2) facilitates grasping and correction of asynclitic head because of its sliding lock. The concavity of the slight pelvic curve should correspond to the side towards which the occiput lies. The posterior blade is inserted directly under guidance of the right hand placed between the head and the hollow of the sacrum. The forceps handles are depressed down and the handle tips are brought into alignment to correct the asynclitism. Piper forceps is a specialized forceps, used to assist the delivery of the after-coming head of breech. Cephalohematoma, facial palsy, skull fractures, cervical spine injury (rotational forceps) laceration or sulcus tear, cervical tear, extension of episiotomy to involve the vaginal vault, complete perineal tear Nerve injury: Femoral (L2, 3, 4), lumbosacral trunk (L4, 5) with midforceps delivery Postpartum hemorrhage may be-(i) traumatic or (ii) atonic, requiring blood transfusion or (iii) both, may cause shock Anesthetic complications (following local or general anesthesia see p. It refers to forceps delivery only to shorten the second stage of labor when maternal and/or fetal complications are anticipated. The indications are: (1) Eclampsia (2) heart disease (3) previous history of cesarean section (4) postmaturity (5) low-birth-weight baby (6) to curtail the painful second stage and (7) patients under epidural analgesia. Prophylactic forceps should not be applied until the criteria of low forceps are fulfilled. The procedure should be conducted in an operation theater keeping everything ready for cesarean section. If moderate traction leads to progressive descent of the fetal head, the delivery is completed vaginally, if not cesarean section is done immediately. Many unnecessary cesarean sections or difficult vaginal deliveries can thus be avoided. Only through skill and judgment, proper selection of the case ideal for forceps can be identified. Even if applied in wrong cases, one should resist the temptation to give forcible traction in an attempt to hide the mistake. The pulling force is dragging the cranium while in forceps, the pulling force is directly transmitted to the base of the skull. Soft cups, silc cup [silicone rubber or disposable plastic (Mityvac)] cups have better adherence to the fetal scalp. These cups could be folded and introduced into the vagina without much discomfort. Rigid plastic cup (Kiwi Omnicup) is safe, effective and is useful for rotational delivery. The cup is connected to a pump through a thick-walled rubber tube by which air is evacuated. Chance of scalp avulsion or subaponeurotic hemorrhage (iii) suspected fetal coagulation disorder and (iv) suspected fetal macrosomia (4 kg). It helps in autorotation is not a space-occupying device like the forceps blades force is less (10 kg) compared to forceps is comfortable and has lower rates of maternal trauma and genital tract lacerations need is less. Pudendal block with perineal infiltration is adequate but for forceps regional or general anesthesia is often needed maternal pelvic floor injuries and is advocated as the instrument of first choice. The fetal head remains inside the protective cage can be employed in anterior face or in after-coming head of breech presentation, where ventouse is contraindicated neonatal scalp trauma, retinal hemorrhage, jaundice or cephalhematoma compared to ventouse rate of successful vaginal delivery as ventouse has got higher failure rates than forceps detachment (Pop-off) occurs when the vacuum is not maintained in ventouse. No such problems once forceps blades are correctly applied of types of forceps (p. The instrument should be assembled and the vacuum is tested prior to its application. The cup is introduced after retraction of the perineum with two fingers of the other hand. The cup is placed against the fetal head nearer the occiput (flexion point) with the "knob" of the cup pointing towards the occiput. Flexion or pivot point is an imaginary site located midsagittally about 6 cm from the center of the anterior fontanel or about 3 cm in front of the posterior 662 Textbook of Obstetrics fontanel. Traction over this flexion point either by ventouse or forceps facilitates flexion and presents the smaller diameter to the pelvis. A check is made using the fingers round the cup to ensure that no cervical or vaginal tissue is trapped inside the cup. The scalp is sucked into the cup and an artificial caput succedaneum (chignon) is produced. The fingers of the other hand are to be placed against the cup to note the correct angle of traction, rotation and advancement of the head Operative vaginal delivery (forceps/ventouse) should be abandoned, where there is no descent of the presenting part with each pull or when delivery is not imminent after three pulls with correctly applied instruments by an experienced operator. On no account, traction should exceed 30 minutes As soon as the head is delivered, the vacuum is reduced by opening the screw-release valve and the cup is then detached. Traction over this flexion or pivot point either by ventouse or forceps promotes flexion and presents smaller diameter to the pelvis. Usually it resolves by one or two weeks (4) subaponeurotic (subgaleal) hemorrhage (not limited by suture line as it is not subperiosteal) (5) intracranial hemorrhage (rare) (6) retinal hemorrhage (no long-term effect) and (7) jaundice. Maternal: the injuries are uncommon but may be due to inclusion of the soft tissues such as the cervix or vaginal wall inside the cup. The sequential use of ventouse and forceps increases the risk of trauma both to the mother and the neonate. The instrument, as deviced by Malmstrom, consists of: (1) suction cup (2) vacuum generator and (3) traction tubing device. The indications are same as those of forceps except that it cannot be employed in face or after coming head of breech. Vacuum: Causes lower rates of maternal trauma and genital tract lacerations, but causes more neonatal scalp trauma and cephalhematoma compared to forceps. The operator must have knowledge, experience and skill to use and also the willingness to abandon the procedure when felt difficult. The risk of fetal injury associated with instrumental vaginal delivery is instrument specific. Many women (79%) desire subsequent vaginal delivery compared with women delivered by cesarean section (39%). The incidence of spontaneous version in breech presentation is nearly 55% after 32 weeks and about 25% after 36 weeks. Internal: the conversion is done principally by one hand introducing into the uterus and by the other hand on the abdomen. Bipolar (BraxtonHicks): the conversion is done introducing one or two fingers through the cervix and by the other hand on the abdomen. When the cephalic pole is brought down to the lower pole of the uterus, it is called cephalic version and when the podalic pole is brought down, it is called podalic version.
Purchase 60mg etoricoxib with mastercard
It can be marked by a line that runs backwards from the main stem of the mandibular nerve ziks arthritis pain relief generic etoricoxib 120 mg, across the neck of the mandible. The nerve then turns upwards passing immediately in front of the tragus (preauricular point). To mark it draw a line continuous with the main stem of the mandibular nerve (see above). It is represented by a line that runs downwards and forwards to reach opposite the lower third molar tooth. It is useful only to mark the extracranial part of the nerve, before it divides into several branches. This foramen lies deep to the middle of the anterior border of the mastoid process (In the adult, the nerve lies at a depth of 2 cm, but the depth is much less in children). From here draw a horizontal line that runs forwards to end just behind the neck of the mandible. This nerve is marked by a line that runs downwards and forwards with a downward convexity. It can be represented by a straight line running down the entire length of the neck. From here draw a line downwards and backwards to reach a point midway between the mastoid process and the angle of the mandible. From this point carry the line further downwards and backwards to reach the middle of the posterior border of the sternocleidomastoid muscle. The nerve then runs across the posterior triangle to reach the anterior border of the trapezius about two inches above the clavicle. From here draw a line downwards and medially to reach the medial end of the clavicle. To mark this chain remember that it runs vertically immediately behind the carotid sheath. In contrast, the peripheral nervous system consists of the cranial nerves and the spinal nerves. The nervous system is made up, predominantly, of tissue that has the special property of being able to conduct impulses rapidly from one part of the body to another. The specialised cells that constitute the functional units of the nervous system are called neurons. Within the brain and spinal cord, neurons are supported by a special kind of connective tissue that is called neuroglia. Nervous tissue, composed of neurons and neuroglia, is richly supplied with blood, but lymph vessels are not present. Most neurons give off a number of short branching processes called dendrites and one longer process called an axon. In a dendrite, the nerve impulse travels towards the cell body whereas in an axon the impulse travels away from the cell body. Peripheral nerves are made up of aggregations of axons (and in some cases of dendrites). During its formation, each axon (and some dendrites) comes to be associated with certain cells that provide a sheath for it. The cells providing this sheath for axons lying outside the central nervous system are called Schwann cells. Axons lying within the central nervous system are provided a similar covering by a kind of neuroglial cell called an oligodendrocyte. Within the central nervous system, it always terminates by coming in intimate relationship with another neuron, the junction between the two neurons being called a synapse. Outside the central nervous system, the axon may end in relation to an effector organ. Neurons vary considerably in the size and shape of their cell bodies (somata) and in the length and manner of branching of their processes. The shape of the cell body is dependent on the number of processes arising from it. The most common type of neuron gives off several processes and the cell body is, therefore, multipolar. Another type of neuron has a single process and is therefore described as unipolar. One of the divisions represents the axon; the other is functionally a dendrite, but its structure is indistinguishable from that of an axon. Depending on the shapes of their cell bodies some neurons are referred to as stellate (star shaped) or pyramidal. These descriptions will be essential in understanding some aspects of the structure of the brain. Sections through the spinal cord or through any part of the brain show certain regions that appear whitish, and others that have a darker greyish colour. The arrangement of the grey and white matter differs at different situations in the brain and spinal cord. In the spinal cord and brainstem the white matter is on the outside whereas the grey matter forms one or more masses embedded within the white matter. In the cerebrum and cerebellum there is an extensive, but thin, layer of grey matter on the surface. Deep to the cortex there is white matter, but within the latter several isolated masses of grey matter are present. Such isolated masses of grey matter, present anywhere in the central nervous system, are referred to as nuclei. Aggregations of the cell bodies of neurons may also be found outside the central nervous system. Examples of sensory ganglia are the dorsal nerve root ganglia of spinal nerves, and the trigeminal ganglion. Chapter 48 Introduction to Central Nervous System and Internal Structure of Spinal Cord 1035 10. Autonomic ganglia include sympathetic ganglia located on the sympathetic chain, and parasympathetic ganglia. Some autonomic neurons are located in nerve plexuses (often called ganglia) present in close relationship to some viscera. The axons arising in one mass of grey matter terminate very frequently by synapsing with neurons in other masses of grey matter. The axons connecting two (or more) masses of grey matter are frequently numerous enough to form recognisable bundles. Large bundles of fibres connecting the cerebral or cerebellar hemispheres to the brainstem are called peduncles. As explained earlier, the cell bodies of these neurons are invariably located in masses of grey matter. The axons may be short, ending in close relation to the cell body, or may be long and may travel to other masses of grey matter lying at considerable distances from the grey matter of origin. The description that follows illustrates some of the basic arrangements encountered. The simplest pathways are those concerned with reflex activities, such as the contraction of a muscle in response to an external stimulus. For example, if the skin of the sole of a sleeping person is scratched, the leg is reflexlydrawnup. The stimulus applied to skin gives rise to a nerve impulse that is carried by the peripheral process of a unipolar neuron to the dorsal nerve root ganglion. From here the impulse passes into the central process that terminates by directly synapsing with an anterior grey column cell supplying the muscle which draws the leg up. The complete pathway constitutes a reflex arc and in the above example it consists of two neurons - one afferent and the other efferent. The central process of the dorsal nerve root ganglion cell ends by synapsing with a neuron lying in the posterior grey column. This neuron has a short axon that ends by synapsing with a neuron in the anterior grey column, thus completingthereflexarc. The third neuron interposed between the afferent and efferent neurons is called an internuncial neuron, or simply an interneuron. Firstly, the axon arising from an interneuron may divide into a number of branches and may synapse with a number of different efferent neurons. As a result an impulse coming along a single afferent neuron may result in an effector response by a large number of efferent neurons. Secondly, afferent impulses brought by a number of afferent neurons may converge on a single efferent neuron through the agency of interneurons.
Effective etoricoxib 90mg
However arthritis in the fingers remedies purchase etoricoxib 120 mg online, the use of uterine relaxant (tocolysis) has made the version at later weeks less difficult. It minimizes chance of reversion and should fetal complications develop, it can be effectively tackled by cesarean section. Successful version is likely in cases of: (i) Complete breech, (ii) Nonengaged breech, (iii) Sacroanterior position (fetal back anteriorly), (iv) Adequate liquor, (v) Nonobese patient. Causes of failure of version: (1) Breech with extended legs-early engagement of presenting part and difficult to flex the trunk because of splinting action of the limbs. Dangers of version: the dangers of version are-(1) premature onset of labor, (2) premature rupture of the membranes, (3) placental abruption and bleeding, (4) entanglement of the cord round the fetal part or formation of a true knot leading to impairment of fetal circulation and fetal death and (5) increased chance of fetomaternal bleed. Immunoprophylaxis with anti-D gammaglobulin is to be administered in nonimmunized Rh-negative mother (Chapter 22). Management, if version fails or is contraindicated: the pregnancy is to be continued with usual checkup and unexpectedly, one may find that spontaneous version has occurred. But if the breech persists, the assessment of the case is to be done with respect to-(1) age of the mother especially in primigravidae, (2) associated complicating factors, (3) size of the baby and (4) pelvic capacity. Elective Cesarean Section: Because of the complications involved in vaginal breech delivery, there is a tendency to liberalize the use of cesarean section in breech. The overall incidence of cesarean section in breech ranges from 15% to 50%, out of which about 80% is elective. Delivery of preterm breech (weight <1,500 g) by cesarean section is commonly done but it should be reserved in selected centers, equipped with intensive neonatal care unit. Vaginal examination is indicated-(a) at the onset of labor for pelvic assessment, (b) soon after rupture of the membranes to exclude cord prolapse. Breech extraction (partial or total): When part or the entire body of the fetus is extracted by the obstetrician. Principles in conduction: (1) Never to rush, (2) Never pull from below but push from above. It is expected that good uterine contractions and maternal expulsive forces will maintain the flexion of the fetal head and result in descent and safe delivery. Never to rush and never to pull-early aggressive and hasty pull affects breech delivery adversely by-(a) Entrapment of the aftercoming fetal head through the incompletely dilated cervix. Steps: the patient is brought to the table when the anterior buttock and fetal anus are visible. She is placed in lithotomy position when the posterior buttock distends the perineum. Pudendal block is done along with perineal infiltration if not epidural has been used earlier. Episiotomy: It should be made in all cases of primigravidae and selected multiparae. Its advantages are-(a) to straighten the birth canal which especially facilitates the delivery of breech with extended legs where lateral flexion is inadequate; (b) to facilitate intravaginal manipulation and for forceps delivery, (c) to minimize compression of the aftercoming head. The best time for episiotomy is when the perineum is distended and thinned by the breech as it is "climbing" the perineum. The patient is encouraged to bear down as the expulsive forces from above ensure flexion of the fetal head and safe descent. The "no touch to the fetus" policy is adopted until the buttocks are delivered along with the legs in flexed breech and the trunk slips up to the umbilicus. The following are to be done: (a) the extended legs (in frank breech) are to be decomposed by pressure on the knees (popliteal fossa) in a manner of abduction and flexion of the thighs. There may be transient abnormality in cord pulsation at this stage which has got no prognostic significance. Delivery of the arms: the assistant is to place a hand over the fundus and keep a steady pressure during uterine contractions to prevent extension of the arms. When the arms are flexed, the vertebral border of the scapula remains parallel to the vertebral column and when extended there is winging of the scapula (parallelism is lost). The arms are delivered one after the other only when one axilla is visible, by simply hooking down each elbow with a finger. Each one is quite safe and effective in the hands of an expert, conversant with that particular technique. The assistant is asked to give suprapubic pressure with the flat of hand in a downward and backward direction, the pressure is to be exerted more toward the sinciput. The aim is to promote flexion of the head so that favorable diameter is presented to the pelvic cavity. When the nape of the neck is visible under the pubic arch, the baby is grasped by the ankles with a finger in between the two. Maintaining a steady traction and forming a wide arc of a circle, the trunk is swung in upward and forward direction. Meanwhile, with the left hand to guard the perineum, slipping the perineum off successively the face and brow. The head should be brought as low down as possible by allowing the baby to hang by its own weight aided by suprapubic pressure. When the occiput lies against the back of the symphysis pubis, an assistant raises the legs of the child as much to facilitate introduction of the blades from below. Piper forceps is especially designed (absent pelvic curve) for use in this condition. The head should be delivered slowly (over 1 minute) to reduce compression-decompression forces as that may cause intracranial bleeding. The baby is placed on the supinated left forearm (preferred) with the limbs hanging on either sides. The middle and the index fingers of the left hand are placed over the malar bones on either sides (modification of the original method, where the index finger was introduced inside the mouth). Resuscitation of the baby: the baby may be asphyxiated and need to be resuscitated. If prophylactic ergometrine is to be given, it should be administered intravenously with the crowning of the head. Simulated teaching using mannequins and model pelvis with an experienced trainer can imporve the skill and performance of such maneuvers. Management: If the outlet is contracted and/or the baby is big, cesarean section even at this stage, is the method of choice. In the absence of outlet contraction and feto-pelvic disproportion: Liberal episiotomy and fundal pressure with or without groin traction (either single groin or both the groins) usually become effective. The index finger(s) is placed in the groin fold and traction (along with uterine contraction) is exerted more toward the trunk than toward the femur (risk of fracture femur). Arrest of the breech at or above the level of ischial spines: the causes may be: (i) Pelvic contraction, (ii) Big baby, (iii) Weak uterine contraction. By the time cervix is fully dilated, the breech should descend down to the perineum. The fetal foot is then grasped at the ankle and breech extraction is accomplished. The diagnosis is made by noting the winging of the scapula and absence of the flexed limbs in front of the chest. Management: the management calls for the urgent delivery of the arms, first the posterior and then the anterior one. The delivery of the arm may be accomplished by adopting any one of the following methods: (a) Classical. In addition, it needs intrauterine manipulation while the patient is under general anesthesia. Left hand is introduced along the curve of the sacrum while the baby is pulled slightly upward. The following are the advantages: (1) Wider applicability-It can be applied even when the classical method becomes difficult. Principles: Because of the curved birth canal, when the anterior shoulder remains above the symphysis pubis, the posterior shoulder will be below the sacral promontory. If the fetal trunk is rotated keeping the back anterior and maintaining a downward traction, the posterior shoulder will appear below the symphysis pubis.
Buy 90 mg etoricoxib with visa
Severity of fetal affection is best assessed by fetal hemoglobin and hematocrit levels as determined by cordocentesis arthritis in knee joints relief buy etoricoxib 90 mg free shipping. Generally a fetus whose hemoglobin deficit is 2 g/dL or more from the mean of a normal fetus of corresponding gestational age (hematocrit < 30%) should be transfused. Procedure: Transfusion is generally made through umbilical cord vessel (vein) near its insertion into the placenta under real time ultrasound. Hematocrit level is checked at intervals during the procedure to determine the volume. Fetal injury, volume overload, preterm labor and fetomaternal hemorrhage are the common complications. Fetal surveillance with ultrasound and continuous electronic fetal monitoring is performed at the posttransfusion phase. Betamethasone (24 mg in three divided doses) should be administered to the mother 24 hours before transfusion from 26 weeks onwards to enhance pulmonary maturity, in case delivery becomes necessary during transfusion. With the advent of wider use of prophylactic anti-D immunoglobulin, less and less problem babies are born and through exchange transfusion, the incidence of kernicterus has also been reduced. Thereafter, the baby is quite capable to get rid of the maternal antibodies by producing sufficiently his own Rh-positive blood. A plastic catheter of 1 mm diameter is passed about 7 cm beyond the umbilicus so as to place it in the inferior vena cava. Entire set should be air tight and to be periodically flushed with heparinized saline (1,000 units in 100 mL) to prevent clotting. For every 100 mL of blood transfused, one milliequivalent of sodium bicarbonate is given to combat metabolic acidosis and 1 mL of 10% calcium gluconate to prevent tetany due to transfusion of citrated blood. To estimate the hemoglobin and bilirubin concentration prior to and after the exchange transfusion. Occasionally, the level of conjugated bilirubin may remain higher and phototherapy should be continued and (4) hypoglycemia (due to increased insulin secretion) is to be checked by blood glucose estimation posttransfusion 4 hourly. Immediate complications: (1) Cardiac failure due to raised venous pressure and overloading of the heart; (2) air embolism; (3) clotting and massive embolism; (4) hyperkalemia; (5) tetany; (6) acidosis; (7) sepsis; (8) hypocalcemia; (9) hypoglycemia and (10) coagulopathies due to thrombocytopenia. Delayed complications: (1) Necrotizing enterocolitis; (2) extrahepatic portal hypertension due to thrombosis of portal vein and (3) other complications are mostly attributed to prematurity, hyperbilirubinemia and hypoxia. These products are water soluble and therefore readily excreted in the bile and urine. Phenobarbitone increases the glucuronyl transferase enzyme activity in the fetal and neonatal liver to conjugate the bilirubin which hastens its clearance. With alloimmunization of the mother, the prognosis of the baby depends on: (1) Genotype of the father; (2) genotype of the fetus; (3) maternal antibody level; (4) history of previous affection of the baby due to hemolytic disease and (5) availability of sophisticated diagnostic and therapeutic facilities for the affected babies (specialist fetal medicine care unit). The age limit is arbitrary and is based on the fact that the outcome of the pregnancy is adversely affected beyond the specified age limit. There are two groups of patients: (1) one with high fecundity-a women married late but conceives soon after and (2) one with low fecundity-woman married early but conceives long after marriage. The latter one is prognostically more unfavorable so far as the obstetric outcome is concerned after conception occurs following treatment of infertility (ovulation induction or assisted reproductive technology). During labor: There is increased incidence of: (1) preterm labor; (2) prolonged labor due to (a) uterine inertia caused by anxiety or malposition (occipito-posterior); (b) impaired joint mobility and (c) inelasticity of the soft tissues of the birth canal; (3) maternal and fetal distress appears early; (4) increased cesarean delivery and (5) retained placenta due to uterine atony and increased association of fibroid. Puerperium: (1) Increased morbidity due to operative interference and (2) failing lactation. The perinatal mortality is increased due to prematurity, increased congenital malformation (trisomy 21) and operative interference. Considering the risks involved in pregnancy and labor, the patients are considered "high risk" They require meticulous antenatal. The following principles are to be followed: (1) result of induction is unsatisfactory and as such cesarean section is a preferred alternative; (2) prenatal diagnosis and sonography (targeted) are done to exclude fetal genetic or structural anomaly and (3) development of other complications should be viewed with concern. The incidence has been gradually declining over the couple of decades due to acceptance of small family norm but it still constitutes to about one-tenth of the hospital population and accounts for one-third of the maternal deaths in the developing countries. Puerperium: (1) Increased morbidity due to sepsis, intranatal hazards; (2) subinvolution and (3) failing lactation. To find out the etiological factor: At the first antenatal visit, detailed in depth relevant history should be taken in an attempt to find out the cause of mishaps. In the developing countries, too often the disaster is linked with inadequate or neglected antenatal, intranatal or neonatal care. Previous history of congenital deformity of the baby, especially a neural tube defect should be excluded as there is likely chance of recurrence (see p. These antibodies are either IgG or IgM or both and bind to negatively charged phospholipids. There is inhibition in release of prostacyclin (vasodilator) from vascular endothelium with rise in the level of thromboxane (vasoconstrictor) from platelets. Other pathological changes like placental vascular atherosis, intervillous and spiral artery thrombosis and decidual vasculopathy with fibrinoid necrosis lead to inadequate maternal blood supply to fetus. Thrombophilias: Some regulatory proteins act as inhibitors in the coagulation cascade. Inherited or acquired deficiencies of these inhibitory proteins are collectively known as thrombophilias. To treat the offending factor: When the responsible factor is detected, appropriate therapy can be directed so as to prevent repetition of the mishaps. A good example is to perform encerclage operation in recurrent midtrimester abortion. Diabetes in pregnancy, if discovered during such investigation, should be adequately supervised all throughout pregnancy and a suitable time is selected for its termination (see p. Proved cases of fetal wastage due to red cell alloimmunization of the mother should be managed in specialized fetal medicine unit to deal with Rh problems. Approximate amount of fetomaternal bleed is estimated by Kleihauer-Betke acid elution test. If environmental factors are involved, extension of adequate antenatal and intranatal care is enough to prevent repetition of the mishaps. Therapy for patients with positive antiphospholipid antibodies and with thrombophilias is low-dose aspirin (50 mg a day). Therapy is started 1 month before conception and is continued in the first trimester. To remain vigilant: In obstetrics, any complicating factor, known or unknown, is likely to recur and if it recurs in two consecutive pregnancies, the chance of its recurrence in the third pregnancy is highly probable. When the cause remains unknown, constant vigilance following hospitalization in early or later months of pregnancy as the case may be, is all that is required. History of unexplained intrauterine death (suspected chronic placental insufficiency) should preferably be terminated at a period, judiciously selected under the guidance of available gadgets for the assessment of fetal well being (see Chapters 12 and 32). Obesity leads to development of type-2 diabetes, dyslipidemia and hypertension (metabolic syndrome). Effects on labor: (1) There is increased incidence of abnormal uterine contraction and prolonged labor; (2) operative interference and cesarean delivery is increased and so also difficulty in cesarean section; (3) shoulder dystocia is likely and (4) anesthetic hazards (difficult intubation) are high. Degree of affection of the fetus depends upon the degree of destruction of the fetal red cells (p. It should be given to the mother within 72 hours or earlier following delivery (p. It is always better to give anti-D immunoglobulin, where there is any doubt about whether to give or not. Findings suggestive of fetal anemia are: skin edema, ascites, pleural or pericardial effusions, increased placental thickness and others (p. Doppler ultrasound and cardiotocography are also informative and are noninvasive methods (p. Rh immune globulin prophylaxis can be given to Rh-negative, nonimmune woman at 28 weeks of pregnancy.
