
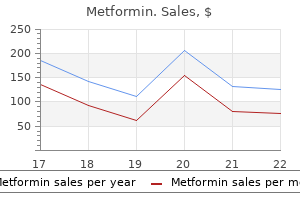
Buy 850 mg metformin free shipping
Follicles that cease growing and undergo atresia usually exhibit a form of granulosa-cell failure diabetes diet hindi pdf metformin 500 mg without a prescription, often characterized by increasing numbers of apoptotic granulosa cells and eventual loss of oocyte viability [6]. This is in contrast to prenatal folliculogenesis, where the oocytes are usually the leading cell type to undergo apoptosis, possibly due to the number of somatic granulosa precursor cells being limiting. This interfollicular communication has been demonstrated in vitro by experiments where follicles that are initially similar are placed in direct contact with each other. Systemic factors, such as circulating hormones, also start to influence the follicle, once its cells have developed the appropriate receptors and post-receptor response mechanisms. By this time the follicle is no longer a solid ball of cells, but contains a fluid-filled intercellular space called an antrum and a surrounding layer of thecal cells recruited from the ovarian stroma, outside the basal membrane. From about 2 mm diameter, the small antral follicle becomes visible by transvaginal ultrasound scanning. The numbers of small antral follicles in the early follicular phase of a menstrual cycle are sometimes used as an indicator of potential ovarian responsiveness to gonadotrophin stimulation in this cycle. However, methods to produce clinically useful oocytes from follicle growth in vitro or in an animal host are now in prospect [8, 9]. Timeline of oogenesis Many events underpinning female gamete competence occur in the prenatal ovary, many years before the onset of fertility. In mice, it is known that the primordial germ cells are descendents of cells found at a particular location during gastrulation in mice. Similar data are not available in humans, but it is Cords form, enclosing many oogonia in nests likely that the germline is kept separate from the somatic components of the developing embryonic disc at an early stage. The reasons for this are not known, but might include, for example, facilitating differential imprinting of the germline. Primordial germ cells then move from the yolk sac to the developing gonads by a process of migration. During the migration process, many cells are lost from the population, and reasons for their loss may include misdirection, apoptosis or too slow progress. However, other cells divide during the journey and the net effect is for a large increase in population size during this time. The term oocyte is not used until the diploid cells have entered meiosis; then they are correctly called oocytes. Oocytes have first been identified from around 10 weeks of gestation in humans, when some of the oogonia initiate meiosis. Oogonia enter meiosis over a period of several weeks, until approximately 24 weeks of gestation. Individual oocytes differ greatly in the rate at which they proceed through meiosis, and some oogonia, perhaps a quarter, fail to enter meiosis at all. This is a highly controversial claim which has undergone intense challenge in the literature, and to date has not been proven [11]. Meiosis is the specialized cell division that eventually results in gametes that have a haploid chromosome constitution, discussed in more detail later. However, prenatal oocytes do not achieve full gamete formation at this prenatal stage. Instead, they become arrested in an immature state early in meiosis, in first meiotic prophase. Oocytes that do not arrest, or do not associate with somatic cells, are unable to sustain further development and are mostly eliminated before birth. From the middle of gestation (week 20) extensive apoptosis takes place among the oocytes, resulting in the loss of more than half of them. In contrast, some of the nascent primordial follicles in the fetal ovary do not arrest but grow further, resulting in primary, secondary and antral follicles before birth. Once the intense folliculogenesis and apoptosis of gestation have resolved, the resulting ovary contains a large population of primordial follicles, together with smaller numbers of follicles at stages up to the antral stage. From birth to the menopause, a small proportion of primordial follicles will become activated each day and begin to grow. Only after puberty, when the hypothalamo-pituitary-gonadal axis has matured, providing an appropriate endocrine environment to support full follicular development, can any follicles progress to Graafian stages and ovulate their oocyte. These ovulatory follicles, at most one 51 Section 1: Mammalian reproductive physiology or occasionally two per month of adult life, represent the tiny minority, selected by a process of intense competition. Inevitably, therefore, the oocytes that give rise to mature gametes and contribute to subsequent generations are those which arrested successfully during prenatal development and formed a competent follicle that remained arrested for many years, initiated growth at an opportune moment and successfully outcompeted other follicles developing at the same time. The ultimate purpose of this complex process of follicle growth is to deliver a competent female gamete for fertilization. However, the process of oogenesis is also complex and there is no guarantee that the resulting gamete will be competent, even when follicle growth has proceeded optimally. In the prenatal period, oocytes complete only the first part of meiosis, namely meiotic prophase I. Shortly before ovulation, when the oocyte resumes meiosis, pairs of homologous chromosomes align on the spindle at metaphase I. Note the different chromosomal contents of the first and second polar bodies of the fertilized oocyte. Axial elements in human oocytes from the second trimester of pregnancy were highlighted using a fluorescently labelled antibody. Axial elements are part of the synaptonemal complex, the protein backbone that holds chromosomes together during meiotic prophase I. At the zygotene stage, longer elements are present and some of them have begun to synapse shown by thicker areas of synaptonemal complex (arrowed). At the pachytene stage, all homologous chromosomes have synapsed completely along their lengths. The synaptonemal complexes break down during the diplotene stage, so this stage is not shown here. This arrested chromosomal configuration persists for all the time that the oocyte is in a primordial and non-atretic growing follicle. Meiotic prophase I comprises four stages: leptotene, zygotene, pachytene and diplotene. These are clearly distinguishable when the synaptonemal complexes, the protein backbone that holds the chromosomes in their meiotic prophase I configurations, are highlighted with specific marker antibodies. However, much of the earlier literature in this field uses histological preparations, which are more challenging to interpret, resulting in wide discrepancies among data sets. Differences have also resulted from considerable variations in the fetal materials available for study. In the leptotene stage, the chromosomes start to condense and homologous chromosomes move together. The homologous chromosomes begin to synapse (adhering together progressively along their length), which marks the entry to the zygotene stage. As zygotene continues, chromosomes synapse for increasing lengths, identifiable as thicker regions of synaptonemal complex markers. During zygotene, the chromosomes must initially be prone to tangling as synapsis proceeds; however, when resolution is achieved, the result is an oocyte in which each of the homologous pairs is fully synapsed along the whole of its length. This is the pachytene stage, which is the most readily identifiable stage of meiotic prophase I. Mainly at the pachytene stage, recombination between adjacent chromatids of different homologues takes place. This results in genetic recombination and reshuffling of genes for the next generation of gametes, a particularly important stage and prone to errors. Each tetrad must have at least one chiasma, or crossing over point, in order to ensure that later separation of the homologous chromosomes takes place correctly. There is also evidence that the crossing over points are non-randomly distributed, and that the chances of 53 Section 1: Mammalian reproductive physiology incorrect separation of chromosomes increase as chiasma location moves proximally or distally [13]. The number of chiasmata varies, but there is evidence that oocytes developing normally contain more chiasmata than those with abnormalities in synapsis of homologous chromosomes [14]. At the diplotene stage, the synaptonemal complexes that have held the oocyte chromosomes in formation break down, and the chromosomes remain attached by their chiasmata only. Although recombination takes place at this early stage in meiosis, the recombined products do not separate from each other until the ejection of the polar bodies during oocyte maturation and fertilization, several years later.
Buy metformin 500mg without a prescription
Clearly there are a number of legal and ethical issues surrounding surrogacy managing diabetes 90 generic 500mg metformin, though it is a successful (and only) form of treatment for many couples. Unexplained infertility For couples with unexplained infertility there is no place for ovarian stimulation treatment using oral drugs such as clomifene citrate, or the lesser used drugs tamoxifen, anastrozole or letrozole. Patients, and doctors, often presume that the boost clomifene gives to ovulation, potentially resulting in multiple ovulation, will increase the chance of conception in women who are already ovulating spontaneously. The explanation may be that the anti-estrogenic effects of clomifene have deleterious effects at the endometrium. This involves giving advice on lifestyle factors, as initially described in this chapter, and excluding pathology that would require immediate recourse to fertility treatment. It is helpful to agree on a time frame with the couple, for instance to continue trying naturally for another six months before review and potentially moving on to active treatment. It is also helpful for the couple to have access to the fertility clinic nurse, counsellor or dietician for consultations. Expectant management is often also appropriate for couples with a diagnosis of minimal-mild endometriosis or mild male factor when there continues to be a reasonable monthly chance of conception for infertility durations of up to 2 or 3 years. While this approach is associated with a higher success rate, it also comes with an increased risk of multiple pregnancy. Whether or not the same outcome can be achieved by using prolonged oral contraceptive pill pretreatment is not currently known. Absent or severely abnormal uterus Women may have an absent uterus due to a congenital abnormality such as Rokitansky syndrome or following hysterectomy for malignancy. Male infertility the most appropriate treatment depends on the degree of semen abnormality and cause, and also the situation with the female partner, for example her age, ovulatory and tubal status. However, this approach risks not having sperm available for insemination and either needing to use donor sperm, or freezing or discarding the uninseminated oocytes. It is possible that such men have an epididymal block that is potentially reversible with surgery. Referral to a urologist is required for contrast studies, though very often the site of the obstruction is not found or cannot be repaired. The success rate of vasectomy reversal is related to the length of time since the vasectomy was performed. Antisperm antibodies may be present in the ejaculate following reversal which may affect the chance of natural conception. If the man has diabetes, a neurological condition or has had prostate surgery, then it is possible he has retrograde ejaculation. Some men with a neurological condition, such as paraplegia, may have erectile failure which responds to electro-ejaculation. The response Advanced maternal age As women age, the chance of conception, whether natural or with fertility treatment, reduces. Clearly this carries a risk of triplet pregnancy, though the absolute risk is very low for women approaching their mid-forties. However, many older women produce insufficient embryos of suitable quality for biopsy and genetic analysis. Donor sperm treatment is used by many couples with an infertility diagnosis of azoospermia. There continues to be debate over the benefits of zinc, vitamins and other supplements to improve male fertility. Furthermore, a recent Cochrane review has suggested improved live birth rates in the partners of men taking anti-oxidants. Conclusion Completion of appropriate and timely investigations allows the physician to discuss and offer suitable fertility treatments with the couple. It is vital to be realistic with the chance of success and to explain the risks and any financial costs of treatment to allow the couple to make an informed decision. Single women or same-sex female couples Single women or lesbian couples may be referred to the fertility clinic for treatment. A full fertility history, as described in the previous chapter, is taken to try to determine underlying pathology which may affect the success of donor sperm treatment. If tubal disease is thought to be unlikely, then donor insemination treatment is commenced. Up to six donor insemination cycles are appropriate, though the majority of successes occur during cycles one to three. If insemination treatment is unsuccessful, or if 168 18 Chapter Social aspects of using reproductive technology Renate Barber and Alison Shaw Social aspects of fertility and infertility the milestones of marriage, parenthood and grandparenthood are taken for granted during a normal life span in most human societies. Couples are expected to have children and grandparents expect to have grandchildren. In societies that permit a man to have more than one wife, it is relatively easy for a woman to observe that her husband does not have children with his other wives either, but the responsibility for childlessness would never be attached to the husband; a wife in this situation might clandestinely contrive to get pregnant by another man (such as a relative). It is only modern investigative technologies including that of the sperm count that have enabled the onus of some infertility cases to be placed firmly on the male. It is reflected in rituals that in many societies originally centred on the agricultural year and are concerned with producing good yields and fertile earth and fauna [1]. Pagan and Christian rituals, for example, include Easter, which marks the start of sowing and growing of crops, autumn harvest festivals to give thanks for the crops and Christmas, the winter solstice, to mark the ending of the dark season. Almost universally in human history, human fertility has been desired and valued, while barrenness has been feared and disapproved, for powerful socioeconomic and cultural reasons. In subsistence societies, children are valuable economically, by providing labour power. Among some African cattle herders, for example, there is a delicate balance between the size of the herds and the size of the families, because there must be enough people to look after the animals, but there can only be a limited number of people who can live off the herd. In societies lacking systems of social security and insurance for old age and sickness, children are also the only guarantee that the elderly will be taken care of. Where there is high infant mortality, it is thus good policy to have many children to ensure that some will survive in to adulthood. Children also represent perhaps the only visible means of continuity in many traditional societies, by perpetuating a line of inheritance and by enabling property to be inherited by descendants. Societies vary worldwide in whether they are patriarchal (investing power and authority in males), matriarchal or allow both males and females to hold positions of power and influence. They also vary as to whether they calculate inheritance patrilineally (in the male line), matrilineally (in the female line) or along both lines of descent (bilaterally). However, a majority of societies worldwide are or tend to be patriarchal and patrilineal. For example, in certain forms of male ancestor Textbook of Clinical Embryology, ed. As a result, there is often considerable pressure not just to have children but to have sons rather than daughters. The social pressure on a couple, and usually particularly on a woman, to have children is particularly acute in societies in which reproduction is understood to be a female domain and where a traditional division of labour by gender provides the central principles around which family life and the wider society is organized. If, after a few years of marriage or even sooner, a new wife does not become pregnant, she may be vulnerable socially and emotionally, for she is failing to fulfil her expected role as a wife and mother. In many other parts of the world today, including at least until recently in the West, the structure of society and the subordinate position of women within it has been derived to a large extent from the fact that women bore and reared children. This distinction may be marked by rituals of gender separation and isolation, and in consequence of this women have been barred from sacred offices such as the priesthood and other positions of power and authority [2]. This is underlined by the fact that older, postmenopausal women tended to enter public life to a greater degree, could become highly influential and, in some situations, could adopt socially male roles. Mothers of important men are admired, though their status really derives from that of their sons. The very fact of being the bearer of sons and heirs gave women of reproductive age and capacity a certain position of power, in that their noncooperation would be a serious threat to a man, but the corollary of this is that women who failed in the childbearing role were at a serious disadvantage and subject to stigma and abuse. Hence women must be under the guardianship of their fathers, brothers, husbands or sons. With a sedentary lifestyle and ownership of property, it became vital that heirs should be of the blood line, and so women had to be closely guarded, their sexuality controlled. The danger of a woman bearing a child conceived from outside the lineage drops away with the menopause and cessation of childbearing. Young as well as older mothers have status by virtue of having given birth, and there is ambiguity as to whether childless women, even those in important positions, are not held in lower esteem than women who are mothers (or mothers as well as having a profession).
| Comparative prices of Metformin | ||
| # | Retailer | Average price |
| 1 | Rite Aid | 566 |
| 2 | Dollar General | 419 |
| 3 | Ahold USA / Royal Ahold | 231 |
| 4 | Save Mart | 174 |
| 5 | Big Lots | 330 |
| 6 | A&P | 484 |
| 7 | Advance Auto Parts | 749 |
| 8 | Army Air Force Exchange | 665 |
| 9 | Dick's Sporting Goods | 746 |
| 10 | Meijer | 138 |
Buy genuine metformin on line
Prostate gland the prostate is the largest accessory sex gland in men and is a muscular single gland that surrounds the first inch of the urethra as it emerges from the bladder diabetes type 2 vaccine purchase 500mg metformin free shipping. The smooth muscle of the prostate gland contracts during ejaculation to contribute to the expulsion of semen from the urethra. While the prostate gland is encapsulated by a fibroelastic tissue layer, the prostate capsule gives rise to septa which extend inward and subdivide the prostate in to five lobes: anterior, posterior, medial and two laterals. Within these lobes are the tubuloalveolar or saecular glands, excretory ducts and dense stroma [4]. This secretion is rich in components such as calcium, zinc, citric acid and acid phosphatase. Phosphatase hydrolyzes phosphorylcholine to choline which is used as a nutrient by the sperm. The mucosa of the vas deferens is lined by a pseudostratified columnar epithelium, and in a manner similar to the epididymis, its cells have long stereocilia. The muscular layer of this duct is very well developed and consists of a thick circular layer of smooth muscle between thinner inner and outer longitudinal layers. The muscularis is the structure that makes the deferent duct palpable in the spermatic cord. During ejaculation, the smooth muscle of the deferent duct contracts reflexively (peristalsis), thus propelling the sperm and fluids forward and transferring them in to the urethra. Urethra the urethra extends from the bladder to the tip of the penis and constitutes a common passageway for semen and urine. The two major sections of the urethra, the pelvic part and the penile part, are differentiated. The pelvic part is first surrounded by the 20 Chapter 3: the male reproductive tract and spermatogenesis molecular weight protein of the seminal coagulum and to help semen liquefy following ejaculation. The presence of testosterone is essential for maintenance of the structural and functional integrity of the prostate gland. It is common for this gland to increase in size with ageing, and this can lead to microturation problems or even malignant hyperplasia. Each gland has a short duct which empties in to the spongy urethra as it enters the root of the penis. As a component of the seminal fluid, this mucin protects the urethra and serves as a lubricant during sexual intercourse. The secretion of gelatinous seminal fluid helps to lubricate the urethra for sperm to pass through, and to help flush out any residual urine or foreign matter. The alkalinity of seminal fluid helps to neutralize the acidic vaginal pH and permits sperm mobility in what might otherwise be an unfavourable environment. Penis the penis is the main external genital organ and is divided in to three portions, which in a proximal to distal order are named the root, body and free portion, or glans. Structurally the penis is built of three erectile components, two corpa cavernosum and one corpus spongiosus. The root consists of two crura of cavernous tissue which attach to the sciatic arch, and a central bulb of spongy tissue which surrounds the urethral duct as it comes out of the pelvic cavity. In the body of the penis, the two crura of cavernous tissue fuse and the spongy urethra runs ventrally throughout the urethral groove. In the free portion, which is covered with a fold of skin called the prepuce, the spongy tissue expands so as to form the glans. Erectile tissue consists of a framework of smooth muscle and connective tissue that contains blood sinuses, which are large, irregular vascular channels. This cavernous tissue is the major erectile component in the body of the penis, as is the spongy tissue in the glans. As the pelvic urethra leaves the pelvic cavity and enters the bulb of the penis, it becomes surrounded by spongy tissue. The spongy or penile urethra ends in an external opening located at the tip of the gland. Erection is induced by tactile stimulation of the genital region or from visual or emotive stimuli that can stimulate descending parasympathetic pathways from the brain. This type of stimulation induces dilatation of arterioles in the penis (via the helicin arteries) and the venous sinuses. As these erectile bodies are surrounded by a strong fibrous coat, the penis becomes rigid, elongated and increases in girth. Contraction of ischiocavernosus and bulbospongiosus muscles over the root of the penis compresses the venous outflow against the sciatic arch without compromising the arterial supply. At the same time, parasympathetic nerves stimulate the bulbourethral glands to produce a mucoid-like substance to aid lubrication. Emission involves contractions of the smooth muscle in the walls of the deferent duct that push sperm in to the proximal part of the urethra. At the same time, the seminal vesicles and prostate gland contract and seminal fluid is released in to the urethra. At ejaculation, the semen is expelled from the posterior urethra by contractions of the bulbocavernous and urethral muscles. Passage of semen from the upper part of the urethra and back in to the bladder is normally prevented by sympathetic contraction of the urethral sphincter. Male reproductive tract development and differentiation the sex of an embryo is determined at fertilization by the introduction of an X or Y chromosome from the spermatozoon in to the fertilized egg. However the gonads, in the early stages of development, are of an indifferent type and can potentially develop in to either testis or ovaries [5]. The primordial germ cells, which are to become eggs and sperm, develop in another part of the embryo entirely from the gonads. At the third week, they then migrate through the tissue of the embryo to the gonad. The germ cells remain in this quiescent state until after birth when they resume proliferation, and some 21 Section 1: Mammalian reproductive physiology migrate to the seminiferous tubules of the testis. By the time they arrive, the gonad has prepared itself by becoming male or female. As the testes develop, their hormones elicit the development of the male secondary sex characteristics or male phenotype. In the presence of testosterone, the mesonephric or Wolff duct develops to become the vas deferens and associated structures. Without androgens, the mesonephric duct atrophies and the paramesonephric, or Muller duct, becomes the oviduct and most of the uterus. In the male, the indifferent gonad responds to the effects of the Y chromosome by developing testicular cords which become horseshoe shaped and enclosed within the thickened tunica albugina of the gonad. The free ends of the horseshoes are in contact with the redundant mesonephric duct. Meanwhile, the mesonephric duct continues to develop and forms the epididymis, the vas deferens and the seminal vesicles. Like the gonads, the structures that develop in to the external genitalia are initially identical in males and females. They develop from the same anlagen: the genital or labioscrotal swelling; the genital or urethral folds; the genital tubercle and the urogenital sinus. The development of the external male phenotype requires the actions of testosterone. In a male fetus, the genital swellings migrate and become the scrotum; the urogenital folds enlarge and enclose the penile urethra and corpus spongiosa; the genital tubercle becomes the glans penis; and the urogenital sinus forms the prostate gland. It is not until the last two-thirds of pregnancy that growth of the male fetal external genitalia takes place and descent of the testes in to the scrotal sac is complete. During this period, the ducts are rearranged to pass from the scrotum back in to the abdominal wall, through the inguinal canal, to unite with the urethra, the terminal duct of the excretory system (refer to Chapter 2). In humans, the entire spermatogenic process is very long and lasts more than 70 days. This complex process is initiated in the male testis at the beginning of puberty, since germ cell proliferation and survival depends upon gonadotrophin-dependent mechanisms [7, 8]. Germ cells multiply first by repeated mitotic divisions and then by meiosis, which involves the duplication of chromosomes, genetic recombination and then reduction of chromosomes through two cell divisions to produce spherical haploid spermatids. The transformation of spherical, haploid spermatids in to elongate, highly condensed and mature sperm that are released in to the seminiferous tubule lumen is called spermiogenesis.
Buy metformin 500 mg lowest price
This permits extensive collaboration between clinical and academic staff on such matters as clinical Communication among workers It is essential to have a system in place to permit efficient and timely communication to all laboratory staff and students diabetes insipidus in dogs prognosis buy generic metformin 850mg on line. Electronic mail is a good way of disseminating important information to everyone, for example, the notification of obligatory meetings and routine service updates. However, regular face-to-face meetings should be compulsory for all managerial, research and technical staff to allow discussion of regulatory changes, ethical requirements, critical laboratory issues such as laboratory cleanliness and safety, Textbook of Clinical Embryology, ed. All embryologists must possess good verbal communication skills to be able to discuss clinical matters with patients and to present results to colleagues. An understanding of administrative procedures is also essential as standardized and highly detailed forms need to be completed by embryologists in the course of their work. White boards in each section of a laboratory are a good way of communicating local information, for example, items that need to be ordered, holiday planning and notification of damaged equipment. It may be more efficient to display information referring to apparatus on the machine itself if there is more than one piece of identical equipment in the laboratory. If unique machines are non-operational, then an email to all personnel may be better. Safety procedures 220 Consideration of safety, for oneself and other laboratory staff, is essential. Many factors have to be taken in to account, as an individual can easily put herself and/or others at risk if safety protocols are not followed. Both long- and short-term work must be considered when creating safety protocols, including the expansion of laboratory work and research teams. Safety policies should be given to any new employee or student before they commence laboratory work and should include instructions on how to proceed in case of fire, where to obtain first aid, waste disposal protocols, health check requirements and how to report accidents. Each individual should be aware of all laboratory policies, their own safety responsibilities, and should understand how specific policies work within the laboratory. Failing to follow the policies of the workplace could be hazardous but could also drastically reduce the productivity of the laboratory. Each procedure in a workplace must be risk assessed, which means that all potential hazards have been assessed and a written record (Risk Assessment Form) created that identifies each risk and the controls necessary to mitigate these risks. The health and safety executive provides guidance of how to assess risks in a workplace [1]. Colour-coded outfits are sometimes used to distinguish staff, for example to identify nurses from embryologists and technicians. For certain duties, disposable laboratory garments may be available, such as when handling blood. In these cases a plastic apron should be worn on top of the laboratory dress code which will prevent spoilage in the case of spillage. Laboratory garments are usually laundered by specialist external companies hired by the unit, and replaced when worn out or damaged. Sensible footwear must be worn at all times and embryologists have specific laboratory shoes or overshoes to wear whenever in regulated clinical areas. Eye injuries can occur in laboratories and it is often compulsory to wear safety glasses when the procedures being undertaken involve splashing. Face visors are also used when necessary, for example, when dispensing liquid nitrogen (N2). Various types of laboratory gloves must be used depending on the task at hand, for example heatresistant gloves, ultra-cold gloves and latex gloves for everyday procedures. It is becoming increasingly common for laboratories to use specialized hypoallergenic gloves, to prevent allergic reactions to latex gloves. Consequently, most laboratories now use latex-free gloves made from nitrile products. Labelling bottles, boxes and cupboards is a very good way of preventing inadvertent loss and experimental error. Appropriate signage also promotes efficient economics, since it prevents the overstocking of common laboratory items. For example, unused or infrequently used items may be stored on top shelves, while everyday equipment and goods should be within easy reach of personnel. An organized laboratory will save time for employees and students and will also save money. Dating chemicals and solutions is also essential, as these may eventually lose potency (for example if they are bio- or photo-degradable). Finally, a cluttered lab is potentially dangerous and can be stressful for staff members. For example, boxes and unfiled paper can create trip and fall hazards when stored on the floor; these should be stored on an appropriate shelf, or within an appropriate cupboard or cabinet. Handling laboratory equipment Before workers commence using apparatus in a laboratory, appropriate training must be received and fully understood. Equipment may be delicate, susceptible to damage if improperly used and expensive to replace. Centrifuge techniques Centrifuge techniques are used routinely in embryology labs and permit the separation of particles of different mass and size, for example the separation of dead and motile sperm during gradient sperm preparation. Many types of centrifuge are available on the commercial market, incorporating various sizes and speeds. The most commonly used centrifuges adopt bench-top, micro-, high-speed and ultra-platforms. Different centrifuge systems exert differential g-forces and may possess different types of rotor to accommodate differing tubes and volume capacities, or may be able to operate over a range of temperatures. The type of rotor used is very important and depends upon the specific nature of the laboratory procedure being undertaken. Fixed angle rotors Signage/labelling in a laboratory Signage is a very important part of laboratory safety as it alerts laboratory users and visitors of specific hazards in various locations within a building. However, it should be noted that signage does not replace basic laboratory training. As well as being useful for hazard warnings, signs can also be an omnipresent reminder for permanent staff. Signs are an extremely useful part of everyday life, although a laboratory should not become overcrowded as may result in confusion. However, these rotors may cause damage to separated particles as they are forced down the side of the tube. Swinging bucket rotors are very versatile since they can accommodate tubes of many different shapes and have a much gentler effect upon the separated particles. However, these rotors have many more moving parts and are generally slower than fixed angle centrifuges. Before a centrifuge can be operated, an appropriate counterweight must be used to balance the mass of the sample and sample tube, and the rotor cover should be closed. For individual protocols, the g-force unit is generally used and may be calculated from rpm as follows: g = 1. Small volumes of liquid can be sterilized by passing through micro-filters attached to a syringe. Clinical embryologists may, therefore, be exposed to fluids that could be infected. Direct exposure often occurs as a result of accidents involving sharp instruments, via open wounds and splashes to the face. Therefore, it is important to apply strict hygiene practice in the workplace and to cover any existing wounds by application of first aid before working with specimens. Eating and drinking are prohibited in the laboratory, and the potential risk for contamination is reduced by having a vigorous decontamination policy in place. Aseptic techniques are used to maintain the absence of pathogens in the clinical setting, thereby protecting both patients and workers. Decontamination and disinfection in the laboratory Sterilization is used to destroy microbial life. Autoclaves kill bacteria, viruses, fungi, spores and work by applying steam under pressure. Not everything may be sterilized in an autoclave and care must be taken to ensure that materials destined for autoclave sterilization can withstand the extreme temperature and steam.
Buy discount metformin 500mg on-line
Radical nephrectomy remains an option when nephron-sparing surgery is not technically feasible or advisable diabetes prevention activities order on line metformin. The guidelines recommend consideration of active surveillance for patients with decreased life expectancy or extensive comorbidities that make them high risk for other management strategies. What is the reported average growth rate of small,4 cm, renal tumors during active surveillance The growth rate of small, 4 cm, renal tumors during active surveillance is approximately 3 mm per year. What is the reported rate of metastatic progression during the active surveillance of small,4 cm, renal tumor The reported rate of metastatic progression is 1% to 2% during follow-up ranging from 3 to 5 years. True/False: Renal tumor biopsy should always be performed prior to thermal ablation. Intraoperatively, what maneuver is recommended prior to proceeding with a partial nephrectomy Ipsilateral multifocal disease is noted in up to 5% of patients at the time of nephrectomy. Patients have abnormal liver function tests, fever, and hepatic necrosis, which typically resolve after nephrectomy. Osteolytic bone metastasis or paraneoplastic syndrome frequently cause hypercalcemia. The presence of a varicocele, leg edema, deep vein thrombosis, recurrent pulmonary emboli, and caput medusae are reported manifestations but are found infrequently. A high index of suspicion for patients with larger, centrally located tumors is an important finding. When vascularized, parasitized vessels from the renal artery typically feed the tumor thrombus. Wilms tumor, transitional cell carcinoma, sarcoma, lymphomas, primitive neuroectodermal tumors, adrenal cortical carcinoma, testis tumors, and pheochromocytoma. Results of a randomized trial did not demonstrate a benefit of routine lymphadenopathy at the time of nephrectomy. For this reason, lymphadenectomy is reserved for select cases with increased risk of lymph node involvement. Ipsilateral adrenalectomy at the time of nephrectomy is recommended only in cases with radiographic adrenal enlargement or in cases when the tumor located immediately adjacent to the adrenal gland. The most common sites are the lung, bone, lymph nodes, liver, adrenal glands, brain, heart, spleen, and skin. Number of risk factors are used to categorize risk (0 low risk, 1-2 intermediate risk, 3 high risk). Cytoreductive nephrectomy can be completed prior to the systemic therapy, for palliation, in conjunction with resection of select solitary metastasis and prior to the initiation of systemic therapy. In fact, randomized series have demonstrated a significant increase in survival in patients undergoing cytoreductive nephrectomy prior to cytokine therapy compared to patients not undergoing nephrectomy. What is the role of cytoreductive nephrectomy for patients who are to be treated with tyrosine kinase inhibitors The role of cytoreductive nephrectomy prior to the use of tyrosine kinase inhibitors for metastatic renal cancer is unknown. The routine use of cytoreductive nephrectomy in this population is based on the data evaluating cytokine therapy and that the majority of patients enrolled in trials evaluating the efficacy of tyrosine kinase inhibitors having undergone nephrectomy prior to treatment. Nephrectomy in conjunction with resection of a solitary pulmonary metastasis has yielded 5-year survival rates of 30% to 35%. Since the introduction of targeted therapy, the use of immunotherapy has decreased significantly. Which receptors are targeted by the tyrosine inhibitors approved for metastatic renal cancer What is the proposed mechanism of action of tyrosine kinase inhibitors for treating metastatic renal cancer Anemia, fatigue, stomatitis, hyperglycemia, dyspnea, pain, infection, rash, edema, and hyperlipidemia. Hand-and-foot syndrome, rash, mucositis/stomatitis, hypertension, neutropenia, hypophosphatemia, anemia, fatigue, hypothyroidism, and diarrhea. True/False: Tyrosine kinase inhibitors have been associated with hypothyroidism during the treatment of metastatic renal cancer. Hypothyroidism has been noted in 21% to 84% of patients treated with tyrosine kinase inhibitors. Leiomyosarcoma accounts for 60% of renal sarcomas and is best treated with surgical removal. Other less common tumors include osteogenic sarcoma, liposarcoma, carcinosarcoma, fibrosarcoma, rhabdomyosarcoma of adults, and malignant fibrous histiocytoma. These are extremely rare, profusely vascular benign tumors that not uncommonly are difficult to locate because of the small size. Patients typically present with severe hypertension, polydipsia, polyuria, myalgia, and headaches. A partial nephrectomy should be considered if the diagnosis is made preoperatively. True/False: Patients with juxtaglomerular cell tumors typically have hyperkalemia. At autopsy, what percentage of hematologic malignancies will have renal involvement Usually hematologic malignancies appear in the kidney as part of the systemic disease process. Besides hematologic malignancies, where are the sites of primary tumors that metastasize to the kidney Lung cancer (squamous cell) frequently metastasizes to the kidney as well as breast cancer and uterine cancer. Angiomyolipoma (hamartoma) have been reported to occur in the bone, heart, lung, brain, and eye. Lesions larger than 4 cm are at increased risk for hematuria, spontaneous rupture, retroperitoneal bleeding, pain, and possibly fever. Asymptomatic patients with small tumors are often followed with serial imaging unless renal function decreases or tumor diameter increases. What is the most common solid enhancing benign renal tumor larger than 1 cm in diameter The abundant mitochondria are responsible for the eosinophilic cytoplasm seen in the polygonal, uniform cells of oncocytomas. Oncocytomas are characterized by loss of the Y chromosome and translocations involving the long arm of chromosome 1. What are the classic radiographic signs associated with the appearance of oncocytomas Oncocytomas are also sharply demarcated, with no calcification, and isodense with a homogeneous pattern of enhancement. Oncocytomas have also been reported in the parathyroid and thyroid glands, salivary glands, and the adrenal glands. True/False: Wilms tumor in adults is typically associated with a better prognosis than presence of Wilms tumor in children. Furthermore, adults typically present with a more advanced stage compared to children. The incidence of Wilms tumor in horseshoe kidneys, however, is much higher than normal kidneys. In patients with unexplained bone pain or elevated serum alkaline phosphatase levels. Approximately one-third will have metastatic disease when their cancer is first diagnosed. The incidence of adrenal metastases at the time of nephrectomy for renal cell cancer is just under 4%. Reports indicate that the prognosis for these cases is generally poor regardless of whether or not an adrenalectomy is done. This suggests that there may be little therapeutic benefit in performing a simultaneous adrenalectomy. During a laparoscopic nephrectomy, the patient develops sudden hypotension and a new "mill-wheel" cardiac murmer is detected. The earliest sign of this entity is an extremely rapid and sudden decrease in end-tidal carbon dioxide, which literally happens in a matter of seconds. This is why all laparoscopic cases should be appropriately monitored for carbon dioxide. Severe hypotension, development of the typical mill-wheel cardiac murmer, and a rapid decline in oxygen saturation occur somewhat later and are associated with a poorer prognosis. Treatment involves immediate removal of carbon dioxide gas from the abdomen and placing the patient in a steep left lateral decubitus/Trendelenburg position to minimize any right ventricular outlet obstruction. Following a partial nephrectomy, a patient develops increased output from their flank drain after their Foley catheter was removed. Urine leak following partial nephrectomy is best managed with Foley catheter drainage. Repeat surgical exploration should not be performed and is associated with the risk of completion nephrectomy. Five days following a partial nephrectomy a patient develops gross hematuria, flank pain, and hypotension.
Syndromes
- Vomiting
- There is any persistent, unexplained nasal flaring, especially in a young child.
- American Heart Association - www.americanheart.org
- Have any other family members had an unusual-shaped chest?
- Anorexia nervosa - resources
- Joint pain
- Nephrocalcinosis
- "Red eye" glow of the pupil is missing in photos, or is different between the two eyes
- Medications to treat symptoms
Purchase metformin 500 mg with mastercard
Paired-greater and lesser sciatic foramina diabetes symptoms wikihow buy metformin with visa, obturator foramina; nonpaired-pelvic inlet and pelvic outlet. What structures are found in Alcock canal and what is another name for Alcock canal The pudendal (Alcock) canal runs approximately 4 cm above the lower ridge of ischial tuberosity and contains the pudendal artery, pudendal veins, and the pudendal nerve; all are invested in connective tissue, binding these structures to the perineal surface of the obturator internus fascia. One must be cautious during ligation and division of the dorsal venous complex, as damage to the striated sphincter can occur. What anatomic reason may account for the relatively higher incidence of axial skeletal and pelvic bone metastases in patients with metastatic prostate cancer, as opposed to lung metastases for example There are numerous interconnections between the pelvic venous plexuses and the emissary veins of the pelvic bones and vertebral venous plexuses, which may be routes of dissemination of infection or tumor from the diseased prostate. What artery has its origin off the inferior epigastric artery and can be identified medial to the femoral vein during pelvic surgery The accessory obturator artery arises from the inferior epigastric artery in 25% of patients and continues on through the obturator canal. Following a radical dissection of inguinal lymph nodes for penile carcinoma, the surgeon decided to cover the area with a rectus myocutaneous flap. The middle rectal artery anastomoses with the superior and inferior rectal arteries to supply the rectum. It also gives small branches to provide additional arterial supply to the seminal vesicles and prostate. What accessory vein drains in to the inferior surface of the external iliac vein in at least 50% of patients Care must be taken to not tear this vein at the time of pelvic lymph node dissection. True/False: Intramural longitudinal vessels run the length of the ureter in 75% of patients. In the other 25% of patients, the intramural ureteral vessels form a fine interconnecting mesh with less collateral flow and render the ureter more prone to ischemic insult. This intramural, interconnecting meshlike vascular pattern is often found in the pelvic ureter, and therefore, this portion of the ureter is less suited for ureteroureterostomy. What is one of the main reasons that the primary repair of the pelvic ureter is often prone to strictures The blood supply of the pelvic ureter is based on longitudinal collaterals that run along it, which are often severed following both the primary injury to the ureter and subsequent mobilization during its repair, thus limiting its blood supply with a high risk for ischemic strictures. In a normal adult male, at what anatomic location are the ureters closest to each other The ureters are closest and are located within 5 cm of each other as they cross the iliac vessels. What is the principal arterial supply to prostatic adenomas in benign prostatic hyperplasia and where are the origin and principal branches of the prostatic artery The inferior vesical arteries have urethral artery branches that enter the prostate posterolaterally at its junction with the bladder and these branches are the principal arterial supply to the adenomas. The short segment at the end of the inferior vesical artery after all the branches to the bladder but before the bifurcation between the capsular and urethral branches is called the prostatic artery. When an accessory pudendal artery is present and is supplementing or replacing the penile arterial supply by the common penile artery, what is its origin An accessory pudendal artery is present in approximately 4% of patients undergoing a radical retropubic prostatectomy and arises from the inferior vesical artery, superior vesical artery, and obturator artery. The internal pudendal artery in the male lies anterior to the piriformis muscle, sacral plexus of nerves, and the inferior gluteal artery. As it crosses the ischial spine, it is covered by the gluteus maximus muscle and overlapped by the sacrotuberous ligament. The pudendal nerve is medial to the artery while the nerve to the obturator internus muscle is lateral to the internal pudendal artery. The aorta gives rise to 2 common iliac arteries at the level of 4th lumbar vertebra. What artery arises posteriorly at the level of the aortic bifurcation and what does it supply It is the middle sacral artery and it supplies the sacral foramina and the rectum. The posterior trunk gives rise to 3 parietal branches: the superior gluteal, the ascending lumbar, and the lateral sacral branches. The anterior trunk gives rise to 7 branches: the superior vesical, the middle rectal, the inferior vesical, the uterine, the internal pudendal, the obturator, and the inferior gluteal branches. What are the sources of collateral blood supply to the pelvic organs in the case of bilateral ligation of the internal iliac arteries due to massive hemorrhage Aortic branches (middle sacral and lumbar arteries) and inferior mesenteric branches (inferior mesenteric artery). True/False: In a nerve-sparing cystoprostatectomy, the unilateral internal iliac artery should be ligated and divided to improve hemostasis and facilitate the nerve-sparing procedure, thereby possibly maintaining erectile function. The internal iliac artery should be preserved and the superior vesical artery should be ligated and divided proximally in order to maintain the integrity of the internal pudendal artery and to prevent vasculogenic erectile dysfunction. The superficial circumflex iliac, external pudendal, and superficial inferior epigastric vessels. At what anatomic site does the internal iliac artery branch in to its anterior and posterior trunks It can arise from the anterior trunk of the internal iliac artery, the inferior epigastric artery, or the inferior gluteal artery. The iliac branches ascend in the iliac fossa and supply the iliacus muscle and ilium, while anastomosing with branches of the iliolumbar artery. The pubic branch arises from the obturator artery just before it leaves the pelvis and ascends inside the pelvis to communicate with the same vessel on the contralateral side and with the inferior epigastric vessels. These arteries are derived from the middle vesical, inferior vesical, and middle rectal arteries. The venous drainage occurs by means of the vaginal plexus of veins along the lateral aspect of the vagina. The vaginal plexuses are drained by 1 or 2 vaginal veins on each side that flow in to the internal iliac veins either directly or through the connections with the internal pudendal veins. These include arterial branches that can arise from the uterine artery, inferior vesical artery, or separate arterial branches directly from the anterior trunk of the internal iliac artery. In what percentage of patients undergoing radical retropubic prostatectomy does the superficial dorsal vein of the penis appear to be absent During a radical cystectomy and pelvic lymph node dissection, care should be taken to avoid dissection below the presacral fascia. What life-threatening complication can occur while dissecting posterior to the rectum Damage to the presacral venous plexus can be massive and very difficult to control. True/False: the external iliac lymph nodes can be further separated anatomically and functionally in to 3 chains. For example, the external chain does not receive any lymphatic drainage from organs within the pelvis and these lymph nodes are located lateral to the external iliac vessels. The lymph node of Cloquet lies within the femoral canal, medial to the external iliac vein, and beneath the inguinal ligament. How many external iliac lymph nodes are usually present in the normal adult and what is their anatomic arrangement There are usually 8 to 10 external iliac lymph nodes that lie along the external iliac vessels. One group is on the lateral aspect, another on the medial aspect, and a third group on the anterior aspect of the external iliac vessels. The third group of lymph nodes on the anterior aspect of the vessels is sometimes absent. The external and internal iliac nodes, obturator nodes, para-aortic nodes (accompanying the drainage of ovary), and superficial inguinal nodes (through round ligament). How does a previous inguinal surgery (ie, orchiopexy) influence the possible distribution of metastatic disease in testicular cancer It can alter the lymphatic drainage, hence allowing additional routes for lymphogenic spread, for example to inguinal, iliac, and obturator lymph nodes. The sutures should be placed in the direction of the muscle fibers and femoral nerve to avoid femoral nerve entrapment or damage due to the nerve passing within the substance of the psoas muscle. Caution must also be taken with retractor blades on the psoas muscle for prolonged periods, as this may also cause a femoral nerve palsy affecting ipsilateral knee extension. During a radical cystectomy in a 65-year-old male patient for clinical T3a transitional cell carcinoma of the bladder, you notice a nerve visible on the surface of the right psoas major muscle has been damaged by an electrosurgical injury. Which nerve is this and what sensory loss do you anticipate this patient may experience if the nerve function cannot be salvaged Sensory loss to the anterior right thigh below the inguinal ligament and the anterior right hemiscrotum may occur. During a sacrospinous colposuspension, which nerve or nerve plexus is at relatively high risk of injury The risk of injury is to the sacral plexus, as it leaves the pelvis via the greater sciatic foramen and is immediately posterior to the sacrospinous ligament. If injured, there may be sensory and motor nerve supply compromise to the posterior thigh and lower leg. The sacral plexus is located on the surface of the piriformis muscle, deep to the endopelvic fascia, and posterior to the internal iliac vessels. What are the anatomic relations of the communicating nerve fibers of the left and right components of the pelvic plexus These fibers communicate posterior to the rectum, as well as anterior and posterior to the bladder neck. True/False: There is no pelvic parasympathetic efferent innervation to the descending and sigmoid colon. Some pelvic parasympathetic efferent fibers travel up the hypogastric nerves to the inferior mesenteric plexus, where they will subsequently provide innervation to the descending and sigmoid colon. True/False: the pelvic ureter has rich adrenergic and cholinergic autonomic nerve supply and will lose its peristaltic activity if it is denervated. The ureter will continue to have peristaltic activity despite its pelvic denervation. True/False: Bilateral pudendal nerve injury will cause loss of striated external sphincter function at the level of the membranous urethra.
Buy metformin 500 mg with visa
When a classic metaphyseal lesion is suspected diabetes support groups cheap 850 mg metformin with mastercard, two radiographic projections of the affected joint are required to avoid confusion with mild physiologic irregularity of the metaphysis or chronic stress such as in malignancy [4]. Metaphyseal fractures of child abuse are most commonly encountered around the knee or elbow. Rib fractures due to abuse can occur anywhere in the ribs, but are most commonly detected posteromedially adjacent to the costovertebral junction and rib head [5]. The routine addition of oblique views of the chest increases the diagnostic accuracy for acute rib fractures [6]. Other pediatric fractures that are highly specific for abuse include scapular, spinous process, and sternal fractures. Fractures in children that have moderate specificity for abuse include vertebral fractures, digital fractures, and bilateral synchronous fractures. Other clues which should raise the suspicion of child abuse include occult or unexpected fractures, multiplicity of fractures, injuries that are out of proportion to the given history, and multisystem injuries. By 16 years of age, approximately onethird of children will have had at least one fracture. There is an inverse relation between the age of the child and rate of nonaccidental fractures. Therefore, the risk of non-accidental injury is the highest in a child under 3 years with a rib or long bone fracture, including the humerus and femur [3]. However, long bone fractures in non-ambulating young children/infants are suspicious. Rib fractures in infants and young children can be due to osteogenesis imperfecta, birth trauma, or long-term ventilator therapy in prematurity. Leukemia, round cell tumors, or metabolic bone disease (rickets, scurvy) may mimic child abuse. Osteogenesis imperfecta results in brittle bones and can lead to multiple fractures of different ages. Importance Skeletal injuries are often the strongest indicators for child abuse and are detected in up to 55% of young children who have been abused [7]. Most of these children are younger than 3 years old and subsequently, clinical history as well as interpretation of symptoms is usually unreliable. If appendicular findings are equivocal for child abuse, additional projections of the bone or joint in question should be obtained. Oblique views of the chest increase diagnostic accuracy for the detection of rib fractures. If skeletal injuries are out of proportion to the history, the suspicion of child abuse should be raised. Which radiological investigations should be performed to identify fractures in suspected child abuse Sport and recreation-related injuries and fracture occurrence among emergency department attendees: implications for exercise prescription and injury prevention. There is a thin rim of calcification connecting the metaphyseal corners (small arrows), resulting in the "bucket-handle" appearance of this classic metaphyseal lesion, which is near pathognomonic for child abuse. At our institution, the imaging protocol for skeletal survey radiographs only includes frontal projections of the extremities, which are reviewed by a radiologist while the patient is still in the department. The subsequently obtained lateral view (B) of the left femur confirms the findings (black arrows). On the contralateral right anterior-posterior femur radiograph (C) a similar metaphyseal corner lesion (whitearrows) and mild periosteal reaction (white arrowhead) are detected. There are acute fractures of the left sixth through eighth ribs (large black arrows) without periosteal reaction. Cortical disruption and mild angulation without periosteal reaction indicate subtle acute right posterior ninth and tenth rib fractures (small white arrows). Additional posteromedial left rib fractures with exuberant callus formation (small black arrows), which appear more bulbous, are indicative of older injury. Section 1 Chapter Mammalian reproductive physiology 1 Sexual reproduction: an overview Suzannah A. Williams Introduction Reproduction is the production of offspring, propagating genes in to the next generation, and exists in many forms within the animal kingdom. Each of these different strategies has advantages and disadvantages, but all strategies have evolved as the optimum for a particular species in a particular niche. Of these individuals, some will be better adapted to exist in the surrounding environment than others, and these better suited individuals are most likely to be more successful. These stages include the production of functional gametes, appropriate behaviour to ensure the released gametes interact, a suitable environment for implantation and subsequent embryo development, birth to occur in to a suitable environment and also for appropriate lactation to ensure the newborn is adequately provided for. Failure at any of these earlier stages can result in infertility ultimately failing to produce viable offspring, and in the worst case, threatens the life of the mother and of the fetus or newborn(s). Understanding how each of these events is regulated is critical for furthering our ability to influence these processes. This is critical not only to assist people who are unable to conceive naturally to have children, but also for other purposes such as to aid fertility in endangered species and to maximize reproduction for food production. Although the focus in this textbook is on the mechanisms of reproduction in humans, there are numerous insights to be drawn from investigating reproductive strategies in other species. Gamete generation and selection the production of gametes for reproduction requires, in the case of the male, sperm that are mobile and functional, and in the female, the ovulation of an egg that is effectively the best of all those developing in the ovary. Millions of spermatozoa are produced by each male on a daily basis, calculated at 1000 per second in the human [1], however the number of sperm that actually reach the site of fertilization is understood to be remarkably low, with only one spermatozoa actually required for fertilization. Therefore, the vast majority of male gametes are unsuccessful in the pursuit of reproduction. Whereas in women, selection occurs in the ovary by a variety of mechanisms with several follicles growing but ultimately only one egg is ovulated in the vast majority of cases. This is key to fully understand ovarian function and fertility regulation in all species including humans. It is not yet known how the egg that is selected for ovulation in a normal cycle differs to those that undergo atresia and die. Therefore, furthering our understanding of ovulation rate and the mechanisms that regulate it are critical to developing more natural ways of obtaining eggs and to enhancing our selection of the best eggs. It is clear that there is considerable wastage of potential female gametes, primarily due to the considerable numbers of oocytes that are generated and develop compared to the very low number ovulated. Indeed, females generate approximately 7 million primordial germ cells [3] (discussed further in Chapter 6) and ovulate around 400 before undergoing menopause at approximately 50 years of age in Western women. An alternative way to think about it is that to select the finest, you need to have a heterogeneous pool to select from. Perhaps, rather than perceive this loss of oocytes as wastage, we should view it as selection. Therefore the generation of a pool of oocytes for each cycle is required so that the most appropriate can be selected. In addition to sperm selection within the female reproductive tract where the sperm that fertilizes has good forward motility and is headed in the right direction at the outset, there is good evidence for elimination of many genetically or otherwise abnormal sperm via cell cycle checkpoints and apoptosis. Anyone who has added sperm to eggs in culture will have observed that an overwhelming number of sperm bind to the eggs. Recently progesterone has been found to have sperm-attracting properties [4] although this may not be the only factor involved. The distance that sperm need to cover to reach the fertilization site in the fallopian tube is considerable, taking in to account the size of the sperm. For many years the sperm was considered to be propelled forward by the tail moving in a side-to-side whiplash motion; however we now know that the tail drives the sperm forward by a corkscrew action. Calculations of the time it takes sperm to travel the distance have revealed that other mechanisms exist to carry the sperm to the fertilization site, including fluid flow to the oviduct. Other species have evolved novel mechanisms for sperm transport in the female tract. For instance the sperm head of the common wood mouse is hookshaped, and these hooks attach to one another forming trains. The hook-shaped head is a characteristic of rodent sperm and the specific shape of this hook affects how the heads are able to join and interact. Furthermore, these trains also contain sacrificial sperm, which sacrifice their acrosome to join the train, thereby rending them unable to fertilize the egg [5].
Generic metformin 500mg on-line
In addition diabetes medications covered by medicare purchase generic metformin on line, it allows placement of the urethra deep within the pelvic ring, enhancing bladder outlet resistance. Finally, it brings the large pelvic floor muscles near the midline, where they can support the bladder neck and aid in eventual urinary control. Why is the combined anterior osteotomy preferred to the classic posterior osteotomy Besides the ease of approximation, combined osteotomy was developed for 3 reasons: 1. Osteotomy is performed with the patient in the supine position, as is the urological repair, thereby avoiding the need to turn the patient. The anterior approach to this osteotomy allows placement of an external fixator device and intrafragmentary pins under direct vision. The cosmetic appearance of this osteotomy is superior to that resulting from the posterior iliac approach. When good callus formation is seen on radiography, the fixation device and pins are removed with the patient under light sedation. Ideally, waiting for the bladder template to grow for 4 to 6 months in the child with a small bladder is not as risky as submitting a small bladder template to closure in an inappropriate setting. This may result in dehiscence and allows the fate of the bladder to be sealed at that point. Proper management is to begin long-term antibiotic therapy to control the infections. It may also be necessary to dilate the urethra or to begin intermittent catheterization. Combined closure of exstrophy and epispadias repair is considered in patients who have had closure surgery delayed beyond the newborn period or in patients in whom the initial newborn closure fails. The primary goal of these procedures is urinary continence, which is defined as a 3-hour dry interval. If this is not achieved within 2 years after bladder neck reconstruction, failure to achieve continence has resulted. What is the innervation pattern of the corporal bodies and bladder in cloacal exstrophy patients Enervation to the duplicated corporal bodies arises from the sacral plexus, travels through the midline, perforates the interior portion of the pelvic floor, and courses medially to the hemibladders. What is the rate of occurrence of intestinal tract abnormalities in cloacal exstrophy Omphalocele was reported to occur between 88% and 100% of cases, with most studies reporting omphalocele in more than 95% of cases. The ureterovesical junction is inherently deficient in complete epispadias, and the incidence of reflux has been reported to be between 30% and 40%. The objectives of repair of penopubic epispadias include achievement of urinary continence with preservation of the upper urinary tract and the reconstruction of cosmetically acceptable genitalia. The term megacystis is often used to describe any condition leading to a distended fetal bladder in utero, without referring to the cause of the dilation. How sensitive is prenatal ultrasound in the diagnosis of posterior urethral valves Ultrasonography is sensitive in detecting fetal hydronephrosis, but the specific diagnosis of posterior urethral valves is more difficult. Nonetheless, a thickened bladder and a dilated posterior urethra are suggestive of posterior urethral valves. In general, endoscopic primary ablation is the preferred surgical procedure to treat posterior urethral valves. Vesicostomy is reserved for very small infants if the endoscopic equipment is too large for safe intervention. What are the prognostic indicators of future renal function in patients with posterior urethral valves There are 4 basic predictors of renal function in patients with posterior urethral valves: ultrasound appearance, serum chemistries, age at diagnosis, and presence of reflux. Nocturnal polyuria can be either absolute, which is usually associated with a derangement of the circadian rhythm of antidiuretic hormone secretion, or relative, mainly due to a reduced functional bladder capacity during sleep at night. Hypospadias, in boys, is defined as a group of 3 anomalies of the penis: (1) an abnormal ventral opening of the urethral meatus that may be located anywhere from the ventral aspect of the glans penis to the perineum, (2) an abnormal ventral curvature of the penis (chordee), and (3) an abnormal distribution of foreskin with a "hood" present dorsally and deficient foreskin ventrally. These include (1) abnormal development of the urethral plate; (2) abnormal, fibrotic mesenchymal tissue at the urethral meatus; and (3) corporal disproportion or differential growth of normal dorsal corpora cavernosal tissue and abnormal corporal tissue ventrally. The theory is that the chemical burden in the mother affects her endocrine function. Approximately 75% of cryptorchid testes will spontaneously descend, usually by 3 months of age. What is the risk for an undescended testis in a newborn male if a family member is already affected Although biopsy findings from children with unilateral cryptorchidism typically demonstrate reduced total germ cell counts, paternity has been found to be significantly compromised in men with previous bilateral, but not unilateral cryptorchidism. The higher the position of the undescended testes, the greater the risk of developing malignancy. Almost half the tumors that develop from undescended testes occur in testes located abdominally, 6-fold higher than for inguinal testes. Radiologic testing does not have a relevant role in the assessment of undescended testes and should not influence surgical management. Bilateral nonpalpable testes warrant immediate assessment in the newborn period to determine the presence or absence of testes and to rule out an intersex state. Surgical intervention on an undescended testis should optimally be performed between 6 and 12 months of age. Viable testicular elements will be present in up to 13% of testicular remnants/nubbins and should therefore be removed. Potter syndrome, or Potter sequence, is a series of changes that occur in a fetus secondary to extreme oligohydramnios. This can be from an inability to produce urine such as renal agenesis, bilateral multicystic renal dysplasia, or juvenile polycystic kidneys. Another reason for oligohydramnios is an impaired ability to void such as posterior urethral valves. In approximately one-third of these cases, upper tract anomalies can also be found. These include renal agenesis or hypoplasia, renal ectopia, pelvic kidney, and horseshoe kidney. Although Type B has been deemed "atypical," it is actually more common than Type A. Patients found to have a missing vas deferens during an infertility workup should be screened for what abnormality and how However, contralateral reflux is found in one-third of children with renal agenesis and is not uncommon in patients with multicystic dysplastic kidney. What is the most common additional urologic abnormality associated with a horseshoe kidney The incidence of horseshoe kidney is 1:400 to 1:1800 with a male predominance of 2:1. Up to 35% of patients with a horseshoe kidney have evidence of significant ureteropelvic junction obstruction, more commonly on the left. It is unclear at this time if there is an increased risk of adult urologic cancers in fused kidneys; however, some studies demonstrate an increased risk of transitional cell carcinoma in these patients. What is the normal direction of rotation of the human kidney as it ascends out of the pelvis Therefore, the renal pelvis, which was originally directed anteriorly, becomes directed medially. Approximately 90% of crossed ectopic kidneys are fused with a normally placed mate. Ureteropelvic junction obstructions are the etiology of 60% to 80% of cases of persistent fetal hydronephrosis. True/False: Most cases of prenatally diagnosed ureteropelvic junction obstruction require urgent surgical intervention following delivery. Debate continues surrounding the management of prenatally diagnosed ureteropelvic junction obstructions. Most often surgery is not necessary or can be performed on an elective basis after an appropriate evaluation and period of observation. In patients found to have ureteropelvic junction obstruction, evidence for bilateral obstruction exists in 10% to 40% of cases. In what percent of patients with ureteropelvic junction obstruction does vesicoureteral reflux coexist Duplex system, agenesis, or ectopia can also been seen in the contralateral kidney. What is the average amount of renal parenchyma drained by the upper pole of a duplicated collecting system About one-third of total renal parenchyma is drained by the upper pole of a duplicated collecting system. A ureteric bud arising on the mesonephric duct in an abnormally low position predisposes to what abnormality What can happen if the ureteral bud originates significantly higher than normal on the mesonephric duct The ureter may not incorporate in to the bladder and instead open in to the urethra or other mesonephric remnants. In the male, an ectopic ureter can end in the epididymis, vas, or seminal vesicle. Because the ectopic ureter always ends above the external urinary sphincter in a male, incontinence is typically not an issue.
Metformin 850mg low cost
Estrogen levels drop due to reduction in follicle number and qualitative effect on granulosa cell aging blood sugar 250 cheap 850mg metformin visa. There is a permanent cessation of progesterone production which can lead to endometrial proliferation and hyperplasia. Menopause is usually defined retrospectively, one year after the last menstrual period (average age 51). Ovarian androstenedione production drops by half in menopause so that the majority is from the adrenals (1:4 ratio). The main source of post-menopausal estrogen is estrone, produced mainly in peripheral adipose tissue and the post-menopausal ovary by aromatization of adrenal androstenedione. Glucocorticoid administration in post-menopausal patients will suppress estrogen 75 Section 1: Mammalian reproductive physiology production, confirming that it is from an adrenal production site. This change results in increased central adiposity (android rather than gynecoid shape) and a decreased lean body mass. Although the hot flush may characteristically start over the face or neck area, it involves the whole body and is often followed by intense sweating, and then by shivering. Hot flushes occur in 70% of Caucasian and Afro-Carribbean women, but are less common in Japanese and Chinese women, possibly due to a cultural mechanism or by a diet rich in isoflavone. It is thought that the mechanism is such that estrogen induces hypothalamic opiod activity, and this loss of activity can then lead to thermo-dysregulation, mediated by noradrenaline. Estrogen also increases alpha2 adrenergic activity, leading to flushing, and hence the rationale for clonidine therapy. Some trials indicate estrogen improves function as indicated by memory and attention improvements. Urogenital factors Women may experience a number of symptoms arising from the urogenital system around the menopause (Table 8. Most of these symptoms are a result of atrophy of vaginal and urethral epithelium (estrogen receptors) with loss of rugations and stenosis. There is a disturbance of the vaginal flora (decreased lactobacilli, increased faecal flora) and a resultant increase in vaginal pH. In the peri-urethral connective tissue there is also a decreased amount of collagen. It then remains relatively stable until the menopause, after which the loss is lifelong. Factors that can affect the bone mass include genetics/race and diet/calcium during adolescence. Factors affecting bone loss include premature menopause, amenorrhea, exercise/diet/weight, smoking/alcohol/caffeine or the use of corticosteroids. Risk factors affecting the chances of fracture include: low bone mass, low body weight, current cigarette Table 8. The depression that is seen at the menopause is partly due to serotonin and noradrenaline deficit. There is however a rapid increase in risk following the menopause, and cardiovascular disease is now a leading cause of death among postmenopausal women. The study was a randomized controlled trial which enrolled more than 16 000 American women. Acknowledgement the author would like to thank Mr Hamnah Bhatti (University of Oxford Medical School) for assistance in preparing the figures. Further reading Illustrated Textbook of Paediatrics 2d rev edn, by Tom Lissaue and Graham Clayde (Mosby, 2001). Management of the Menopause: the Handbook 4th edn, by Margaret Rees and John Purdie. While the use of techniques such as intracytoplasmic sperm injection has meant that most couples are now able to achieve fertilization, many apparently normal embryos fail to implant. One possible cause for this could be that the mother mounts an abnormal immune response to the implanting embryo. The immune paradox of pregnancy was first recognized by the Nobel Prize-winning immunologist Sir Peter Medawar [1]. As this clearly does not happen in normal pregnancy, he speculated about the mechanisms which might be involved in preventing this rejection. Failure of these protective mechanisms to different extents could potentially lead to the poor placentation seen in preeclampsia, miscarriage and in the worst cases, implantation failure. Medawar put forward three proposals as to how the fetus might avoid maternal immune recognition: (1) There is an anatomical separation of the fetal antigens and maternal immune system such that they never come in contact to elicit a response. These ideas have provided a useful framework for exploring the mechanisms of the feto-maternal immune relationship and will be discussed in this chapter to illustrate our current understanding of the field. There are two distinct placental interfaces which are important at different stages of pregnancy. Interface 1 the first interface is that formed initially between the trophectoderm of the implanting embryo and later the developing placenta in the first trimester of pregnancy, and the overlying maternal decidualized endometrium (decidua basalis). Specialized placental cells called extravillous cytotrophoblast invade from the tips of the anchoring villi in to the decidual stroma (interstitial cytotrophoblast) or in to the lumen of the decidual spiral arteries (endovascular cytotrophoblast) which supply maternal blood to the placenta. The endovascular cytotrophoblasts strip away the endothelium of the spiral arteries and destroy the muscle layer, opening out the arteries to convert them from high-resistance/ low-flow vessels carrying an estimated 45 ml blood per minute to low-resistance/high-flow vessels carrying 750 ml blood at term. This is thought to be a crucial mechanism to increase the blood flow to the placenta to sustain the fetus as it grows and protect the Textbook of Clinical Embryology, ed. Interface 2 the second interface is between the syncytiotrophoblast (the epithelium which covers the surface of the chorionic villi) and the maternal blood, and is established towards the end of the first trimester of pregnancy. This interface is more important in the second half of pregnancy as the placenta grows and comprises a large surface area over which the exchange of gases and nutrients occurs to sustain the developing fetus. Thus, fetal red blood cells and leucocytes can be found in the maternal circulation as early as the first trimester where they can interact with maternal immune cells [3]. It is clear from the above that there is no anatomical separation of placental trophoblast and maternal cells per se. However, the key question is whether the trophoblast that comes in contact with maternal immune cells has the ability to elicit an immune response. Chapter 9: Reproductive immunology Cells of the innate and adaptive immune systems Immune cells fall in to two main groups: those of the innate and adaptive immune systems. The adaptive immune system comprises B cells, which produce antibodies, and T cells of which there are four main types: (1) T helper 1 (Th1) cells which interact with monocytes and macrophages to help them destroy intracellular pathogens, (2) T helper 2 (Th2) cells which interact with B cells to help them divide, differentiate and make antibody, (3) T cytotoxic cells (Tc) which destroy foreign cells or host cells infected with virus or intracellular pathogens, and (4) regulatory T cells (Treg) which are a specialized sub-population of T cells that suppress activation of the immune system and are involved in transplantation tolerance. In early pregnancy up to 40% of the cells in the maternal decidua (interface 1) are immune cells [4]. Their function is also very different in that they have a much lower killing Table 9. They are found in close association with the invasive extravillous cytotrophoblast, suggesting that they play an important role in feto-maternal immune interactions. Do the antigens expressed by the trophoblast differ from those expressed by adult tissues In contrast, the non-classical molecules exhibit a limited polymorphism and their tissue expression is also limited. A Th cell response is therefore generated that eventually leads to the production of antibodies against the same peptide antigen. However, these do not lead as would be expected to the destruction of the trophoblast; on the contrary they facilitate trophoblast invasion and placental development. Together, these promote and regulate trophoblast invasion and angiogenesis in the decidua. It displays a low degree of polymorphism but has a large variety of molecular structures as a result of alternative splicing. Soluble forms can also be generated by proteolytic cleavage of membrane anchored molecules. This raises the question as to how decidual T cells are prevented from destroying invasive extravillous cytotrophoblast cells. This is thought to be mediated through induction of regulatory T cells in the decidua. There is an increase in the numbers of circulating regulatory T cells (Tregs) in the late follicular phase of the menstrual cycle, with a further increase in pregnancy, peaking in the second trimester and declining towards term [12]. Higher numbers of Tregs are found in the decidua compared to the peripheral blood. Several studies have reported that the number of Tregs in both the peripheral blood and decidua are reduced in preeclampsia compared to normal pregnant women [12]. Furthermore, it has been reported that there is a bias towards Th17 cells over Tregs in women with preeclampsia. Clearly there cannot be a blanket immune suppression, as pregnant women would be susceptible to all kinds of infections, and this is not the case.
Order metformin 850 mg with amex
As light passes through different gradients within the sample blood glucose quality control purchase metformin now, light is refracted on to the different areas of the modulator, resulting in difference in contrast and the generation of a threedimensional grey-scale image. This technique offers an excellent resolution of details and generates highcontrast images. This means that the entire depth of the specimen can be viewed in sections in excellent resolution. The modulator placed in the back focal plane of the objective is constructed to have three distinct regions, each with different densities. The two light beams pass through the condenser and the specimen, where their path is altered depending on the reflective index and density of the specimen. These differentially modified light waves are collected by the objective and are transmitted through the second Nomarski prism at the rear focal plane of the objective and the analyzer, where they are recombined. The combined light wave passes through the eyepiece to the observer, generating a shadow-effect image with different light intensity and colour at varied areas of the specimen. Also, it is not suitable for analyzing tissue culture specimens, as the plastic tissue culture dish interferes with the optical system, resulting in misleading images. To carry out these techniques, brightfield stereomicroscopes are the preferred choice, as the low-magnification, threedimensional image generated allows embryologists to orient themselves under the microscope and provide enough space for safe movements of oocytes and embryos within/between dishes [7]. Semen analysis While the accurate manipulation of oocytes and embryos is the major consideration when choosing stereomicroscopes, semen analysis involves a more detailed morphological and structural analysis of spermatozoa. Semen analysis routinely involves the evaluation of sperm count, motility and morphology at the microscopic level, which is carried out using an upright compound microscope equipped with phase contrast optics [7]. Phase contrast is used to visualize the otherwise highly transparent spermatozoa against their background and enable accurate analysis. Grading of oocytes and embryos While analysis of spermatozoa on a flat glass slide using an upright compound microscope is suitable for detailed observation, grading of oocytes and embryos requires the use of an inverted microscope equipped with phase contrast illumination [7]. The high magnification and resolution of this optical system enables detailed observation at the intracellular level, which involves grading of pronuclear morphology, number and size of blastomeres, presence of multinucleation, degree of cytoplasmic fragmentation and detailed grading of blastocyst trophectoderm cells and inner cell mass. The phase contrast optical system is used to give contrast and visualize these key markers as indicators of embryo viability and developmental potential. For both procedures, embryologists require excellent visualizing systems that can generate three-dimensional, highly detailed images. Embryo biopsy, however, requires excellent image resolution and contrast for accurate positioning of the laser beam for zona pellucida drilling and the removal of a single blastomere, or a small part of the trophectoderm, to minimize damage to the embryo as much as possible. The Nomarski illumination system is also a good option; however this is less popular as it requires a special injection or biopsy dish to avoid optical interference of plastic and glass dishes. While this method does help to identify morphologically abnormal gametes and embryos, it cannot provide enough information to differentiate between embryos of the same grade. In order to identify novel non-invasive markers, technological advances in the field of microscopy are aimed at visualizing gametes and embryos in even greater detail. Polarized illumination requires the use of a polarizer and an analyzer (second polarizer) within the optical pathway to modify the basic optics of a light microscope. In addition, due to the highly sensitive nature of the spindle to external factors such as temperature and pH, its presence or absence can be used to optimize culture conditions [16, 17]. While current microscopic observation of embryo development is only possible at snapshot intervals and requires the exposure of embryos to unfavourable conditions outside of the incubator, the ultimate goal would be to generate spatial-temporal imaging of the developing embryo within the incubator. The EmbryoScope system, which enables time-lapse imaging of embryos in their culture conditions, represents a new generation technique to gain more information about embryo development. They require regular mechanical and optical maintenance to ensure consistent image quality, which can be affected by contaminants such as dust, grease and dirt. These contaminants can be airborne or originate from the user, especially in areas where hands, eyelashes and moisture from breathing are in direct contact with the instrument. Buildup of dust, smudges on the optical elements of the microscope as well as scratches on the lenses can significantly diminish optical performance. While it is recommended that full maintenance of microscopes be carried out by specialized personnel annually, regular basic maintenance is recommended, especially for heavily used instruments. This may include the systematic cleaning and inspection of the mechanical and optical components of the microscope, as described below. Basic cleaning of mechanical components Mechanical components, such as the microscope stage, focusing knobs and control rods, are in direct contact with the observer and are exposed to skin oil and moisture. Therefore it is essential that these areas are decontaminated regularly with a moistened lintfree cloth or alcohol wipes and dried with a clean cloth. The painted surfaces of the microscope may also be wiped and decontaminated regularly. Basic cleaning of optical components It is essential that lens surfaces are cleaned with appropriate lens cleaning products, as conventional cleaning solvents may cause irreversible damage to the delicate optical components of the microscope. As a routine Chapter 23: Fundamental laboratory skills for clinical embryologists recommendation, loose particles from the eyepiece lenses, objective lens and the condenser should be blown off using an air blower. If required, lint-free lens paper or a cotton swab applicator can be used to remove any contaminant that cannot be removed with the air blower. To remove greasy smudges or immersion oil, lens cleaning solutions may be used as recommended by the manufacturer. Preventive action to reduce accumulation of airborne particles may include the use of microscope covers when the instrument is not in use. The effect of temperature fluctuations on the cytoskeletal organisation and chromosomal constitution of the human oocyte. Light microscopy in clinical embryology: lighting the way for infertility treatment. Of course, many of these skills are also applicable to multidisciplinary laboratories. We hope to have provided sufficient information for young embryologists to establish a basic framework with which to develop their practical laboratory skills. However, it is important to note that this chapter does not describe all of the key points one needs to consider before working in a laboratory, especially a clinical laboratory. It is important to note that each laboratory will have its own set of key rules, and that infrastructure and equipment inventory may vary significantly. Furthermore, while the basic skills required in a laboratory do not change significantly over time, equipment style and operation do change dramatically, as can experimental protocols. Moreover, health and safety guidance regarding recommendations for handling chemicals and equipment are in a constant state of flux, and significant consideration should be afforded to such legislation. Limited recovery of meiotic spindles in living human oocytes after cooling-rewarming observed using polarized light microscopy. High magnitude of light retardation by the zona pellucida is associated with conception cycles. Meiotic spindle and zona pellucida characteristics as predictors of embryonic development: a preliminary study using PolScope imaging. Birefringence characteristics in sperm heads allow for the selection of reacted spermatozoa for intracytoplasmic sperm injection. Embryos with too early first cleavage fail to implant; correlation between exact timing of first cleavage and successful implantation. A handbook of measurements, calculations and other quantitative skills for use at the bench. Male factor infertility contributes to approximately one-third of all assisted reproduction referrals [1]. It is therefore essential when investigating couples presenting for fertility treatment that an accurate analysis of their semen is undertaken. This should be considered the gold standard for all semen analysis and preparation methods and describes them all in detail. Both sets of reference standards will be referred to in this chapter, with the newer values clearly indicated in italics [2, 3]. There are many everyday events that can affect the quality of sperm undergoing analysis, and some of these are discussed in Table 24. Sample production Ideally, sample production rooms should be located as close to the laboratory as possible so that samples can be analyzed as soon after liquefaction as possible. At the Oxford Fertility Unit, hatches adjoin the laboratory so the sample can be handed directly to the laboratory after collection. Washed containers should never be used as they may contain soap or residue from its previous contents.
