
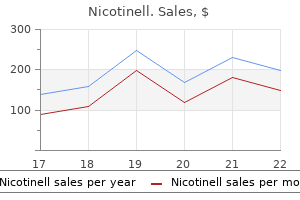
Cheap 17.5mg nicotinell fast delivery
Patients describe acute onset of exquisite pain quit smoking brochures order nicotinell once a day, swelling, erythema, and inability to bear weight on the afflicted joint. Occasionally, patients have constitutional symptoms including fever and chills, with an elevation of sedimentation rate and white blood cell count. The utility of this class of drugs may be limited by renal insufficiency, cardiovascular risk factors, and gastrointestinal bleeding. A randomized, placebo-controlled trial comparing the low-dose and high-dose regimens showed both approaches had equivalent efficacy in pain relief at 24 hours (compared with placebo). However, adverse gastrointestinal events were significantly less common with the low-dose regimen. Oral colchicine is now available in generic and two branded versions (Colcrys, Mitigare). Gastrointestinal symptoms are generally the first clinical signs of colchicine toxicity in patients with normal renal and hepatic function. More serious toxicities do occur and include neuromyopathy, aplastic anemia, and worsening renal and hepatic function. Care should be used in patients with renal or hepatic impairment, and because of potentially serious drug-drug interactions, colchicine should be avoided in patients receiving cyclosporine (Neoral), clarithromycin (Biaxin), verapamil (Calan), and amlodipine (Norvasc). For isolated monoarticular attacks, especially of medium or large joints, aspiration of joint fluid and intraarticular injection with triamcinolone acetonide (Kenalog) 20 to 40 mg can quickly terminate an attack. For polyarticular attacks or attacks in smaller joints, systemic corticosteroids (oral or intramuscular) may be used. Oral prednisone starting at 20 mg twice daily with a taper over 10 to 14 days is very effective. Patients can have rebound attacks if oral steroids are terminated too quickly, and thus methylprednisolone (Medrol) dose packs should be avoided. If intramuscular injection is used, a single dose of triamcinolone 40 mg may be used. In 2013 canakinumab became the first biologic agent approved for acute gout in Europe. Intercritical Gout After an attack subsides, management is directed at preventing recurrent attacks. During acute attacks of gout, normal serum urate concentration is reported in up to 40% of affected patients, and thus it is not an accurate reflection of the true urate pool. Confirmation of hyperuricemia is best achieved either before the resolution of an attack or 2 to 4 weeks after it, to achieve an accurate serum urate concentration. There is a generalizable correlation between the serum urate level and risk for recurrent attack. Prophylaxis of future attacks during early urate-lowering therapy can consist of colchicine at doses of 0. High-dose salicylate therapy lowers serum uric acid by interfering in renal urate transport; low-dose aspirin1 has the opposite effect, but it is often continued in gout patients because of its overriding importance in managing coronary artery disease. With this regimen, colchicine can be used to abort an attack if taken immediately after the development of the first symptom of gout flare. Gout and Hyperuricemia V Endocrine and Metabolic Disorders Long-Term Urate-Lowering (Antihyperuricemic) Therapy the aim of urate-lowering therapy is to reduce and maintain serum urate at concentrations below those at which extracellular fluids are saturated with monosodium urate. Urate lowering can be achieved either by increasing urinary excretion or by decreasing production of urate. Obesity and weight gain are risk factors for gout, and weight loss has been shown to decrease the risk of gout. A purine-restricted diet has often been recommended to patients but is often unpalatable and impractical. Reduction in alcohol intake, namely beer and liquor, can effectively reduce urate levels. Similarly, reduced intake of red meat and shellfish also lowers the risk of recurrent gouty attacks. Studies have shown an increased frequency of attacks in patients who consume fruit juices and soft drinks containing high-fructose corn syrup, an ingredient not found in diet drinks. Once the decision is made to institute serum urate-lowering therapy, the duration of treatment is indefinite and must be long-term to be effective. The majority of patients with gout and tophaceous disease will continue to have attacks if therapy is discontinued, and thus education is a key part of the treatment plan. Patients should be instructed that, with initiation of any urate-lowering therapy, they will be at increased risk for a flareup and thus must continue regular use of prophylactic agents as outlined above. At least 80% to 95% of cases of hyperuricemia and gout are attributable to impaired urate excretion, which is reflected in diminished urate clearance or fractional excretion of uric acid but not usually in low daily urine uric acid excretion. Patients are preferentially treated with xanthine oxidase inhibitors because of the easier dosing schedule and because many patients have contraindications to uricosurics such as renal insufficiency and kidney stones. Uricosurics Relative to medications aimed at urate synthesis, uricosurics are relegated to second-line treatment of patients with elevated urate burden or tophaceous disease. This is a very effective drug that concentrates and promotes urinary excretion of urate. Its utility is limited in patients with renal insufficiency, and probenecid is not recommended as first-line therapy in patients with nephrolithiasis or uric acid overexcretion. The maintenance dose of probenecid required to achieve and maintain serum urate concentration at less than 6. Once goal serum urate concentration is achieved with a uricosuric agent, the risk of uric acid calculi is diminished, because urinary uric acid excretion becomes normal. It is used at a dose of 200 mg/day in combination with a xanthine oxidase inhibitor, including allopurinol (Zyloprim) or febuxostat (Uloric). Duzallo is also available in lesinurad 200 mg and allopurinol 200 mg tablet for patients with renal impairment. Other drugs found to have uricosuric effects include fenofibrate (Tricor)1, a fibric acid derivative used to treat hyperlipidemia, and the antihypertensives losartan (Cozaar)1 and amlodipine (Norvasc)1. These agents have mild uricosuric properties and may be useful adjuncts to urate-lowering therapy. Skim milk ingestion has been shown to lower serum urate levels through uricosuric effects. Lower urate levels have also been seen in patients who consume coffee, but the mechanism of action is unknown. More than 90% of patients with gout treated with urate-lowering medication in the United States are given allopurinol, but dosages of more than 300 mg/day are infrequently employed, and often patients do not achieve serum urate concentrations of 6. There are genuine concerns about allopurinol drug interactions, gastrointestinal intolerance, rashes (ranging from mild to life-threatening), and the rare but sometimes fatal hypersensitivity syndrome. Allopurinol should be avoided with the immunosuppressives azathioprine (Imuran) and 6mercaptopurine (Purinethol) because it can increase the risk of bone marrow toxicity, because these medications are partially metabolized by xanthine oxidase. Effective dosing of allopurinol is often not achieved because of compliance with published but recently disputed recommendations for allopurinol dose reduction in states of renal impairment. Allopurinol should be initiated at 100 mg daily in patients with creatinine clearance of 40 mL/min or greater, and it should be titrated in 100-mg increments every 2 to 4 weeks, with the endpoint of dosing determined by achievement of serum urate concentration of 6. Unlike allopurinol, this is a nonpurine analogue and selective xanthine oxidase inhibitor that is not incorporated into purine nucleotides and does not appear to affect pyrimidine metabolism. Febuxostat is primarily metabolized by oxidation and glucuronidation in the liver, with little renal excretion of drug; this contrasts with the renal elimination of oxypurinol, the main allopurinol metabolite. The recommended starting dose of febuxostat is 40 mg daily, with an increase to 80 mg daily if serum urate concentrations do not reach goal urate levels in 2 weeks in patients with normal renal function. An advantage of febuxostat over allopurinol is that it can safely be taken by patients with creatinine clearance greater than 30 mL/min. Humans lack the enzyme uricase, which converts uric acid to allantoin, a more soluble purine degradation product. Replacement of this missing enzyme allows direct conversion of urate to allantoin, with eventual depletion of increased body urate pools and control of disease, including resolution of tophi. Recombinant uricase therapy profoundly lowers serum urate concentration, as was demonstrated in two large trials.
Diseases
- Mental retardation-polydactyly-uncombable hair
- Spirurida infections
- Angel shaped phalangoep
- Alpha-thalassemia mental retardation syndrome
- Dyschondrosteosis nephritis
- Fiber type disproportion, congenital
- Polychondritis
Nicotinell 35mg low price
In other cases quit smoking 02 purchase nicotinell 35 mg without prescription, however, the onset may be explosive with high fever, impairment of consciousness, vomiting, focal weakness, and seizures. Evolution of the illness is rapid; close to 70% of patients becoming stuporous or comatose within two days of hospital admission [18]. The duration of coma in cases with a favorable outcome has been found to be no more than five days. Although Eastern equine encephalitis accounted for only 30 cases, a total of 2% of pediatric Table 16. Location Principal Vector Animal Hosts Season Facilitating Factors neuroinvasive arboviral infections in the United States between 2003 and 2012, 10 of those patients died [19]. Fever, an elevated white count with elevated neutrophils, and hyponatremia are likely to be found. Spinal fluid examination has shown elevated white cells at an average of 370 cells on first exam, a predominance of neutrophils, protein levels at approximately 100 mg per deciliter, and no reduction in sugar levels [18]. Confirmation requires a fourfold rise in serum hemagglutination inhibition, complement fixation, immunofluorescence, or neutralization titers between acute and convalescent sera. The neuropathology of fatal cases demonstrates the aggressiveness of the process, with neutrophilic perivascular infiltrates and vessel wall infiltration sometimes mimicking arteritis [24]. While a vaccine is available for animals and for exposed personnel such as laboratory workers, it is not available to the general public. Hence, public health measures to control the vector and personal actions to avoid the vector are indicated. These include screening and household air conditioning, use of insect repellents, long sleeves and trousers, and avoidance of outdoor activities at times of heavy mosquito activity. Atlantic Seaboard and Gulf Coast Culiseta melanura to birds, other mosquito species serve as bridge vectors to humans Birds Florida: Throughout the year; Northern Seaboard: July to October Increased rainfall facilitating multiplication of the principal and bridge vectors 16. Eklund and Blumstein reported that of 737,000 horses in Minnesota in the summer of 1937, over 41,000 became sick and 9200 died [25]. Eklund reported that almost 800 human cases of encephalitis occurred in the summer of 1941 in Minnesota [26], and almost 500 human cases were reported from the Saskatchewan epidemic in 1965 [27]. Tsai and Monath suggest that a reduced rural population, changes in land-use patterns and life styles may have contributed to a reduced risk of infection [16]. While humans and horses represent dead-end hosts, mounting an insufficient viremia to sustain a cycle of infection, the Culex tarsalis mosquito and passerine birds are the principal components of the normal cycle of virus replication and transmission. Both older people and infants are at increased risk of infection with a wide range of the inapparent to apparent infection ratios by age group. Stiff neck as part of the whole spectrum of illness has been reported in several cases series. While there is a wide variation in the reported mortality, probably reflecting the different populations studied, overall it has been under 5% [31]. Sequelae in adults have been reported to be related to the duration of coma [32], and to be most severe in Table 16. Neuropathological examination of autopsied cases revealed vascular congestion, with perivascular infiltrates and focal areas of inflammation, necrosis and gliosis to microscopic exam [15,35]. General laboratory studies and neurodiagnostic tests do little to explicitly identify the illness. A vaccine is available for horses and for persons whose occupations put them at special risk. Louis encephalitis is the most widespread of the arbovirus encephalitides in the U. A flavivirus of the Flaviviridae family, until the emergence of West Nile virus, it had been the most common arbovirus to strike the U. However, it has both an epidemic form in Eastern and Mid-Western states, and an endemic form in Western states (Table 16. In 2001, an outbreak of over 60 cases was the largest outbreak ever recorded in Louisiana. Different mosquito vectors transmit the virus to birds in different regions of the country. Explanations for epidemic outbreaks remain incompletely understood and likely include virological factors, changes in vector populations, avian amplifying hosts, and environmental conditions [40]. The incubation period is highly variable, from four to twenty-one days, as is the inapparent to apparent infection 254 Arthropod-borne virus encephalitis Table 16. A prodrome of fever, headache, malaise, and myalgia may precede the onset of frank parenchymal signs of encephalitis. There may be a variety of systemic signs including gastrointestinal disturbances, sore throat and cough, and dysuria [43]. In the 1966 epidemic in Dallas, mental aberration was found in 79%, nuchal rigidity in 65%, and tremor in 53% [44]. Of a total of 95 patients, 11 were classified as aseptic meningitis, 4 as febrile headache, one as non-specific illness, and 79 as encephalitis. Less severe forms of the illness would likely be found more commonly in a community based serosurvey. These have been found to include inadequate screening, lack of air conditioning, or sitting outside a residence [45]. Electromyographic abnormalities may be found compatible with lower motor neuron dysfunction [44]. However, verification requires assays such as serum neutralization because of cross-reactivity with closely related viruses [42]. Metagenomic nextgeneration sequencing has also detected the virus in a fatal case of meningoencephalitis [47]. There is no antiviral therapy available, hence management of the acute phase of the illness requires vigorous supportive treatment. Six patients in the 1995 Dallas epidemic required mechanical ventilation, four had tonic clonic seizures, and one required pentobarbital anesthesia for status epilepticus [46]. It has been commented that reversal of impaired consciousness may be rapid with neurologic improvement after several days. However, convalescence from symptoms such as anxiety, forgetfulness, tremor, headache and unsteadiness can take months, or even years, in some patients [43]. No vaccine is available so that vector control and avoidance are the crucial aspects of prevention. A review of the 1986 outbreak in Baytown and Houston, Texas, emphasized the importance of mosquito surveillance to facilitate vector control. It also suggested that assistance in repairing window screens might be an important preventive measure in impoverished neighborhoods, where the risk of infection is highest. Many mechanisms have been suspected, including migratory birds, imported exotic birds, a viremic human traveler, inadvertent transport of infected mosquitoes, and the suggestion of bioterrorism. The New York West Nile virus strain is most closely related to a West Nile virus isolated in Israel from a goose [10]. That relationship is telling because the 1999 New York human outbreak was also associated with an outbreak in exotic and domestic birds [50]. Crows have been a particular target, with a die-off observed before the human cases in 1999, and isolations of the virus from crows occurring early in the season, as natural sentinels, in subsequent years. The territory of the virus expanded through the early 2000s, likely by the expansion by viremic birds. In August 2002, a major human outbreak occurred in Louisiana and in the neighboring states of Texas and Mississippi. Viral activity in animals had been found in all the continental states but Alaska [51]. The virus was originally isolated from a woman in the West Nile district of Uganda during a yellow fever survey [52]. Cases have been reported from Egypt, Israel, South Africa, Romania, and the former Soviet Union, among other locations. In 1999 when the encephalitis made itself apparent in New York City, the virus caused a massive outbreak in the Volgograd region of Russia [53]. It reemerged causing human cases in Israel in 2000, and was the cause of equine encephalomyelitis in the Camargue, in France as well as 16. Culex and other species Birds Summer to early fall Peridomestic flooding Vector Animal Hosts Season Facilitating Factors in Italy in 1998.
Buy nicotinell 52.5mg with mastercard
Blood ammonia levels lack sensitivity and specificity and correlate poorly with the severity of encephalopathy quit smoking quit key purchase 52.5mg nicotinell fast delivery. Although the exact mechanism responsible for its therapeutic efficacy is still unclear, this agent is degraded by colonic microbiota to short-chain organic acids, resulting in acidification of the intestinal lumen and increased conversion of absorbable ammonia to nonabsorbable ammonium. The cathartic effects of nonabsorbable disaccharides may result in profuse diarrhea, dehydration, and hypernatremia. For these patients, endovascular techniques aimed at decreasing the size of the shunt should be considered. Liver transplantation offers definitive therapy for patients with end-stage liver disease, resulting in restoration of hepatic synthetic function and resolution of complications associated with portal hypertension. However, residual cognitive impairments may persist following liver transplantation, adversely impacting healthrelated quality of life. Regions of the world with intermediate to high incidence of this malignancy (more than 3 cases per 100,000 persons per year) include Asia, sub-Saharan Africa, and Western Europe. Additional features include presence of a capsule and interval growth of the lesion when previous imaging studies are used for comparison. Locoregional therapies include radiofrequency ablation, percutaneous ethanol injection, transarterial chemoembolization, radioembolization, and microwave ablation. Furthermore, active surveillance is recommended to evaluate for tumor recurrence or progression, development of new lesions, and metastatic disease while awaiting liver transplantation. Adverse reactions, tolerability, and potential benefits must be carefully weighed and individualized according to overall health and performance status, as well as severity of hepatic dysfunction. Physical examination may demonstrate jugular venous distention and lower extremity edema, the latter typically being out of proportion to the severity of ascites. Chest radiographs may demonstrate right ventricular enlargement and a prominent pulmonary artery. An estimated right ventricular systolic pressure greater than 50 mm Hg is typically used as a threshold to obtain more accurate direct hemodynamic measurements through right heart catheterization. Pharmacologic therapy has been extrapolated from studies performed in patients with idiopathic pulmonary arterial hypertension and includes endothelin receptor antagonists (bosentan [Tracleer]1 and ambrisentan [Letairis]1), phosphodiesterase inhibitors (sildenafil [Revatio]1), and prostacyclin analogs (epoprostenol [Flolan]1 and iloprost [Ventavis]1). Clinical manifestations include dyspnea of insidious onset and two characteristic clinical findings: platypnea and orthodeoxia (worsening dyspnea and hypoxemia in upright posture, respectively). Other, more obvious but nonspecific clinical findings include spider angiomata, digital clubbing, and cyanosis. Importantly, blood for arterial gas analysis should be obtained with the patient sitting upright, at rest, and breathing ambient air. Two-dimensional contrast-enhanced transthoracic echocardiography offers high sensitivity and is widely available. Agitated saline to produce microbubbles is injected intravenously as contrast, and under normal cardiopulmonary physiology the gas bubbles are rapidly seen in the right atrium and ventricle but then diffuse into alveoli during normal flow through the pulmonary capillaries. Hepatic Hydrothorax Hepatic hydrothorax is a transudative process leading to accumulation of more than 500 mL of fluid in the pleural space in patients with cirrhosis and portal hypertension in the absence of primary cardiopulmonary disease. Hepatic hydrothorax is thought to result from passage of ascitic fluid from the peritoneal cavity into the pleural spaces (typically on the right in up to 85% of patients) via subcentimeter defects and/or microscopic fenestrations in the tendinous portion of the diaphragm and is facilitated by negative intrathoracic pressure generated during inspiration. Clinical features include dyspnea, nonproductive cough, pleuritic chest pain, and even hypoxemia and hypotension in cases of tension hydrothorax. Importantly, indwelling pleural catheters should be avoided because of the high risk for complications including severe infections that may jeopardize possible liver transplant candidacy in the future. Survival after 1 and 5 years following liver transplantation is approximately 80% to 90% and 60% to 75%, respectively. Relative contraindications are usually associated with suboptimal outcomes following liver transplantation and vary widely across different transplant centers. Absolute contraindications imply that a successful outcome following liver transplantation is unlikely; thus it should not be pursued (Table 11). Evaluation for liver transplantation is a multidisciplinary process carried out over multiple encounters aimed to unveil additional medical, surgical, behavioral, social, and economic issues that may affect liver transplantation candidacy and/or outcomes. Living-donor liver transplantation was developed as an alternative owing to ongoing shortage of deceased-donor organs; however, living donation carries important risks for the donor that must be carefully taken into consideration. The advantages and disadvantages of living-donor liver transplantation are summarized in Table 13. Adequate long-term immunosuppression prevents graft rejection and is currently centered on the use of calcineurin inhibitors (tacrolimus [Prograf] primarily, and less often cyclosporine [Neoral]) with or without concomitant antimetabolite agents such as mycophenolic acid (Myfortic) or its prodrug mycophenolate mofetil (CellCept). Long-term care of liver transplant recipients should not by any means focus exclusively on graft function and prevention of rejection, but rather be comprehensive and aimed at maintaining an overall good state of health by instituting preventive health strategies and monitoring for other complications that may ensue, such as diabetes mellitus, hypertension, dyslipidemia, renal dysfunction, obesity, and alcohol relapse, among many others. A false diverticulum is a protrusion of the submucosa and mucosa through a defect in the muscular wall of the alimentary tract. Some diverticula cause symptoms depending on their anatomic location or associated pathophysiologic complications. The exact cause is unclear, but proposed mechanisms suggest a dysfunction in coordinated swallowing muscle movement and increased intraluminal pressure in the esophagus. Although endoscopic direct visualization is possible, caution should be exercised owing to the risk of perforation. A diverticulum is an abnormal saccular protrusion from the wall of the alimentary tract. The wall of the alimentary tract is composed of submucosal, mucosal, and muscular layers. Though it can be asymptomatic for years before the development of symptomatology, patients may experience dysphagia, aspiration, and regurgitation of undigested food. There may be an additive component of long-term upper esophageal sphincter irritation from acid reflux. Partial fundoplication may be indicated depending on the severity of gastroesophageal reflux present as indicated by ancillary testing of a 24-hour pH probe. Stomach Gastric Diverticula Gastric diverticula are rare with an endoscopic incidence of 0. Diagnosis involves endoscopy, barium swallow, or contrast-aided computed tomography scan. If symptomatic, typical treatment includes a proton pump inhibitor and monitoring for symptom improvement. Persistent symptoms may necessitate gastrectomy of the diverticulum especially if concerns for cancer exists. The size and position of the diverticula may lead to complications such as obstruction of the sphincter of Oddi and/or impingement of the hepatobiliary tree drainage.
Nicotinell 52.5 mg overnight delivery
Regardless of prolactin levels quit smoking yahoo discount 52.5 mg nicotinell with amex, secondary causes should be carefully evaluated with medication history, physical examination, and laboratory tests such as thyroid function tests and chemistry panel, and appropriately treated. The latter is suggested by a discordant prolactin level less than 150 ng/mL for a large sellar, or a parasellar mass greater than 1 cm, after hook effect has been ruled out. V Endocrine and Metabolic Disorders 322 prolactinoma (see prior section on laboratory evaluation). A more typical range of prolactin level is 25 to 100 ng/mL for drug-induced hyperprolactinemia. It is not always possible to correlate in time the initiation of the culprit drug with the onset of symptoms, or rise of prolactin levels. The way to confirm medication-related hyperprolactinemia is to discontinue the putative offending agent(s) for three days before repeating a prolactin assay. Some medications may require a longer period of abstinence, and in such cases the level of prolactin can be retested later if the second value is reduced but still elevated. Pseudoprolactinoma refers to a nonfunctioning sellar or suprasellar mass associated with hyperprolactinemia caused by stalk disruption. However, before making such a diagnosis, one must exclude hook effect with a 100-fold diluted sample. Prolactin levels are typically normalized within several days after initiation of dopamine agonists, as lactotrophs are still sensitive to dopamine, but local compressive symptoms do not improve. In contrast, patients with true macroprolactinoma experience more gradual decrease in prolactin levels after they are put on dopamine agonists, but they could expect improvement in compressive symptoms within 12 hours to days, and imaging evidence of tumor shrinkage in weeks. For drug-induced hyperprolactinemia, the responsible medications should be removed or replaced with alternatives. Newer antipsychotics such as aripiprazole (Abilify) may be used in place of older agents such as risperidone (Risperdal) because they have better metabolic/hormonal profiles. For irreversible conditions such as endstage renal disease, hyperprolactinemia can be effectively controlled with dopamine agonists. Ectopic prolactin secretion, which occurs in paraneoplastic syndrome, is a rare exception where dopamine agonists are ineffective, because extrapituitary production of prolactin is driven by alternative promoters, which do not respond to dopamine. Asymptomatic patients with modest hyperprolactinemia may not need treatment, however, and sex hormone replacement may be adequate for correcting hypogonadism if fertility is not desired. The goals for managing prolactinomas are twofold: treating symptomatic hyperprolactinemia, and relief of tumor mass effects. Mass effects are not a concern for microprolactinomas, whereas for patients with giant prolactinomas (defined as >4 cm or >2 cm of suprasellar extension) and extreme hyperprolactinemia, normalization of prolactin levels is less likely, and treatment should focus on reversal or minimization of mass effects. Observation Active surveillance is appropriate for patients with microprolactinoma who are asymptomatic or not troubled by galactorrhea, especially if fertility is not a concern. As long as regular menses are preserved, they seem to be spared from any long-term consequences from hyperprolactinemia. It is noteworthy that a significant fraction of patients may have tumor resolution during surveillance without treatment. Tumor expansion is a rare event, and serial measurements of serum prolactin level are effective for monitoring interval tumor growth. Pituitary imaging is indicated when there is significant increase in prolactin level or emergence of local compression symptoms. Management of Prolactinoma Management of Secondary Hyperprolactinemia Treatment of secondary hyperprolactinemia should focus on correcting the underlying conditions, for example treating Hormonal Replacement For patients with microprolactinoma bothered only by symptoms related to hypogonadism including menstrual abnormalities, sexual dysfunction, and osteoporosis, but who no longer desire fertility, hormonal replacement is a valid alternative to dopamine agonists, especially when the latter are not tolerated or are contraindicated. This can be achieved with oral contraceptive pills in premenopausal women, or testosterone in men. This approach compares favorably to dopamine agonists in terms of cost and side effects. Patients may experience slight increases in prolactin level, but tumor progression has not been associated with use of oral contraceptive pills for up to 2 years. It would be prudent to use lower doses of estradiol (30 g/day) and closely monitor patients for prolactin level and tumor growth. Dopamine Agonists Medical treatment with dopamine agonists has replaced surgery as the first-line treatment for prolactinomas, with excellent efficacy in achieving treatment goals and minimal risk. The therapeutic effects of dopamine agonists are mediated by dopamine D2 receptors in tumor cells, which inhibit prolactin synthesis and secretion, slow cell proliferation, and reduce tumor vascularity. Normalization of prolactin levels and reduction of tumor size can be expected in the majority of patients. A small fraction of prolactinomas is resistant to dopamine agonists, as defined by failure in normalizing prolactin level, reduction in tumor size by 50%, or restoration of gonadal function with standard doses. In general, microprolactinomas are more sensitive to dopamine agonists than macroprolactinomas are, and men are more likely to be drug resistant than are women. For most patients, however, progressive reduction of tumor size occurs over the course of months to years, though some patients may never experience tumor shrinkage despite normalization of prolactin levels at the highest tolerated doses. Patients with microprolactinoma may discontinue treatment upon menopause because their treatment goal has been fulfilled. Patients with macroprolactinoma, on the other hand, may require life-long treatment to prevent tumor regrowth. A meta-analysis showed that a small fraction of patients may enter long-term remission after discontinuing dopamine agonists (21% for microprolactinomas and 16% for macroprolactinomas). The odds are significantly improved if patients have been treated for at least 2 years and tumor size reduced by! The 2011 Endocrine Society practice guidelines suggest that tapering or discontinuing dopamine agonists may be attempted in patients who have been treated for at least 2 years and experienced complete biochemical and radiographic resolution. The risk for recurrence after drug discontinuation is related to the size of adenoma at the time of the diagnosis. For tumors larger than 2 cm, especially giant prolactinomas, tapering the dopamine agonists to a lower maintenance dose for life-long treatment after achieving maximal tumor reduction would be a better strategy for these patients. Three dopamine agonists are currently used for treating hyperprolactinemia, including bromocriptine (Parlodel), cabergoline (Dostinex), and quinagolide (available only in Europe). Bromocriptine was the first dopamine agonist available, and it has the best established safety record. Cabergoline is a more specific agonist of the D2 dopamine receptor, and is superior in many respects to bromocriptine, for example, because of dosing convenience, tolerability, and treatment efficacy. Many patients not controlled with bromocriptine may achieve normal prolactin levels after switching to cabergoline, which has become the drug of choice for cases not involving pregnancy. Common side effects for this class of drugs include nausea, orthostatic hypotension, fatigue, mental fogginess, and, less frequently, nasal stuffiness, Raynaud phenomenon, constipation, depression, and psychosis. Nausea is more common in patients taking bromocriptine; for these patients the intravaginal route1 can be tried. Patients receiving higher doses of cabergoline are at risk of developing cardiac valvulopathy. However, the life-long exposure to high cumulative doses in patients with resistant prolactinoma is considerable, and regular echocardiogram surveillance is recommended for patients taking doses higher than 2 mg/week. In general, patients should be started on the lowest doses and titrated upward monthly based on the serum prolactin level until treatment goals are reached. Surgery With the availability of the second-generation dopamine agonists, surgery is mostly reserved for the following situations: (1) patients intolerant of, or resistant to , dopamine agonists; (2) women with macroprolactinoma who are planning for conception, to forestall tumor expansion during pregnancy; (3) pituitary apoplexy threatening neurological and visual functions if not managed urgently. Perioperative mortality and morbidity are low in the hands of experienced pituitary surgeons in high-volume centers. Craniotomy is occasionally needed for masses with extrasellar extensions that may be inaccessible by the transsphenoidal route, with higher risk for complications. Postoperatively patients need to be monitored for signs of diabetes insipidus and secondary adrenal insufficiency, which may be transient or permanent. Radiotherapy Radiotherapy is inadequate as a primary treatment for prolactinoma, as its efficacy is poor and latency long. It is also associated with long-term complications including permanent hypopituitarism, cerebrovascular accidents, and secondary intracranial malignancies. Hyperprolactinemia and malignant prolactinomas failing medical/surgical treatment. Stereotactic radiosurgery is preferred over conventional fractionated radiotherapy for more convenient dosing, better efficacy, and lower rate of complications. However, radiosurgery should not be attempted for tumors in close proximity to the visual apparatus (less than 5 mm of clearance), as it is associated with an unacceptably high rate of vision loss.
Baneberry (Black Cohosh). Nicotinell.
- What other names is Black Cohosh known by?
- Are there any interactions with medications?
- Are there safety concerns?
- Is Black Cohosh effective?
- Menopausal symptoms such as hot flashes.
- What is Black Cohosh?
- Dosing considerations for Black Cohosh.
- How does Black Cohosh work?
- Premenstrual syndrome (PMS), osteoporosis, painful menstruation, labor induction, upset stomach, muscle pain, fever, sore throat, cough, repelling insects, acne, mole and wart removal, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96830
Nicotinell 17.5mg otc
For unilateral lesions quit smoking sign order nicotinell 35 mg on line, surgical resection of the affected adrenal gland is recommended mainly to obviate the need for prolonged medical treatment and side effects. For bilateral lesions, medical treatment is recommended because surgical risk outweighs benefits. Other lifestyle changes include aerobic exercise, smoking cessation, and weight loss. One study showed that spironolactone had stronger antihypertensive effect than eplerenone, but there is insufficient evidence to choose one medication over another. Subtotal adrenalectomy has been tried, but only a minority of patients have responded with significant blood pressure improvement. Unilateral adrenalectomy, however, may help selected patients by debulking aldosterone-producing tissues. Use of spironolactone can be limited by side effects; antiandrogenic effects can cause gynecomastia in men and progesterone effect can cause menstrual irregularities in women. Spironolactone is not recommended if creatinine clearance is less than 30 mL/ minute. Again, serum potassium and creatinine should be closely monitored for the first 4 to 6 weeks in particular for those with renal insufficiency or diabetes. Potassium should be maintained at normal levels without use of potassium supplements. Serum potassium and creatinine should be closely monitored for the first 4 to 6 weeks, in particular for those with renal insufficiency or diabetes. Eplerenone1 is a competitive and selective antagonist of the aldosterone receptors. It has a lower binding affinity to androgen and progesterone receptors than spironolactone. Eplerenone is 25% to 50% less potent in antagonizing the aldosterone receptors than spironolactone. Other adverse effects include hypertriglyceridemia, increased liver enzymes, headache, and fatigue. Triamterene is dosed at 100 to 300 mg/day in divided doses, and its side effects are mainly dizziness and nausea. Addition of thiazide diuretics can help control blood pressure by relieving volume overload. The exception is when the triglyceride level is greater than 500 mg/dL because of substantial risk of pancreatitis. Hyperlipidemia pregnancy, and medications, should be thoroughly investigated and treated if found. Therapeutic lifestyle changes are also recommended for those with very high, high, or moderately high cardiovascular risk. Pharmacologic agents can be considered from the beginning for those with very high, high, or moderately high cardiovascular risk. Pathophysiology Lipids have two main points of entry into the circulation: the gut (exogenous pathway) and the liver (endogenous pathway). The exogenous and endogenous pathways are interconnected by intermediate pathways (reverse cholesterol transport pathway and others). Exogenous Pathway Lipids in food are emulsified by bile acids and then hydrolyzed into fatty acids and cholesterol by pancreatic lipases in the intestinal lumen. Inside the intestinal cells, fatty acids and cholesterol are reesterified and then packaged with apolipoprotein (Apo) B48 into chylomicrons. Chylomicrons are secreted into the intestinal lymph and delivered to the systemic circulation. Chylomicron remnants are taken up by the liver via the chylomicron remnant receptors. Hyperlipidemia is associated with an increased risk of cardiovascular disease and, if the triglyceride level is greater than 500 mg/ dL, pancreatitis. Unless the triglyceride level is greater than 500 mg/ dL, the primary goal of management of hyperlipidemia is to decrease the risk of cardiovascular disease. In this regard, appropriate treatment of hyperlipidemia is essential in patients with established cardiovascular disease (secondary prevention), whereas detection and treatment of hyperlipidemia are guided by the risk of cardiovascular disease in asymptomatic patients (primary prevention). The prevalence of hyperlipidemia varies with the definition of hyperlipidemia and the population studied. Therefore optimal treatment of hyperlipidemia to reduce cardiovascular risk is of paramount importance. Various societies and professional organizations have published clinical guidelines for hyperlipidemia. Elevated triglycerides, in particular nonfasting levels, also may be an independent cardiovascular risk factor. Even mildly elevated triglycerides (>150 mg/dL) can indicate metabolic syndrome, which is a strong risk factor for cardiovascular disease. Evaluation Global Cardiovascular Risk Assessment the first step in assessing risk is to stratify global cardiovascular risk scores. Individual tools have been developed based on large epidemiology studies examining a limited number of available risk factors. Traditional risk factors such as age, sex, cigarette smoking, cholesterol, diabetes, and blood pressure are able to predict 80% to 90% of the cardiovascular events in people 40 years or older. However, these tools may not accurately estimate cardiovascular risk in individuals with different demographics or unaccounted risk factors. Recently, chronic kidney disease with glomerular filtration rate less than 60 mL/minute/ 1. Established cardiovascular disease itself and diabetes with other cardiovascular risk factor(s) are also considered as very high risk by some authorities (see the Treatment section and Tables 2 and 3). Recent studies showed that differences in triglyceride levels according to fasting time were small. Secondary causes include hypothyroidism, nephrotic syndrome, dysgammaglobulinemia, use of progestin (especially those with androgenic activity), cholestasis, use of protease inhibitors, chronic kidney *Coronary heart disease, stroke, and peripheral arterial disease of presumed atherosclerotic origin. These conditions should be detected and treated, if appropriate, to improve control of hyperlipidemia. Family history of premature cardiovascular disease and hyperlipidemia and physical findings such as xanthomas, xanthelasmas, and premature arcus cornealis may suggest familial hyperlipidemia. Familial hyperlipidemia can be associated with significantly high risk of cardiovascular disease, which could be underestimated by the global risk scores. Established cardiovascular disease itself, diabetes with other cardiovascular risk factor(s), and advanced chronic kidney disease are also considered as very high risk by some authorities. Medications may be added at the same time as therapeutic lifestyle changes for those with very high, high, or moderately high risk. If medications are indicated, statin is preferred because of proven efficacy that has been consistently shown in multiple clinical trials. The new approach recommends treating at-risk patients with statins of appropriate strength (reflecting the design of most published clinical trials), rather than titrating combinations of lipid-lowering medications to a preset target based on baseline cholesterol levels. The new risk prediction algorithm (the Pooled Cohort Equation) was also criticized for overestimating cardiovascular risk when applied to different cohorts. The panel that developed the algorithm countered that the criticism was largely based on data obtained from cohorts that include volunteers who tend to be healthier than the general population. On the other hand, validity of the algorithm has not been established by prospective clinical trials. It is predicted that patients eligible for statin therapy may double according to the new guideline and patients who are at high risk for cardiovascular disease will benefit from wider use of statins. Efficacy of adding fibrates, bile acid sequestrants or niacin to achieve previously recommended target is limited (discussed below), but management of those who are not tolerant or contraindicated to moderate-high-intensity statins is not well addressed. Therapeutic Lifestyle Changes All patients with hyperlipidemia should be counseled on lifestyle modifications. Dietary modification to limit intake of lipids is an essential component, given that the main source of lipids is exogenous dietary fat.
Buy 17.5mg nicotinell mastercard
Cerebrospinal fluid analysis typically revealed a moderate increase in opening pressure quit smoking 90 days ago will thc show in hair order 17.5mg nicotinell. Though von Economo also noted that despite persistent somnolence or other deficits, opening pressure returned to normal after couple of weeks [11,#83]. Rare cases of post-encephalitic Parkinsonism that have been observed in the modern era have found abnormalities in brain metabolism. Sacks reported a patient who developed a postencephalitic syndrome in 1962, 45 years after their original infection [1]. It followed the hyperkinetic form of the illness most commonly and the somnolent-ophthalmoplegic form least commonly. Although it could affect persons of any age, it had a predilection for young adults. In postencephalitic Parkinsonism, stiffness and bradykinesia generally preceded the tremor and the upper limbs were more affected than the lower limbs. A striking finding in this population was "kinesia paradoxica" in which the patient might be akinetic at one moment and perfectly mobile the next without an intermediate stage [1]. Following the introduction of l-dopa in the treatment of postencephalitic Parkinsonism, the incidence approached 100% [1]. It lasted seconds to hours; typically resulted in tonic deviation of the eyes upward or upward and laterally, often with spasmodic deviation of the head. During the spell, consciousness was preserved, but the patient was incapable of voluntarily moving his eyes except momentarily with strong effort. Oculogyric crises were virtually unknown prior to the epidemic of encephalitis lethargica [73]. Other ocular abnormalities observed included slight ptosis, impaired pupillary reaction and Argyll Robertson pupils, nystagmus, squint, impaired convergence and extraocular muscle palsies. An asthenic syndrome in which patients complained of a persistent sense of fatigue, both mental and physical, was frequently seen in Parkinsonians, but could also occur as the sole or main disability. Riddoch described the syndrome in this fashion, "unlike the weakness of myasthenia gravis, the feebleness is not as a rule much diminished by rest, and, unlike the neurasthenic, the patient does not tend to feel better as the day goes by" [64]. Speech abnormalities included a wide gamut of problems, including, logorrhea, echolalia, palilalia, tachyphemia (rapid speech), megaphonia (speaking in an unnecessary loud voice), klazomania (shrieking and crying), and hyperodia (singing and reading outloud). To illustrate the speech abnormalities observed, Kinnier Wilson described one of his patients as follows: "A 47 year old man 16 months after encephalitis began reading out loud. The head is often thrown back, the limbs may perform various grotesque movements, the face may or may be not cyanosed, and, in longer attacks, consciousness is lost for a short time. Turner and Critchley classified the respiratory abnormalities into three types: (1) Disorders of rate (tachypnea and bradypnea); (2) disorders of respiratory rhythm; and (3) respiratory "tics" [74]. Psychiatric manifestations were common as long term consequences of encephalitis lethargica. Neuropsychiatric disturbances were reported in 50% [75] to 100% of survivors [16,76]. Hallucinations, metamorphopsia, and excessive puns, joviality, and silliness referred to as the Witzelsucht of Jastrowitz [9]. The mental changes appeared to be more striking in children, whereas, adults more often had Parkinsonian sequelae [2]. McKenzie described these behavioral disturbances in children as manifesting as a profound emotional instability and a perversion of conduct with poor impulse control that occasionally led to criminal behavior [2]. Mild features of included nervousness, fatiguability, poor concentration, anxiety and depression, Parkinsonism with emotional impoverishment, and intellectual decline. The loss of cognitive function was most commonly observed when encephalitis lethargica occurred in infancy. Metabolic and endocrine disorders were observed on rare occasion and included exophthalmos, tachycardia, sweating, tremor suggestive of hyperthyroidism, and goiter, glucose dysregulation, adiposogenital syndrome in children, precocious puberty and disturbance of sexual function, excessive salivation and sebaceous secretions. Perivascular and tissue inflammatory infiltrates that are chiefly mononuclear cells are accompanied by small hemorrhages secondary to diapedesis, neuronophagia, and microglial nodules. As in the older literature, a contemporary case showed an active encephalitis, mainly centered on the upper brainstem and diencephalon with extensive Purkinje cell loss and marked plasma cell infiltrates and morula cells [78]. Wiesner, who worked with von Economo as a pathologist, showed hyperplasia of tonsils and intestinal follicles in several patients [11]. As von Economo described the microscopic picture: "we have histologically the picture of a polioencephalititis cerebri, pons and medulla with a slight poliomyeltitis; perivascular, inflammatory, and diffusely infiltrating, but no hemorrhagic and only slight neurophagic character" [11]. The gross pathology of chronic encephalitis lethargica is characterized by modest findings of atrophy either focal or generalized. Microscopic findings included neuronophagia, astrogliosis, hemosiderin staining perivascularly, and pigment degeneration in substantia nigra and locus ceruleus. The astrogliosis may be overwhelming involving widespread areas of the brain and occur in the absence of significant other pathologies [80]. Neurofibrillary tangles have been reported in the substantia nigra, locus ceruleus, and raphe nuclei. Hallervorden described the gross pathology as a discoloration of the substantia nigra, the microscopic pathology dominated by neurofibrillary tangles; tangles in the cerebellar cortex or plaques like in Alzheimer disease were never seen. Interestingly, he described the multiple young patients who, even though their substantia nigran showed severe postencephaltic scarring, did not show any of the typical Parkinsonian features, i. The observation of the latter suggested a biochemical means of pathologically distinguishing postencephalitic Parkinsonism from certain other neurodegenerative disorders. Additionally "tuftshaped" (non-reactive) astrocytes have been found in a widespread distribution throughout the central nervous system [84]. In addition to the passage of the infection to animal models from brain tissues derived from patients long after the initial infection, a variety of pathological features suggest the persistence of the virus despite the inability to detect a specific viral antigen. These features include evidence of acute inflammation at autopsy associated with cases of "intermittent progression," the presence of marked inflammation in 30% of Parkinsonian patients and some degree of inflammation in 50% even after many years, and almost all cases have some evidence of perivascular mononuclear cell infiltration. There was discordance between the incidence of illness and of death as some affected persons died during acute phase and others during chronic phase. In Glasgow, not more than 60 of more than 300 affected persons were free of all signs and symptoms two years after the infection [2]. According to Dimsdale, one-third of the patients died during the acute phase of the illness, one-third survived without sequelae, and one-third doped neurological sequelae [87]. Although some investigators believed that recovery seemed to be best in those afflicted with respiratory abnormalities followed by those with sleep inversion, during the Sheffield epidemics, those with early respiratory symptoms had the highest mortality. Those patients developing Parkinsonism or other movement disorders appeared to have the worst prognosis. Many authors [88,89] found most cases of postencephalitic Parkinsonism to occur in the first 5 years after the encephalitis. Up to 36% of their patients did not even have an interval between the acute illness and the Parkinsonian features, however, intervals exceeding 15 years were observed. Beringer described a 56-year-old patient, who was in good health up until 40th year when he developed diplopia, insomnia, fatigue with rapid recovery and new Parkinsonian symptoms 16 years later [88]. Tyndel and Beringer also noticed that there was no direct parallel between the age of the patients at the time of acute illness and the length of the interval of sequelae and no seeming correlation between the length of the interval and the severity of the encephalitis [88,89]. Absolute recovery remained unknown, most cases tending to become worse, although this was extremely variable. Erreurs passees et espoirs decus de la recherche en virologie medicale (editorial). Beitraege zur Geschichte der Schlafsucht, mit besonderer Berucksichtigung der Encephalitis epidemica. The treatment of the Parkinsonian manifestations of encephalitis lethargica included belladonna and hyoscine which were noted to have a salutary effect [2]. Oliver Sacks beautifully records the response of patients with postencephalitic Parkinsonism to l-dopa in his book Awakenings [90].
Buy discount nicotinell 35 mg line
Treatment of symptomatic infections can be accomplished with mebendazole quit smoking 7 years buy nicotinell with a mastercard, albendazole,1 or ivermectin (Stromectal)1; see Table 2 for details. Infection results primarily from parasite penetration into the skin; therefore persons with an agrarian lifestyle and significant soil contact are at greatest risk. Two species are responsible for the majority of human hookworm: Necator americanus and Ancylostoma duodenale. Ancylostoma braziliense, a canine intestinal pathogen, causes cutaneous larval migrans in humans because the pathogen cannot penetrate the human dermis. Of the two common forms of human hookworm, N americanus is smaller and a less aggressive pathogen with a longer life span than A duodenale. Both parasites are found in warm climates throughout the world; A duodenale exists in smaller pockets, whereas N americanus is widely distributed throughout impoverished rural areas of the tropics in the Americas, Asia, and Africa. Infection results from larval penetration of the skin on contact with contaminated soil. An intensely pruritic, erythematous, papulovesicular rash called ground itch can develop at the site of entry. Parasites then enter the venous or lymphatic circulation and travel to the lungs, at which point an urticarial rash with cough can develop. The larvae are swallowed and migrate to the small intestine, where they attach to the bowel wall with teeth or biting plates and take a continuous blood meal by sucking with strong esophageal muscles. As the hookworms lodge in the small intestine, peripheral eosinophilia peaks, and gastrointestinal discomfort with or without diarrhea can result. Large oral ingestion of A duodenale can cause Wakana syndrome, characterized by cough, shortness of breath, nausea, vomiting, and eosinophilia. The most important clinical manifestation of hookworm infection is iron-deficiency anemia, which can be mild or severe and may be accompanied by malabsorption of protein in hosts with heavy burden of disease. Infants and pregnant women can become extremely ill or even die as a result of the anemia. Hookworm may be difficult to diagnose because light infections often do not produce enough eggs to be readily seen on stool examination; stool should therefore be concentrated if infection is suspected. Eggs do not appear in stool until approximately 2 months after infection, so patients with pulmonary complaints will not yet have a positive stool examination. Hookworm infection can be eradicated with benzimidazole antihelminthics; see Table 2 for details. Prevention of hookworm infection, as with other parasites, lies in improved sanitary conditions; 1 wearing shoes is especially important because the majority of infections are acquired through the skin. Mass anthelminthic treatment campaigns have shown some efficacy in reducing disease in children; however, reinfection and concern for development of resistance continue to present significant challenges. Strongyloides Strongyloides stercoralis is a global pathogen that is estimated to affect as many as 100 million people, mostly in tropical regions of the world. In recent years, it has become more commonly recognized in the United States among immigrants as a cause of chronic eosinophilia, as well as symptomatic infection. Strongyloides infection results when filariform larvae dwelling in fecally contaminated soil penetrate the skin or mucous membranes of a susceptible host. Larvae move to the lungs and subsequently to the trachea, where they are coughed up and swallowed. Females, about 2 cm in length, lodge in the lamina propria of the duodenum and proximal jejunum where they begin to oviposit. Rhabditiform larvae emerge from these eggs and either repenetrate the intestinal wall or are passed into the feces, at which point they can begin a free-living cycle and reproduce sexually, or can molt directly into an infectious form ready to enter a subsequent susceptible host. Those who have symptoms might report abdominal discomfort, diarrhea alternating with constipation, or, rarely, blood-tinged stool. Severe intestinal infections can occur and are manifest by chronic watery or mucousy diarrhea. In such cases, colonoscopy reveals excessive bowel wall thickening and copious secretions, or edema (catarrhal enteritis or edematous enteritis). Parasite migration through the dermis can manifest as serpiginous, erythematous, and pruritic patches along the buttocks, perineum, and thighs, known as larvae currens. Strongyloides appear to attain a balanced state in their host, with similar numbers of adult worms throughout the many years of infection. During periods of host immunocompromise, in particular in patients taking corticosteroids, Strongyloides can enter into a state of rapid autoinfection and rampant reproduction called hyperinfection syndrome, which results in devastating illness. Strongyloides has also caused hyperinfection in organ transplant patients whose donor had been infected asymptomatically with the parasite. Although it has long been thought that steroid-induced immune compromise was the major trigger for hyperinfection, growing evidence suggests that steroids themselves may be the culprit by directly inducing the accelerated life cycle in the parasite. The hyperinfection syndrome is characterized by systemic illness with fever, cough, hypoxia, patchy or diffuse pulmonary infiltrates with alveolar microhemorrhages, and dermatitis; it can include myocarditis, hepatitis, splenic abscess, meningitis and cerebral abscess, and endocrine organ involvement. Larvae migrating out of the intestines can drag bacteria with them, resulting in gram-negative or polymicrobial sepsis. The prognosis of Strongyloides hyperinfection syndrome is grave even with highly effective anthelminthic treatment given the diffuse nature of this disease. Diagnosis of uncomplicated Strongyloides infection in endemic areas can be challenging because few larvae are passed in stool, and numerous examinations may be necessary to detect them. It is, however, the test of choice for persons who have migrated to nonendemic areas, and all persons in this setting should be treated. During the first days of treatment, patients can experience intense dermal pruritis as parasites die. Enterobius vermicularis Human pinworm infection, caused by the thread like nematode Enterobius vermicularis, is found throughout the world and continues to be diagnosed commonly in the United States, especially in children. Its persistence is likely related to the fact that pinworm does not require a period of maturation outside the human body, and autoinfection or transmission by very close contact sustains the parasite within communities. E vermicularis is at maximum 1 cm long with a tapered tail, and dwells in the cecum, appendix, and adjacent colon. In scratching the perianal area and subsequently bringing his or her hand to the mouth, the host ingests the embryos, which then hatch in the bowel about 2 months later and continue the cycle of infection. Embryonated eggs can also attach to bedclothes, thereby placing other household members with close contact at risk for infection. In family groups, infection is associated with close living quarters, poor hand washing, and infrequent washing of clothes and sheets. Infection is often asymptomatic, but it can cause perianal itching, which helps to facilitate persistent infection by encouraging frequent touching of the perianal area. Rarely, worms migrate into ectopic foci and produce painful genitourinary tract disease with granulomatous inflammation; pinworm infection rarely results in pain that mimics acute appendicitis. Pinworm infestation is best diagnosed by the classic Scotch tape test, which involves placing and immediately removing a piece of sticky tape firmly across the perianal area early in the morning when the eggs have been deposited. It is also sometimes possible to see the worms directly on the perianal region, although they are so small that they may easily be mistaken for residual bits of toilet paper. E vermicularis is susceptible to standard anthelminthic therapies as listed in Table 2. All household contacts should be empirically treated with the same regimen to avoid reintroducing infection from family members who may be asymptomatically carrying the parasite. Anisakiasis Anisakiasis is a descriptive term for human infection with parasites of two distinct genera: Anisakis and Pseudoterranova. Humans are incidental hosts for these roundworms that inhabit multiple species of fish and other marine animals (tuna, mackerel, hake, cod, sardines, and cephalopods) as intermediate hosts, and marine mammals such as whales, seals, sea lions, and walruses as final hosts. Cases are most commonly reported from Japan but are seen throughout the world in other coastal nations and among restaurateurs. On consumption of fish with anisakid larvae embedded in its musculature, humans can experience immediate symptoms in the form of itching or burning in the throat, which can provoke coughing that expels the parasite. If the parasite is swallowed, the larva attempts to embed in the gastric musculature at the pylorus. This can produce acute, short-lived epigastric abdominal pain and possibly immediate vomiting, at which point the parasite might again be ejected. If the larva does manage to penetrate gastric tissue, it dies because it is incapable of further tissue invasion in humans. An intense inflammatory response to the dead pathogen can then result, with gastric pain, nausea, and occasionally diarrhea with blood or mucus if a gastric ulcerative lesion has resulted. Rare cases have been reported in which the larva penetrates the peritoneum, causing focal peritonitis and abscess formation.

Cheap nicotinell 17.5mg without prescription
Dermatologic Symptoms the most common allergic drug reactions affect the skin and can cause a variety of different exanthems quit smoking zonix discount nicotinell 17.5 mg online. The most common skin reaction is the classic "drug rash," which is a morbilliform eruption originating on the trunk. Other dermatologic symptoms include urticaria, angioedema, acne, bullous eruptions, fixed drug eruptions, erythema multiforme, lupus erythematosus, photosensitivity, psoriasis, purpura, vasculitis, and pruritus. The inner ring may have urticaria, pustules, or necrotic lesions surrounded by macular erythema. There is massive and widespread apoptosis, for which there are several associated cytokines. Patients are usually admitted to the burn unit for electrolyte and infection management. Drug Hypersensitivity Reactions 73 the chemical structure and molecular weight of the drug may help predict the type of hypersensitivity reaction. Larger drugs with greater structural complexity are more likely to be immunogenic. However, drugs with small molecular weight (< 1000 Da) can elicit hypersensitivity reactions by coupling with carrier proteins to form hapten-carrier complexes. Other drug-related factors include the dose, route of administration, duration of treatment, repetitive exposure to the drug, and concurrent illness. Topical and intravenous drug administrations are more likely to cause hypersensitivity reactions than are oral medications. Patient risk factors include age, female gender, infection with human immunodeficiency virus, atopy, specific genetic polymorphisms, previous drug hypersensitivity reactions, and inherent predisposition to react to multiple unrelated drugs. More recent data suggest that granulysin, which is a cationic cytolytic protein released by T lymphocytes, may play a role as well. In addition, the lesions may be limited to the trunk; however, they more commonly involve the palmar surface of the hands and the dorsum of the feet, as well as the mucous membranes. The evidence supporting causality primarily comes from a small number of cases reported in the medical literature. The treatment is immediate cessation of the culprit drug and symptomatic treatment. Glucocorticoids are controversial and depend on the course and extent of the disease. Therefore it is important to recognize the signs and symptoms early to initiate treatment. Most patients will have fever, lymphadenopathy (75%), eosinophilia, and an erythematous morbilliform rash on the face and body in addition to liver and multiorgan damage. The presence of acanthuses and papillomatosis and a personal or family history of psoriasis favor a diagnosis of pustular psoriasis. The eruption usually occurs within 24 hours of the initiation of the drug, and healing occurs quickly after the discontinuation of the drug. The "classic" triad of fever, rash, and eosinophilia is present in less than 5% to 10% of patients. Early recognition is crucial as patients can ultimately develop chronic kidney disease. It is important to establish a temporal relationship to the onset of the medication and the initiation of the symptoms. Oftentimes, the medication may have been discontinued before the appearance of the first symptom, so a review of medications from several weeks before the symptoms is also important. In addition, because the host immune response plays a role in some of the IgE-mediated reactions, it is important to review any immunocompromising chronic or acute illnesses or states that the patient may have or is currently experiencing. This should include vital signs of temperature, respiratory, and hydration status. The skin examination is important, as are appropriate evaluation and documentation of the type of lesion or lesions present. Although additional autoimmune or antibody testing may be done, caution is suggested. There may not be a high yield on these tests, and they can be quite costly for patients. Management Anaphylaxis Anaphylaxis can be a fatal drug hypersensitivity reaction because of its rapid onset. It is often underrecognized and undertreated because it can mimic other conditions and is variable in its presentation. However, respiratory compromise and cardiovascular collapse are of greatest concern, because they are the most common causes of death. Urticaria and angioedema are the most common manifestations but may be delayed or absent. The more quickly anaphylaxis occurs after exposure to the offending agent, the more likely the reaction is to be severe and potentially life threatening. Most anaphylaxis episodes are IgE-mediated reactions resulting in a sudden mast cell and basophil degranulation. Most cases of IgE-mediated drug anaphylaxis in the United States are due to penicillins and cephalosporins. Antibiotics are also the most common cause of perioperative anaphylaxis because skin eruptions may be missed in patients who are draped during surgery. Certain drugs, such as opioids, dextrans, and protamine, can cause a direct release of histamine and other mediators from mast cells and basophils. Finally, there are acute systemic reactions without any obvious triggers or mechanisms (idiopathic anaphylaxis). Anaphylaxis is a clinical diagnosis with a short window of treatment time available. Initially, the patient will describe flushing, pruritus, and a sense of impending doom. This includes any over-the-counter medications, herbal supplements, or Angioedema Angioedema is characterized by a deep dermal, subcutaneous, mucosal swelling. Angioedema can progress rapidly from a mild swelling of the oral mucosal to a life-threatening laryngeal edema. With this rapid sequence of events, the most important part of treatment is obtaining and maintaining a patent airway. Once the airway is patent, the patient should be treated with H1 antihistamines, H2 blockers, and steroids. H1 antihistamines such as diphenhydramine and hydroxyzine (Atarax) are effective in relieving pruritus but can cause significant sedation. Therefore second-generation H1 antihistamines1 (loratadine [Claritin], cetirizine [Zyrtec], desloratadine [Clarinex], fexofenadine [Allegra]) are often chosen for outpatient therapy. Doxepin (Sinequan),1 a tricyclic antidepressant with potent H1 and H2 blocker activities, can be used as an alternative to H1 antihistamines. However, it should not be used as first-line treatment for acute urticaria and angioedema because of its significant side effects of severe sedation, dry mouth, and weight gain. Further trial of the medication is not recommended, because the patient will respond more quickly and with more severe symptoms on reintroduction. The rate of cross-reactivity between penicillin and cephalosporins has been historically cited to be as high as 10%. The degree of cross-reactivity is highest between penicillins and first-generation cephalosporins, which have identical R-group side chains. In this case amoxicillin would be cross-reactive with cefadroxil (Duricef) and cefprozil (Cefzil), whereas ampicillin would be with cefaclor and cephalexin. Because of the differences in the chemical structures, second- and third-generation cephalosporins (cefdinir [Omnicef], cefuroxime [Ceftin], cefpodoxime [Vantin], and ceftriaxone [Rocephin]) are unlikely to be associated with cross-reactivity with penicillin. According to the latest guidelines for acute otitis media from the American Academy of Pediatrics and American Academy of Family Physicians, alternative initial antibiotics in patients with penicillin allergy include cefdinir, cefuroxime, cefpodoxime, or ceftriaxone. Patients with penicillin allergy who have a negative skin-test result to penicillin (major and minor determinants) may safely receive cephalosporins. Cephalosporin treatment of patients with penicillin allergy who did not have a severe or recent penicillin reaction history shows a reaction rate of 0.
Buy cheap nicotinell 35 mg online
This phenomenon quit smoking 17 days order nicotinell us, known as the hook effect, produces a falsely low reading that could lead to the misdiagnosis of a macroprolactinoma as a nonfunctioning pituitary tumor. This artifact can be circumvented by repeating the assay with a 100-fold diluted sample. Many laboratories also opt for an additional washout step to eliminate excess prolactin before adding the signal antibody, preempting the artifact. Macroprolactinemia is another potential diagnostic pitfall masquerading as true hyperprolactinemia. Macroprolactins are Neuroimaging Visual Field Testing A formal visual field test with a perimeter is recommended when suprasellar extension of a pituitary adenoma brings it close to the optic chiasm. Improvement or worsening in visual field often precedes imaging evidence of tumor shrinkage or expansion during treatment. Therefore visual field testing is an excellent monitoring tool for patients under treatment for macroadenoma and visual impairment. Diagnosis Prolactin testing is usually prompted by suggestive signs and symptoms of hyperprolactinemia such as menstrual abnormalities, infertility, and galactorrhea. A careful history, including medication use, physical examination, and routine laboratory evaluation (see preceding sections), is invaluable for uncovering secondary causes. Pituitary imaging should be performed when no other underlying causes are found especially if the levels of prolactin are higher than 100 ng/mL. Differential Diagnosis An exhaustive list of etiologies has been provided in Table 1. Despite its longer half-life, as long as cabergoline is discontinued in early pregnancy, it also has not been found to be associated with adverse outcomes. Until there is incontrovertible evidence for the absolute safety of these dopamine agonists, however, it is prudent to discontinue these drugs as soon as pregnancy is confirmed. Given its shorter half-life and established safety record, bromocriptine is the preferred agent for fertility induction in women with hyperprolactinemia, although cabergoline would also be acceptable if bromocriptine is not tolerated. The major indication to treat prolactinomas medically during pregnancy is the concern for tumor expansion. This risk can be significantly reduced if the patient has been treated with a dopamine agonist for at least a year with evidence of tumor shrinkage, or has undergone pituitary surgery or radiotherapy prior to pregnancy. For patients who fail to achieve tumor shrinkage with dopamine agonists or cannot tolerate them, prophylactic surgery prior to pregnancy may be considered, after careful discussion with the patient on surgical risks and the possibility of permanent hypopituitarism, which further impairs fertility. The Endocrine Society practice guidelines recommend against measurement of serum prolactin levels during pregnancy. They should not take either bromocriptine or cabergoline, however, as both are secreted in the milk. A small fraction of these patients have malignant prolactinoma, which is defined by extrapituitary metastasis; histopathologically, malignant prolactinomas can appear very similar to aggressive prolactinomas. An alkylating agent, temozolomide (Temodar)1, has been successfully used in the treatment of aggressive pituitary adenoma and pituitary carcinoma. In contrast, elderly patients can present with apathetic hyperthyroidism, which can be confused with hypothyroidism. Management of Prolactinoma During Pregnancy Mild hyperprolactinemia is part of normal pregnancy, and there are concerns for the safe use of dopamine agonists in pregnant women. There is convincing evidence that as long as bromocriptine is withdrawn within a week after confirmation of pregnancy, obstetric outcome is not altered. Less robust data to date suggest that continuing bromocriptine treatment till term is also safe. For patients with macroprolactinoma, however, symptomatic tumor expansion during pregnancy can occur in up to about 30% of cases. Until these conditions are met, women of childbearing age with macroprolactinomas should be advised to take nonhormonal contraceptive measures. Instead the patient should be followed clinically for any signs or symptoms of tumor expansion. If tumor expansion is confirmed, the patient should be reinitiated on bromocriptine. Debulking surgery is reserved for patients failing or not tolerating medical treatment. Lactation usually does not cause tumor progression, and patients are encouraged to breastfeed their infants with close surveillance. Management of Resistant and Malignant Prolactinoma Several other treatment options are available for patients who fail the highest tolerated doses of dopamine agonists, surgery, and radiation. Monotherapy with temozolomide has been established as the first-line chemotherapy for these conditions, following documented tumor growth despite standard therapies. Long-term management with radioiodine thyroid gland ablation is often pursued once symptoms are controlled. A small number of patients ($10%) have persistent hypothyroidism after an episode of illness. Like other autoimmune diseases, women are at higher risk (seven to eight times) than men. It usually occurs after age 50 years, is more common in women, and follows several decades of multinodular thyroid disease. Amiodarone is about one third iodine and can cause hyperthyroidism either through iodine-induced thyroid damage or from increased thyroxine synthesis owing to excessive iodine. This condition is most common with mild forms of hyperthyroidism but also can be observed transiently in thyroiditis. Subclinical hyperthyroidism is more common in individuals over age 70 and those with iodinedeficient diets. Epidemiology Risk Factors There are no known environmental or reversible risk factors for any of the causes of hyperthyroidism. Patients who develop a toxic nodular goiter usually have a long history of many other nodules that spontaneously burn out over time, but then develop a single large nodule (usually 2. The inflammation resulting in thyroiditis is thought to be related to subacute viral infections or autoimmune reactions; suppurative thyroiditis is a rare bacterial thyroid infection, usually caused by Staphylococcus aureus. During the acute period of thyroid inflammation, damage to the gland leads to the release of stored thyroxine from thyroid lakes, producing hyperthyroidism. However, after the initial release of thyroid hormone from the stored lakes, damage to the gland inhibits production of new thyroxine. After the initial surge in thyroid hormone levels, thyroxine levels drop, often to levels that can result in transient hypothyroidism. Most patients return to the euthyroid state after the thyroid gland heals, but about 10% of patients with acute thyroiditis remain chronically hypothyroid. Other, less common causes of hyperthyroidism include excessive exogenous administration of thyroid medications. This is most commonly the result of over-replacement of thyroxine (Levoxyl, Synthroid) in patients with hypothyroidism, but it may be intentional for weight loss. Because thyroxine and triiodothyronine (T3) are highly protein bound, over-replacement is most common if patients experience hypoproteinemia, such as in nephrotic syndrome, cirrhosis, or malnutrition. Excessive iodine consumption, referred to as the Jod-Basedow effect, can also lead to thyrotoxicosis. The source of the iodine may include iatrogenic sources such as iodine-containing medications or radiologic contrast agents.
