
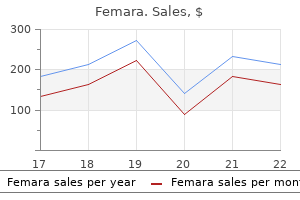
Femara 2.5 mg online
Barbiturates may protect the brain from transient episodes of focal ischemia (eg menstrual type cramps 37 weeks order 2.5mg femara mastercard, cerebral embolism) but probably do not protect from global ischemia (eg, cardiac arrest). Abundant animal data document these effects, but the clinical data are sparse and inconsistent. Some patients relate a taste sensation of garlic, onions, or pizza during induction with thiopental. Barbiturates do not produce muscle relaxation, and some induce involuntary skeletal muscle contractions (eg, methohexital). Renal Barbiturates reduce renal blood flow and glomerular filtration rate in proportion to the fall in blood pressure. Chronic exposure to barbiturates leads to induction of hepatic enzymes and an increased rate of metabolism. On the other hand, binding of barbiturates to the cytochrome P-450 enzyme system interferes with the biotransformation of other drugs (eg, tricyclic antidepressants). Barbiturates promote aminolevulinic acid synthetase, which stimulates the formation of porphyrin (an intermediary in heme synthesis). This may precipitate acute intermittent porphyria or variegate porphyria in susceptible individuals. Sulfur-containing thiobarbiturates evoke mast cell histamine release in vitro, whereas oxybarbiturates do not. Ethanol, opioids, antihistamines, and other central nervous system depressants potentiate the sedative effects of barbiturates. Substitutions at various positions on these rings affect potency and biotransformation. Diazepam and lorazepam are insoluble in water so parenteral preparations contain propylene glycol, which can produce venous irritation. Diazepam and lorazepam are well absorbed from the gastrointestinal tract, with peak plasma levels usually achieved in 1 and 2 h, respectively. In contrast, midazolam and lorazepam are well absorbed after intramuscular injection, with peak levels achieved in 30 and 90 min, respectively. Slow hepatic extraction and a large volume of distribution (Vd) result in a long elimination half-life for diazepam (30 h). Although lorazepam also has a low hepatic extraction ratio, its lower lipid solubility limits its Vd, resulting in a shorter elimination half-life (15 h). Nonetheless, the clinical duration of lorazepam is often quite prolonged due to increased receptor affinity. These differences between lorazepam and diazepam underscore the low utility of individual pharmacokinetic half-lives in guiding clinical practice (see Chapter 7). Enterohepatic circulation produces a secondary peak in diazepam plasma concentration 6 to 12 h following administration. Cardiovascular Benzodiazepines display minimal left-ventricular depressant effects, even at general anesthetic doses, except when they are coadministered with opioids (these agents interact to produce myocardial depression and arterial hypotension). Benzodiazepines given alone decrease arterial blood pressure, cardiac output, and peripheral vascular resistance slightly, and sometimes increase heart rate. This depression is usually insignificant unless the drugs are administered intravenously or given 3 with other respiratory depressants. Ventilation must be monitored in all patients receiving intravenous benzodiazepines (we recommend end-tidal B. The moderate lipid solubility of lorazepam accounts for its slower brain uptake and onset of action. Redistribution is fairly rapid for the benzodiazepines and, like the barbiturates, is responsible for awakening. Although we have used midazolam as an induction agent, none of the benzodiazepines can match the rapid onset and short duration of action of propofol or etomidate. Biotransformation the benzodiazepines rely on the liver for biotransformation into water-soluble glucuronidated end products. Cerebral Benzodiazepines reduce cerebral oxygen consumption, cerebral blood flow, and intracranial pressure but not to the extent the barbiturates do. The mild muscle-relaxing property of these drugs is mediated at the spinal cord level. The antianxiety, amnestic, and sedative effects seen at lower doses progress to stupor and unconsciousness at anesthetic doses. Compared with propofol or etomidate, induction with benzodiazepines is associated with a slower rate of loss of consciousness and a longer recovery. Drug Interactions Cimetidine binds to cytochrome P-450 and reduces the metabolism of diazepam. Erythromycin inhibits metabolism of midazolam and causes a two- to threefold prolongation and intensification of its effects. As previously mentioned, the combination of opioids and benzodiazepines markedly reduces arterial blood pressure and peripheral vascular resistance. This synergistic interaction has often been observed in patients undergoing cardiac surgery who received benzodiazepines for premedication and who received larger doses of opioids during induction of anesthesia. Benzodiazepines reduce the minimum alveolar concentration of volatile anesthetics as much as 30%. Ethanol, barbiturates, and other central nervous system depressants potentiate the sedative effects of the benzodiazepines. Ketamine functionally "dissociates" sensory impulses from the limbic cortex (which is involved with the awareness of sensation). Clinically, this state of dissociative anesthesia may cause the patient to appear conscious (eg, eye opening, swallowing, muscle contracture) but unable to process or respond to sensory input. Ketamine has effects on mood, and infusions of this agent are now being widely used to treat severe, treatment-resistant depression, particularly when patients have suicidal ideation. Small infusion doses of ketamine are also being used to supplement general anesthesia and to reduce the need for opioids both during and after the surgical procedure. Low-dose infusions of ketamine have been used for analgesia in postoperative patients and others who are refractory to conventional analgesic approaches. Ketamine has been identified by the World Health Organization as a key necessary agent. When intravenous access is lacking, ketamine is useful for intramuscular induction of general anesthesia in children and uncooperative adults. Ketamine can be combined with other agents (eg, propofol or midazolam) in small bolus doses or infusions for conscious sedation during procedures such as nerve blocks and endoscopy. Even subanesthetic doses of ketamine may cause hallucinations but usually do not do so in clinical practice, where many patients will have received at least a small dose of midazolam (or a related agent) for amnesia and sedation. Biotransformation Ketamine is biotransformed in the liver to several metabolites, one of which (norketamine) retains anesthetic activity. Patients receiving repeated doses of ketamine (eg, for daily changing of dressings on burns) develop tolerance, and this can only be partially explained by induction of hepatic enzymes. These indirect cardiovascular effects are due to central stimulation of the sympathetic nervous system and inhibition of the reuptake of norepinephrine after release at nerve terminals. Accompanying these changes are increases in pulmonary artery pressure and myocardial work. For these reasons, ketamine should be administered carefully to patients with coronary artery disease, uncontrolled hypertension, congestive heart failure, or arterial aneurysms. The direct myocardial depressant effects of large doses of ketamine, probably due to inhibition of calcium transients, are unmasked by sympathetic blockade (eg, spinal cord transection) or exhaustion of catecholamine stores (eg, severe end-stage shock).
Best femara 2.5 mg
Contemporary management of acute right ventricular failure: A statement from the heart failure association and the Working Group on Pulmonary Circulation and Right Ventricular Function of the European Society of Cardiology pregnancy over 35 cheap femara 2.5mg on line. The role of the vasculature in regulating venous return and cardiac output: Historical and graphical approach. Protective effects of anaesthetics in reversible and irreversible ischemia-reperfusion injury. Peri-operative levosimendan in patients undergoing cardiac surgery: An overview of the evidence. Pharmacologic versus direct-current electrical cardioversion of atrial flutter and fibrillation. Regardless of the level of preoperative blood pressure control, many patients with hypertension display an accentuated hypotensive response to induction of anesthesia, followed by an exaggerated hypertensive response to intubation. Autonomic-mediated increases in heart rate and blood pressure should be controlled with deeper planes of general anesthesia or adrenergic blockade, vasodilators, or a combination of these. The principal hemodynamic goals in managing mitral stenosis are to maintain a sinus rhythm (if present preoperatively) and to avoid tachycardia, large increases in cardiac output, and both hypovolemia and fluid overload by judicious administration of intravenous fluids. Anesthetic management of mitral regurgitation should be tailored to the severity of regurgitation as well as the underlying left ventricular function. Factors that exacerbate the regurgitation, such as slow heart rates and acute increases in afterload, should be avoided. Maintenance of normal sinus rhythm, heart rate, vascular resistance, and intravascular volume is critical in patients with aortic stenosis. Loss of a normally timed atrial systole often leads to rapid deterioration, particularly when associated with tachycardia. The compensatory increase in cardiac preload should be maintained, but excessive fluid replacement can readily result in pulmonary edema. Indirect vasopressors, such as ephedrine, are less effective than direct-acting agents because of the absence of catecholamine stores in myocardial neurons. Cardiovascular diseases-particularly hypertensive, ischemic, congenital, and valvular heart disease- are among the medical illnesses most frequently encountered in anesthetic practice and are a major cause of perioperative morbidity and mortality. The neuroendocrine response to surgical stimulation and the circulatory effects of anesthetic agents, endotracheal intubation, positive-pressure ventilation, blood loss, fluid shifts, and alterations in body temperature impose additional burdens on an often already compromised cardiovascular system. Even anesthetics that have no direct circulatory effects may cause apparent circulatory depression in severely compromised patients who are dependent on the enhanced sympathetic activity characteristic of heart failure or acute blood loss. Decreased sympathetic activity as a consequence of the anesthetized state can lead to acute circulatory collapse. Anesthetic management of patients with cardiovascular disease requires a thorough knowledge of normal cardiac physiology, the circulatory effects of the various anesthetic agents, and the pathophysiology and treatment of these diseases. The same principles used in treating cardiovascular diseases in patients not undergoing surgery should be used perioperatively. In most instances, the choice of anesthetic agent is not terribly important; on the other hand, knowing how the agent is used, understanding the underlying pathophysiology, and understanding how the two interact are critical. Patients with severe cardiovascular illnesses commonly undergo both cardiac and noncardiac surgery. Perioperative Cardiovascular Evaluation and Preparation for Noncardiac Surgery the prevalence of cardiovascular disease increases with advancing age. Moreover, the number of patients older than 65 years of age is expected to increase by 25% to 35% over the next two decades. The relatively high prevalence of cardiovascular disorders in surgical patients has given rise to attempts to define cardiac risk or the likelihood of intraoperative or postoperative fatal or life-threatening cardiac complications. The preoperative history should also address any past procedures, such as cardioverter defibrillator implants, coronary stents, and other interventions. The patient should be queried about other disease processes that frequently accompany heart disease. Cardiac patients often present with obstructive pulmonary disease, reduced kidney function, and diabetes mellitus. Do heavy work around the house like scrubbing floors or lifting or moving heavy furniture Participate in moderate recreational activities like golf, bowling, dancing, doubles tennis, or throwing a baseball or football Participate in strenuous sports like swimming, singles tennis, football, basketball, or skiing A brief self-administered questionnaire to determine functional capacity (the Duke Activity Status Index). The physical examination is especially useful in patients with certain conditions. For example, if a harsh systolic murmur suggestive of aortic stenosis is detected in a candidate for elective surgery, additional ultrasound evaluation will likely be warranted, as aortic stenosis substantially increases the risks in patients undergoing noncardiac surgery. Additionally, they grade the strength of the evidence upon which the recommendations is based as A (multiple randomized trials), B (limited trials, nonrandomized studies), and C (consensus of experts, case studies). Risks accrue secondary both to the nature of surgery and because of patient characteristics. Increased patient age and frailty are likewise associated with greater risk for acute coronary syndromes and stroke. Recently, studies have found a surprising number of asymptomatic patients with elevated levels of troponin after surgery. Some will have been effectively managed, but unfortunately, many others will not have been. Hypertension is a leading cause of death and disability in most Western societies and the most prevalent preoperative medical abnormality in surgical patients, with an overall prevalence of 20% to 25%. Long-standing uncontrolled hypertension accelerates atherosclerosis and hypertensive organ damage. Hypertension is a major risk factor for cardiac, cerebral, renal, and vascular disease. However, systolic blood pressures below 180 mm Hg, and diastolic pressures below 110 mm Hg, have not been associated with increased perioperative risks. When patients present with systolic blood pressures greater than 180 mm Hg and diastolic pressures greater than 110 mm Hg, anesthesiologists face the dilemma of delaying surgery to allow optimization of oral antihypertensive therapy, but adding the risk of a surgical delay versus proceeding with surgery and achieving blood pressure control with rapidly acting intravenous agents. The incidence of adverse cardiac events in patients treated and operated upon may be similar to that in patients delayed to allow for better long-term blood pressure control. Of note, patients with preoperative hypertension are more likely than others to develop intraoperative hypotension. Blood pressure measurements are affected by many variables, including posture, time of day, emotional state, recent activity, and drug intake, as well as the equipment and technique used. A diagnosis of hypertension cannot be made with one preoperative reading, but requires confirmation by a history of consistently elevated measurements. Although preoperative anxiety or pain may produce some degree of hypertension in normal patients, patients with a history of hypertension generally exhibit greater preoperative elevations in blood pressure. Epidemiological studies demonstrate a direct and continuous correlation between both diastolic and systolic blood pressures and mortality rates. The definition of systemic hypertension is arbitrary: a consistently elevated diastolic blood pressure greater than 90 mm Hg or a systolic pressure greater than 140 mm Hg. Whether patients with borderline hypertension are at some increased risk for cardiovascular complications remains unclear. Accelerated or severe hypertension is defined as a recent, sustained, and progressive increase in blood pressure, usually with diastolic blood pressures in excess of 110 to 119 mm Hg. A hypertensive urgency reflects blood pressure elevation of >180/120 mm Hg without signs of organ injury (eg, hypertensive encephalopathy, heart failure). A hypertensive emergency is characterized by severe hypertension (>180/120 mm Hg) often associated with papilledema, encephalopathy, or other organ injury.
| Comparative prices of Femara | ||
| # | Retailer | Average price |
| 1 | Target | 661 |
| 2 | Stater Bros. Holdings | 640 |
| 3 | Costco | 577 |
| 4 | Apple Stores / iTunes | 303 |
| 5 | Darden Restaurants | 949 |
| 6 | H-E-B | 810 |
Buy femara master card
The long axes of the bony and membranous labyrinths and of the pharyngotympanic tube and parallel tensor tympani and levator palatini muscles lie perpendicular to those of the tympanic membrane and cochlea women's health center dallas presbyterian hospital proven 2.5mg femara. Three auditory ossicles stretch from the lateral to the medial wall of the tympanic cavity. The pharyngotympanic tube is a communication between the anterior wall of the tympanic cavity and the lateral wall of the nasopharynx. The internal ear is composed of a closed system of 2190 membranous tubes and bulbs, the membranous labyrinth, which is filled with a fluid called endolymph (orange) and bathed in surrounding fluid called perilymph (purple). The tegmen tympani, forming the roof of the tympanic cavity and the mastoid antrum, is fairly thick in this specimen; usually, it is extremely thin. In this view of the middle ear, the carotid (anterior) wall of the tympanic cavity has been removed. The tympanic membrane forms most of the membranous (lateral) wall; superior to it is the epitympanic recess, in which are housed the larger parts of the malleus and incus. Branches of the tympanic plexus provide innervation to the mucosa of the middle ear and adjacent pharyngotympanic tube. However, one branch, the lesser petrosal nerve, is conveying presynaptic parasympathetic fibers to the otic ganglion for secretomotor innervation of the parotid gland. The contents of the middle ear include the following: Auditory ossicles (malleus, incus, and stapes). The membranous (lateral) wall is formed almost entirely by the peaked convexity of the tympanic membrane; superiorly, it is formed by the lateral bony wall of the epitympanic recess. The handle of the malleus is attached to the tympanic membrane, and its head extends into the epitympanic recess. The labyrinthine (medial) wall (medial wall) separates the tympanic cavity from the internal ear. It also features the promontory of the labyrinthine wall, formed by the initial part (basal turn) of the cochlea, and the oval and round windows, which, in a dry cranium, communicate with the internal ear. The mastoid wall (posterior wall) features an opening in its superior part, the aditus (L. The canal for the facial nerve descends between the posterior wall and the antrum, medial to the aditus. The anterior carotid wall separates the tympanic cavity from the carotid canal; superiorly, it has the opening of the pharyngotympanic tube and the canal for the tensor tympani. This structure forms the tegmental wall (roof) for the ear cavities and is also part of the floor of the lateral part of the middle cranial fossa. The antrum and mastoid cells are lined by mucous membrane that is continuous with the lining of the middle ear. The pharyngotympanic tube is lined by mucous membrane that is continuous posteriorly with that of the tympanic cavity and anteriorly with that of the nasopharynx. The function of the pharyngotympanic tube is to equalize pressure in the middle ear with the atmospheric pressure, thereby allowing free movement of the tympanic membrane. By allowing air to enter and leave the tympanic cavity, this tube balances the pressure on both sides of the membrane. Because the walls of the cartilaginous part of the tube are normally in apposition, the tube must be actively opened. It is opened by a combination of the expanding girth of the belly of the levator veli palatine, as it contracts longitudinally, pushing against one wall and the tensor veli palatini pulling on the other. Because these are 2193 muscles of the soft palate, equalizing pressure ("popping the eardrums") is commonly associated with activities such as yawning and swallowing. The deeply placed ascending pharyngeal artery is the only medial branch of the external carotid artery. It supplies the pharynx, palatine tonsil, pharyngotympanic tube, and the medial wall of the tympanic cavity before it terminates by sending meningeal branches to the cranial cavity. The branches of the first (mandibular) part supply 2194 the external acoustic meatus and tympanic membrane. The middle meningeal artery sends branches to the pharyngotympanic tube before entering the cranium through the foramen spinosum. These ossicles are the first bones to be fully ossified during development and are essentially mature at birth. The ossicles are covered with the mucous membrane lining the tympanic cavity; but unlike other bones, they lack a surrounding layer of osteogenic periosteum. The neck of the malleus lies against the flaccid part of the tympanic membrane, and the handle of the malleus is embedded in the tympanic membrane, with its tip at the umbo; thus, the malleus moves with the membrane. The head of the malleus articulates with the incus; the tendon of the tensor tympani inserts into its handle near the neck. The malleus functions as a lever, with 2196 the longer of its two processes and its handle attached to the tympanic membrane. The long limb lies parallel to the handle of the malleus, and its interior end articulates with the stapes by way of the lenticular process, a medially directed projection. The short limb is connected by a ligament to the posterior wall of the tympanic cavity. The base (footplate) of the stapes fits into the oval window on the medial wall of the tympanic cavity. The base of the stapes is considerably smaller than the tympanic membrane; as a result, the vibratory force of the stapes is increased approximately 10 times over that of the tympanic membrane. Two muscles dampen or resist movements of the auditory ossicles; one also dampens movements (vibration) of the tympanic membrane. The muscle inserts into the handle of the malleus and pulls the handle medially, which tenses the tympanic membrane, reducing the amplitude of its oscillations. This action tends to prevent damage to the internal ear when one is exposed to loud sounds. The tendon of the stapedius enters the tympanic cavity by emerging from a pinpoint foramen in the apex of the eminence and inserts on the neck of the stapes. The stapedius pulls the stapes posteriorly and tilts its base in the oval window, thereby tightening the anular ligament and reducing the oscillatory range. The membranous labyrinth, containing endolymph, is suspended within the perilymph-filled bony labyrinth, either by delicate filaments similar to the filaments of arachnoid mater that traverse the subarachnoid space or by the substantial spiral ligament. These fluids are involved in stimulating the end organs for balance and hearing, respectively. This view of the interior of the base of the cranium shows the temporal bone and the location of the bony 2199 labyrinth. The walls of the bony labyrinth have been carved out of the petrous temporal bone. A similar view of the bony labyrinth occupied by perilymph and the membranous labyrinth is shown. The membranous labyrinth, shown after removal from the bony labyrinth, is a closed system of ducts and chambers filled with endolymph and bathed by perilymph. It has three parts: the cochlear duct, which occupies the cochlea; the saccule and utricle, which occupy the vestibule; and the three semicircular ducts, which occupy the semicircular canals. The lateral semicircular duct lies in the horizontal plane and is more horizontal than it appears in this drawing. The otic capsule is made of bone that is denser than the remainder of the petrous temporal bone and can be isolated (carved) from it using a dental drill. The otic capsule is often erroneously illustrated and identified as being the bony labyrinth. However, the bony labyrinth is the fluidfilled space, which is surrounded by the otic capsule. Thus, the bony labyrinth is most accurately represented by a cast of the otic capsule after removal of the surrounding bone. The modiolus contains canals for blood vessels and for distribution of the branches of the cochlear nerve. The apex of the cone-shaped modiolus, like the axis of the tympanic membrane, is directed laterally, anteriorly, and inferiorly. An isolated, cone-like, bony core of the cochlea, the modiolus, is shown after the turns of the cochlea are removed, leaving only the spiral lamina winding around it like the thread of a screw.
Generic femara 2.5mg online
Overall women's health center southington ct order femara 2.5 mg otc, anticholinergic drugs do not reliably reduce the risk of aspiration pneumonia and can reverse the protective effects of metoclopramide. If the full stomach is due to recent food intake and the surgical procedure is elective, the operation should be postponed. If the risk factor is not reversible (eg, large hiatal hernia) or the case is emergent, proper anesthetic technique can minimize the risk of aspiration pneumonia. Regional anesthesia with minimal sedation should be considered in patients at increased risk for aspiration pneumonia. As in every anesthetic case, the availability of suction must be confirmed before induction. A rapidsequence induction (or, depending upon airway examination, an awake intubation) is indicated. A wide assortment of blades, video laryngoscopes, intubation bougies, and endotracheal tubes are prepared in advance and immediately available. An assistant may apply firm pressure over the cricoid cartilage prior to induction (Sellick maneuver). Because the cricoid cartilage forms an uninterrupted and incompressible ring, pressure over it is transmitted to underlying tissue. The esophagus is collapsed, and passively regurgitated gastric fluid cannot reach the hypopharynx. Excessive cricoid pressure (beyond what can be tolerated by a conscious person) applied during active regurgitation has been associated with rupture of the posterior wall of the esophagus. The patient is not artificially ventilated, to avoid filling the stomach with gas and thereby increasing the risk of emesis. Once spontaneous efforts have ceased or muscle response to nerve stimulation has disappeared, the patient is rapidly intubated. Cricoid pressure is maintained until the endotracheal tube cuff is inflated and tube position is confirmed. A modification of the classic rapid-sequence induction allows gentle ventilation as long as cricoid pressure is maintained. If intubation is still unsuccessful, spontaneous ventilation should be allowed to return and an awake intubation performed. After surgery, the patient should remain intubated until airway reflexes and consciousness have returned. The mainstay of therapy in patients who subsequently become hypoxic is positive-pressure ventilation. Intubation and the institution of positive end-expiratory pressure, or noninvasive ventilation, may be required. Bronchoscopy and pulmonary lavage are usually indicated when particulate aspiration has occurred. Use of corticosteroids is generally not recommended, and antibiotics are administered depending upon culture results. Rapid-sequence inductions are often associated with increases in intracranial pressure, arterial blood pressure, and heart rate. Describe the pathophysiology and clinical findings associated with aspiration pneumonia. Particulate aspirate will also result in small-airway obstruction and alveolar necrosis. The earliest physiological change following aspiration is intrapulmonary shunting, resulting in hypoxia. Other changes may include pulmonary edema, pulmonary hypertension, and hypercapnia. Hypotension signals significant fluid shifts into the alveoli and is associated with massive lung injury. Chest roentgenography may not demonstrate diffuse bilateral infiltrates for several hours after the event. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: Application to healthy patients undergoing elective procedures. An updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Aspiration prophylaxis and rapid sequence induction for elective cesarean delivery; time to reassess old dogma. Preventive acetaminophen reduces postoperative opioid consumption, vomiting, and pain scores after surgery: Systematic review and meta-analysis. Gabapentin for postoperative pain management-a systemic review with meta-analyses and trial sequential analyses. Practice guidelines for the management of postoperative nausea and vomiting: Past, present and future. Neurokinin 1 and novel serotonin antagonists for postoperative and postdischarge nausea and vomiting. Perioperative pulmonary aspiration is infrequent and low risk in pediatric anesthetic practice. The anesthesiologist should not be expected to provide the risk-versus-benefit discussion for the proposed surgery or procedure; this is the responsibility and purview of the responsible surgeon or "proceduralist. Adequacy of long-term blood glucose control can be easily and rapidly assessed by measurement of hemoglobin A1c. In patients deemed at high risk for thrombosis (eg, those with certain mechanical heart valve implants or with atrial fibrillation and a prior thromboembolic stroke), chronic anticoagulants should be replaced by intramuscular low-molecularweight heparins or by intravenous unfractionated heparin. There are no good data to support restricting fluid intake (of any kind or any amount) more than 2 h before induction of general anesthesia in healthy patients undergoing elective procedures; moreover, there is strong evidence that nondiabetic patients who drink fluids containing carbohydrates and protein up to 2 h before induction of anesthesia suffer less perioperative nausea and dehydration than those who are fasted longer. Sensitive tests have a low rate of false-negative results and rarely fail to identify an abnormality when one is present, unnecessarily complicate defending a physician against otherwise unjustified allegations of malpractice. Additionally, this evaluation may include diagnostic tests, imaging procedures, or consultations from other physicians when indicated. An enhanced recovery may require "prehabilitation" with one or more of the following: smoking cessation, nutritional supplementation, an exercise regimen, and adjustment of medications. Inadequate preoperative planning and incomplete patient preparation commonly lead to avoidable delays, cancellations, complications, and costs. One purpose is to identify those patients whose outcomes likely will be improved by implementation of a specific medical treatment (which rarely may require that planned surgery be rescheduled). For example, a 60-year-old patient scheduled for elective total hip arthroplasty who also has unstable angina from left main coronary artery disease 1 the cornerstones of an effective preoperative would more likely survive if coronary artery bypass grafting is performed before rather than after the elective orthopedic procedure. Another purpose of the preoperative evaluation is to identify patients whose condition is so poor that the proposed surgery might only hasten death without improving the quality of life. For example, a patient with severe chronic lung disease, end-stage kidney disease, liver failure, and chronic heart failure likely would not survive to derive benefit from an 8-h, complex, multilevel spinal fusion with instrumentation. For example, the anesthetic plan may need to be adjusted for a patient whose trachea appears difficult to intubate, one with a family history of malignant hyperthermia, or one with an infection near where a proposed regional anesthetic would be administered. Another purpose of the preoperative evaluation is to provide the patient with an estimate of anes2 thetic risk. However, the anesthesiologist should not be expected to provide the riskversus-benefit discussion for the proposed surgery or procedure; this is the responsibility and purview of the responsible surgeon or "proceduralist. Nonstandard monitors Positions other than supine Relative or absolute contraindications to specific anesthetic drugs Fluid management Special techniques Site (anesthetizing location) concerns 5 6 How will the patient be managed postoperatively Management of acute pain Intensive care Postoperative ventilation Hemodynamic monitoring 1 1 E Including need for (or need for avoidance of) muscle relaxation. Practice advisory for preanesthesia evaluation: An updated report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Finally, the preoperative evaluation presents an opportunity for the anesthesiologist to describe the proposed anesthetic plan in the context of the overall surgical and postoperative plan, provide the patient with psychological support, and obtain informed consent for the proposed anesthetic plan from the surgical patient. However, many other risk assessment tools are available, particularly in the area of cardiovascular risk assessment (see Chapter 21). How the patient responded to and recovered from previous anesthetics can be helpful. Elements of the Preoperative History Patients presenting for elective surgery and anesthesia typically require the recording of a focused A. Cardiovascular Issues Guidelines for preoperative cardiac assessment are regularly updated and available from the American College of Cardiology/American Heart Association and from the European Society of Cardiology (see Guidelines). A more complete discussion of cardiovascular assessment is provided in Chapter 21. The focus of preoperative cardiac assessment should be on determining whether the patient would benefit from further cardiac evaluation or interventions prior to the scheduled surgery. In general, the indications for cardiovascular investigations are the same in elective surgical patients as in any other patient with a similar medical condition.
Purchase femara 2.5 mg visa
Cerebral depression menstrual bleeding for 2 weeks generic 2.5mg femara otc, including sedation and amnesia, are prominent after scopolamine. Gastrointestinal Salivary secretions are markedly reduced by anticholinergic drugs. Dosage & Packaging As a premedication, atropine is administered intravenously or intramuscularly in a range of 0. Larger intravenous doses up to 2 mg may be required to completely block the cardiac vagal nerves in treating severe bradycardia. Clinical Considerations heart and bronchial smooth muscle and is the most efficacious anticholinergic for treating bradyarrhythmias. Patients with coronary artery disease may not tolerate the increased myocardial oxygen demand and decreased oxygen supply associated with the tachycardia caused by atropine. Atropine has been associated with mild postoperative memory deficits, and toxic doses are usually associated with excitatory reactions. Atropine should be used cautiously in patients with narrow-angle glaucoma, prostatic hypertrophy, or bladder-neck obstruction. Intravenous atropine is used in the treatment of organophosphate pesticide and nerve gas poisoning. Organophosphates inhibit acetylcholinesterase, resulting in overwhelming stimulation of nicotinic and muscarinic receptors that leads to bronchorrhea, respiratory collapse, and bradycardia. Atropine can reverse the effects of muscarinic stimulation but not the muscle weakness resulting from nicotinic receptor activation. Because of its pronounced mydriatic effects, scopolamine is best avoided in patients with closed-angle glaucoma. Potent inhibition of salivary gland and respiratory tract secretions is the primary rationale for using glycopyrrolate as a premedication. Heart rate usually increases after intravenous-but not intramuscular-administration. Clinical Considerations than atropine and causes greater central nervous system effects. Clinical dosages usually result in drowsiness and amnesia, although restlessness, dizziness, and delirium are possible. The sedative effects may be desirable for premedication but can interfere with awakening following short procedures. Eyedroppers vary in the number of drops formed per milliliter of solution, but average 20 drops/mL. Absorption by vessels in the conjunctival sac is similar to subcutaneous injection. Reactions from an overdose of anticholinergic medication involve several organ systems. The central anticholinergic syndrome refers to central nervous system changes that range from unconsciousness to hallucinations. Other systemic manifestations include dry mouth, tachycardia, atropine flush, atropine fever, and impaired vision. What other drugs possess anticholinergic activity that could predispose patients to the central anticholinergic syndrome Tricyclic antidepressants, antihistamines, and antipsychotics have antimuscarinic properties that could potentiate the side effects of anticholinergic drugs. Cholinesterase inhibitors indirectly increase the amount of acetylcholine available to compete with anticholinergic drugs at the muscarinic receptor. Physostigmine, a tertiary amine, is lipid soluble and effectively reverses central anticholinergic toxicity. Pharmacological treatment of organophosphorous insecticide poisoning: the old and the (possible) new. Clonidine decreases anesthetic and analgesic requirements and provides sedation and anxiolysis. Long-term use of these agents, particularly clonidine and dexmedetomidine, leads to super-sensitization and upregulation of receptors; with abrupt discontinuation of either drug, an acute withdrawal syndrome including hypertensive crisis can occur. As such, its administration should be viewed as a temporizing measure while the cause of hypotension is determined and remedied. Labetalol lowers blood pressure without reflex tachycardia because of its combination of and effects. Esmolol is an ultrashort-acting selective 1-antagonist that reduces heart rate and, to a lesser extent, blood pressure. The clinical effects of these drugs can be deduced from an understanding of the adrenoceptor physiology and a knowledge of which receptors each drug activates or blocks. Another anatomic difference is the greater distance from the sympathetic ganglion to the visceral structures. In contrast, acetylcholine is released by preganglionic sympathetic fibers and all parasympathetic fibers. Norepinephrine transporter located on neuronal cell membranes facilitates removal of norepinephrine from the synapse. Tricyclic antidepressants, cocaine, and amphetamines can inhibit these transporters leading to their clinical effects. In neurons norepinephrine may be metabolized by monoamine oxidase or repackaged into vesicles. Prolonged adrenergic activation leads to desensitization and hyporesponsiveness to further stimulation. Each of these has been further subdivided into at least two subtypes: 1 and 2, and 1, 2, and 3. The -receptors have been further divided using molecular cloning techniques into 1A, 1B, 1D, 2A, 2B, and 2C. The myocardium possesses 1-receptors that have a positive inotropic effect, which might play a role in catecholamine-induced arrhythmia. During myocardial ischemia, enhanced 1-receptor coupling with agonists is observed. Nonetheless, the most important cardiovascular effect of 1 stimulation is vasoconstriction, which increases peripheral vascular resistance, left ventricular afterload, and arterial blood pressure. Activation of these receptors increases intracellular calcium ion concentration, which leads to contraction of smooth muscles. Thus, 1-agonists are associated with mydriasis (pupillary dilation due to contraction of the radial eye muscles), bronchoconstriction, vasoconstriction, uterine contraction, and constriction of sphincters in the gastrointestinal and genitourinary tracts. Stimulation of 1-receptors 2-Receptors In contrast to 1-receptors, 2-receptors are located primarily on the presynaptic nerve terminals. This decreases the entry of calcium ions into the neuronal terminal, which limits subsequent exocytosis of storage vesicles containing norepinephrine. Thus, 2-receptors create a negative feedback loop that inhibits further norepinephrine release from the neuron. More importantly, stimulation of postsynaptic 2-receptors in the central nervous system causes sedation and reduces sympathetic outflow, which leads to peripheral vasodilation and lower blood pressure. Norepinephrine and epinephrine are equipotent on 1 receptors, but epinephrine is significantly more potent than norepinephrine on 2 receptors. The most important 1-receptors are located on the postsynaptic membranes in the heart. Stimulation of these receptors activates adenylyl cyclase, which converts adenosine triphosphate to cyclic adenosine monophosphate and initiates a kinase phosphorylation cascade. Initiation of the cascade has positive chronotropic (increased heart rate), dromotropic (increased conduction), and inotropic (increased contractility) effects. Their relative contribution to the response to intravenous catecholamines increases in patients with chronic heart failure. They share a common mechanism of action with 1-receptors: adenylyl cyclase activation.
Syndromes
- Frequent urination (due to high blood sugar)
- Losing weight
- General illness (from mild illnesses to serious conditions, such as operations, heart attacks, and pneumonia)
- Abdominal MRI
- Empty your bladder and bowel.
- Wash all raw fruits, vegetables, and herbs with cold, running water
- Future strokes
- Lumps or swelling in the testicles or scrotum
Buy discount femara 2.5 mg on-line
Defects of vision caused by compression of the optic pathway women's health center evergreen cheap femara 2.5mg mastercard, as may result from tumors of the pituitary gland or berry aneurysms of the internal carotid arteries (see Chapter 8, Head), may produce only part of the visual losses described here. Patients may not be aware of changes in their visual fields until late in the course of disease, because lesions affecting the visual pathway often develop insidiously. Lesions of the trochlear nerve or its nucleus cause paralysis of the superior oblique and impair the ability to turn the affected eyeball inferomedially. The characteristic sign of trochlear nerve injury is diplopia (double vision) when looking down. Diplopia occurs because the superior oblique normally assists the inferior rectus in depressing the pupil (directing the gaze downward) and is the only muscle to do so when the pupil is adducted. In addition, because the superior oblique is the primary muscle producing intorsion of the eyeball, the primary muscle producing extorsion (the inferior oblique) is unopposed when the superior oblique is paralyzed. Thus, the direction of gaze and rotation of the eyeball about its anteroposterior axis is different for the two eyes when an attempt is made to look downward and especially when looking downward and medially. The person can compensate for the diplopia by inclining the head anteriorly and laterally toward the side of the normal eye. It may be involved occasionally in poliomyelitis ("polio," a viral infantile disease) and generalized polyneuropathy, a disease affecting several peripheral nerves. The sensory and motor nuclei in the pons and medulla may be destroyed by intramedullary tumors or vascular lesions. Loss of the ability to appreciate soft tactile, thermal, or painful sensations in the face. Loss of corneal reflex (blinking in response to the cornea being touched) and the sneezing reflex (stimulated by irritants to clear the respiratory tract). Common causes of facial numbness are dental trauma, herpes zoster ophthalmicus (infection caused by a herpes virus), cranial trauma, head and neck tumors, intracranial tumors, and idiopathic trigeminal neuropathy (a nerve disease of unknown cause). Anesthesiologists often coordinate, or assist with, layout and design of surgical and procedural suites, including workflow enhancements. This article describes the major operating room features that are of special interest to anesthesiologists and the potential hazards associated with these systems. Culture of Safety Patients often think of the operating room as a safe place where the care given is centered around protecting the patient. Anesthesia providers, surgeons, nurses, and other medical personnel are responsible for carrying out critical tasks safely and efficiently. Unless members of the operating room team remain vigilant, errors can occur that may result in harm to the patient or to members of the operating room team. The best way of preventing serious harm to the patient or to the operating room team is by creating a culture of safety, which identifies and stops unsafe acts before harm occurs. One tool that fosters the safety culture is the use of a surgical safety checklist. Such checklists must be used prior to incision on every case and include components agreed upon by the facility as crucial. For checklists to be effective, they must first be used; second, all members of the surgical team must be focused on the checklist when it is being used. An example of a suboptimally executed checklist is one that is read in entirety, after which the surgeon asks whether everyone agrees. A better method is one that elicits a response after each point; eg, "Does everyone agree this patient is John Doe Optimal checklists do not attempt to cover every possibility, but address only key components, allowing them to be completed in less than 90 seconds. Some practitioners argue that checklists waste too much time; they fail to realize that cutting corners to save time often leads to problems later, resulting in a net loss of time and harm to the patient. If safety checklists were followed in every case, significant reductions would be seen in the incidence of preventable surgical complications such as wrong-site surgery, procedures on the wrong patient, retained foreign objects, and administration of a medication to a patient with a known allergy to that medication. Anesthesia providers are leaders in patient safety initiatives and should take a proactive role to utilize checklists and other activities that foster the culture of safety. Medical Gas Systems the medical gases commonly used in operating rooms are oxygen, nitrous oxide, air, and nitrogen. Although technically not a gas, vacuum exhaust for disposal or scavenging of waste anesthetic gas and surgical suction must also be provided, and these are considered integral parts of the medical gas system. Patients are endangered if medical gas systems, particularly oxygen, are misconfigured or malfunction. The anesthesiologist must understand the sources of the gases and the means of their delivery to the operating room to prevent or detect medical gas depletion or supply line misconnection. Oxygen is stored as a compressed gas at room temperature or refrigerated as a liquid. To guard against a hospital gas-system failure, the anesthesiologist must always have an emergency (E-cylinder) supply of oxygen available during anesthesia. If the oxygen is exhausted at a rate of 3 L/min, a cylinder that is half full will be empty in 110 min. Oxygen cylinder pressure should be assessed prior to use and periodically during use. Anesthesia machines usually also accommodate E-cylinders for medical air and nitrous oxide, and may accept cylinders of helium. Compressed medical gases utilize a pin index safety system for these cylinders to prevent inadvertent crossover and connections for different gas types. This pressure-relief "valve" is designed to rupture at 3300 psig, well below the pressure E-cylinder walls should be able to withstand (more than 5000 psig), preventing "overfilling" of the cylinder. Nitrous Oxide Nitrous oxide is almost always stored by hospitals in large H-cylinders connected by a manifold with an automatic crossover feature. Bulk liquid storage of nitrous oxide is economical only in very large institutions. If the liquefied nitrous oxide rises above its critical temperature, it will revert to its gaseous phase. Although a disruption in supply is usually not catastrophic, most anesthesia machines have reserve nitrous oxide E-cylinders. Because these smaller cylinders also contain nitrous oxide in its liquid state, the volume remaining in a cylinder is not proportional to cylinder pressure. By the time the liquid nitrous oxide is expended and the tank pressure begins to fall, only about 400 L of nitrous oxide remains. A higher reading implies gauge malfunction, tank overfill (liquid fill), or a cylinder containing a gas other than nitrous oxide. Because energy is consumed in the conversion of a liquid to a gas (the latent heat of vaporization), liquid nitrous oxide cools during this process. The drop in temperature results in a lower vapor pressure and lower cylinder pressure. The cooling is so pronounced at high flow rates that there is often frost on the tank, and the pressure regulator may freeze in such circumstances. Nitrogen Although compressed nitrogen is not administered to patients, it may be used to drive operating room equipment, such as saws, drills, and surgical handpieces. Nitrogen supply systems incorporate either the use of H-cylinders connected by a manifold or a wall system supplied by a compressor-driven central supply. Vacuum A central hospital vacuum system usually consists of independent suction pumps, each capable of handling peak requirements. Traps at every user location prevent contamination of the system with foreign matter. Excess suction may result in inadequate patient ventilation, and insufficient suction levels may result in the failure to evacuate waste anesthetic gases.
2.5mg femara overnight delivery
When a stimulus is sufficient to depolarize a patch of membrane women's health clinic baulkham hills cheap 2.5 mg femara free shipping, the signal can be transmitted as a wave of depolarization along the nerve membrane (an impulse). In peripheral nerves, A and C fibers have much slower conduction velocities, and their compound action potentials are longer and of less amplitude when compared with those from A fibers. The alpha2adrenergic agonists clonidine and guanfacine produce tonic and phasic block of conduction in rat sciatic nerve fibers. When local anesthetics bind a specific region of the subunit, they prevent channel activation and Na influx through the individual channels. Local anesthetic binding to Na channels does not alter the resting membrane potential. With increasing local anesthetic concentrations, an increasing fraction of the Na channels in the membrane bind a local anesthetic molecule and cannot conduct Na ions. As a consequence of more channels binding a local anesthetic, the threshold for excitation and impulse conduction in the nerve increases, the rate of rise and the magnitude of the action potential decreases, and impulse conduction velocity slows. At great enough local anesthetic concentrations (when a sufficient fraction of Na channels has bound a local anesthetic), action potentials can no longer be generated and impulse propagation is abolished. Local anesthetics have a greater affinity for the Na channel in the open or inactivated state than in the resting state. Depolarizations lead to open and inactivated channels; therefore, depolarization favors local anesthetic binding. Resting Nav channels activate and open when they are depolarized, briefly allowing Na ions to pass into the cell down their concentration gradient, then rapidly inactivate. Inactivated Nav channels return to the resting state as the cell membrane repolarizes. Extracellular Na ions conduct only through open Nav channels that have not bound a local anesthetic molecule. The Nav channel binding site for local anesthetics is nearer to the cytoplasmic than the extracellular side of the channel. Put another way, local anesthetic inhibition of Na channels is both voltage (membrane potential) and frequency dependent. Local anesthetic binding is greater when nerve fibers are firing and depolarizing frequently than with infrequent depolarizations. Conversely, other classes of drugs, notably tricyclic antidepressants (amitriptyline), meperidine, volatile anesthetics, Ca channel blockers, 2receptor agonists, and nerve toxins also may inhibit Na channels. Tetrodotoxin and saxitoxin are poisons that specifically bind Na channels at a site on the exterior of the plasma membrane. Human studies are under way with similar toxins to determine whether they might provide effective, prolonged analgesia after local infiltration, particularly when coadministered with local anesthetics. In comparing nerve fibers of the same type (myelinated versus unmyelinated), smaller diameter associates with increased sensitivity to local anesthetics. Thus, larger, faster-conducting A fibers are less sensitive to local anesthetics than smaller, slowerconducting A fibers. On the other hand, small unmyelinated C fibers are relatively resistant to inhibition by local anesthetics as compared with larger myelinated fibers. In a human peripheral nerve the onset of local anesthetic inhibition generally follow this sequence: autonomic before sensory before motor. But at steady state, if sensory anesthesia is present, usually all modalities are inhibited. Local anesthetics are weak bases that at physiological pH usually carry a positive charge at the tertiary amine group. Physicochemical properties of local anesthetics depend on the substitutions in the aromatic ring, the type of linkage in the intermediate chain, and the alkyl groups attached to the amine nitrogen. Potency is increased by adding large alkyl groups to a parent molecule (compare tetracaine with procaine, or bupivacaine with mepivacaine). The minimum concentration of local anesthetic that will block nerve impulse conduction is affected by several factors, including fiber size, type, and myelination; pH (an acidic environment antagonizes clinical nerve block); frequency of nerve stimulation; and electrolyte concentrations (hypokalemia and hypercalcemia antagonize blockade). Less potent, less lipid-soluble agents (eg, lidocaine or mepivacaine) generally have a faster onset than more potent, more lipid-soluble agents (eg, ropivacaine or bupivacaine). Local anesthetics with a pKa closest to physiological pH will have (at physiological pH) a greater fraction of nonionized base that more readily permeates the nerve cell membrane, generally facilitating a more rapid onset of action. It is the lipid-soluble free-base form that more readily diffuses across the neural sheath (epineurium) and through the nerve membrane. Curiously, once the local anesthetic molecule gains access to the cytoplasmic side of the Na channel, it is the charged cation (rather than the nonionized base) that more avidly binds the Na channel. The importance of pKa in understanding differences among local anesthetics is often overstated. It has been asserted that the onset of action of local anesthetics directly correlates with pKa. This is not supported by data; in fact, the agent of fastest onset (2-chloroprocaine) has the greatest pKa of all clinically used agents. Other factors, such as ease of diffusion through connective tissue, can affect the onset of action in vivo. The importance of the ionized and nonionized forms has many clinical implications for those agents that exist in both forms. As a direct consequence, these commercially formulated, epinephrine-containing preparations may have a lower fraction of free base and a slower onset than solutions to which the epinephrine is added by the clinician immediately prior to use. Similarly, the extracellular base-to-cation ratio is decreased and onset is delayed when local anesthetics are injected into acidic (eg, infected) tissues. Some researchers have found that alkalinization of local anesthetic solutions (particularly commercially prepared, epinephrine-containing ones) by the addition of sodium bicarbonate (eg, 1 mL 8. Interestingly, alkalinization also decreases pain during subcutaneous infiltration. Highly lipid-soluble local anesthetics have a longer duration of action, presumably because they more slowly diffuse from a lipid-rich environment to the aqueous bloodstream. Sustained-release systems using liposomes or microspheres can significantly prolong local anesthetic duration of action. Unfortunately, only bupivacaine and ropivacaine display some clinically useful selectivity (mostly during onset and offset of block) for sensory nerves; however, the concentrations required for surgical anesthesia almost always result in some motor blockade. Systemic absorption of injected local anesthetics depends on blood flow, which is determined by the following factors. Presence of additives-Addition of epinephrine- or less commonly phenylephrine-causes vasoconstriction at the site of administration. The consequent decreased absorption reduces the peak local anesthetic concentration in blood, facilitates neuronal uptake, enhances the quality of analgesia, prolongs the duration of analgesia, and limits toxic side effects. Vasoconstrictors have more pronounced effects on duration of shorter-acting than on longeracting agents. For example, addition of epinephrine to lidocaine usually extends the duration of anesthesia by at least 50%, but epinephrine has limited effect on the duration of bupivacaine peripheral nerve blocks. Epinephrine and clonidine can also augment analgesia through activation of 2-adrenergic receptors. Coadministration of dexamethasone or other steroids with local anesthetics can prolong blocks by up to 50%. Mixtures of local anesthetics (eg, ropivacaine and mepivacaine) produce nerve blocks with onset and duration that are intermediate between the two parent compounds. Local anesthetic agent-More lipid-soluble local anesthetics that are highly tissue bound are also more slowly absorbed than less lipid-soluble agents. Most mucous membranes (eg, tracheal or oropharyngeal mucosa) provide a minimal barrier to local anesthetic penetration, leading to a rapid onset of action. Intact skin, on the other hand, requires topical application of a high concentration of lipidsoluble local anesthetic base to ensure permeation and analgesia.
Femara 2.5mg mastercard
Lymph from the chin and central part of the lower lip drains to the submental lymph nodes women's health weight loss pills purchase femara discount. The hairless region between the eyebrows overlies the glabella, and the prominent ridges that extend laterally on each side above the eyebrows are the superciliary arches. They are joined at each end of the palpebral fissure between the eyelids at the medial and lateral angles (canthi) of the eye. The epicanthal fold 1948 (epicanthus) is a fold of skin that covers the medial angle of the eye in some people, chiefly Asians. The depressions superior and inferior to the eyelids are the suprapalpebral and infrapalpebral sulci. The external nose presents a prominent apex and is continuous with the forehead at the root of the nose (bridge). Inferior to the apex, the nasal cavity of each side opens anteriorly by a naris (plural = nares), bounded medially by the nasal septum and laterally by an ala (wing) of the nose. The vermillion border of the lip marks the beginning of the transitional zone (commonly referred to as the lip) between the skin and mucous membrane of the lip. The skin of the transitional zone is hairless and thin, increasing its sensitivity and causing its color to be different (because of underlying capillary beds) from that of the adjacent skin of the face. The lateral junction of the lips is the labial commissure; the angle between the lips, medial to the commissure, that increases as the mouth opens and decreases as it closes is the angle of the mouth. The median part of the upper lip features a tubercle, superior to which is a shallow groove, the philtrum (G. The musculofibrous folds of the lips continue laterally as the cheek, which also contains the buccinator muscle and buccal fat-pad. The cheek is separated from the lips by the nasolabial sulcus, which runs obliquely between the ala of the nose and the angle of the mouth. The lower lip is separated from the mental protuberance (chin) by the mentolabial sulcus. The lips, cheeks, and chin of the mature male grow hair as part of the secondary sex characteristics, the beard. The looseness of the subcutaneous tissue also enables fluid and blood to accumulate in the loose connective tissue following bruising of the face. As a person ages, the skin loses its resiliency (elasticity) resulting in ridges and wrinkles in the skin perpendicular to the direction of the facial muscle fibers. Skin incisions along these cleavage or wrinkle lines (Langer lines) heal with minimal scarring (see the clinical box "Skin Incisions and Scarring," in Chapter 1, Overview and Basic Concepts). Scalp Injuries Because the scalp arteries arising at the sides of the head are well protected by dense connective tissue and anastomose freely, a partially detached scalp may be replaced with a reasonable chance of healing as long as one of the vessels supplying the scalp remains intact. During an attached craniotomy (surgical removal of a segment of the calvaria with a soft tissue scalp flap to expose the cranial cavity), the incisions are usually made convex and upward, and the superficial temporal artery is included in the tissue flap. Nerves and vessels of the scalp enter inferiorly and ascend through layer two to the skin. Consequently, surgical pedicle scalp flaps are made so that they remain attached inferiorly to preserve the nerves and vessels, thereby promoting good healing. The arteries of the scalp supply little blood to the calvaria, which is supplied by the middle meningeal arteries. Therefore, loss of the scalp does not produce necrosis (death) of the calvarial bones. Because of the strength of this aponeurosis, superficial scalp wounds do not gape, and the margins of the wound are held together. Furthermore, deep sutures are not necessary when suturing superficial wounds because the epicranial aponeurosis does not allow wide separation of the skin. Deep scalp wounds gape widely when the epicranial aponeurosis is lacerated in the coronal plane because of the pull of the frontal and occipital bellies of the occipitofrontalis muscle in opposite directions (anteriorly and posteriorly). Scalp Infections the loose connective tissue layer (layer four) of the scalp is the danger area of the scalp because pus or blood spreads easily in it. Neither can a scalp infection spread laterally beyond the zygomatic arches because the epicranial aponeurosis is continuous with the temporal fascia that attaches to these arches. Because of the loose nature of the subcutaneous tissue within the eyelids, even a relatively slight injury or inflammation may result in an accumulation of fluid, causing the eyelids to swell. Blows to the periorbital region usually produce soft tissue damage because the tissues are crushed against the strong and relatively sharp margin. Ecchymoses (purple patches) develop as a result of extravasation of blood into the subcutaneous tissue and 1951 skin of the eyelids and surrounding regions. Sebaceous Cysts the ducts of sebaceous glands associated with hair follicles in the scalp may become obstructed, resulting in the retention of secretions and the formation of 1952 sebaceous cysts (pilar cysts). This benign condition frequently seen in neonates results from birth trauma that ruptures multiple, minute periosteal arteries that nourish the bones of the calvaria. However, observant clinicians study their action because of their diagnostic value. Habitual mouth breathing, caused by chronic nasal obstruction, for example, diminishes and sometimes eliminates the ability to flare the nostrils. Children who are chronic mouth breathers often develop dental malocclusion (improper bite) because the alignment of the teeth is maintained to a large degree by normal periods of occlusion and labial closure. Antisnoring devices have been developed that attach to the nose to flare the nostrils and maintain a more patent air passageway. The loss of tonus of the orbicularis oculi causes the inferior eyelid to evert (fall 1953 away from the surface of the eyeball). Thus, lacrimal fluid is not spread over the cornea, preventing adequate lubrication, hydration, and flushing of the surface of the cornea. If the injury weakens or paralyzes the buccinator and orbicularis oris, food will accumulate in the oral vestibule during chewing, usually requiring continual removal with a finger. When the sphincters or dilators of the mouth are affected, displacement of the mouth (drooping of its corner) is produced by contraction of unopposed contralateral facial muscles and gravity, resulting in food and saliva dribbling out of the side of the mouth. Weakened lip muscles affect speech as a result of an impaired ability to produce labial (B, M, P, or W) sounds. They frequently dab their eyes and mouth with a handkerchief to wipe the fluid 1954 (tears and saliva), which runs from the drooping lid and mouth. Infra-Orbital Nerve Block For treating wounds of the upper lip and cheek or, more commonly, for repairing the maxillary incisor teeth, local anesthesia of the inferior part of the face is achieved by infiltration of the infra-orbital nerve with an anesthetic agent. The injection is made in the region of the infra-orbital foramen, by elevating the upper lip and passing the needle through the junction of the oral mucosa and gingiva at the superior aspect of the oral vestibule. To determine where the infra-orbital nerve emerges, pressure is exerted on the maxilla in the region of the infra-orbital foramen. Because companion infra-orbital vessels leave the infra-orbital foramen with the nerve, aspiration of the syringe during injection prevents inadvertent injection of anesthetic fluid into a blood vessel. Because the orbit is located just superior to the injection site, a careless injection could result in passage of anesthetic fluid into the orbit, causing temporary paralysis of the extra-ocular muscles. Mental and Incisive Nerve Blocks Occasionally, it is desirable to anesthetize one side of the skin and mucous membrane of the lower lip and the skin of the chin. Injection of an anesthetic agent into the mental foramen blocks the mental nerve that supplies the skin and mucous membrane of the lower lip from the mental foramen to the midline, including the skin of the chin. Buccal Nerve Block 1955 To anesthetize the skin and mucous membrane of the cheek. It is characterized by sudden attacks of excruciating, lightening-like jabs of facial pain. The pain may be so intense that the person winces, thus the common term tic (twitch). In some cases, the pain may be so severe that psychological changes occur, leading to depression and even suicide attempts. The paroxysms are often set off by touching the face, brushing the teeth, shaving, drinking, or chewing. The pain is often initiated by touching an especially sensitive trigger zone, frequently located around the tip of the nose or the cheek (Haines, 2013). In most cases, this is caused by pressure of a small aberrant artery (Kiernan, 2013). Other scientists believe the condition is caused by a pathological process affecting neurons in the trigeminal ganglion.

Cheap 2.5 mg femara free shipping
The law recognizes that there are differences of opinion and varying schools of thought within the medical profession womens health birth control purchase femara 2.5 mg mastercard. An exception is the doctrine of res ipsa loquitur ("the thing speaks for itself"), which permits a finding of negligence based solely on the evidence. For example, if a set of car keys were visualized inside a patient on a chest radiograph after a thoracotomy, the doctrine of res ipsa loquitur would apply. Res ipsa loquitur could not be used in the case under discussion because the plaintiff would have to establish that cardiac arrest could not occur in the absence of negligence and that cardiac arrest could not have been due to something outside the control of the anesthesiologist. An important concept is that causation in civil cases in the United States need only be established by a preponderance of the evidence ("more likely than not")-as opposed to criminal cases, in which all elements of a charged offense must be proved "beyond a reasonable doubt. Thus, the preoperative and postoperative visits with the patient are often the only opportunities to establish a good relationship with the patient. Family members should also be included during these meetings with patients (provided the patient does not object), particularly during the postoperative visit if there has been an intraoperative complication. Adequacy of Informed Consent: Rendering care to a competent patient who does not consent constitutes assault and battery. The patient should be informed of the contemplated procedure, including its reasonably anticipated risks, its possible benefits, and the therapeutic alternatives. The physician may be liable for a complication-even if it is not due to the negligent performance of a procedure-if a jury is convinced that a reasonable person would have refused treatment if properly informed of the possibility of the complication. This does not mean, of course, that a documented consent relieves from liability physicians who violate the standard of care. Quality of Documentation: Careful documentation of the perioperative visits, informed consent, consultations with other specialists, intraoperative events, and postoperative care is essential. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine evidence-based guidelines (third edition). Practice guidelines for preoperative fasting and the use of pharmacological agents to reduce the risk of pulmonary aspiration: Application to healthy patients undergoing elective procedures: An updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Perioperative heparin bridging in atrial fibrillation patients requiring temporary interruption of anticoagulation: Evidence from meta-analysis. Development of a prediction rule for estimating postoperative pulmonary complications. The laryngeal mask airway partially protects the larynx from pharyngeal secretions, but not gastric regurgitation. The earliest evidence of bronchial intubation often is an increase in peak inspiratory pressure. The large negative intrathoracic pressures generated by a struggling patient in laryngospasm can result in the development of negative-pressure pulmonary edema, particularly in healthy patients. This article reviews the anatomy of the upper respiratory tract, describes necessary airway equipment, presents various management techniques, and discusses complications of laryngoscopy, intubation, and extubation. There are two openings to the human airway: the nose, which leads to the nasopharynx, and the mouth, which leads to the oropharynx. The pharynx is a U-shaped fibromuscular structure that extends from the base of the skull to the cricoid cartilage at the entrance to the esophagus. It opens anteriorly into the nasal cavity, the mouth, the larynx, and the nasopharynx, oropharynx, and laryngopharynx, respectively. The nasopharynx is separated from the oropharynx by an imaginary plane that extends posteriorly. At the base of the tongue, the epiglottis functionally separates the oropharynx from the laryngopharynx (or hypopharynx). The epiglottis prevents aspiration by covering the glottis-the opening of the larynx-during swallowing. The mucous membranes of the nose are innervated by the ophthalmic division (V1) of the trigeminal nerve anteriorly (anterior ethmoidal nerve) and by the maxillary division (V2) posteriorly (sphenopalatine nerves). The palatine nerves provide sensory fibers from the trigeminal nerve (V2) to the superior and inferior surfaces of the hard and soft palate. The olfactory nerve (cranial nerve I) innervates the nasal mucosa to provide the sense of smell. The glossopharyngeal nerve also innervates the roof of the pharynx, the tonsils, and the undersurface of the soft palate. The vagus nerve (cranial nerve X) provides sensation to the airway below the epiglottis. The superior laryngeal branch of the vagus divides into an external (motor) nerve and an internal (sensory) laryngeal nerve that provide sensory supply to the larynx between the epiglottis and the vocal cords. Another branch of the vagus, the recurrent laryngeal nerve, innervates the larynx below the vocal cords and the trachea. The muscles of the larynx are innervated by the recurrent laryngeal nerve, with the exception of the cricothyroid muscle, which is innervated by the external (motor) laryngeal nerve, a branch of the superior laryngeal nerve. The posterior cricoarytenoid muscles abduct the vocal cords, whereas the lateral cricoarytenoid muscles are the principal adductors. Anteriorly, the trachea consists of cartilaginous rings; posteriorly, the trachea is membranous. Unilateral denervation of a cricothyroid muscle causes very subtle clinical findings. Bilateral palsy of the superior laryngeal nerve may result in hoarseness or easy tiring of the voice, but airway control is not jeopardized. Unilateral injury to a recurrent laryngeal nerve results in paralysis of the ipsilateral vocal cord, causing deterioration in voice quality. Assuming intact superior laryngeal nerves, acute bilateral recurrent laryngeal nerve palsy can result in stridor and respiratory distress because of the remaining unopposed tension of the cricothyroid muscles. Airway problems are less frequent in chronic bilateral recurrent laryngeal nerve loss because of the development of various compensatory mechanisms (eg, atrophy of the laryngeal musculature). Bilateral injury to the vagus nerve affects both the superior and the recurrent laryngeal nerves. Thus, bilateral vagal denervation produces flaccid, midpositioned vocal cords similar to those seen after administration of succinylcholine. Although phonation is severely impaired in these patients, airway control is rarely a problem. Assessments include: Mouth opening: an incisor distance of 3 cm or greater is desirable in an adult. Class I: the entire palatal arch, including the bilateral faucial pillars, is visible down to the bases of the pillars. Although the presence of these examination findings may not be particularly sensitive for detecting a difficult intubation, the absence of these findings is predictive for relative ease of intubation. Increasingly, patients present with morbid obesity and body mass indices of 30 kg/m2 or greater. Although some morbidly obese patients have relatively normal head and neck anatomy, others have much redundant pharyngeal tissue and increased neck circumference. The anechoic area posterior to the trachea represents shadowing resulting from an attenuation of the ultrasound beam through the dense cartilage of the rings. The arrow points to a subtle area of increased echogenicity just distal to the tracheal cartilage. This area is where movement is most often visualized in real time during an intubation. The airway follows the curvature of the tongue, pulling it and the epiglottis away from the posterior pharyngeal wall and providing a channel for air passage. Oral & Nasal Airways Loss of upper airway muscle tone (eg, weakness of the genioglossus muscle) in anesthetized patients allows the tongue and epiglottis to fall back against the posterior wall of the pharynx. Repositioning the head or a jaw thrust is the preferred technique for opening the airway. Awake or lightly anesthetized patients with intact laryngeal reflexes may cough or even develop laryngospasm during airway insertion. Placement of an oral airway is sometimes facilitated by suppressing airway reflexes, and, in addition, sometimes by depressing the tongue with a tongue blade. The length of a nasal airway can be estimated as the distance from the nares to the meatus of the ear and should be approximately 2 to 4 cm longer than oral airways. Because of the risk of epistaxis, nasal airways are less desirable in anticoagulated or thrombocytopenic patients. Also, nasal airways (and nasogastric tubes) should be used with caution in patients with basilar skull fractures, as there has been a case report of a nasogastric tube entering the cranial vault.
2.5 mg femara sale
There are also many minute openings of the ducts of mucussecreting urethral glands into the spongy urethra breast cancer walk miami cheap femara online master card. Lymphatic vessels from the intermediate part of the urethra drain mainly into the internal iliac lymph nodes (Table 6. The innervation of the intermediate part of the urethra is the same as that of the prostatic part: autonomic (efferent) innervation via the prostatic nerve plexus, arising from the inferior hypogastric plexus. The sympathetic innervation is from the lumbar spinal cord levels via the lumbar splanchnic nerves, and the parasympathetic innervation is from the sacral levels via the pelvic splanchnic nerves. The visceral afferent fibers follow the parasympathetic fibers retrogradely to sacral spinal sensory ganglia. Internally, deep to the scrotal raphe, the scrotum is divided into two compartments, one for each testis, by a prolongation of the dartos fascia, the septum of the scrotum. The testes and epididymides and their coverings are described with the abdomen (see Chapter 5, Abdomen). The scrotum is divided into right and left halves by the cutaneous scrotal raphe, which is continuous with the penile and perineal raphes. The dorsum of the circumcised penis and the anterior surface of the scrotum are shown. The penis contains three erectile masses: two corpora cavernosa and a corpus spongiosum, which contains the spongy urethra. The skin of the penis extends distally as the prepuce, overlapping the neck and corona of the glans penis. Anterior scrotal arteries, terminal branches 1492 of the external pudendal arteries (from the femoral artery), supply the anterior aspect of the scrotum. The scrotum also receives branches from the cremasteric arteries (branches of the inferior epigastric arteries). The scrotal veins accompany the arteries, sharing the same names but draining primarily to the external pudendal veins. Lymphatic vessels from the scrotum carry lymph to the superficial inguinal lymph nodes (Table 6. The anterior aspect of the scrotum is supplied by derivatives of the lumbar plexus: anterior scrotal nerves, derived from the ilioinguinal nerve, and the genital branch of the genitofemoral nerve (Table 6. Sympathetic fibers conveyed by these nerves assist in the thermoregulation of the testes, stimulating contraction of the smooth dartos muscle in response to cold or stimulating the scrotal sweat glands while inhibiting contraction of the dartos muscle in response to excessive warmth. The 1494 anal canal is surrounded by the external anal sphincter, with an ischio-anal fossa on each side. The inferior anal (rectal) nerve branches from the pudendal nerve at the entrance to the pudendal canal and, with the perineal branch of S4, supplies the external anal sphincter. It is composed of three cylindrical cavernous bodies of erectile tissue: the paired corpora cavernosa dorsally and the single corpus spongiosum ventrally. In the anatomical position, the penis is erect; when the penis is flaccid, its dorsum is directed anteriorly. The body of the penis is the free pendulous part that is suspended from the pubic symphysis. The margin of the glans projects beyond the ends of the corpora cavernosa to form the corona of the glans. The corona overhangs an obliquely grooved constriction, the neck of the glans, which separates the glans from the body of the penis. The slit-like opening of the spongy urethra, the external urethral orifice (meatus), is near the tip of the glans penis. The skin of the penis is thin, darkly pigmented relative to adjacent skin and connected to the tunica albuginea by loose connective tissue. The ligament passes inferiorly and splits to form a sling that is attached to the deep fascia of the penis at the junction of its root and body. The fibers of the suspensory ligament are short and taut, anchoring the erectile bodies of the penis to the pubic symphysis. The superficial (dartos) fascia covering the penis has also been removed to expose the deep dorsal vein in the midline flanked by bilateral dorsal arteries and nerves. The ligament splits to surround the penis and then unites and blends inferiorly with 1497 the dartos fascia forming the scrotal septum. The fibers of the fundiform ligament are relatively long and loose and lie superficial (anterior) to the suspensory ligament. In addition, superficial and deep branches of the external pudendal arteries supply the penile skin, anastomosing with branches of the internal pudendal arteries. The deep arteries of the penis are the main vessels supplying the cavernous spaces in the erectile tissue of the corpora cavernosa and are, therefore, involved in the erection of the penis. When the penis is flaccid, these arteries are coiled, restricting blood flow; they are called helicine arteries of the penis (G. This vein passes between the laminae of the suspensory ligament of the penis, inferior to the inferior pubic ligament and anterior to the perineal membrane, to enter the pelvis, where it drains into the prostatic venous plexus. Blood from the skin and subcutaneous tissue of the penis drains into the superficial dorsal vein(s), which drain(s) into the superficial external pudendal vein. Sensory and sympathetic innervation is provided 1498 primarily by the dorsal nerve of the penis, a terminal branch of the pudendal nerve, which arises in the pudendal canal and passes anteriorly into the deep perineal pouch. The penis is richly supplied with a variety of sensory nerve endings, especially the glans penis. Cavernous nerves, conveying parasympathetic fibers independently from the prostatic nerve plexus, innervate the helicine arteries of the erectile tissue. The pudendal nerve 1499 conveys the majority of sensory, sympathetic, and somatic motor fibers to the perineum. Although originating from the same spinal cord segments from which the pudendal nerve is derived, the parasympathetic fibers of the cavernous nerves course independently of the pudendal nerve. With the exception of the cavernous nerves, parasympathetic fibers do not occur outside the head, neck, or cavities of the trunk. The cavernous nerves arise from the prostatic plexus of males and from the vesical plexus of females. They terminate on the arteriovenous anastomoses and helicine arteries of the erectile bodies, which, when stimulated, produce erection of the penis or engorgement of the clitoris and vestibular bulb in females. Reflective of their abdominal origins, lymph from the testes follow a route, independent of the scrotal drainage, along the testicular veins to the intermesenteric portion of the lumbar (caval/aortic) and pre-aortic lymph nodes. Lymphatic drainage from the intermediate and proximal parts of the urethra and cavernous bodies drains into the internal iliac lymph nodes, whereas most vessels from the distal spongy urethra and glans penis pass to the deep inguinal nodes, but some lymph passes to the external inguinal nodes. Details about the attachments, innervation, and actions of these muscles are provided in Tables 6. Lymphatic drainage of male urogenital triangle-penis, spongy urethra, scrotum, and testis. They cross the pelvic outlet like intersecting beams, supporting the perineal body to aid the pelvic diaphragm in supporting the pelvic viscera. Simultaneous contraction of the superficial perineal muscles (plus the deep transverse perineal muscle) during penile erection provides a firmer base for the penis. The bulbospongiosus muscles form a constrictor that compresses the bulb of the penis and the corpus spongiosum, thereby aiding in emptying the spongy urethra of residual urine and/or semen. At the same time, they also compress the deep dorsal vein of the penis, impeding venous drainage of the cavernous spaces and helping promote enlargement and turgidity of the penis. They force blood from the cavernous spaces in the crura into the distal parts of the corpora cavernosa, which increases the turgidity (firm distension) of the penis during erection. Contraction of the ischiocavernosus muscles also 1503 compresses the tributaries of deep dorsal vein of the penis leaving the crus of the penis, thereby restricting venous outflow from the penis and helping maintain the erection. Because of their function during erection and the activity of the bulbospongiosus subsequent to urination and ejaculation to expel the last drops of urine and semen, the perineal muscles are generally more developed in males than in females. Consequently, the helicine arteries straighten, enlarging their lumina and allowing blood to flow into and dilate the cavernous spaces in the corpora of the penis. The bulbospongiosus and ischiocavernosus muscles compress veins egressing from the corpora cavernosa, impeding the return of venous blood. As a result, the corpora cavernosa and corpus spongiosum become engorged with blood near arterial pressure, causing the erectile bodies to become turgid (enlarged and rigid), and an erection occurs. During emission, semen (sperms and glandular secretions) is delivered to the prostatic urethra through the ejaculatory ducts after peristalsis of the ductus deferentes and seminal glands. Prostatic fluid is added to the seminal fluid as the smooth muscle in the prostate contracts.
