
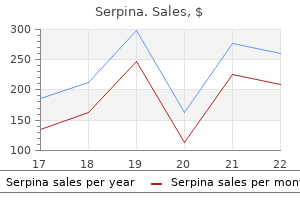
Purchase on line serpina
The media in common usage include carbon dioxide gas delivered through the hysteroflator at a maximum rate of 70 mL/min and pressure less than 100 mmHg anxiety chest tightness purchase 60 caps serpina with mastercard. This gives a clear panoramic view of the interior of the uterine cavity, but flattens soft pedunculated polypi against the uterine lining as against those seen as floating objects when liquid media are used. To provide adequate uterine distension, the intrauterine pressure needs to be 4050 mm of Hg. More sophisticated pressure systems are available for use during prolonged hysteroscopic operative procedures such as myomectomy, septum cutting or endometrial ablation where continuous flow of fluid is essential. In such cases, the distension medium must be nonionic (not normal saline) to prevent spread of electrical energy; also, the medium should not get admixed with blood as this would interfere with proper visualization of the ongoing operative procedure. Hyskon is a concentrated dextran solution (32% dextrose), not miscible with blood and with good optical qualities. Excess glycine can lead to problems of fluid overload and electrolyte disturbances. Hence, it cannot be overemphasized that strict monitoring of the amount of glycine used, its input and output must be accurately documented. Uterine perforation occurs in 110% mostly during insertion of the hysteroscope through the cervix and during operative procedures. This can be avoided by introducing the telescope under direct vision and performing surgery under laparoscopic guidance. Perforation is suspected when the distending medium escapes into the peritoneal cavity and uterine walls collapse with poor vision and fall in the intrauterine pressure. The perforation is managed by observation, laparoscopic coagulation of the bleeder or laparotomy. The injury is not diagnosed at the time of surgery unless perforation also occurs. The bleeding normally occurs as the medium is released and intrauterine pressure drops. The bleeding can be controlled by inserting the Foley catheter, distending its balloon with 30 mL saline and leaving it in the uterine cavity for 24 h for haemostasis. While allowing proper view and surgical procedures, the various distending media can increase the procedure morbidity. Fluid overload occurs in 4% cases, and leads to pulmonary oedema if deficit of fluid is more than 1000 mL and electrolyte imbalance occurs. Saline and dextrose cause hyponatraemia, hypokalaemia, haemolysis and encephalopathy. Hyskon Chapter 7 · Endoscopy in Gynaecology causes anaphylactic reaction, pulmonary oedema and encephalopathy, brain herniation and temporary blindness. Uterine rupture during pregnancy and late diagnosis of endometrial pathology are other complications. Salpingoscopy and Falloscopy In salpingoscopy, a fine salpingoscope 1 mm in diameter is introduced through the fimbrial end of the fallopian tube via the laparoscope, and ampullary portion studied after distending its lumen with saline. Flattening of mucosa, adhesions and mucus polyp can be recognized, and feasibility of tuboplasty considered. Hysteroscopic falloscopy reveals the tubal pathology of the cornual and interstitial end of the fallopian tube. The risks of these endoscopes are perforation, damage to the tubal mucosa, infection and difficulty in inserting the catheters. The colposcope is a binocular instrument providing a magnification of 1020 times and colpomicroscope 100 300 times using external light source. The purpose of the colposcope is to map the abnormal areas on the cervix so that selective biopsy can be obtained under magnification. Colposcopy is not needed routinely in all patients, or patients with obvious lesions. Only those with positive cervical cytology for malignant cells or suspicious cells but clinically normal-looking cervix need colposcopic study. No vaginal examination should be done prior to colposcopy, as with Pap smear, to avoid denuding the epithelium which will yield false-negative findings. Abnormal areas on the vagina and preoperative assessment in early stages of cancer cervix. Technique Colposcopy is best performed during the proliferative phase for optimal findings, though it can be performed any day of the cycle (but not during menstruation). The cervix is moist with mucus and the external os slightly patulous in the proliferative phase and exposes the squamocolumnar junction adequately. The patient is placed in lithotomy position, the cervix is exposed with a bivalve speculum and the colposcope focused on the external os at a distance of about 20 cm. The cervix is gently swabbed and cleaned with saline to remove mucus, taking care not to provoke bleeding. The squamocolumnar junction is brought into view and inspected before and after applying 35% aqueous acetic acid solution. Three per cent acetic acid is applied to a thin epithelium, but it takes more time to turn acetowhite. Viewing the acetowhite areas after interposing a green-light filter permits a more clear assessment of the vascular architecture. In a postmenopausal woman, it is desirable to administer oestrogen daily for 12 weeks to improve colposcopic findings and allow squamocolumnar junction to pout out of external os. Vaginal misoprostol (prostaglandin) 3 h before colposcopy can also dilate the cervix and allow endocervical visualization. Metaplasia is benign but atypical metaplasia developing under the adverse environment such as pH, hormonal influence (oestrogen), virus and mutagens become precursors of cancer cervix. Satisfactory colposcopic examination Columnar epithelium, squamous and squamocolumnar junction seen 2. Acetowhite area shows sharp margins and coarse mosaic pattern with irregular mosaic formed by the vessels running parallel to the surface. The vessels running perpendicular to the surface show up as irregular, large punctuate red spots. Endocervical curettage is required if the squamocolumnar junction is not entirely visible. During pregnancy, intense white appearance with coarse mosaics may be present, but the vessels are normal. Colposcopy can: n n Avoid unnecessary biopsy if the findings are normal Avoid cone biopsy Chapter 7 · Endoscopy in Gynaecology 109 Because of multifocal lesions, wide vaginal wall and viewing at an angle, colposcopic examination of the vagina is difficult. Toluidine blue shows heavy staining but does not give clue to the underlying pathology. Select the appropriate site of biopsy Reduce the size of biopsy and conization Therapeutic application of colposcopy. Colposcopic ablative techniques have been successfully employed in preinvasive cancer of the cervix and vagina. Colposcopy should be preferably restricted to first-trimester pregnancy, as it can cause bleeding, besides causing discomfort once fetal head enters the pelvis. Confocal endomicroscopy studies the depth of tissue up to dermis, and is recently employed as an adjuvant to colposcopy. Extragenital Endoscopy Endoscopic examination of other pelvic viscera of interest to the gynaecologist includes the urethra, urinary bladder, anal canal, rectum and the sigmoid colon. Preoperative ureteric catheterization in gynaecological malignancy or difficult operations involving large fibroids, broad ligament pathology, advanced endometriosis or anticipating dense pelvic adhesions and disturbed tissue plains safeguards against accidental ureteric injuries. Teaming up with a urologist and a proctologist can be mutually beneficial when treating a high-risk patient suffering from advanced pelvic pathology. It was used to visualize the pelvic organs and test the potency of fallopian tubes. Therapeutically, it was performed for tubal sterilization, removal of ectopic pregnancy and adnexal mass. With certain limitations and contraindications to laparoscopy being understood, culdoscopy is now occasionally employed (obesity and pelvic and abdominal scar adhesions contraindicate laparoscopy). Operative hysteroscopy is also performed effectively to correct several menstrual problems, mainly abnormal uterine bleeding. It helps in delineating suspicious areas in the squamocolumnar junction suggestive of preinvasive and invasive cancer of the cervix, and guides the clinician in planning out selective or a cone biopsy of the cervix in suspicious cases. Lifelong follow-up of women undergoing conservative treatment is important with colposcope.
Cheap 60caps serpina free shipping
If a complete tear of the perineum is treated by immediate suture anxiety symptoms 2 buy serpina online, the end result is satisfactory if correct anatomical reposition has been attained. If primary union of the vagina and the perineal skin is not obtained the wound should be kept clean and encouraged to granulate by frequent sitz baths. The end results are often functionally good in spite of the initial breakdown of the suture line. The bowels should be confined for at least 5 days, solid foods withheld and intestinal antiseptics given, along with stool softeners. Lately, instead of end-to-end suturing of the torn sphincter muscles, overlap technique is recommended to yield a stronger sphincteric control. Old-Standing Complete Tears Various degrees of complete perineal tears, usually resulting from careless attempts at immediate suturing, are not unusual. The red glistening mucous membrane of the anal canal and rectum protrudes and fuse directly with the vaginal wall without any of the perineal tissues intervening. Behind the anus are the radial folds in the skin which are corrugated by the underlying contracted subcutaneous sphincter. The external sphincter is only present posteriorly and the absence of the sphincteric grip is appreciated by inserting a finger into the anus. One of the most interesting features of the complete tear of the perineum is that it is very rarely if ever associated with prolapse, although the decussating fibres of the levator ani muscles have been torn through. The reason is that the patient continuously draws together the two levator ani muscles in an effort to close the bowel so that by constant use the tone of the muscles becomes exceptionally good. This firmness and good development of the levator muscles is found on clinical examination when the levator muscles are palpated. The technical difficulties are much greater in old cases than in those operated upon immediately after delivery. The optimum time for operation in the case of old tears is 36 months after delivery. If the operation is attempted earlier than this, healing by first intention is exceptional while if the operation is further delayed, dense scar tissue may be deposited which adds to the operative difficulties. Preoperative preparation is of importance, and the patient should be kept in the hospital for a couple of days before the operation during which time the bowels should be emptied by aperients and enemas, and the vagina disinfected by douching and by insertion of gauze packs soaked in flavine 1 in 1000 or Betadine lotion. The bacterial flora of the bowel should be controlled by phthalylsulphathiazole or neomycin, given in large doses for 3 days before the operation. The patient should be put on a nonresidual diet such as milk and fluid for 2 days prior to surgery. Various techniques have been described in the operative treatment of complete tears of the perineum, but the underlying principles are the same in all. The rectum must be dissected from the vagina by incising the intervening scar tissue and by dissecting upwards in the rectovaginal septum. Perhaps the most important step in the operation is to dissect the rectum clear of scar tissue and to mobilize it so that it can be brought down, without tension to the anal region. The tear in the rectum and anal canal is now repaired by excising scar tissue, freshening the cut edges and suturing them together with fine Vicryl sutures mounted on an atraumatic needle and tied within the bowel. The wound in the bowel is now invaginated with a layer of interrupted Lembert sutures. Next, the deep muscles of the perineal body and the levator ani are identified and sutured together with no. It is important to ensure that the muscles are dissected clear of scar tissue and are mobilized. The next important step in the operation is to suture together the torn edges of the external sphincter. These must be carefully defined, dissected clear of scar tissue and sutured together with three or four separate Vicryl sutures. The remains of the superficial muscles of the perineum are now sutured together with catgut and then the cut edges of the vagina and the perineum are repaired, interrupted catgut sutures being used. These principles are uniformly followed in the various methods described for the treatment of a complete tear of the perineum. Lately, many gynaecologists believe in overlap of sphincteric sutures to strengthen the tone and function of the sphincter, though others feel this overlap technique has no bearing on the surgical outcome. A few patients develop the tone of the levator muscles so well that they only suffer incontinence of flatus. These women will complain of incontinence of faeces only if they develop diarrhoea. The dotted line illustrates the position of the incision made in the operation of repair (a) and (d) represent the two ends of the torn fourchette, the dimples adjacent to (b) and (c) mark the situation of the cut edges of the external sphincter. Chapter 15 · Injuries of the Female Genital Tract 203 Vaginal Lacerations Vaginal lacerations commonly occur following assisted instrumental vaginal deliveries (forceps or vacuum extraction), difficult breech extractions, or following shoulder dystocia. It is a good practice to inspect the lower genital tract under a good light after expulsion of the placenta, identify all tears and suture them meticulously. Sometimes a cervical tear may extend to the vault of the vagina and cause profuse bleeding. Tears extending to the base of the broad ligament may lead to a broad ligament haematoma which may require recourse to a laparotomy for its evacuation. Extensive tears involving the sphincter of the cervix may lead to preterm deliveries or habitual painless mid-trimester abortions due to incompetent cervix, necessitating surgical cerclage in future pregnancies. In women with a flat pelvis, the anterior lip of the cervix may get caught between the fetal head and the pubic symphysis resulting in an anterior bucket handle tear. Rarely in women with a small gynaecoid pelvis, a trial of labour may result in circumferential ischaemic necrosis of the lower part of the cervix and end up with an annular detachment of the cervix. An area of scarred skin is excised and the mucous membrane of the anal canal freshened at the edge. Three structures must be defined, freed of scar tissue and mobilized, namely (A) the mucous membrane of the anal canal, (B) the external sphincter and (C) the levator ani muscles. First the edges of the anal canal mucosa must be sutured together, then the cut edge of the sphincter and lastly the levator muscles. Afterwards the cut edges of the posterior vaginal wall and the skin of the perineum are sutured. Rupture of the Uterus After Treatment the most important part of the after treatment is to keep the wound dry. The perineum should be swabbed after micturition and defaecation with antiseptic solution and subsequently powdered. To achieve this, the patient is given only intravenous fluids for the first 2 days and oral fluids the next 2 days. Sulphathiazole or neomycin administered preoperatively should be continued for at least a week postoperatively. Systemic chemotherapy is necessary to prevent infection and it should be given for a week. Another complication that may develop is a rectovaginal fistula which is usually the result of faulty technique but also may be due to infection and breakdown of sutures. Misuse of oxytocics, or dehiscence of a previous uterine scar (caesarean section), rarely a haematometra or pyometra, may rupture spontaneously as a result of distension and thinning of the atrophic myometrium. Depending upon the cause and extension of tear, suturing or hysterectomy is performed. Perforation of the Uterus In the nonpregnant state, perforation of the uterus occurs mainly during the operation of dilatation and curettage. The perforation is more common if the uterus is soft as in pregnancy and in malignancy. The atrophic uterus of a menopausal woman can easily be perforated during curettage for postmenopausal bleeding. The intrauterine device may perforate the wall of the uterus, but remains within the myometrium. In the presence of pyometra and malignancy, immediate hysterectomy is strongly advised. The repair of the intestinal injury or resection and end-to-end anastomosis will be required depending upon the extent of the damage to the intestine.
| Comparative prices of Serpina | ||
| # | Retailer | Average price |
| 1 | Macy's | 140 |
| 2 | Rite Aid | 565 |
| 3 | H-E-B | 820 |
| 4 | Big Lots | 457 |
| 5 | Neiman Marcus | 764 |
| 6 | Wendy's / Arby's Restaurants | 584 |
| 7 | Ruddick Corp. | 307 |
60 caps serpina
It occurs during adolescence and is symptomatic in up to 60% of those affected anxiety level scale safe 60 caps serpina, although it may also be found by chance on plain spine or chest x-rays requested for other reasons. Although the pathogenesis is uncertain, a hereditary weakening of the vertebral endplates present in affected patients is believed to allow disc material to encroach into the vertebral bodies. Therapy is usually symptomatic and aimed at minimizing the tendency toward kyphosis. Congenital hip dysplasia has an excellent prognosis if recognized soon after birth. Treatment usually involves splinting the legs in abduction, thus allowing the shallow acetabulum to fully contain the femoral head. If the diagnosis is missed, however, later therapy is often much more involved and may require extensive orthopedic surgery. A hip radiograph from an adult with congenital hip dysplasia that was not treated during childhood. BiBliography Castori M, Sinibaldi L, Mingarelli R, et al: Pachydermoperiostosis: an update, Clin Genet 68:477486, 2005. Never advise surgery for mechanical low back pain without objective signs and symptoms of a radiculopathy unresponsive to conservative therapy. Lidocaine injection of the facet joints can determine if facet joint arthritis is the pain generator. In up to 50% of patients, pain can persist long after the acute injury in spite of no abnormality being seen on any imaging study. The exact pathology is unclear although alar ligament injury has been demonstrated in many patients. Clinical variables associated with prolonged symptoms include: female, younger age, stationary vehicle, prior history of neck pain, severity of collision, not being at fault, and bored with present job. Whether or not compensation is available also contributes to the length and severity of symptoms. When evaluating a patient with neck pain, how can you differentiate between a bony or muscular disorder? Comparison of active and passive range of motion is useful for differentiating articular from soft-tissue disorders. Passive neck range of motion is best performed by supporting (cradling) the head while the patient is supine. The full range of the cervical spine may then be tested: flexion, extension, rotation, and lateral bending. During rotation and lateral bending, ipsilateral discomfort elicited in the direction of movement is suggestive of bony pain. Pain and/or tightness produced on the contralateral side usually implicates a muscular disorder. Passive range of motion (and provocative tests) should not be performed if instability or fracture of the cervical spine is suspected. What is the value of provocative tests for diagnosing cervical radiculopathy resulting from nerve root compression within the foramina of the cervical vertebrae? Provocative maneuvers vary in their sensitivity and specificity for diagnosing cervical radiculopathy. The sensitivity for each of the tests is about 30% lower for chronic cervical radiculopathy. The immediate development of pain and/or paresthesias with radiation to the upper limb (see below) is indicative of cervical radiculopathy. What physical findings enable you to identify the approximate level of common cervical nerve root lesions? Radial reflex is also called the supinator jerk (tap on brachioradialis muscle near distal end of radius). List the important questions that should be asked when obtaining a history from a patient with low back pain. P-Provocative and palliative factors: sitting (worse with diskogenic), walking (worse with spinal stenosis, relieved with forward flexion), supine (pain unrelieved if cancer or infection), Valsalva maneuver (worse with intrathecal or radicular process), lumbar extension (worse with spinal stenosis and facet arthritis) versus flexion (worse with lumbar strain or fibromyalgia). What is the position of maximal comfort, and does this reduce or eliminate pain or radicular symptoms? R-Radiation of pain: into leg (radicular), saddle area with bowel/bladder dysfunction (cauda equina syndrome), bilateral buttock or thigh (spinal stenosis, or referred from intra-abdominal pathology)? S-Severity of pain or systemic symptoms: pain scale 1 to 10, fever, weight loss, change in bowel habits, etc. There are sensory nerve fibers in the disks, vertebral end plates, facet joints, ligaments, fascia, blood vessels, spinal nerve roots, and muscles surrounding the lumbar spinal column. Therefore, nonspecific mechanical low back pain could originate from any one or a combination of these sites. Most low back pain is mechanical in nature and should slowly improve over 2 to 6 weeks. The following are symptoms or signs that suggest a more serious etiology of low back pain: · Unrelenting pain unaffected by change in position and not improved by supine position with hips flexed suggests infection, cancer, or infiltrative lesions. The simplest definition of sciatica is back pain that radiates down one leg below the knee. Occasionally, dermatome numbness and paresthesias of the lower limb are also reported. Valsalva maneuvers or flexion and extension of the lumbosacral spine may exacerbate these symptoms. Sciatica pain is suggestive of nerve root irritation and usually occurs as a consequence of nerve root impingement by structures either within the central canal (disk protrusion, facet or ligament flavum hypertrophy, synovial cyst, etc. What physical findings enable you to identify the approximate level of common, lumbar nerve root lesions? With the patient prone, the examiner maximally flexes the knee (80 to 100 degrees). Anterior thigh (L2, L3) or medial leg (L4) pain is suggestive of a lumbar root lesion. Pain produced in the lumbar region, posterior thigh, or between the ranges of 80 and 100 degrees of knee flexion is a positive test. The examiner passively raises the extended leg, by the foot, to 70 degrees of elevation. Dermatome pain radiating below the knee upon raising the leg between 30 and 70 degrees of elevation is a positive test for nerve root irritation. A positive test is more convincing if passive ankle dorsiflexion reproduces the pain after the leg has been lowered to an angle that abolished the radicular pain. It is usually is seen in patients with a herniated disk and is more specific but less sensitive than the straightleg raise test. The examiner gently eases the patient forward to increase stretch on the sciatic nerve. Two midline marks are drawn originating from dimples of Venus (which are inferior to the posterior, superior iliac spines), and 10 cm superior to that location in an upright patient. A difference of less than 5 cm between neutral and flexion is suggestive of an inflammatory spondyloarthropathy. Bilateral compression of the anterior iliac crests toward the midline, on a supine patient, may produce pathologic sacroiliac joint pain. Downward gentle pressure is then increasingly applied on the ipsilateral knee while stabilizing the contralateral anterior iliac crest. The patient then moves one buttock off the examining table edge while extending the leg over the side. Sacroiliitis is suspected if the maneuver provokes sacroiliac discomfort on the side of the dropped leg (see figures in Chapter 34). Lumbar spinal stenosis is compression of nerve roots within the central lumbar canal that may clinically present as radiculopathy, pseudoclaudication, or cauda equina syndrome. Spinal stenosis results from narrowing of the normal oval spinal canal, which assumes a triangular appearance as a result of facet hyperostosis, ligamentum flavum hypertrophy, broad-based central disk protrusion, and spondylosis, or any combination of these. The typical patient has symptoms of lower limb claudication (neurogenic) in the absence of peripheral vascular disease.
60caps serpina free shipping
Chapter 20 · Birth Control and Medical Termination of Pregnancy Because of risk of osteopenia anxiety drugs order serpina discount, this contraceptive is contraindicated in adolescents, and should not be used for more than 2 years in others. Lately, subcutaneous injections are under development to enable self-administration by the woman. Once-a-month intramuscular deep injection of combined oestrogen and progestogen are available in some countries. It should be remembered that the first menstrual period comes 1015 days after the first injection but thereafter every 30 days and lasts for 5 days. There was a need to explore the other routes of progestogen delivery into general circulation with slow, sustained release, long-acting and with reduced side effects. To reduce the frequent visits to the clinics, ensure an even release of the hormone and reduce the side effects while maintaining the efficacy; implants containing various amounts of progestogen have been used subdermally. The implants suppress ovulation in 50% but the main action is suppressing endometrium. The implants are inserted on the first day of the menstrual cycle, within 5 days of abortion, and 3 weeks after the delivery. The woman needs to use barrier contraception or abstain in the first 7 days of insertion. Since the capsules are nonbiodegradable, they need removal at the end of its use or earlier, if side effects are intolerable. The insertion and removal is made easier by using a single rod, Implanon (40 3 2 mm), which contains 67 mg desogestrel and does not require an incision to insert. Requires insertion and removal with nonbiodegradable capsules, which are however minor surgical procedures. The menstrual irregularity in the first 3 months settles down to normal cycles and dysmenorrhoea is also cured. The patch should be applied within 5 days of menses over the buttocks, abdomen but not over the breasts. The breakthrough bleeding (18%) and skin reaction (20%) breast discomfort are the side effects. Combined long-acting norgestrel 12 mg with 3 mg quinestrol, two tablets in the first month followed by one tablet each month is under trial. Three grams daily of percutaneous gel of oestradiol with cyclical progestogen is easy to apply. One should wait for 1 h for the gel to dry up and not to be in contact with other members. In an attempt to reduce the side effects of systemic hormonal contraception and the surgical method of insertion of implants, silastic vaginal rings carrying different progestogens in different doses have been tried. The hormone is safe as it gets absorbed through the vaginal mucosa and bypasses the liver. It is kept in situ for 3 weeks and removed for a week, thus bringing about regular menstrual cycles; failure rate is 1. Recently, some progestin-containing rings (3-keto desogestrel 10 mg) have been left in for 3 months at a time. Nestorone ring releases 150 mcg progestogen plus 15 mcg oestradiol daily-one ring remains effective for 1 year. Centchroman is a synthetic nonsteroidal contraceptive taken as a 30 mg tablet, started on the first day of menses and taken twice weekly for 12 weeks and weekly thereafter (half-life is 170 h). It exhibits a strong antioestrogenic and a weak oestrogenic action peripherally at the receptor Chapter 20 · Birth Control and Medical Termination of Pregnancy level. Centchroman is not teratogenic or carcinogenic, exerts no pharmacological effect on other organs. The drug can also be used as a postcoital pill, given in 60 mg dose within 24 h of coitus (two tablets repeated 12 h later with failure rate of 1%). It has been developed by Central Drug Research Institute, Lucknow, and has been released in India under the name of Saheli. The drug is also contraindicated in a woman with history of thrombophlebitis and migraine. It does not prevent fertilization but by blocking the action of progesterone on the endometrium, it causes sloughing and shedding of decidua and prevents implantation. Ulipristal is a synthetic progesterone hormone receptor modular, attaches to progesterone receptor and prevents/delays ovulation and suppresses endometrium, prevents implantation. Two tablets (60 mg) taken twice in 24 h within 24 h of intercourse can prevent implantation in 99% women. Postcoital Contraception (Interceptives) Postcoital contraceptive agent interferes with postovulatory events leading to pregnancy and is therefore known as interceptive. Emergency contraception is used following rape, unprotected intercourse or accidental rupture of a condom during coitus taking place around ovulation. The hormones may delay ovulation if taken soon after intercourse, cause corpus luteolysis, and bring about cervical mucus changes and endometrial atrophy. One tablet should be taken within 72 h of unprotected intercourse and another 12 h later. The tablets can be offered up to 120 h but its efficacy decreases with the longer coital-drug interval. The hormone is not teratogenic in case pregnancy does occur but risk of ectopic pregnancy remains. Prostaglandin Self-administered vaginal suppository containing prostaglandin following an unprotected intercourse, by virtue of its luteolytic effect on the ovary and its increased motility effect on fallopian tubes and the uterus, prevents implantation and brings about menstruation. Inserted within 5 days of intercourse can prevent implantation of a fertilized ovum. Immunological Methods Immunological approach to family planning is still in a developmental stage. Should immunology prove successful, family planning efforts will be simplified and will be more acceptable to the couples. The antigens which are being experimented upon are: n n the surgical technique should be simple and quick. The technique should be surgically reversible in case of unexpected disaster like death of children. The zona pellucida antibodies can either prevent penetration of ovum by the sperm or prevent shedding of zona after fertilization so that implantation is impossible. Male Sterilization Vasectomy Vasectomy consists of dividing the vas deferens and disrupting the passage of sperms. The couple must therefore abstain from intercourse during this period or use other methods of contraception. Two semen analysis reports must confirm the absence of sperms before the man can be declared sterile. One single incision is made with a special forceps and skin stitch is not required. Surgical Sterilization the sterilization operation is undertaken with the primary objective of preventing further pregnancy permanently. Sterilization is suited to those couples who have completed their families and do not want to bear the inconvenience or cost of the other methods of contraception, and when the other methods are contraindicated. An ideal method of sterilization should have the following criteria: n n It should be an outpatient procedure. The anaesthesia should be local or short general anaesthesia, so that the woman or man can return home in a few hours. This thread prevents migration of plugs and allows easy removal through a small incision. Complications of Vasectomy: n Local pain, skin discolouration, bleeding, haematoma formation (12%). However, the consequence of intravascular injection and excessive destruction of the vas by even a slight increase of instillation can be disastrous and the procedure irreversible. The fallopian tube is drawn up with dissecting forceps in a position where the broad ligament is relatively bloodless and curved clamps are placed in position on each side. Although the operation is simple, it gives excellent results and subsequent adhesions have been shown to cause no trouble. Interval sterilization is done when the woman is not pregnant or any time after 6 weeks of delivery. Indications Apart from multiparity and the need of permanent method of family planning, sterilization may be advisable in women with medical diseases. Laparotomy sterilization is performed when the abdominal incision extends well over 5 cm and is done during caesarean section and during gynaecological surgery. The fallopian tube is identified on each side, brought out through the incision, and the middle portion is formed into a loop which is tied at the base with catgut and excised.
Quality serpina 60caps
Each of these drugs are given in association with a dose of prednisone required to control extrarenal manifestations anxiety symptoms postpartum discount serpina 60 caps mastercard, and prednisone is tapered over time. Calcineurin inhibitors (cyclosporin, tacrolimus) have also been used for maintenance therapy and in patients with refractory disease. A 30-year-old woman with severe nephritis and end-stage renal failure is referred for further evaluation and treatment. The patient, who has been on dialysis for nearly 5 years, is being considered for transplantation but is afraid that her lupus will destroy the donor kidney. Lupus nephritis accounts for up to 1% to 2% of cases of end-stage renal failure requiring dialysis or transplantation. There is some evidence that transplantation before initiation of dialysis may result in improved allograft and patient survival. Furthermore, even in patients with recurrent nephritis, it is unlikely to lead to allograft loss. Retrospective analysis has reported that lupus patients have a similar incidence of graft survival rates as compared with nonlupus patients; however, the presence of antiphospholipid antibodies may decrease the rate of allograft survival. Manifestations of diffuse disease include intractable headaches, generalized seizures, aseptic meningitis, acute confusional state, cognitive dysfunction, psychiatric disease (especially psychosis and severe depression), and coma. Manifestations of focal disease include stroke syndromes such as hemiparesis, focal seizures, movement disorders such as chorea, and transverse myelitis. These autoantibodies are hypothesized to affect neuronal function in a generalized manner. Patients with acute encephalopathy frequently demonstrate elevated levels of antineuronal antibodies or other evidence of autoantibody production in the cerebrospinal fluid. Furthermore, these patients frequently demonstrate significantly elevated serum levels of antiphospholipid antibodies, which are associated with intravascular occlusion. Cardiac emboli should always be ruled out with an echocardiogram (transesophageal more sensitive than transthoracic). A 40-year-old woman with severe lupus nephritis has been treated with 60 mg of prednisone for the past 2 weeks but now seems disoriented and demonstrates bizarre behavior with delusional thinking. Any focal neurological findings would strongly suggest that the change in behavior was not directly caused by the high doses of prednisone. Laboratory tests should exclude the possibility of a new metabolic problem and determine the activity of nephritis and/or other organ involvement. In a patient on high doses of steroids, the possibility of infection must be considered and excluded. If the evaluation is negative, the most likely cause for the change in behavior is steroid-induced psychosis, and the appropriate treatment would be to decrease the dose. This might include increasing the dose of steroids and/or adding a cytotoxic drug. Valvular disease-possibly more frequent in patients with antiphospholipid antibodies. LibmanSacks verrucae occur most commonly on ventricular side of posterior leaflet of mitral valve. If due to lupus, patients do not have antismooth muscle or anti-liverkidney microsome antibodies. Red blood cell indices are otherwise normal, as is the rest of the complete blood count. There is an inability for iron to be handled normally by the reticuloendothelial system, and blood tests frequently disclose a low serum iron concentration as well as a low total iron-binding capacity. Note that a ferritin level >100 ng/mL rules out iron deficiency in a patient with an active inflammatory disease. The evaluation in this patient should rule out the possibility of an autoimmune hemolytic anemia. It is important to determine that the patient has the anemia of a chronic disease because it implies ongoing inflammation, prompting careful follow-up of the patient. Patients demonstrating this form of anemia are more likely to demonstrate flares of lupus activity in the near future. Her prednisone has been tapered to 5 mg/day, and there are no clinical manifestations of active disease. A review of systems and physical examination are negative, except for a mild malar rash. Laboratory tests show no evidence for lupus nephritis or other internal organ involvement. It does imply continued disease activity, so the patient needs to be followed carefully. Some physicians would start hydroxychloroquine in an attempt to lessen the chance for a future lupus flare. Previous bone marrow biopsies showed increased numbers of megakaryocytes and no other abnormalities. Past therapy with high doses of corticosteroids has been successful in raising the platelet count to normal levels, but tapering to 20 mg/day has resulted in a progressive decline in platelet counts to <20,000/mm3. The patient is taking no other medications, and her physical examination and other laboratory evaluation are normal. There are several therapeutic options to consider in this patient with autoimmune thrombocytopenia. However, the value of splenectomy in lupus-related thrombocytopenia has been debated, and its use is controversial. Some studies (retrospective and anecdotal) have suggested a high rate of failure in maintaining adequate platelet counts long term. Rituximab may be considered in patients who have failed steroids, and possible use as a first-line agent is currently under investigation. Rituximab can induce a durable response, but the rate of response at >1 year is only 18% to 35%. Thrombopoietin receptor agonists (romiplostim) are also considered in patients who have failed steroids; however, they are expensive ($55,000/year) and thrombocytopenia usually recurs when they are stopped. One option is the addition of an immunosuppressive or cytotoxic drug such as azathioprine (up to 2. This addition may decrease platelet destruction and allow the prednisone dose to be tapered. Azathioprine and mycophenolate are less toxic than cyclophosphamide and would be preferred in this setting. Cyclosporine A, vincristine, and dapsone have also been used as second-line agents. Another option is danazol, an androgen that increases platelet counts and allows the steroid dose to be decreased. Doses of 800 mg/day may be necessary, and the androgenic side effects in a young female may be troubling. This treatment can be used in preparation for splenectomy or if the patient showed signs of bleeding. For Rh-positive nonsplenectomized patients anti-D is another possible first-line agent. Making the correct diagnosis is essential so appropriate therapy can be instituted. This allows for the accumulation of unusually large multimers of von Willebrand factors secreted by endothelial cells into the plasma. These multimers bind to platelet glycoprotein receptors, causing platelet adhesion and microthrombi. Antiplatelet agents, corticosteroids, and/or immunosuppressive drugs have been used but are not as effective as plasmapheresis and plasma replacement. Lupus anticoagulant refers to a subset of autoantibodies to phospholipids that interfere with certain clotting tests. Patients who develop disease manifestations but do not have another autoimmune disease have the primary antiphospholipid antibody syndrome (see Chapter 23). Complications associated with antiphospholipid antibodies include arterial and venous thrombosis, miscarriage and fetal wastage, thrombocytopenia, livedo reticularis, and autoimmune hemolytic anemia. Although septic arthritis is always a concern, this presentation is worrisome for osteonecrosis of the hip (see Chapter 54). Patients who become cushingoid on steroids, who have antiphospholipid antibodies, and those treated with >20 mg/day of prednisone are at increased risk.
Syndromes
- Endoscopy -- camera down the throat to look at and possibly remove caulk from the esophagus and the stomach
- CO2
- This result usually means the abnormal changes are likely to lead to cervical cancer
- Examination of cerebrospinal fluid
- Control-L (also contains petroleum distillates)
- Muscle spasms
- Bruising (rare)
- Able to hold almost all weight when supported in a standing position
Buy generic serpina 60caps on-line
Other infections observed at higher incidence in patients with iron overload include Yersinia enterocolitica anxiety x blood and bone purchase 60 caps serpina fast delivery, which causes a septic arthritis, Listeria monocytogenes, Salmonella typhimurium, and Mucor, among others. Other joints affected are the proximal interphalangeal joints, radiocarpal joints, knees, hips, ankles, shoulders, and occasionally metatarsophalangeal joints. Treatment is for symptom alleviation using analgesics and nonsteroidal antiinflammatory drugs. Chondrocalcinosis is present in 30% to 60% of patients and can occur without the degenerative arthropathy. Note the degenerative arthritis of the metacarpophalangeal joints with hook-like osteophytes. In the fasting state, transferrin saturation (iron/total iron-binding capacity Ч 100) greater than 60% in men or 50% in women along with elevated ferritin greater than twice the normal level is 95% sensitive and 85% specific for diagnosis of hemachromatosis. Genetic screening is recommended for all patients with transferrin saturation >45% and ferritin >200 g/L. Serum ferritin levels are an accurate measure of peripheral iron stores but may also be increased in the settings of acute liver injury, systemic inflammation, and neoplasia. In addition, synovial biopsies will reveal iron deposition in type B synovial lining cells in patients with arthritis. This pattern of iron deposition is different to that seen in other diseases causing iron deposition in synovial tissue (rheumatoid arthritis, osteoarthritis, pigmented villonodular synovitis, hemophilia, and hemarthrosis). Liver biopsy is not necessary for diagnosis unless severe fibrosis is suspected (serum ferritin >1000 g/L) or the diagnosis is in doubt, as in the case of individuals heterozygous for the C282Y mutation with abnormal iron indices or liver function tests. New hepatic magnetic resonance imaging techniques to quantitate hepatic iron content may replace the need for liver biopsy. Phlebotomy is performed twice weekly until transferrin saturation is <50% and ferritin is <50 g/L (up to 2 to 3 years) and then as required (usually every 3 to 4 months) to maintain low normal serum levels (ferritin <300 g/L in men, < 200 g/L in women). Life expectancy of symptomatic patients is extended considerably by removal of excess iron stores (90% 5-year survival vs 33% survival without therapy). With therapy, hepatomegaly, liver function studies, and pigmentation all improve and cardiac function stabilizes or improves. Hepatocellular carcinoma, a late sequela in one third of those who develop hepatic cirrhosis (risk increased by a factor of 20 to 200), is not diminished by phlebotomy and is the major cause (30% to 45%) of death in treated individuals. Therefore a biannual abdominal scan (ultrasound or computed tomography) and measurement of serum -fetoprotein levels are recommended for hepatocellular cancer screening. Because the life expectancy of homozygotes diagnosed and treated before the development of cirrhosis is the same as that of the general population, the importance of family screening and early therapy cannot be overemphasized. What are the common clinical presentations of Wilson disease (hepatolenticular degeneration)? The hepatic form presents before age 18 years and the neuropsychiatric form in early adulthood (age 20 to 30 years); a late-onset form also exists. Manifestations include the following: · Liver disease: abnormal liver-associated enzymes are seen in over 95% of cases. Liver disease is the initial presentation in 50% of cases and can manifest as asymptomatic transient hepatitis to fulminant hepatitis, chronic active hepatitis, and cirrhosis. A clue to Wilson disease as the etiology for fulminant hepatic failure is the disproportionately low level of aminotransferases (usually <1500 /L) and the marked increase in bilirubin due to associated hemolytic anemia (Coombs-negative). Psychiatric disorders such as mood disturbances, neurosis, hypophonia, and personality changes occur in up to 33% of cases. These manifestations tend to occur later than the hepatic presentation, but abnormal liver transaminases and KayserFleischer rings are invariably seen in these patients. Musculoskeletal manifestations occur in 50% of patients but are rarely the presenting symptom because all patients have other manifestations of Wilson disease. Radiographically, subchondral and cortical fragmentation, as well as marginal, subchondral, and central bony sclerosis of the wrist, hand, elbow, shoulder, and knee, help to distinguish this arthropathy from primary osteoarthritis. Less common radiographic findings include osteochondritis dissecans, chondrocalcinosis, chondramalacia patellae, and vertebral wedging. Generalized osteoporosis or osteomalacia may be present as a result of Fanconi syndrome or renal tubular acidosis, both of which are common in Wilson disease. This is a membrane copper transport protein localized in the trans-Golgi network in hepatocytes that normally facilitates binding of copper to ceruloplasmin and transport of hepatocellular copper into bile. More than 300 mutations have been identified, although one mutation accounts for 30% to 60% of cases. Wilson disease results from excessive copper accumulation in association with ceruloplasmin deficiency. Decreased serum ceruloplasmin (<200 mg/L) and elevated urinary copper excretion (>65 to 100 g/day) are suggestive of Wilson disease. An elevated hepatic copper concentration (>250 g Cu/g dry weight) is the most reliable test early in the course of the illness. Screening of first-degree relatives older than 6 years should include a physical examination, liver function tests, measurement of serum copper, ceruloplasmin, and 24-hour urine copper, and slit lamp examination. Siblings of Wilson disease patients have a 25% risk of having the disease and children of patients have a 1 in 200 risk. Lifelong penicillamine chelation therapy is the preferred choice because it can prevent or improve virtually every manifestation of Wilson disease. Other treatment options include trientine (chelator) and zinc salts (bind copper in the gut). Foods rich in copper such as organ meats, nuts, chocolate, and mushrooms need to be avoided. Patients presenting with fulminant hepatic failure do not respond well to chelation and require urgent liver transplantation. Notably, heterozygotes are unaffected even when challenged with high doses of the precursor amino acids. Microscopic visualization by Virchow demonstrated a yellowish or "ochre" tint to tissues; hence the name ochronosis. The original term for homogentisic acid was alkapton, which referred to its avidity for alkali; hence the name alkaptonuria. In rare cases, exogenous ochronosis causes bluish black cartilage pigmentation in individuals exposed to phenol, benzene, hydroquinone or other noxious substances. The clinical diagnosis is suggested by the following typical triad of findings: · Degenerative arthritis (premature), especially in the spine with disc calcification; the earliest involvement is observed for the lumbar spine · Abnormal pigmentation, usually occurring first in the ear cartilage and sclerae · Urine that turns blue-black on standing (occurs in 75% of patients) Homogentisic acid binds collagen and is therefore deposited in connective tissues throughout the body. Observation of blue-black or gray-brown pigment in tissues (skin, ears, cerumen, sclerae, cartilage) suggests ochronosis. However, confirmation of the diagnosis requires measurement of 24-hour urinary excretion of homogentisic acid. Degenerative joint disease occurs in the third decade of life, with typical symptoms of pain, stiffness, and a limited range of motion for the large joints and spine. The most common site involved is the spine, followed by the knees, hips, and shoulders. Synovial fluid may have a characteristic ground-pepper appearance caused by pigmented cartilage fragments. It has been noted that calcium pyrophosphate deposition disease can coexist with ochronotic arthritis. Patients with alkaptonuria have an increased prevalence of kidney stones (25% of patients) and also develop heart valve and coronary artery calcifications. Prominent intervertebral disc calcification can also be seen in hemochromatosis, hyperparathyroidism, calcium pyrophosphate deposition disease, paralytic poliomyelitis, and amyloidosis. The radiographic appearance of the large peripheral joints in ochronotic arthritis is virtually indistinguishable from that in primary osteoarthritis. Treatment for symptom alleviation of the arthritis as for osteoarthritis is the standard therapy and includes patient education, physical and/or local therapy, and analgesia. Large doses of vitamin C have been used, but there are no studies of its efficacy. Arthroscopy has been of benefit for removal of osteochondral loose bodies in the knee. Nitisinone (Orfadin) is currently under investigation for the prevention and treatment of ochronosis. This drug inhibits the enzyme 4-hydroxyphenylpyruvic acid dioxygenase, which produces homogentisic acid. Balaban B, Taskaynatan M, Yasar E, et al: Ochronotic spondyloarthropathy: spinal involvement resembling ankylosing spondylitis, Clin Rheumatol 25:598601, 2006.
Buy serpina pills in toronto
Progesterone initially from the corpus luteum and later from the placenta is essential for the continuation of pregnancy anxiety symptoms of order serpina now. Progestogens cause hyperplasia of the muscular lining of the fallopian tube and make peristaltic contractions more powerful as well as increase the secretion by the tubal mucous membrane. Progestogen causes hypertrophy of the cervix and makes the cervical mucus more tenacious. During early pregnancy the vagina becomes violet coloured due to venous congestion. A certain percentage of progestogens is metabolized to oestrogen, and it may well be that the oestrogen so produced is responsible for inhibiting pituitary activity. Progestogens cause water and sodium retention and is a contributory factor in premenstrual tension and weight gain. Progestogens exert anabolic effect and this partly accounts for some of the weight gain which may follow their administration. While part of the administered progestogen is metabolized to oestrogen, it is also partly metabolized to testosterone. If administered to a patient during pregnancy, some progestogens have virilizing effect upon a female fetus. Progesterone the corpus luteum is the main source of progesterone and a small amount is derived from adrenal gland (23 mg), seen in the proliferative phase. Although progesterone is an important intermediary product in the synthesis of adrenal corticosteroids, it has little, if any, biological action from this extra ovarian source. The plasma level of progesterone rises after ovulation and reaches a peak level of 15 ng/mL at mid-luteal phase. With the degeneration of the corpus luteum, its level falls and this brings about menstruation. In an anovulatory cycle, progesterone is absent or is in negligible amount (from extra ovarian sources). If pregnancy occurs, the corpus luteum persists, even enlarges and continues to secrete progesterone. This high level of hormone prevents menstruation and leads to amenorrhoea of pregnancy. It is excreted in the urine as sodium pregnanediol 3-glucuronide and recovered as such for assay in the secretory phase of the menstrual cycle. Daily production in the luteal phase is 2040 mg and daily urine excretion is 36 mg. Radioimmunoassay is currently used to estimate the plasma progesterone levels in mid-luteal phase in cases of infertility. Chapter 3 · Physiology 43 Side Effects If given in large doses, progestogen can cause gastrointestinal symptoms, nausea and vomiting. In fact, all symptoms of pseudopregnancy state may be observed-water retention, breast enlargement and tenderness, and moderate uterine enlargement. Virilism has been reported with some synthetic progestogens, especially 19-nortestosterones. Some exhibit adverse effects on lipid metabolism and increases the risk of breast cancer. Thrombosis of deep veins, pulmonary embolism and arterial thrombosis are rare but are reported with third generation of synthetic progestogens (gestodene, desogestrel) Table 3. Although the extraction of purified inhibin is not yet successful, there is a possible hope of its availability in the near future. Relaxin this hormone relaxes the connective tissue and is probably secreted by the ovary. It may have a role in pregnancy and may be responsible for relaxation of pelvic joints and pelvic floor muscles. Its level is related to precocious and delayed puberty, infertility and premature menopause. In in vitro fertilization programme, it carries a prognostic value and helps to decide on donor egg. Inhibin Inhibin is a nonsteroidal water-soluble protein (peptide) secreted by the Graafian follicle. Inhibin consists of two peptides, namely inhibin A (a-fraction) and inhibin B (b-fraction). Administration of inhibin in the early follicular phase can delay folliculogenesis and inhibit ovulation and luteinization. Inhibin may have an important role in the control of fertility both in the males and the females. It causes agglutination of sperms, prevents cervical mucus penetration and interferes with egg interaction. Only free hormones are biologically active and influence their target organs (12%). Oestrogen and thyroid hormones increase the secretion of these proteins, but androgens lower their levels. The normal increase in stromal tissue at ovulation causes a slight increase in the secretion of these hormones. After the menopause, the increased ovarian stroma is responsible for the rise in these hormones and development of hirsutism in some postmenopausal women. At birth, the ovaries are populated with lifetime complement of eggs located in the primordial follicles, but most of these follicles undergo atresia throughout childhood and only about 400 of these primordial follicles are present during reproductive age. Multiple follicles start growing in both the ovaries, but only one dominant Graafian follicle is selected which ripens to full maturity and ovulates, whereas other follicles become atretic. One to two per cent free testosterone remains biologically active and acts at the peripheral targets, i. Physiology of Menstruation the proliferative phase of the endometrium represents the oestrogenic part of the menstrual cycle. The secretory phase of the endometrium is controlled by progesterone, although the effect of progesterone is obtained only after the endometrium has been sensitized with oestrogen. This is because oestrogen produces progesterone receptors to which progesterone acts. It also stimulates the secretion of testosterone and androstenedione by theca cells. The growth of the ovarian follicles and endometrial thickness can be studied by serial ultrasound. In the absence of pregnancy, both oestrogen and progesterone levels decline gradually and the fall in the level of these hormones brings about menstruation. Feedback Mechanism in the HPO axis As mentioned in the beginning, the various hormones liberated by the hypothalamus, anterior pituitary gland and the ovaries are dependent upon each other, each reaching in positive as well as negative feedback at different levels. Leptin Since its discovery in 1994, leptin (adipocyte protein hormone) is linked to nutrition and may bear an important role in the control of hypothalamicpituitaryovarian axis. Menstruation Menstruation is the end point in the cascade of events starting at hypothalamus and ending in the uterus. The menstrual cycle is usually of 28 days, measured by the time between the first day of one period and the first day of the next. The duration of bleeding is about 35 days and estimated blood loss is between 50 and 200 mL. The menstrual rhythm depends on the HPO function, whereas the amount of blood loss depends upon the uterine condition. A study of the coiled arteries of the endometrium shows that there is a slight regression of endometrium shortly after ovulation and that a rapid decrease in thickness can be demonstrated even before menstruation starts. In the regression that starts a few days prior to the onset of menstruation, there is a decreased blood flow which may cause shrinkage of the endometrium from dehydration. During menstruation itself, the reduction in the thickness of the endometrium is determined by both desquamation and resorption. The necrosis of the superficial layers of the endometrium is produced either by local stasis or by the clearly demonstrated vasoconstriction of the coiled arteries. Menstrual bleeding occurs when the open arteries damaged by necrosis relax and discharge blood in the uterine cavity. The important feature of the menstrual changes is the contraction and constriction of the coiled arteries. The regeneration of the vascular system is probably brought about by the development of anastomosing arteries.
Buy 60caps serpina with amex
The vasomotor instability is manifested by a blue and cool area (but occasionally can be warm and erythematous) along with unusual sweating in the area (but occasionally can be dry and scaly) anxiety symptoms during exercise buy cheap serpina 60 caps on line. Contractures of the flexor surface of the hand may occur in the late stage of this disease, leaving a claw-like, nonfunctional hand. He emphasized the association with trauma, the lack of direct injury to the nerve, and the articular nature of this syndrome. Mitchell coined the word causalgia (from the Greek words for heat and pain) for this illness in an article in the United States Sanitary Commission Memoirs. The highest incidence is in the 40- to 60-year age group with a mean age of 50 years. The incidence in children is thought to be underreported because it often goes unrecognized, usually affects the lower extremity, and oftentimes is diagnosed as a psychiatric condition. It occurs most commonly after fractures (1% to 2%), peripheral nerve injury (1% to 5%), and strokes/ myocardial infarctions (5%). The ipsilateral shoulder may become diffusely painful, develop limited range of motion in all directions, and may progress to adhesive capsulitis. Stage 1 (acute stage): typically lasts 612 months, characterized by: Pain in the extremity or shoulder. Stage 2 (dystrophic phase): persists an additional 12 years, characterized by: Pain usually continues. Stage 3 (atrophic stage): persists up to several years, characterized by: Pain remains constant or diminishes. Some have additionally postulated a fourth stage (psychological stage), characterized by loss of job, unnecessary surgery, orthostatic hypotension or hypertension, neurodermatitis, depression. Although these stages can be useful, it is often difficult to place an individual patient into one of them. A patient may stay in one stage for months or years, and another patient may progress rapidly through the stages. Incoordination, tremor (25% to 60%), involuntary movement (myoclonus), dystonia, muscle spasms, paresis, pseudoparalysis. This appearance is especially evident when comparing the involved side with the contralateral side. This patchy osteopenia is helpful in making the diagnosis but is actually seen in less than half the patients in most series. In stage 1, there is an increase in blood velocity and blood pooling with early and delayed hyperfixation. In stage 2, there is normalization of blood velocity and blood pooling but a persistence of early and delayed hyperfixation. In stage 3, there is reduced blood velocity and blood pooling, and a minority of patients have early and delayed hyperfixation. Thus, a bone scan performed early in the disease is usually abnormal, but as the disease progresses, scans can be normal. Findings include synovial edema, proliferation and disarray of synovial lining cells, proliferation of capillaries, fibrosis in the deep synovial layers, and occasional infiltration with chronic inflammatory cells (primarily lymphocytes). These neuropeptides lower the synaptic excitability of the normally silent second-order interspinal synapses making them hyperexcitable. The persistently noxious stimuli leads to peripheral sensitization and further release of inflammatory neuropeptides at the dorsal root ganglion, causing abnormal connections with the sympathetic nervous system, which may potentiate sympathetic mediation of pain. These autoantibodies and the inflammatory neuropeptides may contribute to neurogenically induced inflammation. Many patients develop a small fiber neuropathy with a decrease in epidermal nerve fiber density in the affected limb. Up to 50% of patients with symptoms less than 1 year can improve with these blocks. Baron R, Schattschneider J, Binder A, et al: Relation between sympathetic vasoconstrictor activity and pain and hyperalgesia in complex regional pain syndromes: a case-control study, Lancet 359:1655, 2002. Blaes F, Schmitz K, Tschernatsch M, et al: Autoimmune etiology of complex regional pain syndrome (M. Bruehl S: An update on the pathophysiology of complex regional pain syndrome, Anesthesiology 113:713725, 2010. Brunner F, Schmid A, Kissling R, et al: Bisphosphonates for the therapy of complex regional pain syndrome I systemic review, Eur J Pain 13:1721, 2009. Goebel A, Baranowski A, Maurer K, et al: Intravenous immunoglobulin treatment of the complex regional pain syndrome: a randomized trial, Ann Intern Med 152:152158, 2010. Gorodkin R, Herrick A: Complex regional pain syndrome (reflex sympathetic dystrophy). Kachko L, Efrat R, Ben Ami S, et al: Complex regional pain syndromes in children and adolescents, Pediatr Int 50:523527, 2008. Clinical and histologic studies: evidence for bilaterality, response to corticosteroids and articular involvement, Am J Med 60:321331, 1976a. Roentgenographic and scintigraphic evidence of bilaterality and of periarticular accentuation, Am J Med 60:332338, 1976b. Scintigraphic studies, further evidence for the therapeutic efficacy of systemic corticosteroids, and proposed diagnostic criteria, Am J Med 70:2330, 1981. Schьrmann M, Zaspel J, Lцhr P, et al: Imaging in early posttraumatic complex regional pain syndrome: a comparison of diagnostic methods, Clin J Pain 23:449, 2007. A randomized, controlled, multicenter dose-response study, J Bone Joint Surg Am 89:1424, 2007. The most common benign joint neoplasms are tenosynovial giant cell tumors and synovial chondromatosis. A benign or malignant neoplasm of the joint should be considered in any patient with a nontraumatic hemarthrosis. Why should practicing physicians be concerned with tumors that affect the joints and synovium? Benign and malignant neoplasms affecting articular and periarticular structures may mimic inflammatory arthritis. Awareness of these conditions is crucial to prevent diagnostic delay and to avoid the initiation of ineffective and/or inappropriate therapy. A young adult presents with a solitary, painless mass adjacent to a finger joint that has been slowly enlarging. This benign condition, which occurs with a slightly increased predilection for females, is second only to the ganglion as a source of localized swelling in the hand and wrist. These nodular lesions usually occur in association with a tendon sheath (formerly called giant cell tumor of tendon sheath). Grossly, the synovium is red-brown to mottled orange-yellow and prolific with coarse villi, finer fronds, and diffuse nodularity resembling an Angora rug. Swelling and effusion accompanied by moderate discomfort, decreased range of motion, and increased warmth to palpation are typical. It tends not to be as darkly pigmented and has less villous proliferation than is seen in the diffuse form. Plain radiographs are usually nonspecific except for mild increased density of the soft tissue of the joint resulting from blood and hemosiderin deposits. The tumor may invade into bone causing cysts or scalloped erosive changes with sclerotic borders mimicking gout or tuberculosis. Nodules with sufficient hemosiderin appear dark on both T1-weighted and T2-weighted images. It is characterized by a dense cellular infiltrate composed of synovial cell hyperplasia with surface and subsynovial invasion of mitotically active cells with eosinophilic cytoplasm. Other invading cells are fibroblasts, lipidladen macrophages (xanthoma cells), hemosiderin-containing macrophages, and scattered, frequent, multinucleated giant cells. Surgical treatment with complete synovectomy is standard, either via open or arthroscopic approaches. Intraarticular installation of radioisotopes or low-dose external beam radiation are used in refractory cases. Synovial chondromatosis is characterized by the development of multiple foci of cartilaginous metaplasia (? These foci form nodules that may be invaded by blood vessels leading to endochondral ossification (termed osteochondromatosis).
60 caps serpina free shipping
The leukocyte count is often elevated to extraordinary anxiety related to purchase 60 caps serpina with amex, even leukemoid levels, with a significant left shift (bandemia). Platelet counts are often equally elevated, and thrombocytopenia is inconsistent with the diagnosis. Ferritin level is usually greater than 3000-10,000 ng/mL and fibrin degradation products are increased. Growth retardation and steroid side effects such as osteoporosis and cataracts are frequent (less likely to occur if prednisone doses can be tapered to 5 mg/day). It usually presents as an asymmetric large joint arthritis with the knee most commonly involved. Notably, this disease is unique to pediatric patients because there is no adult equivalent. If the hand is involved, the patient is more likely to develop psoriatic arthritis. The hip and back are not involved; any child complaining of pain in these areas needs an extensive workup to rule out other causes. Half of the children who will develop chronic uveitis will have it present at the first eye appointment. Uveitis incidence diminishes with each subsequent year after joint swelling develops. By 5 to 7 years after joint swelling develops, the risk of new-onset uveitis is quite low. However, slit-lamp screening is necessary within the first 5 to 7 years, even when the joint disease is in remission. A patient presents with poorly localized leg pain sufficient to interrupt sleep and cause a limp. Triamcinolone hexacetonide (Aristospan) is most efficacious at a dose of 1 mg/kg up to 40 mg. However, up to 50% to 67% of patients will have a relapse within 2 years of stopping therapy. Chronic sequellae include leg length discrepancy, joint contractures, and blindness. These patients have an asymmetric onset of arthritis and a higher risk of developing chronic uveitis, similar to that seen in extended oligoarthritis patients. The classic radiographic changes are fusion of the carpal bones, micrognathia, and fusion of the C-spine apophyseal joints. The following are typical doses for patients over 2 years of age: · Methotrexate: start at 5 to 7. Children require and tolerate higher doses than adults owing to differences in metabolism. What are the demographic and clinical characteristics of juvenile psoriatic arthritis? The presence of dactylitis (15% to 37%) and a family history of psoriasis are important clues that the child has psoriatic arthritis. Classic arthritis is subtalar synovitis with inflammation of surrounding tendon sheaths. Spinal symptoms are rare at onset but a subset (about 30%) will develop sacroiliitis and spondylitis during adolescence. Extraarticular manifestations: Uveitis: acute anterior uveitis in 6% to 27% of patients (see Question 11). Most patients require therapy because spontaneous remission rates are less than 50%. Reactive arthritis and inflammatory bowel disease-associated arthritis can occur and resembles their adult counterparts. Because children may have few abdominal symptoms, any child with iron-deficiency anemia and arthritis should have inflammatory bowel disease ruled out. In several published series, there is a remarkable agreement that the risk is 1 in 100. Therefore, there may be a genetic predisposition, although it clearly is not as strong as that for diseases such as hemophilia, cystic fibrosis, or diabetes. These facts suggest that an unidentified environmental agent may also be necessary for disease expression. This requirement depends on the financial status of the individual school district. However, if the school system provides such services for developmentally disabled children or those with cerebral palsy, they must provide them to children with arthritis. Beukelman T, Patkar N, Saag K, et al: 2010 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis: initiation and safety monitoring of therapeutic agents for the treatment of arthritis and systemic features, Arthritis Care Res 62:15151526, 2010. Flato B, Lien G, Smerdel-Ramoya A, et al: Juvenile psoriatic arthritis longterm outcome and differentiation from other subtypes of juvenile idiopathic arthritis, J Rheumatol 36:642650, 2009. Inflammatory myositis in childhood is almost always dermatomyositis and not polymyositis. HenochSchцnlein purpura is an immunoglobulin A (IgA)-mediated process and the most common small-vessel vasculitis in childhood. Localized scleroderma is the predominant childhood form of scleroderma and may respond to early aggressive immunosuppressive therapy. In childhood, the disease generally occurs after age 10 years (60%) and rarely before the age of 5 years (5%). The ratio of girls to boys is about 2:1 before age 10 years and then, in adolescents, is similar to the ratio of adult women to men (5:1 to 10:1). Avascular necrosis as a result of steroid usage rarely occurs in children less than age 14 years. Systemic Manifestations of Systemic Lupus Erythematosus General (90%) Malaise, weight loss, fever Skin (55-70%) Brain (25%) Eye Mouth (20-50%) Chest (15-20%) Heart (15-20%) Digestive system Kidneys (>50%) Extremities (60-80%) Butterfly rash, discoid lupus, vasculitic skin lesions, alopecia, photosensitivity Headache, blurred vision, psychosis, chorea, seizures, neuropathies, cerebrovascular accident, transverse myelitis Cotton-wool spots, retinitis, episcleritis, iritis (rarely) Oral ulcers Pleuritis, basilar pneumonitis, pulmonary hemorrhage, shrinking lung syndrome Pericarditis, myocarditis, LibmanSacks endocarditis Hepatosplenomegaly, mesenteric arteritis, colitis, hepatitis Glomerulonephritis, nephrotic syndrome, hypertension Arthralgia or arthritis, myalgia or myositis, Raynaud phenomenon, thrombophlebitis, aseptic necrosis (6-10% of patients, often associated with corticosteroids) Table 70-2. These two diagnoses may be distinguished by the presence of antibodies to specific histones. If present, their clinical associations are the same as adults, such as anti-Jo-1 identifying those children at increased risk for developing interstitial lung disease. It occurs in 25% to 30% of infants whose mothers have one or both of these antibodies regardless of their underlying disease. The cutaneous and hematologic manifestations are transient, generally resolving within 2 to 6 months after delivery, whereas heart block is frequently permanent and may require a pacemaker. Development of first-degree heart block or a pericardial effusion in the fetus is treated with fluorinated steroids that cross the placenta (dexamethasone, betamethasone). Once third-degree heart block has developed, it cannot be reversed with medications and the infant will require a pacemaker. Kawasaki disease is a uniquely pediatric vasculitis and is discussed in Chapter 71. The median age at presentation is 4 to 6 years, and the male to female ratio is about 1. Approximately 50% of children have a history of preceding upper respiratory tract infection with a variety of organisms. Purpura is usually the initial manifestation but can be preceded by arthritis, edema, testicular swelling, and abdominal pain. Renal disease occurs in 40% to 50% usually within the first 2 months of vasculitis onset. Complement levels are normal but there is evidence of alternate complement pathway activation. Children with renal disease and those >8 years of age are more likely to have recurrences. Up to 5% of children will suffer persistent purpura with or without persistent renal disease. In patients who have renal involvement, 30% develop renal insufficiency and 5% progress to renal failure, especially those who are nephrotic. Each of these triggers involve inflammation at mucosal surfaces where IgA plays a role in mucosal immunity. The mean age of onset is 6 to 9 years old with 25% occurring in children less than the age of 4 years.
Generic 60caps serpina free shipping
Surgery may be needed in the following conditions: n n Syndromic management-laboratory tests take time and delay treatment anxiety scale 0-10 purchase serpina 60caps fast delivery. To avoid sequelae such as blocked tubes, chronic pelvic pain and infertility, ectopic pregnancy, the modern management is to initiate antibiotics while waiting for the final reports. This has a small risk of unnecessary treatment or overtreatment, but it is worth its while or overtreatment, but is worth it. Intravenous fluids in presence of dehydration or vomiting and correction of electrolyte imbalance. Because of the damaging effect of gonococci and chlamydia on the fallopian tubes and polymicrobial nature of the infection, it is mandatory to institute antibiotic therapy at the earliest and not wait for the culture results. Initially, intravenous route is resorted to , but as the infection settles down, oral therapy may be started. When the culture report is available or if the patient fails to respond to the antibiotics, appropriate change in the antibiotic therapy will be needed. Other antibiotics useful are cephalosporins, and penicillin with beta-lactamase inhibitors. After the discharge from the hospital, doxycycline is continued 100 mg for 1014 days. Dilatation and evacuation of septic products of conception or for haemorrhage in postabortal sepsis. Laparotomy, drainage of pus and insertion of corrugated drainage have saved many a life. Ultrasound-guided vaginal aspiration of pelvic abscess with or without drainage yields 70% success. Sequelae include rupture of abscess during aspiration, pelvic vein thrombosis and chronic infection. The minimal surgery has the advantage of minimal ovarian tissue damage in young women. Laparoscopic breaking of external adhesions either by laser or by electrocautery is indicated if the tubal blockage is due to external adhesions. Hysteroscopic balloon plasty or cannulation is successful if the block is due to luminal debris or mild stricture. It has been stated that despite adequate treatment, 15% of patients fail to respond to chemotherapy, 2025% have at least one recurrence and 20% develop chronic pelvic pain (The Linde). About 15% suffer from infertility and 8% of those who conceive will have an ectopic pregnancy. Surgery depends upon the age and parity of the patient, the symptoms and pelvic pathology. In a young woman, conservative surgery in the form of salpingectomy and salpingo-oophorectomy is performed. When extensive damage precludes conservative management or when the patient is multiparous and of an older age group, abdominal hysterectomy with bilateral salpingooophorectomy is needed. Such a patient will need some form of tuboplasty depending upon the site of tubal blockage, or in vitro fertilization. Realizing that the country cannot provide enough beds and that it is not easy for the rural women to come to the urban centres for delivery, the Government of India has started training programme for dais in aseptic techniques. Though one continues to see such postabortal septic cases admitted to the hospitals, the number has definitely come down during the last two decades or so. Thereafter, oral 100 mg/kg daily in divided doses is administered for 312 months. Other antibiotics are tetracycline, erythromycin, clindamycin and chloramphenicol. Septic abortions are often the result of pregnancy termination carried out under unhygienic conditions, often by quacks. Bleeding, anaemia, tissue damage and lack of proper asepsis predispose to this life-threatening eventuality. Clinically the patient suffers from manifestations such as abdominal pain, leucorrhoea, menorrhagia, congestive dysmenorrhoea, dyspareunia, backache and infertility. The uterus is often retroverted with restricted mobility and there may be thickening of the appendages which are painful on palpation. Use of barrier contraceptives, observance of proper asepsis during instrumental manipulations and prompt treatment of suspected infection are the best approaches to safeguard the patient from infections. Natural barriers exist to protect the ascent of organisms from the vagina to the upper genital tract; these include the ciliary movement of the endosalpinx Suggested Reading Arulkumaran S. But the credit for the first authentic description of genital tuberculosis is attributed to Morgagni (1744) who first described the autopsy findings of genital tuberculosis in a young woman aged 20 years who had died of tuberculosis. In his report, he clearly mentioned that the uterus and tubes were filled with caseous material. Since the early part of the twentieth century, the incidence of general tuberculosis and as its consequence, pelvic tuberculosis have progressively declined in the developed countries of the world, so that the disease has become rare in many industrialized countries of Europe and America. The disease continues to be rampant in developing countries of Latin America and Asia. The actual incidence of pelvic tuberculosis is difficult to assess as many patients are asymptomatic, therefore the disease often comes to light only incidentally during the course of investigation for a gynaecological complaint. Schaefer (1970) reported that 412% of women dying from pulmonary tuberculosis manifest evidence of genital involvement. Surveys from Mumbai about the prevalence of tuberculosis amongst infertile women reported by several authors have been mentioned here- Merchant (1989) reported an incidence of 14. Classically, female genital tuberculosis has been described as a disease of young women with 80% of these diagnosed between the ages of 2040 years, although the disease has also been reported in older women around menopause and occasionally even thereafter. Falks (1980) reported that 46% of his patients of genital tuberculosis from Sweden were aged over 50 years. Genital tuberculosis occurs almost always secondary to a primary focus elsewhere, the commonest site being the lungs (50%), but rarely from other sites such as lymph nodes (40%), the kidneys, joints, gastrointestinal tract or as part of a generalized miliary infection. The mode of spread is generally haematogenous or via lymphatics, and rarely from direct contiguity with an intra-abdominal organ or affected peritoneum (Schaefer, 1976; Siegler, 1979). Once the genital tract has been colonized, the granulomata containing viable tubercle bacilli form within the various pelvic organs. Following the development of tubercular hypersensitivity, these foci become generally silent and long intervals of many years, often extending sometimes to over a decade, may pass before reactivation of the focus takes place. The active growth and increase in blood supply to the genital organs around menarche constitutes the event leading to its reactivation and establishment of the disease process. The fallopian tubes may appear normal at first appearance, but in minimal disease, they may appear thickened with the feel of a whip-like consistency. At times, following direct extension of tuberculosis from adjacent organs, the exosalpingitis manifests in the form of diffusely spread miliary tubercles on the serosal surface of the fallopian tube, the ampullary part of the tube appears dilated with the fimbriae end open and pouting. In over 50% cases, the tubes are enlarged in diameter, with their external surfaces appearing roughened due to adhesions or may show presence of greyish tubercles, these may be discrete or confluent. On cut section, the lumen reveals presence of yellowish grey caseous matter or serosanguinous fluid (tuberculous haematosalpinx) and pyosalphinx. At times, violin string adhesions are noted between the right fallopian tube and the undersurface of the liver, known as Fitz-Hugh-Curtis syndrome. Leakage of infected material into the peritoneal cavity causes peritubal abscess, tuberculosis peritonitis and ascites. The tubes remain patent in almost 2550% cases of genital tuberculosis with minimal disease, but as the disease advances, reactive fibrosis sets in and the tubes get occluded. Microscopically, granulomas and chronic inflammatory infiltrate may involve the full thickness of the tubal wall; on occasions these tell-tale granulomas are difficult to find. The ampullary part is the most common to be affected, the fimbriae and interstitial parts of the tubes are often spared. The brunt of the attack is borne by the endosalpinx, it often exhibits focal or widespread reactive adenomatous hyperplasia which may be severe enough to be mistaken for carcinoma. The diagnosis of tubal tuberculosis is based on the demonstration of acid-fast bacilli in the tissues, or by positive cultures or guinea pig inoculation. It is a well-known fact that the tubercle bacilli are difficult to thus acquired in childhood may remain dormant until puberty. As a rule, the fallopian tubes are the first to be involved; hence the disease is commonly bilateral in distribution, with subsequent dissemination to other genital organs and the peritoneum. Primary genital tuberculosis is rare; there are reports in literature of cases of primary genital tuberculosis affecting the vulva and cervix, in which the sexual partner has been suspected to be the source of the disease (1%). Apart from semen being a source of infection, the practice of using saliva for lubrication prior to intercourse by some men may also be a source of infection in cases of open pulmonary tuberculosis.
