
Cheap norfloxacin 400 mg
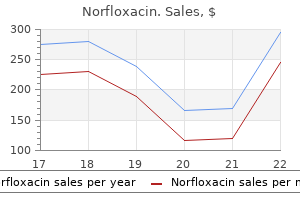
The function of these cells 606 antibiotic purchase cheap norfloxacin on-line, and of the nitrergic nerves in the detrusor is unknown. Calcium may either enter down its electrochemical gradient from the extracellular medium, or be released from intracellular calcium stores. Excitation-contraction coupling describes the link between changes in the membrane potential and tension development, and receptoreffector coupling the pathways between receptor activation and alterations in contractile activity. The involvement of calcium entry through the membrane and store release vary markedly in different smooth muscles. The patterns in bladder and urethra are clearly different, although currently the details in both tissues are poorly understood. The detrusor produces calcium-based action potentials, and it seems likely that the spontaneous contractile activity of strips is triggered by these. The figure shows the results of agarose gel electrophoresis and size fractionation of the products. The spontaneous phasic contractions are usually much smaller than the maximal contraction that can be evoked by nerve stimulation, and thus it appears that Ca2+ entering in the spikes does not elevate the free calcium levels sufficiently to cause much activation of the contractile machinery. In other smooth muscles, calcium entering in the spikes has been shown to activate release of calcium from internal stores by a calcium-activated calcium release channel. Evidence that such channels exist in the detrusor has been provided from studies on the effects of caffeine, a drug known to sensitise these channels and cause Ca2+ release from stores (fig. However the res86 87 ponse to caffeine is transient and much smaller than seen in other smooth muscles. In detrusor muscle from non-human mammals, intrinsic nerve stimulation generates excitatory junction potentials and triggers synchronous action potentials in 46 48 detrusor smooth muscle [46 48]. The junction potentials are mediated by activation of P2x purinoceptors, which open non-selective cation channels, depolarising the membrane, and activating L-type Ca2+ channels. The contractile response can be abolished by L-type Ca channel blockers, implicating Ca2+ entry and possibly Ca2+-induced Ca2+ release from internal stores in the contractile response. This mechanism does not seem to be apparent in normal human detrusor, but is sometimes seen in unstable detrusor [89,- 90]. Activation of muscarinic receptors produces little change in the membrane potential, [84,- 85 but spike fre84 85] quency is increased at concentrations able to elicit large contractions. Whole cell patch clamp studies show that acetylcholine causes an outward K+ current, presumably mediated through calcium activated K+ channels. The rise in intracellular Ca2+ will 63 91, 92 initiate contraction and may open Ca2+-activated K+ channels. This pathway also generates diacylglycerol in the membrane, which can activate protein kinase C which may be involved in generating the tonic element of the response through modulation of Ca2+ and K+ channels (fig. It is currently believed that Ca2+ influx through Ca2+-channels aids in filling intracellular stores and that open K+-channels keep the membrane potential sufficiently negative to prevent too large a Ca2+ influx through this route [39, 39 95]. This has different properties and innervation to the detrusor, [5] and may play a role in preventing reflux up 5 the ureters during micturition. Changes in the properties of the detrusor could clearly result in major alterations in the behaviour of the bladder, and might result in significant dysfunction. Indeed such changes have been clearly demonstrated in patients and animals with unstable bladders, and there is currently argument as to whether such changes are a cause of unstable contractions or the result of other factors which may underlie instability. Those interested in pursuing this are referred to the proceedings of the consensus conference on the overactive bladder [95, 96]. The main constituents are collagen and elastin in a matrix composed of proteoglycans. The passive mechanical properties of the bladder wall depends on the viscoelastic properties of the stroma and of the relaxed detrusor muscle. Collagen 97 98 and elastin are generally thought to be intimately related to bladder compliance. Just under the urothelium there was a superficial portion interwoven densely by thin collagen fibrils running in all directions, forming a felt-like structure. Carbachol (10-4 M) causes a transient elevation of intracellular calcium as does caffeine (10 mM). Caffeine appears to empty the intracellular stores completely, since carbachol applied immediately after caffeine no longer elicits a calcium transient. This triggers release of further calcium from the stores through ryanodine receptors. The rise in intracellular free calcium concentration triggers contraction, and may also open various calcium-activated channels in the membrane (such as calcium activated K channels), which can modulate the response. Superficial (S), middle (M) and deep (D) portions are distinguishable according to the arrangement and density of the collagen fibrils. Numerous small holes for capillaries and nerves are seen in the superficial portion, and canals for larger vessels in the middle and deep portions. A discontinuous muscularis mucosa separated this layer from the deep portion of the mucosa. This portion was the thickest, and contained a loose network of thick twisted strands of thin collagen bundles. These strands were strongly curled in the empty bladder, but straightened as the bladder was filled. The muscular layer consists mainly of muscle bundles, running in various directions. The collagen fibres are arranged in thick bundles often running transversely to the bundle they surround. Within the muscle bundles winding collagen fibrils form thin lace-like sheaths surrounding the individual smooth muscle cells. Outside the muscular layer there is a loose sub-serosal network of collagen bundles. No such detailed morphological analysis exists for bladders from other species, but in the rat most of the collagen fibrils are found in the mucosa and between the muscle bundles [100]. Fibroblasts, which are com100 mon outside the muscle bundles are rarely seen within. Relative amount of interstitial tissue: Most of the bladder wall collagen is found in the connective tissue outside the muscle bundles. Changes in relation between the amount of muscle and non-muscle tissue in the bladder wall would therefore influence collagen concentration. In the rat infravesical obstruction or bladder denervation induce hypertrophy of the detrusor smooth muscle and the collagen concentration 100 102 decreases [100, 102]. In man, the proportion of connective tissue relative to muscle in the bladder is lower in childhood than in the 103 fetus [103]. Ageing is associated with a relative decrease in smooth muscle in both males and females [104]. This could perhaps 99 be related to the decreased packing density of submucosal collagen during ageing [105]. There seems to be a correlation between the ratio of type lll-to-type l collagen content and bladder compliance. In the foetal bovine bladder the increase in compliance during the second and third trimester is paralleled by a decreased ratio of type lll:l collagen [107]. The adult bovine blad107 der has, on the other hand, a decreased compliance and an increased type lll:l ratio. Also, the type lll:l ratio is increased in low compliant dysfunctional human bladders [108] compared with age-matched controls. The 108 increased amount of collagen type lll is mainly between the cells in the smooth muscle bundles [109]. Elastin fibres are sparse in the bladder, compared to 101 collagen [101] but are found in all layers (see fig. Anti-elastin immunohistochemistry [110] has shown 110 that the elastin in the mucosa-submucosa appears to be arranged in fibres parallel to the urothelial lining. Elastin was also found between and in the smooth muscle bundles, although the organisation was less regular. These however, also cause an intense staining of the urothelium, suggesting the presence of microfibrillar protein in the absence of amorphous elastin.
Order generic norfloxacin pills
Using single fibre electromyography bacteria virtual lab norfloxacin 400 mg line, it has also been proposed that partial denervation of the pelvic floor may occur as a consequence of vaginal delivery [303]. Furthermore, 303 women with urinary stress incontinence or genitourinary prolapse (or both) are more likely to demonstrate electrophysiological evidence of partial denervation of the levator ani than are asymptomatic women. These findings imply that nerve damage is an important aetiological factor responsible for weakness of the pelvic floor. Delayed nerve conduction times are indicative of damage which has been localised to the terminal branches of the pudendal nerves supplying the pelvic floor in women with stress incontinence. Histochemical evidence for the occurrence of partial denervation and subsequent reinnervation is provided by the clustering together of fibres that are all of the same type [304]. This fibre-type clustering has been 304 observed in biopsy samples of levator ani removed from patients with rectal prolapse and faecal inconti305 306 nence [305, 306] and in patients with urinary stress incontinence and genital tract prolapse [307]. However, 307 similar fibre-type groupings have been observed in biopsy samples from nulliparous asymptomatic women. On the assumption that these results are representative of normal, it may be that the fibre-type grouping in the levator ani is normal and thus differs from that of a typical limb skeletal muscle. In the event that such an arrangement occurs in the undamaged levator ani, it is evident that fibre-type clustering demonstrated using histochemical methods cannot be regarded as indicative of partial denervation with reinnervation. In this context a recent study [308] has failed to demons308 trate histochemical evidence for partial denervation of the levator ani although structural features of muscle cell damage are reported in association with aging and with vaginal childbirth. Morphological features such as centrally placed nuclei, fibre splitting and striated cell 70 necrosis are generally recognized as indicative of neuromuscular damage in limb skeletal muscle. Interestingly, all these features have been observed in biopsy samples of levator ani from women considered to be normal. Thus the presence of such features in samples of levator ani cannot necessarily be interpreted as indicative of the presence of pathological damage. Nevertheless, vaginal delivery is associated with stress incontinence and urethral hypermobility, the etiology of which is probably multifactorial. Further detailed studies of the distribution of fibre types throughout the normal levator ani are essential before this uncertainty can be resolved. There is a tubular smooth muscle sphincter that encircles the anal canal over a distance of approximately 3-4 cm above the anal verge (fig. The transition to the internal sphincter is marked by a thickening of the circular fibres, by an increase in the amount of collage present in the muscle, and by a change in the shape of the muscle bundles encircling the lumen [313]. Just cephalic and anterior to the external sphincter, and blending with it on its dorsal side is the puborectalis muscle. This sling-like muscle originates from the inner surface of the pubic bones and passes dorsal to the anorectum just above the external anal sphincter. This space receives the downward extension of the conjoined fibres of the levator ani muscles and the longitudinal smooth muscle coat of the intestine [312,- 313]. These fibres suspend and elevate the 312 313 anorectum preventing its downward prolapse. Their relaxation during defecation allows for eversion of the anal skin that is then pulled up into the anal canal at the end of defecation. Because of the fre309 quent occurrence of both faecal and urinary incontinence, this issue is covered by the consultation and a brief overview of anal sphincter anatomy provided here. Although there has been considerable conflict about sphincter nomenclature [310] the actual 310 anatomy of this region is relatively straight forward [311-313]. There is little controversy about the existence of 310 a superficial muscle associated with the perianal skin usually referred to as the subcutaneous sphincter. This is the external anal sphincter that encircles the anterior portion of the anal canal in the perineal body and that occasionally is lacerated during vaginal delivery. Further subdivision of this highly variable muscle into more portions has more academic than practical importance. The external anal sphincter is innervated by S2-4 fibres that travel via the inferior hemorrhoidal portion of the pudendal nerve. While it is well accepted that childbirth leads to neurogenic damage to the innervation of the external anal sphincter [316] and to disruption of the 316 internal and external sphincters [317] little is known on 317 the impact of vaginal delivery on internal sphincter innervation and function even in the presence of an intact peroneum after delivery. Resting anal sphincter tonus is associated with normal internal sphincter function. Resting tone is known to be lower in women after vaginal birth complicated by a third-degree perineal tear compared to controls with rupture of the sphincters, but direct evaluation of the internal anal sphincter remains difficult. The other levels of fuction and dysfuction will be dealt with later in this volume. The urinary bladder and the urethra contain an epithelial lining surrounded by densely innervated smooth muscle and a connective tissue stroma with blood vessels and sensory nerves. We have systematically described the normal function of these tissue elements and have also given some superficial information regarding their pathophysiology. We have chosen this approach in order to give a basic research background to the more clinically-oriented descriptions of pathophysiological processes leading to incontinence that will be presented in later chapters. The reader must keep in mind that the literature on structure and function of the normal bladder and urethra is overwhelming. The papers we refer to represent only a limited (and 72 carbachol-induced tonic contraction of the pig derusor smooth muscle. In: Potassium channels and their modulators: from synthesis to clinical experience. The overactive bladder: from basic science to clinical management consensus conference. Comparison of clearance of locally injected 99m -technetium pertechnate and radioactive microsphere technique in dogs. The urinary bladder: regional distribution, localization on sensory nerves, and species-related differences. Morphological and histochemical studies on developing human pelvic autonomic nerve cells and paraganglia. Faecal incontinence due to external sphincter division in childbirth is associated with damage to the innervation of the pelvic floor musculature: a double pathology. This report provides an overview of teaching strategies and approaches for pupils with special educational needs, the theoretical underpinnings of these strategies and approaches, and the role of specialist knowledge in teaching these pupils. The report also considers how the findings of the scoping study might become embedded in every day teaching practice. Approach the scoping study drew upon national and international publications, including reviews of research findings, individual research reports and professional guidance for teachers. The areas of need are: - Communication and Interaction - Cognition and Learning - Behaviour, Emotional and Social Development - Sensory and/or Physical Key Findings Across all types of special educational need there was variety in the research methods used. There is evidence about the need for explicit, comprehensive and integrated teaching of different aspects of reading linked to spelling and writing. There is little evidence of the need for distinctive teaching approaches for children with specific learning difficulties although responding to individual differences is crucial. The key to appropriate teaching lies in careful and ongoing assessment linked with teaching. Approaches that encourage children to regulate their behaviour by teaching them selfmonitoring, self-instruction and self-reinforcement skills are effective in producing adaptive behaviour change. Approaches using positive reinforcement (where appropriate behaviour is immediately rewarded), behaviour reduction strategies (such as reprimands and redirection), and response cost (a form of punishment in which something important is taken away) appear to be effective in increasing on-task behaviour. The review found that teaching strategies and approaches are associated with but not necessarily related directly to specific categories of special educational need. A range of theoretical perspectives underpins research in each of the strand areas however there is considerable overlap with behavioural, social constructivist and ecological approaches dominating the intervention literature. The review found that there is evidence that a multi-method approach is promising. Research on the efficacy of multiple approach strategies reports that a combination of strategies produces more powerful effects than a single strategy solution. This does not diminish the importance of special education knowledge but highlights it as an essential component of pedagogy.
Purchase online norfloxacin
Less known are the reports of sexsomnia in which sexual behaviour occurs during sleep antibiotics rash toddler buy generic norfloxacin on-line. This has implications for the way in which the phenomenological approachwillbeusedintherapy. Merskeyfurther goesontoproposeasdefinition: Hypnosis is a manoeuvre in which the subject and hypnotist have an implicit agreement that certain events. Both try hard to put this agreement into effect and adopt appropriate behavioural rules, and the subject uses mechanisms of denial to report on the events in accordance with the implicit agreement. This situation is used to implement various motives whether therapeutic or otherwise, on the part of both participants. There is no trance state, no detectable cerebral physiological change, and only such peripheral physiological responses as may be produced equally by non-hypnotic suggestions or other emotional changes. Therelaxationthataccompanies hypnosis may progress to normal sleeping, even during a hypnotic session. These areas represent central nodes of the salience network linking primary and higher motor areas. McGhie A and Chapman J (1961) Disorders of attention and perception in early schizophrenia. RechtschaffenAandKalesA(1968)A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects. Theearliestdetailedstudy of disordered memory from a psychological standpoint was by Ribot (1882). Thephonological loop holds memory traces of verbal information for a couple of seconds combined with subvocal rehearsal(Baddeley,1986;Baddeley,2002). The latter are referred to as organic or true amnesias and can be described by the different functions of memory. Impairmentofretrievalcan be due to a deficit in either direct retrieval, in which a cue elicits a memory automatically, or strategic (indirect) retrieval, in which a cue provokes a strategic search process that produces a result. Direct retrieval is thought to be dependent on medial temporal lobes and related structures, whereas strategic retrieval is dependent on the ventromedial prefrontal cortex. Inotherwords,thephenomenal experience that accompanies the recognition of a previously presented stimulus seems to takeatleasttwoforms. Fantastic confabulation with persecutory content has been described by Roth and Myers (1969). Central to the idea of confabulation is therefore a notion of false reports in the context of memory disorder. At a minimum, it involves both distortions of content as well as temporal context. Then I came to the rehabilitation institute, no I actually went to Jimsburg store and we had a small meeting there. The current view is that memory confabulation usually derives from dual lesions taking in basal forebrain areas and frontal executive systems. These lesions appear to result in impaired strategic retrieval of memory and disturbed verification/monitoring of the abnormal memory output(DeLuca,2009). It occurs with clouding of consciousness and is particularly useful in distinguishing this from dissociative abnormalities (Allison, 1962). Unilateral placement of electrodes accelerates postictal recovery and shortens the duration of amnesia(Fraser,1982). However, decline in intellectual performance (Rogers, 1986), impairment in neuropsychological test batteries (Taylor and Abrams, 1984), sometimes a dementia-likesyndrome(LiddleandCrow,1984)andsubstantialmemorydeficit(Cutting,1985; McKenna etal. Furthermore, there is evidence of impairment of working memory and semantic memory, but procedural or implicit memory is intact. There may be altered states of consciousness such as a fugue, with impairedregistration. Thedegree of confabulation was related to problems in suppressing inappropriate responses and formal thoughtdisorder. Simple, momentary, or provoked confabulations, on the other hand, appear to be commonplace. Dissociative (Hysterical) Fugue the symptoms pertaining to dissociative (conversion) disorders (hysteria) in the International Classification of Diseases (World Health Organization, 1992) are of two types: conversion and dissociation. Thus the features of dissociative fugue are dissociative amnesia, purposeful travel beyond the usual everyday range and maintenance of basic self-care (World Health Organization,1992). Intellectual function had eventually returned to her premorbid, superior level by ninemonths. Recovered memory has been particularly associated with the return of memory for childhoodsexualabuse. Thetermfalse memory syndromecameintousein1992,whentheFalseMemorySyndrome Foundation was set up to represent the interests of parents who had been accused of abusing theirchildrensexually. They report sexual abuse in childhood, which it is claimed has been forgotten and recovered only in adult life, having been repressed from eight to 40 years. HirsteinW(2009)Confabulation: views from neuroscience, psychiatry, psychology, and philosophy. Everything in the world that is presented to us comes to us in space and time and we experience it only in these terms. Jasperscontinues: `If we want to bring these primary things home to ourselves in some neat phraseology we may say that they both represent the sundered existence of Being, separated from itself. A sense of time is clearly very central to the concept of self and its relationship with the outsideworld. This cluster of time characteristics is implicated at all levels of being, from the most physical of planetary movements via physiological rhythms to patterns of social organization, from the taken for granted via the invisible to the obvious, from the imposed via the lived to the culturally constructed. There can be no rejuvenation, no unknowing, no reconstitution of pollution back into aeroplane. Subjectivetimemaybealteredso that the experience of time duration, flow of time, meaning of time, uniqueness of time and successionoftimemaybeaffected. Disorder of knowledge of time is closely associated with disturbanceofconsciousness,attentionandmemory. Suchpatientsweremuchless able than chronic schizophrenic patientswithout age disorientationto answer questionsabout dateandthedurationoftime. Clinically significant disorders of temporal order for past and current events have been reported. It must be getting on for morning now, he thought once as he raised himself and looked around. Thepatientfeels that time is standing still, that in some way everything temporal has come to an end. Sometimes when people run quickly to and fro in the garden or if the wind stirs up the leaves, I would like to live again as before and be able to run interiorly with them in order that time would pass again. When I finish something, I have the feeling of not being able to do anything else afterwards and of doing this thing, going to dinner for example, for the last time. Music, whose source was to his left, sounded very loud and very fast, as if `several radios were all blaring away together. However, if he were addressed directly, the rate appeared quite normal and he could understand it quite well. I am like a burning arrow that you hurl before you; then it stops, falls back, and is finally extinguished as if in a space empty of air. It was a disturbance of the feeling of recognition that accompanies recall in the process of memory. This new time was endless, more manifold than the previous one, hardly deserving the name "time" as we know it. Suddenly it came to me that this time did not only lie in front of and behind me, but spread out in all directions. There is considerable circumstantial, but little direct, evidence that circadian rhythms are causally associated with affective disorders (Thompson, 1984). In depression, changes of body temperature and cortisol levels over the 24 hours have also been interpreted as phase advance of the circadian rhythm, but the results are equivocal.
Cheap 400mg norfloxacin with mastercard
I firmly believe that if the whole materia medica sinus infection order norfloxacin 400mg otc, as now used, could be sunk to the bottom of the sea, it would be all the better for mankind-and all the worse for the fishes. He is geared, not to recognize the question marks that pain raises in him who suffers, but to degrade these pains into a list of complaints that can be collected in a dossier. The pupils of Hippocrates43 distinguished many kinds of disharmony, each of which caused its own kind of pain. Whereas the Chinese tried very early to treat sickness through the removal of pain, nothing of this sort was prominent in the classical West. The Greeks did not even think about enjoying happiness without taking pain in their stride. The human body was part of an irreparably impaired universe, and the sentient soul of man postulated by Aristotle was fully coextensive with his body. In this scheme there was no need to distinguish between the sense and the experience of pain. The body had not yet been divorced from the soul, nor had sickness been divorced from pain. All words that indicated bodily pain were equally applicable to the suffering of the soul. In view of that heritage, it would be a grave mistake to believe that resignation to pain is due exclusively to Jewish or Christian influence. Thirteen distinct Hebrew words were translated by a single Greek term for "pain" when two hundred Jews of the second century B. The history of pain in European culture would have to trace more than these classical and Semitic roots to find the ideologies that supported personal acceptance of pain. For the Neo-Platonist, pain was interpreted as the result of some deficiency in the celestial hierarchy. For the Manichaean, it was the result of positive malpractice on the part of an evil demiurge or creator. This attitude towards pain is a unifying and distinctive characteristic of Mediterranean postclassical cultures which lasted until the seventeenth century. The Neo-Platonist interpreted bitterness as a lack of perfection, the Cathar as disfigurement, the Christian as a wound for which he was held responsible. In dealing with the fullness of life, which found one of its major expressions in pain, people were able to stand up in heroic defiance or stoically deny the need for alleviation; they could welcome the opportunity for purification, penance, or sacrifice, and reluctantly tolerate the inevitable while seeking to relieve it. Opium, acupuncture, or hypnosis, always in combination with language, ritual, and myth, was applied to the unique human performance of suffering pain. One approach to pain was, however, unthinkable, at least in the European tradition: the belief that pain ought not to be suffered, alleviated, and interpreted by the person affected, but that it should be-ideally always-destroyed through the intervention of a priest, politician, or physician. There were three reasons why the idea of professional, technical pain-killing was alien to all European civilizations. Second: pain was a sign of corruption in nature, and man himself was a part of that whole. One could not be rejected without the other; pain could not be thought of as distinct from the ailment. The doctor could soften the pangs, but to eliminate the need to suffer would have meant to do away with the patient. Third: pain was an experience of the soul, and this soul was present all over the body. He constructed an image of the body in terms of geometry, mechanics, or watchmaking, a machine that could be repaired by an engineer. The body became an apparatus owned and managed by the soul, but from an almost infinite distance. The living body experience which the French refer to as "la chair" and the Germans as "der Leib" was reduced to a mechanism that the soul could inspect. These reactions to danger are transmitted to the soul, which recognizes them as painful. Pain was reduced to a useful learning device: it now taught the soul how to avoid further damage to the body. Leibnitz sums up this new perspective when he quotes with approval a sentence by Regis, who was in turn a pupil of Descartes: "The great engineer of the universe has made man as perfectly as he could make him, and he could not have invented a better device for his maintenance than to provide him with a sense of pain. He says first that in principle it would have been even better if God had used positive rather than negative reinforcement, inspiring pleasure each time a man turned away from the fire that could destroy him. From being the experience of the precariousness of existence,53 it had turned into an indicator of specific breakdown. By the end of the last century, pain had become a regulator of body functions, subject to the laws of nature; it needed no more metaphysical explanation. By 1853, barely a century and a half after pain was recognized as a mere physiological safeguard, a medicine labeled as a "pain-killer" was marketed in La Crosse, Wisconsin. From then on, politics was taken to be an activity not so much for maximizing happiness as for minimizing pain. The result is a tendency to see pain as essentially a passive happening inflicted on helpless victims because the toolbox of the medical corporation is not being used in their favor. In this context it now seems rational to flee pain rather than to face it, even at the cost of giving up intense aliveness. It seems enlightened to deny legitimacy to all nontechnical issues that pain raises, even if this means turning patients into pets. Increasingly stronger stimuli are needed to provide people in an anesthetic society with any sense of being alive. Drugs, violence, and horror turn into increasingly powerful stimuli that can still elicit an experience of self. Widespread anesthesia increases the demand for excitation by noise, speed, violence-no matter how destructive. This raised threshold of physiologically mediated experience, which is characteristic of a medicalized society, makes it extremely difficult today to recognize in the capacity for suffering a possible symptom of health. The reminder that suffering is a responsible activity is almost unbearable to consumers, for whom pleasure and dependence on industrial outputs coincide. By equating all personal participation in facing unavoidable pain with "masochism," they justify their passive life-style. Yet, while rejecting the acceptance of suffering as a form of masochism, anesthesia consumers tend to seek a sense of reality in ever stronger sensations. They tend to seek meaning for their lives and power over others by enduring undiagnosable pains and unrelievable anxieties: the hectic life of business executives, the self-punishment of the rat-race, and the intense exposure to violence and sadism in films and on television. In such a society the advocacy of a renewed style in the art of suffering that incorporates the competent use of new techniques will inevitably be misinterpreted as a sick desire for pain: as obscurantism, romanticism, dolorism, or sadism. Ultimately, the management of pain might substitute a new kind of horror for suffering: the experience of artificial painlessness. Lifton describes the impact of mass death on survivors by studying people who had been close to ground zero in Hiroshima. He believed that after a while this emotional closure merged with a depression which, twenty years after the bomb, still manifested itself in the guilt or shame of having survived without experiencing any pain at the time of the explosion. These people live in an interminable encounter with death which has spared them, and they suffer from a vast breakdown of trust in the larger human matrix that supports each individual human life. They experienced their anesthetized passage through this event as something just as monstrous as the death of those around them, as a pain too dark and too overwhelming to be confronted, or suffered. The sufferings for which traditional cultures have evolved endurance sometimes generated unbearable anguish, tortured imprecations, and maddening blasphemies; they were also self-limiting. The new experience that has replaced dignified suffering is artificially prolonged, opaque, depersonalized maintenance. Increasingly, pain-killing turns people into unfeeling spectators of their own decaying selves. In the name of progress, it has now ceased to be the concern of those who are ill. It was to guide the nation in a militant conversion to healthy living which would make medical sick-care less necessary. Each family would again be able to take care of its members, and each village to provide for the sick who were without relatives. A national health service would be in charge of health care and would supervise the enactment of dietary laws and of statutes compelling citizens to use their new freedoms for frugal living and wholesome pleasures.
Order norfloxacin overnight
Spanke infection 7 weeks after abortion norfloxacin 400 mg online, "Tanzmusik in der Kirche des Mittelalters," Neuphilosophische Mitteilungen 31 (1930). Ladner, the Idea of Reform: Its Impact on Christian Thought and Action in the Age of the Fathers (Cambridge: Harvard Univ. For Pelagius death was not a punishment for sin, and Adam would have died even had he not sinned. Kathleen Cohen, Metamorphosis of a Death Symbol: the Transi-Tomb in the Late Middle Ages and the Renaissance (Los Angeles: Univ. Gruesome tombs meant to teach the living appear first in the last years of the 14th century. The fact that around 1500 death assumes strong skeletal features and a new autonomy does not mean that it had not always borne anthropomorphic features, if not in art, then in legend and poetry. Hartlaub, Zauber des Spiegels: Geschichte und Bedeutung des Spiegels in der Kunst (Munich: Piper, 1951). Hartlaub, "Die Spiegel-bilder des Giovanni Bellini," Pantheon 15 (November 1942): 235-41. The "world" depicted as a female figure in medieval art- half angel, half demon-represents the power of this-worldly goods, the beauty of nature, but also the decay of all that is human. Rosalind Moss, the Life After Death in Oceania and the Malay Archipelago (1925; Ann Arbor, Mich. Consult also the following works by James George Frazer: Man, God and Immortality (London: MacMillan, 1927); the Belief in Immortality and the Worship of the Dead, vol. Kurtz, the Dance of Death and the Macabre Spirit in European Literature (New York: Institute of French Studies, 1934). Rosenfeld is the best introduction to the research and gives a detailed up-to-date bibliography. Clark, the Dance of Death in the Middle Ages and the Renaissance (Glasgow: Jackson, 1950). Elf, 1970): reproductions are very clear and are organized according to different themes. Consult the standard iconographies on Western Christian art: Karl Kunstle, Ikonographie der christlicher Kunst, 2 vols. Boase, Death in the Middle Ages: Mortality, Judgement and Remembrance (New York: McGraw-Hill, 1972). On the impact of time on the French death-image, see Richard Glasser, Time in French Life and Thought, trans. On the growing impact of time consciousness on the sense of finitude and death, see Alois Hahn, Einstellungen zum Tod und ihre soziale Bedingtheit: Eine soziologische Untersuchung (Stuttgart: Enke, 1968), especially pp. The response to "natural" death was a profound transformation of behavior at the hour of death. Eberhard Klass, Die Schilderung des 20 Sterbens im mittelhochedeutscken Epos: Ein Beitrag zur mittelhochdeutschen Stilgeschichte, dissertation, Univ. Patch, the Other World According to Descriptions in Medieval Literature (Cambridge, Mass. Emir Rodriguez Monegal, "Death as a Key to Mexican Reality in the Works of Octavio Paz," mimeographed, Yale Univ. Lenz Kriss-Rettenbeck, "Tod und Heilserwartung," in Bilder und Zeichen religtosen Volksglaubms (Munich: Callwey, 1963), pp. Leibowitz, "A Responsum of Maimonides Concerning the Termination of Life," Koroth (Jerusalem) 5 (September 1963): 1-2. Fehr, "Tod und Teufel im alten Recht," Zeitschrift der Savigny Stiftung fur Rechtsgeschichte 67 (1950): 50-75. He was only the master of his life to the extent that he was the master of his death. From the 17th century onward, one began to abdicate sole sovereignty over life, as well as over death. These matters came to be shared with the family which had previously been excluded from the serious decisions; all decisions had been made by the dying person, alone and with full knowledge of his impending death. Maitiand, "The Last Will," in the History of the English Law Before the Time of Edward I (Cambridge: University Press, 1968), vol. Infanticide remained important enough to influence population trends until the 9th century. Death remained a marginal problem in medical literature from the old Greeks until Giovanni Maria Lancisi (1654-1720) during the first decade of the eighteenth century. The same philosophers who were the minority which positively denied the survival of a soul also developed a secularized fear of hell which might threaten them if they were buried while only apparently dead. Philanthropists fighting for those in danger of apparent death founded societies dedicated to the succor of the drowning or burning, and tests were developed for making sure that they had died. Elizabeth Thomson, "The Role of the Physician in Human Societies of the 18th Century," Bulletin of the History of Medicine 37 (1963): 43-51. The hysteria about apparent death disappeared with the French Revolution as suddenly as it had appeared at the dawn of the century. Doctors began to be concerned with reanimation a century before they were employed in the hope of prolonging the life of the old, 41 Theodor W.
Thea viridis (Green Tea). Norfloxacin.
- Is Green Tea effective?
- Preventing colon cancer.
- Dosing considerations for Green Tea.
- Low blood pressure. Green tea might help in elderly people who have low blood pressure after eating.
- Preventing dizziness upon standing up (orthostatic hypotension) in older people.
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96923
Order discount norfloxacin line
These endopelvic fascial sheets prevent the ventral movement of the posterior vaginal wall infection vs colonization buy 400mg norfloxacin free shipping. The majority of the endopelvic fascia fibres atta- Urethral support is important to stress continence in women, as support in symptomatic women may be inadequate [289]. This support is supplied by a combi289 nation of connective tissue and muscle arranged to resist the downward force created by increases in abdo290 minal pressure [290]. The urethra lies adjacent to and is intimately connected with the anterior vaginal wall. The connections of the vagina and urethra to the levator ani muscles and the arcus tendineus fascia pelvis determine the structural stability of the urethra. Portions of the levator ani, lateral vaginal wall and endopelvic fascia have been removed to show midline structures (DeLancey 1994). Some authors have commented on the amount of 297 connective tissue within human pelvic floor muscle compared with quadrapedal animals and have sought associations with the assumption of an upright posture [281]. However, the connective tissue component of the 281 levator ani has not received the same attention as the striated muscle component, although several workers have suggested that deficient or abnormal collagen may be the cause of pelvic floor dysfunction in humans 299 298 [298, 299]. A histological study of vaginal fascial connective tissue carried out in women with and without uterine prolapse reported abnormal histological changes in 7 out of 10 patients with uterine descent [300]. Other workers have shown a significantly higher 300 incidence of pelvic organ prolapse in women with hypermobile joints compared with a control group with no clinical joint laxity, further implicating abnormalities of collagen in pelvic floor dysfunction [301]. Clear301 ly, further studies are required in order to examine the role of contributing factors, such as age, oestrogen activity, obesity, parity and delivery, as well as sexual activity and physical work, on the structure and function of the connective tissue components of the levator ani. Data of this type may prove invaluable in furthering our understanding of the normal functioning of the pelvic floor. The ischium has been removed as have portions of the iliococcygeus muscle and lateral vaginal wall. Note attachment of the vaginal wall by the endopelvic fascia to the inner surface of the iliococcygeal muscle. A study on biopsy samples from a group of women with genuine stress incontinence has shown that both the number and diameters of slow and fast twitch muscle 302 fibres decrease with increasing age [302]. Conclusion the report concluded that questions about whether there is a separate special education pedagogy are unhelpful given the current policy context, and that the more important agenda is about how to develop a pedagogy that is inclusive of all learners. The report considers how the strategies identified from the review as having the potential to raise achievement might be usefully organised in a typology that could be used to create a multi-method response to teaching pupils with special educational needs. A second phase of this research programme should involve systematic, long-term development work across a range of sites and settings, which also allows for the examination of the impact of the innovations upon achievement. Such research is necessary to advance knowledge about teaching and learning, and to understand how combinations of teaching approaches might be used in different contexts and for different purposes. Such a research programme should examine teaching and learning in real settings as it will need to take account of the ways in which teachers do their work in relation to the wide variety of situations they face. The work was undertaken by research teams based at the universities of Manchester and Cambridge. This report presents a considered analysis of the literature on teaching strategies and approaches for pupils with special educational needs together with recommendations for further research on this topic. Make recommendations for the focus and development of future research in this area. The first three questions guided the literature review which was undertaken during July and August 2003. The findings of the review were then analysed in relation to the second three questions which relate to the future development of teaching strategies and approaches for pupils with special educational needs. This scoping study drew upon national and international publications, including reviews of research findings, individual research reports and professional guidance for teachers. Each strand was led by a faculty member from either Cambridge or Manchester who liased with a counterpart in the other institution. In this way team leaders were supported by a link colleague who organised and co-ordinated the contribution of colleagues and research assistants within their institution. It should be noted that the brief for this project was to undertake a scoping study rather than a full-scale systematic literature review. As this scoping study was not commissioned as a systematic review, we did not restrict our search to research which involved controlled clinical approaches to the study of teaching approaches and interventions. This was important as many systematic reviews exclude numerous interventions, not because they are ineffective, but because their effects have not been documented by the specific research designs specified in the selection criteria. A bibliography listing all of the sources identified during the course of the project is included in Appendix B. The work presented here is based on professional knowledge and bibliographic input from the research team as well as online searches of relevant databases. We searched widely for literature 8 reviews and studies which reported on teaching strategies for pupils with special educational needs in order to survey the current scene in terms of topics, approaches, key theoretical concepts and to identify seminal works. Specific review criteria were not applied, nor were sources subjected to the rigorous scrutiny of a systematic review. We are aware of arguments in favour, including, that the re-introduction would facilitate research on outcomes for pupils with special educational needs. Nevertheless, an important element of the scoping study was to consider whether certain teaching approaches are more (or less) appropriate for pupils with particular impairments. To this end we produced strand reports which summarised the literature on teaching strategies and approaches for pupils who experience difficulties in one or more of four areas (cognition and learning needs, behaviour, emotional and social development needs, communication and interaction needs and sensory and/or physical disability needs). Though we found a range of theoretical perspectives underpinning the strategies and approaches these tended to cluster around three principal theoretical perspectives. These are: (1) behavioural (2) social constructivist and (3) ecological perspectives. This theory considers all behaviour is learned according to rules which shape, change or sustain it. Cognitive-behavioural approaches take account of the capacity of individuals to understand and reflect on their behaviour. The advantages of this model lie primarily in the positive, practical outlook, the clear signs of success, and the ways in which the setting of specific targets allows all those involved in teaching and learning to understand the goals and expectations for individuals and groups of pupils. However these approaches have been criticised for an overly narrow focus on measurable learning outcomes, when it is known that many aspects of knowledge and understanding are not directly observable and measurable in the required form. Constructivist models of learning are those in which children are seen as active participants in the processes of seeking out knowledge, making sense of their experiences and gaining intrinsic satisfaction from learning and solving problems. Constructivist learning is seen to be a transformative experience which opens up opportunities for further learning as children gain greater depth of understanding and increasingly flexible ways of representing their knowledge and dealing with new information. In such a model the learner is situated in the centre of the system interacting at various levels each of which are part of a larger system, for example, the level of the classroom (micro level), the level of the school not involving the child directly (macro level) and society (macro level). Teaching strategies and approaches often focus at a micro level but acknowledge or incorporate activity at broader levels. The mesosystem refers to the relationships between two or more settings in which the child participates. Such an approach allows consideration of the role of such things as school or community culture in learning. There is a diversity of communication and interaction needs and, indeed, a wide variation in the terminology used to refer to this group of children. Consequently, for the purposes of this review it was decided to think about the children associated with this strand in terms of in three broad groupings. Here the work of Dockrell and Lindsay, (2000) has been influential in that they went some way towards establishing a common terminology for those children who are unable to express themselves in the normal effortless way as their peers, and where the difficulty cannot be attributed to physical or sensory impairments, (Bishop, 1997; Adams Byers Brown and Edwards, 1997). Children with communication and interaction difficulties associated with severe and profound learning difficulties. This group of children tend to communicate at an early intentional or pre-intentional level. Children in this group are seen as displaying deficits in three key areas, atypical communication and social development, adherence to ritualistic behaviour, plus a resistance to change (Howlin, 1998), with variable age of onset.
Cheap norfloxacin 400mg on-line
Some questions that may be considered before acquiring an access control system are shown in Table 2-1 virus 3 weeks generic norfloxacin 400mg without a prescription. In general, the higher the security requirement and the greater the number of access control devices one must pass through, the lower the throughput rates. The performance of biometric systems is generally based upon the number of data reading errors or false identifications. At this point and at locations inside, access control may be manual or automated in some fashion. Automated equipment may have an entire database resident at the site of the equipment, or the access control device may communicate with a centrally located or remote database. The manner in which authorized user data is handled at any location depends on the overall system and equipment choices and should be carefully considered with access control professionals during the design process. Small facilities or those that have relatively low-security requirements may use personnel to manage the information by hand. Many facilities continue to meet their access control needs with security guards and identification badges or a token driven turnstile system that does not query a database. The operational portions of these databases often maintain just the information reference record used to verify or identify the user. Personal information used to generate the record may reside in archives or may be discarded after the records are generated. Some electronic token and biometric access control systems can verify at the reader without querying the central database. Microprocessor smart cards may carry their own authentication algorithms and templates. Centralized electronic databases are used primarily to manage the pool of authorized personnel and their access privileges and to maintain a record of ingress/egress events. Some software systems allow access privileges to be linked to security threat posture levels, organizational requirements, or other criteria, so that a change in criterion will automatically update the access privileges of each authorized individual. Failure to consider all the factors can result in unacceptable performance, low reliability, or a short useful life. Exterior zones are likely to be affected by the prevailing climate, seasonal extremes, and fluctuations in weather conditions. Man-made environmental factors, such as activity patterns, electrical fields, radio transmissions, and movements of vehicles, trucks, trains, or aircraft also influence the design and performance of integrated security and access control systems. Interior zone access control equipment will generally be located in more controlled climates, but several environmental factors, such as electronic interference, must still be taken into account. The alarm data is displayed on a computer monitor as text or as symbols on a map of the area. In most automated electronic access control systems, several of these capabilities are combined to provide the security operations center personnel with access control and intrusion detection information. Although each access control system is unique in the number and scope of options available, all automated systems perform the basic function of annunciating alarms and displaying the alarm locations in some format. Some operate with proprietary software, written by the manufacturer of the access control system. Most of the new security systems have links to mobile devices for accessing system information. Typically, the alarmed area is automatically displayed on monitors in the operations center and systematically recorded for future detailed analysis. Incorporating mobile devices and laptop computers into many security command and control systems by using wireless technologies provides the responder with the same information as the central monitoring personnel. These capabilities significantly enhance the safety of responding personnel and allow for more efficient and appropriate responses to actual or suspected unauthorized access attempts. Integration of access control technologies with other systems or technologies may require the development of a software interface unless the system has been designed to operate with other technologies. All access control technologies have vulnerabilities and may generate false acceptances or rejections. Many access control systems have the capability to notify security personnel of attempts by unauthorized persons to gain entry; to tamper with, cut, or bypass the access control equipment; or to attack the connectivity between the access control equipment and the processing or command and control stations. Different access control devices can be integrated to reduce the chances of false acceptances and to provide alternatives for false rejections or inabilities to use a certain type of system. The protocol provides mechanisms for building automation devices to exchange information. Occasionally a manufacturer will use a proprietary communications protocol that may limit the possibility for future upgrades and system expansions to the original manufacturer. Some systems may not be able to reset automatically and could require operator intervention to restore operation, while other systems may require time to return to full operational status. Potential intruders may be aware of these vulnerabilities and may seek to cut or interrupt power if they cannot circumvent the system by other means. It is critical that all elements of the system have backup power systems incorporated into the design and operation to ensure uninterrupted operation, alarm reporting, situation assessment, and intrusion response. Backup power sources may include uninterruptible power supplies, generators, or automatic bus power transfer switches. Power, line conditioning, and battery or other backup power requirements should be defined during the system design phase. Often the costs associated with infrastructure changes or the assessment and alarm reporting systems are more than the costs of the access control components. Costs can be minimized by defining threats carefully, performing a detailed site survey, and selecting between several technologies that provide similar categories of protection. Additionally, using suitable existing infrastructure, such as power cabling or conduit, can help mitigate some costs. Upgrade costs can sometimes be mitigated by choosing equipment compatible with existing systems or with parts of existing systems. The key element in protecting buildings is the establishment of an appropriate stand-off distance depending on the vulnerability assessment and the building characteristics. The first line of defense is the design of roadways, approaches, and parking areas in proximity of the building. The topics covered in this section are barriers, bollards, turnstiles and portals, and guard facilities. Barriers generally protect and control vehicular entry points by allowing only authorized vehicles. Many styles of barriers are available, such as wedge or drop arm barriers as well as ornate gates and planters. Retractable or removable barriers are available for situations where occasional access may be needed for authorized or emergency vehicles. Barriers primarily prevent unauthorized vehicles from entering a controlled area by blocking the route of travel. They can also be used to guide or slow traffic near a controlled area, deter vehicles by their presence, absorb the impact of a vehicle, and/or damage a vehicle during intrusion attempts. There are several types of barriers available for specific applications, such as ornamental barriers at the edge of sidewalks and retractable barriers for emergency vehicle access to pedestrian areas. Most traditional barriers are made of steel, concrete, or a combination of both and can be set above or below ground. Active barriers are manually or automatically activated in response to acts of aggression. Passive barriers do not depend on detection or response and are usually stationary structures. Passive barriers are usually used for perimeter protection and at entry points that are rarely used or have restricted traffic. Crash gates are an effective defense mechanism and can be architecturally appealing. Due to its energy absorbing capabilities, the system provides security while preserving much of the integrity of the barrier. This is an important consideration as many barriers are destroyed after a vehicle impact, leaving the site vulnerable while the barrier is restored.

Purchase 400 mg norfloxacin with mastercard
The access control system compares the data entered with the enrollment database and antibiotic 7 days to die purchase cheapest norfloxacin and norfloxacin, if entry is authorized, signals the portal to open or the turnstile to release and allow access. These access control systems usually have an anti-passback feature that prevents an individual from passing their card or badge back to an unauthorized person attempting to gain access. Portals are used in higher security situations in which more scrutiny of each individual is required. Portals are often interlocked as a mantrap when prolonged scrutiny is required of each person seeking access. The specific application of access control technology also influences the performance of equipment. Turnstiles have relatively high throughput, even though people must pass through the opening in a one-by-one sequence rather than as a crowd. Portals have lower throughput than turnstiles, because the device must open and shut for each person passing through. A guard booth is often the first thing a visitor encounters upon entering a secure facility. Many booths on the market today combine aesthetic appeal with a high degree of strength and durability. A guard booth may be nothing more than a physical shelter against the elements, or may be a component of a secure fortress against physical attacks. High-security booths are available that meet or exceed commercial and federal standards for ballistic and explosion protection. For high-security facilities, such as nuclear power plants or government facilities, guard booths may be the first line of defense against unwanted visitors or attacks. High-security booths built to federal explosion resistance standards are designed to provide protection for the booth occupants during an explosion. Personnel greeting or visitor check-in points are prime interior locations for guard booths. Many options are available that range from sliding transaction drawers to full restroom facilities. Portable booths with various levels of ballistic and explosion protection are available. Security managers requiring high-security guard booths should consider incorporating minimum standoff distances for explosives, vehicle barriers, and delay devices into the overall security infrastructure. The access control panel provides control signals to the security devices, such as electric or magnetic locks, based on input from the token reader. A properly designed and installed token-based access control system can be used to monitor physical access, logical access. The token systems discussed in this handbook vary in complexity, from simple to complicated, and for low to high security applications. Identification cards and badges are physical systems that require visual verification at an entry point to be effective. Key card systems only allow those who have a specifically coded key card to pass through a particular door. A common security process, known as two-factor authentication, is to present a token and require an additional piece of information that is usually memorized. A third way to increase access control security levels is to design layered systems, where fewer people have access to more sensitive areas inside the facility. Barcoding, holographic imaging, water marking, and time expiring chemistry are the primary technologies available to customize a particular identification badging system beyond the basic information and photo. Many card or badge systems can accommodate more than one of these customizing technologies. Barcodes use vertical lines of varying height and width which represent an identification security code. The barcode is analyzed by the reader, verified against an access control list, and the card holder is allowed or denied access to the area. Several industries, specifically automotive, electronics, and chemical, have defined standards for their uses and applications. These standards ensure universal compliance within an industry and identification accuracy better than 99 percent. The holographic image is used as an anti-forgery technology on badges; however, the equipment used to create these images can be expensive and may not be cost-effective. Time expiring chemistry is useful for persons who should have only temporary access to a facility or area. A time expiring badge can be printed with information or images, including photos, and then the technology applied and activated. When the time runs out, the color changes or bleeds through on all or some portion of the card or badge. Where guards are present to monitor access, persons entering frequently must show a facility badge or identification card. Visitors and other persons lacking badges are moved aside to apply for authorization to enter. Badge holders are often required to display their badge prominently throughout their time in the controlled area. Cards or badges can be the basis for high-security access control systems that depend on using personnel and administrative techniques instead of electronic infrastructure. For example, some facilities use two photo identification badges for access control. The first badge is given to the portal control person, who matches it against a file of interior access badges. When a match is found, the guard exchanges the badges and allows the individual to access the facility. While this type of system does not rely heavily on technology, it does offer some advantages. When an access privilege is changed or revoked, the interior card is simply updated to reflect the new level of access. The process of issuing, showing, or wearing a badge provides a basic level of access control for many organizations. It identifies the persons authorized access to a controlled facility or services, and provides a quick, reliable means of visual identification. Since potential intruders may try to copy or substitute cards or badges, some facilities use holograms or watermarks to complicate the counterfeiting process. Door mounted key card systems do not interact in real time with a central database. These systems are available in two technologies: magnetic encoded stripe and contact smart card. Systems using magnetic encoded stripes and contact smart cards require a key to be encoded at the point where the card is issued. The stripe normally contains about 140 digits and characters in one to three tracks, the user name, authorized access levels, expiration date, and other information. Types of Keycards Access Control Technologies Handbook the quantity of information on contact smart cards can be much greater than on a magnetic encoded stripe card. The magnetic encoded stripe and contact smart card key card systems should not be confused with the systems capable of very high security access control covered in the technology reviews on magnetic encoded stripe systems and contact smart card systems. Some systems read the presence of a valid card in the slot, and will remain unlocked as long as the card is present. In other systems, such as magnetic encoded stripe, the card must be fully inserted and then removed to cycle the lock. Operating the mechanical latch completes the cycle and resets the lock to the closed position. Fine-grained access control is the ability to permit or deny access through a single door or set of doors. For example, doors can easily be re-keyed whenever a key is lost or stolen, and access can easily be modified for special requirements. Room keys, staff keys, and manager keys can be coded to enhance both security and productivity. Room keys might operate a lock to the room and some common area, while a staff key could operate the locks for a series of rooms, but only within a certain time period. Access for fire and emergency crews can be coordinated and granted to affected areas quickly. In systems where locks are under local control, having emergency policies set in advance can be beneficial. Master keys should be protected from misuse, but still be readily accessible when necessary to protect the lives and possessions of occupants.
