
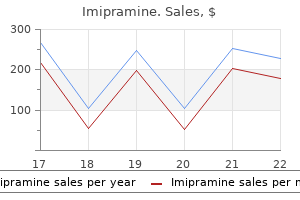
Purchase imipramine 50mg without a prescription
Appraise 1 n Most hernias in adults are para-umbilical anxiety symptoms dry lips imipramine 25mg without a prescription, protruding adjacent to 2 n Some adults, especially of African origin, have true umbilical her3 n Repair umbilical hernia by early operation for fear of strangulanias that have been present throughout life. The contents are most frequently omentum, which is often adherent to the interior of the sac. Closure Close the inguinal canal, subcutaneous tissue and skin as for an inguinal hernia. In particular operate on strangulated, painful (reducible or not) hernias, especially those with small, hard margins. However: n Small para-umbilical hernias (less than 1 cm) can be left untreated if asymptomatic. In some cases there is extensive malignant disease, when surgery is rarely indicated. With a laparoscopic approach the mesh is secured intra-peritoneally against the defect with staples or sutures. For recurrent or periumbilical incisional hernias a laparoscopic approach may be considered. If the hernia is large, make a spindle-shaped incision to include the umbilicus, excising the stretched skin. Rectus muscle Rectus sheath Action 1 n Cut through the thinned-out edge of aponeurosis to expose the 2 n Clear the sac of fatty tissue and cut it right round, at least 2 cm distal to the neck if possible. The contents of the sac are less likely to be adherent here than in the fundus, but free them if necessary. If there is a mass of fibrous omentum, excise it with the fundus of the sac but take care to ligate all the bleeding omental vessels and avoid damaging the transverse colon. Secure the mesh in to good tissue with 2/0 polypropylene sutures allowing a 2-cm margin. Onlay mesh repair Repair 1 n For the underlay repair of a small, well-defined direct defect, take mining of the skin and placement of a foreign body is at risk of seroma formation. At each quadrant insert a 2/0 polypropylene suture through the intact tissue about 8 mm from the edge of the defect, pick up a small bite of the mesh and pass the needle back out through the intact tissue of the posterior wall, close to the point of entry. Hold the suture with an artery forceps and repeat the manoeuvre at each quadrant of the defect. Then parachute the mesh through the defect in to the extra-peritoneal space and tie the four sutures. Additionally, suture the edge of the defect to the surface of the mesh with continuous polypropylene. Closure 1 n If the skin over the fundus was preserved, pick up the undersurface of the navel with a synthetic absorbable stitch and sew it to the rectus sheath to produce a dimple. Each stitch penetrates the upper leaf of the rectus sheath 3 cm from the edge, passes beneath it to catch the lower leaf 1 cm from the edge and passes back 3 cm from the edge. Addition of polyglactin to the polypropylene mesh does not reduce adhesions, although coating with titanium significantly reduces its inflammatory reaction. Polytetrafluoroethylene, as a composite with polypropylene with the polytetrafluoroethylene side in contact with the viscera, significantly lowers the incidence of adhesions. Preparation 1 n Place the anaesthetized patient supine on the operating table 2 n Clean the abdomen with povidone-iodine 10% alcoholic soluwith their arms by their side. Sometimes with mesh placement it is easier to move around the patient and so it is therefore useful to have a monitor on both sides. Access 1 n Obtain access in an area away from any previous incision and away from the hernia, both of which are usually in the midline. Previous incisions may have adhesions or bowel adherent to them, presenting an inherent risk of damage, so gain access to the abdominal cavity as far back laterally as is safe on the insufflated abdomen. Use either an open (Hasson) technique or a closed technique using a Veress needle. The left subcostal area is often suitable for initial insufflation with a Veress needle. Continue to divide any adhesions to allow visualization of the anterior abdominal wall for an area large enough to enable placement of a flat mesh of sufficient size. Action 1 n Define the margins of the hernia defect and ensure that any ad2 n Reduce the contents of the hernia sac using graspers and diahesions are cleared for at least 5 cm from the edge of the hernial defect. Assess If adhesions obscure your view of the hernia, divide them carefully using scissors and diathermy. It is very difficult to dissect a suf4 n Assess the size of mesh required to give a minimum of a 4-cm If initial access to the abdomen is difficult, try placing a 5-mm trocar and cannula in the left subcostal position, then select suitable positions for the lateral insertion of the trocars and cannulas in to the abdomen under direct vision. Mark the centre of the mesh with a marker pen to aid orientation inside the abdomen and ensure you position it centrally over the hernia defect. Unfold it, using two 6 n Make sure that the mesh lies flat over the abdominal wall. Staple graspers, and orientate it centrally over the hernial defect, ensuring equal coverage on all sides. This is sometimes helped by passing a suture from the centre of the mesh through the umbilicus. Although they are more expensive and more difficult to handle, they reduce the risk of adhesions. If you are inserting a large mesh, be willing to apply a second inner row of staples around the defect to fix it securely to the abdominal wall. Closure 1 n Suture the deep surface of the umbilical skin to the aponeurosis n with fine absorbable synthetic material. Checklist 1 n Is the hernial defect well covered with mesh overlapping at least 2 n Check any residual bleeding, using laparoscopic clips if necessary. It will not close spontaneously, so repair it locally through a transverse incision sited directly over the defect. Access 1 n Approach the hernia through a transverse incision curved be2 n Preserve the umbilical skin by turning it upwards as a flap. If there is distal obstruction, relieve this at the same time as closing the fistula. Recurrent infections may require a minor plastic procedure to reduce the depth of the umbilicus. Action 1 n Expose the aponeurosis and the neck of the sac, which is within the 5 n the umbilicus is a rare site for pilonidal sinus, treated by excision. Excise the umbilicus and, if indicated, carry out bilateral block dissection of the inguinal nodes (vide infra). Infected defects can be repaired using biological meshes such as Permacol or Strattice (Lifecell Corporation) but these are very expensive. Otherwise place a piece of polypropylene mesh 2 cm larger than the defect in each direction in the extra-peritoneal plane and secure it, as described for the underlay repair of a well-defined inguinal defect. Action 1 n Deepen the incision until you reach aponeurosis or muscle, then 2 n Dissect the edges cleanly and separate the peritoneum from the deep 3 n If possible, invaginate the sac with a continuous suture. Repair 1 n There is no advantage in attempting to define the layers of the 2 n Herniation may occur early, while the patient is still in hospital. Repairs have a high recurrence rate, reduced by the use of mesh, but this increases the risk of persistent infection or intestinal fistula. Jaundice, malnutrition, obesity, postoperative distension and re-exploration through the same incision after a short interval are other contributory factors, as are steroids and immunosuppression. The mesh may be applied at three levels in the abdominal wall, as described below. Wherever it is placed it must extend at least 2 cm beyond the margin of the defect. Appraise n 1 Large defects are best repaired using a composite mesh to reduce the risk of bowel adhesions (see laparoscopic umbilical hernia 3 n Place another continuous suture to fix the mesh where it lies over the edge of the defect. The tubing tends to curl up in one corner; prevent this by tunnelling the tube under the fascia at one or two points. Extra-peritoneal mesh repair Action 1 n At open operation, make a skin crease incision over the lump and 2 n Once dissected, invert the sac and develop the pre-peritoneal open the external oblique aponeurosis in the line of its fibres, extending the incision medially to open the anterior rectus sheath. The layers of the abdominal wall can usually be closed without tension using a 0 Prolene suture.
Radix Codonopsis (Codonopsis). Imipramine.
- How does Codonopsis work?
- Are there safety concerns?
- What is Codonopsis?
- Dosing considerations for Codonopsis.
- HIV infection, protection against radiotherapy in cancer treatment, brain disorders, anorexia, diarrhea, asthma, cough, diabetes, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96622
Buy cheap imipramine
If contrast does not flow freely to outline the duodenal mucosa anxiety 24 weeks pregnant buy imipramine amex, it may be due to a small stone or ampullary spasm: the administration of 20 mg of intravenous buscopan may be helpful. As a minimum, you must see the right main duct branching in to its anterior and posterior sections and the left duct giving rise to the medial and lateral branches. Occasionally it is necessary to tilt the table slightly head-down in order to see the proximal ducts. Check for filling defects which may represent retained stones and also for the continuity of the vital anatomy. Action 1 n A flexible linear probe is inserted (usually through the epigastric port) and the entire biliary tree from the intra-pancreatic portion of the bile duct to the second order divisions of the intrahepatic ducts may be visualized. The technique has the added advantage of being able to identify the location of both the ductal and vascular structures prior to dissection in cases of severe inflammation. Despite this, there remains a role for single-stage management of gallbladder and ductal stones, retrieval of incidental stones detected on routine intra-operative ductal imaging and for those patients in whom endoscopic clearance has either failed or is technically impossible. Take care in negotiating the junction between the cystic and common bile ducts in order not to injure the posterior wall of the bile duct. It is often possible to retrieve several stones with each pass, depending on their size. Repeat the procedure, adding more contrast as necessary until the duct is seen to be clear. Alternatively, a 3-mm choledochoscope with an instrument channel may also be used, although this is not widely available. Prepare 1 n the 2 n In addition, the necessary supplemental equipment should be same general preparations as for cholecystectomy are required. The basket may be passed through an appropriate choledochoscope, passed through a cholangiogram catheter or simply passed directly down the duct. In all cases, care should be taken to avoid injury to the posterior wall of the bile duct as instruments are inserted. This may drain placed a small amount of bile for a day or two postoperatively, but inevitably dries up quickly provided the closure has been carefully performed. The potential complications of a displaced T-tube or stent may outweigh their benefits in this situation. Thompson, Bookwalter) to optimize the 2 n Transcystic exploration may be performed as described above; view of the gallbladder and structures of the porta hepatis. The choledochoscope should be used with continuous saline irrigation and can be used to push any recalcitrant distal ductal stones onward through the ampulla if they cannot be dislodged proximally. Gently insert a catheter from the distal end of the duct in an attempt to dislodge the stone. If this fails and the stone is palpable above the ampulla through the posterior wall of the duodenum, then a direct incision of the duct and sphincteroplasty can be performed (see below). Stitch the duodenal wall to the bile duct wall on each side of the divided sphincter and bile duct every 3 mm or so as you advance using fine (5/0 or 6/0) absorbable monofilament sutures. Although the surgical technique provides complete division of the sphincter muscle to provide a more reliable and longer lasting drainage procedure than the endoscopic alternative. Avoid instrumentation of the pancreatic duct, but ensure that it has not been narrowed by any of your sphincterotomy sutures. If there is any concern over narrowing the duodenum, then close the duodenotomy transversely as a duodenoplasty rather than longitudinally. In the long term, there is a risk of anastomotic stricture or enteric reflux, which could lead to episodes of cholangitis. If you have trouble identifying the ampulla, pass a catheter from the common bile duct, which should pass in to the duodenum. If a stone is impacted in the ampulla, a catheter from above may help disimpact it when you cut down on to it. Pancreatic papilla 7 n Pass a small cannula in to the duct and aspirate bile to confirm and use small retractors or stay sutures on the margins of the incision to give you an optimal view of the ampulla. It is important to identify and protect the pancreatic papilla when fashioning the sphincteroplasty. Pass the instrument behind the bile duct from medial to lateral to minimize risk of injury to the portal vein, which lies behind and medial to the bile duct. Minimize the amount of dissection of the proximal duct in order to protect its blood supply. For bile duct injuries, it should be dissected down to the upper border of the pancreas, excised and oversewn at that level. In the long term, there is a risk of anastomotic stricture or ascending cholangitis. The former may require biliary balloon dilatations; the latter is treated with antibiotics. Identify an appropriate point to divide the jejunum to provide an optimal blood supply to each end of the bowel, with an adequate length for the Roux loop to reach the bile duct without tension. You may need to make the division further to the right in order to lengthen the Roux loop if the mesentery is short. Open this window with diathermy sufficiently to allow free passage of the Roux loop and its mesentery without any tension. The enterotomy should be just smaller than the bile duct and should be divided through the full thickness of the bowel wall. When you reach the mesenteric border, lock the suture and leave the needle attached on a small clip. If the bile duct is very small, it may be possible to enlarge the lumen available for the anastomosis by spatulating the anterior wall of the bile duct, using a short longitudinal incision, in order to minimize the risk of postoperative stricture formation. In general terms, ducts smaller than 10 mm are most prone to postoperative complications and bile duct injuries where the first or second order branches of the duct are involved are particularly troublesome. Continue the inner posterior layer by taking fullthickness bites of the bowel wall on each side; on reaching the end of the posterior layer continue around on to the anterior layer and close this with sero-submucosal bites to exclude and invert the mucosa. Tie the suture to the looped free end when you finish the inner anterior layer and trim the tails. The role of single-incision laparoscopic surgery in abdominal and pelvic surgery: a systematic review. Meta-analysis suggests antibiotic prophylaxis is not warranted in low-risk patients undergoing laparoscopic cholecystectomy. Hepatobiliary and Pancreatic Surgery: A Companion to Specialist Surgical Practice. Prevalence and outcome of litigation claims in England after laparoscopic cholecystectomy. Meta-analysis of randomized controlled trials on the safety and effectiveness of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Development of symptoms and complications in individuals with asymptomatic gallstones. Prospective randomized trial using cost-utility analysis of early versus delayed laparoscopic cholecystectomy for acute gallbladder disease. Prospective randomized controlled trial of traditional laparoscopic cholecystectomy versus single-incision laparoscopic cholecystectomy: report of preliminary data. Role of laparoscopic cholecystectomy in the early management of acute gallbladder disease. Laparoscopic ultrasound as the primary method for bile duct imaging during cholecystectomy. Comparison of long-term results of laparoscopic and endoscopic exploration of common bile duct.
Generic imipramine 75 mg amex
Tie the inferior mesenteric artery at its origin from the aorta and the inferior mesenteric vein below the inferior border of the pancreas anxiety symptoms in 12 year old boy purchase cheap imipramine line. If the carcinoma involves the abdominal wall, excise the area with the tumour and repair the defect at the end of the procedure. Be prepared to resect a loop of small bowel or excise part of the bladder fundus en bloc if they are attached to the tumour. Involvement of the ureter usually occurs as it crosses the iliac vessels at the pelvic brim: you may be able to resect this portion and reimplant the proximal end in to the bladder using a psoas hitch and/or a Boari flap. Do not hesitate to involve another specialist if you are not experienced enough to deal with an unfamiliar area or technique. If the tumour is situated in the left half of the transverse colon or at the splenic flexure, excise most of the transverse colon and unite the hepatic flexure to the descending or sigmoid colon. Alternatively, perform an extended right hemicolectomy with an ileocolic anastomosis. Do not divide the sigmoid higher than 10 cm above the rectosigmoid junction or you will leave an ischaemic segment distally. Cross-staple or use a Parker-Kerr clamp just distal to the intended site of division. If the carcinoma is distal, preserve the greater omentum by dividing the adhesions between the omentum and the colon proximally to the middle of the transverse colon and entering the lesser sac. If the tumour is situated near the flexure, divide the left side of the gastroepiploic vascular arcade and excise the lesser and greater omentum with the specimen. Identify the inferior mesenteric vein lying laterally and clamp, ligate and divide it below the lower border of the pancreas. Select the 28-mm diameter stapler and take care when advancing it around the rectal valves or you may tear the rectum. If it will not advance to the top of the rectum, resect a further segment of rectum or anastomose the colon end-to-side to the rectum. This cytotoxic washout removes any viable tumour cells that may otherwise implant in the anastomotic line. Action 1 n Splenic flexure mobilization is carried out first, once the tumour 5 mm 5 mm 5 mm 10 mm 5-12 mm 5 mm. The small bowel is kept in the right side of the abdomen by tilting the operating table to the right (right side down position). Using the same device, blunt dissection is carried out in the avascular plane between the descending colon mesentery and the retroperitoneal fascia. The inferior border of the pancreas should be clearly evident: avoid dissecting deep to the pancreas. After completion of the medial dissection, start the lateral dissection at the mid-transverse colon. The greater omentum is peeled off the colon by incising the fascia just above the bowel, caution being taken to avoid damage to either colon or mesocolon. The posterior wall of the stomach should be clearly seen once the lesser sac is entered. By keeping close to the colon at all times, further dissection along the upper and lateral border will allow complete mobilization of the splenic flexure. Sufficient mobilization is achieved when the splenic flexure can be swung to the midline. A head-up (reverse Trendelenburg) tilt helps improve exposure during the final stage of lateral dissection. Insert the circular stapler transanally and perform intra-corporeal anastomosis as for open surgery. The lateral-first approach is easier for the novice as it is the same as for open surgery and is described here. This is continued upwards to the previously dissected area near the splenic flexure. Following this, a window is created in the sigmoid mesentery at the rectosigmoid junction. By grasping the tape and moving it to and fro, the assistant surgeon can provide the necessary countertraction and exposure for subsequent mesenteric division and colon mobilization. Take care to avoid damage to the underlying right hypogastric nerve and right ureter. If adequate lateral dissection has been performed, a generous retromesenteric window is easily made at the base of the mesosigmoid, which should by now look paper-thin. Divide the remaining posterior fascial attachments between the mesentery and the retroperitoneum. At a trial descent, the splenic flexure should reach the pelvis easily without tension. Use a muscle-splitting incision which is less painful than a muscle-cutting incision and results in fewer postoperative hernias. Check again that the colon is long enough to allow for a tension-free anastomosis low down in the pelvis, reaching the symphysis pubis extra-corporeally without tension. Secure the anvil of a circular stapler in the colonic stump with a purse-string suture. Re-establish pneumoperitoneum and reposition the 4 n If the patient presents as an emergency with obstructive symptoms 5 n A few patients with small early carcinomas (T or pain, perform a trephine colostomy (see below) and then undertake a full assessment and appropriate neoadjuvant treatment. Note the relation of the tumour to the peritoneal reflection and decide whether it is mobile, adherent to other organs or fixed within the pelvis. Take your time and deepen the dissection in the mesorectal plane in a circumferential manner. Do not compromise the success of radical resection by breaching the mesorectal plane of dissection. Action 1 n Mobilize the left side of the colon by dividing the congenital adhesions as described for left hemicolectomy. Assess the length of colon required to achieve a tension-free anastomosis: if the planned proximal resection margin will reach to the pubic symphysis, it will reach to the pelvic floor. Identify the left ureter and gonadal vessels and sweep them away from the mesocolon. Push away the tissue containing the pelvic nerve plexus which lies deep to the vessels: both branches of the plexus should be visible as they divide around the rectum at the level of the sacral promontory. Pull the rectum forwards to dissect 5 Make a similar incision in the peritoneum of the left side to produce a window with artery above and nerves below. If the patient is old and atherosclerotic, divide the pedicle further from the aorta, preserving the left colic artery. Select a suitable area to transect the proximal colon and divide the mesentery up to this point. Transect the bowel using a linear cutting stapler and pack the proximal colon and small bowel out of the way in the upper abdomen. If it is below the peritoneal reflection, mobilize the rectum and mesorectum down to the pelvic floor. Remove the specimen containing the rectal carcinoma, the complete mesorectal envelope and inferior mesenteric pedicle. If only a small cuff of sphincter and rectum remains, swab it out with the same solution. Unite Staple or suture the anastomosis, depending upon the level of anastomosis, ease of access to the pelvis and the obesity of the patient. Suture the anterior layer using interrupted seromuscular inverting sutures, again inserting them all before tying them. In the female, dissect distally between the rectum and vagina as far down as necessary to achieve adequate mobilization of the tumour. Carry out the operation exactly as described above but close the rectal stump using a cross stapler. For lower third tumours this degree of clearance is not possible in a restorative procedure.
Cheap imipramine online amex
Hypertension Primary or essential hypertension is the most common form of hypertension in older children and adolescents anxiety keeping you awake buy imipramine 25mg without prescription. Childhood obesity is associated with hypertension in children, which often tracks in to adulthood. Youth with dyslipidemia are treated with a diet low in total and saturated fats and cholesterol. The intake of complex carbohydrates is increased, whereas that of simple sugars is decreased. Diabetes Mellitus Diabetes mellitus is associated with cardiovascular complications, which develop early in childhood and adolescence. Endothelial dysfunction seen in both types of diabetes is recognized to aggravate cardiovascular risk in later life. Optimal daily and longterm glycemic control, maintenance of blood pressure and lipid levels in the normal values for age, regular exercise, healthy diet and avoidance of smoking are necessary. Tobacco Consumption Mechanisms by which smoking exerts its detrimental effects on cardiovascular system include endothelial dysfunction, increased oxidative stress, increased arterial stiffness, alterations in lipoprotein metabolism and induction of prothrombotic state. School based campaigns to prevent smoking and chewing tobacco are appropriate tools to contain this public health concern. Parents should be role models to children by avoiding or quitting smoking and chewing tobacco. Early atherosclerotic disease has been documented in certain conditions in children. The risk category, group of diseases in each category and the prevention oriented treatment targets are shown Table 15. The glomerulus is made of a tuft of capillaries and a central region of mesangium. The capillaries arise from the afferent arteriole andjoin to form the efferent arteriole, the entry and exit being at the hilum of the kidney. The capillary wall consists of fenestrated endothelium, glomerular basement membrane and foot processes (podocytes) of visceral epithelial cells. The Bowman space leads in to the proximal tubule that has an initial convoluted portion, then the straight segment, descending and ascending limbs of the loop of Henle and the distal tubule. Six to eight distal tubules join to form the collecting ducts that finally enter the renal pelvis. The renal artery divides in to segmental arteries that branch to form interlobar and arcuate arteries. The latter give rise to the intralobar arteries, which provide the afferent arterioles for the glomeruli. The efferent arterioles from the glomeruli form a meshwork of peritubular venous capillaries that empty in to intralobar veins. The early part of the distal tubule on its ascent from the medulla to the cortex lies near the glomerulus of the same nephron. The cells of the tubule in contact with the afferent arteriole are denser than the rest and called macula densa. The smooth muscle cells of the afferent arteriole, in this region, contain prominent cytoplasmic granules that are the site of renin activity. Renal Physiology Glomerular filtration depends upon the higher pressure in afferent arterioles. The filtration barrier is constituted by the endothelium with slit pores, basement membrane and podocytes of visceral epithelial cells. Filtration of solutes depends upon their molecular size, shape and electrical charge. The filtrate from the glomerular capillaries passes from the Bowman capsule in to the proximal convoluted tubule, loop of Henle, distal tubule and collecting ducts. The filtrate contains all the diffusible and ultrafiltrable substances present in plasma. Small quantities of protein are usually present, but are reabsorbed in proximal tubule. Bulk of the glomerular filtrate is reabsorbed in to the peritubular capillaries and only 0. Sodium transport is dependent on the parallel transport of bicarbonate, chloride, amino acids and glucose. Tubular reabsorption of sodium and other permeable solutes is promoted by the phenomenon of solvent drag during transport of water across the tubular epithelium. Increased delivery of chloride to the macula densa results in local activation of renin-angio tensin mechanism. The renin-angiotensin-aldosterone system, prostaglandins and natriuretic peptides are involved in sodium handling. Distal tubules and collecting ducts are responsible for urinary acidification, concentration and regulation of sodium balance. Exchange of potassium or hydrogen ions for sodium takes place in the distal tubules under the regulation of aldosterone. Bicarbonate, consumed in the buffering of nonvolatile acids, is regenerated by the renal excretion of titrable acid and ammonia. Division of the ureteric bud within the metanephros induces the development of nephrons. The ureteric bud gives rise to the intrarenal collecting system, renal calyces, pelvis and ureter. Partitioning of the cloaca during the 5th week results in the formation of the urogenital sinus anteriorly and the anal canal posteriorly. The kidneys grow steadily in size between the 12th week and the 40th week, with the renal length increasing from about 1. The fetal bladder is visualized by the 10-14th week, and its capacity increases steadily to about 50 ml at term. Beyond the 16th week, the amniotic volume is principally dependent on urine production. Serum creatinine level is high at birth, reflecting maternal values, but falls rapidly to 0. Infants have reduced sodium and bicarbonate reabsorption and limited ability for hydrogen ion excretion. Plasma Osmolality the capacity of the kidneys to concentrate or dilute urine is limited in neonates. Growing babies utilize most of the protein available for growth rather than catabolize to urea. Decreased production and excretion of urea result in a relatively hyposmolar interstitium and reduced urinary concentration. Thus, delayed feeding and overdiluted or concentrated feeds are potentially harmful. Maturation of Renal Function Renal function continues to improve during the first two years of life, at the end of which, various parameters of renal function approach adult values, if corrected to standard surface area. Abnormal urinary stream or dribbling of urine suggests an anomaly of the distal urinary tract. The causes of acute kidney injury in the newborn are different from those in older children. It is important to diag nose these infections since urinary tract anomalies may be present. An important cause of acute kidney injury, at this age, is hemolytic uremic syndrome. Renal tubular disorders such as renal tubular acidosis and Fanconi syn drome are usually diagnosed at this age. Rickets at this age is rarely due to vitamin D deficiency, unless there is malabsorption or chronic liver disease. Acute-on-chronic renal failure, previously undetected chronic renal failure, symptomatic hypertension and collagen vascular diseases are common. Other conditions, which might impart a red color to urine include hemoglobinuria, myoglobinuria, porphyria and ingestion of beetroot. If fluid intake is not restricted, the edema may increase and involve hands, feet and legs. In nephrotic syndrome, edema develops insidiously, starting with eyelid puffiness most noticeable in the morning. Persistent dribbling indicates abnormal ureteric insertion distal to bladder neck.
Order imipramine 75mg amex
The anastomosis is usually created in one layer anxiety numbness purchase discount imipramine online, using interrupted absorbable sutures. Insert three stay sutures from out to in and in to out evenly spaced around the bowel circumference. Clip the ends and get your assistant to hold the clips to exert traction on the cut edges of bowel. When two segments of narrow intestine must be united, they may both be opened along their antimesenteric borders, which are then joined back-to-back. The mesenteries are now on opposite sides of the anastomosis and cannot always be neatly approximated. Approximate the cut end to the side of bowel to which it End-to-side anastomosis 2 n Incise will be joined and insert a posterior seromuscular suture. Insert the all-coats stitch as before, remove the clamps and complete the seromuscular stitch. Two of the three corner stitches are held taught and interrupted sero-muscular sutures are placed between them with the knots on the outside. Remove 2 It may also be employed as an alternative to end-to-end anastomosis after intestinal resection, in which case the cut ends of bowel should first be closed and invaginated. The advantages of the side-to-side anastomosis are that the segments of bowel to be united have no interruption to their blood supply at all and that the incisions can be made exactly congruous. The disadvantages are that there are more suture lines involved and that there may be some degree of stasis and bacterial overgrowth. Bypass is obsolete: although it may achieve remission of active disease in the defunctioned segment, bacterial overgrowth of the blind loop may aggravate diarrhoea and there is a long-term risk of carcinoma. For short stenotic areas of bowel strictureplasty (see below) is an alternative to resection. Where possible, avoid bypass or exclusion procedures: the defunctioned bowel may still give rise to problems such as bleeding and fistula. Wide resection is the optimal approach, ensuring that at least one side of the subsequent anastomosis employs healthy, nonirradiated, bowel. Prepare 1 n In the presence of an obstructing lesion, ensure that the patient is adequately resuscitated before operation with nasogastric intubation and intravenous rehydration. When side-to-side anastomosis follows bowel resection, suture the cut edge of mesentery to the adjacent intact mesentery on each side of the anastomosis. It is sensible to employ appropriate prophylactic antibiotic cover, such as a cephalosporin plus metronidazole given preoperatively in a single injection, in all operations likely to involve intestinal resection. In the absence or obstruction or fistula, supplemental enteric feeds may reverse the nutritional defect, but some patients require a period of preoperative parenteral nutrition. Resection is sometimes indicated for fistula, diverticulitis, intussusception and a symptomatic blind loop. Small portions of the duodenum and ileum are removed during partial gastrectomy and right hemicolectomy respectively. An accidental perforation is unlikely to be located in a segment of bowel you intended to remove. A multivariate analysis has shown that the only independent predictors of earlier postoperative recurrence after initial operation are an initial presentation with peritonitis secondary to perforation, and a longer preoperative disease duration. Continue by exam2 n If a loop of small bowel has been strangulated in an external herining the stomach, large bowel and remaining abdominal viscera. Except when operating for primary malignant tumours it is quite unnecessary to excise a deep wedge of mesentery, which might increase the extent of small bowel requiring removal. It is more than likely that further resection will be required in future, and microscopic inflammation of the bowel at the resection margin does not appear to increase subsequent anastomotic recurrence. Action 1 n Isolate the diseased loop of bowel from the other abdominal con2 n Hold up the bowel and examine the mesentery against the light. Standard resection 1 n Determine the proximal and distal sites for dividing the bowel, and select the line of vascular section in between; keep close to the bowel wall. The first two clamps are right next to the bowel wall at each point chosen for intestinal transection. Divide the vessels between artery forceps, ligating the mesentery beneath each pair of forceps using 2/0 or 3/0 Vicryl ties, according to the thickness of the mesentery. Proceeding in this manner, divide the mesentery right up to the bowel wall at the further end of the line of peritoneal incision. Take care in placing and tying each ligature: if the knot slips, there can be troublesome haemorrhage. They should be applied obliquely at the points of intended intestinal transection, so that slightly more of the antimesenteric border is resected than of the mesenteric border; the obliquity reduces the risk of a tight anastomosis. Now apply a non-crushing clamp about 5 cm outside each crushing clamp, having milked the intervening bowel free of contents. Place the specimen and the soiled knife in a separate dish, which is then removed. Non-crushing clamp Thin crushing clamps 6 n Perform a single-layer, end-to-end anastomosis, as described in the previous section. In an attempt to limit contamination, some surgeons divide the intestine between two pairs of light crushing clamps. Clamp and cut it off at the neck, then close the defect in two layers as a transverse linear slit. Incise the bowel flush with the outer aspect of each clamp, and close the wall in two layers, leaving a transverse suture line. Approximate the ends of the ellipse, pull apart the sides and close transversely as before. As before, the narrower segment of bowel (on the left) is transected obliquely, removing more of the mesenteric border with the specimen. Check that the bowel is pink, that haemostasis is secure and that all mesenteric defects are closed. A haematoma develops in the mesentery or in the submucosa at the point of intestinal transection. If the bleeding is not fully controlled, incise the peritoneum, find the bleeding point, pick it up with fine artery forceps and ligate it. Non-viable bowel will not heal; so if you are in any doubt excise a few more centimetres and start again. Leave the nasogastric tube on free drainage, aspirated regularly for the first 24 hours. The tube can usually be removed when the volume of aspirate drops below the volume of fluid taken by mouth. If it does develop, remove sufficient sutures to allow the pus to drain, irrigate the wound, obtain bacteriological cultures and, if cellulitis is present, institute appropriate antibiotic therapy. Once the infection is controlled, the wound usually heals without the need for secondary suture. Abscess sites may be subphrenic, subhepatic, pelvic or adjacent to the anastomosis. The management of an established small-bowel fistula is described later in this chapter. Decompress obstructed jejunum by milking the contents upwards until they can be aspirated through the nasogastric tube. The obstructed ileum may be decompressed prior to performing an anastomosis if the obstructed segment is being resected. If no bowel is being resected or anastomosed, do not open the bowel to attempt decompression, 2. In the presence of obstruction there may be marked disparity between the diameters of the bowel ends. In practice, moderate incongruities can be overcome by adjusting the size of suture bites while suturing proximal to distal bowel. The diameter of the distal bowel can be increased by transecting it more obliquely, sparing the mesenteric border, and by opening it along the antimesenteric border. If there is gross disparity, consider a side-to-side sutured or stapled anastomosis.
Purchase online imipramine
Weil-Felix test can be used in developing countries where other tests are not available for diagnosis of rickettsia infection but the test should be interpreted in conjunction with history and clinical presentation anxiety heart rate cheap imipramine 75 mg on-line. If clinical suspicion for rickettsia is high, then empirical therapy should be started without waiting for any confirmatory test. Differential Diagnosis Spotted fever can mimic a great number of febrile illnesses. Other diseases included in differential diagnosis are typhoid fever, secondary syphilis, leptospirosis, toxic shock syndrome, scarlet fever, rubella, Kawasaki disease, parvoviral infection, idiopathic thrombocytopenic purpura, thrombotic thrombo cytopenic purpura, hemolytic uremic syndrome, Henoch Schonlein purpura, hepatitis, dengue fever, infectious mononucleosis and malaria. Chloramphenicol is reserved for patients with doxycycline allergy and for pregnant women. Furthermore, the increased mortality with chloramphenicol compared with tetracycline, when other factors such as severity are considered, have led to preference for doxycycline even in young children. The therapy should be continued for a minimum of 5-7 days and for at least 3 days until the patient is afebrile in order to avoid relapse. Patients treated with one of these regimens usually become afebrile within 48 hr and thus the entire therapy lasts for less than 10 days. In patients with severe disease, admission to an intensive care unit and appropriate supportive therapy may be required. All patients of pulmonary tuberculosis and most cases of extrapulmonary disease are caused by human type strain of Mycobacterium tuberculosis. A few cases of extrapulmonary illness particularly the tubercular lymphadenitis may be due to the bovine strain. The infection is spread by the tuberculous patient, who discharges tubercle bacilli in his sputum or nasopharyngeal secretions during bouts of coughing or sneezing, etc. In the pediatric age groups, few infections may also occur by the transplacental route (congenital tuberculosis). The usual mode of infection is through inhalation of droplets of infected secretions. The infected sputum spitted carelessly by open cases of tuberculosis dries up and the tubercle bacilli are resuspended in the dust and air. Rarely infection may be transmitted through skin, mucous membrane or transplacentally. Health education of people about mode of transmission by ticks and means of personal protection is equally important. Tuberculosis still is one of the deadliest diseases in the world killing nearly 2 million people every yr. More than ninety percent of all tuber culosis cases occur in the developing countries, where limited resources are available for optimal treatment. Tuberculosis continues to be an important cause of morbidity and mortality for children worldwide. Tuberculosis infection and disease among children are much more prevalent in developing countries, where resources for control are scarce. The estimated lifetime risk of developing tuber culosis disease for a young child infected with M. The age of the child at acquisition of infection has a great effect on the occurrence of tuberculosis disease. Tubercle bacilli are not transferred across the healthy placenta but the fetus may be infected from the infected placenta. Frequency of infection with tubercle bacilli increases progressively as the child grows in age. An infant is more likely to develop disease after an infection compared to an older child. Adolescent children, especially girls, are prone to develop active tuberculosis disease during puberty. Undernourished children are more susceptible to develop tuberculosis, probably due to depressed immunological defenses. Tuberculosis may precipitate kwashiorkor or marasmus in an infant with borderline undemutrition. A malnourished patient, who does not respond to the dietary therapy should be promptly investigated for tuberculosis. The diseases that affect the cell mediated immw1ity are more likely to increase the susceptibility. A quiescent tuberculous infection may flare up after an attack of measles or pertussis, that suppresses cell mediated immune response. The risk of acquiring infection has been associated consistently with the extent of contact with the index case, the burden of organisms in the sputum and the frequency of cough in the index case. Patients with smear positive pulmonary tuberculosis are more likely to transmit infection. An increased risk of developing Infections and Infestations - infection has been seen in institutional settings, including nursing homes, correctional institutions and homeless shelters. Pathology the inhaled tubercle bacilli may lodge in the pulmonary alveoli and cause inflammation with hyperemia and congestion. If the host resistance is good, the inflammatory exudate around the primary focus is absorbed and the caseous area inspissated. When the cell mediated immune response is weak, the bacilli continue to multiply and the inflammatory process extends to the contiguous areas. From this stage, the bacilli may spread to other parts of the lobe or the entire lung. Ball-valve effect due to incomplete obstruction may lead to trapping of air distal to obstruction (emphysema). If the host immune system is good, then these foci are contained and disease does not occur. Lowering of host immunity may lead to activation of these metastatic foci and development of disease. This is especially seen in young infants, severely malnourished children and children with immunodeficiency. The commonest site for this type of disease is the apex of the lung (Puhl lesion), because the blood flow is sluggish at apex. Miliary and meningeal tuber culosis usually occur within a yr of the primary lesion. Asymptomatic infection is defined as infection associated with tuberculin hypersensitivity and a positive tuberculin test but with no striking clinical or roentgenographic manifestations. Irritating dry cough can be a symptom of bronchial and tracheal compression due to enlarged lymph nodes. In some children, the lymph nodes continue to enlarge even after resolution of parenchymal infiltrate. Expectoration of sputum and hemoptysis are usually associated with advanced disease and development of cavity or ulceration of the bronchus. Abnormal chest signs consist mainly of dullness, decreased air entry and crepitations. Children with endobronchial tuberculosis may present with fever and troublesome cough (with or without expectoration). Occasionally, the child not responding to bronchodilators may be misdiagnosed as asthma. In a wheezing child not responding to bronchodilators less than 2-yr-old, the possibility of endobronchial tuberculosis should always be considered. Miliary tuberculosis is characterized by hematogenous spread and progressive development of innumerable small foci throughout the body. The child may have high-grade fever, which is quite unlike other forms of tuberculosis. There are hardly any pulmonary findings but fine crepitations and rhonchi may be present. These findings may occasionally be confused with other acute respiratory infections of childhood. The illness may be severe, with the child having high fever, rigors and alteration of sensorium. The other presentation of miliary tuberculosis may be insidious with the child appearing unwell, febrile and losing weight. Pleural effusion follows the rupture of a subpleural focus in to the pleural cavity. If the sensitivity is high, there is significant pleural effusion along with fever and chest pain on affected side. Minor effusions associated with the rupture of primary foci are usually not detected.
Syndromes
- Loss of sense of taste
- Cut down on salt, whether it is table salt, or flavor intensifiers that contain salt such as monosodium glutamate (MSG).
- Sleep problems such as insomnia
- Stomach pain that does not go away after a bowel movement
- Arterial blood gas
- Subtotal or partial thyroidectomy, which removes part of the thyroid gland.
- Coarctation of the aorta
- Bromocriptine (Parlodel)
- You have high levels of the hepatitis B virus in your blood
- Recent flu-like symptoms
Generic imipramine 50mg visa
Separate the anvil and staple cartridge anxiety symptoms eye pain buy imipramine 50 mg cheap, and remove the anvil and the plastic ring. If the doughnut is incomplete, it means that there is a portion of the oesophageal wall that has not been adequately stapled, and patent varices may still be present. When you remove the pack from the upper abdomen, bleeding may not be fully controlled. If so, carefully inspect the anastomosis to identify where the transection is incomplete, or determine the site of bleeding. In both cases insert some additional mattress sutures of Vicryl through the entire thickness of the oesophageal wall to control bleeding from any remaining vessels and seal the anastomosis. Identify, dissect, ligate and divide all the short gastric vessels between the greater curvature of the stomach and the spleen. Check the rest of the greater curvature of the stomach and dissect, ligate and divide any remaining vessels between it and the diaphragm. On the lesser curve of the stomach identify, ligate and divide any vessels passing to it from the lesser omentum. The entire proximal stomach should now be separated from any feeding vessels along its greater and lesser curves. Fortunately, the internal vascularization of the stomach is almost always adequate to prevent any avascular necrosis. Devascularization of the abdominal oesophagus is performed close to the oesophageal wall by ligating and dividing all perforating veins which run transversely. Division of the vagii facilitates the devascularization; because of this, perform a pyloroplasty. Duodenum Postoperative 1 n Since the stomach has been opened give antibiotics for 48 hours. The aim of the shunt is to achieve profound decompression of the portal system and lower portal pressure, thereby stopping the variceal bleeding. Oesophageal varices Short gastric veins Portal vein Splenic vein Coronary vein Superior mesenteric vein Left renal vein C. Appraise 1 n Portal decompression can be portacaval, which may be end-toside or side-to-side. In poor-risk patients perioperative mortality is 50%; in good-risk patients, around 5%. Investigate liver function, identify the nature of the liver pathology and the vascular anatomy. Patients who tolerate this operation well with minimal encephalopathy are those with good liver function, such as patients with portal vein occlusion, primary biliary cirrhosis or hepatic fibrosis. Do not undertake a shunt operation lightly; there is a risk of encephalopathy and consequent intellectual impairment. Therefore the description will be limited to the traditional end-to-side portacaval shunt. There are usually dilated portal-systemic venous anastomotic vessels in this tissue, which may require careful, individual suture ligation. It shunts all the portal blood in to the infrahepatic vena cava, reduces the portal hypertension and stops bleeding from oesophageal varices. During this dissection retract the common bile duct anteriorly and to the left, taking care not to damage the blood supply to its wall. Be careful of preserving an aberrant right hepatic artery if it exists, as it lies behind the bile duct and on top of the portal vein. Flush the now collapsed segment of portal vein distal to the clamp with a solution of heparin 1:500 000 in physiological saline. Access n 1 Place the patient supine on the operating table with slight rotation towards the left. Check 1 n Confirm a good flow through the shunt by feeling for a venous thrill or preferably by observing a measured fall in portal pressure (using a Doppler flow probe or measure portal pressure by manometer) when the clamps are removed. Paracentesis with intravenous colloid replacement is the next step if medical management does not succeed. Monitor progress by weighing the patient daily, measuring urine volume and checking for electrolyte imbalances, azotaemia and encephalopathy. This involves placement of a tube extending from the peritoneal cavity to the jugular vein through a subcutaneous track in the anterior chest wall. A peritoneovenous shunt is indicated only in cirrhotic patients with intractable ascites unresponsive to medical therapy. Contraindications include very poor liver function with encephalopathy, infected ascites, coagulopathy and cardiac failure. Complications are common with peritoneovenous shunts, and include shunt blockage, infection, thrombocytopenia and, occasionally, disseminated intravascular coagulation. Closure 1 n Close 2 n For the abdominal wall in a standard manner, without drainage. To anticipate and manage this: n Manage the patient initially in the intensive care unit with help from an expert medical hepatologist n Maintain accurate fluid balance and correct abnormal clotting n Take steps to prevent or control hepatic encephalopathy. In consultation with the hepatologist prescribe twice-daily phosphate enemas to keep the colon empty, and oral lactulose or lactitol when gastrointestinal activity returns, at a dose producing one or two soft motions a day. Restrict protein intake, starting at 20 g/day and increasing by 10 g every second day. Haemorrhage is the most common reason for conversion, followed by difficulty in mobilizing the spleen due to adhesions or spleen size and injury to adjacent organs. Appraisal n 2 n Elective splenectomy is most commonly carried out for idio- 1 the spleen is an important organ, with both haematological and immunological functions. Its haematological functions include the storage, maturation and destruction of red blood cells. Immunologically it produces peptides necessary for the phagocytosis of encapsulated bacteria (Streptococcus pneumonia, Neisseria meningitidis and Haemophilus influenza). It is a site of antibody synthesis and may be a reservoir for monocytes that are mobilized following tissue injury. When possible, conserve at least part of the spleen, as opposed to total splenectomy. Splenectomy is also required occasionally for other types of splenomegaly with hypersplenism and rarely for conditions such as cyst, abscess, haemangioma or splenic artery aneurysm. Splenectomy is sometimes carried out as a part of other operations, such as total gastrectomy and distal pancreatectomy. Classically, patients are shocked, with pain in the left hypochondrium and shouldertip and evidence of left lower rib fractures. Urgent laparotomy is required to control bleeding if the patient remains unstable after initial resuscitation. Lesser splenic injuries can be managed conservatively with vigilant clinical observation and blood transfusion. Massive splenomegaly presents difficulties in access, vision and manoeuvring the spleen. Identification of accessory splenic tissue may be less thorough than in open surgery but the long-term results are same. Obesity, peritoneal adhesions and the presence of inflammation also add to the difficulties. Long-term follow-up 11 n Preoperative splenic artery embolization may reduce the risk hemicolectomy, was formerly an indication for splenectomy, but the bleeding can usually be controlled by lesser means. This percutaneous radiological technique has been described in conjunction with open splenectomy, primarily in cases of massive splenomegaly. Other advantages of embolization include reduced splenic volume and avoidance of the risk of arteriovenous fistula from stapling across the splenic hilum. Embolization is most frequently performed on the day of surgery to reduce the discomfort associated with splenic ischaemia and infectious complications.
Purchase imipramine without prescription
Coffee ground vomiting suggests a slowly bleeding lesion anxiety symptoms vs heart attack symptoms purchase imipramine on line amex, whereas fresh blood suggests a peptic ulcer that is bleeding at a rapid rate. Action 1 n If the patient is unstable despite resuscitation or requires transfusions to maintain a normal blood pressure, undertake an urgent endoscopy in the operating theatre. If you can identify the bleeding point and have the appropriate expertise, use injection of adrenaline, diathermy or clips to control it. If a bleeding peptic ulcer is unresponsive to endoscopic measures, proceed to emergency laparotomy. Identify the bleeding point, control it with a finger or a swab on a sponge holder and aspirate the remaining blood from the surgical field. Re-insert the nasogastric tube if the patient vomits or abdominal distension recurs. If the patient is bleeding profusely resuscitate aggressively, initially with crystalloid fluids, but give blood transfusion in patients who have lost more than 30% of their circulating volume. If a bleeding ulcer does not respond to radiological or endoscopic measures, open the stomach along the greater curvature, identify the bleeding point and under-run it as for a duodenal ulcer. If you suspect malignancy perform a sleeve resection of the ulcer-bearing area and close the defect as for a gastrotomy. Erosive bleeding which fails to respond to conservative measures requires gastrectomy (partial or total as the situation demands). Bleeding from the lower bowel may be altered or fresh and is usually due to diverticular disease (see Table 4. Classify them in to upper or lower intestinal bleeding; further classify those with upper gastrointestinal bleeding in to variceal and nonvariceal bleeding. Be willing to carry out on-table enteroscopy; if this is unavailable, create a transverse colostomy and perform on-table irrigation of the colon to determine whether the bleeding is right or left-sided. Inspect the wound, looking for redness and swelling and gently palpate for tenderness. If in doubt, insert a needle and syringe through the scar and aspirate for haematoma, seroma or pus. If this demon- altered blood in the bowel lumen absorbs light, resulting in poor visualization, and has not been shown to confer any survival benefit. However, whenever clinical findings and investigations are in opposition, trust your clinical judgement. If you suspect a catastrophe do not put off the decision to re-operate by ordering unnecessary investigations. Assess 1 n Note any gas, blood or other fluid, and take a specimen for mi- n croscopy and culture. Manage con- 3 n Remember your objective and aim is to carry out the simplest 4 n If the patient does not recover satisfactorily, will you wish that 2 Expose the site of the previous operation and look for bleeding, anastomotic dehiscence, infection or ischaemia. This allows time for the cause to be investigated and the nutritional status of the patient to be corrected. Provided the fistula output continues to reduce do not rush in to operative management. You may feel that since you performed the first operation it is your responsibility to correct whatever has gone wrong. Your primary responsibility is to ensure that the patient has the best chance of recovery. Action 1 n If you are re-operating for bleeding, scoop out any blood clot and wash out the abdomen with large quantities of warmed normal saline. Early detection of continuing primary or reactionary haemorrhage may be difficult as the vital signs vary during the immediate postoperative period for a variety of reasons including pain, analgesia and vascular dilatation as the patient is warmed. Repair gastro-duodenal perforations using an omental patch; exteriorize or defunction injured small or large-bowel. If you find a localized abscess and this is compatible with the clinical picture, drain the sepsis and avoid further exploration, which may spread the infection more widely. It is sometimes possible to repair a limited leak, but more usually it is necessary to refashion the anastomosis after resecting devitalized tissue and carrying out further mobilization to avoid tension. When refashioning a gastrointestinal anastomosis ensure that there is no distal obstruction. If you cannot exteriorize, resect or bypass the leak, reduce the inflow by proximal aspiration or a stoma, insert a sump drain near the defect and commence gentle continuous suction. A bypass procedure may help to protect a re-anastomosis, for example gastrojejunostomy following repair of a duodenal leak. Alternatively, wear 2 n After cleansing the skin, gently separate the wound edges and remove the deep sutures. Treat 6 n Evacuate any residual blood, pus or other intra-abdominal fluid and provide adequate drainage to the operation site. Like burst abdomens, re-opened wounds seldom break down completely, though superficial dehiscence may complicate infection. A surgical safety checklist to reduce morbidity and mortality in a global population. Adhesion-related hospital re-admission after abdominal and pelvic surgery: a retrospective cohort study. Role of abdominal drains in perforated duodenal ulcer patients: a prospective controlled Study. Current practice of abdominal wall closure in elective surgery - is there any consensus Effect of stitch length on wound complications after closure of midline incisions. Comparison of sutured versus nonsutured subcutaneous fat tissue in abdominal surgery. Challenges in complex ventral hernia repair: examining the role of specialized techniques and mesh materials. Abdominal wall reconstruction using biological tissue grafts: present status and future opportunities. Temporary closure of the open abdomen: a systematic review on delayed primary fascial closure in patients with an open abdomen. A novel regenerative tissue matrix technology for connective tissue reconstruction. Supplement to wounds: a compendium of clinical research and practice, October 2005. Component separation method for closure of abdominal wall defects: an anatomic and clinical study. On-table colonic irrigation in the treatment of left-sided large-bowel emergencies. A meta-analysis of selective versus routine nasogastric decompression after elective laparotomy. Urgent colonoscopy for evaluation and management of acute lower gastrointestinal hemorrhage: a randomized controlled trial. Explain the benefits of laparoscopic surgery, which include; small scars, quicker recovery and a reduction in post-operative pain. Most anaesthetists avoid premedication in patients admitted on the day of surgery. Patients undergoing major laparoscopic procedures may still need opiates, albeit in reduced dosage. Their requirements may be further reduced by the use of intraperitoneal local anaesthesia or abdominal wall nerve blocks. Almost all general surgical procedures can be performed with minimal access techniques. Consumables are particularly expensive and re-usage of disposable equipment is inadvisable. Theatre times are increased initially, although they decrease as surgeons gain experience.
Order generic imipramine canada
Avoid fogging by warming the laparoscope: use a thermos of warm sterile water or other proprietary system anxiety grounding imipramine 50 mg without a prescription. Rehearse a routine with the camera holder for efficient cleaning of a contaminated lens, such as washing in warm water followed by a wipe with a dry swab. Left hand port Right hand port Camera port 3 n Camera Holder: the surgeon stands behind the telescope. The General anaesthesia is usually augmented with muscle relaxation, intubation and ventilation so that a pneumoperitoneum can be induced without causing cardiorespiratory embarrassment. Abdominal distension affects venous return, heart rate and consequently blood pressure. A profound bradycardia is not uncommon even in fit individuals, particularly on induction of the pneumoperitoneum. Abdominal distension also affects chest-wall compliance and the ease with which patients can be ventilated. Aim to use the lowest pre-set intra-abdominal pressure compatible with adequate surgical exposure. The ergonomics of this arrangement are sometimes better facilitated if the camera holder is seated on a stool next to the Surgeon. Once the first port is established you can introduce additional ports under direct vision and with relative safety. There are open and closed methods of producing a pneumoperitoneum: n the open (Hasson) method of port insertion is safer, especially if there has been previous surgery. Observe the transverse fibres of the linear alba at the base of the umbilical ligament. Incise the linea alba at this point between two stay sutures and open the peritoneum under direct vision. The stay sutures can be tied together to close the port site at the end of the procedure, by using a box stitch. If you have difficulty locating the linea alba in an obese patient, evert the base of the umbilical ligament upwards, using a clip. Insert a finger to sweep away any adhesions around the insertion site before introducing a blunttipped trocar. The main disadvantage of this method is the increased incidence of gas leaks around the port. When the Access 1 n Patient positioning: Patients are placed in a supine position with the legs either abducted (allowing the surgeon to operate from between the legs, for example in a hepatectomy) or elevated in stirrups (for access to the pelvis), or in the lateral decubitus position (access to the retroperitoneum when performing a nephrectomy). All pressure points must be adequately padded to prevent neuropathies and skin damage and strapping may be used to stabilise the patient especially when the table is tilted. The arms are usually tucked to the sides to allow ease of movement of the surgeon as she lines up instruments with target tissue. Blind introduction risks injury to underlying viscera (bowel, bladder) or even deeper structures (aorta, vena cava). Insert a 10-mm trocar and cannula, aiming the tip anterior to the sacral promontory, parallel to the aorta. Use a drilling action from the wrist while lifting up the abdominal wall below the insertion site. This will confirm appropriate intraperitoneal needle placement B Stay suture inserted on each side Linea alba incised vertically between the stay sutures If there has been too much gas introduced in to the abdomen, let some gas out via one of the ports 5. Following previous surgery, particularly through a vertical midline incision, avoid the umbilical region. Use a modified Hasson technique to access the peritoneum, by performing a cutdown through the various layers of the abdominal wall through a small laterally placed skin incision. The first is as the tip perforates musculature, then as it perforates the peritoneum. When you expect multiple intraperitoneal adhesions consider using the laparoscope to provide visual passage of the tip of the trocar though abdominal wall structures. Effect this by using a hollow trocar to accommodate the laparoscope and a seethrough blunt plastic tip. If burning does not directly cause a perforation, it may lead to necrosis and perforation at a later date. Prior to incision until the pre-set pressure is achieved, then insert the warmed laparoscope. Inspect the abdomen immediately below the first port to identify structures that could have been damaged. Perform a general laparoscopy looking for any expected or unexpected pathology (see below). The inspection helps general orientation as well as the identification of safe sites for additional ports. Instruct the assistant to follow the tip of each trocar carefully to detect potential visceral damage. In more obese individuals these additional ports often need be passed obliquely through the abdominal wall, so lying in the direction in which they are most useful during the procedure. The result is poor function at the active electrode and an unnoticed burn from the second instrument. Assess 1 n Upper abdomen: Now survey the abdomen prior to performing the intended procedure. In the right upper quadrant visualize the liver, gallbladder and the underside of the right hemidiaphragm. Now manipulate the laparoscope under the ligamentum teres to look at the left lobe of the liver and the spleen. Inspect both the left and right paracolic gutters, facilitating the exposure by inserting an atraumatic grasper to manipulate the bowel if necessary. Insert an atraumatic grasper to manoeuvre the bowel while you examine it from distal to proximal. While the patient is in the head-down position, examine the pelvis; this is especially important in female patients presenting with lower abdominal pain of unknown cause. This may lead to inadvertent heating of other structures, for example heat injury at laparoscopic cholecystectomy can lead to a late stricture of the common bile duct. During laparoscopy a capacitor may be formed inadvertently so current induced in a metal port then flows in to neighbouring bowel and causes a burn. If you are using a metal port ensure that it makes good contact with the abdominal wall. Dissecting technique 1 n Challenges: As in open surgery a safe and effective approach to tissue dissection is crucial to patient outcome. In the main these relate to a loss of tactile feedback from tissues and instruments, challenges in exposure/retraction and difficulties in maintaining haemostasis. The area of interest becomes obscured by blood and the image darkens because of light absorption by blood. The most common diathermy injury (monopolar and bipolar) results from misidentification and a burn to the wrong structure. Remember that the body wall acts as a fulcrum and forces applied at the hand piece are modified as they are transmitted to tissues at the tip. There are a range of purpose built, mainly disposable instruments, that now enable you to develop tissue planes and transect structures without the penalty of major delays in maintaining haemostasis. The choice of any particular combination depends on the specific procedure, personal preference, instrument availability and cost as follows: 2 n Inadvertent activation: Inadvertent activation of the diathermy n 62 pedal risks damaging other structures in the abdominal cavity, especially when the electrode is outside the field of view. This is the classic combination for laparoscopic cholecystectomy, while occasionally exchanging the hook diathermy for a dissector. This is a low-cost combination and it can be remarkably effective for some of the simpler procedures such as appendicectomy and adhesiolysis. The bipolar forceps act both as atraumatic graspers and diathermy for small vessels. Ultrasonic shears require a separate generator and are manufactured as a disposable item by a number of companies. It is easy to become overconfident with the instrument as it is so effective at rapidly transecting tissue and leaving behind an avascular plane. In particular, avoid haste when using the ultrasonic shears and tissue sensing bipolar diathermy.
75mg imipramine visa
Anti-cysticercal therapy is contraindicated for spinal or ocular disease as drug induced inflammation may produce irreversible organ damage symptoms 9f anxiety buy imipramine 25mg line. These lesions, as well as those within the ventricular system, are best managed surgically. Additionally, other diseases may present with symptoms attributed to the gastro intestinal tract. Appropriate evaluation requires an assess ment of symptoms and signs, listing differential diagnosis and planning investigations in order of least to most invasive. Investigations the chief tools for evaluating gastrointestinal disorders are broadly classified as follows: Stool examination. Vomiting Vomiting refers to acute expulsion of gastric contents through the mouth. Regurgitation is the involuntary and effortless expulsion of small amounts of gastric contents that is not accompanied by nausea. Persistent vomiting may be complicated by dehydration, hypokalemic hypochloremic metabolic alkalosis, malnutrition and constipation. Vigorous vomiting can uncommonly result in esophageal tear (Mallory-Weiss syndrome) or rupture (Boerhaave syndrome). Vomiting is a common, but often nonspecific, symptom that may be acute, chronic or recurrent (Table 11. Short lasting vomiting with acute onset is the most common form and is often caused by viral infections. It is important to remember that children with cyclic vomiting should be evaluated during symptomatic attack before starting intravenous fluids since test results are typically non contributory during asymptomatic periods. Evaluation of a child with acute vomiting should include assessment of hydration, electrolytes, creatinine and plain X-ray abdomen (in suspected surgical causes). Promethazine and ondansetron are useful in postoperative vomiting and to abort episodes of cyclical vomiting. Ondansetron, given alone or with dexamethasone, is preferred for chemotherapy related vomiting. Some common disorders presenting with vomiting are described below: Idiopathic Hypertrophlc Pyloric Stenosls Hypertrophic pyloric stenosis is the most common surgical disorder of the gastrointestinal tract in infants. The pylorus is thickened and elongated with narrowing of its lumen due to hypertrophy of the circular muscle fibers of pylorus. While chronic vomiting is usually caused by a gastrointestinal etiology, cyclic vomiting is predominantly due to neurologic, metabolic and endocrine causes. Lesions beyond the ampulla of Vater cause bilious vomiting and those proximal to it lead to nonbilious vomiting. The classical presentation is with non bilious vomiting that gradually increases in frequency and severity to become projectile in nature. Recurrent and persistent vomi ting causes dehydration, malnutrition and hypochloremic alkalosis. As the stomach muscles contract forcibly to overcome the obstruction, a vigorous peristaltic wave can be seen to move from left hypochondrium to umbilicus, particularly on examination after feeding. Gastroesophageal reflux disease, cow milk protein allergy, antral or pyloric web are considered in patients without a palpable pyloric mass and normal ultrasound. The treatment includes rapid correction of dehydration and electrolyte abnormalities. Cyclic Vomiting this is defined as occurrence of stereotypic episodes of intense nausea and vomiting as defined previously, with complete normalcy between episodes and the absence of a metabolic, neurologic or gastrointestinal disorder. The patient should have had at least 5 episodes in all or 3 episodes during a 6-month period. A thorough history and physical examination at presentation helps identify children that require further diagnostic testing. It is also used to evaluate the efficacy of anti secretory therapy and to correlate symptoms. It is thus superior to pH monitoring alone which detects only acid reflux episodes. Cow milk protein allergy is sometimes a cause of unexplained crying and vomiting in infants. Therefore, formula-fed infants with recurrent vomiting may benefit from a 2-4 weeks trial of an exten sively hydrolyzed protein formula. Infants with inadequate weight gain because of losses by regurgitation may benefit from increasing the energy density of formula. Histological features like elongated rete pegs, basal cell layer hyperplasia and dilated intercellular spaces, alone or in combination, are suggestive of reflux esophagitis. Histamine2 receptor antagonists like ranitidine decrease acid secretion by inhibiting receptors on gastric parietal cells. The cartilaginous type occurs in distal esophagus and should be differentiated from achalasia and peptic stricture. Children with this type of congenital stenosis have high risk of perforation on endoscopic dilatation and should be treated surgically. Sometimes the ingestion is unwitnessed and the foreign body is completely asymptomatic initially, presenting days to weeks later with complications like abscess, fistula or bleed. Guidelines for management recommend that no foreign body should be left in esophagus for more than 24 hr. Children present with dysphagia, vomiting, weight loss, respiratory symptoms and slow eating whereas toddlers present with coughing and feeding aversion with failure to thrive. The onset is gradual and the average age at diagnosis in children is around 8-9 yr. The esophagus is dilated and the scope passes through the gastroesophageal junction with some gentle pressure. Botulinum toxin injection has been tried but due to short duration of action (a few months) and limited experience, it cannot be recommended as a first line of treatment in children. Diagnosis is based Dysphaga i Dysphagia refers to a sensation of food being hindered in its passage from the mouth to the stomach, i. Odynophagia is painful swallowing and globus is the sensation of a lump in the throat. Dysphagia can be divided in to two distinct groups: Oropharyngeal or transfer dysphagia. Presence of drooling, choking, coughing and nasal regurgitation suggests oropharyngeal dysphagia. Disorders involving chewing, oral transfer or pharyngeal phase of swallowing cause this. The main causes are cerebral palsy, bulbar poliomyelitis, muscular dystrophy, brainstem tumors and neuropathy. Etiology of esophageal dysphagia can be broadly divided in to two groups: motor causes. Differential Diagnosis and Evaluation the important causes of dysphagia and their evaluation are shown in Table 11. This may be of three types: web or diaphragm, fibromuscular stenosis and stenosis due to cartilaginous tracheobronchial remnants. Eosino philic esophagitis in children and adults: a systematic review and con sensus recommendations for diagnosis and treatment. It is increasingly being recognized as a very common problem in children and is associated with both physical and psychological morbidity and a poor quality of life. The normal stool frequency decreases from 4 or more per day during infancy to once per day at 4 yr of age. Treatment options include the use of elemental formula, elimination diets, or topical corticosteroids. Resolution of the condition with food elimination diets provides evidence that it is a food-antigen driven process. A detailed history and physical examination is the most useful tool for making a diagnosis of constipation. A predominantly liquid and low fiber diet (milk based) is common and contributes to constipation. Examination for features of spina bifida (pigmentation or tuft of hair on lower back), power in lower limbs, perianal sensation, voluntary contraction and tone of anal sphincter and amount and consistency of stool in rectum on per rectal examination are extremely useful for diagnosis. Functional Constipation the increase in intake of low residue diet and sedentary lifestyle is responsible for the increase in functional consti pation in children.
