
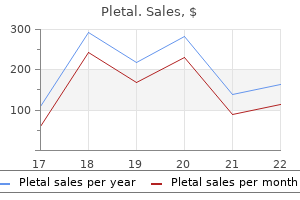
Pletal 100mg with visa
Vasopressive agents are most commonly used in patients where fluid resuscitation is inadequate to restore blood pressure muscle spasms 72885 order pletal online from canada. The 1-adrenoceptor-mediated effects in the heart result in an increase in cardiac output with minimal peripheral vasoconstriction. Specific dopamine receptors in the vasculature of the renal, coronary, and splanchnic systems allow for reduced arterial resistance and increased blood flow. At higher doses, there is a peripheral -adrenoceptor effect that overrides dopamine receptor-mediated vasodilation and results in vasoconstriction. The combination of renal blood-flow preservation, while supporting the blood pressure, is desirable in conditions of shock. Prolonged high doses of dopamine can result in peripheral tissue necrosis because of the -adrenoceptor-mediated vasoconstriction that reduces blood flow to the extremities, particularly in the digits. Receptor selectivity: Preferential binding (greater affinity) of a drug to a specific receptor group or receptor subtype at concentrations below which there is little, if any, interaction with another receptor group or subtype. Some are nonselective (eg, ephedrine), whereas some have greater affinity for -adrenoceptors (eg, phenylephrine, metaraminol, methoxamine) or 1-adrenoceptor (eg, dobutamine) or 2-adrenoceptor (eg, terbutaline, albuterol) subgroups. However, selectivity is often lost as the dose of a sympathomimetic agent is increased. Compared to nonselective -receptor agonists (isoproterenol), a 1-selective sympathomimetic agents may increase cardiac output with minimal reflex tachycardia. The clinical utility of a particular sympathomimetic agent depends, among other factors, on the specific organ system and receptor subtypes that are involved. In the cardiovascular system, a reduction in blood flow by relatively selective -adrenoceptor sympathomimetic agents is used to achieve surgical hemostasis (epihephrine), reduced diffusion of local anesthetics (epinephrine), and a reduction of mucous membrane congestion in hay fever and for the common cold (ephedrine, phenylephrine). Sympathomimetic agents such as epinephrine are also used for emergency short-term treatment of complete heart block and cardiac arrest. Treatment of bronchial asthma represents a major use of a2-selective sympathomimetic agents (eg, terbutaline, albuterol). Its effect is bronchodilation and relaxation of the smooth muscles of the bronchioles. Ophthalmic examination is facilitated with the use of the directly acting -adrenoceptor sympathomimetic agonist, phenylephrine. Apraclonidine (and the indirectly acting sympathomimetic agent, cocaine) is used to confirm the diagnosis of Horner syndrome. In addition to -adrenoceptor-blocking agents, 2-selective agents (eg, apraclonidine, brimonidine) are used to lower intraocular pressure in glaucoma. The peripheral adverse effects of the sympathomimetic agents are generally an extension of their pharmacologic effects. These are most often cardiovascular in nature, particularly when they are administered parenterally, and may include increased blood pressure, arrhythmias, and cardiac failure. Structure Sympathomimetic agents, as well as norepinephrine and epinephrine, are derived from phenylethylamine. Substitutions on the amino group, the benzene ring or the - or -carbon, markedly alter the selectivity, activity, and metabolism of the sympathomimetic agents. For example, alkyl substitutions on the amino group tend to markedly increase -adrenoceptor selectivity. Indirectly acting sympathomimetic agents mimic the actions of norepinephrine by either displacing it or inhibiting its reuptake from adrenergic nerve endings. Administration Sympathomimetic agents are available for administration by topical, nasal, oral, ophthalmic, and parenteral routes depending on the drug and condition being treated. Norepinephrine increases blood pressure by causing peripheral vasoconstriction by acting on 1-adrenoreceptors. Terbutaline and albuterol are preferred over ephedrine for relieving the bronchoconstriction of asthma, and other bronchial conditions, because of their greater bronchiolar selectivity. Use of long-acting beta-agonists and inhaled steroids in asthma: meta-analysis of observational studies. Molecular mechanisms of beta(2)-adrenergic receptor function, response, and regulation. Both the nonselective -adrenoreceptor antagonists and the 1-adrenoceptor selective antagonists are used to treat hypertension. Contrast the differences between the nonselective and relatively 1-selective adrenoceptor antagonists. Phentolamine, a nonselective, competitive -adrenoceptor antagonist, and phenoxybenzamine, a nonselective, noncompetitive -adrenoceptor antagonist, are used for the preoperative management of the marked catecholamine-induced vasoconstriction associated with pheochromocytoma. Prazosin and other 1-adrenoceptor selective antagonists (doxazosin, terazosin) are used to manage chronic mild-to-moderate hypertension and benign prostatic hypertrophy. Ischemic heart disease is managed with nonselective -adrenoceptor antagonists, propranolol, timolol, and nadolol, as well as 1-adrenoceptor selective antagonists, metoprolol, atenolol, bisoprolol, nebivolol, and esmolol. Cardiac arrhythmias are managed, depending on the arrhythmia, with propranolol and esmolol. Timolol and other -adrenoceptor antagonists are used to manage glaucoma by decreasing aqueous humor production and thereby reducing intraocular pressure. Labetalol (and several other agents, including carvedilol), in formulations used clinically, blocks both - and 1-adrenoceptors in a 3:1 ratio. Labetalol lowers blood pressure by decreasing systemic vascular resistance without any major effect on heart rate or cardiac output. It is used to treat hypertensive emergencies and hypertension from pheochromocytoma. The major adverse effects of nonselective -adrenoceptor antagonists are cardiac stimulation, primarily tachycardia because of baroreflex-mediated sympathetic discharge, and postural hypotension. Additional cardiac stimulation by phentolamine may be caused by antagonist activity at presynaptic 2-adrenoceptors that result in increased norepinephrine release. The major adverse effects of nonselective -adrenoceptor antagonists are related to their effects on smooth muscle, carbohydrate metabolism. In patients, with insulin-dependent diabetes, nonselective -adrenoceptor antagonists increase the incidence and severity of hypoglycemic episodes. The use of selective 1-adrenoceptor antagonists in patients with this condition offers some potential benefits. The latter effect is particularly prevalent with the nonselective -adrenoreceptor antagonists. Combined - and -adrenoreceptor antagonist (labetolol) or -adrenoreceptor antagonists with sympathomimetic activity (acebutolol or pindolol) have no effect on serum tricglycerides. Mechanism of Action -Adrenoceptor antagonists and -adrenoceptor antagonists interact directly, and either competitively or irreversibly with, respectively, -adrenoceptors and -adrenoceptors to block actions of the endogenous catecholamines (norepinephrine and epinephrine), and exogenously administered sympathomimetic agents. Antagonists of this receptor will therefore promote smooth muscle relaxation; in blood vessels, where these receptors are largely expressed, this leads to dilation. In the heart, activation of 1-receptors causes an increase in the force of contraction of cardiac muscle and an increase in heart rate. Administration - and -adrenoceptor antagonists are administered orally or parenterally. Esmolol is ultra-short-acting as a result of its ester linkage that is rapidly metabolized by plasma esterases. The effect on the cardiovascular system is a result of its action as an antagonist at which of the following Prazosin is an -adrenoceptor antagonist that will block epinephrinemediated contraction of the radial smooth muscle of the eye that results in mydriasis. All the other actions listed are mediated by -adrenoceptors, which would be blocked by -adrenoceptor antagonists like propranolol. It lowers blood pressure by decreasing systemic vascular resistance (-adrenoceptor antagonist activity), without any major effect on heart rate or cardiac output (-adrenoceptor antagonist activity). Beta blockers, especially at higher doses, will cause erectile dysfunction and hence it would not be ideal in this patient. Beta blockers have proven to reduce morbidity and mortality in patients with systolic, diastolic, and mixed dysfunction heart failure as well as in those with coronary artery disease. It also is very effective in controlling the symptoms of tachycardia and tremors in Grave disease. The major clinical uses for -adrenoceptor antagonists include ischemic heart disease, cardiac arrhythmias, hypertension, hyperthyroidism, and glaucoma. The major adverse effects of nonselective a-adrenoceptor antagonists are related to their effects on bronchial smooth muscle (increased airway resistance in asthmatics) and on carbohydrate metabolism (hypoglycemia in insulin-dependent diabetics).
Sawi (Marijuana). Pletal.
- Are there any interactions with medications?
- Are there safety concerns?
- How does Marijuana work?
- Treating multiple sclerosis (MS).
- Treating increased pressure in the eyes (glaucoma).
- Stimulating appetite in people with AIDS.
- What is Marijuana?
- Dandruff, hemorrhoids, obesity, asthma, urinary infections, leprosy, preventing rejection after kidney transplants, and other conditions.
- Dosing considerations for Marijuana.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96910
Generic 100 mg pletal with amex
Toxins and drugs (see Table 23) are common causes acting here spasms around the heart discount pletal 50mg amex, as are pellagra and other vitamin deficiencies and food allergies. Systemic autoimmune diseases such as scleroderma and Whipple disease are also important. Mesenteric artery insufficiency or obstruction should be considered both here and in the colon. I-Infectious agents such as bacillary dysentery (Shigella), Escherichia coli, Campylobacter, Yersinia, and amebiasis may ulcerate or inflame the colon. N-Neoplasms such as carcinomas and polyps cause chronic irritation and exudates from the colon with hypermotility and diarrhea. D-Degenerative lesions of the muscularis that cause diverticulosis and allow overgrowth of bacteria and chronic inflammation may lead to diarrhea, but this may be classified under the idiopathic category as well. I-Intoxicating substances, osmotic cathartics, and antibiotics (by allowing overgrowth of bacteria and fungi) may involve the colon. C-Congenital lesions of the colon include the solitary diverticulum of the cecum, malrotation (more frequently associated with intestinal obstruction), and familial polyposis. A-Autoimmune disease of the colon is common and includes both ulcerative colitis and granulomatous colitis. Table 22 Diarrhea-Anatomic Classification T-Trauma is not a common cause of diarrhea anywhere in the intestinal tract, but certainly surgically induced fistulas may occur in the colon or anywhere else. Having considered the local causes of diarrhea, do not forget reflex diarrhea from diseases of other organs, such as pyelonephritis, salpingooophoritis, and central nervous system diseases. Using Table 23, the reader can develop the differential diagnosis of diarrhea with physiology. Approach to the Diagnosis If possible stop all drugs that may be the cause immediately. Whichever method is applied (anatomic or physiologic), most causes of diarrhea can be recalled before interviewing the patient. Then one can proceed to ask the right questions to eliminate each suspected cause. Combinations of symptoms and signs will assist greatly in narrowing the differential diagnosis. For example, chronic diarrhea and copious mucus without blood suggests irritable bowel syndrome. Physical examination is often unrewarding but it may disclose a hepatic, rectal, or pelvic source for the diarrhea; it may also indicate that the diarrhea is a sign of a systemic disease. A warm stool examination for pus, pH (acid stool suggests lactase deficiency), fat and meat fibers, blood, ova, and parasites is most essential. He had also noted frequent indigestion and heartburn and occasional midepigastric pain. Utilizing the methods provided above, what is your list of possibilities at this point Further history reveals that he has had occasional black stools and does not abuse alcohol or drugs. His physical examination is unremarkable, but stools test positive for occult blood. Mechanical obstruction may result from intrinsic disease of the pharynx, larynx, and esophagus or extrinsic disease of the organs around the esophagus. I-Inflammatory should suggest pharyngitis, tonsillitis, esophagitis, and mediastinitis. N-Neoplasm should bring to mind esophageal and bronchogenic carcinoma, and dermoid cysts of the mediastinum. C-Congenital and acquired anomalies should suggest esophageal atresia and diverticula. T-Trauma would prompt the recall of ruptured esophagus, pulsion diverticulum, and foreign bodies that obstruct or injure the wall of the esophagus. Table 23 Diarrhea-Physiologic Classification E-Endocrine disorders suggest the enlarged thyroid of endemic goiter and Graves disease. Physiologic obstruction results from neuromuscular disorders at the end organ, myoneural junction, and lower and upper motor neurons. End organ: this should suggest myotonic dystrophy, dermatomyositis, achalasia, and diffuse esophageal spasm. Lower motor neuron: In this category one would recall poliomyelitis, diphtheritic polyneuritis, and brainstem tumors or 272 infarctions. It should also bring to mind Parkinson disease and other extrapyramidal disorders. Approach to the Diagnosis the age of onset is significant because carcinoma of the esophagus is rare before age 50, whereas achalasia and reflux esophagitis are more common in young and middle-aged adults. The onset is gradual in carcinoma and aortic aneurysms but more acute in reflux esophagitis and foreign bodies. Patients with achalasia have trouble swallowing both food and water, but those with carcinoma suffer the most, and often the only difficulty is swallowing food. Neurologic findings will focus on the diagnosis of bulbar and pseudobulbar palsy whereas hematemesis and heartburn will suggest esophageal carcinoma or reflux esophagitis. However, esophagoscopy and biopsy will lead to a definitive diagnosis in most cases of mechanical obstruction. If esophagoscopy is negative, one may resort to a Mecholyl test to diagnose achalasia, a Tensilon test to exclude myasthenia gravis, and esophageal manometry to diagnose reflux esophagitis, scleroderma, and diffuse esophageal spasm. Difficulty urinating must be distinguished from dysuria (page 148), which is painful urination, and anuria or oliguria (page 60), which is absent or reduced volume of urine. If we then visualize the urinary tree from the prepuce on up to the bladder, we can visualize the causes of obstruction at each level. Prepuce-Phimosis and paraphimosis Meatus-Meatal stricture Urethral-Urethral stricture, urethral calculus Prostate-Prostatitis, prostatic hypertrophy, prostatic carcinoma, prostatic calculus Bladder-Bladder neck obstruction due to stricture, median bar hypertrophy, calculus or neoplasm Extrinsic lesions of the bladder or urethra-Uterine fibroids, pregnant retroverted uterus, or carcinoma of the vagina Lesions of the innervation of the bladder wall-This may be due to lower motor neuron disorders such as poliomyelitis, cauda equina tumors, or disks; tabes dorsalis; or diabetic neuropathy. Approach to the Diagnosis the first thing to do is to establish that there is an obstruction to the flow of urine. This may now be done with ultrasonography, but catheterization may still be done in the acute situation. Difficulty voiding in a young person will most likely point to a urethral stricture or prostatitis from previous gonorrhea or urethral injury, whereas difficulty voiding in an older man would suggest prostatic hypertrophy. A history of hematuria would suggest the possibility of a vesicle or urethral calculus. A complete physical including a rectal and pelvic examination (in women) is done next. If these tests are negative, an urologist needs to be consulted for cystoscopy and cystometric testing. A dilated pupil, however, may also signify a lesion of the optic nerve and its pathways. Lesions of the oculomotor nerve and pathways End organ: Lesions of the eye that cause dilated pupils include glaucoma, high myopia, anticholinergic drugs. Peripheral portion of the oculomotor nerve: Important lesions here include aneurysms of the internal carotid artery and its branches; herniation of the brain in brain tumors, subdural hematomas, and other space-occupying lesions; cavernous sinus thrombosis; sellar and suprasellar tumors; tuberculosis and syphilitic meningitis; and sphenoid ridge meningiomas. Diabetic neuropathy of the third cranial nerve does not usually 275 cause mydriasis. Most of these lesions are associated with ptosis and paralysis of the other extraocular muscles supplied by the oculomotor nerve. Barbiturates and other drugs may cause dilated pupils by their central nervous system effects. Optic nerve and pathways End organ: Keratitis, cataracts, retinitis, and occlusion of the ophthalmic artery are included here. Peripheral portion of the optic nerve: Aneurysms; optic neuritis; sellar and suprasellar tumors; optic nerve gliomas; primary optic atrophy from lues and other conditions; orbital fractures; exophthalmos; and cavernous sinus thrombosis are recalled in this category. Brainstem: the lesions involving the optic tract here are similar to those that involve the oculomotor nerve discussed above.
Buy pletal 100 mg cheap
I-Inflammatory diseases include the most common causes of sore throat spasms right side abdomen buy cheapest pletal and pletal, streptococcal or viral pharyngitis, but one must also consider the less frequent infectious diseases here. Next, bacterial causes such as group A hemolytic Streptococcus (with or without scarlet fever), diphtheria, Listeria monocytogenes, and meningococcemia should be considered. Tuberculosis should also be mentioned, although it is rare in contemporary affluent societies. Consider among bacterial causes sinusitis, tonsillar or peritonsillar abscess (quinsy), and retropharyngeal abscess: Staphylococcus organisms may cause these, but they rarely cause the common sore throat. Moving to the next largest organisms, the spirochetes, think of syphilis and Vincent angina. D-Degenerative diseases are an unlikely cause of sore throat, just as they are unlikely to cause pain anywhere. Agranulocytosis may also be included in this category, because it is so often drug induced. C-Congenital diseases are an infrequent cause of sore throat, but a hiatal hernia with reflux esophagitis may cause recurrent sore throat, because there may be reflux of gastric juice all the way to the posterior pharynx in the recumbent position. A-Allergic diseases include angioneurotic edema of the pharynx or uvula and allergic rhinitis; otherwise, this category is a rare cause of sore throat. E-Endocrine causes of sore throat should remind one of subacute thyroiditis; although the pain is really in the neck, the patient will report a "sore throat. In resistant cases, repeated cultures (especially for diphtheria, gonorrhea, and Listeria organisms) and a monospot test will be useful. Case Presentation #80 A 16-year-old black girl presents to your office with a sore throat. Examination reveals exudative tonsillitis and enlarged anterior cervical lymph nodes. The patient is given a course of penicillin, but 1 week later she returns to the office with no improvement. In addition to the previous findings, there is now splenomegaly and posterior cervical lymphadenopathy. Knowledge of neuroanatomy is extremely useful in developing a differential diagnosis. Spinal cord: this prompts the recall of space-occupying lesions of the spinal cord, amyotrophic lateral sclerosis, Friedreich ataxia, transverse myelitis, neurosyphilis, multiple sclerosis, and anterior spinal artery occlusion. Cerebral hemispheres: Once again, space-occupying lesions are important to recall but hemorrhage, embolism, and thrombosis are also prominent causes. In children it is wise to consider cerebral palsy, encephalitis, and Schilder disease. There are many degenerative disorders of the cerebrum that eventually develop spasticity, but the diagnosis will be well established by that time. Multiple sclerosis that predominantly involves the cerebral cortex also is unlikely to cause spasticity until late in the course of the disease. Miscellaneous: Stiff man syndrome is associated with stiffness of the muscles of the neck, trunk, and extremities. A spinal tap will be useful in establishing the diagnosis of multiple sclerosis, encephalitis, and neurosyphilis if a space-occupying lesion has been ruled out. V-Vascular disorders suggest a large aortic aneurysm that may damage 756 the vertebrae by compression, but this category is used with the prime purpose of recalling the spinal deformities associated with various congenital heart diseases. I-Inflammatory disorders recall osteomyelitis and tuberculosis of the spine; one should also remember infectious diseases of the nervous system such as poliomyelitis. N-Neoplasms include metastatic tumors, myeloma, Hodgkin lymphoma, and primary tumors of the spinal cord. D-Degenerative and deficiency diseases include degenerative disk disease, osteoarthritis, and spondylosis along the spine. In this category should be mentioned the kyphosis associated with pulmonary emphysema and fibrosis. I-Intoxication includes kyphosis associated with pneumoconiosis and osteoporosis from menopause or long-term corticosteroid therapy. C-Congenital disorders are perhaps the largest category, including congenital scoliosis, kyphoscoliosis, Hurler disease, hemivertebra, muscular dystrophy, Friedreich ataxia, achondroplasia, and spondylolisthesis. A-Autoimmune disease suggests rheumatoid spondylitis with the characteristic "poker spine. E-Endocrine diseases remind one of the kyphosis associated with menopausal osteoporosis and osteomalacia of hyperparathyroidism. Approach to the Diagnosis Obviously, a good family history and a thorough physical and neurologic examination are essential. The busy physician who does not have the time to perform a neurologic examination should refer the patient to a neurologist or orthopedist. The bone scan has become especially useful in diagnosing early rheumatoid spondylitis. The mass has a hard, smooth surface with a notch on the edge and descends on inspiration. Think about the histologic components: parenchyma, supporting tissue, arteries, veins, and a capsule. It is nothing more than the components of the blood: red cells, white cells, lymph tissue, and platelets. Increased numbers of red cells recall polycythemia; increased numbers of white cells recall leukemia and infection. Increased lymph tissue suggests Hodgkin lymphoma, whereas increased supporting tissue indicates reticuloendotheliosis and acromegaly. If the artery has a local increase in size, an aneurysm forms, compressing the splenic veins. It is also able to form red cells and other components of the blood when the bone marrow is atrophied, as in extramedullary erythropoiesis. More important, it is involved in the destruction of old or damaged red cells and platelets. Extramedullary erythropoiesis recalls the splenomegaly of aplastic anemia and myeloid metaplasia, just as destruction or sequestration of cells brings to mind the splenomegaly of hemolytic anemias. The hypertrophy to fight infection or diffuse inflammation of the body should suggest the splenomegaly of bacterial endocarditis, kala azar, infectious mononucleosis, miliary tuberculosis, and rheumatoid arthritis. Only one category of splenomegaly is not brought to mind by this approach, but it is easily remembered because it is an exception- infiltration of inert material. Table 52 summarizes the above discussion and gives additional causes of splenomegaly to consider in the differential. The combination of symptoms and signs will eliminate certain causes and make others more plausible. For example, splenomegaly with jaundice but no hepatomegaly suggests hemolytic anemia. If the spleen is very large, it should suggest myeloid metaplasia, chronic myelogenous leukemia, Gaucher disease, and kala azar. If a specific disease is 760 strongly suspected, consult Appendix A for appropriate tests. A nonbloody discharge is almost invariably due to inflammation, infection, or allergy, but a few important exceptions are worth mentioning here. Many toxic substances can produce severe acute inflammation or moderate-tosevere chronic inflammation and fibrosis. Lipoid pneumonia is mentioned in most textbooks of differential diagnosis but is seldom seen. Adult respiratory distress syndrome may result from injection of heroin, shock, and septicemia. In diseases of the larynx and trachea, sputum production is usually scanty, but several viruses. In bacterial infection, the sputum is usually yellow, whereas in bronchial asthma it is white, thick, 762 and mucoid.
Generic pletal 100mg line
I-Inflammations such as ulcerative colitis with perforation muscle relaxant spray discount 100mg pletal free shipping, granulomatous colitis with perforation, amebic colitis, and ischemic colitis. Pain in the hypogastrium may also be caused by a dissecting aneurysm 115 of the aorta or phlebitis of the iliac veins or the inferior vena cava. The lumbosacral spine may be the site of pain in M-Malformations such as spondylolisthesis and scoliosis, but these are usually associated with back pain. I-Inflammatory conditions of the spine such as tuberculosis and rheumatoid spondylitis are much more likely to cause hypogastric pain. N-Neoplasms, particularly metastatic carcinoma, multiple myeloma, and Hodgkin lymphoma, may cause hypogastric pain. T-Trauma of the spine may cause a herniated disc fracture or hematoma of the spine and surrounding muscles, producing hypogastric pain from a distended bladder or paralytic ileus, among other things. The appendix and small intestine may occasionally end up in the pelvis; therefore, appendicitis and regional ileitis should not be forgotten as possible causes of hypogastric pain. Approach to the Diagnosis In cases of hypogastric pain, it is most important to do a good pelvic and rectal examination. Because the most common cause of hypogastric pain is cystitis or another urinary tract infection, it is essential to examine the urine (personally) and to do a culture sensitivity and colony count regardless of the findings on routine urinalysis. That is why a gynecologist should be consulted early if these conditions are suspected in acute cases. If a problem in the lower bowel is suspected, colonoscopy or barium enema may be necessary. Proceeding down the 117 tree to the aorta we have dissecting aneurysm, Takayasu disease, and coarctation of the aorta as prominent causes of absent or diminished pulses. A large saddle embolism at the terminal aorta may cause absent or diminished pulses in the lower extremities. Arteriosclerosis of the terminal aorta as seen in Leriche syndrome may produce a similar picture. Proceeding further down the tree to the larger arteries, we are reminded of the subclavian steal syndrome in the upper extremities and femoral artery thrombosis, embolism, or arteriosclerosis affecting the lower extremities. Extrinsic pressure from a thoracic outlet syndrome may also affect the subclavian artery. Finally reaching the peripheral arteries, we encounter peripheral arteriosclerosis, embolism, and thrombosis. These arteries also may be affected by external compression in fractures, tumors, and other masses of the extremities. An arteriovenous fistula of the extremity arteries may produce an absent or diminished pulse also. Significant anemia or dehydration may produce a diminished pulse in all extremities, but of course, this is usually associated with shock. Approach to the Diagnosis Clinically it is useful to take the blood pressure on all four extremities and do a thorough examination of the optic fundus and heart. Ultrasonography of the vessels involved is an excellent noninvasive technique for further evaluation. Arteriography of the vessel or vessels involved will ultimately be necessary in most cases. Magnetic resonance angiography is an expensive but adequate alternative in some cases when contrast arteriography is considered hazardous. This should call to mind diabetic acidosis, lactic acidosis, and starvation as diagnostic possibilities when one is faced with a patient within acidosis. Transport: If there is inadequate transport of acid to the kidney for excretion (as occurs in various forms of shock [prerenal azotemia]), acidosis may develop. Primary diseases of the kidney that may cause uremia acidosis are glomerulonephritis, collagen disease, toxic nephritis from various drugs, and end-stage renal disease from a host of causes. Chronic obstructive uropathy from renal stones, bladder neck obstruction, and congenital anomalies may also lead to uremic acidosis. Acidosis is also produced by a decrease in production of bicarbonate by the kidney or an increased excretion of bicarbonate in the intestinal tract. Consequently, one must add to the differential list renal tubular acidosis and Fanconi syndrome, which are associated with decreased production of bicarbonate while not producing uremia at the same time. In addition, diarrhea of many causes must be added to the list because it is associated with increased excretion of bicarbonate. Finally, the mechanism of regulation of bicarbonate production should bring to mind conditions with acidosis related to decreased production of bicarbonate. In Addison disease, there is little or no aldosterone hormone to induce the kidneys to produce bicarbonate; lack of this 119 hormone leads to acidosis. Approach to the Diagnosis the laboratory will be of greatest assistance in determining the cause of acidosis. An elevated blood sugar and serum acetone level will help diagnose diabetic acidosis. In addition, diseases of the bone such as osteogenic sarcoma and Paget disease may cause an elevation in acid phosphatase level. If either one or both of these are positive, an urologist should be consulted for prostate biopsy. As with other laboratory values, we need to know where alkaline phosphatase is produced, how it is transported, and how it is degraded or excreted. Alkaline phosphatase is produced in many tissues but in terms of pathophysiology, only the osteoblasts of the bone need be recalled. Thus, disorders that increase osteoblastic activity such as metastatic tumors of the bone, osteogenic sarcoma, Paget disease, and primary and secondary hyperparathyroidism may cause the alkaline phosphatase level to increase and must be considered in the differential. However, the excretion of alkaline phosphatase seems to take place in the liver by an undetermined pathway, but anything that blocks the cholangioles or biliary tree will usually cause an elevation of alkaline phosphatase. Consequently, carcinoma of the head of the pancreas, common duct stones, carcinoma of the ampulla of Vater, and drugs that produce cholestasis (such as chlorpromazine) may cause an elevated alkaline phosphatase. Metastatic carcinoma of the liver probably produces an elevated alkaline phosphatase by blocking individual cholangioles. In addition to the above diagnostic possibilities, there are disorders that cause an elevated alkaline phosphatase level by an unknown mechanism such as pregnancy, sepsis, and gynecologic malignancies that must be included in the differential. Approach to the Diagnosis If the elevated alkaline phosphatase level is related to liver disease, the clinical examination will often show jaundice or hepatomegaly. If it is related to bone disease, the clinical examination will show bone pain, pathologic fracture, or bone mass. A skeletal survey will usually reveal bony metastasis and other disorders of the bone, but a bone scan may be necessary to show early metastasis to the bone. Excessive production of bicarbonate occurs in primary or secondary aldosteronism where the hormone aldosterone induces increased bicarbonate production and excessive excretion of the hydrogen (H+) ion in exchange for sodium (Na+) reabsorption. The same mechanism occurs in exogenous steroid administration and Bartter syndrome. Excretion: this mechanism should help recall salicylate toxicity and hyperventilation as causes of alkalosis. Excessive excretion of acid also occurs in pyloric stenosis, intestinal obstruction, and other causes of excessive vomiting leading to alkalosis. Chronic antacid use, various diuretics, and Cushing disease may also induce alkalosis. Approach to the Diagnosis Taking a drug history and noting hyperventilation or vomiting during the clinical evaluation will assist in the diagnosis. Serial electrolytes, arterial blood gases, and drug screen are first-line laboratory tests to assist in the diagnosis. However, it is wise to have a systematic method of remembering the many etiologies to avoid mistakes in diagnosis. V-Vascular disorders include cerebral arteriosclerosis, hemorrhage, 126 thrombosis, embolism, and migraine. I-Inflammatory disorders include meningitis, encephalitis, cerebral abscess, malaria and other cerebral parasites, and neurosyphilis. Amnesia and delirium may be caused by high fever regardless of the cause of the fever.
Order discount pletal on-line
She is a former cigarette smoker muscle relaxant side effects discount pletal 50mg line, having a 30 pack-year history and having quit 20 years ago. She occasionally has a glass of wine with dinner and walks three or four times a week for exercise. You order a bone density test, which shows a significant reduction of density in the spine and hips. Continuous delivery, for example, as a consequence of a parathyroid tumor, results in bone resorption. Following menopause, with the resultant decrease in circulating estrogen levels, there is a relative increase in osteoclastic activity and resorption of bone, with a net loss of bone mineral density. This retards the progression of bone density loss and may allow for increases in density, because osteoblastic activity is not affected. It may produce esophagitis, and even esophageal perforation, if the pill were to get caught in the esophagus while swallowing. For that reason, patients taking alendronate are instructed to take it on an empty stomach with a full glass of water and to remain upright for at least 30 minutes after ingesting the medication. Describe the structure, synthesis, actions, and uses of vitamin D and its metabolites. Know the secondary agents that affect calcium homeostasis and their characteristics. It has diverse roles-including enzyme activation, secretion, excitation-contraction coupling in all muscle types, and neuronal function-and is a critical structural element in bone and teeth. This is the biologically active fraction, and it is maintained at approximately 2. An additional 40 percent is bound to serum proteins and the remainder is complexed to ions such as phosphate, citrate, and bicarbonate. The serum concentration of Ca2+is tightly regulated by several endocrine systems and three major tissues: the gut, kidney, and bone. Normal bone is continuously reabsorbed by the action of osteoclasts, and new bone is formed by the action of osteoblasts; if these two processes are not equal in magnitude, excess bone can be lost, as in osteoporosis, or too much bone can be formed. The third endocrine system that has effects on bone is vitamin D3 and its metabolites. Vitamin D3 is synthesized from cholesterol in the skin in a two-step photo-dependent reaction. These include calcium gluconate, calcium lactate, calcium carbonate, and calcium citrate. They vary in the percentage of calcium by weight from a low of 9 percent for calcium gluconate to a high of 40 percent for calcium carbonate. Selection of which agent to use depends on the desired onset of action, duration of effect, and the presence of underlying liver or kidney disease. Thiazide diuretics act on the kidney to increase Ca2+ reabsorption in the distal convoluted tubule and can be used in the treatment of hypocalcemia. Treatment of Hypercalcemia Hypercalcemia has a number of pathophysiologic causes including hyperparathyroidism, Paget disease, and hypercalcemia of malignancy. Bisphosphonates are analogs of pyrophosphate in which the phosphodiester (P-O-P) bond is replaced by a nonhydrolyzable bisphosphonate (P-C-P) bond. Second-generation aminobisphosphonates include risedronate, alendronate, pamidronate, tiludronate, clodronate, zoledronate, and ibandronate. The two classes of bisphosphonates have different mechanisms of action and different potencies. For example, risedronate is 1000 times more potent as an inhibitor of bone resorption than etidronate. All bisphosphonates bind to and accumulate in bone, and this provides a measure of tissue specificity. This leads to impaired posttranslational modification of a number of proteins that are critical to osteoclast function. Etidronate is available for oral use; the aminobisphosphonates may be administered orally or by infusion. Administered orally, all the bisphosphonates have very poor (approximately 5%) bioavailability, but sufficient drug is absorbed to achieve therapeutic concentrations in bone. All bisphosphonates are approved for treatment of Paget disease; alendronate, risendronate, zoledronate, and ibandronate are also approved for prevention and treatment of osteoporosis (pamidronate is approved for treatment of osteoporosis). Bisphosphonates are associated with lower esophageal erosion, and the recommendation with alendronate and risedronate is to avoid lying down for 30 minutes after oral administration to avoid reflux. There have been reports of bisphosphonate use associated with the osteonecrosis of the jaw. Although rare, this seems to occur most often in cancer patients receiving bisphosphonate therapy. Treatment of Osteoporosis Osteoporosis, loss of bone mass, affects nearly 30 percent of women aged 65 years and older and a smaller but significant percentage of men. Historically, osteoporosis has been divided into postmenopausal osteoporosis, which occurs in women and is related to the loss of ovarian hormones after menopause, and senile osteoporosis, which is age related and affects both sexes. Histologically and biochemically, they seem indistinguishable disorders of bone metabolism caused by excessive bone reabsorption or inadequate bone formation. Adequate dietary Ca2+ and vitamin D (to facilitate Ca2+ absorption) is critical in patients at risk for osteoporosis. Administered intermittently, once a day by injection, teriparatide increases bone formation in excess of resorption. This treatment has been shown to increase bone mass and decrease the incidence of fractures. Studies in rats receiving very high doses of teriparatide for 2 years demonstrated an increased frequency of osteosarcoma. Estrogens (see Case 40) have been shown to reduce the rate of bone loss in the postmenopausal period when the rate of loss can be as high as 10 percent per year. Estrogens increase bone mineral density and decrease the incidence of vertebral and nonvertebral fractures. Raloxifene is approved for the prevention and treatment of osteoporosis; tamoxifen and toremifene are used to treat breast cancer. Raloxifene is a polyhydroxylated nonsteroidal compound that binds to the estrogen receptor, but it has estrogen-agonist activity only in bone and the liver; it has no effect on the uterus, and it is an estrogen antagonist in breast tissue and in the brain. It increases bone mineral density and has been shown to decrease the incidence of vertebral and nonvertebral fractures. More serious adverse effects include an approximate threefold increase in deep vein thrombosis and pulmonary embolism. In men with nonmetastatic prostate cancer, denosumab reduced the incidence of vertebral fracture. Sodium fluoride has been examined in a number of clinical trials for the treatment of osteoporosis. Early studies using relatively high doses reported an increase in bone mineral density but no decrease in the incidence of fractures, probably because of the formation of abnormal hydroxylapatite crystals in bone. She is brought into the emergency department for near comatose state, thought to be caused by the hypercalcemia. She tried a short course of teriparitide a year ago but complained of serious depression and mood changes. Thiazide diuretics promote renal reabsorption of Ca2+; loop diuretics have the opposite effect. Bisphosphonates can lead to severe esophageal erosions; patients are advised to not lie down for 30 minutes after taking them. She indicates that she was 14 when her periods first started and that they had never really been very regular. She has mild acne on her face and shoulders and a more-thannormal amount of facial hair. There is a darkening of the skin at the base of her neck and across her shoulders. It is frequently associated with obesity and the concomitant insulin resistance and hyperinsulinemia. The excessive insulin increases production of ovarian androgens such as androstenedione and dehydroepiandrosterone, which can act peripherally and increase both sebum production and hair growth.
Discount pletal 50 mg
A combination of tricyclics in conjunction with oxybutynin may be used cautiously for a synergistic effect muscle relaxant used for migraines buy 50 mg pletal free shipping. Tolterodine, solifenacin, arifenacin, and fesoterodine are "second-generation" antimuscarinics with reduced central nervous system penetration and have better selectivity for the M3 subclass of acetylcholine receptors, resulting in improved tolerability. Tolterodine is better tolerated than oxybutynin with less moderate-tosevere dry mouth and fewer dropouts because of medication side effects but is not as effective. Solifenacin in another antimuscarinic that has proven effective in patients with urge incontinence who have not responded to tolterodine or oxybutynin. Tricyclics such as amitriptyline or imipramine can be useful in mild or moderate cases. Estrogen can be used as an adjunct in postmenopausal women with stress incontinence. There are many surgical procedures that have been developed for urinary incontinence. It supplied as a mixture of the (R)- and (S)enantiomers; the (S)-enantiomer has little anticholinergic activity. Adverse Effects Common adverse effects associated with oxybutynin and other antimuscarinic anticholinergics include dry mouth, difficulty in urination, constipation, blurred vision, drowsiness, and dizziness. Dry mouth may be particularly severe especially with oxybutynin; one estimate is that 25 to 50 percent of patients who begin oxybutynin treatment may have to stop because of dry mouth. N-Desethyloxybutynin is an active metabolite of oxybutynin that is thought to be responsible for much of the adverse effects of the drug. This has not improved after 2 months of pelvic floor training including Kegel exercises, and a trial of tolterodine. Common side effects of antimuscarinic drugs are dry mouth, blurred vision, fatique, and dizziness. Antimuscarinic drugs also reduce sweating; this increases the risk of overheating and heat stroke. Pharmacologic treatment of stress incontinence includes sympathomimetics such as pseudoepedrine, which would be contraindicated here because of the hypertension. A combination of a tricyclic like amitriptyline and an anticholinergic appears to provide a synergistic effect that can work in refractory cases. Use of anticholinergics have modest but important benefits to the quality of life, but discontinuation of drugs is high. Her family history is significant also for obesity and multiple obesity-associated complications such as osteoarthritis, type 2 diabetes, obstructive sleep apnea, and coronary artery disease. Her mother told her that 25 years ago she was treated with a medication for obesity, and the patient wonders if this would help her. How would this patient be classified in terms of obesity and what comorbidities is she now at risk for Based on evidence-based guidelines, what treatment options should be offered to this patient Patients who are obese are at risk of morbidity from associated conditions such as (but not limited to) hypertension, dyslipidemia, type 2 diabetes, coronary heart disease, stroke, gallbladder disease, osteoarthritis, sleep apnea and respiratory problems, and endometrial, breast, prostate, and colon cancers. Higher body weights are also associated with increases in all-cause mortality, psychiatric illnesses, asthma, and various somatic dysfunctions. Regardless of the diet or exercise regimen, trials have shown that those that are successful long term are those patients who continue the regimen. Its effectiveness is variable based on the literature as many trials have many confounding variables. Phentermine may cause tachycardia, elevations in blood pressure, and psychomotor agitation, and have a high abuse/dependency potential. Obesity is second only to smoking as a cause of preventable death in the United States. Obesity contributes to morbidity and mortality through its effects on diabetes, hypertension, hyperlipidemia, atherosclerosis, stroke, sleep apnea, cancer, arthritis, and depression. Although metabolic syndrome is a serious cause of illness, treatment consists of management of each individual component and aggressive screening for other components. When obesity is associated with metabolic syndrome or other risk factors, it requires aggressive intervention. Metabolic syndrome: the co-occurrence of several clinical findings, including diabetes, obesity, and cardiovascular disorders. Most experts agree that a truly successful strategy involves a combination of diet, exercise, and behavioral changes, with or without surgery and medications. Many diets have been promoted and studies show that all have similar effectiveness in the long term. Restricted calorie diets in overweight or obese individuals generally promote 8 percent weight loss per year. The most successful diets include support groups that incorporate behavioral modifications. Exercise added to dietary change is more successful, as exercise prevents the slowing of metabolism from caloric deficit. Behavioral modifications emphasize portion control, emotions associated with eating, and adherence to dietary plans. During the intervention period they usually produce up to 10 percent weight loss; however, weight is often regained after the program ends. Surgical treatments of obesity have the single greatest efficacy, but also pose the greatest risk. Surgical procedures can reduce body weight by 35 to 40 percent with maintenance for 15 years. Success is higher with surgery in patients who are committed to lifestyle changes (diet/exercise/portion control/appropriate food choices) and those who have ongoing support mechanisms and psychological support. Risks of surgery include prolonged postoperative recovery, infection, electrolyte derangements, dehydration, excess skin, nutritional deficiencies, dumping syndrome, deep vein thrombosis, and cholecystitis. Perioperative mortality can reach 1 percent and is reduced when medical and psychiatric conditions are controlled preoperatively. Even when surgery is completely successful without complications, patients can be expected to have malabsorption issues requiring supplementation with calcium, thiamin, iron, and vitamin B12. In addition, many medications will have altered pharmacokinetics following successful surgery. The surgery results in reduced surface area for absorption and will significantly reduce absorption of extended-release drugs. Absorption of medications that are pH sensitive will be altered by the alkaline environment. Orlistat is the only lipase inhibitor currently produced and, unlike all other antiobesity medications, is approved for long-term treatment of obesity. It is available in both prescription and over-the-counter forms and is dosed three times a day with meals. The over-the-counter formulation is a 50 percent reduced dose of the prescription strength medication. Orlistat is not systemically absorbed, and side effects are concentrated on the gastrointestinal tract. Most common adverse events include flatulence, greasy/loose stools, and abdominal pain. They are approved only for short-term treatment of obesity and are typically administered once daily. Phentermine is the most commonly prescribed sympathomimetic and has been available since the 1970s. A recently approved weight-loss drug combines phentermine with the antiepilepsy drug, topiramate. All of the sympathomimetics can produce hypertension, tachycardia, insomnia, and other symptoms of sympathetic activation. Food intake can be reduced by serotonin; therefore, serotonin receptors have long been targeted for the development of weight-loss drugs. Topiramate is an antiepileptic drug that is also indicated for migraine prophylaxis. Side effects that limit its use include induction of cognitive deficits and peripheral neuropathy. Hence, avoidance of overexpenditure, avoidance of drugs/herbs/supplements that promote weight loss, and optimizing caloric intake would be ideal if other organic causes have been ruled out. However, trials have shown that in addition to diet and exercise they are more effective than any modality alone.
Syndromes
- Enzyme tests
- Amount swallowed
- Loss of movement (paralysis) of the hips, legs, or feet (lower extremities)
- Apply a warm cloth or warm water bottle to the affected ear.
- Long periods of travel to tropical destinations
- Injuries to the back
Order 50 mg pletal visa
A serum procalcitonin will distinguish bacterial infections from viral infections spasms brain purchase pletal with paypal. Case Presentation #27 A 16-year-old white boy is referred to you with a history of sore throat and intermittent fever for 10 days. He was treated with penicillin by his family physician 1 week ago but failed to respond. Utilizing the methods discussed above, what is your list of possibilities at this point However, if the clinician immediately focuses on the kidney, he or she may be sadly mistaken because one forgets the other significant organs in the area. Looking at the adrenal gland, one need only recall the tumors of this gland such as a neuroblastoma, adrenocortical carcinoma, or pheochromocytoma. Surprisingly, other organs located near the flank may be palpated as a flank mass. As in the right upper quadrant, a carcinoma or collection of stool can be palpated in the flank. Moving into the retroperitoneal area, we again may find hematomas of the wall of the flank, bony tumors, and retroperitoneal sarcomas. Approach to the Diagnosis the history of trauma will be helpful in narrowing the diagnosis. Obviously, if there is fever a perinephric abscess, pyonephrosis, or tuberculosis is more likely. It is wise to consult an urologist before ordering any x-ray procedure to help decide which is the most cost-effective approach. Visualizing the anatomy of the right flank and crossindexing each structure with the etiology classification, what would be your list of possible causes at this point Further history reveals the patient has noted painless hematuria on a couple of occasions but is otherwise asymptomatic. Physical examination is unremarkable aside from the large nontender mass in the right flank. As is shown in Table 29, however, jumping to that conclusion in any given case may be hazardous. In addition to the kidney (pyelonephritis and perinephric abscess), inflammation of the skin (herpes zoster), the colon (diverticulitis and colitis), the gallbladder (cholecystitis), and the spine (epidural abscess and Pott disease) may also cause flank pain. Neoplasms of the kidney and colon are less likely to produce pain unless they are complicated by infection. However, trauma of the kidney and spine and renal calculi-whether due to hyperparathyroidism, idiopathic etiologies, or hyperuricemia-are important causes. If these are negative, bone scans, arteriogram, and other tests listed below may be 362 required. Utilizing the methods discovered above, what would be your list of possibilities at this point Physical examination is unremarkable except for hyperesthesia and hyperalgesia in the distribution of T12 dermatome on the left. Retina: Conditions of the retina to be considered in this symptom are exudative choroiditis, retinal detachment, venous thrombosis, and embolism. Optic cortex: Transient ischemic attacks in the posterior cerebral circulation and epileptic auras may cause this symptom. Arterial circulation to the eye and brain: Migraine, cerebral thrombosis, and emboli present with this symptom. Approach to the Diagnosis this is similar to the workup of blurred vision (see page 76). The increase of gas in the intestinal tract depends on three physiologic mechanisms: 1. Increased intake of air: this is probably one of the most frequent causes of flatulence and borborygmi. However, compulsive eating, compulsive drinking, excessive smoking, or excessive talking may produce the same effect. When we overeat, however, or when we drink too much, the amount of gas taken in may exceed our ability to absorb it. Salesmen and public speakers have an additional problem because talking increases salivation and swallowing, and frequently air is swallowed between sentences. Some people have a particular beverage they are fond of, such as cola, coffee, or alcohol. In addition, some of these beverages release gas after ingestion (carbonated beverages especially), which causes flatulence. Increased production of gas in the intestinal tract: In acute bacterial gastroenteritis. The diarrhea or vomiting associated with these disorders usually makes 364 the diagnosis easy. A more obscure cause of increased production of gas is chronic mild intestinal obstruction leading to excessive bacterial overgrowth. Adhesions, intestinal polyps, regional ileitis, and the various causes of paralytic ileus. Gas production is also increased when bacteria are allowed to accumulate in large numbers in chronic intestinal disorders. The blind loop syndrome, diverticulitis, and Meckel diverticulum fall into this category. Some types of irritation in the intestinal tract cause a mild paralytic ileus and allow bacteria to multiply and ferment: Esophagitis and hiatal hernia, chronic gastritis, ulcers, regional ileitis, and ulcerative and mucous colitis may cause mild paralytic ileus on this basis. When the amount of digestive juices is insufficient to digest food, more food is available for bacterial fermentation. Thus, in chronic atrophic gastritis, the reduced level of hydrochloric acid leaves undigested food for bacterial action. In cholecystitis and partial bile duct obstruction or liver disease, there are insufficient bile acids for digestion and more food is left for bacterial fermentation. In chronic pancreatitis, the reduction in pancreatic enzymes causes the same problem. In celiac disease, the atrophied villi cannot pick up food and gas, and these are passed through the intestines. Intestinal parasites may preempt food from absorption and produce excessive gas in their own digestive processes. Approach to the Diagnosis If excessive food, beverages, or air swallowing from nervous tension or talking can be excluded, reflux esophagitis and diverticulitis must be considered. If these findings are questionable, a more definitive diagnosis may be made with endoscopy. When the outcome is still 365 uncertain, evaluation of the adequacy of the intestinal digestive secretions is worthwhile. Gastric analysis with Histalog and duodenal analysis for bicarbonate, bile, and pancreatic enzymes is done. If the digestive secretions are adequate, a small-bowel biopsy may be necessary to exclude a malabsorption syndrome. Therapeutic trial of proton pump inhibitors (reflux esophagitis) Case Presentation #31 A 46-year-old white woman complained that for the past year she has had increasing episodes of flushing of the face and neck, especially during exercise or stress. What diagnosis should you entertain considering the physiology involved in this symptom Further history reveals that she has had chronic diarrhea for a couple of years as well. Physical examination revealed telangiectasias of the face and neck and mild hepatomegaly. A flushed face may result from an increased amount of circulating blood (polycythemia) or from any factor that may dilate the blood vessels in the face. Polycythemia may be primary, as in polycythemia vera, or secondary, as in Cushing syndrome, unilateral renal disease, hypernephroma, and pulmonary or cardiovascular disease associated with chronic anoxia. It is less commonly found in the use of belladonna, alkaloids, histamine headaches (usually unilateral), and cirrhosis of the liver, but it is common in chronic skin diseases of the face such as acne rosacea. A flushed face with a heart murmur would suggest mitral stenosis or a right to left shunt with polycythemia. A flushed face and chronic diarrhea would prompt one to consider a carcinoid syndrome. If Cushing syndrome is suspected, a serum cortisol level and a cortisol suppression test could be done. Blood volume (polycythemia vera) Serum erythropoietin level (primary and secondary polycythemia) Serum gastrin level (gastrinoma) Pulmonary function tests (pulmonary emphysema) 24-hour vanillylmandelic acid test (pheochromocytoma) Bone marrow examination (polycythemia vera) Case Presentation #30 A 67-year-old white man complained of increasing burping, indigestion, and hiccoughs for the past year. Physical 369 examination is unremarkable except for pale conjunctiva and a smooth tongue. Other anatomic components of the foot and toes may cause pain as well, so a consideration of the differential diagnosis of foot and toe pain must include diseases of these structures. Painful conditions of the skin include warts, calluses, bunions, and corns, conditions often caused by bad posture and poor-fitting shoes. Moving to the subcutaneous tissue and fascia, cellulitis and plantar fasciitis are suggested.
Order cheap pletal
Inhaled insulin uses a device similar to an asthma inhaler for fixed insulin dosage prior to meals spasms stomach area buy cheap pletal 50 mg on-line. Structure Human insulin derived by recombinant technology in bacteria or yeast has supplanted the use of bovine or pork insulins. The insulin receptor consists of an extracellular -subunit that forms the insulin-binding site and a transmembrane -subunit that possesses tyrosine kinase activity. Insulin binds its receptor in the picomolar range within a binding pocket formed by the two -subunits. Binding produces conformational changes in the receptor that activate intrinsic tyrosine kinase activity that results in autophosphorylation of one -subunit by the other. Phosphorylation of various substrates in this insulin pathway also increases glycogen synthesis, lipogenesis, protein synthesis, and activation of transcription factors that mediate effects on cell growth and division. Administration Most currently available preparations are injected subcutaneously or delivered by continuous infusion. Oral Hypoglycemic Agents Oral hypoglycemic agents increase the secretion of insulin by the pancreas or alter tissue sensitivity to insulin. Sulfonylureas Sulfonylureas act to increase the release of insulin from the pancreas. Firstgeneration sulfonylureas include tolbutamide, chlorpropamide, tolazamide, and acetohexamide. Second-generation agents include glyburide, glipizide, gliclazide, and glimepiride, which are considerably more potent than the earlier agents. All are substituted arylsulfonylureas with different substitutions on the benzene ring and at one nitrogen residue of the urea moiety. A limitation in the use of the sulfonylureas is secondary failure, that is, failure to maintain glucose levels with chronic use. Adverse effects of sulfonylureas include hypoglycemia, nausea and vomiting, anemia, and dermatologic reactions. Mechanism of Action Sulfonylureas bind to a high-affinity sulfonylurea receptor on B cells that inhibits a K+-efflux channel. This leads to depolarization of the cell with an increase in Ca2+ entry through voltage-gated Ca2+ channels. Sulfonylureas also stimulate the release of pancreatic somatostatin, which can reduce the secretion of glucagon. Pharmacokinetics First-generation sulfonylureas have relatively long half-lives: Chlorpropamide is 32 hours, tolazamide is 7 hours, and tolbutamide is 5 hours. Lingaglipin Meglitinides: Repaglinide, Nateglinide Increase insulin release and Can cause hypersensitivity reacdecrease glucagon production tions. Nausea, weight loss Decreases breakdown of incretins Cold-like symptoms, runny nose, sore throat. May be due to inhibition of cytokine breakdown Caution in elderly, renal, or hepatic insufficiency. Both of these agents act by decreasing the activity of K+ channels as described for the sulfonylureas. Chemically, repaglinide is a meglitinide, and nateglinide is a D-phenylalanine derivative. Metabolized in the kidney and should be used cautiously in patients with renal impairment. The hormone is present at significant plasma concentrations but is ineffective in reducing plasma glucose. Biguanides Metformin lowers plasma glucose levels in the absence of functioning a cells; it does not increase insulin secretion but decreases insulin resistance by increasing glucose uptake and decreasing glucose production. Biguanides are cleared by the kidney and are contraindicated in patients with renal disease. Polypeptide Analogs Pramlintide is a synthetic analog of amylin, which is produced by the pancreas in concert with insulin. It decreases postprandial hyperglycemia and improves glucose control when administered with insulin. Exenatide mimics the enhancement of glucose-dependent insulin secretion and other antihyperglycemic actions of incretins. Several clinical trials have demonstrated the effectiveness of exenatide either with metformin or in combination with metformin and a sulfonylurea. Exenatide has been associated with weight loss and early satiety partly due to its side effect of nausea. Other Enzyme Inhibitors Monosaccharides such as glucose and fructose can be absorbed across the intestine and into the portal circulation. Complex disaccharides, starches, and disaccharides that comprise a significant percentage of the carbohydrates ingested must be broken into monosaccharides before they can be absorbed. Pancreatic -amylase and -glucosidases are primarily responsible for this hydrolysis of more complex carbohydrates. Inhibitors of `-glucosidase such as acarbose and miglitol inhibit the intestinal breakdown of complex carbohydrates. Miglitol is five to six times more potent than acarbose and inhibits the same -glucosidase, as well as isomaltase and -glucosidases (responsible for hydrolysis of lactose). Inhibition of these digestive enzymes reduces postprandial absorption of complex carbohydrates and thereby reduces plasma glucose levels. Adverse effects include flatulence, diarrhea, and abdominal pain, most likely caused by the increase in carbohydrates in the distal small intestine and colon. Which of the following agents would help with her prandial or mealtime glucose control without persisting in her system to cause later hypoglycemia The goal in treating diabetes is tight control of serum glucose to avoid the complications of hyperglycemia. In general, the most common adverse effect of the agents for diabetes is hypoglycemia. Repaglinide is a fair option, however, in general patients on sulfonylureas should not be on repaglinide or nateglinide as they have similar mechanisms of action. Biguanides such as metformin are cleared by the kidney and are contraindicated in patients with renal disease. Effectiveness of quality improvement strategies on the management of diabetes: a systematic review and meta-analysis. She takes hydrochlorothiazide for hypertension, levothyroxine sodium for hypothyroidism, and a multivitamin. Metformin is an oral antidiabetic agent that causes metabolic changes that decrease serum glucose and insulin levels. Acanthosis nigricans: A velvety darkening of the skin commonly seen at the nape of the neck, elbows, axilla, and knuckles usually caused by hyperinsulinemia. The ovaries accumulate benign cysts produced by abnormal follicular development and lack of ovulation due to endocrine dysfunction. The elevated insulin level due to the insulin resistance is a potent stimulator of steroidogenesis, especially of androgens, in the ovary. Serum testosterone concentrations were also found to decrease by approximately 50 percent. These side effects tend to decline with continued use and can be minimized by initiating therapy with low doses of metformin. Asymptomatic vitamin B12 deficiency was reported with metformin monotherapy in 9 percent of patients during clinical trials. The risk of hypoglycemia is much less common with metformin than with the sulfonylureas. In patients unsuccessfully treated with clomiphene alone, addition of metformin may increase the ovulation and conception rates. Metformin infrequently causes hypoglycemia and hypersensitivity reactions, for instance in the skin, are rare. Metformin does not increase insulin production; it appears to act by decreasing plasma glucose by affecting metabolism rather than altering the sensitivity of tissues to insulin. Further history reveals that he has smoked one pack of cigarettes a day for 30 years. A sputum Gram stain reveals gram-positive cocci, and subsequent sputum and blood culture results confirm the diagnosis of pneumonia caused by Streptococcus pneumoniae (pneumococcus). They do this by binding to the active site of the penicillin-binding protein (an enzyme) that is involved in maintaining cell-wall stability.
Order pletal 50 mg with visa
Any neoplasm that metastasizes to the cervical spine may spread into the neck; a plasmacytoma is likely to do this in multiple myeloma muscle relaxant india order pletal with paypal. Abnormal accumulations of fluid, air, or other substances in colloid cysts and bronchial cleft cysts have already been mentioned, but what about carbuncles, sebaceous cysts, and angioneurotic edema Cystic hygromas present from birth contain a serous or mucoid material and may be huge. Approach to the Diagnosis the clinical picture will help to determine the diagnosis in many cases. For example, a neck mass with hemoptysis suggests carcinoma of the lung with metastasis to the lymph node. If the mass increases in size after swallowing food or liquid, an esophageal diverticulum is likely. If the mass is suspected to be an enlarged lymph node, exploration and biopsy may be appropriate. One can 616 now see that the diagnostic workup can be developed by visualizing the anatomy of the area. First, the anatomic components are distinguished, then the various etiologies are 618 applied to each (Table 48). Moving from the skin to the spinal cord layer by layer, we encounter the fascia, muscles, arteries, veins, brachial and cervical plexus, and lymph nodes. Finally, there is the cervical spine encircling the spinal cord and meninges and designed to allow uninfringed exit of the cervical nerve roots. The skin may be involved by herpes zoster, cellulitis, contusions, and lacerations. In the muscle and fascia, one encounters fibromyositis, dermatomyositis, and trichinosis as well as traumatic contusions and pulled or torn ligaments (strains). Remember Ludwig angina, which is a painful swelling under the chin caused by the spread of a dental abscess to the neck! The muscles may be involved by tension headache, poor posture, and occasionally by epidemic myalgia. Torticollis causes painful spasms, but the jerking of the neck makes the condition obvious. Table 48 Neck Pain the arteries of the neck are infrequently tender or painful as are most aneurysms (aside from dissecting aneurysms) unless they compress 619 adjacent structures. Arteritis is unusual here, but a common carotid thrombosis may be tender and painful. As with the arteries, it is rare for the jugular veins and smaller veins of the neck to cause pain by thrombosis or rupture; however, it occasionally happens in superior vena cava obstruction. They are usually enlarged and tender in association with pharyngitis, otitis media, sinusitis, dental abscesses, and mediastinitis. The brachial plexus may be involved by a primary neuritis or by compression from a scalenus anticus syndrome, a Pancoast tumor, the clavicle (costoclavicular) syndrome, or a cervical rib. More often, the roots are compressed by diseases of the spine, such as a herniated disk, fracture, cervical spondylosis, tuberculous or nontuberculous osteomyelitis, and primary or metastatic tumors of the spine and spinal cord. In the case of the spinal cord, one should also remember the meninges as a cause of neck pain in meningitis, arachnoiditis, and subarachnoid hemorrhage. The esophagus is not usually a cause of neck pain, but pain may be referred to the neck from a hiatal hernia or subdiaphragmatic abscess. Pulsion diverticula of the esophagus may also compress adjacent structures and cause painful symptoms. Like the esophagus, the trachea is an infrequent source of neck pain, but occasionally acute laryngotracheitis will be the source of severe pain. Finally, subacute thyroiditis and inflammatory or obstructive lesions of the salivary glands may be the offenders in neck pain, even though the patient complains of a sore throat. Approach to the Diagnosis the patient who presents with neck pain most commonly has a cervical sprain or muscle contraction headache. However, we must rule out more serious pathology such as meningitis, subarachnoid hemorrhage, herniated disks, and neoplasms before we send the patient home with a collar and a bag of pills. This means checking for nuchal rigidity, doing a thorough neurologic examination, and checking for a thyroid or lymph node mass. If the neurologic examination is abnormal, referral to a neurologist or a neurosurgeon is indicated before ordering expensive diagnostic tests. If the neurologic examination is normal and there are no neck masses or other significant findings, conservative treatment may be initiated without ordering expensive diagnostic tests. However, most physicians consider it 620 wise to at least do plain films of the cervical spine. Careful and close follow-up is necessary so that something serious is not missed in these cases. Always keep in mind that the pain may be referred from the heart, lungs, esophagus, or gallbladder. Neurologic examination revealed loss of sensation to touch, pain in the right thumb, and diminished right biceps reflex. I-Inflammation prompts the recall of nightmares associated with systemic infections, and intoxication brings to mind the nightmares due to alcohol and drugs such as the benzodiazepines. Alcohol- or drug-induced nightmares may be diagnosed by the history and a drug screen. The history should also be useful in cases of head injury, especially when questioning the family or closely associated persons. If epilepsy is suspected, a wake-and-sleep electroencephalogram should be ordered; a trial of anticonvulsants may be necessary to rule out epilepsy. A pathophysiologic analysis of the symptoms would indicate that the patient is producing excessive urine at night, there is an obstruction to the output of urine so that the bladder cannot be emptied fully on one voiding, or there is an irritative focus in the urinary tract stimulating the patient to urinate more frequently. Excessive urine production at night: this category includes all the causes of polyuria: diabetes insipidus, diabetes mellitus, hyperthyroidism, diuretic drugs, nephrogenic diabetes insipidus, and chronic nephritis. In addition, the one condition that produces excessive urine output almost exclusively at night-congestive heart failure-must be considered. In heart failure, edema accumulates in the extremities during the day while the patient is in the upright position and is returned to the circulation and poured out through the kidneys at night while the patient is in the 622 recumbent position. Obstructive uropathy: Bladder neck obstruction by a calculus, enlarged or inflamed prostate, median bar hypertrophy, or urethral stricture is a condition to consider here. Neurogenic bladder from poliomyelitis, multiple sclerosis, and other spinal cord diseases must also be considered. Irritative focus in the urinary tract: Nocturia may result from inflammation of the bladder, prostate, urethra, and kidney on this basis. Inflammation of the vagina, fallopian tubes, and rectum are also occasionally responsible. Approach to the Diagnosis the workup of nocturia is essentially the same as the workup of polyuria and urinary frequency (see page 345). Venous pressure, circulation time, and pulmonary function studies to rule out congestive heart failure should be done if the urinary tract is clean. I-Inflammation prompts the recall of disorders that destroy the palate such as syphilis, leprosy, and tuberculosis. T-Trauma should make one suspect palatal fenestration from gunshot wounds or surgery, posttonsillectomy weakness, and trauma to the brain stem. Approach to the Diagnosis Cleft palate and many other conditions will be diagnosed by a careful nose and throat examination; all that is necessary is a referral to an otolaryngologist. If the local examination is negative, a referral to a neurologist is probably in order. The muscles of the neck may be rigid from Parkinsonism or pyramidal tract disease. Diseases of the spine such as cervical spondylosis, rheumatoid spondylitis, and tuberculosis may cause nuchal rigidity. An acute fracture of the cervical spine should be considered if no history can 625 be obtained. The respiratory tree recalls retropharyngeal abscess, mediastinal emphysema, and endotracheal intubation. Finally, the spinal cord and meninges may be involved by meningitis, epidural abscess, subarachnoid hemorrhage, and primary and metastatic tumors, resulting in nuchal rigidity. Approach to the Diagnosis 626 the workup of nuchal rigidity requires a good history, but if one is unobtainable, no spinal tap should be performed until the cervical spine is x-rayed and the eyegrounds are examined. Even with a good history, a spinal tap should be withheld if there is papilledema: A neurosurgeon should be consulted immediately under these circumstances. In a patient with fever, nuchal rigidity, no papilledema, and no focal neurologic signs (particularly a dilated pupil), a spinal tap can be performed for diagnosis and immediate therapy.
Trusted 50mg pletal
In cases of prerenal azotemia spasms under ribs order generic pletal online, there will be decreased skin turgor and orthostatic hypotension if the cause is volume depletion. Patients with postrenal azotemia may have an enlarged prostate, a distended bladder, and other signs of obstructive uropathy. Patients with renal azotemia may have bilateral flank masses (polycystic kidney), hypertension, peripheral emboli (embolic glomerulonephritis), or a rash (collagen disease, interstitial nephritis). The bladder is catheterized for residual urine; if this is significant, postrenal azotemia is likely and an urologist is consulted. Ultrasonography can be used to determine if there is significant residual urine also. The laboratory studies will determine whether there is prerenal or renal azotemia. If the sodium concentration in the spot urine is <10 mEq/L, prerenal azotemia is likely. If volume depletion is the cause, intravenous saline and plasma volume expanders are given while carefully monitoring the urine output. If this is ineffective, furosemide and a mannitol drip can be utilized to reestablish urine output. If these measures are ineffective, the patient obviously has a renal cause for his or her anuria, and an urologist should be consulted. If intravascular hemolysis is suspected, a serum haptoglobin test should be ordered. If dissecting aneurysm or bilateral renal artery stenosis is suspected, aortography and angiography would be done. Aphasia must be distinguished from dysarthria, which could also be due to involvement of the brain stem or cerebellum. Patients with dysarthria have no difficulty recognizing or interpreting words or phrases, but speech is garbled and difficult to understand by the clinician. D-Degenerative disorders include Alzheimer disease, Pick disease, Huntington chorea, and dementia with Lewy bodies. I-Intoxication should suggest the possibility of alcohol or drug intoxication and Korsakoff psychosis. C-Congenital disorders include cerebral palsy, the leukodystrophies, and congenital abnormalities of the brain such as hydrocephalus and microcephaly. Cerebral aneurysm and atrioventricular (A-V) anomalies might also be brought to mind in this category. A-Autoimmune disorders include multiple sclerosis, lupus erythematosus, thrombotic thrombocytopenic purpura, and other collagen disorders. T-Trauma should bring to mind epidural, subdural, and intracerebral hematomas related to trauma. E-Endocrine disorders are not particularly suggestive of cerebral pathology, but an amniotic fluid embolism may rarely be responsible for aphasia, apraxia, or agnosia. Hypoparathyroidism may bring about seizures which could cause transient aphasia in the postictal phase. The history would be very important in ruling out alcohol or drug intoxication, trauma, or autoimmune disorders. These studies would be most definitive for an infarct, spaceoccupying lesion, or degenerative disorders. Pain may be referred from more proximal portions of the extremity such as the shoulder. Beginning with the skin and subcutaneous tissue, one recalls herpes zoster, cellulitis, contusions, and a variety of dermatologic conditions that should be obvious. Rheumatoid and rheumatic nodules may occur on the skin and are, of course, painful. Beneath the skin the muscles, fascia, and bursae are frequent sites of inflammation and trauma. Contusions, rupture of the ligaments, and bursitis (particularly tennis elbow) are common acute traumatic conditions (bursitis, however, is more likely the result of chronic strain). Inflammatory lesions of the muscles include epidemic myalgia, trichinosis, nonarticular rheumatism, and dermatomyositis. Muscle cramping from hypocalcemia or other electrolyte disturbances must be considered in the differential diagnosis of arm pain. The superficial and deep veins are the site of thrombophlebitis and hemorrhage, both prominent causes of arm pain. When one moves centrally along the arterial pathways, additional causes of pain come to mind. For example, dissecting aneurysms or acute subclavian steal syndrome may 152 cause severe pain down the arm, but pain is referred to the arm from a myocardial infarct as well. When superficial or deep infections of the arm spread to the lymphatics, lymphangitis may develop and cause arm pain. Neuromas may cause focal pain in the distribution of the involved peripheral nerve. Carpal tunnel syndrome, which may be caused by rheumatoid arthritis, amyloidosis, acromegaly, hypothyroidism, or multiple myeloma, may compress the median nerve (and occasionally the ulnar nerve) to cause pain in the hand and even up the arm. Moving up the nerve pathways, another frequent spot for nerve compression is the brachial plexus. Pancoast tumors, cervical ribs, and the scalenus anticus syndrome may be the cause of arm pain originating from the plexus. The cervical nerve roots may be compressed by diseases of the spine and spinal cord. A herniated disc, cervical spondylosis, metastatic carcinoma, tuberculosis of the spine, multiple myeloma, and cord tumors. Syringomyelia and tabes dorsalis are other sources of arm pain that originate in the spinal cord. As one moves up the cord to the brainstem, one recalls the thalamic syndrome (usually caused by occlusion of the thalamogeniculate artery) as a cause of pain in the arm. They prompt the diagnosis of osteomyelitis, primary and metastatic bone tumors, and diseases of the joints such as osteoarthritis, rheumatoid arthritis, gout, gonococcal arthritis, and Reiter syndrome. Systemic diseases that cause arm pain from peripheral nerve involvement include diabetes mellitus (with ischemic neuropathy), periarteritis nodosa, and macroglobulinemia. Approach to the Diagnosis the association of other symptoms and signs found on a good history and physical examination is most important in pinpointing the diagnosis. Thus, arm pain with tenderness and limitation of motion at the elbow suggests 156 tennis elbow, gout, or rheumatoid arthritis. Arm pain with loss of sensation in the distribution of the median nerve suggests carpal tunnel syndrome. The laboratory workup should include x-rays of the involved area and of the cervical spine, especially if there is a radicular distribution of the pain. Arteriogram, phlebogram, lymphangiogram, electromyogram with nerve conduction studies, myelogram, and nerve blocks will be necessary in specific cases. Dermatomal somatosensory evoked potentials (neuropathy, radiculopathy, demyelinating disease) 3. Utilizing the methods described above, what are the possible diagnoses that you would entertain at this point Further history reveals that the patient was involved in an auto accident 1 year ago. He complained of neck pain at that time but was treated in the emergency room and released. Neurologic examination at this time reveals a diminished biceps reflex and hypesthesia and hypalgesia in the left thumb and index finger. This translates into hepatitis, myocardial infarction, and dermatomyositis as the principal conditions to consider in the differential diagnosis. Approach to the Diagnosis Obviously, the first condition to rule out is myocardial infarction. A discharge may arise from the external canal, the middle ear, the mastoids and petrous bone, the inner ear, or the cerebrospinal fluid. As elsewhere in the body, nonbloody discharge signifies inflammation and infectious or allergic conditions, but foreign bodies and malignancies can trigger an infection by causing an obstruction or lowering resistance.
