
Order silvitra cheap
Functions: Detection of direction and accessing the frequency of sound originates loudness erectile dysfunction treatment cost in india buy silvitra 120mg on line, pitch and quality. Speech area Sensory speech area (area 39) Location: Same as that of higher visual area. Functions: this area receives the input from hearing, vision, touch and proprioception. These are the large masses of grey matter, situated within the cerebral hemispheres ii. All the basal nuclei are joined to the cortex at the anterior perforated substance iii. Some gray matter present just below the corpus striatum close to the anterior perforated substance described as ventral striatum 4. Part of the globus pallidus lies below the level of the anterior commissure known as ventral pallidum. Band of gray matter connect the head to the putamen traversing the anterior limb of internal capsule just above the anterior perforated substance. Medially: Stria terminalis which lodges in a groove known as sulcus terminalis situated between the caudate nucleus and thalamus. It is further partly divided in to two parts by the anterior limb of internal capsule: a. The head of caudate nucleus and lentiform nucleus are connected by a band of gray matter through the anterior limb of internal capsule as a result the whole nuclear mass appears striated hence, it is called corpus striatum iii. According to structures, connections and functions the caudate nucleus and putamen are similar and they are called neostriatum iv. The caudate nucleus is continuous with the putamen by disrupting the lower part of the anterior limb of internal capsule vi. The greater part of the corpus striatum is situated in front of the postcentral sulcus. Corona radiata which are the projection fibers of the cerebral cortex converge to the periphery of the corpus striatum forming fanshaped arrangement. It is subdivided in to two parts by external medullary lamina (a thin layer of white matter): a. Situation: It is situated deep to the insular cortex, from which it is separated by the following: i. Relations Medially: Internal capsule which is separated from the thalamus in the posterior part and the head of the caudate nucleus in the anterior part. Anterior commissure (grey matter) which produces a deep groove just behind the anterior perforated substance ii. Sublentiform part of internal capsule which separates it from the optic tract, tail of caudate nucleus and inferior horn of lateral ventricle Superiorly: Fibers of corona radiata. Globus pallidus Afferents: the globus pallidus receive afferent fibers from following: i. Situation Roof of the inferior horn of the lateral ventricle in the temporal lobe close to its tip. Corticomedial part: It receives olfactory fibers via the lateral olfactory stria 2. Basolateral part: It receives fibers mostly from the cerebral cortex of the parahippocampal gyrus. Efferents: the efferent fibers unite to form stria terminalis on the posterior end of the amygdaloid body. Association of olfactory and autonomic systems Claustrum It is a thin sheet of gray matter. Situation Between the external capsule medially, and white matter of insula laterally known as extreme capsule. Continuation Inferiorly it is thickest and continuous with the anterior perforated substance and amygdaloid body. If tumor compress the anterior twothirds of the posterior limb of the internal capsule produce progressive spastic hemiplegia on the opposite side of the body iii. The most posteriorly situated tumors produce impairment of sensation on the opposite side of the body. Situation It is situated in the inferomedial part of the cerebral hemisphere between the head of caudate nucleus and thalamus medially and the lentiform nucleus laterally. Controls skilled and manipulated activities of the body, like threading the needle 3. Loss of automatic associated movements and also facial expressions (mask-like face), 3. Involuntary movements like tremor, choreiform and other types of abnormal movements. As the internal capsule lies between the caudate and lentiform nuclei, which produces compression on the internal capsule therefore may cause severe motor boundaries Above Corona radiata. Anterior Limb Situation Between the head of the caudate nucleus medially and lentiform nucleus laterally. Carrying fibers from the frontal lobe to the nuclei pontis then to the opposite neocerebellum. Carrying fibers from the anterior and dorso-medial nuclei of the thalamus to the cortex of the frontal lobe. These fibers form a pathway of Papez circuit for the emotional integration and recent memory. Corticostriate fibers: Some of these fibers reach the caudate nucleus after passing through the subcallosal bundle and anterior limb of internal capsule. Fibers of the medial forebrain bundle: these fibers connect the orbital surface of the frontal lobe with the hypothalamic nuclei. Situation It is situated between the lentiform nucleus laterally and the posterior part of head of caudate nucleus and anterior end of thalamus medially. Corticoreticular and some fibers of superior thalamic radiation: these fibers connect between the thalamus and the cerebral cortex. Corticospinal tract: Fibers arise from the areas 4 and 6 of the cerebral cortex forming the corticospinal tract. Few corticostriate fibers: these fibers connect the cerebral cortex with caudate nucleus and putamen. Frontopontine and parietopontine fibers: these fibers extending from the frontal and parietal lobes to the pontine nuclei. They connect anterior ventral and intermediate ventral nuclei of thalamus with areas 4 and 6 and posterior ventral thalamic nuclei with the areas 3, 1, 2 of the postcentral gyrus. Fasciculus subthalamicus: Fibers between the globus pallidus with the subthalamic nucleus. Nigrostriate fibers: Fibers between the substantia nigra with the caudate nucleus and putamen. Thalamostriate fibers: Fibers connect the intra-laminar and centro-median nuclei of the thalamus with the caudate nucleus and putamen. Fibers of posterior thalamic radiation extend from the pulvinar of the thalamus to the areas 18, 19, 39 and 40. Sublentiform Part Situation It is situated most posterior end of the internal capsule, below the posterior part of the lentiform nucleus. Fibers of olfactory radiation: Fibers arise from the medial geniculate body extend in to the superior temporal gyrus (areas 41 and 42). Retrolentiform Part Supplied by the striate branches from posterior cerebral artery. Fibers of optic radiation: Arise from the lateral geniculate body and terminate in the Venous Drainage i. Minimum hemorrhage in internal capsule may cause hemiplegia of the opposite side of lesion, as the lesion is in the upper motor neuron type. This is because of pyramidal tract is located in the genu and posterior limb of internal capsule causes widespread effects on the opposite side of the body. The uncinate fasciculus: It connects the motor speech areas (44 and 45) and the orbital gyri of the frontal lobe with the cortex in the temporal pole. The superior longitudinal fasciculus: It connects the frontal lobe to the occipital cortex (areas 18 and 19) and with the temporal lobe. The inferior longitudinal fasciculus: It connects the areas 18 and 19 of the occipital lobe with the temporal lobe. The fronto-occipital fasciculus: It connects the frontal pole to the occipital and temporal lobes. The white matter of cerebrum consists mainly of the myelinated fibers and are derived from the axons and their collaterals of pyramidal cells of the cerebral cortex.
Order silvitra uk
The pars compacta is cell-rich area and cells are medium and small multipolar neurons erectile dysfunction doctors augusta ga discount 120 mg silvitra otc. The nucleus of the trochlear nerve is present in the ventromedial area of the central gray matter iii. The mesencephalic nucleus of the trigeminal nerve gray matter in whole length of the midbrain b. It is ventral to the tectospinal tracts or slightly dorsal to the medial parts of the substantia nigra c. The fibers of the superior cerebellar peduncles arises from the dentate nucleus of the cerebellum d. Some of its fibers end in the red nucleus and other fibers ascend to the ventral lateral nucleus of the thalamus. Dorsal to the decussation of the superior cerebellar peduncles on each side of the median plane present following: a. The fibers of the trochlear nerve after arising from the trochlear nucleus pass dorsolaterally through the central gray matter medial to the mesencephalic nucleus of the trigeminal nerve to reach the upper end of the superior medullary velum where they decussate and emerge lateral to the frenulum. These are connected to the corresponding medial geniculate bodies of the thalamus by inferior brachium. Gives efferent fibers to the medial geniculate body then via the auditory radiation to the auditory areas (41 and 42) of the cerebral cortex 5. Crus cerebri: It is already described in the transverse section at the level of inferior colliculi. Substantia nigra: It is already described in the transverse section at the level of inferior colliculi. Edinger-Westphal nucleus: It is the part of the oculomotor complex supply the ciliaris muscle and the sphincter pupillae. The mesencephalic nucleus of the trigeminal nerve: It lies along the lateral part of the central gray matter. The fibers arise from the red nucleus and decussate to form the rubrospinal tract. It is connected with the corresponding lateral geniculate bodies of the thalamus via the superior brachium. It receives fibers from the cortex (from the areas 18 and 19) via the corticotectal fibers. It also receives fibers from the inferior colliculus which impulse is cochlear origin. To the nuclei of the oculomotor, trochlear and abducent nerves via the tectobulbar tracts. It controls the reflex movements of the eyes, head and neck towards the source of the sudden visual stimuli. Tumor of the midbrain or pressure on the midbrain by a tumor of outside origin often compress the cerebral aqueduct resulting hydrocephalus iv. The oculomotor and trochlear nerves nuclei and also corticospinal and cortico-nuclear tracts will be involved and provide symptoms and signs. It is caused by occlusion of a branch of the posterior cerebral artery resulting necrosis of the brain tissue affecting the oculomotor nerve and crus cerebri ii. There is ipsilateral ophthalmoplegia and contralateral paralysis of the face, the tongue, arm and leg iii. Eyeball deviated laterally due to paralysis of the medial rectal muscle, drooping (ptosis) of the upper eyelid, pupil is dilated and fix to light and accommodation. Parkinson`s disease (paralysis agitans): It is characterized by rigidity and tremor caused by degenerative changes in the substantia nigra and globus pallidus with marked reduction of dopamine in the striatum and substantia nigra. The vertebral arteries while pass through the suboccipital triangle it is winding in course and becomes clinically significant when blood flow through them is reduced, as occurs with arteriosclerosis ii. Under above condition, may cause dizziness and other symptoms due to interference of blood supply to the brainstem. The arteries convey deoxygenated blood from the fetus to the chorionic villi of the placenta. Later the right vein disappears and the left one persists to convey oxygenated blood from the placenta to the fetus, where it joins with the left branch of portal vein at the porta hepatis of liver. It is a mucoid connective tissue formed by the mucoid degeneration of the primary mesodermal cells of the connecting stalk. Distal part of the allantoic diverticulum: the distal part of the diverticulum is fibrosed to form urachus and the proximal part incorporates with the apex of the urinary bladder. It is a tubular cord-like structure connecting the body of the fetus with the placenta and carries fetal blood to and from the placenta. One end of the umbilical cord is attached approximately to the anterior abdominal wall other end to the center of the fetal surface of the placenta. Measurements Length (at full term) 50 cm Breadth (at full term) 2 cm Sometimes the cord is unusually long and may encircle the neck of the fetus producing strangulation or may prolapse in to the cervical canal, whereas a short cord may cause premature separation of placenta from the wall of the uterus during delivery. Presence of false knots because of umbilical vessels are longer than the cord therefore bending of the vessels are common and producing false knots 592 Human Anatomy for Students. The oval line of reflection appears between the amnion and embryonic ectoderm is known as primitive umbilical ring. Further development shows the amniotic cavity, and the amnion begins to envelop the connecting stalk and the yolk stalk (vitelline viii. The yolk sac present in the chorionic cavity is connected to the umbilical cord by its stalk. At the end of third month the amnion has expanded and comes in contact with the chorion, as a result obliterate the chorionic cavity. Approximately, the intestinal loops are drawn in to the body of the embryo and the cavity in the cord is obliterated when the allantois and the vitelline duct and its vessels are also obliterated. Between the choroionic and basal plates: Stem velli and intervillous space occupied with the maternal blood. Growth of the Placenta In the First Half of Pregnancy the placenta increases both in surface area and thickness. Pressure in the spiral arteries helps flow of blood in to the intervillous spaces and baths the numerous small villi of the villous tree in oxygenated blood. As the pressure decreases, blood flows back from the chorionic plate toward the decidua, where it enters the endometrial veins. Hence, blood from the intervillous spaces drain back in to the maternal circulation through the endometrial veins. The intervillous spaces of mature placenta contain about 150 ml of blood is replenished about 3 or 4 times per minute. However, placental exchange does not take fetal circulation is maintained between maternal and fetal circulations. This surface is marked by 15 to 20 slightly bulging areas called cotyledons which producing this surface is rough and irregular. Principal Margin It is continuous with the fetal membrane which consists from outside inwards: i. Storage Organ the placenta acts as a storage for glucose, calcium and iron in the first few months of pregnancy. Normal Site of Implantation of Ovum Normally, placenta is attached to the upper uterine segment, which includes the fundus and the greater part of the body of the uterus. The attachment of the placenta may extend partially or completely in to the lower uterine segment, which includes the lower part of the body and the cervix of the uterus, this condition is called placenta previa. First degree: the attachment of the placenta extend in to the lower uterine segment, but does not reach the internal os. Second degree: the margin of the placenta reaches the internal os, but does not cover it. Third degree: the margin of the placenta covers the internal os, but when the os dilates during childbirth, the placenta no longer occludes it. Fourth degree: the placenta completely covers the internal os, and occludes the internal os even after it has dilated. Interstitial tubal implantation: the placenta may get implanted in the part of the fallopian tube passing through the uterine wall. Layers of Placental Barrier Up to the Third Month of Pregnancy From fetus to mother: i. The placenta acts as transport of oxygen, water, electrolytes and nutritions between the maternal to fetal blood.
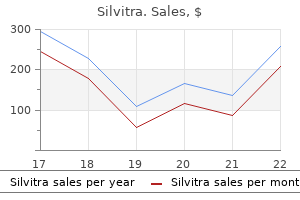
| Comparative prices of Silvitra | ||
| # | Retailer | Average price |
| 1 | H-E-B | 865 |
| 2 | Nordstrom | 913 |
| 3 | Albertsons | 175 |
| 4 | Michaels Stores | 853 |
| 5 | AT&T Wireless | 291 |
Generic silvitra 120mg amex
These values are contained on a chip which comes with the catheter and which is inserted in to the monitoring device erectile dysfunction treatment hypnosis purchase silvitra. Following insertion and fixation, an equilibration time must elapse before the measured values can be considered reliable and representative of cerebral oxygenation. Normally, the oxygen challenge test will lead to a substantial increase in brain tissue oxygen, thus confirming adequate catheter functioning [141]. Catheter malposition or malfunction should be suspected in the absence of a catheter response to increasing FiO2. Low values and an absence of response to an oxygen challenge test may be caused by a small local hematoma around the probe tip. The term "run-in time" was coined by the Rotterdam group and corresponds to the effective ptbO2 stabilization time after catheter insertion. This period represents the damage caused by the insertion of tissue oxygen catheter. Apparently, the run-in time is also affected by the presence of secondary injury factors. It is assumed that a longer run-in time period could be associated with hypotension and hypoxia. The accuracy, reliability and utility of this technique have been extensively studied in the clinical setting [15,18,10,142]. This may be interpreted as indicating that oxygen status may be disturbed at all levels of severity. Moreover, we should remember that tissue oxygenation is heterogeneous in both normal and pathologic situations [27,29]. It should be noted that the intent of ptbO2 monitoring as performed by the Rotterdam group was to monitor in a relatively undamaged part of the brain [15,144]. In contrast, the Houston group preferentially placed the catheter in close proximity to a brain contusion. Moreover, they found a significant relationship between lower ptbO2 values and outcome when the probe was positioned in the penumbra of (operated) mass lesions. Further studies are required to determine the pros and cons of monitoring in the penumbra versus in a relatively undamaged part of the brain where ptbO2 may be considered more representative of global cerebral oxygenation. The relationship between pupillary response and ptbO2 was studied by the Rotterdam group [15,144]. They found an association between lower ptbO2 values and a negative response of both pupils in the initial 24 hours after injury, suggesting an association between lower values and more severe injury. After 24 hours there was a mixed pattern and no apparent difference between lower and higher ptbO2. Although the relationship between lower blood pressure levels and poorer outcome is continuous, particular attention has been paid in the literature to episodes of systolic blood pressure 90 mmHg [8,100]. This is easily explained by the fact that hypotensive episodes may have been already corrected by the time that monitoring was initiated. Nevertheless, experimental and clinical studies have documented that ptbO2 monitoring after shock trauma can be a useful guide to improve oxygen delivery. Studies by the Rotterdam group have clearly shown lower values of ptbO2 in nonsurvivors versus survivors during the first 24 hours after injury [144]. Over the next days, however, there was no clear difference in the average values between the groups. According to the Rotterdam studies, low ptbO2 values are most often observed during the first 24 hours after injury. In a series of 100 patients, values <15 mmHg occurred in 57 patients, values <10 mmHg in 42, and values 5 mmHg in 22. It was subsequently suggested that this period can be characterized by "oxygen depression". In the 36-48-hours after injury, the average ptbO2 values increased to approximately 46 mmHg. This period was therefore considered to represent an "overshoot" likely due to vasodilation secondary to the initial ischemia. Over the following days, the average tissue oxygen remained stable at around 30 mmHg and was considered as the "stabilization stage". The three phases of evolution of brain tissue oxygen over time are summarized in Table 8. Further work is needed to determine appropriate thresholds for initiating treatment to improve cerebral oxygenation. Such critical levels may need to be individualized, as they can vary between patients and over time. Evolution over time is a highly relevant factor and not always recognized in studies. Many do not report the time of monitoring initiation [30], the stage of ptbO2 evolution [17,30], the duration of trends or report only average values [16,17]. We have found that an individualized analysis may yield additional relevant insights. The Rotterdam group found no relationship between patient age and ptbO2, whereas the Robertson group did [15,136]. This difference may be explained by the fact that they preferentially placed the probe in the penumbra of a damaged area, thus introducing bias toward older patients. The Stocchetti group described lower mean ptbO2 in the pericontusional tissue (19. The prognostic value of low ptbO2 values has been studied in multivariate logistic Regression analysis. These studies confirmed an independent prognostic effect of ptbO2; the probability of death increased 3. The local one was measured in the healthy brain, while the global parameter was positioned in the damaged brain. Lower ptbO2 values are also associated with poorer cognitive functioning in survivors, resulting in more problems in work re-integration [149]. These results clearly demonstrate an association between brain tissue hypoxia and increased mortality and poorer outcome in survivors [15, 142,144,150]. Thus, it would seem appropriate to prevent brain tissue hypoxia from occurring, and if it does, to correct it rapidly. The correlation between hypoperfusion induced by bleeding and ptbO2 is very close. The first trail tested the ptbO2 response on the initial 24 hours in comparison with the 72 hours response. The authors tested ptbO2 response only on a mean of 62 hours over time, ptbO2 increased 5 mmHg. Its practical efficacy will, however, be influenced by individual factors such as the time after injury and the degree to which autoregulation is disturbed [15,30,140,147,151]. The results from two studies illustrate the time-dependency of the effectiveness of increasing blood pressure [30,147]. Increasing blood pressure with norepinephrine during the "depression stage" after injury produced an average increase in ptbO2 of 7 mmHg, with a 30% increase in mean arterial pressure and improved cerebral perfusion. No data exist that specifically describe the response of ptbO2 to vasopressors during the overshoot phase. The Cambridge group described an increase of 5 mmHg after vasopressors administration at 72 hours after injury. This is not completely correct, however, as increasing blood pressure does not necessarily translate in to a reduction in ischemia. Hypoxic regions of the brain may not be capable of extracting sufficient oxygen due to oxygen diffusion gradients resulting in a diffusion barrier [152]. Microvascular collapse and vascular edema may contribute to this diffusion barrier [153]. The efficacy of increasing blood pressure to improve ptbO2 will also depend on the degree to which autoregulation is intact or disturbed [154]. Unfortunately, few cases have been studied during the critical period of the first 24 hours. Further studies are needed to identify which patient subgroups are at particular risk of ischemia and may likely respond to this treatment modality.
Silvitra 120mg with mastercard
In a retrospective study erectile dysfunction normal testosterone buy silvitra 120 mg otc, Imai and colleagues reported their experience on primary transluminal angioplasty and stenting in 28 patients with occlusive lesion of the intracranial vertebrobasilar artery within 7 days of onset. Nevertheless, 3 patients in each group died of myocardial infarction or anterior circulation stroke, and 1 endovascular patient had a non-fatal anterior circulation stroke. Another mechanical device, named the Penumbra System, was evaluated in a prospective, single-arm study within 8 hours of onset of stroke due to intracranial artery occlusion. Altogether, 21 arteries of 20 patients were successfully recanalized, the mortality rate was 45%, and good outcomes were seen in 45% of patients. Percutaneous transluminal angioplasty and stenting was performed in case of severe residual stenosis. Recanalization was achieved in 72%, a good outcome was seen in 34%, and the mortality rate was 38%. When there was persistent basilar artery occlusion, endovascular mechanical thrombectomy was performed to achieve recanalization. Of 16 patients, 15 achieved recanalization, 7 required mechanical thrombectomy, 4 were dead at 3 months, and 7 had a good outcome. In addition to supportive care and rehabilitation, secondary prevention should be achieved by effective control of vascular risk factors, use of a statin, use of antiplatelet agents in atherothrombotic strokes, and use of anticoagulation in cardioembolic strokes. Intracranial large artery stenosis, including basilar artery stenosis, carries a higher risk of recurrent stroke. Warfarin treatment cannot be recommended because of its association with a higher rate of myocardial infarction, sudden death and hemorrhage. Angiographically documented acute vertebrobasilar occlusion is a clinical catastrophe with a mortality rate approaching 90% despite standard medical therapy including anticoagulation. As new and newer modalities of therapy become available, randomized studies are required to prove the effectiveness of these treatment options. In addition, studies on outcome predictors and appropriate selection of newer therapeutic modalities are needed. A guidelines from the American Heart Association/ American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups. The Penumbra System: a mechanical device for the treatment of acute stroke due to thromboembolism. Transluminal angioplasty and stenting for intracranial vertebrobasilar occlusive lesions in acute stroke patients. Therapy of basilar artery occlusion: a systematic analysis comparing intra-arterial and intravenous thrombolysis. Results of a multicentre, randomised controlled trial of intra-arterial urokinase in the treatment of acute posterior circulation ischaemic stroke. Young patient have different characteristics from the adults and therefore deserve an independent analysis. From the public health point of view, stroke in young patients carries a great challenge not only for individuals but for society as a whole. The disability acquiered early in life means a significant loss of years of productivity of the patient, resulting in a significant economic burden for the entire population. In this chapter we review the epidemiology, more frequent etiologies and prognosis of ischemic stroke in young patients. Cerebral venous pathology and bleeding, as well as therapeutic alternatives in patients with stroke are treated in their respective chapters. The inclusion criteria for this study included: 1) individuals over 20 years of age; 2) diagnosis of first stroke; and 3) at least 3 months of residence in the area of northern Manhattan. Of these, 74 were individuals between 20 and 44 years of age with an estimated age-specific annual incidence of stroke of 23 per 100,000 inhabitants. Cardioembolic stroke is observed more frequently in adults; in comparison, younger patients have a higher rate of cryptogenic stroke. This suggests that the causes of ischemia in young patients are more heterogeneous and that the evaluation of this group should differ significantly from that of adult patients with typical cardiovascular risk factors. Subtype mechanism of ischemia in patients between 20 and 44 (white bar) and more than 45 years (black bar) of age at first stroke in the Northern Manhattan Stroke Study [Jacobs, 2002]. In younger patients, the relative risk of stroke in Hispanic or African-Americans is about 2. Even more significant are the racial differences observed in the Greater Cincinnati/Northern Kentucky Stroke Study which involved 3136 patients with first stroke. Relative incidence of first stroke by age in African-Americans as compared to whites in the Northern Manhattan Stroke Study [Jacobs, 2002]. Compared to Caucasians, the relative risk of first stroke in African-Americans was 2. Although the causes of these differences have not been determined, epidemiological studies suggest differences in vascular risk factors. Population studies show an increased prevalence and suboptimal control of cardiovascular risk factors (hypertension, diabetes, and obesity) in populations with low socioeconomic status and a higher prevalence of smoking in middle-high socioeconomic levels. The study used randomly generated telephone numbers for questioning the civilian outpatient population over 18 years of age. Subjects had to answer the question "Have you ever been told by a doctor or other health professional that you had a stroke On the basis of the data obtained from this survey, it has been estimated that the prevalence of cerebrovascular disease is 0. This suggests that the prevalence of this disease is in the general population underestimated. Due to the design of this study, no data are available for patients younger than 55 years. However, the prevalence of subclinical ischemic stroke in relatively young individuals (55-65 years) was 9. Similar to what was observed with incidence, the prevalence of ischemic stroke in relatively young African-Americans (55-65 years) was significantly higher (28. These results confirm that the prevalence of stroke in the general population, even in relatively young patients, is greater than estimated. The presence, severity and suboptimal control of these co-morbidities increase the risk of small-vessel atherosclerotic disease, large-vessel occlusive disease, cardiomyopathy, valvulopathy, and cardiac conduction disorders. A worrying observation is the exponential increase observed in the last two decades in the prevalence of vascular risk factors related to eating habits, sedentary lifestyle, obesity and diabetes. Population studies conducted in the United States indicate that these conditions affect mostly African-Americans and Hispanics. Cardiovascular risk factors are the pathophysiological basis for the vast majority of strokes in adults. In young patients suffering from cerebral ischemia, the prevalence of cardiovascular risk factors is significantly higher than in the general youth population. As in adult patients, the severity of these risk factors is directly related to the risk of developing cerebral ischemia. Causes of ischemic stroke in young patients (15-44 years) in the Baltimore-Washington Cooperative Young Stroke Study [Kittner, 1998]. As a corollary of this phenomenon, the vast majority of studies carried out to delineate the causes, evaluation, management and prognosis of cerebral ischemia have been conducted in groups of adult patients. However, as noted above, stroke in young patients differs significantly from that of adults. With a sample of 428 subjects, the Baltimore-Washington Cooperative Young Stroke Study is perhaps the largest epidemiological study carried out in 15 to 44 year-old patients with first stroke. The biracial population analyzed included approximately 60% of African Americans and 36% of Caucasians. In this study, about 50% of patients had at least one probable cause of stroke, 20% had at least one possible cause of stroke, and 30% had no probable or possible causes of stroke. Drug abuse, contraceptive use, thrombophilia and non-atherosclerotic arterial disease (including vasculitis and vascular dissection) are relatively uncommon causes of stroke in adult patients. However, in this study, these conditions were the etiologic factor for approximately 50% of cases of cerebral ischemia. Like other epidemiological estimates, vascular risk factors and causes of stroke vary with race or ethnic group studied. The most prevalent risk factors were hyperlipidemia (53%), smoking (50%), hypertension (46%) and family history of stroke (29%). Observed subtypes of stroke in epidemiological studies that include younger patients belonging to certain races or ethnic groups are summarized in Table 46. It is highly probable that the actual incidence is higher than that reported because most of the cases are asymptomatic or present with pain often considered "benign" and not investigated properly. It is estimated that between 10% and 25% of cerebral ischemia in patients under age 45 years are due to this disease, making arterial dissection of the second cause of stroke in young patients.
120mg silvitra overnight delivery
Origin It arises from the bifurcation of common carotid artery at the level of upper border of thyroid cartilage erectile dysfunction pills buy silvitra australia, opposite C3 and C4 vertebrae. From its origin to the base of the skull at the carotid canal through which it enters the skull ii. Superior cervical ganglion crossed by superior laryngeal nerve, close to the internal jugular vein iv. In the lower part, crossed by hypoglossal nerve, facial and lingual veins, posterior belly of digastric and stylohyoid muscles ii. In the upper part, covered by the parotid gland with external carotid artery, styloid process and its attached muscles iv. Then it emerges at the apex of petrous part and at the posterior part of the foramen lacerum iv. Then it passes upwards and medially above the cartilage covering the foramen lacerum Relations i. It begins from the foramen lacerum and passes upwards to the medial aspect of lingula of sphenoid bone ii. In the cavernous sinus, it is situated in a sulcus on each side of the sella turcica and runs forwards iv. Within the cavernous sinus, it lies on its floor and medial wall separated from blood by endothelium. Termination Finally, this part ends by piercing the dura mater forming the roof of the cavernous sinus between the middle and anterior clinoid processes. At first, it runs backwards along the roof of cavernous sinus in the subarachnoid space and lies below the optic nerve iii. Ultimately, it runs upwards on the side of optic chiasma to reach, anterior perforated substance iv. Its function is to maintain a regular flow of blood to the brain of damping down the pulsation of the artery. Anteriorly Internal carotid artery (between vein and artery lies 912 cranial nerves). Beginning It is the direct continuation of the sigmoid sinus from the base of the skull. End It joins with the subclavian vein and forms the brachiocephalic vein behind the sternoclavicular joint. After beginning the vein comes out from the skull through the posterior compartment of jugular foramen ii. Then, the vein descends downwards nearly vertical through the neck passing through the carotid sheath iii. Finally, it meets with the subclavian vein to form brachiocephalic vein behind the sternoclavicular joint. Right lymphatic duct, at the union of right internal jugular and right subclavian veins. This vein is easily accessible deep to the lesser supraclavicular fossa for introducing cannula or venous pulse tracing ii. The vein is markedly engorged and dilated in case of congestive cardiac failure or any disease when venous pressure is raised iii. As deep cervical lymph nodes are intimately related with the vein, it may causes followings: a. During removal of the lymph nodes in operation, a part of the vein is sometimes to be resected. Pulsations of the internal jugular vein may be palpable above the medial end of the clavicle during the contraction of the atrium b. Because of brachiocephalic vein and superior vena cava are valve less, a wave Head, Neck and Face 445 of contraction passes up through these vessels to the inferior bulb of the internal jugular vein. Before puncture, the internal jugular vein should palpate the common carotid artery c. The needle should introduce through the lesser supraclavicular triangle (between the sternal and clavicular heads of the sternocleidomastoid) upward and inward direction to avoid puncture of the pleural sac. The internal jugular vein acts as a guide for surgeons during excision of the deep cervical limb nodes vii. Sometimes internal jugular vein may required ligature to prevent spread of septic emboli from infected middle ear viii. For recording pressure in the right atrium, the right internal jugular vein is used because of this vein lies in a same line with the right brachiocephalic vein, superior vena cava and the right atrium. The articular surfaces are covered by the fibrocartilage but an intraarticular disk divided the joint cavity in to upper and lower parts. Below Mandibular neck: Between these attachments, it is also attached along the circumference of articular disk. Inferiorly, it is reflected upwards to cover the neck of the mandible and lateral pterygoid tendon to reach the articular cartilage of the condyle. The upper part allows gliding movements and lower part rotator and gliding movements vi. Below To the lateral surface and the posterior border of the neck of the mandible. Stylomandibular Ligament Attachments Above To the apex and adjacent anterior aspect of the styloid process of the temporal bone. Movements Depression Muscles involved Lateral pterygoid against resistance of both sides of a. Retraction Muscles involved Temporalis (posterior fibers) assisted by the middle and deep parts of both sides: 448 a. In this position, the mandible remains depressed and the person is unable to close their mouth iv. The reduction can be corrected by manipulation by giving pressure of thumbs on the lower molar teeth and pushing the jaw backwards. Temporomandibular joint arthritis: this joint may inflamed by degenerative arthritis which may cause dental malocclusion and joint clicking (crepitus) sound due to detached articular disk with pain during movements of jaw. The strong lateral temporomandibular ligament prevents dislocation of head of the mandible backwards and fracture of the tympanic plate when a severe blow falls on the chin. The head of the mandible occasionally dislocated forward caused by any sudden violence or during yawning due to sudden contraction of lateral pterygoid muscles ii. Epicranial aponeurosis or galea aponeurotica along with occipitofrontalis muscle iv. It is attached to the epicranial aponeurosis or galea aponeurotica through the dense superficial fascia. Posteriorly To the external occipital protuberance, and the superior nuchal lines. It is freely mobile on the pericranium along with the overlying adherent skin and fascia Attachments Anteriorly: It is attached to the insertion of the frontalis. Posteriorly: It is attached to the insertion of the occipitalis and also attached to the external occipital protuberance and to the highest nuchal lines. It is thin and continuous with the temporal fascia and attached to the zygomatic arch. Pericranium It is the periosteum of cranial bones and forms the fifth layer of the scalp. Attachments: It is loosely attached to the surfaces of the cranial bones and firmly attached to the sutures of the bones. Out of ten nerves, five nerves enter the scalp anterior to the auricle and remaining five nerves enter the scalp behind to the auricle. Posterior branch of great auricular nerve (sensory) from C2 and C3 of the cervical plexus b. Danger area (layer) of scalp: the layer of subaponeurotic loose areolar tissue (4th layer) is known as danger area of scalp. Any infection in this layer spreads quickly and may infect dural sinuses through the communicating emissary veins ii. Accumulation of blood due to any injury without producing much localized swelling. Wounds of scalp bleed profusely: When vessels of the scalp are torn in wounds they are unable to retract and produce profuse bleeding due to following reasons: i.
Syndromes
- Medical records for chronic illnesses or recent major surgery
- White blood cells, especially lymphocytes, the cells that attack bacteria in the blood
- Bowlegs
- Time it was swallowed
- Permanent scarring
- Protoporphyrin levels: 16 to 60 mcg/dL
- Low blood pressure
- Tell your health care provider if you have been drinking a lot of alcohol, more than 1 or 2 drinks a day.
- Avoid drinking alcohol whenever swimming or boating.
- Alcoholic cardiomyopathy
Order silvitra in india
Among the pituitary hormones erectile dysfunction 18 years old generic silvitra 120 mg otc, only prolactin secretion is increased in the absence of hypothalamic influence, since it is mainly under tonic suppression through prolactin inhibitory factor (dopamine) (Table 23. All anterior pituitary hormones are secreted in a pulsatile fashion and tend to follow a diurnal pattern. The blood supply of the hypothalamus is provided by the small branches of the arteries of the circle of Willis. Arterial supply to the anterior pituitary gland, median eminence, and stalk is derived from the superior hypophyseal arteries. These arteries form the primary vascular plexus and converge in to venules to form the long and short hypophyseal portal veins. These veins descend to the pars tuberalis and pars distalis of the anterior lobe, where a secondary plexus of sinusoidal capillaries is formed. The long portal veins pass through the diaphragma sella, thus being vulnerable to mechanical compression from brain or pituitary swelling or direct stalk injury. The anterior pituitary lobe, particularly its lateral aspects, receives its blood supply indirectly after passage through the median eminence and portal vessels. Any interruption of the portal vessels may result in anterior pituitary dysfunction. In contrast, the neurohypophysis receives its direct arterial blood supply from the inferior hypophyseal arteries. Components of the hypothalamic-pituitary-adrenal axis: hormones secreted by the pituitary gland, hypothalamus and target organs. Major physiologic effects of pituitary hormones and the clinical findings of pituitary hormone deficiencies. The brain, hippocampus and amygdala in particular, are closely involved in the stress response. The stress system also influences other hypothalamopituitary axes (those controlling gonadal, thyroidal, and growth functions) and exerts complex effects on immune/inflammatory reactions. The end hormones of the neuroendocrine system, particularly glucocorticoids and catecholamines, act to maintain behavioural, cardiovascular, metabolic, and immune homeostasis during stress. Following road accidents or during major surgery or sepsis, the human body can increase its glucocorticoid production by 5- to 10-fold. An adequate increase in glucocorticoid production is therefore crucial for survival and is required to cope with the severe stress during critical illness. Recent data revealed differences between alterations in hypothalamic-pituitary function in the acute phase (the first hours to days) and those in the prolonged phase or chronic phase (from 10 to 15 days beyond) of critical illness. During the acute phase, the secretory pattern of pituitary hormones inactivates anabolic target hormones. In prolonged critical illness when the patient continues under intensive medical care, the pulsatile secretion of the anterior pituitary hormones generally decreases because of decreased hypothalamic stimulation, and this underlies the impaired anabolism in critical care patients. Changes in circulating hormone levels become apparent during the first hours or days after trauma and may persist for the duration of the acute critical illness. These hormonal alterations reflect the acute adaptive response to the injury and may be influenced by the type of injury and pharmacological therapy given to treat the critical illness (glucocorticoids, narcotic analgesics or dopaminergic agents). The basic philosophy of the neuroendocrine response after acute brain injury may be summarized as follows: these adaptations are initially protective for the human body; however, if they are inadequate, as in pituitary dysfunction or excessive, they may be harmful and cause endocrine, metabolic and immune disturbances. Therefore, the most important target for intensive care should be to differentiate adaptive response from pathological hormonal changes and to avoid unnecessary interventions. These changes may persist up to 10 to 15 days after brain injury and are essential for maintaining vascular tone and endothelial integrity. Some investigators concluded that higher cortisol values are associated with more severe head trauma and with a worse clinical outcome, whereas others found lower cortisol values in the most severely injured patients with brainstem dysfunction or in brain-dead victims. The only difference between primary adrenal failure and secondary adrenal failure is the presence of mineralocorticoid deficiency. However, because the common clinical problem is due to hypocortisolism, it is not practical to differentiate primary from secondary adrenal failure in routine clinical management, commonly called adrenal failure. Although the data are heterogeneous, critically ill patients with nontraumatic brain injury may also experience adrenal failure. Therefore, such clinical signs/symptoms should prompt their urgent investigation as a possible cause of adrenal insufficiency during acute care. Algorithm for Diagnostic Testing and Management the adequacy of cortisol secretion in critical illness, including brain injury, remains a diagnostic challenge because the normal range for baseline or stimulated cortisol levels in critically ill patients is inadequately defined. Although a morning cortisol test is recommended by some authors, stress will decrease the normal diurnal variation in cortisol release, making random values acceptable. The actual concentration that defines a low value is somewhat controversial because of the expected increase in cortisol in response to brain-injury-induced stress. The amount of cortisol required cannot be predicted from the severity of injury and it may change as the clinical status changes. In patients lower values and clinical findings consistent with adrenal insufficiency, there is no need for further stimulation testing in routine clinical practice. As mentioned, differentiation between primary and secondary adrenal failure is not warranted in critically ill brain-injured patients in routine clinical practice. Algorithm for the management of adrenal insufficiency in brain-injured patients in the acute phase. But a recent study showed no positive correlation between this criterion and survival. Therefore, we do not recommend using this criterion in the diagnosis of adrenal insufficiency in patients with acute brain injury. Measurement of free cortisol has been suggested as a more accurate assessment of adrenal output. Several research groups have recently investigated the use of salivary cortisol concentration as a surrogate marker for serum free cortisol levels. Salivary cortisol measurement is simple to obtain and easy to measure in most laboratories. The data on the utility of salivary cortisol in critically ill brain-injured patients are currently insufficient. It is generally agreed, however, that therapy should be provided for patients with confirmed hypoadrenalism in whom clinical circumstances, such as hypotension, hyponatremia and hypoglycemia, warrant intervention. In patients with adrenal insufficiency as determined according to previously discussed criteria. Dexamethasone or methylprednisolone at equivalent hydrocortisone doses could be used as alternatives. It is important to note that dexamethasone does not have any mineralocorticoid activity. Addition of a mineralocorticoid is not usually required, but may be considered when hyponatremia is significant and the patient has proven primary adrenal failure. The Thyroid Axis Several changes in circulating thyroid hormone concentrations occur in acute critical illnesses including brain injury. The conversion of T4 (thyroxine) to T3 (triiodothyronine) in peripheral tissues is dramatically reduced and an altered form of T3, reverse T3 (rT3), is generated. These changes appear immediately after brain injury, 473 Intensive Care in Neurology and Neurosurgery can persist for at least 2 weeks and may normalize after the acute illness has resolved. True "central" hypothyroidism occurs in 4 to 15% of patients following brain injury. In critically ill burn or medical patients, acute thyroid hormone replacement therapy was not shown to produce short-term improvement. Therefore, based on current evidence we do not recommend thyroid hormone replacement in the acute phase of brain injury. In a recent randomized, prospective, double blind, placebo controlled study by Hatton et al. The magnitude of the decline in testosterone was correlated with head trauma severity in some studies but not in others. The current data suggest that these changes in the gonadotropic axis in the acute phase of brain injury are adaptive and transient; therefore, gonadotropin replacement is not recommended in the acute phase. Although the mechanism and the effects are not known, this response is thought to be adaptive. In critically ill patients, the main clinical findings are increased daily urinary volume (>3 litres) and hypernatremia.
Best purchase for silvitra
Due to the small number of patients studied erectile dysfunction medication shots order 120mg silvitra visa, it is unclear whether enzyme replacement can reduce the recurrence of cerebral ischemia. In heterozygous individuals with ischemic stroke the use of antiplatelet agents or anticoagulants (depending on the case) and the correction of vascular risk factors are recommended. In the nervous system, mitochondrial dysfunction and consequent energy deficit present with stroke-like episodes. Clinically the patient presents with neurological deficits that correlate with parenchymal brain lesions. On magnetic resonance imaging, these are typically hyperintense hyperintense on diffusion-weighed image sequences and apparent diffusion coefficient, suggesting the presence of vasogenic edema. These lesions are not located in a defined vascular area, have a predilection for the posterior regions of the brain and may progressively extend to other areas. It has been postulated that mitochondrial failure of intracerebral small vessels causes vascular dysfunction affecting the perfusion of the brain parenchyma (the "mitochondrial angiopathy" theory). Coenzyme Q10 is usually used alone or in combination with creatine and lipoic acid. The latter is related to the occurrence of stroke-like events and recurrent seizures. Several of these entities have therapeutic peculiarities that can considerably change the prognosis and natural history. It should be emphasized that the evaluation of these cases can be complex, extensive and expensive. Diagnosis and individualized plans for each patient are in the hands of the treating specialist who, according to personal experience, will select diagnostic studies at a reasonable cost. Nevertheless, these data should be analyzed carefully since the size of the samples is usually small. Studies based on administrative data show a lower mortality at discharge in young patients with stroke. Note: this table simply summarizes the most frequent complementary studies in the etiological diagnosis of stroke in young people. The goal is to simply provide a guide, not an exhaustive reference for the reader. The order of the studies should be individualized depending on the past medical history, family history, and physical exam findings. These data confirm that age is one of the two most important prognostic factors in patients with ischemic stroke (after stroke severity). As in adults, the prognosis in young patients depends, at least in part, on the degree of complexity of the disease and the experience of the medical team. Characteristics of patients younger than 55 years with stroke treated in Eastern and Western Stroke in Young Patients pared the mortality and disability (measured by the Barthel Index) at 3 months in patients younger than 55 years with stroke treated in Eastern Europe and Western Europe. A total of 201 cases were detected, which were uniformly distributed in the two study groups. In patients treated in Western Europe, where health care services are superior, the prognosis was significantly better than in those treated in Eastern Europe. These results confirm that, as in adult patients, the level of expertise of the medical centre, the intensity of treatment and quality of service provided in the acute post-stroke period all have a direct impact on the prognosis of young patients suffering from this condition. In younger patients, however, about 50% do not have these risk factors, suggesting the existence of alternative pathophysiological mechanisms. Identifying the cause of ischemia is the first step in developing therapeutic plan that will improve the prognosis of individuals with this devastating condition. Additional population studies are needed to precisely delineate the etiology, assessment, management and prognosis of adult patients with cerebral ischemia of different origins. Age-dependent differences in demographics, risk factors, co-morbidity, etiology, management, and clinical outcome of acute ischemic stroke. Stroke in the young: access to care and outcome; a Western versus eastern European perspective. Meta-analysis of genetic studies in ischemic stroke: thirty-two genes involving approximately 18,000 cases and 58,000 controls. Stroke epidemiology: a review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Nature and prevalence of pain in Fabry disease and its response to enzyme replacement therapy-a retrospective analysis from the Fabry Outcome Survey. Stroke in young patients with hyperhomocysteinemia due to cystathionine beta-synthase deficiency. Cerebral infarction in young adults: the Baltimore-Washington Cooperative Young Stroke Study. Prevalence of Fabry disease in patients with cryptogenic stroke: a prospective study. Circulation 2008; 117: e25-146 Saposnik G, Jeerakathil T, Selchen D, et al; Stroke Outcome Research Canada Working Group. Vascular involvement in a patient with mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes. The first presents epidemiological, anatomical and pathophysiological concepts, clinical manifestations and a diagnostic approach. The fifth and final section analyzes the treatment strategies for the frequent presentation of concomitant coronary and carotid disease. The approach to carotid artery disease is presented from a practical point of view, addressing problems of clinical relevance and a review of the available scientific literature. He mused that "it is conceivable that vascular surgery will some day find a way to bypass the occluded segment of an artery during the period of ominous transient symptoms. Since then, a growing body of scientific evidence endorses both medical treatment and surgical procedures for the reduction of cerebrovascular risks. According to international series, between 10 and 15% of ischemic strokes occur in a setting of carotid disease [4,5]. Of an estimated incidence of 100,000 ischemic strokes per year in Argentina, 11,000 could be due to carotid disease. The first segment is the cervical segment (C1), comprising the carotid bulb and the ascending portion. The C4 or cavernous segment begins at the petrolingual ligament, courses across the cavernous sinus and consists of three subsegments: posterior-ascendant, horizontal and anterior-ascendant. The union of the second subsegment with the first and third form the posterior and anterior genu, respectively. The C5 or clinoid is a short, wedge-shaped segment that begins at the proximal dural ring and ends at the distal dural ring. This notwithstanding, the relevance of the structural conformation of atheromatous plaque has recently been emphasized [11], which is why it seems more adequate to use the term "carotid artery disease" instead of "carotid stenosis". This dysfunction triggers the formation of carotid atheromatous plaque, which begins with cholesterol internalization and the incorporation of inflammatory cells in to the vascular wall [12]. Local rheological factors and shear stress produced by the blood flow on certain regions of the arterial tree such as the carotid sinus favor these pathological phenomena. Unless there is early intervention to reduce risk factors, the atheromatous plaque becomes increasingly vulnerable: reduced thickness of the fibrous capsule [13], ulceration, intraplaque hemorrhage due to vasa vasorum rupture, large necrotic lipidic core (>40%) [16,17] or in situ thrombosis [18]. Histologically, the vulnerable plaque shows an intense inflammatory-macrophagic infiltrate [19].
Buy line silvitra
The patient should be rechecked after 2 hours and feeding can be restarted if the gastric residual is less than the stated value shakeology erectile dysfunction buy silvitra 120 mg lowest price. This route of administration of nutrients may not be used in neurocritical patients because of the risk of aspiration. The tube should be placed distal to the Treitz ligament to decrease the risk of aspiration. The technique for tube placement may be blind (high failure rate) or by endoscopy, fluoroscopy or ultrasound-guided. The use of prokinetic agents facilitates, at least in theory, the passage of the pylorus, regardless of the technique. Also, these tubes can be positioned by invasive methods such as endoscopic percutaneous jejunostomy, radiological percutaneous jejunostomy and traditional surgery or by laparoscopy. Use of enteral nutrition, mainly jejunal nutrition, is suitable for early postoperative feeding, is safe and effective, as intestinal paralysis is predominant in the stomach and colon, and also it causes poor pancreatic stimulation. Bolus administration of hyperosmolar solutions in the small intestine can cause bloating, diarrhea and electrolyte disturbances. To avoid these adverse effects, volumetric pumps can be used and solutions with half of the desired concentration should be started at infusion rate of 50 ml/hour. If undesirable effects do not occur, then the gastrointestinal volume can be increased from 25 to 50 ml/hour every 24 hours until the daily volume is reached. The concentration of the solutions must be increased till the total osmolality of the nutritional formula is obtained. The most important limiting factor in intolerance to the diet is the osmolar load (intake per unit time) received by the digestive tract, so a gradual increase in the infusion rate, 410 Nutritional Support in Critically Ill Patients but not the concentration of the formula, is recommended, while maintaining a caloric density of 1 kcal/ml. Accordingly, protocols has been devised under which the quantity should be 20 ml/hour for the first 6 hours and then incremented by 10 ml/hour every 6 hours until the desired volume is reached, or to start with 20 ml/hour for 8 hours with increments of 20 ml/ hour every 8 hours until the infusion rate matches the requirements. If the patient develops diarrhea, and antidiarrhetic may be given, but if it persists or other adverse effects arise, feeding should be suspended for 48 hours. The presence of abdominal distention, diarrhea or other side effects have to be checked periodically. Homogenized diets are prepared with natural foods under technical homogenization; they differ from normal food only in consistency and method of administration through a catheter. These diets are prepared from milk, yogurt and ice cream, and other nutrients are added. Milk-based diets use milk as the main protein source and other sources of protein like eggs are added; calories are provided as lactose, dextrins, milk fat and soybean or corn oil. They are poorly tolerated in patients with disaccharidase deficiency and can cause diarrhea. Nonproteic calories are provided as oligosaccharides from glucose, dextrin and fat derived from soybean or corn oil. These diets are useful in patients with lactase deficiency, have low viscosity, and can be administered via small-calibre tubes. Nutritionally complete diets can be normal in protein, with a protein intake <20% of total calories, or high in protein, which contain 20% or more protein in relation to the supply of calories. Basic diets or formula-defined (monomeric or oligomeric) diets (also called chemically defined diets or peptides diets) are composed of nutrients that require minimal digestion, so they are easily absorbed by the duodenum and proximal jejunum. They consist of carbohydrates as oligosaccharides, sucrose and glucose, short-chain peptides (oligopeptides) or L-amino acids and medium-chain fatty acids, and small amounts of essential fatty acids and vegetable oils. These factors cause little gastric residue and small intestinal contents, which reduce the frequency of bowel movements and decrease colonic bacterial flora. Osmolality is high due to the low-molecular-weight nutrients; they are lactose-free and can be low in fat. They have a calorie density of 1 kcal/ml, reduce gastric acid secretion, but are expensive. They may be useful in patients with reduced inte411 Intensive Care in Neurology and Neurosurgery stinal absorption surface and in those with impaired digestion or absorption ability. They have high molecular density and may be useful in patients who require fluid restriction. Diets for special situations have been created to cover the nutritional needs in specific diseases. In addition, there are immuno-enriched diets with arginine or omega 3 fatty acids and diets enriched with glutamine which is involved in intestinal barrier integrity. Because of the vast variety of formulas for enteral nutrition, the diet composition and the proportion of different nutrients in the formulas should be reviewed before use. Intracranial insertion of the tube has been described in patients with skull fracture of the anterior fossa. These complications can be reduced with the use of flexible, small diameter tubes, changing the tube position and with the use of lubricants and topical decongestants. Also intestinal tract injuries can uoccur, such as: gastresophageal reflux, esophagitis, esophageal stricture, tracheesophageal fistula, rupture of esophageal varices, and mumps. Gastrostomy and jejunostomy include: technique-related complications, separation of the stomach or jejunum of the abdominal wall, surgical wound infections, cellulitis at the site of tube entry at the skin, abdominal wall abscess, necrotizing fasciitis, suture dehiscence and hernia, bleeding, gastric prolapse through the gastrostomy. Complications related to stroma care may cause skin irritation if there is extravasation of digestive juices. Other mechanical complications are: accidental tube displacement or migration, tube obstruction by foods or drugs (can be prevented by irrigating the catheter with 20 ml of water after use), and gastresophageal reflux due to lower esophageal sphincter insufficiency. Metabolic Complications Hypertonic dehydration is caused by hyperosmolar formulas that cause extracellular fluid leakage in to the intestinal lumen resulting in intracellular dehydration. Hyperhydration is due to the administration of large amount of liquids with the nutritional solutions, especially in patients with heart, renal or liver diseases. Hyperosmolality is a severe form of dehydration which occurs in elderly patients and situations of stress. Patients present as pseudodiabetics with sufficient reserves of insulin to prevent ketosis but inadequate to control hyperglycemia, resulting in polyuria, glycosuria, osmotic diuresis and nonketotic hyperosmolar coma. Tube feeding should be reduced or discontinued, and simple insulin and hypotonic fluids should be given. Essential fatty acid deficiency is when fat intake is inadequate or poorly tolerated. Hypoglycemia can occur in diabetic patientswho receive insulin or because of their disease (pancreatitis, stress, etc. Electrolyte imbalances can occur, with sodium, potassium, magnesium or other electrolyte impairment. Other possible complications are: hypoprothrombinemia, renal failure, and vitamin deficiency. Various factors are involved, such as inappropriate body position, gastric distension, formula consistency, osmolar load concentration, fat and amino acid concentration in the diet, as well as neuroendocrine imbalance or use of drugs that reduce gastric motility (anticholinergics, antacids, analgesics, sympathetic-mimetics, antihistamines, etc. When this complication appears, the diet should be temporarily suspended for 1 to 6 hours and prokinetic agents as metoclopramide or cisapride should be given. Vomiting or regurgitation is caused by gastric intolerance and problems related to diet such as osmolality, fat and bacterial contamination. They are more common in intermittent nutrition regimes (bolus) and agitated patients. When it occurs, the diet should be temporarily suspended, the causes determined and corrected, and prokinetic drugs initiated. Abdominal distension is caused by microbial contamination of the diet and an imbalance between nutrient supply and functional capacity of the intestinal tract, as well as intestinal diseases. Constipation is caused by increased intestinal water absorption in patients with inadequate blood volume or on a low-residue diet. Criteria to raise the diagnosis depend on stool frequency, consistency and volume (3 or more loose stools per day or >2000 ml/day). Infectious Complications Aspiration pneumonia is more common in patients with an altered level of consciousness, gastric retention, vomiting or regurgitation. The gastric content goes in to the lungs and causes injuries aggravated by the hyperosmolality and acidity of the aspirated content. It is necessary to determine if gastric retention occurs and if so, then nutrition must be suspended. Tracheal colonization is caused by gastric or nasopharyngeal flora that infect the lungs and cause nosocomial bronchopneumonia. This can be avoided by washing the tube after use; equipment and connections must also be changed daily, and the nutritional formula should not be retained for more than 4 to 6 hours at room temperature.
Purchase 120 mg silvitra visa
Inferior Extremity 317 Cutaneous Branches Along the lower one-third of the lateral side of the leg and greater part of the dorsum of the foot impotence groups order silvitra overnight. Medial Branch After passing the ankle joint it divides in to two dorsal digital nerves-one for the medial side of the great toe and other for the adjoining sides of the 2nd and 3rd toes. Lateral Branch Divides in to two dorsal digital nerves for the adjoining sides of the third-fourth and fifth toes. Termination It ends under the flexor retinaculum by dividing in to medial and lateral plantar nerves. Sural Nerve It is joined with sural communicating branches of the common peroneal nerve. Vascular Branches Supplies the arteries accompanying tibial nerve and its branches. Beginning It is the larger division of the sciatic nerve in the back of the thigh proximal to the knee. Tibial nerve injury is less common because it lies deeply in the popliteal fossa and posterior compartment of the leg. The nerve may be injured in case of posterior dislocation of the knee joint or deep lacerated injury in the popliteal fossa. Ligaments Fibrous capsule with synovial membrane Attachments At the hip bone Superiorly: It extends about 5 to 6 mm beyond the acetabular margin. Medial Band It is vertical attached to the lower part of the intertrochanteric line. Lateral Band It is oblique attached to the tubercle in the upper part the intertrochanteric line. Attachments Its apex is attached to the pit on the head of the femur, but its base is attached to the margins of the acetabular notch and also blends with the transverse acetabular ligament. Attachments Apex Blends with the capsular ligament and with the deep aspect of the medial band of the iliofemoral ligament. Base Attached to the iliopubic eminence, superior ramus of the pubis and to the obturator crest. Injuries to the hip joint: At young age: Green stick fracture of neck of femur and displacement of the head of femur. Sciatic nerve injury: Sciatic nerve may be injured in case of posterior dislocation of hip joint because hip joint posteriorly related to the sciatic nerve. Disease of the hip may cause referred pain on the knee due to common (femoral, sciatic and obturator) nerves supplying both the joints. It is caused by the under development of the acetabulum and head of the femur iii. Although dislocation occurs after birth, but the abnormality of the bones develops during intrauterine life iv. Correction: this condition must be diagnosed at birth with early treatment by splinting the joint in abduction, obtain excellent result. Effects: About 25 percent of the arthritis of the hip joint in adults is the direct result of residual defects from congenital dislocation of the hip joint. This injury is common among the childrens between the three to nine years of age ii. Fractures of the neck of the femur: It is the most troublesome of all the fractures. Radical hip replacement: It is indicated in severe traumatic injury and degenerative disease of the hip joint. The iliofemoral ligament is rarely torn during dislocation which helps in reduction of the joint. Modification of the capsular ligament Coronary ligament: the part of the capsular ligament between the menisci and the tibia sometimes called as coronary ligament. Other structures strengthened the capsular ligament Anteriorly: By the medial and lateral patellar retinacula. Attachments Above: To the adjoining margin and rough area on the lower part of the posterior surface of the patella. Oblique Popliteal Ligament It is present in the floor of the popliteal fossa in contact with the popliteal artery. Attachments Above: Lateral part of the inter-condylar line and lateral condyle of the femur. Anterior limb: Lateral condyle of femur and connected with the lateral head of gastrocnemius. Tibial Collateral Ligament Attachments Above: Whole of the medial epicondyle of the femur, just below the adductor tubercle. Below: Medial condyle of the tibia and upper posterior part of the medial surface with medial border of the shaft of the tibia. Fibular Collateral Ligament Attachments Above: Lateral epicondyle of the femur just above the groove for the tendon of the popliteus. Below: To the intermediate area on the proximal surface of the tibia, immediately anterior to the anterior attachment of the lateral meniscus. Below: Posterior part of the posterior intercondylar area of the tibia, just posterior to the posterior end of the medial meniscus.
Purchase silvitra overnight delivery
Extensor hallucis longus-from middle twofourths medial to the extensor digitorum longus erectile dysfunction shake cure discount 120mg silvitra free shipping. Anterior Border Character: Begins from the lower part of the anterior aspect of the head and ends below where it divides in to two limbs to form a triangular area at the lateral aspect of the lower end. Intermuscular septum between the extensor and peroneal muscles in upper three-fourths. Opposite the lower one-fourth this border divides to form a rough triangular area lies just above the medial surface of the lower end. Anterior and posterior tibiofibular ligaments- to the anterior and posterior limbs of the rough triangular area respectively. Interosseous membrane-from below the head to the apex of the rough triangular area. The lower end of the fibula projects downwards below the level of the lower end of the tibia and is known as lateral malleolus. Posterior Surface Character: It resents a vertical groove, which is bounded laterally by a sharp margin. Attachment: Superior peroneal retinaculum-at the lateral margin of the vertical groove. Inferior Border Character: It continuous with the anterior margin and presents a notch in its middle part. Primary center: One primary center for the shaft appears eighth week of the intrauterine life. Below and behind the triangular articular facet a deep nonarticular fossa called malleolar fossa. Articulation: Triangular articular facet articulates with the lateral surface of the body of the talus. Among the tarsal bones three cuneiform bones are wedge shaped and form an important part of the transverse arch of the foot. The talus forms the key bone amongst the tarsus and overrides the anterior part of calcaneus. Superiorly talus articulates with the bones of the leg and anteriorly with the navicular bone. Here calcaneus and talus form the bones of proximal row and the cuneiform bones form the bones of distal row. The navicular bone is interposed between the talus and cuneiform bones cuboid is placed laterally in front of calcaneus. Comma shaped facet on the medial surface Side Determination the triangular facet on the lateral surface of the body, will determine the side to which bones belongs. Its anterior or distal surface has a oval, convex articular surface which articulates with the proximal or posterior surface of the navicular bone iii. These are short bones seven in number and they form the posterior part of the foot ii. The bones are the talus, calcaneus, navicular, the medial, intermediate and lateral cuneiform bones and the cuboid 792 Human Anatomy for Students. Infront and lateral to the posterior impression there is another facet which articulates with the similar facet on the anterior part of the superior surface of the calcaneus c. Medial to the calcaneal facets a rounded impression, contact with the spring ligament or the plantar calcaneonavicular ligament. The neck and the body presents a certain angle, measured about 18 degrees Osteology 793 iv. The angle varies from 0 degree in old age to 30 degrees in newborn or may be as much as 50 degrees in clubfoot of new born Surfaces i. The capsular ligament of the talocrural joint (ankle joint) Plantar aspect of neck: Gives attachment to the interosseous talocalcaneal ligament. Lateral aspect of the neck: Gives attachment to the anterior talofibular ligament. Lateral surface Articulation: It is fully articulates with the lateral malleolus, bearing a triangular articular facet, the apex of which is directed downwards. Attachments: For lateral talocalcaneal ligament and posterior talocalcaneal ligament (lower margin). Posterior part: an ill-defined triangular area-articulates with the inferior transverse tibiofibular ligament. Anterior margin of the triangular facet give attachment to capsular ligament of talocrural joint and anterior talofibular ligament. Upper part comma-shaped articular surface- articulates with the medial malleolus b. Lower margin:Gives attachment to medial talocalcaneal ligament Posterior surface Features: It is rough, small, marked by a shallow groove, bounded by medial and lateral tubercles. Posterior process/tubercle Attachment: It gives attachment to the posterior talocalcaneal ligament. Movements: Above the talus, the movements are dorsiflexion and plantar flexion at the ankle joint. It helps to form three joints such as subtalar, calcaneocuboid and talocalcaneonavicular joint iv. It provides the leverage for the action of muscles (calf muscles) attached to the broader posterior surface v. Anterosuperiorly, there is a shelf-like projection, called sustentaculum tali Anatomical Position i. Anterior surface bears a concavoconvexo triangular facet looks forwards and upwards ii. Laterally, the superior surface bears a facet in its intermediate area looks upwards Side Determination Sustentaculum tali will determine the opposite side of the bone. Articulation: To the cuboid bone on the proximal surface, forming calcaneocuboid joint. Attachment: Its margin gives attachment to the capsular ligament of calcaneocuboid joint. The rough impression on the middle area gives insertion of the tendocalcaneus Ossification 1. Os trigonum: It is a condition sometimes during ossification the lateral tubercle of the Osteology 795 Medial Surface From above downward: a. Sustentaculum tali: It is a shelf like bony projection passes medial wards and forwards form anteromedial part and overhang the anterior part of the medial surface. The groove on the upper part of this surface transmits the tendon of the flexor hallucis longus b. The medial margin of the sustentaculum tali is attached to the tendon of flexor digitorum longus and provides attachments to: i. A slip of insertion of the tibialis posterior Plantar or Inferior Surface Features a. The anteromedial aspect of the lateral process: Gives origin of abductor digiti minimi f. Between anterior and posterior process/ tubercle: (A rough strip): Gives attachment to long plantar ligament h. The lower area: Gives attachment to some fibrofatty tissue 796 Human Anatomy for Students Lateral Surface Features a. The peroneal trochlea or tubercle: Gives attachment to the inferior peroneal retinaculum ii. The groove above the peroneal trochlea: Transmits the tendon of peroneus brevis and below it transmits the tendon of peroneus longus iii. The low rounded elevation behind the tubercle: Gives attachment to calcaneofibular part of the lateral ligament of the talocrural joint iv. Above and in front of the tubercle: Gives attachment to the lateral talocalcaneal ligament Dorsal or superior surface: It is also divided in to anterior, posterior and intermediate areas. Intermediate area: It occupies by the an oval facet, posterior facet for the talus. Attachments: the anterior part of the dorsal surface, (lateral part of nonarticular area)-gives attachment to: i. Fracture of the calcaneus: It occur when fall from a ladder on the heal or landing on the heel from high place ii.
