
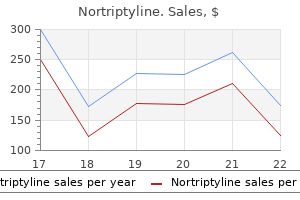
Nortriptyline 25 mg discount
Tumor masses are surgically resected and fragmented and the cells cultured with a T-cell growth factor anxiety symptoms knot in stomach nortriptyline 25 mg low cost, such as interleukin-2. Antitumor T cells can be selected, expanded, and then adoptively transferred into patients with cancer. Next-generation sequencing (whole exome and whole transcriptome) is performed on tumor and matched normal cells to identify nonsynonymous somatic mutations expressed by the cancer (left). At the end of the expansion, the beads are removed, and the cell culture can be either concentrated or cryopreserved until usage. An overview of the clinical results is provided below in Clinical outcomes of adoptive cell therapies. While the quest for the adequate candidates continues, several strategies have been attempted to improve safety and efficacy. Whether the abrogation of negative immune regulators would lead to increased challenges with control needs to be addressed in clinical trials. Summary papers are published every few years outlining recommendations with respect to the best practice guidelines for indications for allograft, though these remain controversial for many conditions, and continue to evolve over time as new data from clinical trials emerge. Checkpoint inhibitors are a class of drug that interrupt this interaction between the cancer cell and the T cell and allow the T cell to "see" the malignant cell and thus destroy it. He was treated with a checkpoint inhibitor (pembrolizumab), achieved a partial response, and was clinically well at 1 year since the commencement of pembrolizumab. Antimyeloma therapy has made incredible progress over the last decade, with the development of proteasome inhibitors such as bortezomib and carfilzomib; immunomodulatory drugs such as thalidomide, lenalidomide, and pomalidomide; and monoclonal antibodies targeting plasma cell antigens, such as daratumumab and elotuzumab. Subsequent trials employing modified T cells with higher-affinity binding achieved higher response rates (25%) but also demonstrated on-target off-tumor toxicity in many patients. There have also been some unexpected toxicities, some of them fatal, which have slowed the pace of progression. Lymphodepleting regimens commonly contain classic chemotherapeutic agents such as fludarabine, cyclophosphamide, pentostatin, or bendamustine. These drugs are often associated with nausea, fatigue, and other common side effects of chemotherapy and may cause cytopenias, which can predispose the patient to infection or bleeding. Thus, it seems that toxicity and efficacy with respect to lymphodepletion, in particular the inclusion of fludarabine, may be two sides of the same coin, and research into identifying the improved regimens for lymphodepletion is ongoing. Fractionated dosing also offers the added benefit of reduced morbidity in the event of an infusion-related adverse event. Despite this, patients remain clinically well, and the risk of opportunistic infection due to reduced humeral immunity is low and may be ameliorated by gamma globulin replacement. Aberrant/Unexpected Cross-Reactivity In rare cases, toxicity has occurred due to unexpected binding of modified T cells to an antigen expressed by a physiological tissue in vivo. After extensive investigation, it was found that the cardiac toxicity was due to cross-reactivity against a striated muscle peptide titin expressed in cardiac tissue. The manifestations of this toxicity vary from altered conscious state, encephalopathy, aphasia, seizures, and obtundation. It is generally "brief and self-limited, resolving over several days without intervention or apparent long-term sequelae",101 and can include atypical features such as word-finding difficulties in the absence of an identifiable cerebral vascular or inflammatory pathology. The mechanism of the neurotoxicity remains poorly understood; however, there is evidence of endothelial cell activation and disruption of the blood-brain barrier in 2 autopsy cases. The common manifestation of similar neurological toxicities despite the targeting of different antigens suggests that the toxicity is unlikely to be antigen-specific. Research is ongoing to improve specificity of the targets being recognized by the transfused T cells to reduce on-and off-target toxicity. The other route of relapse identified to date is via emergence of antigen-negative cells-that is, the emergence of a population of malignant cells that lack the antigen against which the modified T cells are targeted and are therefore immune to its surveillance and cytotoxic effect. It is unclear if these cells are present in the initial cancer and gain a selective advantage under pressure from the T-cell therapy or if they develop mutations to facilitate their survival. A detailed analysis of the public health considerations on the pricing of gene-modified cells is beyond the scope of this chapter, but some aspects have been summarized. The scientific community is intensively studying strategies to increase T-cell efficacy, to optimize T-cell production, to develop off-the-shelf T cells, to reduce clinical toxicity, to reduce T-cell exhaustion, to avoid tumor-microenvironment immunosuppression, and finally to test commercialization approaches. There is therefore much to be done in the field to ensure that most cancer patients respond in the long term. Immunotherapy is now a pillar of cancer treatment and will likely represent the backbone of future treatment algorithms. Combination treatments and off-the-shelf cellular products will hopefully also be available to patients in the next few years. Delivering these treatments to patients in a fair and sustainable way will be the next challenge. T-cell production has achieved high levels of efficiency; however, there is still a significant difference in efficiency between products, and studies are evaluating the expansion of T cells in the presence of small molecules potentially able to improve their effect in vivo. Other groups are selecting specific T-cell subsets that are potentially endowed with higher antitumor activity (naive, memory-stem cell subsets). Antileukemic effect of graft-versus-host disease in human recipients of allogeneic-marrow grafts. Allogeneic immunotherapy to optimize the graft-versus-tumor effect: concepts and controversies. Sorting through subsets: which T-cell populations mediate highly effective adoptive immunotherapy Early lymphocyte recovery predicts superior survival after autologous hematopoietic stem cell transplantation in multiple myeloma or non-Hodgkin lymphoma. Lymphocyte recovery after allogeneic bone marrow transplantation predicts risk of relapse in acute lymphoblastic leukemia. Biology and clinical effects of natural killer cells in allogeneic transplantation. Immune checkpoint inhibitors enhance cytotoxicity of cytokine-induced killer cells against human myeloid leukaemic blasts. Mining exomic sequencing data to identify mutated antigens recognized by adoptively transferred tumorreactive T cells. Different affinity windows for virus and cancer-specific T-cell receptors: implications for therapeutic strategies. Cardiovascular toxicity and titin cross-reactivity of affinity enhanced T cells in myeloma and melanoma. New strategies in engineering T-cell receptor gene-modified T cells to more effectively target malignancies. Editing T cell specificity towards leukemia by zinc finger nucleases and lentiviral gene transfer. Expression of immunoglobulin-T-cell receptor chimeric molecules as functional receptors with antibody-type specificity. Expression of chimeric receptor composed of immunoglobulin-derived V regions and T-cell receptor-derived C regions. Overcoming the immunosuppressive tumor microenvironment of Hodgkin lymphoma using chimeric antigen receptor T cells. Targeting the tumour profile using broad spectrum chimaeric antigen receptor T-cells. Complete remission of lung metastasis following adoptive immunotherapy using activated autologous gammadelta T-cells in a patient with renal cell carcinoma. Induction of antigen-specific T cell anergy: an early event in the course of tumor progression. Alterations in signal transduction molecules in T lymphocytes from tumor-bearing mice. Myeloid-derived suppressor cell impact on endogenous and adoptively transferred T cells. Adoptively transferred immune T cells eradicate established tumors despite cancer-induced immune suppression. Effectiveness of donor natural killer cell alloreactivity in mismatched hematopoietic transplants. Chimeric antigen receptor T cells persist and induce sustained remissions in relapsed refractory chronic lymphocytic leukemia.
Discount nortriptyline generic
Unless this is per formed while the pelvis is distended anxiety in dogs generic 25mg nortriptyline free shipping, it is easy to mark it wrongly. Cut through the ureter near the pelviure teric junction, and thread it behind the lower pole vessels, slit up, and spatulate in the lateral aspect. It is important to use only absorbable suture material for the anastomosis, but whether interrupted or continuous sutures are used is of little consequence. If there is no lower pole vessel, there is no need to detach the ureter and either a simple flap or the Culp spiral modification can be adapted. Using either method, the anastomosis is made in a long ellipse to prevent subse quent contraction, and there must be no tension. To some extent this kind of result, which is fortunately rare, represents a failure of selection of candidates for an operation; in retrospect, it is easy to say that it would have been better to have advised a nephrectomy. In the majority, the outcome is excellent in terms of the absence of symptoms, infection, stones, and dete rioration of renal function, but when assessed by the appearance of the kidney in a urogram, the patient and the surgeon need to be warned that the kidney often continues to look disappointingly dilated. However, it does mean that once there has been a thinning of the renal paren chyma and a deterioration in the muscular capacity of the renal pelvis, then the pyelographic appearances are unlikely to return to normal. This need not mat ter; the important point is that the obstruction has been permanently overcome and things will not dete riorate any further. This is a rare anomaly where the ureter surrounds the vein at the level of the third and fourth lumbar vertebra. It almost invariably affects the right ureter, and its pres ence should be suspected with a Sshaped ureter on imaging. Type I is more common (90%) and results in hydronephrosis due to compression of the ureter between the inferior vena cava and the vertebra. Management of obstruc tion is surgical with either open or laparoscopic pyelo pyelostomy with transposition of the ureter anterior to the inferior vena cava. Nearly 1% of postmortem examinations have been found to show upper urinary tract duplication to varying degrees [34]. Duplication anomalies show an incomplete penetrance and are an autosomal dominant trait affecting 8% of member of affected fami lies. The majority of upper tract duplications unite above the ureteric orifice and usually have minimal clinical man ifestations. On the contrary, complete duplications often cause symptoms and affect renal functionality. In incomplete ureteric duplication, the ureteric bud arises normally from the mesonephric duct but then undergoes variable degrees of bifurcation. Complete duplication occurs when two separate ureteric buds arise separately from the mesonephric duct. The inci sion can be done by either an endopyelotomy knife or laser through either percutaneous or ureteroscopic approaches. Success rates do not approach that of lapa roscopic or robotic pyeloplasty but have been shown to be as high as 87. Antegrade (via percutaneous tract) and retrograde approaches have been described as well as retrograde cautery wire balloon endopyelotomy and balloon endodilatation. The benefits include shorter operative time with reduced hospital stays and postoperative recovery. Upper moiety ureters are usually associated with dysplastic nonfunctioning upper renal moiety. Ectopic ureter is any ureter, single or duplex, that does not enter the trigonal area of the bladder. In females, the ectopic ureter may be suprasphincteric, at the level of the striated sphincter, or distal either at distal vagina or introitus. In contrast, male ectopic ureters are always suprasphincteric, connecting to the seminal vesicles, ejaculatory ducts, or the vas deferens, causing pain and infection rather than urinary incontinence clinically. These can also be single or duplex systems (usually in the ureter drain ing the upper pole moiety). There are several classifica tions of ureteroceles with the most clinically useful being intravesical (entire ureterocele above bladder neck) or extravesical (some part of ureterocele permanently at bladder neck or urethra). It will easily identify upper tract dilatation in both a single and duplex system, as well as help differentiate a dilated the lower moiety ureter (the MeyerWeigart law). This can lead the upper moiety to ectopic insertion, which may the urethra or the urogenital sinus. The ectopic ureter is prone to obstruction because of its long intramural course through the bladder wall, which can cause severe hydronephrosis. The goals of therapy are preserva tion of renal function, elimination of obstruction, infec tion and reflux, and maintenance of urinary continence. However, if the renal moiety is poorly functioning, a heminephrectomy and ureterectomy would be the treatment choice. Normally a physiological sphincter is formed by the ureters passing obliquely through the bladder wall for about 2 cm. Other causes include ureteric reimplantation without antireflux techniques or incis ing a ureterocoele open. High bladder pressure leading to significantly high bladder pressures, overcoming the physiological sphincter mechanism. Smith classified megaureters into four categories: obstructed, refluxing, refluxing with obstruction, and nonrefluxing and nonobstructing [37]. The challenge with this condition is to promptly treat obstructing ure ters and preventing unnecessary intervention in dilated nonobstructing stable ureters. Nonobstructive megaureters can be safely observed with serial sonography and the majority resolve spon taneously within the first two years. Studies have shown that ureters greater than 10 mm prove more difficult to manage and only 17% resolve with 21% of cases requiring surgical intervention [39]. The procedure of choice for babies older than one year old is ureteric reimplantation with or without ureteral tapering. In grossly dilated ureters in infantile bladders of babies younger than one, temporising methods such as ureteric stenting, endoscopic balloon dilatation, endouretostomy, cutaneous ureterostomy, and refluxing ureteral reimplantation is favoured. The upper normal limit diameter of the ureter in Ureteral strictures can be either congenital (rare) or acquired. The acquired causes include ureteral calculi, traumatic surgical instrumentation, malignancy, radia tion, ischaemia, infection, and periureteral fibrosis. Ureteroscopic damage to the ure ter causes a flap or perforation or ureteric anastomoses. For exclusion of malignancy, retrograde pye lography and ureteroscopy with or without biopsy is commonly necessary. Endourological treatments include: Ureteral stent placement: indicated in the sympto matic frail elderly patient Balloon dilatation or endoureterotomy If these treatments are unsuccessful, or in carefully selected patients, ureteric reconstruction according to site and size of disease and patient factors can achieve good success rates. Nephrectomy is also an option if the renal function is poor (<15%) Expert Opinion There are many causes for hydronephrosis, spanning both benign and malignant conditions. It is essential to thoroughly investigate to better determine the pathological process causing it and help establish either definitive treatment or further investigations. Its relation to pelvic reabsorption, to hydronephrosis and to accidents of pyelography. Relationship between renal blood flow and ureteral pressure during 18 hours of total unilateral uretheral occlusion: implications for changing sites of increased renal resistance. Altered expression of major renal Na transporters in rats with 11 12 13 14 15 16 17 18 bilateral ureteral obstruction and release of obstruction. Recovery following complete chronic unilateral ureteral occlusion: functional, radiographic and pathologic alterations. Recovery of distal nephron enzyme activity after release of unilateral ureteral obstruction. The Society for Fetal Urology consensus statement on the evaluation and management of antenatal hydronephrosis. Ureteropelvic junction obstruction: its occurance in 3 members of a single family. Prenatally diagnosed 30 31 32 33 34 35 36 37 38 39 hydronephrosis: the Great Ormond Street experience. British Association of Paediatric Urologists consensus statement on the management of the primary obstructed megaureter.
Diseases
- Boucher Neuhauser syndrome
- Flavimonas oryzihabitans
- Stickler syndrome, type 3
- Fibrosarcoma
- Hyperferritinemia, hereditary, with congenital cataracts
- Ceroid lipofuscinois, neuronal
Discount nortriptyline 25 mg online
Pancytopenia is com mon anxiety quiz buy nortriptyline 25 mg mastercard, as a result both of the replacement of normal bone marrow and of the defective capacity for maturation of the leukaemic clone. The neoplastic clone is characterized by defective maturation so that haemopoiesis is usually both morphologically dysplastic and functionally inef fective. This process, which leads to various combinations of anaemia, neutropenia and thrombocytopenia, is designated ineffective haemopoiesis. The myelodysplastic syndromes may therefore be regarded as preleukaemic conditions. In different patients, cells of the leukaemic clone show various patterns of differentiation and maturation. As a consequence of pancytopenia, patients commonly exhibit pallor and bruising and show susceptibility to infection. A normal or low count is most often observed in acute promyelocytic leukaemia, acute megakaryo blastic leukaemia and acute panmyelosis with myelofibrosis. In adults, acute megakaryoblastic leukaemia commonly presents with the features of acute myelofibrosis, i. The bone marrow trephine biopsy is of secondary impor tance except in those cases in which an adequate aspirate cannot be obtained. It is based on the pattern of differentiation shown (for example: granulocytic, monocytic, erythroid, megakaryo cytic) and the extent of maturation (for example: myeloblast, promyelocyte, granulocyte). Both dif ferentiation and maturation are assessed and the predominant cell types in peripheral blood and bone marrow are determined. Acute myeloid leukaemia occurs at all ages but becomes increasingly common with advancing age. The incidence rises from one to 10 per 100 000 per year between the ages of 20 and 70 years and is somewhat higher in men than in women. It can also be essential for the recognition of pure erythroleukaemia since the primitive cells may be cytologically unrecogniz able. In addi tion, flow cytometry provides a means of identi fying minimal residual disease during followup if a specific leukaemiaassociated phenotype is demonstrated at diagnosis. It has declined in importance since immu nophenotyping became widely available but retains a role when flow cytometric immunop henotyping is not readily and rapidly accessible. However, when the peripheral blood features are not diagnostic and bone marrow aspiration is difficult or impossible it can be essential for diagnosis. This is most likely to occur when there is either a hypocellular bone marrow or fibrosis. The marrow is hypocellular with preservation of fat cells; however, normal haemopoietic cells are not seen. Fibrosis, either reticulin or collagen, generally prevents an adequate aspirate and trephine biopsy histology is then essen tial for diagnosis. Occasionally, in patients presenting with myeloid sarcoma, there is nodular infiltration with intervening marrow being normal [13]. It is our practice to per form immunohistochemical staining whenever there is diagnostic difficulty, for example when bone marrow aspiration has failed and there are only low numbers of circulating blast cells. It is also possible to use immunohistochemistry to establish the baseline immunophenotype to permit compari son with followup samples. The presence of hypogranular neutrophils may provide a clue to the myeloid nature of the leukaemia. The granulocytic differentiation may be mainly neutrophilic or mainly eosinophilic. The diagnosis can often be made from cytological features but is facilitated by a double esterase stain. There is an excess of immature erythroid cells, some of which have characteristic elongated nucleoli abutting on the nuclear membrane. In patients with fibrosis, aspiration may be difficult or impossible; histology and immunohisto chemistry are then important in the diagnosis. Peripheral blood the peripheral blood may show large blast cells with basophilic cytoplasm, a prominent Golgi zone and often a single, long, thin Auer rod, together with mor phologically abnormal maturing cells (mainly neutro philic lineage but sometimes including eosinophils). In addi tion to dysplastic maturing cells of neutrophil line age, there are often increased eosinophils, which are usually cytologically normal. Cytochemistry Cytochemistry is not usually essential since granu locytic differentiation is obvious. Bone marrow histology There is usually a marked increase in cellularity with both increased blast cells and maturing cells of neutrophil and eosinophil lineages. Acute myeloid leukaemia with recurrent cytogenetic abnormalities Acute myeloid leukaemia with t(8;21) (q22;q22. Cytogenetic and molecular genetic analysis Cytogenetic analysis shows t(8;21)(q22;q22. Peripheral blood the peripheral blood usually shows blast cells and maturing cells of monocyte lineage. The cells of eosinophil lineage are a mixture of myelocytes and mature eosinophils. In the great majority of cases the eosinophil myelocytes are morphologically abnormal with prominent proeosinophilic gran ules, which are basophilic in their staining char acteristics, mixed with typical eosinophilic granules. The mature eosinophils may show cytological abnormalities such as nuclear hyper lobation or hypolobation or the presence of occa sional proeosinophilic granules. There is usually retention of maturation in the monocyte lineage so that mature monocytes Acute myeloid leukaemia with inv(16) (p13. Bone marrow histology Trephine biopsy sections show a hypercellular marrow with the same abnormalities as described in the aspirate. The abnormal promyelocytes are large cells, usually two to three times the diameter of an erythrocyte. The nucleus is round, oval or bilobed but cytoplas mic granulation is so marked that the nuclear outline can be difficult to discern. Abnormal promyelo cytes are characteristically more frequent in the peripheral blood in the variant form than in cases with hypergranular promyelocytes. The nucleus is usu ally deeply lobed, often with two large lobes joined by a narrow bridge. The cytoplasm is usually weakly or moderately basophilic but some cases have pro myelocytes with more marked basophilia and cyto plasmic protrusions or blebs. A careful search in cases of the variant form often discloses a minor population of more typical, hypergranular promye locytes, occasionally with multiple Auer rods. Immunophenotype Flow cytometric immunophenotyping shows a mixed population of cells. Cytogenetic and molecular genetic analysis Cytogenetic analysis shows either inv(16)(p13. The most frequent additional abnormalities are trisomy 8 and trisomy 22 (the latter fairly specific for this subtype). Molecular analysis is diagnosti cally important since the cytogenetic abnormality is subtle and can be missed. Rapid, correct diagno sis is of critical importance so that specific targeted treatment can be used and early death from haem orrhage avoided. However, the bone marrow aspirate is important in diagnosis since there may be only infrequent leukaemic cells in the peripheral blood and, in the variant form, the bone marrow often contains a higher proportion of typi cal hypergranular cells than does the blood. The predominant cells may be hypergranular promye locytes or hypogranular bilobed promyelocytes with a variable admixture of hypergranular forms. Erythroid cells and megakaryocytes are also considerably reduced in number but are cyto logically normal. Cytochemistry Cytochemical stains are unnecessary in typical hypergranular acute promyelocytic leukaemia but 201 can be important in confirming a diagnosis of the variant form. The leukaemic cells have a characteristic appearance; they have prominent large granules that fill the cytoplasm and often obscure the nucleus. In the variant form the granules are much smaller and may be inconspicuous; the nuclei are often bilobed. Because of their hypergranularity, the leukaemic cells of typical cases can be readily recognized in haematoxylin and eosin (H&E)stained sections of trephine biopsy specimens. A proportion of cases of the variant form can also be recognized from cyto logical features. There is an accompanying reactive increase in small blood vessels in the bone marrow stroma [17]. During follow up after treatment with arsenic trioxide, increased osteoblasts surrounding trabeculae have been observed [21].
Purchase nortriptyline 25 mg free shipping
Acute rejection can also anxiety before period order nortriptyline 25mg without prescription, less commonly, be predominantly mediated by antibodies (humoral rejection). Acute rejection can be initiated by failure to take the drugs, infection, or a blood transfusion. Transplant biopsy is required, showing dense cellular infiltration and oedema and can determine the type of rejection and its severity. Biopsy shows interstitial the immune response mounted depends on antibodies, unspecific cellular reactions as well as specific cytotoxic cells and cytokines. Antibodies can fix complement, especially complement component 4d (C4d), which recruits macrophages and activates endothelial cells. The point of entry, and therefore, the site of the most severe inflammatory reaction and destruction is the endothelial structure of the graft. Destruction of the small vessels of the graft occurs primarily and can be seen histologically while parenchymal changes are secondary to destruction of the vasculature. Chronic rejection is a slow process which seems to occur in many renal transplants over the years and is held responsible for the slow but steady decline of transplant function starting many months or years after successful transplantation. They also inhibit the migration of monocytes to areas of inflammation such as acute rejection. Prednisone and prednisolone are metabolised in the liver where prednisone is converted to prednisolone. Their halflives are increased in hepatic disease and shortened if taken together with drugs that induce hepatic enzymes. Side effects of steroids are numerous, and considerable and most protocols today aim at tapering the steroid dose shortly after transplantation or using a steroidfree maintenance protocol. Both calcineurin inhibitors are given orally, and drug levels have to be controlled. This can occur early in kidneys with marked ischemic damage or within weeks associated with high serum levels, or there can be late, chronic nephrotoxicity, leading to progressive loss interstitial graft fibrosis. Gastrointestinal side effects (diarrhoea, indigestion, and reflux) and bone marrow toxicity occur. Sirolimus (rapamycin) is the product of a microorganism first isolated from soil from the Easter Island (Rapa Nui), giving it its name, and everolimus is a synthetic analogue. Specific side effects are changes in lipid metabolism, delayed graft function, bone marrow suppression, and disturbed wound healing [23]. It is catabolised by xanthine oxidase, and thus, there is an interaction with allopurinol. Azathioprine has been largely replaced by mycophenolate, but it is an inexpensive drug still used in many countries. By immunising animals with human lymphocytes, heterogenous polyclonal sera can be obtained, which contain many antibodies with largely undefined specificities. Polyclonal antibodies react with many different antigens and the animal proteins can cause allergic or anaphylactic responses. With cell hybridization, monoclonal antibodies (mAb), which suppress Tcells and their subsets, are available. It mediates complement dependent cell lysis and rapidly clears Tcells from the circulation. Polyclonal and monoclonal preparations with antiT cell antibodies are used for the treatment of steroid resistant rejection. Infectious agents not dangerous to immunocompetent hosts can be lifethreatening in transplant recipients. The incidence of de novo malignancies is increased about 10fold with immunosuppression, the most common being skin cancers. Induction immunosuppression is intensive treatment used to suppress immune responsiveness at the time of transplantation. Maintenance treatment is less potent but is tolerable for longterm use in a steady state. It is given as an induction treatment and during the first weeks after transplantation. Induction treatment should be an individualised decision because side effects can be severe. Most centres have their preferred maintenance regimen based on experience which is adjusted to individual circumstances (Table 8. All immunosuppressive agents have side effects which occur with time even after years of treatment. Corticosteroids induce diabetes, osteoporosis, obesity, and other unwanted effects. Conception is possible after the first transplant year, provided immunosuppression is stable, and there have been no rejections. There are very few data on any effects of immunosuppression on intrauterine development or during breast feeding. Immunosuppression and compliance with treatment, especially in children and adolescents, need to be supervised. Maintenance immunosuppression requires blood level measurements at defined intervals. Limitations are the need for lifelong immunosuppression and chronic graft failure, which limits the survival of a graft in most patients. Kidney graft survival in Europe and the United States: strikingly different longterm outcomes. European Renal Best Practice Guideline on kidney donor and recipient evaluation and perioperative care. Each additional hour of cold ischemia time significantly increases the risk of graft failure and mortality following renal transplantation. Endovascular interventions for managing vascular complication of renal transplantation. Influence of test technique on sensitization status of patients on the kidney transplant waiting list. Modulating Tcell costimulation as new immunosuppressive concept in organ transplantation. During the fourth and fifth weeks of gestation, the ureteral bud begins to develop from the distal portion of the mesonephric duct. The cranial end of the ureteric bud meets the metanephrons and continues in its cephalic migration. During this process, it forms the pelvis, calyces, and part of the collecting ducts. At the same time, the metanephros differentiates into organised renal parenchyma around the collecting system. The blood supply changes during the migration; initially the kidneys are supplied by the middle sacral artery, then by the common iliac, and finally by the aorta [2]. If a complete ureteric duplication occurs (around 50% of cases), the supernumerary kidney is likely to be cranial. There is usually one extra kidney, but cases of multiple extra kidneys have been reported. The supernumerary kidney has its own blood supply and capsule, is usually smaller, less functioning, and in a third of cases, is associated with other pathological changes. Many cases remain asymptomatic throughout life and are picked up incidentally on ultrasound. When complications occur, these are generally correlated with obstruction or infections and presents with typical symptoms of pain, abdominal mass, or fever [3]. Most of those are asymptomatic, but hydrocolpos or hematocolpos due to a blind vagina might develop at puberty with a pelvic mass or cyclical pain or cryptomenorrhoea.
Purchase 25 mg nortriptyline amex
Bilateral osteotomies are performed because usually the closure is delayed and the pubic diastasis is wide anxiety symptoms breathing buy 25 mg nortriptyline with amex. These should allow for a tensionfree closure, but if this is not possible, then the use of a silo to cover the residual abdominal wall defect is advisable. Preserving as much bowel tissue possible is essential to enhance absorption and avoid complications of short bowel, thus helping the survival rate of these patients [59]. Also, any possible distal bowel and appendices should be preserved because they may be used for future reconstruction and stoma formation. When the child is older and if an adequate hindgut exists and there are no neurologic deficits, then a pull through procedure could be performed via the posterior sagittal approach. The majority of these patients however have been reported incontinent of faeces [4, 45]. Intermittent catheterization is likely to be needed for emptying especially in the presence of spinal defects. Surgery to produce a continent reservoir should be delayed until the child is old enough to participate in selfcare. The choice between a catheterisable urethra and catheterisable stoma should be made according to the adequacy of the urethra and bladder neck, bladder capacity, gender, and orthopaedic status [60, 61]. However, when adequate corporal tissue is present, epispadias repair can be performed at the same time of initial closure or later [62]. Also, when performed by experts, the Kelly procedure offers a great perspective in the cosmetic appearance of the external genitalia of boys [4]. Genital reconstruction in girls is usually done at the time of bladder closure and osteotomy. It is acceptable to leave the vaginas in situ, but further surgery will be needed to bring one of these to the perineum. This is called a vesicourachal diverticulum and is asymptomatic; very rarely it can be cause of infection or stone formation due to urinary stasis within. If the umbilicus becomes infected, then there is periumbilical swelling, tenderness, and drainage. The excision is done through an extraperitoneal approach and the urachus needs to be excised completely, including a part of the bladder dome. Episodic infections of the sinus can lead to purulent drainage from the umbilicus and periumbilical tenderness. Treatment is again complete excision if the sinus persists for more than two months [65, 66]. It is usually an incidental finding, or it can present as a suprapubic mass with fever, pain, and dysuria. In delayed diagnosis, the cyst may rupture towards the peritoneum, causing acute abdomen and peritonitis. The most common organism isolated is Staphylococcus aureus (in >50% of cases) [67]. For very inflamed cysts, initial incision and drainage (twostage approach) is preferable [67, 68]. The treatment of asymptomatic remnants remains controversial, but it is suggested that the presence of microcalcifications seen in imaging is in favour of excision [67, 75]. These calcifications seem to be related to chronic inflammation, which maybe in turn a predisposing factor for carcinogenesis. Cystoscopy shows a cherrysized lump at the air bubble, and a much larger mass outside it; biopsy reveals adenocarcinoma. Therefore, many surgeons favour preventive removal of urachal remnants when diagnosed. In the adult male, they commonly accompany an inguinal hernia into the inguinal canal. It can also be related to other conditions such as posterior urethral valves, Ehlers Danlos syndrome, and urethral diverticula. It presents more commonly with functional neonatal intestinal obstruction and urinary retention [84]. It can be partial or complete, with the duplication being in the sagittal or coronal plane. In complete duplication, there are two hemibladders usually in a sagittal plane, with the corresponding ipsilateral ureter draining within each hemi bladder and in continuation with a duplicated urethra. Associated anomalies include a duplicated penis, duplicated vagina and uterus, vertebral anomalies (usually lumbar), and hindgut anomalies. Congenital diverticula are usually solitary and usually located near the ureteric orifice [81]. The most common causes are urethral valves, urethral strictures, neuropathic bladders, detrusorsphincter dyssynergy, or can occur after antireflux surgery. Diverticula are also related to voiding dysfunction, but there is always a dilemma of cause versus effect correlation. Urinary stasis within the diverticulum may cause the formation of stones or epithelial dysplasia [81, 83]. Treatment is mandatory when diverticula are symptomatic, and it includes open or laparoscopic or vesicoscopic excision of the diverticulum with ureteric reimplantation where indicated. Bladder septations are fibromuscular or mucosal septations that divide the bladder into equal or unequal compartments. They are diagnosed when they are symptomatic because of complications such as upper tract drainage impairment. They are associated with hydroureteronephrosis, renal dysplasia or agenesis, agenesis of the prostate, seminal vessels, epididymis, penis, or vagina, and spinal, orthopaedic or hindgut anomalies. This can lead to hypertension, proteinuria, renal impairment, or even renal failure in adult life. The infection of the urinary tract is most commonly due to ascending infection and any condition predisposing for this increases the risk of infection. The child is born with an absence of most of the sacrum, and a lesion of the cauda equina leading to a neuropathic bladder. The diagnosis is obvious from a plain radiograph of the pelvis, but it is all too easy to miss the absence of the sacrum. Clinically, they may present with bizarre symptoms, few of which are serious unless the cyst becomes infected. Surgical intervention is only required if the cyst is causing obstruction or is associated with a cauda equina lesion and carries a high risk of producing a neuropathic bladder even if not already present. Classification according to episode: A single infection is treated successfully and does not recur. The child should be examined from head to toe, looking for palpable masses, lymph nodes, tenderness, phimosis, labial adhesions, and stigmata of spina bifida or sacral agenesis. It is important to take into consideration the sample collection method while interpreting the culture reports (Tables 18. If a clean catch urine sample cannot be obtained, other noninvasive methods such as urine collection bags should be used. In an infant or child with a high risk of serious illness, it is highly preferable that a urine sample is obtained; however, treatment should not be delayed if a urine sample is unobtainable. If urine is to be cultured and it cannot be cultured within four hours of collection, the sample should be refrigerated or preserved with boric acid immediately. It has poor sensitivity and specificity, especially in children younger than three years of age. Dipstick testing for leukocyte esterase and nitrite is diagnostically as useful as microscopy and culture and can safely be used. Antibiotic treatment should be started if the urine test was carried out on a fresh sample of urine. Leukocyte esterase may be indicative of an infection outside the urinary tract which may need to be managed differently.

Purchase generic nortriptyline on line
However anxiety symptoms vs depression symptoms buy nortriptyline 25 mg free shipping, bulking agents might be considered in patients who are not fit for more invasive surgery, or those who do not want to undertake the risks of other surgery. Repeat injections are often needed to maintain a significant improvement of symptoms [47, 48]. Patients need to have good manual dexterity and cognitive function to understand the principle and be able to work the pump mechanism. To void, the patient squeezes the pump, which deflates the fluidfilled cuff, transferring the fluid to the balloon. A trocar is introduced through incisions in the labia majora laterally of the urethra and balloons are placed paraurethrally just under the bladder neck. Complications requiring revision include urethral atrophy or erosion, mechanical failure, and infections. Other complications include de novo bladder overactivity and urinary retention due to urethral strictures or bladder neck contracture. Other names for this condition are interstitial cystitis (largely historical) and bladder pain syndrome. It has no easily identifiable aetiology; multiple triggers may manifest as a final common bladder response to different types of stimuli or insult. It can be considered a major part of the painful bladder disease complex that includes other painful bladder conditions with established aetiology such as radiation cystitis. The presence of antinuclear antibodies has suggested that an autoimmune process might be responsible. Symptoms include pain, discomfort, or pressure localised to the bladder, accompanied by at least one other symptom such as urinary frequency or nocturia. Hydrodistension of the bladder under anaesthesia was used to assess for worsening pain (the patients grunt Bacterial cystitis The underlying lamina propria is full of chronic inflammatory cells, amongst them mast cells, which are present in 30% of patients. However, the lesion described is not an ulcer but a vulnerable weak area of bladder wall that can ulcerate on distension. Urine dipstick and urine microscopy, culture, and sensitivity should be performed on all patients. A positive biopsy shows inflammatory infiltrates or detrusor mastocytosis or granulation tissue or intrafascicular fibrosis. Patients might perceive pain during anaesthetic, and the anaesthetist needs to be informed to look for signs of pain (Table 23. All patients need to complete a threeday bladder diary, including fluid intake, timing and volume of micturition, and timing of 1) Conservative treatment or lifestyle modification A key consideration is to build realistic expectations at the outset. The patient must understand that there is no definite cure, and the aim of treatment is to control symptoms. The patient should be asked to look for and avoid any triggers, which will vary from patient to patient. Some drugs, chilli, caffeine, alcohol, tomatoes, spices, chocolate, citrus beverages, highacid foods, and artificial sweeteners may all contribute to bladder irritation and inflammation. It has multimodal actions such as analgesic properties, antiinflammatory, muscle relaxant, and collagen dissolution and effects histamine release). Botulinum toxin A injection can provide both symptomatic and urodynamic benefit by its antinociceptive effect on afferent pathways in the bladder. Efficacy is variable; studies have shown some shortterm benefits and requires repeated treatments every few months. Neuromodulation studies of sacral and pudendal nerve stimulation have shown benefits, although explantation (28%) and reimplantation (50%) rates have been found to be high [58]. Pudendal nerve stimulation has shown to be superior compared to sacral nerve stimulation [59]. Most patients will undergo trials with different agents and may or may not find one beneficial (trial and error). If there is no improvement with medical or intravesical therapy, early referral to a pain clinic is advisable. Transurethral resection, laser coagulation, or diathermy of Hunner ulcer is recommended for painful bladder syndrome type 3 C only. More complex surgery is reserved for resistant cases after careful counselling regarding side effects. Patients should have failed to respond to all medical treatment and failed to respond to any other options offered at the specialist pain clinic. A single episode of nocturia does not usually affect quality fo life, but two or more voids per night may. Patients will vary in their assessment of this and should be counselled accordingly. Incidence of nocturia (two episodes or more) increases with age from the sixth decade of life onwards, with around 50% of the population affected by age 80. Comparative prevalence is greater in young females than young males, but greater in elderly males than elderly females. Depending on the results of history, examination and baseline investigations, it may be appropriate to refer the patient to other specialists for further assessment, such as the cardiologist, sleep specialist, neurologist, psychologist, or endocrinologist. In patients with nocturnal polyuria not responsive to other measures, desmopressin (a synthetic analogue of vasopressin antidiuretic hormone) therapy can be used, provided serum sodium is >135 mmol l-1. Sodium levels should be monitored at three and seven days for hyponatraemia, detection of which is an indication to discontinue treatment. Polydipsia causes polyuria, and depending on timing, may cause nocturia and nocturnal polyuria. Medical conditions which may cause nocturia and should be excluded are diabetes, coronary heart disease, congestive cardiac failure, obstructive sleep apnoea. Diuretic use should also be considered, and if possible, the timing of intake should be altered. One must remember that nocturia could also occur if the person wakes for any other reason and decides to void before returning to sleep. As such, the potential list of causes could include any sleep disturbance such as insomnia, dementia, depression, anxiety, chronic pain, a baby crying in the house, or noisy neighbours! In patients who have undergone surgery, the more common causes are poorly controlled diabetes, diuresis seen in patients with highpressure retention once obstruction is relieved, postoperative loading with saline, and primary polydipsia. It is often helpful to ask partners regarding snoring or interrupted breathing during sleep because the patient themselves may not know. In patients who are polyuric, urine osmolality to determine if solute (>250 mOsml kg-1) or water (<250 mOsml kg-1) diuresis. A careful history often reveals storage symptoms and may reveal dyspareunia or any relationship with the menstrual cycle or previous hysterectomy. Examination may be negative but may reveal a urethral caruncle (which is a mucosal prolapse) or bladder tenderness. Detrusor failure or atonic bladder is the worst situation in this spectrum, whereby no detrusor activity can be demonstrated. With absent bladder sensation, the individual reports no sensation of bladder filling or desire to void. A degree of detrusor underactivity can be reversible, and this is likely related to the length of time with the condition and the degree of overstretching of the bladder that has occurred. Symptoms may not be evident to the patient until significant bother is caused by the symptoms or until retention occurs, seemingly suddenly. A poor urine flow rate may suggest detrusor underactivity, but normal flow does not exclude it. The diagnosis is confirmed during pressure or flow urodynamics because only then that specific information about the detrusor becomes available. Equally, the relative contribution to urine flow rate from detrusor pressure and abdominal straining are only distinguished during invasive urodynamics. The bladder can then be reassessed as to whether reasonable function has returned.
Caricae Fructus (Fig). Nortriptyline.
- Are there safety concerns?
- Constipation, diabetes, and other conditions.
- How does Fig work?
- What is Fig?
- Dosing considerations for Fig.
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96454
25 mg nortriptyline with visa
Therefore anxiety blanket purchase nortriptyline with american express, the mainstay of treatment is surgical excision with either radical or partial nephrectomy where possible. These are easily distinguishable from a pathological renal mass in that they have the same density as the rest of the renal parenchyma. Renal artery aneurysms and arteriovenous malformations will be discussed in another chapter. The acid mutates the p53 gene on codon 139 and is very rarely seen in the nonexposed population Consumption of more than 7 cups a day. Senna) and chemical laxatives Weakening of the urothelium predisposes to carcinogenesis. Other benign upper tract lesions include fibroepithelial polyps, villous adenomas, squamous papillomas, leiomyoma, neurofibromas, fibrous histiocytomas, haemangiomas, periureteric lipomas, and hibernomas [163]. Morphological variants of urothelial carcinomas have been reported and are exceedingly rare, limited to case reports or series. Alarming systemic symptoms such as anorexia, weight loss, malaise, fatigue, fever, night sweats, or coughs or palpable lymphadenopathy or hepatomegaly are suggestive of metastatic disease [164]. However, its use in routine practice has been questioned due to the variable sensitivity (due to interobserver discrepancy in analysis and sampling of the specimen) and additional costs [169, 170]. Ta, papillary, noninvasive; Tis, carcinoma in situ; T1, not invading muscle; T2, invading muscle; T3, invading renal parenchyma or outside muscle; T4, invading outside kidney. Both open and laparoscopic approaches have similar oncological outcomes, although laparoscopic approach has better early surgical outcomes [179]. Ipsilateral ureteric cuff excision is imperative because recurrences in the ipsilateral ureteral stump or orifice range between 30 and 64% [178]. In an extravesical technique, the entire ureter is dissected till the bladder, and then ureter is clamped with a portion of the bladder. The Semple manoeuvre (endoscopic technique) is the least invasive for tumours arising in the upper part of the ureter [181]. With the patient in the cystoscopy position, the bladder is kept semidistended to prevent excessive extravasations. The ureter is checked for complete removal by identifying the coagulated edge of the bladder cuff at the distal ureteral end. A Semple manoeuvre is not appropriate for a tumour in the lower third of the ureter, and it should not be used for ureters that are surrounded by fibrosis because that can cause injury to the common iliac artery. NephronSparing Approaches In recent years with the evolution of endoscopic and laser technology nephron sparing approaches have gained popularity. Nephron sparing surgery is commonly considered for patients with a single functioning kidney or a patient with renal insufficiency. In patients with normal contralateral kidney, nephronsparing surgery can be considered in carefully selected patients with lowgrade and stage disease, which are less than 1 cm in size [164]. For tumours in the renal pelvis or collecting system, the percutaneous approach can be implemented. Recent evidence has suggested that the application of photodynamic diagnosis assistance has the potential to improve the detection rates of superficial flat lesions [153, 172]. It has a similar technique as that of a radical nephrectomy with a midline incision; the kidney is mobilised and its pedicle divided. If performed using a laparoscopic Segmental Resection Distal ureterectomy and ureteral reimplantation can be considered for distal ureteric tumours. Ureteral resection of diseased section with ureteroureterostomy can be performed for midupper ureteral tumours. Resectoscope loop Ureter cut across Right ureteric orifice Intramural course of ureter reduction in risk is 40%, and the number needed to treat to prevent one bladder tumour is nine) [184]. Although evidence to date is scanty, platinumbased chemotherapy has been suggested to achieve recurrencefree rate of up to 50% [164, 185]. Meticulously close followup regimes for patients treated both surgically and conservatively are vital to detect recurrences either locally, distantly, or in the bladder (Table 13. Although local recurrence after radical surgery is rare, bladder recurrence ranges between 14 and 54% [179]. The local and bladder recurrence rate for patients managed ureteroscopically is 52% and 37% for patients managed with percutaneous endoscopy is 34% and 24%, respectively [177]. Hence, it is imperative that patients being treated with nephon sparing surgery are kept under strict and stringent surveillance. Unfortunately the inability of current investigative modalities to accurately stage, grade, and measure volume of disease makes advocacy of nephronsparing approaches questionable, particularly in patients with normally functioning contralateral kidneys. Maturity of these technologies in the future may allow for confident recommendation of nephronsparing approaches in the future. Direct administration into the ureter, employing retrograde or antegrade approaches, has shown to reduce recurrence in a few studies. Blood pressure and risk of renal cell carcinoma in the European prospective investigation into cancer and nutrition. Obesity is associated with improved survival in patients with organconfined clearcell kidney cancer. Family history and risk of renal cell carcinoma: results from a case control study and systematic metaanalysis. A populationbased familial aggregation analysis indicates genetic contribution in a majority of renal cell carcinomas. Genetic basis of kidney cancer: a model for developing moleculartargeted therapies. BirtHoggDube syndrome: mapping of a novel hereditary neoplasia gene to chromosome 17p12q11. Correlation between symptom graduation, tumor characteristics and survival in renal cell carcinoma. Paraneoplastic signs and symptoms of renal cell carcinoma: implications for prognosis. Interferonalfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. Intraoperative ultrasound during renal parenchymal sparing surgery for hereditary renal cancers: a 10year experience. Low incidence of asymptomatic brain metastases in patients with renal cell carcinoma. The Bosniak renal cyst 36 37 38 39 40 41 42 43 44 45 46 classification: 25 years later. Multicenter determination of optimal interobserver agreement using the Fuhrman grading system for renal cell carcinoma: assessment of 241 patients with > 15year followup. A populationbased competingrisks analysis of survival after nephrectomy for renal cell carcinoma. A preoperative prognostic model for patients treated with nephrectomy for renal cell carcinoma. Comparison of predictive accuracy of four prognostic models for nonmetastatic renal cell carcinoma after nephrectomy: a multicenter European study. Systematic review of oncological outcomes following surgical management of localised renal cancer. Systematic review of perioperative and qualityoflife outcomes following surgical management of localised renal cancer. Robotic versus laparoscopic partial nephrectomy: a systematic review and metaanalysis. Surgical management, complications, and outcome of radical nephrectomy with inferior vena cava tumor thrombectomy facilitated by vascular bypass. The Mayo Clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus. Perioperative outcomes following surgical resection of renal cell carcinoma with inferior vena cava thrombus extending above the hepatic veins: a contemporary multicenter experience.
Purchase nortriptyline 25mg with mastercard
Patients present with nonspecific itching and burning of the glans and prepuce with associated discoloration anxiety symptoms mind racing discount nortriptyline online american express. There are several causes of balanitis that can be broadly classified as acute or chronic. Predisposing factors include being uncircumcised (particularly when phimosis is present), poor hygiene, buildup of smegma, diabetes, and immunosuppression [3]. General advice for all patients is to improve hygiene by retracting the prepuce and washing with warm water daily, using emollient creams, and avoiding soaps, which can cause further irritation. On clinical examination, the glans will appear erythematous, and in severe cases, there may be preputial oedema with discharge and a foul odour. The main organism implicated in infectious balanitis is Candida albicans, accounting for up to 35% of all cases [5]. The treatment for candida balanitis is topical antifungal cream in the form of 1% clotrimazole or 2% miconazole applied twice daily until symptoms have settled [6, 7]. After an incubation period of approximately 21 days, the chancre of primary disease is formed. The classical Hunterian chancre starts as a dull red papule of variable size on the prepuce, glans or coronal sulcus. If left untreated, 25% will develop secondary syphilis, which results in a widespread mucocutaneous rash and lymphadenopathy. To a lesser degree, hepatitis, glomerulonephritis, and neurological complications can occur [14]. It should be considered in a case of balanoposthitis when the female partner has undiagnosed vaginal discharge. The most common presentation is with urethritis and urethral discharge, but this can develop into balanitis [16]. Treatment is with metronidazole either as a 2 g single dose or 500 mg twice daily for five to seven days [18]. Stricturing of the meatus and urethra leads to symptoms of bladder outflow obstruction and urinary retention in severe circumstances [23]. Management Conservative management measures include using soap alternatives for washing and the use of barrier creams to avoid contact with urine [24]. In early disease, treatment should begin with daily application of a mediumstrength topical corticosteroid. If there is a good response, application can reduce to alternate days for up to 16 weeks or a less potent steroid could be used [23]. This is can be curative, not only for disease of the prepuce, but also for the glans in the majority of cases [25]. When disease of the glans does not resolve, a glansresurfacing procedure with splitthickness skin graft may be indicated [25]. Disease extending to the urethral meatus and urethra can be treated by urethroplasty with buccal mucosa. In some cases of severe panurethral stricturing (image), a perineal urethrostomy may be indicated. The incidence of a general uncircumcised male population is about 1%, while reported to be as high as 15% in specialist dermatology clinics [19, 20]. Aetiology the aetiology of disease is unclear and likely multifactorial with autoimmune disease, infection, metabolic disease, and contact with urine all implicated [21]. Histologically, there is a loss of the rete pegs that fix the epidermis to the dermis, so the dermis tends to flake off. There is a thickening of the collagen layer of the dermis into which lymphocytes invade, and this collagen tends to contract so that the skin shrinks. The most common presenting symptom is male dyspareunia as a consequence of preputial dysfunction [22]. It is a disease of unknown aetiology affecting middle aged and elderly uncircumcised men. Patients are often completely asymptomatic but may complain of a small amount of discharge from the affected area. Temporary relief may be gained from the use of topical antibiotic or steroid creams [27]. Fournier who, in 1883, described several cases of fulminant gangrene of the penis and scrotum in young men [34]. Baurienne first described necrotising fasciitis of the genital region in 1764 [33]. However, the disease is commonly credited to Parisian venerologist JeanAlfred Infection is polymicrobial, and it is thought that synergy between these bacteria allows rapid multiplication and spread of infection. An obliterative endarteritis develops which leads to subcutaneous vascular necrosis and localised ischaemia. This usually starts in the superficial facial planes of the perineum (Colles fascia) and extends to the scrotum via dartos fascia, penis via Buck fascia, and abdominal wall via Scarpa fascia. Because of the attachments of Colles fascia to the perineal body posteriorly and pubic rami laterally, the extension of disease is limited in these areas [40]. Testicular involvement is rare because of the separate blood supply to the testes. The systemic signs of infection are often out of proportion with the local disease, which can range from local cellulitis to large areas of necrotic tissue and slough in the scrotum and perineum. Crepitus of the subcutaneous is also a common sign because of the presence of gas forming organisms [38]. Debridement is often more extensive than first imagined because subcutaneous involvement is greater than cutaneous appearances might suggest. General surgical input may also be required if the source of infection is perianal and a defunctioning stoma is being considered. It may also be appropriate to involve plastics surgeons at this point to consider approaches for management of large softtissue defects. On mucosal surfaces, they tend to be soft and fleshy, on hairbearing skin firmer and keratinised. Other than the psychological impact of the growth, patients tend to be asymptomatic. More commonly seen in uncontrolled diabetes or in patients who are immunocompromised. It can initially present with a painful lump, urethral discharge if the abscess bursts into the urethra, scrotal swelling if it tracks down, and obstructive urinary symptoms because of mass effect on the urethra. Treatment is early recognition and incision and drainage of the abscess with debridement of any necrotic tissue. Where there are single or few warts, cyrotherapy is considered firstline treatment, with topical therapies second. In patients who are pregnant, podophyllotoxin and imiquimod should not be used [43]. It responds to antibiotics, but the follow up must include tests for unsuspected syphilis. Highrisk subtypes 16 and 18 do not tend to cause warty lesions, but do cause dysplastic lesions and cancers. If the swelling progresses, the oedema can constrict the blood supply to the glans as well. Treatment is focused on attempting to protract the foreskin from its constricting retracted position just proximal to the glans. The majority of urethral strictures are iatrogenic in nature, accounting for approximately 45% [49]. Iatrogenic causes include urethral catheterisation, transurethral procedures, and hypospadias repair. Iatrogenic strictures tend to occur at the junction of the bulbar and penile urethra and are thought to be ischaemic secondary to pressure exerted by the instrument in use. Idiopathic strictures are the next most common, accounting for approximately 30% [48].
Buy discount nortriptyline line
This process is performed in an automated thermal cycling instrument preset with specific temperatures and times that are optimized for each primer pair anxiety attack symptoms yahoo buy nortriptyline 25 mg with mastercard. Because of a variable number of terminal repeats in the circular episomal forms of the virus, a polyclonal lymphoid population with a variety of forms of the virus can be distinguished from a monoclonal population with a single form. Because of the presence of introns, a gene may be very large so that satisfactory ampli fication is difficult. A higher success rate may be achieved with frozen biopsy specimens and split ting a biopsy specimen in two and fixing only half has therefore been recommended [61]. Negative results can result from sampling error when tissue infiltration is focal. Multicentre studies have sometimes shown a high rate of falsepositive reactions so that inclusion of a negative control in each assay is considered to be critical [64]. It must also be noted that sensitive techniques have detected gene rearrangements typical of leu kaemia and lymphoma in people who do not have an identifiable neoplastic condition. There are also problems in knowing when the detection of minimal residual disease is clinically significant. Detection of a residual clonal abnormal ity for a year or more after cessation of treatment is sometimes compatible with continued diseasefree survival. Microarray analysis is currently mainly a research tool but there is potential to use it for: (i) diagnosis; (ii) determining prognosis; (iii) stratify ing patients for treatment; and (iv) identifying tar gets for moleculedirected treatment. Without the need for sequential, selec tive, singlegene testing, established molecular genetic associations can be demonstrated efficiently in a single assay from blood or aspirated bone mar row samples. New diseaseassociated mutations are also being identified that will potentially provide new approaches to disease classification and tar geted treatment. Currently, whole exome/genome approaches are not cost effective in most health economies and remain research tools. The infor matics infrastructure needed to analyse the huge datasets generated is also only partly developed. They are also proving valuable for the diagnosis of constitu tional bone marrow failure syndromes. Automated detection of fluorescent signals is followed by computer analysis of the results, which can be either supervised or unsupervised. For example, large Bcell lymphomas were found to fall into two or three different classes that differed in prognosis Other molecular genetic techniques Other molecular genetic techniques are rarely used in routine diagnosis but have research uses. In polyclonal populations of lympho cytes there are a large number of different rearrangements and no single discrete band can be visualized. In a clonal population, since all the cells share the same rearrangement, there is a single dis crete band on electrophoresis, which is separate from the germline band. In clonal populations, there is amplifica tion of a single rearranged fragment, which appears as a discrete band separate from the germline band on electrophoresis. Knowledge of such mechanisms in Tcell maturation is much less advanced than it is for the Bcell lineage. Basic understanding of the somatic mutation processes underlying affinity maturation of immunoglobulin molecules, which occur within germinal centres, allows distinction between lymphomas derived from pregerminal centre, germinal centre and postgerminal centre lymphoid cells. The application of molecular genetic techniques in the investigation of leukaemia and lymphoma Molecular genetic techniques have two principal applications in the investigation of haematological neoplasms. Firstly, they can be used to demonstrate that a monoclonal population is present and can give information on the nature of the lymphoid cell in which a mutation occurred (see later). During rearrange ment single V, D and J regions are combined with a constant (C) region and simultaneously nucleotides (known as N) are added and removed between the V, D and J regions. Problems and pitfalls the polymerase chain reaction is sensitive for detecting small clonal populations but will not detect all rearrangements. The negative results in follicular and certain other lymphomas are consequent on the high rate of somatic muta tion, which is responsible for a failure of consensus primers to bind to rearranged genes [60]. However, this technique is only applicable if the breakpoint occurs in a relatively constant position and the fusion gene is not too long. However it should be noted that, using these sensitive techniques, fusion genes char acteristic of leukaemia or lymphoma are sometimes detected in normal tissues or tissues showing only reactive changes. For example, the rearrangement characteristic of follicular lymphoma has been detected in tonsils removed surgically for reactive conditions. Detection of leukaemia/lymphoma associated fusion genes As discussed earlier, many haematological neo plasms are associated with a specific nonrandom chromosomal abnormality. The genes involved in many of these rearrangements have been identi fied, permitting the use of molecular genetic tech niques for their detection. This is because of the necessity for a chromosomal abnor mality to have been fully characterized so that spe cific primers for each breakpoint can be designed. It should also be noted that, in contrast to standard cytogenetic analysis, molecular genetic techniques permit the detection only of those abnormalities that are being specifically sought. Ultrastructural examination Ultrastructural examination, in which the structure of cells is studied by electron microscopy, can be applied to peripheral blood and bone marrow but is little used in routine diagnostic haematology. Ultrastructural examination can also be applied to trephine biopsy specimens but it is rarely neces sary for diagnosis. Shortterm culture the major current use of shortterm culture in clin ical practice is for assessment of harvested bone marrow or peripheral blood stem cells prior to their use for engraftment. The starting cells are seeded at a sufficiently low concentration that individual colonies localized around each single multipoten tial parent cell can be visualized separately from any neighbouring colonies. The colonies can then be counted at low power magnification by standard light microscopy. Occasionally, the erythropoietic potential of primitive haemopoietic cells requires assessment. Erythroid colonies are readily seen by light microscopy because of the orange/red colour of their cytoplas mic haemoglobin. Apart from the use of culture systems as assays for predicting haemopoietic function in transplan tation, spontaneous colony formation. This potential for falseposi tive results and a relatively high falsenegative rate in true cases of essential thrombocythaemia and polycythaemia vera, together with the cum bersome nature of the assays, has limited the diag nostic application of shortterm colonyforming assays. Longterm culture Longterm cultures, in which haemopoietic precur sor cells are seeded onto layers of pregrown mar row stroma, can potentially permit assessment of the activity of stem cells even more primitive than those that survive in shortterm cultures. Assay of seeded cells is achieved, once they have adhered to the stroma, by replacing liquid medium with methylcellulose or agarcontaining semisolid medium and assessing colony formation as above. It is mainly employed in research, despite its possible value in predicting engraftment. Longterm cultures have also been used for ex vivo purging and expansion of haemopoietic cells for engraftment but these approaches have yet to find widespread clinical application. Bone marrow culture for microorganisms Bone marrow culture for microorganisms, for example mycobacteria, Leishmania donovani or Histoplasma capsulatum, can be of use in diagnosis and will be discussed in the next chapter. A study of hairy cell leukemia and mantle cell lym phoma involvement of the bone marrow trephine specimen by histologic, immunohistochemical, and polymerase chain reaction techniques. The response differs according to whether the infection is bacterial, rickettsial, viral or fungal. The periph eral blood and bone marrow responses to infection are nonspecific and similar changes occur in many other conditions, including trauma and other tissue damage, administration of growth factors, carcinoma, Hodgkin lymphoma, nonHodgkin lymphoma and autoimmune disorders such as systemic lupus erythematosus. Only a minority of patients with an infection show peripheral blood or bone marrow changes suggestive of a particular microorganism. Some bacterial infections, specifically typhoid, paratyphoid, tularaemia and brucellosis, are characterized by neutropenia rather than neu trophilia. Typhoid fever can also cause monocyto sis, left shift and toxic changes in neutrophils, thrombocytopenia, anaemia, bicytopenia or pancy topenia; occasionally there are circulating phago cytic cells [1]. Invasive meningococcal infection can be associated with apoptosis of neutrophils and lymphocytes, neutropenia and the presence of cocci within neutrophils, all these correlating with the severity of infection [2]. In severe infection, particularly if there is shock or hypoxia, nucleated red blood cells may appear in the blood, the presence of both granulocyte precursors and nucleated red cells being referred to as leucoerythroblastosis. The lymphocyte count is reduced but a few atypical lymphocytes, including plasmacytoid lymphocytes, may be present; plasma cells are sometimes seen. The eosinophil count is reduced during acute infection but eosinophilia can occur during recovery. Children may respond to bacterial infection with lymphocytosis rather than neutrophilia, and cer tain bacterial infections, particularly whooping cough and sometimes brucellosis, are characterized by lymphocytosis. In bacterial infection, the platelet count is often reduced but sometimes increased.
25mg nortriptyline with mastercard
Bone marrow aspirate films and trephine biopsy sections should be examined carefully for fea tures of systemic mastocytosis symptoms 0f anxiety buy 25mg nortriptyline with visa, which occasion ally presents with striking eosinophilia. Immunophenotyping of peripheral blood lymphocytes is indicated and, when an aberrant population is found, a diagno sis of idiopathic hypereosinophilic syndrome is not made. Tcell receptor gene analysis can be used to determine whether such a population is monoclonal. Patients suffer from albinism, neurological abnormalities and recurrent infections. Haematological abnor malities are most apparent in the granulocyte series although anaemia and thrombocytopenia also occur. With disease progression, there is development of anaemia, neutropenia and thrombocytopenia. Disorders of platelets Congenital thrombocytopenia Congenital thrombocytopenia may be inherited or may be secondary to intrauterine infection, muta gen exposure or platelet destruction by maternal antiplatelet antibodies. Inherited thrombocytope nia can be an isolated abnormality or part of a syn drome. Patients with the grey platelet syndrome can develop splenomegaly and extramedullary haemopoiesis [122]. Peripheral blood Morphological features are dependent on which specific defect is responsible for thrombocytopenia [1]. In the grey platelet syndrome they are increased in size and lack normal azurophilic gran ules. When thrombo cytopenia is secondary to intrauterine platelet destruction or damage to megakaryocytes, the plate lets are usually normal in size and morphology. Patients with Fanconi anaemia or dyskeratosis congenita can also initially present with an isolated thrombocytopenia with later progression to aplastic anaemia. In one family with autosomal domi nant thrombocytopenia with normal platelet size, the megakaryocytes tended to be reduced in num ber and small with low ploidy [123]. In autosomal recessive dysmegakaryopoietic thrombocytopenia, the megakaryocytes are normal or increased in number but are small and dysmorphic [136]. When thrombocytopenia results from intrauter ine damage to megakaryocytes these cells are usu ally reduced in number. When platelets have been destroyed by exposure to maternal antiplatelet antibodies, megakaryocytes are present in normal or increased numbers. Bone marrow histology A bone marrow biopsy is not often needed in determining the cause of congenital thrombocyto penia but it can be useful in permitting an accurate assessment of megakaryocyte numbers and mor phology. Thrombocytopenia may also result from platelet consumption, as in thrombotic thrombo cytopenic purpura or disseminated intravascular coagulation. Autoimmune thrombocytopenia and, rarely, amegakaryocytic thrombocytopenic purpura can be a feature of large granular lympho cytic leukaemia [65]. It is similarly advised in children who (i) have atypical features; (ii) relapse; or (iii) require corticosteroid therapy [152]. In autoimmune thrombocytopenic purpura, the major mechanism of thrombocytopenia is shortened survival of platelets and megakaryocyte numbers are usually normal or increased. However, there can also be ineffective thrombopoiesis resulting from immune damage to megakaryocytes [153]. In acquired megakaryocytic hypoplasia, for example as an adverse drug effect, megakaryocytes are usually morphologically normal although reduced in num ber. In these cases, megakaryocyte numbers are reduced and mega karyocytes are small when the platelet count is fall ing. When the count is rising, they are normal or increased in number and cytologically normal [148]. Cyclical amegakaryocytic thrombocytopenic purpura can occur as a stem cell as well as an auto immune disorder; in these cases also there is varia tion in megakaryocyte numbers in synchrony with the platelet count [154]. Thrombocytopenia, result ing from development of antithrombopoietin anti bodies, can develop in subjects to whom pegylated Peripheral blood When thrombocytopenia is caused by a sustained increase in peripheral destruction or consumption of platelets there is usually an increase in platelet size with some giant platelets being present. When thrombocytopenia is due to failure of production, as in sepsis or during chemotherapy, the platelets are small. Bone marrow cytology If thrombocytopenia resulting from peripheral destruction or consumption of platelets has devel oped acutely, the bone marrow may show no rele vant abnormality, megakaryocytes being present in normal numbers. There is often very little morphological evidence of platelet production despite the increased platelet turnover that can be demonstrated by isotopic studies. Because of the possibility of underlying carcinoma, bone marrow aspiration and trephine biopsy should be considered in mid dleaged and elderly patients with suspected auto immune thrombocytopenic purpura. There is increased vari ation in size so that, although small megakaryocytes predominate, there are also increased numbers of large forms. There is no abnormal localization of megakaryocytes and clusters are not usually seen [156]. Reticulin fibrosis is present at diagnosis in a minority of patients with autoimmune thrombo cytopenia, three of 32 patients in one series hav ing Baurmeister grade 2 reticulin deposition [157]. In cyclical antibodymediated amegakaryocytic thrombocytopenia, megakaryocyte numbers are 577 reduced when the platelet count is falling and normal when it is rising [148]. Leukaemia is unlikely if the haemoglobin concentration and white cell count are normal. This has led to controversy as to whether a bone marrow aspirate is required in children with iso lated thrombocytopenia [158]. Investigation of parents and siblings is therefore indicated when persistent unexplained thrombocytosis is found in a child or adolescent. Peripheral blood the blood film and count show thrombocytosis, usually as an isolated abnormality. Bone marrow cytology the bone marrow aspirate shows increased num bers of megakaryocytes of normal morphology. The aver age megakaryocyte diameter is increased and there is increased variation in size. Problems and pitfalls the differential diagnosis of reactive thrombocyto sis includes hyposplenism and essential thrombo cythaemia. Sovinz P and BehamSchmid C (2008) Intramedullary aggregation and phagocytosis of neutrophils in chronic benign neutropenia of childhood. The molec ular basis of congenital; thrombocytopenias: insights into megakaryopoiesis. Thiele J and Fischer R (1991) Megakaryocytopoiesis in haematological disorders: diagnostic features of bone marrow biopsies. Some patients have neutrophil leucocytosis, eosinophilia, monocytosis or thrombocytosis. Bone marrow cytology Erythropoiesis often shows the features of anaemia of chronic disease. Megakaryocytes are often increased, as are macrophages, plasma cells and sometimes mast cells. Dyserythropoiesis, abnormal localization of immature granulocytes and dysplastic mega karyocytes are sometimes noted [1]. Stromal changes can include paratrabecular fibrosis, sinusoidal congestion, oedema and bone remodel ling [1]. In patients with advanced disease there can be gelatinous transformation, which is sometimes extensive. Patients with parathyroid hormone secreting tumours can show changes of hyperpara thyroidism.
