
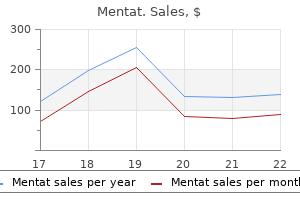
Buy mentat 60caps otc
Resident liver macrophages medicine kit for babies generic mentat 60 caps overnight delivery, called Kupffer cells, are involved in red blood cell turnover. Bile produced by the liver is stored and concentrated in the gallbladder, which has a three-layered structure consisting of a mucosa, muscularis, and adventitia/serosa. Two or more minor calyces join to form a major calyx, and major calyces ultimately join to form the renal pelvis, which then narrows to form the ureter. The calyces, pelvis, and ureter are part of the extrarenal structures involved in transporting urine to the bladder. The renal sinus is the space created when the fat between the calyces and renal vessels is dissected away. In addition, waste products produced by cells must be eliminated, while at the same time useful organic molecules such as glucose must be retained. The functional unit of the kidneys that accomplish this are microscopic tubes called nephrons; each kidney is endowed with almost a million nephrons at birth. In this sequence of chapters, the first three will focus on the histology of the kidneys. Sacral plexus Right ductus deferens Rectum Ureterovesical junction Urinary bladder Pubic symphysis Median umbilical ligament Left inferior epigastrica a and v. A renal lobe includes a renal pyramid as well as its associated cortex (including portions of the renal columns on either side of the pyramid). Urine produced by the nephrons in a renal lobe drains into the minor calyx associated with that lobe. Human kidneys have 10 to 20 of these lobes, each oriented such that the renal papilla is close to the renal sinus. In this scanning view of a portion of the kidney, a nearly complete lobe is outlined in black, including the cortex, medulla (pyramid), and papilla. To the right of this lobe is most of a second lobe (yellow outline), with cortex and medulla, but the papilla and minor calyx are out of the plane of section. The bottom of the slide contains adipose tissue of the renal sinus, including blood vessels, which will be examined later. The dotted green line represents the border between the cortex (above) and medulla (below). One lobe, which includes a renal pyramid and associated cortex, is outlined in black. This fluid then flows down the tubular system (in the order listed), and the ultrafiltrate is modified by cells of the tubules. The final product, urine, flows out the end of the collecting ducts into a minor calyx. Each nephron ultimately drains its product (urine) into a minor calyx via a collecting duct. The region at the bottom of the slide below the lobes is the renal sinus, which contains renal vessels and adipose tissue. The dotted line indicates the border between the cortex (above dotted line) and medulla (below). Ureter Minor calyx As mentioned, all renal papillae are directed toward the renal pelvis. The renal corpuscle of these nephrons is located in the outer region of the cortex. A very short loop of Henle in these nephrons extends only a short distance into the medulla. Juxtamedullary nephrons have a renal corpuscle in the cortex, located adjacent to the medulla. The loops of Henle of juxtamedullary nephrons are long and extend into the deeper portions of the medulla. Juxtamedullary nephrons are important for setting up the concentration gradient in the medulla used in concentration of urine. Helpful Hint Each lobule shares a border with an adjacent lobule; the exact border between lobules is not easily identified but is about halfway between medullary rays, as shown by the rectangle. The cortex contains medullary rays (above black brackets), seen as collections of tubules oriented in the same direction extending from the corticomedullary junction toward the outer surface (capsule) of the kidney. Note that, due to sectioning, it is unusual to see an entire medullary ray from one end to the other; in this region, most can be seen clearly at the corticomedullary junction but "disappear" about one-third to one-half the way toward the 34. The pars convoluta is the portion of the cortex not including the medullary rays. The dotted line indicates the border between the cortex (above) and medulla (below). The regions between the medullary rays form the pars convoluta (blue bracket), in which the tubules are in many different orientations. A lobule (outlined in yellow) is defined as a medullary ray plus the tubules within the adjacent partes convolutae that are connected to . In a section such as this, half of each pars convoluta "belongs" to one medullary ray (or lobule), and the other half belongs to the adjacent medullary ray. Medullary rays (partes radiatae, black brackets) and partes convolutae (blue brackets) are shown. The central region of each lobule is a medullary ray (outlined in yellow), which can be recognized because all the tubules in this region are cut in cross section in this orientation. Peripheral to each medullary ray is the pars convoluta (between yellow and black outlines), in which the tubules (proximal and distal convoluted tubules) are cut in a variety of orientations. Renal vessels enter and leave the kidney at the hilus (indentation on the medial side of the kidney). These segmental arteries give rise to interlobar arteries, which run in the renal columns between the renal pyramids. At the junction of the medulla and cortex, the interlobar arteries branch at right angles, forming arcuate arteries that are oriented parallel to the capsule, between the cortex and medulla. Branching from the arcuate arteries at right angles are interlobular arteries, which run in the cortex toward the capsule. Helpful Hint the microvasculature of the kidney-afferent and efferent arterioles, glomerulus, peritubular capillaries, and vasa recta-will be discussed in subsequent chapters. The medullary rays are within the yellow outlines; the partes convolutae are between the yellow and black outlines. Vessels within the sinus (black arrows) are either renal or segmental (they cannot be differentiated in this section). Helpful Hint It cannot be stressed enough here: All the arteries in the kidney look like arteries, and all the veins look like veins. It is true that the arteries get smaller as they branch, and the veins get larger as they return to the renal vein, and this may be useful, but do not lose sight of the fact that the definitive way to identify these vessels is by their position in the context of the kidney. Orange arrows indicate interlobar vessels; green arrows mark arcuate vessels; blue arrows indicate interlobular vessels. Black arrows indicate segmental or renal vessels; orange arrows point to interlobar vessels; green arrows mark arcuate vessels. Arcuate vessels (green arrows) can be seen more clearly along the corticomedullary junction. Longitudinal and cross-sectional profiles of interlobular vessels (blue arrows) can be seen in the middle of the pars convoluta. In fact, the presence of these vessels signifies the border between adjacent lobules (thus the name interlobular vessels). For all of the vessels shown in these figures at low magnification, there are both arteries and veins present. Differentiating between them may be possible at these magnifications but usually requires higher magnification to examine the thickness of the wall, as described in the chapters on vessel morphology.
Buy cheapest mentat and mentat
This can only mean that long-chain bonded alkylsilanes are substituted with short trimetylsilanes that actually have higher bonding energy medicine 968 mentat 60 caps free shipping. Chromatographic testing usually shows the decrease of peak tailing and other effects usually attributed to the influence of a reduced amount of a residual silanols. Overall packing material becomes more hydrophobic, since the amount of accessible silanols decreases with end-capping, but carbon content is decreased also. An enormous amount of publications are devoted to the classification, standardization, and comparison of these phases. At the same time, they refer to the comparison of C18-type columns from different manufacturers and find dramatic variation in the retention of both polar and nonpolar compounds at the same conditions on different columns. Surface area of base material, pore size, bonding density, end-capping, and even the column history all can significantly affect analyte retention. The only valuable comparison of different columns found so far is so-called methylene selectivity. Compared to common alkyltype phases, phenyl columns show lower methylene selectivity; in other words, the separation of members of homologous series will be less selective on phenyl columns than on alkyl-modified phases. The introduction of polar embedded stationary phases was inspired by the need to develop reversedphase methods in high aqueous mobile phases for separation of either highly polar or ionic compounds. At these conditions, the hydrophobic surface of chemically bonded material has limited wettability. The consequence of this "phase collapse" is that after some period of time the retention of any analytes on the column dramatically decreases, although it does not become equal to the void volume, but very close to it. The first proposed explanation was that bonded alkyl ligands are "collapsed" or do not allow analyte penetration between bonded chains. They tend to minimize their energy by assuming such conformations that allow the maximum number of contacts between these chains. The study of apparent viscosity of alkyl-bonded layers showed that it is approximately three orders of magnitude higher than the viscosity of corresponding free n-alkanes. Recall that n-octadecyl is solid at room temperature; this means that octadecyl chains immobilized on the surface form a rock solid material. Recent studies of the "phase collapse" effect show that after steady removal of a wetting agent (any previously used organic mobile-phase modifier), water does not wet the hydrophobic inner surface of porous material, and the flow of the mobile phase through the porous space and corresponding transport of the analyte molecules to the surface inside the pores is suppressed. The effect is essentially equivalent to an approximately 100-fold decrease of the adsorbent surface area (the majority of the surface area is inside the pores of packing material). Polar embedded stationary phases include a nonionizible polar group embedded into the bonded chain. Another example is Synergi Fusion, (Phenomenex) which uses a polar embedded ligand and a hydrophobic ligand. The second reason in the introduction of polar groups in the bonded ligands is that these groups interact with residual silanols, which make the silanols effectively inactive for the interaction with polar or basic analytes. These phases also show a significant difference in selectivity compared to conventional C18type phases. The main goal of chemical modification of the surface is to create a preferably uniform surface with a selected type of interactions. An additional desirable feature is hydrolytic stability, which in most cases is achieved by proper shielding of anchoring bonds. Shielding of the base material, leading to the elimination of the influence of residual silanols, is essentially the main focus in the development of most recent packing materials. Distribution of bonded ligands at low, average, and high bonding density for island, random, and uniform bonding. Three different types of surface ligand distribution could be distinguished: random, uniform, and island-like. Type of bonding distribution is significantly dependent on the conditions under which the bonding reaction is performed. Type of catalyst (usually amine), reagent concentration, temperature, and presence of residual adsorbed water on the substrate surface affect this process. Arrangement of the bonded ligands on the surface, along with conformation of these ligands and their occupied volume, is also important for understanding of the shielding effect. Recently, this obvious decrease of adsorbent pore volume was correlated with molecular volume of bonded ligands [63]. Molecular conformation of bonded ligands and their degree of freedom is dependent on bonding density. The higher the bonding density, the lower the number of possible conformations and thus the less mobility the bonded chains have. Immobilization of ligands on the surface already restrict their mobility, so if we compare the state of free C18 molecules (n-octadecyl) with immobilized octadecyl, we can expect more rigid (or solid-like) behavior of immobilized chain. Correlation of molecular volume of bonded n-alkyl ligands with that for liquid n-alkanes [63]. The higher the bonding density, the more hydrophobic the adsorbent surface, the better the shielding of residual silanols, and the higher the hydrolytic stability. Above we briefly discussed the limitations on possible values of bonding density (Section 3. If the most stretched conformation of a ligand has length l and its molar volume is v, then the minimum area, it occupies on the surface will be w = v/l and the maximum bonding density will be dmax = 1/w. Maximum density means that the whole volume of a surface layer of thickness l is actually filled with bonded ligands and is calculated for a uniform cylindrical surface. Comparison of the Carbon Load and Surface Density Values Adsorbent 1 2 Carbon Load (%w/w) 0. We have to emphasize that this is highly misleading because it is not related to the available surface area. As an illustration we can compare two adsorbents modified with C18 chains (Table 3-3). On the other hand, the second adsorbent has 80 times higher surface area and all these bonded ligands are spread on this surface, yielding lower bonding density than the first adsorbent. It is advisable to compare the data obtained at the different combustion conditions (amount of oxygen in the oven, speed of heating of inductive oven, etc. In the case of polymeric bonding, the effect of crosslinkage should be taken into account, although it is usually insignificant. In the case of a vertically polymerized bonded phase, decomposition may involve a siloxane backbone, and association of the weight loss with the ligands molecular weight is essentially impossible. Carbon content, on the other hand, is only dependent on the original reagent structure. Detailed study of thermogravimetric analyses of chemically modified adsorbents shows some significant deviations. This weight loss is the major source of errors in bonding density determination, and it is not related to the decomposition of any organic but rather dehydroxylation of base silica and loss of water molecules occluded in the silica matrix. Series of thermograms and their derivatives for adsorbents modified with alkysilanes of different chain length. In fact, at least half of the original silanols on the silica surface remain unreacted after chemical modification. Silanols have acidic nature, but their ionization constants are highly dependent on the surface environment and on silica purity.
Generic mentat 60 caps on line
If the diode array spectra is the same across this distorted peak medicine website buy cheap mentat 60 caps on-line, it can be deemed as spectrally homogenous and may be possibly due to a diluent effect. If the diluent was changed to 95% aqueous, pH 2/5% acetonitrile, the sample may not be soluble in this diluent. Therefore serial dilutions may be made such that the compound is first diluted in a diluent in which it is most soluble in and then further diluted to target concentration with a diluent that would be as similar as possible to the staring mobile-phase composition. If the diluent was 95% aqueous, pH 2/5% acetonitrile and the sample does show a good peak shape but reinjection of the same solution over time shows an additional impurity that is increasing, this may suggest reaction with the diluent. Multiple steps may be taken here; use an autosampler with a tray cooler to decrease the rate of reaction, adjust the pH of the diluent if pH is catalyzing the reaction in the protic solvent, and/or increase the amount of organic in the diluent. If increasing the organic concentration in the diluent does help in suppressing the formation of the additional impurities but as a consequence peak splitting is observed, then it would be recommended to try another column in order to enhance the retention of the early eluting component such that the compound/impurity would be more retained at a higher initial organic composition. Also, precolumn derivatization may be required to ensure that the desired product is not reacting with diluent prior to analysis. If derivatization is to be employed, then the type, concentration, and derivatization time all need to be explored. Other approaches may include the use of aprotic solvents as a diluent and the use of normal-phase chromatography. Generally, reaction with diluent and mobile phase is sometimes observed for compounds that contain keto functionalities (gem diol, oxycontin [9], active aldehyde [10], active esters such as mesyl sulfonates [11, 12], and enolate intermediates [13]), so protic solvents such as aqueous/methanol should be avoided or derivatizatoin may be required either precolumn or in situ. Ionizable species are prone to solvation by the mobile-phase components and the solvation equilbira may lead to poor peak shapes. This could be related to the solvation of ionizable species by both the methanol and water which, due to the different secondary equilibria processes, leads to peak distortion. Therefore, if area% normalization is to be used, then all the impurities and the active pharmaceutical ingredient must have similar relative response factors (area response/weight). This is sometimes difficult because the impurities may have different electron-donating or electron-withdrawing functional groups, attached to the aromatic ring and/or the impurities may have more complex conjugated systems and the absorption spectra have been shifted to longer or shorter wavelengths compared to the parent compound. A wavelength must be chosen such that adequate response is obtained for the active and that at least a 0. The wavelength chosen should not be on a distinct slope of the spectrum, and the relative difference in the absorbance at a certain wavelength is not significantly different from the impurities/degradation products present. Although at 250 nm all the compounds have similar absorbance and even higher absorbance compared to 280 nm for some of the components. If an analysis were to be carried out at 250 nm the spectral bandwidth becomes very important. The linearity of the detector is inversely proportional to the spectral bandwidth (as the spectral bandwidth gets narrower, the linearity gets better). However, even if the diode array spectra do overlay, this does not absolutely ensure that the peak does not contain any coeluting impurities, because the impurities could have similar diode array spectra and/or if there is a low level of a coeluting species with a different diode array spectrum, it may not be determined by this approach. This does not absolutely ascertain that the peak is homogeneous since isomers of the same compound will have the same [M + H] and is indistinguishable from the parent compound. Also, the impurity that may be coeluting may not have an appreciable ionization efficiency at the particular mobile-phase and mass spectrometric conditions. Note that for this reaction mixture (convergent synthesis) the desired product 1 has the same diode array spectra as synthetic precursors 2 and 3. If these two synthetic precursors had coeluted with 1, they would not have been able to be deconvoluted. Reaction conversion of a convergent synthesis (2 + 3) to 1 and overlay of diode array profiles. Also, since it is not known if dimeric species or more hydrophobic compounds are present in the sample solutions during the initial method development or are formed in stability studies, gradient elution should always be performed with a hold at higher organic conditions (or up to the buffer stability limit). Sample preparation is a critical step of method development that the analyst must investigate. For example, the analyst should investigate if centrifugation (determining the optimal rpm and time) shaking and/or filtration of the sample is needed, especially if there are insoluble components in the sample. The objective is to demonstrate that the sample filtration does not affect the analytical result due to adsorption and/or extraction of leachables. A word of caution here is that filter studies should be performed to ensure that no adsorption of the compound on the filter is observed. Note that for proteins and peptides the impact of centrifugation (speed and time) must be investigated because this may lead to increased aggregate formation. Also, for protein and peptides the initial concentration of the sample could also have an impact on the concentration gradient of the sample in the centrifuge tube, and the concentration of the top, middle, and bottom portions should be assessed. The effectiveness of the syringe filters is largely determined by their ability to remove contaminants/insoluble components without leaching undesirable artifacts. Extractables are often the result of inappropriate material construction and improper handling of the device during the manufacturing process. Particular attention should be paid to potential extractables from the membrane and housing material. The analytical procedure must specify the manufacturer, type of filter, and pore size of the filter media. Also, it must be known if the particular filter type is compatible with the type of analyte, organic solvents, and pH of the solution to be filtered. The following procedure may be used to determine if there is any absorption on the filter. One aliquot of the stock solution is centrifuged, and other aliquots from the centrifuged stock solution are filtered through the desired filters (pre-wet with 5 mL of diluent) and the results compared. If any additional peaks are observed in the filtered samples, then the diluent must be filtered to determine if a leachable component is coming from the syringe filter housing/filter. The initial stock solution was centrifuged (no filter) and two additional samples from the centrifuged solution were filtered with a nylon filter and a cellulose filter. The area counts (Table 8-4) of all three solutions were compared, and it was shown that significant absorption was observed on the nylon 66 filter. Further optimization of the sample preparation would include removing the centrifugation step and just filtering the supernatant (solution above the undissolved excipients) with the cellulose acetate filter. The data in the Table 8-5 demonstrates that the two methods of sample clarification are equivalent and that the filtration procedure (0. Comparison of filtered (nylon filter versus cellulose filter) versus no filter (centrifuged). Area Counts for Centrifuged/Filtered Solutions Type of Sample Preparation 30-mm Nylon filter, 0. Other considerations for sample preparation include incorporation of methanol in the sample preparation scheme, especially if a second dilution is used (check for sample reactivity). The impact on peak shape (diluent/mobile phase mismatch for components with k < 2) should also be considered. Sample preparation usually constitutes approximately 70% of solvent usage, and incorporating methanol for routine sample preparation can lead to reduction in solvent costs. For a given stationary phase the k of a particular component can be controlled by changing the solvent composition of the mobile phase. However, the impact of eluent composition will depend on the type of stationary phase and the nature of the components in the mixture. Thus, to optimize a chromatographic separation, the concentration of the organic modifier is adjusted so that the k of the components in the sample are in the range of 1 to 10. However, sometimes due to the hydrophobic nature of the compound, even high concentrations of organic modifier will not allow elution of all components in a single run and the chromatographer can try one or a combination of the following approaches: (1) Use a stronger modifier; (2) apply a steeper gradient; (3) use a less hydrophobic stationary phase. Detailed discussion of the reversed-phase separation principles and separation optimization is given in Chapter 4. The type of column chosen for a particular separation depends on the compound and the aim of analysis. Pharmaceutical companies may have a preferred list of columns that have good demonstrated performance in regard to pH/temperature stability. These columns that have been selected by a specific laboratory are known to be stable within predefined pH and temperature regions in which method development/column screening are employed. A good understanding of the chemical stability of the stationary phases is needed, and some examples are shown in Section 8.
Buy generic mentat on line
We will generate the dynamical medications japan travel buy discount mentat on line, personalized data clouds that permit the extraction of individual actionable possibilities, which, if acted upon, allow individuals to optimize wellness and minimize disease. We will generate a multiparameter, biomarker panel for wellness that in time, we believe, will allow us to disentangle the physiological and the psychological components of wellness quantitatively from the blood. It will facilitate individuals moving up their well of wellness to maximize their own human potential. We will delineate the wellness to disease transitions for the common diseases and open the possibilities for early diagnosis followed by early treatment-thus moving individuals quickly from Systems medicine and cancer: a postscript A reader of this book might ask just what systems medicine (and P4 medicine) might offer cancer. It is clear that the systems approach to cancer has much to offer and we will briefly outline a few examples. Cancers shed rare cells into the blood that can be isolated and characterized, especially with the new techniques of single-cell analysis. These cells may provide new opportunities for early diagnosis, following the progression of the cancer, identifying the recurrence of cancer, and possibly even localizing the distant sites of metastases. One can assess the network dynamics of cancer progression in mouse model systems (as we did for prion-induced neurodegeneration) and gain insights into early disease-perturbed networks, which in turn provide opportunities for developing early diagnostics and potential therapeutic targets to attack cancer at its early inception. We have studies underway in mouse models for glioblastoma with striking results that demonstrate 1908 the future of oncology that disease-perturbed networks explain many of the most fundamental properties of cancer. One can develop blood diagnostics for cancer, follow its progression, follow the response to therapy, identify recurrences, and even identify disease-perturbed networks that provide insights into possible therapeutic drug candidates (see our earlier description of an approach to lung cancer diagnostics). A key aspect of future cancer treatment will be triple drug therapies that are initiated at the outset of the treatment of the disease. An understanding and analysis of the disease-perturbed networks of cancer is the key to identifying multiple potential drug target candidates that can act synergistically with one another. Moreover, systems strategies can be deployed to identify appropriate combinations of three or more drugs through combinatorial analyses. The longitudinal study of well people as described above will ultimately allow us to identify the wellness to disease transitions in cancers and begin to investigate early disease-perturbed networks. An understanding of these early transitions will open new possibilities for early diagnostics and therapies. We can apply longitudinal wellness studies to individuals undergoing cancer treatment to optimize their wellness during this difficult process. Moreover, we can do the same for patients that have already undergone successful (cytotoxic, chemotherapeutic) cancer treatments to once again optimize their wellness. These are just a few examples of how P4 medicine can address cancer-and we are just at the beginning of imagining all of the P4 opportunities that lie ahead of us for cancer research. The key is to bring P4 medicine into the healthcare systems rapidly so that medicine can begin to exploit these opportunities. A major challenge, quite obviously, is how to bring an understanding of these opportunities to physicians-who often can be quite conservative in their willingness to accept new ideas. In a similar manner, the digitization of medicine, together with the other changes noted above, will strikingly reduce the costs of healthcare and that, in turn, will democratize P4 healthcare for the poor as well as the rich. It is difficult to comprehend, within the next decade, how many individuals, rich and poor alike, might be in a position to transform their human potential through optimizing wellness and minimizing disease. As we move into the twenty-first century, medicine will increasingly become predictive, preventive, personalized, and participatory. It will focus on each of us as individuals and optimize our health according to each of our individual and unique characteristics. Acknowledgments We thank the individuals in the Pioneer 100 project for their participation in this adventure and the many wonderful team members (too numerous to mention) who have made this project possible. We thank Gretchen Sorensen and Jennifer Lovejoy for many valuable comments on the manuscript. We also thank the Institute for Systems Biology for providing philanthropic support to this project, the Robert Wood Johnson Foundation, and the M. P4 medicine: how systems medicine will transform the healthcare sector and society. Systems cancer medicine: towards realization of predictive, preventive, personalized and participatory (P4) medicine. Analysis of the human neurexin genes: alternative splicing and the generation of protein diversity. Integrated genomic and proteomic analyses of a systematically perturbed metabolic network. The democratization of wellness and healthcare Our vision for the future of healthcare is that patients will participate by taking responsibility for their own health, the digitization of medicine, and our more effective understanding of how to use personalized data clouds to optimize wellness and avoid disease that we can substantially reduce the cost of healthcare while enhancing its effectiveness. We are convinced that this will happen through a focus on wellness and the early identification of disease transitions that can be identified and treated rapidly and effectively. As costs come down and concrete discoveries are made, P4 medicine will be brought not only to the developed world but to the developing world as well. Who would have thought in 1990 that a woman in a rural village in India could make a living for her family using a cell phone A blood-based proteomic classifier for the molecular characterization of pulmonary nodules. Historic and Projected Data from the Period and Cohort Life Tables, 2012-Based Revised. In most cases, nuclear shape reflects the shape of the cell; for example, a round cell will have a round nucleus (blue arrows), while a spindle-shaped cell (yellow outline) has a longer, narrower nucleus. Second, and maybe more importantly, the size of the nucleus typically reflects the activity level of the cell. Therefore, the nucleus provides a clue as to whether the cell is very active (blue arrows) or relatively inactive (black arrows). The outer border of the nucleus is the nuclear envelope (tips of the black arrows), which consists of two lipid bilayers that cannot be distinguished at the light microscopic level. The large dark structure in the center of the nucleus is the nucleolus, which is the site of ribosome synthesis. Smaller nuclei (yellow arrow) are composed mostly of heterochromatin, suggesting a less active cell. Note that numerous structures within the cytoplasm that are not evident in light microscopy are readily evident in electron micrographs; these will be discussed in detail in the next chapter. Heterochromatin is scattered throughout this nucleus, but mostly against the inner part of the nuclear envelope. The nucleolus is prominent, suggesting assembly of ribosomes necessary for protein synthesis. Note that the first three phases of the cell cycle, G1, S, and G2, are collectively referred to as interphase; cells in these phases are indistinguishable by light microscopy. Many of the cells in tissues such as the epidermis of the skin or the gut epithelium are continually regenerating to replace damaged cells and, therefore, are continuously progressing through the cell cycle. However, cells in many tissues stop dividing and may differentiate into specialized cell types. For example, after development is complete, neurons in the brain stop dividing and function to transmit action potentials; these cells are considered to be in the G0 phase because they are no longer actively dividing. In other tissues, cells may enter the G0 phase temporarily, returning to the cell cycle when necessary. For example, fibroblasts in the skin are relatively quiescent but can be stimulated to divide in order to regenerate damaged tissue. The nuclear envelope consists of two membranes (two lipid bilayers); each shows up as a linear structure at this magnification. The outer membrane is indicated by the series of red arrows and is studded with round structures (ribosomes). The inner membrane (yellow arrows) is less distinct due to the heterochromatin (labeled and at 3) adjacent to it. The black arrows indicate nuclear pores, openings in the nuclear envelope that allow molecular trafficking between the nucleus and cytoplasm. The label 2 indicates rough endoplasmic reticulum in the cytoplasm, discussed in the next chapter.
60caps mentat sale
It develops by superficial telangiectasia in the papillary dermis treatment head lice purchase mentat from india, and is generally due to traumatism with reactive hyperkeratosis. It appears in youngsters and adults, more frequently in the lower extremities, although it can also manifest in the upper limbs and trunk. Their dermoscopic appearance also varies depending on their time of evolution and the presence or absence of thrombosis. Later-stage angiokeratomas contain multiple lacunae with the characteristic blue-red or blue-black color, though darker. However, these lacunae are not well demarcated and often lie on a white-yellowish background, due to epidermal acanthosis and hyperkeratosis. Targetoid Hemosiderotic Hemangioma It is an uncommon, vascular, benign solitary lesion that can be misdiagnosed as other tumors including melanomas. The epidermis covering the lesion is usually hyperplastic, with elongated epidermal ridges and hyperpigmentation in the basal layer. Clinical diagnosis of dermatofibroma is simple and dermoscopy helps with the more uncommon forms. Delicate peripheral pigment network: It is not a true pigment network since it is due to melanic rather than melanocytic pigmentation. Central white pach or area: It has a scar-like appearance and is due to the superficial dermic fibrosis of this tumor. The collagen fasciae are birefringent and these give rise to a rapid randomization of the polarized light. It is a dynamic polarized dermoscopy since by rotating the dermoscope while keeping it in contact with the cutaneous surface, the orientation of the crystalline structures changes. This is owing to the angular dependence of the polarized light, reflecting the non-randomized distribution of the collagen fibers in the dermis. Dermoscopy of pigmented skin lesions: results of a consensus meeting via the internet. Central white scarlike patch: a dermoscopic clue for the diagnosis of dermatofibroma. Central white network: an additional dermoscopic feature for the diagnosis of dermatofibroma. Dermoscopic findings of haemosiderotic and aneurysmal dermatofibroma: report of six patients. These lesions are more frequent in fair-skinned, lighteyed, and blond-haired people. Nevertheless, they can manifest in any kind of skin, depending on the level of solar exposure. Inner gray halo, a novel dermoscopic feature for the diagnosis of pigmented actinic keratosis: Clues for the differential diagnosis with lentigo maligna. Pitfalls in the clinical and dermoscopic diagnosis of pigmented actinic keratosis. It is the result of the pigmentation of the basal keranocytes surrounding the hair follicle. Dermoscopically, it is characterized by the presence of mainly thick hairpin vessels with peripheral distribution and central hyperkeratosis. The white circles are located around the dilated infundibulum filled with a central keratin plug (yellowish keratotic plug) and observable as a yellow or an orange area (clods); these structures do not correspond to keratin pearls. In most cases, its clinical manifestation is a welldemarcated pink and scaly (squamous) plaque. Its clinical manifestation is a well-demarcated pink or brownish macula or squamous plaque. The differential diagnosis includes pigmented actinic keratosis, solar lentigo, seborrheic keratosis, lichen planus-like keratosis, pigmented basal cell carcinoma, nevi, and melanomas. The vessels, spiral or loop-like, are arranged in linear fashion in the periphery of the lesion or in clusters or groups. Dermoscopically, it is possible to observe, in the center of the lesion, areas without structure, white, yellow, or light brown in color, and amorphous areas corresponding to hyperkeratosis usually located in the central part; also blood spots distributed in the keratin and white circles surrounding the dilated infundibulum filled with a central keratin plug resembling yellow or orange clods. Cutaneous squamous cell carcinomas of the lower extremity: a distinct subset of squamous cell carcinomas. Dermoscopic characteristics of nodular squamous cell carcinoma and keratoacanthoma. Dermatoscopy of actinic keratosis, intraepidermal carcinoma and invasive squamous cell carcinoma: a progression model. Clinically, it appears as a solitary pink nodule, generally located at acral level (palms and soles) in adults. Dermoscopy has proved to be especially useful since it enables the evaluation of vascular structures showing a polymorphic vascular pattern, with hairpin vessels, dotted vessels, irregular linear vessels, and pink lacunae surrounded by a whitish halo looking like "frog eggs. Dermoscopic features of nonpigmented eccrine poromas in association with their histopathological features. Under dermoscopic examination, it is possible to observe dotted or globular vessels with linear arrangement, like a "string of pearls. They appear as dome-shaped erythematous nodules, solitary or multiple, and generally localized in the head and neck, although they can also appear in the upper trunk. Clinically, it appears as a pink papule or nodule, usually occurring on the face in young individuals. Solitary trichoepithelioma in an 8-year-old child: clinical, dermoscopic and histopathologic findings. They are more frequent in children and young adults, occurring in hands, feet, and limbs. These structures may be surrounded by a white halo that betrays the presence of papillomatosis. Exceptionally, it is possible to observe polymorphous vessels (hairpin, dotted, spiral, or irregular linear vessels) and ulceration areas. It is more frequent in children, but can also appear in adults, in which case it is considered a sexually transmitted infection. When these vessels surround the lesion completely, the lesion is called "mixed flower-like pattern. Dermoscopy of molluscum contagiosum: a useful tool for clinical diagnosis in adulthood. From a clinical point of view, it presents as a white-yellowish papule, sometimes umbilicated, of <1 cm. The classic cutaneous lesion is a flat polygonal papule slightly erythematous or purplish, in whose upper part it is possible to observe reticular or whitish dotted formations. In the borders, there may appear linear vessels (capillary vessels) and erythematous globules. These structures may be surrounded by a white halo that betrays the presence of papilomatosis. These structures are surrounded by a white halo which betrays the presence of papillomatosis (white arrow). If it is a melanocytic lesion, the physician must continue with the second step, which means differentiating a benign melanocytic lesion from a melanoma. In this articler, we include concepts of Nevogenesis, the different types of nevus, such as congenital, acquired, atypical, blue nevus, combined and recurrent nevus. The different types of melanoma, superficial spreading melanoma, nodular melanoma, lentigo maligna melanoma and acral melanoma will be included as well. The first step involves determining if the lesion is melanocytic or nonmelanocytic. If it is a melano cytic lesion, the physician must continue with the second step, which means differentiating a benign melanocytic lesion from a melanoma. Therefore, in order to proceed to the second step, it is essential to know the different criteria that may be used to determine if a pigmented lesion is melanocytic or not. Streaks or Projections At present, we include branching (radial streaming) and pseudopods under this name.
Chromium Proteinate (Chromium). Mentat.
- Preventing chromium deficiency.
- Athletic conditioning.
- You are pregnant or breast-feeding.
- You have kidney problems.
- How does Chromium work?
- Are there any interactions with medications?
- What is Chromium?
- Dosing considerations for Chromium.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96895
Order mentat with amex
This is largely achieved by a specialized inner lining of the airways medications that interact with grapefruit purchase 60 caps mentat free shipping, referred to as respiratory mucosa. The thick basement membrane of the respiratory epithelium is indicated by the green bracket in the lower right of the image. Above the basement membrane is a pseudostratified columnar epithelium, with cilia and goblet cells (respiratory epithelium, goblet cells indicated by the arrows). Basal cell nuclei of the respiratory epithelium are adjacent to the basement membrane. The respiratory epithelium also has sensory cells called brush cells and neuroendocrine cells called granule cells (Kulchitsky cells); neither of these cells are evident on routinely stained slides. Basic Science Correlate: Physiology the epithelial goblet cells and glands in the lamina propria secrete mucus, which coats the inner surface of the respiratory tract and prepares the incoming air (filtering, moisturizing) before exposure to the delicate alveoli. This mucus is produced continuously; cilia sweep this mucus toward the pharynx, where it is swallowed. Because the general direction of movement of most of the mucus is upward (an exception is the nasal cavity), this process is commonly referred to as the mucociliary escalator. The pseudostratified ciliated columnar epithelium (respiratory epithelium, black bracket) is shown. Numerous serous and mucous glands in that layer are outlined, which excrete their product onto the surface through a duct (arrow). The thick basement membrane (green bracket) and goblet cells (black arrows) are indicated. For example, in cystic fibrosis, a defective chloride channel results in thick mucus that is difficult for cilia to move properly. Mechanical disruption and drugs that break down the mucus are part of the treatment regimen for these patients. Because mucus movement is not optimal, patients with cystic fibrosis have lifelong complications caused by repeated respiratory infections. Now that the features of respiratory mucosa have been discussed, the histologic features of each structure of the upper respiratory system can be considered. Microtubules are responsible for the active movement characteristic of these surface modifications. Clinical Correlate Ciliary motility disorders such as primary ciliary dyskinesia (Kartagener syndrome) also cause difficulty with mucus clearance. As mentioned, the airways are designed to filter, warm, and moisturize incoming air. These structures increase turbulence of incoming air within the nasal cavity, maximizing the efficiency of conditioning the air. Conchae are supported by cancellous bone; other parts of the respiratory tract are supported by cartilage and smooth muscle. Nevertheless, this figure shows that the lining of the concha is a respiratory mucosa, which includes the respiratory epithelium and a lamina propria that has numerous glands (G) and veins (V), which are part of the venous plexus. Bone, respiratory epithelium, and lamina propria are indicated, as well as (G) glands and (V) venous plexus. Clinical Correlate Because the pharynx is the common pathway for both ingested food and air, it is not uncommon for food or liquid to be accidentally introduced into the respiratory system, causing irritation of the inner lining of the respiratory tract or, worse, choking. The olfactory epithelium is similar to respiratory epithelium but has specialized olfactory receptor cells that detect chemical odorants and transmit information to the brain via the olfactory nerve (cranial nerve I). Clinical Correlate Allergic reactions and infections cause the plexus of vessels in the nasal cavity to dilate and become leaky. The resulting edema in the lamina propria results in the characteristic congestion associated with these conditions. The epiglottis helps guide swallowed food toward the esophagus by covering the opening into the larynx. The supporting element of the epiglottis is elastic cartilage, which is firm but flexible. Most of the remaining elements of the epiglottis are typical: connective tissue, glands, and so forth. Before discussing the histology of the epiglottis, it helps to describe its orientation. The pharynx is mostly lined by stratified squamous epithelium and was discussed in detail in Chapter 31. During swallowing, the anterior side of the epiglottis comes to face the pharynx and is exposed to food sliding down toward the 38. In the image to the left, food is in the oral cavity, and the epiglottis (black arrows) is in the vertical position such that the opening into the larynx is open. As the bolus of food passes the epiglottis, muscles involved in swallowing result in movement of the epiglottis to cover the opening to the larynx (right image). Because of this, the anterior surface of the epiglottis is covered by a stratified squamous nonkeratinized epithelium (similar to the pharynx in this region). The posterior side of the epiglottis faces the lumen of the larynx during swallowing and, therefore, is covered mostly by respiratory epithelium. In the scanning view in the center, the anterior side is down and the posterior side is up (the tip is to the left). Helpful Hint the preceding discussion was a little long-winded, however, putting the epiglottis in the context of swallowing and considering the function of these epithelia will aid in remembering which epithelium is covering which aspects of the epiglottis. Red arrows represent areas covered by stratified squamous epithelium; blue arrows indicate regions covered by respiratory epithelium. Since this is a cross section through the tip of the epiglottis, both sides are lined by stratified squamous epithelium (only one side is shown). As in the rest of the respiratory system, the inner lining of the larynx is a mucosa. The laryngeal ventricle is the space (recess) between the vestibular and vocal folds (not labeled here, see subsequent images). The vocal and vestibular folds are bulges created by ligaments of the same name that lie just underneath the mucosa. The vocal and vestibular ligaments are ligaments, but when they are covered with mucosa, the entire structure (ligament + mucosa) is referred to as a fold. Helpful Hint the basic histologic features of the larynx are not too tricky, but getting oriented to these images is a little challenging, especially without the benefit of gross anatomy. It may be useful to take a moment and think about these drawings before proceeding. As mentioned, the opening to the larynx is covered by the epiglottis during swallowing. The larynx is supported by the hyoid bone, laryngeal cartilages (thyroid and cricoid cartilages and the epiglottis), and supporting ligaments. This section passes through the epiglottis and the thyroid and cricoid cartilages (although the cricoid cartilage is not in this drawing). The vocal fold contains the vocal ligament, and an adjacent vocalis muscle, also cut in cross section. The vocalis muscle and other skeletal muscles seen within the larynx are involved in speech. Helpful Hint As with the vessels in the kidney, proper identification of structures of the larynx depends largely on position. Pharyngeal tonsil Torus tubercle Nasal cavity opening via choana into nasopharynx Stylohyoideus Digastric muscle, posterior belly Soft palate M. The thyroid gland is included in this image, but it will be discussed along with the endocrine system (Chapter 42). This specimen was taken from an infant, so the cartilage and other tissues are not very well developed. Helpful Hint Remember this is a coronal section, so the folds are cut in cross section. Also, remember that the vocal folds include the epithelium and underlying connective tissue, including the vocal ligament. Note that the vestibular fold contains numerous glands, while the true vocal fold is devoid of glands. The epithelium lining each surface is indicated (green arrows point to respiratory epithelium; black arrows indicate stratified squamous nonkeratinized).
Syndromes
- Medical history
- Nausea and vomiting
- Acne or skin infections
- Blue skin, lips, or fingernails (cyanosis)
- Do you drink alcohol? How much?
- Phenothiazines
- Avoid future problems with sexual function
- Deepening of the voice
Purchase mentat 60caps amex
Diagnosis is usually made in a clinical basis but dermoscopy might be helpful to reveal equivocal lesions medications beginning with z order cheapest mentat. Histopathological dotted vessels correspond to dilated capillaries on papillary dermis and some might be thrombosed leading to the hemorrhages. Some series of patients demonstrated that naked eye evaluation was less accurate to define persistent warts after cryotherapy than dermoscopy; therefore, it should be used to optimize therapies. It is more common among children, especially with atopy and immunosuppressed individuals. It can be clinically diagnosed presenting as normochromic to erythematous papules with umbilicated center. Some cases might be challenging and dermoscopy can also lead to a correct evaluation. It is more common among children and present clinically as a patch of alopecia with tonsured hair. Definitive diagnosis is performed by culture but dermoscopy might be of great value for the initial suspiciousness. Onychomycosis Fungal infection of the nail plate is very common being responsible for 50% of the nail disorders. Clinical inspection and cultural examination are usually sufficient to diagnose the offending agent. Clinical manifestations may vary substantially but it usually occurs as erythematous excoriated papules on the axillae, wrists, interdigital spaces, and genital area. Although skin scrapping and observation of epithelial material under an optic microscope is the gold standard method for the identification of the mite, dermoscopy might play a major role in the evaluation of suspicious cases. Dermoscopy is less invasive, faster, and more practical to evaluate every necessary lesion and shows good accuracy for scabies diagnosis. These structures correspond, respectively, to the anterior aspect of the mite and to the scabiotic furrow. One clinical trial compared dermoscopy to skin scrapping for the diagnosis of scabies. They found, respectively, sensitivities of 91% and 90% and accuracies of 89% and 95% for the methods. Interestingly, patients preferred to have dermoscopy performed as it is a painless noninvasive tool. Moreover, time to evaluate the patients was significantly less also for dermoscopy corroborating that it is a fast method for this purpose. It affects most commonly the lower extremities, like the plantar region, the periungual tissue or the toes. It is usually self-limited but in some cases, if not recognized early, the infestation might lead to pain and secondary infection. In order to avoid contamination of the dermatoscope, it is recommended to use a protective plaster on the lens when touching ulcerated skin. If they do not occur, it can be safely removed only by holding the maggot with tweezers and gently pulling out. Direct transmission is very common, and prompt recognition and treatment are recommended. It is usually characterized by pruritus and by the visualization of the louse on the scalp and nits attached to the hair shafts. It is also possible to monitor treatment efficacy as empty or filled nits might be seen. Furuncular Myiasis Furuncular myiasis occurs after infestation of the skin by Dermatobia hominis maggots. Clinically, it is characterized by a painful inflammatory nodule with a central opening that does not relieve after topical or systemic antibiotics. A single lesion is usually observed but infestations by multiple maggots and consequently a variable number of lesions might be seen. Dermoscopy can be extremely important in these cases for early observation of the maggot. It is visualized better with contact dermoscopy closing the nodule opening for some minutes. If the opening is not occluded by the dermatoscope lens, Larva Migrans Larva migrans is caused by the worm Ancylostoma braziliense. It is typically transmitted after barefoot walk on contaminated soil with dogs and cats feces. Clinical history Entomodermoscopy 291 Lupus Vulgaris Lupus vulgaris is a variant of cutaneous tuberculosis and may present with distinct clinical forms ranging from isolated or multiple nodules to large plaques with "apple jelly" aspect. On dermoscopy it is possible to observe orange to golden structures and linear vessels as well as whitish streaks. Clinical aspects are variable depending on the agent and might be confounded with other skin conditions. Dermoscopy of Leishmania infantum demonstrates an erythema and other vascular structures in 100% of the cases. Additionally, yellowish tears and a whitish starbust-like pattern that correspond, respectively, to follicular plugs and parakeratosis were also described. The lesion tends to increase in length making a serpiginous pathway until the worm dies. Differential diagnosis of plantar wart from corn, callus and healed wart with the aid of dermoscopy. Epiluminescence microscopy: a new approach to in vivo detection of Sarcoptes scabiei. A case report of an irritative dermatitis with erythematous papules on interdigital areas and wrists mimicking scabies was reported. The visualization of the small black spicules instead of a potential scabies infestation reveals the correct origin of the reaction. If they are small (1 mm), it might be confounded with a pigmented lesion, even melanocytic nevi. Dermoscopy easily facilitates the differentiation and also permits us to observe remaining portions of the tick after mechanical removal. Characteristic symptoms and signs added to a particular dermoscopic pattern or structures then increase the level of suspiciousness of these groups of diseases. Although the majority of the inflammatory cutaneous diseases might not show a pathognomonic dermoscopic pattern, the observation of several structures or also the absence of others may help in characterizing them. As they show few pigmented structures, the observation of vascular patterns and colors are generally of great help. This phenomenon is seen, for example, in some melanocytic nevi (Meyerson nevus) or irritated seborrheic keratosis. Especially, the current chapter will present dermoscopic patterns and aspects of different major cutaneous inflammatory diseases that have been reported. It is always important to stress that clinical history and physical examination findings remain highly necessary in this scenario. Nevertheless, histopathologic examination should be performed in equivocal clinicodermatoscopic lesions. The clinicodermoscopic information of a homogeneous and symmetric vascular pattern occurring in an erythematosquamous reaction suggests the diagnosis of psoriasis. Histologically, it is characterized by hyperkeratosis, acanthosis, and parakeratosis; elongated rete ridges; and capillary loop dilatation. Scales are also seen in dermoscopy and their quantity may be used as a parameter for treatment. It is possible to visualize in the majority of the cases White streaks (92% of the cases), which correspond to the Wickham streaks, that can be observed frequently with the naked eye. Acute forms may show a generalized erythema with vesiculation observed with the dermatoscope. Genital lichen sclerosus lesions usually have linear vessels while extragenital lesions show keratotic plugs. Morphea also show linear vessels and a lilac ring and keratotic plugs are not observed. Generally, it is possible to observe a yellow to orange background, sometimes whitish. It might be confounded with other dermatoses and dermoscopy can also help in its recognition.
Cheap mentat 60 caps with amex
The bilaminar germ disk will elaborate into a fully developed fetus treatment bursitis buy mentat overnight delivery, a process addressed in an embryology course or text. The amniotic cavity is a fluid-filled space bounded by the amnion or amniotic membrane. The amnion is composed of two layers: an inner layer in contact with amniotic fluid (blue), which is an epithelium referred to as amnioblasts or extraembryonic ectoderm, and an outer layer of extraembryonic mesenchyme (red). As will be discussed subsequently, the amniotic cavity expands, and the amnion makes contact with the chorion to become part of the fully formed placenta. The cells of the inner cell mass differentiate, and organize into a bilaminar germ disk, flanked by a yolk sac and amnion. The connecting stalk, composed of extraembryonic mesoderm, connects the entire structure to the chorion. As implantation occurs, the uterine endometrium can be divided into three regions; the decidua basalis is between the organism and myometrium, the decidua capsularis is a thin layer covering the embedded organism, and locations away from the site of implantation are referred to as the decidua parietalis. The chorionic villi adjacent to the decidua basalis elaborate; this portion of the chorion is called the chorion frondosum (villous chorion). Villi adjacent to the decidua capsularis do not grow; this region of the chorion is called the chorion laeve (smooth chorion). Because of this, the endometrial tissue of the uterus is now referred to as the decidual layer. That portion of the decidua between the implanted embryo and myometrium is called the decidua basalis, which will form part of the placenta. The decidua covering the implanted embryo is called the decidua capsularis, which thins as the embryo expands, eventually degenerating. Early on, villi are well distributed on the chorion, surrounding the entire embryo. However, as development progresses, the villi closest to the decidua basalis continue to grow, and this region of the chorion is referred to as the villous chorion (chorion frondosum). Villi adjacent to the decidua capsularis regress; as this region of the chorion thins, it is referred to as the smooth chorion (chorion laeve). Finally, the amniotic cavity expands, and the amnion becomes apposed to the chorion. Starting from the amniotic cavity and moving to the right, the placenta consists of: 1. The amnion (amniotic membrane) contains an inner epithelium, covered by extraembryonic mesenchyme. The chorion frondosum (villous chorion) contains extraembryonic mesenchyme, cytotrophoblast, and syncytiotrophoblast. The chorion is tightly attached to the maternal decidua when the organism implants into the uterine lining. In contrast, expansion of the amniotic cavity brings the amnion adjacent to the chorion, obliterating the chorionic cavity. However, the amnion is only loosely apposed to the chorion, and these layers will separate during tissue preparation. The mature placenta is a disk-shaped structure and is ejected as part of the afterbirth. This occurs via separation of the decidua basalis from the uterine wall (somewhat similar to menstruation). The placenta consists of three layers (from fetus to myometrium): the amnion, villous chorion, decidua basalis. As the fetus grows, the lumen of the uterus is obliterated, and the smooth chorion and decidua capsularis thins. At this magnification, the amnion and flat portion of the chorion are not distinguishable (green bracket). This section includes one edge of the placenta; the thinner, curling tissue to the left is the tissue adjacent to the placenta (amnion, smooth chorion, and decidua parietalis). Again, note the amnion/chorion (green bracket), villous space (black bracket), and decidua (red bracket). Because this is a placenta at term, sloughed from the uterus as part of the afterbirth, the myometrium is not included. The maternal side includes the decidua (blue bracket) and myometrium (red bracket). The myometrium is covered by a very thin perimetrium; the space to the left of the myometrium/perimetrium is the pelvic cavity. The amnion and chorion are fused at the bottom of the slide (black bracket) but have come apart in the middle; the point of separation is indicated by the black arrow. Only the chorion is intact at the top (green bracket), and the torn amnion peels off to the right (green arrows). The point of separation is indicated by the black arrow; below that point the fetal side includes both amnion and chorion (black bracket), above that point it is simply chorion (green bracket). There is a large fetal blood vessel (X) in the chorion above the separation point. The green dashed line represents the approximate border between these two layers. The amniotic fluid on the fetal side and maternal blood in the villous space are indicated. Amniotic epithelium (amnioblasts) are indicated by the blue arrows, as well as cytotrophoblasts (yellow arrow) and syncytiotrophoblast (red arrows). Fused extraembryonic mesenchyme from the amnion and chorion forms the core of this structure; the approximate fusion point is indicated by the green dashed line. Villi are covered by cytotrophoblasts (blue arrows) and syncytiotrophoblast (red arrows). A stem villus (black arrow) projects directly from the chorion; branch villi (blue arrows) are indicated. They contain fetal blood vessels and are the site of molecular exchange between maternal and fetal circulations. Branches from the stem villi, called branch villi (blue arrows), are quite numerous and vary in shape and size. The empty space (Xs) between the villi, normally filled with maternal blood, is the intervillous space. Since villi are projections of the chorion, they are composed of a core of mesenchyme with fetal blood vessels covered by trophoblast. The outermost layer, the syncytiotrophoblast (red arrows), is a complete layer in contact with maternal blood. The nuclei of the syncytiotrophoblast are typically small and round or oval shaped; the cytoplasm is darkly eosinophilic. Cytotrophoblasts (blue arrows) form an incomplete cell layer underneath the syncytiotrophoblast. Maternal blood normally occupies the intervillous space; a few maternal red blood cells can be seen on the outer surface of the villus in the bottom left. Cytotrophoblasts (blue arrows) typically have larger, more euchromatic nuclei and paler cytoplasm than the syncytiotrophoblast layer (red arrows). The syncytiotrophoblast layer, on the other hand, is very active metabolically, with prominent rough and smooth endoplasmic reticulum, Golgi apparatus, and secretory vesicles, which accounts for its darkly stained cytoplasm. This layer has numerous microvilli, seen as a brush border on the surface in contact with maternal blood (most obvious on the surface of the largest villus). Villi are covered by cytotrophoblasts (blue arrows) and syncytiotrophoblast (red arrows); the latter shows a brush border in contact with maternal blood. The placenta at 5 months has a villus network able to provide sufficient exchange of nutrients and waste products between maternal and fetal blood. Fetal blood vessels (yellow arrows) are close to the edge of the villi, adjacent to the thinner regions of the syncytiotrophoblast. The basement membranes of the fetal endothelial cells and syncytiotrophoblast cell layer fuse. Therefore, the final barrier between maternal and fetal blood is as thin as the air-blood barrier in the lung: Syncytiotrophoblast fused basement membrane fetal endothelial cells Video 48. As the placenta develops during pregnancy, the villi continue to branch, resulting in a larger number of smaller villi that provide more surface area for molecular exchange.
Generic 60caps mentat free shipping
Each myofibril has an alternate dark-light banding pattern when viewed from the side medications with weight loss side effect 60 caps mentat with mastercard. Typically, within a single muscle, all muscle cells are the same diameter; the apparent difference seen in the diameters of these cells is due to sectioning. During development, muscle cell precursors called myoblasts fuse together to make large, multinuclear muscle cells (muscle fibers). These cells synthesize contractile proteins, which organize into myofibrils in the cytoplasm, pushing the nuclei to the periphery of the cell. Nuclei are indicated: muscle cell nuclei indicated by black arrows, fibroblast nuclei indicated by blue arrows. The blue arrows represent the path of an action potential along the surface of the muscle fiber and into the T tubule system (discussed subsequently). When skeletal muscle cells are cut in perfect cross section, stippling in the cells can be seen owing to the myofibrils cut in cross section. The alternating dark and light banding pattern (explained in detail in the next section) is caused by the alternating light and dark bands of each myofibril in the cell; and the myofibrils are arranged so that their dark bands line up side by side, as do the light bands. Because the myofibrils are in register, most individual myofibrils cannot be seen. However, during fixation, some myofibrils "slide," putting them out of register with their neighbors. That is because a section through the diameter of the cell will cut through only some of the myofibrils. As mentioned, the banding pattern seen in light micrographs of skeletal muscle is created by the collective banding present on each myofibril. Less obvious is a pale region within the A band, referred to as the H zone or H band (maroon arrows). The functional contractile unit of skeletal muscle, the sarcomere, extends from one Z line to the next (blue bracket). The yellow bracket spans an A band, and the black bracket spans an I band; the blue bracket spans a sarcomere. Helpful Hint Because a sarcomere extends from Z line to Z line, an I band is shared by two adjacent sarcomeres. Adjacent sarcomeres share the Z line; for example, in this orientation, a single Z line is the "upper" end of one sarcomere and the "lower" end of another. The banding pattern seen in the light micrographs can be visualized in greater detail in the electron micrograph, including the lighter I bands (2) and dark A bands (3). Note the Z lines (1), I band (2 and orange bracket) and A band (3 and green bracket). Orange bracket: I band; green bracket: A band; yellow bracket: H zone; red arrows indicate the M line. The red bracket indicates a myofibril that has "slid" relative to neighboring myofibrils. In other words, the thick filaments to the right of the M line are mirror images of the ones to the left. Also note that thin and thick filaments extend past each other, creating a new component of the sarcomere, the zone of overlap. It should also be pointed out that the myofibrils are cylindrical structures, not flat. Therefore, although the terms "Z lines" and "M lines" are used in reference to longitudinal sections of muscle, these structures are actually disk shaped and can be better called Z disks and M disks. The thin filaments extend into the A band (between the thick filaments) to create the zone of overlap. To solidify understanding of the organization of a sarcomere, it is useful to think about the proteins that are present in cross sections through each region of a sarcomere. Remember that the thick filaments on either side of the M line are mirror images of each other. Lines indicate cross sections, each containing a different set of sarcomere proteins. In addition, in the presence of calcium, the myosin heads can bind to and release actin thin filaments. In this way, during contraction, each head domain in the cocked position can cross bridge with an adjacent thin filament, flex, and then release. By repeating the cycle, and with all myosin heads working in the same fashion, the Z lines in a sarcomere can be pulled toward the M lines. During contraction, as a result of the action of the myosin heads, the thin filaments are pulled toward the M line. The thin and thick filaments slide past each other, a phenomenon known as the sliding filament model of muscle contraction. Note that the lengths of the thick and thin filaments do not change during contraction. However, because the thin and thick filaments "telescope" past each other, the width of the zone of overlap increases, while the H zone and I band both decrease in width. Helpful Hint Understanding how structures and zones in a sarcomere change during contraction will solidify understanding of the structure and function of skeletal muscle. Myofibrils are connected to the sarcolemma of the muscle fiber, so if all the myofibrils in a muscle fiber (muscle cell) shorten at the same time, this results in a significant and powerful shortening of the muscle cell. Since muscle cells are attached to the surrounding connective tissue (endomysium, perimysium, and epimysium), which is continuous with tendons or other structures, contraction of muscle cells in a muscle can generate movement. These action potentials travel down the T tubule system to bring the excitation wave to the center of the cell (curved blue arrows). The elaborate sarcoplasmic reticulum is highlighted by dilations called terminal cisternae, which are adjacent to the T tubules. Upon arrival of an action potential in the T tubule, calcium channels in the membrane of the sarcoplasmic reticulum open, and calcium diffuses into the cytoplasm. A-band I-band b Z-line Sarcomere contracted M-line In some tissues, the T tubules are flanked on either side by terminal cisternae. The three tubules together, a central T tubule flanked by two terminal cisternae, form a triad. Human cardiac muscle has only one terminal cisterna associated with each T tubule, forming diads. Clinical Correlate the attachment of myofibrils in muscle cells to , ultimately, the surrounding connective tissue occurs through a number of intracellular, membrane-bound, and extracellular proteins that interact with each other. One such protein is dystrophin, which is a cytoplasmic protein that anchors actin filaments to the sarcolemma. The two most common forms of muscular dystrophy, Duchenne muscular dystrophy and Becker muscular dystrophy, are caused by mutations in dystrophin. They are often challenging to identify clearly, and often only one or two components of the triad can be seen. In this case, the central vesicle is the T tubule, which is usually more elongated, flanked by rounder terminal cisternae on either side. Calcium concentration in the cytoplasm of most cells, including resting muscle cells, is very low. Calcium is stored in the sarcoplasmic reticulum, and muscle contraction is stimulated by a release of this calcium from the sarcoplasmic reticulum into the cytoplasm. The large diameter of skeletal muscle fibers requires an elaborate cellular architecture to ensure that all myofibrils receive this calcium signal at the same time. Helpful Hint the specific identification of these components in electron micrographs is not likely to be high yield. In addition, the images were oriented so that most of the muscle fibers were cut longitudinally. However, routine preparations of tissues containing skeletal muscle (embedded in paraffin instead of plastic) are not as ideally positioned as these images, so it is useful to consider these because they represent the more common presentation of skeletal muscle tissue. Note the intense cytoplasmic eosinophilia due to the tremendous amount of contractile proteins in these cells.
