
Cheap doxazosin 2mg mastercard
Terminal branch of the deep ramus that lies on the interosseous membrane in the distal third of the forearm beneath the extensors and extends to the wrist joint gastritis diet ayurveda purchase 1 mg doxazosin fast delivery. Branch that runs along the brachioradialis together with the radial artery, crosses under its accompanying muscle and then arrives at the dorsum of the hand and fingers as a cutaneous nerve. Rami of lateral cutaneous branches arising from T4-6 and passing anteriorly to the mammary region. Lateral cutaneous rami arising usually from T1, but also from T1-3 and passing to the upper arm. Branch that emerges medially and anteriorly and divides to form medial and lateral branches. Terminal rami of the superficial branch passing 25 on the radial and ulnar sides of the extensor aspect of the lateral 21/2, sometimes also 31/2 fingers. Two to three branches from the brachial plexus (supraclavicular part or posterior cord) supplying the subscapularis and teres major muscles. It courses along the lateral margin of the scapula and supplies the latissimus dorsi. It appears at the lateral margin of the psoas and courses between the kidney and quadratus lumborum, then between the transversus abdominis and internal abdominal oblique (muscular branches) to enter the inguinal canal. Sensory branches to the anterior skin of the scrotum, mons pubis and adjacent skin of the thigh. Branch that courses through the inguinal canal and supplies the cremaster muscle, skin of scrotum (labium majus) and adjacent skin of the thigh. Branch that passes through the vascular lacuna (between femoral artery and iliopectineal arch), then through the saphenous hiatus to supply the skin located there. It appears at the lateral margin of the psoas and courses beneath the iliac fascia and through the lateral part of the muscular lacuna into the thigh, where it proceeds below or above the sartorius to the lateral skin of the thigh. It passes beneath the psoas, behind the internal iliac artery and lateral to the ureter, then through the obturator canal to the adductor group and to the medial skin of the thigh. Nerve that courses on top of the adductor brevis and obturator externus muscles and beneath the adductor longus and pectineus muscles. Lateral rami of L1-3 supplying the skin up to the greater trochanter (buttock region). Sensory branch for the skin over the coccyx formed by the union of sensory fibers from the posterior rami of S1-3. They penetrate the gluteus maximus and supply the skin of the medial, upper gluteal region. Collective term for the combined lumbar and sacral plexuses joined together by fibers from L4 and mutually supplying the lower limb. Nerve network formed by spinal nerves L1-4 which lie at the anterior side of the leg. Nerve that contains sensory and motor fibers from T12 and L1 for the abdominal muscles. It traverses the psoas major, then courses between the transversus abdominis and internal abdominal muscles and pierces the latter medial to the anterior superior iliac spine. It frequently penetrates the aponeurosis of the external oblique just above the superficial inguinal ring and supplies the skin in this area. Variable terminal branch which appears between the adductor longus and gracilis muscles and supplies the distal 2/3 of the skin of the thigh. It pierces the obturator externus and supplies it and the adductor magnus and brevis. It frequently arises as an additional obturator nerve from L3-4 to supply the pectineus and hip joint. It appears at the lateral margin of the psoas and runs between the iliac and psoas major muscles to pass through the muscular lacuna. Main branches for the distal 3/4 of the anterior surface of the thigh up to the patella. It begins in the femoral triangle, passes beneath the "vastoadductor membrane", which it pierces, arrives beneath the skin between the sartorius and gracilis muscles and, together with the great saphenous vein, proceeds as far as the medial side of the foot. Plexus arising from L5-S3 and a part of L4 and S4, lying anterior to and beneath the fascia of the piriformis muscle beneath its fascia. Nerve that arises from L5-S2 and passes through the greater sciatic foramen into the ischioanal fossa from which it extends to the obturator internus muscle. Nerve that arises from L4-S1, passes through the greater sciatic foramen and proceeds down to the quadratus femoris and the hip joint. Nerve that arises from L4-S1, passes through the greater sciatic foramen cranial to the piriformis [["suprapiriform foramen"]] and then between the gluteus medius and minimus as far as the tensor fasciae latae. Nerve that arises from L5-S2, passes through the infrapiriform foramen and supplies the gluteus maximus. Nerve that arises from S1-3, passes through the greater sciatic foramen below the piriformis [["infrapiriform foramen"]] and supplies the skin on the posterior side of the thigh and proximal portion of lower leg. Branches that arise from the lower margin of the gluteus maximus and pass beneath the ischial tuberosity medially to the scrotum (labia). It leaves the pelvis through the greater sciatic foramen below the piriformis [[infrapiriform foramen]] and passes downward lateral to the ischial tuberosity, beneath the gluteus maximus and the long head of the biceps. Nerve that arises from L4-S2, branches off from the sciatic nerve at a variable level, passes in company with the biceps tendon as far as the posterior aspect of the head of the fibula and then crosses obliquely forward between the skin and fibula. It usually arises in the popliteal fossa and supplies the skin on the lateral aspect of the proximal 2/3 of the posterior side of the lower leg. It passes beneath the fascia over the lateral head of the gastrocnemius and joins the medial sural cutaneous nerve to form the sural nerve. It runs over the extensor retinacula and supplies the skin of the dorsum of the foot, the medial side of the big toe and the halves of the 2nd and 3rd toes facing one another. Lateral cutaneous branch of the superficial fibular nerve to the middle and lateral aspect of the dorsum of the foot. It proceeds beneath the peroneus longus, then lateral to the tibialis anterior muscle to supply the dorsum of the foot. Rami passing to the tibialis anterior, extensor hallucis longus and brevis, and extensor digitorum longus and brevis muscles. A 28 Dorsal digital nerves of lateral surface of great toe and of medial surface of second toe. It passes through the popliteal fossa, disappears beneath the tendinous arch of the soleus muscle and proceeds, accompanied by the posterior tibial artery, around the medial malleolus to the sole of the foot. Rami to the gastrocnemius, plantaris, soleus and the deep flexors at the lower leg. Two branches, one passing to the little toe and giving off a branch to the flexor digiti minimi brevis, the other proceeding to the interval between the 4th and 5th toes. They pass to the fibular and tibial sides of the little toe as well as to the fibular side of the 4th toe. Muscular branch passing in company with the plantar arch to the interossei, adductor hallucis and the lateral three lumbrical muscles. Arising from S2-4, it passes through the greater sciatic foramen below the piriformis [["infrapiriform foramen"]] to the ischioanal fossa. It is accompanied by the anterior tibial artery and contains fibers for the bones and tibiofibular joint. Nerve that arises from the tibial nerve in the popliteal fossa, then descends subfascially lateral to the small saphenous vein and joins the communicating branch of the com- 18 mon fibular nerve to form the sural nerve. Continuation of the medial sural cutaneous nerve after its union with the communicating branch of the common fibular nerve. It passes to the lateral aspect of the dorsum of the foot and anastomoses with the intermediate dorsal cutaneous nerve. It proceeds beneath the flexor retinaculum and the abductor hallucis to the sole of the foot which it supplies, as well as the skin and the flexor hallucis brevis and flexor digitorum brevis. They course in the interval between toes 1-4 and divide to form the proper plantar digital nerves. Cutaneous nerves passing on the tibial and fibular sides of the flexor aspect of the medial 31/2 toes. It passes beneath the flexor digitorum brevis medial to the lateral plantar artery as far as the base of the 5th metatarsal bone. Paired nerves lying on the dorsum of the penis with branches also to the underside of the penis.
Order 2 mg doxazosin with visa
Numerous rami containing sensory and taste fibers from the anterior two-thirds of the lingual mucosa gastritis ulcer diet cheap 4mg doxazosin mastercard. Synaptic station for preganglionic fibers of the chorda tympani with postganglionic fibers for the sublingual and submandibular glands. It passes 1 cm behind the lingual nerve and through the mandibular foramen into the mandibular canal. Parasympathetic ganglion located medial to the mandibular nerve below the foramen ovale. It communicates with the glossopharyngeal nerve via the lesser petrosal nerve and sends secretory fibers into the parotid gland. It exits the brain in the angle between the pons and pyramid, penetrates the dura at the level of the middle of the clivus, passes laterally into the cavernous sinus and then through the inferior orbital fissure into the orbit where it supplies the rectus lateralis muscle. Coursing in the mylohyoid groove and then below the mylohyoid muscle, this motor nerve supplies the mylohyloid muscle and the anterior belly of the digastric. It exits between the pons and olive, passes with the vestibulocochlear nerve into the petrous temporal bone and leaves it through the stylomastoid foramen. Bend in the facial nerve just below the anterior wall of the petrous temporal bone. Ramifies beneath the stylomastoid foramen, passes upward between the mastoid process and the external acoustic meatus and supplies the posterior ear muscles and the occipital belly of the occipitofrontalis muscle. It arises from the brainstem independently between the facial and vestibular nerves and transports autonomic and taste fibers. After anastomosing with various vessels, it ultimately unites with the facial nerve in the petrous part of the temporal bone. It is located in the petrous part of the temporal bone at the bend of the facial nerve. Nerve bundle with parasympathetic fibers for the submandibular gland and sensory fibers from the taste buds occupying the anterior two-thirds of the tongue. It returns to the tympanic cavity where it passes between the malleus and incus, then goes through the petrotympanic fissure [[Glaser] or sphenopetrosal fissure to subsequently join the lingual nerve. Parasympathetic ganglion located in its respective fossa near the sphenopalatine foramen. It receives preganglionic fibers from the facial nerve via the greater petrosal nerve and sends postganglionic secretory fibers to the lacrimal and nasal glands. Facial nerve plexus situated in the space accessible anteriorly between the two parotid lobes. Rami ascending over the zygomatic arch to the muscles of facial expression above the palpebral fissure and along the ear. Rami supplying the lateral part of the orbicularis oculi and the muscles of facial expression between the palpebral and oral fissures. Rami supplying the buccinator muscle and the muscles of facial expression around the mouth. It passes to the chin and supplies the muscles of facial expression below the oral fissure. It contains parasympathetic (facial nerve), sympathetic and sensory fibers destined for the pterygopalatine ganglion. Branch of facial nerve emerging from the anterior wall of the petrous part of the temporal bone. It incorporates parasympathetic and sensory fibers, and penetrates the covering plate of the foramen lacerum lateral to the internal carotid artery where it is joined by the deep petrosal nerve. Nerve carrying sympathetic fibers from the internal carotid plexus; it joins the greater petrosal nerve to form the nerve of the pterygoid canal. This parasympathetic ganglion is the synaptic site between preganglionic fibers from the chorda tympani and postganglionic fibers to the sublingual and submandibular glands. C 24 12 25 13 26 21 22 23 24 18 16 27 17 28 29 25 Sympathetic branch (to the submandibular ganglion). Its fibers arrive at the submandibular ganglion above the facial artery and pass through the ganglion without synapsing. Small rami at the inferior margin of the submandibular ganglion that supply the submandibular gland. Nerve that exits at the lower margin of the pons and passes through the internal acoustic meatus to the vestibular (equilibrium) and auditory organs. It supplies the anterior and lateral semicircular canals, utricle and anterior part of saccule. Superior branch of vestibular nerve with fibers from the macuala and ampullary crest of the superior (anterior) and lateral semicircular canals. Helical band of ganglion cells directed towards the axis of the cochlea and situated along the base of the osseous spiral lamina. It leaves the brain through the posterolateral sulcus behind the olive, courses through the jugular foramen and passes obliquely downward posterior to the stylopharyngeus muscle. It contains motor fibers for the pharyngeal constrictors and stylopharyngeus muscle and sensory fibers for the pharyngeal mucosa, tonsils and posterior third of the tongue (taste fibers) and parasympathetic fibers to the otic ganglion via the tympanic and lesser petrosal nerves. B C 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 Inferior (petrous) ganglion. It branches off from the inferior ganglion and passes between the jugular foramen and carotid canal, then through the tympanic canaliculus to the tympanic cavity. Irregularly scattered ganglion cells forming a dilatation in the course of the tympanic nerve. Sympathetic fibers of the tympanic plexus derived from the internal carotid plexus. C Communicating branch of glossopharyngeal nerve with auricular branch of the vagus nerve. It also passes to the carotid body and communicates with the sympathetic trunk and vagus nerve. Taste fibers from the posterior third of the tongue including the valate papillae which are also supplied by the lingual nerve via the chorda tympani. It receives preganglionic fibers from the glossopharyngeal nerve via the lesser petrosal nerve and sends postganglionic secretory fibers to the parotid gland. It emerges from the tympanic plexus, penetrates the anterior wall of the petrous temporal bone and leaves the middle cranial fossa through the sphenopetrosal fissure. On the right, it loops around the subclavian artery whereas, on the left, it curves around the arch of the aorta before ascending in the groove between the trachea and esophagus. Its terminal branch penetrates the inferior pharyngeal constrictor and enters the larynx, where it supplies Superior (jugular) ganglion. Branch that nal branch of the recurrent laryngeal nerve, arises from the superior ganglion of the vagus which supplies the intrinsic muscles of the nerve, passes through the mastoid canal, exits larynx except the cricothyoid and projects a through the tympanomastoid fissure and supplies communicating branch to the internal laryngeal the posterior surface of the pinna and the posterionerve. Anastorent) laryngeal nerve to the internal laryngeal motic branch from the auricular ramus to the glosnerve. A plexus below the middle pharyngeal constrictor formed by the glossopharyngeal and vagus nerves 22 Pulmonary plexus. Nerve plexus located anterior and posterior to the and the cervical sympathetic trunk. A hilum of the lung for innervation of bronchi, vesSuperior cervical cardiac branches. Branches given off at variably high cervical levels; they travel to the 23 Esophageal plexus. Nerve plexus around the esophagus formed directly by deep part of the cardiac plexus. A Nerve that arises from the inferior ganglion and passes downward medial to the internal carotid 24 Anterior vagal trunk. A esophageal plexus and containing fibers from the External branch of superior laryngeal nerve both vagi. Nerve that branches to the inferior pharyngeal Better developed posterior nerve plexus arising constrictor and then, covered by the infrahyoid from the esophageal plexus and containing fibers musculature, passes to the cricothyroid muscle. A laryngeal artery, it penetrates the thyrohyoid membrane and emerges below the mucosa of the 27 Posterior gastric branches. A epiglottic valleculae, the epiglottis and the larynx as far down as the level of the vocal folds. Its two roots unite in the they pass to the superficial part of the cardiac skull and pass through the jugular foramen toplexus accompanied by the vagus nerve. Fibers from the nucleus ambiguus which leave the accessory nerve in the jugular foramen and join the vagus nerve. They arise from the base of the anterior horn of the cervical spinal cord (C1-6) and form a trunk which ascends into the subarachnoid space of the skull where it unites temporarily with fibers from the cranial roots.
Cheap doxazosin 4mg line
Middle segment of the epididymis consisting of the convolutions of the duct of the epididymis gastritis lettuce purchase doxazosin 2mg mastercard. Inferior, terminal portion of the epididymis consisting of the convolutions of the duct of the epididymis. Wedge-shaped lobules in the head of the epididymis separated by connective tissue and formed by one or two efferent ductules. Coiled duct, 5-6 meters long, beginning at the end of the head of the epididymis where it receives the efferent ductules. It terminates at the end of the tail where it is continuous with the ductus deferens. Blind branches of the efferent ductules and duct of the epididymis representing vestiges of the caudal mesonephric tubules. Bilateral blind ductules superior to the head of the epididymis and in front of the spermatic cord (remnant of mesonephric tubules). Oval enlargement of ductus deferens just prior to joining the duct of the seminal vesicle. Mucous membrane of ductus deferens lined by pseudostratified, stereociliated, columnar epithelium. Spermatic duct formed by the union of the ductus deferens and the duct of the seminal vesicle. Erroneously designated as a receptacle for sperm, this organ is a vesicular gland which consists of a coiled tube, about 12 cm in length. Multilocular mucous membrane of the seminal vesicle lined by a simple secretory epithelium. It consists of the ductus deferens, accompanying vessels, nerves and connective tissue, together with its coverings. Outer covering of the spermatic cord, which is continuous with the fascia of the external oblique m. The fingerlike inner covering of the spermatic cord, which is derived from the transverse fascia. It lies beneath the cremaster muscle and surrounds the testis, epididymis and ductus deferens together with blood vessels and nerves. Remnant of the not completely obliterated embryological vaginal process of the peritoneum. Double-layered serous 19 covering of the testis, a remnant of the vaginal process of the peritoneum. Reflected fold of the tunica 23 vaginalis testis located superiorly at the head of the epididymis. Reflected fold of the tunica vagi- 24 nalis testis situated inferiorly at the tail of the epididymis. It is accessible laterally and is bordered above and below by the superior and inferior ligaments of 26 the epididymis. It descends from the peri- 28 toneal cavity into the scrotal sac via the inguinal canal. Fetal connective tissue band which arises from the caudal gonadal fold and guides the testis during its descent. Median part of the prostate located in front of the urethra and connecting the right and left lobes. It tends to undergo hormone-induced hypertrophy in the elderly, thus closing the urethral canal like a valve. Tracts of smooth muscle contained within the puboprostatic (pubovesical) ligament extending from the pubic symphysis to the prostate. Mucosal fold in the dorsal wall of the prostatic urethra continuous with the uvula of the urinary bladder. Elevated portion (verumontanum) of the urethral crest containing the openings of the ejaculatory duct. Blind sac in the colliculus seminalis measuring up to 1 cm in length and representing a rudiment of the paramesonephric duct. Furrow on both sides of the colliculus seminalis containing the openings of the prostatic ductules. Connective tissue tracts within the corpus spongiosum interspersed with smooth muscle. B D Cavernae corporis spongiosi Blood-filled, finely meshed spongy network within the corpus spongiosum. Delicate subcutaneous fascia with individual smooth muscle fibers, continuous with the tunica dartos of the scrotum. Numerous outpocketings in the urethral mucosa with the openings of the urethral glands. Place of entry and exit of the ovarian vessels and attachment site of the mesovarium. Thin organ capsule beneath the epithelial covering of the ovary, sometimes called the "germinal epithelium. Immature ovarian follicles, each consisting of an ovum surrounded by a single layer of follicular epithelial cells without a lumen. Endocrine gland arising from the follicular and thecal cells of the ruptured follicle. Thin connection tube, about 10 cm in length, extending from the region of the ovary to the uterus. Opening at the base of the infundibulum which communicates with the peritoneal cavity. An especially long fimbria projecting from the base of the infundibulum to the ovary where it is attached. Mucous membrane lined by ciliated columnar epithelium with glandular cells forming abundantly branched folds. Pointed extension of the uterus at the entrance of the uterine tube owing to the incomplete union of both paramesonephric ducts. Blunt lateral margins of the uterus to which the broad ligament of the uterus is attached. Cone-shaped portion of the cervix that projects into the vagina and is covered on all sides by vaginal epithelium. Transient developmental diverticulum of the peritoneum extending through the inguinal canal. Tubules derived from the caudal part of the mesonephros and situated between the lowermost branches of the ovarian artery. Posterior fornix of the vagina with its clinically very significant relationship to the peritoneal cavity. Lateral connection between the anterior and posterior parts of the fornix vaginae. Cutaneous fold emanating especially from the posterior wall of the vagina and, as a virginal membrane, partially closing off the entrance (introitus) to the vagina. Mucous membrane of the vagina lined by glycogen-rich, stratified, nonkeratinized squamous epithelium. Two longitudinal ridges in the anterior and posterior walls of the vagina produced by underlying venous plexuses. Longitudinal ridge produced by the urethra in the lower part of the anterior column of the rugae. Remains of 10-20 transversely coursing mesonephric tubules which open into the duct of the epoophoron. Dispersed remains of mesonephric tubules in the vicinity of the infundibulum of the uterine tube. Sharp-edged fold in front of the posterior labial commissure where the labia minora meet. Body of erectile tissue corresponding to the male corpus spongiosum, found primarily at the root of the labia majora. Itopensintothelowerthirdofthe vestibule between the labium minus and hymen or hymenal caruncle. Its two cavernous bodies unite at the anterior ends of the labia minora to form the glans clitoridis. Acorn-shaped cap of the clitoris connected with the bulb of the vestibule by a thin cord. Glandular duct, 1-2 cm long, which opens into the female urethra near the urethral orifice.
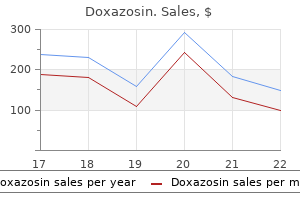
| Comparative prices of Doxazosin | ||
| # | Retailer | Average price |
| 1 | Kroger | 242 |
| 2 | Macy's | 724 |
| 3 | OSI Restaurant Partners | 922 |
| 4 | Sports Authority | 174 |
| 5 | ShopKo Stores | 290 |
| 6 | AT&T Wireless | 484 |
| 7 | Ahold USA / Royal Ahold | 457 |
Order doxazosin once a day
The lower the intensity gastritis xarelto buy doxazosin visa, or the longer the duration of exercise at the same intensity, the higher the contribution of fat as an energy source. Carbohydrate and protein molecules contain about 4 kilocalories (kcal) of energy each. One fat molecule, in contrast, contains about 9 kcal of energy, over twice the amount of carbohydrates and proteins. Many a weight-conscious person has set out to take off those extra few pounds of unwanted fat. In order for someone to reduce body fat content, he or she must reduce total caloric intake as well as engage in light-intensity aerobic exercises that will allow fat stores to be used instead of glycogen or protein stores as energy sources. Also, the rate of fat metabolism increases as duration of exercise time increases. Therefore, aerobic exercises engaged in for longer periods of time help to maximize fat metabolism. In diabetes, there is a decreased rate of entry of glucose into many tissues and an increased rate of release of glucose from the liver into the circulation, causing an extracellular glucose excess and an intracellular deficiency. With a lack of intracellular glucose, energy requirements are met by greatly increasing the rate of catabolism of fat and protein. There is decreased conversion of glucose to fatty acids (because of the low intracellular glucose level) and an acceleration of lipid catabolism because of the increased rate of lipid catabolism. The plasma level of free fatty acids may more than double, with a corresponding jump in the formation of acetyl CoA (see fig. Thus, in untreated diabetes, the blood plasma pH drops (the plasma becomes more acidic), and hydrogen ions are secreted into the kidney tubules and excreted in the urine. The resultant electrolyte and water losses may lead to dehydration, hypovolemia (decreased blood volume), depressed consciousness, and, finally, coma. Ketone bodies are found in the body under normal conditions and are used for energy by many of the body organs. Under conditions of fasting or in the case of diabetes mellitus, however, there is an increase in the rate of formation of free fatty acids from adipose tissue, which results in the production of large amounts of ketone bodies. Ketone bodies in high concentrations may lead to a fruity breath odor, a state of acidosis, coma, and even death. Therefore, people with this condition must be given food in the case of fasting, or given insulin if they are diabetics, in order to reverse these symptoms. Objective G To learn how to measure the energy content of foods and to know the terms used to express body energy expenditure. The basic unit of energy is the joule (J); but for energy as heat, one frequently uses the calorie (cal), where Su rvey 1 cal 4. The energy obtainable from a sample of food can be determined by placing it in a sealed chamber surrounded by a jacket filled with water of known volume and temperature, the whole being thermally insulated from the environment. The energy liberated by oxidation of food in the body is measured by placing a person in a chamber that is sensitive to the heat loss from the body. The oxygen taken in by way of the respiratory system is consumed in cellular oxidations. Therefore, standard tables may be used to translate the minute respiratory volume (see problem 18. The ratio of the volume of carbon dioxide produced (in a given period) to the volume of oxygen consumed (in the same period) is obtained. The total rate of body metabolism, or metabolic rate, can be measured by either the amount of heat generated by the body or the amount of oxygen consumed by the body per minute. The test is usually taken in the morning before rising, the person having fasted for at least 12 hours and having slept for 8 hours. Increases in body size, body temperature, activity, levels of thyroid hormone, and sympathetic stimulation all increase metabolic rate. The metabolic rate is 10% higher in men than in women and decreases with increasing age. Objective H To identify the essential vitamins and minerals, their sources in the diet, uses in the body, and the syndromes of their deficiency. The essential vitamins and minerals necessary for body function are summarized in tables 20. They are absorbed from the small intestine along with water and are generally not stored in the body. Heat is continually being produced as a by-product of metabolism and is continually being lost rvey to the surroundings. Transfer of heat, in the form of electromagnetic waves, from the surface of the body to the surrounding environment. Molecule-to-molecule transfer from the surface of the body to objects in direct contact with it. A cool breeze results in movement of air over the body and a consequent loss of body heat. Although fevers can result from abnormalities of the thermoregulatory mechanism or from clinical problems, they are usually caused by bacterial or viral infections. When these pyrogens are active, the body thermostat "setting" is raised, and the person feels a desire to be warmer. A slight fever may actually assist the immune system in fighting the infection, and thus help to maintain homeostasis. Heat exhaustion and heat stroke are two malfunctions of the thermoregulatory system. Heat exhaustion occurs when a person is exposed to high temperatures without drinking any liquids. The resulting drop in blood pressure due to the drop in blood volume is not countered by peripheral vasoconstriction (due to the external heat), and therefore the central nervous system receives a less-than-adequate blood supply. If body temperatures are not reduced rapidly, brain, liver, and kidney cells can be destroyed. In order to provide our bodies with the proper amounts of energy sources, we must ingest the rvey proper amounts of nutrients. Senate Select Committee on Nutrition and Human Needs recruited dietary experts to formulate U. Decrease saturated fat intake to represent only 10% of caloric intake; increase polyunsaturated and monounsaturated fats to approximately 10% of caloric intake. The synthesis of glycogen molecules for cellular storage is referred to as (a) glycogenolysis, (b) beta oxidation, (c) glyconeogenesis, (d) glycogenesis. Between meals, the blood glucose level is maintained by (a) insulin, (b) glycogenolysis, (c) lipogenesis, (d) glycogenesis. Within the cell, Krebs cycle reactions occur in (a) the neurotransmitter chemicals, (b) the ribosomes, (c) the nucleolus, (d) the mitochondria. Anabolic metabolism includes (a) processes by which substances are synthesized, (b) changes of larger molecules into smaller ones, (c) glycolysis, (d) all processes needed to maintain life. The primary role of oxygen in the body is to (a) help build amino acids, (b) allow glycolysis within the mitochondria of the cell, (c) accept electrons in the electron transport chain, (d) facilitate lipolysis within adipose cells. Vitamins are essential in metabolism because they (a) serve as structural components, (b) serve as sources of energy, (c) act as coenzymes, (d) cannot be stored in the body. The synthesis of glucose from proteins or lipids is referred to as (a) glycogenesis, (b) glucose oxidation, (c) glucosynthesis, (d) gluconeogenesis. Which hormone increases the rate of amino acid uptake by cells, protein synthesis, and glycogenolysis Reduced growth, hair loss, and vomiting may result from a deficiency of (a) iron, (b) copper, (c) potassium, (d) zinc. Important mechanisms for heat transfer include (a) evaporation, (b) conduction, (c) radiation, (d) all of the preceding. When the body is engaged in long-duration, low-intensity exercise, the principal energy source is (a) carbohydrates, (b) fats, (c) proteins, (d) glycogen. As the intensity of exercise increases, the body begins to use glucose as its sole source of energy.
Cheap doxazosin 4 mg
Four arteries arising from the dorsal carpal branch or the dorsal carpal network and passing dorsally in the direction of the interdigital spaces gastritis diet and yogurt purchase doxazosin line. Two short arteries arising from each of the dorsal metacarpal arteries and supplying the dorsum of the individual fingers. It originates from the radial artery after its entrance into the 1st dorsal interosseus muscle and divides at the flexor side of the thumb. Frequent branch of the princeps pollicis artery the radial side of the index finger. It runs beneath the pronator teres, then accompanies the flexor carpi ulnaris to terminate as the superficial palmar arch. Retrograde branch of the ulnar (or brachial) artery with the two branches listed below. Three to four arteries running along the sides of the fingers, which they principally supply. It ascends medial to the brachialis muscle to anastomose with the inferior ulnar collateral artery. Their origin is very variable but often at the level of the bifurcation of the trachea. They supply the airways up to the respiratory bronchioles including the interlobular connective tissue and the visceral pleura. Numerous fine branches to the lymph nodes and the connective tissue of the posterior mediastinum. Small branches from the lower thoracic aorta to the adjacent parts of the diaphragm. It passes through the 12th intervertebral foramen to supply the spinal cord and its membranes. Portion of the aorta extending from its entrance into the diaphragm to its bifurcation at the level of the body of L4. Branch passing through the intervertebral foramen to supply the spinal cord and its membranes. Branches passing through the intervertebral foramina to supply the spinal cord and its membranes. Mass containing arteriovenous anastomoses and epithelioid cells located at the end of the median sacral artery in front of the tip of the coccyx. Common stem of the left gastric, common hepatic and splenic arteries at the level of T12. Artery ascending in the left gastropancreatic fold to the cardiac portion of the stomach and continuing along the lesser curvature. Branch arising in the vicinity of the costal angle and running parallel to the intercostal artery. It proceeds anteriorly along the upper margin of the next lowest rib and anastomoses with the internal thoracic artery. Branch running laterally beneath the skin and ramifying both anteriorly and posteriorly. Small branches that supply the esophageal segment above the cardia of the stomach. Branch of the celiac trunk (occasionally also the superior mesenteric artery) passing to the right side toward the liver and dividing into the gastroduodenal artery and the hepatic artery proper. Besides supplying the liver, it also partially supplies the stomach, duodenum and pancreas. It passes to the upper margin of the pylorus, then along the lesser curvature of the stomach to anastomose with the left gastric artery. It passes to the right side of the hilum of the liver and supplies the right lobe. Originating from the right branch of the hepatic artery proper, it passes to the anterior and posterior surfaces of the gallbladder. Behind the lower margin of the pylorus, it divides into an anterior supraduodenal artery and the right gastro-omental artery. Inconstant first branch that supplies the anterior 2/3 and the posterior 1/3 of the duodenum. Arising behind the pancreas it follows the duodenum somewhat and anastomoses with the inferior pancreaticoduodenal artery. Branches of gastroduodenal artery that supply posterior surface of duodenum and head of pancreas. It originates at the level of the inferior margin of the pylorus and, as the continuation of the gastroduodenal artery, passes in the greater omentum different distances from the greater curvature of the stomach. Terminal branch that passes inferiorly on the pancreas and anastomoses to the inferior pancreaticoduodenal artery. It runs along the upper margin of the pancreas then through the splenorenal ligament to the spleen. Arising just at the beginning of the splenic artery, it passes downward behind the neck of the pancreas partially embedded in pancreatic tissue. Branch of the dorsal pancreatic artery passing toward the left to the lower posterior surface of the body of the pancreas. Anastomosis between the main branch of the dorsal pancreatic artery and the anterior superior pancreaticoduodenal artery. It passes from near the middle of the splenic artery downward onto the posterior surface of the pancreas, which it supplies, and anastomoses with the inferior panceatic artery. It originates from the distal end of the splenic artery or from one of its terminal branches and anastomoses with the inferior pancreatic artery in the tail of the pancreas. Arises from the gastrosplenic ligament, then passes in the greater omentum to anastomose with the right gastro-omental artery. Small vessels from the splenic artery or its branches that mainly supply the fundus of the stomach. Five to six branches of the splenic artery arising in front of the entrance into the spleen. It extends from behind the pancreas to the uncinate process and passes with its branches into the mesentery and mesocolon. It arises behind the pancreas and passes between the duodenum and pancreas to anastomose with the superior pancreaticoduodenal artery. It passes in the root of the mesentery downward and to the right toward the ileocecal junction. Anastomoses with the a scending branch of ileocolic artery and middle colic artery. Arising at the level of L3-4, it passes to the left to supply the descending colon, sigmoid colon and rectum. It passes behind the rectum into the lesser pelvis and divides into right and left branches which, after penetrating the musculature, supply mainly the mucosa up to the anal valves. It arises from the aorta in front of L1 and divides into several branches which enter the kidney. It supplies the lower segment of the kidney extending up to the posterior surface. Located on the aorta at the level of L2, crosses over the urethe adductor brevis; it anastomoses with the ter and, with the ductus deferens, passes medial circumflex femoral artery. It arises from the aorta at the level of L2 and passes to the ovary 20 Superficial branch. It lies between the gluteus maximus and medius and within its suspensory ligament. It runs along the upper margin of the gluteus minimus as far Branches that supply the infundibulum of the as the tensor fasciae latae. It below the piriformis muscle [[infrapiriform extends from the bifurcation of the descending foramen]]; its branches are distributed beneath aorta at L4 to its division into the internal and the gluteus maximus. They anastomose with external iliac arteries in front of the sacroiliac the superior gluteal, obturator and circumflex joint. It begins at the division of the common iliac artery, 25 Accompanying artery of sciatic nerve (sciatic artery). It passes cumflex femoral artery and perforating beneath the psoas muscle and the internal iliac branches.
Buy doxazosin american express
Septic shock is a subset of severe sepsis gastritis diet salad purchase doxazosin us, defined as persistence of sepsisinduced hypotension, despite adequate fluid resuscitation, which can lead to death. These are superantigen toxins that non-selectively activate the immune system (T cell) which causes a cytokine storm, followed by a multisystem disease. The staphylococcus aureas type symptoms include high fever, accompanied by low blood pressure, malaise and confusion, which can rapidly progress to stupor, coma, and multiple organ failure. In spite of medical progresses in the care of patients with septic shock during the last decades, this condition remains associated with high mortality. Early recognition and multidisciplinary management are key to the care of patients with streptococcal toxic shock syndrome. This may require: rapid diagnosis of infectious source(s) and antibiotics to treat the infection, intensive support of failing organs with oxygen to help with breathing and fluids to help prevent dehydration and organ damage, and in severe cases, surgery to remove any dead tissue. The incidence of invasive group A streptococcal infections in industrialised countries is in the order of 3 per 100,000. The use of Ig in patients, including neonates, with sepsis or septic shock will be treated in the chapter 2. The conclusions were based on a Cochrane review looking at sepsis and septic shock141 and 2 meta-analysis from 2007. The primary outcome studied was mortality at 30 days and their results showed a reduction from 33. The annual incidence for children aged below 5 years in Europe is 1/12,500-1/11,000. An attempt was made to contact the authors of the study in order to clarify these results, but no answer was received before the publication of this report. Non significant differences in any of the outcomes studied were identified when the two high-dose regimes were compared. The quality of the evidence was considered high for the primary outcomes and moderate for secondary outcomes. It is characterized by progressive, muscle weakness and atrophy, exempt of sensory impairment. Symptoms may include weakness in the hands and lower arms; cramping; and or involuntary contractions or twitching. Most people are diagnosed in their 40s or 50s, but it is a disease that can affect all ages. Since different disability scales were used in the studies, the primary outcome was defined as the proportion of patients experiencing an improvement in disability between week 2 and 4 week after treatment, compared to baseline. Primary outcomes included mean maximal grip strength of the more affected hand, and disability. The 22 participants were randomised to receive either Kiovig first for 21-25 weeks, followed by IqYmune for a further 21-25 weeks (n=12), or IqYmune, followed by Kiovig (n=10). No significant differences were found either for any of the secondary outcome measurements. The study period was 48 weeks overall, with patients receiving 24 weeks of each treatment. No statistically significant differences were found for any of the secondary outcomes studied. It is defined by too few platelets in the blood, normal bone marrow and the absence of other causes of thrombocytopenia. It causes a characteristic purpuric rash and can lead to easy or excessive bruising and bleeding. Most often the disease manifests as an acute condition in children (usually after an infection), while in adults the disease is often long term (chronicity, defined as lasting over 6 months), and has an unknown cause. In mild cases, careful observation may be enough, but very low counts or significant bleeding would usually require treatment with corticosteroids, Ig, anti-D Ig, or immunosuppressive medications. The studied outcomes included reduction in bleeding, deferred splenectomy, and time to a platelet count of greater than or equal to 20x109/L or greater than or equal to 50x109/L. Bleeding response was assessed in 4 studies only and the presence of some heterogeneity impeded clear conclusions on this regard. The authors highlighted that the overall quality of the studies was low (according to the Cochrane RoB criteria). This was used for reference checking purposes in our review of economic evidence section. It often appears days or weeks after an infection (of the respiratory or digestive tracts) and is characterized by rapid development of weakness and numbness of the limbs and often also of the facial, swallowing or breathing muscles. Treatment must be quickly put in place to limit nerve damage and most often patients are hospitalised. Originally published in 2001, it was updated in three occasions, with the last update dating from 2007. The primary outcome studied was change in a seven-grade disability scale 4 weeks after randomisation. Secondary outcomes included mortality, the proportion of patients disable at 12 months, the proportion of patients with 1 disability grade improvement at week 4 and the proportion of patients experiencing a relapse at week 12. No significant differences were captured either for any of the secondary outcomes. The evidence was rated as of having a moderate quality and a variable risk of bias. Update primary studies Our review of primary studies published after the Cochrane review by Hughes et al. Indications commonly covered in (at least 3 out of the 4) countries analysed in our international comparison. Evidence limited to kidney transplantation and in different subpopulations, limiting generalisability. As a result, the signal from the nerve to the muscle can no longer be passed on, which leads to clinical symptoms of muscle fatigue and weakness that can be generalized across multiple muscle groups but mostly skeletal muscles (and not smooth muscles and heart muscle). Myasthenia may have a stable course (called chronic) or be associated with exacerbations. Usually, the start is characterized by ocular symptoms, which in most cases changes to a generalized form. Although there is no cure for this syndrome there are well recognised treatments: cholinesterase inhibitors, corticosteroids and immunosuppressiva to reduce the production of antibodies, and thymectomy as the thymus is thought to trigger antibody production. This study was excluded from the Cochrane review because few data were available and the authors gave no response to a request for further information. It had an unclear allocation concealment for which it was considered as unclear risk of bias. These adverse events would be considered subjectively as less severe than with plasma exchange where arterial bleeding, bleeding disorders, septicaemia and venous thrombosis were reported (Gajdos 1997; Ronager 2001) but, given the available data, no statistical comparison is possible. The primary outcome was changes in the myasthenia muscle score, or quantitative myasthenia gravis score between day 1 and 15 days after the start of treatment. Conclusions Due to heterogenecity in patients, comparators and outcomes, the conclusion was broken down accordingly. They may both occur in association with gastrointestinal, pulmonary and cardiac dysfunction, while only dermatomyositis has skin involvement. They are categorised a broad group of idiopathic inflammatory diseases, also including Inclusion Body Myositis. Treatment is aimed at alleviating symptoms and often based on long-term treatment of corticosteroids. There is a frequent need to use additional treatment both to improve the disease response and to reduce the side effects of corticosteroids. Additional treatment includes immunosuppressant and immunomodulating agents such as methotrexate or azathioprine. Details on included studies can be found in the extraction tables (Supplement chapter 2).
Order doxazosin with paypal
Also eligible are patients with a hematopoietic stem-cell transplantation experiencing a hypogammaglobulinemia and life-threatening gastritis unspecified icd 9 code purchase discount doxazosin on line, or recurrent clinical significant infection, for which antimicrobial treatment is necessary. The proliferation of the plasma cell in the bone marrow can lead to bone pain and osteoporosis, and can suppress the remaining normal plasma cells. The latter may results in a shortage of normal antibody production (hypogammaglobulinaemia) with an increased risk of infections. Lymphocytes are important in the development of the different aspects of the immune response. In Belgium 1035 new diagnosis of lymphoid leukaemia were made in 2017 (age adjusted incidence rate of 8. In these malignancies, hypogammaglobulinemia can be an intrinsic aspect of the disease or may follow chemo-immunotherapy treatment regimens (iatrogenic hypogammaglobulinemia see further). Prophylaxis to prevent potentially dangerous infections due to the affected immune response can be provided with antibiotics or with Ig replacement therapy. The primary endpoints were all-cause mortality and clinically documented infections. Only for incidence of pain were similar responses recorded in both arms of patients, though not statistically significant. Most reported side-effects were mild, although in three patients they required treatment discontinuation (2 local reactions and 1 extensive skin reaction). Secondary hypogammaglobulinemia (iatrogenic hypogammaglobulinemia) caused by drug therapy Chemo-immunotherapy targeting B cells, or immune-suppressive therapy in autoimmune diseases or in transplantation intentionally target the immune system and therefore can cause hypogammaglobulinemia, especially when used as maintenance therapy. Originally introduced in clinical practice for the treatment of haematological malignancies, it has become a commonly used immunomodulatory strategy for the treatment of many refractory or poorly controlled autoimmune or inflammatory disorders. Patients receive high doses of chemoradiotherapy about 1 week before the transplantation to destroy the malignant cancer cells. This period of immunological incompetence usually starts from 1 week before allogeneic transplantation and lasts around 6 to 12 months after. This discrepancy between clinically and microbiologically documented infections could stem either from the small number of trials (only two for each comparison) or from the different definitions. The techniques and supportive treatments for patients undergoing transplantation for haematological malignancies have changed considerably during the last two decades which might need to be kept in mind when interpreting the results here mentioned. Secondary hypogammaglobulinemia in Solid organ transplantation Often, immunosuppressive therapy is necessary for 6 to 12 months after transplantation. This therapy can induce hypogammaglobulinemia which make patients after solid organ transplant susceptible to infections (iatrogenic hypgammaglobulinemia). This indication may be eligible for reimbursement in Belgium if the patient suffers from lifethreatening or recurrent clinically significant infections requiring antibiotic treatment. The primary outcome in this indication is the decrease in the prevalence of severe infections. Therapy with Ig for antibody medicated rejection is described in a separate section (see section 2. Six studies (189 enrolled patients) compared polyvalent IgG with placebo106 or no treatment. Four studies (294 enrolled patients) compared ganciclovir 117-119 or acyclovir120 combined with IgG to antiviral medication alone. One patient treated with Ig showed deterioration in mental state the day after the first infusion; the patient recovered but no further Ig was administered. It was a crossover study with two 12 week treatment periods separated by a 12 week washout period. Secondary outcomes included overall number of infections, through IgG level, hospital admissions, antimicrobial use, serious bacterial infections, acute rejection, spirometry and mortality. Mild systemic reactions including fever, chills, headache, dizziness, nausea or vomiting, diarrhoea, allergic reaction, and malaise. The disorder is caused by damage to the myelin sheath (the layer of fat covering and protecting nerve fibres) of the peripheral nerves. Physiotherapy may improve muscle strength, function and mobility, and minimize the shrinkage of muscles and tendons, and distortions of the joints. Secondary outcomes included change in mean disability score on the scale used in the original study, change in the mean disability score at 24 weeks or more, as well as (serious) side effects. Only one placebo-controlled study (n = 117), with a low risk of bias, included in this review had a long-term follow-. However, no info on the proportion of treatment responders was available, therefore, no reporting on the primary outcome was possible. The primary outcome was change in muscle strength evaluated at isokinetic dynamometry. Other side effects were mild with two fever and nausea, two a dermatological reaction and six a headache. There were in total six dropouts but no information was available on whether this was related to side effects. One acute allergic skin reaction occurred in the low-dose group which led to treatment discontinuation. Signs of sepsis include fever, hypothermia, rapid heart rate and respiration; and a laboratory finding of increased or decreased white blood cell count138. They looked at the evidence for immunotherapy in adult patients with definite or probable dermatomyositis or polymyositis. This is achieved with immunosuppressive agents such as systemic glucocorticoids, usually administered for a long duration and often in a combination with corticosteroid-sparing immunosuppressant agents such as azathioprine, mycophenolate mofetil/mycophenolic acid and rituximab. Time to escape from protocol was significantly prolonged in the 400-mg group but not in the 200 mg group, when these groups were compared to placebo; and a significant dose-response relationship among the 3 treatment groups was observed (P<0. Five patients relapsed, but attained complete remission after a second dose of IgG. Depending on the cause, the course can be acute and selflimiting or chronic with rare spontaneous remissions. Acquired anemia may be primary or secondary to a variety of neoplastic, autoimmune, or infectious diseases especially B19 parvovirus; or to exposure to various drugs. In patients unresponsive to corticoids, immunosuppressants are used as well as hematopoietic stem cell transplantation. Because of the diversity of the pathogenicity, different treatment approaches are necessary. No optimal dosing strategy exists but as reported in a retrospective study on 133 cases, most cases use 2g/kg usually divided over 5 days (400 mg/kg/d (similar as in immune thrombocytopenic purpura). Adverse events were seen in 18/133 patients: acute renal failure in 9 (including 6 kidney transplant recipients); fever, rash, and joint pain in 7; and left ventricular failure in 2 patients. This is justified in view of the limited evidence which appears to focus in these particular populations. On the subgroup of patients with hypogammaglobulinemia (11 cases described in a nonsystematic review). There are different mechanisms of rejection, depending on which part of the immune system is primarily activated, either the cellular T cell response or the humoral antibody mediated response. After transplantation, the development of de novo donor-specific antibodies increase the possibility of rejection, which can occur either acutely. The therapeutic strategy is to neutralise and stop the production of the donor specific antibodies. These studies showed some benefit, however, they failed to show a statistically significant reduction of transplant rejection. The thrombocytopenia is caused by maternal alloantibodies against fetal platelet antigens that the foetus has inherited from the father. As maternal screening is not routinely performed, and first pregnancies can be affected, most cases are diagnosed at delivery of a first affected pregnancy. However, in the absence of neonatal screening, it is likely that the true incidence is higher. The treatment started at Postnatal treatment of severe foetal thrombocytopenia considers the administration of antigen-negative platelets until the platelet count recovers, usually 7 to 10 days following birth. Although underpowered, the study did not found differences of a lower weekly dose of 0,5g/kg compared to the standard 1g/kg/ week. However, they also identified other potentially interesting indications for which very limited evidence exists at present, but that would still be worthwhile mentioning.

Order doxazosin on line amex
It weighs about 255 grams in the female and 310 grams in the male gastritis diet 411 purchase doxazosin 2 mg with amex, accounting for about 5% of the body weight. The pericardial sac is the actual compartment formed by the pericardium that encloses the heart. The pumping action of the heart then circulates the oxygenated blood through the body and returns deoxygenated blood to the lungs for removal of carbon dioxide. The inner serous layer of the pericardium secretes pericardial fluid that lubricates the surface of the heart. Pericarditis is an inflammation of the parietal pericardium that increases the secretion of pericardial fluid into the pericardial cavity. Because the fibrous layer of the pericardium is inelastic, the increase in fluid pressure impairs ventricular contraction and blood flow through the heart (cardiac tamponade). Objective B Su To trace the development of the embryonic heart from day 18 through day 25. Development of the heart from undifferentiated mesoderm requires only 7 or 8 days. On day 19 rvey after conception, specialized cells within the cardiogenic area begin to migrate toward each other medially from the two longitudinal bands of splanchnic (visceral) mesoderm. By day 21, a hollow center has developed in each cluster, and the structure is called a heart tube (fig. By day 23, the heart tubes have fused into a single medial endocardial heart tube. By day 25, fusion is complete, dilations are occurring, and blood is being pumped. Partitioning of the heart chambers begins during the middle of the fourth week and is complete by the end of the fifth week. It is during this crucial period that congenital conditions such as heart murmurs, septal defects, patent foramen ovale, and stenosis may develop. Objective C Su To contrast the three layers of the heart wall with respect to structure and function. The myocardium, especially in the ventricular walls, where forceful contraction is necessary to pump the blood throughout the body. The fibers of cardiac muscle are arranged in such a way that the intrinsic contraction results in an effective squeezing or wringing of the chambers of the heart. It consists of upper right and left atria that pulse together, and lower right and left ventricles that also contract together. The atria are separated by the thin, muscular interatrial septum, and the ventricles are separated by the thick, muscular interventricular septum. As blood is ejected from the atria, the chordae tendineae are relaxed, with valvular opening. But as the ventricles (and with them the papillary muscles) contract, the chordae tendineae are pulled taut, preventing eversion of the valves and backflow of blood from the ventricles into the atria. The pulmonary circuit (through the lungs) involves the right ventricle, which pumps deoxy- rvey genated blood to the lungs; the pulmonary trunk and pulmonary arteries; a capillary network in the lungs; the pulmonary veins; and the left atrium, which receives the oxygenated blood from the lungs. The systemic circuit involves the left ventricle and the remainder of the arteries, capillaries, and veins of the body. The right atrium of the heart receives deoxygenated blood from the systemic circuit. The healthy heart is able to pump the circulating blood volume through both the pulmonary and systemic systems. When the heart is damaged (by myocardial infarctions or long-standing high blood pressure, for example), it is unable to maintain the delicate balance between blood volume and the ability to pump. Fluid backs up in the lungs when the left ventricle fails, resulting in shortness of breath, cough, and respiratory distress. When the right ventricle weakens, fluid builds up in the peripheral tissues, leading to edema (swelling in the extremities) and liver engorgement. The ventricles then contract, forcing blood into the ascending aorta and pulmonary trunk (fig. The softer "dub," or second sound, is produced by the closing of the semilunar valves. Objective F Su To explain how the fetal circulation differs from the circulation of a newborn. Fetal circulation involves an umbilical cord that connects the placenta and the fetal umbilicus. The umbilical cord consists of an umbilical vein that transports oxygenated blood toward the heart and two umbilical arteries that return deoxygenated blood to the placenta. A ductus venosus allows blood to bypass the fetal liver, a foramen ovale permits blood to flow directly from the right atrium to the left, and a ductus arteriosus shunts blood from the pulmonary trunk to the aortic arch. The cardiovascular structures of the fetus undergo gradual transformations following birth to become other structures that persist throughout life. The umbilical vein forms the round ligament of the liver; the umbilical arteries atrophy to become the lateral umbilical ligaments; the ductus venosus forms the ligamentum venosum, a fibrous cord in the liver; the foramen ovale closes at birth and becomes the fossa ovalis, a depression in the interatrial septum; and the ductus arteriosus closes shortly after birth, atrophies, and becomes the ligamentum arteriosum. Many newborn babies with congenital heart defects have insufficient oxygenated blood in the systemic circulation. One common congenital problem is a patent foramen ovale, in which the interatrial opening fails to close. The result of this and the other congenital heart defects is cyanosis, a bluish discoloration, and the infant is commonly called a "blue baby. Blood supply to the myocardium is provided by the right and left coronary arteries, which exit rvey the ascending aorta just beyond the aortic semilunar valve (fig. The left coronary artery gives rise to its major branches, the anterior interventricular and circumflex arteries, and the right coronary artery gives rise to the posterior interventricular and marginal arteries. The great cardiac vein and the middle cardiac vein return blood from the myocardial capillaries to the coronary sinus, and from there to the right atrium (fig. If a branch of a coronary artery becomes constricted or obstructed by an embolus (clot), the myocardial cells it supplies may experience a blood deficiency called ischemia. Death of a portion of the heart from ischemia is called myocardial infarction (heart attack). The conduction system consists of nodal tissues (specialized cardiac muscle fibers) that initicause the coordinated contractions that empty the heart chambers. It typically depolarizes spontaneously at the rate of 70 to 80 times per minute, causing the atria to contract. Stimulation of the conduction myofibers causes the ventricles to contract simultaneously. These autonomic impulses are regulated by the cardiac centers in the hypothalamus and medulla oblongata. The effects of the two neurotransmitters-the former secreted by sympathetic postganglionic neurons, the latter by parasympathetic postganglionic neurons-are antagonistic. The atria and ventricles go through a sequence of events that are repeated with each beat. Consequently, no blood moves for this brief period of time, and pressure increases dramatically. At the moment the pressure within the ventricles is greater than the pressure Ventricular within the pulmonary trunk or aorta, the semilunar valves open. As the blood exits the ventricles, the pressure within them decreases until the ventricular pressure is lower than the pressure of the aorta and the pulmonary trunk, in which case, the semilunar valves close once again. This interval begins when the semilunar valves close at the end of Isovolumetric ventricular systole and concludes at the moment that pressure within the relaxation ventricles is lower than the blood pressure within the atria. Valves damaged by disease may fail to open or close completely, thereby causing turbulence. Cardiac output, which is the volume of blood pumped by the left ventricle in 1 minute, may be calculated from the formula Cardiac output (C. By the Fick principle, the amount of a substance taken up by an organ (or the whole body) per unit time is equal to the arterial level (A. It also initiates the release of epinephrine and norepinephrine from the adrenal medulla, which increase the cardiac output. Both conditions produce a decrease in the total peripheral resistance, and therefore an increased cardiac output.
