
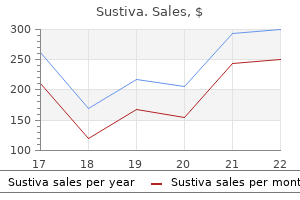
Buy sustiva 200 mg mastercard
The expression of Lhx3 and Lhx4 is in fact dependent on Pitx factors 9 medications that cause fatigue discount sustiva 600mg mastercard, and thus, the Pitx pair of factors may be considered to be at the top of a regulatory cascade for pituitary development. Interestingly, the double Lhx32/2Lhx42/2 mutant mice pituitary exhibits blocked development at the early pouch stage; it is thus a phenocopy of the double Pitx1/2 mutant [24]. The single Lhx3 and Lhx4 mutants have less-pronounced phenotypes, indicating that the actions of the two Lhx factors are also partly redundant with each other [25]. The phenocopy of the Pitx12/2Pitx22/2, and Lhx32/2/Lhx42/2 pituitary phenotypes clearly suggests that many of the actions of the Pitx factors are mediated through the Lhx3/4 factors. It thus marks the two sides of the developing neuroendocrine hypothalamo-pituitary system [28,29]. The expression of critical transcription factors for either pituitary organogenesis or cell differentiation is listed in the middle column whereas the consequence of their gene inactivation is listed on the left. The position of the various mouse genotypes along the developmental time sequence indicates the stage at which pituitary development is interrupted by these mutations. Inactivation of the mouse Hesx1 gene results in complex brain, optic and olfactory developmental defects; pituitary development is also perturbed, ranging from complete absence to multiple invaginations and nascent glands [32]. Other Tle-related proteins are expressed during pituitary development and interestingly, inactivation of Aes that is transiently expressed in the pituitary results in bifurcated pouches and dysplastic pituitaries [33]. A striking demonstration of the importance of tissue interactions for pituitary development was provided by the reproduction in tissue culture of self-forming pituitary pouches in association with aggregates of neural cells [34]. This culture system thus reproduces the normal developmental scheme, highlighting the critical role of interactions between neural and surface ectoderms. However, Prop1 is also required for activation of the Pit1 transcription factor gene, as indicated by its name [35,40], which is itself required for differentiation of the somatotroph, lactotroph, and thyrotroph lineages. Hence, Prop1 mutants are deficient in these lineages [35,40,41] but the mutation does not prevent corticotroph, melanotroph, or gonadotroph differentiation. The early phases of pituitary development are accompanied by complex and dynamic patterns of expression for many signaling molecules involved in development and organogenesis [45,46]. The portion of this pouch that is in close contact with the infundibulum will differentiate into the intermediate lobe. The first sign of glandular development is observed at the ventrorostral tip of the early gland where cells appear to leave the epithelial layer to take a more disorganized mesenchymal appearance. This period of transition is accompanied by intense cell proliferation and differentiated cells appear at the same time, as discussed below. At early stages, this mutant gland appears to be larger than normal but it then decreases in size through cell loss by apoptosis [38,39]. We are thus still lacking a coherent and complete picture for the multiple actions of these signaling molecules. Another important signaling molecule for pituitary development is Sonic Hedgehog (Shh). In contrast, Shh target genes such as Patched1 are expressed in the developing pituitary, indicating that it is responsive to Shh signaling. These patterns are thus suggestive of an important role for the Shh pathway in pituitary induction. However, the Shh2/2 mutant mouse was not extremely informative in precisely defining this role since Shh is critical for formation of midline structures and the bulk of these structures are affected in the Shh mutants [50]. Nonetheless, the importance of Shh signaling for early pituitary development is also supported by mouse mutants for the Gli zinc finger transcription factors that mediate the effects of the Shh pathway. Indeed, the double mouse mutant Gli12/2; Gli22/2 fails to develop the pituitary whereas the single Gli22/2 mutant exhibits variable defects in pituitary formation [51]. The Wnt pathway also appears important for proliferation and/or survival of pituitary cells, but again the large number of Wnt molecules and their receptors expressed in and around the developing pituitary make it difficult to develop a coherent and complete picture of their role. Canonical Wnt signaling involves beta-catenin and targeted deletion of this gene using a Pitx1-Cre transgene resulted in a small pituitary, together with deficient Pit1 expression and Pit1-dependent lineages [30]. It was suggested that beta-catenin is acting directly on the Pit1 gene to regulate its expression through interaction with the upstream factor Prop1. Finally, the Notch pathway is also active in early pituitary development and recent work has suggested that its major involvement may be in pituitary progenitor cells; hence, this aspect is discussed below. The hormonecoding genes have also served as a starting point to identify cell-autonomous transcription factors that are involved in their own expression but also in lineagerestricted functions and differentiation. Hence, most of what we know about pituitary cell differentiation relates to the terminal stages of differentiation for each lineage and involves cell-restricted transcription factors that are responsible for terminal differentiation. However, the analysis of their loss-of-function mutations has provided considerable insight into the relationships between different lineages. Investigation of the Jackson and Snell dwarf mice that carry Pit1 mutations thus revealed the requirement for this Pou-homeo transcription factor for differentiation of three lineages, the somatotrophs, lactotrophs, and thyrotrophs [56,57]. Analyses of Pit1 mutants in both mice and humans thus supported the model of a common precursor for these three lineages [58]. Similarly, the Tpit2/2 mutant mice revealed an antagonistic relationship between corticotrophs/ melanotrophs and gonadotrophs, suggesting that these lineages share a common precursor [59]. Although consistent with current data, this model has not been ascertained more directly. A scheme for sequential differentiation of cells in the developing pituitary was derived from studies of mutants for the critical cell-restricted regulators of differentiation. The salient features of this model and its regulatory molecules are discussed below in greater detail for each lineage. This idea was challenged by the discovery that all somatotrophs are interconnected and form a homotypic network [60]. The exchange of signals between cells of homotypic networks may serve to mount a strong and coordinated secretory response and to adjust local blood flow accordingly. Network plasticity is also implicated in adaptation of the prolactin response to lactation and this is mediated through changes in gap junctions between lactotrophs [63]. The relationship of the corticotroph network to the capillary bed is also striking as this network is often the furthest away from capillaries, whereas the gonadotroph network is closer to capillaries. Nonetheless, cells of both lineages have direct intimate contact with capillaries and these also rely on cytonemes [64,65]. Indeed, upon differentiation, newly differentiated cells migrate towards each other to establish homotypic contacts [65]. The first cells to reach terminal differentiation and to organize into a network are the corticotrophs that form streaks on the ventral surface of the developing pituitary; the streaks then infiltrate dorsally into the soma of the developing gland. It is presently not clear whether the initial establishment of the corticotroph network might serve a scaffolding role for organization of the other homotypic networks and, further, the molecular basis of these interactions remains undefined, although lineage-specific patterns of cadherin expression were described [66]. These cells exit the cell cycle upon expression of the cell cycle inhibitor p57Kip2 and the same cells coexpress detectable levels of cyclin E [69]. These double-positive cells do not express any markers of hormone-producing cells and thus appear to be progenitors or precursors that have recently exited the cell cycle. These differentiated cells switch off p57Kip2 expression and switch on the related p27Kip1 in its place. Expression of p27Kip1 is maintained throughout adulthood in normal differentiated pituitary cells, I. The expression of various cyclins and cell cycle inhibitors of the Cip/Kip family is shown below a diagram representing different stages of pituitary cell differentiation, starting from cycling progenitors to differentiated adult hormone-producing cells. Distinct developmental roles of cell cycle inhibitors p57Kip2 and p27Kip1 distinguish pituitary progenitor cell cycle exit from cell cycle re-entry of differentiated cells. Both loss-of-function mutations for p57Kip2 and gain-of-function transgenic experiments have supported the model that p57Kip2 is responsible for driving pituitary progenitors out of the cell cycle [69,70]. Expression of p27Kip1 in differentiated cells is required to restrain cell cycling of these cells as supported by the presence of cycling differentiated cells in p27Kip12/2 pituitaries [69]. These later observations clearly indicate that mechanisms of cell differentiation are independent of cell cycle exit. Conversely, at least one model of blocked pituitary differentiation, the Tpit2/2 intermediate lobe, indicated that expression of p27Kip1 is not dependent on differentiation, although switch-off of p57Kip2 expression appears to be partly dependent on this process [69]. However, p27Kip1 participates in silencing the pluripotency state by directly repressing the pluripotency Sox2 gene [74].
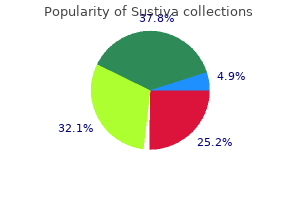
Buy sustiva australia
Latent and Acquired (De Novo) Liver Disease Liver diseases that develop post-transplant and not related to the original native liver disease may occur mueller sports medicine generic sustiva 200 mg overnight delivery. Additionally obesity is a major post-transplant complication, with up to one-fifth of patients becoming obese within 2 years after surgery; consequently de novo non-alcoholic fatty livers may develop post-transplant in a large minority of patients, and non-alcoholic steatohepatitis has also been reported. The histologic features of the acquired diseases are the same as those seen in the non-transplant patients, with treatment modalities the same. Of note is that it is not uncommon for liver biopsies performed greater than 1 year post-transplant to show only mild non-specific changes not related to rejection or disease recurrence. This can occur in anywhere from 20 to 30% of patients during the first 3 years post-transplant, the prevalence considerably increasing with time. Work-up often reveals no known cause such as biliary tract disease or known infection. These features may then persist and most likely represent an acquired or de novo liver disease of undetermined origin; alternately the changes could represent an unusual atypical variant of mild acute cellular rejection. The portal tract exhibits a lymphocytic and plasma cell infiltrate with periportal interface inflammatory activity. High power shows an increase in portal plasma cells which are arranged in small clusters. It is seen in recipients of bone marrow transplants for various hematologic disorders such as leukemias resistant to appropriate chemotherapy, and in recipients of small bowel transplants, with the risk and severity of the disease related to the degree of lymphoid cells infused and the genetic mismatch between donor and recipient. The transaminases are increased to variable degrees, the alkaline phosphatase is usually elevated and sometimes markedly so, and jaundice occurs in about half of the patients and can worsen with ongoing disease progression. It usually occurs >100 days post-transplant and is characterized by wasting, skin and pulmonary involvement. Veno-occlusive disease (sinusoidal obstruction syndrome) also is seen in up to one-fifth of patients and is related in part to pre-transplant irradiation and high dose conditioning regimens (busulfan, cyclophosphamide) for bone marrow ablation. Additional risk factors include female gender, pre-existing liver disease (in particular hepatitis C infection), and allogenic transplantation. It usually occurs within 30 days post-transplant with a mortality of up to 50% in the more severe cases. Local activation of the coagulation cascade and stellate cells with luminal narrowing of the terminal hepatic venules, endothelial cell injury, and resultant impediment of vascular blood flow with ischemic damage occurs. Rapid diagnosis and early intervention with use when necessary in severe cases of various anti-thrombotic agents. Lymphocytes can be seen infiltrating beneath the duct basement membrane, although this feature is usually mild. The interlobular ducts show considerable cytologic distortion, with cytoplasmic vacuolization, nuclear irregularity, and distortion of the duct lumen. With time duct loss may occur, with portal fibrosis of variable degrees sometimes seen. The parenchyma may show spotty inflammation and mild steatosis, with cholestasis present in some instances. Infrequently a more prominent lobular inflammation sometimes associated with perivenular necrosis can be seen and can mimic an acute hepatitis. Hemosiderin deposits within the Kupffer cells, portal macrophages and sometimes within periportal hepatocytes are common and are related to the multiple transfusions usually associated with hematologic malignancies. This enables a more succinct correlation with the numerous etiologic factors aiding tumor development. With the exception of cavernous hemangiomas, the benign lesions are significantly less common than the malignant tumors and are also not associated with underlying chronic liver diseases. Although in many instances the histologic diagnoses are straightforward, many times there is a definite challenge in differentiating these tumors from their malignant counterparts. The incidence has decreased over the years due to a decrease in dosages and the types of hormones used. In addition, hepatocellular adenomas associated with the glycogen storage diseases tend to be multiple, occur more commonly in men than women (ratio 2: 1), and often develop before the age of 20 years. Hepatocellular adenomas, however, also develop spontaneously with no definite risk factor and affect men and women equally. In addition, these tumors do not tend to occur associated with any primary liver disease. About one-third are asymptomatic with the diagnosis made on chance discovery with slightly abnormal liver tests; however almost half present with abdominal pain and discomfort. In addition, in about 20% of patients, symptoms with severe pain arise due to intra-tumor necrosis and hemorrhage, and occur generally with larger tumors Hepatocellular Adenoma (Liver Cell Adenoma) Epidemiology and Clinical Presentation Hepatocellular adenomas are rare benign epithelial neoplasms composed entirely of hepatocytes arranged in normal sized hepatic cords. These tumors were exceptionally rare before the advent of oral contraceptive usage in the 1960s, with only very rare case reports. The greatest risk occurs in women older than 30 years who have been taking oral contraceptives for greater Pathology of Liver Diseases, First Edition. Rarely patients can also present as an abdominal emergency due to massive intraperitoneal hemorrhage, and infrequently the tumor may also occur in children. Liver tests may be normal or show only slight elevations of the aminotransferases. Hepatocellular adenomas appear as cold nodules on technetium-99m (99mTc) sulfur colloid scans. Withdrawal of oral contraceptives is the treatment of choice, although tumors may still remain. Surgical resection is an option but often favored, especially in the larger lesions >5 cm, in symptomatic patients with the risk of hemorrhage and rupture, and in the subgroup of patients with the -catenin-activated mutation who are at risk for the development of hepatocellular carcinoma. Arterial embolization can be used to control bleeding, and radiofrequency ablation can be used in the smaller tumors. Finally liver transplantation is also an option in those patients with symptomatic multiple adenomas involving both right and left lobes. Of note is that because of the awareness of malignant potential in this subgroup of patients, surgery with complete resection has made this complication much less common. Pathogenesis with Gene Alterations and Mutations the pathogenesis of hepatocellular adenomas is multifactorial. The adenomas are monoclonal and can be classified into subcategories related to specific gene alterations and mutations (Table 13. Subclassification is particularly important in identifying the -catenin-activated mutation, where the adenomas show (1) diffuse strong staining of overexpressed glutamine synthetase, and (2) nuclear staining with -catenin. Although the overall frequency of malignant transformation 268 13 Hepatic Tumors, Benign Table 13. Hepatocellular adenoma management and phenotypic classification: the Bordeaux experience. Male patients tend not to occur more frequently in the -catenin subgroup, although the male population is still at high risk of developing hepatocellular carcinoma in this subgroup of patients. In about a quarter of cases multiple nodules (two to five) can occur, this feature often seen in patients with glycogen storage diseases. Additionally in about 10% of cases numerous nodules (>5) scattered in both lobes can also be seen (adenomatosis). The tumor is usually well circumscribed, and although a distinct capsule is not usually present, a thin fibrous capsule can occur in the larger lesions. The hepatocytes are cytologically benign with small nucleoli and a normal to minimally increased nuclear: cytoplasmic ratio, forming hepatic cords one to two cells thick. Areas of dense white discoloration can also occasionally be seen secondary to reactive scar formation from previous tumor necrosis. The cells also tend to be slightly larger than the adjacent non-tumor hepatocytes. The nuclei are usually regular with small to inconspicuous nucleoli; sometimes bi-nucleated forms can also be seen. Sometimes the definite cord-sinusoid pattern cannot be appreciated when the cells are hydropic, whereby a reticulin stain confirms the one to two cell thick cords.
| Comparative prices of Sustiva | ||
| # | Retailer | Average price |
| 1 | Walgreen | 740 |
| 2 | SUPERVALU | 528 |
| 3 | Best Buy | 108 |
| 4 | Michaels Stores | 499 |
| 5 | Bon-Ton Stores | 159 |
| 6 | Ross Stores | 710 |
| 7 | Dell | 417 |
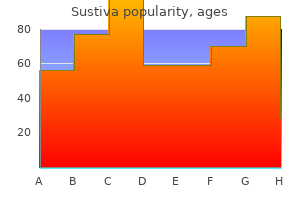
Buy cheap sustiva 200mg online
However treatment centers of america buy cheap sustiva 600mg on line, recent studies, using a visual analogue scale, have demonstrated that the onset of thirst occurs at a considerably lower plasma osmolality than was previously recognized; the values were similar to those of the threshold for vasopressin release [84,85]. The presence of such cold-sensitive oropharyngeal receptors may explain the desire of severely dehydrated patients, i. There are considerable variations between individuals in osmoreceptor sensitivity and in the threshold for vasopressin release; however, these individual values remain constant for a relatively short period of time [90]. To determine whether these interindividual differences are genetically influenced, Zerbe [90] compared vasopressin osmolality relationships within monozygotic and dizygotic twin pairs. The threshold and sensitivity values correlated significantly within monozygotes but not within dizygotes, suggesting a genetic determinant for the set of the osmoregulatory system. Pregnancy causes a lowering of the threshold for vasopressin secretion without altering the gain of the osmoreceptors in both rats [91] and humans [92], thus accounting for the hypoosmolality of pregnancy. A role for human chorionic gonadotrophin in lowering this osmotic threshold has been postulated [93]. Baroregulation It is now well established that afferent neural impulses arising from stretch receptors in the left atrium, carotid sinus, and aortic arch inhibit the secretion of vasopressin. Conversely, when the discharge rate of these receptors is reduced, vasopressin secretion is enhanced (for review see Ref. Moreover, the relative potency of the cardiac and sino-aortic reflexes in the release of vasopressin appears to vary among species. For example, the increase in plasma vasopressin that occurs during moderate hemorrhage in the dog is attributable primarily to reflex effects from cardiac receptors; sino-aortic receptors appear to exert only minor influences on vasopressin release in this situation. In contrast, sino-aortic receptors appear to play the dominant role in eliciting vasopressin secretion during blood loss in nonhuman primates and humans [94]. An enhanced osmoreceptor sensitivity, but blunted baroregulation, has been described in elderly subjects [99]. Hormonal Influences on the Secretion of Vasopressin Studies on the direct effects of various peptides and other biological substances on the release of vasopressin may be confounded by the hemodynamic effects of these substances, which indirectly modulate vasopressin release via the cardiovascular reflexes. For example, the infusion of pressor doses of norepinephrine increases both arterial blood pressure and left atrial pressure. Each of these changes is capable of eliciting a reflex inhibition of vasopressin release which should reduce plasma vasopressin. However, the inhibitory effects of the sino-aortic and cardiac reflexes on vasopressin release seem to be offset by the direct stimulatory effect of circulating norepinephrine. A similar situation may exist with the possible stimulation of vasopressin release by angiotensin. The direct stimulatory effect of angiotensin may be offset by inhibitory influences elicited from the cardiovascular reflexes. Angiotensin is a well-known dipsogen and has been shown to cause drinking in all the species tested [100]. These effects occurred at plasma angiotensin concentrations that were well above those measured under physiological conditions associated with thirst and vasopressin secretion, such as water deprivation. Minus numbers to the left indicate percent fall, and positive numbers to the right, percent rise in blood volume or pressure. The presence of endogenous opioid peptides and opioid receptors [109] in the neural lobe has led to the suggestion that opioid peptides play a role in the release of neurohypophyseal hormones. Vasopressin coexists with dinorphin in large dense core vesicles of magnocellular cells [12]. It is now recognized that opioid drugs exert their pharmacologic effects through an interaction with specific receptors. Agonists such as morphine and methadone are responsible for the classical opiate effects of analgesia, respiratory depression, and physical dependence. In contrast, agonists have analgesic properties, but do not cause respiratory depression or physical dependence at the dose required for analgesia. They have been shown to cause a water diuresis in experimental animals and in humans, probably by the inhibition of vasopressin secretion [111]. Vasopressin secretion is under the influence of glucocorticoid-negative feedback [114] and the vasopressin responses to a variety of stimuli (hemorrhage, hypoxia, hypertonic saline) in normal humans and animals appear to be attenuated or eliminated by pretreatment with glucocorticoids. In all other cases of suspected central diabetes insipidus, these nonosmotic stimulation tests will not give additional clinical information. These are four of 701 members of the rhodopsin family within the superfamily of guanine nucleotide (G)-protein-coupled receptors (see also the perspective by Perez [118] and comments on X-ray structure breakthroughs in the transmembrane-spanning region [119]). The V2 receptor, on the other hand, preferentially activates the G-protein, Gs, resulting in the activation of adenylyl cyclase. V1b receptors are expressed in the anterior pituitary [122] and kidney [123] as originally reported and also in brain, uterus, thymus, heart, breast, and lung. V2 transcripts are abundantly expressed in cells of the renal collecting ducts (in humans and rodents) and in cells of the thick ascending limbs of the loops of Henle (in rodents only) [126]. Species specificity and partial agonist activity have frustrated the search to discover antidiuretic hormone receptor antagonists that are effective aquaretic agents in vivo. The orally effective nonpeptide V2 antagonists are aquaretic drugs potentially useful to treat various clinical syndromes with abnormal water retention [128]. The 2003 Nobel Prize in chemistry was awarded to Peter Agre and Roderick MacKinnon, who solved two complementary problems presented by the cell membrane: how does a cell let one type of ion through the lipid membrane to the exclusion of other ions This contributed to a momentum and renewed interest in basic discoveries related to the transport of water and indirectly to diabetes insipidus. The topology of adenylyl cyclase is characterized by two tandem repeats of six hydrophobic transmembrane domains separated by a large cytoplasmic loop and terminates in a large intracellular tail. Microtubules and actin filaments are necessary for vesicle movement toward the membrane. It is unlikely that loss of function of this gene results in a severe phenotype in humans. These specialized permeability properties permit the excretion of large volumes of hypotonic urine formed during intervals of water diuresis. Similar results are obtained by sectioning the hypophyseal hypothalamic tract above the median eminence. Sections below the median eminence, however, produce only transient diabetes insipidus. This antidiuresis is probably due to vasopressin release from injured axons and may last from a few hours to several days (because urinary dilution is impaired during this phase, continued water administration can cause severe hyponatremia); and (3) a final period of diabetes insipidus. The extent of the injury determines the completeness of the diabetes insipidus and, as already discussed, the site of the lesion determines whether the disease will be permanent. Twenty-five percent of patients studied after transsphenoidal surgery developed spontaneous isolated hyponatremia, 20% developed diabetes insipidus, and 46% remained normonatremic. Normonatremia, hyponatremia, and diabetes insipidus were associated with increasing degrees of surgical manipulation of the posterior lobe and pituitary stalk during surgery [145]. Central diabetes insipidus is observed both before but mainly after surgery for craniopharyngiomas [147]. The etiologies of central diabetes insipidus in adults and children are listed in Table 8. A solid symbol indicates a codon with a missense or nonsense mutation; a number indicates more than one mutation in the same codon; other types of mutations are not indicated in the figure. There are 95 missense, 18 nonsense, 46 frameshift deletion or insertion, seven inframe deletion or insertion, four splice-site and 22 large deletion mutations, and one complex mutation. These actions of vasopressin in the distal nephron are possibly modulated by prostaglandin E2, nitric oxide [141], and by luminal calcium concentration. However, mice lacking E-prostanoid-3 receptors for prostaglandin E2 were found to have quasi-normal regulation of urine volume and osmolality in response to physiological stimuli [142]. This possible link between calcium and water metabolism may play a role in the pathogenesis of renal stone formation [143]. This definition excludes osmotic diuresis, which occurs when excess solute is being excreted, as with glucose in the polyuria of diabetes mellitus. Other agents that produce osmotic diuresis are mannitol, urea, glycerol, contrast media, and loop I. Expression of the vasopressin gene in autosomal dominant and autosomal recessive diabetes insipidus in humans is described above. An unusual incidence of psychiatric symptoms has also been described in patients with this syndrome.
Cheap sustiva 200mg visa
From the yolk sac facial treatment purchase sustiva cheap, the hematopoietic stem cells migrate to the liver and then to the bone marrow and, to some extent, to the spleen, lymph nodes, and thymus. Extramedullary hematopoiesis in the liver and the spleen subsides after birth, and the bone marrow remains the primary blood-forming organ. As the organism matures, the red bone marrow of the long bones is replaced by fat. The thymus and lymph nodes remain sites of lymphocytopoiesis in infancy and adolescence, but the thymus usually involutes after puberty. Lymph nodes form lymphocytes, but in adults these organs do not produce red blood cells or granulocytic leukocytes. However, if the hematopoietic bone marrow is destroyed, extramedullary hematopoiesis may resume in the spleen, liver, and lymph nodes. The mature blood cells are descendants of developmentally pluripotent hematopoietic stem cells. The term pluripotent means that these cells can differentiate and develop into more than one mature cell type. The mother stem cell differentiates into several developmentally committed stem cells, which are the precursors of distinct cell lineages, the ultimate product of which are the mature blood cells. The lymphoid stem cell gives rise to B-cells, which finally mature into immunoglobulin-secreting plasma cells, and T-cells, most of which assume their function in mediating cell-mediated immune reactions after they have passed through the thymus (T-thymus! The myeloid stem cell, also known as the trilineage-myeloid stem cell, gives rise to three subsets of stem cells, which are the precursors of mature erythrocytes, megakaryocytes, and nonlymphoid white blood cells such as neutrophils, monocytes, eosinophils, and basophils. The stem cells of various cell lineages are small, undifferentiated cells that are indistinguishable from one another; however, they differ with regard to their development potential. Many other growth factors, such as interleukins produced by macrophages and T-lymphocytes, also stimulate blood cell formation. Only the growth factor for the erythroid cell lineages-erythropoietin-is produced outside of the bone marrow (in the kidney). Taller men have more blood than shorter men, and females typically have less blood than males. Blood cells can be separated from the plasma by allowing the formed elements to form sediment over a period of several hours at the bottom of a tube coated with anticoagulant. This can be achieved much faster by centrifuging the blood at high speed for 2 to 3 minutes. The volume of packed red blood cells, expressed as a percentage of the total peripheral blood, is called the hematocrit. In healthy adults, formed blood cell elements constitute 40% to 45% of the total blood volume, whereas the plasma accounts for 55% to 60%. Isolation of the genes for erythropoietin and other hematopoietic growth factors made it possible to produce them commercially using recombinant gene methodology. Anemic patients who do not have endogenous erythropoietin, because their kidneys have been destroyed by disease, can be treated successfully with recombinant erythropoietin. Most of this second phase consists of red blood cells, except for the top layer, called the buffy coat, which contains leukocytes and platelets. The coagulation proteins are consumed in this process, which leads to transformation of plasma into serum. It contains all the proteins except fibrinogen, prothrombin, and other coagulation factors. Some blood tests can be performed only on plasma, whereas others can be performed on serum. By contrast, blood collected in "red top" tubes, which do not contain anticoagulants, will coagulate and on centrifugation will yield serum. In general, clinical laboratories specify the requirements for each test, and one must check the hospital manual before drawing blood for a specific test. Overview of Major Diseases Hematologic diseases occur as a result of abnormal formation, increased destruction, or abnormal structure and function of blood cells. Erythrocytes are ideally suited for their primary function: transport of oxygen from the lungs to the peripheral tissues. The red color is derived from hemoglobin, an iron-containing pigment that constitutes 90% of the dry weight of each normal, mature erythrocyte. In peripheral blood smears, the thinner central portion, spanning half the cell diameter, appears paler than the peripheral part. The erythrocytes are round but can easily be deformed while passing through small capillaries and other small vessels. Erythrocytes do not have nuclei or organelles that would interfere with their transport function. Because of their biconcave shape, they have a large surface that allows easy diffusion of gases. Hemoglobin is a complex molecule that consists of four heme groups and four globins. Heme is composed of four pyrrole rings held together with a centrally placed iron in ferrous form (Fe2+). The globin part of hemoglobin consists of four polypeptide chains designated by the Greek letters alpha, beta, gamma, and delta. Mutations of these genes cause hemoglobinopathies and are marked by abnormal hemoglobins; for example, sickle cell anemia is characterized by an abnormal B chain, and the hemoglobin is known as hemoglobin S (HbS). Deficiency or malabsorption of these nutrients also results in anemia; anemia may develop because the nutrient is not available in food, because it cannot be absorbed, or because the loss exceeds the intake. The aging cells are sequestered in the spleen, which removes the old and defective red blood cells from circulation and serves as their primary "graveyard. The remainder is excreted in the form of urobilinogen and stercobilinogen in urine and feces. Normal synthesis of hemoglobin occurs only in the presence of nutrients, iron, vitaminB12,andfolicacid. Objective measurements of red blood cell parameters are done with instruments that estimate the mean size of red blood cells and their hemoglobin content. Analysis of blood has become highly automated and is performed with sophisticated instruments. Low values (<80 fL) indicate microcytic anemia, whereas high values (>100 fL) indicate macrocytic anemia. Neutrophils are the most abundant white blood cells in the blood, accounting for 60% to 70% of all nucleated cells. The main function of neutrophils is to defend the body against bacterial infections. Neutrophils are most qualified for this job, because they have remarkable mobility. Eosinophils account for 1% to 3%, and basophils for less than 1%, of all white blood cells in the blood. The release of these substances causes blood vessels to dilate and increases their permeability. Neutrophils are short-lived cells that survive no more than 4 days in the peripheral circulation. Therefore, these cells must be replaced constantly, and the bone marrow produces new neutrophils at a very fast pace. Because the life span of neutrophils is about 300 times shorter than the life span of erythrocytes, the bone marrow contains three times more white blood cell precursors than erythroid precursors. The abundant cytoplasm of megakaryocytes forms buds, which are released into the circulation as platelets. Platelets do not have nuclei; however, they survive 8 to 10 days in the circulation. Malignant transformation of hematopoietic cells may result in solid tumors or leukemia. Lymphomas, resulting from malignant transformation of lymphoid cells, occur most often in lymph nodes. These malignant cells may remain localized to their site of origin, extend into the adjacent tissues, or enter the circulation.
Buy sustiva overnight
Precocious puberty may be associated not only with hypothalamic hamartomas [29] but also with other benign or malignant neoplasms such as craniopharyngiomas medication 3 checks buy sustiva 200 mg with amex, gliomas, and astrocytomas or with infiltrative and inflammatory lesions. In both sexes, accelerated growth velocity is observed initially with tall stature for age. This, however, is associated with increased velocity of bone maturation and premature growth cessation and final short stature, the severity of which is generally dependent on the age of onset of the disorder. The most important physiologic stimuli are suckling, stress, and increased levels of ovarian steroids, primarily estrogens [36]. The general view is that lactotrophs exhibit spontaneously high secretory activity. These actions constitute the physiological basis for the therapeutic effect of dopamine agonists in hyperprolactinemia [37]. Women present with the classic amenorrhea-galactorrhea syndrome, whereas men may ignore symptoms of erectile dysfunction, decreased libido, and gynecomastia caused by hyperprolactinemia. Menstrual abnormalities, libido, and erectile disorders are difficult to assess because of the high frequency of concomitant gonadotrophin deficiency. Kallmann syndrome is the most common form of congenital isolated gonadotrophin deficiency and can occur sporadically or in a familial setting as an Xlinked, autosomal-dominant, or autosomal recessive trait with incomplete penetrance and variable phenotypic expression [39]. In boys, who are more often affected than girls, cryptorchidism and microphallus may be observed at birth (lack of fetal gonadotrophins which do not stimulate testosterone secretion from the fetal testes). However, clinical diagnosis does not occur until the time of expected puberty when there is a failure of gonadotrophins to increase testicular size, and development of secondary sexual characteristics. In girls, primary amenorrhea is observed together with absent mammary gland development. Other components of this syndrome include color blindness, nerve deafness, cleft palate, exostosis, and renal abnormalities [39]. Men experience gradual loss of body and pubic hair, decreased muscular development, testicular atrophy, decreased libido, and erectile dysfunction. With longstanding hypogonadism, both sexes may develop fine wrinkling around the corners of the eyes and lips and osteopenia. Approximately one-third of these patients develop hormone abnormalities due to a traumatic transection of the pituitary stalk during delivery, while others have defective induction of mediobasal brain structures, which results in failure of pituitary lobes to fuse, and an absence or hypoplasia of the pituitary stalk [47,51]. Both autosomal recessive and X-linked recessive transmission have been described, although most cases appear to be sporadic [1]. Most of these patients exhibit a rise in anterior pituitary hormones following bolus injections of the releasing hormones, but not in response to provocative stimuli that work through the release of endogenous hypothalamic releasing hormones. In fact, relevant decreases in growth velocity or arrested growth can be observed (short stature is not a frequent finding due to the relatively acute onset of signs and symptoms) [47]. Growth retardation generally becomes apparent during the latter part of the first year, and both height age and bone age are delayed. Untreated patients develop proportional short stature, increased subcutaneous fat, "pinched facies" with a high forehead, and fine wrinkling of the skin around the corners of the mouth and eyes. Clinical manifestations of hypothalamic hypothyroidism are similar, but less severe than those found with primary hypothyroidism [1,9]. Acute adrenocortical insufficiency rarely occurs spontaneously, but may be precipitated with stresses such as surgery, infections, or trauma. Unlike patients with primary adrenocortical insufficiency, hyperpigmentation and electrolyte abnormalities that reflect aldosterone deficiency (hyponatremia and hyperkalemia) are not seen [1,9]. If the osmoreceptor mechanism is intact and the patient is conscious and has access to fluids, plasma osmolarity may be maintained within the normal range. However, if the thirst center osmoreceptors are damaged, or if the patient is unable to ingest adequate quantities of water, hypernatremic dehydration may occur and result in rapid deterioration of the sensorium from lethargy to stupor to coma. However, in both conditions, administration of exogenous vasopressin to a dehydrated patient will result in a further increase in urine osmolarity, while dehydrated normal individuals will show little or no further increase in urine osmolarity after a standard dehydration test. The medication is administered sublingually or by oral tablets, by nasal inhalation, or rarely by intramuscular injection [61]. Affected individuals have impaired thirst mechanism, demonstrating hypodipsia or adipsia despite marked serum sodium elevations. Nevertheless, these patients have normal extracellular fluid volume and are not dehydrated, and, therefore, maintain normal blood pressure, pulse rate, blood-urea nitrogen, serum creatinine, and creatinine clearance. Clinically, few symptoms reflecting hypernatremia are found with serum sodium concentrations below 160 mmol/L. Above this level, patients develop fatigue, lethargy, weakness, muscle tenderness and cramps, anorexia, depression, and irritability. Although the pituitary gland at autopsy is normal, anterior pituitary hormone deficiencies are found, reflecting a hypothalamic etiology for the hypopituitarism. They demonstrate recurrent hypernatremia, hypodipsia, obesity, hyperprolactinemia, hypothyroidism, hyperlipidemia, lethargy, increased perspiration and, in some cases, central hypoventilation. These findings suggest an involvement of the osmoreceptors and the ventral medial nucleus [63]. Damage to the osmoreceptors in the anterior medial and anterior lateral preoptic this condition is characterized by serum hypoosmolarity (Posm,275 mOsm/kg) and hyponatremia, an inappropriately concentrated urine (Uosm. It has also been noted in some patients with hydrocephalus, craniopharyngiomas, germinomas, pinealomas, central pontine myelinolysis, and acute intermittent porphyria [64]. An idiopathic, cyclic form of the syndrome has been described in young women with menstrual irregularities and enlarged lateral ventricles [1]. Besides symptoms from the underlying disease, these patients demonstrate clinical findings of water intoxication. In fact, clinical features depend on the rate of decrease of serum sodium, as well as absolute serum sodium concentration. At serum sodium levels,120 mmol/L patients become symptomatic with anorexia, headache, weakness, lethargy, nausea, vomiting, and mental confusion; at very low levels, with seizure and coma [65]. Abnormal brain natriuretic peptide secretion is also implicated in this syndrome [65,66]. Most patients with hypothalamic obesity have large lesions or extensive involvement of multiple areas of the hypothalamus. Bilateral destruction of the ventromedial nucleus results in obesity in humans, as it does in experimental studies in animals [6]. In patients with documented structural involvement, about 90% harbor a neoplasm, most often craniopharyngioma (approximately 60%) [67]. Approximately 6% are the result of inflammatory or granulomatous processes including sarcoidosis, tuberculosis, arachnoiditis, and encephalitis, 5% are posttraumatic, and 2% are due to leukemic infiltration [1]. Defective hypothalamic leptin signal transduction may play a role in hypothalamic obesity. In fact, when circulating leptin derived from adipocyte energy storage transduces hypothalamic signals, anorexigenesis is achieved, which increases sympathetic tone, with resultant increases in energy expenditure and decreased vagal tone, appetite, and energy storage. Conversely, defective leptin signaling, or "leptin resistance," leads to orexigenesis, with decreased sympathetic tone and increased vagal tone, and with resultant increased appetite and energy storage [3]. Leptin signaling may be disrupted by exceptionally rare leptin deficiency with obesity documented as early as 6 months of age and extremely low or not measurable serum leptin levels, which is reversible after treatment with recombinant leptin [68]. In many instances, the abnormality appears to reflect resetting of the satiety set-point, especially observed in patients with obesity that develops following head trauma. Most affected individuals gain weight for approximately 6 months following trauma, followed by a period of stabilization as energy expenditure equals the caloric content of ingested food, with a subsequent gradual decrease in food intake and a loss of weight. Similarly, patients with tumor destruction of ventromedial nuclei may develop hyperphagia and rapid weight gain, followed by a plateau and then further weight gain as the neoplasm grows [1].
Syndromes
- Rapid pulse
- Committing crimes to get money to gamble
- Name of the product (ingredients and strengths, if known)
- Hydromorphone
- Bluish skin (fingernails and lips)
- Fluphenazine (Prolixin)
- These wires will be connected to a small current generator outside of your body that you carry like a cell phone.
- You take blood thinning medication, like warfarin.
- Persistent vomiting
Order sustiva with amex
Blood from the cavernous sinuses drains into the superior and inferior petrosal sinuses xerogenic medications order sustiva american express, the emissary veins, and the pterygoid plexus. Using T1-weighted magnetic resonance imaging, the posterior pituitary is visually distinguishable from the anterior lobe as a bright small area in the posterior part of the gland. The posterior pituitary is the distal component of the hypothalamo-neurohypophyseal tract, which also includes the infundibular stalk, the hypothalamic median eminence, and the tuber cinereum, a part of the base of the hypothalamus. The posterior pituitary comprises a collection of axon terminals originating from the magnocellular secretory neuron bodies located in the hypothalamic paraventricular and supraoptic nuclei. These axons traverse the infundibular stalk, terminating at the posterior pituitary, and secrete vasopressin and oxytocin into the systemic circulation. The anterior lobe of the pituitary can be divided into the pars distalis (pars glandularis), which constitutes B80% of the gland, the pars intermedia, and the pars tuberalis, which engulfs the posterior pituitary stalk. The pars intermedia is rudimentary in the human, although in other species it is more developed. Gonadotroph cells are scattered throughout the anterior pituitary and constitute B10% of cells. These cells are primarily located in the lateral wings of the anterior lobe, but can also be scattered in the median wedge [26]. They mostly cluster in the central mucoid wedge in the center of the gland, but are also scattered in the lateral wings, and are the predominant cell type in the poorly developed human intermediate lobe. Thyrotrophs are the least abundant cell type in the anterior pituitary, comprising approximately 5% of the total cell population, and are mostly found in the anteromedial portion of the gland [26], but are also found in the pars tuberalis [28]. Supporting and/or non-neuroendocrine cells are scattered throughout the anterior pituitary, including follicular cells surrounding follicles [26,29], agranular folliculostellate cells with long-branched cytoplasmic processes [30,31], incompletely differentiated null cells that do not secrete specific hormones [32], and mitochondria-rich oncocytes [26]. The second control level involves the release of pituitary hormones to the circulation, reaching target glands and organs. The third control level constitutes the distal target organs secreting hormones that elicit the required effect on peripheral tissues. Local factors including cytokines, growth factors, nutrients, neuropeptides, and neurotransmitters, add further paracrine/autocrine complexity and can alter the delicate hormonal balance along each respective axis. The first tier comprises hypothalamic releasing and inhibiting hormones impinging directly upon the pituitary. The second tier involves secretion/inhibition of paracrine and autocrine intrapituitary hormone, cytokine, and growth factor signals. The third tier involves feedback regulation by hormones secreted from target glands and organs regulating pituitary or hypothalamic control. Both receptor subtypes also mediate increased calcium levels in vitro, mainly via Gs but also to a lesser degree through Gq [67], an effect that is mediated through stimulation of phospholipase-C, -, and - [67]. Females exhibit more synapses, and synapse number varies with the estrous cycle [113]. These clinical conditions result in somatotroph hyperplasia and, sometimes, adenomatous transformation [118]. Somatostatin 28, a 28-amino-acid somatostatin peptide that is a longer form of somatostatin 14, was discovered immediately thereafter [82]. The human somatostatin gene is located on the long arm of chromosome 3 and comprises two exons and one intron. The two exons encode preprosomatostatin, and exon 2 encodes somatostatin 14 and somatostatin 28. Somatostatins are cyclic peptides with a single covalent bond between 2 Cys residues and a bioactive core composed of a PheTrp-Lys-Thr amino acid sequence. Somatostatin 14 is predominant in the brain, while somatostatin 28 predominates in the gastrointestinal tract [82]. Moreover, in some tissues, somatostatin 14 exhibits both stimulatory and inhibitory acute actions [136]. Somatostatin 14 is identical in all vertebrates and exhibits a high degree of homology to somatostatin 14 in invertebrates and protozoa [82]. Somatostatin 14 is the main form in the brain including the hypothalamus, while cortistatin is mostly expressed in the hippocampus and cortex [82]. Hypothalamic somatostatin is produced predominantly in the anterior periventricular nucleus, and is also produced in the paraventricular, arcuate, and ventromedial nuclei. Some neuronal axons course through the neural pituitary stalk and terminate directly in the posterior pituitary [137]. The primary function of somatostatin is to inhibit pituitary hormone secretion, accomplished by inhibition of hypothalamic peptides responsible for pituitary hormone synthesis and secretion and by direct effects on pituitary cells. Somatostatin also inhibits its own secretion from the periventricular nucleus [82]. Receptor activation also initiates opening of potassium channels and closure of calcium channels. Glucocorticoids have a dual effect on somatostatin release from the hypothalamus: at low doses, glucocorticoids induce somatostatin, but high doses inhibit somatostatin expression [82]. In contrast, somatostatin receptor expression is downregulated by ghrelin and chronic glucocorticoid exposure. These two hormones, in turn, stimulate gonads to produce and release estradiol and testosterone and regulate germ cell function. Neurokinin B and dynorphin are coexpressed in most kisspeptin neurons in the human hypothalamic infundibular nucleus, which corresponds to the rodent arcuate nucleus. Studies in rats demonstrated that hypothalamic dopamine is released from neurons located in the arcuate and anterior periventricular nuclei. The anterior pituitary also receives inhibitory dopaminergic input from the posterior and intermediate pituitary through interconnecting short portal veins [180]. Dopamine is a member of the catecholamine neurotransmitter group that shares a common synthetic pathway. In dopaminergic neurons, further metabolism of dopamine does not occur, but in noradrenergic neurons, dopamine is subsequently hydroxylated to norepinephrine by dopamine hydroxylase, and then to epinephrine by phenylethanolamine N-methyl transferase. Dopamine binds dopamine receptor subtype 2 (D2R) on pituitary lactotrophs, inhibiting both prolactin synthesis and release and lactotroph proliferation. D2R null mice develop lactotroph hyperplasia, hyperprolactinemia, and lactotroph adenomas, indicating that, at least in mice, D2R is the predominant dopamine receptor mediating the dopamine effect on prolactin [183]. Lactotroph prolactin secretion increases as dopamine levels reaching the pituitary are decreased. In contrast, low-dose oxytocin injections reduce basal and stress-induced prolactin secretion in male rats, and blocking vasopressin activity with antiserum attenuates the suckling-induced rise of plasma prolactin in females [179]. Prolactin receptors are expressed on all dopaminergic neurons that supply the pituitary, enabling a short negative feedback loop of prolactin on dopamine synthesis. Increasing prolactin levels increases tyrosine hydroxylase expression, which, in turn, increases dopamine expression and leads to decreased prolactin levels [191,192].
Sustiva 600 mg low price
Although fulminant hepatitis is very uncommon (<1% of infections) treatment junctional tachycardia quality 600mg sustiva, it is seen almost exclusively in patients greater than 50 years of age. The viral titers are highest in the stool during this time and can reach 108 virions/mL, this titer usually peaking at 2 weeks before symptoms, with this time being the highest period of infectivity. The short duration of viremia and absence of a carrier state are reasons why transfusion-transmitted disease is rare. An estimated 400 million persons have chronic infection with almost half a million people dying annually from complications of advanced liver disease including hepatocellular carcinoma. In the low-risk areas the main mode of transmission is percutaneous (via intravenous drug use) and sexual exposure, while in the high endemic areas perinatal transmission and person-to-person contact are the more common routes. The risk of developing chronic hepatitis B from perinatal transmission is approximately 90%, with these infants usually asymptomatic. The highest prevalence is in Africa, the eastern Mediterranean region, and in the western Pacific (3. The mode of spread is by percutaneous, sexual, and perinatal routes, with the prevalence in intravenous drug users who share needles approximately 70% after 1 year and rising to >90% after many years. Sexual transmission can occur but is rare, is usually associated with other co-factors, and is estimated at 1. The risk of transfusion-acquired hepatitis C with current hepatitis C antibody testing is extremely low (<0. Usually patients are asymptomatic with less than 20% having symptoms with jaundice. In addition, chronic infection develops in up to two-thirds of adults and about one-half of children after acute infection. The outcome for these patients is frequently an acute severe hepatitis with a high mortality, although if the patient survives, immunity for both viruses occurs, without progression to chronic disease. Parenteral transmission is the most common route, with sexual and perinatal transmission uncommon. The incubation period varies from 20 to 140 days, with viremia detectable from 2 days to 2 weeks after exposure. The portal tract exhibits a prominent inflammatory infiltrate consisting predominantly of lymphocytes. Scattered plasma cells, eosinophils, neutrophils, and histiocytes may also be seen at times but when present are few in number and scattered within the portal tracts. Rarely lymphocytes can appear attached to the endothelium of the portal and rarely terminal hepatic venules when the lymphocytic infiltrates are marked. Although periportal interface inflammatory activity (lymphocytes surrounding individual and small groups of periportal hepatocytes, a feature of active chronic viral hepatitis) may appear to be present, this is not truly the case, with lymphocytes sometimes "spilling over" into the adjacent periportal zones, but without true periportal activity targeting the hepatocytes. Interlobular bile ducts are normal in number and generally normal in appearance (hepatitis C an exception, see discussion later). Bile ductular (cholangiolar) proliferation, most often seen at the borders of the portal tracts, may also occur to variable degrees but in the usual case of acute viral hepatitis this feature is mild. These portal tract changes are usually diffuse and affect all of the portal tracts simultaneously, although some variation in the degree of portal inflammation from one portal tract to another may occur. Although many portal tracts are enlarged and expanded in acute hepatitis, this is because of the prominent portal inflammatory component and not from fibrosis. The parenchyma exhibits diffuse lobular necroinflammatory change with Kupffer cell hyperplasia, the inflammatory cells chiefly lymphocytes. Although this feature involves the entire hepatic lobule, accentuation of this necroinflammatory process may occur in the perivenular zones. Viral Hepatitis Secondary to Infection by the Hepatotropic Viruses 33 in the early acute phase there is oftentimes a predominance in the perivenular zones. Kupffer cell hyperplasia is also prominent, with many clusters of Kupffer cells seen in the areas of necrosis, and responsible for phagocytosis and clearance of the damaged hepatocytes. These Kupffer cells may be pigmented due to condensation of the lipochrome pigment, bile, or even hemosiderin (positive on iron stain) from the phagocytized hepatocytes. Bi-nucleated hepatocytes, especially those in the perivenular zone, may occur and are seen more often in the elderly population. Although true multinucleated syncytial giant cell changes of hepatocytes characteristic of acute hepatitis in the neonate can at times occur, this feature is infrequent in the adult. Cholestasis may occur and may be intracanalicular (as in this example) and intracytoplasmic within the hepatocytes. The cholestasis may extend into the midzone and even in the more severe cases can be panlobular, often with bile plugs also present within dilated bile ductules. The reticulin stain can confirm that the hepatic plates are up to two cells thick. Within a few months and almost always by 6 months the hepatic lobules return to normal. Not infrequently apoptosis (formation of Councilman bodies, acidophil bodies) can be seen scattered within the lobules. Although all of the viruses show features as described earlier in the acute phase, more specific characteristics may sometimes occur for each of the viruses. The lobular inflammation at times may be granulomatous without true epithelioid histiocytes. The proliferation of bile ductules and cholangioles may also be associated with bile plugs within these dilated ductules. Also the degree of lobular necroinflammatory change is oftentimes not prominent and is outweighed by the cholestasis, although a severe hepatitis with focal confluent necrosis has been reported. Usually the portal and lobular inflammatory infiltrates are quite mild and non-specific compared to the other viruses, with speculation as to whether a true acute hepatitis even occurs. Portal tracts may at times show an increase in plasma cells although usually the degree is not prominent. Although usually necroinflammatory changes are diffuse throughout the lobule, at times there may be some degree of periportal (zone 1) accentuation. The injured liver cells may be focally infiltrated by lymphocytes that can sometimes be seen directly within the liver cell cytoplasm ("emperipolesis"). In addition sometimes a centrally located interlobular bile duct showing mild cytologic atypia may be seen within these aggregates and is manifested by the duct epithelium somewhat swollen with irregular nuclei and lymphocytes infiltrating beneath the duct basement membrane. Bile can be seen within slightly dilated canaliculi, with the surrounding hepatocytes forming pseudo-rosettes or acinar structures. Acute Viral Hepatitis with Confluent Necrosis ("Fulminant" Hepatitis) with time considerably enlarging, coalescing, and eventually reforming a normal liver. The viable hepatocytes in the remaining zones show prominent necroinflammatory changes with apoptosis and with cholestasis frequent, although the latter feature is seldom seen in the areas of confluent necrosis. The degree of necroinflammatory change can be patchy throughout the lobule but more often involves a specific hepatic zone. The perivenular zone is usually first affected, but in the more severe cases the necrosis can extend to involve the midzones, can connect with adjacent lobules (bridging necrosis), and in the worst cases can involve all three zones (multilobular, panacinar, massive necrosis) with total loss of all hepatocytes. The bridging necrosis can be portal-to-perivenular or A severe (fulminant) hepatitis is uncommon, usually occurring with a few exceptions (see Table 2. The parenchyma shows extensive liver cell necrosis and dropout (confluent necrosis), the inflammatory cells mostly lymphocytes.

Sustiva 200 mg without prescription
In lymphomas in general medicine upset stomach purchase sustiva us, the immunoperoxidase markers directly parallel those of the nodal involvement. Primary hepatic involvement is very rare, accounting for less than 1% of all cases of extranodal involvement by lymphomas. In order to make that diagnosis there must be documentation of no nodal involvement, and there must be no evidence of leukemia as well. These lymphomas occur twice as often in men and usually present in middle-aged individuals. Prominent sinusoidal infiltrates by the monoclonal lymphocytes are seen in this T-cell lymphoma. Low-grade fever, weight loss, hepatomegaly, and fatigue may also be presenting signs. The primary lesions are usually well circumscribed and vary in size but can at times be single, quite large (up to 15 cm), or can present as multiple smaller lesions. Microscopically they are classified as nodular or diffuse, with the diffuse large B-cell type the most common, others including the lymphoblastic and Burkitt lymphomas, follicular lymphomas, diffuse histiocytic lymphomas, and T-cell lymphomas. The diagnosis is most suspected by a monomorphic clonal population of cells that considerably expand the portal tracts and can infiltrate within the sinusoids, the specific cell types identified with appropriate immunohistochemical stains. Hepatomegaly may occur as a response, with jaundice sometimes developing when the infiltrates are massive. The hepatic manifestations of acute and chronic leukemias are related to the degree of hepatic portal and lobular infiltrates. The portal tract is markedly expanded by leukemic infiltrates which can also be seen within the sinusoids. Secondary changes can also occur in the leukemias as well as the myeloproliferative disorders. Various vascular features including sinusoidal dilatation, hepatic vein thrombosis, veno-occlusive changes, peliosis hepatis, and nodular regenerative hyperplasia can occur. Extramedullary hematopoiesis within the sinusoids is common secondary to myelofibrosis, and hemosiderin deposition within the Kupffer cells and portal macrophages secondary to hemolysis and multiple blood transfusions is frequent as well. The diagnosis on liver biopsy is usually not a problem in that most often the leukemias have already been clinically affirmed; however, in some instances a markedly elevated white blood cell count can occur and initially can mimic a leukemia, examples being alcoholic hepatitis (neutrophilia) and infectious mononucleosis (lymphocytosis). Further review of the clinical history and laboratory tests, however, most often easily resolves any problem in diagnosis. Multiple myeloma, an abnormal synthesis of -globulins, may secondarily involve the liver in advanced stage disease in a minority of patients either as focal lesions or as diffuse hepatic infiltrates. Hepatomegaly can occur in these conditions, sometimes associated with ascites and portal hypertension when the hepatic involvement is striking. Sinusoidal infiltrates can also occur, and at times distinct hepatic masses can also develop. Portal and sinusoidal deposits of amyloid, confirmed by positive Congo Red stain, is not uncommon; in addition, an eosinophilic non-amyloid material within the sinusoids that represents light chains can be seen in the space of Disse in about 10% of patients. Monoclonality of the light chains as or confirms the diagnosis of multiple myeloma. A prominent infiltrate by monoclonal plasma cells and plasma cell precursors is seen. It is associated with the deposition of Langerhans cells either locally to the bone or systemically throughout many organ systems including the liver, skin, spleen, bone marrow, lungs, and lymph nodes. Langerhans cell histiocytosis is brought on by an uncontrolled clonal proliferation of these cells with sustained T-cell reaction. Although there is some debate as to whether the disorder is a reactive versus a neoplastic proliferation of these cells, the Hematopoietic Neoplasms with Hepatic Involvement 329 monoclonality of the cells and the successful treatment using chemotherapy favors a neoplastic process. The disorder is seen predominantly in the Caucasian population and there is a 2: 1 female predominance in the pediatric group of patients. The disease may also present in young to middle-aged adults with males and females equally affected, with the incidence about 1: 560,000. It occurs sporadically and is not hereditary although familial clustering has been noted. Diabetes insipidus is a complication of involvement of the pituitary gland, and solitary bone lesions may also be seen. Liver involvement occurs in systemic disease in about 15% of patients, with hepatosplenomegaly, pruritus and sometimes jaundice with marked increase in the alkaline phosphatase values occurring. The prognosis is excellent for single bone lesions but with multiple organ involvement about 60% have a chronic course with an overall mortality of about 10% of patients; however about onethird can achieve remission. In the liver the portal tracts show variably sized aggregates of Langerhans cells that have moderate eosinophilic cytoplasm and round to oval and often lobulated clear nuclei with small to inconspicuous nucleoli. Numerous eosinophils, neutrophils, plasma cells and macrophages are present surrounding these Langerhans cell clusters. Duct damage and duct loss can also occur due to these Langerhans cells infiltrating into the ducts. Metastatic Tumors Metastatic neoplasms are by far the most common cause of hepatic tumors. Jaundice was present in about 15% of cases due to either massive replacement of the liver by tumor or secondary to bile duct obstruction from tumor involvement of the hepatic hilum. Portal hypertension can also be a complication when the portal and/or hepatic veins are involved. Oftentimes the percentage of these tumors that metastasize to the liver depends on the primary location. For example, gallbladder tumors comprised only 35 total cases in the series; however, 18 of those cases (51. The same also goes with pancreatic tumors (109 total cases in the series with 63 [57. Metastatic Tumors 331 testicular tumors (only 25 total cases with hepatic metastases in 19 [76%]) was undoubtedly related to the fact that these tumors metastasize early and generate a disproportionate number of metastatic sites (average of 5. Usually the liver shows multiple scattered variably sized nodules that can focally or diffusely involve the hepatic lobes; however, in about 10% of cases only a single mass may be seen on gross inspection that can also at times be quite large, mimicking a primary tumor. Microscopically tumor cells that retain the specific morphology from the primary lesion are seen. Involvement of the portal veins, lymphatic channels, and sinusoids is common, although these features may be difficult to appreciate when massive tumor involvement is present. Compression from the tumor growth with variable degrees of atrophy of adjacent hepatocytes is frequent. Cholestasis, bile duct and ductular proliferation, and acute bile duct damage (acute cholangitis) can also occur when tumor impedes bile flow with secondary bile duct obstruction. The diagnosis rests on comparing the histology seen in liver biopsy material to that of the primary malignancy, when possible; however, at times only a history of a non-hepatic tumor is known but the original material is not available for histologic comparison with the liver lesion. Additionally a biopsy of a liver mass that appears to be a metastatic malignancy yet no extrahepatic tumor is known is an unfortunate additional complication. The moderately to poorly differentiated tumor demonstrates the production of mucin. Moderately differentiated compact glands are seen within a fibroconnective tissue stroma. Then, various additional immunohistochemical stains can be performed and be extremely useful in determining the possible primary site, examples being the synaptophysin and chromogranin stains for neuroendocrine tumors and calcitonin for medullary thyroid carcinomas. When the tumor is poorly differentiated, then various screening staining protocols can be approached to first determine whether the tumor is epithelial or non-epithelial followed by other more specific markers. An unfortunate problem also is that at times there may be de-differentiation of the tumor whereby the metastatic lesion does not resemble the original primary.
Order sustiva
These studies showed that Gata2 is important for optimal thyrotroph and gonadotroph function but not for thyrotroph and gonadotroph cell fate specification [20] medicine 751 m buy 200mg sustiva amex. Studies in zebrafish have identified a role for Sox4b in specification of thyrotroph and gonadotroph cells and induction of Gata2 [21] A population of multipotent stem cells in the adult pituitary [22,23] are distinct from the embryonic precursor cells. These nestin- and Sox2-containing stem cells reside in a localized niche within the perilumenal region of the gland, have the capacity to expand into all of the terminally differentiated pituitary cell types after birth, and may contribute to pituitary tumors [22]. These newly discovered cells may, in fact, contribute to the dynamic changes in cell growth that occur in the pituitary gland under certain physiologic or pathologic states, such as the marked thyrotroph hyperplasia/hypertrophy seen following severe hypothyroidism [24]. The gene is 4527 base pairs (bp) in size, and is located on the short arm of chromosome 1 at position 13. Most of this information has been obtained from studies performed in mouse thyrotrophic tumors and rodent pituitary glands. Thyrotroph cells are believed to contain specific transcription factors that bind to the regulatory regions of the genes and interact with ubiquitous factors to initiate transcription. The coding region is contained in the second (163 bp) and third (326 bp) exons, which are separated by a 0. In contrast to the human gene, both the mouse and the rat genes have two transcriptional start sites. While these sequences defined the minimal promoter, other studies have shown that enhancer sequences located more than 6 kb upstream are also required for the promoter to express in pituitary thyrotrophs in transgenic mice [29]. Between these two sites are 16 bp that include overlapping putative Pou1F1 and Gata2 sites. This 16 bp intervening sequence is critical for high promoter activity, independent of the actual spacing between the flanking Pou1F1 and Gata2 sites [19]. Med1 was originally defined as part of a transcriptional mediator complex that interacts with hormone-occupied thyroid/steroid hormone receptors in a ligand-dependent manner [32]. The numbers above the line denote the position of the nucleotides relative to the transcriptional start site set at 11. The boxes under the line indicate the regions important for the responses to the various factors that regulate transcription, as shown (top panel). The placental-specific, gonadotroph-specific, and thyrotroph-specific activities of the glycoprotein hormone -subunit are shown. However, Pou1F1 plus Gata2 resulted in a 10-fold activation, demonstrating synergistic cooperativity, and addition of Med1 resulted in a further dose-dependent stimulation up to 25-fold that was promoter-specific [34]. Interaction studies showed that Med1 or Gata2 each bound the homeodomain of Pou1F1, whereas Med1 interacted independently with each zinc finger of Gata2, and Med1 interacted with Gata2 and Pou1F1 over a broad region of its N-terminus. The genomic organization of the mouse (located on chromosome 4), rat, and cow -subunit genes are similar, except that in the rat and cow the second intron is located 12 bp downstream, resulting in a peptide sequence that is four amino acids longer. A single transcriptional start site has been found in the glycoprotein hormone -subunit genes of all the species that have been studied. This indicates that an enhancer region of the promoter located several thousand base pairs upstream of the transcriptional start site is required along with key cis-acting proximal promoter elements for maximal in vivo expression of the glycoprotein hormone -subunit gene in pituitary thyrotrophs and gonadotrophs. These elements interact with cell-specific and/or ubiquitous trans-acting factors to allow regulated expression in the appropriate cell type. Whereas the region downstream of 2200 is sufficient for placental expression [39], gonadotrophs require sequences between 2225 and 2200 [40], and regions further upstream appear to be critical for thyrotroph expression [41]. Some of these regions binding to similar factors also play a role in pituitary -subunit expression. Several sequences within the region from 2480 to 2300 appear to be important for mouse -subunit expression in thyrotrophs but not gonadotrophs [51]. Among these is the sequence from 2434 to 2421 that interacts with the developmental homeodomain transcription factor Msx1 [52]. In spite of significant advances in this area, thyrotroph-specific factors that determine -subunit gene expression have not yet been completely identified. These signal peptides are hydrophobic, allowing insertion through the lipid bilayer of the membrane of the rough endoplasmic reticulum. Excess free -subunit is glycosylated at an additional site, the threonine residue at position 39 [66]. Symbols represent the oligosaccharide chain residues as indicated in the key (bottom panel). In the proximal Golgi, oligosaccharide chains are modified and the final steps of sulfation and sialation occur in the distal Golgi apparatus. This mannose-rich oligosaccharide is progressively cleaved in the rough endoplasmic reticulum and Golgi apparatus. An intermediate with only six residues is produced, and then other residues are added resulting in complex oligosaccharides [67]. The residues added include N-acetylglucosamine, fucose, galactose, and N-acetylgalactosamine. Oligosaccharides prior to the six-residue intermediate are termed high-mannose and are sensitive to endoglycosidase H that releases the oligosaccharide from the protein, whereas the intermediate and the complex oligosaccharides are endoglycosidase H-resistant. Complex oligosaccharides usually consist of two branches (biantennary) but sometimes three or four branches are seen, as well as hybrid oligosaccharides consisting of one complex and another high-mannose branch. Sulfation and sialation occur late in the pathway, within the distal Golgi apparatus. Sulfate is bound to N-acetylgalactosamine residues, and sialic acid, or its precursor N-acetylneuraminic acid, is bound to galactoside residues [68]. Thus, the activation of the enzymes sulfotransferase and N-acetylgalactosamine transferase may be important regulatory steps I. For example, after an 11-minute pulse labeling with [35S]methionine and a 30-minute chase only a few -subunits were endoglycosidase H-resistant and only 76% reached this stage after an 18-hour chase [70]. It may be important to note that many of the studies described were carried out in thyrotrophic tumor tissue obtained from hypothyroid mice, and glycosylation may differ in the euthyroid as compared to the hypothyroid state. The long loops (L2) in each subunit extend from the opposite side of the central cystine knot. Novel insights into the molecular mechanisms of human thyrotropin action: structural, physiological, and therapeutic implications for the glycoprotein hormone family. Nuclear magnetic resonance studies suggested that the -subunit carbohydrate moieties project outward and may be freely mobile [76]. In this tertiary structure, the glycoprotein hormones share features in common with transforming growth factor, nerve growth factor, platelet-derived growth factor, vascular endothelial growth factor, inhibin, and activin, all of which are now grouped in the family of "cystine knot" growth factors [77]. It has been shown that proper folding is dependent on glycosylation, since the drug tunicamycin that prevents the initial oligosaccharide transfer to the asparagine residue results in peptides that do not fold properly and are degraded intracellularly [78]. Folding is a critical step that allows correct internal disulfide bonding that stabilizes the tertiary structure of the protein allowing subunit combination. Subunit combination then accelerates and modifies oligosaccharide processing of the -subunit [80]. In fact, studies have suggested that the conformation of the -subunit differs after combination with each type I. InsP3 diffuses from the cell surface membrane to the endoplasmic reticulum, where it causes the release of sequestered Ca21. This activates the movement of secretory granules to the cell surface and their exocytosis. However, additional hypothalamic factors and circulating hormones have important modifying effects. Changes in sulfation and sialylation of the oligosaccharide residues also modulate bioactivity [100,102,103]. Thus, multiple interactions between transcription factors and hormonal regulators appear to converge on sequences close to the transcriptional start site. T4 serves as a minimally active prohormone that is converted into a metabolically active T3 by a family of tissue deiodinases termed D1, D2, and D3. These selenoprotein enzymes are membrane-bound and can activate or inactivate substrate in a time- and tissue-specific manner [105]. D2 activity is rapidly lost in the presence of its substrate T4 by a ubiquitin proteasomal mechanism [106].

Order generic sustiva canada
The incidence ranges from 1/10 symptoms irritable bowel syndrome generic sustiva 600mg otc,000 to 1/15,000 live births in the United States but is higher in Southeast Asia and the Far East with a predominance in Asian females. The disorder can be subdivided into early (embryonal/fetal, about one-third of cases) and late (perinatal, about two-thirds of cases) phases, the latter associated with normal bile ducts at birth with subsequent duct injury shortly thereafter. There is also an association with viral infections (cytomegalovirus, rubella, varicella, reovirus 3, group C rotavirus). Pathophysiology inflammatory infiltrates and gradually diminishing ducts (infantile obstructive cholangiopathy, obliterative cholangiopathy) implies that biliary tract damage may also be an acquired disorder. This gene encodes a glypican-1 heparan sulfate proteoglycan responsible for regulation of the Hedgehog signaling pathway that helps proper development of embryonic cells. Similar liver pathology in animal species (zebra fish) has been identified associated with this gene mutation. Clinical Presentation and Surgical Treatment the mechanisms associated with the disease may be related in part to viral infection, but an aberrant immune-mediated process (Th1, interferon-) targeting the biliary system also is felt to play a role. Conjugated hyperbilirubinemia with marked elevations of the alkaline phosphatase activity occurs. The treatment is by correction using a Roux-en-Y anastomosis of the jejunal loop to the porta hepatis (portoenterostomy, Kasai procedure), with a good prognosis usually occurring when the duct size at the hilum is greater than 150 m in diameter. A minority of patients can live into adulthood with few Biliary Atresia 201 complications; however, biliary cirrhosis with time can occur as well as eventual intrahepatic bile duct loss, necessitating liver transplantation. Pathology the extrahepatic biliary system usually shows complete absence of the ducts in over twothirds of cases, with the remainder showing focal partial atresia or hypoplasia. The duct loss can primarily involve (1) the common bile duct with the proximal ducts patent, (2) the common hepatic duct, or (3) the main right and left hepatic ducts which is the most common and seen in about 90% of cases of biliary atresia. The ductules can also form an anastomosing network at the border of the portal tracts. A mild portal lymphocytic and sometimes neutrophilic infiltrate occurs with variable portal edema. High power of a portal tract shows prominent bile duct and ductular proliferation. A mild inflammatory infiltrate consisting of lymphocytes with some neutrophils is also present. This wedge biopsy performed at the time of a Kasai procedure shows portal fibrosis of a biliary type with focal bridging. A fibrous septa from a cirrhotic liver still shows bile duct and ductular proliferation. Cirrhosis can develop as early as 6 months in some infants if surgery is not performed. More than one subtype can occur within each duct at the same time at different foci. In addition the extrahepatic ducts as well as the large intrahepatic hilar ducts may also contain inspissated bile. The parenchyma shows cholestasis and syncytial giant cell formation of some of the hepatocytes. Increase in hepatic copper (rubeanic acid, rhodanine stains) and copper-binding protein (orcein stain) is also present within the periportal and periseptal liver cells. Importantly the numbers of interlobular bile ducts begin to decrease towards the fourth to fifth months and can progress so that by 9 months the interlobular bile ducts may be totally absent. The cause may be due to a number of factors that include recurrent duct inflammation and damage, an immune-mediated response targeted to the ducts, and a complication of biliary surgery with secondary inflammation and scarring. The extrahepatic bile ducts and the ducts at the hepatic hilum may show any of the following histologic features: Patients initially present with signs and symptoms of neonatal hepatitis, with numerous potential causes at the outset (see Table 10. Most of the conditions can be excluded with appropriate clinical data, laboratory tests including cultures and serologies, and pertinent imaging studies of the biliary tract; however, difficulties may ensue in diagnosis in the very early stages of the diseases (within a few weeks) when many of the morphologic changes in some of the disorders (such as extrahepatic biliary atresia) have not yet fully developed. Intrahepatic Biliary Atresia (Paucity of Ducts) Biliary atresia that targets the intrahepatic bile ducts and is associated with duct loss is termed paucity of ducts, can be subdivided into syndromatic and non-syndromatic types, and is responsible for about 5% of all cases of neonatal cholestasis. The mutations result in a halt in the normal development of the ducts and biliary channels. It is inherited in an autosomal dominant pattern with low penetrance and involves both sexes equally, with the incidence approximately 1: 70,000 live births. The earliest symptoms of Alagille syndrome are jaundice during the first 3 months with associated pruritus and hepatomegaly. Characteristic facial features occurring in most patients include a prominent forehead, hypertelorism, flattened nose, small chin, and wide cheek bones. Elevations in conjugated bilirubinemia and sometimes markedly elevated alkaline phosphatase activity occur, with elevations in the serum bile acids, predominantly cholic acid. Although the overall prognosis is generally favorable in most patients, one-quarter of the patients have progression of the liver disease requiring liver transplantation. The non-syndromatic type is uncommon and includes a variety of associated disorders such as metabolic diseases, perinatal infections, chromosomal anomalies, abnormalities in bile metabolism and transport, and a large miscellaneous group (see the list of various causes of interlobular bile duct loss in Table 4. The outcome often parallels the underlying disease, although the prognosis is not as favorable as in Alagille syndrome. Biliary cirrhosis occurs in from half to three-quarters of cases within the first decade of life and often necessitates liver transplantation for survival. Pathology the most characteristic feature in paucity of ducts syndrome, both syndromatic and non-syndromatic, is a decrease and eventual loss of interlobular bile ducts (absent to less than 0. Although a mild portal lymphocytic infiltrate may be seen, sometimes the portal tracts are devoid of an inflammatory infiltrate. Small hepatic arterioles are present; however, no interlobular bile ducts are seen. The parenchyma exhibits cholestasis with only mild lobular inflammation and variable syncytial giant cell transformation of hepatocytes in the perivenular zones. In non-syndromatic disease, diffuse interstitial fibrosis may also be seen within the lobules, with portal fibrosis progressing to a biliary cirrhosis more commonly occurring than in the syndromatic cases. In addition an increase in hepatic copper (rubeanic acid, rhodanine stains) and copper-binding protein (orcein stain) is also present within the periportal and periseptal hepatocytes. Differential Diagnoses presentations, pertinent imaging and laboratory data, and histology point towards the correct diagnosis in most instances. Developmental and Congenital Cystic Diseases of the Intra- and Extrahepatic Biliary System Developmental and acquired disorders of cystic dilatation of the hepatobiliary system can occur anywhere in the biliary tract. The most common, the choledochal cyst, involves only the extrahepatic bile ducts; however, intrahepatic ducts alone or both intra- and extrahepatic duct abnormalities can also occur in various disorders. These types of biliary cysts are uncommon with the highest incidence in Japan (1: 13,000 live births versus 1: 150,000 in the Western countries and 1: 2,000,000 in England). Between 40 and 60% are diagnosed before age 10 years and up to 90% before 30 years. An example of the type V classification As in extrahepatic biliary atresia, the differential diagnoses rest on the various causes of neonatal cholestasis and bile duct loss (Table 10. The pathogenesis suggests that these cystic diseases are both congenital and acquired. A feature that favors congenital malformations is that the diagnosis has been reported as early as fifteen weeks gestation, although it can present at an older age. Associated anomalies of the biliary tree such as double common bile duct and double and multi-septate gallbladders, biliary atresia, congenital hepatic fibrosis, and an annular pancreas can be associated. Failure of canalization of the fetal biliary tract resulting in obstruction and eventual duct dilatation is a possible etiology as well. A feature that favors acquired malformations is that the cysts are said to develop from an anomalous arrangement of the distal pancreaticobiliary tree. In choledochal cysts, the common bile duct merges with the pancreatic duct from a longer distance (high insertion) than normal from the ampulla (>2 cm) and at a right angle, affecting the normal sphincter function at the pancreaticobiliary junction. Because the secretory pressure of the pancreas is higher than that of the liver, there is reflux of the pancreatic fluid into the bile duct system in the absence of a sphincter mechanism, resulting in duct damage with recurrent cholangitis, fibrosis with bile duct obstruction, and possibly the development of neoplasms.
