
Buy cheap plavix 75 mg line
Compared to older methods of resistance testing arrhythmia surgery cheap plavix 75mg with mastercard, such identification can yield clinically important information much quicker. Even more promising is the development of genetic markers for resistance in Mycobacterium tuberculosis, where resistance testing with classical methods may take weeks. Summary Subtyping of pathogens is an important tool for public health which has been improved and refined for over a century. Many times subtyping may be of limited clinical value, but the determination of antimicrobial resistance is a good counterexample. Genomic surveillance elucidates Ebola virus origin and transmission during the 2014 outbreak. There are a large number of books on medical statistics, and it is difficult to mention one before the others. Two that I like are Practical Statistics for Medical Research by Douglas Altman, Chapman & Hall, 1991, and Essential Medical Statistics, 2nd edition, by Betty Kirkwood and Jonathan Sterne, Blackwell, 2003. A very good complement to the book you have just read is Infectious Disease Epidemiology: Theory and Practice, 3rd edition, edited by Kenrad Nelson and Carolyn Williams. This book goes much further into the epidemiology of a long list of specific diseases than I have done and is also clearly more public health oriented. Most of the chapter authors come from Johns Hopkins University, where there has been a long tradition in infectious disease epidemiology, and this book can be regarded as something of a standard work in the field, published by Jones & Bartlett Learning, 2014. The best book on the history of infectious diseases, and the one which got me into this field is Plagues and Peoples by William McNeill, Anchor Press, 1998. If you want to learn everything there is to know about field epidemiology, you should read Field Epidemiology, 3rd edition, edited by Michael Gregg, Oxford University Press, 2008. A book which is now getting a bit old, but which you may want to have a look at if you have a special interest in zoonoses (and if you can find it), is Veterinary Epidemiology by Michael Thrusfield, Butterworth-Heinemann, 1991, which is well written and readable. In general, hyposecretion is treated with drug therapy in the form of hormone replacement. Most hormone deficiencies result from genetic defects in the glands, surgical removal of the glands, or production of poor-quality hormones. For diagnosis, treatment, and management of endocrine disorders, the medical services of a specialist may be warranted. Endocrinology is the branch of medicine concerned with endocrine glands and hormones. The physician who specializes in the diagnosis and treatment of endocrine disorders is known as an endocrinologist. Thyroid Disorders Thyroid gland disorders are common and may occur at any time during life. They may be the result of a developmental problem, injury, disease, or dietary deficiency. Deficiency of thyroid hormone (hypothyroidism) that develops in infants is called cretinism. If not treated, this disorder leads to mental retardation, impaired growth, low body temperatures, and abnormal bone formation. The signs and symptoms of this disease include edema, low blood levels of T3 and T4, weight gain, cold intolerance, fatigue, depression, muscle or joint pain, and sluggishness. Hyperthyroidism is a condition in which the thyroid gland produces excessive amounts of thyroid hormone. The most common form is Graves disease, also known as thyrotoxicosis/autoimmune hyperthyroidism, an autoimmune disorder in which the immune system produces autoantibodies that stimulate the production of excessive thyroid hormone. Another cause of hyperthyroidism is the formation of nodules or lumps on the thyroid gland (toxic nodular or multinodular hyperthyroidism), causing the excess production of thyroid hormone. Signs and symptoms of hyperthyroidism include an elevated metabolic rate, abnormal weight loss, excessive perspiration, muscle weakness, and emotional instability. Also, the eyes are likely to protrude (exophthalmos) because of edematous swelling in the tissues behind them. Disease Focus 489 Treatment for hyperthyroidism may involve drug therapy to block the production of thyroid hormones or surgical removal of all or part of the thyroid gland. Another method for treating this disorder is to administer a sufficient amount of radioactive iodine to destroy the thyroid secretory cells. Parathyroid Disorders As with the thyroid gland, dysfunction of the parathyroids is usually characterized by inadequate or excessive hormone secretion. This condition can result from an injury or from surgical removal of the glands, sometimes in conjunction with thyroid surgery. The primary effect of hypoparathyroidism is a decreased blood calcium level (hypocalcemia). When this condition is the result of a benign glandular tumor (adenoma) of the parathyroid, the tumor is removed. Adrenal Gland Disorders the adrenal cortex and adrenal medulla have their own structures and functions and their own sets of associated disorders. Adrenal Cortex the adrenal cortex is mainly associated with Addison disease and Cushing syndrome. Addison Disease Addison disease, also called corticoadrenal insufficiency, is a relatively uncommon chronic disorder caused by a deficiency of cortical hormones. Other clinical manifestations include muscle weakness, anorexia, gastrointestinal symptoms, fatigue, hypoglycemia, hypotension, low blood sodium (hyponatremia), and high serum potassium (hyperkalemia). If treatment for this condition begins early (usually with adrenocortical hormone therapy), the prognosis is excellent. If untreated, the disease will continue a chronic course with progressive but relatively slow deterioration. Regardless of the cause, Cushing syndrome alters carbohydrate and protein metabolism and electrolyte balance. Overproduction of mineralocorticoids and glucocorticoids causes blood glucose concentration to remain high, depleting tissue protein. In addition, sodium retention causes increased fluid in tissues, leading to edema. Other symptoms include fatigue, high blood pressure, and excessive hair growth in unusual places (hirsutism), especially in women. The treatment goal for this disease is to restore serum cortisol to normal levels. Nevertheless, treatment varies with the cause and may necessitate radiation, drug therapy, surgery, or a combination of these methods. Adrenal Medulla No specific diseases can be traced directly to a deficiency of hormones from the adrenal medulla. The most common disorder is a neoplasm known as pheochromocytoma, which produces excessive amounts of epinephrine and norepinephrine. These hypersecretions produce high blood pressure, rapid heart rate, stress, fear, palpitations, headaches, visual blurring, muscle spasms, and sweating. When body cells are deprived of glucose, their principal energy fuel, they begin to metabolize proteins and fats. Fat metabolism produces ketones, which enter the blood, causing a condition called ketosis. Hyperglycemia and ketosis are responsible for the host of troubling and, commonly, life-threatening symptoms of diabetes mellitus. Disease Focus 491 Although genetics and environmental factors, such as obesity and lack of exercise, seem significant in the development of this disease, the cause of diabetes is not always clear. Blood glucose levels are monitored by the patient several times a day using a glucometer to determine the amount of insulin needed to control blood sugar levels. Insulin injections should be administered in a different subcutaneous site each time to avoid injury to the tissues. Type 2 diabetes is the most common form and is distinctively different from type 1. Its onset is typically later in life; however, it has become more prevalent in children as the incidence of obesity has increased.
Discount plavix 75mg with mastercard
Additional external myelin sheath that is formed by Schwann cells and found only on axons in the peripheral nervous system Because the neurilemma does not disintegrate after injury to the axon blood pressure when to worry purchase 75 mg plavix free shipping, its enclosed hollow tube provides an avenue for regeneration of injured axons. Organ chamber or cavity that receives or holds fluid In the nervous system, cerebrospinal fluid flows through the ventricles of the brain into the spinal cavity and then returns to the brain, where it is absorbed into the blood. Depending on the direction in which they transmit information, neurons and nerves are classified as afferent (when the impulse moves toward the brain or spinal cord) or efferent (when the impulse moves away from the brain or spinal cord). Its branching cytoplasmic projections are (3) dendrites that carry impulses to the cell body and (4) axons that carry impulses from the cell body. Dendrites resemble tiny branches on a tree, providing additional surface area for receiving impulses from other neurons. Axons are threadlike extensions of nerve cells that transmit impulses to dendrites of other neurons and to muscles and glands. This covering acts as an electrical insulator that reduces the possibility of an impulse stimulating adjacent nerves. On nerves in the peripheral nervous system, the myelin sheath is formed by a neuroglial cell called a (6) Schwann cell that wraps tightly around the axon. If the neurilemma covering remains intact after an injury to the nerve, it forms a tube that provides a pathway for possible neuron regeneration after injury. Oligodendrocytes, rather than Schwann cells, form the myelin sheath that covers the axons in the central nervous system. Oligodendrocytes do not produce neurilemma, and thus injury or damage to neurons located in the central nervous system is irreparable. The short, unmyelinated spaces between adjacent segments of the myelin sheath are called (8) nodes of Ranvier. The functional connection between two neurons or between a neuron and its effector organ (muscle or gland) is a gap or space called a (9) synapse. Impulses must travel from the (10) axon terminal of one neuron to the dendrite of the next neuron or to its effector organ by crossing this synapse. The impulse within the transmitting axon causes a chemical substance called a (11) neurotransmitter to be released at the end of its axon. The neurotransmitter diffuses across the synapse and attaches to the receiving neuron at specialized receptor sites. When sufficient receptor sites are occupied, it signals an acceptance "message" and the impulse passes to the receiving neuron. The receiving neuron immediately inactivates the neurotransmitter and prepares the site to receive another impulse. Neuroglia Neuroglia are cells that support neurons and bind them to other neurons or other tissues of the body. Although they do not transmit impulses, they provide a variety of activities essential to the proper functioning of neurons. The term neuroglia literally means "nerve glue" because these cells were originally believed to serve only to bind neurons to each other and to other structures. They are now known to supply nutrients and oxygen to neurons and assist in other metabolic activities. They also play an important role when the nervous system suffers injury or infection. The four major types of neuroglia are astrocytes, oligodendrocytes, microglia, and ependyma. They provide three-dimensional mechanical support for neurons and form tight sheaths around the capillaries of the brain. Even so, small molecules, such as water, carbon dioxide, oxygen, and alcohol, readily pass from blood vessels through the barrier and enter the interstitial spaces of the brain. Oligodendrocytes, also called oligodendroglia, are responsible for developing myelin on the axons of neurons in the central nervous system. Microglia, the smallest of the neuroglia, possess phagocytic properties and become very active during times of infection. Ependyma are ciliated cells that line the fluid-filled cavities of the central nervous system, especially the ventricles of the brain. Nervous System Divisions the two major divisions of the nervous system are the central nervous system and the peripheral nervous system. The central nervous system consists of all nervous tissue located in the brain and spinal cord. The peripheral nervous system includes all nervous tissue located outside the central nervous system and consists of cranial and spinal nerves. Table 15-1 N e rvo us S ys t em Str u ctu r es an d Fu n ction s this table lists the structures of the nervous system, along with their functions. Unmyelinated fibers, dendrites, and nerve cell bodies make up the gray matter of the brain and spinal cord. Anatomy and Physiology 519 Cerebrum the (1) cerebrum is the largest, uppermost portion of the brain. A structure called the (2) corpus callosum joins these hemispheres, permitting communication between the right and left sides of the brain. Four of these lobes are named for the bones that lie directly above them: (3) frontal, (4) parietal, (5) temporal, and (6) occipital. A thin layer called the cerebral cortex covers the entire cerebrum and is composed of gray matter. The remainder of the cerebrum is primarily composed of white matter (myelinated axons). Major functions of the cerebrum include sensory perception and interpretation, language, voluntary movement, and memory. The limbic system is essential for survival and works in conjunction with the "thinking brain. Mental and emotional illnesses are commonly the result of an imbalance in brain chemicals or electrical activity in the limbic system. Cerebellum the second largest structure of the brain, the (7) cerebellum, occupies the posterior portion of the skull. When the cerebrum initiates muscular movement, the cerebellum coordinates and refines it. Diencephalon the (8) diencephalon (also called the interbrain) is composed of many smaller structures, including the thalamus and the hypothalamus. The (9) thalamus receives all sensory stimuli except olfactory stimuli and processes and transmits them to the appropriate centers in the cerebral cortex. In addition, the thalamus receives impulses from the cerebrum and relays them to efferent nerves. The (10) hypothalamus regulates involuntary activities, such as heart rate, body temperature, and fluid balance. Brainstem the brainstem is composed of three structures: the (11) midbrain (also called the mesencephalon), separating the cerebrum from the brainstem; the (12) medulla, which attaches to the spinal cord; and (13) the pons, or "bridge," connecting the midbrain to the medulla. In general, the brainstem is a pathway for impulse conduction between the brain and spinal cord. The brainstem is the origin of 10 of the 12 pairs of cranial nerves and controls respiration, blood pressure, and heart rate. The brainstem is the site that controls the beginning of life (initiation of the heartbeat in a fetus) and the end of life (cessation of respiration and heart activity). Spinal Cord the spinal cord transmits sensory impulses from the body to the brain and motor impulses from the brain to the muscles and organs of the body. The sensory nerve tracts are called ascending tracts because the direction of the impulse is upward. Conversely, motor nerve tracts are called descending tracts because they carry impulses in a downward direction to muscles and organs. A cross-sectional view of the spinal cord reveals an inner area of gray matter composed of cell bodies and dendrites and an outer area of white matter composed of myelinated tissue of the ascending and descending tracts. The entire spinal cord is located within the spinal cavity of the vertebral column, with spinal nerves exiting between the intervertebral spaces throughout almost the entire length of the spinal column. Unlike the cranial nerves, which have specific names, the spinal nerves are identified by the region of the vertebral column from which they exit. Meninges the brain and spinal cord receive limited protection from three coverings called meninges (singular, meninx). Beneath the dura mater is a cavity called the subdural space, which is filled with serous fluid.
Cost of plavix
It serves as an etiological agent of lobar pneumonia hypertension 40 mg plavix 75 mg generic, an infection characterized by acute inflammation of the bronchial and alveolar membranes. These organisms are gram-positive cocci, tapered or lancet-shaped at their edges, and occur in pairs or as short, tight chains. Because of these properties (short-chain formation, -hemolysis, and failure of the capsule to stain on Gram staining), the organisms closely resemble Streptococcus viridans species. The pneumococcus, as it is called, is the causative agent of lobar pneumonia (lung), otitis media (middle ear), and meningitis (meninges) infections. It is currently the leading invasive bacterial disease in children and the elderly. Presently a vaccine is available for people who are designated as high risk for infection with this organism. The formation of a zone of inhibition greater than 15 mm on the left indicates the presence of alpha-hemolytic S. No zone of inhibition on the right indicates the presence of other alpha-hemolytic streptococcal species. Following incubation, the acid resulting from inulin fermentation will change the color of the culture from red to yellow. Cultures that are not capable of fermenting inulin will not exhibit a color change, which is a negative test result. Quellung (Neufeld) reaction: this capsular swelling reaction is a sensitive and accurate method of determining the presence of S. The reaction of the pneumococcal capsular polysaccharide, a hapten antigen, with an omnivalent capsular antiserum (Abcam, Inc. Mouse virulence test: Laboratory white mice are highly susceptible to infection by S. Examination of the peritoneal fluid by Gram stain and culture will reveal the presence of S. Aseptically add 2 loop-fulls of the test organisms to the appropriately labeled sterile test tubes to effect a heavy suspension. After incubation, examine the tubes for the presence or absence of turbidity in each culture. Record your observations of the appearance (clear or turbid) and bile solubility of each test organism in the Lab Report. With a glassware marking pencil, divide the bottom of a blood agar plate into two equal sections and label one section S. Using a sterile cotton swab, heavily inoculate the surface of each section with its respective test organism in a horizontal and then vertical direction, being careful to stay within the limits of each section. Using alcohol-dipped and flamed forceps, apply a single Taxo P disc (optochin) to the surface of the agar in each section of the inoculated plate. Label two phenol red inulin broth tubes with the name of each test organism to be inoculated. Using aseptic technique and loop inoculation, inoculate each experimental organism in its appropriately labeled tube of medium. Spread a loop-full of each test culture on a separate labeled clean glass slide and allow the slides to air-dry. Place a loop-full of the omnivalent capsular antiserum and a loop-full of methylene blue on each of two coverslips. Prepare a Gram-stained preparation of each test organism and observe under oil immersion. Examine blood agar plates for the presence of hemolysis and optochin activity by measuring the zone of inhibition, if any, surrounding the disc. Record the measurement in the Lab Report and indicate whether each organism is optochin-sensitive (zone of inhibition greater than 15 mm) or optochin-resistant (no zone or less than 15 mm). Describe the similarities between Streptococcus pneumoniae and Streptococcus viridans. A two-year-old toddler was brought to the emergency room as he had been pulling at his right ear and crying incessantly. On examining him, the doctor said that the child was suffering from a middle ear infection. Name the infection that the child was suffering from and the bacteria that caused it. Laboratory procedures designed to identify enteric pathogens using commercial multitest microsystems. The family consists of a number of genera whose members vary in their capacity to produce disease. Members of other genera, particularly Escherichia and Enterobacter, and to a lesser extent Klebsiella and Proteus, constitute the natural flora of the intestines and are generally considered to be avirulent. They are mesophilic, nonfastidious organisms that multiply in many foods and water sources. They are resistant to destruction by low temperatures and can therefore frequently survive in soil, sewage, water, and many foods for extended periods. From a medical point of view, the pathogenic Enterobacteriaceae are salmonellae and shigellae. Salmonellae are responsible for enteric fevers, typhoid, the milder paratyphoid, and gastroenteritis. In typhoid, Salmonella typhi penetrates the intestinal mucosa and enters the bloodstream, thus infecting organs such as the gallbladder, intestines, liver, kidney, spleen, and heart. Ulceration of the intestinal wall, caused by the release of the lipopolysaccharide endotoxin into the blood over a long febrile period, and enteric symptoms are common. Symptoms associated with this type of food poisoning include abdominal pain, nausea, vomiting, and diarrhea, which develop within 24 hours of ingestion of contaminated food and last for several days. Several shigellae are responsible for shigellosis, a bacillary dysentery that varies in severity. Ulceration of the large intestine, explosive diarrhea, fever, and dehydration occur in the more severe cases. Isolation and identification of enteric bacteria from feces, urine, blood, and fecally contaminated materials are of major importance in the diagnosis of enteric infections. In the past, several multitest systems have been developed for differentiation and identification of members of the Enterobacteriaceae. The obvious advantages of these units are the need for minimal storage space, the use of less media, the rapidity with which results may be obtained, and the applicability of the results to a computerized system for identification of organisms. There are also certain disadvantages with these systems, including difficulty in obtaining the proper inoculum size since some media require heavy inoculation while others need to be lightly inoculated, the possibility of media carryover from one compartment to another, and the possibility of using inoculum of improper age. Despite these difficulties, when properly correlated with other properties such as Gram stain and colonial morphology on specialized solid media, these systems are acceptable for the identification of Enterobacteriaceae. This needle can touch a single isolated colony and then in one operation be drawn through all 12 compartments, thereby inoculating all of the test media. In this manner, 15 standard biochemical tests can be performed in one inoculating procedure. The media become hydrated during inoculation of a suspension of the test organism, and the strip is then incubated in a plastic-covered tray to prevent evaporation. Each positive reaction is indicated by circling the number directly below its compartment. The circled numbers in each bracket are added together, and the sum is placed in the box below. A 7-digit number is obtained by totaling the positive values of each of the seven groups of three. In the hospital environment these often result from colonization of intravascular catheters, leading to bacteremia that can progress rapidly to sepsis and septic shock. Once identification of the infectious agent has been made, treatment with effective antimicrobials may be used.
Generic plavix 75mg on-line
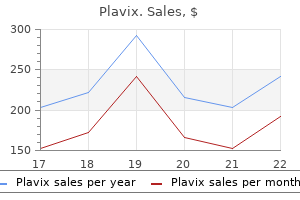
The number of cases detected in each country may be very small arrhythmia recognition chart purchase plavix 75 mg amex, but by combining data from the different home countries of tourists who stayed in the same hotel, it becomes possible to elucidate the cause of the outbreak and to instigate preventive measures. Validity of Notification Data the most important problem in the interpretation of notification data concerns their validity: Do they really measure what we want them to measure Is the yearly number of notified cases of a certain disease equal to the incidence Can observed changes over time be safely interpreted to represent changes in the underlying incidence Routine Surveillance of Infectious Diseases 143 the number of patients reported with a certain disease will be influenced by many factors that may well change over time or between places, and this will create biases when comparisons are made. The distance to the nearest hospital or clinic will play a role, as will costs and waiting times. Media reports of an outbreak will always bring more people to the clinic, and a portion of these will probably have milder infections which would not ordinarily have made them attend. Diagnostic methods Obviously, new tests that make it possible to diagnose atypical or asymptomatic cases of a disease will lead to an increased reported incidence. There seemed to be a substantial increase in incidence of chlamydia infections during the first part of the decade, with a doubling of cases from 1983 to 1987. However, what happened was that more and more of the microbiological laboratories started to set up chlamydia testing and make it available to the clinicians during this time. The second graph shows an almost perfect parallel increase in samples taken and patients diagnosed between 1983 and 1986. Therefore, the apparent epidemic of chlamydia was most likely due to improved diagnostic facilities and not to increased transmission. There is no reason to believe that there were fewer cases in 1983 than in 1987; we just could not find them at that time. In my experience it is often difficult for a doctor to specify this precisely; there may be several factors behind the decision to perform a test, and the request to single out one is often artificial. Reporting propensity Even though many countries have statutory notification for a number of diseases, adherence to this legislation varies enormously between them. Comparison between countries of figures published in national statistics is for the most part meaningless unless one has good information on the notification completeness behind those figures. Generally, notification works better in countries with a nationalized healthcare system than in countries with many independent clinics and laboratories. Also within countries, notification percentages may vary, and doctors often show a similar behaviour as patients: when there is increased media awareness of a certain disease, those cases become diagnosed and notified more readily. Attendance patterns, diagnostic methods, screening, and reporting propensity are all examples of biases (a term for this type of bias would be ascertainment bias) that could enter notification data, and they underline the caution with which such data should be approached. To this end, it does not matter if only a portion of all physicians report their cases as long as this portion is roughly constant over time. If, for example, a steady 15% of the doctors in a country are careful about sending in their notifications, incidence changes on a national scale will be detected anyhow. Also, the other sources of bias listed above will tend to be less problematic when the time scale is short. Routine Surveillance of Infectious Diseases 145 There is another, somewhat philosophical, problem connected to the use of notification data to describe routes of transmission. There were also some early reports of small family outbreaks of campylobacter diarrhoea after eating undergrilled chicken. The connection between chicken and this infection soon became well known to most clinicians, and they started asking their campylobacter patients if they had eaten chicken during the week or so before onset. Most physicians will feel quite content when their interview with the patient has revealed one established risk factor, and in situations like these a notification system may tend to overestimate the importance of this factor and instead fail to detect other important routes of transmission. This obviously has consequences for prevention, and you will find that the majority of reported point-source outbreaks in the literature had actually subsided well before they were detected. Published surveillance statistics usually date cases by the day the form was received (which is always known), not by actual date of diagnosis or of onset (which is often not reported). A curve showing, for example, weekly incidence over one year may indicate low incidence during holiday periods, when staff are short and everyone is too busy to fill out notification forms, and then a notable peak when all forms were mailed at the same time. Such a peak could easily deceive a novice reader that there had been a real epidemic just after the holiday period. The issue of notification delays is quite important for surveillance, but has received limited attention. One exception is a study from the United Kingdom in 1987 [4], which used the information on notification slips to estimate the time from diagnosis to receipt of the form for 15 different diseases. Delay was found to vary by region and by disease, being 5 days on average for measles but more than 2 months for tuberculosis. Accurate knowledge of past incidence was critical for projections on the future size of the epidemic. Second, even for notified cases there were often long delays, so that typically only 80% were reported in the year of diagnosis, with some cases still being reported two or more years after they had first been diagnosed. The epidemic was thus described by year of death, but even this reporting contained delays. The increasing use of electronic notification of findings directly from the microbiological laboratory to the surveillance centre cuts down delay considerably. Such reports usually contain very little epidemiological information, but if the name of the doctor requesting the test is included, it will be possible to contact her directly for a fuller picture. Feedback of Information the most important part of a surveillance system that builds on the active participation of a large number of physicians is probably information feedback: if the central agency just collects the data and analyses it, but fails to report back relevant findings to the people in the field, their interest in reporting will wane. They must feel that the information they get in return for spending time filling out forms is relevant to them in their daily work with patients. Adequate and timely information could aid in making diagnoses, choosing treatments and also in increasing vigilance for specific diseases. You will find solemn declarations like the above paragraph in any text on surveillance, but proper feedback is a difficult task. In most epidemic situations it has to be rapid, because there is little use in being told about an epidemic that has already subsided. It also has to be clinically relevant which is why it is important that the people responsible for the dissemination of the collated information keep in constant contact with the physicians who are the recipients. The Internet has facilitated feedback considerably, and many national surveillance centres now display their data publicly almost as soon as they have been checked and corrected. The problem is more becoming one of supplying the periphery with just the relevant information and not drowning practitioners with undigested floods of data. Sentinel Systems A sentinel system should ideally build on a random sample of the general practitioners in the country. This is seldom achievable, since reporting takes time, and many doctors may not have any special interest in mild to moderate infections. One therefore tries to get as good a geographical spread as possible from including interested colleagues. The average density of sentinel doctors in various European systems is usually around 1 per 30,000 to 100,000 population. Sentinel systems generally only report weekly number of patients with a certain disease, such as gastroenteritis or influenza-like illness, with little or no information about each Routine Surveillance of Infectious Diseases 147 case. Since they are based solely on clinical diagnosis, sensitivity is often very good, but specificity may be low. In order to compare data between doctors and over time, some kind of denominator must be used. This denominator takes care of holidays, absence for meetings and other events that may disturb the regular weekly pattern. Other Data Sources Active surveillance cannot rely only on notifications; it must make use of all available sources. These include laboratory reports, informal contacts with colleagues, media items and sometimes even rumours.
Buy plavix with visa
The kidneys compensate by increasing the reabs rption of sodium in the proximal tubule arteria hepatica comun order plavix uk. This results in a decrease in the amount of filtrate that reaches the dista tubule and thus decreased water excretion. She ceases nocturia almost entirely and daytime symptoms are being controlled as well. Once inside the cell, lithium impairs the action of aquaporin 2 ch nnels, esulting in the excretion of excess water. In a large single-center study, 31% of patients who underwent transsphenoidal surgery for pituitary adenoma developed polyuria immediately postoperation. This pattern begins with an init a polyuric phase that begins within 12 to 24 hours postoperatively and can last 2 o 4 days. An antidiuretic phase then ensues usually beginning around days 5 to 10 postoperatively. Patients with primary polydipsia must be educated that their symptoms are a normal response to their water consumption. Diabetes insipidus as a complication after pituitary surgery Nat Clin Pract EndocrinolMetab. Prevalence, predictors, and patterns of postoperative polyuria and hyponatremia i he immediate course after transsphenoidal surgery for pituitary adenomas. Pharmacokinetics, pharmacodynamics, long-term efficacy and safety of oral 1-deamino-8-D-arginine vasopressin in adult patients with central diabetes insipidus. Labs/Tests: Urinalysis reveals a urine osmolality of 180 mOsm/kg H2O with no other abnormal findings. A basic metabolic panel shows a serum osmolali y of 295 mOsm/kg, serum sodium of 142 mEq/L, glucose of 96 mg/dL, and calcium of 9 7 mg/dL, with all other values normal, including an absence of protein or glucose in the urine. She describes the pain as "behind the right eye" and radiating along the right side of the scalp toward the occiput. She went to bed with the pain but was awoken in the middle of the night when it worsened. The vision in her right eye is blurry, which prompted her to seek attention e 31 Ted Lyu What findings should point you toward an eye problem a the etiology of a headache Although headaches come in many shapes and sizes, it is important to remember that they may be the presenting complaint in atients with acute eye problems. If there is an ass ciat on with eye redness, tearing, light sensitivity, or blurry vision, an eye etiology should be high on the differential. In addition to the persistent headache, the patient complains of worsening right eye redness and tearing. She had one episode of vomiting en route to the emergency department and is complaining of "halos" around lights. This acronym stands for Onset, Provocation/Palli tio, Qual ty Radiation, Severity, and Timing and is useful to discern reasons for a par icu ar symptom. She complains of abdominal pain in addition to her headache and begins to wretch during the encounter. The right cornea is cloudier than the left, and it is more difficult to v sualize the pupil. You discover that it is larger than the left pupil and not reactive to ligh Th patient is unable to read the "E" (20/400) on the eye chart and can only count fingers near her face. Other medical history is significant for well controlled hypertension and hyperlipidemia. When the pumping mechanism of these cells becomes overwhelmed in the setting of elevated intraocula p essure, the cornea becomes edematous, putting the corneal nerves on stretch this is the etiology of pain in angle closure glaucoma. Beware of the patient who presents to the emergency room with nausea and vomiting along with a headache. The differential should also include uveitis, scleritis, keratitis, endophthalmitis, orbital cellulitis, giant cell arteritis, and, of course, intracranial causes of acute headache uch as subarachnoid hemorrhage, aneurysm, and so on. This produces a pressure gradient between the two chambers, resulting in the peripheral part of the iris bowing forward and ealing off the trabecular meshwork. In order to break the attack, a conduit must be created between the posterior and anterior chamber to reequilibrate the pressure and a low the angle to reopen. Laser peripheral iridotomy is the treatment of choice for angle closure caused by pupillary block. These medications work by two mechanisms: (1) by decreasing aqueous production and (2) by i cre ing aqueous outflow. Medications that decrease aqueous production include topical beta blockers (levobunolol, betaxolol, carteolol, metipranolol, and timolol), oral carbonic anhydrase inhibitors (acetazolamide and methazolamide), topical carbonic anhydrase inhibitors (dorzolamide and brinzolamide), and alpha-2 agonists (apraclonidine and brimonidine tartrate). Medications that improve aqueous outflow include prostaglandin analogs (latanoprost, travoprost, bimatopros, nd unoprostone isopropyl), topical miotic agents (pilocarpine and echothiophate), and epinephrin preparations (Epifrin and Propine). B,Theirishas become opposed to the lens blocking the flow of aqueous and causing it to back up in the posterior chamber. The only selective topical beta blocker is betaxolol, which is not as effective as the nonselective beta blockers. Carteolol has intrinsic sympathom metic activity, which may counteract some of the systemic beta blocking effects Also, be aware that carbonic anhydrase inhibitors contain sulfa and are therefo e contraindicated in patients with sulfa allergies. Forty-five minutes later, the in raocular pressure is 36 mm Hg, and the cornea appears to be clearer. A p ume of aqueous is seen through the iridotomy, and the anterior chamber begins to d epen. A laser iridotomy may spontaneously close due to tissue fibrosis, so this eye should be monitored very closely, and the patient should be warned of this possibility. Also, because of the apposition of the iris to the trabecular meshwork, the angle may become sealed due to the development of peripheral anterior synechiae. If this is the case, surgical intervention would be indicated to create an alternate pathway for the drainage of aqueous. The most important next step is to look at the angle structure in the other eye with gonioscopy. If narrow, as in this patient, many ophthalmologists advocate placing a prophylactic laser iridotomy. Cataract extraction is also a good alternative to laser iridotomy in pupillary block and angle crowding, especially in the elderly. This is seen p imarily in diabetics due to formation of neovascular vessels n the angle Always evaluate the structure of the uninvolved eye as it can provide clues about the disease in the other eye. High pressure can result in cil ary body ischemia, which means aqueous production decreases, but this i usually temporarily. Pilocarpine n concen rations greater than 2% can result in forward rotation of the ciliary body, pushing the lens-iris diaphragm anteriorly and worsening the attack. In this case, an anteriorly rotated ciliary process pushes the peripheral iris forward, closing the angle. Other considerations would be malignant glaucoma, lens-induced glaucoma, choroidal effusion/ciliary body rotation, or even tumor. Findings: Elevated intraocular pressure, corneal edema, shallow anterior chamber, decreased vision in the right eye. Labs/Tests: Slit lamp exam, gonioscopy with indentation, visual field testing after the acute episode has resolved. In a patient who has fever and an extremity that is erythematous, swollen, warm, and tender, c llulitis should be the primary concern. Cellulitis is an infection of the dermal layers of the skin and the immediate subcutaneous tissue. The leukocytosis with left shift (immature neutrophils, such as bands) is consistent with this infectious process and the left inguinal mass represents swelling of the draining lymph node(s) (lymphadenitis), a c mmon sequelae of cellulitis. Therefore, a Doppler ultrasound of the leg veins is commonly performed in the emergency department to distinguish between the two conditions.
Elaeis melanococca (Palm Oil). Plavix.
- Vitamin A deficiency.
- How does Palm Oil work?
- Decreasing symptoms of malaria.
- What is Palm Oil?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97083
Buy 75mg plavix
Surgical correction involves removing part of the stapes (stapedectomy or prehypertension and chronic kidney disease plavix 75 mg on line, more commonly, stapedotomy) and implanting a prosthetic device that allows sound waves to pass to the inner ear. Oncology Oncological disorders can occur in almost any structure of the eye or ear as a primary malignancy or spread from other areas of the body to the eye or ear via metastasis. Eye Two major neoplastic diseases account for more than 90% of all primary intraocular diseases: retinoblastoma, found primarily in children, and melanoma, found primarily in adults. Vision is impaired, and in about 30% of patients, the disease is found in both eyes (bilateral). Melanoma may occur in the orbit, the bony cavity of the eyeball, the iris, or the ciliary body, but it arises most commonly in the pigmented cells of the choroid. The disease is usually asymptomatic until there is a hemorrhage into the anterior chamber. If malignancy occurs in the choroid, it usually appears as a brown or gray mushroom-shaped lesion. Treatment for retinoblastoma usually involves the removal of the affected eye(s) (enucleation), followed by radiation. Ear Malignant and nonmalignant tumors can arise in the external ear, the canal, or the middle ear. Malignant tumors of the ear include basal cell carcinoma and squamous cell tumors. The most common ear malignancy is basal cell carcinoma, which usually occurs on the top of the pinna as the result of sun exposure. However, failure to treat it in a timely manner may result in the need for extensive surgery to remove the tumor. In appearance, it closely resembles basal cell carcinoma, and biopsy is required to make a definitive diagnosis. Squamous cell carcinoma grows more slowly than basal cell carcinoma; however, because of its tendency to metastasize to the surrounding nodes and the nodes of the neck, it must be removed. Surgery combined with radiation therapy is the most effective treatment for squamous cell carcinoma. Disease Focus 577 Diseases and Conditions this section introduces diseases and conditions of the eye and ear, along with their meanings and pronunciations. Visual defect in which the eyeball is too short, and the image falls behind the retina; also called farsightedness Correction of hyperopia requires the use of biconvex lenses. Visual defect in which the eyeball is too long, and the image falls in front of the retina; also called nearsightedness Correction of myopia requires the use of biconcave lenses. Small, hard tumor developing on the eyelid, somewhat similar to a sebaceous cyst; also called meibomian cyst Inflammation of the conjunctiva and inner eyelids with vascular congestion; also called pinkeye Causes of conjunctiva include irritants, allergy, and viral, bacterial, or fungal infections. Small yellowish deposits composed of retinal pigment cells that develop under the retina and are associated with an increased risk of developing age-related macular degeneration Eversion, or outward turning, of the edge of the lower eyelid, causing it to pull away from the eye, generally associated with aging and weakness of the small muscles around the eyelid Inversion, or inward turning, of the edge of the lower eyelid, commonly causing friction as the eyelashes and outer eyelid rub against the surface of the eye Abnormal overflow of tears Epiphora is sometimes caused by obstruction of the tear ducts. Localized, circumscribed, inflammatory swelling of one of the several sebaceous glands of the eyelid; also called stye Hordeola are commonly caused by a bacterial infection. Visual distortion of objects Metamorphopsia is commonly associated with errors of refraction, retinal disease, choroiditis, detachment of the retina, and tumors of the retina or choroid. Impaired vision in dim light; also called night blindness Common causes of nyctalopia include cataracts, vitamin A deficiency, certain medications, and hereditary causes. Hearing loss refers to impairment in hearing, and the individual may be able to respond to auditory stimuli, including speech. Blocking of sound waves as they pass through the external and middle ear (conduction pathway) Inflammation of the inner ear that usually results from an acute viral disease, such as mumps, measles, or influenza Labyrinthitis may lead to sudden incapacitating vertigo, nausea, and various degrees of hearing loss. Impairment of hearing resulting from old age; also called presbyacusia In presbyacusis, patients are generally able to hear low tones but lose the ability to hear higher tones. This condition usually affects speech perception, especially in the presence of background noise, as in a restaurant or a large crowd. Perception of ringing, hissing, or other sounds in the ears or head when no external sound is present Tinnitus may be caused by a blow to the head, ingestion of large doses of aspirin, anemia, noise exposure, stress, impacted wax, hypertension, and certain types of medications and tumors. Sensation of a spinning motion of oneself or of the surroundings Vertigo usually results from damage to inner ear structures associated with balance and equilibrium. Disease Focus 581 Diagnostic, Surgical, and Therapeutic Procedures this section introduces diagnostic, surgical, and therapeutic procedures used to diagnose and treat eye and ear disorders. Test that uses different water temperatures to assess the vestibular portion of the nerve of the inner ear (acoustic nerve) to determine whether nerve damage is the cause of vertigo In the caloric stimulation test, cold and warm water are separately introduced into each ear while electrodes placed around the eye record nystagmus. Eyes move in a predictable pattern when the water is introduced, except with acoustic nerve damage. The electrodes record eye movement relative to the position of the ground electrode. Visual examination of the interior of the eye using a handheld instrument called an ophthalmoscope, which has various adjustable lenses for magnification and a light source to illuminate the interior of the eye Ophthalmoscopy helps detect eye disorders and other disorders that cause changes in the eye. Evaluation of refractive errors of the eye by projecting a light into the eyes and determining the movement of reflected light rays Retinoscopy is especially important in determining errors of refraction in babies and small children who cannot be refracted by traditional methods. Stereoscopic magnified view of the anterior eye structures in detail, which includes the cornea, lens, iris, sclera, and vitreous humor the application of fluorescein dye during a slit-lamp examination makes it easier to detect and remove foreign bodies and treat infection, corneal ulcers, and abrasions. Evaluation of intraocular pressure by measuring the resistance of the eyeball to indentation by an applied force Tonometry is a standard eye test to detect glaucoma and part of most routine ophthalmic examinations. The applanation method of tonometry uses a sensor to depress the cornea and is the most accurate method of tonometry. Sensorineural hearing loss involves impairment of the inner ear, auditory nerve, or brain. In a normal test, air conduction provides longer and louder sound perception than does bone conduction. Tuning fork test that determines whether hearing loss occurs in the middle ear (conductive hearing loss) or in the auditory nerves or hair cells of the inner ear (sensorineural); also called conductive and sensorineural hearing loss test In the Weber test, a vibrating tuning fork placed on the center of the forehead directs sound to each ear simultaneously. Part of an eye examination that determines the smallest letters that can be read on a standardized chart at a distance of 20 feet and commonly expressed as a fraction the top number refers to the distance from the chart, and the bottom number indicates the distance at which a person with normal eyesight can read the same line. For example, 20/40 indicates that the patient correctly read letters at 20 feet that can be read by a person with normal vision at 40 feet. Evaluation of blood vessels and their leakage in and beneath the retina after injection of fluorescein dye, which circulates while photographs of the vessels within the eye are obtained Fluorescein angiography facilitates the in vivo study of retinal blood flow circulation and is particularly useful in the management of diabetic retinopathy and macular degeneration, two leading causes of blindness. Removal of the contents of the eye while leaving the sclera and cornea intact Evisceration is performed when the blind eye is painful or unsightly. The eye muscles are left intact, and a thin prosthesis called a cover shell is fitted over the sclera and cornea. Procedure using a specialized laser passed through a temporary flap made in the cornea to reshape underlying corneal tissue this procedure corrects farsightedness, nearsightedness, and astigmatism. Corrective surgery for a deformed or excessively large or small pinna Otoplasty is also performed to rebuild new ears for those who lost them through burns or other trauma or were born without them. Pharmacology 587 Pharmacology Disorders of the eyes and ears are commonly treated with instillation of drops onto the surface of the eye or into the cavity of the ear. The eyes and ears are typically irrigated with liquid solution to remove foreign objects and provide topical application of medications. Pharmacological agents used to treat eye disorders include antibiotics for bacterial eye infections, beta blockers and carbonic anhydrase inhibitors for glaucoma, and ophthalmic decongestants and moisturizers for irritated eyes. Mydriatics and miotics are used not only to treat eye disorders but also to dilate (mydriatics) and contract (miotics) the pupil during eye examinations. Ear medications include antiemetics to relieve the nausea associated with inner ear infections, products to loosen and remove wax buildup in the ear canal, and local anesthetics to relieve the pain associated with ear infections. Increase aqueous humor outflow or decrease its production, resulting in decreased intraocular pressure Combinations of antiglaucoma drugs that work by different mechanisms are commonly used. Constrict the small arterioles of the eye, decreasing redness and relieving conjunctival congestion Ophthalmic decongestants are over-the-counter products that temporarily relieve the itching and minor irritation commonly associated with allergy. Treat and prevent nausea, vomiting, dizziness, and vertigo by reducing the sensitivity of the inner ear to motion or inhibiting stimuli from reaching the part of the brain that triggers nausea and vomiting Antiemetics are commonly used to treat vertigo. Provide temporary relief from pain and inflammation associated with otic disorders Otic analgesics may be prescribed for otitis media and otitis externa.
Syndromes
- Location in which surgery is not possible
- Upper body obesity (above the waist) and thin arms and legs
- Know about and practice fire escape routes at home, work, and school.
- Shock
- If you are or could be pregnant
- Weakness
- Hypoparathyroidism
Buy online plavix
The confounding in this example comes from the fact that the population of rock fans are younger than the general population blood pressure medication rebound effect purchase 75mg plavix mastercard, on average, and chlamydia infection is most common among people between 18 and 23. The 40 Modern Infectious Disease Epidemiology authorities wanted to recall all these cars to look at their steering mechanisms. An alternative explanation to the finding was that such used cars were often bought by young men who wanted a relatively inexpensive but fast car. The proper definition is that a confounder is a factor which is associated with the exposure one is studying and at the same time associated with the outcome. In the rock concert example above, age is a confounder even though it is not the cause of chlamydia infection. If you read other textbooks on epidemiology, you will find that they devote much more space, often entire chapters, to the subject of confounding. If you think that you have found an exposure associated with an outcome and you divide your population into those exposed and those not exposed, you should immediately ask yourself: Is there any other factor linked to this exposure and to this outcome that might confound the association I have found Are people in the exposed group different from the non-exposed ones in any other way Epidemiology is just as much a question of common sense as of rigid definitions and thorny statistics. If you read that coffee drinkers are at higher risk of pancreatic cancer, you should immediately ask yourself: Is there some other factor that is more common in coffee drinkers than in non-coffee drinkers The coffee consumption could just be a marker of some more relevant risk factor and the association due to confounding. Prevalence of chronic hepatitis B infection is much higher in many countries outside Europe. However, this requires that one realizes beforehand what the possible confounders might be, which is again a question of common sense. If we had forgotten to ask about mayonnaise, we would have believed that the fish was the culprit. Furthermore, if there is complete overlap between two exposures, if everyone who had eaten fish had also had mayonnaise, and vice versa, it would be impossible to differentiate between these two exposures in the epidemiological analysis. Consider a situation in which I hit my thumb hard with a hammer, trying to hang a painting on the wall. The improved general economical situation in the country which made it possible for me to buy a new house Or, is it the inflammatory reaction with oedema and vasoactive peptides in the tissue of my thumb This is a silly example, but it underlines the problem of defining exactly at what level of explanation we want to stop when we talk about the cause of a disease. Another example: known risk factors for pneumococcal septicaemia are: smoking; alcoholism; asplenia; old age; exposure to a pneumococcus. If you see a patient with a severe pneumococcal pneumonia in the emergency ward, how could you tell which of these risk factors was really the cause of this particular case of disease When trying to think about causation it is often helpful to make the distinction between necessary and sufficient causes. In the above example, exposure to a pneumococcus is a necessary cause: without it there would be no pneumococcal pneumonia. It is not sufficient to explain the case, however, since most people who are exposed to the bacteria will not develop any disease at all. Ingestion of a high number of Campylobacter jejunii bacteria is a sufficient cause of gastroenteritis. There are very few diseases for which such a single cause exists, also among the non-infectious ones. The main pillar for our scientific understanding of the concept of cause is the experiment. If a certain set of conditions always produces the same outcome, then we say that we have discovered the cause of this event. From millennia of practical experimentation we know that if we throw a stone in the air, it will fall down on the ground, and ever since Newton we are satisfied with the explanation that gravitation pulls the stone towards Earth. Just as in the above example with my hurting thumb, there is obviously an explanation at a higher level: What is it that causes this gravitational force We are content that we have found a cause when this cause explains and predicts events in the world around us. Much of the progress in clinical medicine during the last century is also due to experiments, either in the laboratory or in clinical trials involving real patients. In this way, the underlying pathological causes of many diseases and conditions have been revealed. We can almost never set up precisely the same set of original conditions and watch the outcome over and over again. Nor can we systematically change the original conditions slightly, one by one, to see how this affects the outcome. In the absence of the possibility to do experiments, how can we make any statements at all about causes of disease from epidemiological studies The epidemiological literature is full of discussions about this problem, and the best-known example comes from a paper by the British statistician Sir Austin Bradford Hill in 1965 [6]. He lists nine criteria to support that an observed risk factor is really the cause of the disease we are observing, but I will only address three, with some personal comments. Temporality this criterion is almost self-evident: in order for a risk factor to be a cause of a disease, it must affect the patient before she develops the disease. An example comes from the discussion of the association between infection with Chlamydia pneumoniae and coronary heart disease: genetic material from C. Biologic Gradient this is one of the strongest criteria for causation: if increasing levels of exposure to a risk factor either raises incidence, or produces more severe disease, then this is strong support that we have found a cause. In Chapter 12, we describe in some detail the discovery that tick bites transmit Lyme disease, but here I would only point out that the relation between reported number of tick bites and risk of disease was one of the early findings that put the researchers on track. Values above 100, with nice narrow confidence intervals, however, should generally make you feel quite comfortable. You should be very careful with this one: there are few observed associations between an exposure and an outcome that could not be given an elegant, highly credible explanation by a creative research mind. There is still so much within the area of medicine that is unknown or halfknown, and so much contradictory knowledge, that most findings could always get some support. One of the best examples from the last decades comes from discussions on the aetiology of childhood allergy and asthma. Causes suggested include: mites, diet, animals and pets, indoor ventilation, the anaerobic gut flora, excessive cleanliness, and so on. Each of these hypotheses has had proponents who very convincingly explained the biologic basis for their findings. Summary If we lack information about exposures and outcomes in a clearly defined population, we can make a case control study. Since we are usually only looking at a sample of all possible cases and controls, there is a statistical uncertainty in the exact figures which is measured by calculating a confidence interval. The most difficult part of a case control study is to choose appropriate controls. Controls should not be picked to be as similar as possible to the cases, but rather to inform us how common a certain risk factor or exposure is in the background population from which the cases arose. Even if a factor is significantly associated to disease, this may just be a statistical finding, where the division according to exposure also divides the people into high-risk and lowrisk groups according to some real risk factor. The concept of confounding is closely coupled to the concept of cause, and the observational science of epidemiology will always have a problem with proving that it has found a proper cause of a disease. Importance of heterosexual activity in the transmission of hepatitis B and non-A, non-B hepatitis. Assessment of the protective efficacy of vaccines against common diseases using case control and cohort studies.
Buy plavix 75mg cheap
Brief blood pressure medication isn't working purchase plavix without a prescription, bilateral convulsions may be seen with syncope as well (termed convuls ve syncope), but this can be confusing because some seizures, namely myoclonic seizures, might look similar. A typical seizure lasts for 2 to 3 minutes, so seizure durations of longer than 5 minutes either indicate status epilepticus or a nonepileptic event. A patient returning to baseline quickly (within a few seconds) without a period of postictal confusion or lethargy after a prolonged, convulsive event is less likely to have had a true epileptic seizure. Responsiveness during an event of bilateral clonic activity is also less likely to be an epileptic seizure, as involvement of the bilateral motor regions is unlikely to be seen in isolation without diffuse bilateral cerebral dysfunction causing altered state of awarene s On the other hand, patients may vocalize incoherently during partial-onse seizures, and odd, complex, and almost psychotic-appearing behavior is commo with frontal lobe seizures. An ictal cry is a disturbing sound made during tonic contracti n of the diaphragm usually during a generalized tonic-clonic seizure. Lateral tongue bites, urinary or bowel incontinence, and injuries such as fractures or dislocations are also strongly suggestive of epileptic seizures. Cataplexy seen in narcolepsy may be another seizure mimic, but cataplexy is a sudden loss of muscle tone often at the knees that is tr ggered by an emotional response and has preserved consciousness. He thinks the seizure lasted less than 5 minutes altogether He thinks his friend wet himself and bit his tongue because blood was coming out of his mouth. On exam, the patient is afebrile, blood pressure s 125/80 mm Hg, pulse rate is 90/min, respiration rate is 14/min, and oxygen saturation is 100% on room air, and he is currently arousable but disoriented to time and p ace His general exam reveals abrasions on his scalp and elbows and a left lateral tongue laceration His pupils are 4 mm and equally reactive to light, and on his motor exam his left arm and leg dr ft downward slightly when raised. The history provided by the witness is fairly convincing for a true ep leptic seizure, likely a tonicclonic seizure. At this point, we do not know whether he has had similar seizures in his history, in which case perhaps he ha epilepsy. Epilepsy is defined as the presence of two or more unprovoked seizures occurring greater than 24 hours apart, or a single seizure with a risk of recurrence greater than 60% in the next 10 years. A phenytoin level is measured a 8 mg/dL which is subtherapeutic (normal range is 10 to 20 mg/dL). At this time his fath r arrives and explains that the patient has a history of epilepsy since he was a teenager and was taking phenytoin for years. The patient is still not completely awake and er, and has a milder left-sided hemiparesis. The emergency room orders a fosphenytoin load of 10 mg/kg and he is admitted to the medicine service after having a seizure without returning to baseline mental status. Status epilepticus is defined as a single seizure lasting more than 5 minutes or two or more seizures without a return to baseline mental status in between. This may simply be a case of a prolonged postictal state, but he might have ongoing subclinical or nonconvulsive seizures and might be at isk o having further convulsive seizures. The shaking ceases but the patient is still lethargic, he is tachycardic to 120/min, respiration rate is 18/min, and his oxygen sa uration is 95% on room air. He appears to not be in danger of respiratory failure, thus intubation at this time is not necessary; however, admission to an intensive care unit would be appropriate. Another phenytoin level may be drawn but in the meantime, a second antiepileptic medication can be considered Valproate or leveti acetam is commonly used next in the algorithm. Pulse oximetry remains above 95%, but oxygen is now administered via nasal cannula. His outpatient pharmacy is contacted, and he is actively prescribed two antiepileptic medications: phenytoin and levetiracetam. What should be considered in the follow up of this patient and need for specialist care In this patient with epilepsy on chronic antiepileptic medication, nonadherence to the medication regimen is a probable trigger for status epilepticus. Adverse reactions to medications can cause patients not to adhere to their medication regimens. Other triggers for seizures in patients with epilepsy include underlying infections, substance use, and sleep deprivation. In approximately one third of patients with epilepsy, their seizures can be refractory to medical management alone and surgical options such as resective surgery (often of the temporal lobe) r neurostimulation. The specialist will reconfirm the epilepsy diagnosis usually through epilepsy monitoring, and consider surgical approaches to treatment://t. He reports compliance with both medications but says that last night he woke up with his tongue bitten aga n and the bed sheets wet. The patient is exper e cing ataxia and sedation due to slight phenytoin toxicity, and his irritability is probably an adverse ffect of levetiracetam. Diagnosis: Medically refractory epilepsy and status epilepticus rs es s errs the patient returns for follow-up visit 1 year later asking for medical clearance for a temporal lobectomy. He is currently taking lamotrigine and oxcarbazepine as his antiepileptic medications. He reports a much better mood and lower side effects, but he still has occasional seizures and wishes to proceed with surgery. His exam is normal, but his lab work demonstrates a sodium level of 131 mmol/L (the normal threshold is 134 mmol/L). Hyponatremia is a common side effect of medications including oxcarbazepine, carbamazepine, and phenytoin. Mild decreases in sodium can be monitored, but more severe decreases should be addressed with the neurologist for a possible therapy change as hyponatremia may provoke se zures. However, some medications are indicated for partialonset seizures rather than for generalized seizures: oxcarbazepine and carbamazepine are two of these. These two may even worsen generalized epilepsy such as juvenile myoclonic epilepsy. For primary generalized epilepsy, valproate or divalproex is considered to be most efficacious, although several safety conce ns especially teratogenicity for women of childbearing age, limit its use n many patients. For example if a pat ent has both epilepsy and migraine, topiramate or divalproex may be useful to help treat both disorders. Patients who have a history of bipolar disorder may have both conditions managed with medications such as lamotrigine, divalproex carbamazepine, or oxcarbazepine. In some states, a physician is required to report a patient who had a seizure or any loss of consciousness to the State Department of Motor Vehicles. A specialized epilepsy surgery center will have various options for surgical treatment of epilepsy for patients who do not have good control or seizure freedom with medication alone. For patients with severe refractory generalized epilepsy with falls, a corpus callosotomy can reduce falls and morbidity but does not cure seizures Vagus nerve stimulation can reduce the frequency of seizures. Temporal lobectomy however, can bring about complete seizure freedom in up to 70% of patients. Other types of surgeries, such as frontal lobectomy and multiple subpial transections, can bring about seizure freedom at lower rates. Responsive neurostimu ation is a newer technology designed for patients who cannot have respective surgery because of the location of their seizure onset zone. It is thought to be due to an abnormal vascular response, causing vasoconstriction of the digital arteries and cutaneous arterioles. This phase is followed by a cyanotic phase, as the residual blood in the finger desaturates. The red phase is due to hyperemia as the attack subsides and blood flow is restored. The author prefers these screening questions: Do your fingers change colors in the cold Cutaneous exam reveals sclerodactyly of both hands as well as skin induration of the forearms and ante io chest. Often, cardiac involvement is a result of pulmonary hypertension, but primary cardiac involvement has been recognized. Erythrocyte casts characterize a nephritic urin sediment and indicate the presence of glomerulonephritis. During the procedure, lavage aliquots are progressively more hemorrhagic, confirming the diagnosis. Findings include intimal proliferation with concentric "onion-skin" hypertrophy, leading to significant vessel narrowing; these findings are nonspecific and can be found in other causes of thrombotic microangiopathy. In instances where there is concern for overlap with other systemic rheumatic diseases, other antibodies. This would include a "pulse" dose of methylprednisolone 1000 mg daily for 3 days, followed by prednisone or equivalent 1 mg/kg/day.
Purchase plavix without a prescription
The Difference between Risk and Rate Another way to analyse the data in the example we just used would be to calculate the rate of infection per person-month arterial blood gases 75 mg plavix free shipping, just as we did in the little example in Chapter 6. Initially, they are all susceptible and during the first year of our study we diagnose 12 cases. However, if we extrapolate to 10 years it appears as if the risk of getting herpes will be 120% which cannot be true since a risk can never be higher than 100%. Just as has been mentioned before, a figure for a risk must always include the time period we are considering. If exposure to a pathogen is continuous, then the probability of observing an infection in a study subject will obviously be greater the longer he is followed. In an influenza epidemic lasting from November through February, the risk of becoming infected in November will be lower than the risk of becoming infected at any time during the four-month epidemic. If we instead calculate the rate, this problem of having to state the time period of observation can be evaded: assume that the 12 cases in the herpes example above appear evenly over the year. We will then follow 100 children for 1 month, but after this one child will have had an infection with herpes type 1. We then follow 99 susceptibles for another month, but after that one more will have had the disease. The total number of person-months added during the 1-year study will thus be: 100 + 99 + 98 + 97 +. Just as in the example with speed, it does not matter which time unit we choose to measure rate; a speed of 72 km/h is the same as 1. We see that the rate per year is slightly higher than the risk of getting herpes during 1 year. If one out of every 100,000 persons in a country get meningococcal meningitis each year, this does not change the number at risk appreciably, and in this case the risk and the rate are both 1/100,000 per year. Now to get back to the bednet and malaria example that we have spent the greater part of this chapter analysing by survival methods. The number of person-months in this study is easily calculated from the second table in the example: the total for all 12 subjects is 58. There were three children who developed malaria, and the rate thus becomes 3/58 cases per person-month = 0. When rates are being calculated as above, it is always assumed that the incidence rate is constant over time. The survival analysis gives much more information about changes in rate over time. This is especially true if the times are long, giving considerable problems with losses to follow-up during the study. In survival analysis, the time in the cohort is divided into smaller units, like months or years, and for each time unit the number of subjects who could experience the event under study. By calculating rates, it becomes possible to get an incidence measure that is independent of time period. A simple model for an epidemic is presented, and the restrictions of such models are discussed. The regular recurrence of epidemics and the similar shapes of consecutive epidemics of a disease have for a long time tempted people with a mathematical inclination to make some kind of model. With the exception of 1948, the epidemic peaks evidently occur every second year, and the highest number of cases during an epidemic always seems to be in the first quarter of the year. If this way of thinking about infectious diseases in terms of models seems somewhat unfamiliar, one should only consider all the results of similar models that we meet daily in other circumstances. One of the most complex examples is given by the weather forecasts which are made using supercomputers, where large systems of equations are linked to huge libraries of previous meteorological patterns. The present situation is compared with these data, and the most probable future course calculated. Another ramification has been to try and 107 108 Modern Infectious Disease Epidemiology predict sociological developments, for although the future actions of an individual may be impossible to foresee, it might be feasible to say something about how large groups of people will behave. The fact that these forecasts rarely turn out to agree with the actual economical development does not seem to diminish their news value: a good example of our insatiable need to see into the future. In contrast to the prophecies of cards or crystal balls, such predictions about the future that are based on a scientific way of thinking are often phrased in mathematical terms. This can make them difficult to understand for the non-mathematician, and it also lends them an air of exactitude that they seldom merit. No model will be better than the assumptions on which it was built, and these assumptions are usually quite easy to understand and question, even if the formulae look deterring. It is sometimes difficult to see the exact assumptions underlying the model, but in any good publication they should be stated clearly. By giving a simplified picture of a development, where less important factors have been removed, they can aid us in understanding complex contexts. They may consequently also help us to realize which factors are the most important determinants of the development, and which we thus should study closer and try to measure more exactly. Finally, models make quite good tools for teaching infectious disease epidemiology. Basic Reproductive Rate We have already come across the concept of reproductive rate in Chapter 2, and we have seen that it measures the potential for an infection to spread in a population. One of these does not spread the infection, but the other infects one more, and so on. We see that the average number of persons directly infected by each case is: (1 + 2 + 0 + 1 + 3 + 2 + 1 + 2 + 1 + 2)/10 = 1. The actual reproductive rate thus decreases as the infection spreads, but the basic rate is unaffected by this. In order to calculate an average R0, we would first introduce an infectious case into a population and count the number of secondary cases. The strict definition above thus becomes quite theoretical, but we can usually get a good estimate of R0 by counting the secondary cases as long as the number of already immune contacts is negligible, that is, at the beginning of an epidemic. Once an epidemic is under way, the current reproductive rate is usually denoted just by R. From the reasoning here, it may not come as a total surprise that the necessary condition for an epidemic is that R0 is greater than 1. In words, this means that every infected person on average infects more than one new person. In fact, the three possible situations are: R0 < 1 the disease will eventually disappear R0 = 1 the disease will become endemic R0 > 1 there will be an epidemic If R0 < 1, then every new wave of infection in the population will consist of fewer people than the one before, and eventually the disease will die out. If R0 is equal to 1, then there will be approximately the same number of people infected all the time which is the definition of an endemic, and if R0 > 1, there will be an ever increasing number of infected people. As time goes by more and more people are becoming immune, and at some time point half the population will have become immune to the disease. This means that of all the contacts an infectious case will have with other people, only one half will actually transmit the infection, and R will have fallen from the original value of 2 to 1. As even more people become immune, the actual R will continue to fall below 1, and the epidemic will eventually die out. This way of reasoning has important implications for the issue of vaccination coverage. Well, if the basic reproduction rate is R0, this means that on average R0 contacts will be infected by someone who has the infection. In the unvaccinated, natural stage, a primary case of disease will thus infect four people. However, if 25% of the population have already been immunized against the disease, then one of the four people who should have become infected by the primary case will escape infection.
