
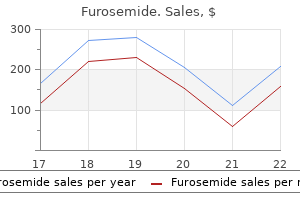
Buy furosemide 100 mg without a prescription
Phenothiazines and thioxanthenes often display erratic and unpredictable patterns of absorption after oral administration (highly lipid soluble and accumulate in well-perfused tissues such as the brain) hypertension table discount 40mg furosemide free shipping. Metabolism of phenothiazines and thioxanthenes is principally by oxidation in the liver followed by conjugation. Most oxidative metabolites are pharmacologically inactive, with a notable exception being 7-hydroxychlorpromazine. Despite the common occurrence of side effects, these drugs have a large margin of safety and overdoses are rarely fatal. Tardive dyskinesia may occur in 20% of patients who receive antipsychotic drugs for longer than 1 year. Manifestations of tardive dyskinesia include abnormal involuntary movements (tongue, facial and neck muscles, upper and lower extremities, truncal musculature, and, occasionally, skeletal muscle groups involved in breathing and swallowing). Acute dystonic reactions occur in approximately 2% of treated patients and are most likely to occur within the first 72 hours of therapy. Acute skeletal muscle rigidity and cramping may develop, usually in the musculature of the neck, tongue, face, and back. Neuroleptic malignant syndrome is characterized by (a) hyperthermia; (b) generalized hypertonicity of skeletal muscles; (c) instability of the autonomic nervous system manifesting as alterations in systemic blood pressure, tachycardia, and cardiac dysrhythmias; and (d) fluctuating levels of consciousness. Mortality is 20% to 30%, with common causes of death being ventilatory failure, cardiac failure and/or dysrhythmias, renal failure, and thromboembolism. The cause of neuroleptic malignant syndrome is not known and, as a result, treatment is empirical and includes supportive measures and the administration of dantrolene and the dopamine agonists bromocriptine or amantadine. Malignant hyperthermia associated with anesthesia as well as the central anticholinergic syndrome may mimic the neuroleptic malignant syndrome. A distinguishing feature is the ability of nondepolarizing muscle relaxants to produce flaccid paralysis in patients experiencing the neuroleptic malignant syndrome but not in those experiencing malignant hyperthermia. Sedation appears to be due to antagonism of 1-adrenergic, muscarinic, and histamine (H1) receptors. The antiemetic effects of antipsychotic drugs reflect their interaction with dopaminergic receptors in the chemoreceptor trigger zone of the medulla (seem most effective in preventing opioidinduced nausea and vomiting). Obstructive jaundice that is considered to be an allergic reaction occurs rarely 2 to 4 weeks after administration of phenothiazines or thioxanthenes. The ventilatory depressant effects of opioids are likely to be exaggerated by antipsychotic drugs. The miotic and sedative effects of opioids are increased, and the analgesic actions are likely to be potentiated. Clozapine is the only antipsychotic that does not seem to cause tardive dyskinesia or extrapyramidal side effects. Among the most common side effects are sedation, nausea and vomiting, and orthostatic hypotension. A presumed manifestation of a parasympatholytic effect is sustained mild sinus tachycardia. Agranulocytosis is a particularly serious side effect of clozapine, occurring in less than 1% of patients. Haloperidol has a longer duration of action than droperidol and lacks significant -adrenergic antagonist effects such that decreases in systemic blood pressure are unlikely (principal use is for treatment of agitation and delirium in the intensive care unit). Side effects of butyrophenones resemble those described for phenothiazines and thioxanthenes. The outwardly calming effect of droperidol may mask an overwhelming fear of surgery. Akathisia (most often a feeling of restlessness in the legs) may accompany administration of droperidol as preoperative medication. As a dopamine antagonist, droperidol evokes extrapyramidal reactions in about 1% of patients and should not be administered to patients who are concurrently being treated for Parkinson disease. Acute laryngeal dystonia (laryngospasm) is a rare extrapyramidal reaction to the butyrophenones. Droperidol is a cardiac antidysrhythmic and protects against epinephrine-induced dysrhythmias. Since droperidol was approved in 1970, there has not been a single case report where droperidol in doses used for the management of postoperative nausea and vomiting has been associated with cardiac dysrhythmias or cardiac arrest. Resting ventilation and the ventilatory response to carbon dioxide are not altered by droperidol. Neuroleptanalgesia is produced with a 50:1 combination of droperidol with fentanyl. This fixed combination of drugs is not associated with enhanced depression of ventilation as compared with either drug alone. Droperidol is a powerful antiemetic agent as a result of inhibition of dopamine2 receptors in the chemoreceptor trigger zone of the medulla. Cannabis has been used for thousands of years and is presently the most commonly used illicit drug in the world. Cannabinoids undergo substantial hepatic first-pass metabolism following oral administration such that only 10% to 20% of the ingested dose reaches the systemic circulation (produces large amounts of active metabolite, 11-hydroxy- -9-tetrahydrocannabinol). Acute intoxication may cause perceptual alterations, distortion of time, intensification of normal sensory experiences, decreased reaction times, poor motor skills, increased appetite, impairment of skilled activities, tachycardia, and hypotension. The greatest concern is the creation of long-term toxicity, development of physical dependence associated with withdrawal symptom during a period of abstinence after frequent use. Chronic inhalation of cannabis smoke is associated with an increased incidence of chronic obstructive lung disease and carcinoma of the lung and larynx. Although use of cannabis for analgesia introduces the potential for psychic and physical dependence, there is considerably less risk of life-threatening side effects compared to those associated with opioids. Methylphenidate is a psychostimulant used for the treatment of attention deficit hyperactivity disorder and narcolepsy. The risk of intraoperative hemodynamic instability and arrhythmias may be increased. Increased physiologic demands may place a significant burden on organ systems that have not yet developed normal adult functional reserve. Neonatal oxygen consumption is approximately 6 mL/kg/minute compared to 3 mL/kg/minute in the adult. Even under normal physiologic circumstances, the immature cardiac and respiratory systems operate near the edge of their functional reserve to support this metabolic demand. The newborn infant is in a state of transition from the fetal, intrauterine to the newborn, extrauterine circulatory pattern. Expansion of the lungs at birth increases Po2 and causes a rapid decline in pulmonary vascular resistance and an increase in pulmonary blood flow. Increasing blood return to the heart via the pulmonary veins raises the pressure of the left atrium above that of the right, causing a functional closure of the foramen ovale. Anatomic closure of the foramen ovale usually occurs between 3 months and 1 year of age, but the foramen remains anatomically patent in 10% to 30% of people throughout life (described as having a "probe patent" foramen ovale). Because the foramen ovale and ductus arteriosus are only functionally closed in the neonatal period, the neonatal circulation is able to readily revert to the fetal pattern, particularly in response to physiologic stresses (hypoxemia, hypercarbia, acidosis). Right-to-left shunting, by causing arterial hypoxemia, causes a further increase in pulmonary vascular resistance, thus creating a vicious cycle (persistent pulmonary hypertension may be seen in premature neonates). The neonatal myocardium contains immature contractile elements and is less compliant than the adult myocardium. Because stroke volume cannot be significantly augmented by volume loading, and because contractile reserve is limited, neonatal cardiac output is exquisitely dependent on heart rate. To meet the elevated metabolic demand, neonatal cardiac output, relative to body weight, is twice that Immature - 8. This is achieved with a relatively rapid heart rate (140 beats per minute) because stroke volume cannot be significantly increased.
Order furosemide us
The otic and submandibular ganglia are also derived from myelencephalic neural crest and may receive contributions from the glossopharyngeal and facial cranial nerves hypertension blood pressure readings generic furosemide 40mg on line, respectively. Neural crest from the region located between the otic placode and the caudal limit of somite 3 has been termed cardiac neural crest. Cells derived from these levels migrate through pharyngeal arches 3, 4 and 6, where they provide, among other things, support for the embryonic aortic arch arteries, cells of the aorticopulmonary septum and truncus arteriosus. Somites are indicated on the right, and vertebral levels are indicated on the left. Sensory innervation of the heart is from the inferior ganglion of the vagus, which is derived from the nodose placodes. Neural crest cells migrating from the level of somites 1 to 7 are collectively termed vagal neural crest; they migrate to the gut along with the sacral neural crest. ParasympatheticGanglia SympatheticGanglia Neural crest cells migrate ventrally within the body segments to penetrate the underlying somites and continue to the region of the future paravertebral and prevertebral plexuses, notably forming the sympathetic chain of ganglia as well as the major ganglia around the ventral visceral branches of the abdominal aorta. There is cell-specific recognition of postganglionic neurones and the growth cones of sympathetic preganglionic neurones. They meet during growth, and this may be important in terms of guidance to their appropriate target. The position of postganglionic neurones, and the exit point from the spinal cord of preganglionic neurones, may influence the types of synaptic connections made and the affinity for particular postganglionic neurones. When a postganglionic neuroblast is in place, it extends axons (and dendrites), and synaptogenesis occurs. The earliest axonal outgrowths from the superior cervical ganglion occur at about stage 14; although the axon is the first cell process to appear, the position of the neurones apparently does not influence the appearance of the cell processes. The local environment is the major factor that controls the appropriate differentiation of the presumptive autonomic ganglion neurones. The factors responsible for subsequent adrenergic, cholinergic or peptidergic phenotype have yet to be identified, although it has been proposed that fibronectin and basal lamina components initiate adrenergic phenotypical expression at the 45 Chapter 3 Section I / General expense of melanocyte numbers. Neuropeptides are expressed by autonomic neurones in vitro and may be stimulated by various target tissue factors in sympathetic and parasympathetic neurones. Some neuropeptides are expressed more intensely during early stages of ganglion formation. EntericNervousSystem the enteric nervous system is different from the other components of the autonomic nervous system because it can mediate reflex activity independently of control by the brain and spinal cord. The number of enteric neurones that develop is believed to be of the same magnitude as the number of neurones in the spinal cord. Preganglionic fibres that supply the intestine, and therefore modulate the enteric neurones, are much fewer. Premigratory neural crest cells are not prepatterned for specific axial levels; rather, they attain their axial value as they leave the neuraxis. Once within the gut wall, there is a regionally specific pattern of enteric ganglia formation that may be controlled by the local splanchnopleuric mesenchyme. Cranial neural crest from somite levels 1 to 7 contributes to the enteric nervous system, forming both neuroblasts and glial support cells. The most caudal derivatives of neural crest cells from the lumbosacral region, or somite 28 onward, form components of the pelvic plexus after migrating through the somites toward the level of the colon, rectum and cloaca. Initially the cells lie within the developing mesentery, then transiently between the layers of the differentiating muscularis externa, before finally forming a more substantial intramural plexus characteristic of the adult enteric nervous system. Of the neural crest cells that colonize the bowel, some in the foregut may acquire the ability to migrate outward and colonize the developing pancreas. The condition is characterized by a dilated segment of colon proximally and lack of peristalsis in the segment distal to the dilatation. Chromaffin cells are derived from the neural crest and found at numerous sites throughout the body. They are the classic chromaffin cells of the suprarenal medulla, bronchial neuroepithelial cells, dispersed epithelial endocrine cells of the gut (formerly known as argentaffin cells), carotid body cells and paraganglia. The sympathetic ganglia, suprarenal medulla and chromaffin cells are all derived from the cells of the sympathoadrenal lineage. In the suprarenal medulla these cells differentiate into a number of types consisting of small and intermediate-sized neuroblasts or sympathoblasts and larger, initially rounded phaeochromocytoblasts. Large cells with pale nuclei, thought to be the progenitors of chromaffin cells, can be detected from 9 weeks in human fetuses, and clusters of small neuroblasts are evident from 14 weeks. Intermediate-sized neuroblasts differentiate into the typical multipolar postganglionic sympathetic neurones (which secrete noradrenaline at their terminals) of classic autonomic neuroanatomy. The large cells differentiate into masses of columnar or polyhedral phaeochromocytes (classic chromaffin cells), which secrete either adrenaline (epinephrine) or noradrenaline (norepinephrine). These cell masses are termed paraganglia and may be situated near, on the surface of or embedded in the capsules of the ganglia of the sympathetic chain or in some of the large autonomic plexuses. The largest members of the latter are the para-aortic bodies, which lie along the sides of the abdominal aorta in relation to the inferior mesenteric artery. During childhood the para-aortic bodies and the paraganglia of the sympathetic chain partly degenerate and can no longer be isolated by gross dissection, but even in the adult, chromaffin tissue can still be recognized microscopically in these various sites. The neuroblasts of the lateral walls of the tube are large and initially round or oval (apolar). However, one process is withdrawn, and the neuroblast becomes unipolar, although this is not invariably so in the case of the spinal cord. Further differentiation leads to the development of dendritic processes, and the cells become typical multipolar neurones. In the developing cord they occur in small clusters, representing clones of neurones. Development of a longitudinal sulcus limitans on each side of the central canal of the cord divides the ventricular and intermediate zones in each lateral wall into a basal (ventrolateral) plate or lamina and an alar (dorsolateral) plate or lamina. Caudally the central canal of the cord ends as a fusiform dilatation, the terminal ventricle. The cells of the ventricular zone are closely packed at this stage and arranged in radial columns. Their disposition may be determined in part by contact guidance along the earliest radial array of glial fibres that cross the full thickness of the early neuroepithelium. This enlargement outlines the anterior (ventral) column of the grey matter and causes a ventral projection on each side of the median plane; the floor plate remains at the bottom of the shallow groove produced. As growth proceeds, these enlargements, which are further increased by development of the anterior funiculi (tracts of axons passing to and from the brain), encroach on the groove until it becomes converted into the slit-like anterior median fissure of the adult spinal cord. The axons of some of the neuroblasts in the anterior grey column cross the marginal zone and emerge as bundles of ventral spinal nerve rootlets on the anterolateral aspect of the spinal cord. These constitute, eventually, both the -efferents, which establish motor end-plates on extrafusal striated muscle fibres, and the -efferents, which innervate the contractile polar regions of the intrafusal muscle fibres of the muscle spindles. In the thoracic and upper lumbar regions, some intermediate zone neuroblasts in the dorsal part of the basal plate outline a lateral column. Their axons join the emerging ventral nerve roots and pass as preganglionic fibres to the ganglia of the sympathetic trunk or related ganglia, the majority eventually myelinating to form white rami communicantes. The axons within the rami synapse on the autonomic ganglionic neurones, and axons of some of the latter pass as postganglionic fibres to innervate smooth muscle cells, adipose tissue or glandular cells. Other preganglionic sympathetic efferent axons pass to the cells of the suprarenal medulla. It gives origin to the preganglionic parasympathetic fibres that run in the pelvic splanchnic nerves. The anterior region of each basal plate initially forms a continuous column of cells throughout the length of the developing cord. This soon develops into two columns (on each side): one is medially placed and concerned with innervation of axial musculature, and the other is laterally placed and innervates the limbs. At limb levels the lateral column enlarges enormously, but it regresses at other levels. Axons arising from ventral horn neurones-that is, -, - and -efferent fibres-are accompanied at thoracic, upper lumbar and midsacral levels by preganglionic autonomic efferents from neuroblasts of the developing lateral horn. Numerous interneurones develop in these sites (including Renshaw cells); it is uncertain how many of these differentiate directly from ventrolateral lamina (basal plate) neuroblasts and how many migrate to their final positions from the dorsolateral lamina (alar plate). In the human embryo, the definitive grouping of ventral column cells, which characterizes the mature cord, occurs early; by the fourteenth week (80 mm), all the major groups can be recognized. The layer becomes less thick until it ultimately forms the single-layered ependyma that lines the ventral part of the central canal of the spinal cord. It occasionally gives rise to congenital cysts in the neighbourhood of the coccyx. In the definitive state, the upper cervical spinal nerves retain their position at roughly right angles to the cord.
Diseases
- Young Mc keever Squier syndrome
- Glucocorticoid sensitive hypertension
- Aspergillosis
- Irritable bowel syndrome
- Glaucoma sleep apnea
- Epiphysealis hemimelica dysplasia
- Cervical hypertrichosis neuropathy
40 mg furosemide otc
A triglyceride molecule to which one of the terminal fatty acids is replaced with a phosphate ion is known as a phospholipid heart attack nursing diagnosis buy furosemide toronto. Triglycerides, after absorption from the gastrointestinal tract, are transported in the lymph and then, by way of the thoracic duct, into the circulation in droplets known as chylomicrons. Triglycerides are used in the body mainly to provide energy for metabolic processes similar to those fueled by carbohydrates. An intrinsic feedback control system increases the endogenous production of cholesterol when exogenous intake is decreased, explaining the relatively modest lowering effect on plasma cholesterol concentrations produced by low-cholesterol diets. Amino acids are relatively strong acids and exist in the blood principally in the ionized form. Immediately after entry into cells, amino acids are conjugated under the influence of intracellular enzymes into cellular proteins. These proteins can be rapidly decomposed again into amino acids under the influence of intracellular liposomal digestive enzymes. This response is especially apparent in relation to protein synthesis in cancer cells. Plasma proteins are represented by (a) albumin, which provides colloid osmotic pressure; (b) globulins necessary for innate and acquired immunity; and (c) fibrinogen, which polymerizes into long fibrin threads during coagulation of blood. Essentially, all plasma albumin and fibrinogen and 60% to 80% of the globulins are formed in the liver. Within hours, amino acids of the administered protein become distributed throughout cells of the body to form proteins where they are needed. Albumin is the most abundant plasma protein and is principally responsible for maintaining plasma osmotic pressure. In addition, albumin is important as a transporter of plasma-bound substances often including exogenously administered drugs. Normal daily synthesis of albumin is about 10 g and the half-time for this protein may be as long as 22 days (serum albumin concentrations may not be noticeably decreased in early states of acute hepatic failure). Despite the fact that low serum albumin is a poor prognostic factor in critical illness, supplementation has not been shown to improve prognosis. Once cells contain a maximum amount of amino acids, any additional amino acids are deaminated (oxidative deamination) to keto acids that can enter the citric acid cycle. The conversion of amino acids to glucose or glycogen is gluconeogenesis, and the conversion of amino acids into fatty acids is ketogenesis. Conversely, administration of glucose in the presence of starvation decreases gluconeogenesis and lipolysis. The ability to conserve energy in the form of adipose tissue would at one time have conferred a survival advantage. Today, the combination of easy access to calorically dense foods and a sedentary lifestyle has made the metabolic consequences of these presumed genes maladaptive. In addition, certain medications are commonly associated with weight gain (Table 33-5). Increased waist circumference (102 cm in adult males and 88 cm in adult females) is associated with an increased risk for ischemic heart disease, diabetes mellitus, and systemic hypertension. Treatment of obesity by decreasing caloric intake and increasing metabolic rate (exercise) directed toward a long-term decrease in body weight is largely ineffective. Both proteins and carbohydrates can be metabolically converted to fat, and there is no evidence that changing the relative proportions of protein, carbohydrate, and fat in the diet without decreasing caloric intake will promote weight loss. Orlistat inhibits lipases in the gastrointestinal lumen, thus antagonizing triglyceride hydrolysis and decreasing fat absorption by about 30% (weight loss with orlistat is modest, an average of 2. The sequence of events that occur during emesis are controlled by the vomiting center, which lies in the medulla oblongata. Agonists and antagonists of these neurotransmitters are used to prevent nausea and vomiting. Antiemetic agents should be used for the prevention and treatment of nausea and vomiting when indicated but not routinely. Transdermal application of a scopolamine patch has been shown to exert significant antiemetic effects in patients treated with patient-controlled analgesia or epidural morphine for the management of postoperative pain. Scopolamine and atropine can enter the central nervous system and produce symptoms characterized as the central anticholinergic syndrome. The central anticholinergic syndrome is often mistaken for delayed recovery from anesthesia or confusion. Deliberate or accidental overdose with an anticholinergic drug produces a rapid onset of symptoms characteristic of muscarinic cholinergic receptor blockade (dry mouth, swallowing and talking is difficult, vision is blurred, photophobia is present, and tachycardia is prominent). Small children are particularly vulnerable to drug-induced increases in body temperature (atropine fever). Benzamides: Metoclopramide stimulates the gastrointestinal tract via cholinergic mechanism that results in increased gastric and small intestinal motility. Corticosteroids: Dexamethasone has efficacy similar to ondansetron and droperidol and with a minimal side effect profile associated with one-time use. Obese and diabetic patients are at increased risk for perioperative hyperglycemia when they receive a single dose of dexamethasone. As a result, ondansetron is free of neurologic side effects common to droperidol and metoclopramide. The most significant feature of ondansetron prophylaxis and treatment is the relative freedom from side effects. This drug is also effective in the treatment of symptoms related to carcinoid syndrome and may also possess gastrokinetic properties. Aspiration during general anesthesia occurs in approximately 1 in 8,500 adults and 1 in 4,400 children younger than 16 years of age (increased risk for emergency operations, especially bowel obstruction). Factors associated with pulmonary complications of aspiration include the volume and acidity of the aspirated gastric contents. Drugs that increase the pH of gastric contents (antacids) and that decrease the volume of gastric contents (prokinetic drugs) have a role in decreasing the severity of the sequelae of aspirating gastric contents. Enforcement of the American Society of Anesthesiologist Task Force Fasting Recommendations can also reduce the risk of pulmonary aspiration. Antacids are drugs that neutralize (remove hydrogen ions) acid from gastric contents or decrease the secretion of hydrogen chloride into the stomach. Occasional failure of particulate antacids to increase gastric fluid pH may reflect inadequate mixing with stomach contents or an unusually large volume of gastric fluid. Pneumonitis associated with functional and histologic changes in the lungs may reflect a foreign body reaction to inhaled particulate antacid particles. Nonparticulate (clear) antacids (sodium citrate) are less likely to cause a foreign body reaction if aspirated, and their mixing with gastric fluid is more complete than is that of particulate antacids. The onset of effect is more rapid with sodium citrate than with particulate antacids that require a longer time for adequate mixing with gastric fluid. Histamine receptor antagonists bind to receptors on effector cell membranes, to the exclusion of agonist molecules, without themselves activating the receptor (histamine receptor antagonists do not inhibit release of histamine). H1-receptor antagonists are characterized as first-generation and second-generation receptor antagonists. First-generation drugs tend to produce sedation, whereas second-generation drugs are relatively nonsedating (Table 35-2). H1-receptor antagonists are well absorbed after oral administration, often reaching peak plasma concentrations within 2 hours (Table 35-3). H1-receptor antagonists prevent and relieve the symptoms of allergic rhinoconjunctivitis (sneezing, nasal and ocular itching, rhinorrhea, tearing, and conjunctival erythema) but they are less effective for the nasal congestion characteristic of a delayed allergic reaction. First-generation H1-receptor antagonists have sedating effects that result in delayed reaction times. Use of antihistamines in the acute treatment of anaphylactic reactions is directed at blocking further histamine-mediated vasodilation and resulting hemodynamic instability, as well as decreasing respiratory and other systemic complications. The histamine receptors on the basolateral membranes of acid-secreting gastric parietal cells are of the H2 type and thus are not blocked by conventional H1 antagonists. The relative potencies of the four H2-receptor antagonists for inhibition of secretion of gastric hydrogen ions varies from 20- to 50-fold, with cimetidine as the least potent and famotidine the most potent (see Table 35-3). The duration of inhibition ranges from approximately 6 hours for cimetidine to 10 hours for ranitidine, famotidine, and nizatidine.
Furosemide 40mg discount
The nucleus of Onuf blood pressure medication muscle weakness purchase genuine furosemide on-line, which is thought to innervate the perineal striated muscles, is a ventrolateral group of cells in the first and second sacral segments. The basic arrangement is that medial cell groups innervate the axial musculature, and lateral cell groups innervate the limbs. The basic building block of the somatic motor neuronal populations is represented by a longitudinally disposed group of neurones that innervate a given muscle and in which the and motor neurones are intermixed. The various groups innervating different muscles are aggregated into two major longitudinal columns: medial and lateral. The medial longitudinal motor column extends throughout the length of the spinal cord. Basically, epaxial muscles include the erector spinae group (which extend the head and vertebral column), and hypaxial muscles include prevertebral muscles of the neck, intercostal and anterior abdominal wall muscles (which flex the neck and the trunk). The epaxial muscles are innervated by branches of the dorsal primary rami of the spinal nerves, and the hypaxial muscles are innervated by branches of the ventral primary rami. In the medial column, motor neurones supplying epaxial muscles are sited ventral to those supplying hypaxial muscles. The lateral longitudinal motor column is found only in the enlargements of the spinal cord. The motor neurones in this column in the cervical and lumbar enlargements innervate muscles of the upper and lower limbs, respectively. In the cervical enlargement, motor neurones that supply muscles intrinsic to the upper limb are situated dorsally in the ventral grey column, and those innervating the most distal (hand) muscles are located farther dorsally. Motor neurones of the girdle muscles lie in the ventrolateral part of the ventral horn. There is a further somatotopic organization, in that the proximal muscles of the limb are supplied from motor cell groups located more rostrally in the enlargement than those supplying the distal muscles. For example, motor neurones innervating intrinsic muscles of the hand are sited in segments C8 and T1, whereas motor neurones of shoulder muscles are in segments C5 and C6. A similar overall arrangement of motor neurones innervating lower limb muscles applies in the lumbosacral cord. The main afferent connections to motor neurones are direct monosynaptic connections from proprioceptive dorsal root afferents in the same or nearby segments, connections from axonal collaterals of dorsal horn and other interneurones and direct monosynaptic connections from the vestibulospinal and corticospinal tracts. The intrinsic connections of the spinal cord and brain stem subserve a number of reflexes by which the functions of peripheral structures are modulated in response to afferent information in a relatively automatic or autonomous fashion. However, in all but the simplest of reflexes, interneurones intervene between the afferent and efferent components and confer the capacity to increase the versatility and complexity of reflex responses. Nevertheless, they are strongly influenced and modulated by descending connections. In the case of spinal reflexes, these descending controls come from both the brain stem and the cerebral cortex. Relative positions of these columnar groups, as well as their extension through varying series of spinal segments, are indicated. Stretch reflex - the stretch reflex is the mechanism by which stretch applied to a muscle elicits its reflex contraction. It is essential for the maintenance of both muscle tone and an upright stance (via innervation of the postural muscles of the neck, back and lower limbs). Anatomically, it is the simplest of reflexes-it consists of one afferent and one efferent neurone. The left side of the figure shows the subdivision of the lateral and medial longitudinal motor columns; the right side depicts these in more detail. Descending motor pathways and the spinal motor system: limbic and non-limbic components. Posterior iliopsoas transplantation in the treatment of paralytic dislocation of the hip. The motor neurones of antagonistic muscles are simultaneously inhibited via collateral connections to inhibitory interneurones. Gamma reflex - In addition to motor neurones innervating extrafusal muscle fibres, muscles receive motor neurones that innervate intrafusal muscle fibres. Activation of motor neurones increases the sensitivity of the intrafusal fibres to stretch. Therefore, changes in activity have a profound effect on the stretch reflex and on muscle tone. Like motor neurones, motor neurones are under the influence of descending pathways from the brain stem and cerebral cortex. Changes in the activity of the stretch reflex 132 Chapter 8 / Spinal Cord and Nerve Roots A 1a afferent Intrafusal muscle fibre Quadriceps muscle Lumbar cord Interneurone Patellar tendon Alpha motor neurone Cutaneous afferent neurone B Quadriceps muscle Alpha motor neurones Knee flexor muscles Knee flexor muscles Inhibitory interneurone. Flexor reflex - Painful stimulation of the limbs leads to reflex flexion withdrawal mediated by a polysynaptic reflex in which interneurones are interposed between afferent and efferent elements. Thus, activation of nociceptive primary afferents indirectly causes activation of limb flexor motor neurones. Collateralization of fibres to nearby spinal segments mediates flexion of a limb at several joints, depending on the intensity of the stimulus. In principle, virtually any cutaneous stimulus has the potential to induce a flexor reflex, but with the exception of noxious stimuli, this response is normally inhibited by descending pathways. When descending influences are lost, even harmless cutaneous stimulation can elicit flexion of the limbs. The Babinski (extensor plantar) reflex, which is generally regarded as pathognomonic of damage to the corticospinal tract, at least in adults, is part of a flexion withdrawal of the lower limb in response to stimulation of the sole of the foot. Fibres of related function and those with common origins or destinations are grouped to form ascending and descending tracts within the funiculi. Narrow dorsal and ventral white commissures run between the two halves of the cord. Here, the tracts are considered under three main headings: ascending, descending and propriospinal. Ascending tracts contain primary afferent fibres, which enter by dorsal roots, and fibres derived from intrinsic spinal neurones, which carry afferent impulses to supraspinal levels. Descending tracts contain long fibres, which descend from various supraspinal sources to synapse with spinal neurones. Propriospinal tracts, both ascending and descending, contain the axons of neurones that are localized entirely to the spinal cord and link nearby and distant spinal segments. Most regions contain a wide spectrum of fibre diameters, from 1 mm or less to 10 mm. Some tracts, including the dorsolateral tract, fasciculus gracilis and central part of the lateral funiculus, typically contain only small fibres. The fasciculus cuneatus, anterior funiculus and peripheral zone of the lateral funiculus contain many large-diameter fibres. Although the ascending and descending tracts are to a large extent discrete and regularly located, significant overlap between adjacent tracts occurs. The following account of spinal tracts is concerned with the human cord; findings in animals are discussed only when adequate clinicopathological data are unavailable in humans. Dorsal columns - the dorsal funiculus on each side of the cord consists of two large ascending tracts-the fasciculus gracilis and fasciculus cuneatus. The dorsal columns contain a high proportion of myelinated fibres carrying proprioception (position sense and kinaesthesia) and exteroceptive (touch-pressure) information, including vibratory sensation, to higher levels. These fibres come from several sources: long primary afferent Ascending Tracts Spinal White Matter the spinal white matter surrounds the central core of grey matter. Examination demonstrates weakness distally in both lower extremities, with spasticity and a spastic gait. Sensory examination demonstrates striking impairment of vibratory sense and proprioception in both feet, with mild shading impairment of pain appreciation distally in the legs. Discussion: Weakness, spasticity and hyperreflexia in the legs suggest involvement of the corticospinal tracts within the spinal cord. Impaired vibratory and position sense indicates involvement of the posterior columns, with relative sparing of the spinothalamic sensory pathways. This is a typical clinical presentation of subacute combined degeneration of the cord due to vitamin B12 deficiency, documented with appropriate testing.

Discount furosemide 100mg amex
Causes of iron-deficiency anemia include inadequate dietary intake of iron blood pressure normal child discount furosemide 100 mg free shipping, increased iron requirements due to pregnancy or blood loss, or interference with absorption from the gastrointestinal tract. Partial gastrectomy, malabsorptive bariatric surgery, and sprue are causes of inadequate iron absorption. Iron deficiency initially results in a decrease in iron stores and a parallel decrease in the erythrocyte content of iron. Plasma ferritin concentrations of less than 12 g/dL are diagnostic of iron deficiency. Prophylactic use of iron preparations should be reserved for individuals at high risk for developing iron deficiency (pregnant and lactating females, lowbirth-weight infants, females with heavy menses). In iron-deficiency anemia, administration of medicinal iron increases the rate of erythrocyte production resulting in a rise in hemoglobin concentration within 72 hours. There is no justification for continuing iron therapy beyond 3 weeks if a favorable response has not occurred. Ferrous sulfate administered orally is the most frequent choice for the treatment of irondeficiency anemia and is available as syrup, pills, or tablets. Parenteral iron acts similarly to oral iron but should be used only if patients cannot tolerate or do not respond to oral therapy. Copper is present is a constituent of enzymes and is an essential component of several proteins. Zinc is an enzymatic cofactor essential for cell growth and the synthesis of nucleic acid, carbohydrates, and proteins. Epinephrine is a circulating hormone synthesized, stored, and released from the adrenal medulla. Its natural functions upon release into the circulation include regulation of myocardial contractility, heart rate, vascular and bronchial smooth muscle tone, glandular secretions, and metabolic processes such as glycogenolysis and lipolysis. It is a potent activator of -adrenergic receptors and also activates 1 and 2 receptors. Epinephrine is poorly lipid soluble, preventing its ready entrance into the central nervous system and accounting for the lack of cerebral effects. Clinical uses of epinephrine include treatment of life-threatening allergic reactions/anaphylaxis, treatment of severe asthma and bronchospasm, administration during cardiopulmonary resuscitation as a vital therapeutic drug, administration during periods of hemodynamic instability to promote myocardial contractility and increase vascular resistance, and continuous infusion for continuous support of myocardial contractility and vascular resistance. Epinephrine is added to local anesthetic solutions to decrease systemic absorption prolonging the duration of action of the anesthetic for regional and local anesthesia. The cardiovascular effects of epinephrine result from stimulation of - and adrenergic receptors (see Table 18-1). Smooth muscles of the bronchi are relaxed by epinephrine-induced activation of 2 receptors. The bronchodilating effects of epinephrine are not seen in the presence of -adrenergic blockade. Epinephrine has the most significant effect on metabolism of all the catecholamines. Release of endogenous epinephrine and the resulting glycogenolysis and inhibition of insulin secretion is the most likely explanation for perioperative hyperglycemia. Selective 2-adrenergic agonist effects of epinephrine are speculated to reflect activation of the sodiumpotassium pump in skeletal muscles, leading to a transfer of potassium ions into cells. The observation that serum potassium measurements in blood samples obtained immediately before induction of anesthesia are lower than measurements 1 to 3 days preoperatively is presumed to reflect stress-induced release of epinephrine. In making therapeutic decisions based on a preinduction serum potassium measurement, especially in patients without a reason to experience hypokalemia, one should consider the possible role of preoperative anxiety and the release of epinephrine. Epinephrine causes contraction of the radial muscles of the iris, producing mydriasis. Epinephrine, norepinephrine, and isoproterenol produce relaxation of gastrointestinal smooth muscle. Activation of -adrenergic receptors relaxes the detrusor muscle of the bladder, whereas activation of -adrenergic receptors contracts the trigone and sphincter muscles. Hepatosplanchnic vasoconstriction occurs as well as impaired renal blood flow as cardiac output is diverted to the dilated skeletal muscle vasculature. Norepinephrine is the endogenous neurotransmitter synthesized and stored in postganglionic sympathetic nerve endings and released with sympathetic nerve stimulation. A continuous infusion of norepinephrine, 2 to 16 g per minute, may be used to treat refractory hypotension. The primary utility of norepinephrine is as a potent vasoconstrictor to increase total peripheral vascular resistance and mean arterial pressure. It is a first-line agent in the treatment of refractory hypotension during severe sepsis. Norepinephrine-induced vasoconstriction and redistribution of flow may increase splanchnic blood flow and urine output in severely hypotensive septic patients. Excessive vasoconstriction and decreased perfusion of renal, splanchnic, and peripheral vascular beds may lead to end-organ hypoperfusion and ischemia. Dopamine is an endogenous catecholamine that regulates cardiac, vascular, and endocrine function and is an important neurotransmitter in the central and peripheral nervous systems. Dopamine receptors may also be associated with the neural mechanism for "reward" that is associated with cocaine and alcohol dependence. Traditionally, the pharmacokinetics of dopamine has been attributed to dose-dependent effects on varying receptors (too simplistic as even in healthy individuals there are a wide range of clinical responses depending on individual variability in pharmacokinetics). The effects of dopamine cannot be predicted based on the dose, and the drug must be titrated to effect. Dopamine increases cardiac output by stimulation of 1 receptors, increasing stroke volume (less dysrhythmogenic than epinephrine). Rapid metabolism of dopamine with an elimination half-life of 1 to 2 minutes mandates its use as a continuous infusion (1 to 20 g/kg/ minute) to maintain therapeutic plasma concentrations. The divergent pharmacologic effects of dopamine and dobutamine make their use in combination potentially useful (infusions of dopamine and dobutamine produce a greater improvement in cardiac output, at lower doses, than can be achieved by either drug alone). The objective of combination therapy is to increase coronary perfusion and cardiac output while decreasing afterload, similar to an intraaortic balloon pump. The term renal-dose dopamine or low-dose dopamine refers to the continuous infusion of small doses (1 to 3 g/kg/minute) of dopamine to patients to promote renal blood flow. In healthy individuals, low-dose dopamine increases renal blood flow and induces natriuresis and diuresis. In the absence of data confirming the efficacy of dopamine in preventing acute renal failure, renal-dose dopamine cannot be recommended. Dopamine is associated more than dobutamine or epinephrine with dose-related sinus tachycardia and the potential to cause ventricular arrhythmias and may predispose to myocardial ischemia by precipitating tachycardia, increasing contractility, increasing afterload, and precipitating coronary artery vasospasm. There is no evidence that low-dose dopamine has beneficial effects on splanchnic function or reduces the progression to multiorgan failure in sepsis. Dopamine disrupts metabolic and immunologic functions through its effects on hormones and lymphocyte function. In the acute phase of an illness, dopamine induces the pattern of hypopituitarism seen in prolonged critical illness and chronic stress. The infusion of low-dose dopamine interferes with the ventilatory response to arterial hypoxemia and hypercapnia, reflecting the role of dopamine as an inhibitory neurotransmitter at the carotid bodies (result is depression of ventilation in patients who are being treated with dopamine to increase myocardial contractility). Isoproterenol is the most potent activator of all the sympathomimetics with 1 and 2 receptor activity (two to three times more potent than epinephrine and at least 100 times more active than norepinephrine, devoid of agonist effects). The cardiovascular effects of isoproterenol reflect activation of 1 receptors in the heart and 2 receptors in skeletal muscle. Although cardiac output may increase thereby increasing systolic blood pressure, the mean arterial pressure may decrease due to decreases in systemic vascular resistance and associated decreases in diastolic blood pressure. Compensatory baroreceptor-mediated reflex slowing of the heart rate does not occur during infusion of isoproterenol because mean arterial pressure is not increased. Metabolism of isoproterenol in the liver by catechol-O-methyltransferase is rapid, necessitating a continuous infusion to maintain therapeutic plasma concentrations. A continuous infusion of isoproterenol, 1 to 5 g per minute, is effective in increasing the heart rate in adults in the presence of heart block. Isoproterenol is used to provide sustained increases in heart rate before insertion of a temporary or permanent cardiac pacemaker. The combination of decreased diastolic blood pressure and increased heart rate and dysrhythmias may lead to myocardial ischemia.
Order cheap furosemide
Typically blood pressure medication and weight loss discount furosemide 40 mg without a prescription, there is narrowing of the intervertebral disc space at the involved segment. Nucleus pulposus Anulus fibrosus Posterior longitudinal ligament Herniation of nucleus pulposus Cauda equina Compressed spinal nerve root Cauda equina Defect in anulus fibrosus Herniation of nucleus pulposus Nucleus pulposus Annulus fibrosus. They are most common on the anterior aspect of the body and never involve the ring epiphysis. Osteophytic spurs are frequently asymptomatic but may result in diminished movements within the spine. A comprehensive and detailed source of information on the functional anatomy, tissue biology and biomechanics of the lumbar spine. Sagittal plane segmental motion of the cervical spine: a new precision measurement protocol and normal motion data of healthy adults. Functional anatomy of the lumbar spine, described as a basis for the clinical management of low back pain. Review of the morphological, developmental and topographical aspects of the spinal epidural space. Three-dimensional analysis of active cervical motion: the effect of age and gender. Through them it receives primary afferent fibres from peripheral receptors located in widespread somatic and visceral structures. It also sends motor axons to skeletal muscle and provides autonomic innervation of cardiac and smooth muscle and secretory glands. They allow higher centres to monitor and perceive external and internal stimuli and modulate and control spinal efferent activity. It gives rise to 31 pairs of segmentally arranged spinal nerves, which are attached to the cord by a linear series of dorsal and ventral rootlets. Dorsal rootlets contain afferent nerve fibres, and ventral rootlets contain efferent fibres. These cross the subarachnoid space and unite to form functionally mixed spinal nerves as they pass through the intervertebral foramina. The dorsal roots bear dorsal root ganglia, which contain the cell bodies of primary afferent neurones. The spinal cord, its blood vessels and nerve roots lie within a meningeal sheath, the theca, which occupies the central zone of the vertebral canal and extends from the foramen magnum, where it is in continuity with the meningeal coverings of the brain, to the level of the second sacral vertebra in the adult. Distal to this level the dura extends as a fine cord, the filum terminale externum, which fuses with the posterior periosteum of the first coccygeal segment. Between the theca and the walls of the vertebral canal is the epidural (spinal extradural) space (Ch. Three-dimensional appreciation of the anatomy of the spinal theca and its surroundings is essential for the efficient management of spinal pain, spinal injuries, tumours and infections. Equally significant clinically is the anatomy of the often precarious blood supply of the spinal cord and its associated structures. The increasing application and refinement of diagnostic imaging and endoscopic procedures lend new importance to topographical detail here. Its average length in European males is 45 cm; its weight is approximately 30 g (for dimensional data, consult Barson and Sands 1977). It extends from the upper border of the atlas to the junction between the first and second lumbar vertebrae; this lower level varies, and there is some correlation with the length of the trunk, especially in females. The termination may be as high as the caudal third of the twelfth thoracic vertebra or as low as the disc between the second and third lumbar vertebrae, and its position rises slightly in vertebral flexion. The spinal cord is enclosed in the dura, arachnoid and pia mater, separated from each other by the subdural and subarachnoid spaces, respectively. The cord is continuous cranially with the medulla oblongata and narrows caudally to the conus medullaris, from whose apex a connective tissue filament, the filum terminale, descends to the dorsum of the first coccygeal vertebral segment. The spinal cord varies in transverse width, gradually tapering craniocaudally, except at the levels of the cervical and lumbosacral enlargements. It is not cylindrical, being wider transversely at all levels, especially in the cervical segments. The cervical enlargement is the source of the spinal nerves that supply the upper limbs. It extends from the third cervical to the second thoracic segments; its maximal circumference (approximately 38 mm) is in the sixth cervical segment. The greatest circumference (apprpoximately 35 mm) is near the lower part of the body of the twelfth thoracic vertebra, below which it rapidly dwindles into the conus medullaris. An anterior median fissure and a posterior median sulcus and septum almost completely separate the cord into right and left halves, but they are joined by a commissural band of nervous tissue that contains a central canal. The anterior median fissure extends along the whole ventral surface with an average depth of 3 mm, although it is deeper at caudal levels. Perforating branches of the spinal vessels pass from the fissure to the commissure to supply the central spinal region. The posterior median sulcus is shallower, and from it a posterior median septum of neuroglia penetrates more than halfway into the cord, almost to the central canal. The septum varies in anteroposterior extent from 4 to 6 mm, and it diminishes caudally as the canal becomes more dorsally placed and the cord contracts. Dorsal roots (strictly rootlets) of spinal nerves enter the cord along this sulcus. The white substance between the posterior median and posterolateral sulcus on each side is the posterior funiculus. In cervical and upper thoracic segments, a longitudinal posterointermediate sulcus marks a septum dividing each posterior funiculus into two large tracts: the fasciculus gracilis (medial) and the fasciculus cuneatus (lateral). Between the posterolateral sulcus and anterior median fissure is the anterolateral funiculus. This is subdivided into anterior and lateral funiculi by ventral spinal roots that pass through its substance to issue from the surface of the cord. The anterior funiculus is medial to , and includes, the emerging ventral roots; the lateral funiculus lies between the roots and the posterolateral sulcus. The filum terminale, a filament of connective tissue approximately 20 cm long, descends from the apex of the conus medullaris. Its upper 15 cm, the filum terminale internum, is continued within extensions of the dural and arachnoid meninges and reaches the caudal border of the second sacral vertebra. Its final 5 cm, the filum terminale externum, fuses with the investing dura mater and then descends to the dorsum of the first coccygeal vertebral segment. A few strands of nerve fibres, which probably represent roots of rudimentary second and third coccygeal spinal nerves, adhere to its upper part. A capacious part of the subarachnoid space surrounds the filum terminale internum and is the usual access site for lumbar puncture. They cross the subarachnoid space and traverse the dura mater separately, uniting in or close to their intervertebral foramina to form the (mixed) spinal nerves. The section has opened up the subarachnoid space as far as the first sacral vertebra. Note the difference in levels between the inferior limits of the spinal cord and meninges. Note that there are two inaccuracies in this figure: the epidural space is not shown, and the fibres of interspinous ligaments should slope dorsocranially. Lumbar enlargement than the vertebral column, the more caudal spinal roots descend for varying distances around and beyond the cord to reach their corresponding foramina. In so doing they form, mostly distal to the apex of the cord, a divergent sheaf of spinal nerve roots, the cauda equina, which is gathered around the filum terminale in the spinal theca. Ventral spinal roots contain efferent somatic and, at some levels, efferent sympathetic nerve fibres that emerge from their spinal sources. The rootlets constituting each ventral root emerge from the anterolateral sulcus over an elongated vertical elliptical area. Dorsal spinal roots bear ovoid swellings, the spinal ganglia, one on each root proximal to its junction with the corresponding ventral root in an intervertebral foramen. Each root fans out into six to eight rootlets before entering the cord in a vertical row in the posterolateral sulcus. Dorsal roots are usually said to contain only afferent axons (both somatic and visceral) from unipolar neurones in spinal root ganglia, but they may also contain a small number (3%) of efferent fibres and autonomic vasodilator fibres.
Smooth Alder. Furosemide.
- Sore throat and bleeding of the intestines.
- What is Smooth Alder?
- Dosing considerations for Smooth Alder.
- Are there safety concerns?
- How does Smooth Alder work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96997
Purchase furosemide 40 mg without a prescription
In infants blood pressure numbers for seniors buy furosemide 40mg online, the fossa is a relatively large blind tunnel under the anterior semicircular canal. The squamous part of the occipital bone displays a median internal occipital crest, which runs posteriorly from the foramen magnum to an internal occipital protuberance and gives attachment to the falx cerebelli. The internal occipital protuberance is close to the confluence of the sinuses and is grooved bilaterally by the transverse sinuses. The latter curve laterally, with an upward convexity, to the mastoid angles of the parietal bones. The groove for the transverse sinus is usually deeper on the right, where it is generally a continuation of the superior sagittal sinus; on the left, it is frequently a continuation of the straight sinus. Below the transverse sulcus, the internal occipital crest separates two shallow fossae, adapted to the cerebellar hemispheres. The margins of the grooves for the transverse sinus and superior petrosal sinus, together with the posterior clinoid process, all provide anchorage for the attached margin of the tentorium cerebelli. Neuro-ophthalmological examination shows 20/25 vision bilaterally, bitemporal visual field defects, normalappearing optic discs, intact pupillary function and normal extraocular motility. Discussion: Bitemporal hemianopsia localizes the lesion to the optic chiasma, with involvement primarily of the decussating fibres originating in the nasal portion of the retina. Tumours in this area can compress both the optic nerves and optic chiasma, sometimes producing a mixed defect consisting of bitemporal visual field disturbances (as in this woman) and a superimposed monocular visual field disturbance-a so-called junctional defect. Such a combination of monocular and bitemporal visual field defects can be diagnostically challenging. As this case demonstrates, patients with bitemporal visual field defects may be unaware of the vision loss. Posterior Cranial Fossa the posterior cranial fossa is the largest and deepest of the cranial fossae. It is bounded in front by the dorsum sellae, posterior aspects of the sphenoidal body and basilar part of occipital bone; behind by the squamous part of the occipital bone; laterally by the petrous and mastoid parts of the temporal bone and by the lateral parts of the occipital bone; and above and behind by the mastoid angles of the parietal bones. The region corresponds extracranially with the posterior part of the cranial base. The most prominent feature in the floor of the posterior cranial fossa is the foramen magnum in the occipital bone. A sloping surface called the clivus-formed successively by the basilar part of the occipital bone, the posterior part of the body and the dorsum sellae of the sphenoid bone-lies anterior to the foramen magnum. On each side it is separated from the petrous part of the temporal bone by a petro-occipital fissure, filled by a thin plate of cartilage and limited behind by the jugular foramen. A large jugular foramen, sited at the posterior end of the petro-occipital fissure, lies above and lateral to the foramen magnum. The ontogeny of cranial base angulation in humans and chimpanzees and its implications for reconstructing pharyngeal dimensions. It is sited in the posterior cranial fossa, and its ventral surface lies on the clivus. It contains numerous intrinsic neurone cell bodies and their processes, some of which are the brain stem homologues of spinal neuronal groups. These include the sites of termination and cells of origin of axons that enter or leave the brain stem through the cranial nerves. They provide the sensory, motor and autonomic innervation of structures that are mostly in the head and neck. Additional groups of neurones receive input related to the special senses of hearing, vestibular function and taste (Ch. The reticular formation is an extensive and often ill-defined network of neurones that extends throughout the length of the brain stem and is continuous caudally with its spinal counterpart. Some of its nuclei are concerned with cardiac, respiratory and alimentary control; some are involved in aspects of many neural activities, and others provide or receive massive afferent and efferent cerebellar projections. The brain stem is the site of termination of numerous ascending and descending fibres and is traversed by many others. Prominent corticospinal projections descend through the brain stem, and corticobulbar projections end within it. This is because it is a structurally and functionally compact region, where even small lesions can destroy vital cardiac and respiratory centres, disconnect forebrain motor areas from brain stem and spinal motor neurones and sever incoming sensory fibres from higher centres of consciousness, perception and cognition. Irreversible cardiac and respiratory arrest follows complete destruction of the neural respiratory and cardiac centres in the medulla. This chapter starts with a brief systematic overview of the cranial nerves that attach to the brain stem, their central origins and their connections within the cranial nerve nuclei. Many structures, including nuclei and tracts, extend longitudinally across their boundaries. The structure and function of the most notable of these are discussed in detail at the most appropriate point in the text. As is customary, transverse sections of the brain stem are included to illustrate the relationships between structures and the regional variation that occurs at different levels. The nuclei are either the origin of efferent cranial nerve fibres or the site of termination of cranial nerve afferents. For convenience, they are considered to be organized into six discontinuous, longitudinal cell columns that correspond to the columns that can be identified in the embryo. The trigeminal sensory nucleus, which extends throughout the length of the brain stem and into the cervical spinal cord, represents a general somatic afferent cell column. General visceral afferents carried by the facial, glossopharyngeal and vagus nerves end in the nucleus solitarius of the medulla. The special visceral afferent column corresponds to the vestibular and cochlear nuclei, which are located beneath the vestibular area of the floor of the fourth ventricle. The general somatic efferent cell column consists of four nuclei that lie near the midline and give rise to motor fibres that run in nerves of the same name. From rostral to caudal, these are the oculomotor, trochlear and abducens nuclei, which innervate the extraocular muscles, and the hypoglossal nucleus, which innervates all but one of the muscles of the tongue. Cells in the special visceral efferent column innervate muscles derived from the branchial arches and lie in the trigeminal motor nucleus, facial nucleus and nucleus ambiguus. All but 2 of the 12 pairs of cranial nerves attach to the brain stem; this chapter is therefore an appropriate place to describe their structure and function. The cranial nerves are individually named and numbered (using roman numerals) in a rostrocaudal sequence (see Table 1. Cranial nerve I (olfactory) terminates directly in cortical and subcortical areas of the frontal and temporal lobes. It is closely associated functionally with the limbic system and is described in that context (Ch. Cranial nerve V (trigeminal) attaches to the pons, medial to the middle cerebellar peduncle. The ventral surface of the medulla is separated from the basilar part of the occipital bone and apex of the dens by the meninges and occipito-axial ligaments. Caudally, the dorsal surface of the medulla occupies the midline notch between the cerebellar hemispheres. Caudally, the ventral median fissure is interrupted by the obliquely crossing fascicles of the pyramidal decussation. Rostrally, it ends at the pontine border in a diminutive depression, the foramen caecum. Immediately lateral to the ventral median fissure is a prominent elongated ridge called the pyramid, which contains descending pyramidal, or corticospinal, axons. From this emerges, in line with the ventral spinal nerve roots, a linear series of rootlets that constitute the hypoglossal nerve. The abducens nerve emerges at the slightly narrowed rostral end of the pyramid, where it adjoins the pons. The glossopharyngeal, vagus and accessory nerves join the brain stem along the line of this sulcus, in line with the dorsal spinal nerve roots. The spinal central canal extends into the caudal half of the medulla, migrating progressively more dorsally until it opens out into the lumen of the fourth ventricle. Most fibres in the fasciculi synapse with neurones in their respective nuclei, and these project to the contralateral thalamus, which in turn projects to the primary somaesthetic cortex.
Buy cheapest furosemide and furosemide
Ask the patient whether he or she is right- or left-handed (to help determine the likely dominant hemisphere blood pressure 9070 buy cheapest furosemide, which is in the left brain in most right-handed people). Next ask the patient to name an object pointed at,2 then to point to a named object in the room. Cerebellar disease (and acute alcoholic intoxication) causes slurring and staccato speech. In nominal dysphasia, this is the only abnormality (dominant posterior temporoparietal lesion). Patients with conductive and receptive dysphasia have difficult repeating words or phrases. Look for craniotomy scars, which suggest previous surgery that has required opening of the skull. The use of a systematic approach is the only way to be sure nothing important is left out. The first (olfactory) nerve Testing is not performed routinely but is required if there is suspected loss of smell (anosmia). Each nostril is tested separately using non-pungent substances in a series of sample bottles. The patient sniffs these delicately and should be able to identify common smells, such as coffee and vanilla. Always test visual acuity with the patient wearing his or her reading spectacles, if required. The ability to read the letters normally visible at this distance is called 6/6 vision. The ability to read only larger letters normally visible at 60 m is called 6/60 vision. If visual acuity is poor, the fields are mapped using the fingers instead of a pin. Ask the patient to say when your first and second fingers become visible as they are brought into the quadrants of the visual fields. With practice the fields can be mapped with your fingers-this is how ophthalmologists perform the test. It is usually possible to see through the fingers and vision is therefore not occluded completely. Look at the pupils, noting the shape, relative sizes and any associated ptosis (complete or partial involuntary eyelid closure). Use a pocket torch, shining the light from the side to gauge the reaction of the pupils to light. Assess quickly both the normal direct (constriction of the illuminated pupil) and normal consensual (constriction of the other pupil) responses. Remember that both pupils should normally contract briskly and equally when a light is shone into one. Test accommodation (the constriction of the pupils that occurs when the eyes focus on a near object) by asking the patient to look into the distance and then at an object. Assess eye movements with both eyes first, getting the patient to follow the pin or your finger laterally right and left, then up and down (in an H pattern). Ask about diplopia (double vision) and in which direction of gaze the diplopia is most pronounced. The separation of the images is greatest in the direction in which the affected muscle has its dominant effect. Test the corneal reflexes gently using a wisp of cottonwool to touch the cornea and ask the patient whether the touch can be felt. Start on one side of the forehead and move to the other side, pressing the pin into the skin and asking the patient to tell you what he or she internalmedicinebook. If areas of reduced sensation (dull) are found, map them by moving the pin until normal sensation is again present (sharp). Test light touch by touching but not stroking the skin with a piece of cottonwool. Note the presence of sensory dissociation (usually loss of pain and temperature sensation and preservation of light touch). This is rare but occurs typically in syringobulbia, where enlargement of the central canal of the brainstem and upper spinal cord interrupts crossing pain and temperature fibres first. Examine the motor division of the fifth nerve by asking the patient to clench the teeth while you feel the masseter muscles. Then to open his or her mouth while you attempt to force it closed (not too hard); this should not be possible if the pterygoid muscles are working. Test the jaw jerk by tapping the reflex hammer on your own thumb placed on the chin of the patient, whose mouth is partly open. This is present in healthy people, but is exaggerated, with brisk bilateral contraction of the masseter internalmedicinebook. This is preserved in an upper motor neuron lesion because of bilateral cortical representation of these muscles. Both upper and lower unilateral facial weakness can lead to incomplete closure of the eye on the same side, but a lower motor neuron lesion has a more pronounced effect. The eighth (acoustic) nerve Quantitative hearing assessment is not possible without special equipment, but useful qualitative information can be obtained at the bedside. It takes practice to know at what level of loudness a whisper is normally audible. With a unilateral lesion of the tenth nerve the uvula is drawn towards the unaffected (normal) side. It may be unwise to test even gently for a gag reflex (the ninth nerve is the sensory component and the tenth nerve the motor component), whereby a spatula is touched onto internalmedicinebook. The normal response is gagging with contraction of the palate on both sides, or even vomiting. To test the sensory (afferent) limb of the gag reflex, it is preferable to touch the pharynx on each side, and ask whether the touch can be felt and seems the same on each side. Then ask the patient to turn his or her head against the eleventh (accessory) nerve trapezius as you push the shoulders down. Nerve palsy (a lower motor neuron lesion) causes weak contraction of the sternocleidomastoid muscle ipsilateral to the lesion. An upper motor neuron lesion may cause weakness of contralateral head version because of ipsilateral sternomastoid weakness. While examining the mouth, inspect the tongue for wasting and fasciculation (random flickering movements of small muscle groups), which is characteristic of a lower motor neuron lesion. A unilateral lesion causes the tongue to deviate towards the weaker (affected) side. Examples include lesions of the cortex, internal capsule, brainstem and spinal cord. These are associated with increased tone (spasticity) in the affected muscle groups. The reflexes are exaggerated and clonus (a rhythmical muscle contraction) may be present, but muscle wasting and fasciculations are absent. Weakness is present in all muscle groups of the lower limb but may be more marked in the flexor muscles. In the upper limb, weakness may be more marked in the extensors (pattern-extended leg, flexed arm). Increased tone is present (may be clasp-knife-initial resistance that gives way suddenly) and is often associated with clonus. Weakness may be more obvious distally than proximally, and the flexor and extensor muscles are equally involved.
Cheap furosemide 40 mg visa
These dynamic forces can vary in magnitude and are influenced by occupation blood pressure chart pdf discount furosemide online, locomotion and posture. Each presacral segment (except the first two cervical) is separated from its neighbour by a fibrocartilaginous intervertebral disc. The functions of the column are to support the trunk, protect the spinal cord and nerves and provide attachments for muscles. The total length of the vertebral column is approximately 70 cm in males and 60 cm in females. The intervertebral discs contribute about onequarter of this length in young adults, although there is some diurnal variation in this contribution. Approximately 8% of overall body length is accounted for by the cervical spine, 20% by the thoracic, 12% by the lumbar and 8% by the sacrococcygeal regions. Although the usual number of vertebrae is 7 cervical, 12 thoracic, 5 lumbar, 5 sacral and 4 coccygeal, this total is often variable, with reports of between 32 and 35 bones. Thus, there may be thoracic costal facets on the seventh cervical vertebra, giving it the appearance of an extra thoracic vertebra; lumbar-like articular processes may be found on the lowest thoracic vertebra or the fifth lumbar vertebra may be wholly or partially incorporated into the sacrum. As a result of these changes in transition between vertebral types, there may be 23 to 25 mobile presacral vertebrae. Deformity and bony deficiency may occur at several sites within the posterior elements. The laminae may be wholly or partially absent, or the spinous process alone may be affected, even without overlying soft tissue signs (spina bifida occulta). A defect may occur in the part of the lamina between the superior and inferior articular processes (pars interarticularis); this condition is called spondylolysis, and it may be developmental or result from acute or fatigue fracture. If such defects are bilateral, the column becomes unstable at that level, and forward displacement of that part of the column above (cranial to) the defects may occur; this is called spondylolisthesis. Abnormality of the laminar bone or degenerative changes in the facet joints may lead to similar displacement in the absence of pars defects. The deformity of the vertebral canal, resulting from severe spondylolisthesis, may lead to neural damage. Much more rarely, bony defects may occur elsewhere in the posterior elements, such as in the pedicles. Detailed anatomical relations of all aspects of the vertebral column at the various levels are best appreciated by the study of horizontal (axial) sections and images. Structural Defects of the Posterior Bony Elements the embryonic body appears flexed. Functional muscle development leads to the early appearance of secondary cervical and lumbar spinal curvatures in the sagittal plane. The cervical curvature appears at the end of the embryonic period and reflects the development of function in the muscles responsible for head extension, an important component of the `grasp reflex. Ultrasound investigations support the role of movement in the development of these curvatures. The early appearance of the secondary curves is probably accentuated by postnatal muscular and nervous system development at a time when the vertebral column is highly flexible and is capable of assuming almost any curvature. It is particularly flexible and, if dissected free from the body, can easily be bent (flexed or extended) into a perfect half circle. The thoracic part of the column is the first to develop a relatively fixed curvature, which is concave anteriorly. An infant can support its head at approximately 3 or 4 months, can sit upright at 9 months and commences walking between 12 and 15 months. These functional changes exert a major influence on the development of secondary curvatures in the vertebral column and changes in the proportional size of the vertebrae, particularly in the lumbar region. The secondary lumbar curvature becomes important in maintaining the centre of gravity of the trunk Curvatures Embryonic and Fetal Curvatures Neonatal Curvatures Anterior Aspect the anterior aspect of the column is formed by the anterior surfaces of the vertebral bodies and of the intervertebral discs. It has important anatomical relations at all levels and should be considered in continuity. Adult Curvatures also develop to cope with pelvic obliquity, such as that imposed by unequal leg lengths. The sagittal curvatures are present in the cervical, thoracic, lumbar and pelvic regions. These curvatures developed with rounding of the thorax and pelvis as an adaptation to bipedal gait. In adults, the cervical curve is a lordosis (convex forward) and is the least marked. It extends from the atlas to the second thoracic vertebra, with its apex between the fourth and fifth cervical vertebrae. It extends between the second and the eleventh or twelfth thoracic vertebrae, and its apex lies between the sixth and ninth thoracic vertebrae. This curvature is caused by the increased posterior depth of the thoracic vertebral bodies. It has a greater magnitude in females and extends from the twelfth thoracic vertebra to the lumbosacral angle; there is increased convexity of the last three segments as a result of the greater anterior depth of the intervertebral discs and some posterior wedging of the vertebral bodies. The pelvic curve is concave anteroinferiorly and involves the sacrum and coccygeal vertebrae. The presence of these curvatures means that the cross-sectional profile of the trunk changes with the spinal level. The anteroposterior diameter of the thorax is much greater than that of the lower abdomen. In the normal vertebral column there are well-marked curvatures in the sagittal plane and no lateral curvatures other than in the upper thoracic region, where there is often a slight lateral curvature that is convex to the right in right-handed persons and to the left in left-handed persons. Compensatory lateral curvature may Vertebral Column in the Elderly In older people, age-related changes in the structure of bone lead to broadening and loss of height of the vertebral bodies. The bony changes in the vertebral column are accompanied by changes in the collagen content of the discs and by decline in the activity of the spinal muscles. This leads to progressive decline in vertebral column mobility, particularly in the lumbar spine. Overall, these changes in the vertebral column lead directly to loss of total height in the individual. In men, there is a relative decrease of posterior-to-anterior body height; in both sexes anterior height decreases relative to width. Twomey and coworkers (1983) observed a reduction in bone density of lumbar vertebral bodies with age, principally as a result of a reduction in transverse trabeculae (more marked in females owing to postmenopausal osteoporosis); this was associated with increased diameter and increasing concavity in the juxtadiscal surfaces (end-plates). Osteophytes (bony spurs) may form from the compact cortical bone on the anterior and lateral surfaces of the bodies. Pain is increased with coughing or straining or with attempted back movement and is accompanied by pins and needles paraesthesia down the lateral calf to the ankle. Examination demonstrates paravertebral muscle spasm, impaired pain appreciation along the right lateral calf, weakness of the extensor hallucis longus muscle and loss of the right Achilles tendon reflex. Each ganglionic neurone has a single short stem that divides into a medial branch, which enters the spinal cord via a dorsal root, and a lateral branch, which passes peripherally to a sensory end-organ. The central branch is an axon, whereas the peripheral one is an elongated dendrite (but when traversing a peripheral nerve it is, in general structural terms, indistinguishable from an axon). The region of spinal cord associated with the emergence of a pair of nerves is a spinal segment, but there is no actual surface indication of segmentation. The spinal dura mater forms a tube whose upper end is attached to the edge of the foramen magnum and to the posterior surfaces of the second and third cervical vertebral bodies, as well as to the posterior longitudinal ligament by fibrous bands, especially toward the caudal end of the vertebral canal. It invests the thin spinal filum terminale, descends to the back of the coccyx, and blends with the periosteum. The meningeal coverings of the spinal roots and nerves are described later in this chapter. The epidural space lies between the spinal dura mater and the tissues that line the vertebral canal. It is closed above by fusion of the spinal dura with the edge of the foramen magnum, and below by the posterior the single layer of dura that lines the cranial cavity divides into two layers as it passes downward through the foramen magnum, although it is still a single layer as it forms the anterior and posterior atlanto-occipital membranes. Within the vertebral column, it has been suggested that the outer endosteal Epidural Space 118 Chapter 8 / Spinal Cord and Nerve Roots. Note the fusiform cervical and lumbar enlargements of the cord and the changing obliquity of the spinal nerve roots as the cord is descended.
Discount furosemide online master card
Octreotide may be a lifesaving treatment in patients experiencing an acute carcinoid crisis although bolus injection of this somatostatin analog may be accompanied by bradycardia and second- and third-degree heart block blood pressure chart height purchase furosemide 100mg free shipping. Gonadotropins are used most often for the treatment of infertility and cryptorchism. Induction of ovulation can be stimulated in females who are infertile because of pituitary insufficiency. Photic information from the retina is transmitted to the pineal gland through the suprachiasmatic nucleus of the hypothalamus and the sympathetic nervous system. In humans, the circadian rhythm for the release of melatonin from the pineal gland is closely synchronized with the habitual hours of sleep. It is unclear whether the beneficial effect of exogenous melatonin on symptoms of jet lag are due to a hypnotic effect or resynchronization of the circadian rhythm. Diabetes insipidus is due to inadequate secretion of vasopressin by the posterior pituitary. Neurotrauma and surgery of the pituitary and hypothalamus, cerebral ischemia, or cerebral malignancy can cause diabetes insipidus. Vasopressin may be effective to treat hypotension from anaphylaxis and from severe catecholamine deficiency after resection of a pheochromocytoma. Excess generation of nitric oxide, activation of the renin-angiotensin system, and low plasma concentrations of vasopressin contribute to progressive loss of vascular tone during sepsis. Vasopressin is more effective than epinephrine for management of asystole and the treatment of refractory cardiac arrest. Vasopressin may serve as an adjunct in the control of bleeding esophageal varices and during abdominal surgery in patients with cirrhosis and portal hypertension. Infusion of 20 units over 5 minutes results in marked decreases in hepatic blood flow lasting about 30 minutes. Vasoconstriction and increased systemic blood pressure occur only with doses of vasopressin that are much larger than those administered for the treatment of diabetes insipidus. Vasopressin, even in small doses, may produce selective vasoconstriction of the coronary arteries, with decreases in coronary blood flow manifesting as angina pectoris, electrocardiographic evidence of myocardial ischemia, and, in some instances, myocardial infarction. Oxytocin stimulates uterine muscle and is administered to induce labor at term, reduce and prevent uterine atony, and decrease hemorrhage in the postpartum or postabortion period. All preparations of oxytocin used clinically are synthetic, and their potency is described in units. Synthetic preparations are identical to the hormone normally released from the posterior pituitary but devoid of contamination by other polypeptide hormones and proteins found in natural proteins. High and bolus doses of oxytocin are more likely to decrease systolic and diastolic blood pressure via a direct relaxant effect on vascular smooth muscles. There is no evidence that administration of estrogens delays the progression of atherosclerosis in postmenopausal women. There is evidence that administration of estrogen to postmenopausal women prevents bone loss (protects against osteoporosis) and also prevents vertebral and femoral bone fractures. The presence of receptors for estrogen increases the likelihood of a palliative response to estrogen therapy in women with metastatic breast cancer. The absorption of most estrogens and their derivatives from the gastrointestinal tract is prompt and nearly complete. The most frequent unpleasant symptom associated with the use of estrogens is nausea. Tamoxifen is administered for a period of 5 years to postmenopausal women with breast cancer that was characterized by estrogen-responsive receptors (tamoxifen has estrogenic activity in some tissues, including bone). Raloxifene is a nonsteroidal benzothiophene that acts as a selective estrogen-receptor modulator (preserves the beneficial effects of estrogens including prevention of bone loss and lowering of plasma cholesterol concentrations without any associated effects on reproductive organs). Orally active derivatives of progesterone are designated progestins (often combined with estrogens as oral contraceptives). Dysfunctional uterine bleeding can be treated with small doses of a progestin for a few days, with the goal being induction of progesterone-withdrawal bleeding. Antiprogestins inhibit the hormonal effects of progesterone and are the most effective and safest means of medical abortion. Mifepristone has been used as a postcoital contraceptive within 72 hours of unprotected intercourse. Oral contraceptives are most often a combination of an estrogen and a progestin (inhibits ovulation, presumably by preventing release of follicle-stimulating hormone by estrogen and luteinizing hormone by progesterone). Estrogens in combined preparations are believed to be responsible for most, if not all of the side effects of oral contraceptives (increased incidence of thromboembolism). Nausea, vomiting, weight gain, and breast discomfort resembling early pregnancy are attributed to the estrogen component of oral contraceptives. Oral contraceptives containing high doses of estrogen may produce alterations in the glucose tolerance curves of patients with preclinical diabetes mellitus. Depression of mood and fatigue have been attributed to the progestin component of oral contraceptives. Androgens are administered to males to stimulate the development and maintenance of secondary sexual characteristics. The most common indication of androgen therapy in females is palliative management of metastatic breast cancer. Androgens enhance erythropoiesis by stimulation of renal production of erythropoietin. Testosterone administered orally is readily absorbed but is metabolized so extensively by the liver that therapeutic effects do not occur. Dose-related cholestatic hepatitis and jaundice are particularly likely to accompany androgen therapy for palliation in neoplastic disease. Androgens increase the potency of coumarin anticoagulants and the likelihood of spontaneous hemorrhage. The low androgenic activity of danazol makes it the preferred androgen for treatment of hereditary angioedema. As with other androgens, danazol therapy has been associated with abnormal liver function tests and jaundice. Finasteride is administered orally (5 mg once daily) for the treatment of benign prostatic hyperplasia. Treatment of male pattern baldness, hirsutism, and acne may represent other potentially useful applications for finasteride. The excessive use of antimicrobials (antibiotics) for the treatment of conditions for which these drugs provide little or no benefit (upper respiratory tract infections, bronchitis) has contributed to the emergence of bacterial resistance. Misuse of antibiotics in the general population is in contrast to the proven benefit of antibiotic prophylaxis for selected surgical procedures, which has been part of a national initiative to enhance compliance (Table 41-1). The use of antimicrobial prophylaxis in surgery involves a risk-to-benefit evaluation, which varies depending on the nature of the operative procedure (Table 41-2). Because of their wide therapeutic index and low incidence of side effects, cephalosporins (most often a cost-effective first-generation cephalosporin such as cefazolin) are the antimicrobials of choice for surgical procedures in which skin flora and normal flora of the gastrointestinal and genitourinary tracts are the most likely pathogens. The surgical care improvement project and prevention of post-operative infection, including surgical site infection. In patients with documented IgE-mediated anaphylactic reactions, -lactam antibiotics can usually be substituted with clindamycin or vancomycin. Routine prophylaxis with vancomycin is not recommended for any patient population in the absence of documented or highly suspected colonization or infection with methicillin-resistant Staphylococcus aureus (recent hospitalization or nursing home stay and hemodialysis patients) or known IgE-mediated response to -lactam antibiotics. Prompt identification of the causative organism is essential for the selection of appropriate antimicrobial drugs to treat ongoing infection. Nearly 80% of nosocomial infections occur in three sites (urinary tract, respiratory system, and bloodstream). Intravascular access catheters are the most common cause of bacteremia or fungemia in hospitalized patients. The organism infecting access catheters most commonly comes from the colonized hub or lumen and reflect skin flora (S. Initial therapy of suspected intravascular catheter infection usually includes vancomycin because of the high incidence of methicillin-resistant S.
