
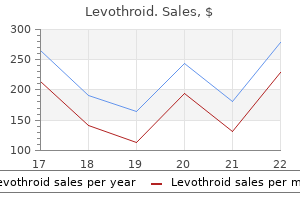
Best levothroid 50mcg
Monitor closely the patency of the chest tubes and the amount of chest tube drainage thyroid hormone resistance levothroid 100 mcg with amex. Notify the physician if the chest tube drainage is greater than 200 mL/hour for more than 2 to 3 hours, which may indicate a postoperative hemorrhage. Help the patient sit up in the bedside chair and assist the patient to ambulate as soon as possible. Secretions may become thick and difficult to expectorate when the patient is having radiation therapy. Percussion, postural drainage, and vibration can be used to aid in clearing secretions. The patient may experience less anxiety if allowed as much control as possible over his or her daily schedule. Explaining procedures and keeping the patient informed about the treatment Lung Cancer 717 plan and condition may also decrease anxiety. Allow for the time needed to adjust while helping the patient and family begin the grieving process. Patients were diagnosed with the following cancers: bladder, brain, breast, colon/rectum, head/neck, liver, kidney, lung, ovary, pancreas, and prostate as well as leukemia and lymphoma. The authors suggest that the answer to the single question can determine the overall burden of a given set of treatments. Provide the patient with the names, addresses, and phone numbers of support groups, such as the American Cancer Society, the National Cancer Institute, the local hospice, the Lung Cancer Alliance, and the Visiting Nurses Association. The course of disease is variable and unpredictable, with episodes of remission and relapse. These complexes are deposited in the basement membranes of the skin and kidneys, disrupting the function of these organs. The most common causes of death are renal failure and infections, followed by neurological and cardiovascular disorders. In the last decades, therapy has reduced mortality from lupus, with 5-year survival rates of more than 90% and 20-year survival rates of 70%. A familial association has been noted that suggests a genetic predisposition, but a genetic link has not been identified. Environmental factors, susceptibility to certain viruses, and an immune system dysfunction with production of autoantibodies are possible causes. Some drugs have been implicated as initiating the onset of lupus-like symptoms and aggravating existing disease; they include hydralazine hydrochloride, procainamide hydrochloride, penicillin, isonicotinic acid hydrazide, chlorpromazine, phenytoin, and quinidine. Possible childhood risk factors include low birth weight, preterm birth, and exposure to farming pesticides. Heritability is estimated at 43%, and there Lupus Erythematosus 719 are now over 80 loci that are associated with lupus erythematosus. Genes encoding proteins of the complement system appear to have the strongest association with lupus erythematosus. It is also more prominent in people with Asian, Latino/Hispanic, and African American ancestry than in other populations. Prevalence is higher in white people living in Western Europe and in people from the Caribbean living in Europe, and it is lower in Africa and China. The patient may report musculoskeletal and cutaneous symptoms, including joint and muscle pain, puffiness of hands and feet, joint swelling and tenderness, hand deformities, and skin lesions such as the characteristic "butterfly rash" (fixed reddish and flat rash that extends over both cheeks and the bridge of the nose). Other symptoms may include maculopapular rash (small, colored area with raised red pimples), sensitivity to the sun, photophobia, vascular skin lesions, leg ulcers, oral ulcers, and hair loss. Other symptoms originate in the genitourinary tract (menstrual abnormalities, amenorrhea, spontaneous abortion) or central nervous system (visual problems, memory loss, mild confusion, headache, seizures, psychoses, loss of balance, depression). Establish a history of symptoms related to the hematologic system (venous or arterial clotting, bleeding tendencies), cardiopulmonary system (chest pain, shortness of breath, lung congestion), or gastrointestinal system (nausea, vomiting, difficulty swallowing, diarrhea, and bloody stools). Ask if the patient has a history of hormonal abnormality or ultraviolet radiation. Ask the patient if he or she is taking or has taken any of the medications implicated as initiating lupus-like symptoms. Inspect the integumentary system thoroughly, including the mucous membranes, to determine the site of skin rashes and lesions. Check for lesions and necrosis on the fingertips, toes, and elbows; these may be caused by inflammation of terminal arterioles. Determine the extent of range of motion and movement of extremities and level of joint discomfort. Auscultate the lungs and heart to determine the presence of a pleural or pericardial friction rub. Palpate the spleen and liver to determine the presence of tenderness, splenomegaly, or hepatomegaly. Assess for fever, pallor, and signs of bleeding, including petechiae and bruising. The patient may have problems maintaining professional and family roles and may experience loss over a deteriorating health status. Lupus is associated with an increased incidence of spontaneous abortion, fetal death, and prematurity. To make the diagnosis of lupus, the American College of Rheumatology developed the following list. General supportive therapy includes adequate sleep and avoidance of fatigue because mild disease exacerbations may subside after several days of bedrest. A physical therapy program is important to maintain mobility and range of motion without allowing the patient to get overtired. Encourage the patient to maintain activity when the symptoms are mild or in remission. Encourage the patient to use a hair stylist or barber who specializes in caring for people with scalp disorders and to protect all body surfaces from direct sunlight. The patient should use sunscreen with a protective factor of at least 20 and wear a hat and long sleeves while in the sun. Note that certain drugs (tetracycline) and foods (figs, parsley, celery) augment the effects of ultraviolet light and therefore should be avoided. Explore the meaning of the chronic illness and coping strategies with the patient. A total of 2,527 surveys were returned; 94% of the surveys were returned by females. The most common self-reported symptoms that interfered with daily life were fatigue/weakness (91%) and joint/pain swelling (77. Seventythree per cent acknowledged having problems from their symptoms as they carried out their usual daily activities. Thirty-two per cent of the respondents were using non-traditional therapies such as acupuncture and massage to manage their symptoms. Explain to the patient the disease process, the purpose of treatment regimens, and the importance of compliance. Teach the patient to wear a Medic Alert bracelet noting the disease and medications so appropriate action can be taken in an emergency. Encourage the patient to keep all vaccinations current such as the meningococcal vaccine, pneumococcal vaccine, and routine flu vaccines. Teach the female patient the importance of planning pregnancies with medical supervision because pregnancy is likely to cause an exacerbation of the disease. Discuss all precipitating factors that need to be avoided, including fatigue, vaccination, infections, stress, surgery, certain drugs, and exposure to ultraviolet light. Encourage the patient to contact the Arthritis Foundation, the Lupus Foundation, and other appropriate support groups that are available in the area. This disease is named for the town in Connecticut where it was first recognized in the 1970s. Although the number of cases vary from L Lyme Disease 723 year to year, approximately 30,000 cases are reported annually in the United States, making it the leading tick-borne disease in the country. Lyme disease typically begins in summer or early fall and develops in three stages with varying, progressive symptoms over weeks and months if untreated. The most frequent carrier of the disease is the deer tick, a small insect the size of a poppy seed.
Quittenbaum (Quince). Levothroid.
- How does Quince work?
- Dosing considerations for Quince.
- Are there any interactions with medications?
- Are there safety concerns?
- What is Quince?
- Digestive disorders, diarrhea, coughs, stomach and intestinal inflammation, skin injuries, inflammation of the joints, eye discomfort, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96398
Buy generic levothroid 50mcg on-line
In 2017 thyroid nodules sore throat cheap levothroid 100 mcg on-line, the American Cancer Society reported that there were 13,360 new cases of laryngeal cancer and 3,660 people died from the disease in the United States. Global rates of the disease in countries with high tobacco and alcohol use are high. Most laryngeal cancer begins in the glottis (the true vocal cords), 35% begins in the supraglottis (false vocal cords), and 5% begins in the subglottis (downward extension from the vocal cords). If it is confined to the glottis, laryngeal cancer usually grows slowly and metastasizes late because of the limited lymphatic drainage of the cords. Laryngeal cancer that involves the supraglottis and subglottis tends to metastasize early to the lymph nodes in the neck because of the rich lymphatic drainage of this area. In early stages, the 5-year survival rates are approximately 60%, and in later stages, they are 35%. Complications include airway obstruction, disfigurement, dysphagia, and metastatic cancer. Each substance poses an independent risk, but their combined use causes a synergistic effect. Other risk factors include a familial tendency, a history of frequent laryngitis or vocal straining, chronic inhalation of noxious fumes, poor nutrition, human papillomavirus, and a weakened immune system. The increased incidence likely occurs because men have higher rates of cigarette and alcohol use, although the incidence in women is rising as more women smoke and drink. Women are more likely to get laryngeal cancer between the ages of 50 and 60 and men between the ages of 60 and 70. Laryngeal cancer is 50% more common in African American individuals than in white individuals of European origin. The incidence is twice as high in developed regions of the world as compared to developing regions, likely because of the patterns of risk behaviors in developed countries. Be aware as you interview the patient that hoarseness, shortness of breath, and pain may occur as the patient speaks. Obtain a thorough history of risk factors: alcohol or tobacco usage, voice abuse, frequent laryngitis, and family history of laryngeal cancer. Ask the patient how many packs of cigarettes he or she has smoked per day for how many years, as well as the use of other tobacco products. Most patients describe hoarseness or throat irritation that lasts longer than 2 weeks and may report a change in voice quality. Ask about dysphagia, persistent cough, hemoptysis, weight loss, dyspnea, or pain that radiates to the ear, which are late symptoms of laryngeal cancer. The patient may experience guilt, denial, or shame because of the association with cigarette smoking and alcohol consumption. Efforts to cure patients of this disease often result in a loss of normal speech and permanent lifestyle changes. Patients may experience radical changes in both body image and role relationships (interpersonal, social, and work). A multidisciplinary team of speech pathologists, social workers, dietitians, respiratory therapists, occupational therapists, and physical therapists provides preoperative evaluation and postoperative care. The goal is to eliminate the cancer and preserve the ability to speak and swallow. Radiation therapy may be used if the cancer is small, particularly if preserving the voice quality is a priority. To prevent recurrence after surgery, radiation therapy is used to kill any small areas of cancer that might remain. Chemotherapy has not been found to be beneficial in treating this type of cancer and, if used, is always employed in conjunction with surgery or radiation. Chemotherapy may be useful in treating cancer that has metastasized beyond the head and neck, however, and it may be useful as a palliative treatment for cancers that are too large to be surgically removed or for cancer that is not controlled by radiation therapy. Stage 0 cancer is treated either by surgical removal of the abnormal lining layer of the larynx or by laser beam vaporizing of the abnormal cell layer. A common course of radiation therapy consists of daily fractions or doses administered 5 days a week for 7 weeks. Radiation therapy is frequently used as the primary treatment of laryngeal cancer, especially for patients with small cancers. A Laryngeal Cancer 685 partial laryngectomy is an alternative treatment; however, voice results are generally better with radiation. Almost always, a total laryngectomy is performed, although a few laryngeal cancers may be treated by partial laryngectomy. The patient loses her or his voice and sense of smell; the patient breathes through a permanent tracheostomy stoma. A radical neck dissection is done, in conjunction with a partial or a total laryngectomy, to remove carcinoma that has metastasized to adjacent areas of the neck. Newer treatments combining laser therapy and radiation for early-stage laryngeal cancer have promising outcomes. Postoperatively, the most immediate concern is maintaining a patent airway, and aspiration is a high risk. Assess the skin flap for any signs of infection or necrosis and notify the physician of any problems. Patients can use an electrolarynx, an electrical device that is pressed against the neck to produce a "mechanical voice. Through the use of a small one-way shunt valve that is placed into a small puncture at the stoma site, patients can produce speech by covering the stoma with a finger and forcing air out of the mouth. Pharmacologic Highlights Medication or Drug Class Analgesics Dosage Varies with drug Description Morphine sulfate, fentanyl Rationale Relieve pain Other Drugs: Chemotherapy (usually 5-fluorouracil, carboplatin, cisplatin, docetaxel, paclitaxel, epirubicin) may be used in certain circumstances; however, no improvement in overall survival rate has been demonstrated. Targeted therapies (monoclonal antibodies such as cetuximab) may be used in larynx preservation. Explain that the patient may need to breathe through a stoma in the neck, learn esophageal speech, or learn to use mechanical devices to speak. Encourage the expression of feelings about a diagnosis of cancer and offer to contact the appropriate clergy or clinical nurse specialist to counsel the patient. Reposition the patient carefully; after a total laryngectomy, support the back of the neck when moving the patient to prevent trauma. Provide frequent mouth care, cleansing the mouth with a soft toothbrush, toothette, or washcloth. After a partial laryngectomy, the patient should not use his or her voice for at least 2 days. The patient should have an alternative means of communication available at all times, and the nurse should encourage its use. After 2 to 3 days, encourage the patient to use a whisper until complete 686 Laryngeal Cancer healing takes place. As soon as possible after surgery, the patient with a total laryngectomy should start learning to care for the stoma, suction the airway, care for the incision, and self-administer the tube feedings (if the patient is to have tube feedings after discharge). Patients were diagnosed with the following cancers: bladder, brain, breast, colon/rectum, head/neck/larynx, liver, kidney, lung, ovary, pancreas, and prostate as well as leukemia and lymphoma. Teach the patient signs and symptoms of potential complications and the appropriate actions to be taken. Complications include infection (symptoms: wound drainage, poor wound healing, fever, achiness, chills); airway obstruction and tracheostomy stenosis (symptoms: noisy respirations, difficulty breathing, restlessness, confusion, increased respiratory rate); vocal straining; fistula formation (symptoms: redness, swelling, secretions along a suture line); and ruptured carotid artery (symptoms: bleeding, hypotension). Teach the patient the appropriate devices and techniques to ensure a patent airway and prevent complications. Encourage the patient to wear a Medic Alert bracelet or necklace that identifies her or him as a mouth breather. Provide the patient with a list of referrals and support groups, such as visiting nurses, American Cancer Society, American Speech-Learning-Hearing Association, International Association of Laryngectomees, and the Lost Cord Club. In small children, the air passages in the lungs are smaller than those of adults, making them more susceptible to obstruction by edema and spasm. Croup is the most common pediatric illness and causes 15% of all clinic and emergency department visits for child-related respiratory infections. Acute spasmodic laryngitis is particularly common in children with allergies and those with a family history of croup. Complications include secondary bacterial infections such as pneumonia, pulmonary edema, pneumothorax, dehydration, and otitis media.
100 mcg levothroid free shipping
As men become older thyroid symptoms hives order levothroid with mastercard, the incidence of symptoms increases to more than 75% for those over age 80 and 90% by age 85. Of those men with symptoms, approximately 50% of men are symptomatic to a moderate degree and 25% of those have severe symptoms that require surgical interventions. Distinguish between these obstructive symptoms and irritative symptoms such as dysuria, frequency, and urgency, which may indicate an infection or inflammatory process. A "voiding diary" can also be obtained to determine the frequency and nature of the complaints. Each question allows the patient to choose one of six answers on a scale of 0 to 5 indicating the increasing degree of symptoms; the total score ranges from 0 (mildly symptomatic) to 35 (severely symptomatic). Incomplete emptying: Over the past month, how often have you had the sensation of not emptying your bladder completely after you have finished urinating Frequency: Over the past month, how often have you had to urinate again less than 2 hours after you finished urinating Intermittency: Over the past month, how often have you stopped and started again several times when urinating Urgency: Over the past month, how often have you found it difficult to postpone urination Straining: Over the past month, how often have you had to push or strain to begin urination Nocturia: Over the past month, how many times did you most typically get up to urinate from the time you went to bed until the time you got up in the morning How would you feel if you were to spend the rest of your life with your urinary condition just the way it is now Some men have enlarged prostates that extend out into soft tissue without compressing the urethra. Screening for prostate cancer remains controversial (see diagnostic highlights above). Men with mild or moderate symptoms but without complications, and who are not bothered by their symptoms, may be monitored by "watchful waiting. Those patients with the most severe cases, in which there is total urinary obstruction, chronic urinary retention, and recurrent urinary tract infection, usually require surgery. Prostatectomy can be performed, in which the portion of the prostate gland causing the obstruction is removed. Minimally invasive procedures include heat from laser energy, microwaves, radiofrequency energy, highintensity ultrasound waves, and high-voltage electrical energy. Several minimally invasive therapies are continuously being tested and refined to increase efficacy and safety. Postsurgical care involves supportive care and maintenance of the indwelling catheter to ensure patency and adequacy of irrigation. Ongoing monitoring of the drainage from the catheter determines the color, consistency, and amount of urine flow. If the patient develops frank hematuria or an abrupt change in urinary output, the surgeon should be notified immediately. In patients who are not candidates for surgery, a permanent indwelling catheter is inserted. If the catheter cannot be placed in the urethra because of obstruction, the patient may need a suprapubic cystostomy. Conservative therapy also includes prostatic massage, warm sitz baths, and a short-term fluid restriction to prevent bladder distention. If there is resistance during insertion, stop the catheterization procedure and notify the physician. In addition, assess the patient for signs of shock from postobstruction diuresis after catheter insertion. Encourage the patient to drink at least 2 L of fluid per day to prevent stasis and infection from a decreased intake. Encourage the patient to avoid the following medications, which may worsen the symptoms: anticholinergics, decongestants (over-the-counter and prescribed), tranquilizers, alcohol, and antidepressants. Some patients would prefer to talk to a person of the same gender when discussing sexual matters. Provide supportive care of the patient and significant others and make referrals for sexual counseling if appropriate. The effect of nocturia on sleep quality and daytime function in patients with lower urinary tract symptoms: A crosssectional study. The larger the number of voids at night, the more people experienced daytime sleepiness and poor sleep quality. Patients younger than 65 years experienced more dysfunction than older patients experienced. Instruct patients about the need to maintain a high fluid intake (at least 2 L/day) to ensure adequate urine output. Teach the patient to monitor urinary output for 4 to 6 weeks after surgery to ensure adequacy in volume of elimination combined with a decrease in volume of retention. Explain that the patient should not do any heavy lifting or undergo strenuous exercise for several weeks after surgery. Provide instructions about all medications used to relax the smooth muscles of the bladder or to shrink the prostate gland. Provide instructions on the correct dosage, route, action, side effects, and potential drug interactions and when to provide this information to the physician. Instruct the patient to report any difficulties with urination to the physician immediately. A diet low in fat and high in protein and vegetables may reduce the risk of the disorder. Encourage the patient to discuss any sexual concerns he or his partner may have after surgery with the appropriate counselors. Reassure the patient that a session can be set up by the nurse or physician whenever one is indicated. Usually, physicians recommend that patients have no sexual intercourse or masturbation for several weeks after invasive procedures. It accounts for approximately 4% of all cancers and 2% of deaths from cancer in the United States. The American Cancer Society estimates that in 2018, there will be approximately 80,000 new cases of bladder cancer and 17,000 people will die from the disease. Urothelial tumors are classified as invasive or noninvasive and according to their shape (papillary or flat). Noninvasive urothelial cancer affects only the innermost layer of the bladder, whereas invasive urothelial cancer spreads from the urothelium to the deepest layers of the bladder. Papillary tumors have fingerlike projections that grow into the hollow of the bladder. Flat urothelial tumors involve the layer of cells closest to the inside of the bladder. Most bladder tumors are multifocal because the environment of the bladder allows for the continuous bathing of the mucosa with urine that contains tumor cells that can implant in several locations. Direct extension can occur to the sigmoid colon, rectum, and, depending on the sex of the patient, the prostate or uterus and vagina. Given these risks, the following occupations expose people to possible toxic substances: beauticians and barbers, painters, dry cleaners, and people working in the rope and paper industries. Cancer-causing chemicals enter the bloodstream, are filtered through the kidneys, become concentrated in the urine, and then damage the endothelial cells that line the inside of the bladder. Other associated factors include chronic bladder irritation and infection, vesical calculi, and exposure to cyclophosphamide (Cytoxan). Incidence is highest among European American men, with a rate twice that of African American men and four times that of European American women. Women and black/African American men have a lower incidence of bladder cancer but a poorer prognosis than do European American men.
Discount levothroid 100mcg amex
To establish the diagnosis of small bowel obstruction thyroid boosting foods trusted 100 mcg levothroid, ask about vomiting fecal contents, wavelike abdominal pain, or abdominal distention. A paralytic ileus usually causes a distended abdomen, with or without pain, but usually without cramping. To establish the diagnosis of large bowel obstruction, which has a slower onset of symptoms, ask about recent constipation with a history of spasmodic abdominal pain several days afterward. Neurogenic obstruction characteristically produces diffuse abdominal discomfort rather than colicky pain. Establish a history of vomiting; ask the patient to describe the vomitus, which may consist of gastric and bile contents but rarely fecal contents. Always auscultate the abdomen for up to 5 minutes for bowel sounds before palpation. Palpate all four quadrants of the abdomen to determine areas of localized tenderness, guarding, and rebound tenderness. Assess the patient for tachycardia, a narrowed pulse pressure, urine output less than 30 mL per hour, and delayed capillary blanching- all indicators of severe hypovolemia and impending shock. The patient with an intestinal obstruction is acutely ill and may need emergency intervention. If the patient is a child, the family will have significant concerns about the emergency and surgical outcomes. A growing number of procedures can be handled with laparoscopic surgery, which may have shorter recovery time and reduced number of needed diagnostic procedures prior to laparoscopy. The patient may require temporary endotracheal intubation and mechanical ventilation to manage airway and breathing. The circulation usually needs support from parenteral fluids, and total parenteral nutrition may be prescribed if the patient has protein deficits. Care for the surgical site and notify the physician if you observe any signs of poor wound healing, bleeding, or infection. Antibiotics are generally given to cover both gram-negative aerobic and gram-negative anaerobic organisms. Analgesic medication may be ordered after the cause of the obstruction is known, but it may be withheld until the diagnosis of intestinal obstruction is confirmed so as to not mask Intestinal Obstruction 645 pain, which is an important clinical indicator. Usually, until the patient is stabilized, her or his condition precludes any oral intake. Position the patient in the Fowler or semi-Fowler position to ease respiratory discomfort from a distended abdomen. Frequent mouth care and lubrication of the mucous membranes can assist with patient comfort. Explain the diagnostic tests and treatments, preparing the patient for the possibility of surgery. Early laparoscopic adhesiolysis for small bowel obstruction: Retrospective study of main advantages. They evaluated the records of 107 patients admitted with the diagnosis of adhesional small bowel obstruction. Patients underwent medical treatment, early surgery, emergency surgery, or delayed surgery after failure of medical management. Medical treatment and delayed surgery also resulted in longer fasting time, double the number of radiological examinations, and more major complications than the early surgery group. The laparoscopic group had the earliest regain of function as well as shorter fasting time, reduced number of radiological examinations, and reduced hospital stay. Emphasize that in the case of recurrent abdominal pain, fever, or vomiting, the patient should go to the emergency department for evaluation. Although they are more frequently associated with closed-head injuries, they can also occur as a result of an open or penetrating injury or a depressed skull fracture. They can also occur deep within the hemispheres in the paraventricular, medial, or paracentral areas in association with the shearing strain on small vessels that occurs with diffuse axonal injuries. The patient can experience deterioration in cerebral functioning at the time of injury or in the first 48 to 72 hours after injury. Late hemorrhage into a contused area is possible for as long as 7 to 10 days after injury. A high-velocity penetration (bullet) can produce shock waves that are transmitted throughout the brain in addition to the injury caused by the bullet directly. A low-velocity penetrating injury (knife) may involve only focal damage and no loss of consciousness. Stroke results from hypertensive damage to the blood vessel wall, rupture of an aneurysm, or bleeding from an arteriovenous malformation. Males ages 15 to 24 are three times more likely than females to be injured in a crash. People of black/African American ancestry have higher rates of intracerebral hemorrhage due to hypertension. The peak incidence occurs in childhood (ages 3 to 12) and in older adults (ages 50 to 70). In trauma patients, if the patient is not able to report a history, question the prehospital care provider, significant others, or witnesses about the situation and timing of the injury. Determine if the patient experienced momentary loss of reflexes, momentary arrest of respirations, and possible retrograde or antegrade amnesia (loss of memory for events immediately before the injury or loss of memory for events after the injury). If the patient has a suspected stroke, determine the onset of symptoms and whether the patient has a history of hypertension. Elicit a history of headache, drowsiness, confusion, seizures, focal neurological deficits, dizziness, irritability, giddiness, visual disturbances (seeing stars), and gait disturbances. The most common symptoms are alterations in level of consciousness, headache, nausea, and vomiting. When you examine the patient, note that, just as in cerebral contusions, small frontal lesions may be asymptomatic, whereas larger bilateral lesions may result in a frontal lobe syndrome of inappropriate behavior and cognitive deficits. Other signs of basilar skull fracture include raccoon eyes (periorbital ecchymosis or bruising around the eyes) and Battle sign (bleeding and swelling behind the ear). Several signs to look for include ipsilateral miosis (Horner syndrome), in which one pupil is smaller than the other with a drooping eyelid; bilateral miosis, in which both pupils are pinpoint in size; ipsilateral mydriasis (Hutchinson pupil), in which one of the pupils is much larger than the other and is unreactive to light; bilateral midposition, in which both pupils are 4 to 5 mm and remain dilated and nonreactive to light; and bilateral mydriasis, in which both pupils are larger than 6 mm and nonreactive to light. Endoscopic evacuation is being attempted as a very early-stage treatment for intracerebral hemorrhage. A ventriculostomy (creation of a hole within a cerebral ventricle for drainage) allows for external drainage for patients experiencing ventricular bleeding. Because bleeding and swelling can progress over several days after injury, the patient is monitored for deterioration even up to 10 days after injury. During periods of frequent assessment, the patient should not be sedated for longer than 30 minutes at a time; longer-acting sedation may mask neurological changes and place the patient at risk for lack of detection. Blood pressure needs to be regulated carefully, keeping the mean arterial pressure less than 130 mm Hg but avoiding hypotension so that the brain is adequately perfused. Fluid and electrolytes need careful adjustment to maintain brain perfusion but reduce the potential for cerebral edema. Phytonadione and protamine may be used to reverse coagulopathies, and famotidine may be used to prevent gastric ulcers. Avoid hip flexion by maintaining the patient in a normal body alignment, limiting venous drainage. Maintain a quiet, restful environment with minimal stimulation; limit visitors as appropriate. Strategies to maximize the coping mechanisms of the patient and family are directed toward providing support and encouragement. Teach the patient and family appropriate rehabilitative exercises, as appropriate. Help the significant others and family face the fear of death, disability, and dependency; involve the patient and the family in all aspects of care. Traumatic brain injury in children under age 24 months: Analysis of demographic data, risk factors, and outcomes of post-traumatic seizure. Four patients had experienced child abuse, and 10 patients developed posttraumatic seizures. Fifty-five of the 60 patients improved resulting in a good outcome, and 3 experienced moderate disability. Teach the patient and caregiver the signs and symptoms that necessitate a return to the hospital. Teach the patient to Intrauterine Fetal Demise 651 recognize the symptoms and signs of postinjury syndrome, which may last for several weeks.
Buy levothroid american express
Thalidomide neuropathy: A clinical electrophysiological thyroid cancer shirts order levothroid 100 mcg otc, and histological follow-up study. Severe refractory erythema nodosum leprosum successfully treated with the tumor necrosis factor inhibitor etanercept. Restoration by levamisole of low E-rosette forming cells in patients suffering from various diseases. There are instances when the treating physician or dermatologist encounters life-threatening adverse effects, for example, dapsone hypersensitivity syndrome, methemoglobinemia, hemolytic anemia, agranulocytosis, thrombocytopenia, hepatitis, fatal enteropathy, etc. Alternative drugs such as minocycline, ofloxacin, and clarithromycin are infrequently used or their serious side effects are very rare; so these conditions are not covered in this chapter. Supportive treatment should include fluid and electrolyte balance, regulation of body temperature, nutritional support, and antibiotics when necessary. Skin care with emollients and avoidance of irritants are 545 546 Leprosy: Therapy-related emergencies Table 59. There are no well-controlled trials to evaluate the effectiveness of any drug to treat such a serious condition. Dapsone-induced methemoglobinemia Methemoglobin is an abnormal form of hemoglobin resulting from the oxidation of iron in the normal heme molecule from the ferrous form (Fe2+) to the ferric (Fe3+) form. The presence of ferric heme molecules causes a structural change in the hemoglobin, resulting in reduced oxygen-carrying capacity and impaired oxygen delivery at the tissue [26,27]. Naturally, red blood cells maintain a steady-state level of methemoglobin of less than 1% via two main enzymatic pathways. Exogenous oxidizing agents can challenge the cytochrome b5 reductase system, leading to increased production of methemoglobin [26]. Clinical symptoms of methemoglobinemia depend on the serum concentration of methemoglobin. Diagnosis of methemoglobinemia is normally based on characteristic clinical symptoms and raised serum methemoglobin level. Therefore, the typical oxygen "saturation gap" observed between arterial blood gas analysis and pulse oximetry readings is very helpful for making the diagnosis of methemoglobinemia. Agranulocytosis is an acute condition characterized by a sudden drop in white cell production leaving the body susceptible to bacterial infection and septicemia. The mechanism is the same as for methemoglobinemia and hemolytic anemia, that is, formation of hydroxylamine, the toxic metabolite of dapsone that ultimately leads to depression of bone marrow. Agranulocytosis due to dapsone is not dose related, and when severe, can also involve platelets causing thrombocytopenia [35,36]. Fever, pallor, and pharyngitis in a patient of leprosy on the first few months of dapsone should be taken as warning symptoms. This situation, where oxygen saturation levels measured with pulse oximetry are substantially lower than arterial blood gas oxygen saturation levels, should alarm the treating physician. Initial management of patients with methemoglobinemia is supportive care with discontinuation of the offending agent. Severely affected patients may benefit from adjunctive treatment with blood transfusion, exchange transfusion, and/or hyperbaric oxygen [30,31]. Cimetidine, an inhibitor of cytochrome P450, can be used as a prophylactic drug when a higher dosage of dapsone is required [32]. Clofazimine-induced enteropathy Clofazimine is a lipophilic iminophenazine dye, having both antimicrobial and anti-inflammatory activities. Being lipophilic, it concentrates well in the lipid-rich tissues, particularly the reticuloendothelial system and intestine, breast, and liver. The skin, gastrointestinal tract, and eyes are the most common sites affected by clofazimine. However, the higher dosage commonly used in lepra reactions can cause enteritis [6,8,9]. Patients present with epigastric distress, occasional vomiting unrelated to meals, intermittent abdominal pain, malabsorption, and abdominal rebound tenderness. Barium swallow shows coarsening of the mucosal pattern and segmentation of barium in the ileum and distal jejunum. Clofazimine-induced crystal-storing histiocytosis [41] Cessation of clofazimine induces clinical improvement in most cases; however, abdominal symptoms may persist for several months to years [42]. Hemolytic anemia is one of 548 Leprosy: Therapy-related emergencies Emergencies due to rifampicin A single dose of rifampicin every month is very rarely reported to cause any side effects in cases of leprosy. However, the treating physician should be watchful for serious side effects such as hemolysis, renal failure, and thrombocytopenia. Multiple ecchymoses, bleeding from gums, and very low platelet count (<20,000/cmm) can be the presentations of thrombocytopenia. For major or life-threatening bleeding, platelet transfusions should be administered without delay [43,44]. Understanding the pharmacology of the drugs, monitoring their use, watching for subtle alarming signs and symptoms, and having a high index of suspicion can save many valuable lives. Dapsone is the most common drug to cause serious adverse effects such as dapsone hypersensitivity syndrome, methemoglobinemia, hemolytic anemia, and agranulocytosis. Clofazimine can cause enteropathy, and rifampicin can lead to hepatotoxicity and thrombocytopenia. Idiosyncratic drug reactions: Possible role of reactive metabolites generated by leukocytes. The dapsone hypersensitivity syndrome revisited: A potentially fatal multisystem disorder with prominent hepatopulmonary manifestations. Acquired methemoglobinemia: A retrospective series of 138 cases at 2 teaching hospitals. Pathophysiologic mechanisms, diagnosis, and management of dapsone-induced methemoglobinemia. Cimetidine: A review of the recent developments and reports in cutaneous medicine. Hemolytic anemia in patients receiving daily dapsone for the treatment of leprosy. Dapsoneinduced hemolytic anemia: role of glucose-6-phosphatodehydrogenase in the hemolytic response of rat erythrocytes to N-hydroxydapsone. Dapsone associated agranulocytosis and severe anemia in a patient with leukocytoclastic vasculitis. A case report of total dapsone induced agranulocytosis in an Indian midborderline leprosy patient. Intra-abdominal, crystal storing histiocytosis due to clofazimine in a patient with lepromatous leprosy and concurrent carcinoma of the colon. Clofazimine-induced crystalstoring histiocytosis producing chronic abdominal pain in a leprosy patient. Clofazimine enteropathy: A rare and under recognized complication of mycobacterial therapy. Many of these diseases when untreated can develop systemic complications, which may present to an emergency department. The complication itself may be the initial presentation of the condition; hence, it is pertinent to have adequate knowledge of these so as to arrive at a correct diagnosis. This infection is caused by the spirochete Treponema pallidum acquired through sexual contact. In case of untreated syphilitic infection, it persists as asymptomatic syphilitic meningitis or progresses to acute syphilitic meningitis and subsequently leads to meningovascular syphilis. The inflammatory infiltrate consisting of lymphocytes and plasma cells is located in the perivascular spaces of the meninges as well as the ependyma. Cranial nerve abnormalities are due to compression by basilar exudate or due to increased intracranial pressure.
Levothroid 200 mcg line
Ask the patient about the pattern of attacks; some mistake severe gallbladder attacks for a heart attack until they recall similar thyroid symptoms cats levothroid 100mcg fast delivery, less severe episodes that have preceded it. An acute attack of cholecystitis is often associated with gallstones, or cholelithiasis. The classic symptom is pain in the right upper quadrant that may radiate to the right scapula, called biliary colic. If the flow of bile has become obstructed, the patient may pass clay-colored stools and dark urine. The pain may radiate to the right shoulder or scapula and may be accompanied by nausea and vomiting. The patient with an acute gallbladder attack appears acutely ill, is in a great deal of discomfort, and sometimes is jaundiced. A low-grade fever is often present, especially if the disease is chronic and the walls of the gallbladder have become infected. Right upper quadrant pain is intense in acute attacks and requires no physical examination. A positive Murphy sign, which is positive palpation of a distended gallbladder during inhalation, may confirm a diagnosis. Elderly people may present with vague symptoms such as localized tenderness and without pain and fever. The patient with an acute attack of cholelithiasis may be in extreme pain and very upset. The experience may be complicated by guilt if the patient has been advised by the physician in the past to cut down on fatty foods and lose weight. Supporting tests include phosphatase, aspartate amino transferase, lactate dehydrogenase, alkaline phosphatase, serum amylase, and serum bilirubin levels; oral cholecystogram; and computed tomography. Antibiotics may be given to manage infection along with bowel rest, intravenous hydration, correction of electrolyte imbalances, and pain management with follow-up care. Criteria for outpatient treatment include that the patient is febrile, with no evidence of obstruction on laboratory assessment and sonogram, no underlying medical problems, adequate pain control, and proximity to an acute care facility if needed from home. However, given the effectiveness of laparoscopic cholecystectomy, the only patients who will receive medical dissolution are generally those who are nonobese patients with very small cholesterol gallstones and a functioning gallbladder. The one seen most commonly today is a laparoscopic cholecystectomy, which is performed early (within 48 hours of acute onset of symptoms) in the course of the disease when there is minimum inflammation at the base of the gallbladder. It is considered the standard of care for the surgical management of cholecystectomy. The procedure is performed with the abdomen distended by an injection of carbon dioxide, which lifts the abdominal wall away from the viscera and prevents injury to the peritoneum and other organs. A laparoscopic cholecystectomy is done either as an outpatient procedure or with less than 24 hours of hospitalization. After the surgery, the patient may complain of pain from the presence of residual carbon dioxide in the abdomen. The traditional open cholecystectomy is performed on patients with large stones as well as with other abnormalities that need to be explored at the time of surgery. This procedure is particularly appropriate up to 72 hours after onset of acute cholecystitis. Early cholecystectomy has the advantage of resolving the acute condition early in its course. Delayed cholecystectomy can be performed after the patient recovers from initial symptoms and acute inflammation has subsided, generally 2 to 3 months after the acute event. Extracorporeal shock wave lithotripsy, similar to the type used to dissolve renal calculi, is now also used for small stones. For those patients who are not good surgical candidates, both methods have the advantage of being noninvasive. However, they have the disadvantage of leaving in place a gallbladder that is diseased, with the same propensity to form stones as before treatment. The anticholinergics relax the smooth muscle, preventing biliary contraction and pain. If inflammation of the gallbladder has led to gallstones and obstruction of bile flow, replacement of the fat-soluble vitamins is important to supplement the diet. Bile salts may be prescribed to aid digestion and vitamin absorption as well as to increase the ratio of bile salts to cholesterol, aiding in the dissolution of some stones. Independent During an acute attack, remain with the patient to provide comfort, to monitor the result of interventions, and to allay anxiety. Although most patients return from surgery or a procedure breathing on their own, if stridor or airway obstruction occurs, create airway patency with an oral or nasal airway and notify the surgeon immediately. The high incision makes deep breathing painful, leading to shallow respirations and impaired gas exchange. Splinting the incision while encouraging the patient to cough and breathe deeply helps both pain and gas exchange. Cholecystitis and Cholelithiasis 277 Patients not undergoing surgery or a procedure need a thorough education. Teach the patient to avoid high-fat foods; dairy products; and, if the patient is bothered by flatulence, gas-forming foods. Cost-effectiveness of emergency versus delayed laparoscopic cholecystectomy for acute gallbladder pathology. They examined the cost-effectiveness of emergency versus delayed cholecystectomy for acute gallbladder disease. The patients in the emergency group had the surgery during the time of the emergency admission. Those in the delayed group were admitted as an emergency and then readmitted for surgery at a later date. The authors concluded that using the emergency procedures was more efficient and effective in terms of quality of life. After a laparoscopic cholecystectomy, provide discharge instructions to a family member or another responsible adult as well as to the patient because the patient goes home within 24 hours after surgery. Explain the possibility of abdominal and shoulder pain caused by the instillation of carbon dioxide so that if the pain occurs, the patient will not experience unnecessary anxiety about a heart attack. Teach the patient to avoid submerging the abdomen in the bathtub for the first 48 hours, to take the prescribed antibiotics to provide further assurance against infection, and to watch the incisions for signs of infection. Following a 3- to 5-day hospital stay for an open cholecystectomy, instruct the patient on the care of the abdomen wound, including changing the dressing and protection of any drains. Reinforce pain control and deep-breathing exercises until the incision is completely healed. The continued use of opiate-type analgesics for 7 to 10 days may necessitate the use of laxatives or suppositories, which are generally prescribed by the physician before discharge. Explain that gradual resumption of both a normal diet and activity aids normal elimination. Instruct the patient to report to the physician if any new symptoms occur, such as the appearance of jaundice accompanied by pain, chills and fever, dark urine, or light-colored stools. Usually, the patient has no complications and is able to resume normal activity within a few weeks. Instruct the patient who has been treated nonsurgically with bile salts or extracorporeal shock wave lithotripsy about a low-fat diet to avoid recurrence of gallstones. Leukocytes in the membranes are maternal in origin; leukocytes in the amniotic fluid (amnionitis) or in the umbilical cord (funisitis) are fetal in origin. Chorioamnionitis, which can occur with subtle or acute signs and symptoms, can happen at any time during the prenatal or intrapartal period. Chorioamnionitis can also cause premature rupture of the membranes and preterm labor. In fact, chorioamnionitis is associated with a neonatal mortality rate of 1% to 4% for term infants and up to 10% for preterm infants. Occasionally, pelvic inflammatory disease can develop if the infection is not totally resolved. The prognosis for the infant varies depending on the degree of infection that is transmitted to the fetus.
Syndromes
- Provide an unbreakable mirror
- Lymphocytes: 20% to 40%
- Children: 15 to 40
- Abnormal nerve reflexes
- Unusual looking face
- Damage to the blood vessels
- Clipping used to be the most common way to repair an aneurysm. This is done during an open craniotomy.
- Nuclear medicine, which includes such tests as a bone scan, thyroid scan, and thallium cardiac stress test
- Heimlich maneuver on self
- Meningitis - H. influenzae
Order levothroid 100 mcg on-line
Review article: Maximising quality of life while aspiring for quantity of life in end-state liver disease thyroid symptoms wrinkled fingers levothroid 200 mcg on-line. They recommended early recognition and management of these complications, along with early palliative care, to improve quality end-of-life care. Assist the patient to individualize a diet plan to maximize personal choices, including a dietitian if necessary. Encourage sodium-restricted patients to read labels on all canned soups, sauces, and vegetables and on all over-the-counter medications. Be sure the patient understands any pain medication prescribed, 712 Lung Cancer including dosage, route, action, and side effects. Teach the patient and family the need to limit the rise of infections by good hand washing, avoidance of others with colds, and prompt treatment by a healthcare provider when an infection occurs. The Centers for Disease Control and Prevention also reported that it is the second-most common cancer diagnosis after breast cancer for women and prostate cancer for men. It accounts for 28% of all cancer deaths and accounts for more deaths than prostate, breast, and colon cancer combined. The American Cancer Society reports that annually, more than 220,000 people are diagnosed with lung cancer and 160,000 die from the disease. The 1-year survival rate remains approximately 41%, and the 5-year survival rate is 15%, depending on stage and type of cancer. Only 16% of lung cancers are found at an early, localized stage, when the 5-year survival rate is 49%. Sometimes a lung cancer shows characteristics of both types and is labeled small cell/large cell carcinoma. They start multiplying quickly into large tumors and can spread to the lymph nodes and other organs. At the time of diagnosis, approximately 70% have already metastasized, often to the brain. Squamous cell carcinoma, also associated with smoking, tends to be located centrally, near a bronchus, and accounts for approximately 25% to 30% of all lung cancers. Adenocarcinoma, accounting for 40% of all large cell carcinoma, is usually found in the outer region of the lung. One type of adenocarcinoma, bronchioloalveolar carcinoma, tends to produce a better prognosis than other types of lung cancer and is sometimes associated with areas of scarring. Large cell undifferentiated carcinoma starts in any part of the lung, grows quickly, and results in a poor prognosis owing to early metastasis; approximately 10% to 15% of lung cancers are large cell undifferentiated carcinoma. L Lung Cancer 713 the hilus of the lung, close to the larger divisions of the bronchi, is the most frequent site of lung cancer. As the cells grow into a carcinoma, they make the bronchial lining irregular and uneven. The tumor may penetrate the lung wall and surrounding tissue or grow into the opening (lumen) of the bronchus. In more than 50% of patients, the tumor spreads into the lymph nodes and then into other organs. Systemic effects of the lung tumor that are unrelated to metastasis may affect the endocrine, hematologic, neuromuscular, and dermatologic systems. These changes may cause connective tissue and vascular abnormalities, referred to as paraneoplastic syndromes. Complications of lung cancer include emphysema, bronchial obstruction, atelectasis, pulmonary abscesses, pleuritis, bronchitis, and compression on the vena cava. In particular, squamous cell and small cell carcinoma are associated with smoking. Other risk factors include exposure to carcinogenic industrial and air pollutants. Of the total number of deaths from lung cancer each year, 57% are men and 43% are women. There has been an observable decline in deaths among younger men, and this is probably related to the diminishing number of young men who smoke. Deaths among women have been rising, although the rate of increase has slowed in recent years. Incidence rates appear to be higher in African American men than in white or Asian American men. The World Health Organization expects the number of new cases to rise by 70% over the next two decades. Tobacco use is the most important causal agent for cancer worldwide and is estimated to cause 22% of all cancer deaths. The global incidence of lung cancer is approximately 13 per 100,000 females per year and 31 per 100,000 males per year. The incidence is four to five times higher in developed than in developing countries, with the highest incidence in Hungary, Serbia, Poland, and Korea. As smoking rates increase in developing countries such as India and China, experts expect rates of lung cancer to increase. While most patients will have a history of tobacco use, many will not report symptoms of lung cancer until they have advanced disease. Establish a history of persistent cough, chest pain, dyspnea, weight loss, or hemoptysis. Ask if the patient has experienced a change in normal respiratory patterns or hoarseness. Some patients initially report pneumonia, bronchitis, epigastric pain, symptoms of brain metastasis, arm or shoulder pain, or swelling of the upper body. Ask if the sputum has changed color, especially to a bloody, rusty, or purulent hue. Obtain a smoking history with the type of tobacco use and the quantity and frequency of use. Elicit a history of exposure to risk factors by determining if the patient has been exposed to industrial or air pollutants. The clinical manifestations of lung cancer depend on the type and location of the tumor. Because the early stages of this disease usually produce no symptoms, it is most often diagnosed when the disease is at an advanced stage. In 10% to 20% of patients, lung cancer is diagnosed without any symptoms, usually from an abnormal finding on a routine chest x-ray. Approximately 25% have regional metastasis and 55% have distant metastasis with symptoms that reflect the organ affected (brain, spinal cord, bone, liver). Note rapid, shallow breathing and signs of an airway obstruction, such as extreme shortness of breath, the use of accessory muscles, abnormal retractions, and stridor. Typically, pleural effusion causes dullness on percussion and breath sounds that are decreased below the effusion and increased above it. Monitor the patient for oxygenation problems, such as increased heart rate, decreased blood pressure, or an increased duskiness of the oral mucous membranes. Metastases to the mediastinal lymph nodes may involve the laryngeal nerve and may lead to hoarseness and vocal cord paralysis. The superior vena cava may become occluded with enlarged lymph nodes and cause superior vena cava syndrome; note edema of the face, neck, upper extremities, and thorax. The patient undergoes major lifestyle changes as a result of the physical side effects of cancer and its treatment. The patient is faced with a psychological adjustment to the diagnosis of a chronic illness that frequently results in death. Unless the tumor is small without metastasis or nodes when discovered, it is often not curable. Surgical treatment ranges from segmentectomy or wedge resection (removal of a part of a lobe) to lobectomy (removal of a section of the lung) to pneumonectomy (removal of an entire lung). These procedures all require general anesthesia and a thoracotomy (surgical incision in the chest). Video-assisted thoracoscopic surgery is a minimally invasive procedure used for both diagnosis and treatment. It involves a shorter hospital stay, less pain, and a lower perioperative mortality. Outcome measures along with recurrence rates are currently being followed and compared with those from more invasive procedures. If patients are unable to undergo a thoracotomy because of other serious medical problems or widespread cancer, laser surgery 716 Lung Cancer may be performed to relieve blocked airways and diminish the threat of pneumonia or shortness of breath.
Purchase levothroid 50 mcg line
Obtain a diet history to determine the normal sodium and fluid consumption patterns thyroid lab values order 50mcg levothroid visa. Ask the patient and family if they have noted any change in mental status or behavior. Often, the patient with hyponatremia experiences confusion, a flat affect, and personality changes. Symptoms vary depending on the extent of the electrolyte imbalance and the speed that it develops. Slowly developing hyponatremia may be asymptomatic, whereas more rapidly progressing imbalances may be accompanied by headache, muscle cramps, confusion, reduced mental awareness, and coma. In hyponatremia, a low diastolic blood pressure, tachycardia, orthostatic hypotension, and a weak pulse may be noted. Assess the patient for decreased muscle strength and decreased deep tendon reflexes. Auscultate the lung fields bilaterally and note that you may hear adventitious breath sounds with congestive heart failure. Auscultate the bowel sounds and note any hyperactivity that may accompany hyponatremia. Assess the patient for anxiety, hostility, and the level of orientation to reality. The patient may progress rapidly from confusion and agitation to seizure activity or coma. Hypovolemic hyponatremic patients should be treated with isotonic saline to correct the volume deficit. If hyponatremia is severe (serum sodium 115 mEq/L), an infusion of 3% to 5% sodium Hyponatremia 607 chloride solution may be administered slowly in small volumes via an infusion device. Monitor the patient carefully for signs and symptoms of circulatory overload (dyspnea, crackles, engorged veins). A diuretic may be given concurrently to avoid the occurrence of circulatory overload. Monitor the effectiveness of fluid administration by following the serum sodium and osmolality levels, as well as daily weights and intake and output. Hypervolemic or edematous patients are treated with a fluid restriction: 800 to 1,000 mL of fluid is allowed per day. If indicated, encourage the patient to drink liquids high in sodium, such as broth. Report the signs and symptoms of water intoxication (increased irritability, change in sensorium, headache, hyperreflexia) to the physician immediately. If the patient is confused, provide frequent orientation to person, place, and time. Because seizures are a possible consequence of hyponatremia, institute seizure precautions. Keep the side rails padded and raised, if that is appropriate for the patient, and the bed in the low position. In addition, alterations in magnesium, phosphate, and calcium may all change neurological function and cognition. If fluid restriction is indicated, tell the patient that using ice chips, iced pops, or lemon drops may reduce thirst. Teach the family that hyponatremia can recur with persistent vomiting or diarrhea because sodium is abundant in the gastrointestinal tract; this fact is especially important for infants, children, and elderly and debilitated patients. Calcium and phosphorus have a reciprocal relationship in the body; high levels of calcium lead to low levels of phosphorus. Although both hypocalcemia and hyperphosphatemia result from hypoparathyroidism, hypocalcemia accounts for the majority of clinical manifestations. The seriousness of the disease is variable with the degree of hypocalcemia and the speed with which it develops. Acute hypoparathyroidism follows swiftly after trauma or removal of the parathyroid glands. The acute form, as with most hormone deficiencies, can result in life-threatening complications such as tetany, hypocalcemic seizures, cardiac dysrhythmias, and respiratory obstruction caused by laryngospasm. Most clinical manifestations are reversible with treatment; those caused by calcification deposits associated with chronic hypoparathyroidism (such as cataracts, malformed teeth) and parkinsonian symptoms are not. Acquired hypoparathyroidism is irreversible and is most commonly caused by damage to or removal of the parathyroid gland therapeutically (parathyroidectomy) to treat hyperparathyroidism. Some patients receive an autotransplantation of a segment of a parathyroid gland in the forearm or neck to prevent hypoparathyroidism after a parathyroidectomy. Acquired hypoparathyroidism may also occur as an Hypoparathyroidism 609 iatrogenic complication during thyroid or other neck surgery in about 1% to 3% of all patients postoperatively, but with repeated neck explorations, the incidence increases to 10%. Reversible hypoparathyroidism occurs in children before age 16 as a result of a rare autoimmune disease. It has also been known to occur as a rare side effect of 131I treatment for Graves disease or with metastases of malignant tumors. No specific life span considerations exist, although most people living with hypoparathyroidism are over the age of 40. In several epidemiological studies in the United States and Europe, 75% of the people with hypoparathyroidism were female and 25% were male. History may reveal damage to the parathyroid glands during some form of neck surgery. Signs of hypocalcemia- such as paresthesia (numbness and tingling in the extremities), increased anxiety, headaches, irritability, and sometimes depression- may be reported. Some patients complain of difficulty swallowing, hoarseness, wheezing, or throat tightness. Most common symptoms are numbness and tingling of the extremities and around the mouth, anxiety and irritability, muscle cramps, seizures, hoarseness, and wheezing. Note dry skin, thin hair with patchy areas of hair loss, ridged fingernails, and teeth in poor condition. The patient may have neuromuscular irritability with involuntary tremors and muscle spasms. Check for Trousseau sign (development of a carpal spasm when a blood pressure cuff is inflated above systolic pressure for 3 minutes) and Chvostek sign (twitching facial muscles when the facial nerve is tapped anterior to the ear). Patients may have altered behavior, exhibiting irritability, depression, and anxiety. The patient and significant others may describe an inability to cope with the physical manifestations of the disease and the stressors of daily life. Note that alkalosis augments calcium binding to albumin and increases the severity of symptoms of hypocalcemia. When the patient is acutely hypocalcemic, generally calcium chloride or gluconate is rapidly administered intravenously. Hypoparathyroidism 611 Give oral calcium supplements with meals but not with foods that interfere with calcium absorption, such as chocolate. The individual with hypoparathyroidism needs a diet that is rich in calcium, low in phosphorus, and includes a high fluid and fiber content. Alkalosis worsens the symptoms of hypocalcemia because more free calcium binds with proteins when the blood pH increases. Strategies that increase carbon dioxide retention, such as breathing into a paper bag or sedating the patient, can control muscle spasm and other symptoms of tetany until the calcium level is corrected. In addition to a careful, ongoing assessment for the symptoms of hypocalcemia, the patient should have a calm environment. Tell the patient to notify you immediately if he or she has difficulty swallowing or has tightness in the throat. Once the acute phase is over and the patient has been switched to oral medications and foods, begin patient teaching about a diet high in calcium and medications. The neuromuscular irritability and weakness place the patient at increased risk for falls. Assist the patient to identify both stressors and coping mechanisms to deal with the stressors. In particular, the patient needs to learn to avoid stressors such as fatigue and infection. Milk, milk products, meat, poultry, fish, egg yolks, and cereals, although high in calcium, should be limited because of their phosphorus content. Remind the patient to take medications exactly as prescribed and not to substitute over-thecounter medications for prescribed calcium.
Levothroid 200 mcg cheap
Approximately one-third of all hemophiliacs have no family history of bleeding disorders thyroid symptoms low cheap 100 mcg levothroid, which indicates that there may be factors other than heredity involved and that the illness is a result of a new mutation. Daughters of men with hemophilia are obligate carriers, but sons of affected men are normal. When a carrier woman has a son, his risk of disease is 50% and each of her daughters has a 50% risk of also being a carrier. Female offspring have a 50% chance of being affected with hemophilia if an affected male mates with a carrier female. Most females with the defective gene do not develop clinical manifestations because they usually inherit a normal X chromosome from the other parent. Hemophiliac males do not transmit the disease to their sons because the Y chromosome is not affected. However, all daughters of afflicted males become carriers of the trait because they inherit the defective X chromosome. Half of the daughters become carriers, and half of their sons have manifestations of hemophilia. Hemophilia A and B are found in all ethnic and racial groups, although a lower prevalence may exist in the Chinese population. Bleeding abnormalities associated with hemophilia are usually noticed when the child becomes active and learns to walk, but mild cases may go undetected until adulthood. Approximately 40% of children have their first bleeding during their first year of life, and by age 4, 90% of children with hemophilia have had episodes of persistent bleeding from minor injuries. Bleeding episodes seem to decrease at or after adolescence, which may be because of the decreased risk of trauma as well as stabilization of the disease process. Experts suggest that about 10,000 infants are born with hemophilia each year worldwide. Underdiagnosis of hemophilia in developing nations is a critical problem because of little access to care, no money for screening, lack of diagnostic tests to identify patients, and no factor replacement therapies. Estimates of nondiagnosis are as high as 75% in developing nations, and many infants born with hemophilia die during childhood. Question the patient, parents, or caregiver about any history of prolonged bleeding episodes, either spontaneous or following any injury in the patient or family. Ask if the patient has any signs of internal bleeding or excessive blood loss like weakness, lethargy, fast heart rate, or orthostasis. The hemorrhage extends from this center concentrically, with each successive outer circle becoming lighter in color. Signs of excessive blood loss are tachycardia, hypotension, shortness of breath, dizziness, and orthostatic changes in blood pressure. Bleeding disproportionate to the extent of a traumatic injury is characteristic of hemophilia. Typically, the bleeding is an intermittent oozing type that develops over several hours or days after the injury or procedure. Acute hemarthrosis is often preceded by a warm tingling sensation in the affected joint. If absorption of the blood from around the periarticular structures is incomplete, the remaining blood can cause chronic inflammation of the synovial membranes. Other long-term clinical sequelae of hemarthrosis include impaired joint mobility, bone deformity and demineralization, and stunted growth. Approximately 40% of hemophilia patients have splenomegaly; there have been some reported cases of spontaneous splenic rupture. Patients with hemophilia and their families contend with the challenges of a rare chronic illness and the constant threat of life-threatening hemorrhage. Children often feel isolated from their peers because of the activity restrictions. Also, children who have a greater understanding of hemophilia and its treatment are less likely to experience psychological distress. The current recommendation is to use recombinant (synthetic) products initially and thereafter in all newly diagnosed cases. Intracranial hemorrhage is the most common cause of death in people with hemophilia; approximately 50% of these are associated with acute head injury. Pharmacologic Highlights Medication or Drug Class Desmopressin, 1deamino-8-darginine vasopressin Dosage 0. Independent To prevent trauma that may precipitate bleeding episodes, avoid intramuscular injections and minimize the number of venipuncture attempts. Avoid sources of mucosal irritation such as rectal temperatures, urinary catheters, and suppositories. Ensure that tourniquets or blood pressure cuffs are applied no longer than necessary. Perform nasopharyngeal or oropharyngeal suctioning very gently and only when needed. Prevent skin breakdown through the use of frequent turning and preventive skin care. When bleeding occurs, apply firm, direct pressure for at least 5 minutes or until bleeding has stopped completely to sites of subcutaneous injections and venipuncture sites. Use sandbags and pressure dressings to maintain pressure on large puncture sites after hemostasis has been established. Initiate mobilization within a few days after the bleeding is controlled to facilitate restoration of normal joint range of motion. Encourage the patient and family members to verbalize their feelings openly and clearly with staff and with each other. The articles point to the unique challenge of living with the psychological, social, and medical consequences of a lack of knowledge about the condition in both the social and healthcare settings. Emphasize the importance of carrying identifying medical information at all times. Describe immediate actions the patient or caregiver should take to control bleeding. Teach the patient or caregiver the purpose of each medication, the correct procedure for administration, and potential adverse effects. Provide the patient or family with a list of referrals for genetic counselors, social workers, vocational counselors, or psychologists to assist in the long-term adjustment as necessary. In the United States, at least 10 million people have hemorrhoids, and up to one-third of these people seek treatment. Internal hemorrhoids, produced by dilation and enlargement of the superior plexus, cannot be seen because they are above the anal sphincter, whereas external hemorrhoids, produced by dilation and enlargement of the inferior plexus, are below the anal sphincter and are apparent on inspection. Hemorrhoids develop when increased intra-abdominal pressure produces increased systemic and portal venous pressure, thus causing increased pressure in the anorectal veins. The arterioles in the anorectal area send blood directly to the swollen anorectal veins, further increasing the pressure. Recurrent and repeated increased pressure causes the distended veins to separate from the surrounding smooth muscle and leads to their prolapse (enlarged internal hemorrhoids that actually protrude through the anus). Some factors associated with increased pressure and hemorrhoids are occupations that require prolonged sitting or standing; heart failure; anorectal infections; anal intercourse; alcoholism; pregnancy; colorectal cancer; and hepatic disease such as cirrhosis, amoebic abscesses, or hepatitis. Straining because of diarrhea, coughing, sneezing, or vomiting and loss of muscle tone because of aging, rectal surgery, or episiotomy can also cause hemorrhoids. Experts also suggest that prolonged sitting on the toilet while reading leads to reduced venous return and enlarged hemorrhoids. A familial tendency toward weak rectal vein walls and/or valves and varicose veins would increase susceptibility. Young people who are engaged in heavy weightlifting and exercise are prone to hemorrhoids, and college students who do not eat balanced diets or who eat low-fiber diets are also at risk. Men and people with high socioeconomic status are more likely to pursue medical care for the treatment of hemorrhoids than women and people from underresourced communities. In later life, congestive heart failure and obesity contribute to the development of hemorrhoids. There are no known racial or ethnic considerations with respect to prevalence, but people requesting treatment are most likely to be white/European American, with middle or upper range in income. Establish a history of anal itching, blood on the toilet tissue or in the toilet bowl after a bowel movement, and anorectal pain or discomfort. The most common symptoms are anal itching, rectal bleeding after a bowel movement, and anorectal pain.
Generic levothroid 100 mcg
A quiet thyroid symptoms prevention order levothroid without prescription, wellorganized environment at a temperature comfortable for the patient ensures rest and recovery. If the patient experiences pruritus, help the patient clip the fingernails short and keep the nail tips smooth. Use skin emollients liberally, avoid harsh soaps, and bathe the patient only when necessary. Frequent turning and range-of-motion exercises assist in preventing skin breakdown. If the patient is taking medications that cause frequent stools, clean the perineum and buttocks frequently to maintain skin integrity. Before contacting the physician about a decreasing urinary output in an acutely or critically ill patient, make sure that the catheter is patent. If institutional policy permits, irrigate the Foley catheter using sterile technique with 30 mL of normal saline to check for obstruction. If institutional policy permits, replace the indwelling Foley catheter with a new catheter and urinary drainage system to ensure it is functioning adequately. If the patient is on bedrest, maintain the bed in the low position and keep the side rails up. Provide the patient with ongoing, repeated information about what is happening and why. Early versus late initiation of renal replacement therapy in patients with acute kidney injury: A meta-analysis of randomized clinical trials. Patients who have recovered viable renal function still need to be monitored by a nephrologist for at least a year. Teach the patient that she or he may be more susceptible to infection than previously. Explain that the patient should tell the healthcare professional about the medications if the patient needs treatment such as dental work or if a new medication is added. Patients who have not recovered viable renal function need to understand that their condition may persist and even become chronic. If chronic renal failure is suspected, further outpatient treatment and monitoring are needed. Discuss with significant others the lifestyle changes that may be required with chronic renal failure. Since World War I, terms such as stiff lung, wet lung, shock lung, adult hyalinemembrane disease, and others were used to describe the acute respiratory distress that occurs after catastrophic events such as major surgical procedures, serious injuries, or other critical infections. They have bilateral pulmonary infiltrates and severe hypoxemia, but these changes are not due to heart failure. Other contributors include bacterial toxins and oxygen free radicals, among others. The onset of symptoms generally occurs within 24 to 72 hours of the original injury or illness. This deficiency is thought to be partly responsible for the alveolar collapse and the decrease in lung volumes that occur. In addition, fibroblasts proliferate in the alveolar wall, migrate into the intra-alveolar fluid, and ultimately convert the exudate (fluid with high concentration of protein and cellular debris) into fibrous tissue. Refractory hypoxemia occurs as the lungs are perfused but not ventilated (a condition called capillary shunting) owing to the damage to the alveoli and developing fibrosis. Complications include pneumothorax, infection, ventilator-associated pneumonia, inadequate nutrition, hemorrhage, and deep vein thrombosis. These conditions can be classified into two categories: direct lung injury and indirect lung injury. Direct injury occurs from situations such as gastric aspiration, near drowning, chemical inhalation, and oxygen toxicity. Indirect injury occurs from mediators released during sepsis, multiple trauma, thermal injury, pancreatitis, hypoperfusion or hemorrhagic shock, disseminated intravascular coagulation, drug overdose, and massive blood transfusions. Mortality rates vary and have been estimated to be between 30% and 50%, but older patients and patients with severe infections have a higher rate. Survivors generally have almost normal lung function a year after the acute illness. People over 70 years of age have a higher incidence and rate of mortality than younger persons. Hypoxemia usually leads to restlessness, confusion, agitation, and even combative behavior. Blood pressure may be normal or elevated initially and then decreased in the later stages. If airway and breathing are not maintained, the patient becomes fatigued and apneic. When the patient is intubated and mechanically ventilated, the lungs may sound extremely congested, with wheezes and coarse crackles throughout. Patients may exhibit anxiety and fear because of hypoxemia and the real threat of death. Feelings of social isolation and powerlessness can occur as the patient is placed on mechanical ventilation and is unable to verbalize. The family and significant others will exhibit anxiety, fear, and significant concern. Other supporting tests include pulmonary function tests, pulse oximetry, and pulmonary capillary wedge pressure. Common methods for mechanical ventilation include pressure-controlled ventilation with an inverse inspiratory-expiratory ratio. This mode alters the standard inspiratory-expiratory ratio of 1:2 to 1:3 by prolonging the inspiratory rate and changing the ratio to 1:1 or even higher. Another strategy includes improving oxygenation by turning patients from the supine to a prone position, with care to keep all tubes and intravenous devices intact. Nutrition support, generally with enteral nutrition delivered by a feeding tube, is recommended after 48 hours of the start of mechanical ventilation. Simvastatin, a hydroxymethylglutaryl-coenzyme A reductase inhibitor, may improve oxygenation and respiratory mechanics in some patients. While inhaled nitric oxide may improve oxygenation, its administration has not improved survival rates. Medication or Drug Class Neuromuscular blocking agents: vecuronium (Norcuron), rocuronium (Zemuron), atracurium (Tracrium), cisatracurium (Nimbex) Propofol (Diprivan) Dosage Dosage varies with drug Description Increases chest wall compliance and minimizes the work of breathing Rationale Used to paralyze the skeletal muscles when patients are difficult to ventilate with poor gas exchange; must be used with analgesics and sedation To sedate the patient to decrease work of breathing and decrease stress of the intensive care unit and mechanical ventilation experience 0. Prior to suctioning, hyperventilate and hyperoxygenate the patient to prevent the ill effects of suctioning, such as cardiac dysrhythmias or hypotension. Turn the patient as often as possible, even every hour, to increase ventilation and perfusion to all areas of the lung. Although restraints are frustrating for the patient, they may be necessary to reduce the risk of self-extubation. If the patient requires neuromuscular blocking agents for skeletal muscle paralysis, provide complete care and make sure the medical management includes sedation. Reposition the patient at least every 2 hours for comfort and adequate gas exchange and to prevent skin breakdown. Assist the patient to conserve oxygen and limit oxygen consumption by spacing all activities, limiting interruptions to enhance rest, and providing a quiet environment. Answer all questions and provide methods for the patient and family to communicate, such as a magic slate or point board. Patients may need physical therapy to restore muscular strength after a debilitating illness. Addison disease, or primary adrenal insuf- ficiency, occurs rarely, but when it occurs, there is loss of at least 90% of the adrenal cortex. The medulla is responsible for the secretion of the catecholamines epinephrine and norepinephrine; the cortex is responsible for the secretion of glucocorticoids, mineralocorticoids, and androgen. The principal glucocorticoid, cortisol, helps regulate blood pressure, metabolism, anti-inflammatory response, and emotional behavior. The principal mineralocorticoid, aldosterone, is important for regulating sodium levels. Adrenal insufficiency is characterized by the decreased production of cortisol, aldosterone, and androgen. Cortisol deficiency causes altered metabolism, decreased stress tolerance, and emotional lability. Aldosterone deficiency causes urinary loss of sodium, chloride, and water, resulting in dehydration and electrolyte imbalances.
