
Discount hydrochlorothiazide 25mg mastercard
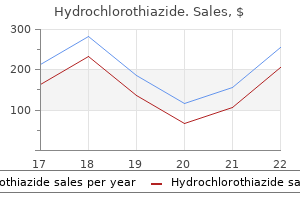
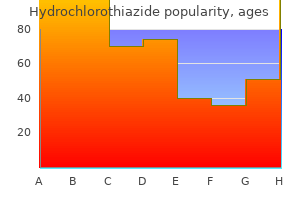
As they are renally excreted hypertension 33 weeks pregnant purchase hydrochlorothiazide without prescription, they can cause accumulation in patients with renal insufficiency. It can cause delirium, hyper-reflexia, myoclonus, and seizures in any patient following overdose, long-term use, especially in patients with renal insufficiency. Due to the short duration of action and the potential for toxicity, pethidine should only be used for short-term (48 hours) management of pain. Pethidine should not be used in elderly patients or in those with renal insufficiency, hepatic insufficiency, pre-existing 290 14. On the transdermal route, the onset of pain is delayed up to 12 hours; however, on subsequent administration, the analgesic effect is sustained for prolonged periods in patients. However, it has the analgesic activity and side effects similar to those of codeine but less antitussive action. Its dextro form is found to be analgesic; therefore, it is used as dextropropoxyphene. It is absorbed well after oral administration reaching higher concentration at 1 to 2 hours. The average half-life is longer than codeine and it is metabolized into norpropoxyphene which is reported to have a half-life of more than 30 hours. In moderate toxic doses, norpropoxyphene is reported to show respiratory depression, convulsions, delusion, hallucination, confusion, cardiac side effects, etc. Buprenorphine is very lipophilic and has a longer duration of action due to its high affinity for the opioid receptors when compared to morphine. Because of the partial agonist activity, buprenorphine provides a "ceiling effect," causing less euphoric effects and a lower abuse potential than that of full agonists. Certain formulations (for example, sublingual and subdermal) are approved for use in medication-assisted treatment of opioid addiction due to its ability to provide prolonged suppression of opioid withdrawal, the ability to block other agonists, and less frequent dosing requirements. In contrast to methadone, which is available only at specialized clinics when used for opioid detoxification or maintenance, buprenorphine is approved for office-based treatment of opioid dependence. Adverse effects include respiratory depression that cannot easily be reversed by naloxone and decreased (or, rarely, increased) blood pressure, nausea, and dizziness. Buprenorphine is used in opiate detoxi cation because it has a less severe and shorter duration of withdrawal symptoms compared to methadone. Severity of withdrawal Heroin Buprenorphine Methadone 0 5 10 Days since last drug dose Symptoms last longest with methadone, but are less severe than those of heroin withdrawal. Pentazocine produces less euphoria compared to morphine, but in higher doses respiratory depression, increased blood pressure, tachycardia, and hallucinations can occur. Pentazocine should be used with caution in patients with angina or coronary artery disease, since it can increase blood pressure. Butorphanol is available in a nasal spray that has been used for severe headaches, but it has been associated with abuse. Their propensity to cause psychotomimetic effects is less than that of pentazocine. It is used to manage moderate-to-severe acute and chronic pain, including neuropathic pain associated with diabetic peripheral neuropathy. Because tapentadol does not produce active metabolites, dosing adjustment is not necessary in mild-to-moderate renal impairment. As with other agents that bind the opioid receptor, tramadol has been associated with misuse and abuse. Diphenoxylate and loperamide Diphenoxylate and loperamide are used for the treatment of diarrhea. Therefore, diphenoxylate is combined with atropine to reduce the chance of abusing liability. Definoxin is a metabolite of diphenoxylate which is also being marketed along with atropine as a fixed-dose combination. Abdominal cramps and constipation are the common side effects observed with these agents. In opioid-dependent patients, antagonists rapidly reverse the effect of agonists, such as morphine or any full agonist, and precipitate the symptoms of opioid withdrawal. Since naloxone has a half-life of 30 to 81 minutes, a patient who has been treated for an overdose and recovered may lapse back into respiratory depression, depending on the opioid ingested and dosage form of that opioid. Naloxone is available in an autoinjector and a nasal inhaler for community distribution for treatment of opioid overdose involving heroin 294 14. It is imperative that prescribers counsel the patient and family members regarding the availability of these products, proper instructions for use, and the importance of calling emergency services in the case of overdose. Naltrexone has been reported to cause hepatotoxicity, and monitoring of hepatic function is recommended. A morphine overdose can be effectively treated with naloxone, and morphine is a phenanthrene. Naloxone antagonizes the opioid by displacing it from the receptor, but there are cases in which naloxone is not effective. Pethidine is a phenylpiperidine, not a phenanthrene, and the active metabolite, norpethidine, is not reversible by naloxone. Naloxone is effective for fentanyl overdoses; however, fentanyl is a phenylpiperidine, and not a phenanthrene. It is very important to use a low dose and monitor closely for proper pain control and adverse effects. Pethidine should not be used for chronic pain, nor should it be used in a patient with renal insufficiency. Morphine is not the best choice due to the active metabolites that can accumulate in renal insufficiency. She reports that the pain has been uncontrolled with tramadol and it is decided to start treatment with an opioid. Buprenorphine has a much higher incidence of opioid-induced respiratory depression compared to other agonists. Buprenorphine has many dosage formulations and all formulations can be prescribed for the treatment of pain or opioid dependence. Buprenorphine has a lower incidence of opioid-induced respiratory depression compared to the agonists due to the ceiling effect created by the partial agonist activity. Buprenorphine is available in many different dosage formulations but these formulations are indicated for either pain management or medication-assisted treatment of opioid dependence, not both. Tapentadol has a unique mechanism of action in comparison to the other choices given. Tapentadol has a dual mechanism of action (agonist and norepinephrine reuptake inhibition) which has been shown to effectively treat neuropathic pain associated with diabetic peripheral neuropathy. All other agonists could help manage neuropathic pain, but in some situations, higher doses of opioids are needed to achieve efficacy. Based on the mechanism of action, which opioid could be considered in this patient to treat both nociceptive and neuropathic pain The equianalgesic potency of methadone is extremely variable based on many factors, and only providers familiar with methadone should prescribe this agent. The drug interactions associated with methadone are numerous due to the multiple liver enzymes that metabolize the drug. Hydrocodone is a commonly used short-acting agent that is commercially available in combination with either acetaminophen or ibuprofen. Fentanyl is available in formulations for treatment of breakthrough pain for cancer treatment.
Order 12.5mg hydrochlorothiazide
Azole antifungals Azole antifungals are made up of two different classes of drugsimidazoles and triazoles 1 5 buy hydrochlorothiazide 12.5mg cheap. In general, imidazoles are applied topically for cutaneous infections, whereas triazoles are administered systemically for the treatment or prophylaxis of cutaneous and systemic mycoses. The inhibition of ergosterol biosynthesis disrupts fungal membrane structure and function, which, in turn, inhibits fungal cell growth. Additionally, some strains of fungi develop efflux pumps that pump the drug out of the cell or have reduced ergosterol in the cell wall. Patients on concomitant medications that are substrates for this isoenzyme may have increased concentrations and risk for toxicity. It is the least active of all triazoles, with most of its spectrum limited to yeasts and some dimorphic fungi. It is highly active against Cryptococcus neoformans and certain species of Candida, including. It is the drug of choice for Cryptococcus neoformans after induction therapy with amphotericin Band flucytosine and is used for the treatment of candidemia and coccidioidomycosis. The most common adverse effects with fluconazole are nausea, vomiting, headache, and skin rashes. Antifungal Drugs of infections due to Candida and Aspergillus species because of the availability of more effective agents. The capsule and tablet should be taken with food, and ideally an acidic beverage, to increase absorption. By contrast, the solution should be taken on an empty stomach, as food decreases the absorption. Liver toxicity can also occur, especially when given with other hepatotoxic drugs. Drugs that increase gastric pH (for example, proton pump inhibitors) may decrease the absorption of oral posaconazole and should be avoided if possible. Voriconazole has replaced amphotericin B as the drug of choice for invasive aspergillosis. Inhibitors and inducers of these isoenzymes may impact levels of voriconazo/e, leading to toxicity or clinical failure, respectively. High trough concentrations have been associated with visual and auditory hallucinations and an increased incidence of hepatotoxicity. Because of significant interactions, use of voriconazole is contraindicated with many drugs (for example, rifampin, rifabutin, carbamazepine, and St. Echinocandins Echinocandins interfere with the synthesis of the fungal cell wall by inhibiting the synthesis of P(1,3)-o-glucan, leading to lysis and cell death. The echinocandins have potent activity against Aspergillus and most Candida species, including those species resistant to azoles. Caspofungin should not be coadministered with cyclosporine due to a high incidence of elevated hepatic transaminases with concurrent use. Micafungin is also indicated for the prophylaxis of invasive Candida infections in patients who are undergoing hematopoietic stem cell transplantation. Therapy is prolonged (usually about 3 months) but considerably shorter than that with griseofulvin. It may also be effective against Candida, Epidermophyton, and Scopulariopsis, but the efficacy in treating clinical infections due to these pathogens has not been established. The bioavailability after oral administration is only 40% due to first-pass metabolism. A prolonged terminal half-life of 200 to 400 hours may reflect the slow release from these tissues. The drug should be avoided in patients with moderate to severe renal impairment or hepatic dysfunction. Taste and visual disturbances have been reported, as well as elevations in serum hepatic transaminases. Naftifine cream and gel are used for topical treatment of tinea corporis, tinea cruris, and tinea pedis. Duration of therapy is dependent on the rate of replacement of healthy skin and nails. Ultrafine crystalline preparations are absorbed adequately from the gastrointestinal tract, and absorption is enhanced by high-fat meals. The drug is negligibly absorbed from the gastrointestinal tract, and it is not used parenterally due to systemic toxicity (acute infusion-related adverse effects and nephrotoxicity). Ciclopirox is active against Trichophyton, Epidermophyton, Microsporum, Candida, and Malassezia. Tavaborole is active against Trichophyton rubrum, Trichophyton mentagrophytes, and Candida albicans. A topical solution is approved for the treatment of toenail onychomycosis, requiring 48 weeks of treatment. Amphotericin B Is the best choice since nephrotoxicity Is commonly associated with this medication. Although the dose of fluconazole must be adjusted for renal insufficiency, it is not associated with causing nephrotoxicIty. Fluconazole, flucytosine and ketoconazole do not have reliable in vitro activity and ~re therefore not recommended. There is a black box warning that warns against the use of itraconazole in patients with evidence of ventricular dysfunction, Including patients with heart failure. Terbinafine Is better tolerated, requires a shorter duration of therapy, and is more effective than either itraconazole or griseofulvin. Mlcafungln, terblnaflne, and griseofulvin are not active for this type of infection. The treatment of choice for initial therapy for cryptococcal meningitis is the combination of amphotericin Band flucytosine. Flucytosine should not be given alone because of the rapid development of resistance. Caspofungin Is the only drug listed that requires a loading dose before starting the maintenance dosing. They lack both a cell wall and a cell membrane, and they do not carry out metabolic processes. However, a few virus groups respond to available antiviral drugs, and some antiviral agents are useful as prophylactic agents. However, antiviral agents are used when patients are allergic to the vaccine or outbreaks occur. Administered prior to exposure, neuraminidase inhibitors prevent infection and, when administered within 24 to 48 hours after the onset of symptoms, they modestly decrease the intensity and duration of symptoms. Mechanism of action: Influenza viruses employ a specific neuraminidase that is inserted into the host cell membrane for the purpose of releasing newly formed virions. Oseltamivirand zanamivirselectively inhibit neuraminidase, thereby preventing the release of new virions and their spread from cell to cell. Pharmacokinetics: Oseltamivir is an orally active prodrug that is rapidly hydrolyzed by the liver to its active form. Due to widespread resistance, the adamantanes are not recommended in the United States for the treatment or prophylaxis of influenza A. Adverse effects: Adverse effects of ribavirin include dose-dependent transient anemia. The aerosol may be safer, although respiratory function in infants can deteriorate quickly after initiation of aerosol treatment. Ribavirin Interferons are a family of naturally occurring, inducible glycoproteins that interfere with the ability of viruses to infect cells. In "pegylated" formulations, bis-monomethoxy polyethylene glycol has been covalently attached to interferon-a to increase the size of the molecule. The larger molecular size delays absorption from the injection site, lengthens the duration of action of the drug, and also decreases its clearance. Adverse effects: these include flu-like symptoms, such as fever, chills, myalgias, arthralgias, and Gl disturbances. The principal dose-limiting toxicities are bone marrow suppression, severe fatigue and weight loss, neurotoxicity characterized by somnolence and behavioral disturbances, autoimmune disorders such as thyroiditis and, rarely, cardiovascular problems such as heart failure.
Diseases
- Cervical hypertrichosis peripheral neuropathy
- Biliary atresia, intrahepatic, syndromic form
- Papular urticaria
- Thiele syndrome
- Hyperp Hypers
- Myhre Ruvalcaba Kelley syndrome
Purchase hydrochlorothiazide american express
Anticonvulsants such as valproic acid arteria rectalis superior hydrochlorothiazide 12.5 mg low cost, carbamazepine, and lamotrigitne have been used extensively either alone or as adjunct to lithium therapy. Although many cellular processes are altered by treatment with lithium, the mode of action is unknown. Adverse effects due to higher plasma levels may indicate toxicity and include ataxia, slurred speech, and coarse tremors. Treatment of toxicity includes discontinuation of lithium, hemodialysis, and the use of anticonvulsants. Therefore, caution should be used when dosing this drug in renally impaired patients. Sodium depletion results in increased renal reabsorption of lithium and increased chance for toxicity. Sodium depletion is increased by low-salt diets, thiazide diuretics, furosemide, ethacrynic acid, or severe diarrhea or vomiting. Chances of lithium toxicity increase by some nonsteroidal anti-inflammatory drugs such as indomethacin due to decreased renal clearance of lithium. Lithium is contraindicated during the first trimester of pregnancy and lactation because of the possible fetal congenital abnormalities and neonatal dysfunction. Other drugs Several antiepileptic drugs, including carbamazepine, valproic acid, and lamotrigine, are approved as mood stabilizers for bipolar disorder. Other agents that may improve manic symptoms include the older (chlorpromazine and haloperidol) and newer antipsychotics. Quetiapine, lurasidone, and the combination of olanzapine and fluoxetine have been approved for bipolar depression. After 6 weeks of therapy with fluoxetine, his symptoms improved, but he complains of sexual dysfunction. Which of the following drugs might be useful for management of depression in this patient He realizes that his behavior is interfering with his ability to accomplish his daily tasks, but cannot seem to stop himself. Because of its potent antimuscarinic activity, amitriptyline should not be given to patients with glaucoma because of the risk of acute increases in intraocular pressure. Lithium is the only agent for bipolar disorder that does not require hepatic metabolism and, thus, may be dosed without issue in a hepatically impaired patient. Mirtazapine is the only antidepressant with this combination of mechanisms of action that are believed to contribute to its therapeutic effects. Lithium is best known for causing a drug-induced hypothyroidism in patients after long-term use. Though it is possible with other mood stabilizers, lithium has the most reported cases, and thus, thyroid function tests should be performed at baseline and during follow-up to monitor for this possible effect. Venlafaxine, bupropion, and escitalopram have very little effect on decreasing blood pressure (no 1 receptor antagonism) and are considered acceptable choices for treatment of depression in the elderly. Amitriptyline is associated with a high risk for orthostasis in the elderly and should be avoided due to its adverse effect profile and risk for falls. Schizophrenia has a strong genetic component and probably reflects some fundamental developmental and biochemical abnormality, possibly a dysfunction of the mesolimbic or mesocortical dopaminergic neuronal pathways. First-generation antipsychotics the first-generation antipsychotic drugs (also called conventional) are competitive inhibitors at a variety of receptors, but their antipsychotic effects reflect competitive blockade of dopamine D2 receptors. Refractory patients: Approximately 10% to 20% of patients with schizophrenia have an insufficient response to first- and second-generation antipsychotics. However, its clinical use is limited to refractory patients because of serious adverse effects. The risk of severe agranulocytosis necessitates frequent monitoring of white blood cell counts. Actions the clinical effects of antipsychotic drugs reflect a blockade at dopamine and/or serotonin receptors. It is unknown what role, if any, these actions have in alleviating the symptoms of psychosis. Antipsychotic effects: All antipsychotic drugs can reduce hallucinations and delusions associated with schizophrenia (known as "positive" symptoms) by blocking D2 receptors in the mesolimbic system of the brain. The "negative" symptoms, such as blunted affect, apathy, and impaired attention, as well as cognitive impairment, are not as responsive to therapy, particularly with the first-generation antipsychotics. Many second-generation agents, such as clozapine, can ameliorate the negative symptoms to some extent. Extrapyramidal effects: Dystonias (sustained contraction of muscles leading to twisting, distorted postures), Parkinson-like symptoms, akathisia (motor restlessness), and tardive dyskinesia (involuntary movements, usually of the tongue, lips, neck, trunk, and limbs) can occur with both acute and chronic treatment. Blockade of dopamine receptors in the nigrostriatal pathway is believed to cause these unwanted movement symptoms. Antiemetic effects: the antipsychotic drugs have antiemetic effects that are mediated by blocking D2 receptors of the chemoreceptor trigger zone of the medulla (see Chapter 42). Relative a nities at D2 receptors Clozapine Chlorpromazine Haloperidol Low a nity High a nity Most antipsychotic drugs have a nities at D2-dopaminergic receptors that parallel clinical potency. Clozapine di ers from typical antipsychotic drugs in having a similar a nity for both D1- and D2-dopaminergic receptors. Relative a nities at D1 receptors elative Clozapine Chlorpromazine Haloperidol Low a nity High a nity 2. These effects include blurred vision, dry mouth (the exception is clozapine, which increases salivation), confusion, and inhibition of gastrointestinal and urinary tract smooth muscle, leading to constipation and urinary retention. Other effects: Blockade of -adrenergic receptors causes orthostatic hypotension and light-headedness. In the pituitary, antipsychotics that block D2 receptors may cause an increase in prolactin release. Sexual dysfunction may also occur with the antipsychotics due to various receptor-binding characteristics. Weight gain is also a common adverse effect of antipsychotics and is more significant with the second-generation agents. Treatment of schizophrenia: the antipsychotics are the only efficacious pharmacological treatment for schizophrenia. The first-generation antipsychotics are generally most effective in treating the positive symptoms of schizophrenia. Also, risperidone and aripiprazole are approved for the management of disruptive behavior and irritability secondary to autism. Many antipsychotic agents are approved for the management of the manic and mixed symptoms associated with bipolar disorder. Some antipsychotics (aripiprazole, brexpiprazole, and quetiapine) are used as adjunctive agents with antidepressants for treatmentrefractory depression. Some metabolites are active and have been developed as pharmacological agents themselves (for example, paliperidone is the active metabolite of risperidone, and the antidepressant amoxapine is the active metabolite of loxapine). These formulations usually have a therapeutic duration of action of 2 to 4 weeks, with some having a duration of 6 to 12 weeks. Blocking dopamine receptors alters this balance, causing a relative excess of cholinergic influence, which results in extrapyramidal motor effects. Parkinson-like symptoms of bradykinesia, rigidity, and tremor usually occur within weeks to months of initiating treatment. Tardive dyskinesia (see below), which can be irreversible, may occur after months or years of treatment. If cholinergic activity is also blocked, a new, more nearly normal balance is restored, and extrapyramidal effects are minimized. Akathisia may respond better to blockers (for example, propranolol) or benzodiazepines, rather than anticholinergic medications. Tardive dyskinesia: Long-term treatment with antipsychotics can cause this motor disorder. A prolonged holiday from antipsychotics may cause the symptoms to diminish or disappear within a few months. However, in many individuals, tardive dyskinesia is irreversible and persists after discontinuation of therapy. Tardive dyskinesia is postulated to result from an increased number of dopamine receptors that are synthesized as a compensatory response to long-term dopamine receptor blockade. Treatment necessitates discontinuation of the antipsychotic agent and supportive therapy. Those antipsychotics with potent antimuscarinic activity often produce dry mouth, urinary retention, constipation, and loss of visual accommodation.
Purchase hydrochlorothiazide 12.5 mg free shipping
Pharmacodynamics A lipid-soluble drug di uses across the cell membrane and moves to the nucleus of the cell prehypertension statistics buy hydrochlorothiazide cheap. Potency: Potency is a measure of the amount of drug necessary to produce an effect. For example, candesartan and irbesartan are angiotensin receptor blockers used to treat hypertension. The therapeutic dose range for candesartan is 4 to 32 mg, as compared to 75 to 300 mg for irbesartan. Efficacy: Efficacy is the magnitude of response a drug causes when it interacts with a receptor. Similarly, even though an antagonist occupies 100% of the receptor sites, no receptor activation results and Emax is zero. Efficacy is a more clinically useful characteristic than potency, since a drug with greater efficacy is more therapeutically beneficial than one that is more potent. Relationship of drug binding to pharmacologic effect the law of mass action can be applied to drug concentration and response providing the following assumptions are met: 1) the magnitude of the response is proportional to the amount of receptors occupied by drug, 2) the Emax occurs when all receptors are bound, and 3) one molecule of drug binds to only one molecule of receptor. In this case, [E] [Emax] = [D] Kd + [D] (2) Response nse Affinity describes the strength of the interaction (binding) between a ligand and its receptor. The higher the Kd value, the weaker the interaction and the lower the affinity, and vice versa. Repeated administration of an agonist (such as epinephrine) over a short time period results in diminished response of the cell. Time 0 50 10 50 50 0 10 50 50 0 10 40 30 20 40 30 20 Repeated injection of drug Following a period of rest, administration of the drug results in a response of the original magnitude. Many drugs and most neurotransmitters can bind to more than one type of receptor, thereby causing both desired therapeutic effects and undesired adverse effects. Pharmacodynamics Drug A is more potent than Drug B, but both show the same e cacy. Full agonists bind to a receptor, stabilizing the receptor in its active state and are said to have an intrinsic activity of one. For example, phenylephrine is a full agonist at 1-adrenoceptors, because it produces the same Emax as the endogenous ligand, norepinephrine. Upon binding to 1-adrenoceptors on vascular smooth muscle, both norepinephrine and phenylephrine stabilize the receptor in its active state, thereby increasing Gq activation. The diameter of the arteriole decreases, causing an increase in resistance to blood flow through the vessel and an increase in blood pressure. Thus, effects of agonists on intracellular molecules, cells, tissues, and intact organisms are all attributable to interaction of the drug with the receptor. Even when all the receptors are occupied, partial agonists cannot produce the same Emax as a full agonist. Even so, a partial agonist may have an affinity that is greater than, less than, or equivalent to that of a full agonist. As the number of receptors occupied by the partial agonist increases, the number of receptors that can be occupied by the full agonist decreases and therefore Emax would decrease until it reached the Emax of the partial agonist. This potential of partial agonists to act as both an agonist and an antagonist may have therapeutic utility. For example, aripiprazole, an atypical antipsychotic, is a partial agonist at selected dopamine receptors. This might explain the ability of aripiprazole to improve symptoms of schizophrenia, with a small risk of causing extrapyramidal adverse effects (see Chapter 11). Typically, unbound receptors are inactive and require interaction with an agonist to assume an active conformation. The circled letters in the figure represent agonists with varying affinities for 1 and 2 receptors. However, from the data provided, it becomes clear that 1 receptors only mediate changes in blood pressure, while 2 receptors only mediate changes in bronchodilation. Antagonists Antagonists bind to a receptor with high affinity but possess zero intrinsic activity. An antagonist has no effect on biological function in the absence of an agonist, but can decrease the effect of an agonist when present. Pharmacodynamics A full agonist produces complete activation of a receptor at high drug concentrations. Partial agonist binding results in less than 100% activation, even at very high concentrations. Competitive antagonists: If the antagonist binds to the same site on the receptor as the agonist in a reversible manner, it is "competitive. For example, the antihypertensive drug terazosin competes with the endogenous ligand norepinephrine at 1-adrenoceptors, thus decreasing vascular smooth muscle tone and reducing blood pressure. Irreversible antagonists: Irreversible antagonists bind covalently to the active site of the receptor, thereby permanently reducing the number of receptors available to the agonist. A classic example is the functional antagonism by epinephrine to histamine-induced bronchoconstriction. Histamine binds to H1 histamine receptors on bronchial smooth muscle, causing bronchoconstriction of the bronchial tree. Epinephrine is an agonist at 2-adrenoceptors on bronchial smooth muscle, which causes the muscles to relax. In this example, a portion of the receptors show constitutive activity (without stimulation), such that 12% of maximal response is seen. Graded responses can be transformed to quantal responses by designating a predetermined level of the graded response as the point at which a response occurs or not. Key: Full agonist Partial agonist Fully active receptor Partially active receptor A. High levels of agonist may activate all receptors and produce unwanted overstimulation. In these cases, though more adverse effects may be experienced, the risk of experiencing adverse effects should be weighed against the risk of leaving the disease untreated. Cytotoxic agents, used in cancer chemotherapy and antiepileptic drugs, are examples of drugs where there is little difference between the therapeutic dose and the toxic dose. Other examples of some drugs with a narrow therapeutic index are lithium, digoxin, gentamicin, phenytoin, and carbamazepine. These drugs have a recommended therapeutic range with lower and upper values of the concentration of the drug in blood at which majority of the users can expect a clinical effect with minimal adverse effects. In this case, bioavailability does not critically alter the therapeutic or clinical effects. The presence of partial agonist displaces some agonist, resulting in diminished receptor response. This variability continues to be a major public health problem due to serious and apparently unpredictable adverse drug reactions. The reasons for failure of drug treatment can be due to interindividual variation in physiological and pharmacokinetic parameters, which cannot always be evaluated prior to initiation of drug therapy (for example, genetic metabolic differences) or pharmacodynamics (for example, drug hypersensitivity), and drug tolerance (diminished pharmacologic responsiveness to the drug). Response to a drug can be altered by disease state and draw attention to dosage individualization. The dosage regimen needs to be further modified in case of no-response to therapy or due to the appearance of undesirable effects. A Warfarin: Small therapeutic index Therapeutic window Percentage of patients 100 A. Factors affecting drug response 50 Desired therapeutic e ect Unwanted adverse e ect 0 Log concentration of drug in plasma (arbitrary units) Variability in drug responses can be observed due to genetic difference and pharmacokinetic and pharmacodynamic variability. Variation in response due to changes in pharmacokinetics: Diseases of the liver and the kidneys are responsible for large variations in drug pharmacokinetics. Circulatory disorders and diminished vascular perfusion of one or more parts of the body as in cardiac failure are also an important cause of pharmacokinetic variability.
Generic 25 mg hydrochlorothiazide fast delivery
To minimise disease transmission to sex partners blood pressure high diastolic effective hydrochlorothiazide 25mg, persons treated for chlamydia should be instructed to abstain from sexual intercourse for seven days after single-dose therapy or until completion of a seven-day regimen and resolution of symptoms, if present. To minimise risk for reinfection, patients also should be instructed to abstain from sexual intercourse until all of their sex partners are treated. In men urethritis is associated with mucopurulent discharge, dysuria and pruritus, whilst in women cervicitis is associated with a mucopurulent vaginal discharge. Symptoms usually develop within three to five days, but may present up to two weeks following exposure. Untreated infection may lead to systemic gonococcal infection with bacteraemia, arthritis and dermatitis. However, the majority of patients are asymptomatic, resulting in a large reservoir for transmission. Although gonococcal cervicitis is most commonly acquired through ano-receptive intercourse, between 35% and 50% of infected women will have a concomitant rectal infection, believed to have spread contiguously. Although the perineum is generally not involved, purulent discharge on the rectal walls or within the lumen can be seen on anoscopy. Occasionally, non-specific findings such as erythema, oedema and friability may be present. However, because of the colonisation of the rectum with other organisms, rectal cultures are felt to be less efficient than cultures from other sites. These tests have demonstrated better sensitivity (100% vs 56%) and equivalent specificity (99. Due to the high prevalence of tetracycline resistance in the United States, doxycycline is no longer recommended as a second antimicrobial in either the recommended or alternative dual treatment regimen. Patients with urethritis are advised to refrain from sexual intercourse for seven days after completing therapy. Individuals who have engaged in sexual intercourse with an affected patient within 60 days of the infection should be examined and presumptively treated. An elicited history of oro-anal contact should prompt treatment of pharyngeal gonorrhoea. Routine follow-up is not necessary after treatment for gonorrhoea, as therapy is usually effective. In the case of recurrent symptoms, the patient should be re-examined; the physician must inquire about compliance with initial therapy and the possibility of re-exposure. Suspected treatment failures first should be retreated routinely with the recommended therapy as reinfections are more likely than actual treatment failures. Dual treatment with single doses of oral gemifloxacin 320 mg plus oral azithromycin 2 g or dual treatment with single doses of intramuscular gentamicin 240 mg plus oral azithromycin 2 g can be considered. Note the undermined edges of this completely painless superficial lesion around the anal canal. In 2000 and 2001, the national rate of reported primary and secondary syphilis cases was 2. Primary syphilis of the rectum usually occurs two to ten weeks after ano-receptive intercourse but may not appear for six months. Lesions in the anal canal can be tender and difficult to distinguish from anal fissures. Eccentric location, multiple lesions, irregular edges and location above the dentate line suggest that the lesion is not simply an idiopathic fissure. Therefore any but the most classical appearing fissures should have testing performed, especially prior to any contemplated surgery. Proctoscopy may reveal ulcerations that may be difficult to distinguish from carcinomas or solitary ulcers. Secondary syphilis usually occurs 2 to 12 weeks after appearance of the initial lesions. Systemic symptoms include fever, malaise, arthralgias, weight loss, sore throat and headache. In addition, patients often have a classic maculopapular rash on the palms of the hands and soles of the feet; these may be diffuse. Anorectal lesions such as condyloma latum can be seen during this stage in patients with anorectal syphilis. The presence of spirochetes distinguishes anorectal syphilis from other perineal conditions. It results in cardiac, ophthalmic and auditory abnormalities, as well as gummatous lesions secondary to obliterative small vessel arteritis. Lesions of the gastrointestinal tract may result in polypoid masses or areas of constriction. These multiple warts occur in the perianal region and often within the anal canal as well. Penicillin G, administered parenterally, is the preferred drug for treating persons in all stages of syphilis. Stage and clinical presentation further determine the preparation, dosage and length of treatment. Additional medications, such as azithromycin and ceftriaxone, may have a role in management. Partners of patients with syphilis should be identified, as partner identification has been shown to reveal a large number of additional infected persons. Partners of individuals who have had syphilis of unknown duration and who have a high non-treponemal serologic test (>1:32) should be assumed to have early syphilis, and any additional sexual partners should be notified. Longterm partners of patients with latent syphilis should be evaluated clinically and serologically. It has become more and more infrequently reported in the United States with only six cases reported in 2014. Clinically, it is characterised by papules that may form within 24 hours of infection and may be associated with erythema. These papules become pustules within two to five days and evolve into ulcers over a period of days or weeks; the ulcers may persist for up to three to six weeks. Sequential testing with the same test from the same laboratory should be used to evaluate clinical response at three and six months after therapy. A fourfold reduction in titre levels must be seen in order for a response to be considered significant. The nontreponemal tests become non-reactive after treatment, although low titres may persist whereas reactive treponemal titres remain active forever. Although inguinal adenopathy is not always present, when present it is painful and is usually unilateral. A recent study in the United States during an outbreak of chancroid in New Orleans demonstrated that only 32% of patients present with the classic clinical findings. Patients should experience symptomatic improvement within three days and objective improvement within seven days. However, it is prevalent in such areas as Papua New Guinea, South Africa, India, Brazil and within the Aboriginal community in Australia. Donovanosis is usually transmitted sexually, although it can also be transmitted through faecal contamination and auto-inoculation. Based on case series, authors have reported that incubation ranges from 1 to 360 days. It predominantly affects the perineal area in men and women, and inguinal lymphadenopathy isreported in only 10% of cases. The infections begin as firm nodules that ulcerate with four subtypes: 1) the ulcerogranulomatous variant, which is the most common and has beefy red, non-tender ulcers that bleed when touched and proliferate if not treated; 2) hypertrophic or verrucous ulcers, which are often dry and have an irregular border; 3) necrotic lesions, which are malodorous and destroy tissue and 4) dry sclerotic ulcers, which are associated with fibrous and scar tissue and may cause anal stenosis. However, given its rarity in the Western world, confirmation is made by the identification of intracellular Donovan bodies within large mononuclear cells from smears or tissue biopsy. Sexual partners should be offered screening and treatment, although there are no data to suggest that this is beneficial. Review of the literature identifies several recommended antibiotic regimens of varying time courses. Alternative regimens include doxycycline 100 mg twice a day for three weeks, trimethoprim-sulfamethoxazole one doublestrength (160 mg/800 mg) tablet orally twice a day for at least three weeks, ciprofloxacin 750 mg orally twice a day for at least three weeks or erythromycin base 500 mg orally four times a day for at least three weeks.
Buy genuine hydrochlorothiazide line
Patients with gastrointestinal involvement can present with symptoms mimicking inflammatory bowel disease where diarrhoea blood pressure medication for asthmatics best hydrochlorothiazide 12.5mg, abdominal pain, intermittent fever, anorexia and weight loss are common features. Rarely, in severe cases, gastrointestinal bleeding and colonic perforation may result. Histoplasmosis Like paracoccidiodomycosis, this is a common endemic mycotic disease that exists in both as an oval budding yeast and as a mycelium. Other diagnostic methods include serological tests for histoplasma-specific antibodies. The Organism Histoplasma capsulatum is a dimorphic fungus that remains in a mycelial form at ambient temperatures and grows as a yeast at body temperature in mammals. In the United States, it is seen most commonly in the valleys of the Mississippi, Missouri and Ohio Rivers. Transmission Spores of Histoplasma species reside in the soil in areas endemic for histoplasmosis. Pathogenesis Infection occurs following inhalation of these spores resulting in a patchy interstitial pneumonitis. Spores undergo metamorphosis to yeast cells, which are engulfed by macrophages, in which they multiply. Infection then spreads through the lymphatics and bloodstream to adjacent lymph nodes and to other parts of the reticuloendothelial system like the liver, spleen and bone marrow. Pathogenesis 1571 administered in a dose of 200 mg orally three times daily for three days followed by 200 mg twice daily for a further 12 weeks. Alternatively, amphotericin B may be used in moderate to severe infections at a minimum dose of 40 mg/kg for several weeks. It is an increasingly important nosocomial infection particularly in the immunocompromised and those requiring prolonged intensive care treatment. In the gastrointestinal tract it is pathogenic particularly in the immunocompromised and in patients receiving prolonged broad spectrum antibiotics with severe abdominal sepsis. There are several species of candida yeasts, the most common of which is Candida albicans. The candida yeasts can form true hyphae and pseudohyphae, which are chains of budding cells that fail to separate. Pathogenesis Although Candida are considered as normal flora of skin and mucous membranes of the gastrointestinal and genitourinary tracts, they can result in opportunistic infections when there is a breach in the mucosal barrier or a host with a compromised immune status. Colonisation of indwelling vascular catheters is an increasingly important source of sepsis. Penetration and absorption through the gastrointestinal mucosal barrier from an overgrowth of yeasts in the bowel lumen is probably the most common mode of candidial infection, particularly in immunocompromised hosts. Clinical Features Clinical presentation can vary from non-specific fever to full-blown sepsis in invasive candidiasis characterised by haematogenous spread to multiple organs. Intestinal involvement generally produces profuse watery diarrhoea, nausea, vomiting, fever with chills and abdominal discomfort. Confirmation of diagnosis is achieved by microscopic examination and culture of material obtained by biopsy. In patients with severe infections, Candida may be detected in the stools in vast numbers. Other members of the family Entamoebidae are generally regarded as being non-pathogenic and rarely cause intestinal disease in humans (see Table 88. A recent study has shown that blood cultures can be negative in as many as 50% of patients with invasive candidiasis. Epidemiology Amoebiasis occurs worldwide, but it has a higher prevalence in developing countries due to poor socioeconomic conditions and sanitation levels. Areas with high rates of amoebic infection include Africa, India and parts of Central and South America. The overall prevalence of amoebic infection may be as high as 50% in some parts of Africa and Asia. A cross sectional study in western Malaysia on the prevalence of the different types of Entamoeba species and their pathogenicity using a molecular method reported from a random collection of 500 stool specimens from three different Orang Asli (indigenous) tribes (see Table 88. Similarly, other gastrointestinal symptoms such as abdominal pain, weight loss, loss of appetite, vomiting and nausea (v2 = 14. The trophozoite are able to invade the intestinal wall and are responsible for the production of intestinal disease. The cyst, on the other hand, can survive for extended periods in the environment, provided the climatic conditions are suitable. Infection occurs following ingestion of amoebic cysts; this is usually from contaminated food or water but can be associated with venereal transmission through a faecal-oral Life Cycle contact. There is no sex preference for the acquisition of amoebic infection, but symptomatic amoebic dysentery is more common in men. Amoebic infection does appear to have an increased prevalence and severity in pregnant women. The cysts can survive for days to weeks in the external environment and are responsible for transmission, whereas the trophozoites are rapidly destroyed. In many cases, the trophozoites remain confined to the intestinal lumen (non-invasive infection) of individuals who are asymptomatic carriers, who pass cysts in the stool. In some patients the trophozoites invade the intestinal mucosa (intestinal disease) or through the bloodstream to extraintestinal sites such as the liver, brain and lungs (extraintestinal disease), with resultant pathologic manifestations. Centers for Disease Control and Prevention, Division of Foodbarne, Waterborne and Environmental Diseases. Protozoal Infections 1575 during sexual contact (in which case not only cysts, but also trophozoites could prove infective). This is thought to be mediated initially by an amoeba-specific protein called amoebapore, which in its monomeric form has an apparent molecular weight of 14kDa. Amoebapore is an ion channel-forming protein, and its release leads to entry of calcium into the host epithelial cell, resulting in cell death. Proteolytic and hydrolytic enzymes released by trophozoites also contribute to the process of invasion. Intestinal bacteria are also thought to be involved in the pathogenesis of invasive amoebiasis by increasing parasite virulence. Enteric bacteria are required to produce invasive amoebic disease in gnotobiotic guinea pigs. Loss of virulence of in-vitro-cultured amoebae can be restored by transient co-culture with bacteria. Fulminant colitis with bowel necrosis leading to perforation and peritonitis122 has been observed in approximately 0. Chronic Amoebic Colitis Rarely, intestinal amoebiasis may present as a chronic syndrome of intermittent diarrhoea, weight loss and abdominal pain, persisting over years and mimicking inflammatory bowel disease. Symptoms may remit cyclically, with return to normal bowel function or even constipation. In general, patients with amoebic dysentery do not appear to be severely unwell, since fever is either low-grade or absent; furthermore, water and electrolyte disturbance is unusual. In less than 10% of patients with amoebic colitis, a mass of fibrotic granulation tissue develops in the colon, often with a necrotic core usually in the caecum or rectosigmoid mimicking a cancer. Other rare presentations of amoebiasis include perianal cutaneous and rectovaginal fistulae. Clinical Features There are four major presentations of intestinal amoebiasis: 1) the asymptomatic carrier, 2) asymptomatic amoebiasis, 3) acute intestinal amoebiasis and 4) chronic intestinal amoebiasis. Current available techniques include stool microscopy, immunological and molecular tests as well as colonoscopy with histologic examination. Stool Microscopy Demonstration of cysts or trophozoites in the stool would suggest intestinal amoebiasis, however, microscopy cannot differentiate between the different strains of Entamoeba. Microscopic examination of fresh stool samples may reveal the presence of trophozoites with ingested red blood cells. The Asymptomatic Carrier State this is the most common form of the disease and probably accounts for 80% of cases.
androst-4-ene-3,6,17-trione (Androstenetrione). Hydrochlorothiazide.
- Dosing considerations for Androstenetrione.
- Improving athletic performance and other conditions.
- How does Androstenetrione work?
- Are there safety concerns?
- What is Androstenetrione?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97037
Purchase hydrochlorothiazide online from canada
In three to four cycles of treatment over a period of 6 to 8 days blood pressure medication vitamin k buy hydrochlorothiazide american express, it is enough to get the extensive parasite clearance from blood. Owing to its tolerable side effect profile, it is recommended for nonpregnant adults and children. Other derivatives are also available for intramuscular (artesulate and artemether), 644 36. Antiprotozoal Drugs intravenous (artesunate), and rectal (artesunate) modes of administration. This combination had extensive use in the clinical settings for malaria, especially for the erythrocyte stage. Resistance for this combination occurred due to the point mutations in the dihydroperoate synthase gene in the malaria. Due to sulfonamide moiety, adverse effects such as exfoliative dermatitis and Stevens-Johnson syndrome are observed. Tablets with sulfadoxine or sulfamethopyrazine at a dose of 500 mg along with pyrimethamine 25 mg are available. It is usually administered as a single dose of three tablets (1500 mg sulfadoxine with 75 mg pyrimethamine) for adults. Chemotherapy for Trypanosomiasis 645 not routinely used in endemic areas due to propensity for emergence of high-level resistance. Other antibiotics Tetracycline, doxycycline, and clindamycin are used for the treatment of malaria. These are slow-acting blood schizonticides and are used in areas where the use of chloroquine and mefloquine in resistant malaria is predominant. Due to their slow onset of action, these drugs are not recommended for clinical management. Pentamidine is also an alternative for prophylaxis or treatment of infections caused by P. Pharmacokinetics: Pentamidine is administered intramuscularly or intravenously for the treatment of trypanosomiasis and pneumonia caused by P. Adverse effects: Serious renal dysfunction may occur, which is reversible on discontinuation. Renal insufficiency may occur, but tends to resolve with discontinuation of treatment. The drug reacts with sulfhydryl groups of various substances, including enzymes in both the organism and the host. The host readily oxidizes melarsoprol to a relatively nontoxic, pentavalent arsenic compound. Other adverse effects include peripheral neuropathy, hypertension, hepatotoxicity, and albuminuria. Chemotherapy for Leishmaniasis 647 anemia has been seen in patients with glucose-6-phosphate dehydrogenase deficiency. Inhibition of this enzyme halts the production of polyamines in the parasite, thereby leading to cessation of cell division. Adverse effects are common following chronic administration, particularly among the elderly. Major toxicities include hypersensitivity reactions (anaphylaxis, dermatitis) and gastrointestinal problems that may be severe enough to cause weight loss. Peripheral neuropathy is relatively common, and headache and dizziness may also occur. It tends to be better tolerated than nifurtimox and is an alternative for the treatment of Chagas disease. Adverse effects include dermatitis, peripheral neuropathy, insomnia, and anorexia. For visceral leishmaniasis, parenteral treatments may include amphotericin B (see Chapter 33) and pentavalent antimonials, such as sodium stibogluconate or meglumine antimoniate with pentamidine and paromomycin as alternative agents. Antiprotozoal Drugs of Leishmania, host factors, and resistance patterns noted in area of the world where the infection is acquired. The precise mechanism of action is not known, but miltefosine appears to interfere with phospholipids and sterols in the parasitic cell membrane to induce apoptosis. Amphoterincin B Pharmacology of the polyene antifungal amphotericin B has been discussed in this chapter. It is a hydrophobic agent known to exhibit nephrotoxicity; therefore, it is formulated as liposomal amphotericin B to reduce the higher concentrations reaching kidney. Moreover, liposome amphotericin B is used for safety, and liposomes (phospholipid vesicles) are also capable of delivering amphotericin inside the circulating macrophages and reticuloendothelial cells in spleen and liver where amastigotes survive. Liposome amphotericin B, administered at a dose of 15 mg/kg over 3 to 5 days, showed a cure rate of 98%. Chemotherapy for Lymphatic Filariasis 649 sulfamethoxazole, are alternative treatments. Trimethoprim/sulfamethoxazole is used for prophylaxis against toxoplasmosis (as well as P. While the infection may be acquired during childhood, its visible manifestations may occur later in life, causing temporary or permanent disability. In endemic countries, lymphatic filariasis has a major social and economic impact. The disease is caused by three species of thread-like nematode worms, known as filariae-Wuchereria bancrofti, Brugia malayi, and Brugia timori. The adult male and female worms together form "nests" in the human lymphatic system. The vast majority of infected people are asymptomatic, but virtually all of them have subclinical lymphatic damage and as many as 40% have kidney damage, with proteinuria and hematuria. If the urine is alkalinized, renal excretion of the unchanged drug is prevented and the half-life of the drug increases. Drug reactions due to dying worm may commence after the start of the medical treatment. Systemic reactions include fever, headache, myalgia, vomiting, weakness, and asthma; they usually result from the rapid destruction of microfilariae and perhaps adult worms, specially in heavily infected individuals. Local reactions include lymphadenitis, abscess formation, and transient lymphedema. These symptoms develop within 2 days, often within 12 hours, after initiation of the treatment, and persist for 3 to 4 days. The risk and severity of the adverse reactions are related to Loa loa microfilarial density. The drug is not recommended during pregnancy though no teratogenic effect has been reported so far. Antiprotozoal Drugs of obstructive lesions, hence reducing the incidence of chyluria. The drug is rapidly excreted and nontoxic; it can be repeated at 1 month following completion of the first course. Multiple courses of treatment may be required which may be repeated at an interval of 6 months. Peripheral eosinophilia often accompanies the infection with this parasite that should resolve with the response of the treatment. If peripheral eosinophilia and/or clinical symptoms persist after treatment, peripheral blood should be re-examined for microfilaremia/or circulating antigen. Ivermectin kills microfilariae only but not the adult worm and can be given as a single dose of 400 mg/kg. Albendazole 400 mg as a single dose in combination with ivermectin is more effective in clearing microfilariae than albendazole or ivermectin alone.
Cheap generic hydrochlorothiazide uk
On presentation blood pressure medication interaction with grapefruit hydrochlorothiazide 25mg otc, he is tachycardic, hypertensive, tachypneic, and complaining of flank pain. A metabolic panel is obtained, and the patient has a large anion gap acidosis, an increased creatinine, and hypocalcemia. The formation of calcium oxalate crystals, which can be found on urinalysis, leads to hypocalcemia and renal failure. The treatment regimen for this patient would include intravenous fomepizole, if some of the parent compound was still present, and hemodialysis. Methanol may produce a metabolic acidosis as well, but its target organ of toxicity is the eyes instead of the kidneys as with ethylene glycol. Acetaminophen toxicity may produce upper quadrant pain within the first 24 hours, but vital sign abnormalities are not usually found during this time frame. N-acetylcysteine should be started empirically on the basis of the history, and then, once the level returns and is plotted on the Rumack-Matthew nomogram, a final decision on whether to continue therapy can be made. Therefore, initiation of N-acetylcysteine therapy should happen, if possible during the optimal time frame. The doctor diagnoses him with lead toxicity when the blood lead level returns as 75 g/dL. Dual parenteral therapy with dimercaprol and calcium disodium edetate is indicated if encephalopathy is present, or if the lead level is greater than 70 g/dL in a child. Dimercaprol intramuscular therapy is initiated 4 hours prior to the intravenous administration of calcium disodium edetate when both medications are required. After flumazenil administration, resedation usually occurs, since the duration of the benzodiazepine is longer than that of the flumazenil. Multiple doses of activated charcoal would lower the concentration of both medications, rendering the phenytoin subtherapeutic. The salicylate level was 50 mg/dL (15 to 35 mg/dL therapeutic range) and the phenytoin level was 15 mg/L (10 to 20 mg/L therapeutic range). Envenoming is a significant public health problem in tropical and subtropical regions. It is a preventable public health hazard often faced by rural population in tropical and subtropical countries with heavy rainfall and humid climate. Snakebite is a common occupational hazard affecting farmers, plantation workers, and others, resulting in thousands of deaths each year. Since snakebite is an environmental, occupational, and climatic hazard and mostly affect farmers, plantation workers, herdsmen, fishermen, snake restaurant workers, and other food producers, it results in tens of thousands of deaths each year and chronic physical handicap in many cases. There are more than 2000 species of snakes in the world and about 300 species are found in India out of which 52 are venomous. The venomous snakes found in India belong to three families Elapidae, Viperidae, and hydrophinae (Sea Snakes). The clinical effects of envenoming by the same species of snake are almost similar except a few regional variations. Kraits are active during night hours, often biting a person sleeping on the floor bed. Maximum Viper and Cobra bites occur during the day or early darkness, while watering the plantation or walking barefoot in grown grass or soybean crops. Although the total number of bites may be more than 5 to 6 lakhs, only 30% are venomous bites. Snakes are found all over the world except in Antarctica, Iceland, Greenland, Madagascar, Ireland, and New Zealand. They eat their prey whole and are able to consume prey three times larger than the diameter of their head. Venomous snakes inject their prey with venom, while constrictors squeeze their prey. This article provides an overview of the types of poisonous snakes, their toxins, and clinical manifestations and management of a snake bite. It is discharged with the purpose of killing prey or disabling predators and delivered by grooved or hollow fangs in the upper jaw. Snake venom is mostly made up of water, but its venomous effects are from a complex mixture of proteins, enzymes, nonenzymatic polypeptide, toxins, and nontoxic proteins. The clinical features may be localized to the site of the bite or they may be systemic. The pathological effects of venom on one hand may not be noticed for about 6 hours; on the other hand, the effects may last for a few weeks. Local effects Local effects are confined to the part of the body that has been bitten (local bleeding, pain, inflammation, blistering, necrosis around the fang marks). Systemic effects Systemic effects are on the organs and tissues away from the part of the body that has been bitten. These effects may be neurologic, cardiovascular, or thrombogenic depending on the type of snake and its toxin released. The neurotoxins can cause pre- or postsynaptic blockade, depending on the type of the snake that has bitten. They bind to the acetylcholine receptor on the muscle end-plate, blocking neurotransmitter binding, thus causing paralysis. The presynaptic neurotoxins are modified phospholipase A2 toxins which target the terminal axon of the neuromuscular junction causing first the release of the neurotransmitter and then extensive damage to the axonal structure with progressive flaccid paralysis thereafter as seen in Krait poisoning. This leads to spontaneous systemic bleeding from gums, epistaxis, bleeding into the tears, bleeding into the mucosae, hemoptysis, hematemesis, rectal bleeding or melena, hematuria, vaginal bleeding, antepartum hemorrhage in pregnant women, and intracranial hemorrhage. Certain cardiotoxins are phospholipases causing cellular injury of skeletal, smooth, and cardiac muscles to produce paralysis and cardiac asystole. Some cardiotoxins cause irreversible depolarization of the cell membrane and systolic cardiac arrest. As muscles undergo lysis and also following massive hemolysis or rhabdomyolysis, there is hyperkalemia that depresses cardiac function. The effects include collapse, shock, hypotension, cardiac arrhythmias, cardiac failure, pulmonary edema, and respiratory failure. Assess circulation, airway, and breathing and deal with any life-threatening symptoms on presentation. Neuroparalytic patients presenting with respiratory paralysis, tachypnea or bradypnea or paradoxical respiration (only moving abdomen), obtunded mentation, and peripheral skeletal muscle paralysis need urgent ventilator management with endotracheal intubation, ventilation bag, or ventilator assistance. Other noncritical patients can be evaluated to decide the severity of their illness. The Glasgow Coma scale cannot be used to assess the level of consciousness of patients paralyzed by neurotoxic venoms. If clotted, carry out every 1 hour from admission for 3 hours and then 6 hourly for 24 hours. Take one smart phone photograph of the snake, dead or alive, if available, for confirmation by an expert. Fang marks or their patterns have no role to determine whether the biting species was venomous or nonvenomous or the amount of venom injected, severity of systemic poisoning, and nature of poisoning-Elapidae or viperidae venom. They may persist for a few weeks or may be debilitating, sometimes permanently, due to local necrotic effects of venom and complicating infections. Though to a large extent the manifestation of snakebite depends upon the species of snake, unfortunately, in many cases the biting snake is not seen, and if it is, its description by the victim is often misleading. The clinical manifestations of the patient may not correlate with the species of snake brought as evidence. Thus, clinicians may have difficulties in determining whether envenoming occurred or not. If no other transport is available, a motorbike may be used but a third person should sit behind the patient.
Cheap hydrochlorothiazide 12.5 mg on-line
Absorption is impaired if isoniazid is taken with food arrhythmia band chattanooga hydrochlorothiazide 25 mg with mastercard, particularly high-fat meals. The drug diffuses into all body fluids, cells, and caseous material (necrotic tissue resembling cheese that is produced in tuberculous lesions). Adverse effects: Hepatitis is the most serious adverse effect associated with isoniazid. The incidence increases with age (greater than 35 years old), among patients who also take rifampin, or among those who drink alcohol daily. Peripheral neuropathy, manifesting as paresthesia of the hands and feet, appears to be due to a relative pyridoxine deficiency caused by isoniazid. In rapid acetylators, isoniazid has a short half-life (1 hr) In slow acetylators, isoniazid has a long half-life (3 hrs) Subjects (n) 20 10 0 50 100 150 200 250 Half-life (min) 5. Antimicrobial spectrum: Rifampin is bactericidal for both intracellular and extracellular mycobacteria, including M. It is effective against many gram-positive and gram-negative organisms and is used prophylactically for individuals exposed to meningitis caused by meningococci or Haemophilus influenzae. Rifampin can induce hepatic cytochrome P450 enzymes and transporters (see Chapter 1), leading to numerous drug interactions. Unrelated to its effects on cytochrome P450 enzymes, rifampin undergoes autoinduction, leading to a shortened elimination half-life over the first 1 to 2 weeks of dosing. However, the drug should be used judiciously in older patients, alcoholics, or those with chronic liver disease. There is a modest increase in the incidence of hepatic dysfunction when rifampin is coadministered with isoniazid and pyrazinamide. When rifampin is dosed intermittently, especially with higher doses, a flu-like syndrome can occur, with fever, chills, and myalgia, sometimes extending to acute renal failure, hemolytic anemia, and shock. This may necessitate higher dosages for coadministered drugs, a switch to drugs less affected by rifampin, or replacement of rifampin with rifabutin. Rifabutin is a less potent inducer (approximately 40% less) of cytochrome P450 enzymes, thus lessening drug interactions. Rifabutin has adverse effects similar to those of rifampin but can also cause uveitis, skin hyperpigmentation, and neutropenia. Ethambutol inhibits arabinosyl transferase, an enzyme important for the synthesis of the mycobacterial cell wall. Both the parent drug and its hepatic metabolites are primarily excreted in the urine. The most important adverse effect is optic neuritis, which results in diminished visual acuity and loss of ability to discriminate between red and green. Take baseline hepatic enzyme measurements; repeat if abnormal or patient is at risk or symptomatic. Take baseline hepatic enzymes and uric acid measurements; repeat if abnormal or patient is at risk or symptomatic. Avoid concomitant ingestion with antacids, multivitamins or drugs containing di- or trivalent cations. In general, these agents are less effective and more toxic than the first-line agents. Cycloserine: Cycloserine is an orally effective, tuberculostatic drug that disrupts d-alanine incorporation into the bacterial cell wall. The mechanism of action is not identical to isoniazid, but there is some overlap in the resistance patterns. Azithromycin may be preferred for patients at greater risk for drug interactions, since clarithromycin is both a substrate and an inhibitor of cytochrome P450 enzymes. Bedaquiline is administered orally, and it is active against many types of mycobacteria. The treatment classification is based on the status of the organism in terms of resistance. The combination of drugs and their duration of treatment is divided into two phases: 1) intensive and 2) continuous phases. Fluoroquinolones1 Levofloxacin Moxifloxacin Gatifloxacin Amikacin Capreomycin Kanamycin (Streptomycin)2 Ethionamide/ prothionamide Cycloserine/terizidone Linezolid Clofazimine I. Four to seven drugs are selected from these groups, for which the pathogen is susceptible for a better outcome. Intensive phase: the duration of the intensive phase is 4 months (extended up to a maximum of 6 months in case of lack of sputum smear conversion) and includes the following drugs: gatifloxacin (or moxifloxacin), kanamycin, prothionamide, clofazimine, highdose isoniazid, pyrazinamide, and ethambutol. Continuation phase: the duration of the continuation phase is 5 months and includes the following drugs: gatifloxacin (or moxifloxacin), clofazimine, pyrazinamide, and ethambutol. Dapsone is also used in the treatment of pneumonia caused by Pneumocystis jirovecii in immunosuppressed patients. The drug is well absorbed from the gastrointestinal tract and is distributed throughout the body, with high concentrations in the skin. Adverse reactions include hemolysis (especially in patients with glucose-6-phosphate dehydrogenase deficiency), methemoglobinemia, and peripheral neuropathy. Its redox properties may lead to the generation of cytotoxic oxygen radicals that are toxic to the bacteria. Patients typically develop a pink to brownish-black discoloration of the skin and should be informed of this in advance. Eosinophilic and other forms of enteritis, sometimes requiring surgery, have been reported. The patient received self-administered isoniazid, rifampin, pyrazinamide and ethambutol. At his regular clinic visit, he complains of a "pins and needles" sensation in his feet. He has had no seizures in 5 years; however, upon return to clinic at 1 month, he reports having two seizures since his last visit. Concurrent administration of pyridoxine (vitamin B6) prevents the neuropathic actions of isoniazid. Isoniazid can cause peripheral neuropathy with symptoms including paresthesias, such as "pins and needles" and numbness. Rifampin (as well as rifabutin and rifapentine) and its metabolites may color urine, feces, saliva, sputum, sweat, and tears a bright red-orange. Patients should be counseled that this is an adverse effect which is not harmful, but can stain clothes and contact lenses. Rifabutin + ethambutol isoniazid isoniazid + + pyrazinamide pyrazinamide + + Correct answer = B. He states he feels fine, but now is having difficulty reading and feels he may need to get glasses. Visual disturbances generally are dose-related and more common in patients with reduced renal function. Pyrazinamide and ethambutol-induced hyperuricemia may be controlled by use of anti-gout medications, such as xanthine oxidase inhibitors. Her physician recently noticed she appears confused and anxious and has a slight tremor. Peripheral neuropathy is one of the most common adverse effects seen with the drug. Clofazimine is a phenazine dye and causes bronzing (the skin pigment color will change color, from pink to brownish-black), especially in fairskinned patients. This occurs in a majority of patients and generally is not considered harmful but may take several months to years to fade after discontinuing the medication. Unlike bacteria, fungi are much more complex organisms, are eukaryotic, with rigid cell walls composed largely of chitin rather than peptidoglycan (a characteristic component of most bacterial cell walls), and often grow slowly. Consequently, only a few drugs are aimed at interfering with cell division and have limited use. In addition, the fungal cell membrane contains ergosterol rather than the cholesterol found in mammalian membranes. Fungi are generally resistant to antibiotics; conversely, bacteria are resistant to antifungal agents. The incidence of mycoses such as candidemia, though not as frequent as bacterial or viral infections, has been on the rise for the last few decades.
Buy generic hydrochlorothiazide 12.5mg online
To break this cycle the stool consistency may need to be softened by laxatives and stool softeners heart attack high dead end counterpart purchase 25 mg hydrochlorothiazide free shipping. In a systematic review,19 chemical sphincterotomy with glyceryl trinitrate or botulinum toxin has been found ineffective or only marginally better than placebo for chronic fissures in children, but it is often tried. Haemorrhoids Haemorrhoids are uncommon in children except in those with portal hypertension. Haemorrhoids are more common in patients with extrahepatic portal hypertension than in those with intrahepatic disease. Usually there are no symptoms but the child or parents have noticed something protruding from the anal opening. A more common finding, especially in constipated children, is a prominent venous plexus around the anal opening. Adulttype hemorrhoids begin to occur in adolescents and may be complicated by thrombosis of the external component. It is primarily a mucosal ischaemic lesion due to shunting of blood from the submucosal vessels. In the early stages the deeper layers of the gut wall and the mucosa are well vascularised, but with secondary bacterial invasion, septicaemia and endotoxic shock, there is shunting of blood away from the splanchnic circulation, causing mucosal ischaemia. Disseminated intravascular coagulation, which is manifested by thrombocytopaenia and platelet aggregation, also occurs, causing gut ischaemia. The main clinical presentation in the baby is a functional obstruction with abdominal distension, vomiting and usually the passage of loose stools containing blood and mucus. Plain radiography demonstrates diffuse dilatation of the gut with fluid levels, and there may be evidence of mucosal oedema. At a later stage, there is submucosal pneumatosis with the characteristic doublewall-shadow. It is rare in children, but should be kept in mind in patients with local anal symptoms. Rectal prolapse has been reported to occur in a significant percentage of 1534 Chapter 85 Paediatric Surgery: What the Adult Surgeon Needs to Know cases. Juvenile Polyposis Syndrome Juvenile polyposis syndrome is the most common of the hamartomatous polyp syndromes. Characteristically, symptoms include acute or chronic blood loss, mucous discharge, diarrhoea, intussusception or rectal prolapse and protein-losing enteropathy. There is an increased risk of colorectal malignancy but also upper gastrointestinal carcinoma associated with juvenile polyposis syndrome. Close upper and lower gastrointestinal endoscopic surveillance including polypectomies is warranted in all patients. Those with diffuse polyposis and significant symptoms are best managed by proctocolectomy and ileal pouch anastomosis, which can be performed laproscopically and in a single stage. Infantile Proctocolitis Probably the most common cause of haematochezia in infants younger than three months of age is proctocolitis. Usually there are no other symptoms, and the growth and development of the infant is normal. Colonoscopy shows colitis that is often patchy and rarely extends beyond the left colon. An allergic aetiology (milk protein is a common culprit) has been suggested because of these findings. Inflammatory Bowel Disease Inflammatory bowel disease presents in children and must be ruled out as a cause of rectal bleeding. Infective colitis is the most obvious differential diagnostic problem and should be ruled out. Extraintestinal malignancies include pancreatic, breast, ovarian and testicular carcinoma in children and uterine cervical carcinoma. Abdominal pain, chronic blood loss and intussusception are the most common complications. Small bowel contrast studies may show the polyps, but significantly more reliable is wireless capsule endoscopy. Appropriate surveillance for colorectal and extraintestinal malignancies is indicated in probands and in first-degree relatives. Diagnosis can be made in most cases by Technetium scan, which visualises the gastric mucosa in the diverticulum. Treatment is by early resection of the diverticulum by laparoscopy or open surgery. Polyps and the Polyposis Syndromes Juvenile Polyps Juvenile polyps are amongst the most common lesions responsible for rectal bleeding in children. They are more common in the left colon and rectum and multiple in 35% to 50% of cases. The polyp typically has a smooth, glistening, reddish surface and the histology is characteristic. Polyps are hamartomatous and non-malignant and may be selflimiting by autoamputation. Sometimes a polyp may form the apex of an intussusception and as such may present with obstructive symptoms. Colorectal cancer develops very rarely in children but the risk rises to 80% by age 40 years and 100% by age 50 years. The intestinal adenomatous polyps occur in association with osteomas of bone (particularly the mandible) and desmoid tumours, as well as soft tissue tumours. There are associated malignant tumours of the central nervous system, most of which are medulloblastomas or glioblastomas. Primary colonic cancer is exceedingly rare in childhood, and if it occurs, the prognosis is poor,33,34 generally because of the delay in diagnosis. Radical resection of the tumour with the vessels and draining lymphatics and primary anastomosis is the procedure of choice. Sexual abuse rarely causes death but its consequences can be serious and persist through adulthood. In child sexual abuse the significance of findings in the vagina and hymen are well recognised. In the context of anal abuse the findings are more controversial and difficult to verify. Pierce40 found that a majority of children with a strong or definite history of anal abuse had anal fissures or scars. However, an anal fissure is far too common a finding in routine clinical practice to be regarded as a cause for suspicion of sexual abuse. This sort of forensic evidence is rarely found in children because there is usually a significant time lapse between the abuse and medical examination. If a child displays passiveness and indifference to physical examination, or to inspection and examination of the anus, with no attempt to withdraw or tighten the striated muscle complex when a rectal examination is attempted, the clinician should be alerted to the possibility of sexual abuse. Perianal warts caused by the human papillomavirus should always raise the possibility of sexual abuse, as this is the most likely mode of transmission. However, although herpes infection may be indicative of sexual abuse, it could also represent self-infection from herpes around the mouth. Semen found on or in prepubertal boys or girls, gonococci cultured from the rectum, Trichomonas identified in the urine, herpes and chlamydial infections are more definitive signs of sexual abuse. Risto Rentala and Norman Williams who were the authors of the previous edition of this chapter. A prospective, randomized, double-blind, placebo-controlled trial of glyceryltrinitrate ointment in the treatment of children with anal fissure. Double blind randomised controlled trial of topical glyceryl trinitrate in anal fissure. Experience with juvenile polyps in North American children: the need for pancolonoscopy. Hamartomatous polyposis syndromes: Molecular genetics, neoplastic risk, and surveillance recommendations. A prospective trial comparing small bowel radiographs and video capsule endoscopy for suspected small bowel disease. Prognostic factors and outcome in patients 21 years and under with colorectal carcinoma.
