
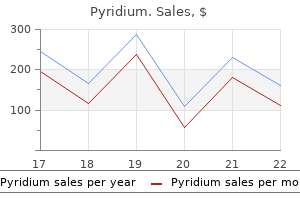
Discount pyridium online mastercard
The electrodes are pulled into the pocket via a stab wound through the abdominal wall created with a tonsil clamp gastritis diet 1000 buy discount pyridium 200mg. The stimulator is sutured to the abdominal wall with three stitches of a 2-0 Ethibond suture. Two stitches are placed through the anterior rectus fascia and one of the plastic tracts and one stitch is placed through one tract and the abdominal wall and then through the abdominal wall and the second tract, being tied on top. The stimulator has to be positioned so that the writing is toward the skin, because only in that position can the interrogator change the settings of the stimulator. The important issue is to note the distance between the end af an electrode and the first clip. In follow-up for worsening symptoms, one needs to re-examine that distance and if greatly increased, the electrode may have pulled out of the stomach. Cllapter 3& Gastric Electrical Stimulation for Chronic Gastroparesis into the pocket the stimulator is interrogated a second time and the load impedance rechecked. The subcutaneous tissue is closed in two layers with interrupted 30 chromic sutures, and skin is closed with a running subcuticular 4-0 absorbable suture. Then they are advanced to clear sips the second day, clear liquids the third day, full liquids the fourth day, a soft mechanical diet the fifth day, and discharged on the sixth day. The day after surgery the patients should get a flat and upright of the abdomen to establish the initial position of the electrodes relative to the medium clips, in order to allow for a check later on whether the electrodes had moved. If a jejunostomy feeding tube had been placed, the tube is put to gravity for the first 24 hours. The next day feedings are started at 10 mL/hour of a 1 Kcal/mL formulation and are slowly advanced by 10 mL/hour every 6 hours until goal is reached. If the patient is severely malnourished, the rate may need to be advanced more slowly. The tuba placed at surgery can be exchanged for a low-profile Mickey tuba at 2 weeks, if the patient needs to have small bowel access for the long term. Most patients will not need long-term access and the tube can be simply removed when both the patient and the gastroenterologist are comfortable doing so. After placement of the stimulator and its activation, some patients feel better almost immediately; we feel we need to wait 3 months to see the maximum effect of the stimulator. An upper endoscopy should also be considered to verify that the electrodes have not eroded through the gastric wall and thus are visible from within the lumen. Fluid collections around the stimulator need to be carefully aspirated and the fluid cultured. Not all such collections are infected; even if the cultures are negative, such patients need extended antibiotic therapy. Clearly, if there is infection in the pocket and around the stimulator, the stimulator, the electrodes, and the plastic disks are all removed. Infections that do not clearly involve the system, even intra abdominal abscesses, have been successfully treated without removing the device. When patients develop pain associated with the stimulator, the stimulator may be moving. Unfortunately, the stimulators have become detached from the rectus fascia due to trauma and abdominal wall movement; this has been seen in patients who lean over a tub in their job washing clothes and or in patients whose stimulator is too close 380 Part V Other Gastric Operations to the right costal margin. If the stimulator has completely loosened, it can coil up the electrodes and pull out the electrodes from the stomach wall. Patients with diabetic and postoperative gastroparesis seem to do better than those with idiopathic gastroparesis. Gastroparesis is characterized by a dysfunctional stomach that no longer pushes food into the duodenum. Cutric electrical stimulation improves outcomes of patients with gastroparesis for up to 10 years. Diagnosis: Sarcoidosis Model answer this is a frontal chest radiograph of an adult male patient. There is diffuse reticulonodular shadowing in both lungs without a zonal predominance. In summary, there is diffuse reticulonodular shadowing with no other significant features. If the patient were acutely unwell, I would consider lymphangitis carcinomatosis, acute drug reactions, viral pneumonia and pulmonary oedema. To take this further, I would review the clinical history and any previous imaging to assess for chronicity. The interstitium is the supporting tissue around the airways and contains lymphatics, connective tissue and pulmonary vasculature. These are large and prominent at the hila and gradually reduce in size and prominence towards the periphery, becoming too small to see. Abnormality of the lung interstitium presents as increased lines (reticular), nodules (nodular), or lines and nodules (reticulonodular pattern). The abnormalities fall into two main categories: those caused by abnormal fluid in the interstitium. In contrast to interstitial disease, air space opacification is due to the filling of the gas-containing structures of the lung with fluid. There is usually a more homogeneous increased lung density with indistinct margins. It is not easy to spot or tell the difference between normal, hazy increased density, reticular, nodular or reticulonodular patterns. Look for the pertinent negatives such as lymphadenopathy, volume loss, cardiomegaly, pleural effusions or mastectomy. Lymphangitis carcinomatosis is usually associated with adenocarcinoma, most commonly of the breast, lung, colon, stomach, pancreas and larynx. There is no soft tissue abnormality; in particular, no axillary surgical clips or asymmetry of the breast shadows can be seen. In summary, there are multiple, bilateral pulmonary nodules of non-uniform size associated with bilateral pleural effusions. To take this further, I would correlate these findings with the clinical history and review previous imaging to establish chronicity. It may appear early in a viva exam, so it is important to give a polished performance. In the absence of any distinguishing features, it may not be possible to reach a diagnosis for a case of multiple lung nodules, so delivering a concise and organised list of differential diagnoses, as presented in the model answer, will help you to impress the examiner and move on to the next case as quickly as possible. Metastatic disease is the most likely cause of multiple pulmonary nodules (larger than miliary nodules). Pearls the most likely cause of multiple pulmonary nodules of varying sizes is metastases. This mnemonic can also apply to multiple cavitating lung nodules and solitary pulmonary nodules. There is no evidence of previous surgery, such as asymmetry of the breast shadows or metallic surgical clips. In summary, there are multiple small pulmonary nodules throughout both lungs in a miliary pattern. Primary tumours that may cause miliary metastases include thyroid, melanoma, breast, gastric, pancreatic, bronchus and prostate. If the patient were relatively well, I would also consider sarcoidosis and pneumoconioses such as uncomplicated silicosis. Further management of this patient should include a review of their medical history for a previous malignancy. I would compare this film with any previous chest radiographs for signs of progression. Discussion Films showing multiple pulmonary nodules are common and can be divided into subcategories based on appearance: their size and the presence or absence of calcification and cavitation.
Cheap pyridium american express
Primary metabolism Primary excretion Onset of action Duration of action Adverse Effects: Propranolol is well tolerated and common adverse effects such as nausea definition of gastritis in english discount pyridium 200 mg without prescription, vomiting, and diarrhea generally diminish as therapy progresses. Other frequent adverse effects include fatigue, insomnia, drowsiness, bradycardia, and confusion. Serious adverse effects include agranulocytosis, bronchospasm, Stevens-Johnson syndrome, and anaphylaxis. Black Box Warning: Abrupt withdrawal is not advised in patients with angina or heart disease. Dosage should gradually be reduced over 1 to 2 weeks and the drug should be reinstituted if angina symptoms develop during this period. Patient and Family Education: Take radial pulse before each dose, and report irregular pulse, or a pulse that drops below the value recommended by the health care provider. Contraindications/Precautions: Because of its depressive effects on the heart, propranolol is contraindicated in cardiogenic shock, sinus bradycardia, greater than first-degree heart block, and severe heart failure. Patients with cardiac impairment must be monitored carefully to prevent worsening of their condition. Propranolol should be used cautiously in patients with diabetes because it interferes with glucose metabolism and can cause hypoglycemia. The drug can also mask signs of impending hypoglycemia such as tachycardia and tremors. Propranolol should be used with caution in patients with reduced renal output, because the drug may accumulate to toxic levels in the blood and cause dysrhythmias. When given with other beta blockers, effects on the cardiovascular system may be additive and bradycardia or hypotension may result. Because both propranolol and calcium channel blockers such as verapamil (Calan) and diltiazem (Cardizem) suppress myocardial contractility, concurrent use may lead to additive bradycardia. All nonselective betaadrenergic blockers have the same actions but differ in their pharmacokinetics and therapeutic applications. Those prescribed exclusively for glaucoma, including betaxolol (Betoptic), carteolol (Ocupress), levobunolol (Betagan), and metipranolol (OptiPranolol), are discussed in Chapter 77. In addition to being a nonselective beta-receptor blocker, carvedilol blocks alpha1-adrenergic receptors. Patients with asthma or chronic lung disorders may experience dyspnea or wheezing due to the bronchoconstriction effects of the drug. Labetalol (Normodyne, Trandate): Like carvedilol, labetalol has nonselective beta-blocking action as well as the ability to selectively block alpha1-adrenergic receptors. The most common adverse effects are generally mild and include insomnia, drowsiness, fatigue, decreased libido, and tingling of the scalp. Off-label uses of nadolol include suppression of ventricular dysrhythmias, migraine prophylaxis, treatment of essential tremor, and anxiety. Given by the oral route, it has a long half-life of 20 to 24 hours, which offers the benefit of once-daily dosing. Unlike many beta blockers, it is not metabolized by the liver and is excreted mostly unchanged by the kidneys. Adverse effects are generally mild and similar to those of propranolol and include drowsiness, fatigue, and decreased libido. Penbutolol (Levatol): Penbutolol is a nonselective betaadrenergic antagonist that has a long duration of action, which offers the benefit of once-daily dosing. Adverse effects are generally mild and temporary and include nausea, vomiting, insomnia, fatigue, and dizziness. Sotalol (Betapace, Sorine): Although all nonselective beta blockers affect heart rate and rhythm, sotalol is one of the few drugs in this class used exclusively as an antidysrhythmic. By slowing the action potential crossing the myocardium, the heart is able to regain normal rhythm. Adverse effects are those typical of beta blockers but they occur more frequently. For example, fatigue may occur in 20% of patients, dyspnea in 21%, and sinus bradycardia in 16%. Patients with a history of dysrhythmias are more likely to experience serious adverse effects. Approved in 1992, the role of sotalol in the pharmacotherapy of dysrhythmias is presented in Chapter 40. Systemic adverse effects are generally mild and transient and include nausea, vomiting, diarrhea, bradycardia, fatigue, and dizziness. Approved in 1978, timolol (Timoptic) is presented as a prototype for glaucoma in Chapter 77. Because of their specificity for beta1 receptors in the myocardium, the beta1-adrenergic antagonists exert fewer noncardiac adverse effects than nonselective agents such as propranolol. This selectivity is not absolute, however; some of these agents affect beta2 receptors at higher doses, and a few have intrinsic sympathomimetic activity. Some are also used in the pharmacologic management of chronic angina pectoris and heart failure. Although used for the same indications as the nonselective agents, the beta1 blockers have certain advantages. The major advantage is that they have little effect on beta2 receptors in bronchial smooth muscle. The beta1 blockers also have less effect on glucose and lipid metabolism than the nonselective agents. Beta blockers must be used with great caution in patients with a history of heart failure because both the nonselective and selective beta1 blockers depress the myocardium. In patients with healthy hearts, this effect is a clinical problem only at high doses. In patients with diseased hearts, however, this depression can worsen cardiac impairment and lead to heart failure. Cardiac failure may develop gradually in patients taking beta blockers for prolonged periods; therefore, the patient should receive regular assessments of cardiac function during therapy. Generally, beta blockers are discontinued or their doses adjusted as soon as heart failure is suspected. Overdose with beta1 antagonists is treated in a manner similar to the nonselective beta blockers. An anticholinergic agent such as atropine or a beta agonist such as isoproterenol may be given to promote bronchodilation and increase the heart rate. Severe hypotension may require the administration of an emergency vasopressor such as dopamine (a beta agonist). Other common adverse effects include dizziness, fatigue, insomnia, bradycardia, heartburn, and dyspnea. Serious adverse effects include agranulocytosis, laryngospasm, complete heart block, and thyroid storm in patients with thyrotoxicosis. Bronchospasm and dyspnea are rare because the drug has little effect on beta2 receptors in bronchial smooth muscle. From what you learned in Chapter 19, identify other catecholamines that are used to quickly raise blood pressure in acute care situations. The therapeutic effects of metoprolol include decreases in heart rate (both resting and during exercise), cardiac output, and blood pressure (both systolic and diastolic). Because it slows the rate and force of myocardial contraction, metoprolol can reduce oxygen demands on the heart and benefit patients with chronic stable angina. Off-label uses include stable, symptomatic heart failure, essential tremor, migraine prophylaxis, and the control of heart rate in patients with atrial dysrhythmias. This agent is contraindicated in cardiogenic shock, severe bradycardia, and heart block greater than first degree. Metoprolol should be used with caution in patients with severe hepatic disease because its major route of excretion is the liver. Metoprolol should be used with caution in patients with asthma and those with a history of bronchospasm because the drug may affect beta2 receptors at high doses. Drug Interactions: Beta1 blockers such as metoprolol have the potential to interact with many different drugs. Because certain calcium channel blockers such as verapamil suppress myocardial contractility, concurrent use with metoprolol can lead to additive bradycardia and even heart block. Use with other antihypertensive drugs has the potential to cause additive hypotension. Certain drugs, including cimetidine and oral contraceptives, can also add to the hypotensive effect of metoprolol.
Syndromes
- Metal cleaners
- Lesions or tumors in the lungs
- Dairy products
- Breathing problems
- Cardiology
- Deciding to breastfeed
- Healthy young people do not need most blood tests.
- Mother who is over 40 years old
- Leave lights on at night so you can see better when walking around your house.
- HIV infection in the mother
Proven pyridium 200 mg
The somatic nervous system consists of nerves that provide for the voluntary control of skeletal muscle gastritis diet education 200 mg pyridium overnight delivery. Process and integrate the environmental changes that are perceived and determine an appropriate response. Respond to the environmental changes as needed by producing an action or response. Some of these drug actions produce desirable, therapeutic effects, whereas others produce adverse effects. The remainder of this chapter reviews the structure and function of this complex system. With its immense potential and complexity, the human brain requires a continuous flow of information to accomplish its functions. In addition, the brain would be useless without a means to carry out its commands. The peripheral nervous system provides the brain the means to communicate with and receive sensory messages from the outside world. For example, one branch causes cardiac muscle to contract faster and with greater force; the other causes it to relax. The ultimate action of the cardiac muscle, smooth muscle, or gland depends on which branch is sending the most signals at any given time. It is essential for the student to learn these actions early in the study of pharmacology because knowledge of autonomic effects is used to predict the actions and adverse effects of many drugs. The sympathetic nervous system is activated under emergency conditions or stress and produces a set of actions called the fight-or-flight response. Activation of this branch prepares the body for heightened activity and for an immediate response to a threat. Heart rate and blood pressure increase and blood is shunted to skeletal muscles, thus preparing the body for sudden, intense physical activity. The bronchi dilate to allow maximum airflow into the lungs, and breathing becomes faster and deeper. At the same time the body is preparing for the threat, nonemergency maintenance functions such as peristalsis and urine formation are temporarily suspended. The parasympathetic nervous system is activated under nonstressful conditions and produces a set of symptoms known as the rest-and-digest response. Digestive secretions increase, peristalsis propels substances along the alimentary canal, and defecation is promoted. The student should notice that the actions of the parasympathetic division are opposite to those of the sympathetic division. Because they have opposite effects, homeostasis may be achieved by changing one or both branches. For example, sympathetic nerves are constantly firing, keeping arterioles in a constant state of constriction. This sympathetic tone allows for faster changes in blood pressure because the vessels are in a constant state of readiness. On the other hand, parasympathetic tone on the smooth muscle of the alimentary and urinary tracts maintains continuous contractions and keeps intestinal peristalsis and urine flow steady. With the important exception of the vascular system, the predominant tone of autonomic tissues is from the parasympathetic nervous system. The sympathetic and parasympathetic divisions do not always have opposite effects. For example, the constriction of arterioles is controlled entirely by the sympathetic branch. Sympathetic stimulation causes constriction of arterioles, whereas lack of stimulation causes vasodilation. The sympathetic division is also solely responsible for the release of renin by the kidneys, an action that increases blood pressure. Metabolic effects such as increases in blood glucose and mobilization of lipids for energy are uniquely sympathetic functions. Erection of the penis is a function of the parasympathetic division, and the sympathetic branch controls ejaculation. For information to be transmitted throughout the nervous system, neurons must communicate with each other and with muscles and glands. A ganglion (singular of ganglia) contains the neuron cell body of the postganglionic neuron, which is waiting to receive the action potential. Before the message can be transferred from one nerve to another, however, it must cross the synapse, a physical space between the two neurons. The communication of the message from one cell to another, or synaptic transmission, utilizes chemical messengers called neurotransmitters. It is important to study the details of synaptic transmission because a large number of drugs affect this process. The process of synaptic transmission is illustrated in Pharmacotherapy Illustrated 16. The second (postganglionic) neuron terminates on smooth muscle, cardiac muscle, or a gland at a specialized synapse called the neuroeffector junction. The neurotransmitter is synthesized in the cell body of the neuron or in the axon terminal where the synapse is located. Over 50 different neurotransmitters have been identified, the most common of which are shown in Table 16. Because nerve impulses travel rapidly from neuron to neuron, there must be an ample and continuous supply of the neurotransmitter. At the terminal ends of each axon lie millions of granules or vesicles loaded with neurotransmitters, waiting for an action potential to release them. When the nerve impulse reaches the end of the axon, it stimulates some of the vesicles to release their stored neurotransmitter into the synapse. The neurotransmitter enters the synaptic cleft, which must be bridged for the impulse to reach the postganglionic neuron or organ. The neurotransmitter travels by simple diffusion across the synaptic cleft to reach receptors that lie on the surface of the postsynaptic cell. Once the neurotransmitter binds to its receptor, the message is conveyed to the postsynaptic cell. The neurotransmitter induces the target muscle cell, glandular cell, or another neuron tissue to elicit its characteristic response. Generally, the more neurotransmitter released into the synapse, the greater and longer lasting the response. Once the message is transmitted, the neuron and the effector cell must return to baseline conditions and ready themselves for future messages. The neurotransmitter is either degraded in the synaptic cleft by enzymes, or it diffuses back into the preganglionic neuron, thus stopping the action of the muscle or gland. Because somatic nerves are myelinated and have no ganglia, impulses more quickly reach their target tissues. Autonomic messages must cross the synaptic cleft, and postganglionic nerves are unmyelinated, which slows the action potential. These drugs cause the neurotransmitter to remain in the synapse for a longer time and will stimulate autonomic actions. Thus when an "autonomic drug" is administered, the goal is not to treat an autonomic disease; it corrects disorders of target organs through its effects on autonomic nerves. The reason is that a large number of drugs affect autonomic function by altering neurotransmitter activity. Some medications are identical to endogenous neurotransmitters, or have a very similar chemical structure, and are able to directly activate a gland or muscle. Other drugs are used to stimulate or block the actions of natural neurotransmitters. A firm grasp of autonomic physiology is essential to understanding the actions of hundreds of drugs. A second potential site for drug action is at the ganglia, the synapse where the preganglionic and postganglionic neurons meet. Yet a third possible site is at the end of the chain, at the neuroeffector junction of the target organs. Located on postganglionic or neuroeffector cell membranes, cholinergic receptors bind Ach and either continue the impulse (at the ganglia) or cause an autonomic action (at the neuroeffector organ).
Order generic pyridium on line
Medial orbital wall invasion or intracranial extension into the anterior cranial fossa is often seen at the time of diagnostic imaging chronic gastritis diet mayo clinic order pyridium no prescription. Internal foci of calcification have also been described, although the presence of calcification does not differentiate this mass from meningioma. MetastaticDisease Sinonasal epithelial malignancy is an important diagnostic consideration. These lesions demonstrate a transcompartmental morphologic pattern, reflecting the primary pattern of tumor progression through direct extension and infiltration of the intracranial contents from the sinuses, classically from the ethmoid air cells. In the sample case, infiltration that appears to be aggressive is noted through the floor of the anterior cranial fossa One of the most common etiologies for intraparenchymal cerebral mass lesions is hematogenous dissemination of metastatic disease. Of the known biopsy-proven neoplasms, lung cancer leads the list (as high as 80% in some series), followed by other common primary neoplasms including breast cancer, melanoma, and colorectal cancer. The presented case is a biopsy-proven metastatic colon cancer focus to the anterior cranial fossa. Note that a key point of distinction from the aforementioned transcompartmental lesions is the intraaxial localization of the lesion within the parenchyma of the frontal cortex. The mass appears transcompartmental, extending from the paranasal sinuses through the floor of the anterior cranial fossa and bilateral medial orbital walls. This lesion is radiographically indistinguishable from a sinonasal epithelial carcinoma, with the diagnosis hinging on pathologic sampling. These neoplasms have the propensity to be quite large at the time of presentation, with involvement of the nasal cavity and paranasal sinuses, and they often extend into the anterior cranial fossa directly through the cribriform plate and ethmoid roof. Anosmia can occur from invasion of the olfactory bulb or nerves or from blockage of air flow to the upper nasal cavity. Infiltration of the skull base foramina also can result in cranial nerve V nerve deficits, with specific extension into the middle cranial fossa and involvement of the foramen ovale and/or foramen rotundum. Meningiomas uncommonly can undergo malignant degeneration into meningosarcoma or atypical meningiomas. Symptoms can range from headaches and hearing loss or vestibular dysfunction to facial paralysis or diplopia. Most benign processes are related to the presence of petrous apex pneumatization, a normal physiologic variant that occurs in up to 30% of the population. The neoplastic processes include both benign entities, such as meningiomas and schwannomas of the facial, trigeminal, or abducens nerves and their branches, and malignant processes, consisting of primary neoplasms. Neoplasms that can arise in multiple locations, including schwannomas, paragangliomas, and meningiomas, are covered in other chapters and will not be discussed here. Asymmetric pneumatization of the petrous apices is commonly observed but can be misconstrued as a pathologic process. The pneumatized apex will be hypointense on T1-weighted imaging, leading to asymmetric T1-hyperintense fat signal in the bone marrow of the contralateral nonpneumatized petrous apex. The presence of fluid signal within the otherwise normally developed petrous apex cells and the absence of expansion or destructive changes in the adjacent bone suggest the diagnosis of trapped fluid in the petrous apex. Some centers continue to monitor these lesions with imaging to ensure stability and to exclude more aggressive entities. However, the presence of an intermediate or hyperintense T1 signal suggests either proteinaceous fluid or a developing cholesterol granuloma, in which case correlation with clinical history and imaging follow-up is necessary in all cases. Cholesterol granulomas (or cholesterol cysts) are expansile, T1- and T2-hyperintense lesions of the petrous apex that may demonstrate peripheral enhancement and are thought to represent inflammatory granulation tissue, which develops in response to cholesterol crystals in the isolated petrous apex cells. Mucoceles of the petrous apex are even more rare than cholesteatomas in this location. Additional imaging features include expansion and smooth scalloping of the adjacent bony margins and absence of enhancement. Occasional "prolapse" of the normally mildly enhancing Gasserian ganglion into the meningocele/cephalocele should not be mistaken for enhancement. The presence of trabecular breakdown in opacified petrous air cells with concurrent mastoid air cell opacification and rimlike enhancement of the fluid-filled cells is highly suspicious for petrous apicitis. Advanced cases of petrous apicitis may demonstrate thickening and enhancement of the adjacent meninges, venous sinus thrombosis, fistulization into the labyrinth, petrous carotid pseudoaneurysm, and findings of skull base osteomyelitis. The presence of osseous destruction and septal erosion should raise concern for one of the neoplastic processes that tend to involve the petrous apex, such as a chordoma, chondrosarcoma, or those that can arise in any osseous structure, such as plasmacytoma or metastatic disease. In a child, histiocytosis and various sarcomas also can arise in or involve the petrous apex. Observation of fat signal intensity in the petrous apex, similar to that of orbital fat and the absence of enhancement or destructive changes, suggests this diagnosis, which can be confirmed with fat-saturation techniques. In children, the marrow may not have converted to fat, but the lack of bony expansion or erosion and stability over time can suggest the diagnosis. Some persons consider mucoceles to be part of a spectrum with cholesterol granulomas (cysts) rather than a distinct entity. Peripheral enhancement in the appropriate clinical setting should suggest this diagnosis; however, aggressive neoplasms could have a similar radiologic appearance. Although chordomas tend to arise in the midline (originating from notochord remnants) and chondroid tumors usually emanate from the petrooccipital synchondrosis, the differentiation between these two entities often is difficult on imaging. However, the presence of chondroid matrix and an off-midline locale is more suggestive of a chondroid neoplasm. The combination of imaging findings with clinical signs and symptoms results in a correct diagnosis in most cases. On the other hand, care must be taken in diagnosing benign findings, such as fluid or asymmetric bone marrow, to avoid aggressive or incorrect management. Although cholesterol granulomas and cholesteatomas are benign lesions, they can result in hearing loss and fistulous communications. Neoplasms and aneurysms must be differentiated from other entities affecting the petrous apex, because they may lead to devastating consequences if incorrectly managed. Some of these entities have distinguishing characteristics, whereas others share overlapping imaging appearances. Dermatologic lesions affecting the pinna are not discussed here and are better evaluated clinically. They are composed of stratified squamous epithelium and exfoliated keratinous material. On imaging, cholesteatomas are erosive, rather than expansile as they are in the middle ear, and may contain bony fragments ("flecks"). On imaging it appears as a homogenous soft tissue density/intensity mass that may remodel, but usually does not erode, the surrounding bone. Keratosis obturans usually affects young male patients, is frequently bilateral, and may lead to conductive hearing loss or otalgia. Cholesteatomas, conversely, usually are unilateral and generally affect elderly persons. Medial canal fibrosis usually presents in the setting of chronic otitis externa, with symptoms ranging from otorrhea to conductive hearing loss. The lesion conforms to the surrounding structures without bony remodeling or erosive changes. Mild peripheral enhancement may occur early in the course, reflecting inflammation and edema. The overlying soft tissues are normal in appearance, with no associated destructive changes. As with exostoses, these lesions can be found in persons with a history of prolonged exposure to cold water, and although an association appears to exist with cholesteatomas and prior surgery, many lesions are found in patients without these predisposing factors. On imaging they demonstrate attenuation/signal characteristics consistent with bony matrix, without aggressive features. Malignant otitis externa (or necrotizing otitis externa) is an invasive infection by Pseudomonas aeruginosa or, less commonly, by Aspergillus fumigatus. It always should be considered in an elderly person with diabetes or in an otherwise immunocompromised patient. The classic route of spread is inferiorly into the soft tissues beneath the temporal bone and then medially beneath the skull base where multiple cranial nerves can be affected. As progressive involvement of the skull base occurs, adjacent dural venous and cavernous sinuses should be evaluated for signs of thrombosis. Other potential complications are related to intracranial extension and include meningitis and cranial nerve palsies. Nuclear imaging offers little additional information in the acute setting, demonstrating increased uptake of the radiopharmaceutical in the affected region.
Order 200mg pyridium free shipping
There is no evidence of adjacent bony remodelling or widening of the neural foramina gastritis diet ������ generic 200 mg pyridium overnight delivery. In summary, there is an intradural extramedullary mass lesion at the level of the conus, which demonstrates increased T1 signal and contrast enhancement. As this is an adult patient, the most likely diagnosis is a spinal metastasis, perhaps secondary to melanoma. The differential diagnoses for an intradural extramedullary lesion also include nerve sheath tumours and meningioma. To take this further, I would like to know if there is a history of malignancy and review any relevant previous imaging. Discussion Intradural extramedullary masses are positioned outside of the spinal cord but within the dural sac. Neurofibromatosis is an important multisystem disorder in the context of the exams. If you suspect this condition, knowledge of the defined diagnostic criteria and other associated manifestations should be used to formulate your management plan for further imaging. It may not be possible to distinguish reliably between a neurofibroma and schwannoma as they share similar imaging characteristics. This appearance occurs when the tumour has both an extradural and an intradural component and is narrowed in the middle as it passes through the neural foramen. These features will allow you to distinguish a nerve sheath tumour from metastases and meningiomas. This situation is relatively common in the viva setting and tests your ability to process information sensibly when confronted with a number of imaging features. In this case, enhancement is a usual feature of a nerve sheath tumour and a meningioma but the high T1 signal is not. Haemorrhage and fat (lipoma/dermoid) can have a high T1 signal but neither enhance. Melanin produces a high T1 signal and melanoma metastases can enhance, therefore a melanoma metastasis is a sensible proposition in this case. Substances with a high signal on T1-weighted imaging include subacute haemorrhage (methaemoglobin), fat, protein, melanin and contrast. There is extensive, intermediate T1 and T2 signal material within the spinal canal. This surrounds the cauda equina at the level of L3 and L4, and extends superiorly in the posterior aspect of the spinal canal to at least the T10 level and beyond the upper limit of the provided images. On the axial image, the lesion is positioned outside the thecal sac, in keeping with an extradural location. In summary, there is an extensive extradural collection in the thoracolumbar spine with peripheral rim enhancement. Discussion Intraspinal masses may be extradural (as in this case), intradural extramedullary (Case 43) or intramedullary (Case 42). It is vital to localise accurately a spinal mass to one of these three compartments early in your description of a case, as this will lead you to the correct list of differential diagnoses. In daily practice, there are several conditions that require urgent action when diagnosed. Good examples of these include a tension pneumothorax, leaking abdominal aortic aneurysm, suspected non-accidental injury and spinal cord compression. In the viva, the examiner will want to see that not only can you diagnose these conditions quickly and confidently but also that you recognise the urgency of the situation. A spinal epidural abscess is a surgical emergency due to the risk of spinal cord compression and subsequent paraplegia. The appearances are characteristic and can be differentiated from the other diagnoses described in the table. By beginning your management plan with the simple phase "this is a surgical emergency" you will effectively convey to the examiner that you are a safe radiologist. Failure to clearly demonstrate this understanding may raise doubts about your ability to practice safely. An extradural abscess usually occurs as a result of local extension from discitis, vertebral osteomyelitis or via haematogenous spread from other sources. Plain films may show a loss of intervertebral disc space height, vacuum phenomenon and bony sclerosis of the adjacent vertebral end plates. You should understand and use the defined descriptions of disc disease such as bulge, protrusion, extrusion and sequestration. In the presence of spinal trauma or anticoagulation, an extradural haematoma is an important additional differential diagnosis to consider. Pearls A diffuse multi-level epidural abnormality with peripheral enhancement is suggestive of epidural abscess. Lung, breast and prostate are the most common tumours to metastasise to the spine. There is a thick asymmetrical periosteal reaction involving both tibial diaphyses, the right radial diaphysis and the whole mandible. In summary, there is marked diffuse periosteal reaction affecting the diaphyses of multiple long bones and the whole mandible. The differential diagnoses include infection, malignancy and prostaglandin therapy. To take this further, I would review the clinical history and any relevant previous imaging. In particular, I would like to know if there is any history of malignancy and to look for evidence of congenital heart disease on chest radiographs. A periosteal reaction is defined as new subperiosteal bone formed in response to soft tissue or osseous disease, detectable by radiographs. There is bilateral symmetrical cortical thickening of varying density ranging from subtle periosteal reaction to solid cortical new bone. Once you have identified diffuse periosteal reaction, important factors to consider and mention are the bone mineral density, the presence or absence of lucent/lytic lesions and whether there is involvement of the metaphyses. Diffuse periosteal reaction with bilateral proximal tibial metaphyseal erosions is typical for congenital syphilis (an "Aunt Minnie"). Also comment on bone mineral density, the presence of bone lesions and the state of the metaphyses. Other important causes of periosteal reaction in children, such as trauma, nonaccidental injury and osteomyelitis, are usually focal rather than diffuse. The sagittal alignment of the C-spine is normal, with no significant prevertebral soft tissue swelling. In the absence of a trauma history, the most likely diagnosis would be a vertebra plana due to eosinophilic granuloma. There is a marked and uniform loss of height of the C5 vertebral body, which has a normal bone marrow signal and no evidence of significant oedema. There is mild indentation of the thecal sac by the collapsed vertebral body but no cord compression or evidence of significant associated soft tissue abnormality. Mycobacterial infection and malignancy should be considered, however, no features of these are demonstrated on these selected images. In long bones, diaphyseal involvement is common and epiphyseal lesions are very rare. The lytic lesions in the pelvis, ribs and long bones may be well or ill-defined, with or without variable periosteal reaction and sclerosis. Differential involvement of the outer and inner skull tables results in a bevelled edge appearance with a double contour. In the mandible and maxilla, destruction of the tooth-bearing alveolar bone can generate a typical "floating teeth" appearance. Pearls Eosinophilic granuloma is the most common cause of a single vertebra plana in a child. In an adult, metastases and infection are the two most common causes of vertebra plana.
Cheap 200mg pyridium overnight delivery
Other differentiating features include the presence of a dural tail gastritis yeast infection safe 200 mg pyridium, 76 Brain and Coverings Vestibular schwannoma (70%-80%) Meningioma (10%-15%) Extraaxial Metastasis Vascular. These lesions become symptomatic only when they are large as a result of their insinuating growth pattern. Because of their softness, epidermoid cysts frequently are observed to surround and even stretch traversing nerves and vessels, as demonstrated in Case D. They can cause trigeminal neuralgia, and on rare occasions they can even cause posterior circulation ischemia. In contrast, arachnoid cysts tend to have a more rounded contour and displace adjacent neural and vascular structures. They also result in smooth deformity of adjacent brain parenchyma and scalloping of adjacent bones because of a slow remodeling process. Unlike supratentorial lipomas, posterior fossa lipomas usually are not associated with congenital malformations. Because of extensive calcification, the mass is markedly T1 and T2 hypointense, susceptibility is present on the gradient echo sequence, and the mass enhances less avidly than does a noncalcified meningioma. An additional small homogeneously enhancing mass consistent with a vestibular schwannoma is seen in the ipsilateral internal auditory canal. Cerebellopontine Angle Cisterns 79 Meningiomas may have prominent dural tails, calcification in 20%, and adjacent bone hyperostosis. Spontaneous or traumatic intracystic hemorrhage can complicate arachnoid cysts but occurs rarely. Rare acute hemorrhagic expansion of a schwannoma also may result in the sudden onset of vertigo or emesis. Bonneville F, Savatovsky J, Chiras J: Imaging of cerebellopontine angle lesions: an update. Purely intracisternal schwannomas may remain asymptomatic until reaching a large size. Patients with choroid plexus carcinomas can receive adjuvant chemotheraphy and/or radiotherapy. Key imaging features that help differentiate these lesions are provided in the following sections. Rare diagnostic considerations include neurocysticercosis, neurosarcoidosis, cavernous malformation, and epidermoid or dermoid cysts. They typically are T1 isointense and T2 hyperintense compared with brain parenchyma. Ependymomas usually occur in the fourth ventricle in children and in the lateral and third ventricles in adults. They typically grow rapidly and enhance and can invade adjacent ependyma and brain parenchyma. They grow slowly and frequently demonstrate little or no enhancement and have intratumoral cystic changes. Ependymomas are more commonly periventricular (70%) than truly intraventricular (30%) when arising supratentorially; therefore they require close scrutiny for parenchymal origin. Other primary tumors that metastasize to the lateral ventricles are melanoma, gastric carcinoma, colon carcinoma, and lymphoma. Central neurocytomas are tumors of young adults (age 20 to 40 years), usually with broad-based apposition to the septum pellucidum. Intraventricular meningiomas typically occur in middle-aged (age 30 to 60 years) females (female/male, 2:1) in the atrium of the lateral ventricle. Furthermore, masses that arise from the suprasellar and pineal regions often appear to be arising from the third ventricle. Rarely, chordoid gliomas have small cystic areas and vasogenic edema along the optic pathways. The cyst also may be mobile within the ventricular system and migrate between examinations. Their location in the anterior third ventricle predisposes them to obstruction of the foramina of Monro and acute hydrocephalus (which may be intermittent), with rare cases of sudden death reported. They usually densely enhance and frequently are marked by cysts, calcification, and hemorrhage. Other Differential Diagnoses Discovered in 1998 and named for its microscopic resemblance to chordomas, all chordoid glioma lesions described to date have been located in the third ventricle. Choroid Plexus Papilloma and Carcinoma Masses that arise from the suprasellar and pineal regions often appear to be arising from the third ventricle. Craniopharyngiomas and germinomas should be considered in the differential diagnosis when an anterior third ventricular mass is visualized. Pineal region tumors and germinomas should be considered when a posterior third ventricular mass is visualized. Restricted diffusion (low apparent diffusion coefficient) is typical because of high tumor cellularity. Extension through the foramina of Magendie (~60%) and Luschka (~15%) frequently occurs. In children, medulloblastomas and ependymomas are the most common masses found in the fourth ventricle. Other pediatric posterior fossa primary neoplasms, including pilocytic astrocytoma and brainstem glioma, occasionally may grow exophytically into the fourth ventricle and mimic a mass of ventricular origin. Although a hemangioblastoma rarely arises within the fourth ventricle, it should be considered in the setting of von Hippel Lindau disease. Subependymomas are often small (<2 cm), but mean lesion size is approximately 4 cm in symptomatic patients with hydrocephalus. Choroid Plexus Papilloma and Carcinoma Choroid plexus tumors occur in the lateral ventricle (50% of cases), fourth ventricle (40% of cases), and third ventricle (10% of cases). Choroid plexus tumors occur most commonly in young adults (median age, 23 years) when they appear in the fourth ventricle. In adults, a cerebellar hemispheric location is more common; this finding is thought to be related to the superolateral migration of undifferentiated cells with oncogenic potential originating in the posterior medullary velum. In less clear-cut cases, a careful search for parenchymal or cisternal disease will increase diagnostic specificity. Ependymomas are differentiated from medulloblastomas by a higher likelihood of demonstrating calcifications, hemorrhage (T2 imaging), higher diffusivity, and "plastic" tumor behavior with extrusion through the foramina of Magendie and Luschka. Thought to arise from subependymal glia, subependymomas are benign (World Health Organization grade I), often incidental tumors that are most commonly seen in middle-aged or elderly men. Approximately 10% demonstrate an admixture of ependymoma on histopathologic examination. Modern microsurgical techniques yield good outcomes, even with subtotal resection. A sagittal postcontrast fat-saturated image demonstrates an irregular, mildly thickened, and mildly nodular rim of enhancement. Although solid or vascular lesions related to the optic nerves or chiasm, the circle of Willis, the hypothalamus, or pituitary infundibulum present at this site, the identification of a cystic-appearing lesion significantly narrows the differential diagnosis. When evaluating a cystic suprasellar lesion, the presence of nodular or frankly solid enhancing components suggests a neoplastic lesion, the most common of which is an adamantinomatous craniopharyngioma. Craniopharyngiomas may be sellar and suprasellar, exclusively suprasellar, or purely intrasellar. They demonstrate a bimodal distribution, with two thirds of them presenting in childhood/adolescence and a second smaller peak generally presenting in middle to late adulthood. Childhood craniopharyngiomas tend to be adamantinomatous and present as predominantly cystic or solid and cystic lobulated masses with hemorrhage and calcification. Adult craniopharyngiomas tend to be papillary and present more often as predominantly solid or mixed solid and cystic masses. As noted, careful inspection for the presence of nodular or frankly solid enhancing components should be performed. Nodular or rimlike calcification involving cyst walls or solid components is highly suggestive of this diagnosis. The hallmark characteristics of predominantly cystic craniopharyngiomas are calcification, cyst formation, and nodular and/or rim enhancement. Furthermore, other less common neoplastic lesions that typically present as cystic and solid masses, such as hypothalamic/optic pathway juvenile pilocytic astrocytomas, should be considered in the appropriate clinical setting. Approximately 80% of these lesions are seen between the anterior and posterior pituitary lobes.
W-3 Fatty Acid (Epa (Eicosapentaenoic Acid)). Pyridium.
- Psoriasis.
- What is Epa (eicosapentaenoic Acid)?
- Treating symptoms of cystic fibrosis.
- Reducing the risk of heart attack, stroke, and other cardiovascular problems in people with heart disease.
- Reducing growths in the uterus.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96955
Cheap pyridium 200 mg overnight delivery
Enhancement is noted along the surgical tract gastritis znacenje discount 200mg pyridium overnight delivery, most likely representing postoperative granulation tissue. Imaging findings supportive of a pyogenic infectious etiology, such as Staphylococcus aureus infection involving the disk space, include the presence of paraspinal and/or epidural inflammation and phlegmonous change, disk enhancement, T2 hyperintensity in the disk space, and erosion or destruction of the adjacent endplates. One of the most valuable signs of infection is the identification of paraspinal or epidural inflammatory/phlegmonous change, though it is not entirely sensitive, especially in early infection. Infected disks almost always enhance; in particular, rim enhancement of the disk appears to be more specific for infection than partial or diffuse disk enhancement. Partial or heterogeneous vertebral marrow involvement beyond the endplates can be seen and even involve the entire vertebral body. Early infection may not demonstrate these classic imaging features; therefore the presence of T2 isointensity or hypointensity within the disk does not exclude infection. Conversely, although T2 hyperintensity of the disk suggests infection, it is not a specific sign and may also be seen in inflammatory conditions. Imaging features seen with tuberculous spinal infections include subligamentous spread, marked paraspinous inflammatory change, paraspinal abscesses with thick peripheral enhancement, calcifications within the paraspinous inflammatory change, and fragmentary osseous destruction. A relatively preserved disk space in the setting of such findings is an especially strong marker of tuberculous infection. Tuberculous spinal infections tend to involve the thoracic spine more often than the lumbar spine. Slow progression and chronic symptoms suggest tuberculous rather than pyogenic infection. In severe and/or chronic cases, progression to kyphotic angulation, vertebral body destruction, or even vertebra plana may be seen. Although two or three adjacent vertebral bodies often are involved, noncontiguous vertebral body involvement may be seen. Because tuberculous spinal infection may involve multiple noncontiguous vertebral bodies and spare the disk space, it may be confused with metastatic disease. However, paravertebral abscesses/phlegmonous change and subligamentous spread are strong indicators of tuberculous infection. However, given the imaging overlap between these two states, correlation with clinical markers of infection is essential. This can include a suggestive physical examination and set of patient symptoms, fever, and blood test results, such as elevated erythrocyte sedimentation rate, C-reactive protein, and white blood cell count. A hypointense fracture line can be seen parallel to the inferior endplate on T1 and T2 images, and there is mild retropulsion of a small fracture fragment from the posteroinferior corner of the vertebral body. Low signal completely replaces the normal T1 bright marrow signal on T1-weighted imaging. On contrast-enhanced imaging, diffuse heterogeneous enhancement of the vertebral body is present with confluent paraspinal and epidural soft tissue extension. Additional enhancing lesions can be seen in the S1 vertebral body and the L5 spinous process. Causes of benign compression fractures include osteoporosis, trauma, eosinophilic granuloma, Paget disease, and hemangioma; malignant compression fractures can arise from metastatic disease or primary neoplasms, such as multiple myeloma, lymphoma, leukemia, and primary bone tumors. Distinguishing benign from malignant fractures is sometimes difficult and may have important implications for patient treatment and prognosis. Diffuse homogeneous replacement of normal bone marrow signal with low signal on T1-weighted images suggests a malignant fracture, whereas benign fractures often demonstrate partial or more inhomogeneous replacement. Other features that suggest a malignant etiology include involvement of the pedicles and/or posterior elements, a diffuse convex bulge of the posterior vertebral body cortex, and a paraspinal and/or epidural mass. Malignant fractures usually show diffuse or patchy heterogeneous enhancement of the vertebral body on postcontrast images, and additional metastases may be visualized elsewhere in the spine (with or without associated fractures) in many cases. Signs that support benign osteoporotic fractures include the presence of fluid signal adjacent to the fractured endplate (fluid sign); a retropulsed fracture fragment, a low signal intensity band adjacent to the fractured endplate corresponding to the fracture line, and an intravertebral vacuum cleft. Other malignant signs include a paraspinal mass larger than 5 mm or an epidural mass. Visualization of distinct fracture lines (as opposed to destruction, diffuse vertebral sclerosis, or an intravertebral vacuum cleft) are features suggestive of a benign etiology. The presence of multiple compression fractures does not allow generalization about their etiology, so the features of each of the fractures should be individually evaluated. In addition, the above criteria are not reliable in acute traumatic compression fractures, which can resemble malignant fractures, or in fractures associated with multiple myeloma, which can mimic benign fractures. The fluid sign can support a benign, osteoporotic etiology for a compression fracture and is rarely seen in persons with malignant fractures. A sagittal short T1 inversion recovery image demonstrates linear hyperintense signal adjacent to the fractured superior endplate (arrow). This patient later underwent a vertebral augmentation procedure, and a bone biopsy obtained during that procedure confirmed the benign, osteoporotic nature of the fracture. Adjacent osseous permeative lytic changes are noted within the left temporal bone and mastoid air cells. Intracranial extension of the fluid collection into the left temporal epidural space is observed, with mass effect and edema within the adjacent left temporal lobe. First branchial apparatus anomalies are congenital anomalies that occur during the development and differentiation of the mesodermal arches, ectodermal cleft, and endodermal pouch. Internally, the first and second arches are separated by an endodermally lined pouch that gives rise to the eustachian tube and middle ear cavity. Either failure of the cleft/pouch to be completely obliterated or the presence of cell rests or remnants of the branchial apparatus can result in an external or internal sinus, a fistula, and/or an isolated cyst. Recurrent, chronic otorrhea in the absence of chronic otitis should raise the suspicion for first branchial apparatus anomalies. They often are located within the parotid gland, with a variable association with the facial nerve. Treatment involves complete surgical excision with a parotidectomy and dissection to preserve the facial nerve; otherwise, recurrence is common. The variable location of first branchial apparatus lesions that are lying superficial, deep, or even in between branches of the facial nerve may complicate surgical resection. Important lesions to consider in the differential diagnosis of a branchial cleft cyst include diseases arising in the lymph nodes, such as suppurative infection or metastases, as well as other causes of parotiditis, abscess, or cystic parotid neoplasms. In adults or elderly patients, it is extremely important to consider and exclude cystic, necrotic lymph node metastases as a primary differential diagnosis. Metastatic lesions most commonly arise from cutaneous squamous cell carcinomas or cutaneous malignant melanoma of the upper face or scalp. Metastases and lymphatic malformations will appear more heterogeneous and may extend across neck compartments. Infected branchial cleft cysts may be difficult to differentiate from metastases or granulomatous infections, but clinical clues often help. When considering metastases as a differential diagnosis, look for a primary lesion typically arising from the skin of the face or scalp. In older patients presenting with a cystic lesion, primary lesions, cutaneous metastatic squamous cell carcinoma, or melanoma should be suspected. These lesions may be removed with a retroauricular incision, keeping the skin of the external auditory meatus intact. Type 2 lesions, which may have both mesodermal and ectodermal components, may present as cysts, sinuses, or fistulae. They may lie more inferior than type 1 lesions, lying below the angle of the mandible and deeper within the parotid gland, anterior to the sternocleidomastoid muscle. To safely remove Work type 2 lesions at surgery, it is important to first identify the facial nerve in relation to the lesion at the stylomastoid foramen and trace it distally. These lesions also may involve the tympanic membrane or middle ear structures, which will affect the surgical procedure. The first branchial pouch anomaly most commonly manifests as a short eustachian tube, clinically presenting in children with recurrent otitis media. A rare lateral nasopharyngeal cyst also may represent a first, or possibly a second, branchial pouch remnant, lying between the posterior pillar and the pharyngeal opening of the pharyngeal eustachian tube.
Buy pyridium 200mg overnight delivery
If present gastritis university of maryland buy generic pyridium canada, the classic clinical history of a young patient (between 10 and 20 years) with intensely painful scoliosis that is worse at night and is relieved by aspirin or other nonsteroidal antiinflammatory drugs may help clinch the diagnosis. Osteoblastomas are similar pathologically to osteoid osteomas but are larger, measuring more than 1. They usually affect the posterior elements, although progression to involve the vertebral body is common. The imaging appearance of osteoblastomas may be identical to that of large osteoid osteomas, but osteoblastomas are more likely than osteoid osteomas to be expansile and contain multifocal matrix calcification (which may simulate chondroid matrix). Osteoblastomas may also appear to be quite aggressive, with bone destruction and extension into the adjacent soft tissues. Spinal osteochondromas can arise from any portion of the vertebra but predominately arise from the posterior elements and are most often encountered in the atlantoaxial region of the cervical spine. They most often are found in the posterior elements but frequently grow to involve the vertebral body. Many other lesions may affect the posterior elements, although without a clear posterior predilection per se. These lesions include metastases, which are the most common spinal tumors overall. Other lesions include lymphomas, myelomas, chondrosarcomas, osteosarcomas, Ewing sarcomas, giant cell tumors, and chondroblastomas. T1-weighted precontrast and postcontrast images show heterogeneous enhancement of an amorphous T1 hypointense sacral mass with extension into both the presacral and epidural spaces. Primary sacral tumors include malignant entities such as chordomas, osteosarcomas, Ewing sarcomas, and plasmacytomas as well as more benign entities such as giant cell tumors, hemangiomas, aneurysmal bone cysts, and osteoblastomas. Secondary malignancies may result from hematogenous or direct spread of metastatic disease. Nearly half of all chordomas occur in the sacrum, whereas only 15% occur in the remainder of the spine; 35% occure in the clivus, the second most common site of involvement. Chordomas originate from intraosseous notochordal remnants and almost always occupy a midline or paramedian location in the distal sacrum. Giant cell tumors are the second most frequent primary tumor of the sacrum and occur in this location in 1% to 8% of cases. Most of these lesions arise in long bones, typically the distal femur and proximal tibia. In contrast to chordomas, sacral giant cell tumors are frequently eccentric and abut or extend across the sacroiliac joint. Multiple myeloma is the second most common primary sacral malignancy after chordoma and represents a monoclonal proliferation of malignant plasma cells of the bone marrow. Plasmacytoma is the unifocal form of multiple myeloma and usually has a better prognosis than multiple myeloma. The classic appearance of multiple "punched out" lesions is an alternative appearance. These lesions include primary lesions of bone, including those described in this chapter; primary neural tumors; and metastatic lesions. Primary bone lesions presenting as sacral masses are overwhelmingly lytic in appearance. Another osteolytic mass is the sacral osteoblastoma, which constitutes 17% of all spinal osteoblastomas and often occurs in association with aneurysmal bone cysts. Although chondrosarcoma is the most common malignant primary bone neoplasm in adults, involvement of the sacrum is unusual. This appearance is distinct from that of chordomas, which tend to occupy a central position. Primary neural tumors presenting as sacral masses may include nerve sheath tumors, such as neurofibromas and schwannomas. These tumors originate from lumbar or sacral nerve roots and appear as intradural extramedullary masses, frequently with extradural components that assume a characteristic dumbbell shape and extend through the neural foramina. Both neurofibromas and schwannomas may exhibit a "target" appearance on T2-weighted sequences, with central low signal surrounded by high signal. Axial computed tomography image demonstrates a large multiloculated expansile lytic cyst in the left lower sacrum. A dominant loculation demonstrates a fluidfluid level, a characteristic finding of these lesions. An axial computed tomography image illustrates a large, destructive lytic lesion centered about the right sacroiliac joint, with a characteristic ring-and-arc matrix typical of cartilaginous lesions. Conversely, giant cell tumors often exhibit a conspicuous absence of calcification or osseous matrix. Chondrosarcomas may have a ring and arc pattern of calcification typical of cartilaginous lesions. Giant cell tumors occur in patients between 20 and 40 years of age and affect women more frequently than men. A coronal reformatted image from a computed tomography scan demonstrates widening of the left L5-S1 neural foramen and destruction of the left hemisacrum by a large neurofibroma in a patient with neurofibromatosis type 1. Other neurologic symptoms such as numbness, weakness, radicular pain, and incontinence can ensue from nerve root compression or infiltration. Sacral chordomas are slowly growing tumors that may present with metastases in the lung, liver, lymph nodes, or bone. However, local malignant transformation occurs in up to 2%, often after radiotherapy is administered. Multiple myeloma often occurs in the setting of osteopenia and is frequently complicated by a pathologic fracture. Additional complications, such as infection and anemia, may result from marrow failure. Chemotherapy and local radiation are preferred treatments for persons with multiple myeloma. Multiple myeloma may appear as a solitary, large, infiltrative lesion with soft tissue components that span the intraosseous and extraosseous compartments. Giant cell tumors, by contrast, are usually eccentric in location and may abut or traverse the sacroiliac joints. Sacral myeloma may appear anywhere within the sacrum but rarely crosses disk spaces. Dermoid/EpidermoidCyst Although dermoid and epidermoid cysts may appear identical to branchial cleft cysts, dermoid cysts often contain fat. No calcifications are identified within the structure or are associated with the structure. Parotiditis Other causes of parotiditis may be included in the differential for first branchial cleft anomalies. Note that the masses appear solid and contain small, hypodense, cystic-appearing components. These masses were proven by pathology to be Warthin tumors, although the differential diagnosis based on imaging included matted lymph nodes, metastases from squamous cell carcinoma, or other primary parotid tumors. In contrast to first branchial cleft anomalies, cystic parotid gland tumors, including Warthin tumors, are found in an older population and usually have solid components or septations. These cystic parotid lesions may be considered in the differential diagnosis for first branchial cleft cysts. Suppurative Lymphadenitis: Suppurative lymph nodes within the parotid gland or along the cervical lymph node chain may be a differential diagnosis for infected first and second through fourth branchial cleft cysts, respectively. Similar to infected branchial apparatus lesions, suppurative lymphadenopathy may develop following another head and neck infection, beginning as reactive nodes and developing into an intranodal abscess. Cold Abscess: Tuberculous or nontuberculous mycobacterial infection may present as cystic-appearing necrotic lymph nodes without significant surrounding inflammatory change. Necrotic Lymph Node Metastases: Most parotid lymph node metastases are from cutaneous squamous cell carcinomas or melanomas of the upper face or scalp.
Cheap pyridium 200 mg fast delivery
The diagnosis the diagnosis of fibromyalgia is a clinical construct and should not be dependent upon fulfilling criteria for an individual patient gastritis ibs diet cheap 200 mg pyridium with mastercard. Criteria for fibromyalgia were primarily developed to ensure homogeneity of patient cohorts for the purpose of research. A diagnosis of fibromyalgia should be considered when a patient presents with widespread body pain Neuropathic Pain, ed. The physical examination will help to exclude most other conditions that can present with diffuse pain such as arthritic or neurological diseases, while simple blood testing will exclude most other medical conditions. Additionally, a definitive diagnosis does not require confirmation by a specialist. Physicians should be satisfied in making a definitive diagnosis in the clinic and avoid unnecessary investigations. The hallmark of fibromyalgia has for years been the presence of tender points which simply represent increased sensitivity to soft tissue palpation and a reduced pain threshold. Although pain is usually assessed as intensity, pain quality which represents the emotional component of pain is equally important, and should be addressed. Sleep complaints include difficulty falling asleep, frequent wakening, early morning wakening, and feeling unrefreshed. Overall, non-restorative sleep with fragmentation and reduction in the length of stage 2 sleep is an important element and associates with pain complaint. Abnormal components of sleep that have been measured include sleep latency, sleep disturbance, and fragmented sleep leading to impaired daytime function [6]. Poor quality and short duration of sleep impacts fatigue, affect, and pain, with improvement in these parameters when sleep is specifically addressed. Other sleep disorders such as restless leg syndrome or sleep apnea may also occur in patients with fibromyalgia. The typical patient with fibromyalgia the typical patient is female in her 40s, with a history of ill-defined musculoskeletal pain over a number of years. Onset of symptoms is usually gradual, but may be more abrupt following an identifiable event, such as medical illness or trauma. Fibromyalgia should not be diagnosed by exclusion but rather positively, following a comprehensive medical history and physical examination, and with only limited laboratory testing in most cases [4,5]. The clinical presentation of fibromyalgia can be quite diverse with some areas of the body more painful than others, fluctuations in intensity of pain and other associated symptoms. This heterogeneity within the fibromyalgia patient population is increasingly appreciated. Almost all patients will have a symptom complex characterized by the presence of four major complaints of widespread pain, sleep disturbance, fatigue, and cognitive changes, all of variable intensity [3]. Additional symptoms include mood changes, irritable bowel syndrome, migraine headaches, and hypersensitivity phenomena. Each of these symptoms plays a discrete role in the presentation of an individual patient, and all contribute towards poor well-being. Fatigue Fatigue is a prominent feature with important implications regarding function. Patients awaken in the mornings feeling tired and unrefreshed and may require extraordinary effort to perform even simple tasks such as maintaining a household. Fatigue is gauged by subjective patient report and is probably the most difficult symptom to address in patients with fibromyalgia. Pain Pain occurs throughout the body, with some patients reporting pain from the top of the head to the bottom of the feet. Pain quality is described as diffuse, aching, or burning, often with a waxing or waning pattern. Almost a third of patients describe a neuropathic-like pain by using words such as "burning," "prickling," and "pins and needles. Mood disorder plays a role in global health status, with depression and/ or anxiety present in up to three-quarters of persons with fibromyalgia. Anxiety commonly coexists with depression, but is also independently increased in fibromyalgia patients. Depression is influenced by factors such as low family cohesion, high pain, helplessness, and passive coping skills. Although there remains considerable overlap between fibromyalgia and major depressive disorder with regard to neuroendocrine abnormalities, psychological characteristics and physical symptoms, the body of evidence currently suggests that these are two distinct disorders rather than subsidiaries of the same construct [9]. The sensitivity to pressure is reflective of hyperalgesia which represents a reduced pain threshold and an exaggerated perception of a painful stimulus. Expression of pain or pain behaviors may be present but should not imply faking of symptoms. Testing There is no laboratory investigation that confirms a clinical diagnosis of fibromyalgia. Unnecessary investigations should be avoided and fibromyalgia should not be a diagnosis of exclusion [5]. Appropriate additional testing, which might include referral for sleep evaluation or formal psychological evaluation, may be required in selected patients. Excessive and unnecessary testing may be detrimental to patient well-being by promoting an illness-centered focus and fostering a sense of uncertainty. Other symptoms Other symptoms that may occur in fibromyalgia patients include irritable bowel syndrome, migraine headaches, severe menstrual pain, lower urinary tract symptoms, myofascial facial pain, and temporomandibular pain. Some patients complain of hypersensitivity to outside stimuli such as sound, light, and odors [4]. Sexual dysfunction, previously unrecognized, is also present for many fibromyalgia patients. Breast implants were at one time implicated in causation of fibromyalgia, however the weight of the evidence is against any association. Similarly, cigarette smoking has been associated with more severe fibromyalgia symptoms, rather than fibromyalgia per se. Conditions that may be confused with fibromyalgia There are some medical conditions that may be confused with fibromyalgia and fibromyalgia may also coexist with some other illnesses [5,10]. Inflammatory arthritis in the early stages may present as generalized body pain, but objective physical and laboratory abnormalities will soon be manifest. Myofascial pain syndromes present with pain that is more localized and there may be associated trigger points. Endocrine conditions that may cause pain are hypothyroidism and hyperparathyroidism. Multiple sclerosis may masquerade as ill-defined body pain, whereas neuropathies will more likely have localized pain. Some patients with depression report pain, although local tenderness is more common in fibromyalgia patients compared with those with depression. Persons with personality and substance abuse disorders may falsely Examination the physical examination in patients with fibromyalgia is within normal limits except for tenderness of soft tissues. Specifically, the musculoskeletal and neurological examination is usually normal, including absence of joint or muscle abnormality. Some patients may demonstrate a sensitivity to light touch, not in any recognizable neurological distribution and interpreted as dysesthesia or touch allodynia (unpleasant sensation or pain after a non-painful stimulus). The presence of tenderness on 207 Section 5: the Specific Condition: Other Causes of Neuropathic Pain report the presence of diffuse pain, with the objective for secondary gain. Infectious diseases such as Lyme disease, hepatitis C infection, and human immunodeficiency virus may have symptoms mimicking fibromyalgia, but any testing in this regard should be dependent upon a clinical suspicion of these infections. Medications that may induce body pain include the lipid lowering agents, aromatase inhibitors used to treat breast cancer, bisphosphonates for the treatment of osteoporosis and bone metastases, and opioids that can induce hyperalgesia. Chemotherapy agents, which are more commonly recognized to cause peripheral neuropathy, may also cause diffuse pain symptoms. Evidence for a genetic predisposition to fibromyalgia, which is likely polygenetic, is based on abnormalities attributed to the serotoninergic, catecholaminergic, and dopaminergic systems, with possible links with the stress-response system [11]. Psychological and stress-related factors Psychological and stress-related factors may also contribute to the development of fibromyalgia. Psychosocial distress predicts onset of diffuse pain in population studies conducted in England. Early life adversity such as the death of a mother, being in institutional care, or family financial hardships was linked to adult diffuse pain. Abuse which may have been sexual, physical, or psychological, particularly in childhood, has been reported with greater frequency in fibromyalgia patients than in controls [14].
200 mg pyridium with amex
Different hypotheses have been proposed to explain why some patients with chronic shunting and pachymeningeal enhancement are asymptomatic and do not have a sunken appearance of the supratentorial structures; these hypotheses are beyond the scope of this text gastritis diet 21 buy discount pyridium 200mg line. It also is noteworthy that the case presented is an extreme example of pachymeningeal thickening and enhancement and a wide spectrum of findings may be seen with shunting, ranging from minimal enhancement to prominent enhancement with marked thickening. Even without any leptomeningeal enhancement, pachymeningeal enhancement can be seen with metastatic disease, especially in the presence of skull metastases, as in Case C. Such pachymeningeal thickening and enhancement does not necessarily represent neoplastic invasion of the dura and can represent an inflammatory reaction. Presumably, such enhancement may be seen with metastases from any primary malignancy, but common extracranial sources include breast and prostate metastases. Pachymeningeal enhancement also can be seen with hematologic malignancies, as in Case D. Neurosarcoidosis and Wegener granulomatosis are included in these conditions, among others. Evaluation of the sinus too far medially or laterally may result in erroneous interpretation. A high index of suspicion is required for accurate diagnosis of this treatable condition. The lesion also is hyperintense on T2-weighted imaging, and chemical shift artifact is noted. The lesion is markedly hyperintense on T1-weighted imaging and hyperintense on T2-weighted imaging, with chemical shift artifact. The lesion does not enhance and is hypointense on the fat-saturated T1 postcontrast sequence. The lesion demonstrates heterogeneous signal on T2-weighted imaging, with areas of both hypointensity and hyperintensity and subtle chemical shift artifact. Susceptibility artifact is associated with the lesion on the gradient echo sequence. On follow-up imaging for a severe headache 9 years later, multiple foci of T1 hyperintense signal are now seen in the subarachnoid space adjacent to the posterior right vermis. The T2 signal within these foci is now more homogeneous and isointense to the adjacent parenchyma. The T2 sequence demonstrates the chemical shift artifact associated with these foci of fat. Teratomas are usually heterogeneous, often contain calcification and soft tissue density in addition to lipid, and usually are in the pineal region. Intracranial dermoid cysts are benign ectodermal inclusion cysts that arise from inclusion of cutaneous elements at the time of neural tube closure. On imaging, dermoids are round or lobulated unilocular cystic masses with well-circumscribed margins. They typically occur at or near midline and are most commonly found in the suprasellar, parasellar, or frontonasal regions. They also can occur in the posterior fossa, typically adjacent to the vermis or within the fourth ventricle. A fistulous connection to the skin (dermal sinus) may be present with spinal, anterior, or posterior fossa lesions. Dermoid cysts do not enhance, although the capsule may demonstrate minimal linear enhancement. Intracranial lipomas are congenital malformations rather than true neoplasms or hamartomas. They are thought to arise from 40 Brain and Coverings abnormal persistence and maldifferentiation of the meninx primitiva, a mesenchymal derivative of the neural crest. Lipomas tend to occur in the subarachnoid spaces, including the dorsal pericallosal, quadrigeminal, ambient, interpeduncular, and chiasmatic cisterns. Dermoid cysts tend to be less lobulated than lipomas and will displace blood vessels and nerves rather than encase them. Capsular calcification can vary from none to extensive but typically is seen only with pericallosal interhemispheric lipomas and occurs less commonly than with dermoid cysts. These lesions will become hypointense on fat-suppressed images and do not enhance. Dermoids typically demonstrate higher average Hounsfield units when compared with lipomas. This observation may be due to the presence of sebaceous lipid in dermoids rather than mesodermal (adipose) fat or could reflect the greater heterogeneity of dermoids because of the presence of additional ectodermal elements (such as hair follicles, apocrine glands, and proteinaceous debris). Whereas epidermoids are lined solely by squamous epithelium, dermoid cysts contain dermal elements, including hair follicles and sebaceous and sweat glands. Their etiology is similar, but epidermoids are thought to occur slightly later in embryogenesis and typically are found off of midline. These lesions tend to occur almost exclusively in the cerebellum and are thought to have high protein concentrations. These lesions will be T1 hyperintense because of the protein content but extremely hypointense on T2-weighted imaging. Dermoid cysts can rupture, with subarachnoid and intraventricular spread of contents. Extensive leptomeningeal enhancement is seen in the setting of rupture in patients with chemical meningitis. Interhemispheric/pericallosal lipomas can occur in two subtypes, which are named according to their morphology. The tubulonodular subtype tends to occur anteriorly and can demonstrate rim calcification. The curvilinear subtype is typically posterior, curving around the callosal body and splenium. Lipomas of the sylvian fissure can be associated with aneurysms of the middle cerebral arteries. C and D, Magnetic resonance imaging reveals that the lesion has only minimal linear foci of T1 hyperintense signal centrally. Initially this lesion was thought to be an epidermoid cyst, but at surgery it was found to be a dermoid. Whereas dermoids typically are frontobasalar, suprasellar, parasellar, vermian, or fourth ventricular lesions, lipomas most frequently are located in the region of the corpus callosum, as well as near the tuber cinereum, the quadrigeminal plate, and the ambient cistern. Lipomas encase and engulf vessels and nerves, whereas dermoid cysts displace them. Dermoids tend to be more heterogeneous, with higher Hounsfield units and greater standard deviations compared with lipomas. C and D, Magnetic resonance imaging reveals T1 hyperintense signal within the fat fluid level and chemical shift artifact associated with the fatty component of the lesion. The tubulonodular subtype of pericallosal interhemispheric lipomas can have rim calcification, but this finding is rare in parasellar and posterior fossa lesions. Lipomas also tend to show striking chemical shift artifact, which often is less apparent with dermoid cysts. A fat density lesion with peripheral calcification centered in the interhemispheric fissure is partially imaged. Magnetic resonance imaging reveals a lobulated, markedly T1 hyperintense lesion abutting the superior margin of the corpus callosum.
