
Reminyl 8mg fast delivery
Calcium-channel Blockers: increased risk of myocardial depression and asystole when flecainide given with medicine logo cheap 8 mg reminyl. Diuretics: increased cardiac toxicity with flecainide if hypokalaemia occurs with. Cytotoxics: fludarabine increases intracellular concentration of cytarabine; increased pulmonary toxicity when fludarabine given with. Anti-arrhythmics: possible increased risk of bradycardia when fingolimod given with. Calcium-channel Blockers: possible increased risk of bradycardia when fingolimod given with. Anxiolytics and Hypnotics: fosamprenavir possibly increases plasma concentration of. Lipid-regulating Drugs: possible increased risk of myopathy when fosamprenavir given with atorvastatin; possible increased risk of myopathy when fosamprenavir given with. Pentamidine Isetionate: increased risk of hypocalcaemia when foscarnet given with parenteral. Antivirals: plasma concentration of both drugs increased when fusidic acid given with. Lipid-regulating Drugs: risk of myopathy and rhabdomyolysis when fusidic acid given with. Antivirals: ganciclovir possibly increases plasma concentration of didanosine; profound myelosuppression when ganciclovir given with. Anti-arrhythmics: grapefruit juice increases plasma concentration of amiodarone; grapefruit juice increases plasma concentration of. Antihistamines: grapefruit juice reduces plasma concentration of bilastine; grapefruit juice increases plasma concentration of. Cytotoxics: grapefruit juice possibly increases plasma concentration of axitinib; grapefruit juice possibly increases the plasma concentration of. Lipid-regulating Drugs: grapefruit juice possibly increases plasma concentration of atorvastatin; grapefruit juice increases plasma concentration of. Anticoagulants: increased risk of haemorrhage when other anticoagulants given with. Antifungals: histamine H2-antagonists reduce absorption of itraconazole; avoidance of histamine H2antagonists advised by manufacturer of posaconazole (plasma concentration of posaconazole possibly reduced); cimetidine reduces plasma concentration of. Antivirals: manufacturer of atazanavir advises adjust doses of both drugs when cimetidine and nizatidine given with atazanavir-consult atazanavir product literature; famotidine and ranitidine reduce the plasma concentration of. Cytotoxics: cimetidine possibly enhances myelosuppressive effects of carmustine and lomustine; cimetidine increases plasma concentration of. Ulipristal: avoidance of histamine H2-antagonists advised by manufacturer of high-dose. Cytotoxics: increased risk of ventricular arrhythmias when ondansetron given with. Antivirals: increased risk of convulsions when imipenem with cilastatin given with. Aldesleukin: plasma concentration of indinavir possibly increased by aldesleukin Anti-arrhythmics: indinavir possibly increases plasma concentration of. Colchicine (continued) colchicine (avoid concomitant use in hepatic or renal impairment) Corticosteroids: plasma concentration of indinavir possibly reduced by dexamethasone. Cytotoxics: indinavir possibly increases plasma concentration of axitinib (reduce dose of axitinib-consult axitinib product literature); indinavir possibly increases the plasma concentration of. Lipid-regulating Drugs: possible increased risk of myopathy when indinavir given with atorvastatin; possible increased risk of myopathy when indinavir given with. Antivirals: caution with peginterferon alfa advised by manufacturer of adefovir; increased risk of peripheral neuropathy when interferon alfa given with. Anti-arrhythmics: increased risk of ventricular arrhythmias when ivabradine given with. Antifungals: plasma concentration of ivabradine increased by fluconazole-reduce initial dose of ivabradine; plasma concentration of ivabradine possibly increased by. Antimalarials: increased risk of ventricular arrhythmias when ivabradine given with. Antipsychotics: increased risk of ventricular arrhythmias when ivabradine given with. Beta-blockers: increased risk of ventricular arrhythmias when ivabradine given with. Pentamidine Isetionate: increased risk of ventricular arrhythmias when ivabradine given with. Antiepileptics: plasma concentration of lamotrigine often reduced by carbamazepine, also plasma concentration of an active metabolite of carbamazepine sometimes raised (but evidence is conflicting); plasma concentration of lamotrigine reduced by phenobarbital and phenytoin; plasma concentration of lamotrigine increased by. Cytotoxics: lapatinib increases plasma concentration of pazopanib; possible increased risk of neutropenia when lapatinib given with docetaxel; increased risk of neutropenia when lapatinib given with. Calcium-channel Blockers: plasma concentration of lenalidomide possibly increased by. Dapoxetine: possible increased risk of serotonergic effects when lithium given with. Antiepileptics: plasma concentration of lopinavir possibly reduced by carbamazepine. Cytotoxics: manufacturer of ruxolitinib advises dose reduction when lopinavir given with. Lipid-regulating Drugs: possible increased risk of myopathy when lopinavir given with atorvastatin; possible increased risk of myopathy when lopinavir given with. Analgesics: erythromycin increases plasma concentration of alfentanil Antacids: absorption of azithromycin reduced by antacids Anti-arrhythmics: increased risk of ventricular arrhythmias when parenteral erythromycin given with. Antihistamines: manufacturer of loratadine advises erythromycin possibly increases plasma concentration of loratadine; macrolides possibly inhibit metabolism of. Antivirals: plasma concentration of both drugs increased when clarithromycin given with atazanavir; plasma concentration of clarithromycin reduced by efavirenz, also plasma concentration of active metabolite of clarithromycin increased; plasma concentration of clarithromycin reduced by. Cytotoxics (continued) possible increased risk of neutropenia when clarithromycin given with. Tadalafil: clarithromycin and erythromycin possibly increase plasma concentration of tadalafil. Theophylline: clarithromycin possibly increases plasma concentration of theophylline; erythromycin increases plasma concentration of. Calcium-channel Blockers: profound hypotension reported with concomitant use of parenteral magnesium and. Antibacterials (continued) Appendix 1: Interactions Melphalan 929 plasma concentration of maraviroc reduced by. Anti-arrhythmics: increased risk of ventricular arrhythmias when mefloquine given with. Antibacterials: increased risk of ventricular arrhythmias when mefloquine given with. Antipsychotics: possible increased risk of ventricular arrhythmias when mefloquine given with. Atomoxetine: increased risk of ventricular arrhythmias when mefloquine given with. Allopurinol: enhanced effects and increased toxicity of mercaptopurine when given with. Antibacterials: increased risk of haematological toxicity when mercaptopurine given with. Sympathomimetics, Beta2: acute hypotension reported when methyldopa given with infusion of. Antibacterials: absorption of methotrexate possibly reduced by neomycin; excretion of methotrexate possibly reduced by ciprofloxacin (increased risk of toxicity); increased risk of haematological toxicity when methotrexate given with. Antidepressants: possible increased serotonergic effects when mirtazapine given with fluoxetine, fluvoxamine or venlafaxine; mirtazapine should not be started until 2 weeks after stopping. Antidepressants: moclobemide should not be started for at least 1 week after stopping. Dopaminergics: caution with moclobemide advised by manufacturer of entacapone; increased risk of sideeffects when moclobemide given with levodopa; avoid concomitant use of moclobemide with. Anxiolytics and Hypnotics: increased sedative effect when baclofen or tizanidine given with anxiolytics and hypnotics Beta-blockers: enhanced hypotensive effect when baclofen given with beta-blockers; possible enhanced hypotensive effect and bradycardia when tizanidine given with beta-blockers; effects of muscle relaxants enhanced by propranolol Calcium-channel Blockers: enhanced hypotensive effect when baclofen or tizanidine given with calcium-channel blockers; effects of non-depolarising muscle relaxants possibly enhanced by calciumchannel blockers; possible increased risk of ventricular arrhythmias when intravenous dantrolene given with diltiazem-manufacturer of diltiazem advises avoid concomitant use; effects of non-depolarising muscle relaxants and suxamethonium enhanced by verapamil; avoidance of intravenous dantrolene advised by manufacturer of verapamil Cardiac Glycosides: possible increased risk of bradycardia when tizanidine given with cardiac glycosides; risk of ventricular arrhythmias when suxamethonium given with cardiac glycosides Clonidine: enhanced hypotensive effect when baclofen or tizanidine given with clonidine Corticosteroids: effects of pancuronium and vecuronium possibly antagonised by corticosteroids Cytotoxics: effects of suxamethonium enhanced by cyclophosphamide and thiotepa Deferasirox: avoidance of tizanidine advised by manufacturer of deferasirox Diazoxide: enhanced hypotensive effect when baclofen or tizanidine given with diazoxide Diuretics: enhanced hypotensive effect when baclofen or tizanidine given with diuretics Dopaminergics: possible agitation, confusion and hallucinations when baclofen given with levodopa Lithium: effects of muscle relaxants enhanced by lithium; baclofen possibly aggravates hyperkinesis caused by lithium Magnesium (parenteral): effects of non-depolarising muscle relaxants and suxamethonium enhanced by parenteral magnesium Memantine: effects of baclofen and dantrolene possibly modified by memantine Methyldopa: enhanced hypotensive effect when baclofen or tizanidine given with methyldopa Metoclopramide: effects of suxamethonium enhanced by metoclopramide Moxonidine: enhanced hypotensive effect when baclofen or tizanidine given with moxonidine Nitrates: enhanced hypotensive effect when baclofen or tizanidine given with nitrates Oestrogens: plasma concentration of tizanidine possibly increased by oestrogens (increased risk of toxicity) Parasympathomimetics: effects of non-depolarising muscle relaxants possibly antagonised by donepezil; effects of suxamethonium possibly enhanced by donepezil; effects of non-depolarising muscle relaxants antagonised by edrophonium, neostigmine, pyridostigmine and rivastigmine; effects of suxamethonium enhanced by edrophonium, galantamine, neostigmine, pyridostigmine and rivastigmine Progestogens: plasma concentration of tizanidine possibly increased by progestogens (increased risk of toxicity) Sympathomimetics, Beta2: effects of suxamethonium enhanced by bambuterol Vasodilator Antihypertensives: enhanced hypotensive effect when baclofen or tizanidine given with hydralazine; enhanced hypotensive effect when baclofen or tizanidine given with minoxidil; enhanced hypotensive effect when baclofen or tizanidine given with sodium nitroprusside Appendix 1: Interactions 934 ants Relaxants Appendix 1: Interactions Nevirapine. Antibacterials: bioavailability of mycophenolate possibly reduced by metronidazole and norfloxacin; plasma concentration of active metabolite of mycophenolate reduced by. Lipid-regulating Drugs: increased risk of myopathy when nicotinic acid given with.
Order reminyl 8mg free shipping
The suitability of food products for patients requiring a vegan medications 3605 reminyl 4mg sale, kosher, halal, or other compliant diet should be confirmed with individual manufacturers. Note Feeds containing more than 6 g/100 mL protein or 2 g/100 mL fibre should be avoided in children unless recommended by an appropriate specialist or dietician. Sugar content varies with flavour 975 Appendix 2: Borderline substances Appendix 2: Borderline substances 976 A2. Sugar content varies with flavour Appendix 2: Borderline substances Appendix 2: Borderline substances 978 A2. Nutritional values vary with flavour-consult product literature Appendix 2: Borderline substances Appendix 2: Borderline substances 982 A2. Nutritional values vary with flavour-consult product literature 983 Appendix 2: Borderline substances Appendix 2: Borderline substances 984 A2. Flavour not suitable for child under 3 years 985 Appendix 2: Borderline substances Appendix 2: Borderline substances 986 A2. Fibre content varies with flavour Appendix 2: Borderline substances Appendix 2: Borderline substances 990 A2. Flavour not suitable for child under 3 years 991 Appendix 2: Borderline substances Appendix 2: Borderline substances 992 A2. Nutritional supplement for patient hydration in the dietary management of dysphagia. Not suitable for children under 1 year except in cases of failure to thrive Carobel, Instant (Cow & Gate) Powder, carob seed flour. Maxamum products are generally intended for use in children over 8 years and adults 2. Not suitable for children under 4 years Isoleucine50 (Vitaflo) Powder, isoleucine 50 mg, carbohydrate 3. Nutritional supplement for the dietary management of phenylketonuria in children over 1 year and adults ProZero (Vitaflo) Liquid, carbohydrate 8. For patients suffering from dry mouth as a result of having (or having undergone) radiotherapy, or sicca syndrome. Counselling needs to be related to the age, experience, background, and understanding of the individual patient. The pharmacist should ensure that the patient understands how to take or use the medicine and how to follow the correct dosage schedule. Any effects of the medicine on driving or work, any foods or medicines to be avoided, and what to do if a dose is missed should also be explained. Other matters, such as the possibility of staining of the clothes or skin by a medicine should also be mentioned. For some preparations there is a special need for counselling, such as an unusual method or time of administration or a potential interaction with a common food or domestic remedy, and this is indicated where necessary. Care should be taken not to obscure other relevant information with adhesive labelling. It is the usual practice for patients to take standard tablets with water or other liquid and for this reason no separate label has been recommended. Patients should be aware that a dispensed medicine should never be taken by, or shared with, anyone other than for whom the prescriber intended it. The label or labels for each preparation are recommended after careful consideration of the information available. However, it is recognised that in some cases this information may be either incomplete or open to a different interpretation. Appendix 3: Cautionary and advisory labels Original packs Most preparations are dispensed in unbroken original packs that include further advice for the patient in the form of patient information leaflets. More general leaflets advising on the administration of preparations such as eye drops, eye ointments, inhalers, and suppositories are also available. Scope of labels In general no label recommendations have been made for injections on the assumption that they will be administered by a healthcare professional or a well-instructed patient. The labelling is not exhaustive and pharmacists are recommended to use their professional discretion in labelling new preparations and those for which no labels are shown. Individual labelling advice is not given on the administration of the large variety of antacids. It is recognised that there may be occasions when pharmacists will use their knowledge and professional discretion and decide to omit one or more of the recommended labels for a particular patient. The exact wording that is required instead should then be specified on the prescription. Pharmacists label medicines with various wordings in addition to those directions specified on the prescription. All of the existing labels were user-tested, and the revised wording selected reflects terminology that is better understood by patients. If separate labels are used it is recommended that the wordings be used without modification. If changes are made to suit computer requirements, care should be taken to retain the sense of the original. Doxycycline, lymecycline, and minocycline are less liable to form chelates and therefore only require label 6 (see above). Also to be used on preparations that contain a drug whose withdrawal is likely to be a particular hazard. Keep taking this medicine until the course is finished, unless you are told to stop To be used on preparations where a course of treatment should be completed to reduce the incidence of relapse or failure of treatment. Do not drink alcohol To be used on preparations for adults that can cause drowsiness, thereby affecting coordination and the ability to drive and operate hazardous machinery; label 1 is more appropriate for children. Some of these preparations only cause drowsiness in the first few days of treatment and some only cause drowsiness in higher doses.
Order online reminyl
Talc is a lubricant but it does not absorb moisture; it can cause respiratory irritation 6 mp treatment cheap reminyl 4 mg with mastercard. These amounts are usually suitable for an adult for twice daily application for 1 week. The recommendations do not apply to corticosteroid preparations-for suitable quantities of corticosteroid preparations, see section 13. If a patch test indicates allergy to an excipient, products containing the substance should be avoided (see also Anaphylaxis, p. The following excipients in topical preparations are associated, rarely, with sensitisation; the presence of these excipients is indicated in the entries for topical products. The appropriate diluent should be used and heating should be avoided during mixing; excessive dilution may affect the stability of some creams. Their effects are short-lived and they should be applied frequently even after improvement occurs. They are useful in dry and eczematous disorders, and to a lesser extent in psoriasis (section 13. The choice of an appropriate emollient will depend on the severity of the condition, patient preference, and the site of application. Emollient preparations contained in tubs should be removed with a clean spoon or spatula to reduce bacterial contamination of the emollient. Emollients should be applied in the direction of hair growth to reduce the risk of folliculitis. The use of aqueous cream as a leave-on emollient may increase the risk of skin reactions, particularly in eczema. The risk is greater when these preparations are applied to large areas of the body, and clothing or dressings become soaked with the ointment. Patients should be told to keep away from fire or flames, and not to smoke when using these preparations. The risk of fire should be considered when using large quantities of any paraffin-based emollient. Urea is a keratin softener and hydrating agent used in the treatment of dry, scaling conditions (including ichthyosis) and may be useful in elderly patients. It is occasionally used with other topical agents such as corticosteroids to enhance penetration of the skin. The quantities of bath additives recommended for adults are suitable for an adult-size bath. Proportionately less should be used for a child-size bath or a washbasin; recommended bath additive quantities for children reflect this. They are used on the skin around stomas, bedsores, and pressure areas in the elderly where the skin is intact. Where the skin has broken down, barrier preparations have a limited role in protecting adjacent skin. The rash may clear when left exposed to the air and a barrier preparation, applied with each nappy change, can be helpful. The barrier preparation should be applied after the corticosteroid preparation to prevent further skin damage. Preparations containing hydrocortisone should be applied for no more than a week; the hydrocortisone should be discontinued as soon as the inflammation subsides. The occlusive effect of nappies and waterproof pants may increase absorption of corticosteroids (for cautions, see section 13. If the rash is associated with candidal infection, a topical antifungal such as clotrimazole cream (section 13. Hydrocortisone may be used in combination with antimicrobial preparations if there is considerable inflammation, erosion, and infection. Pruritus that occurs in otherwise healthy elderly people can also be treated with an emollient. Levomenthol cream can be used to relieve pruritus; it exerts a cooling effect on the skin. Pruritus is common in biliary obstruction, especially in primary biliary cirrhosis and drug-induced cholestasis. Topical antihistamines and local anaesthetics are only marginally effective and occasionally cause sensitisation. For insect stings and insect bites, a short course of a topical corticosteroid is appropriate. Calamine preparations are of little value for the treatment of insect stings or bites. Corticosteroids suppress the inflammatory reaction during use; they are not curative and on discontinuation a rebound exacerbation of the condition may occur. They are generally used to relieve symptoms and suppress signs of the disorder when other measures such as emollients are ineffective. They should not be used indiscriminately in pruritus (where they will only benefit if inflammation is causing the itch) and are not recommended for acne vulgaris. Systemic or very potent topical corticosteroids should be avoided or given only under specialist supervision in psoriasis because, although they may suppress the psoriasis in the short term, relapse or vigorous rebound occurs on withdrawal (sometimes precipitating severe pustular psoriasis). For the role of topical corticosteroids in the treatment of psoriasis, see section 13. In general, the most potent topical corticosteroids should be reserved for recalcitrant dermatoses such as chronic discoid lupus erythematosus, lichen simplex chronicus, hypertrophic lichen planus, and palmoplantar pustulosis. Potent corticosteroids should generally be avoided on the face and skin flexures, but specialists occasionally prescribe them for use on these areas in certain circumstances. When topical treatment has failed, intralesional corticosteroid injections (section 10. These are more effective than the very potent topical corticosteroid preparations and should be reserved for severe cases where there are localised lesions such as keloid scars, hypertrophic lichen planus, or localised alopecia areata. Lotions may be useful when minimal application to a large or hair-bearing area is required or for the treatment of exudative lesions. Occlusive polythene or hydrocolloid dressings increase absorption, but also increase the risk of side-effects; they are therefore used only under supervision on a short-term basis for areas of very thick skin (such as the palms and soles). The inclusion of urea or salicylic acid also increases the penetration of the corticosteroid. Cautions Avoid prolonged use of a topical corticosteroid on the face (and keep away from eyes). Psoriasis the use of potent or very potent corticosteroids in psoriasis can result in rebound relapse, development of generalised pustular psoriasis, and local and systemic toxicity. Contra-indications Topical corticosteroids are contra-indicated in untreated bacterial, fungal, or viral skin lesions, in acne, in rosacea, and in perioral dermatitis; potent corticosteroids are contra-indicated in widespread plaque psoriasis (see notes above). Perioral lesions Hydrocortisone cream 1% can be used for up to 7 days to treat uninfected inflammatory lesions on the lips. Hydrocortisone and miconazole cream or ointment is useful where infection by susceptible organisms and inflammation co-exist, particularly for initial treatment (up to 7 days). Side-effects Mild and moderately potent topical corticosteroids are associated with few side-effects but care is required in the use of potent and very potent corticosteroids. Absorption is greatest where the skin is thin or raw, and from intertriginous areas; it is increased by occlusion. However, concern about the safety of topical corticosteroids in children should not result in the child being undertreated. The aim is to control the condition as well as possible; inadequate treatment will perpetuate the condition. In an acute flare-up of atopic eczema, it may be appropriate to use more potent formulations of topical corticosteroids for a short period to regain control of the condition.
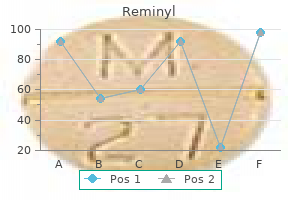
| Comparative prices of Reminyl | ||
| # | Retailer | Average price |
| 1 | O'Reilly Automotive | 938 |
| 2 | Burger King Holdings | 697 |
| 3 | Big Lots | 829 |
| 4 | Trader Joe's | 368 |
| 5 | Neiman Marcus | 980 |
| 6 | Hy-Vee | 404 |
| 7 | Wendy's / Arby's Restaurants | 365 |
| 8 | Ruddick Corp. | 655 |
| 9 | Menard | 282 |
| 10 | Stater Bros. Holdings | 393 |
Buy reminyl 8mg amex
Structure Depending on whether there are two or three nitrogen atoms in the azole ring medicine 3202 purchase line reminyl, azole antifungal agents are subclassified, respectively, as either imidazoles (ketoconazole, clotrimazole, miconazole) or triazoles (itraconazole, fluconazole, voriconazole). Mechanism of Action Nystatin and amphotericin B bind to ergosterol, a major component of fungal cell membranes. This disrupts the stability of the cell by forming pores in the cell membrane that result in leakage of intracellular constituents. Azoles (imidazoles less so) have a greater affinity for fungal than human cytochrome P450 enzymes and, therefore, more effectively reduce the synthesis of fungal cell ergosterol than human cell cholesterol. The allylamine antifungal agents, naftifine and terbinafine, decrease ergosterol synthesis and increase fungal membrane disruption by inhibiting the enzyme squalene epoxidase. It acts only on growing skin cells and has been reported to interfere with nucleic acid synthesis and disrupt microtubule function, among other activities. Echinocandins are the first antifungals to specifically target the fungal cell wall. They inhibit the -1,3-glucan synthase, an enzyme required for the synthesis of an important cell-wall component, glucan, rendering cell walls more susceptible to lysis. Administration Amphotericin B is insoluble in water and, therefore, is generally administered as a colloidal suspension with sodium deoxycholate. It is too toxic for systemic use and, therefore, is mostly used topically to treat fungal infections of the skin and mucous membranes (eg, oropharyngeal thrush, vaginal candidiasis). The absorption of the azole antifungal agent, itraconazole, is reduced by antacids that block acid secretion. Through their actions on hepatic microsomal enzymes, itraconazole and voriconazole significantly decrease the metabolism of numerous other drugs (eg, the rifamycins, phenytoin, carbamazepine, digoxin, cyclosporine). In the presence of a number of these other drugs, the metabolism of itraconazole and voriconazole may be increased. In the circulation, they are highly bound to proteins and do not cross the blood-brain barrier. Caspofungin can affect hepatic cytochrome P450 enzymes and has significant potential drug-drug interactions. Micafungin is metabolized by arylsulfatase, catechol-O-methyltransferase, and hydroxylation, and has few drugdrug interactions. Bone marrow suppression is a common adverse effect of which of the following drugs Amphotericin B, like nystatin, binds to ergosterol to create pores in fungal membranes. Fluconazole binds fungal cell cytochrome P450 enzymes to reduce the synthesis of ergosterol. Terbinafine decreases ergosterol synthesis by inhibiting the enzyme squalene epoxidase. A common adverse effect of griseofulvin is hypersensitivity (fever, skin rash, serum sickness-like syndrome). Echinocandins are the first class of drug to affect synthesis of the fungal cell wall. Polyene macrolides bind to ergosterol, a major component of fungal cell membranes. The allylamine antifungal agents decrease ergosterol synthesis and increase fungal membrane disruption by inhibiting the enzyme squalene epoxidase. Echinocandins are the first-line drug of choice for a variety of systemic fungal infections. Antifungal drug resistance: mechanisms, epidemiology and consequences for treatment. For several years he has had scaly, rough growths on his face, forehead, and scalp. He has had individual lesions removed by previous physicians, but keeps getting more and more. He has a long history of sun exposure and multiple sunburns, primarily as a consequence of working outdoors and playing golf. On examination of his skin, you note multiple 4- to 7-mm lesions on the face and scalp that are flat, pink, and scaly. Untreated, actinic keratoses may progress to become squamous cell carcinomas of the skin. Other pharmacologic treatments for actinic keratosis include topical imiquod cream and ingenol mebutate gel. Outline the principles of cancer chemotherapy and the development of resistance to chemotherapeutic agents. List the antimetabolite and alkylating chemotherapeutic agents and describe their mechanisms of action, therapeutic uses, and adverse effects. To be most effective, the drugs used in combination chemotherapy should each have therapeutic activity with different dose-limiting toxicities and should be administered during several cycles of treatment to allow recovery from acute adverse effects. The drugs used to treat cancer are classified as alkylating agents, antimetabolites, cytotoxic antibiotics, plant alkaloids, hormonal agents, and miscellaneous agents. Depending on the tumor type, they are often used in combinations or as adjunct therapy to surgical and radiation procedures. Primary resistance to anticancer drugs is thought to occur because of some inherent genetic characteristics of tumor cells. Acquired resistance of tumor cells to a specific anticancer drug may occur via several different mechanisms that usually involve either amplification or overexpression of one or more genes. Alternatively, after exposure of a tumor cell to a number of structurally different agents, a so-called multidrug, or pleiotropic, resistance may develop to chemotherapeutic agents because of decreased uptake or retention of the drugs. Multidrug resistance is the major form of resistance to vinca alkaloids, etoposide, paclitaxel, anthracyclines, and dactinomycin. Other Classes of Selected Anticancer Drugs Cytotoxic antibiotics: Dactinomycin (actinomycin D), bleomycin, doxorubicin. Plant alkaloids: Vinblastine, vincristine, vinorelbine, etoposide, paclitaxel, topotecan. Miscellaneous agents: Cisplatin, imatinib, hydroxyurea, mitotane, arsenic trioxide, procarbazine. The product, in this case 6-thioinosinic acid, inhibits purine nucleotide interconversion. Pharmacokinetics Cyclophosphamide is not itself cytotoxic but must first be converted by hepatic microsomal enzymes to form the cytotoxic agents, phosphoramide mustard and acrolein. Combination chemotherapy early in therapy increases the likelihood of destroying drug-resistant populations of cells that are refractory to treatment and therefore is generally more effective than monotherapy. To be most effective, the drugs used in combination chemotherapy should each have therapeutic activity with different dose-limiting toxicities and should be administered during several cycles of treatment to allow recovery from acute adverse effect. Development of a mild leukopenia is evidence of the adequate absorption of orally administered alkylating agents. She currently takes only promethazine as needed for nausea and a combination of hydrocodone and acetaminophen as needed for pain. She is diagnosed with recurrent metastatic ovarian cancer and placed on a chemotherapeutic regimen that includes paclitaxel. Its mechanism of action is to promote the formation of and inhibit the disassembly of stable microtubules in the M phase of cell division. Paclitaxel is used for the treatment of metastatic ovarian, breast, and small cell lung cancers. List the plant alkaloids used as cancer chemotherapeutic agents and describe their mechanisms of action, therapeutic uses, and adverse effects. Paclitaxel is a complex diterpene derived from the Western and European yew (Taxus brevifolia and Taxus baccata). Etoposide is a semisynthetic podophyllotoxin, an extract from the Mandrake root (Mandragora officinarum) or May apple root (Podophyllum peltatum). Mechanism of Action Vinca alkaloids (vinblastine, vincristine, vinorelbine): Bind tubulin to terminate microtubule assembly and cause cell arrest in metaphase (M) by blocking mitosis and chromosomal aggregation and causing mitotic spindle dissolution. Taxanes (paclitaxel): Bind to microtubules resulting in their stabilization and in an enhancement of aberrant tubulin polymerization that result in cytotoxicity, including mitotic arrest. Administration Hypersensitivity to paclitaxel can be reduced by premedication with dexamethasone and histamine H1- and H2-receptor blockers. Pharmacokinetics Abraxane is a formulation of paclitaxel bound to albumin, approved for treatment of breast cancer, that does not cause hypersensitivity reactions, and is less likely to result in severe neurotoxicity or myelosuppression.
Purchase reminyl 8 mg line
Interstitial infiltrate is composed primarily of eosinophils associated with myocyte damage (seen in center left) medicine keychain buy genuine reminyl line. Giant cells are often present and zone of inflammation may be extensive and confluent. A band-like infiltrate of primarily eosinophils with occasional lymphocytes is seen to traverse between (but not damage) the myocyte fibers. Lipofuscin pigment is prominent and there may be a mild chronic lymphocytic inflammation. There is myocyte hypertrophy, interstitial fibrosis, and thickened intramyocardial arterioles. It should be noted that small areas of disarray may occur in normal hearts, especially at the junction of the interventricular septum and right ventricle. Note presence of lipofuscin granules adjacent to several nuclei, which is unusual for this age. At 8 weeks of age, this is one of the youngest patients showing myocyte hypertrophy and focal disarray. Arrhythmogenic right ventricular dysplasia/cardiomyopathy is characterized by arrhythmia and right heart dilatation with focal replacement of myocardium by fat and fibrous tissue. There is loss of myocytes with intermingling of fat, fibrous tissue, and myocytes. Normal fat infiltration of the right ventricle is seen in obese patients and may be difficult to distinguish on biopsy. More often, it is seen in association with congenital cardiac malformations and other cardiomyopathies. Cardiac hemochromatosis may be due to autosomal recessive hemochromatosis, hemosiderosis due to chronic transfusion for anemia (thalassemia or sickle cell anemia), or rarely due to chronic ingestion of iron salts. Increased iron may also accumulate in patients with Wilson disease (copper toxicity). Ultrastructurally, there is evidence of myofibrillar loss with disorganized Z-band material and preservation of transverse tubules. Drug cardiotoxicity can occur with many cytotoxic drugs20 of which Adriamycin is the most common. Glycogen storage diseases are caused by a deficiency in one or more of the enzymes involved in the synthesis or degradation of glycogen, leading to the accumulation of glycogen in various tissues. Mucopolysaccharidoses are a family of hereditary diseases characterized by the accumulation of mucopolysaccharides due to deficiency in a lysosomal enzyme normally responsible for their degradation. These conditions lead to changes in cardiac valves, skin, cartilage, and bone, presumably due to the effect of acid mucopolysaccharides on collagen. Mucopolysaccharidosis I is characterized by reduced activity of -L-iduronidase; excessive urinary secretion of dermatan sulphate and heparan sulphate; and the presence of large, oval, or rounded connective tissue cells (Hurler cells) within the valves, endocardium, myocardium, coronary arteries, and aorta. These cells are filled with numerous clear vacuoles containing acid mucopolysaccharide material. Molecular genetic investigation can reveal the genetic defect, which is located on the short arm of chromosome 4 (4p16. Cardiovascular disease is part of the spectrum for the majority of patients with either the mild or the severe form of disease. Clear cells are also present in the myocardium and endocardium but not in coronary arteries. Molecular genetic investigation can reveal the genetic defect on the X chromosome (Xq27. Microscopically, intracellular deposits are localized in small granular cells, but large Hurler-like cells are not always described. Myocytes are enlarged and contain lipid vacuoles that can be confirmed with special stains for lipids. Sphingolipidosis: Fabry (Anderson-Fabry) disease is an X-linked inborn error of glycosphingolipid metabolism (3p21-23). The incidence is variable, depending on a variety of factors, but is estimated to be between 10% and 20%. Clinically, there is evidence of hemodynamic compromise (hypotension, shock, decreased cardiac output). Acute cellular rejection is characterized by an inflammatory infiltrate of lymphocytes, macrophages, and occasional eosinophils and can occur from days to years after transplantation. Clinically, it is usually asymptomatic and is estimated to occur at least once in up to 80% of cardiac allograft recipients. Smaller intramyocardial branches reveal diffuse concentric narrowing with luminal stenosis. Quilty lesion/effect was named after the first transplant patient it was observed in. It is an aggregate of lymphocytes found primarily in the endocardium of the ventricles which may extend into underlying myocardium. Diffuse mild rejection (G1B/G1R) Focal moderate rejection (G2/G1R) Multifocal moderate rejection (G3A/G2R) Severe rejection (G3B and G4/G3R) Few activated lymphocytes between myocytes No eosinophils or muscle damage Single focus of activated lymphocytes, which may include eosinophils, macrophages, and few plasma cells with focal myocyte damage Two or more foci of infiltrate with associated myocyte damage Rarely seen with current therapy Manifested by diffuse infiltrates (lymphocytes, eosinophils, and neutrophils) with myocyte necrosis and damage R denotes revised 2005 criteria. Quilty A lesions are composed of an endocardial infiltrate of mature small lymphocytes, often associated with small capillaries, with no involvement of the myocardium. Large endocardial infiltrate of mature lymphocytes extending in to the underlying myocardium. The infiltrate of cellular rejection (described previously) contains larger lymphocytes with scattered, occasional eosinophils and is associated with myocyte damage. Site of previous biopsy changes are very common in the early posttransplant period because the bioptome tends to go back to the same site, and biopsies are being performed frequently. Inflammation is present but usually insignificant and should not be confused with rejection. Clinically, patients may present with fever, with shortness of breath, with chest pain and/or tachycardia, and have elevated cardiac enzymes. Fungal infection is characterized by multifocal areas of myocyte necrosis and acute inflammation often with granuloma formation. Viral and parasitic infections may present with a nonspecific lymphocytic myocarditis. In the case of toxoplasmosis, cysts may be present in a normal-appearing myocardium. However, note the presence of fibrin, macrophages, and fibroblasts which differentiate it from rejection. Benign tumors include cardiac myxoma, rhabdomyoma, fibroma, hemangioma, lipoma, and lipomatous hypertrophy of interatrial septum. Malignant tumors, mainly sarcomas, are exceedingly rare in children (and adults) with an estimated incidence between 0. Sometimes, they appear as fine basophilic granules within myocytes and may resemble Toxoplasma organisms. Separation of myofibers is often seen secondary to rapid histologic processing and should not be interpreted as edema. With this finding, a careful search for epicardium is warranted to rule out perforation. This should be differentiated from just contraction bands, which would not have coagulative necrosis. Incidence of three presentations of acute myocarditis in young men in military service. The evolving approach to paediatric myocarditis: a review of the current literature. Detection of viral and bacterial protein in endomyocardial biopsies of patients with inflammatory heart muscle disease Arrhythmogenic right ventricular cardiomyopathy: an update on pathophysiology, genetics, diagnosis, and risk stratification. Primary endocardial fibroelastosis: an underappreciated cause of cardiomyopathy in children. Cardiomyopathy of Duchenne muscular dystrophy: current understanding and future directions. Mucopolysaccharidosis type I: current knowledge on its pathophysiological mechanisms. Evidence for an iduronate-sulfatase pseudogene near the functional Hunter syndrome gene in Xq27.
Reminyl 4mg line
Current of injury predicts adequate active fixation in permanent pacemaker/defibrillation leads medicine 3604 pill order 4 mg reminyl amex. Video-assisted thoracoscopic implantation of the left ventricular pacing lead for cardiac resynchronization therapy. Acute complications of permanent pacemaker implantation: their financial implications and relation to volume and operator experience. Decrease in fluoroscopic cardiac silhouette excursion precedes hemodynamic compromise in intraprocedureal tamponade. Severe symptomatic tricuspid valve regurgitation due to permanent pacemaker or implantable cardioverter-defibrillator leads. Venous thrombosis and stenosis after implantation of pacemakers and defibrillators. Therapy of cardiac device pocket infections with vacuum-assisted wound closure-Long-term follow-up. Cardiac implantable electronic device infections: presentation, management, and patient outcomes. Implantationrelated complications of implantable cardioverter- 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 defibrillators and cardiac resynchronization therapy devices: a systematic review of randomized clinical trials. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management. Diagnosis and management of infections involving implantable electrophysiologic cardiac devices. Lead extraction is preferred for lead revisions and system upgrades: When less is more. Risks of spontaneous injury and extraction of an active fixation pacemaker lead: report of the Accufix multicenter clinical study and worldwide registry. Clinical study of the laser sheath for lead extraction: the total experience in the United States. Intravascular pacemaker and defibrillator lead extraction: a state-of-the-art review. Initial experience with the Evolution mechanical dilator sheath for lead extraction: Safety and efficacy. Extraction of old pacemaker or cardioverter-defibrillator leads by laser sheath versus femoral approach. Pacemakers have become highly complex due to the addition of multiple specialized features in an attempt to treat different cardiac conditions, such as sick sinus syndrome with or without chronotropic incompetence, cardioinhibitory vasovagal syndrome, and paroxysmal atrial arrhythmias, and avoid some adverse effects of chronic pacing, such as heart failure, induction of atrial and supraventricular arrhythmias, etc. Thus, a deep understanding of the different pacing modes, pacemaker timing cycles, and special features is paramount to identify normal versus abnormal pacemaker function. Timing cycles are based on cardiac events such as atrial- and ventricular-sensed and -paced events. Thus, appropriate pacemaker function depends on the ability of these devices to properly recognize atrial- and ventricular-sensed events. Timing cycles include different blanking periods, refractory periods, and intervals. The number and complexity of these timing cycles depend and vary based on the number of leads, pacing mode, and/ or rate sensor. Accurate examination of timing cycles and pacemaker behavior requires device interrogation and analysis of "event markers" as they provide the actual pacemaker interpretation and response to different cardiac signals. For the rest of the chapter, the following abbreviations will be used to describe common pacemaker marker events: "P" native atrial depolarization, "A" an atrial-paced event, "R" a native ventricular depolarization, and "V" a ventricular-paced event. Pacing nomenclature A three-letter code describing the basic function of the various pacing systems was first proposed in 1974 by a combined task force from the American Heart Association and the American College of Cardiology. As pacemakers have become more complex with multiple features, the basic function of pacemakers is now denoted as a generic fiveletter code (Table 6. Some manufacturers also use "S" in both the first and the second positions to indicate that the device is capable of pacing only a single cardiac chamber. The third position refers to the mode of sensing, or how the pacemaker responds to a sensed event. An "I" indicates that a sensed event inhibits the pacing stimulus and causes the pacemaker to reset or re-initiate one or more timing cycles. Similar to the first two positions, a "D", means that there are dual modes of response. An event sensed in the atrium inhibits atrial output but triggers ventricular output, also referred to as P-synchronous pacing. Finally, if a native ventricular signal or R wave is sensed, it inhibits ventricular output and possibly even atrial output, depending on where sensing occurs. An "R" indicates that the pacemaker incorporates a sensor to control the rate independently of intrinsic electrical activity of the heart, so-called rate-modulated pacing. The fifth position indicates whether multisite pacing is not present (O) or present in the atrium (A), ventricle (V), or both (D). Multisite pacing is defined for this purpose as stimulation sites in both atria, both ventricles, more than one stimulation site in any single chamber, or any combination of these. This fifth position has become relevant with the introduction of biventricular devices. Pacing modes Pacing modes have evolved with technology and each pacing mode has specific and general indications, as well as unique advantages and disadvantages (Table 6. The timing cycles of each of these pacing modes are discussed in the following section. This pacing mode may be transiently used in pacemaker-dependent patients to avoid inappropriate pacing inhibition during interventions or surgeries associated with noise (Table 6. Historically, this pacing mode was used to prevent inappropriate inhibition from oversensing in a patient without a stable native escape rhythm. However, arrhythmias could be initiated if non-cardiac signals are inappropriately sensed. This pacing mode is commonly programmed as a mode switch to avoid tracking of these atrial tachyarrhythmias. This pacing mode allows atrial sensing but does not provide P-synchronous pacing (non-tracking mode). It is an alternative pacing mode in patients with atrial fibrillation and flutter, and it is available as a mode switch feature in some pacemakers. Pacing is only inhibited (I) and reset by ventricular-sensed events, but ignores all intrinsic atrial complexes. The most common use of this pacing mode is in devices with a single-pass lead which integrates an atrial-sensing electrode with a ventricular-pace/sense electrode. Timing cycles A given timing period or interval can continue until it completes its cycle; completion results in either the release of a pacing stimulus or the initiation of another timing cycle. Alternatively, a given period or interval can be reset by an intrinsic cardiac event, at which point it restarts the timing period again or initiates another timing period. Each portion of the pacemaker timing cycle should be considered in milliseconds (a thousandth of a second) and not in beats per minute (bpm). Blanking and refractory periods All pacing modes that can sense cardiac events must include blanking and refractory periods in their basic timing cycle. The presence or absence of these periods depends on the pacemaker system as well as the pacing/sensing mode. These periods are essential to the appropriate pacemaker function as they prevent sensing of known but clinically inappropriate signals, such as the evoked potential and repolarization. The blanking and refractory periods of a pacemaker are analogous to the absolute and relative refractory periods of the heart, respectively, during which a stimulus delivered to the heart is ineffective because the myocardium is already depolarized and a subsequent depolarization cannot occur until the resting membrane potential is re-established. Once this period ends, the sense amplifier becomes alert and is receptive to the detection of native signals. Timing cycles based on pacing mode Cardiac events and timing cycles are based on a single, dual, or biventricular pacemaker systems and programmed pacing modes (Table 6. These intervals are never reset, because the pacing mode is insensitive to any atrial or ventricular activity. After the blanking period, the ventricular-sensing channel is again operational, or "alert. Overall, pacemaker behavior depends on the programmed pacing mode and base rate behavior. Thus, atrial pacing artifact inappropriately sensed by the ventricular-sensing amplifier could result in ventricular pacing inhibition, referred to as cross-talk. In a pacemaker-dependent patient, inhibition of ventricular output by cross-talk results in ventricular asystole. Sensing during this window will result in a triggered rather than an inhibited output.
Buy reminyl with paypal
In the absence of carbidopa 5 medications that affect heart rate discount reminyl uk, pharmacologic doses of pyridoxine (vitamin B6) will increase the peripheral metabolism of L-dopa and thereby reduce its therapeutic effect. Signed patient consent is required for use of tolcapone, as is continuous evaluation of liver function. His last seizure was 3 months ago, and usually is controlled if he takes his medication regularly. His initial labs including a blood count, comprehensive metabolic panel, and urine drug screen are negative. Rare but potentially fatal adverse effects include agranulocytosis (bone marrow failure) and Stevens-Johnson syndrome (fatal sever rash with skin shedding and mucosal involvement) and hepatotoxicity. It works by binding to and prolonging the inactive state of the Na+ channel, thus blocking use-dependent Na+ conductance and the generation of action potentials. Phenytoin is metabolized in the liver by microsomal enzymes through parahydroxylation and glucuronide conjugation. Rates of oral absorption and metabolism can vary significantly from one patient to the next. At very low doses elimination is first-order; however, even within the therapeutic range, the liver enzymes responsible for its metabolism are near saturation, resulting in an increase in its half-life. Common side effects include nystagmus, ataxia, confusion, hirsutism, and gingival hyperplasia in children (up to 50%). Its use should be avoided, if possible, during pregnancy, because it is teratogenic. Phenytoin induces hepatic metabolism by microsomal enzyme induction and can lower plasma levels of other drugs. Caution and close monitoring of blood levels of phenytoin must be undertaken when phenytoin is used in combination with other drugs. List and discuss the common adverse effects and toxicities of major antiseizure agents. First-pass effect: the extensive metabolism by the liver of many drugs administered orally that may limit bioavailability to such an extent that an effective therapeutic dose cannot be achieved. In addition to phenytoin, carbamazepine is another major first-line antiseizure drug used to treat both partial seizures and generalized tonic-clonic seizures. Serum levels of carbamazepine must be monitored closely, especially early in therapy because this drug induces hepatic enzymes responsible for its metabolism and thus blood levels will fall over time. Idiosyncratic reactions include serious skin rash (StevensJohnson syndrome) and rarely a fatal aplastic anemia. Carbamazepine is also used therapeutically to treat bipolar disorder and trigeminal neuralgia. Oxcarbazepine was developed from carbamazepine to overcome the problems with induction of hepatic metabolic enzymes. Its side effects are similar to carbamazepine, except it is more likely to produce significant hyponatremia. Blood levels must also be monitored because it is influenced by the presence of hepatic P450 enzymes. Ethosuxemide is only used in the treatment of absence seizures and is not effective in other types of seizures. Lorazepam and diazepam are frequently used to treat acute seizures in the hospital setting. Phenobarbital is an older drug used for treating partial and generalized tonicclonic seizures. Although it can be used in the hospital setting, its use is limited by its potential for addiction and drug-drug interactions. However, because of the potential for an idiosyncratic hepatotoxicity, it is reserved for patients with concomitant generalized tonic-clonic seizures. It is also used to control myoclonic seizures and for the treatment of bipolar disorder and for prophylaxis of migraine headache. Gabapentin and levetiracetam are used as an add-on therapy, with the advantage that both are well tolerated and have no known drug-drug interactions. Mechanism of Action Phenytoin, carbamazepine, oxcarbazepine, and lamotrigine share a common mechanism of action, the inhibition of neurotransmission through the prolongation of the inactive state of voltage-dependent Na+ channels. Ethosuximide reduces low threshold T-type Ca2+ current in the thalamus that appears to provide pacemaker activity responsible for cortical generation of absence seizures. Because phenytoin may precipitate at its site of injection, it has been replaced for intravenous injection by the more watersoluble fosphenytoin, which is only available for parenteral administration. Carbamazepine, ethosuximide, gabapentin, levetiracetam, and topiramate are only available for oral administration. Valproic acid is hydroscopic and therefore is available for oral administration as a capsule in corn oil or, for pediatric use, in syrup. It is also available as a more patient preferred enteric-coated tablet formulated as divalproex sodium, which is a 1:1 compound of valproic acid and sodium valproic acid. With continuous administration, carbamazepine induces the synthesis of liver microsomal enzymes responsible for its own metabolism resulting in a substantially decreased half-life requiring significant dose adjustment. Through the same induction mechanism, carbamazepine can also alter the metabolism of a number of other drugs. Likewise, there are a number of drugs that can alter the metabolism of carbamazepine by induction of the appropriate microsomal enzymes. Oxcarbamazepine is a closely related anticonvulsant that is less likely to induce microsomal enzyme synthesis. Valproic acid inhibits its own metabolism and the metabolism of other drugs, including phenytoin. The anticonvulsant activity of ethosuximide when used to treat absence seizures is due to its blockade of T-type calcium currents in the thalamus. Carbamazepine and phenytoin, which are not used to treat absence seizures, block sodium channels. Carbamazepine induces the synthesis of liver microsomal enzymes responsible for its own metabolism, necessitating a significant dose adjustment with its continued administration. A small change in the bioavailability of phenytoin may result in a disproportionate increase in its blood level because its metabolic enzymes become saturated even at therapeutic doses. Antiseizure drugs increase the risk of congenital malformations, including the "fetal hydantoin syndrome" (phenytoin) and spina bifida (valproic acid). Hepatic metabolic enzyme levels are frequently altered by these drugs, resulting in a low therapeutic index, and therefore blood levels of antiseizure medications must be closely monitored. Efficacy and tolerability of the new antiseizure drugs I: treatment of new onset epilepsy. On examination, his heart rate is 60 beats per minute, and respiratory rate is 8 per minute and shallow. In addition to its therapeutic actions, what other effects might this medication produce Certain individuals seek the euphoria obtained from the intravenous injection of opioids such as heroin. There are three different cell receptors specific for opioids: mu, kappa, and delta (,), all of which exist as multiple subtypes. This patient has the classic signs of opioid overdose: somnolence, respiratory depression, and miosis. Stimulation of the mu receptor results in analgesia (supraspinal and spinal), respiratory depression, euphoria, and physical dependence. Continuous, heavy use of opioids can result in tolerance, where more drug is required to obtain the same euphoric "high," and also to physical dependence. Its intravenous administration leads to an almost immediate reversal of all effects of the opioids. In individuals who are physically dependent, administration of naloxone will immediately precipitate opioid withdrawal, which consists of a constellation of signs and symptoms that include nausea and vomiting, muscle aches, lacrimation or rhinorrhea, diarrhea, fever, and dilated pupils. In general, physical dependence induced by opioids with a short half-life tends to result in a rapid severe withdrawal, while physical dependence induced by opioids with a long half-life tends to be associated with a less severe and more gradual course of withdrawal. The opioid methadone may be administered in a daily dose to individuals physically dependent on opioids, most notably heroin, as a "maintenance therapy" or to ameliorate the symptoms of opioid withdrawal. List the major opioid agonists and antagonists, their therapeutic uses, and their important pharmacokinetic properties. Drug tolerance: Decreased response to a drug with its continued administration that can be overcome by increasing the dose. Also, in addition to a cellular tolerance, a metabolic tolerance can develop to the effects of some drugs because they increase the synthesis of enzymes responsible for their own metabolism (alcohol, barbiturates).
Purchase 8 mg reminyl mastercard
Concunent twodimensional radiotherapy and weekly docetaxel in the treatment of stage Ill non-small cell lung cancer: a good local response but no good survival due to radiation pneumonitis treatment zoster ophthalmicus discount reminyl 8mg with mastercard. Peribronchiolar metaplasia: a common histologic lesion in diffuse lung disease and a rare cause of iDterstittd lung disease: clinicopathologic features of 15 cases. Airway-centered interstitial fibrosis: a distlDct form of aggressive diffuse lung disease. Pleuroparenchymal fibroelastosis: a spectrum of histopathological and imaging phenotypes. Pleuropa-renchymal llbroelastosls in patients with pulmonary disease secondary to bone marrow transplantation. Dendriform ossification showing the typical pattern of irregular, somewhat branched, masses of osteoid filling airspaces. Idiopathic pleuroparenchymal fibroelastosis: description of a novel clinicopathologic entity. Pulmonary hypertension and amyloidosis-an uncommon association: a case report and review of the literature. Localized interstitial pulmonary amyloid: a case report and review of the literature. Pulmonary light chain deposition disease: report of five cases and review of the literature. Imaging of pulmonary-cutaneous disorders: matching the radiologic and dermatologic findings. Pleuropulmonary pathology of vascular Ehlers-Danlos syndrome: spontaneous laceration, haematoma and fibrous nodules. Significant pulmonary hemorrhage is seen in various clinical settings, of which the most common are mechanical causes such as tumors or cavities that typically produce localized hemorrhage. Patients with diffuse hemorrhage commonly pres-ent with hemoptysis, but hemoptysis is absent in up to one-third of cases. Patients with pulmonaryveno-occlusive disease always have pulmonary hypertension but usually not hemoptysis. Patients with chronic hemorrhage secondary to cardiac disease may or may not have pulmonary hypertension and sometimes have small hemoptyses, but the cardiac disease usually overshadows the pulmonary disease. The patiem was a 45-yearold woman with Wegener granulomatosis and recurrent pulmonary hemorrhage. Pathologic Patterns of Hemonhage and lid-Like Reactions to Hemorrhage Acute alveolar hemorrhage. Thus, in the absence of hemoptysis or clinical evidence of hemorrhage, caution should be exercised in labeling pure acute hemorrhage as a pathologic reaction. The presence of hemosiderin-laden macrophages indicates that the hemorrhage is real but provides no indication of chronicity, as hemosiderin-laden macrophages form in a few days and can persist for months or years. Low- and high-power views of chronic alveolar hemorrhage in a patiem with miaoscopic polyangiitis leading to interstitial fibrosis. Note tfle interstitial hemosiderin (black atrows), an indication that the fibrosis is secondary to hemorrhage. In contrast, in veno-occlusive disease and fibrosis secondary to cardiac disease, the fibrosis is usually localized to the subpleural region. Similar venous changes, minus thromboses, can be found in the veins in patients with heart failure or mitral valvular diseases. Pulmonary function tests show a restrictive impairment with decreased dillusing capacity. If tumor gains access to the small pulmonary anery branches, cor pulmonale may develop. Statistically lung, breast, stomach, pancreas, ovary, and prostate are the most frequent sites of origin. Associated findings may include discrete nodules representing metastases, pleural effusion, and hilar, or mediastinal lymph node enlargement. Tumor spreads in a lymphangitic fashion and outlines the imerlobular septa (atrow$) and bronchovasa. Kaposi sarcoma: Tumor spreads in a lymphangitic fashion around around a bronchovascular bundle. High-power view of Kaposi sarcoma showing spindle cells and extravasated red cells. In this example dte lymphangitic rumor appears at low-power view as hemorrhage in the walls of the airway and vessel. High-grade lymphomas are cytologically obvious and frequently infiltrate vessels, but low-grade lymphomas with a lymphangiti. The patiem was a 64-year-old woman with pulmonary T-cell lymphoma following heart transplam. Lymphoma spreading in a lymphangitic fashion along the bronchovascular bundles and interlobular septa. Gough (1-mm-thick: whole lung) section showing lymphoma along the interlobular septa (arrows) and bronchovascular bundles; i. However, residual germinal centers around bronchovascular bundles can produce a spurious appearance of a polymorphous population, and Hodgkin disease with a lymphangitic pattern can also appear polymorphous. In lymphomas the interstitial infiltrates may coalesce to give rise to true tumor masses. Leukemias can also spread in the interstitium to produce a pattern of lymphangitic or diffuse interstitial infiltration. With time tumor tends to escape from lymphatics and can be found in the airspaces and/or in the vessels. Collapse cannot be avoided in ttansbronchial biopsies but inflation of surgical lung biopsies, wedge resections, and resected lobes/lungs is the best way to avoid collapse artifacts (see Chapter 3). Pulmonary interstitial fibrosis as a presenting manifestation in perinuclear antineutrophilic cytoplasmic antibody microscopic polyangiitis. Pulmonary involvement in Kaposi sarcoma: correlation between imaging and pathology. Another example of a case in which one lobule has been inflated and the other not. The parenchyma in the inflated lobule is nonnal whereas that in the collapsed lobule appears to have interstitial inflammation. The interlobular seprum (*) is artifactually widened as a result of inflating the biopsy. Gradual transitions from obviously normal to increasingly "fibrotic" should be examined with care, because this is a common pattern of collapse, and often one can trace individual alveolar walls into the "fibrotic" area. Skin changes the blood circulation to the skin is stopped resulting in pallor and loss of elasticity. Eye changes An early change in eye seen as opacity of cornea and flaccidity of eyeball due to loss of intraocular tension, which progressively comes down to zero in about 2 hours. Algor mortis (Postmortem cooling) Is a progressive loss of heat due to; conduction, convection and radiation after death resulting in cooling of body. Livor mortis (Postmortem lividity) A passive pooling imparts reddish-purple or bluish discoloration of skin in dependent parts of the dead body is called as livor mortis with "contact flattening" on pressure areas of the body. Cadaveric Spasm/Instantaneous Rigor In cases of sudden death from excitement, fear, severe pain, exhaustion etc. This condition is known as Cadaveric Spasm or Instantaneous Rigor or Cataleptic Rigidity of the body. Mummification Skeletonization is the removal of tissues from the bones or skeleton, it may be complete; where all soft tissues are removed and partial, where only a few portions of the bones are exposed. Postmortem artefacts are due to any changes caused or features introduced in a body after death. It is duty of medicolegal expert to differentiate artefacts from that of injuries thereby preventing false interpretation of finding and misleading of investigation. Medicolegally wound can be defined as any lesion external or internal caused by violence with or without loss of continuity of skin. Mechanical injuries can be defined as "Damage to any part of the body due to application of mechanical force". Contusions/bruises: Extravascular collection of blood due to damage of blood vessels without loss of continuity of skin. Incised wound/cut/slash/slice: Clean cut separation of skin and/or deeper tissues caused by sharp cutting weapon without contusion and crushing of margins.
