
1mg anastrozole mastercard
They mainly engage in oxidative reactions that use molecular oxygen; they contain oxidative enzymes such as catalase and uric oxidase breast cancer x ray images discount anastrozole online. Functions include cell respiration, fatty acid metabolism, alcohol degradation, transamination, regulation of H2O2, and bile acid metabolism. Peroxisomes also synthesize specialized phospholipids, such as plasmalogen, which is needed for myelination of nerve cells. Like lysosomes, they have one plasma membrane, but it is thinner and more permeable than that of lysosomes. The most common and severe, Zellweger, or cerebrohepatorenal, syndrome, leads to abnormalities in brain, kidneys, and liver. Affected infants die soon after birth, which is most likely due to faulty neural cell myelination in utero. The primary defect is an inability to import newly formed proteins across peroxisomal membranes. Plasmalogens, which are produced in peroxisomes, are the most abundant phospholipid in myelin sheaths of nervous tissue. Thus, peroxisomal disorders usually lead to serious neurologic defects, including abnormal myelin caused by deficient plasmalogen. Aggregates of glycogen particles form irregular patches called alpha particles (or rosettes). Usually metabolic byproducts or stored nutrients, they include glycogen, lipid droplets, and pigment granules. Glycogen is a D-glucose polymer, which is mostly stored in cytoplasm of hepatocytes and in skeletal muscle cells. They often form larger, rosette-like aggregates termed alpha particles, with diameters of 90-95 nm. It leads to an abnormal accumulation of glycogen in muscle and liver cells, which causes clinically important end-organ disease and morbidity. Here, several fat cells (adipocytes) contain lipid (*), which pushes nuclei to the periphery. Fats are insoluble in water, so they form spherical lipid droplets that vary widely in size. Adipocytes (fat cells) are the main storage sites for lipid in the body, with functions of thermal insulation, physical padding, and shock absorption. In these cells, droplets often coalesce to form one large droplet (up to 90 mm in diameter) that fills the cytoplasm and pushes other organelles to the cell periphery. Lipid is released from cells into the bloodstream for other cells to use as needed. Lipid droplets normally lack a plasma membrane and consist of triglycerides and esters of cholesterol. Hepatocytes, the main sites of cholesterol synthesis, contain variable numbers of lipid droplets. Cholesterol is a precursor to steroid hormones, so steroid-secreting cells (such as those in adrenal cortex, testis, and ovary) also contain many small lipid droplets. Adrenal cortex cells typically look spongy because of lipid content and are thus called spongiocytes. Organic solvents used for histologic specimen preparation commonly extract lipid unless special methods are used, so in routine sections, lipid-containing areas are usually clear, vacuolated spaces. In atherosclerotic plaque formation, arterial smooth muscle cells and macrophages accumulate lipid droplets, giving these so-called foam cells their frothy appearance. In some infectious diseases, lipid droplets engage in pathogenesis of viruses and bacteria. Chlamydia-caused by the bacterium Chlamydia trachomatis-is a common sexually transmitted disease. During the initial stages of infection, the intracellular pathogen interacts with lipid droplets, which supply components needed for bacterial replication in host cells. Details of caveolae (arrows) and cytoplasmic vesicles (*) are seen in this capillary endothelial cell. In transcytosis, they pinch off from the surface to form vesicles, which enter the cytoplasm, travel across the cell, and discharge contents to the opposite surface. The terminal end of a nerve cell contains many small, smooth-surfaced synaptic vesicles (arrows). They hold the neurotransmitter acetylcholine, which is discharged by exocytosis into the synaptic cleft. Mitochondria (Mi), which supply energy, are in the cytoplasm of both the nerve cell and muscle cell. They then enter the cytoplasm by pinching off from the surface and are transported to other parts of the cell. Endocytosis uses vesicles for cell uptake of extracellular fluid, macromolecules, and solutes. A nonselective form, called fluid-phase endocytosis (pinocytosis, meaning cell drinking), involves smooth-surfaced vesicles (diameter: 5080 nm) that pinch off from cell membranes to enter cells. Receptormediated endocytosis is highly selective uptake of macromolecules such as hormones and growth factors. Shallow surface depressions, named coated pits, give rise to clathrin-coated vesicles (diameter: about 200 nm). Specific macromolecules bind with more than 20 distinct types of transmembrane receptors. This pathway is used in metabolism of cholesterol, which most cells need for their membranes. Selective endocytosis is also mediated by small flask-like invaginations of plasma mem- 1. Many caveolae in endothelial cells mediate transcytosis, whereby vesicles derived from caveolae are taken across a cell and release their contents at another surface. Caveolae function in signal transduction, uptake of pathogenic bacteria, and oncogenesis. Other kinds of cytoplasmic vesicles, most derived from the Golgi complex, engage in exocytosis. In this pathway, vesicles move to the cell surface, fuse with plasma membrane, and discharge contents to the cell exterior. Synaptic vesicles of neurons and secretory vesicles of most secretory cells release products in this way. Defective receptors lose an affinity for coated pits, so cell uptake of cholesterol is blocked. Greatly elevated serum cholesterol may lead to premature atherosclerotic lesions in walls of blood vessels such as coronary arteries. An untreated disorder may result in myocardial infarction, stroke, and death in midlife. Treatments include low-saturated-fat diets, aerobic exercise, and cholesterol-lowering drugs. This cultured fibroblast from monkey kidney was treated immunocytochemically to reveal microtubules. The fluorescent immunolabel- an antibody to tubulin -shows the extensive network of microtubules in the cytoplasm. Microtubules originate from the microtubuleorganizing center (arrow), which is named the centrosome. Microtubules resemble railroad tracks, on which other organelles such as mitochondria are transported from one part of a cell to another. Of uniform diameter (25 nm), they are unbranched and extremely variable in length. They are found in most cells but are especially abundant in neurons, platelets, leukocytes, and dividing cells. They also help provide mechanical strength and establish cell shape as a major part of the cytoskeleton. They engage in intracellular transport of organelles (such as mitochondria and cytoplasmic vesicles), ciliary and flagellar motility, and cytokinesis during cell division. They have no membrane; their walls are composed of linear polymers (protofilaments) of the globular protein tubulin. The 13 protofilaments in each microtubule are formed by alternating alpha and beta subunits in a staggered assembly, which gives rise to a helical design of tubulin heterodimers in the cylinder wall.
Order anastrozole now
Diurnal variation of aldos terone and plas ma renin activity: timing relation to melatonin and cortis ol and cons is tency after prolonged bed res t menstrual questions answered discount anastrozole 1 mg mastercard. The excessive concentration o circulating cortisol causes degradation o muscle protein and an increase in the rate o gluconeogenesis. Symptoms o Cushing syndrome include muscle weakness (limbs may show muscle wasting), wide purplish striae, at deposition above the collar bone, and obesity (especially in the ace, neck, trunk, and abdomen). The elevated concentration o glucocorticoids also leads to insulin resistance (the mechanism o this alteration remains unknown). Synthetic glucocorticoids are used in supraphysiological concentrations in the treatment o allergies, rheumatoid arthritis, organ transplantation, ulcerative colitis, and multiple sclerosis. Examples include hydrocortisone, prednisone, dexamethasone, betamethasone, and triamcinolone. Long-term use o high-dose glucocorticoids leads to the same adverse ef ects as in Cushing syndrome, such as edema, muscle wasting, shi ing o at depots, and osteoporosis. These angiotensins stimulate the adrenal glands to synthesize and release aldosterone. Aldosterone in turn stimulates the synthesis o transporters in the kidneys that increase recovery o Na + rom the tubules in the kidneys. This recovery leads to an increase in blood pressure and in the concentration o Na + in the blood. Aldosterone def ciency leads to low blood pressure and aldosterone excess to high blood pressure. When blood pressure and the concentration o Na+ in blood are too low or when the concentration o K+ in blood is too high, angiotensin stimulates aldosterone synthesis. At low blood pressure, high [Na+], or low [K+] in blood, the activity o renin in blood increases. Aldosterone binds to the mineralocorticoid receptor in the kidneys and thus increases transcription o transport proteins in the renal tubules that take up Na+ rom the glomerular ltrate and transport it back into the blood. Secondarily, Na+ uptake af ects the transport o water and K+, such that aldosterone avors excretion o K+. Angiotensin receptors are ound not only in the adrenal glands but also throughout the vasculature; when activated in blood vessels, these receptors increase blood pressure via vasoconstriction. The aldosterone antagonists are the oldest drugs in this class and include spironolactone, eplerenone, and canrenone. These drugs prevent aldosterone rom activating the mineralocorticoid receptor in the kidneys. The Chvos tek s ign indicates hyperexcitability of the facial nerve, which is due to hypokalemia. The Trous s eau s ign is obs erved after 3 minutes of occluding the brachial artery; it indicates hyperexcitability and is due to hypokalemia. The concentration o aldosterone is unusually high due to overproduction, whereas the activity o renin is unusually low due to the high blood pressure; that is, the reninangiotensin system unctions normally. As a consequence o persistent hyperaldosteronism, compensatory processes become active such that the concentration o Na+ is high but still in the normal range, and the concentration o K+ is normal or low. Congenital adrenal hyperplasia is characterized by impaired production o both cortisol and aldosterone. Both glucocorticoid and mineralocorticoid synthesis are impaired, because the two classes o steroids share precursors and steroid-producing enzymes. The most common cause o congenital adrenal hyperplasia is a de ciency o 21 -hydroxylase. The severe, classic orms o this disorder are seen in ~1 in 15,000 newborns, whereas a less severe, nonclassic orm occurs in ~1 in 1,000 newborns. For this reason, in patients who have a 21 -hydroxylase de ciency, 17 hydroxylase converts 17 -hydroxyprogesterone to androstenedione, which then gives rise to excess testosterone. In the most severe 21 -hydroxylase de ciency, lack o aldosterone synthesis leads to salt wasting rom birth, which needs to be treated immediately. In girls, this de ciency also leads to masculinization in utero and hence ambiguous genitalia at birth. In a less severe classic orm o the disorder that does not entail salt wasting, there is similar masculinization in girls and boys. Finally, the mildest, nonclassic orm o 21 -hydroxylase de ciency leads to early virilization in boys and to hirsutism and male pattern baldness in women. Newborn screening or 17 hydroxyprogesterone allows the detection o babies who have a classic orm o 21 -hydroxylase de ciency. Patients who have the severe, salt-wasting orm o 21 -hydroxylase de ciency are typically treated with udrocortisone to restore blood pressure and the concentration o electrolytes in the blood. All patients who have classic 21 -hydroxylase de ciency are treated with a glucocorticoid, such as dexamethasone, in su cient amounts to reduce the excessive testosterone production. Some o the antibodies are directed against 21-hydroxylase (the same enzyme that is missing in most individuals who have congenital adrenal hyperplasia; see. Like other autoimmune diseases, predisposition to Addison disease is linked to certain major histocompatibility alleles. Calciol gives rise to calcidiol, which is stored in blood and is the major storage orm o vitamin D. In response to a low concentration o calcium or phosphate in the blood, calcidiol is hydroxylated to the biologically active calcitriol. Calcitriol stimulates transcription o certain genes with the e ect o increasing the concentrations o calcium and phosphate in the blood. Vitamin D is an umbrella term or several related compounds that play a role in calcium and phosphate homeostasis; the main biologically active compound is calcitriol. Vitamin D is not a steroid but rather a secosteroid; that is, a steroid with a broken ring. Vitamin D can be synthesized in the skin via a reaction that requires light or it can be obtained rom the diet. Vitamin D 3 (calciol, cholecalci erol) is synthesized rom cholesterol in the skin and is also ound in some animal products, such as oily sh, sh oil, or milk orti ed with vitamin D. Ergocalci erol dif ers rom cholecalci erol in the multicarbon substituent o the D-ring, but it seems to be as ef ective in humans as cholecalci erol. Calcidiol bound to vitamin D binding protein is the major storage orm o vitamin D. A similar reaction occurs with vitamin D2, but vitamin D3 is commonly the predominant orm o vitamin D. Measurement o bloodborne calcidiol is a common screening tool or vitamin D adequacy; this is typically done out o concern or ractures due to osteoporosis. Calcitriol (1,25-dihydroxycholecalci erol, 1,25dihydroxyvitamin D3), the biologically active orm o vitamin D3, is produced in the kidney in response to low blood calcium or phosphate concentrations. Calcitriol binds to a nuclear hormone receptor and increases transcription o certain genes. This heterodimer binds to a vitamin D response element in the promoter region o several genes, thereby avoring transcription o these genes. When the concentrations of calcium and phos phate in the blood are low, the pathway generates a higher concentration of circulating calcitriol. Calcitriol leads to an increase in the concentrations o calcium and phosphate in the blood via increased absorption in the intestine, increased recovery in the kidneys, and, when a special need arises, increased release rom hydroxyapatite in bone. These changes are a result o increased expression o transporters in the intestine and kidneys as well as increased activity o osteoclasts, which degrade bone. Vitamin D de ciency (see Chapter 12) results in a low concentration o calcium and phosphate in the blood, which in turn leads to insu cient mineralization o bone with calcium phosphate. In children, vitamin D de ciency leads to rickets, a condition characterized by so, pliable bones. In adults, vitamin D de ciency leads to osteomalacia, a condition in which bones are susceptible to racture due to demineralization. Vitamin D de ciency is also associated with increased rates o in ection, cancer, muscle weakness, and skin disorders including psoriasis. Steroids are membrane permeable and bind to receptors that are transcription actors. The selective estrogen receptor modulator clomiphene is used to treat in ertility.
Order anastrozole in united states online
Some o these transporters are Na+:amino acid cotransporters that use the inwarddirected concentration gradient o Na+ to pump amino acids into the epithelial cells (the same cells also contain a Na+:glucose cotransporter; see Section 3 women's health editorial calendar order anastrozole toronto. Other transporters use the membrane potential to pump positively charged amino acids into epithelial cells, and still others exchange intracellularly accumulated amino acids or other amino acids in the lumen o the intestine. With a weight-maintaining, typical Western diet, the total concentration o amino acids in the blood changes by less than ~20%. Plas ma amino acid pro les are as s ociated with ins ulin, C-peptide, and adiponectin levels in type 2 diabetic patients. Whole-blood and plas ma amino acid analys is: gas -liquid and cation-exchange chromatography compared. Amino acids in human blood plas ma after s ingle meals of meat, oil, s ucros e, and whis key. Cystine orms by the spontaneous oxidation and condensation o two cysteine molecules. Inside cells, an enzyme uses glutathione to reduce virtually all cystine to cysteine (or glutathione, see Chapter 21). However, in blood plasma, the concentration o cystine is about six times higher than that o cysteine. Cystine in the renal tubular uid crystallizes when its concentration exceeds the limit o solubility. The transporter is embedded in the brush border membrane o the epithelia o the kidney tubules. In England, Spain, and the Eastern Mediterranean region, cystinuria is ound in ~1 in 2000 newborns; in other populations, the disorder is somewhat less common. On average, about 10% o all children who present with kidney stones have cystinuria. About 10% o these patients show symptoms and there ore have Hartnup disease (its incidence is thus ~1 in 300,000 persons). The symptoms arise rom a de ciency o tryptophan, and some o the symptoms resemble those o pellagra (a de ciency o nicotinic acid; see. Later, they may have intermittent cerebellar ataxia (lasting a ew days), emotional lability, and psychosis. T ose patients who have a low concentration o amino acids in the blood should also consume a high-protein diet. O the 21 amino acids needed or translation, humans can synthesize about hal; they must consume the remainder with the diet. Humans must consume a minimum o about 50 g o protein per day because an equivalent amount o amino acids is oxidized or used or the synthesis o nonprotein compounds. The term nitrogen balance is a measure o the dif erence between protein intake and nitrogen loss (see Section 5 in Chapter 35). Cystinuria is treated by alkalinizing the urine with oral potassium citrate (at a higher pH, cystine is more soluble) and by maintaining a large ow o urine (to lower the concentration o cystine). Patients are also advised against consuming a lot o protein or salt; protein contains cysteine, and salt increases the excretion o cystine or unknown reasons. I these measures do not provide satis actory results, patients can o en be given penicillamine (a degradation product o penicillin), meso-2,3-dimercaptosuccinic acid, or -mercaptopropionyl glycine (also called thiopronin). For growing children, this list has to be expanded; they must consume Arg because they commonly do not produce enough o it in the urea cycle (see Section 2. In Europe, this raction is 20% to 30%; in A rica, it is 0% to 30%; and in Asia, it is generally 10% to 20%. Children, pregnant women, and patients who are recovering rom surgery or trauma need more protein in the diet than the World Health Organization recommends or healthy people. Hospitalized patients who receive parenteral nutrition, or example, are commonly given 0. Humans can synthesize Ala, Asp, Asn, Gln, Glu, Pro, and Ser starting with intermediates o glycolysis and the citric acid cycle. Because humans can synthesize these amino acids and do not need them in the diet, they are called nonessential or dispensable amino acids. Flux into the blood mainly depends on intestinal uptake o amino acids rom dietary protein and on the degradation o body protein. In the asting state, muscle is the major producer o amino acids, and the liver is the major user. It is not clear which proteins participate in this cycle o protein synthesis and protein degradation; the regulation o the cycle is likewise incompletely understood. Accordingly, leucine stimulates protein synthesis and inhibits protein degradation postprandially. In the asting state, when muscle protein is degraded, leucine is transaminated within muscles and only the resulting keto acid is released into the blood (the same is true o the other branchedchain amino acids, isoleucine and valine). Sources o dietary protein can be rated or their quality, or how well they match the needs o the human body. For instance, gelatin (as contained in Jell-O) is a very low-quality protein because it consists mostly o collagen, which contains mostly glycine, proline (some o it as hydroxyproline), and alanine (see Chapter 12). In contrast, human breast milk is a source o very high-quality protein or in ants because the amino acid composition o milk proteins closely matches the requirements. For people who eat mostly a vegan diet, methionine is usually the limiting essential amino acid. Individuals who eat a high-protein diet consume as much as 3 g o protein per kilogram o body weight per day. A er a meal, the pancreatic islets secrete insulin in response to glucose and presumably an increase in the concentrations o leucine, glutamine, and arginine (details are not certain; see Section 3. Protein synthesis lowers the concentrations o branched-chain and other essential amino acids in blood plasma. Glucagon stimulates gluconeogenesis in the liver and in the kidneys (see Section 3 in Chapter 25), which lowers the concentration o amino acids in the blood. In the asting state, 378 Diges tion of Dietary Protein and Net Synthes is of Protein in the Body the pancreas secretes glucagon in response to epinephrine and a lower concentration o glucose. Note that muscle does not have appreciable numbers o glucagon receptors and hence does not respond to glucagon. Cortisol stimulates degradation o muscle protein, oxidation o branched-chain amino acids in muscle, and use o the released amino acids in gluconeogenesis by the liver and the kidneys. The adrenal medulla secretes cortisol in a diurnal ashion so that the concentration o cortisol in the blood is highest in the early morning and lowest in the early evening. Patients who are treated with high doses o glucocorticoids and patients who have a high concentration o circulating cortisol due to Cushing syndrome both show muscle wasting (see Section 4. In the acidic lumen o the stomach, pepsinogens autocatalytically activate to become active pepsins, which cleave dietary proteins. The pancreas secretes bicarbonate, which raises the pH o chyme in the duodenum to a value greater than 7. Enterokinase on the sur ace o the intestinal brush border membranes, when activated by bile salts, cleaves trypsinogen to produce trypsin. Pancreatitis is associated with activation o trypsin and other digestive enzymes inside the pancreas. In most cases, pancreatitis is due to blockage o the common bile duct or due to the alcohol dependence syndrome. In patients with cystic brosis, inadequate ushing o zymogens out o the pancreas into the intestine causes pancreatitis and loss o pancreatic unction. Patients who express mutant trypsinogen or mutant pancreatic trypsin inhibitor develop pancreatitis at a young age. The brush border membrane o the epithelium o the small intestine contains aminopeptidases that hydrolyze single amino acids rom the N-terminus o oligopeptides. A large number o dif erent transporters acilitate amino acid transport rom the intestinal epithelium into the blood, rom the blood into peripheral cells, and rom the renal glomerular ltrate into tubular cells and rom there to the blood. Patients who have cystinuria cannot e ciently remove cystine rom the glomerular ltrate and orm cystine stones in the kidneys. Patients with Hartnup disease show symptoms o tryptophan de ciency that is caused by de cient transport o neutral amino acids into the intestinal and renal epithelial cells. Humans must consume certain amino acids in their diet because they cannot synthesize them. These amino acids are called essential amino acids and comprise Arg, His, Ile, Leu, Lys, Met, Phe, T r, rp, and Val.
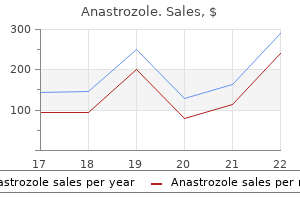
| Comparative prices of Anastrozole | ||
| # | Retailer | Average price |
| 1 | Aldi | 914 |
| 2 | Dollar General | 271 |
| 3 | ShopRite | 615 |
| 4 | Verizon Wireless | 976 |
| 5 | CVS Caremark | 561 |
| 6 | Bon-Ton Stores | 604 |
Generic anastrozole 1mg on-line
Computed tomography reveals thickening of the bowel menopause that 70s show cheap anastrozole 1mg line, and barium enema examination reveals classic spicules of the mucosa, strictures, or loss of haustral markings. Therefore, most clinicians choose colonoscopy over barium enema, although the latter is helpful in select cases. Initial treatment usually starts with a variety of antiinflammatory agents, such as sulfasalazine (the former top choice) or mesalamine. Research and university centers may use sophisticated indices to evaluate the course and end points of treatments. Their lifetime incidence of colorectal cancer approaches 6%, and the cancer-related mortality rate is approximately 3%. Ekbom A, Helmick C, Zack M, et al: Ulcerative colitis in colorectal cancer: a population-based study, N Engl J Med 323:1228-1232, 1990. This chapter lists all the complications, but detailed discussions of each may be found throughout this text and in the literature. More than one extracolonic manifestation occurred in approximately 25% of patients. The cause of the extracolonic manifestations is unknown; Box 145-1 lists the sites most often involved. However, the literature includes reports of scattered cases in the bronchopulmonary, renal and genitourinary, cardiac, endocrine, and neurologic organs. Manifestation may occur without active disease, but it occurs more frequently when disease activity is increased. Therefore, it is imperative that the disease be controlled and treated to ameliorate the extraintestinal manifestations. Pyoderma gangrenosum is a classic manifestation for which intensive therapy may be necessary. Treatment of the pyoderma may require corticosteroids, which would not be used for the disease itself. Once again, each manifestation must be treated individually, in accordance with the experience readily available in the literature. Biological therapy is now being used more frequently in an attempt to control the symptoms rapidly when steroids are not immediately effective. Sclerosing cholangitis may progress to liver failure and liver complications, resulting in liver transplantation. Therefore, patients must be diligently placed on calcium and vitamin D intake and any necessary bone-stimulatory drugs. Free perforation may result from small lesions, which require good surgical support with appropriate surgical intervention as each case indicates. Once a stricture is identified, the clinician should investigate whether a lesion is local. Because stent placement may be attempted, obtaining a specimen through biopsy or resection of the area is recommended, so as not to overlook a malignancy. Careful surveillance and surgical intervention are required whenever a severely dysplastic lesion is suspected. It is essential to control the diarrhea to control the irritation of the anal ring. Reassurance and frequently psychotherapy are needed for them to cope with the recurrent manifestations of the disease. However, complications or extraintestinal manifestations such as sclerosing cholangitis can occur even after total colectomy. Fortunately, the rate of extraintestinal manifestations and complications is less than 50%, and those unaffected can lead normal lives. Monsen U, Sorstad J, Hellers G, Johansson C: Extracolonic diagnosis in ulcerative colitis: an epidemiologic study, Am J Gastroenterol 85:711-716, 1990. Olsson R, Danielsson A, Jarnerot G, et al: Prevalence of primary sclerosing cholangitis in patients with ulcerative colitis, Gastroenterology 100:13191323, 1991. Fortunately, massive hemorrhaging from the bowel is not as frequent as once believed. However, when a massive hemorrhage does occur and bleeding does not stop with standard intravenous therapy, colectomy may be necessary. Deficiencies of other vitamins or of folic acid that occur with sulfasalazine therapy are treated with replacement of those vitamins. Free perforation usually complicates toxic megacolon; therefore, toxic dilated bowel requires immediate surgical intervention when medical therapy fails. Socalled crypt abscesses are usually described in the acute form and contain neutrophils. An often-described, ambiguous feature is an excess of intraepithelial neutrophils or lymphocytes, in which the infiltrate in the lamina propria is not severe. Basal plasmocytosis, when at least three plasma cells are found below the crypt area, may be a significant finding. Infectious colitis causes an acute inflammatory response, but rarely are crypt areas distorted. Chronic radiation disease and chronic graft-versus-host disease may elicit similar responses. Eosinophilic gastroenteritis may be included in the differential diagnosis (see Chapter 117). Although it is difficult to differentiate the three categories, certain criteria can establish a category. The clinician must emphasize the importance of a correct diagnosis to the pathologist interpreting the specimens. Low-grade dysplasia can be defined as "nuclear crowding," with some stratification of nuclear pleomorphism and hyperchromasia. High-grade dysplasia has more marked nuclear pleomorphism, hypochromasia, and stratification, and there may or may not be architectural abnormalities such as villi-formed surfaces. Whenever there is marked inflammation and apparently significant reparatory changes, it may be difficult or impossible to distinguish reactive changes from true dysplasia. The bowel with no dysplasia presumably goes through a formation process of indefinite dysplasia, low-grade dysplasia, high-grade dysplasia, and then carcinoma. Other changes in genetic regulation, such as induction of the K-ras oncogene, and loss of other functioning tumor-suppressor genes, in addition to the p53 gene function, appear to permit adenoma to progress to carcinoma. Typical figures judged as "presence" of crypt atrophy, which was recognized by generally increased distance of more than one crypt diameter between crypts (D), or a general increase in the distance between crypts and the muscularis mucosae (E). If no dysplasia or adenoma formation is seen on first colonoscopy, it is safe to monitor the patient every 2 years. Although no random clinical trials have been conducted, several cohort and case series indicate that monitoring does have a role in preventing cancer. Surveillance colonoscopy includes thorough evaluation of the colon, with specimens for mucosal biopsy taken every 5 to 10 cm. Physicians disagree on the number of biopsy specimens needed, but most agree at least 10 areas should be sampled. Controversy surrounds whether low-grade dysplasia is an indication for surgery, but most agree that the presence of high-grade dysplasia, or adenoma within active disease, warrants total colectomy. Itzkowitz S: Colon carcinogenesis in inflammatory bowel disease: applying molecular genetics to clinical practice, J Clin Gastroenterol 36:S70-S74, 2003. During the past decade, ileal pouch anastomosis has become the treatment of choice. However, some patients do not have the appropriate body build for a pouch, or they may have a relative contraindication. For these patients, total colectomy with ileostomy is the treatment of choice (see Chapters 148 and 149). Ileostomy is a safe procedure, and long-term analysis now reveals that ileoanal pouches are safe, although some patients do experience pouchitis. After the ileostomy is created, the patient is given several months to recover, and then the rectum is removed and the perineum closed. This procedure is associated with less sexual dysfunction than other procedures and does not hinder female reproduction.
Cheap 1mg anastrozole otc
Congenital neural tube de ects are partially preventable with supplemental olic acid menopause depression treatment purchase anastrozole 1 mg visa. Epidemiological studies revealed that 30% to 70% o the neural tube de ects can be prevented with supplements o olic acid given to women who contemplate pregnancy or who have just become pregnant. Accordingly, some countries require that grain products be enriched with olic acid. This change reduced the birth prevalences o spina bi da and anencephaly by about 30% in the United States and by about 45% in Canada. One-Carbon Metabolis m, Folate De ciency, and Cobalamin De ciency 413 acid to accommodate the needs or tissue production in the mother and etus. The C677 mutation results in an Ala Val substitution, which renders the enzyme less stable. When olate intake is low, this mutant enzyme is associated with an increased concentration o homocysteine in the blood. A low intake o olic acid early in pregnancy is also associated with an increased incidence o conotruncal heart de ects, cle lip, and cle palate. In contrast, once a tumor has developed, olate de ciency has the bene cial ef ect o slowing the replication o cells (this is the basis o the ef ect o methotrexate and other anti olate chemotherapeutic agents; see Chapter 37). Cysteine, in turn, is used or the synthesis o glutathione, taurine, and conjugated bile salts. Catabolism o cysteine yields sul ate, some o which is conjugated with xenobiotics and drugs. The transsul uration pathway commonly re ers to the conversion o homocysteine to cysteine. The pathway is most active in the liver and, to a lesser extent, the kidneys, intestines, and pancreas. The enzymes that convert homocysteine to cystathionine and then cysteine require pyridoxal phosphate (a derivative o vitamin B6). For yet unknown reasons, cystathionine is present in the brain at millimolar concentrations and is needed or the proper unction o the brain. A cystathionine -synthase de ciency is the cause o classical homocystinuria; patients with this disease have severe hyperhomocysteinemia, mental retardation, osteoporosis in childhood, thromboembolisms in their teens and twenties, subluxation o their lenses be ore age 30 years, and a reduced li e span. The disease is inherited in autosomal recessive ashion and occurs in 1 o about 50,000 newborns. Most patients are treated with a low-methionine diet and given a supplement o cystine. Some patients respond to large doses o vitamin B6, which gives rise to pyridoxal phosphate, the co actor o cystathionine -synthase. Many patients who do not respond to extra vitamin B6 do respond to supplemental betaine; betaine helps methylate homocysteine to methionine in a reaction that occurs parallel to the one that is catalyzed by methionine synthase. Free cysteine is used or the synthesis o glutathione, an antioxidant and radical scavenger (see Chapter 21). Many cells contain millimolar concentrations o glutathione, and glutathione also serves as a reservoir or cysteine. The concentration o cysteine is the rate-limiting actor in the synthesis o glutathione. Free cysteine itsel, together with iron, orms toxic ree radicals, and the intracellular concentration o cysteine is kept relatively low (~<0. Patients who have megaloblastic anemia most o en have a primary or secondary olate de ciency. Laboratory data that support a primary olate de ciency include a low concentration o olate and a normal concentration o cobalamin and methylmalonic acid in the serum. Laboratory data that support a cobalamin de ciency are a low concentration o cobalamin and an elevated concentration o methylmalonic acid in the serum. Because a cobalamin de ciency damages the nervous system and high doses o olates can cure the megaloblastic anemia, it is important that olate-de cient patients be tested or cobalamin de ciency and given cobalamin i needed. A olate de ciency is treated with oral olic acid or with oral or injected leucovorin. Methanol poisoning causes the transient accumulation o millimolar concentrations o ormate in the blood, which can cause severe metabolic acidosis as well as severe damage to the optic nerve. The accumulation o ormate can be prevented with omepizole (an inhibitor o alcohol dehydrogenase) or with ethanol (another substrate o alcohol dehydrogenase). In patients poisoned with ethylene glycol, omepizole or ethanol are used in a similar manner. One-Carbon Metabolis m, Folate De ciency, and Cobalamin De ciency 415 Free cysteine is toxic. Cysteine is needed or the synthesis o glutathione, which is used or diverse redox reactions. Degradation o glutathione yields cysteine, and glutathione thus also serves as a reservoir or cysteine. When cysteine is metabolized, it can give rise to taurine, which serves as an intracellular osmolyte and which the liver conjugates with bile acids. In addition, intravenous administration o which one o the ollowing would be most appropriate to prevent damage to her optic nerve An anemic patient is ound to have a low serum olate level and a serum cobalamin level that is inconclusive. A common test to distinguish primary olate de ciency rom cobalamininduced secondary olate de ciency involves measuring which o the ollowing Red blood cell olate Serum antibodies to haptocorrin (R-binder) Serum homocysteine Serum methylmalonic acid 3. Based on preliminary data, investigators hypothesized that cobalamin de ciency is a side ef ect o met ormin treatment. A signi cantly elevated concentration in met ormin-treated patients o which one o the ollowing metabolites would be the strongest indication that the hypothesis is correct This enzyme can be inhibited by hydroxyurea or the active metabolite of gemcitabine. Hydroxyurea is also used to reduce the frequency of sickle cell crises in patients who have a sickle cell disease. Describe the ribonucleotide reductase reaction and its regulation, and explain its role in cancer chemotherapy with hydroxyurea or gemcitabine. Compare and contrast the effects of 5- uoruracil, pemetrexed, and methotrexate on the synthesis of thymidine, paying special attention to the mechanisms of action. Glycogen synthesis, glycosylation reactions, and glucuronidation reactions require U P (see Chapters 7, 14, and 24). Most pyrimidine nucleotide synthesis takes place in the liver and in dividing cells, such as intestinal epithelial cells, erythropoietic cells in the bone marrow, and tumor cells. The liver provides a service to other cells by synthesizing uridine and releasing it into the blood. The concentration o orotate in the urine is used to determine the cause o urea cycle de ects. The early steps in orotate synthesis take place in the cytosol and nucleus, but the nal step takes place in the intermembrane space o mitochondria. Dihydroorotate dehydrogenase is an integral protein o the inner mitochondrial membrane that oxidizes dihydroorotate in the intermembrane space. T ereby, the enzyme reduces ubiquinone in the membrane to ubiquinol, which is part o the electron transport chain. In the body, le unomide is metabolized to teri unomide, which inhibits dihydroorotate dehydrogenase and thus leads to a de ciency o pyrimidine nucleotides, particularly in lymphocytes. Uridine and other unphosphorylated nucleosides cross cell membranes through nucleoside transporters, some o which of er acilitated passive dif usion, whereas others actively pump nucleosides. The de ciency is usually a consequence o the direct inhibition o the enzyme by Pb2+ in lead poisoning; an inherited de ciency is rare. Chemotherapeutic and antiviral drugs that are analogs o normal pyrimidine nucleosides enter cells through transporters or uridine or thymidine. Examples o such chemotherapeutic drugs are 5- uorouracil and gemcitabine (2,2-di uoro-2deoxycytidine). C P is used in the synthesis o phospholipids, such as phosphatidylinositol, phosphatidylcholine, phosphatidylethanolamine, and phosphatidylserine (see Chapter 11; phospholipid synthesis is not covered in this book). Ribonucleoside diphosphate reductase is the target o the antineoplastic drugs hydroxyurea and gemcitabine.
Buy 1mg anastrozole amex
Indeed women's health health magazine cheap 1 mg anastrozole mastercard, a er a moderate to large dose o ethanol, there is a mild increase in plasma urate and a more pronounced increase in urine uric acid. Alcohol also leads to a small increase in the concentrations o lactate and ketone bodies in the blood. Both lactate and ketone bodies decrease uric acid excretion by the kidneys (see Chapter 38). Consumption o beer or liquor at the world average o about 11 g o ethanol per day is associated with an increased concentration o urate in blood plasma, as well as an increased incidence o gout; this is not the case with a similar amount o alcohol consumed as wine. The reasons or these dif erences are not entirely clear, except that beer contains a signi cant amount o guanine, some o which is taken up and degraded to urate. Ge ne ral Co mme nts Abo ut Alc o ho l De pe nde nc e Syndro me Alcoholism is considered a mental disorder. In the United States in 2012, approximately 7% o people aged 18 years or older had alcohol use disorder. In the United States, the National Institute on Alcohol Abuse and Alcoholism de nes binge drinking as drinking that results in a blood alcohol content o 80 mg/dL or higher. Many adults reach this concentration by consuming our to ve drinks during a 2-hour period. The same institution considers low-risk drinking as the consumption o ewer than 3 to 4 drinks in one day and ewer than 7 to 14 drinks per week (lower numbers are or women, higher numbers or men). Chronic, excessive use o alcohol is associated with chronic disease, accidents, social problems, and increased domestic violence. In the United States, s alcohol-induced chronic disease is responsible or about hal o all alcohol-attributable deaths and about one-third o alcohol-attributable potential li e years lost. Metabolis m of Ethanol and the Cons equences of Alcohol Dependence Syndrome 333 Alcoholism is partly hereditary. Of spring o one alcoholabusing parent are about ve times more likely to abuse alcohol than of spring o nonabusing parents. Studies o twins show that genetic actors account or about 50% o the interindividual variation or alcoholism. Linkage studies implicate mutations that af ect enzymes o ethanol metabolism and proteins that likely also play a role in neurotransmission. People who experience acetaldehyde-induced ushing and nausea a er alcohol consumption are least likely to become alcohol dependent. Mitochondrial acetaldehyde dehydrogenase unctions as a tetramer, and the Glu487Lys variant shows a dominant negative ef ect (see Chapter 5). Homozygotes have virtually no risk o becoming alcohol dependent, whereas heterozygotes have only about one- ourth the risk o patients with normal acetaldehyde dehydrogenase activity. A er consumption o alcohol, this variant enzyme completes about 30 catalytic cycles in the time the normal enzyme completes one cycle. Patients who chronically consume large quantities o alcohol o en develop malnutrition. One gram o ethanol provides about 7 kcal (carbohydrates and proteins provide 4 kcal/g, and at provides 9 kcal/g). Many alcohol-dependent individuals consume only about hal as much ood as alcohol abstainers do. In addition, alcohol intake diminishes the absorption o phosphate and some vitamins in the intestine. Acetaldehyde adducts and mixed adducts o acetaldehyde and malondialdehyde are immunogenic. The concentration o acetaldehyde in cells depends on the rates o its production and oxidation. Normally, most acetaminophen is detoxi ed via glucuronidation or sul ation, and only about 15% is eliminated via the P450 system. In alcohol-dependent individuals, due to higher activity o alcohol-metabolizing cytochromes P450, a much greater raction o acetaminophen is detoxi ed through the P450 system. Drug s That He lp Patie nts Fre e the ms e lve s Fro m Alc o ho l De pe nde nc e Current treatment programs or alcohol-dependent patients are only moderately ef ective. The major drugs used or the treatment o alcohol dependence are acamprosate, naltrexone, and disul ram. De novo atty acid synthesis normally contributes only a minor portion o the atty acids in triglycerides; this is also true or patients who consume excessive amounts o alcohol. T us alcohol and its metabolite acetaldehyde have direct toxic ef ects on proteins; they induce the expression o alcohol-metabolizing cytochromes P450 that generate ree radicals, and they stimulate excessive synthesis o extracellular matrix components. In the absence o treatment, the combination o alcohol-induced atty liver and in ammation is particularly dangerous; survival or more than 4 months is only approximately 70%. Stellate cells (at-storing cells, Ito cells, lipocytes) in the liver play a key role in the pathogenesis o ethanol-induced brosis. Stellate cells are normally the major producers o extracellular matrix in the liver, and they also store retinoic acid esters in lipid droplets. In response to alcohol and acetaldehyde, stellate cells morph into broblasts that store little retinoic acid and produce extracellular matrix at an increased rate. In the upper digestive tract, particularly the esophagus, some resident microbes convert ethanol to acetaldehyde, which is mutagenic to epithelial cells. Cancer risk rom smoking and alcohol abuse is greater than the sum o the individual risks. The combination o alcohol and smoking is a particularly strong risk actor or the development o cancer o the oral cavity, pharynx, and esophagus. Procarcinogens in smoke converted to who regularly abuse alcohol drink alcohol because it makes them eel better or because it alleviates symptoms o withdrawal. Naltrexone, an opioid receptor antagonist, reduces the craving or alcohol and also diminishes the "elevated" eeling a er alcohol. However, when a disul ramtreated patient consumes alcohol, headache, nausea, vomiting, chest pain, and other symptoms set in due to an excessive concentration o acetaldehyde; this discourages the patient rom consuming more alcohol. A disul ram-treated patient who nonetheless drinks a large quantity o alcohol risks severe pathologic ef ects. An extract o the root o kudzu, a traditional Chinese medicine, also inhibits alcohol consumption. All orms o liver disease together account or about one- h o all alcohol-attributable deaths and potential li e years lost. Fatty liver (hepatic steatosis) is an early and common consequence o chronic alcohol abuse. The steatosis is the result o increased production and decreased export o triglycerides (see Section 3. The populations are as follows: gray line, J apan; black line, Italy and Switzerland; red and blue lines, meta-analys is of 51 s tudies in divers e countries. Genetic polymorphis ms of alcohol and aldehyde dehydrogenas es and glutathione S-trans feras e M1 and drinking, s moking, and diet in J apanes e men with es ophageal s quamous cell carcinoma. Es timating dos e-res pons e relations hip between ethanol and ris k of cancer us ing regres s ion s pline models. Less severe pathological ef ects o alcohol consumption are seen in about 1% o all newborns. Y only a racet, tion o such alcohol-abusing mothers gives birth to a child with the complete etal alcohol syndrome, most likely because genetic actors also play a role. Alcohol exposure early in pregnancy and in the last trimester (a period o extensive synaptogenesis) is especially damaging to the of spring. Whether there is a sa e amount o alcohol that can be consumed during pregnancy is unknown. In the etus, alcohol leads to apoptosis o cranial neural crest cells as well as the abnormal migration o neurons and glial cells. Children who are af ected with the most severe orm o etal alcohol syndrome have abnormal acial eatures. Un ortunately, a high raction o such persons spends time in prison or in a mental institution. The mechanisms by which alcohol causes neural crest cells to die by apoptosis are incompletely understood, but retinoic acid likely plays a role. Retinoic acid activates several transcription actors that play a role in development.
Anastrozole 1mg sale
Inspection and digital examination are essential in all evaluations of external hemorrhoids pregnancy countdown cheap anastrozole 1mg on line. Proctologic or sigmoidoscopic examination is required when internal hemorrhoids are suspected: these are visualized in the rectal vault. Floch 163 P rolapse of the rectum is a condition in which one or more layers of the rectum or anal canal protrudes through the anal orifice. Partial prolapse involves only the mucosa, which usually extends no more than 1/2 to 1 inch (2. The mass is larger and bulbous, and it may eventually contain a hernial sac of peritoneum with a segment of bowel in the interior. Prolapse occurs with defecation, usually reduces spontaneously with conservative treatment, and is self-limited. It is associated with poor pelvic musculature tone, chronic straining, fecal incontinence, and often neurologic or traumatic damage associated with the pelvis. Its etiology remains unknown, but a defect in the supporting structures may permit increased intraabdominal pressure to produce the prolapse. In elderly or debilitated persons, prolapse is usually caused by a loss of sphincteric tone. Procidentia necessitates digital rectal examination, and an attempt should be made to reduce the mass. For these patients, a colorectal surgeon should be involved in evaluating the procidentia. Some are simple and others are complex, involving a combined procedure in which the rectum is fixed to the sacral hollow and the redundant sigmoid colon is removed. The type of procedure and the outcome vary and depend on the degree of the prolapse and the experience of the colorectal surgeon. In very elderly patients, simple extraabdominal approaches through perineal rectosigmoidectomy are possible. Some studies of these approaches in this select patient group have shown great success. Careful history reveals they can feel there is prolapse of tissue with defecation. Prolapse is often associated with straining and with a sensation of incomplete evacuation and of the mass. Complete rectal prolapse (procidentia) is large, and patients seek treatment fearing that the mass they can sense is malignant. When incontinence becomes a problem, or when the prolapse is complete, various surgical interventions are possible. A 90% success rate is reported in very elderly patients who require an extraabdominal approach. If the patient has uncontrolled prolapse and colostomy is necessary, prognosis depends on the debilitating disease, but colostomy is usually successful. At times, the diagnosis cannot be made in this position, and the patient must be placed in the upright position, or sitting, so that straining will produce the prolapse. A detailed workup is needed to rule out malignancy and should include colonoscopic examination and computed tomography of the pelvis to ensure that no perirectal lesion increases intraabdominal pressure on the rectum. The cause of an anal fissure typically is unknown, but it is clearly associated with increased resting anal pressure. Some may experience incontinence, although the rate of this surgical complication is extremely low. Course and Prognosis As indicated, outcomes are excellent for most patients with anal fissure, and cure rates range from 50% to 70% after medical therapy and 70% to 90% after surgical therapy. Some fecal incontinence may occur after surgical treatment, but recurrence is low. Clinical Picture the classic presentation of anal fissure is acute, severe pain on defecation that may persist for hours after passage of the fecal bolus. Bleeding may be associated with the fissure, with blood on the toilet paper or in the bowl. However, the pain is significant and is the hallmark of the clinical presentation. Treatment for pruritus ani is whichever therapy is necessary for the primary disease and symptoms. For troublesome pruritus, the patient should discontinue irritating soap and use hypoallergenic soap instead, apply a hydrocortisone cream regularly, keep the anal area clean, and use a protective ointment such as zinc oxide. If the fissure is seen and is in the midline, it is not secondary to other diseases, and treatment can be used as a therapeutic trial. If there is any uncertainty about the diagnosis, sedation and anesthesia may be necessary to enable appropriate examination of the patient. Medical therapy should be tried first, including a course of Sitz baths, psyllium fiber supplements to soften the stool, or emollient suppositories. Some clinicians have used Sitz baths plus bran supplementation, at least 15 g daily, which has also been successful. Use of 2% lidocaine ointment plus 2% hydrocortisone cream has proved to be successful in approximately 60% of patients. When simple medical therapy does not succeed, other options include topical therapy. Healing has been reported in as many as 77% of patients with the use of four suppositories for 8 weeks. Botulin toxin (Botox) has yielded excellent results and healing rates of 82% and 79% at 3 and 6 months, respectively. Gradually, the hypertrophic papillae may develop a stalk and then change to a so-called fibrous polyp, which may produce the sensation of a foreign body in the anal canal. Cryptitis may remain restricted to circumscribed reactions in and around the crypts, or it may spread to the surrounding tissues, including the formation of abscesses and fistulae (see Chapter 165). Symptoms of cryptitis occasionally resemble those of a fissure and often include itching and radiation of pain, which is aggravated by defecation. Visualization of the cryptitis and any purulent discharge or granulation tissue, or of the hypertrophied papillae, is necessary. Freuhauf H, Fried M, Wegmueller B, et al: Efficacy and safety of botulinum toxin A injection compared with topical nitroglycerine ointment for the treatment of chronic anal fissure: a prospective randomized study, Am J Gastroenterol 101:2107-2112, 2005. Floch 165 L ocalized infection with a collection of pus in the anorectal area is designated an anorectal abscess. Usually, it results from the invasion of the normal rectal flora into the perirectal or perianal tissues. The pathologic process seems to start with inflammation of one or more of the crypts (see Chapter 164), spreads to the anal ducts and anal glands, and then spreads submucosally, subcutaneously, or transsphincterally to the surrounding tissue. This sequence of events closes with the spontaneous rupture of the abscess, either into the anorectal canal or through the perianal skin, if the abscess has not been drained surgically. After the abscess has perforated, the cavity and its outlet shrink, leaving a tubelike structure, an anorectal fistula, which invariably is the result of the abscess. The levator ani plane, demarcating the various perineal pelvic spaces, is used to classify anorectal abscesses according to localization. Retrorectal, pelvirectal, and submucosal abscesses belong to the supralevator abscesses and have a somatic sensory nerve supply; therefore, these cause a sensation of discomfort from pressure rather than from pain in the anorectal region. Retrorectal and pelvirectal abscesses originate from infectious processes in other pelvic organs and thus are not anorectal lesions in the strict sense, although they usually rupture into the rectum or the anal canal. Infralevator abscesses are also divided according to site into subcutaneous, intramuscular, fistulorectal, and cutaneous abscesses. The fistula is called complete when both openings, the primary and the secondary, can be detected and are accessible. Such a complete variety usually connects the rectal lumen with the anal or perianal skin. Other diseases may cause a similar picture, such as diverticulitis and Bartholin abscesses. Past treatments used setons, but this form of therapy alone is now used less often and is combined with other therapy, such as infliximab. For large abscesses or those in patients with underlying disease, surgery is necessary. Mortality is as high as 50% if surgery is delayed and a necrotizing anorectal infection develops. Although antibiotics may not be necessary for small lesions, most clinicians believe antibiotics are important, especially if the patient has an underlying associated disease. Antibiotic therapy must treat the aerobic and the anaerobic flora and therefore is usually a combination of drugs.

Buy generic anastrozole 1 mg on line
Furthermore zeid women's health center order anastrozole without prescription, if the dietary fiber intake is heavy in soluble fiber, such as from fruits and vegetables or psyllium seed, the bacterial flora will increase and flourish and will be larger than if the dietary fiber consists of cellulose and insoluble fibers from bran. In the latter case, the stool volume might still be large, but this results from the waterholding property of insoluble fiber rather than increased bacterial flora. When acute diverticulitis develops, physicians usually restrict the amount of dietary fiber the patient can consume until the episodes have been resolved. Some large national studies reveal, however, that subjects on high-fiber diets experience less polyp formation and fewer coronary artery diseases. Consequently, most clinicians recommend a high-fiber diet to prevent diverticulosis of the colon, polyp formation, and atherosclerotic disease. Recent studies also indicate that subjects who eat high-fiber diets tend to experience less morbid obesity. Naturally, these subjects eat less fat and sugar; thus, their high-fiber diet decreases their nutrient energy intake. The therapeutic recommendation for the intake of dietary fiber is 20 to 35 g daily, depending on the meal size and caloric intake. The recommendation also states that broad types of dietary fiber should be consumed, and that the intake should include a mixture of soluble and insoluble fiber. Also, colon diverticula are less common in those who eat high-fiber diets, and diverticular formation may be prevented in susceptible subjects. It is recommended that the patient with diverticular disease maintain a high-fiber diet. Table 268-1 Dietary Fiber Food Sources Serving Size Soluble Fiber Content per Serving (g) 0. Dietitians and clinicians usually recommend five portions of fruits, vegetables, or grains, averaging 4 to 5 g each, and thus meeting the necessary requirement of 20 to 35 g daily. Trowell H, Burkett D, Heaton K: Dietary fibre, fibre-depleted foods and disease, London, 1985, Academic Press. Serum triglyceride levels should be checked at least weekly to prevent serum levels from exceeding 500 mg/dL. Indications for home parenteral nutrition include short bowel syndrome, severe radiation enteritis, distal intestinal fistula, and mechanical intestinal obstruction when surgery is not immediately possible. Hospital case managers should be directly involved in arranging hospital discharge, ensuring all criteria are met for insurance reimbursement. Home parenteral nutrition is associated with complications that must be recognized and addressed appropriately. Multiple trace elements, which include manganese, copper, chromium, selenium, and zinc, should be checked at least every 6 months. Cholestatic liver disease increases the risk for manganese and copper toxicity because these two trace elements are excreted primarily through the hepatobiliary system. Access for parenteral nutrition can be through a peripheral vein, if the dextrose concentration will be less than 5%, or through a central vein if the dextrose concentration will be greater than 5%. Administering a dextrose concentration greater than 5% through a peripheral vein can result in thrombophlebitis. When administering central parenteral nutrition, direct subclavian vein placement has traditionally been the method of placement. However, a peripherally inserted central catheter inserted through the brachial vein and advanced to the superior vena cava is the preferred method because it averts the risk for pneumothorax associated with the placement of subclavian lines. Before infusion is initiated, proper insertion of the catheter tip in the superior vena cava should be confirmed by chest radiograph. Total parenteral nutrition is usually given as a 2-L, 3-in-1 (3: 1) solution containing carbohydrate, protein, and lipid mixed together. The patient should be started on half the rate (40 mL/hr) for the first 24 hours; this can be increased to full rate (80 mL/hr) if tolerated by the patient. If blood glucose levels are higher than 200 mg/dL, regular insulin may need to be added P Malnutrition James S. Scolapio 270 expected weight for height, and children often have greatly impaired longitudinal growth. Diminished skinfold thickness and reduced midarm muscle circumference and temporal wasting illustrate the loss of fat and skeletal muscle, respectively, in these patients. Diagnostic features of kwashiorkor include pitting edema of the feet and legs, skin ulceration, and epidermal sloughing. In contrast to marasmus, kwashiorkor occurs in the United States predominantly in patients with acute, highly metabolic illness, such as trauma and burns. Subcutaneous fat and muscle mass are often preserved, although careful inspection usually reveals more muscle wasting. The most common biochemical findings in kwashiorkor are reduced serum albumin level, lymphopenia, and anemia. Rapid refeeding with oral, enteral, or parenteral nutrition can result in acute decreases in serum phosphorus, potassium, and magnesium levels, resulting in cardiac arrhythmia and death. Primary malnutrition is caused by inadequate food supply, which is common in many countries in the developing world, but less common in the United States. Patients with gastrointestinal disease are most predisposed to secondary malnutrition because of reduced oral intake of food, intestinal obstruction, altered absorption, and digestion of nutrients. Malnutrition, which can be defined as unintentional weight loss of more than 10% of usual body weight over 3 months, may occur in hospital patients. Malnutrition has been associated with increased infections, impaired wound healing, increased postoperative complications, longer hospital stay, and higher mortality. Dietary energy and protein deficiencies usually occur together, although one form may predominate. Kwashiorkor is the term used when severe protein deficiency is the primary cause of malnutrition, and marasmus is the term used when severe energy or calorie deficiency is the primary cause of the malnutrition. Marasmic kwashiorkor is the term used to describe the combination of chronic energy and protein deficiency. The diagnosis of marasmus includes a clinical history of inadequate calorie intake, usually from a chronic illness, and physical findings of severe wasting of muscle and subcutaneous fat. Sibutramine is a monoamine reuptake inhibitor that inhibits the reuptake of norepinephrine, serotonin, and dopamine. It can cause increases in blood pressure and therefore should not be given to patients with uncontrollable hypertension. Of the various types of obesity surgery, the gastric bypass procedure, also known as the Roux-en-Y, is the most accepted. A small pouch is created in the cardia of the stomach, which drains into a segment of bypassed jejunum. In addition, gastric bypass surgery can cause dumping syndrome, and postoperative dietary changes may be necessary. In the last 30 years, the prevalence of obesity has more than doubled, from 13% to 27%. Persons with increased abdominal fat are at increased risk for diabetes, hypertension, hyperlipidemia, and ischemic heart disease (metabolic syndrome) compared with those with increased gluteal and femoral fat. In all persons, obesity is caused by the ingestion of more calories than are expended. The marked increase in obesity in the last 20 years cannot be attributed to genetic factors alone and are most likely caused by changes in the environment. Treatment of obesity centers on modifying behavior, including diet and physical activity. Diet modification should encourage patients to eat three meals daily, to avoid snacking between meals, to avoid energy-dense and high-fat foods, and to increase the intake of fruits and vegetables. Aerobic exercise has additional health benefits independent of weight loss itself. Patients receiving pharmacotherapy for obesity should also be involved in efforts to change their lifestyles, including developing the habits of healthy eating and adequate exercise. In patients with chronic pancreatitis, the cause of malnutrition is multifactorial, including fear of postprandial abdominal pain (sitophobia), steatorrhea, anorexia, and often coexistent alcoholism. Steatorrhea and azotorrhea (fecal protein loss) occur when lipase and trypsin secretion are reduced by 90%. Analgesics should be given at least 30 minutes before meals to prevent postprandial exacerbation of pain. Meta-analysis failed to show a beneficial effect of exogenous pancreatic enzyme replacement in relieving abdominal pain.
